
Submitted:
28 April 2024
Posted:
30 April 2024
You are already at the latest version
Abstract
Bacillus Calmette-Guérin (BCG) therapy for patients with non-muscle invasive bladder cancer (NMIBC) faces limitations in efficacy and significant side effects, aggravated by a recent global shortage. In this prospective clinical study, we report outcomes of sequential intravesical adminis-tration of gemcitabine and docetaxel (Gem/Doce) as the first-line treatment in BCG-naïve patients with high-risk NMIBC (HR NMIBC). From October 2019 until April 2022, we enrolled 52 patients and followed treatment protocol set by the University of Iowa. Follow-up assessments were con-ducted every 3 months. In this cohort, 25 (48.1%) patients were diagnosed with T1HG bladder cancer, 10 (19.2%) patients had carcinoma in situ (CIS), and 17 (32.7%) patients had a combination of CIS+T1HG. Median time to first recurrence in T1HG, CIS and T1HG+CIS groups was 11, 10.5 and 8.8 months, respectively. The recurrence-free survival was 98.1%, 94.2% and 80.8% at 6, 9 and 12 months, respectively. The rate of progression-free survival was 100%, 98.1% and 92.3% at 6, 9 and 12 months, respectively. We demonstrated the safety and efficacy of Gem/Doce therapy in BCG-naïve patients with HR NMIBC during a one-year follow-up. Further research with extended follow-up, as well as direct comparison of Gem/Doce and other anticancer agents, are essential.
Keywords:
BCG shortage
; Non-muscle invasive bladder cancer
; BCG-Naïve
; Docetaxel
; Gemcitabine
1. Introduction
Bladder cancer is a significant public health problem, ranking as the eleventh most prevalent cancer in the world and the fifth most common cancer in the European Union [1]. It is estimated that approximately 550,000 new cases of bladder cancer are diagnosed annually, with a higher prevalence in developed countries [2]. Smoking and occupational exposures such as aromatic amines, polycyclic aromatic hydrocarbons, and benzenes are the strongest established risk factors but the contributions of other environmental and genetic factors to the development of bladder cancer are increasingly being recognized [3,4]. The development and progression of bladder cancer are governed by complex molecular processes within bladder cells which control how tumors start, develope, and spread. Changes in important cell signaling pathways, disruptions in the regulation of cell division, and the ability of cancer cells to evade detection by the immune system are crucial factors in the transformation of normal bladder cells into cancerous ones [5]. Most bladder cancers are of urothelial histology, and localized urothelial carcinoma of the bladder is broadly categorized into non-muscle invasive bladder cancer (NMIBC) and muscle-invasive disease. Commonly used TNM staging system defines NMIBC as noninvasive papillary tumour (Ta), carcinoma in situ (CIS), or with invasion limited to the lamina propria (T1). NMIBC accounts for 70%-75% of all bladder cancer cases and almost 75% of the noninvasive papillary tumors detected are Ta stage. Noninvasive papillary lesions or Ta stage tumors have a low risk for progression to invasive disease; altough their biologic behavior is dependent on the grade of the papillary lesion. The rest 25% have invasion into lamina propria or pT1 stage which tend to be fragile and therefore bleed easily causing the symptom of hematuria early in the disease. Also, they tend to recur; and between 31% and 78% of these tumors will recur, either at the same stage of the initial tumor or at an advanced stage [6,7]. A flat lesion that extends throughout the mucosal layer without invading the basement membrane is termed carcinoma in situ (CIS) according to TNM staging criteria and all are classified as high grade thus warrant investigation for specific genetic mutations and histopathologic characteristics [8]. Upon histopathological examination following transurethral resection of the bladder tumor (TURBT), the lesion typically displays flat morphology with cytological abnormalities throughout the full thickness of the tissue and an intact basement.
A T2 tumor is classified as invasive because it breaches the basement membrane and penetrates the muscular layer of the bladder wall. This invasion marks a significant deterioration in prognosis, with a notable decrease in the 5-year survival rate. Progression to T3 disease occurs when the cancer extends further into the detrusor muscle and involves the surrounding perivesical tissues. T4 disease is characterized by invasion beyond the bladder into adjacent organs such as the prostatic stroma, seminal vesicles, uterus, vagina, pelvic wall, or abdominal wall. The depth of invasion serves as the primary determinant of both prognosis and treatment decisions for localized bladder cancer with radical cystecomy as golden standard [9].
In NMIBC, patient risk is estimated using prognostic models, which allow stratifying patients into risk groups, based on clinical and pathological characteristics. Various models and stratification tables that outline the clinical characteristics of different risk groups are created by reputable organizations like the European Association of Urology (EAU), the American Urological Association (AUA), as well as independent research entities. A recent risk model, formulated by the EAU, aims to predict the time until progression in patients diagnosed with Ta/T1 NMIBC who undergo TURBT followed by intravesical chemotherapy. This model incorporates several predictive factors including age, tumor count, stage, maximum tumor diameter, tumor grade according to either the WHO 1973 or the WHO 2004/2016 grading systems, and the presence of carcinoma in situ.
The EAU, whose guidelines have been endorsed by more than 50 urological societies and associations, recommends stratification of patients into three prognostic factor risk groups: low, intermediate, and high risk, which includes a subgroup of the highest risk tumors. Patients with high-risk NMIBC (Ta/T1 with high grade, and/ or CIS) represent a challenging group with an increased 5-year risk of recurrence (up to 80 %) and progression (up to 50 %) according to the EORTC risk stratification tables [10]. Despite advancements in diagnostic and therapeutic options, NMIBC continues to pose a significant therapeutic challenge due to its high recurrence and progression rates [11].
The focus in this study is a group of patients with high-risk NMIBC. Bacillus Calmette-Guérin (BCG) therapy, even after 40 years since its approval, retains its status as the gold standard for intravesical treatment in NMIBC, despite its ineffectiveness in 30% to 77% of patients who may experience disease recurrence within 5 years and its association with significant side effects [12,13,14,15,16,17,18,19]. The global shortage of Bacillus Calmette-Guérin (BCG) vaccine, primarily utilized in the treatment of bladder cancer, has emerged as a significant concern in recent decade. Increasingly, intravesical chemotherapy with Gemcitabine/Docetaxel (GEM/DOCE) has been utilized in many published studies.
In this prospective clinical study, we demonstrated the safety and efficacy of Gem/Doce therapy in BCG-naïve patients with HR NMIBC during a one-year follow-up.
2. Materials and Methods
2.1. Study Design and Patients
This study was revised and approved by the Ethics Committee of the Zagreb University Hospital Center (02/21 AG: 8.1-20/81-2) and is in accordance with the Helsinki Declaration. Informed consent was obtained from all participants.
From October 2019 until April 2022, our institution enrolled 52 BCG-naïve patients diagnosed with high-risk NMIBC following complete transurethral resection of bladder tumor (TURBT) in this prospective cohort study. Patients were scheduled to undergo a treatment plan consisting of 6 weekly intravesical instillations of sequential 1 g gemcitabine and 37.5 mg docetaxel, followed by monthly maintenance instillations for one or two years in those showing no evidence of high-grade (HG) tumor relapse.
We collected comprehensive data, including information on sex, age, height, weight, body mass index (BMI), chronic diseases, therapy details, prior NMIBC treatment history, along with cystoscopic, operative, and pathologic findings, and follow-up records.
Risk stratification followed the criteria outlined by the European Urological Association [5]. Patients with a history of prior BCG treatment for any duration were excluded, and so were those who did not undergo the recommended follow-up surveillance during the study period.
2.2. Gem/Doce Instillation
The Gem/Doce treatment protocol followed the well-established guidelines set forth by Steinberg et al. at the University of Iowa [16]. After a negative finding of urinary infection (urine dipstick or culture test), induction was sequentially administered intravesically once a week for 6 consecutive weeks. After catheter placement and bladder emptying, slow instillation of one gram of gemcitabine in 50 mL of normal saline solution (NSS) was conducted, followed by clamping the catheter for 90 minutes.
A catheter was placed into the bladder and the bladder was drained. One gram of gemcitabine in 50 mL of NSS was slowly instilled into the bladder and the catheter was clamped for 90 minutes. Afterwards, the bladder was emptied, and gradual instillation of 37.5 mg of docetaxel in 50 mL of NSS was administered. Following the instillation, the catheter was removed, and patients were instructed to urinate after 90-120 minutes. In subsequent instillations, patients were asked about any discomfort, side effects, or changes in their quality of life that may have arisen due to therapy. In patients without HG relapse at the initial follow-up after induction, monthly maintenance therapy was initiated.
2.3. Surveillance
Follow-up assessments were conducted every 3 months, involving office cystoscopy, cytologic examination of urine, blood tests, and imaging studies (ultrasound, computed tomography, magnetic resonance imaging). All biopsy and cytology findings were evaluated by genitourinary pathologists and cytopathologists for evidence of disease recurrence/progression. If suspicious cystoscopic or imaging findings, or positive cytologic results were observed during the follow-up, patients underwent additional procedures including random bladder biopsies, urethral biopsies, bilateral upper tract barbotage cytology tests, and bilateral retrograde pyelograms. Treatment was continued in patients who did not show signs of disease recurrence or showed low-grade recurrence, while it was discontinued in those with HG recurrence.
2.4. Statistical Analysis
Statistical analysis was performed using STATISTICA 6.1 program (StatSoft Inc., Tulsa, OK, USA). Numerical data were described by descriptive statistics (mean, median, range, standard deviation), and descriptive data by frequency tables. Follow-up data of disease progression and patient survival were analyzed by Kaplan-Meier method. Comparison of two or more groups of patients was performed by χ2-test and log-rank test, respectively. The level of statistical significance was set at 95% (α=0.05).
3. Results
3.1. Patient Demographics
This study included 52 patients with HG NMIBC who had not previously received BCG. The mean age of patients at the time of study inclusion was 69.27±11.45 (44 to 93) years. There were 44 (84.6%) male and 8 (15.4%) female patients. The mean BMI was 27.55±5.09 (19.15-41.97), lower urinary tract symptoms were detected in 15 (28.8%) patients, and 14 (26.9%) patients had diabetes mellitus (Table 1).
In this cohort, after final complete TURBT, 25 (48.1%) patients were diagnosed with high-grade T1 (T1HG) bladder cancer, 10 (19.2%) patients had carcinoma in situ (CIS), and 17 (32.7%) patients had a combination of CIS+T1HG (Table 2).
There was a planned delay of at least 20 days in the first weekly induction course of Gem/Doce after TURBT. The mean delay was 1.55±1.07 (0.73-6.57) months. In patients with extreme delay in starting treatment, cystoscopic assessment and radiological diagnostics were performed to verify the state of no recurrence.
Induction course was completely performed in 50 (96.1%) patients. One patient had only 2 induction instillations due to unrelated medical complications, while one patient had urinary infection due to which he missed one more instillation to complete the induction cycle.
3.2. Survival Outcomes
There were 10 (19.2%) patients with bladder recurrence during the follow-up. There was no recurrence in the first 4 months of follow-up with TURBT performed in 6 patients for cystoscopy suspicion of bladder cancer. In all patient groups, there were 14 TURBT performed during the follow-up with no bladder cancer diagnosed in the specimens collected, which could be explained by excessive caution for the sake of new therapy initiation. In 2 (3.8%) patients, at 11-month follow-up after TURBT, downstaging to TaLG cancer was observed and therapy was continued. There were 3 (5.8%) cases of progression upon TURBT, which occurred at 11- and 12-month follow-up, and 1 (1.9%) case of radiologically diagnosed progression involving retroperitoneal mass and lymphadenopathy, with no evidence for bladder cancer at 9-month follow-up. In 2 (3.8%) patients with variant histology, no recurrences occurred in the follow-up with one TURBT performed for recurrence suspicion.
At the time of first recurrence, 3 (12%) patients were in T1HG group, 2 (20%) patients in CIS group, and 5 (29.4) patients in T1HG+CIS group. Median time to first recurrence in T1HG, CIS and T1HG+CIS groups was 11, 10.5 and 8.8 months, respectively (Table 3).
The recurrence-free survival (RFS) was 98.1%, 94.2% and 80.8% at 6, 9 and 12 months, respectively. The HG RFS was 98.1%, 94.2% and 84.6% at 6, 9 and 12 months, respectively. The rate of progression-free survival (PFS) was 100%, 98.1% and 92.3% at 6, 9 and 12 months, respectively (Table 3, Figure 1).
Table 2. test showed that there was no statistically significant difference in the number of patients with no recurrence compared to the initial histopathologic diagnosis (p=0.295) (Figure 2.). The rate of disease recurrence was 12% and occurred at 11-month follow-up in the T1HG group, whereas in the T1HG+CIS group it was 79.6% and occurred after 5 months (mean, 8.8 months). Due to the small number of patients in these two categories, this difference was not statistically significant (p=0.129) (Figure 3).
χ2=2.445, df 3, p=0.295
χ2-test indicated that there was no statistically significant difference in the number of patients without recurrence according to histopathology groups (p=0.295).
Log-rank test
Test statistic = 1.518, p=0.129
Test statistic = 1.518, p=0.129
Log-rank test indicated that there was no statistically significant difference in the number of patients without recurrence between the T1HG and T1HG+CIS histopathology groups (p=0.129). The rate of disease recurrence was 12% in the T1HG histopathology group, where it occurred at 11 months, whereas it was 79.6% in the T1HG+CIS histopathology group, where it occurred at 5 months (mean, 8.8 months). The between-group difference did not reach statistical significance due to the small number of patients in these two groups (p=0.129).
3.3. Progression and Survival
There were no bladder cancer related deaths during the observed time and cancer-specific survival was 100% at 12 months. At 10-month follow-up, 1 (1.9%) patient died from a medical condition unrelated to bladder cancer, and overall survival was 98.1%. One patient with TURBT diagnosed T2 progression underwent radical cystectomy. (Table 4) Definitive pathology reported it as pT3bN0. In one patient with radiologically diagnosed progression involving retroperitoneal mass and lymphadenopathy, chemotherapy was initiated.
4. Discussion
A team-based approach to managing non-muscle invasive bladder cancer (NMIBC) involves healthcare professionals from different specialties working together to provide the best possible care and results for patients. This method acknowledges the intricate nature of NMIBC treatment, which often demands input from urologists, oncologists, radiologists, pathologists, and other specialists. The process begins with ensuring an accurate diagnosis and staging of NMIBC using procedures like cystoscopy, imaging scans, and examining tissue samples under a microscope. Urologists lead this initial phase, conducting the necessary tests and coordinating the initial treatment plans. After diagnosis, treatment decisions are tailored to each patient’s specific situation, considering factors such as the tumor’s stage, grade, and risk level. Treatments may include procedures like reTURBT, intravesical therapy or radical surgery. Oncologists and urologists collaborate closely to determine the most suitable treatment plan for each patient.
BCG intravesical treatment involves an initial regimen of 6 weekly administrations, beginning a couple of weeks post-tumor removal. This is then succeeded by a maintenance plan, with extra BCG administrations every 3 to 6 months, spanning 1 to 3 years [20]. Many studies have been published on BCG efficacy and usual findings are that induces initial complete response rates of 55–65% for high-risk papillary tumours and 70–75% for CIS [14,20,21]. Maintenance plans vary widely across published research and healthcare institutions, often adapting based on patient tolerance and adherence. These variations have undergone testing in clinical studies, with specific factors explored including the frequency and dosage of BCG instillations [22]. In the SWOG 8507 protocol, which involves 6 instillations over 6 weeks followed by a maintenance regimen of weekly BCG instillations for 3 weeks at 3-month intervals up to 36 months, has shown superior efficacy in preventing recurrence and progression compared to induction therapy alone. In high-risk patients, a full-dose induction course combined with a 3-year BCG maintenance schedule, following the SWOG 8507 protocol, led to reduced recurrence rates compared to a 1-year maintenance schedule, though no significant differences were observed in long-term outcomes related to progression or mortality. In the last decade, partly because of the global BCG shortage, ongoing efforts aim to assess the efficacy of reducing the number of BCG instillations during the induction phase, as explored in the NIMBUS trial [23].
However global shortage of BCG, primarily attributed to manufacturing challenges and disruptions in vaccine production, coupled with a high global demand, has significantly impacted the availability of this essential treatment option for bladder cancer patients [24,25]. To address these challenges, a range of strategies has been implemented, including the recommendation to reserve BCG for patients at the highest risk of progression. Furthermore, efforts have been made to optimize treatment protocols, with special emphasis on research into novel immunotherapies, chemotherapies, and treatments for bladder cancer. Unfortunately, many studies suffer from notable bias, particularly retrospective ones involving small groups of patients, making it challenging to accurately distinguish between BCG failure and tumor risk levels, or sometimes this information isn’t even provided. Despite these limitations, alternative intravesical therapies have long been explored for NMIBC. These include Mitomycin C (MMC), valrubicin, gemcitabine, docetaxel, and combination therapy. In studies with BCG-naïve patients receiving MMC, results demonstrated a 5-year RFS of 34%. MMC monotherapy after failing 1 induction course of BCG was found to have a 3-year RFS of 19% [26]. Valrubicin has been studied in the treatment of CIS for patients with previous exposure to BCG. DFS was 21% at 6 months in Steinberg et al. study in which 99% of patients had at least 2 induction courses [27]. Docetaxel induction provided 1- and 3-year RFS rates of 40% and 25% in a BCG failure cohort without maintenance [28]. Intravesical gemcitabine was found to have RFS rates of 28% at 1 year and 21% at 2 years post-therapy [29]. Among the examined mono- and combination therapies, sequential intravesical administration of gemcitabine and docetaxel (Gem/Doce) has emerged as a promising therapeutic strategy for patients with NMIBC and the main aim of our study was to investigate the approaching alternative to BCG therapy.
Gemcitabine and docetaxel are both FDA-approved anti-cancer drugs. The effectiveness of combining docetaxel and gemcitabine for treating bladder cancer stems from several factors. Firstly, the cooperative action of these drugs enhances their ability to kill cancer cells, leading to better treatment outcomes. Secondly, using them together may help overcome resistance that can develop against single-drug chemotherapy, thus making the treatment more effective at halting tumor growth. Moreover, this combination therapy is well-tolerated by patients, allowing for longer treatment durations, which in turn improves disease control and patient outcomes.
Gemcitabine and docetaxel were initially introduced in 2014 as an alternative for patients who did not respond to BCG treatment [30]. However, given the ongoing and severe scarcity of BCG within both our health system and others, and based on the available data at the time, our multidisciplinary team at the institution decided to implement the use of Gem/Doce in a BCG-naïve setting. While conducting therapy, our decision to use Gem/Doce in BCG-naïve patients was validated by publication of two pivotal papers, emphasizing the safety and efficacy of this approach [31,32]. Gemcitabine, a nucleoside analog, and docetaxel, a taxane chemotherapy agent, administered directly into the bladder, demonstrate localized cytotoxic effects without causing systemic toxicity. The use of this principle involving two or more drugs is justified and has proven effective in other urologic or malignant diseases, thus it is reasonable to expect that the combination of drugs will yield better results than using either of them alone.
Mostly since 2014, Gem/Doce has been reported as being efficacious and well tolerated in patients with BCG failure, or as a salvage therapy, with 54% one-year treatment success [30]. Catalyzed by the BCG shortage and encouraging initial results, more studies have reported favorable outcomes, including improved disease-free survival, reduced recurrence rates, and acceptable tolerability profiles [33,34].
In this prospective, single-arm, cohort study, we examined the efficacy of Gem/Doce in BCG-naïve patients with high-risk NMIBC and examined its use as maintenance therapy in HG relapse-free patients on the first check-point surveillance after full induction.
Our institutional experience with Gem/Doce therapy in high-risk BCG-naïve patients indicated good efficacy with RFS of 98.1% and 80.8%, at 6 and 12 months, respectively. HG RFS was 84.6% and PFS 92.3% at 12-month follow-up. During the one-year follow-up, 81% of our patients were free of cancer and 84.6% had HG RFS; slightly better results of HG RFS 87% at 12-month follow-up have been reported by McElree et al. We had more patients with CIS comparing to their study (52% vs. 44%), and they also showed that the majority of first recurrences had a component of CIS, additionally confirming its importance in disease recurrence. Furthermore, they included patients with HG Ta bladder cancer, and all this may be potential explanations for their slightly better results [31].
MeElree et al. published a large study of 312 patients, of which almost 44% had CIS (alone or in combination) and almost one-third of them had a Ta cancer with HG RFS in 71% of patients with BCG treatment and 85% of patients with Gem/Doce [32], which is actually the same as we found in our study confirming the efficacy of this therapy especially in older patients who may be increasingly immunosenescent and therefore less suitable for BCG treatment. These authors also demonstrated that patients were less likely to quit Gem/Doce treatment because they had better quality of life and less toxic effects compared to BCG [32], confirming the findings reported from other studies [35]. In our study, only one patient reported probably unrelated complication which postponed treatment, thus verifying the safety and tolerability of this treatment.
Daniels et al. evaluated Gem/Doce therapy in a cohort of patients having a mean of 11.6 intravesical treatments prior to Gem/Doce, with the majority (>80%) of them being BCG but also including mitomycin C and valrubicin making this cohort relatively heterogeneous with the possible bias related to previous therapy and not to Gem/Doce, showing only 10.2% of HG recurrence in 24-month median follow-up. Anyhow, all these data show that Gem/Doce therapy is at least as good as BCG treatment for HG RFS rates which are closer to 80% [36]. There is also the question how long Gem/Doce therapy should be administered to obtain optimal result? Will prolonged use give our patients even better results as it has been shown with BCG treatment?
As we have shown in the Results section, during the observation period, 14 TURBT were performed in which bladder cancer was not proven. Most of them were performed in the initial follow-up period, which we can attribute to the increased caution on introducing new therapy in the NMIBC treatment protocol. In such patients, cystoscopic examination showed a solid formation, with a non-papillary appearance. The histopathologic finding mainly indicated an area of necrosis and inflammatory infiltrate, perhaps with anticancer impact [37]. In further course of the observation period, the number of biopsies that did not indicate recurrence decreased and the number of positive cancer findings increased, which indicated a learning curve for cystoscopic examination in patients on Gem/Doce therapy.
In the financial aspect, an induction course of GEM/DOCE is roughly 125% the cost of an induction course of BCG and 1/3 of the cost of induction MMC, with docetaxel making up most of that cost [36]. Valrubicin has been shown to cost $20,000 per induction course [38]. Avoiding cystectomy can be financially beneficial, considering that the average cost of the initial hospital stay for cystectomy patients is $33,202, with additional mean costs of $14,417 for readmissions [39]. Cost reduction, even in small amounts, when dealing with the costliest cancer at a population level, holds significant importance for patients, healthcare providers, and insurance companies alike. This is particularly crucial as the healthcare landscape increasingly emphasizes enhancing the value of care delivered. Bladder cancer, being one of the most expensive cancers to treat, places a substantial financial burden on patients, healthcare systems, and insurers. Therefore, any reduction in costs associated with treatments, such as avoiding the expense of cystectomy and subsequent readmissions, can have notable benefits across the board.
Regarding the limitations, although our study was prospective, the lack of a control group may be considered a limitation. However, given the global shortage of BCG over an extended period, and the limited effectiveness of some other types of intravesical therapy for patients with NMIBC, we chose to administer Gem/Doce to all our patients. After completing the therapy, we intend to present the results recorded in this cohort.
While the initial findings are promising, further research is necessary to refine the dosage and treatment schedule, as well as to identify markers that predict how patients will respond to this therapy. Exploring potential combinations with targeted therapies or immunotherapy agents is also crucial. Ongoing clinical trials are actively investigating the efficacy of docetaxel and gemcitabine combination therapy across different subtypes of bladder cancer and treatment scenarios. The aim is to solidify its position as a standard treatment option for managing this complex disease.
Further research with extended follow-up, as well as direct comparison of Gem/Doce and BCG, or combinations of BCG with other drugs such as mitomycin, is essential to unequivocally establish the role of Gem/Doce in NMIBC.
Author Contributions
Conceptualization, M.B., T.H., M.Ga. and Z.K.; Methodology, M.B., T.H., M.Gnj. and N.K.; Validation, M.B., T.H., N.K. and Z.K.; Formal Analysis, M.B., Z.Z., J.A. and I.J.; Investigation, M.B., Z.Z., J.A. and I.J.; Resources, Z.K.; Data Curation, M.B., J.A. and M.Gnj.; Writing – Original Draft Preparation, M.B.; Writing – Review & Editing, T.H., N.K. and Z.K.; Visualization, M.B. and T.H.; Supervision, Z.K.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Zagreb University Hospital Center (02/21 AG: 8.1-20/81-2)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
None to declare
Conflicts of Interest
The authors declare no conflicts of interest.
Clinical trial registration number: NCT05247775
References
- European Cancer Information System. https://ecis.jrc.ec.europa.eu/explorer.php (accessed 2023-05-30).
- Sung, H.; Ferlay, J.; Siegel, R. L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021, 71 (3), 209–249. [CrossRef]
- Burger, M.; Catto, J. W. F.; Dalbagni, G.; Grossman, H. B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L. A.; La Vecchia, C.; Shariat, S.; et al. Epidemiology and Risk Factors of Urothelial Bladder Cancer. Eur Urol 2013, 63 (2), 234–241. [CrossRef]
- Semeniuk-Wojtaś, A.; Poddębniak-Strama, K.; Modzelewska, M.; Baryła, M.; Dziąg-Dudek, E.; Syryło, T.; Górnicka, B.; Jakieła, A.; Stec, R. Tumour Microenvironment as a Predictive Factor for Immunotherapy in Non-Muscle-Invasive Bladder Cancer. Cancer Immunol Immunother 2023, 72 (7), 1971–1989. [CrossRef]
- Hurst, C. D.; Knowles, M. A. Mutational Landscape of Non-Muscle-Invasive Bladder Cancer. Urologic Oncology: Seminars and Original Investigations 2022, 40 (7), 295–303. [CrossRef]
- Flaig, T. W.; Spiess, P. E.; Agarwal, N.; Bangs, R.; Boorjian, S. A.; Buyyounouski, M. K.; Chang, S.; Downs, T. M.; Efstathiou, J. A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network 2020, 18 (3), 329–354. [CrossRef]
- Magers, M. J.; Lopez-Beltran, A.; Montironi, R.; Williamson, S. R.; Kaimakliotis, H. Z.; Cheng, L. Staging of Bladder Cancer. Histopathology 2019, 74 (1), 112–134. [CrossRef]
- Minoli, M.; Kiener, M.; Thalmann, G. N.; Kruithof-de Julio, M.; Seiler, R. Evolution of Urothelial Bladder Cancer in the Context of Molecular Classifications. IJMS 2020, 21 (16), 5670. [CrossRef]
- Alfred Witjes, J.; Max Bruins, H.; Carrión, A.; Cathomas, R.; Compérat, E.; Efstathiou, J. A.; Fietkau, R.; Gakis, G.; Lorch, A.; Martini, A.; et al. European Association of Urology Guidelines on Muscle-Invasive and Metastatic Bladder Cancer: Summary of the 2023 Guidelines. European Urology 2024, 85 (1), 17–31. [CrossRef]
- Babjuk, M.; Böhle, A.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E. M.; Hernández, V.; Kaasinen, E.; Palou, J.; Rouprêt, M.; et al. EAU Guidelines on Non-Muscle-Invasive Urothelial Carcinoma of the Bladder: Update 2016. Eur Urol 2017, 71 (3), 447–461. [CrossRef]
- David, K. A.; Mallin, K.; Milowsky, M. I.; Ritchey, J.; Carroll, P. R.; Nanus, D. M. Surveillance of Urothelial Carcinoma: Stage and Grade Migration, 1993-2005 and Survival Trends, 1993-2000. Cancer 2009, 115 (7), 1435–1447. [CrossRef]
- Hall, M. C.; Chang, S. S.; Dalbagni, G.; Pruthi, R. S.; Seigne, J. D.; Skinner, E. C.; Wolf, J. S.; Schellhammer, P. F. Guideline for the Management of Nonmuscle Invasive Bladder Cancer (Stages Ta, T1, and Tis): 2007 Update. J Urol 2007, 178 (6), 2314–2330. [CrossRef]
- Chang, S. S.; Boorjian, S. A.; Chou, R.; Clark, P. E.; Daneshmand, S.; Konety, B. R.; Pruthi, R.; Quale, D. Z.; Ritch, C. R.; Seigne, J. D.; et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J Urol 2016, 196 (4), 1021–1029. [CrossRef]
- Sylvester, R. J.; Rodríguez, O.; Hernández, V.; Turturica, D.; Bauerová, L.; Bruins, H. M.; Bründl, J.; van der Kwast, T. H.; Brisuda, A.; Rubio-Briones, J.; et al. European Association of Urology (EAU) Prognostic Factor Risk Groups for Non-Muscle-Invasive Bladder Cancer (NMIBC) Incorporating the WHO 2004/2016 and WHO 1973 Classification Systems for Grade: An Update from the EAU NMIBC Guidelines Panel. Eur Urol 2021, 79 (4), 480–488. [CrossRef]
- Balasubramanian, A.; Gunjur, A.; Weickhardt, A.; Papa, N.; Bolton, D.; Lawrentschuk, N.; Perera, M. Adjuvant Therapies for Non-Muscle-Invasive Bladder Cancer: Advances during BCG Shortage. World J Urol 2022, 40 (5), 1111–1124. [CrossRef]
- Zlotta, A. R.; Fleshner, N. E.; Jewett, M. A. The Management of BCG Failure in Non-Muscle-Invasive Bladder Cancer: An Update. Can Urol Assoc J 2009, 3 (6 Suppl 4), S199-205. [CrossRef]
- Sfakianos, J. P.; Kim, P. H.; Hakimi, A. A.; Herr, H. W. The Effect of Restaging Transurethral Resection on Recurrence and Progression Rates in Patients with Nonmuscle Invasive Bladder Cancer Treated with Intravesical Bacillus Calmette-Guérin. J Urol 2014, 191 (2), 341–345. [CrossRef]
- Kamat, A. M.; Colombel, M.; Sundi, D.; Lamm, D.; Boehle, A.; Brausi, M.; Buckley, R.; Persad, R.; Palou, J.; Soloway, M.; Witjes, J. A. BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer: Recommendations from the IBCG. Nat Rev Urol 2017, 14 (4), 244–255. [CrossRef]
- Oddens, J.; Brausi, M.; Sylvester, R.; Bono, A.; Van De Beek, C.; Van Andel, G.; Gontero, P.; Hoeltl, W.; Turkeri, L.; Marreaud, S.; et al. Final Results of an EORTC-GU Cancers Group Randomized Study of Maintenance Bacillus Calmette-Guérin in Intermediate- and High-Risk Ta, T1 Papillary Carcinoma of the Urinary Bladder: One-Third Dose Versus Full Dose and 1 Year Versus 3 Years of Maintenance. European Urology 2013, 63 (3), 462–472. [CrossRef]
- Lamm, D. L.; Blumenstein, B. A.; Crissman, J. D.; Montie, J. E.; Gottesman, J. E.; Lowe, B. A.; Sarosdy, M. F.; Bohl, R. D.; Grossman, H. B.; Beck, T. M.; et al. Maintenance Bacillus Calmette-Guerin Immunotherapy for Recurrent TA, T1 and Carcinoma in Situ Transitional Cell Carcinoma of the Bladder: A Randomized Southwest Oncology Group Study. J Urol 2000, 163 (4), 1124–1129.
- Askeland, E. J.; Newton, M. R.; O’Donnell, M. A.; Luo, Y. Bladder Cancer Immunotherapy: BCG and Beyond. Advances in Urology 2012, 2012, 1–13. [CrossRef]
- Yokomizo, A.; Kanimoto, Y.; Okamura, T.; Ozono, S.; Koga, H.; Iwamura, M.; Tanaka, H.; Takahashi, S.; Tsushima, T.; Kanayama, H.; et al. Randomized Controlled Study of the Efficacy, Safety and Quality of Life with Low Dose Bacillus Calmette-Guérin Instillation Therapy for Nonmuscle Invasive Bladder Cancer. Journal of Urology 2016, 195 (1), 41–46. [CrossRef]
- Rezaee, M. E.; Ismail, A. A. O.; Okorie, C. L.; Seigne, J. D.; Lynch, K. E.; Schroeck, F. R. Partial Versus Complete Bacillus Calmette-Guérin Intravesical Therapy and Bladder Cancer Outcomes in High-Risk Non-Muscle-Invasive Bladder Cancer: Is NIMBUS the Full Story? Eur Urol Open Sci 2021, 26, 35–43. [CrossRef]
- Harvey, M.; Chislett, B.; Perera, M.; Lawrentschuk, N.; Bolton, D.; Jack, G. Critical Shortage in BCG Immunotherapy: How Did We Get Here and Where Will It Take Us? Urol Oncol 2022, 40 (1), 1–3. [CrossRef]
- American Urological Association. https://www.auanet.org/bcg-shortage-notice (accessed 2023-05-21).
- Malmström, P. U.; Wijkström, H.; Lundholm, C.; Wester, K.; Busch, C.; Norlén, B. J. 5-Year Followup of a Randomized Prospective Study Comparing Mitomycin C and Bacillus Calmette-Guerin in Patients with Superficial Bladder Carcinoma. Swedish-Norwegian Bladder Cancer Study Group. J Urol 1999, 161 (4), 1124–1127.
- Steinberg, G.; Bahnson, R.; Brosman, S.; Middleton, R.; Wajsman, Z.; Wehle, M. Efficacy and Safety of Valrubicin for the Treatment of Bacillus Calmette-Guerin Refractory Carcinoma in Situ of the Bladder. The Valrubicin Study Group. J Urol 2000, 163 (3), 761–767.
- Barlow, L. J.; McKiernan, J. M.; Benson, M. C. Long-Term Survival Outcomes with Intravesical Docetaxel for Recurrent Nonmuscle Invasive Bladder Cancer After Previous Bacillus Calmette-Guérin Therapy. Journal of Urology 2013, 189 (3), 834–839. [CrossRef]
- Skinner, E. C.; Goldman, B.; Sakr, W. A.; Petrylak, D. P.; Lenz, H.-J.; Lee, C. T.; Wilson, S. S.; Benson, M.; Lerner, S. P.; Tangen, C. M.; et al. SWOG S0353: Phase II Trial of Intravesical Gemcitabine in Patients with Nonmuscle Invasive Bladder Cancer and Recurrence after 2 Prior Courses of Intravesical Bacillus Calmette-Guérin. Journal of Urology 2013, 190 (4), 1200–1204. [CrossRef]
- Steinberg, R. L.; Thomas, L. J.; O’Donnell, M. A.; Nepple, K. G. Sequential Intravesical Gemcitabine and Docetaxel for the Salvage Treatment of Non-Muscle Invasive Bladder Cancer. Bladder Cancer 2015, 1 (1), 65–72. [CrossRef]
- McElree, I. M.; Steinberg, R. L.; Martin, A. C.; Richards, J.; Mott, S. L.; Gellhaus, P. T.; Nepple, K. G.; O’Donnell, M. A.; Packiam, V. T. Sequential Intravesical Gemcitabine and Docetaxel for Bacillus Calmette-Guérin-Naïve High-Risk Nonmuscle-Invasive Bladder Cancer. J Urol 2022, 208 (3), 589–599. [CrossRef]
- McElree, I. M.; Steinberg, R. L.; Mott, S. L.; O’Donnell, M. A.; Packiam, V. T. Comparison of Sequential Intravesical Gemcitabine and Docetaxel vs Bacillus Calmette-Guérin for the Treatment of Patients With High-Risk Non–Muscle-Invasive Bladder Cancer. JAMA Netw Open 2023, 6 (2), e230849. [CrossRef]
- Milbar, N.; Kates, M.; Chappidi, M. R.; Pederzoli, F.; Yoshida, T.; Sankin, A.; Pierorazio, P. M.; Schoenberg, M. P.; Bivalacqua, T. J. Oncological Outcomes of Sequential Intravesical Gemcitabine and Docetaxel in Patients with Non-Muscle Invasive Bladder Cancer. Bladder Cancer 2017, 3 (4), 293–303. [CrossRef]
- Steinberg, R. L.; Thomas, L. J.; Brooks, N.; Mott, S. L.; Vitale, A.; Crump, T.; Rao, M. Y.; Daniels, M. J.; Wang, J.; Nagaraju, S.; et al. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol 2020, 203 (5), 902–909. [CrossRef]
- Pareek, T.; Parmar, K.; Sharma, A. P.; Kumar, S. Quality of Life, Efficacy, and Safety of Sequential Intravesical Gemcitabine + Docetaxel versus BCG for Non-Muscle Invasive Urinary Bladder Cancer: A Pilot Study. Urol Int 2022, 106 (8), 784–790. [CrossRef]
- Daniels, M. J.; Barry, E.; Milbar, N.; Schoenberg, M.; Bivalacqua, T. J.; Sankin, A.; Kates, M. An Evaluation of Monthly Maintenance Therapy among Patients Receiving Intravesical Combination Gemcitabine/Docetaxel for Nonmuscle-Invasive Bladder Cancer. Urologic Oncology: Seminars and Original Investigations 2020, 38 (2), 40.e17-40.e24. [CrossRef]
- Kastelan, Z.; Lukac, J.; Derezić, D.; Pasini, J.; Kusić, Z.; Sosić, H.; Kastelan, M. Lymphocyte Subsets, Lymphocyte Reactivity to Mitogens, NK Cell Activity and Neutrophil and Monocyte Phagocytic Functions in Patients with Bladder Carcinoma. Anticancer Res 2003, 23 (6D), 5185–5189.
- Marchetti, A.; Wang, L.; Magar, R.; Barton Grossman, H.; Lamm, D. L.; Schellhammer, P. F.; Erwin-Toth, P. Management of Patients with Bacilli Calmette-Guérin-Refractory Carcinoma in Situ of the Urinary Bladder: Cost Implications of a Clinical Trial for Valrubicin. Clinical Therapeutics 2000, 22 (4), 422–438. [CrossRef]
- Chappidi, M. R.; Kates, M.; Stimson, C. J.; Johnson, M. H.; Pierorazio, P. M.; Bivalacqua, T. J. Causes, Timing, Hospital Costs and Perioperative Outcomes of Index vs Nonindex Hospital Readmissions after Radical Cystectomy: Implications for Regionalization of Care. Journal of Urology 2017, 197 (2), 296–301. [CrossRef]
Figure 1.
Survival outcomes graph, by months.
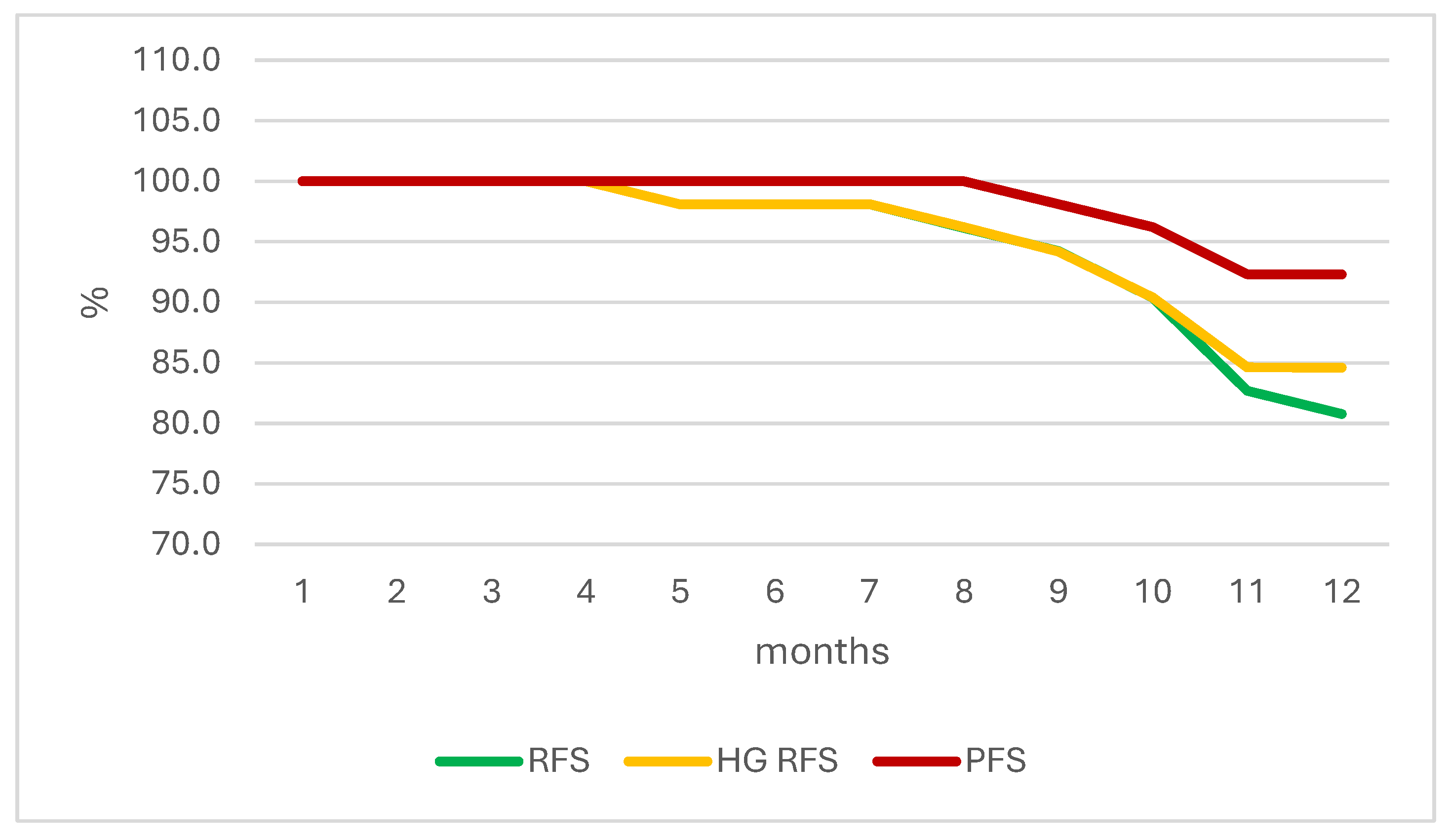
Figure 2.
Tumor recurrence compared to the initial histopathologic diagnosis.

Figure 3.
Tumor reccurence in groups with/without concomitant CIS.


Table 1.
Patient descriptive statistics.
| Valid N | Mean | Median | Minimum | Maximum | SD | |
| Age (yrs) | 52 | 69.27 | 68.20 | 44.70 | 93 | 11.45 |
| BMI | 52 | 27.55 | 26.78 | 19.15 | 41.97 | 5.09 |
| TURBT to 1st therapy (months) | 52 | 1.55 | 1.23 | 0.73 | 6.57 | 1.07 |
| SD – standard deviation; BMI – body mass index; TUR – transurethral resection of bladder cancer. | ||||||
| Sex | n | Percent | ||||
| M | 44 | 84.6 | ||||
| F | 8 | 15.4 | ||||
| Total | 52 | 100.0 | ||||
| M – male; F – female. | ||||||
| DM | n | Percent | ||||
| No | 38 | 73.1 | ||||
| Yes | 14 | 26.9 | ||||
| Total | 52 | 100.0 | ||||
| DM – diabetes mellitus. | ||||||
| LUTS | n | Percent | ||||
| No | 37 | 71.2 | ||||
| Yes | 15 | 28.8 | ||||
| Total | 52 | 100.0 | ||||
| LUTS – lower urinary tract symptoms. | ||||||
Table 2.
Hystopathology after complete TURBT.
| Histopathology | n | Percent |
| T1HG | 25 | 48.1 |
| CIS | 10 | 19.2 |
| T1HG+CIS | 17 | 32.7 |
| Total | 52 | 100.0 |
T1HG – T1 high-grade; CIS – carcinoma in situ.
Table 3.
Tumor relapse.
| Histopathology | Relapse in total | Median time to relapse (months) |
| T1HG | 3 (12%) | 11 |
| CIS | 2 (20%) | 10.5 |
| T1HG+CIS | 5 (29.4%) | 8.8 |
HG – high grade; CIS – carcinoma in situ.
Table 4.
Survival outcomes by months.
| Month of Therapy | RFS | HG RFS | PFS |
|---|---|---|---|
| 1 | 100.0 | 100.0 | 100.0 |
| 2 | 100.0 | 100.0 | 100.0 |
| 3 | 100.0 | 100.0 | 100.0 |
| 4 | 100.0 | 100.0 | 100.0 |
| 5 | 98.1 | 98.1 | 100.0 |
| 6 | 98.1 | 98.1 | 100.0 |
| 7 | 98.1 | 98.1 | 100.0 |
| 8 | 96.2 | 96.2 | 100.0 |
| 9 | 94.2 | 94.2 | 98.1 |
| 10 | 90.4 | 90.4 | 96.2 |
| 11 | 82.7 | 84.6 | 92.3 |
| 12 | 80.8 | 84.6 | 92.3 |
HG – high grade; RFS – recurrence-free survival; PFS – progression-free survival.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



