
Submitted:
29 April 2024
Posted:
30 April 2024
You are already at the latest version
Abstract
Some glucagon-like peptide-1 receptor agonists (GLP-1 RAs), first used in the treat-ment of type 2 diabetes mellitus (T2DM), have been approved for the treatment of obe-sity in patients with or without T2DM (liraglutide – LIR, semaglutide - SEM, and tir-zepatide - TIR). Social media had an important influence on the off-label use of GLP-1 RAs for obesity, especially for SEM. We analysed the Google queries related to SEM to assess people's interest in this drug. We also investigated the occurrence of adverse drug reactions (ADRs) by searching the EudraVigilance database (EV) for Individual Case Safety Reports (ICSRs) that reported SEM as the suspected drug and performed a descriptive and a disproportionality analysis. Data obtained for SEM were compared to other GLP-1 RAs. SEM had the highest proportions of searches on Google associated with the term “weight loss” and presented the lowest number of severe ADRs, but it also had the highest number of ICSRs reported in EV. Even though no unexpected safety issues have been reported for it until now, SEM has a high tendency for overdose reports. The most frequent off-label use was reported for SEM and TIR. In order to lower the ADRs’ risks, the off-label use should be reduced and carefully monitored.
Keywords:
semaglutide
; obesity
; weight loss
; overdose
; underdose
; off-label use
; EudraVigilance
; GLP-1
1. Introduction
Obesity is considered one of the most common metabolic disease, often associated with an elevated risk of developing type 2 diabetes mellitus (T2DM), non-alcoholic fatty liver disease, cardiovascular disorders, like hypertension and heart failure with preserved ejection fraction etc., thus reducing the life expectancy of patients [1,2,3,4].
Recent studies show that obesity increases the number of hospitalizations, the need for mechanical ventilation and the incidence of death in patients with SARS-CoV-2 [5].
According to the World Health Organization (WHO), in 2022, 2.5 billion adults were overweight, and of them, 890 million were obese (~12.5%). The same report pointed out that the number of overweight children under the age of 5 was 37 million. In the 5 to 19 years group, above 390 million children and teenagers were overweight, of which 160 million were obese [6].
Known as one of the biggest challenges of modern society at a global level, the fight against obesity has been declared a real public health emergency [1,5]. On the other hand, diabetes is considered one of the most widespread worldwide medical conditions and T2DM is the most common form [7] with both acute and chronic consequences which decrease the quality of life, reduce life expectancy and increase the mortality rate [8].
One of the global goals of WHO is to stop the increase in diabetes and obesity by 2025 [6]. Unfortunately, until now, lifestyle changes in terms of daily diet and physical exercise have often proved insufficient to achieve significant weight loss [7,9]. The connection between obesity and diabetes is very close, so a large part of obese people are affected by diabetes or have a very high risk of developing T2DM in a very short period, and many patients with diabetes, especially those with T2DM, start to gain weight, soon becoming overweight or obese [10].
Significant evidence attests that an effective improvement of insulin sensitivity and at the same time reducing the risk of diabetes associated with obesity can be achieved through weight loss [10]. Over time, several molecules have been administered for the treatment of obesity, but their limited efficacy and/or adverse reactions led to the limitation of their use or even their withdrawal from the market (e.g. sibutramine, amfepramone, rimonabant, benfluorex, dexfenfluramine etc.) [5,11,12,13]. In this context, the approval of new drugs with adequate efficiency and safety in obesity treatment has been sought. Thus, the approval of the first glucagon-like peptide-1 (GLP-1) receptors agonist (GLP-1 RAs), with similar structures with endogenous hormone, in the treatment of T2DM opened a new era in promoting weight loss and improving health outcomes in obese people, including those with comorbidities [14].
GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) are two of the main incretin peptide hormones excreted in the intestinal tract [15], responsible for increasing the secretion of insulin after eating food and also inhibiting the secretion of glucagon [16,17,18,19]. GLP-1 reduces gastrointestinal motility, which in turn extends the period when nutrients might be absorbed. It also determines the feeling of satiety, enhances resting metabolic rate, and decreases free fatty acid concentrations in plasma [20]. Extra-pancreatic effects of GLP-1 include delayed gastric emptying [21] thus reducing the amount of food ingested and suppressing the appetite [19] by increasing satiety, reducing glycosylated haemoglobin A1c (HbA1c) in patients with T2DM. These effects determined that the use of GLP-1 RAs has a high potential to reduce body weight and to be considered for the treatment of obesity [15] (Figure 1). In addition, their clinical use for the treatment of T2DM and obesity has increased interest in the way in which physiological and pharmacological levels of GLP-1 behave on essential tissues important to the pathophysiology of diabetes and its complications. [17,22]. Preclinical studies have shown that GIP can decrease body weight by diminishing food intake and enhancing energy expenditure and, in combination with GLP-1 RAs, can have a greater lowering effect on blood glucose and body weight in patients [19,20].
GLP-1 RAs have been approved in the treatment of T2DM for improving HbA1c and for reducing the risk of major adverse cardiac events (MACE) in diabetes patients with cardiovascular risk. More recently, some of them (liraglutide – LIR, semaglutide - SEM, and tirzepatide - TIR) have been approved in chronic weight management [22,24].
On the other hand, GIP also triggers glucose-dependent insulin excretion and is responsible for a larger fraction of the incretin effect than GLP-1. Depending on glycemic status, the glucagon secretion could be increased in normoglycemic or hypoglycemic patients (glucagonotropic effect) or inhibited in hyperglycemic patients (glucagonostatic effect) [21,25,26].
Currently, there are several GLP-1 RAs approved worldwide, mainly for the treatment of diabetes and obesity, of which TIR is a novel dual GLP-1 RA and GIP receptor agonist (GIP/RAs). Exenatide (EXE) was the first GLP-1 RA in the world approved by the Food and Drug Administration (FDA), in 2005, in the treatment of T2DM, with two administrations per day, before meals [27]. Later, the European Medicines Agency (EMA) (2009) and FDA (2010) approved the second agonist, LIR, as an adjuvant to diet associated with physical exercises in patients with T2DM. Compared to its predecessor, the latter presents a longer half-life with a greater effect on the reduction of HbA1C; at the same time, it showed cardiovascular benefits in addition to its effects of lowering blood sugar. In addition, it can be administered once a day regardless of meals. Moreover, FDA (December 2014) and EMA (March 2015) approved LIR for the treatment of chronic weight management [27,28].
The short-acting time of EXE was improved by the manufacturer and a new formulation was approved in 2012 by the FDA. Compared to the old formulation, the prolonged-release suspension of EXE is administered once a week [29]. In 2014, the second GLP-1 RA with weekly administration, albiglutide (ALB), was approved by the FDA, and indicated in the treatment of T2DM in patients who cannot reach glycemic goals. In 2018, the manufacturer withdrew ALB for commercial reasons [30,31].
Also in 2014, dulaglutide (DUL) was approved by the FDA. It had the big advantage of reaching the therapeutic concentration faster compared to other GLP-1 RAs with weekly administration. SEM was launched in 2017 in injectable form, and it had an extended half-life of 7 days, and in 2019 the oral form of SEM received approval from the FDA, thus being the first oral GLP-1 RA treatment for adults with T2DM [30,32]. TIR is the latest one launched on the market, approved in 2022.
LIR was the first GLP-1 RA approved for weight loss in patients without a history of T2DM. In 2014, it was approved by the FDA in adult patients with a body mass index (BMI) larger than 30 kg/m2 on its own or with a BMI greater than 27 kg/m2 associated with at least one comorbidity related to weight, such as hypertension, diabetes, or dyslipidemia [23,33]. SEM only received approval from the FDA for weight control in 2021 [33]. In the clinical studies carried out in this respect, SEM was superior in comparison to other long-acting GLP-1 RAs from the same class, namely EXE [34] and DUL [35]. Moreover, in addition to its beneficial effects in T2DM and in controlling body weight, it also showed a significant decrease in the rates of deaths due to cardiovascular issues, non-fatal myocardial infarction and non-fatal stroke in T2DM patients at risk of cardiovascular diseases [33].
The off-label use of SEM for weight loss was promoted by social media and heavily influenced by famous public figures [7]. This intense media coverage led to numerous shortages of this drug with major consequences for patients with T2DM. Beyond these shortages, the incorrect and inadequate use of GLP-1 RAs can have major consequences on the health status of the population. Until now, various studies have shown the negative impact of these drugs [36,37,38,39]. This study aimed to identify public interest in searching for information about SEM online and also to analyse the secondary real-world data regarding the use of inadequate doses (overdose, underdose or incorrect dose) or even the off-label use of SEM. In this respect, after the analysis of data presented on the Google Trends Tool, a detailed analysis of the Individual Case Safety Reports (ICSRs) uploaded in EudraVigilance (the European adverse reaction reporting database), was carried out. The evaluation of SEM popularity and safety profile was performed by comparison with other GLP-1 RAs (including ALB, which was withdrawn from the market).
2. Materials and Methods
2.1. Study Design
The present study started with an analysis of the popularity of search queries that were entered into Google Search between December 2005 and March 2024. The data obtained from the Google Trends Tool were analysed considering peoples’ interest in searching for information about GLP-1 RAs. The interest score is presented on a scale of 0 to 100, where 100 indicates the highest level of popularity and 0 represents the least amount of interest. Subsequently, the popularity by region of each GLP-1 RAs was analysed. For each molecule, 100 points were allocated to the country with the highest popularity and to the other countries the number of points was allotted proportional to the number of searches. Furthermore, we identified the first 25 queries for each molecule and we analysed the frequency of terms related to “side effects” and “weight loss”.
A retrospective pharmacovigilance analysis was performed based on the ICSRs uploaded in the EudraVigilance database until March 31st, 2024 [40]. Firstly, a descriptive study of ICSRs reported for SEM was performed. The results obtained were compared with individual or total results obtained for all other GLP-1 RAs (ALB, DUL, EXE, LIR, lixisenatide − LIX, TIR). ALB was withdrawn by the manufacturer because of commercial reasons, not for safety or efficiency reasons. In this context, we decided to use ALB for comparison, too. On the other hand, the ICSRs reported for the combination of LIR and degludec insulin were excluded from the present study. In the next step, a disproportionality analysis was performed to compare the reporting probability of ADRs for SEM versus each GLP-1 RA and the entire group. No ethics approvals were required for the present study because no patients’ personal information was included in the ICSRs [41]. Healthcare or non-healthcare professionals fill out the reports from the European Economic Area (EEA) or non-EEA [42].
2.2. Materials
The chronologic data from Google Trends Tool reported for SEM was compared to the series of the other GLP-1 RAs. Regarding ALB and LIX, the search interest compared to SEM represents < 1%. Thus, both molecules were excluded from this analysis.
According to the Medical Dictionary for Regulatory Activities (MedDRA) hierarchy, many preferred terms (PTs) were used for reported ADRs. Each PT can describe “a symptom, sign, disease diagnosis, therapeutic indication, investigation, surgical or medical procedure, and medical social or family history characteristic”. In the next level, related PTs form the “High Level Terms” (HLT) group, and related HLTs form “High Level Group Terms” (HLGTs). The final level for classification is represented by “System Organ Classes” (SOCs), each SOC being formed from many related HLGTs [43]. At the moment, the total number of SOC is 27.
2.3. Data Analysis
A descriptive analysis of cases reported in patients treated with SEM was performed. Data were compared to other GLP-1 RAs. Based on ICSRs, the share of each GLP-1 RAs was calculated and compared. For a better evaluation, the number of ADRs was divided by the number of ICSRs uploaded in EV for each GLP-1 RA. The resulting quotient for SEM was compared with all other GLP-1 RAs. The descriptive analysis was structured taking into account the general characteristics presented in ICSR forms. In the next step, the distribution of ADRs by SOC was compared for SEM with all other GLP-1 RAs.
To evaluate the risk of incorrect dosage or off-label use, many PTs were identified for each of the 4 HLT (categories of ADRs): modified dose (11), overdose (5), underdose (10), and off-label use (9) (Table 1). The total number of ADRs for each HLT was determined and compared between SEM and all other GLP-1 RAs. Subsequently, the outcome of ADRs grouped in HLT was also compared. According to EMA rules, the outcomes cases are classified into 6 categories: (i) fatal, (ii) not recovered/not resolved (NR/NRS), (iii) recovered/resolved with sequelae, (iv) recovering/resolving, (v) recovered/resolved, (vi) not specified, (vii) unknown [45].
A disproportionality analysis was performed to evaluate the probability of reporting reactions included in the four categories. According to EMA recommendations, the reporting odds ratios (ROR) and 95% confidence intervals (95% CI) were calculated for each evaluated HLT [46]. To calculate ROR we used data representing the evaluated ADR for targeted drug (a); other ADRs for targeted drug (b); evaluated ADR for the drug used for comparison (c); other ADRs for the drug used for comparison (d). The disproportionate signal was obtained when the number of ADRs was ≥5 for each HLT and ROR was statistically >1 (lower limit of 95% CI > 1) [46]. Data calculated for SEM were compared with each other GLP-1 RA and with the entire group of all other GLP-1 RAs.
3. Results
3.1. Analysis of Searching Google Popularity
Based on the Worldwide chronologic series obtained from Google Trends, starting with May 2019, the interest in SEM showed a constantly increasing tendency. Thus, for SEM the highest level of interest was in March 2024. For other GLP-1 RAs the interest was lower than for SEM. For example, for LIR the highest number of searches was in June 2023 (7% of total searches for SEM) and for DUL was in February 2023 (3% of the total searches for SEM). Since January 2022, the search interest has been increasing for TIR, the newest molecule approved on the market from the GLP-1 RA class. Thus, in March 2024, the inquiry proportion for TIR was about 29% of total SEM searches (Figure 2). According to the same series, the search for ALB and LIX compared to SEM represents 1%. Thus, both molecules were excluded from this analysis [47].
The searches for SEM were more frequent in Puerto Rico (100), the United States (71), Australia (32), United Kingdom (26), Ireland and Canada (22). The highest level of popularity for LIR was in Qatar, for DUL in New Zealand, EXE in Qatar and Australia, and TIR in the United States (Figure 3) [47].
Regarding the terms that are most frequently searched with “semaglutide”, during the analysed period could be observed a high concern regarding “weight loss”. Thus “weight loss semaglutide” was the most frequent query for SEM. Also, other two terms were identified in the first 25 queries for SEM: “semaglutide for weight loss” and “ozempic weight loss”. An interesting observation was in TIR series, where “semaglutide weight loss” was one of the twenty-fifth more frequent terms associated with TIR queries. At the same time, people had a high interest for side effects of SEM (“side effects semaglutide”). The queries related to weight loss were more frequent than for side effects for all other GLP-1 RAs, except EXE [47].

Table 2.
Comparison between the most frequent queries related to “side effects” and “weight loss” [47].
Table 2.
Comparison between the most frequent queries related to “side effects” and “weight loss” [47].
| Terms associated with “weight loss” | Terms associated with “side effects” | |
|---|---|---|
| SEM | weight loss semaglutide | side effects semaglutide |
| semaglutide for weight loss | ||
| ozempic weight loss | ||
| LIR | liraglutide weight loss | liraglutide side effects |
| liraglutide for weight loss | ||
| TIR | tirzepatide weight loss | tirzepatide side effects |
| tirzepatide for weight loss | ||
| semaglutide weight loss | ||
| DUL | dulaglutide weight loss | dulaglutide side effects |
| EXE | exenatide weight loss | exenatide side effects |
3.2. Descriptive Analysis
3.2.1. Analysis of ICSRs
From a total number of 72,548 ICSRs uploaded in EV until March 31st, 2024 for GLP-1 RAs analysed, 21,012 ICSRs have been reported for SEM. SEM had the largest share (29.0%) of the total, followed by LIR (25.0%) and DUL (23.9%) (Figure 4).
The proportion of ADRs reported from total cases treated with SEM (1.99) is less than for the group of all other GLP-1 RAs (2.08). Also, higher proportions were observed for ALB (2.85), EXE (2.72), and LIX (2.08). Opposite, for LIR and DUL, other very used GLP-1 RAs, the proportion of ADRs from total ICSRs was lower (1.81, respectively 1.90). However, for TIR the proportion (1.98) was similar to SEM (Figure 5).
According to data published in EV, ADRs reported in the 18-64 years group of patients treated with SEM (39.7%) had a close frequency with all other GLP-1 RAs (41.8%), ALB (42.2%) and DUL (37.9%). Also, in the 65-85 years group, no high differences have been observed for SEM (21.6%) compared to the group of all other analogues (22.7%) and ALB (18.8%) (Table 3).
The most frequent cases have been reported in the female group that used SEM (57.7%) compared to the group of all other GLP-1 RAs (53.6%). Also, a similar frequency can be observed for LIR (59.8%). The most reported cases from EEA were for SEM (52.6%), similar to DUL (51.1%), but more frequent than the entire group of all other GLP-1 RAs. Healthcare professionals have been the ones to most often report ADRs related to SEM (61.3%). The same situation was noticed for all other GLP-1 RAs, except ALB (45.6%). Regarding the severity, the cases reported in EV as serious represented 74.2% (n = 38,215) of the total number related to all GLP-1 RAs. It can be noticed that serious cases reported for SEM (n = 12,029; 57.2%) had the lowest frequency compared to all other analogues (Table 3).
3.2.2. Comparative Evaluation of ADRs Grouped in SOC
Firstly, a comparison between the distribution of ADRs by SOC was conducted between SEM and all other GLP-1 RAs. Thus, it could be observed that the ADRs of SEM were most frequently reported in the following SOCs: “Gastrointestinal disorders” (25.0%; n = 10,468), “Injury, poisoning and procedural complications” (10.6%; n = 4,414), “General disorders and administration site conditions” (10.2%; n = 4,264). Similar situations were obtained for ADRs reported in SOCs “Gastrointestinal disorders” and “General disorders and administration site conditions” for all comparators. Also, in SOC “Injury, poisoning and procedural complications” similar situations were observed for ALB (11.8%) and TIR (10.0%). Among the SOCs with the lowest ADR reporting frequency were: “Congenital, familial and genetic disorders”, “Pregnancy, puerperium and perinatal conditions”, and “Social circumstances” (Figure 6).
3.2.3. ADRs Reported for Incorrect Dosage
Figure 7 presents the frequency of ADRs related to dosage in GLP-1 RAs class. Thus, for SEM the most frequent are ADRs related to improper dose (0.79%), a percentage higher than for DUL (0.68%), TIR (0.52%), and LIR (0.49%), but lower than for EXE (1.90%) and the entire group of all other analogues (1.02%). Overdoses have been reported for SEM (0.59%) with a lower frequency than for DUL (0.66%), but higher than for all other comparators. Underdoses have the lowest frequency (0.33%) in HLTs related to the dosage of SEM. This percentage is similar to LIR (0.32%) and inferior to all other comparators.
3.2.4. ADRs Reported as “Off-Label Use”
According to Figure 8, for the ADRs reported for off-label use, their frequency in SEM series (6.16%) is similar to TIR (6.08%), but higher than other comparators, including the entire group of all other GLP-1 RAs.
3.2.5. Distribution of ADRs by Outcome
ADRs Reported for SEM
Regarding the outcomes, Figure 9 shows that unfavourable outcomes were reported as follows: (i) 4 cases related to overdoses were fatal; (ii) 41 cases related to incorrect dosage were not recovered or not resolved (23 for improper doses; 9 for overdosage, respectively 9 for under dosage); (iii) 356 cases related to off-label use were not recovered or not resolved.
The Frequency of ADRs with Unfavourable Outcomes Reported for SEM Compared to All Other GLP-1 RAs
The unfavourable outcomes of cases reported in EV (fatal or not recovered / not resolved) are represented below. Thus, Figure 10a presents the frequency of fatal ADRs reported for incorrect dosage. Fatal ADRs were reported only for overdosage, with a higher frequency in LIR series (2.7%) than for SEM (1.6%). Also, for off-label use, no fatal ADRs were reported for any GLP-1 RAs.
The frequency of not recovered / not resolved outcomes is presented in Figure 10b. According to this data, SEM presented a higher frequency in all three HLT, compared with all other GLP-1 RAs, with the following exceptions (Figure 10b):
- improper doses: SEM – 7.0% and EXE – 8.4%
- overdose: SEM - 3.7% and EXE – 8.2%
- underdose: SEM – 6.6%, EXE – 9.7%, and LIR – 6.8%
Regarding the frequency of not recovered / not resolved ADRs related to off-label use, SEM (7.2%) had also a higher frequency of reporting compared to other GLP-1 RAs, except EXE (17,8%) (Figure 10c).
3.3. Disproportionality Analysis
3.3.1. Incorrect Doses
According to data published in EV, the results of disproportionality analysis show a higher probability of reporting ADRs related to improper doses for SEM compared to LIR (ROR: 1.6169, 95% CI: 1.3379 – 1.9542) and TIR (ROR: 1.5200, 95% CI: 1.0032 – 2.3031). Also in Figure 11a, a lower probability of ADRs for SEM compared to EXE (ROR: 0.4087, 95% CI: 0.3579 – 0.4667) and the entire group of all other GLP-1 RAs (ROR: 0.7722, 95% CI: 0.6823 – 0.8740) could be observed. No difference could be observed for SEM compared to DUL and ALB.
For ADRs related to overdose, SEM had a higher probability of reporting compared to EXE (ROR: 2.4174, 95% CI: 1.8878 – 3.0956), LIR (ROR: 1.7434, 95% CI: 1.3913 – 2.1845), and TIR (ROR: 3.3868, 95% CI: 1.6736 – 6.8535). The same results could be noticed by comparison with the group of all other GLP-1 RAs (ROR: 1.4764, 95% CI: 1.2608 – 1.7288). Also, compared to DUL no difference could be noticed (Figure 11b).
If for overdosage, SEM had a higher probability of reporting, for under-dosage the situation is reversed. Thus, no difference could be observed by comparison with LIR and LIX, but a lower probability of reporting could be observed by comparison with all other analogues and with the entire group of all other GLP-1 RAs (Figure 11c).
3.3.2. Off-Label Use
Figure 12 showed a higher probability of reporting off-label use for SEM compared to all other analogues, except TIR: ALB (ROR: 4.4375, 95% CI: 2.6615 – 7.3988), DUL (ROR: 8.3830, 95% CI: 7.3359 – 9.5796), EXE (ROR: 2.9018, 95% CI: 2.6680 – 3.1560), LIR (ROR: 2.8377, 95% CI: 2.6052 – 3.0910), and LIX (ROR: 6.5330, 95% CI: 3.2525 – 13.1221). Also, compared to the group of all other GLP-1 RAs the probability of reporting is higher (ROR: 3.3226; 95% CI: 3.1270 – 3.5304).
4. Discussion
Reduced appetite and food intake were observed after GLP-1 RAs administration. Thus, their benefits in weight loss are exploited by using them in obese patients with or without diabetes [48]. Improving the patients’ adherence to GLP-1 RAs treatment by possible oral administration [49] was an important objective of the researchers following their approval on the market. Only a few years after the EXE approval in therapy, new molecules have been authorised. SEM presents some differences in pharmacokinetics due to the modifications in GLP-1 structure: (i) improved stability against dipeptide-peptidase-4 enzyme (DPP-4) by substitution of alanine with aminoisobutyric acid; (ii) increased binding to albumin by introducing of a linker and a C18 di-acid chain; (iii) preventing the binding of fatty acid at the wrong site by substitution of Lys with Arg [50]. On the other hand, to improve the patients' adherence to SEM, its absorption across gastric mucosa was improved by obtaining a co-formulation with sodium N-(8-[2-hydroxybenzoyl]amino)caprylate. Based on this formulation, SEM was the first GLP-1 RAs suitable for oral administration [51]. Thus, SEM was expected to be very popular in the media and widely used in therapy, often as off-label or as auto medication. Because of this issue, the dosing errors were expected to be quite frequent.
The first item analyzed was the popularity of SEM in Google searches. The term “weight loss semaglutide” was the most frequently used. Also, the queries related to weight loss have a higher frequency for the other GLP-1 RAs. Additionally, the search interest on Google for each molecule was related in a smaller frequency with the side effects. Based on this information, it could be considered that the people interested in these molecules had a similar search behaviour regarding the safety of the products. Our results are comparable to the ones in the study performed by Han et al., which showed that the greatest relative search was obtained for one of the SEM brand names [7]. Also, a study published in 2024 showed that SEM was one of the most popular pharmacological and surgical obesity methods searched on Google [52]. The popularity of SEM on TikTok (an online social media platform), is also very high. 57 of the first 100 video searches under the hashtag “#Ozempic” were related to “weight loss” (44 million views), and 29 of 100 were related to “common side effects, toxicity” (24 million views). The “off-label” use was a search term only in 3 of 100 videos (2.8 million views) [53].
Although SEM was approved on the market more recently than LIR, DUL, EXE, and ALB, the descriptive analysis showed the highest number of ICSRs reported in EV (29% of the total). Its popularity and indication in obesity could contribute to an increase in the prescription numbers and implicitly in its consumption. In 2022, the global market of SEM and LIR increased by 43% from 9.9 to 14.2 billion USD [54]. Moreover, according to a study published in 2023, prescriptions for SEM increased by 150% / year [55]. This increase could be justified by a higher efficiency of SEM in weight loss and by a lower cost of treatment [56,57]. Other studies showed superior efficiency of SEM compared to LIX [58], EXE [58,59], DUL [59] and, LIR [60]. For example, SEM led to an average reduction of body weight of 12.4% in 68 weeks compared to LIR (-5.4% in 56 weeks) [60]. Therefore, SEM had an improved value for money in weight reduction compared with LIR (estimated cost of 1845 USD per 1% reduction in body weight for SEM, compared to 3256 USD for LIR) [60].
Regarding the demographic characteristics of patients, in the present study, most of the reports were in the 18-64 years group. Also, the most frequent reports were for females (57.7%), similar to the results of another study performed on the data from the Food and Drug Administration Adverse Event Reporting System (FAERS) between 2018–2022 (54.4%) [61].
According to the present study, SEM had the lowest number of severe ADRs compared to the analysed molecules. These results are similar to other studies that reported a safety profile consistent with other GLP-1RAs, with a low incidence of severe ADRs for SEM [59,62,63]. Generally, SEM is well tolerated, and most ADRs induced are mild-to-moderate and transient. Although a fatal outcome was reported only for overdosing on SEM and LIR. Anyway, until now, no unexpected safety issues have been reported for SEM [62,63]. However, another interesting result of the present study suggests that SEM had a higher number of ADRs reported by each case than DUL and LIR, and similar with TIR. Considering that TIR was recently authorized, it is expected that this situation will be different over time.
This study revealed a higher tendency to report ADRs related to overdosing of SEM (except DUL and EXE), and incorrect dosing compared to LIR and TIR. According to the American Association of Poison Control Centers, a total of 2941 cases related to SEM overdosing were reported between January – November 2023, more than double compared to 2022 [64]. The overdosing cases reported in the scientific literature were associated with notable gastrointestinal symptoms, even with medical evaluation and treatment with antiemetics and intravenous fluids [65,66].
On the other hand, the off-label use of SEM was more frequently reported in EV than other GLP-1 RAs (except TIR). Probably, its advantages (high efficiency and safety, improved value for money in weight reduction, and increased benefits-risk ratio) represent factors for increasing the off-label use of SEM. According to the study performed by Chiappini et al., off-label use of SEM was the fifth most frequent cause of reporting in FAERS (6%) [61].
Finally, media attention fuels the demand for this type of medication and, at the same time, generates an increase in illegal sales. Thus, the authorities in countries such as Austria, Denmark, Great Britain, Ireland, Switzerland, etc. seek to repress illegal activity with these drugs, approaching different methods of social media monitoring, even reporting the confiscation of falsified pens with SEM in some EEA states [67]. Moreover, both manufacturers and regulatory agencies in the field of medicine issued warnings about the penetration of counterfeit products into the drug supply chain, finding them in retail pharmacies [68,69,70]. In this context, greater attention must be paid, both to the way of prescribing and also to the counselling of patients regarding the identification of fakes and the judicious use of medicines.
Limitations of the Study
Certain limitations should be considered for this study. Our searches included only active pharmaceutical ingredients. The online environment is extensive; besides Google, other search engines and social media platforms are widely used. We acknowledge that these results may not offer the full depiction of the off-label use for weight loss phenomenon. Some ADRs from the EudraVigilance spontaneous reporting system are related to the low reporting rate or to the inaccuracy of the information contained in the reports. The number of ADRs reported could be influenced by the extent of drug use, the awareness of the reporter, the severity and outcome of the reaction, etc. Moreover, information such as concomitant medication or other suspected drugs, comorbidities, medical status, etc. could be missing, thus affecting this analysis. Other limitations are the lack of a denominator or the lack of certainty of a causal relationship between the reported ADRs and the suspected drug. Not at least, off-label use could be a factor in the underreporting of adverse drug reactions. Further studies are needed for an extensive evaluation of the safety profile of SEM and other GLP-1 RAs.
5. Conclusions
Our study highlights the SEM risk of improper or off-label use and completes the information presented in the main information flux. To reduce these risks, especially of severe ADRs or unfavourable outcomes, stakeholders should promote the correct use and dispensing of drugs based on semaglutide. Also, an increased carefulness of patient counselling could improve healthcare outcomes. Likewise, new studies must be performed to obtain information regarding dosing errors or off-label use. The information obtained from such studies does not provide a clear picture of what is meant by modified dose, underdose, overdose and off-label use of a medicinal substance, but based on the signals detected following the analysis of ICSRs and the results obtained following the analysis compared to other substances or similar substances, useful information can be provided for clinical practice in monitoring and managing adverse effects and possible events related to abuse.
Author Contributions
Conceptualization A.B., C.D., A.A., C.M., A.F. and L.V.; methodology, A.B., C.D., A.A., C.M., L.R., S.G, A.J., F.G. and L.V.; software, A.B., C.D., A.A., A.M., A.L., C.M., and A.F. validation, A.B., C.D., A.A., S.G., C.M., and L.V.; formal analysis, A.B., A.A., C.D., C.M., L.R., S.G, A.M., F.G. and L.V.; investigation, A.B., A.M., A.C., A.J., A.L., C.M., and L.V.; data curation, A.B., C.D., A.A., S.G., C.M., L.R. and L.V.; resources, A.B., C.D., A.F. and L.V.; writing—original draft preparation, A.B., C.D., A.A., A.F., A.C., C.M. and L.V.; writing—review and editing, A.B., C.D., A.A., A.F., A.C., L.R., A.M., A.L., C.M. and L.V.; visualization, A.B., C.D., A.A., A.F., A.C., L.R., A.J., A.M., S.G., A.L., F.G., C.M. and L.V.; supervision, A.A., S.G., F.G., C.M. and L.V. All authors have read and agreed to the published version of the manuscript.
Funding
Project financed by Lucian Blaga University of Sibiu through the research grant LBUS-IRG-2023/No. 3523, 24 July 2023.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Prasad-Reddy, L.; Isaacs, D. A Clinical Review of GLP-1 Receptor Agonists: Efficacy and Safety in Diabetes and Beyond. Drugs Context 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.D.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Stoicescu, L.; Crişan, D.; Morgovan, C.; Avram, L.; Ghibu, S. Heart Failure with Preserved Ejection Fraction: The Pathophysiological Mechanisms behind the Clinical Phenotypes and the Therapeutic Approach. Int. J. Mol. Sci. 2024, Vol. 25, Page 794 2024, 25, 794. [Google Scholar] [CrossRef] [PubMed]
- Pop, C.; Ștefan, M.G.; Muntean, D.M.; Stoicescu, L.; Gal, A.F.; Kiss, B.; Morgovan, C.; Loghin, F.; Rochette, L.; Lauzier, B.; et al. Protective Effects of a Discontinuous Treatment with Alpha-Lipoic Acid in Obesity-Related Heart Failure with Preserved Ejection Fraction, in Rats. Antioxidants 2020, Vol. 9, Page 1073 2020, 9, 1073. [Google Scholar] [CrossRef] [PubMed]
- Qin, W.; Yang, J.; Deng, C.; Ruan, Q.; Duan, K. Efficacy and Safety of Semaglutide 2.4 Mg for Weight Loss in Overweight or Obese Adults without Diabetes: An Updated Systematic Review and Meta-Analysis Including the 2-Year STEP 5 Trial. Diabetes. Obes. Metab. 2024, 26, 911–923. [Google Scholar] [CrossRef] [PubMed]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 11 April 2024).
- Han, S.H.; Safeek, R.; Ockerman, K.; Trieu, N.; Mars, P.; Klenke, A.; Furnas, H.; Sorice-Virk, S. Public Interest in the Off-Label Use of Glucagon-like Peptide 1 Agonists (Ozempic) for Cosmetic Weight Loss: A Google Trends Analysis. Aesthetic Surg. J. 2023, 44, 60–67. [Google Scholar] [CrossRef]
- Morgovan, C.; Cosma, S.A.; Valeanu, M.; Juncan, A.M.; Rus, L.L.; Gligor, F.G.; Butuca, A.; Tit, D.M.; Bungau, S.; Ghibu, S. An Exploratory Research of 18 Years on the Economic Burden of Diabetes for the Romanian National Health Insurance System. Int. J. Environ. Res. Public Heal. 2020, Vol. 17, Page 4456 2020, 17, 4456. [Google Scholar] [CrossRef] [PubMed]
- Chiappini, S.; Vickers-Smith, R.; Harris, D.; Papanti Pelletier, G.D.; Corkery, J.M.; Guirguis, A.; Martinotti, G.; Sensi, S.L.; Schifano, F. Is There a Risk for Semaglutide Misuse? Focus on the Food and Drug Administration’s FDA Adverse Events Reporting System (FAERS) Pharmacovigilance Dataset. Pharm. 2023, Vol. 16, Page 994 2023, 16, 994. [Google Scholar] [CrossRef]
- Larsen, P.J. Mechanisms behind GLP-1 Induced Weight Loss. 2008, 8, S34–S41. [Google Scholar] [CrossRef]
- Onakpoya, I.J.; Heneghan, C.J.; Aronson, J.K. Post-Marketing Withdrawal of Anti-Obesity Medicinal Products Because of Adverse Drug Reactions: A Systematic Review. BMC Med. 2016, 14. [Google Scholar] [CrossRef]
- Czernichow, S.; Batty, D. Withdrawal of Sibutramine for Weight Loss: Where Does This Leave Clinicians? Obes. Facts 2010, 3, 155. [Google Scholar] [CrossRef] [PubMed]
- EMA Confirms Recommendation to Withdraw Marketing Authorisations for Amfepramone Medicines | European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/ema-confirms-recommendation-withdraw-marketing-authorisations-amfepramone-medicines-0 (accessed on 11 April 2024).
- Waldrop, S.W.; Johnson, V.R.; Stanford, F.C. Inequalities in the Provision of GLP-1 Receptor Agonists for the Treatment of Obesity. Nat. Med. 2024 301 2024, 30, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Rohani, P.; Malekpour Alamdari, N.; Bagheri, S.E.; Hekmatdoost, A.; Sohouli, M.H. The Effects of Subcutaneous Tirzepatide on Obesity and Overweight: A Systematic Review and Meta-regression Analysis of Randomized Controlled Trials. Front. Endocrinol. (Lausanne). 2023, 14, 1230206. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Verma, S.; Vaidya, S.; Kalia, K.; Tiwari, V. Recent Updates on GLP-1 Agonists: Current Advancements & Challenges. Biomed. Pharmacother. 2018, 108, 952–962. [Google Scholar] [CrossRef]
- McLean, B.A.; Wong, C.K.; Campbell, J.E.; Hodson, D.J.; Trapp, S.; Drucker, D.J. Revisiting the Complexity of GLP-1 Action from Sites of Synthesis to Receptor Activation. Endocr. Rev. 2021, 42, 101–132. [Google Scholar] [CrossRef] [PubMed]
- Vosoughi, K.; Salman Roghani, R.; Camilleri, M. Effects of GLP-1 Agonists on Proportion of Weight Loss in Obesity with or without Diabetes: Systematic Review and Meta-Analysis. Obes. Med. 2022, 35, 100456. [Google Scholar] [CrossRef]
- Evolution of GLP-1 Receptor Agonists for Diabetes Treatment | Biopharma PEG. Available online: https://www.biochempeg.com/article/299.html (accessed on 11 April 2024).
- Prasad-Reddy, L.; Isaacs, D. A Clinical Review of GLP-1 Receptor Agonists: Efficacy and Safety in Diabetes and Beyond. Drugs Context 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.; Raj, R.; Elshimy, G.; Zapata, I.; Kannan, L.; Majety, P.; Edem, D.; Correa, R. Adverse Events Related to Tirzepatide. J. Endocr. Soc. 2023, 7. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycaemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetol. 2022 6512 2022, 65, 1925–1966. [Google Scholar] [CrossRef]
- Tilinca, M.C.; Tiuca, R.A.; Burlacu, A.; Varga, A. A 2021 Update on the Use of Liraglutide in the Modern Treatment of ‘Diabesity’: A Narrative Review. Med. 2021, 57. [Google Scholar] [CrossRef]
- Taylor, S.I. GLP-1 Receptor Agonists: Differentiation within the Class. Lancet Diabetes Endocrinol. 2018, 6, 83–85. [Google Scholar] [CrossRef]
- Blonde, L.; Umpierrez, G.E.; Reddy, S.S.; McGill, J.B.; Berga, S.L.; Bush, M.; Chandrasekaran, S.; DeFronzo, R.A.; Einhorn, D.; Galindo, R.J.; et al. American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan-2022 Update. Endocr. Pract. 2022, 28, 923–1049. [Google Scholar] [CrossRef]
- Committee, A.D.A.P.P. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S125–S143. [Google Scholar] [CrossRef] [PubMed]
- Blind, E.; Janssen, H.; Dunder, K.; de Graeff, P.A. The European Medicines Agency’s Approval of New Medicines for Type 2 Diabetes. Diabetes. Obes. Metab. 2018, 20, 2059. [Google Scholar] [CrossRef] [PubMed]
- Iepsen, E.W.; Torekov, S.S.; Holst, J.J. Liraglutide for Type 2 Diabetes and Obesity: A 2015 Update. Expert Rev. Cardiovasc. Ther. 2015, 13, 753–767. [Google Scholar] [CrossRef]
- Acosta, A.; Camilleri, M.; Burton, D.; O’Neill, J.; Eckert, D.; Carlson, P.; Zinsmeister, A.R. Exenatide in Obesity with Accelerated Gastric Emptying: A Randomized, Pharmacodynamics Study. Physiol. Rep. 2015, 3. [Google Scholar] [CrossRef]
- Chudleigh, R.A.; Platts, J.; Bain, S.C. Comparative Effectiveness of Long-Acting GLP-1 Receptor Agonists in Type 2 Diabetes: A Short Review on the Emerging Data. Diabetes, Metab. Syndr. Obes. Targets Ther. 2020, 13, 433. [Google Scholar] [CrossRef] [PubMed]
- UK Government Letters Sent to Healthcare Professionals in September 2017 - GOV.UK. Available online: https://www.gov.uk/drug-safety-update/letters-sent-to-healthcare-professionals-in-september-2017 (accessed on 11 April 2024).
- Hughes, S.; Neumiller, J.J. Oral Semaglutide. Clin. Diabetes 2020, 38, 109. [Google Scholar] [CrossRef]
- Singh, G.; Krauthamer, M.; Bjalme-Evans, M. Wegovy (Semaglutide): A New Weight Loss Drug for Chronic Weight Management. J. Investig. Med. 2022, 70, 5–13. [Google Scholar] [CrossRef]
- Ahmann, A.J.; Capehorn, M.; Charpentier, G.; Dotta, F.; Henkel, E.; Lingvay, I.; Holst, A.G.; Annett, M.P.; Aroda, V.R. Efficacy and Safety of Once-Weekly Semaglutide Versus Exenatide ER in Subjects With Type 2 Diabetes (SUSTAIN 3): A 56-Week, Open-Label, Randomized Clinical Trial. Diabetes Care 2018, 41, 258–266. [Google Scholar] [CrossRef]
- Pratley, R.E.; Aroda, V.R.; Lingvay, I.; Lüdemann, J.; Andreassen, C.; Navarria, A.; Viljoen, A. Semaglutide versus Dulaglutide Once Weekly in Patients with Type 2 Diabetes (SUSTAIN 7): A Randomised, Open-Label, Phase 3b Trial. lancet. Diabetes Endocrinol. 2018, 6, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, Q.; Tan, Y.; Chen, Y.; Zhou, X.; Liu, S.; Yu, J. GLP-1RAs Caused Gastrointestinal Adverse Reactions of Drug Withdrawal: A System Review and Network Meta-Analysis. Front. Endocrinol. (Lausanne). 2023, 14, 1149328. [Google Scholar] [CrossRef]
- Sodhi, M.; Rezaeianzadeh, R.; Kezouh, A.; Etminan, M. Risk of Gastrointestinal Adverse Events Associated With Glucagon-Like Peptide-1 Receptor Agonists for Weight Loss. JAMA 2023, 330, 1795–1797. [Google Scholar] [CrossRef]
- Shetty, R.; Basheer, F.T.; Poojari, P.G.; Thunga, G.; Chandran, V.P.; Acharya, L.D. Adverse Drug Reactions of GLP-1 Agonists: A Systematic Review of Case Reports. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102427. [Google Scholar] [CrossRef]
- Filippatos, T.D.; Panagiotopoulou, T. V.; Elisaf, M.S. Adverse Effects of GLP-1 Receptor Agonists. Rev. Diabet. Stud. 2014, 11, 202. [Google Scholar] [CrossRef]
- European Database of Suspected Adverse Drug Reaction Reports. Available online: https://www.adrreports.eu/ (accessed on 11 April 2024).
- Postigo, R.; Brosch, S.; Slattery, J.; van Haren, A.; Dogné, J.M.; Kurz, X.; Candore, G.; Domergue, F.; Arlett, P. EudraVigilance Medicines Safety Database: Publicly Accessible Data for Research and Public Health Protection. Drug Saf. 2018, 41, 665–675. [Google Scholar] [CrossRef]
- Medicines Agency, E. Guideline on Good Pharmacovigilance Practices (GVP) - Product- or Population-Specific Considerations IV: Paediatric Population. 2018. [Google Scholar]
- Guo, Y.; Shen, Z.; Zhao, W.; Lu, J.; Song, Y.; Shen, L.; Lu, Y.; Wu, M.; Shi, Q.; Zhuang, W.; et al. Rational Identification of Novel Antibody-Drug Conjugate with High Bystander Killing Effect against Heterogeneous Tumors. Adv. Sci. 2024, 11. [Google Scholar] [CrossRef] [PubMed]
- Morgovan, C.; Dobrea, C.M.; Chis, A.A.; Juncan, A.M.; Arseniu, A.M.; Rus, L.L.; Gligor, F.G.; Ardelean, S.A.; Stoicescu, L.; Ghibu, S.; et al. A Descriptive Analysis of Direct Oral Anticoagulant Drugs Dosing Errors Based on Spontaneous Reports from the EudraVigilance Database. Pharm. 2023, Vol. 16, Page 455 2023, 16, 455. [Google Scholar] [CrossRef] [PubMed]
- Medicines Agency, E. Note for Guidance-EudraVigilance Human-Processing of Safety Messages and Individual Case Safety Reports (ICSRs). 2010. [Google Scholar]
- Medicines Agency, E. GUIDELINE ON THE USE OF STATISTICAL SIGNAL DETECTION METHODS IN THE EUDRAVIGILANCE DATA ANALYSIS SYSTEM. 2006. [Google Scholar]
- Google Trends: Semaglutide, Liraglutide, Tirzepatide, Dulaglutide, Exenatide. Available online: https://trends.google.com/trends/explore?date=2005-12-01 2024-03-31&q=semaglutide,liraglutide,tirzepatide,dulaglutide,exenatide&hl=ro (accessed on 20 April 2024).
- Popoviciu, M.S.; Păduraru, L.; Yahya, G.; Metwally, K.; Cavalu, S. Emerging Role of GLP-1 Agonists in Obesity: A Comprehensive Review of Randomised Controlled Trials. Int. J. Mol. Sci. 2023, 24. [Google Scholar] [CrossRef]
- Isaacs, D.M.; Kruger, D.F.; Spollett, G.R. Optimizing Therapeutic Outcomes With Oral Semaglutide: A Patient-Centered Approach. Diabetes Spectr. 2021, 34, 7. [Google Scholar] [CrossRef]
- Kalra, S.; Sahay, R. A Review on Semaglutide: An Oral Glucagon-Like Peptide 1 Receptor Agonist in Management of Type 2 Diabetes Mellitus. Diabetes Ther. 2020, 11, 1965–1982. [Google Scholar] [CrossRef] [PubMed]
- Aroda, V.R.; Blonde, L.; Pratley, R.E. A New Era for Oral Peptides: SNAC and the Development of Oral Semaglutide for the Treatment of Type 2 Diabetes. Rev. Endocr. Metab. Disord. 2022, 23, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Kamiński, M.; Miętkiewska-Dolecka, M.; Kręgielska-Narożna, M.; Bogdański, P. Popularity of Surgical and Pharmacological Obesity Treatment Methods Searched by Google Users: The Retrospective Analysis of Google Trends Statistics in 2004–2022. Obes. Surg. 2024, 34, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Basch, C.H.; Narayanan, S.; Tang, H.; Fera, J.; Basch, C.E. Descriptive Analysis of TikTok Videos Posted under the Hashtag #Ozempic. J. Med. Surgery, Public Heal. 2023, 1, 100013. [Google Scholar] [CrossRef]
- Liraglutide and Semaglutide Market Share Report, 2023-2032. Available online: https://www.gminsights.com/industry-analysis/liraglutide-and-semaglutide-market (accessed on 14 April 2024).
- Miriam, E. Tucker Semaglutide Prescribing Surged in the Past Year. Available online: https://www.medscape.com/viewarticle/997956?form=fpf (accessed on 14 April 2024).
- Patoulias, D.; Popovic, D.S.; Stoian, A.P.; Janez, A.; Sahebkar, A.; Rizzo, M. Effect of Semaglutide versus Other Glucagon-like Peptide-1 Receptor Agonists on Cardio-Metabolic Risk Factors in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Head-to-Head, Phase 3, Randomized Controlled Trials. J. Diabetes Complications 2023, 37, 108529. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Lin, Y.H.; Dai, L.Z.; Lin, C.S.; Huang, Y.; Liu, S.Y. Efficacy and Safety of GLP-1 Receptor Agonists versus SGLT-2 Inhibitors in Overweight/Obese Patients with or without Diabetes Mellitus: A Systematic Review and Network Meta-Analysis. BMJ Open 2023, 13, e061807. [Google Scholar] [CrossRef] [PubMed]
- Chubb, B.; Gupta, P.; Gupta, J.; Nuhoho, S.; Kallenbach, K.; Orme, M. Once-Daily Oral Semaglutide Versus Injectable GLP-1 RAs in People with Type 2 Diabetes Inadequately Controlled on Basal Insulin: Systematic Review and Network Meta-Analysis. Diabetes Ther. 2021, 12, 1325. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, X.Z.; Chen, J.Q.; Ren, T.S.; Zhang, Y.S.; Wang, Y.N.; Zhao, Q.C. Comparative Efficacy and Safety of Glucagon-like Peptide 1 Receptor Agonists for the Treatment of Type 2 Diabetes: A Network Meta-Analysis. Medicine (Baltimore). 2023, 102, E34122. [Google Scholar] [CrossRef] [PubMed]
- Azuri, J.; Hammerman, A.; Aboalhasan, E.; Sluckis, B.; Arbel, R. Liraglutide versus Semaglutide for Weight Reduction—a Cost Needed to Treat Analysis. Obesity 2023, 31, 1510–1513. [Google Scholar] [CrossRef]
- Chiappini, S.; Vickers-Smith, R.; Harris, D.; Papanti Pelletier, G.D.; Corkery, J.M.; Guirguis, A.; Martinotti, G.; Sensi, S.L.; Schifano, F. Is There a Risk for Semaglutide Misuse? Focus on the Food and Drug Administration’s FDA Adverse Events Reporting System (FAERS) Pharmacovigilance Dataset. Pharmaceuticals 2023, 16, 1–13. [Google Scholar] [CrossRef]
- Smits, M.M.; Van Raalte, D.H. Safety of Semaglutide. Front. Endocrinol. (Lausanne). 2021, 12, 645563. [Google Scholar] [CrossRef] [PubMed]
- Amaro, A.; Sugimoto, D.; Wharton, S. Efficacy and Safety of Semaglutide for Weight Management: Evidence from the STEP Program. Postgrad. Med. 2022, 134, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Poison Centers See Nearly 1,500% Increase in Calls Related to Injected Weight-Loss Drugs as People Accidentally Overdose | CNN. Available online: https://edition.cnn.com/2023/12/13/health/semaglutide-overdoses-wellness/index.html (accessed on 14 April 2024).
- Lambson, J.E.; Flegal, S.C.; Johnson, A.R. Administration Errors of Compounded Semaglutide Reported to a Poison Control Center—Case Series. J. Am. Pharm. Assoc. 2023, 63, 1643–1645. [Google Scholar] [CrossRef] [PubMed]
- Wiener, B.G.; Gnirke, M.; Vassallo, S.; Smith, S.W.; Su, M.K. Challenges with Glucagon-like Peptide-1 (GLP-1) Agonist Initiation: A Case Series of Semaglutide Overdose Administration Errors. Clin. Toxicol. 2024, 1–3. [Google Scholar] [CrossRef]
- Surge in Fake Ozempic Reveals Dark Side of Weight-Loss Frenzy. Available online: https://medwatch.com/News/other/article16935969.ece (accessed on 16 April 2024).
- News Details. Available online: https://www.novonordisk-us.com/media/news-archive/news-details.html?id=166119 (accessed on 16 April 2024).
- Counterfeit Ozempic Found in US Retail Pharmacy - National Association of Boards of Pharmacy. Available online: https://nabp.pharmacy/news/blog/regulatory_news/counterfeit-ozempic-found-in-us-retail-pharmacy/ (accessed on 16 April 2024).
- EMA Alerts EU Patients and Healthcare Professionals to Reports of Falsified Ozempic Pens | European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/ema-alerts-eu-patients-healthcare-professionals-reports-falsified-ozempic-pens (accessed on 16 April 2024).
Figure 1.
The main biological activities of GLP-1 RAs [23]. SBP – systolic blood pressure; HR – heart rate; MC – myocardial contractility; ↑ – increase; ↓ – decrease.
Figure 1.
The main biological activities of GLP-1 RAs [23]. SBP – systolic blood pressure; HR – heart rate; MC – myocardial contractility; ↑ – increase; ↓ – decrease.
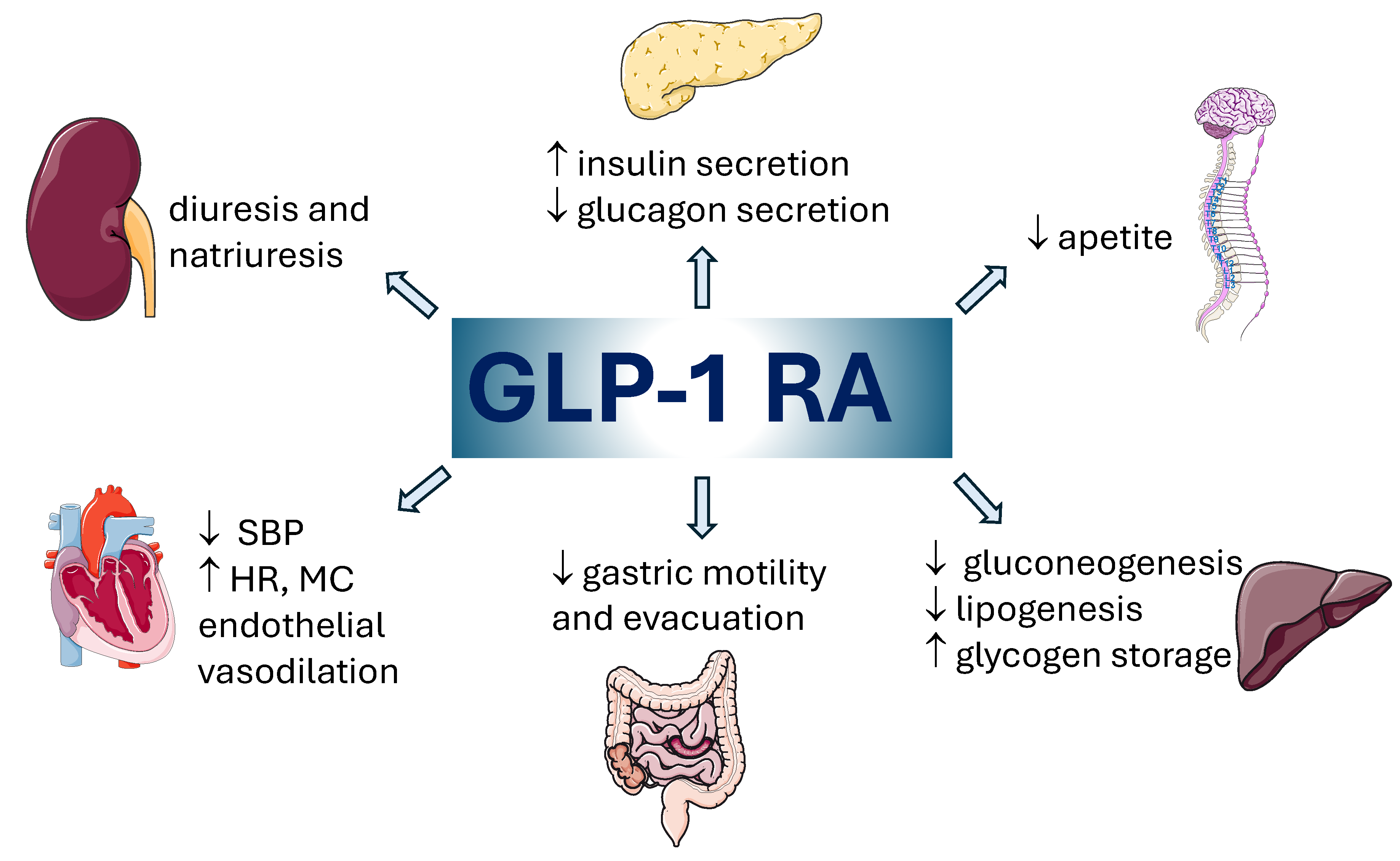
Figure 2.
Comparison regarding the search interest related to GLP-1 RAs, according to Google Trends Tool (December 2005 – March 2024) [47].
Figure 2.
Comparison regarding the search interest related to GLP-1 RAs, according to Google Trends Tool (December 2005 – March 2024) [47].
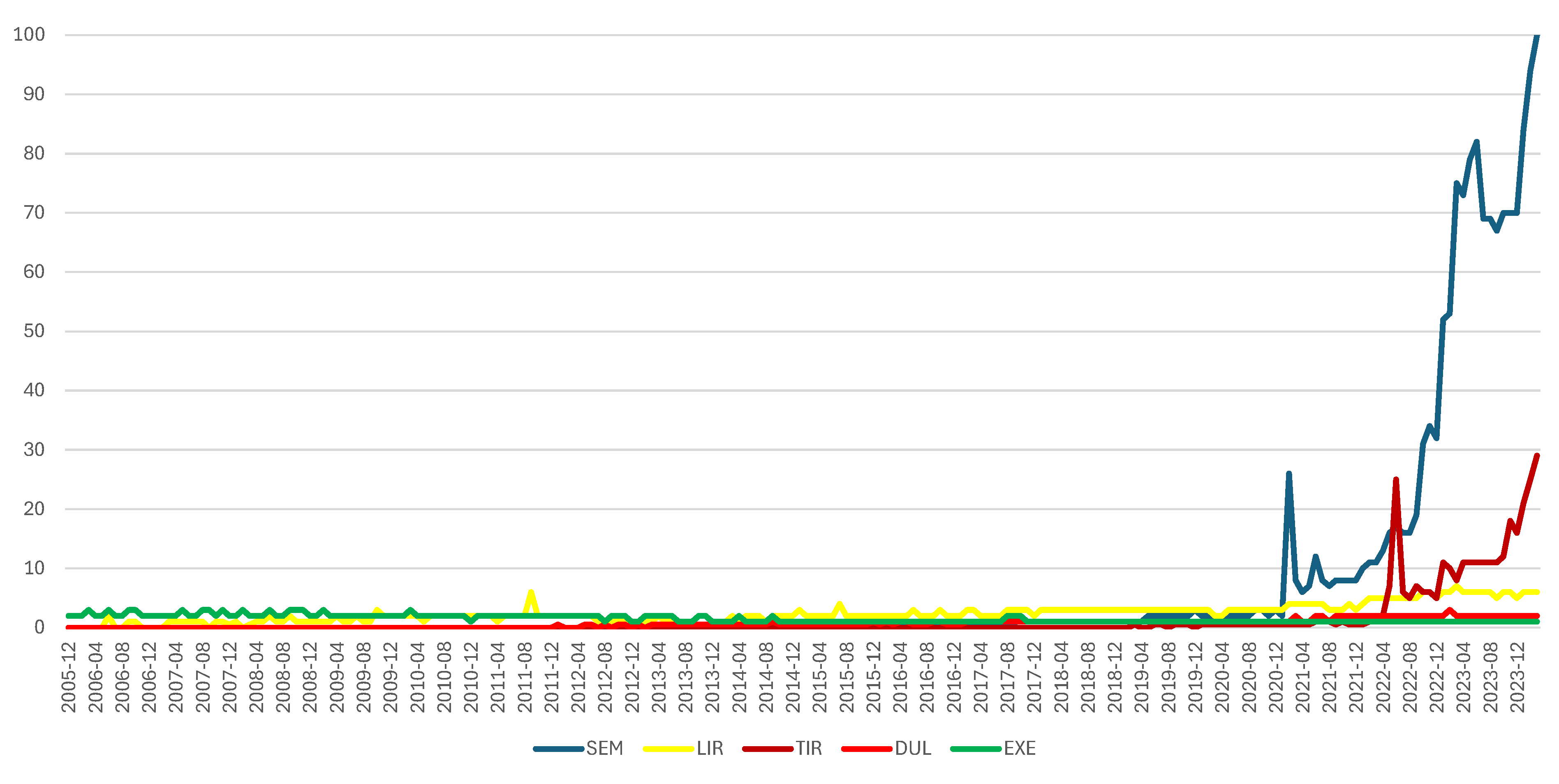
Figure 3.
Comparison of interest in searching information about GLP-1 RAs on Google by region [47].
Figure 3.
Comparison of interest in searching information about GLP-1 RAs on Google by region [47].
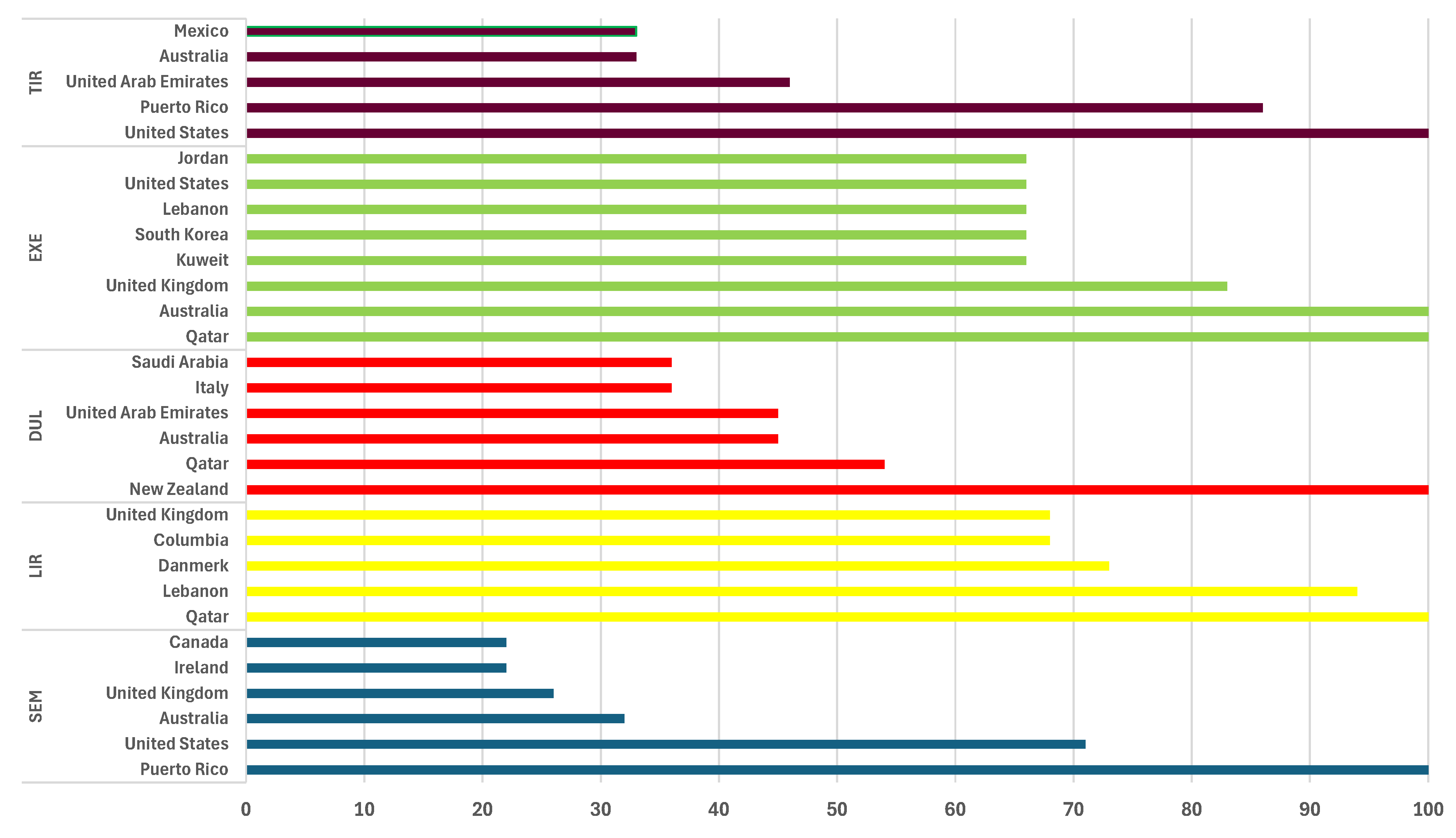
Figure 4.
The shares of ICSRs reported GLP-1 RAs. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
Figure 4.
The shares of ICSRs reported GLP-1 RAs. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
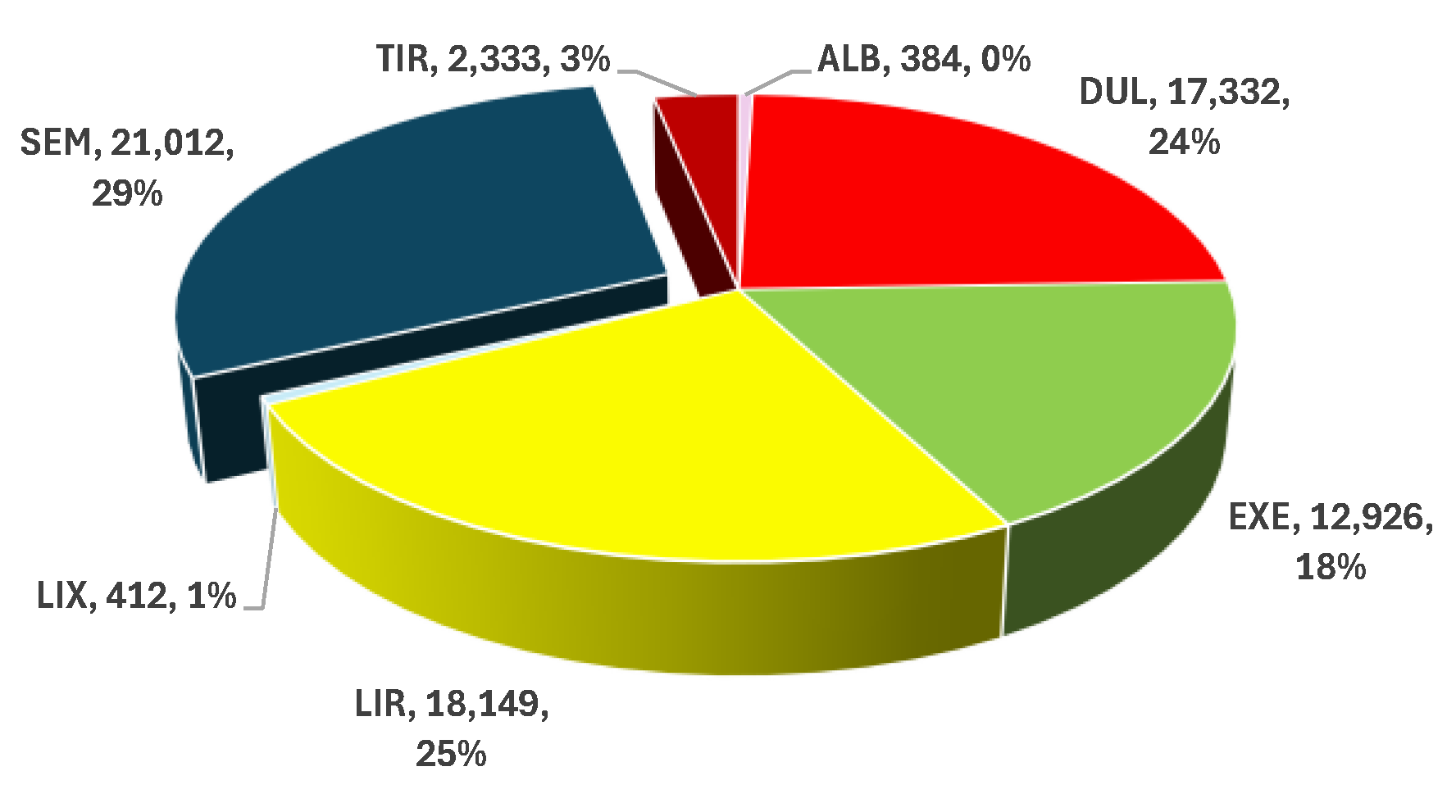
Figure 5.
The proportion of ADRs reported from total ICSRs. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
Figure 5.
The proportion of ADRs reported from total ICSRs. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
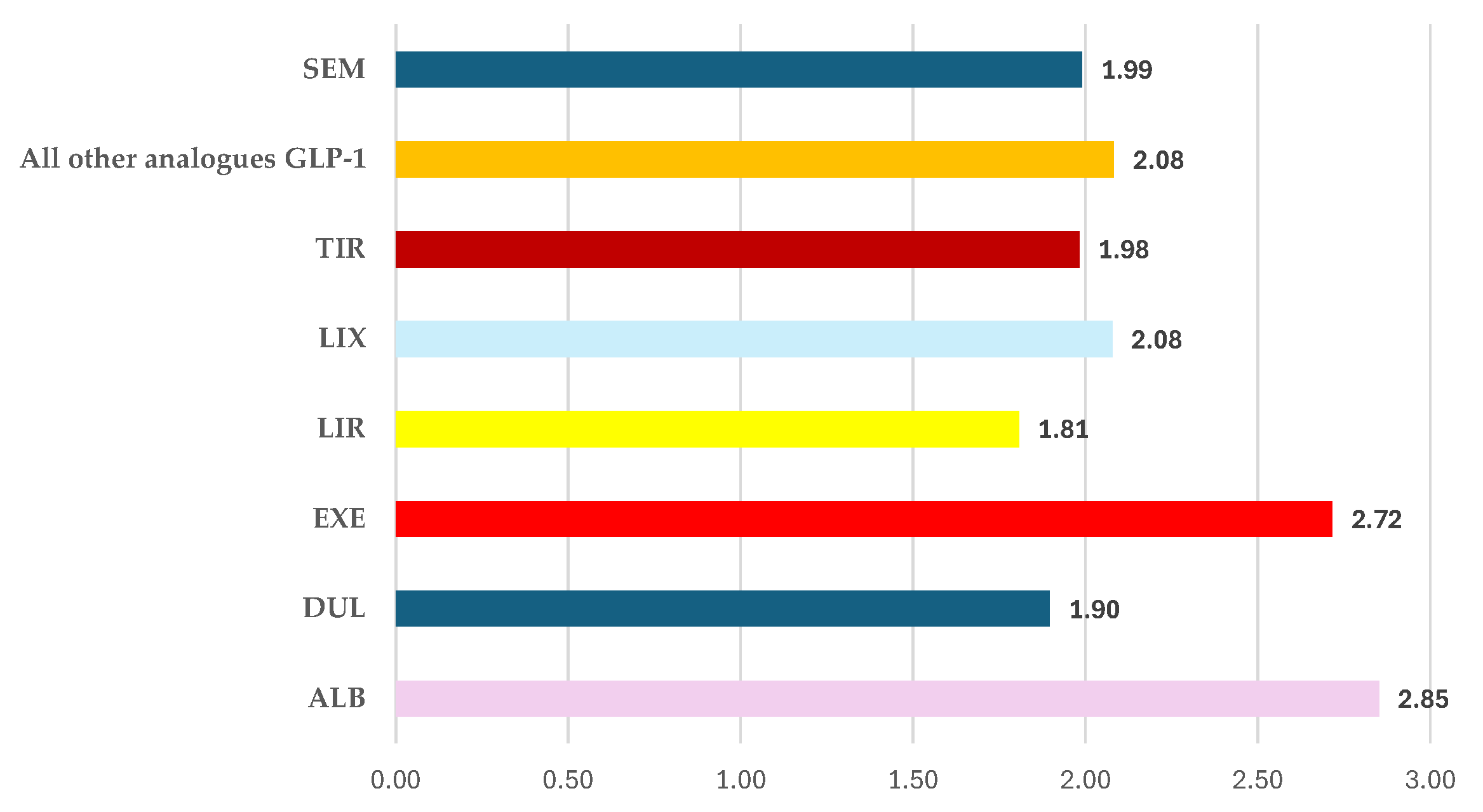
Figure 6.
Distribution of ADRs reported for SEM by SOC.
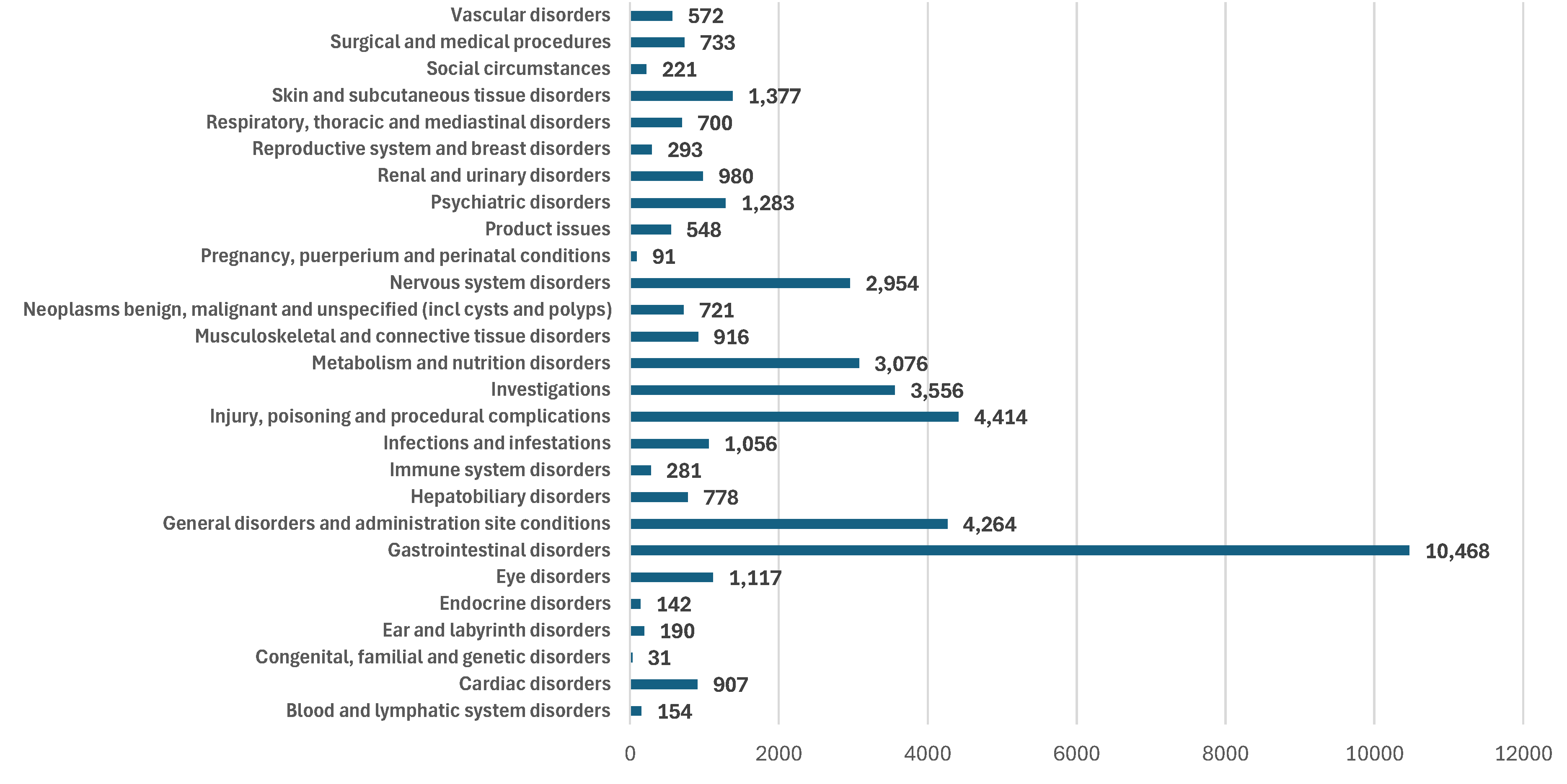
Figure 7.
Frequency of ADRs related to dosage in GLP-1 RA series. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
Figure 7.
Frequency of ADRs related to dosage in GLP-1 RA series. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
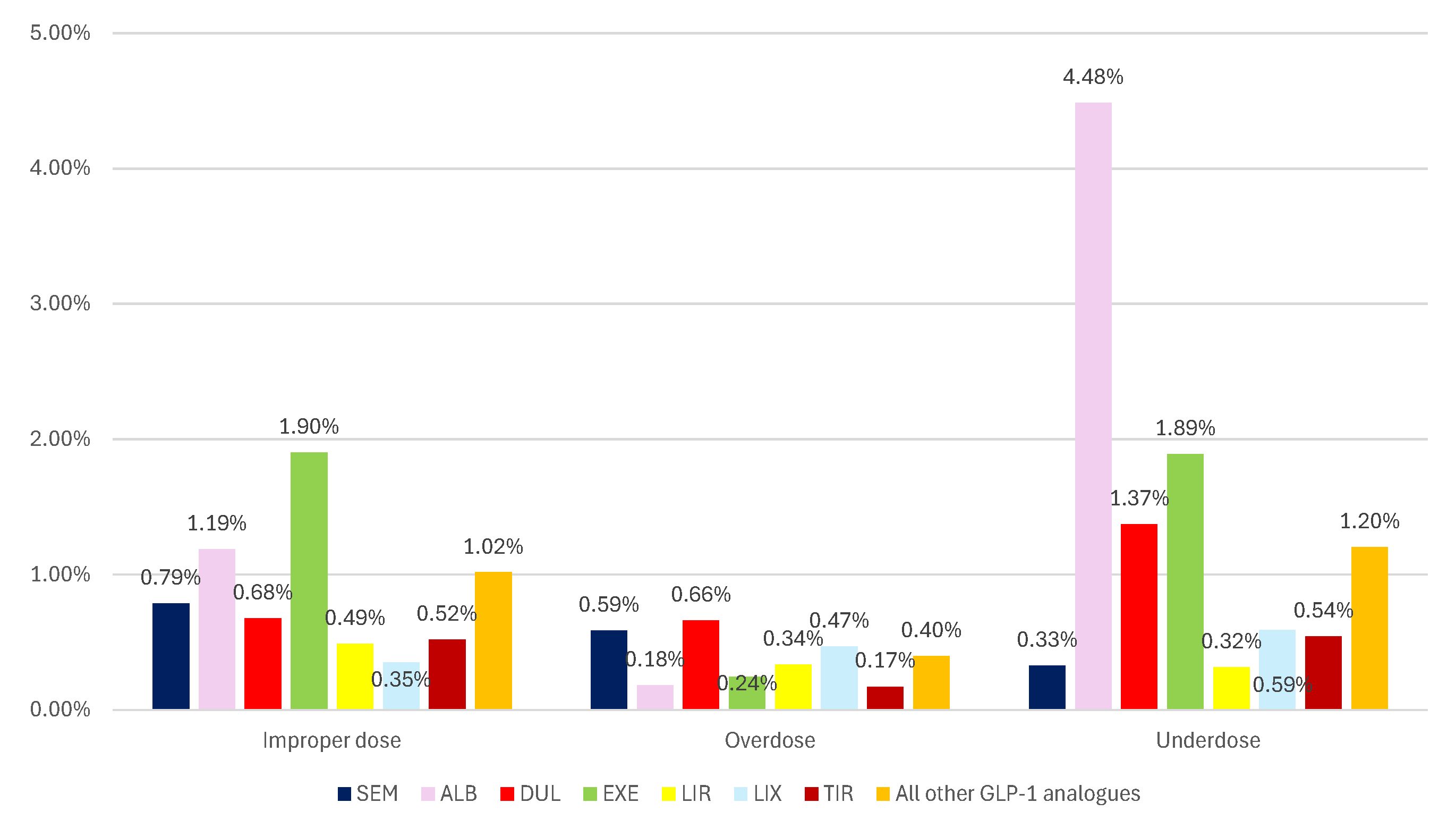
Figure 8.
Frequency of ADRs related to off-label use in GLP-1 RA series. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
Figure 8.
Frequency of ADRs related to off-label use in GLP-1 RA series. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
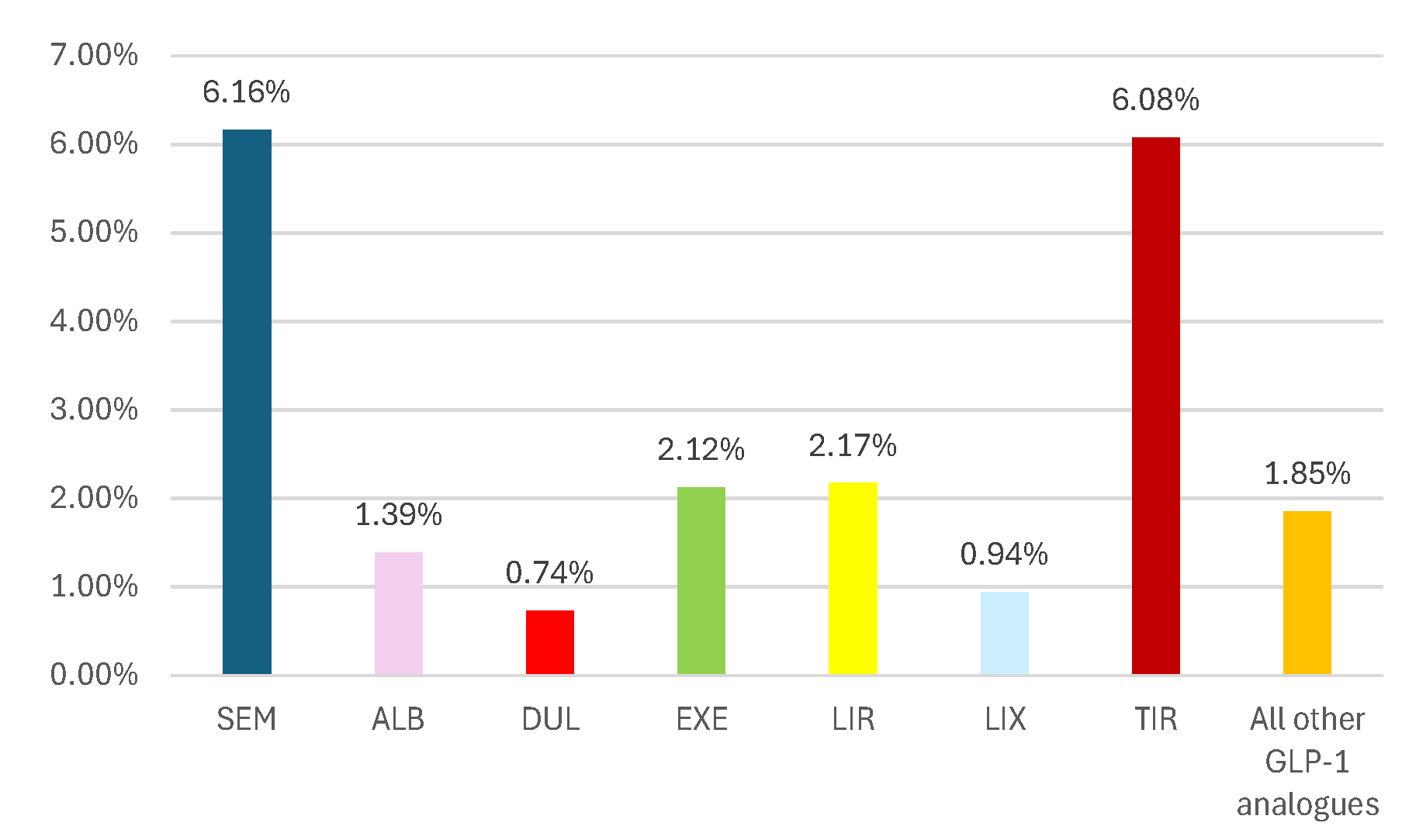
Figure 9.
Distribution of ADRs of semaglutide by outcome: (a) – related to dosage; (b) – related to off-label use. NR/NRS – not recovered/not resolved; NS – not specified; R/RS – recovered/resolved; ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
Figure 9.
Distribution of ADRs of semaglutide by outcome: (a) – related to dosage; (b) – related to off-label use. NR/NRS – not recovered/not resolved; NS – not specified; R/RS – recovered/resolved; ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
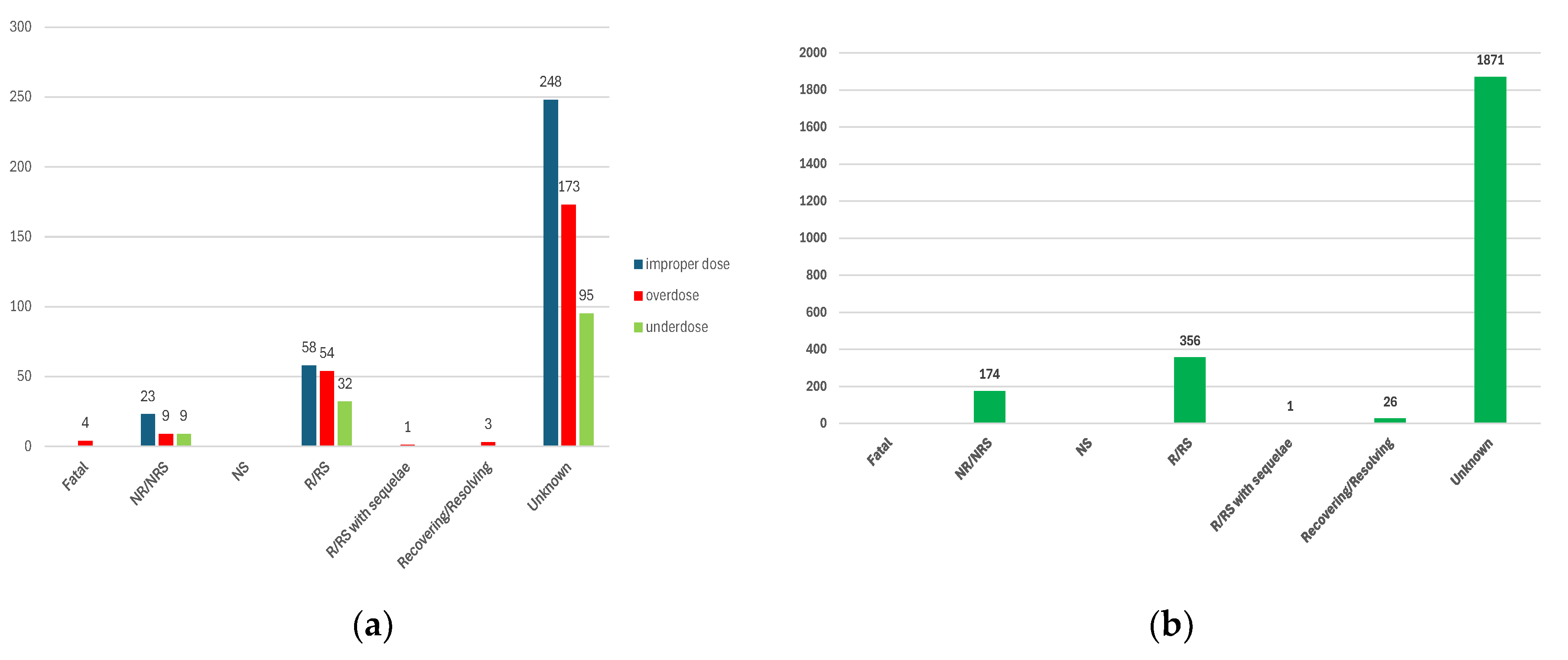
Figure 10.
The frequency of ADRs with unfavourable outcomes. (a) – fatal outcomes of ADRs related to incorrect dosage; (b) – not recovered / not resolved outcomes of ADRs related to incorrect dosage; (c) - not recovered / not resolved outcomes of ADRs related to off-label use. NR/NRS – not recovered/not resolved; NS – not specified; R/RS – recovered/resolved; ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
Figure 10.
The frequency of ADRs with unfavourable outcomes. (a) – fatal outcomes of ADRs related to incorrect dosage; (b) – not recovered / not resolved outcomes of ADRs related to incorrect dosage; (c) - not recovered / not resolved outcomes of ADRs related to off-label use. NR/NRS – not recovered/not resolved; NS – not specified; R/RS – recovered/resolved; ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
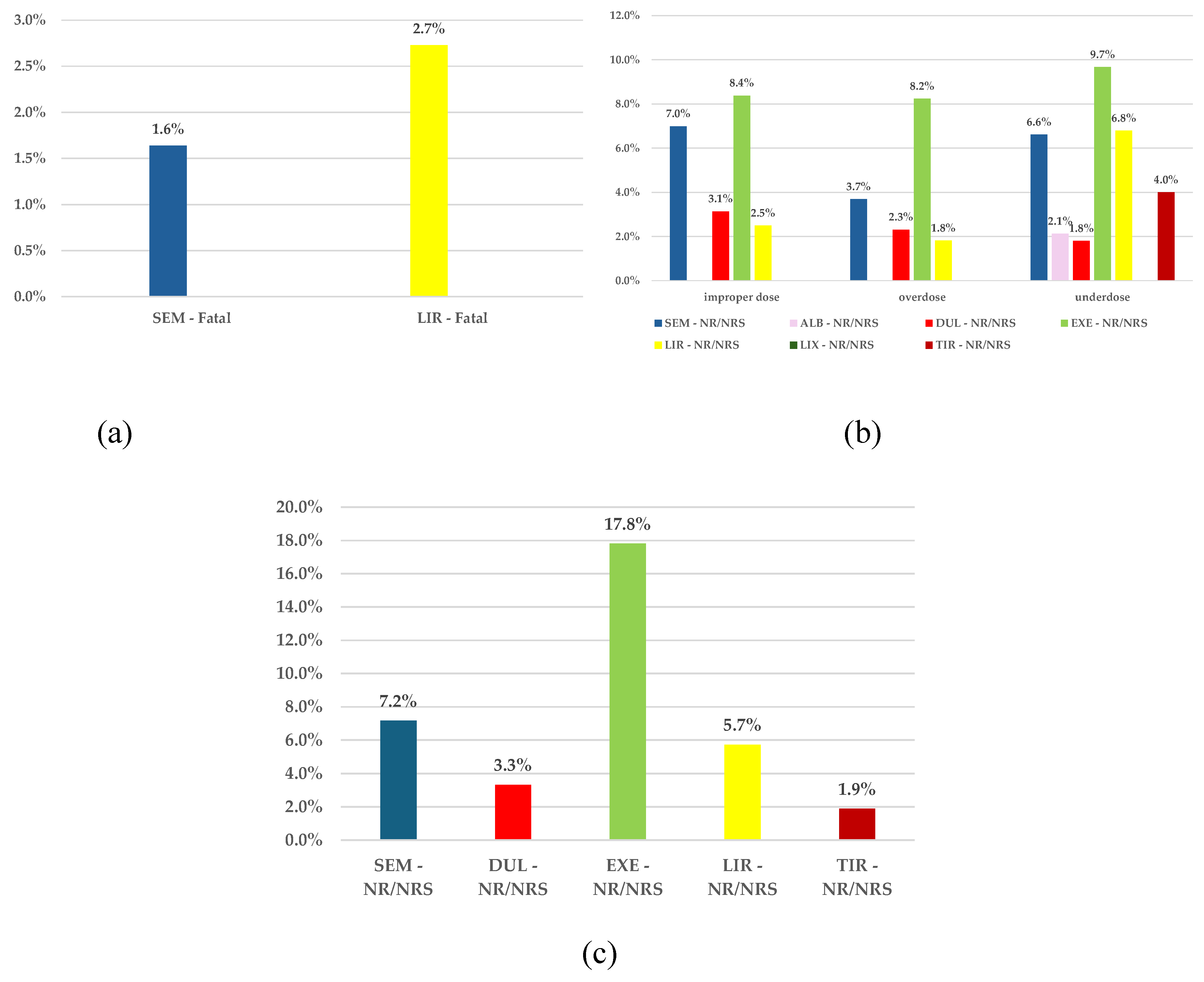
Figure 11.
Disproportionality analysis for incorrect dosage of SEM. (a) – improper dosage; (b) – overdose; (c) – underdose. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide. * p <0.05; ** p ≤ 0.01; p ≤ 0.001; **** p ≤ 0.0001.
Figure 11.
Disproportionality analysis for incorrect dosage of SEM. (a) – improper dosage; (b) – overdose; (c) – underdose. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide. * p <0.05; ** p ≤ 0.01; p ≤ 0.001; **** p ≤ 0.0001.
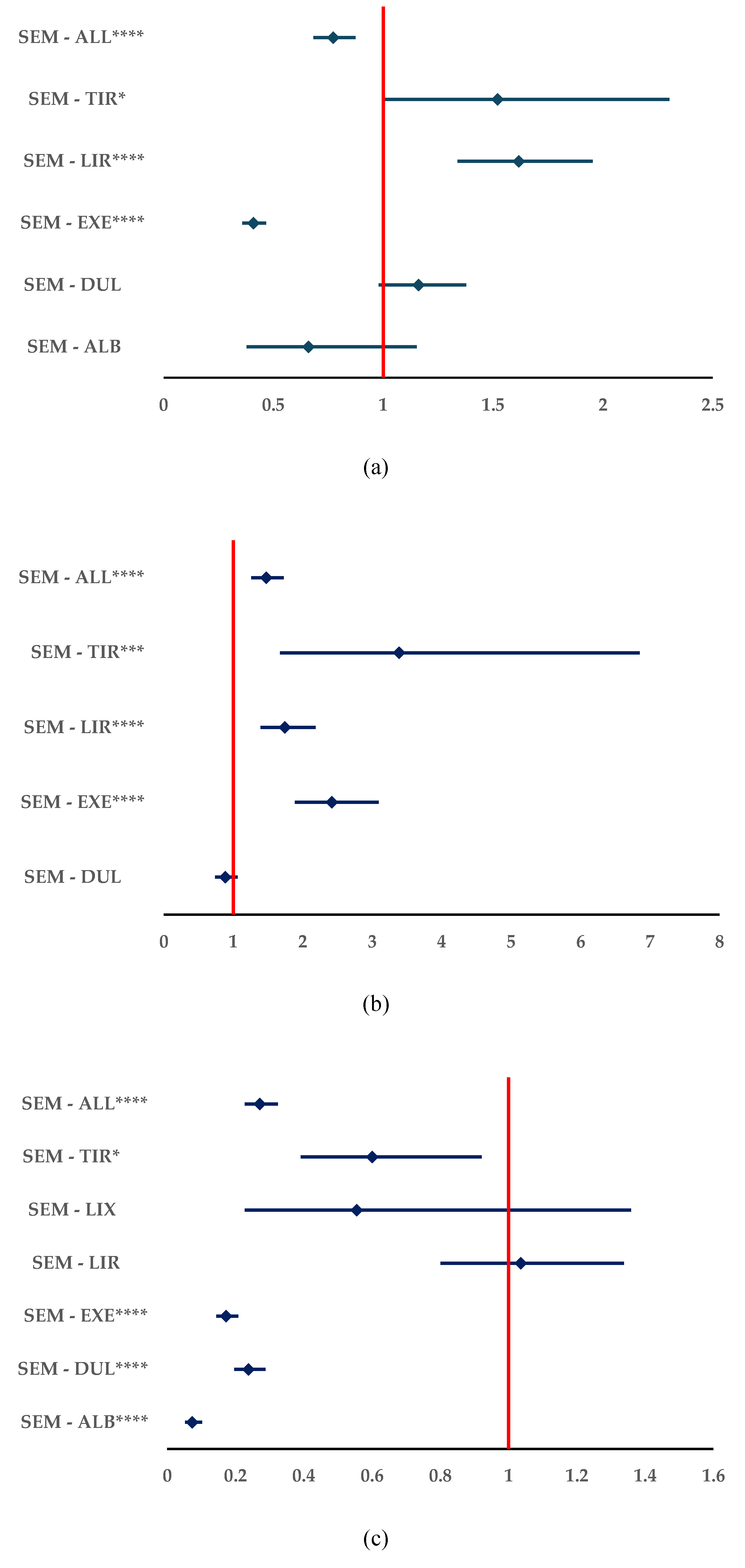
Figure 12.
Disproportionality analysis for off-label use of SEM. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide. * p <0.05; ** p ≤ 0.01; p ≤ 0.001; **** p ≤ 0.0001.
Figure 12.
Disproportionality analysis for off-label use of SEM. ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide. * p <0.05; ** p ≤ 0.01; p ≤ 0.001; **** p ≤ 0.0001.
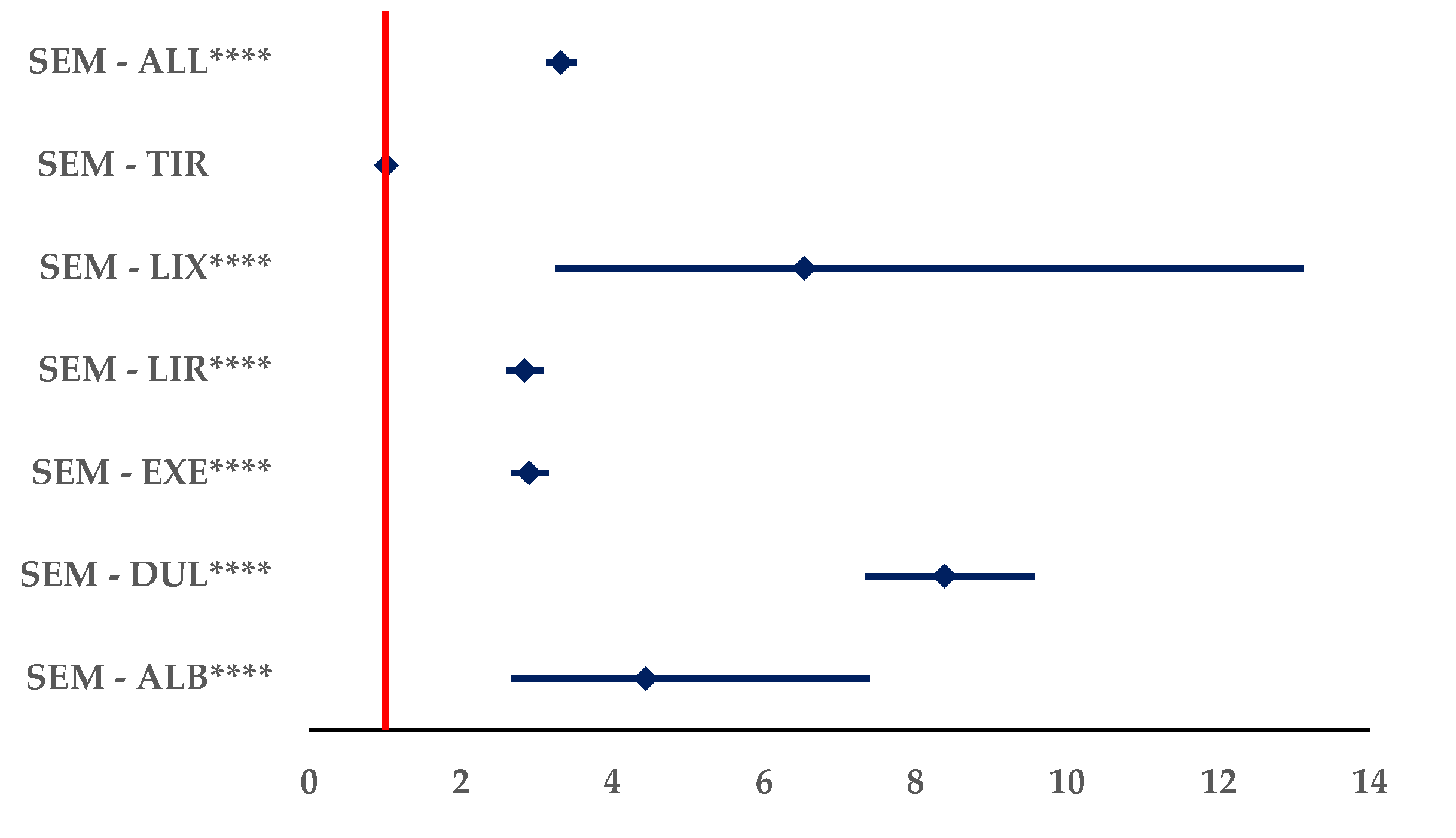
Table 1.
The preferred terms used for analysis.
| HLT | PT |
|---|---|
| modified dose | Dose calculation error |
| Dose calculation error associated with device* | |
| Drug dose titration not performed | |
| Drug titration error | |
| Incorrect dosage administered | |
| Incorrect dose administered | |
| Incorrect dose administered by device | |
| Incorrect dose administered by product | |
| Incorrect product dosage form administered* | |
| Product dosage form confusion* | |
| Wrong dose | |
| overdose | Accidental overdose |
| Intentional overdose | |
| Extra dose administered | |
| Overdose | |
| Prescribed overdose | |
| underdose | Accidental underdose |
| Drug dose omission by device | |
| Incomplete dose administered* | |
| Intentional dose omission | |
| Intentional underdose | |
| Prescribed underdose | |
| Product dose omission* | |
| Product dose omission in error | |
| Product dose omission issue | |
| Underdose | |
| off label use | Contraindicated product administered |
| Contraindicated product prescribed | |
| Drug effective for unapproved indication* | |
| Off label use | |
| Off label use of device | |
| Product use in unapproved therapeutic environment* | |
| Product use in unapproved indication | |
| Product used for unknown indication* | |
| Unintentional use for unapproved indication |
* PT with no reports.
Table 3.
Characteristics of ICSRs reported for SEM. EEA – European Economic Area; HP – healthcare professional; NS – not specified; ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
Table 3.
Characteristics of ICSRs reported for SEM. EEA – European Economic Area; HP – healthcare professional; NS – not specified; ALB – albiglutide; DUL – dulaglutide; EXE – exenatide; LIR – liraglutide; LIX – lixisenatide; SEM – semaglutide; TIR – tirzepatide.
| SEM | ALB | DUL | EXE | LIR | LIX | TIR | All GLP-1 RA | |
|---|---|---|---|---|---|---|---|---|
| n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
n (%) |
|
| Total | 21,012 | 384 | 17,332 | 12,926 | 18,149 | 412 | 2,333 | 51,536 |
| Age category | ||||||||
| NS | 7,942 | 148 | 5,476 | 4,160 | 6,668 | 105 | 1,138 | 17,695 |
| (37.8) | (38.5) | (31.6) | (32.2) | (36.7) | (25.5) | (48.8) | (34.3) | |
| 0-1 Month | 1 | 0 | 1 | 6 | 4 | 0 | 0 | 11 |
| (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | |
| 2 Months - 2 | 2 | 0 | 3 | 1 | 4 | 0 | 0 | 8 |
| Years | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) |
| 3-11 Years | 9 | 0 | 2 | 1 | 9 | 0 | 0 | 12 |
| (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | |
| 12-17 Years | 23 | 0 | 6 | 6 | 64 | 0 | 2 | 78 |
| (0.1) | (0.0) | (0.0) | (0.0) | (0.4) | (0.0) | (0.0) | (0.2) | |
| 18-64 Years | 8,345 | 162 | 6,576 | 5,519 | 8,236 | 186 | 863 | 21,542 |
| (39.7) | (42.2) | (37.9) | (42.7) | (45.4) | (45.1) | (37.0) | (41.8) | |
| 65-85 Years | 4,546 | 72 | 4,951 | 3,153 | 3,104 | 118 | 307 | 11,705 |
| (21.6) | (18.8) | (28.6) | (24.4) | (17.1) | (28.6) | (13.2) | (22.7) | |
| More than 85 | 144 | 2 | 317 | 80 | 60 | 3 | 23 | 485 |
| Years | (0.7) | (0.5) | (1.8) | (0.6) | (0.3) | (0.7) | (1.0) | (0.9) |
| Sex | ||||||||
| Female | 12,122 | 211 | 8,443 | 6,741 | 10,851 | 210 | 1,180 | 27,636 |
| (57.7) | (54.9) | (48.7) | (52.2) | (59.8) | (51.0) | (50.6) | (53.6) | |
| Male | 8,206 | 158 | 7,676 | 5,825 | 6,189 | 169 | 685 | 20,702 |
| (39.1) | (41.1) | (44.3) | (45.1) | (34.1) | (41.0) | (29.4) | (40.2) | |
| NS | 684 | 15 | 1,213 | 360 | 1,109 | 33 | 468 | 3,198 |
| (3.3) | (3.9) | (7.0) | (2.8) | (6.1) | (8.0) | (20.1) | (6.2) | |
| Geographic origin | ||||||||
| EEA | 11,060 | 12 | 8,864 | 3,226 | 7,309 | 265 | 115 | 19,791 |
| (52.6) | (3.1) | (51.1) | (25.0) | (40.3) | (64.3) | (4.9) | (38.4) | |
| NON-EEA | 9,952 | 372 | 8,468 | 9,700 | 10,839 | 147 | 2,218 | 31,744 |
| (47.4) | (96.9) | (48.9) | (75.0) | (59.7) | (35.7) | (95.1) | (61.6) | |
| NS | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | |
| Reporter | ||||||||
| HP | 12,877 | 175 | 11,001 | 8,751 | 12,316 | 333 | 1,470 | 34,046 |
| (61.3) | (45.6) | (63.5) | (67.7) | (67.9) | (80.8) | (63.0) | (66.1) | |
| NHP | 8,135 | 209 | 6,331 | 4,168 | 5,832 | 79 | 863 | 17,482 |
| (38.7) | (54.4) | (36.5) | (32.2) | (32.1) | (19.2) | (37.0) | (33.9) | |
| NS | 0 | 0 | 0 | 7 | 1 | 0 | 0 | 8 |
| (0.0) | (0.0) | (0.0) | (0.1) | (0.0) | (0.0) | (0.0) | (0.0) | |
| Seriousness | ||||||||
| Non serious | 8,983 | 5 | 7,051 | 1,383 | 4,637 | 119 | 120 | 13,315 |
| (42.8) | (1.3) | (40.7) | (10.7) | (25.5) | (28.9) | (5.1) | (25.8) | |
| NS | 0 | 0 | 0 | 3 | 3 | 0 | 0 | 6 |
| (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | (0.0) | |
| Serious | 12,029 | 379 | 10,281 | 11,540 | 13,509 | 293 | 2,213 | 38,215 |
| (57.2) | (98.7) | (59.3) | (89.3) | (74.4) | (71.1) | (94.9) | (74.2) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



