
Submitted:
27 April 2024
Posted:
29 April 2024
You are already at the latest version
Abstract
Calcium sulphate (CS) is currently used as a bioabsorbable, completely synthetic and sterile material in the management of infected tissues and dead spaces (DS) mainly resulting from surgical procedures. Residual DS in the postoperative, may create an environment where hematomas fill up and bacteria can proliferate, leading to a high incidence of postoperative infections. Considering the available reviews in the literature, CS has been mainly studied in orthopedic surgery mostly giving brilliant results and low complication rates. Nowadays, orthopedists avail it in the form of pearls both as a bone void filler and as an “off-label” delivery agent for antibiotics in arthroplasty, chronic osteomyelitis and open fractures, paving the way of its application in many other contexts given its natural dis-position to biodegradation. In the last years, CS beads have been gaining ground in the general, vascular and endocrinological surgical specialties. Despite its clear potential and the increasing number of scientific evidences on the safety and effectiveness of CS application in the prophylaxis and treatment of infections, there are not many studies reporting on its application in fields other than orthopedics, with a substantial paucity in plastic and reconstructive surgery literature. This is some-how surprising, since reconstructive surgery often deals with complex wounds secondary to bone and soft tissue exposure, suture dehiscence, trauma, and surgical site infections.
As far as we know this is the first updated systematic review assessing the state of the art, indications and new perspectives on the application of CS beads in plastic and reconstructive surgery.
Keywords:
Calcium sulfate
; Calcium sulphate
; Calcium sulfate beads
; Calcium sulphate beads
; Stimulan
; Stimulan beads
; Antibiotic beads
; Calcium sulphate beads and Plastic Surgery
Introduction
Calcium sulphate (CS) is a bioabsorbable, high-purity, versatile, completely synthetic and sterile material. It largely owes its reputation in the orthopaedic field as a bone filler, and more recently it is gaining renown as a tool in the management of dead spaces and infected tissues when mixed with lyophilised antibiotics. [3] First reported in 1892 by Dreesmann et al. who described a blend of calcium sulphate and phenol as a filler in the treatment of eight patients with bone voids [6], it took over half a century later for its safety to be proven. As a matter of fact, in 1961 Leonard Peltier et al. were the first to conclude that implanting calcium sulphate into bone or soft tissue did not cause a foreign body reaction. Moreover, he demonstrated that CS promoted new bone formation when periosteum or bone was present, finally proving the biodegradable nature of the materials. [6] In fact, no substrate remains “in vivo” thus avoiding potential bacterial colonization or biofilm formation. Therefore, no additional procedures are required for removal since the inserted material completely dissolves over the course of 3 to 6 weeks in soft tissue, or 6 to 12 weeks into the bone. [7]
Calcium sulphate powder can be mixed with freeze-dried antibiotics to make beads of varying diameters (3 to 6 mm), depending on the size of the dead space as a result of the surgical procedure. Drug combinations most frequently involve the use of gentamicin, tobramycin and vancomycin according to the underlying infection. [5] Once the mixture is obtained, it is modelled on the beads mat during the operating session and then directly inserted into tissues in the form of pearls.
There are multiple studies in the literature reporting on the safety and advantages of using CS, and it recently gained a role in the modern orthopedic practice as an alternative to Polymethylmethacrylate (PMMA), that has been shown to reduce infection rates when filled with antibiotics in the form of spacers or pellets as well, in the presence of infection, non-union or bone loss. [1,8]
However, PMMA is non-absorbable and requires re-intervention to remove it, thus, it acts as a potential foreign body for bacterial colonization. For this reason, the necessity of finding an absorbable cement paved the way for the use of calcium sulphate, receiving increasing acceptance for its exploitation. In this regard, in 2014, McConoughey et al. compared PMMA and calcium sulphate as carriers for the local delivery of antibiotics to infected surgical sites, being the first to demonstrate the safety of calcium sulphate beads and their comparable results to the PMMA beads in inhibition of bacterial growth [9].
As this practice has increased, so has the understanding of the associated benefits and potential complications. The most frequent side effects include transient hypercalcemia, wound drainage and hetero-topic ossification (HO) [10,11]. Particularly, there has been a rising occurrence of seroma when higher volumes of CS beads are used, especially in subcutaneous structures and in patients with comorbidities such as diabetes and long- term steroid use, with rates of 4% to 51% of cases [12,13].
Despite the increasing number of reports and scientific evidence on the safety and effectiveness of CS beads application in the prophylaxis and treatment of infections, there are not many studies on its application in fields other than orthopedics [2].
Currently, the medical branches in which the use of calcium sulphate beads is gaining ground are mainly general, vascular and endocrinological surgery, but there is still a paucity of data evaluating its role in plastic and reconstructive surgery [14,15].
Optimal results are pursued by leveraging the evolution and application of innovative devices and biomaterials as well as when the full set of multidisciplinary skills is available. In this regard, as plastic surgeons we are often called upon to deal with complex wounds secondary to bone and soft tissue exposure, suture dehiscence, trauma, and surgical site infections [16]. Standard practice includes debridement of infected or dead tissue, while the coverage is achieved with vascularized muscle or fascio-cutaneous flaps whenever vital structures are exposed [17,18,19]. Although several interesting protocols have been proposed to handle these events, often treatment and eradication of a complex infection remains a challenge for patients as well as physicians [20]. In fact, the presence of critical structures or prostheses often precludes a complete removal of heavily colonized tissue and adequate bioburden reduction. In such cases, calcium sulphate absorbable antibiotic beads may be used with promising results just as in any other surgical field. As far as we know, this is the first updated systematic review to focus the attention on the role of CS beads in the field of Plastic and Reconstructive surgery.
Material and Methods
1. Eligibility Criteria
All studies concerning the use of CS beads or plates for the management of plastic surgery procedures were eligible for the analysis. Articles concerning the handling of a surgical site infection were included in the study despite this scenario being commonly experienced by several medical fields, but still frequent in plastic and reconstructive surgery. The other reviews analyzing the use of CS for the management of procedures belonging to other specialist fields were not considered eligible. To facilitate the eligibility of data, the PRISMA guidelines were adhered to throughout this study. [13] Eventually, only articles written in English and in-vivo studies were included.
2. Research Strategy
Collections of case studies and scientific reviews were searched using the following Medical Subject Headings (MeSH) keywords: “Calcium sulfate”, “Calcium sulphate”, “calcium sulfate beads”, “calcium sulphate beads”, “Stimulan”, “Stimulan beads”, “Antibiotic beads”, “calcium sulphate beads and Plastic Surgery”. The terms were searched in various combinations in order to collect as many items as possible that might be eligible for the study. The websites where the research was carried out were PubMed, Cochrane Library, Medicine plus, OpenAIRE and Medscape. Each abstract from the search results was reviewed by two authors (AM and MM) for relevant papers. All references cited in relevant articles were also checked for other studies not found during the initial search. In duplicate cases only one review was considered.
3. Data Selection
The following variables were collected from the selected scientific literature, both open-access and subscription-based articles: author, year of publication, study setting, journal, nationality, level of impact, bead characteristics, outcomes measured (infection eradication, healing, healing time, revision surgery, wound leakage, other complications), body district, minimum follow-up, age, sex, underlying pathology, microorganisms detected, antibiotic regimen used.
Results
The PRISMA diagram illustrates the search strategy and research selection process applied for this study (Figure 1). A review of the entire database yielded 721 titles. Based on these titles, 656 were deemed suitable for abstract review once the 65 duplicate studies were removed. These 656 abstracts were reviewed by two authors considering the inherent nature of plastic and reconstructive surgery, sorting out 91 records from all the databases selected by this study. After applying the exclusion criteria (3.1 Eligibility criteria) and using the NIH study Quality Assessment Tool for case series [21] to assess paper quality, 8 reviews were deemed eligible for inclusion (Table 1).
Summary of Studies
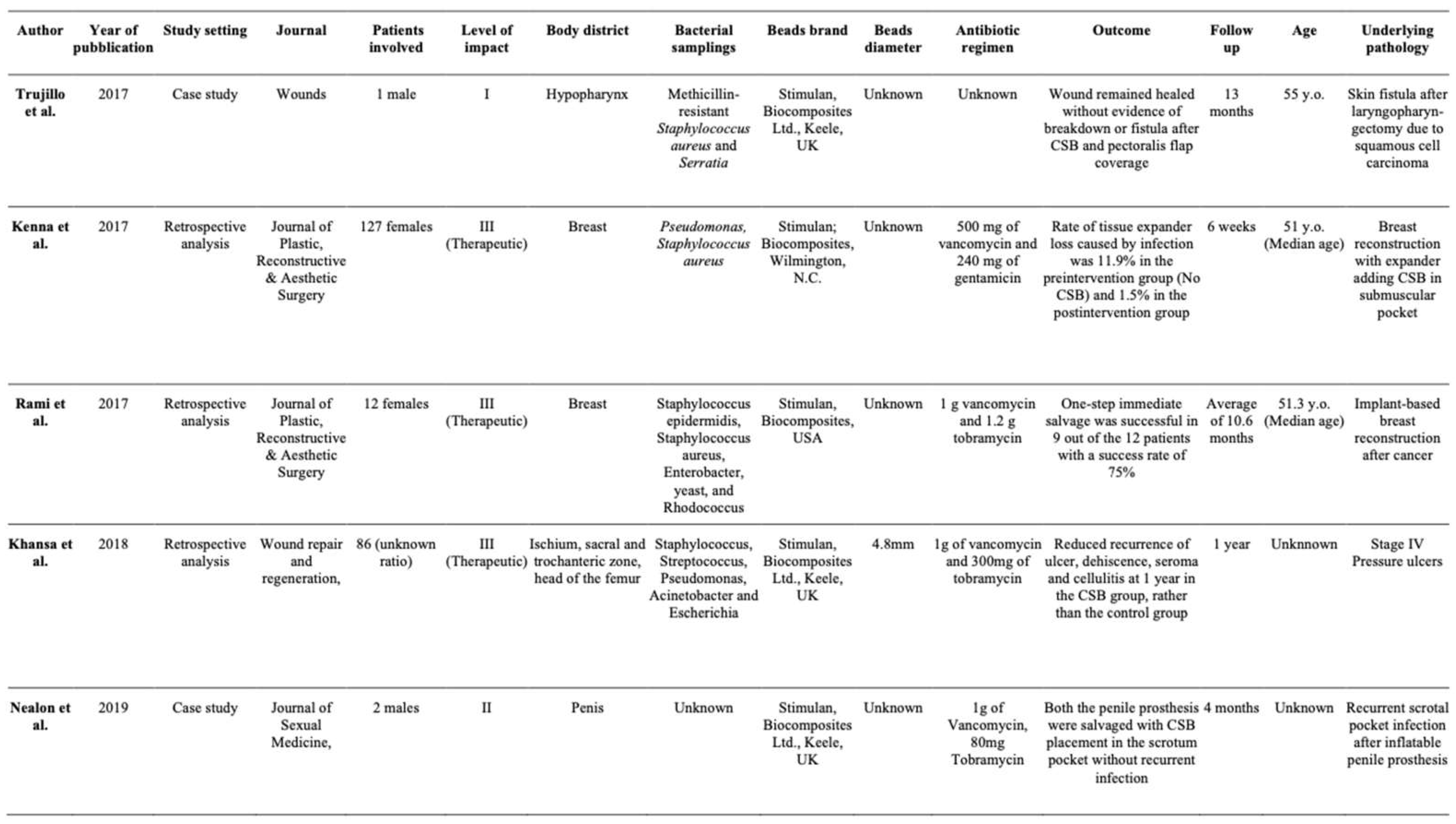
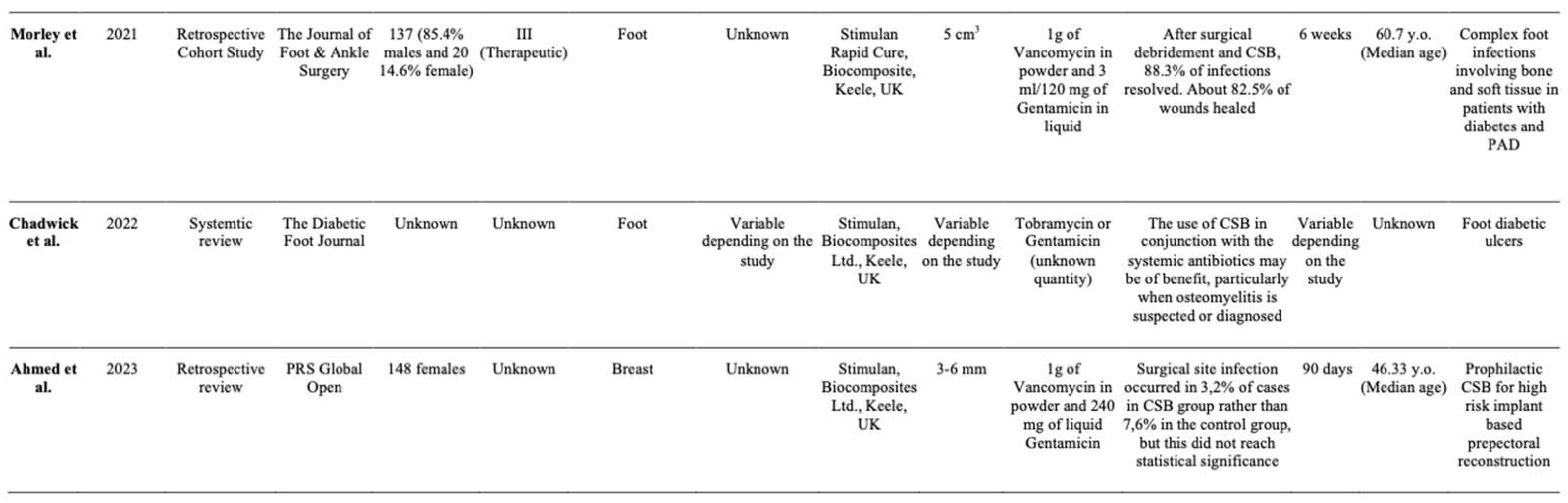
8 articles [22,23,24,25,26,27,28,29] met the inclusion criteria (Table 2). The 8 studies were published between 2017 and 2023. These studies included a total amount of 513 patients excluding the group involved in one systematic review. [28] All patients had a primary or a revision surgery followed by the implantation of CS beads in the surgical wounds. The mean follow-up varied from 6 weeks up to 13 months. With regard to the body districts considered, the following were involved: the hypopharynx, breasts, penis, foot, and the ischium, sacral, trochanteric and head of the femur zones. The male: female ratio has been reported in 5 papers. The most commonly used antibiotic mixes were vancomycin – tobramycin and vancomycin – gentamicin. Only three studies reported the size of the involved CS beads: Khansa [25], 4.8 mm of diameter; Morley [27], 5 cm3 of volume and Ahmed [29], 3-6 mm of diameter. 4 of 7 reviews were considered impact level III, or therapeutic level. A wide spectrum of bacteria was found in the several samplings carried out in the studies, the most common were Staphylococcus aureus, Streptococcus, Pseudomonas, Acinetobacter, Pseudomonas and Escherichia coli. Using the United States National Institute of Health (NIH) Quality Assessment Tool for case series studies [21], 5 studies (Kenna [23], Rami [24], Khansa [25], Morley [27] and Chadwick [28] were rated as a “Good” quality and 3 studies (Trujillo [22], Nealon [26] and Ahmed [29] at a “Fair” quality rating (Table 1). Trujillo [22] used CS beads in the management of a skin fistula after laryngopharyngectomy due to squamous cell carcinoma, Kenna [23] and Rami [24] both involved CS beads in breast reconstruction for the first time, the former with an expander, the latter with a prosthesis. Recently, Ahmed [29] proposed calcium sulphate beads as prophylactic practice in high risk – implant based prepectoral breast reconstruction. Khansa [25] involved calcium sulphate beads in the treatment of stage IV pressure ulcers and Nealon [26] used it in two cases of recurrent scrotal pocket infection after inflatable penile prosthesis implant. Lastly, Morley [27] and Chadwick [28] treated it in the context of complex foot wound management in patients with diabetes and/or peripheral arterial diseases.
Discussion
According to this review, the considered authors have reported promising results with the use of CS beads in multiple conditions related to the discipline of plastic and reconstructive surgery. Trujillo et al. [22] concluded that the addition of antibiotic-loaded CS beads in a prophylaxis regimen seems to improve the outcomes of soft tissue surgical site infections in the management of complex wounds, with a 10,56% re-operation rate. In their study, each patient received CS beads during orthopedic, breast, thoracic, and vascular graft surgeries depending on their respective categories. Although the average age, gender, comorbidities, and characteristics of the beads used were not mentioned, of a total of 142 patients treated at two different hospital facilities with the same prophylaxis protocol, only 15 needed re-intervention at 30 days after CS implantation, demonstrating how local antibiotic delivery can dramatically decrease the persistence rate of surgical site infections. As evidence of this, they reported a case study in which CS beads were used in a single male patient with a history of T2N1 (Stage IIb) squamous cell carcinoma of the hypopharynx undergoing chemoradiation therapy and laryngopharyngectomy. A persistent fistula occurred; therefore, coverage with a chest perforator flap was required to manage the progressive loss of substance. As the reconstruction went into partial necrosis, another operation with debridement, CS beads implant and a skin-covered pectoralis muscle flap was performed. At 13-months follow-up, the wound remained healed without evidence of breakdown or fistula.
The objective of promoting further protocols involving CS beads in the management of complex surgical wounds was shared by Morley et al. [27] (2021) and Chadwick et al. [28] (2022). Their purpose was to investigate whether surgical debridement and implantation of antibiotic loaded calcium sulphate was effective in the resolution of foot infection and wound healing. Morley et al. [27] in a double-center cohort study retrospectively reviewed the use of calcium sulphate beads impregnated with gentamicin and vancomycin on the foot ulcers of 137 individuals with osteomyelitis (n=127) or significant soft tissue infection (n=10) following surgical debridement. [28] In 137 cases, 88.3% of infections were resolved, with 22 patients not-requiring postoperative systemic antibiotics. About 82.5% of wounds healed, with a mean healing time of 11.3 weeks. Recovery time was significantly prolonged in patients with diabetes and peripheral artery disease (p = < 0.05) and long-term postoperative systemic antibiotics were required. The only adverse effect observed was that the resolution of CS beads caused skin maceration in some cases to varying degrees which may have affected healing times. However, Khansa et al. [25] found that overall complication rates between patients packed with CS and those that were not, appeared similar (43.8% vs 51.9%, p = .54) in 120 stage IV pressure ulcers involving various districts of the lower limbs.
Although these rates are almost comparable, the benefits of using calcium sulphate beads in sacral, trochanteric, ischium, and femoral head ulcers were significant. They drastically reduced the wound re-occurrence rate at 1 year after excision, CS beads application and flap coverage. In the CS group, the rates were 12.5%, compared to 39.4% in the non-CS group. The rates of dehiscence were 18.8% versus 10.6%, seroma 12.5% versus 0%, and cellulitis 0% versus 1.9%. Through the use of a scanning electron microscope (SEM), they suggested that surgical procedure alone, even if performed widely and demolishingly, may not eliminate biofilm. A biofilm is a community of bacteria enclosed in a self- produced polymeric matrix and adherent to a surface. [30] Infections associated with biofilms are highly resistant to traditional antimicrobial therapy, as the matrix protects the bacteria from antibiotics and the host defenses. [30] Moreover, it was observed that conventional bacterial culture techniques are inadequate to diagnose bacterial biofilm infection, since 6 patients had SEM evidence of biofilm infection but only 1 of those 6 patients had positive wound cultures. In the light of this evidence, they concluded that antibiotic beads in conjunction with debridement may have utility in the eradication and healing of ulcered wounds. [25]
Chadwick et al. [28] similarly supported the use of loaded calcium sulphate beads for treating infected foot ulcers in diabetic individuals. Their aim was to offer physicians a clear clinical pathway for safely and effectively using loaded CS beads in treatment. Their shrewd guideline consists of 4 steps: First, assess the suitability for calcium sulphate beads, paying particular attention to the vascular status of the lower limbs and wound assessment. Next, prescribe and apply CS beads, possibly after conducting surgical debridement. Finally, monitor the application of calcium sulphate beads based on wound progression and infection status.
Furthermore, they proposed a recommendation to prevent the increase in exudate, representing the main side-effect of using CS beads reported in literature. In 2021, Patel et al. [31] suggested reducing the number of beads applied to the wound, whereas Chadwick et al. [28] assessed that it is generally not recommended due to the increased risk of beads detaching from the injury bed. The risk of maceration in the wound perimeter should not preclude the use of CS beads given the several products available to prevent this and effectively manage exudate, i.e., a non-adhesive silicone transparent dressing.
The use of CS beads has been described in the urological-reconstructive field for the first time by Nealon et al. [26], presenting two cases in which the use of antibiotic beads in the scrotum allowed prosthesis salvage. In one case, an inflatable penile prosthesis (IPP) was explanted and replaced with a semi-rigid penile prosthesis (SRPP) and calcium sulphate beads were inserted to prevent recurrence of infection. In the second case, a patient with complications who had previously undergone SRPP due to infection had recurrent scrotal infections and recovered with beads placement in the scrotal pocket. Although the brief review lacks statistical data, beads featuring description and personal comorbidities history references of the two patients involved, they reported that both patients prevailed post operatively without recurrent infection.
Rami et al. [24], Kenna et al. [23] and Ahmed et al. [29] analyzed the effectiveness of antibiotic loaded CS beads in breast surgery, respectively involving CS beads in breast reconstruction with only implants [24], tissue expanders [23], and both [29].
Postoperative infection is a significant concern with this procedure. It can range from mild complications that need only a short course of antibiotics to more severe infections leading to the loss of the expander. Rami et al. [24] were the first to present a single-center case series demonstrating the use of CS beads infused with vancomycin and tobramycin.
Patients with breast implant infections underwent a treatment process that included the removal of the prostheses, debridement, partial capsulectomy, implantation of CS beads, and immediate implant replacement. This approach aimed to maximize the salvage rate of the infected prostheses and minimize the use of intravenous antibiotics, which could increase morbidity. This study demonstrated that the one-step immediate salvage was successful in 9 out of the twelve patients, with an attainment rate of 75%, higher than most other conservative attempts at implant salvage. Moreover, it is declared that the remaining 25% of unsaved implants is represented by exceptionally complicated situations: a lost follow-up, a failure due to insufficient soft tissue coverage secondary to radiation treatment, and the occurrence of an atypical infection with antibiotic-resistant Rhodococcus. In this view, Rami et al. [24] suggested how a not-specific target drug regimen could represent a limitation in the treatment of bacterial infections, thus, the future use of the CS beads in multiple plastic and reconstructive surgery scenario (such as orthoplastic, oncoplastic, post-traumatic reconstructions, microsurgery, breast reconstruction, complicated wound healing surgical management etc…) could benefit from tailoring the drug therapy on the specific antibiogram evidence.
Promising comparable outcomes have been evidenced by Kenna et al. [23] In a retrospective study, they demonstrated how adding calcium sulphate pearls loaded with vancomycin and gentamicin in the submuscular pocket during tissue expander breast reconstruction could reduce the risk of periprosthetic implant infection necessitating implant removal. Out of 127 breast reconstructions with TE covered by an acellular dermal matrix, 68 adhered to such an “off-label” prophylactic protocol, while the remaining 59 only washed with chlorhexidine several days before surgery and received intravenous antibiotics in the post-surgery time.
The rate of TE loss due to infection was 1.5% in the cluster using CS beads (p=0.02) and 11.9% in the cluster not using it, considering as an “infection” at least one of the following criteria: purulent drainage, spontaneous dehiscence of the surgical incision with positive bacterial swabs, evidence of abscess, or diagnosis by the surgeon of a deep infection occurring up to 1 year postoperatively. [32,33]
The demonstrated efficacy in reducing the rate of implant removal is due to the ability of CS beads to attack biofilm, which is involved in resistant infections [34] and capsular contracture [35,36] and has recently been studied in relation to implant associated anaplastic large cell lymphoma [37]. In this regard, Howlin RP et al. [38] published a study finding that high concentrations of an antibiotic released from calcium sulphate significantly reduced biofilm formation over several days.
More recently, Ahmed et al. [29] proposed calcium sulphate beads as prophylactic practice in high risk – implant based prepectoral breast reconstruction in a retrospective review. Indeed, several strategies are employed to tackle the challenge of breast implant infection. These include antibiotic irrigation and the “no-touch” technique in implant positioning, especially in high-risk patients. [39,40] In this study antibiotic loaded calcium sulphate beads were placed behind the implant over the pectoralis major muscle and anterior to the prosthetic between the subcutaneous adipose layer and the implant itself. Surgical site infection or implant-loss in high-risk patients receiving prophylactic antibiotic loaded calcium sulfate beads during implant-based pre-pectoral reconstruction occurred in 3,2% compared with the 7,6% in the control group. However, this did not reach enough statistical significance.
Conclusion
To our knowledge, this systematic review represents the first comprehensive analysis documenting the utilization of antibiotic-loaded calcium sulphate beads in managing all cases reported in the literature within the field of plastic and reconstructive surgery. Further trials and long term data are needed to fully determine the impact of these beads in such different and variable setting and target of patients. However, their effectiveness and safety are supported by the above-mentioned scientific evidence and antibiotic impregnated calcium sulphate beads could significantly reduce patient morbidity and improve outcomes also in well-thought-out clinical complex cases usually managed by plastic and reconstructive surgeons. Furthermore, additional research is needed to verify whether this method of administration can improve the healing rate of complex wounds and prevent infection in a prophylactic regimen, potentially reducing the need for systemic antibiotics in terms of dosage and duration of treatment.
Informed Consent Statement
Not applicable.
Conflicts of interest
The authors declare that they have no conflict of interest.
Financial Disclosure Statement
This research received no external funding.
Ethical approval
Not required.
Illustrations attached
1 video (0:48 min).
Caption of the video attached
50-year-old female patient with history of neurological bladder disease undergoing bladder stimulator electrode insertion surgery, after which a local infection that expanded to the soft tissues of her left hip was developed. Despite massive antibiotic therapy based on antibiogram performed on local subcutaneous discharge, the infection did not resolve so a surgical toilet of the affected site was required. The beneficial effect of the lavage was implemented with site insertion of calcium sulphate beads loaded with daptomycin (indicated as effective by antibiogram) during the same operative session, allowing local delivery of antibiotic that assisted in the progressive resolution of the infection.
References
- R. Kallala, W. Edwin Harris, M. Ibrahim, M. Dipane, E. McPherson. Use of Stimulan absorbable calcium sulphate beads in revision lower limb arthroplasty: Safety profile and complication rates. Bone Joint Res 2018 and 10.1302/2046-3758.710., 7:570–579. DO.
- Jogia RM, Modha DE, Nisal K, et al. Use of highly purified synthetic calcium sulfate impregnated with antibiotics for the management of diabetic foot ulcers complicated by osteomyielitis. Diabetes Care 2015 and 38(5):79e80.
- Fillingham Y, Jacobs J. Bone grafts and their substitutes. Bone Joint J. 2016 and 98B(1_Supple_A):6–9.
- Piovan, G., Farinelli, L., Screpis, D. et al. The role of antibiotic calcium sulfate beads in acute periprosthetic knee infection: a retrospective cohort study. Arthroplasty 4, 42 (2022).
- Sheridan GA, Falk DP, Fragomen AT, Rozbruch SR. Calcium sulfate in the management of osteomyelitis: A systematic review and meta-analysis of comparative studies. Medicine 2022 and 101:45(e31364).
- McKee MD, Li-Bland EA, Wild LM, Schemitsch EH. A prospective, randomized clinical trial comparing an antibiotic-impregnated bioabsorbable bone substitute with standard antibiotic-impregnated cement beads in the treatment of chronic osteomyelitis and in.
- Peltier LF. The use of plaster of paris to fill large defects in bone. Am J and 97:311-315.
- McPherson E, Dipane M, Sherif S. Dissolvable Antibiotic Beads in Treatment of Peripros-thetic Joint Infection and Revision Arthroplasty - The Use of Synthetic Pure Calcium Sulfate (Stimulan®) Impregnated with Vancomycin & Tobramycin. Reconstr Rev 2013.
- McConoughey, Stephen J., Howlin RP, Wiseman J, Stoodley P, Calhoun JH. Comparing PMMA and calcium sulfate as carriers for the local delivery of antibiotics to infected surgical sites. J Biomed Mater Res B App Biometer. 2015 May;103 (4):870-7.
- Kallala R, Haddad FS. Hypercalcaemia following the use of antibiotic-eluting absorbable calcium sulphate beads in revision arthroplasty for infection. Bone Joint J 2015 and 97-B:1237-1241.
- Kelly CM, Wilkins RM, Gitelis S, et al. The use of a surgical grade calcium sulfate as a bone graft substitute: results of a multicenter trial. Clin Orthop Relat Res. 2001:42–50.
- Ziran BH, Smith WR, Morgan SJ. Use of calcium-based demineralized bone matrix/allograft for nonunions and posttraumatic reconstruction of the appendicular skeleton: Preliminary results and complications. J Trauma. 2007 and 63:1324–8.
- Sheridan GA, Falk DP, Fragomen AT, Rozbruch SR. Calcium sulfate in the management of osteomyelitis: A systematic review and meta-analysis of comparative studies. Medicine 2022 and 101:45(e31364).
- Gallo G, Guaitoli E, Barra F, Picciariello A, Pasculli A, Coppola A, Pertile D, Meniconi RL and Itali, SPIGC Surgical Training Working Group. Restructuring surgical training after COVID-19 pandemic: A nationwide survey on the Italian scenario on behalf of the.
- Marcasciano M, Kaciulyte J, Mori FLR, Lo Torto F, Ribuffo D, Casella D. Plastic surgery in the time of Coronavirus in Italy. Maybe we should say: “Thanks Darwin we are Plastic Sur-geons!”. J Plast Reconstr Aesthet Surg. 2021 Jul and doi:, 74(7):1633-1701.
- Lo Torto F, Turriziani G, Donato C, Marcasciano M, Redi U, Greco M, Miraldi F, Ribuffo D. Deep sternal wound infection following cardiac surgery: A comparison of the monolateral with the bilateral pectoralis major flaps. Int Wound J. 2020 Jun and 17(3):683-69.
- Greco M, Vitagliano T, Fiorillo MA, Greto Ciriaco A. A new technique of upper eyelid blepharoplasty using the orbicularis muscle flap. Aesthetic Plast Surg. 2012 Feb and 21674294., 36(1):18-22. [CrossRef]
- Cigna E, Pierazzi DM, Sereni S, Marcasciano M, Losco L, Bolletta A. Lymphatico-venous anastomosis in chronic ulcer with venous insufficiency: A case report. Microsurgery. 2021 Sep and 10.1002/micr.30753., 41(6):574-578.
- Baker HP, Straszewski AJ, Dahm JS, Dickherber JL, Krishnan P, Dillman DB, Strelzow JA. Gunshot-related lower extremity nerve injuries. Eur J Orthop Surg Traumatol. 2023 May and 7., 33(4):851-856. [CrossRef]
- Maruccia M, Onesti MG, Sorvillo V, Albano A, Dessy LA, Carlesimo B, Tarallo M, Marcasciano M, Giudice G, Cigna E, Ribuffo D. An Alternative Treatment Strategy for Complicated Chronic Wounds: Negative Pressure Therapy over Mesh Skin Graft. Biomed Res Int.
- Inoue, T., Maeda, K., Nagano, A., Shimizu, A., Ueshima, J., Murotani, K., Sato, K., & Tsu-baki, A. (2020). Undernutrition, Sarcopenia, and Frailty in Fragility Hip Fracture: Advanced Strategies for Improving Clinical Outcomes. Nutrients.
- Trujillo JM, Logue ME, Kunkel R, Demas CP. Off-label Usage of Absorbable Beads Containing Antibiotics for Prevention of Surgical Site Infections. Wounds. 2017 Oct and 29(10):E84-E87.
- Kenna DM, Irojah BB, Mudge K, Eveler K. Absorbable Antibiotic Beads Prophylaxis in Immediate Breast Reconstruction. Plast Reconstr Surg. 2018 Apr and 141(4):486e-492e.
- Sherif, RD, Ingargiola M, Sanati-Mehrizy P, Torina PJ, Harmaty MA. Use of antibiotic beads to salvage infected breast implants. J Plast Reconstr Aesthet Surg. 2017 Oct;70(10):1386-1390.
- Khansa I, Barker JC, Ghatak PD, Sen CK, Gordillo GM. Use of antibiotic impregnated resorbable beads reduces pressure ulcer recurrence: A retrospective analysis. Wound Repair Regen. 2018 Mar;26(2):221-227.
- S. Nealon, A. Baumgarten, R. Carrion, J. Parker, 297 The Use of Antibiotic Impregnated Beads in Setting of Penile Implant Infection: A Single Institution Experience, The Journal of Sexual Medicine, Volume 16.
- Robert Morley, MSc, Matt Rothwell, MSc, John Stephenson, PhD, Liza McIlvenny, MSc, Frank Webb, MSc, Aaron Barber, MSc, Complex Foot Infection Treated With Surgical Debridement and Antibiotic Loaded Calcium Sulfate—A Retrospective Cohort Study of 137.
- Chadwick P, Ahmad N, Dunn G et al. (2022) Local antibiotic delivery: early intervention in infection management strategy. The Diabetic Foot Journal 25(2): 44–52.
- Ahmed, Shahnur MD; Lee, Jason T. C. MD, MSc; Roth, Dylan BS; Sinha, Mithuan PhD; Fisher, Carla MD; Fan, Betty DO; Imeokparia, Folasade MD; Ludwig, Kandice MD; Lester, Mary E. MD; Hassanein, Aladdin H. MD, MMSc. Prophylactic Absorbable Antibiotic Beads for HIgh Risk, Implants-based Prepectoral Reconstruction. Plastic & Reconstructive Surgery- Global Open.
- Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM. Microbial biofilms. Annu Rev Microbiol. 1995 and 49:711–745.
- Patel P, Singh R, Agarwal A et al. (2021) Diabetic foot ulcers and osteomyelitis: use of biodegradable calcium sulphate beads with antibiotics for treatment of multidrug-resisteant organists. Wounds 33(3): 70–6.
- Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveil- lance definition of health care associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008 and 36:309–332.
- Marco Marcasciano, Juste Kaciulyte, Riccardo Di Giuli, Fabio Marcasciano, Federico Lo Torto, Maristella Guerra, Giovanni Dal Prà, Leonardo Barellini, Marco Mazzocchi, Donato Casella, Diego Ribuffo, “Just Pulse it!” Introduction of a conservative implant.
- Deva AK, Adams WP Jr, Vickery K. The role of bacterial biofilms in device-associated infection. Plast Reconstr Surg. 2013 and 132:1319–1328.
- Rieger UM, Mesina J, Kalbermatten DF, et al. Bacterial biofilms and capsular contracture in patients with breast implants. Br J Surg. 2013 and 100:768–774.
- Giordano S, Peltoniemi H, Lilius P, Salmi A. Povidone-iodine combined with antibiotic topical irrigation to reduce capsular contracture in cosmetic breast augmentation: A comparative study. Aesthet Surg J. 2013 and 33:675–680.
- Hu H, Johani K, Almatroudi A, et al. Bacterial biofilm infection detected in breast implant associated anaplastic large- cell lymphoma. Plast Reconstr Surg. 2016 and 137:1659–1669.
- Howlin RP, Brayford MJ, Webb JS, Cooper JJ, Aiken SS, Stoodley P. Antibiotic-loaded synthetic calcium sulfate beads for prevention of bacterial colonization and biofilm formation in periprosthetic infections. Antimicrob Agents Chemother. 2015 and 59:111.
- Bamba R, Tran PC, Mailey BA, et al. Comparison of breast recon- struction outcomes using oxychlorosene versus triple antibiotic solution for pocket irrigation. Plast Reconstr Surg Glob Open. 2022 and 10:e3975.
- Dawson SE, Bamba R, Tran PC, et al. Implant-based breast recon- struction outcomes using oxychlorosene for pocket irrigation. Plast Reconstr Surg. 2021 and 148:518e–520e.
- Luchette FA, Bone LB, Born CT, et al. EAST Practice Man- agement Guidelines Workgroup: practice management guidelines for prophylactic antibiotic use in open fractures. Eastern As-sociation for the Surgery of Trauma. 2000.
Figure 1.
PRISMA flowchart. * The 5 journals of plastic and reconstructive surgery with the highest impact factor according to Google Metrics were considered relevant to our study (“Plastic and Reconstructive Surgery”; “Journal of Cosmetic Dermatology”; “Aesthetic Surgery Journal”; “Plastic and Reconstructive surgery. Global Open”; “JPRAS Open”). In order to broaden the search, the following journals were arbitrarily considered relevant due to similarity of scenarios shared by plastic surgery and other surgical specialities: “Wounds”; “Wound repair and regeneration”; “Journal of Sexual Medicine”; “The Journal of Foot & Ankle Surgery”; “The Diabetic Foot Journal”.
Figure 1.
PRISMA flowchart. * The 5 journals of plastic and reconstructive surgery with the highest impact factor according to Google Metrics were considered relevant to our study (“Plastic and Reconstructive Surgery”; “Journal of Cosmetic Dermatology”; “Aesthetic Surgery Journal”; “Plastic and Reconstructive surgery. Global Open”; “JPRAS Open”). In order to broaden the search, the following journals were arbitrarily considered relevant due to similarity of scenarios shared by plastic surgery and other surgical specialities: “Wounds”; “Wound repair and regeneration”; “Journal of Sexual Medicine”; “The Journal of Foot & Ankle Surgery”; “The Diabetic Foot Journal”.
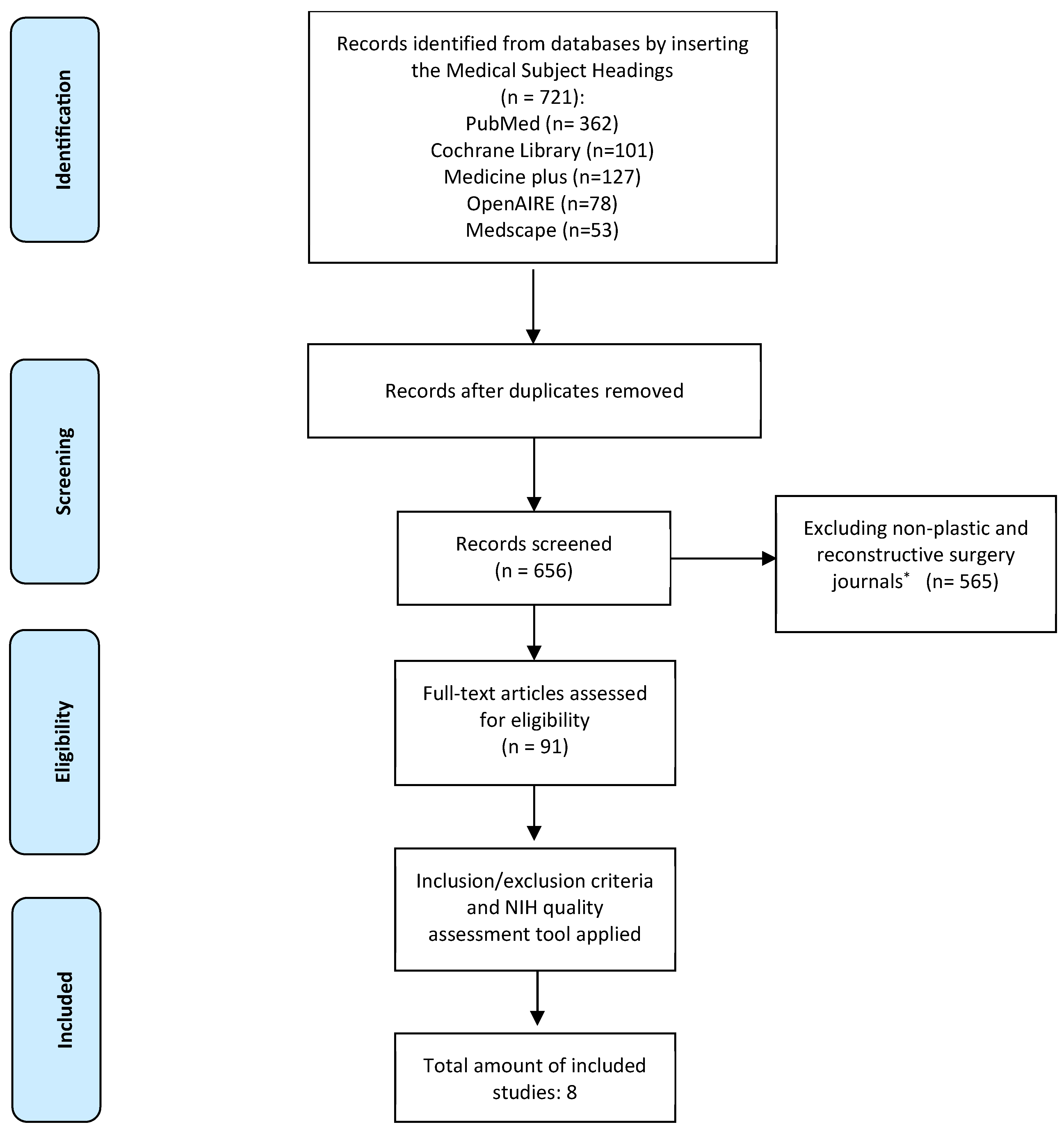

Table 1.
The result of NIH Quality Assessment tool.
| Criteria/author | Trujillo 2017 [22] | Kenna 2017 [23] | Rami 2017 [24] | Khansa 2018 [25] | Nealon 2019 [26] | Morley 2021 [27] | Chadwick 2022 [28] | Ahmed 2023 [29] |
| 1. Was the study question or objective clearly stated? | YES | YES | YES | YES | YES | YES | YES | YES |
| 2. Was the study population clearly and fully described, including a case definition? | NO | YES | YES | YES | NO | YES | YES | NO |
| 3. Were the cases consecutive? | NO | NO | YES | YES | NO | YES | YES | YES |
| 4. Were the subjects comparable? | YES | YES | YES | YES | YES | YES | YES | NO |
| 5. Was the intervention clearly described? | NO | YES | YES | YES | YES | YES | YES | YES |
| 6. Were the outcome measures clearly defined,valid, reliable, andimplemented consistentlyacross all study participants? | YES | YES | YES | YES | YES | YES | YES | NO |
| 7. Was the length of follow-up adequate? | YES | YES | YES | YES | NO | YES | YES | YES |
| 8. Were the statistical methods well-described? | NO | NO | YES | YES | NO | YES | YES | YES |
| 9. Were the results well-described? | YES | YES | YES | YES | YES | YES | YES | NO |
| Quality Rating, ≥ 7 = Good, 5-6 = fair, ≤ 4 = poor | FAIR | GOOD | GOOD | GOOD | FAIR | GOOD | GOOD | FAIR |
Table 2.
Review description. CSB: Calcium sulphate beads. PAD: Peripheral artery disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



