
Submitted:
29 April 2024
Posted:
30 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
At the beginning of December 2019, a new type of coronavirus emerged, SARS-CoV-2. This virus causes COVID-19, a highly contagious disease that can initially present asymptomatically and can also lead to death. Our ecological study goal was to evaluate the incidence, mortality, and lethality rates for COVID-19 between the states of Espírito Santo and Minas Gerais, with time series analysis using secondary and public databases on COVID-19 from January 2020 to July 2022. Prais-Winsten linear regression was used for trend analyses. In 2020, the rate in Espírito Santo was 2.19 times greater than Minas Gerais. This trend continued in 2021, with Espírito Santo's rate being 1.29 times greater. In 2022, Espírito Santo's rate remained 2.65 times higher than Minas Gerais. Furthermore, Espírito Santo had the highest mortality, with the exception of 2021. In turn, Minas Gerais had the highest fatality rate throughout the analyzed pandemic period. The state of Espírito Santo had a higher incidence of COVID-19, as well as higher mortality, when compared to the state of Minas Gerais. In turn, Minas Gerais had a higher fatality rate. Furthermore, both states showed similar trends for mortality, lethality, and incidence in the years 2020 and 2021.
Keywords:
coronavirus
; COVID-19
; mortality
; incidence
; lethality
1. Introduction
COVID-19 has become a milestone in the history of epidemiology. Like other diseases, it brought with it several challenges, given its global spread, which ended up having a general impact on public health. As it is a new type of virus, the importance of the role of epidemiologists in the search for understanding, patterns, as well as risk factors is understood, in order to corroborate the mitigation of the devastating effects of the virus, as well as to promote strategies for prevention and control.
The story begins in December 2019, more specifically in the city of Wuhan (China), where a new type of coronavirus, SARS-CoV-2, was identified. Since then, measures have been adopted to combat the virus that caused the pandemic, considering that this new type of coronavirus has resulted in the manifestation of COVID-19, which is a disease that spreads quickly and is difficult to control. forms of transmission [1,2].
Regarding the impacts caused, in the economic sphere, for example, jurisdictional tax measures and exemptions were adopted in response to combating COVID-19. Such measures were taken in order to encourage acceptance by the population. Regarding social impacts, it also reveals that there were changes in lifestyle, limitations on travel, bans on meetings, among others [2].
Currently, data provided through the WHO Coronavirus (COVID-19) Dashboard shows that by the month of August 2023, globally, 770,085,713 confirmed cases of COVID-19 infection have been recorded. In addition, 6,956,173 deaths have been confirmed due to the disease. Among these records, Europe is the continent with the highest cumulative number of confirmed cases [3].
According to data highlighted in the Weekly epidemiological update on COVID-19 made available by the World Health Organization (2023) [4], there was a global increase in the number of new cases and deaths due to COVID-19 until mid-January 2023, which is why they included it in the new document updates on the variants and subvariants of concern, as well as records on the increase in the number of hospitalizations in several countries, including in the Intensive Care Unit (ICU).
However, in the last update of the global document made available by Who (2023) [5], which concerns the month of August 2023, there is information on the decrease in the number of deaths (50%), despite the increase (38%) in the number of confirmed cases, in addition to the decrease in the number of ICU admissions.
Having been considered a new disease, the virus in question behaves similarly to viruses that cause pandemics, which results in similar adoption of measures to contain transmission, which in turn is considered community transmission. SARS-CoV-2 is a virus that remains stable on surfaces, such as plastic and stainless steel materials, for up to three days, in addition to being transmissible in the form of aerosols for hours, when outside the human body. In materials such as copper and cardboard, viability was reduced in a few hours [6,7].
Furthermore, Li et al., [8] describe that infection with SARS-CoV-2 can initially be asymptomatic and can progress seriously and even lead to death, and can affect all ages. In this sense, Zhang et al., [9] point out that SARS-CoV-2 variants represent a great threat to the prevention and control of COVID-19 transmission, given the ability of new strains to be imported between different countries.
In this context, Abate et al., [10] point out in research on admissions to Intensive Care Units, where the mortality rate reached 39% of patients infected with the new coronavirus admitted to this sector. Furthermore, it points out that around 66% of patients admitted to the ICU had associated comorbidities, which in turn, through regression analysis, detected that the comorbidity increased the risk of death by 39%.
However, in May 2023, the end of the Public Health Emergency of International Importance regarding COVID-19 was declared, following statements about the decreasing trend in deaths due to COVID-19, a decrease in hospitalizations and ICU admissions, as well as, increase in the population's level of immunity to SARS-CoV-2 [11].
Despite the declaration, in terms of comparison between countries, Brazil is currently in 6th position in the ranking of cumulative cases, totaling 37,717,062 confirmed cases, behind countries such as the United States of America, China, India, France and Germany [3]. In turn, considering the southeastern region of Brazil, more specifically the states Espírito Santo (ES) and Minas Gerais (MG), 1,339,629 confirmed cases and 15,110 deaths from COVID-19 were registered in ES, while MG recorded 4,209,719 cases and 65,740 deaths, until the beginning of September 2023, as published by the coronavirus panel [12].
Given this scenario, the question arises: what are the incidence, mortality and lethality rates for COVID-19 in the states of Espírito Santo and Minas Gerais between 2020 and 2022?
The study is justified by the emerging need to carry out research in order to understand the profile of infected people in terms of incidence, mortality and lethality rates due to infection by the new coronavirus in the states of Espírito Santo and Minas Gerais. In this way, deepening this theme may contribute to better coping with the disease by policymakers, through robust and specific evidence, in order to contribute to the development and implementation of local interventions, thus making coping with the pandemic in the states are more efficient.
Therefore, the objective of the present study is to evaluate the incidence, mortality and lethality rates for COVID-19 between the states of Espírito Santo and Minas Gerais, Brazil, from 2020 to 2022.
2. Materials and Methods
2.1. Study Design
This is an ecological study, of a quantitative nature, with time series analysis using a secondary and public database on COVID-19, made available by the Brazilian Ministry of Health through the website https://covid. saude.gov.br/.
2.2. Location and Period of Research
The states Espírito Santo and Minas Gerais were selected to carry out this research, considering that both are part of the Southeast region of Brazil (Figure 1) and border each other, where Espírito Santo has 23 cities bordering Minas Gerais [15,16,17].
According to the last census carried out by the Brazilian Institute of Geography and Statistics (IBGE) [15] in the year 2022, the state of Espírito Santo (Figure 2) had a total population of 3,833,486 people. The state has a total territorial area of 46,074.448 km², with a Human Development Index (HDI) in 2021 of 0.771, occupying 5th position in the national ranking and per capita income of R$1,723.
In turn, the state of Minas Gerais (Figure 2), in 2022, presented in the census the equivalent of 20,538,718 people, in a total territorial area of 586,513,983 km². The state presented a Human Development Index (HDI) in 2021 of 0.774, occupying 4th position in the national ranking and nominal monthly income per capita of R$ 1,529 [16].
The period for data collection was between January 2020 and December 2022.
2.3. Study Population and Eligibility Criteria
The population of the states of Espírito Santo and Minas Gerais was used and all confirmed cases and deaths related to COVID-19 were included in the study using the International Classification of Diseases, 10th edition (ICD-10), of “B34.2, Coronavirus infection of unspecified location” and “U07.1 COVID-19, identified virus” or “U07.2 COVID-19, unidentified virus”. It should be noted that all cases and deaths included in the research are confirmed.
Data that did not provide complete information regarding the state or city were excluded from collection, making identification unfeasible.
2.4. Data Collection
The data were extracted from the Coronavirus Panel, available on the website https://covid.saude.gov.br/, on February 8, 2023. This panel was created by the Brazilian Ministry of Health and developed to be the official and public communication about the epidemiological situation of COVID-19 in the country. This database uses as a reference the number of cases and deaths confirmed by COVID-19 that were registered by the State and Municipal Health Departments ( https://covid.saude.gov.br/ ).
Specifically, the cases and deaths in the state of Espírito Santo were removed from the website https://coronavirus.es.gov.br/painel-covid-19-es, while those in the state of Minas Gerais were removed from the website https://coronavirus.saude.mg.gov.br/dadosabertos.
Data on the resident population of the states of Espírito Santo and Minas Gerais were extracted from the projection base of the population of Brazil of the Federation Units by sex and year for the period 2000-2030 from the Brazilian Institute of Geography and Statistics (IBGE) [15,16] available in the database of the Department of Informatics of the Unified Health System (DATASUS) [18], on the website https://datasus.saude.gov.br/informacoes-de-saude-tabnet/.
DATASUS provides information that can serve to support objective analyzes of the health situation, evidence-based decision making and the development of health action programs. It is important to highlight that data collection was carried out by two researchers independently to mitigate collection bias and guarantee the quality and reliability of the data. After extraction, the data was organized into Microsoft Excel spreadsheets.
2.5. Study Variables
Dependent (outcome): confirmed cases, confirmed deaths, fatality rate, mortality and incidence.
Independent (explains the outcome): years 2020, 2021 and 2022.
2.6. Data Analysis
The data were tabulated in a Microsoft Excel 365 spreadsheet, version 2019, to ensure the organization of absolute frequencies, taken from the public platform, by variable, with the independent and dependent variables. Thus, the relative frequency was calculated, obtaining data on the number of cases and deaths confirmed by COVID-19 in the month and/or year and divided by the total number of the period evaluated and multiplied by 100, expressed as a percentage (%).
Incidence and mortality rates were expressed per 100,000 inhabitants and lethality expressed as a percentage (%), following the formulas, respectively:
For trend analyses, the methods proposed by Antunes and Cardoso [13] were used, where time series construction rates were calculated using the Prais-Winsten regression model, which allowed first-order autocorrelation corrections to be performed. in values, organized by time. Thus, the following values were estimated: angular coefficient (β) and respective probability (p), considering a significance level of 95% confidence interval (95% CI).
The data modeling process included transformation rates (dependent variable = Y value) into a base 10 logarithmic function. The independent variable (X value) was the days or months of the historical series. The Durbin–Watson test was also used to measure the existence of first-order autocorrelation of the time series composed of daily coefficients and to verify whether the correlation was compatible with the hypothesis of random distribution regression residuals.
The results of the logarithmic rates (β) of the Prais-Winsten regression made it possible to estimate the percentage variation in daily change (Daily Percent Change – DPC) in each state, with the respective confidence intervals (95% CI), expressed by the following formulas:
In this way, it was possible to determine the rates as increasing, decreasing or stationary and quantify the percentage variation in daily incidence, mortality and lethality rates. The trend was considered stationary when the coefficient was not significantly different from zero (p>0.05). When the coefficient value was statistically significant (p<0.05), the trends were classified as increasing or decreasing according to the β value. To facilitate visualization of lethality trends, random variation in the graph was reduced using the five-order moving average technique. All statistical analyzes were performed using STATA 17.0 statistical software [19].
2.7. Legal and Ethical Aspects
By using only aggregated secondary data from the public domain, the work meets the ethical considerations set out in Resolution of the National Health Council (CNS) No. 466, of December 12, 2012 and in Resolution 510, of April 7, 2016, being exempt from evaluation by the Research Ethics Committee and the National Commission for Ethics in Research on Human Beings.
3. Results
In the state of Espírito Santo, from January 2020 to December 2022, a total of 1,313,710 cases and 15,400 deaths confirmed by COVID-19 were recorded. Table 1 shows the monthly distribution of cases and deaths confirmed by COVID-19 in Espírito Santo over time (2020 to 2022).
In the state, the first confirmed case of COVID-19 was registered in February 2020, corresponding to 0.0001% of the total cases throughout the analyzed period. As for deaths, the first records appeared in April of the same year, corresponding to a relative frequency of 0.75% of total deaths.
In 2020, in Espírito Santo, 268,768 cases and 5,371 confirmed deaths from COVID-19 were recorded, with a monthly average of 22,397 and 448 respectively. The months with the highest number of confirmed COVID-19 cases were July (2.84%), November (3.53%) and December (4.16%). In relation to deaths confirmed by COVID-19, the months that stood out were June (6.88%), July (5.87%) and December (5.59%).
Continuing the pandemic period, in 2021, 371,295 cases and 8,257 confirmed deaths from COVID-19 were recorded, with an average of 30,941 and 688, respectively. Here, the months of January, March and April stand out for confirmed cases, being 3.42%, 5.02% and 3.84%, respectively, in relation to the total period. However, for deaths, the months with the highest number of records were March (8.27%), April (13.71%) and May (8.27%).
In turn, in 2022, 673,647 cases and 1,772 deaths from COVID-19 were recorded, with an average number of cases and deaths of 56,137 and 148, respectively. The month of January stands out, corresponding to 19.46% of the total cases, followed by the month of February, with 10.48% of cases and July, with 5.87%. For all the months mentioned above, the relative frequencies of deaths also behaved as the highest, equivalent to 1.94%, 4.02% and 1.50% respectively. It was noted that, in the annual comparison for the state of Espírito Santo, in 2022 there was a greater number of case records, with a lower number of deaths.
In turn, in the state of Minas Gerais, between January 2020 and December 2022, a total of 3,430,099 cases and 64,498 deaths confirmed by COVID-19 were recorded. In the state, the first confirmed cases of COVID-19 were registered in January 2020, corresponding to 0.004% of the total cases throughout the analyzed period and one death, in the same month.
The monthly distribution of cases and deaths confirmed by COVID-19 in Minas Gerais can be seen in Table 2.
In 2020, in the state of Minas Gerais, the average number of cases and deaths confirmed by COVID-19 was 52,890 and 1,111, totaling 634,681 and 13,336, respectively. The months with the highest number of confirmed COVID-19 cases were July (2.87%), August (2.54%) and December (4.48%). In relation to deaths confirmed by COVID-19, the months mentioned above were also highlights, corresponding in sequence to 3.76%, 3.77% and 4.07%.
In 2021, the average number of cases was 124,184 and the number of deaths confirmed by COVID-19 was 3,658. Here, the months of March, May and June stand out for confirmed cases, being 7.77%, 5.98% and 5.75%, respectively, in relation to the total period. However, for deaths, the months with the highest number of records were March (13.15%), April (14.36%) and May (9.64%). That year, 1,490,204 cases and 43,894 deaths were recorded. It is noteworthy that this year stands out among those analyzed for presenting the highest number of cases, as well as deaths.
In 2022, the total number of cases was 1,305,214, with a monthly average of 108,768, with the months of January (16.57%), February (8.83%) and June (5.33) standing out.As for death records, there is a total of 7,268, with a monthly average of 606, highlighting the months of January, February and July, with rates of 2.09%, 3.53% and 1.29%, respectively.
When comparing the incidences of COVID-19 between states, Espírito Santo (ES) stands out compared to the state of Minas Gerais (MG), presenting the highest rates, as in 2020 (A), where the rate was higher in 2, 19 times and in 2021 (B), in which the rate was 1.29 times higher than the other state. In the year 2022 (C), the highest incidence rate for COVID-19 continued to be in Espírito Santo, with a total of 15,979.12/100,000 inhabitants, compared to a rate of 6,029.64/100,000 inhabitants in the state of Minas General, which corresponds to 2.65 times higher.
To better visualize the data, see Figure 3 below, with comparative graphs between the states, year by year.
Now, when comparing the lethality rates between the states of Minas Gerais and Espírito Santo, it was noted that during the period analyzed, the total rate remained higher in the state of Minas Gerais, with the months of April/2020 being highlighted (D ) with 3.07, April/2021 (E) with 4.73 and December/2022 (F) with 20.69.
Below is Figure 4, which concerns the comparison of lethality between states.
Although lethality in Minas Gerais was higher throughout the analyzed period, mortality was higher than in the state of Espírito Santo only in the year 2021 (H), reaching a rate of 203.67/100,000 inhabitants. For the years 2020 (G) and 2022 (I), the state of Espírito Santo recorded a mortality rate 2.09 and 1.25 times higher than the state of Minas Gerais, respectively, as shown in Figure 5.
In addition, an analysis of trends in mortality, lethality and incidence rates of COVID-19 in the states of Espírito Santo and Minas Gerais was carried out, which can be seen in Table 3.
For analyzes considered statistically significant ( p<0.05 ), the daily percentage change (DPC) reveals the percentage of daily change, as well as its respective confidence interval, demonstrating the increase or decrease for the variables studied.
Thus, it was observed that for the years 2020 and 2021, the trends in both states were the same for mortality, lethality and incidence. However, in 2022, there will be different behaviors between states for each variable analyzed. In the state of Espírito Santo, that year, for the variables mortality, lethality and incidence, there was a stationary trend. In turn, Minas Gerais presents decreasing mortality (-0.62%/day), increasing lethality (+1.39%/day) and decreasing incidence (-1.80%/day).
4. Discussion
After individual analyzes of the total number of cases and deaths confirmed by COVID-19 in the states of Espírito Santo (ES) and Minas Gerais (MG), in the period from 2020 to 2022, it is clear that for the year 2021, the state of Minas Gerais recorded a higher number of cases, as well as deaths. For the state of Espírito Santo, the highest number of cases recorded during the pandemic period occurred in 2022, however, with a lower number of deaths already recorded.
When comparing the states, it is clear that, in proportion, ES had the highest incidence and mortality rates, while MG had the highest fatality rate.
Furthermore, in detail, there is a certain similarity with regard to the months that stood out due to the relative frequency in the distribution of cases and deaths for both states, with the vast majority being months at the beginning, middle and end of the years. analyzed, such as January, February, June, July, November and December. Another similar factor between states is the behavior of the increase in the number of deaths occurring in the current month or subsequent to the increase in the number of cases.
Nevertheless, the estimates demonstrated a stationary trend for incidence, mortality and lethality in Espírito Santo in the year 2022, while in the state of Minas Gerais there is a decreasing trend for incidence and mortality and an increasing trend for lethality in the same period. The daily increase in lethality is 1.39% (95%CI 1.11: 1.66).
Regarding the increase in the number of cases and deaths in months with specific holidays, a study carried out by Ren and Hwang [20] corroborates this research, which shows that in approximately six to eight days after a holiday, there was an increase of 1.30 to 1.41 times the incidence rate. This expected time is directly related to the period of manifestation of symptoms and/or the results of the exam performed. Another study, carried out by Hadianfar et al., [21] also agrees with the results found, where an approximate increase of up to 1,872 new cases was observed after holidays (p<0.001).
For the analyzes of a study carried out in the United States, federal holidays were considered, such as New Year, Martin Luther King Day, Good Friday, Independence Day, Memorial Day, Labor Day, Christmas, elections, vacations, among others [20]. This finding is in line with the results of the current study, considering that these are months that have similar holidays in Brazil, such as Christmas, New Year, elections, in addition to the vacation period, which leads to an increase in the number of people circulating, as well as, group meetings.
In this context, the results of the present study demonstrate an increase in incidence, mortality and lethality in November and December 2022. During this period, a major event that may have favored this increase in cases and deaths was the election. There were two rounds of presidential elections, where for both the state of Espírito Santo and the state of Minas Gerais, approximately 80% of eligible electorates in each state turned out to vote [22].
Other factors may also be associated with the increase in the number of cases and, consequently, the number of deaths. For Wu et al., [23], information on demographic density, average family income, percentage of the population in poverty, education, etc., provides support for a better understanding of the disease's behavior. In this aspect, the state of Espírito Santo has a demographic density 2.38 times greater than the state of Minas Gerais, with 83.20 inhabitants/km² against 35.02 inhabitants/km² [15,16].
Demographic density is important in influencing the impacts of an epidemic, considering its population groups and their vulnerabilities, assuming that the greater the population density, the greater the difficulty of distancing, given that distancing is related to human behavior and be challenging, contributing to reducing or increasing the damage caused by virus transmission [24].
In this sense, it may be a factor that justifies the state of Espírito Santo presenting higher incidence and mortality rates, when compared to the other state. On the other hand, a study carried out by Sutton et al., [25] revealed that mortality from COVID-19 was higher in regions with lower population density, linking this to two factors: rural regions and a higher proportion of elderly people in these regions. It is noteworthy that these specificities end up being important, as they point out that these standards contribute information for the implementation of specific health policies for these areas and populations.
With regard to intervention measures, Wong and Li [24] report that implementations can occur according to population density, thus considering more stringent policies in high density areas, compared to those with lower density, which would result in optional measures.
As measures, many countries have implemented different types of blockades, some as compulsory, others with penalties applied to non-compliance. Among the measures, blockades in transport areas were adopted, such as stations, airports, highways, in order to reduce population movement. Thus, Tsuboi, Fujiwara and Itoh [26] state that blockades, information and changes in the population's behavior to the detriment of the pandemic contribute to reducing the risk of infection.
However, in order to effectively control the spread of the virus and consequently the disease, early implementation of measures is necessary. Among the measures, social distancing is influential in reducing daily cases of COVID-19 and for every day of delay in its implementation, there is a 2.41 day delay in containing the pandemic [21,27]. Corroborating this idea, Remuzzi and Remuzzi [28] argue that the exponential increase in mortality in the population may be linked to the late implementation of control measures.
A study carried out in different countries such as Spain, China, the United States, Japan and Sweden, demonstrated that in 2021, compared to 2020, people reacted with less sensitivity to the suggested measures, arguing that in the first year of the pandemic, the measures were more effective [26].
However, when analyzing the results of this research, a divergence from the previously mentioned study is noted. For the states of Espírito Santo and Minas Gerais, in 2021, the result was a decreasing trend for incidence, mortality and lethality due to COVID-19, while in the first pandemic year, such trends were increasing, with the exception of lethality.
A study carried out in Curitiba, Brazil, covering the period from 2020 to mid-2022, resulted in the incidence in 2022 being twice as high compared to previous years, but with the lowest lethality ever recorded. In this aspect, the authors argue that in 2022, lethality was already in a declining phase, considering that around 70% of the population had completed the current vaccination schedule for SARS-CoV-2 [29].
Furthermore, with the emergence of new variants, especially Omicron, it was noted that in previously infected or vaccinated people in the United States, cases were classified as mild, which made it possible to reopen gathering spaces. However, it appears that although there was a risk of an increase in the number of cases, the scenario did not increase lethality [30,31]. In view of this, Adamoski et al., [29] reinforce that, although it is milder, the increase in number can lead to overload of the health service.
In this aspect, the process of understanding the course of the disease, as well as its trend throughout the pandemic period in the states of Espírito Santo and Minas Gerais, is understood as important, considering that the robustness of information is capable of bringing greater understanding about the disease, as well as on the interventions implemented over the years studied.
Such information, in addition to contributing to the present time, assuming that there are still records of new cases of COVID-19 in both states and that specific measures continue to be adopted, can support the process of evaluating the interventions carried out, as well as, new measures to be implemented in future epidemics, especially actions to promote, prevent, monitor and control the disease.
Given the stationary trend in most rates in 2022, it is suggested that the measures were important, from their first implementations to their revocations and/or changes, for maintaining a controlled state in a pandemic period, which reinforces the need for new studies to further understand the profile of the disease, thus ensuring that there are specific measures and better control of COVID-19.
The present study stands out for bringing a comparative analysis of epidemiological outcomes between two states in the period from 2020 to 2022, however, it presents aspects of limitations regarding the information analyzed, considering that the process of updating information in municipalities, states and at the federal level it is dynamic and complex, where data undergoes changes every day.
5. Conclusions
There were 15,400 deaths in the state of Espírito Santo and 64,498 deaths in the state of Minas Gerais confirmed by COVID-19 in the period from January 2020 to December 2022.
When comparing the rates studied during this period, it was possible to observe that the state of Espírito Santo had a higher incidence of COVID-19, as well as higher mortality, when compared to the state of Minas Gerais. In turn, with regard to lethality, Minas Gerais stood out throughout the period of analysis, presenting the highest rate. Although divergent, both states had higher records in similar months, with specific months of greater festivities.
Furthermore, it was observed that both states showed equal trends for mortality, lethality and incidence in the years 2020 and 2021. For the year 2022, Minas Gerais presents decreasing mortality and incidence and increasing lethality, while the state of Espírito Santo presents a stationary trend for all variables.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chen, S.; et al. COVID-19 control in China during mass population movements at New Year. Lancet. 2020, 395, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Triukose, S.; et al. Effects of public health interventions on the epidemiological spread during the first wave of the COVID-19 outbreak in Thailand. PLoS One. 2021, 16, e0246274. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard, 2023. Available at: <https://covid19.who.int/>. Accessed: August 30, 2023.
- World Health Organization. COVID-19 weekly epidemiological update, edition 126, January 19, 2023. Available at: <https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---19 -january-20232023>. Accessed: January 24, 2023.
- World Health Organization. COVID-19 weekly epidemiological update, edition 158, September 1, 2023. Available at: <https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---1 -september-2023>. Accessed: September 01, 2023.
- Centers for Disease Control and Prevention. Implementation of Mitigation Strategies for Communities with Local COVID-19 Transmission [Internet]. Coronavirus Disease 2019 (COVID-19).
- Van Goethem, N.; et al. Clinical severity of SARS-CoV-2 Omicron variant compared with delta among hospitalized COVID-19 patients in Belgium during Autumn and Winter Season 2021–2022. Viruses. 2022, 14, 1297. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; et al. Coronavirus infections and immune responses. J Med Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Zhang JJ.; et al. Risk and protective factors for COVID-19 morbidity, severity, and mortality. Clin Rev Allergy Immunol. 2022:1-18.
- Abate, SM.; et al. Rate of Intensive Care Unit admission and outcomes among patients with coronavirus: A systematic review and Meta-analysis. PLoS One. 2020, 15, e0235653. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Statement on the fifteenth meeting of the IHR (2005) Emergency Committee on the COVID-19 pandemic. Available at: <https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency- committee-regarding-the-coronavirus-disease-(covid-19)-pandemic>. Accessed: August 16, 2023.
- Brazil. Panel of coronavirus disease 2019 (COVID-19) cases in Brazil by the Ministry of Health, 2023. Available at: <https://covid.saude.gov.br/>. Accessed: September 06, 2023.
- Antunes JL, Cardoso MRA. Use of time series analysis in epidemiological studies. Epidemiol Serv Saude. 2015, 24:565-576.
- Abreu LC, Elmusharaf K, Siqueira CEG. A time-series ecological study protocol to analyze trends of incidence, mortality, lethality of COVID-19 in Brazil. J Hum Growth Dev. 2021, 31, 491–495.
- IBGE. Brazilian Institute of Geography and Statistics. Cities and States. Holy Spirit. Available at: <https://www.ibge.gov.br/cidades-e-estados/es.html>. Accessed: January 01, 2023.
- IBGE. Brazilian Institute of Geography and Statistics. Cities and States. Minas Gerais. Available at: <https://www.ibge.gov.br/cidades-e-estados/mg.html>. Accessed: January 01, 2023.
- Holy Spirit. State Department of Health of Espírito Santo. Available at: <https://www.es.gov.br/Noticia/sesa-moradores-de-23-cidades-da-divisa-com-minas-serao-imunizados-contra-febre-amarela>. Accessed: August 02, 2023.
- DATASUS. Department of Informatics of the Unified Health System. 2022. Available at: <https://datasus.saude.gov.br/informacoes-de-saude-tabnet/>. Accessed: August 12, 2022.
- StataCorp, LLC Stata Statistical Software: Release 17.0 College Station, TX, 2019.
- Ren B, Hwang WT. Modeling post-holiday surge in COVID-19 cases in Pennsylvania counties. PLoS One. 2022, 17, e0279371.
- Hadianfar, A. Effects of government policies and the Nowruz holidays on confirmed COVID-19 cases in Iran: An intervention time series analysis. PLoS One. 2021, 16, e0256516. [Google Scholar] [CrossRef] [PubMed]
- Superior Electoral Court. Electoral statistics, 2022. Available at: <https://sig.tse.jus.br/ords/dwapr/r/seai/sig-eleicao-comp-abst/home?session=3835825175764>. Accessed: August 01, 2023.
- Wu X.; et al. Air pollution and COVID-19 mortality in the United States: Strengths and limitations of an ecological regression analysis. Sci Adv. 2020, 6, eabd4049. [CrossRef]
- Wong DWS, Li Y. Spreading of COVID-19: Density matters. PLoS One. 2020, 15, e0242398. [Google Scholar]
- Sutton, J.; et al. Population density and spread of COVID-19 in England and Wales. PLoS One. 2022, 17, e0261725. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi K, Fujiwara N, Itoh R. Influence of trip distance and population density on intra-city mobility patterns in Tokyo during COVID-19 pandemic. PLoS One. 2022, 17, e0276741. [Google Scholar]
- Du, Z.; et al. Effects of proactive social distancing on COVID-19 outbreaks in 58 cities, China. Emerg Infect Dis. 2020, 26, 2267. [Google Scholar] [CrossRef]
- Remuzzi A, Remuzzi G. COVID-19 and Italy: what next? Lancet. 2020, 395, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Adamoski, D.; et al. SARS-CoV-2 Delta and Omicron variants emerge in Curitiba, Southern Brazil, and its impact on overall COVID-19 lethality. Viruses. 2022.
- CDC COVID Response Team. SARS-CoV-2 B.1.1.529 (Omicron) variant—United States, December 1–8, 2021. Morbidity and Mortality Weekly Report. 2021, 70, 1731. [Google Scholar] [CrossRef] [PubMed]
- Johnson, AG. COVID-19 incidence and death rates among unvaccinated and fully vaccinated adults with and without booster doses during periods of Delta and Omicron variant emergence—25 US Jurisdictions, April 4–December 25, 2021. MMWR Morb Mortal Wkly Rep. 2022, 71. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Map of Brazil with representation of the states Espírito Santo and Minas Gerais. Source: IBGE (2023).
Figure 1.
Map of Brazil with representation of the states Espírito Santo and Minas Gerais. Source: IBGE (2023).
Figure 2.
Map of the states of Espírito Santo and Minas Gerais. Source: IBGE (2023).

Figure 3.
Comparative incidence graph (100,000 inhabitants) for the states Espírito Santo (ES) and Minas Gerais (MG) for the years 2020 (A), 2021 (B) and 2022 (C). Source: Prepared by the author (2023).
Figure 3.
Comparative incidence graph (100,000 inhabitants) for the states Espírito Santo (ES) and Minas Gerais (MG) for the years 2020 (A), 2021 (B) and 2022 (C). Source: Prepared by the author (2023).
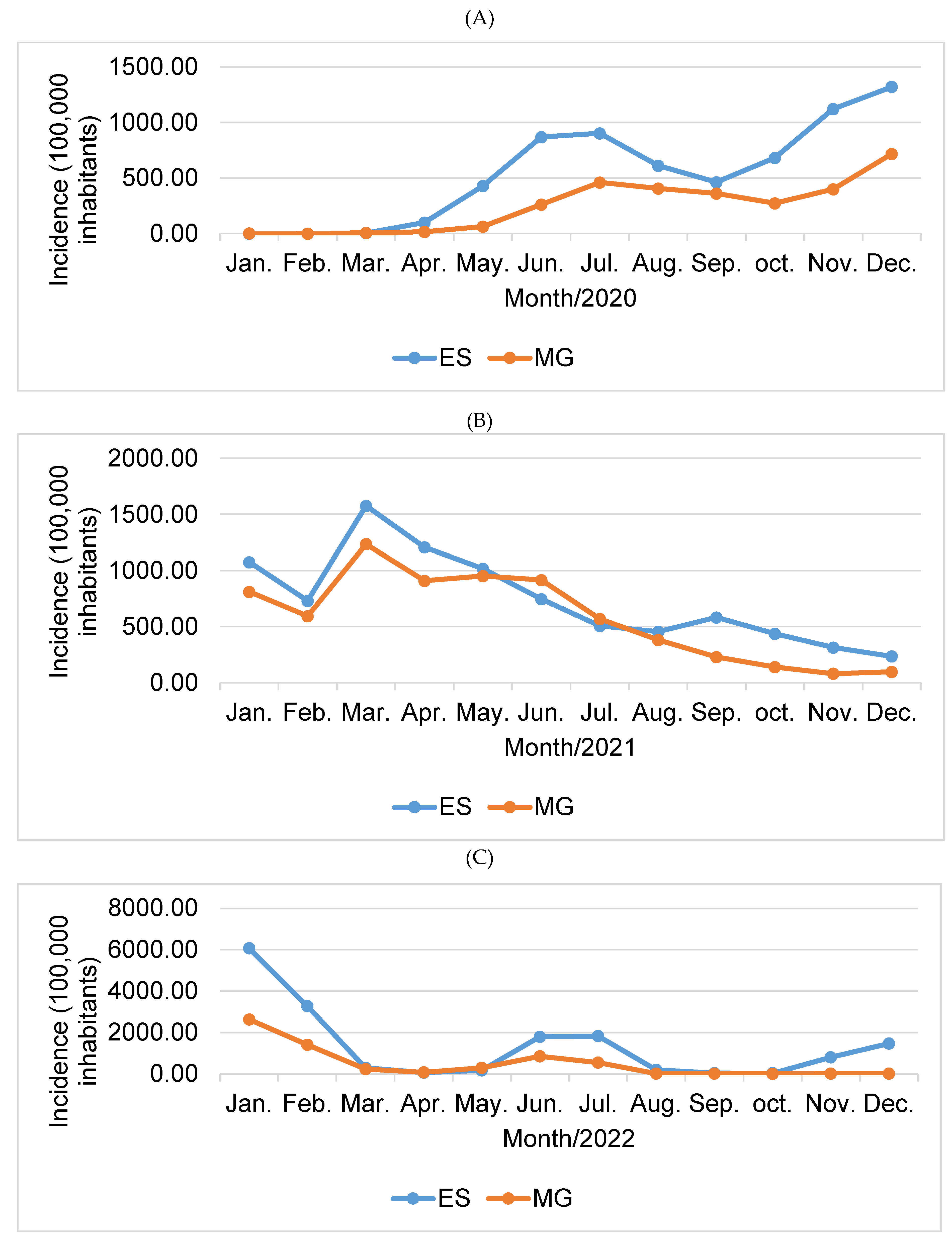
Figure 4.
Comparative graph of lethality (%) for the states of Espírito Santo (ES) and Minas Gerais (MG) for the years 2020 (D), 2021 (E) and 2022 (F). Source: prepared by the author (2023).
Figure 4.
Comparative graph of lethality (%) for the states of Espírito Santo (ES) and Minas Gerais (MG) for the years 2020 (D), 2021 (E) and 2022 (F). Source: prepared by the author (2023).
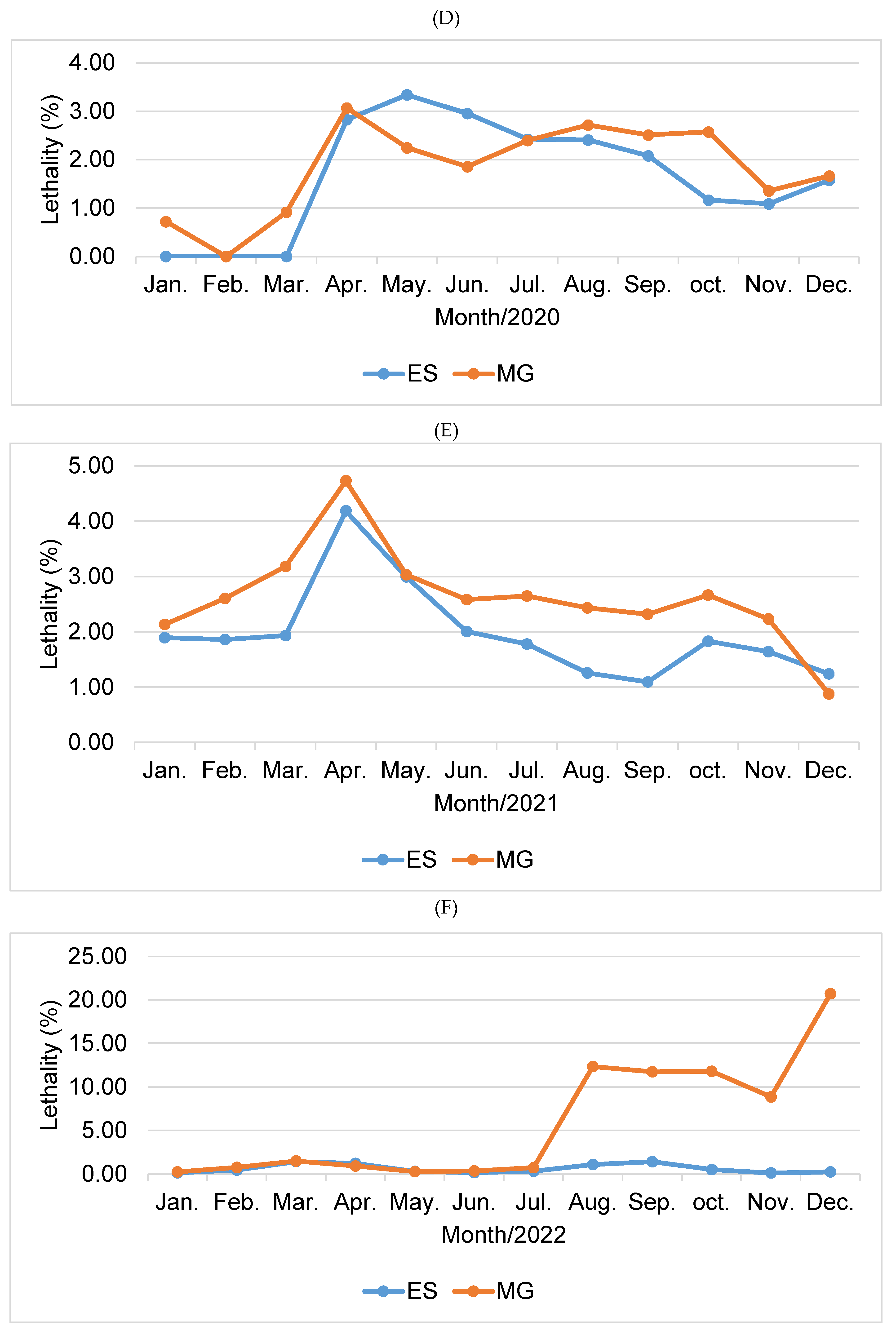
Figure 5.
Comparative mortality graph (100,000 inhabitants) for the states Espírito Santo (ES) and Minas Gerais (MG) for the years 2020 (G), 2021 (H) and 2022 (I). Source: prepared by the author (2023).
Figure 5.
Comparative mortality graph (100,000 inhabitants) for the states Espírito Santo (ES) and Minas Gerais (MG) for the years 2020 (G), 2021 (H) and 2022 (I). Source: prepared by the author (2023).
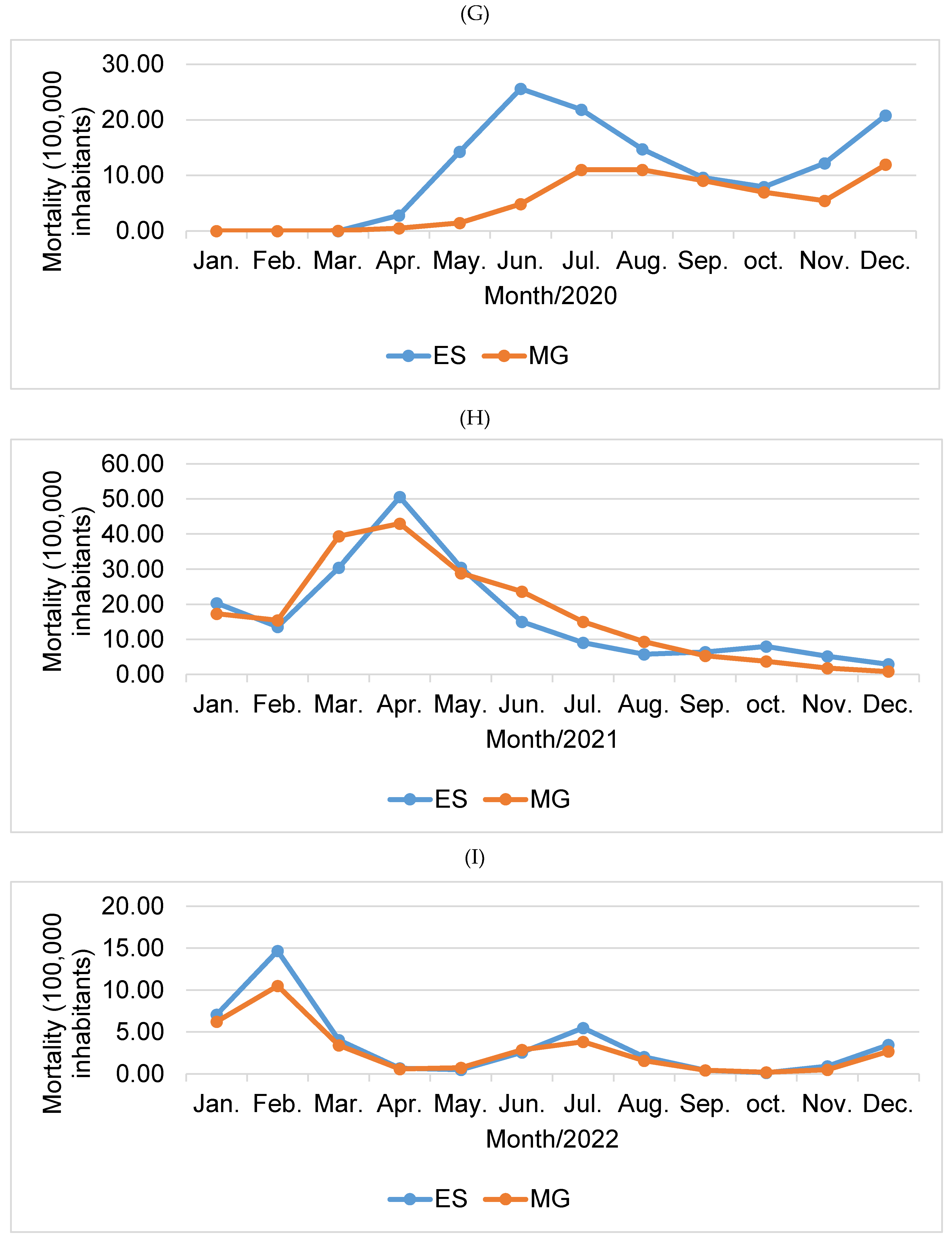

Table 1.
Monthly distribution of cases and deaths confirmed by COVID-19 in the state of Espírito Santo, Brazil, from January 2020 to December 2022.
Table 1.
Monthly distribution of cases and deaths confirmed by COVID-19 in the state of Espírito Santo, Brazil, from January 2020 to December 2022.
| Year | Month | Confirmed cases | Confirmed deaths | ||
|---|---|---|---|---|---|
| Frequency absolute (n) |
Frequency relative (%) |
Frequency absolute (n) |
Frequency relative (%) |
||
| 2020 | January | 0 | 0.00 | 0 | 0.00 |
| February | 1 | 0.00 | 0 | 0.00 | |
| March | 151 | 0.01 | 0 | 0.00 | |
| April | 4101 | 0.31 | 116 | 0.75 | |
| May | 17704 | 1.35 | 591 | 3.84 | |
| June | 35880 | 2.73 | 1060 | 6.88 | |
| July | 37305 | 2.84 | 904 | 5.87 | |
| August | 25285 | 1.92 | 609 | 3.95 | |
| September | 19108 | 1.45 | 397 | 2.58 | |
| October | 28160 | 2.14 | 328 | 2.13 | |
| November | 46414 | 3.53 | 505 | 3.28 | |
| December | 54659 | 4.16 | 861 | 5.59 | |
| Total | 268,768 | 20.46 | 5,371 | 34.88 | |
| 2021 | January | 44897 | 3.42 | 851 | 5.53 |
| February | 30527 | 2.32 | 568 | 3.69 | |
| March | 65900 | 5.02 | 1274 | 8.27 | |
| April | 50456 | 3.84 | 2112 | 13.71 | |
| May | 42498 | 3.23 | 1273 | 8.27 | |
| June | 31201 | 2.38 | 626 | 4.06 | |
| July | 21211 | 1.61 | 377 | 2.45 | |
| August | 19037 | 1.45 | 239 | 1.55 | |
| September | 24322 | 1.85 | 266 | 1.73 | |
| October | 18278 | 1.39 | 334 | 2.17 | |
| November | 13116 | 1.00 | 215 | 1.40 | |
| December | 9852 | 0.75 | 122 | 0.79 | |
| Total | 371,295 | 28.26 | 8,257 | 53.62 | |
| January | 255645 | 19.46 | 298 | 1.94 | |
| February | 137628 | 10.48 | 619 | 4.02 | |
| March | 12073 | 0.92 | 171 | 1.11 | |
| April | 2394 | 0.18 | 29 | 0.19 | |
| May | 7262 | 0.55 | 21 | 0.14 | |
| June | 75481 | 5.75 | 108 | 0.70 | |
| July | 77148 | 5.87 | 231 | 1.50 | |
| 2022 | August | 7938 | 0.60 | 85 | 0.55 |
| September | 1372 | 0.10 | 19 | 0.12 | |
| October | 1202 | 0.09 | 6 | 0.04 | |
| November | 33716 | 2.57 | 39 | 0.25 | |
| December | 61788 | 4.70 | 146 | 0.95 | |
| Total | 673,647 | 51.28 | 1772 | 11.51 | |
| Total | 1,313,710 | 100.00 | 15,400 | 100.00 | |
Source: Information extracted by the author from the Coronavirus Panel, (2023).
Table 2.
Monthly distribution of cases and deaths confirmed by COVID-19 in the state of Minas Gerais, Brazil, from January 2020 to December 2022.
Table 2.
Monthly distribution of cases and deaths confirmed by COVID-19 in the state of Minas Gerais, Brazil, from January 2020 to December 2022.
| Year | Month | Confirmed cases | Confirmed deaths | ||
|---|---|---|---|---|---|
| Frequency absolute (n) |
Frequency relative (%) |
Frequency absolute (n) |
Frequency relative (%) |
||
| 2020 | January | 139 | 0.00 | 1 | 0.00 |
| February | 38 | 0.00 | 0 | 0.00 | |
| March | 1090 | 0.03 | 10 | 0.02 | |
| April | 3261 | 0.10 | 100 | 0.16 | |
| May | 13596 | 0.40 | 305 | 0.47 | |
| June | 55809 | 1.63 | 1035 | 1.60 | |
| July | 98548 | 2.87 | 2360 | 3.66 | |
| August | 87196 | 2.54 | 2365 | 3.67 | |
| September | 77405 | 2.26 | 1941 | 3.01 | |
| October | 58327 | 1.70 | 1499 | 2.32 | |
| November | 85455 | 2.49 | 1160 | 1.80 | |
| December | 153817 | 4.48 | 2560 | 3.97 | |
| Total | 634,681 | 18.50 | 13,336 | 20.68 | |
| 2021 | January | 174870 | 5.10 | 3730 | 5.78 |
| February | 127810 | 3.73 | 3329 | 5.16 | |
| March | 266414 | 7.77 | 8483 | 13.15 | |
| April | 195856 | 5.71 | 9262 | 14.36 | |
| May | 205034 | 5.98 | 6220 | 9.64 | |
| June | 197379 | 5.75 | 5100 | 7.91 | |
| July | 122518 | 3.57 | 3243 | 5.03 | |
| August | 82423 | 2.40 | 2006 | 3.11 | |
| September | 49316 | 1.44 | 1143 | 1.77 | |
| October | 30301 | 0.88 | 807 | 1.25 | |
| November | 17368 | 0.51 | 388 | 0.60 | |
| December | 20915 | 0.61 | 183 | 0.28 | |
| Total | 1,490,204 | 43.44 | 43,894 | 68.05 | |
| January | 568480 | 16.57 | 1348 | 2.09 | |
| February | 302803 | 8.83 | 2275 | 3.53 | |
| March | 49652 | 1.45 | 739 | 1.15 | |
| April | 13956 | 0.41 | 127 | 0.20 | |
| May | 63177 | 1.84 | 157 | 0.24 | |
| June | 182948 | 5.33 | 619 | 0.96 | |
| July | 116177 | 3.39 | 829 | 1.29 | |
| 2022 | August | 2792 | 0.08 | 345 | 0.53 |
| September | 792 | 0.02 | 93 | 0.14 | |
| October | 381 | 0.01 | 45 | 0.07 | |
| November | 1253 | 0.04 | 111 | 0.17 | |
| December | 2803 | 0.08 | 580 | 0.90 | |
| Total | 1,305,214 | 38.05 | 7,268 | 11.27 | |
| Total | 3,430,099 | 100.00 | 64,498 | 100.00 | |
Source: Information extracted by the author from the Coronavirus Panel, (2023).
Table 3.
Prais-Winsten regression estimates and daily change variation (DPC) of mortality, lethality and incidence rates of COVID-19 in the states of Espírito Santo and Minas Gerais, Brazil, from January 2020 to December 2020 2022.
Table 3.
Prais-Winsten regression estimates and daily change variation (DPC) of mortality, lethality and incidence rates of COVID-19 in the states of Espírito Santo and Minas Gerais, Brazil, from January 2020 to December 2020 2022.
| RATE/YEAR | β | DPC (IC95%) | P | Trend |
|---|---|---|---|---|
| ESPÍRITO SANTO | ||||
| MORTALITY | ||||
| 2020 | 0.0023056 | 0.53 (0.16 : 0.90) | 0.005* | Growing |
| 2021 | -0.002948 | -0.68 (-0.80: -0.55) | <0.001* | Descending |
| 2022 | -0.0011957 | -0.27 (-0.58 : 0.03) | 0.076 | Stationary |
| LETHALITY | ||||
| 2020 | -0.0019347 | -0.44 (-0.57 : -0.32) | <0.001* | Descending |
| 2021 | -0.0008737 | -0.20 (-0.29 : -0.11) | <0.001* | Descending |
| 2022 | -0.0000461 | -0.01 (-0.39 : 0.37) | 0.957 | Stationary |
| INCIDENCE | ||||
| 2020 | 0.0084347 | 1.96 (1.26 : 2.67) | <0.001* | Growing |
| 2021 | -0.0020619 | -0.47 (-0.56 : -0.38) | <0.001* | Descending |
| 2022 | -0.0020398 | -0.47 (-1.20 : 0.27) | 0.209 | Stationary |
| MINAS GERAIS | ||||
| MORTALITY | ||||
| 2020 | 0.0063002 | 1.46 (1.03 : 1.90) | <0.001* | Growing |
| 2021 | -0.0041913 | -0.96 (-1.25 : -0.67) | <0.001* | Descending |
| 2022 | -0.002702 | -0.62 (-1.07 : -0.16) | 0.008* | Descending |
| LETHALITY | ||||
| 2020 | -0.0008331 | -0.19 (-0.31 : -0.07) | 0.002* | Descending |
| 2021 | -0.0008216 | -0.19 (-0.29 : -0.09) | <0.001* | Descending |
| 2022 | 0.0059761 | 1.39 (1.11 : 1.66) | <0.001* | Growing |
| INCIDENCE | ||||
| 2020 | 0.0122493 | 2.86 (2.26 : 3.46) | <0.001* | Growing |
| 2021 | -0.0034395 | -0.79 (-0.93 : -0.65) | <0.001* | Descending |
| 2022 | -0.0078885 | -1.80 (-2.35 : -1.25) | <0.001* | Descending |
β – regression coefficient; P – p-value; DPC – daily percentage change; 95% CI - 95% confidence interval. ( * ) Statistical difference detected by the Prais-Winsten regression test, p<0.05. Source: prepared by the author (2023).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



