
Submitted:
28 April 2024
Posted:
29 April 2024
You are already at the latest version
Abstract
Chronic kidney disease (CKD) is a progressive condition that affects more than 10% of the world's population. Monitoring urine albumin and creatinine ratio (µACR) has become the gold standard for nephropathy diagnosis and control. The objective of the present study was to develop a simple, accurate, sensitive, and rapid point-of-care test (PoCT) device - MYμALBUMIN that community healthcare professionals can use in resource-limited facilities and by patients in their own homes for screening the risk and monitoring the progress of CKD. Albumin and creatinine concentrations in urine samples were determined using spectrophotometric dye (tetrabromophenol blue)-binding and colorimetric Jaffe’assay, respectively. Urine samples were diluted with distilled water (1:80) and mixed separately with albumin and creatinine reaction mixture. The creatinine reaction was incubated at room temperature (25oC) for 30 minutes before analysis. Optical density (OD) was measured at the wavelengths of 625 nm (albumin) and 515 nm (creatinine). All calibration curves (2-60 mg/L and 0.25-2 mg/dL for albumin and creatinine) yielded linear relationships with correlation coefficients (r2) of > 0.999. Good accuracy (%DMV < + 2.88%) and precision (%CV < 3.0%) were observed from both the intra- or interday assays for the determination of albumin and creatinine by MYµALBUMIN. The limit of quantification (LOQ) of albumin and creatinine in urine samples determined by MYµALBUMIN and laboratory spectrophotometer were 2 mg/L and 0.1 mg/dL, respectively, using 37.5 μL urine samples. The device was well applied with clinical samples from 13 CKD patients. The median (range) of %DMV of the central (hospital) laboratory method (immune-based assay) was 3.18 (-10.11 to 14.12)%, with a high correlation coefficient (r2 >0.99). In conclusion, MYμALBUMIN showed satisfactory test performance in terms of accuracy, reproducibility, sensitivity, and specificity. The device would have significant economic benefits besides obviously improving clinical decision-making processes.
Keywords:
Albumin
; Albumin-Creatinine ratio
; Creatinine
; Microalbumin
; Point-of-Care medical device
1. Introduction
Nephropathy is one of the global health problems, with an increasing prevalence worldwide in recent years [1]. The leading causes of nephropathy are generally diabetes and hypertension, which can lead to kidney damage, chronic kidney disease (CKD), kidney failure, and even death [2]. CKD is defined as either kidney damage or a glomerular filtration rate (GFR) < 60 mL/min per 1.73 m2 for three months or more, irrespective of cause, and stages of CKD severity are classified based on GFR [3]. In its early stages, CKD shows very few signs or symptoms. As the disease progresses, patients may experience nausea, vomiting, fatigue, sleep problems, shortness of breath, lower back pain, and swelling of the feet and ankles. In severe cases, CKD may also result in vascular disease, cognitive dysfunction, anemia, osteoporosis, and fractures [4]. Early detection of nephropathy, especially in patients with diabetes and hypertension is urgently required to prevent the progression of kidney damage.
Kidney function disorders and kidney disease are commonly diagnosed through 24-hour urine tests, where urine is collected over 24 hours to obtain a more reliable evaluation of the body’s condition [5]. Creatinine and microalbuminuria detection are standard and widely used laboratory tests for kidney disorders. However, such tests are not only inconvenient from the patient’s perspective but may also carry the risk of low adherence to instructions. Random urine albumin-to-creatinine ratio (uACR) is highly correlated with 24-hour urine albumin, which is of great significance for accurate and practical early detection and ongoing monitoring of the progression of CKD [6,7,8,9,10]. Nephropathy occurs when the uACR is >30 mg/g creatinine or microalbuminuria is present (urinary albumin 30–300 mg/24 hours) [11]. Without early detection and treatment, microalbuminuria may progress to irreversible macroalbuminuria (>300 mg/24 hours) [12], which increases the risk of CKD progression and cardiovascular events. This emphasizes the need to develop highly sensitive point-of-care testing (PoCT) devices for rapid microalbuminuria tests to facilitate early CKD detection, monitoring, and management.
The objective of the present study was to develop a simple, accurate, sensitive, and rapid PoCT device - MYμALBUMIN that can be used by community healthcare professionals in resource-limited facilities and by patients in their own homes, for screening the risk and monitoring the progress of CKD. The clinical applicability of the device was validated in comparison with the gold standard test used in the central laboratory (immune-based assay) in urine samples obtained from CKD patients.
2. Materials and Methods
2.1. Chemicals and Reagents
Creatinine, tetrabromophenol blue (TBPB), picric acid (PA), and human serum albumin (HSA) were obtained from Sigma-Aldrich (Missouri, USA). Sodium sulfate anhydrous was purchased from QReC, New Zealand. Trisodium citrate dehydrate, calcium chloride, ammonium chloride, magnesium sulfate heptahydrate, and disodium oxalate were obtained from Loba Chemie (Mumbai, India). Urea was purchased from Bio-Rad Laboratories (California, USA). Potassium chloride and sodium chloride were obtained from Ajax Finechem (Wollongong, Australia). Sodium phosphate monobasic monohydrate and sodium phosphate dibasic heptahydrate were purchased from Carlo Erba (Emmendingen, Germany) and Merck (Darmstadt, Germany), respectively. Sodium bicarbonate was obtained from (Pennsylvania, USA).
A stock solution (20 mg/mL) of HSA and creatinine was prepared with deionized water and stored at 4 °C. The working solutions were obtained by diluting the stock solution with water before use.
2.2. Instrumentation and Measurement Platform
MYµALBUMIN was developed as a colorimetric-based spectroscopic PoCT device to determine µACR utilizing a dual optical sensor. The test platform of the MYµALBUMIN device is shown in Figure 1, and the schematic diagram of the system operation is shown in Figure 2. The MCU (microcontroller unit) sends a signal to the constant current source circuit to transmit UV light at 625 nm and 515 nm to pass through the cuvette and photodiode amplifier circuit. The detector receives Vout-1 and Vout-2 signals, converts them to ADC (analog-to-digital converter), and filters out only the desired frequency signals. The noise from outside ambient light is removed and used to calculate the absorbance value according to the equation:
T = I/Io
A = log10 (1/T) or A = 2 − log10 (%T)
Where T = transmittance, I = transmitted light, Io = incident light, A = absorbance.
The absorbance value at 625 nm is used to calculate albumin concentration according to the equation:
Albumin = [(A-intercept)/slope] ∗ Dilution factor
Where A is an absorbance at 626 nm and slope, and intercept are from the linear calibration.
The absorbance value at 515 nm is used to calculate creatinine concentration according to the equation:
Creatinine = [(A-intercept)/slope] ∗ Dilution factor
Where A is an absorbance at 515 nm and slope and intercept are from the linear calibration.
The albumin-creatinine ratio (uACR) is calculated according to the equation:
uACR = (Albumin ∗ 100)/Creatinine
Results are displayed and interpreted as follows: i) normal urinary albumin if uACR < 30 mg/g creatinine, ii) microalbuminuria if uACR = 30-300 mg/g creatinine, and iii) macroalbuminuria if uACR >3,000 mg/g creatinine [14,15].
Figure 1.
(a) MYµALBUMIN device and (b) measurement platform.
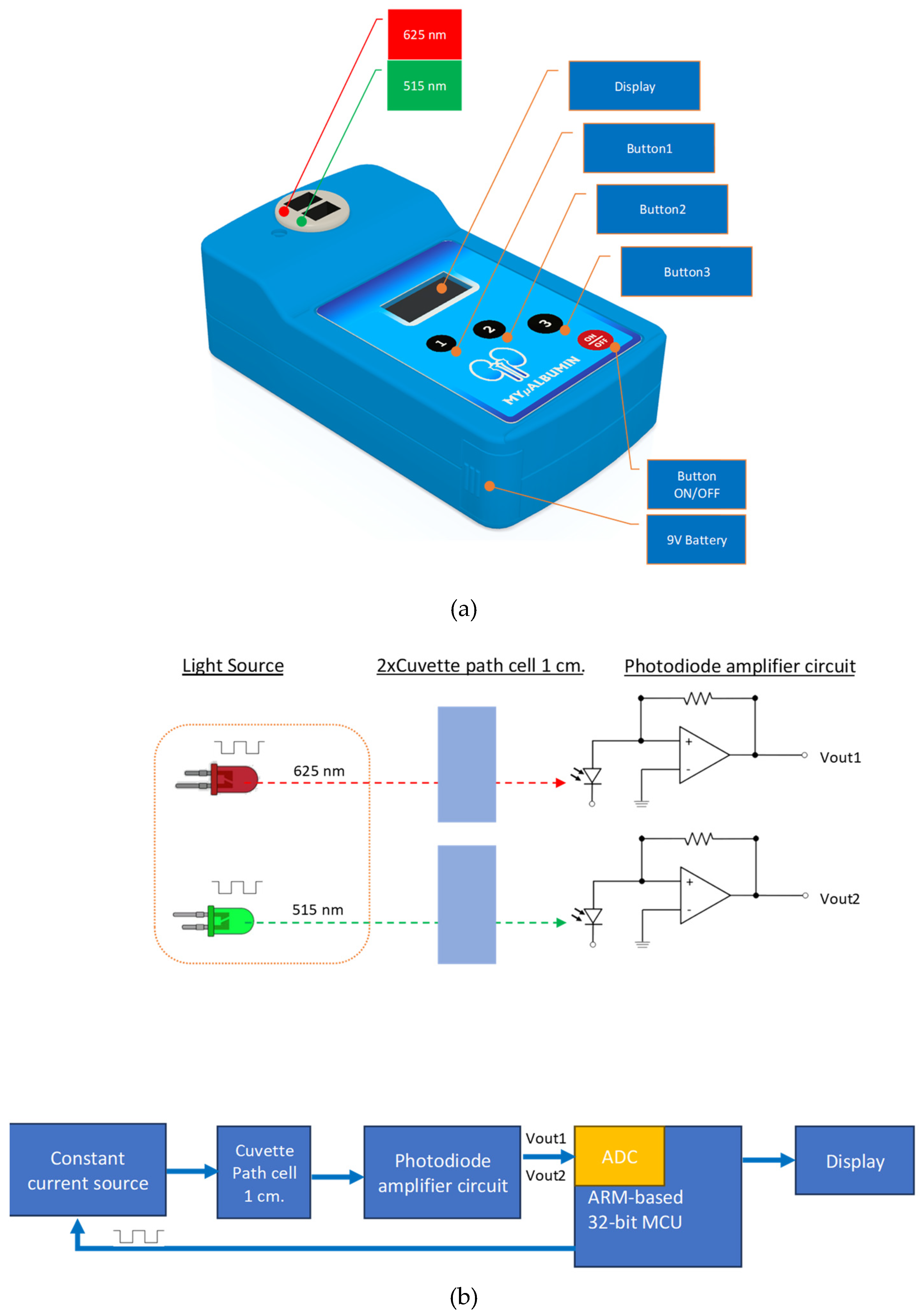
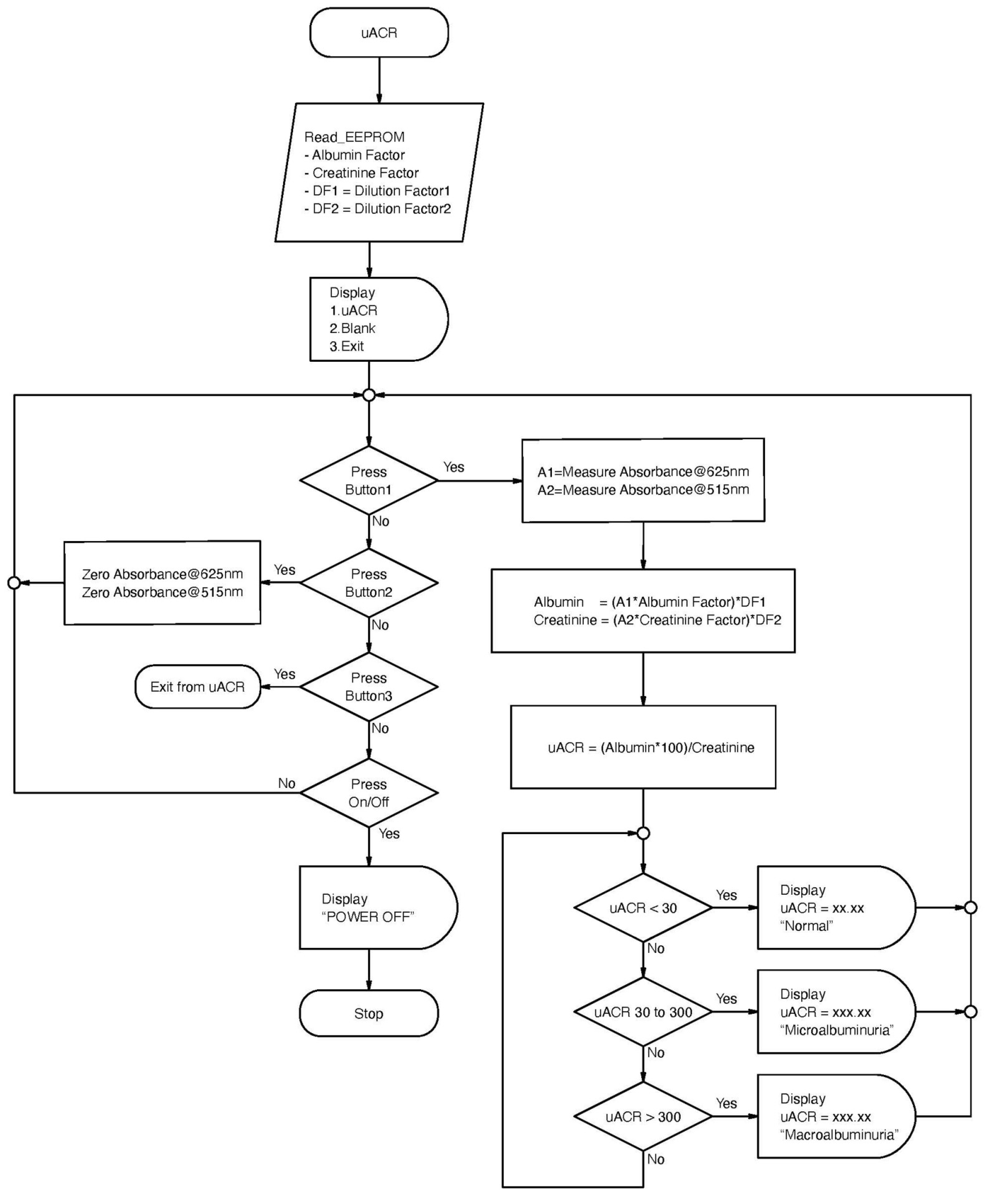
Figure 2.
Schematic diagram showing the operational workflow of MYµALBUMIN.
2.3. Colorimetric Detection of Albumin and Creatinine
Albumin concentrations in urine samples (artificial and clinical samples) were determined using a spectrophotometric dye-binding assay. The dye used in the reaction was tetrabromophenol blue (TBPB) [16].
Albumin + tetrabromophenol blue in acetate buffer (pH 3.2) → ALB-TBPB Complex
Concentrations of creatinine (artificial and clinical samples) were determined using the colorimetric Jaffé reaction in alkaline conditions [17].
Creatinine + Picric Acid + NaOH → CRE-Picrate Complex
The reaction mixture of creatinine was incubated at room temperature (25 °C) for 30 minutes, and uACR was determined using MYµALBUMIN.
2.4. MYµALBUMIN Detector Linearity
UV-visible absorbance of standard solutions of albumin (3 concentrations: 10, 40, and 60 mg/L) and creatinine (3 concentrations: 0.25, 1, and 2 mg/dL) following the reactions described above were recorded using MYµALBUMIN at the absorbance of 625 nm and 515 nm, respectively. The measured values of both albumin and creatinine at all concentrations were within acceptable limits, i.e., ≤ ±10% deviation from the values measured using a laboratory spectrophotometer (PERSEE T6U UV/VIS Spectrometer, California, USA).
2.5. Measurement of Albumin and Creatinine in Urine Samples
For albumin reaction, 2 mL of the mixture of tetrabromophenol (TBPB, 5 × 10−5 M) and 1% Triton X-100 in 0.05 M acetate buffer (pH 3.2) was thoroughly mixed with diluted urine (37.5 μL) sample in distilled water (1:80) [16]. For the creatinine reaction, the alkaline picrate reaction mixture of picric acid (1 mL) and sodium hydroxide (1 mL) was thoroughly mixed with a diluted urine sample in distilled water (1:80) and incubated at room temperature for 30 minutes before analysis [17]. The optical density (OD) of the mixture of urine sample (3 mL each) for determination of albumin and creatinine concentrations were measured against respective blank solutions in sample holders No. 1 (absorbance at 625 nm) and 2 (absorbance at 515 nm), respectively. The color intensity was corrected into Δintensity (absolute value) by subtracting the blank intensity and adjusting with the dilution factor (1:80).
2.6. Validation of Test Performance of MYµALBUMIN
2.6.1. Calibration Curves
For analysis of albumin in artificial urine samples, calibration curves were prepared by replicate analysis of seven samples (37.5 μL each) spiked with varying concentrations of albumin (0, 2, 5, 10, 20, 40, and 60 mg/L. Samples were analyzed as described above.
To analyse creatinine in artificial urine samples, calibration curves were prepared by replicate analysis of six samples (37.5 μL each) spiked with varying concentrations of creatinine (0, 2.5, 5, 10, 15, and 20 mg/dL). Samples were analyzed as described above.
2.6.2. Accuracy
The accuracy of MYµALBUMIN for determination of albumin in artificial urine samples was determined by replicate analysis of five sets of samples spiked with three different concentrations of albumin (10, 40, and 60 mg/L).
The accuracy of MYµALBUMIN for the determination of creatinine in artificial urine samples was determined by replicate analysis of five sets of samples spiked with three different concentrations of albumin (0.25, 1, and 2 mg/dL).
The accuracy of the assay method was reported as the percentage deviation of the mean value (%DMV) from the theoretical value (laboratory spectrophotometer):
Accuracy (%) = [(mean − nominal)/nominal] × 100
2.6.3. Precision
The precision of MYµALBUMIN for determination of albumin in artificial urine samples based on within-day (repeatability) and day-to-day (reproducibility) variation was determined by replicate analysis of five sets of samples spiked with three different concentrations of albumin (10, 20, and 60 mg/L).
The precision of MYµALBUMIN for the determination of creatinine in artificial urine samples based on within-day and day-to-day variation was determined by replicate analysis of five sets of samples spiked with three different concentrations of creatinine (0.25, 1, and 2 mg/dL).
The coefficient of variation (CV) was calculated from the ratio of standard deviation to the mean and expressed as a percentage:
% CV = standard deviation/ mean × 100
2.6.4. Limit of Quantification
The limit of quantification (LOQ) of MYµALBUMIN for determination of albumin and creatinine in artificial urine samples was determined from the lowest concentration of albumin or creatinine (in spiked urine samples) that produced CV ≤ ±25% of spiked concentrations.
2.7. Application of MYµALBUMIN to Clinical Samples
The study was approved by the Ethics Committee, Faculty of Medicine, Thammasat University (Project number MTU-EC-OO-2-1-168/66, approval number 266/2566). The study was conducted at Thammasat Chalermprakiet Hospital and the Thammasat University Center of Excellence in Pharmacology and Molecular Biology of Malaria and Cholangiocarcinoma, following the guidelines outlined in the Declaration of Helsinki. Written informed consent was obtained from all subjects before study participation.
Random urine samples (2-3 mL) were collected from 13 CKD patients. All samples were stored at −20 °C until analysis. Concentrations of albumin and creatinine in urine samples were measured as described above, and the uACR values of each sample were determined using the MYµALBUMIN device and compared with a laboratory spectrophotometer and central (hospital) laboratory method (immune-based assay). The immune-based assay (Dimension Clinical Chemistry System, SIEMENS, Germany) was performed by Bangkok Pathology Laboratory, Bangkok, Thailand. The microalbumin method is based on particle-enhanced turbidimetric inhibition immunoassay. The creatinine method measures creatinine enzymatically.
2.8. Statistical Analysis
Statistical analysis was performed using SPSS 17.0 software. Quantitative variables are summarized as median (range) values. Deviation from the mean of the uACR values measured using MYµALBUMIN and those measured using the standard spectrophotometer were calculated and are expressed as %DMV (% deviation from mean value). The correlation between the uACR values measured using both equipment was determined using Spearman’s correlation test at a statistical significance level of α = 0.05.
3. Results
3.1. Validation of Test Performance of MYµALBUMIN Device
3.1.1. Calibration Curves
3.1.2. Accuracy
Good accuracy was observed from both the intra- or interday assays for determination of albumin and creatinine by MYµALBUMIN, as indicated by the minimal deviation of mean values found with measured samples from that of the theoretical values (actual amount added), with %MDV of lower than ±2.88 % at all investigated concentrations (Table 2a-b).
3.1.3. Precision
Slight variation (intra- and inter-assay variation) of albumin and creatinine assays in urine samples was observed with CV below 3 % at all investigated concentrations (Table 3a-b).
3.1.4. Limit of Quantification
The LOQ of albumin and creatinine in urine samples determined by MYµALBUMIN and laboratory spectroscopy were 2 mg/L and 0.25 mg/dL, respectively, using 37.5 µL urine samples.
3.2. Application to Clinical Samples
To evaluate the clinical applicability of MYµALBUMIN, the uACR values in urine samples of 13 CKD patients measured by MYµALBUMIN were compared with those measured by the laboratory spectrophotometer and central (hospital) laboratory (immune-based assay) methods. The median (range) of %DMV of the spectrophotometer and immune-based method were -2.15 (-14.18 to 11.65)% and 3.18 (-10.11 to 14.12)%, respectively. The correlation of the values measured between the two methods was high, with r2 of ≥0.99 (Figure 5a,b).
4. Discussion
Of all proteins, albumin, synthesized in the liver, is very important as an active substance in the human body. In healthy individuals, the albumin content in urine is typically less than 30 mg/g creatinine, and any value higher than this may indicate potential kidney disease [18]. Creatinine is the ultimate metabolite of nitrogen elements in the human body, primarily excreted from the blood by the kidneys, specifically through glomerular filtration. Low urinary excretion of creatinine reflects impairment of kidney function and corresponding renal diseases [19].
The use of the urine (random) albumin to creatinine ratio (uACR) is currently recommended as the preferred screening strategy for the risk and monitoring of the progress of CKD [20]. The standard method for uACR determination involves measuring albumin and creatinine separately using automated machines. The available analytical techniques used for detecting each substance are complex, time-consuming, and expensive and require modern and less portable instruments, high-cost analyses, large sample and reagent volumes, and the services of skilled medical technicians. Due to the low concentration of microalbuminuria in urine, it is difficult to measure the concentration level using a spectrophotometer and colorimetric methods [21] and more specific methods such as immunoturbidimetry [22,23], immunoassays [24,25], radioimmunoassay [26], and liquid chromatography have been applied [27]. In addition, several sensitive methods have been developed to determine microalbuminuria and/or uACR. These include paper-based analytical devices (PAD) [8,28,29,30,31,32], microfluidic sliding PAD [33], sequential injection analysis (SIA) [34,35], and mono-segmented sequential injection lab-at-valve (SI-LAV) system [36]. Although the performance of some tests is considered good, they are time-consuming and require complicated devices or external tools such as pumps and high voltage-machines, which are impractical for PoCT. Therefore, developing a simple device with a short analysis time is needed to be portable, cost-effective, and affordable for the PoCT of CKD.
Research articles on developing PoCT devices for uACR measurement have highlighted technological advances, biosensor-based approaches, microfluidic systems, smartphone-based technologies, clinical validation studies, and challenges in translation and implementation. Biosensors typically involve immobilizing specific antibodies or aptamers on a sensor surface to capture albumin, followed by detecting creatinine or albumin-creatinine complexes. Such biosensors offer the advantages of rapid analysis, minimal sample volume requirements, and potential for PoCT. However, they may be susceptible to interference from matrix components or substances in biological samples, leading to false-positive or false-negative results. Some biosensors may exhibit limited sensitivity, particularly when detecting low concentrations of albumin or creatinine in urine samples [37]. Microfluidic-based PoCT devices have gained attention for their ability to perform complex sample handling and analysis tasks on a miniaturized platform [8,9,28,31]. Microfluidics have been integrated with sensing elements for uACR measurement, enabling precise control of sample flow and reaction kinetics. These systems may, however, encounter challenges related to sample handling, such as sample evaporation, air bubble formation, and clogging of microchannels. Smartphone-based PoCT devices have emerged as promising platforms for decentralized testing [38,39,40]. These devices leverage smartphones’ computational power and connectivity to perform uACR analysis using built-in cameras, sensors, and dedicated mobile applications. The measurement modes include colorimetric assay, fluorescence detection, and paper-based microfluidics. Smartphone-based assays may face compatibility issues with different smartphone models or operating systems, limiting their universal applicability.
The PoCT devices commercially available for determining uACR are immune-based assays. These include the DCA Vantage Analyzer (Siemens, Germany), AfinionTM AS100 Analyzer (Abbotts, USA), NycoCardTM READER II (Abbotts Rapid Diagnostics, USA), and QuikRead goTM Instrument (Orion Diagnostica, Finland) [41]. While PoCT devices offer numerous advantages for uACR measurement, including rapid results, point-of-care testing, minimal sample volume, ease of use, and portability, they also present limitations related to cost, quality control, interference, regulatory compliance, and data management.
In this study, we developed MYμALBUMIN as a PoCT for screening the risk and monitoring the progress of CKD using µACR as a biomarker. The device is portable, user-friendly, accurate, reproducible, and cost-effective, with comparable performance to laboratory spectrophotometer. The analysis runtime is relatively short (reaction time = 30 minutes and analysis time < 1 minute). The test procedure is also simple, making the device suitable for use at patients’ homes and in community healthcare facilities with limited laboratory facilities. Unskilled users can operate MYμALBUMIN, and minimal to no auxiliary equipment is needed. The methods are based on colorimetric dye-forming reactions, in which the optical density of the color complex formed from each reaction is measured using visible UV at wavelengths of 515 nm (for creatinine) and 625 nm (for albumin). Moreover, the proposed system utilized the slimmer cuvettes (12.5 × 7.5 × 45 mm) than the conventional cuvettes (12.5 × 12.5 × 45 mm) in a spectrophotometer with the same pathlength (10 mm) to reduce the measuring solution volume. The device can simultaneously measure both compounds and provide uACR for each sample. The Jaffe reaction is the most commonly used method for creatinine determination, relying on the formation of an absorbing complex during the reaction of creatinine with picric acid. Several dyes have been used in the albumin reaction, including methyl orange, bromocresol green and bromocresol purple [42], bromophenol blue [43], tetrabromophenol blue [44], bromochlorophenol blue [45], Commassie Brillant Blue G [46], and eosin [47] dyes. Calibration curves for both compounds can be prepared only once when the device is first used, and the information is recorded in the device database. uACR can be measured in a single random urine sample without the requirement of batch analysis. The accuracy and reproducibility of both assay methods are within acceptable ranges (%DVM < +2.88%, %CV < 3.0%). Although the methods are based on spectroscopic assays, the sensitivity of albumin and creatinine analyses is in an acceptable range. It is adequate to detect microalbuminuria (LOQ) of 2 mg/L and 0.25 mg/dL for albumin and creatinine, respectively). Quality control (QC) samples (with three concentrations: low, medium, and high) should be integrated into the analysis at least once every two weeks. An acceptable deviation of uACR values from each QC sample is ±5%. New calibration curves are required to accurately analyse uACR in case of deviation outside this acceptable limit. The clinical applicability of MYμALBUMIN to determine uACR was well demonstrated in urine samples collected from 13 CKD patients. An excellent correlation (r2 > 0.994) was found between the values measured by the device compared with laboratory spectrophotometer and the gold standard method used in the central (hospital) laboratory (immune-based assay).
5. Conclusions
MYµALBUMIN, a simple platform based on colorimetric detection for the determination of uACR was developed for use as a PoCT for determining the risk and monitoring the progress of CKD. The device showed satisfactory accuracy, reproducibility, sensitivity, and specificity test performance. The device would have significant economic benefits besides obviously improving clinical decision-making processes. Validation of the clinical application of the device in a large sample size, including healthy subjects, CDK patients, and different groups of patients at risk of CKD (particularly those with diabetes and hypertension), is underway.
6. Patents
The innovation patent ‘MYμALBUMIN’ is approved by the Department of Intellectual Property of Thailand (No. 2302005386).
Author Contributions
Conceptualization, all authors; methodology, N.M., K.N., T.P., N.Y. and W.C.; software, W.M.; validation, N.M., K.N. and N.Y.; formal analysis, N.M. and K.N.; investigation, N.M., N.Y. and W.C.; writing—original draft preparation, N.M. and K.N.; writing—review and editing, N.M. and K.N.; funding acquisition, W.C. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by Chulabhorn International College of Medicine, Thammasat University, and the National Research Council of Thailand under the Research Team Promotion grant.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Thammasat University (protocol number 122 and date of approval 2 February 2024) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article.
Acknowledgments
The authors would like to thank Dr. Arthitaya Tiengsusuk and Mrs. Rehab Osman Taha for their assistance in technical support and sample collection.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Neuen, B.L.; Chadban, S.J.; Demaio, A.R.; Johnson, D.W.; Perkovic, V. Chronic kidney disease and the global NCDs agenda. BMJ Glob Health 2017, 2, e000380. [Google Scholar] [CrossRef] [PubMed]
- Hypertension and chronic kidney diseases. Cor et Vasa 2013, 55, e397–402. [CrossRef]
- Feher, M. Diabetes: Chronic Complications. Edited by Kenneth M Shaw and Michael H Cummings. 2nd Edition © John Wiley & Sons Ltd., 2005 ISBN: 0470865792 Paperback, 270 pages. Pract Diabetes 2005, 22, 327–327. [Google Scholar] [CrossRef]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C.W. Chronic kidney disease: global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Chen, T.K.; Knicely, D.H.; Grams, M.E. Chronic Kidney Disease Diagnosis and Management: A Review. Jama 2019, 322, 1294–1304. [Google Scholar] [CrossRef]
- Sumida, K.; Nadkarni, G.N.; Grams, M.E.; Sang, Y.; Ballew, S.H.; Coresh, J.; Matsushita, K.; Surapaneni, A.; Brunskill, N.; Chadban, S.J.; et al. Conversion of Urine Protein-Creatinine Ratio or Urine Dipstick Protein to Urine Albumin-Creatinine Ratio for Use in Chronic Kidney Disease Screening and Prognosis: An Individual Participant-Based Meta-analysis. Ann Intern Med 2020, 173, 426–435. [Google Scholar] [CrossRef]
- Ying, T.; Clayton, P.; Naresh, C.; Chadban, S. Predictive value of spot versus 24-hour measures of proteinuria for death, end-stage kidney disease or chronic kidney disease progression. BMC Nephrol 2018, 19, 55. [Google Scholar] [CrossRef]
- Chaiyo, S.; Kalcher, K.; Apilux, A.; Chailapakul, O. A Novel Paper-based Colorimetry Device for the Determination of the Albumin to Creatinine Ratio. Analyst 2018, 143. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Hsu, J.-L.; Tseng, C.-C.; Lee, G.-B. An integrated microfluidic system for the determination of microalbuminuria by measuring the albumin-to-creatinine ratio. MicrofluidNanofluidics 2011, 10, 1055–1067. [Google Scholar] [CrossRef]
- Weaver, R.G.; James, M.T.; Ravani, P.; Weaver, C.G.W.; Lamb, E.J.; Tonelli, M.; Manns, B.J.; Quinn, R.R.; Jun, M.; Hemmelgarn, B.R. Estimating Urine Albumin-to-Creatinine Ratio from Protein-to-Creatinine Ratio: Development of Equations using Same-Day Measurements. J Am Soc Nephrol 2020, 31, 591–601. [Google Scholar] [CrossRef]
- Mogensen, C.E. Microalbuminuria predicts clinical proteinuria and early mortality in maturity-onset diabetes. N Engl J Med 1984, 310, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Ansar, M.M.; ShahrokhiRad, R.; Lebady, M.K. Risk Factors of Microalbuminuria and Macroalbuminuria in Type 2 Diabetic Patients in North of Iran - Rasht. Nephro-Urol Mon 2017, 9, e40031. [Google Scholar] [CrossRef]
- Chutipongtanate, S.; Thongboonkerd, V. Systematic comparisons of artificial urine formulas for in vitro cellular study. Anal Biochem 2010, 402, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Keane, W.F.; Eknoyan, G. Proteinuria, albuminuria, risk, assessment, detection, elimination (PARADE): a position paper of the National Kidney Foundation. Am J Kidney Dis 1999, 33, 1004–1010. [Google Scholar] [CrossRef]
- American Diabetes Association Clinical Practice Recommendations 2001. Diabetes Care 2001, 24 (Suppl. 1), S1–S133.
- Ratanawimarnwong, N.; Ponhong, K.; Teshima, N.; Nacapricha, D.; Grudpan, K.; Sakai, T.; Motomizu, S. Simultaneous injection effective mixing flow analysis of urinary albumin using dye-binding reaction. Talanta 2012, 96, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Sittiwong, J.; Unob, F. Detection of urinary creatinine using gold nanoparticles after solid phase extraction. Spectrochim Acta A Mol Biomol Spectrosc 2015, 138, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.C.; Ryu, S.; Lee, J.Y.; Lee, S.H.; Cheong, E.; Hyun, Y.Y.; Lee, K.B.; Kim, H.; Byrne, C.D. Urine Albumin/Creatinine Ratio Below 30 mg/g is a Predictor of Incident Hypertension and Cardiovascular Mortality. Journal of the American Heart Association 2016, 5, e003245. [Google Scholar] [CrossRef] [PubMed]
- Myers, G.L.; Miller, W.G.; Coresh, J.; Fleming, J.; Greenberg, N.; Greene, T.; Hostetter, T.; Levey, A.S.; Panteghini, M.; Welch, M.; et al. Recommendations for improving serum creatinine measurement: a report from the Laboratory Working Group of the National Kidney Disease Education Program. Clin Chem 2006, 52, 5–18. [Google Scholar] [CrossRef]
- Tziakas, D.; Chalikias, G.; Kareli, D.; Tsigalou, C.; Risgits, A.; Kikas, P.; Makrygiannis, D.; Chatzikyriakou, S.; Kampouromiti, G.; Symeonidis, D.; et al. Spot urine albumin to creatinine ratio outperforms novel acute kidney injury biomarkers in patients with acute myocardial infarction. Int J Cardiol 2015, 197, 48–55. [Google Scholar] [CrossRef]
- Schosinsky, K.H.; Vargas, M.; Luz Esquivel, A.; Chavarria, M.A. Simple spectrophotometric determination of urinary albumin by dye-binding with use of bromphenol blue. Clin Chem 1987, 33, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Teppo, A.M. Immunoturbidimetry of albumin and immunoglobulin G in urine. Clin Chem 1982, 28, 1359–1361. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, V.R.; Khese, V.B.; Jadhav, S.L.; Kakrani, A.L. Urinary Albumin Excretion, Estimated Glomerular Filtration Rate, and Prevalence of Microalbuminuria in Obese Nondiabetic and Nonhypertensive Adults: A Cross-Sectional Study. Indian J Nephrol 2019, 29, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhang, R.; Chen, H.; Weng, W.; Lin, Q.; Deng, D.; Li, Z.; Kong, J. Sensitive polydopamine bi-functionalized SERS immunoassay for microalbuminuria detection. Biosens Bioelectron 2019, 142, 111542. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, M.O.; Zhu, P.Y.; Wang, C.C.; Du, Y.C.; Chuang, C.H. Electrochemical immunosensor utilizing electrodeposited Au nanocrystals and dielectrophoretically trapped PS/Ag/ab-HSA nanoprobes for detection of microalbuminuria at point of care. Biosens Bioelectron 2019, 126, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Floyd, M.; Cannon, D.C.; Kahan, B. Radioimmunoassay for urinary albumin. Clin Chem 1978, 24, 1464–1467. [Google Scholar] [CrossRef] [PubMed]
- Comper, W.D.; Jerums, G.; Osicka, T.M. Differences in urinary albumin detected by four immunoassays and high-performance liquid chromatography. Clinical Biochemistry 2004, 37, 105–111. [Google Scholar] [CrossRef]
- Hiraoka, R.; Kuwahara, K.; Wen, Y.C.; Yen, T.H.; Hiruta, Y.; Cheng, C.M.; Citterio, D. Paper-Based Device for Naked Eye Urinary Albumin/Creatinine Ratio Evaluation. ACS Sens 2020, 5, 1110–1118. [Google Scholar] [CrossRef]
- Chagas, C.L.S.; de Souza, F.R.; Cardoso, T.M.G.; Moreira, R.C.; da Silva, J.A.F.; de Jesus, D.P.; Coltro, W.K.T. A fully disposable paper-based electrophoresis microchip with integrated pencil-drawn electrodes for contactless conductivity detection. Anal Methods 2016, 8, 6682–6686. [Google Scholar] [CrossRef]
- Heist, C.A.; Bandara, G.C.; Bemis, D.J.; Pommerenck, J.C.; Remcho, V.T. New paper-based microfluidic tools for the analysis of blood serum protein and creatinine built via aerosolized deposition of polycaprolactone. Anal Methods 2018, 10, 2994–3000. [Google Scholar] [CrossRef]
- Cai, Y.; Niu, J.-C.; Liu, Y.-Q.; Du, X.-L.; Wu, Z.-Y. Online sample clean-up and enrichment of proteins from salty media with dynamic double gradients on a paper fluidic channel. Analytica Chimica Acta 2020, 1100, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Nurrahmah, N.; Amalia, K.T.; Sulistyarti, H.; Sabarudin, A. Fast colorimetric detection of albumin-to-creatinine ratio using paper-based analytical devices with alkaline picrate and Bromothymol Blue reagents. 2021, 12, 140–148. [Google Scholar] [CrossRef]
- Chen, S.J.; Tseng, C.C.; Huang, K.H.; Chang, Y.C.; Fu, L.M. Microfluidic Sliding Paper-Based Device for Point-of-Care Determination of Albumin-to-Creatine Ratio in Human Urine. Biosensors 2022, 12, 496. [Google Scholar] [CrossRef] [PubMed]
- Siangproh, W.; Teshima, N.; Sakai, T.; Katoh, S.; Chailapakul, O. Alternative method for measurement of albumin/creatinine ratio using spectrophotometric sequential injection analysis. Talanta 2009, 79, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Sabarudin, A. Sequential Injection at Valve Mixing (SI-VM) for Determination of Albumin-Creatinine Ratio in Urine. Orient J Chem 2018, 34, 730–734. [Google Scholar] [CrossRef]
- Kiwfo, K.; Wongwilai, W.; Sakai, T.; Teshima, N.; Grudpan, K. Determination of Albumin, Glucose, and Creatinine Employing a Single Sequential Injection Lab-at-Valve with Mono-Segmented Flow System Enabling In-Line Dilution, In-Line Single-Standard Calibration, and In-Line Standard Addition. Molecules 2020, 25, 1666. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.C.; Ko, C.H.; Lu, S.Y.; Yang, C.E.; Fu, L.M.; Li, C.Y. Rapid electrochemical-biosensor microchip platform for determination of microalbuminuria in CKD patients. Anal Chim Acta 2021, 1146, 70–76. [Google Scholar] [CrossRef]
- Thakur, R.; Maheshwari, P.; Datta, S.K.; Dubey, S.K.; Shakher, C. Machine Learning-Based Rapid Diagnostic-Test Reader for Albuminuria Using Smartphone. IEEE Sens J 2021, 21, 14011–14026. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, G.; Zong, X.; Sun, J. Performance evaluation of Hipee S2 point-of-care testing urine dipstick analyser: a cross-sectional study. BMJ Open 2022, 12, e063781. [Google Scholar] [CrossRef]
- Jia, Y.; Liu, G.; Xu, G.; Li, X.; Shi, Z.; Cheng, C.; Xu, D.; Lu, Y.; Liu, Q. Battery-free and wireless tag for in situ sensing of urinary albumin/creatinine ratio (ACR) for the assessment of albuminuria. Sens Actuators B Chem 2022, 367, 132050. [Google Scholar] [CrossRef]
- Luppa, P.B.; Müller, C.; Schlichtiger, A.; Schlebusch, H. Point-of-care testing (POCT): Current techniques and future perspectives. Trends Analyt Chem 2011, 30, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y. Reaction between pH indicators with a large pKa value and human serum albumin and its application to the determination of the serum albumin concentration. Bunseki Kagaku 2003, 52, 939–944. [Google Scholar] [CrossRef]
- Jung, K.; Nickel, E.; Pergande, M. A microalbuminuria assay using bromphenol blue. Clinica Chimica Acta 1990, 187, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Pugia, M.J.; Lott, J.A.; Profitt, J.A.; Cast, T.K. High-sensitivity dye binding assay for albumin in urine. J Clin Lab Anal 1999, 13, 180–187. [Google Scholar] [CrossRef]
- Yoshimoto, K.; Kaneko, E.; Yotsuyanagi, T. Analytical Chemistry for Environmental and Human Health. Visual determination of protein in urine using Bromochlorophenol Blue and a membrane filter. Bunseki Kagaku 2000, 49, 363–367. [Google Scholar] [CrossRef]
- Marshall, T.; Williams, K.M. Interference in the Coomassie Brilliant Blue and Pyrogallol Red protein dye-binding assays is increased by the addition of sodium dodecyl sulfate to the dye reagents. Anal Biochem 2004, 331, 255–259. [Google Scholar] [CrossRef]
- Waheed, A.A.; Rao, K.S.; Gupta, P.D. Mechanism of dye binding in the protein assay using eosin dyes. Anal Biochem 2000, 287, 73–79. [Google Scholar] [CrossRef]
Figure 3.
Calibration curves of albumin at the concentration range of 0-60 mg/dL determined by (a) MYµALBUMIN and (b) laboratory spectrophotometer.
Figure 3.
Calibration curves of albumin at the concentration range of 0-60 mg/dL determined by (a) MYµALBUMIN and (b) laboratory spectrophotometer.
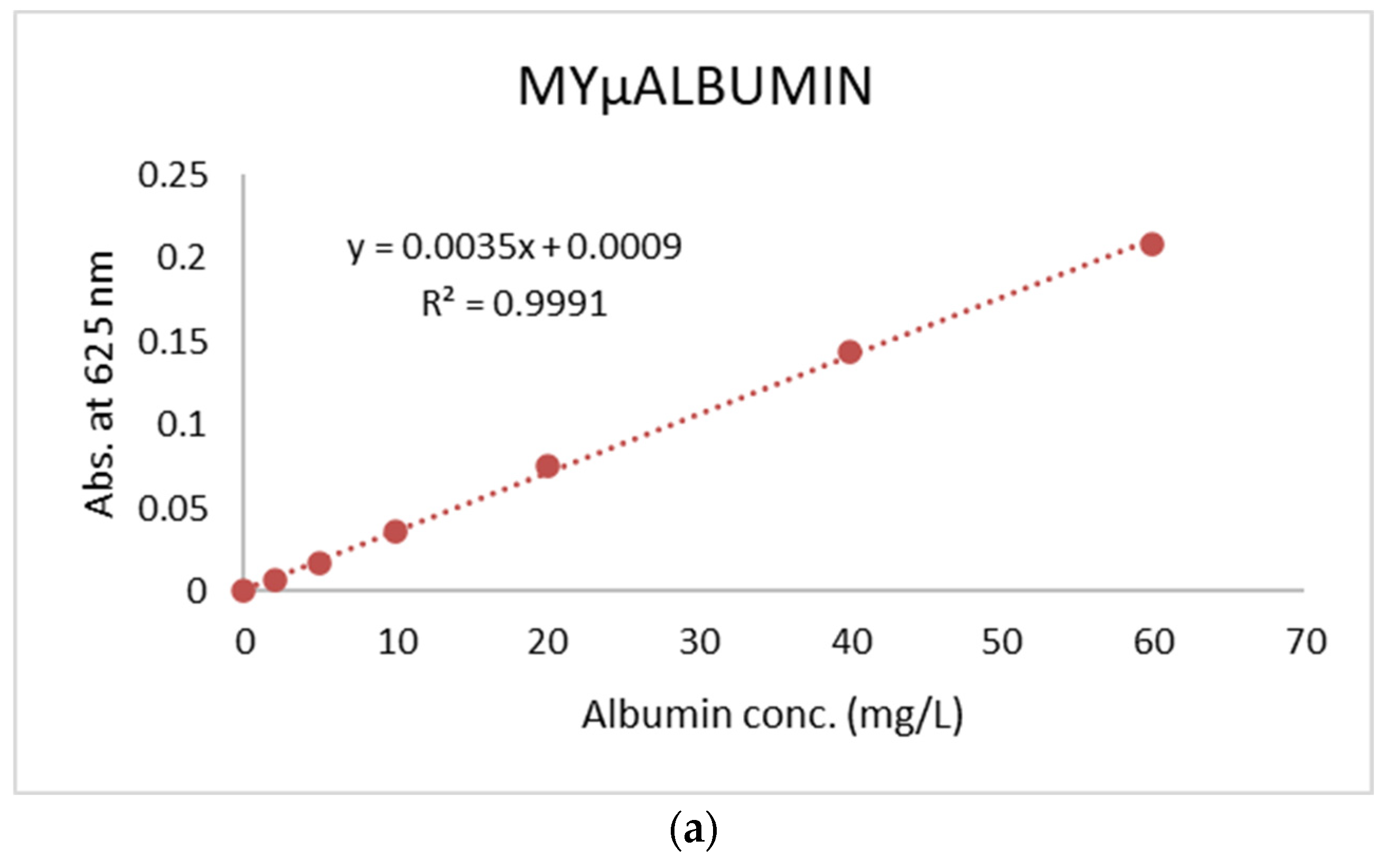
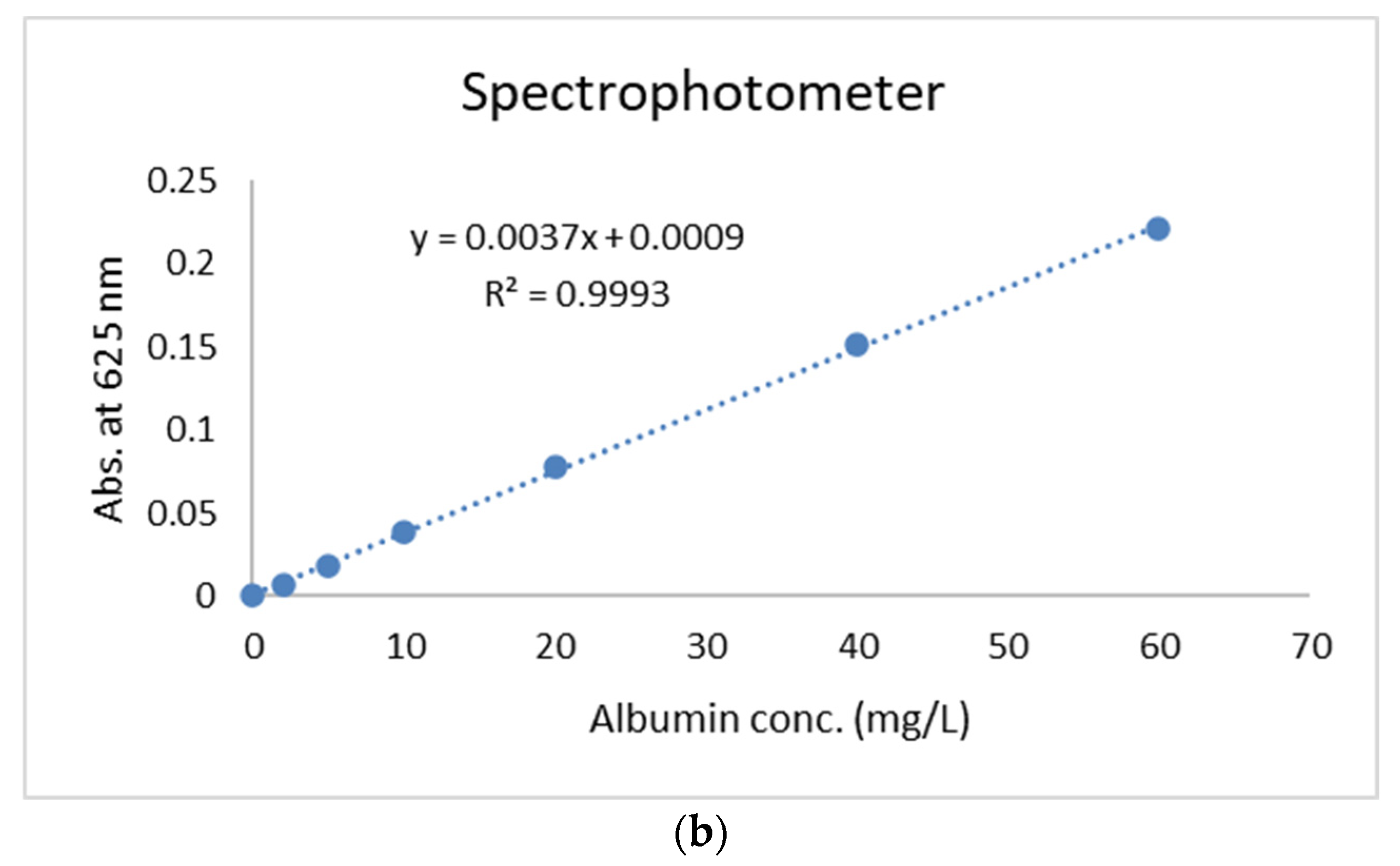
Figure 4.
Calibration curves of creatinine at the concentration range of 0-2 mg/dL determined by (a) MYµALBUMIN and (b) laboratory spectrophotometer.
Figure 4.
Calibration curves of creatinine at the concentration range of 0-2 mg/dL determined by (a) MYµALBUMIN and (b) laboratory spectrophotometer.
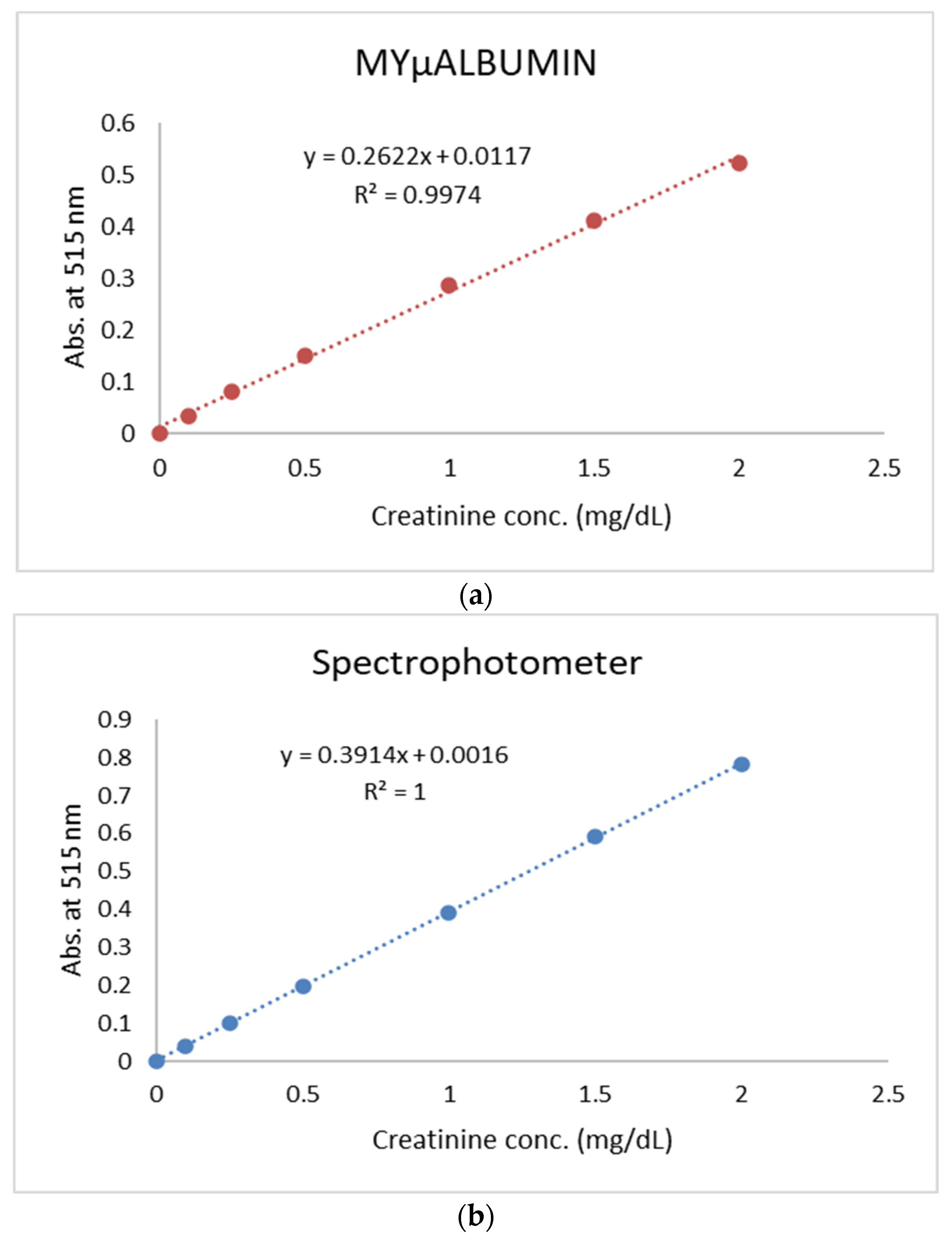
Figure 5.
Correlation between µACR measured by (a) MYµALBUMIN vs. laboratory spectrophotometer and (b) MYµALBUMIN vs immune-based assay (gold standard).
Figure 5.
Correlation between µACR measured by (a) MYµALBUMIN vs. laboratory spectrophotometer and (b) MYµALBUMIN vs immune-based assay (gold standard).
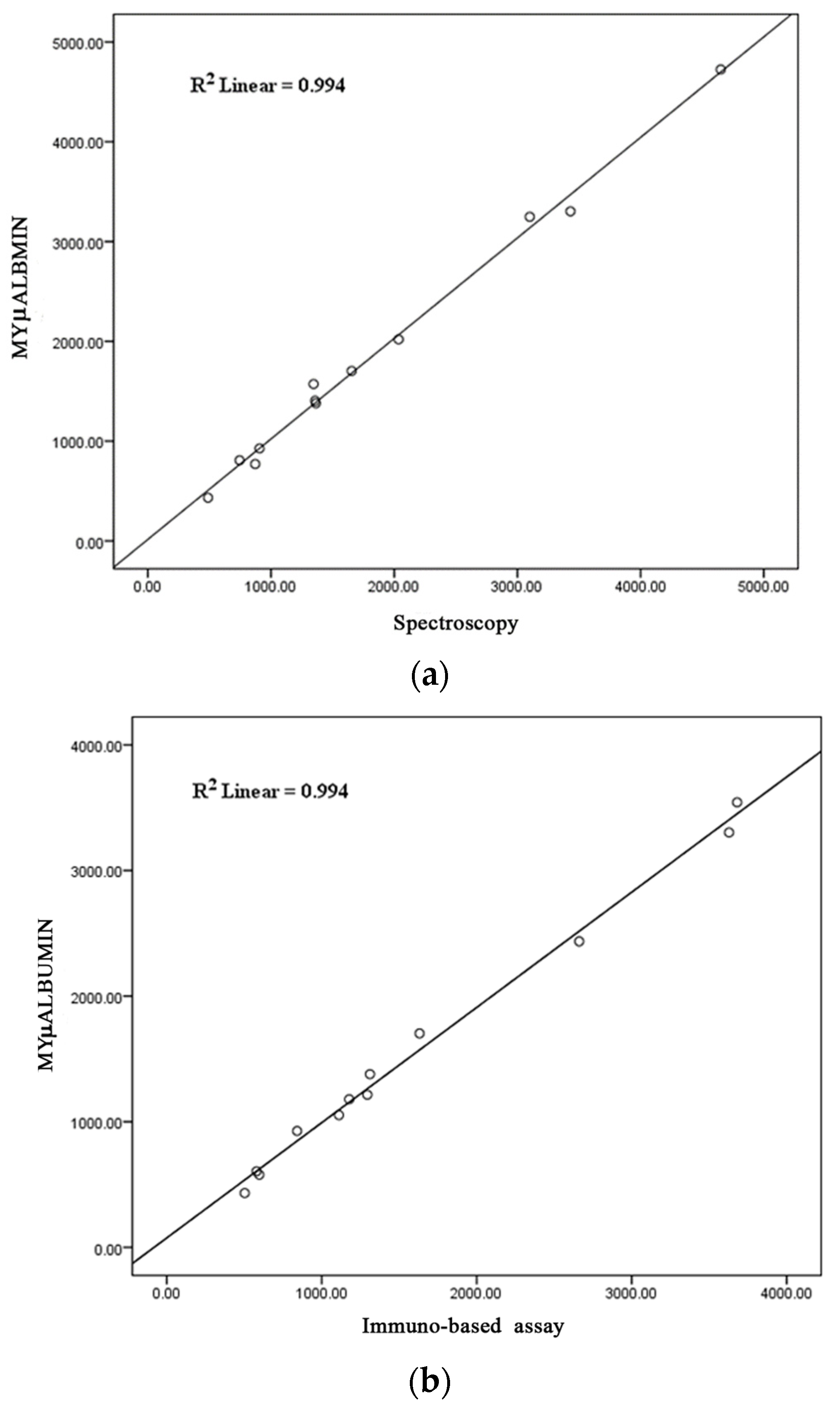

Table 1.
Composition of artificial urine used to evaluate the test performance of MYµALBUMIN [13].
Table 1.
Composition of artificial urine used to evaluate the test performance of MYµALBUMIN [13].
| Composition | Molecular formula | Molecular weight (g/mol) | Final concentration (mM) |
|---|---|---|---|
| Sodium sulfate anhydrous | Na2SO4 | 142.04 | 9 |
| Trisodium citrate dehydrate | Na3C6H5O7·2H2O | 294.1 | 5 |
| Urea | CH4N2O | 60.06 | 200 |
| Potassuium chloride | KCl | 74.55 | 30 |
| Sodium chloride | NaCl | 58.44 | 54 |
| Calcium chloride | CaCl2 | 110.99 | 3 |
| Ammonium chloride | NH4Cl | 53.49 | 15 |
| Magnesium sulfate heptahydrate | MgSO4·7H2O | 246.47 | 2 |
| Sodium phosphate monobasic monohydrate | NaH2PO4·H2O | 137.99 | 3.6 |
| Sodium phosphate dibasic heptahydrate | Na2HPO4·7H2O | 268.03 | 0.4 |
| Sodium bicarbonate | NaHCO₃ | 84.01 | 2 |
| Disodium oxalate | Na2C2O4 | 134 | 0.1 |
Table 2.
Intra- and inter-assay precision and accuracy of albumin assay determined by MYµALBUMIN compared with laboratory spectrophotometer.
Table 2.
Intra- and inter-assay precision and accuracy of albumin assay determined by MYµALBUMIN compared with laboratory spectrophotometer.
| Albumin concentration added (mg/L) | Precision (%CV) | Accuracy (%DVM) | ||
|---|---|---|---|---|
| Intraday | Interday | Intraday | Interday | |
| MYµALBUMIN | ||||
| 10 | 2.52 | 4.58 | 1.43 | 4.29 |
| 40 | 1.34 | 3.02 | 2.36 | 1.07 |
| 60 | 1.44 | 2.75 | -0.90 | -1.57 |
| Spectrophotometer | ||||
| 10 | 2.86 | 3.77 | 3.51 | 6.22 |
| 40 | 0.30 | 1.00 | 1.96 | 2.50 |
| 60 | 1.42 | 0.87 | -0.95 | -0.95 |
Table 3.
Intra- and inter-assay precision and accuracy of creatinine assay by MYµALBUMIN compared with laboratory spectrophotometer.
Table 3.
Intra- and inter-assay precision and accuracy of creatinine assay by MYµALBUMIN compared with laboratory spectrophotometer.
| Creatinine concentration added (mg/L) | Precision (%CV) | Accuracy (%DVM) | ||
|---|---|---|---|---|
| Intraday | Interday | Intraday | Interday | |
| MYµALBUMIN | ||||
| 0.25 | 1.21 | 12.69 | 5.42 | -2.82 |
| 1 | 1.08 | 4.54 | 4.77 | 1.03 |
| 2 | 1.35 | 3.53 | -2.57 | -4.14 |
| Spectrophotometer | ||||
| 0.25 | 1.99 | 2.35 | 2.61 | 3.83 |
| 1 | 1.25 | 2.32 | -0.15 | 1.43 |
| 2 | 1.42 | 2.40 | -0.20 | 1.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



