
Submitted:
30 April 2024
Posted:
01 May 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Myalgic Encephalomyelitis, also known as Chronic Fatigue Syndrome (ME/CFS) and Long COVID are characterized by debilitating post-exertional malaise and other core symptoms related to immune dysregulation resultant from post-viral infection, including mitochondrial dysfunction, chronic neuroinflammation and gut dysbiosis. The reported associations between altered microbiota composition and cardinal symptoms of ME/CFS and Long COVID, suggesting that use of microbial preparations, such as probiotics, by restoring the homeostasis of the brain-immune-gut axis may help in the management of symptoms in both conditions. Therefore, this review aims to investigate the implications of alerted gut microbiome and assess the evidence supporting use of microbial-based preparations, including probiotics, synbiotics, postbiotics alone and/or in combination with other nutraceuticals in the management of fatigue, inflammation, as well as neuropsychiatric and gastrointestinal symptoms among patients with ME/CFS and Long COVID.
Keywords:
probiotics
; gut microbiota
; gut-brain axis
; chronic fatigue syndrome
; myalgic encephalomyelitis
; long covid
; prebiotics
; dietary supplementation
; antioxidants
; inflammation
; psychobiotics
1. Introduction
Myalgic Encephalomyelitis, also referred to as Chronic Fatigue Syndrome (ME/CFS) is a complex and debilitating condition affecting ~67 million people worldwide [1] characterized by persistent fatigue not improved by the rest or sleep, and post-exertional malaise (PEM) resultant from minor physical or mental activity; consequently, leading to decline in cognitive impairment, including problems with concentration, thinking and memory [2]. In addition, individuals with ME/CFS may also experience a constellation of other non-specific symptoms of pain, headaches, disrupted sleep, myalgias and arthralgias, orthostatic intolerance, autonomic dysfunction [2], as well as gastrointestinal (GI) problems [3] which greatly interfere with their ability to function and significantly compromise individual productivity and quality of life [4]. Although there is no specific testing available for ME/CFS, the diagnosis of this condition is made through the medical history, physical examination and laboratory tests along with clinical assessment including use of consensued diagnostic criteria [5], which requires a presence of four key symptoms for at least period of 6 months, including debilitating fatiguability, post-exertional malaise, unrefreshing sleep and cognitive difficulties [6] possibly accompanied by other manifestations, of which the most common are orthostatic intolerance and autonomic dysfunction (e.g., dizziness; palpitations; fainting; nausea when standing or sitting upright); pain (e.g., myalgias, headaches, abdominal pain or joint pain); neuromuscular symptoms (e.g., twitching and myoclonic jerks); flu-like symptoms (e.g., sore throat, tender glands, nausea, chills or muscle aches) and hypersensitivities to temperature, certain foods and sensory exposures of light, noise, touch and smell [7].
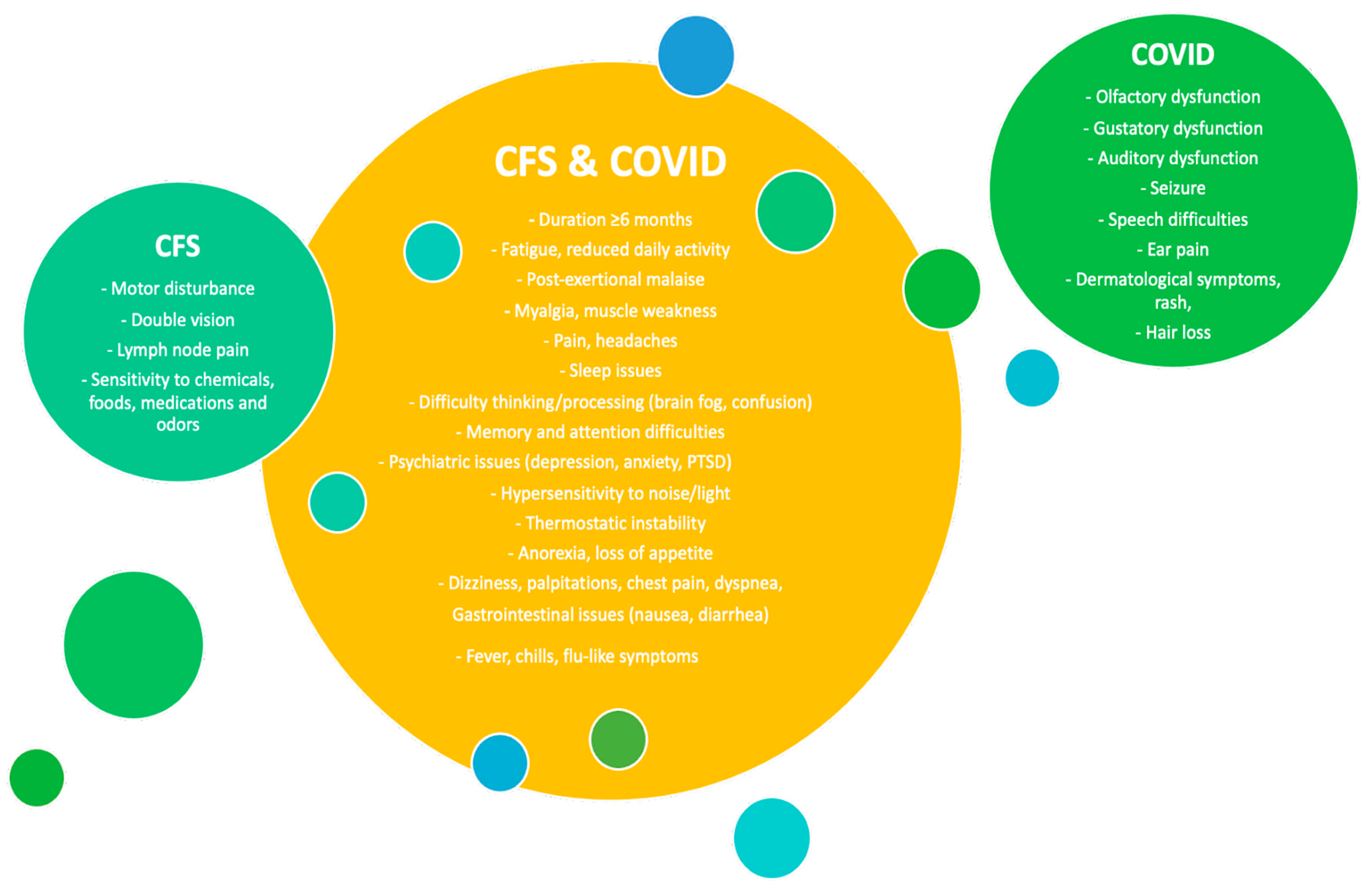
Complex and non-specific symptomology of ME/CFS may lead to many misdiagnoses, with other serious illnesses, including fibromyalgia, primary sleep disorders (sleep apnea), nutritional disorders (iron deficiency, obesity), musculo-skeletal conditions, anxiety and depression, as well as GI diseases (coeliac disease, irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD)) [8]. In addition, recent studies conducted shortly after the onset of the COVID-19 pandemic, suggested that symptoms of ME/CFS are similar to those reported by approximately 87% of patients recovering from acute infection with SARS-CoV-2 [9,10], which significantly interfered with their ability to function and execute daily tasks condition referred as Long COVID [10]. Despite lack of evidence for the major injury in organs caused by the infection, these individuals have been shown to experience 25 out of 29 known ME/CFS symptoms at least once, also including those, considered as the key features used by the diagnostic criteria for ME/CFS including reduced daily activity, PEM and fatigue, being the dominant one. Interestingly, Long COVID patients also have reported other dysfunctions, which previously were associated with, including neurologic pain, neurocognitive and psychiatric symptoms, however with no cases of rash, as well as olfactory and gustatory dysfunction [11] (Figure 1).
Figure 1.
Comparison of symptoms reported in ME/CFS and Long COVID. Based on [11].
Figure 1.
Comparison of symptoms reported in ME/CFS and Long COVID. Based on [11].
Although the exact aetiology of ME/CFS, neither Long COVID still needs to be determined, evidence to date indicate as post-viral syndromes, being most likely triggered by the infectious agent, such as Epstein Barr Virus [12] and SARS-CoV-2 in Long COVID [13], respectively, also share biological abnormalities, with examples of the cognitive deficits, including impaired attention and information processing speed, dysregulation of the hypothalamic-pituitary (HP) axis, and abnormal immune cytokine profile [14], characterized by high auto-antibodies titres against neural and autonomic targets [15,16] including neurotransmitter receptors against nuclear and membrane structures, such as cardiopin and phospholipids, neurotransmitter receptors (e.g., muscarinic M1 acetylcholine receptor (AChR) and ß1- and ß2-adrenergic receptors (AdR) and M2/3 [17]); as well as and increased levels of proinflammatory mediators, interleukin (IL) IL-1 (IL-1α, IL-1β), IL-4, IL-5, IL-6, and IL-12, TNF-α, IL-10, IL-13, IL-16, INF-γ, and IL-17, IL-17A (but reduced IL-17F) [18,19,20], further linked with severity of after mentioned symptoms [21]. In particularly, metabolic abnormalities along with mitochondrial dysfunction and impaired redox balance [22] characterized by increased oxidative toxicity and lowered antioxidant defenses were associated with the development of symptoms of pain and hyper-sensitivity [23] and severity of neuropsychiatric symptoms in both ME/CFS [18] and Long COVID [24]. Noteworthy, mitochondrial dysfunction, as an important contributor to both ME/CFS and Long COVID-19 conditions [25,26] through increasing production of free radicals can promote chronic inflammation, which along aberrant immune responses reported in ME/CFS and COVID-19 [27] attributed to diminished natural killer cell function, T cell exhaustion/abnormalities, overactivation of mast cell along associated with possible viral reactivation, triggered by viral infection/infectious agent may increase risk of autoimmunity and hyper-inflammation [28] including systemic inflammation and neuroinflammation [29], which were associated with muscle weakness [30], fatigue and pain [31], as well as other comorbidities, such as major depression [32] postural tachycardia syndrome [33] and GI conditions, like development allergic reactions and sensitivities to odors, chemicals and foods including alcohol, caffeine, sweeteners, and food additives [34]. Some studies suggest that Long COVID patients may acquire new food allergies and sensitivities, especially to wheat and gluten with the incidence of GI symptoms ranging from 3% to 79% [35]. Similarly, GI symptoms are also considered as frequent comorbidity for up to 92% ME/CFS patients, who are co-diagnosed with irritable bowel syndrome (IBS) [2], while GI complaints, including abdominal pain and bloating, along with extraintestinal symptoms of fatigue, headache and cognitive impairments could be developed due to chronic gut inflammation compromised intestinal epithelium barrier [36], followed by significantly increased proportion of mucosal associated invariant T (MAIT) cells [37], which are implicated in the recognition of microbial antigens on the MHC Class I-related molecule [38], and response upon cytokine-induced stimulation during microbial infection [39].
Furthermore, the proposed hypothesis indicating that persistent infection or unviable pathogen residues can stimulate chronic inflammation, as both enteric viruses and bacterial infections can affect the microbiome [40]; the alteration in the composition of the gut microbiota in both Long COVID and ME/CFS patients along with reported GI symptoms of nausea, diarrhea and abdominal pain [41] may suggest a potential role of gut dysbiosis in the development of both conditions. Research to date have shown that gut dysfunction, characterized by altered intestinal microbiota composition, gut barrier dysfunction, and gut inflammation can be a potential factor in ME/CFS development [3]; whereas in Long COVID patients w persisted symptoms of inflammation and poor cognitive performance for few months after acute infection, alterations in the gut microbiota along with reduced microbial diversity was linked to disease severity and reported by patients Long COVID symptoms, including lung, all supporting a potential contribution of disturbed gut microbiome in Long COVID sequelae [42].
Microbial preparations, not limited to use of live probiotic strains, but also their by-products alone or with combination with other naturally sourced bioactives (naturaceuticals) with antioxidant and anti-inflammatory properties may offer potential benefits for individuals affected by Long COVID and ME/CFS, in particularly that both conditions are lacking effective treatment strategies [43,44]. Evidence to date, indicate that intake of probiotics, e.g., live bacteria and yeasts either as dietary supplements or food sources, such as yogurt, kefir, sauerkraut, miso, and tempeh, due to their positive effects on the gut health and immune function. Clinical trials conducted in the ME/CFS indicated that probiotic supplementation may help in restoring gut microbiota homeostasis and reducing inflammation and cognitive dysfunction [45]. Similarly, symbiotic supplementation consisting of probiotic/prebiotic blend of Lactobacteria strains with inulin have been shown to improve health status of individuals with Long COVID, leading to reduced cough, fatigue and gut symptoms [46].
Given the possible role of microbiome dysbiosis in shared manifestations reported in Long COVID and ME/CFS, along with beneficial effects of the therapeutic interventions with microbial preparations on the restoring gut homeostasis, might serve a novel approach for management of shared by ME/CFS and Long COVID symptoms, including chronic inflammation, cognitive and bowel dysfunctions. The main aim of this review is to investigate the implications of alerted gut microbiome and assess the evidence supporting use of microbial-based preparations, including probiotics, synbiotics, postbiotics alone and/or in combination with other nutraceuticals in the management of fatigue, inflammation, as well as psychiatric and gastrointestinal symptoms among patients with ME/CFS and Long COVID.
2. Role of the Alerted Gut Microbiome in ME/CFS and Long COVID Pathogenesis
The gut microbiota is a tightly regulated microbial community of more than more than 10^14 microorganisms [47] of archaea, viruses, fungi and protists, which in humans is dominated by Firmicutes, Bacteroidetes, Proteobacteria, and Actinobacteria [48]. Microbiota works in partnership with host immune system to fulfill essential roles for optimal health and wellbeing, by supporting immunity and metabolism directly, as well as through of bioactive compounds, including short chain fatty acids (SCFA, e.g., acetate, propionate and butyrate; amino acids (e.g. γ-aminobutyric acid (GABA)) and vitamins, which acting on the gut-brain axis, which actively modulate digestive and cognitive functions [49]. The gut microbiota is also an essential component of the host's defense mechanisms against infections, additionally contributing to maintenance of intestinal homeostasis and gut barrier integrity [50]. Nevertheless, exposure to various factors, including diet, medications/antibiotics and certain lifestyle habits (e.g., smoking) can influence gut microbiota composition, leading to the colonization of opportunistic pathogens and intestinal barrier dysfunction. Imbalance of the gut microbiota community, also referred as gut dysbiosis, was linked with increased intestinal permeability and tight junction dysfunction, which allowing the entry of commensal microbes, microbial-derived products, and other luminal components [51] contribute to aberrant immune responses and increasing the risk of infections and chronic diseases, including obesity, diabetes, IBD, cardiovascular disease (CVD) [52].
The reported alterations in the gut composition from ME/CFS and Long COVID patients warrant attention as they were associated with shared by both conditions’ symptoms of fatigue, PM, pain, sleep problems, mental and GI disturbances [11] as well as immunological abnormalities. Although these observations may suggest the role of gut dysbiosis in the symptom development [53] a specific microbial signature has not been found yet [2]. Investigations of the microbiome dysbiosis was intensively studied in ME/CFS, with results indicating for a potential link between changes gut composition, including deficient butyrate-producing capacity and bacterial network disturbances, increased immune activation [54,55,56], and symptoms of fatigue symptoms [2,57]. That decreased availability of butyrate, along with other key mediators of the gut-brain axis produced during microbial fermentation, including serotonin and γ-aminobutyric acid (GABA) via influencing on intestinal permeability may have considerable impact on the neuro-immunoendocrine system [58]. In addition, studies from physically fit populations indicated for a strong correlation between increased gut microbial diversity, high fecal butyrate levels and extent of physical fitness characterized by the higher VO2 peaks and consequently reduced LPS levels and lower inflammation [59], thereby suggesting that the decreased abundance of anti-inflammatory bacteria, such as Firmicutes and Actinobacteria [54] along with butyrate-producers may result in PEM followed by inactivity and increased LPS-induced inflammation in ME/CFS. In addition, ME/CFS patients, compared to healthy controls, seem to have also higher levels of pro-inflammatory gram-negative bacteria species, such as Alistipes, Bacteroidetes and Enterobacteriaceae [54,56,60] which may worsen disease course, leading to increased severity of feeling of fatigue, pain, and confusion [54]. In addition, ME/CFS was associated with the reduction of certain bacteria taxa of the Firmicutes phylum, including Faecalibacterium, Roseburia and Clostridium genera, of which a decrease of butyrate-producer Faecalibacterium was considered as potential biomarker with diagnostic value in ME/CFS [56]. Noteworthy, associations between reduced abundance of Faecalibacterium increased fatigue perception were found in the IBD, cancer and autoimmune patients, such as MS and diabetes type 1 [2], thereby suggesting that presence of systemic inflammation along with gut microbiota dysbiosis [61] may affect the bidirectional connection with other vital organs [62], and lead to development of psychiatric and GI symptoms, also reported in ME/CFS. Previous studies have shown that reductions in the Firmicutes a gram-positive bacterium which include beneficial lactic acid bacteria such as Actinobacteria, (e.g., Collinsella and Bifidobacterium spp. Bifidobacteria), in expense of gram-negative bacteria, such as Bacteroidetes, and Proteobacteria, can alter immune response, promote pro-inflammatory cytokine production and increase gut barrier permeability further leading to chronic inflammation [63], which in case of ME/CFS was implicated in development of cognitive disfunctions, as well as sleep problems, and various physical symptoms like muscle aches, flu-like symptoms, and weight changes [45]. Therefore, a reported presence of gut inflammation in MS/CFS may contribute to neuroimmune dysfunction followed by the gradual activation of innate responses in the brain-via vagus nerve and a reduction of energy-consuming activities in ME/CFS [2]. For instance, a reduced abundance of Actinobacteria reported in in ME/CFS patients [64] was previously associated with GI conditions, including IBD, IBS; as well as neuropsychiatric diseases, such as anxiety and depression. Interestingly, ME/CFS patients who reported IBS and high anxiety/depression symptoms, had significantly lower alpha diversity of gut microbiome, compared to healthy controls and IBS-only cohorts, suggesting that comobid IBS and anxiety/depression may be linked with higher Proteobacteria, Prevotella/Prevotellaceae, Bacteroides and lower Lachnospiraceae abundances relatively to controls [65]. This complex crosstalk between the HPA axis, immune factors, and the autonomic nervous system highlight the role of dysregulated gut-brain axis in the establishment of low-grade gut mucosal barrier inflammation, followed by increased visceral hypersensitivity and increased intestinal permeability leaky gut in ME/CFS patients [2].
Previous evidence obtained over pandemic, has revealed that gut dysbiosis is associated with the severity of acute COVID-19 infection and long-lasting multisystem complications after disease recovery [66], with currently growing number of studies reporting changes in the intestinal composition in Long COVID patients, who recovered from acute infection. These individuals have been shown to have significant changes in the gut composition, characterized by reduction of commensal species remaining low up to 30 days, including Eubacterium rectale, Faecalibacterium prausnitzii and bifidobacterial species (e.g., Lactobacillus, Bifidobacterium, Bacteroides and Faecalibacterium; whereas the richness of the microbial community seem to not recover even after six months of convalescence [67,68,69]. Noteworthy, the reduced abundance of Faecalibacterium prausnitzii, as well as decrease in anti-inflammatory species, Alistipes onderdonkii and Faecalibacterium prausnitzii, reflected by increased levels of pro-inflammatory cytokine levels, including IL-2, IL-7, IL10, TNF-α, was strongly associated with disease severity [70] and increased severity of symptoms, including respiratory, neuropsychiatric, gastrointestinal and fatigue issues [71]. In addition, an observational study conducted in group of patients who developed Long COVID symptoms 6 months after initial diagnosis (76% of initial sample of 106 patients) had significantly higher levels of Ruminococcus gnavus, Bacteroides vulgatus and lower levels of Faecalibacterium prausnitzii, which were correlated with persistent respiratory symptoms, as well as neuropsychiatric complaints and fatigue, including Clostridium innocuum and Actinomyces naeslundii. Interestingly, butyrate-producing bacteria, including Bifidobacterium pseudocatenulatum and Faecalibacterium prausnitzii, showed the largest inverse correlations with Long COVID symptoms at 6 months [72]. Interestingly, a prospective follow up study conducted in symptomatic patients recovered from COVID-19 reported a presence of certain gut microbiota dysbiosis including significantly reduced bacterial diversities and lower relative abundance of SCFAs producers, such as Eubacterium hallii, Subdoligranulum, Ruminococcus, Dorea, Coprococcus, and Eubacterium ventriosum a year after discharge. Interestingly, individuals experiencing that long-term symptom of physical function impairment, psychiatric disorders, mainly in anxiety or depression; lung functions reduction, and radiographic abnormalities persisted to 12 months in individuals with altered gut microbiota was significantly correlated with clinical indices of the recovery stage, thereby suggesting that gut microbiota may play an important role in Long COVID-19 [74].
3. Use of Probiotic in the Management of ME/CFS and Long COVID Symptoms
Probiotics along with prebiotics are the two components in our diet that can affect the microbiome [74]. Probiotics, as live microorganisms which are administered in adequate amounts [75] utilizing non-digestible fibers of prebiotics, can bring health benefits to the host [74], including improved digestion and immunity, and by modulating immune signaling pathways and enhancing gut microbiota function within the gut-lung and gut-brain axes [76], reduce common symptoms of infection [77], and increase resistance to the infectious agent. In addition, probiotic preparations can help with management of neurodegenerative and psychiatric comorbidities related to low mood, sleep problems, depression and anxiety-like symptoms [78,79] as well as those associated with chronic GI conditions, including as IBS [80].
Probiotics have been also evaluated in the context of ME/CFS, as the previous studies have shown that they can lead to a significant improvement in anxiety/depression symptoms and promoting the overall well-being. In addition, immunomodulatory and anti-inflammatory properties of certain probiotic strains have been shown to reduce inflammation and lower oxidative stress in ME/CFS patients [81,82] consequently leading to improved cognitive function and reduced fatigue severity. In addition, metabolites of microbial origin, by acting on the gut-brain axis can influence brain function [83] with favorable effects on mood and sleep; as well as reduced depression, anger and fatigue [84]. Similar benefits were also observed in hospitalized COVID patients, who after receiving probiotic supplementation, especially with Lactobacillus and Bifidobacterium strains [85] had reduced overall symptoms, including lowered inflammatory reactions, decreased the duration of hospitalization and recovery time, what may suggest that probiotics may have potential to reduce mortality resultant from this condition [86].
Examples of studies conducted in both ME/CFS and COVID cohorts investigating the effect of interventions based on probiotic strains in the context of the most common symptoms reported, such as inflammation and fatigue; psychiatric and GI symptoms are presented in Table 1.
3.1. Effects of Probiotics on Fatigue and Inflammation in ME/CFS and Long COVID
Post-infectious fatigue is a common complication linked with chronic/abnormal inflammation that can significantly decrease physical and mental efficiency, cause depression/anxiety, perturb sleeping patterns, and overall decrease the quality of life. Evidence to date, demonstrated the beneficial role of probiotics and their metabolites in modulating immunity, reducing inflammation and damage arising from oxidative stress. This can be especially important in reducing severe fatigue and exertion intolerance linked with ongoing chronic inflammation resulting from abnormal immunity and mitochondrial dysfunction [53,87]. Consequently, use of probiotics in the treatment of ME/CFS and Long COVID has been intensively studied, owing to their potential to reduce inflammation and restore immune homeostasis, while promoting immunity and recovery [66], might be beneficial for reducing their shared symptoms of post-infectious fatigue and leading to improved overall health.
Interventions conducted in patients with ME/CFS were focused predominantly on use of Bifidobacteria and Lactobacillus strains, which consistently demonstrated good efficiency in reducing inflammation and oxidative stress, which were accompanied by reduced perception of fatigue. For example, use of probiotic treatments with Lactobacillus casei strain Shirota over 8 weeks significantly reduced inflammatory markers in ME/CFS patients [88]; whereas an oral intake of Bifidobacterium infantis 35624 for 8 weeks decreased concentrations of proinflammatory markers, including CRP and IL-6, compared to the baseline in 70% of ME/CFS patients, thereby suggesting that B. infantis 35624 benefits are not limited to mucosal responses and they can exert an effect systemically [89]. In addition, use of multistrain probiotic formulations, which previously have been shown to counteract antibiotic-resistant pathogens, strengthen mucosal barrier and regulate immune responses, including preparations: Lactobacillus rhamnosus combined with Lactobacillus casei (Ramnoselle); and Lactobacillus casei combined with Bifidobacterium lactis (Cytogenex) after 8 weeks were effective in ameliorating the fatigue (Chadler's score), what has been attributed to reduced inflammation, which was reported as almost 30% reduction in CRP levels compared to baseline; and enhanced immunity, characterized as a significant increase of IgM (3x times over the baseline values) and reduced CD4/CD8 ratio. Must be noted that high variability between patients warrant further studies to justify the immunomodulatory potential of probiotic regime [82]. Nevertheless, supplementation of multistrain probiotic formulation containing Lactobacillus paracasei ssp. paracasei F19, Lactobacillus acidophilus NCFB 1748 and Bifidobacterium lactis Bb12 demonstrated a limited efficacy in reducing fatigue and disability scores among ME/CFS patients, as 4 week long treatment followed by a 4 weeks of follow up period improved patient scoring on the SF-12 Health Survey in the area of neurocognitive functioning, there was no significant improvements in fatigue and physical activity scores assessed on the Visual Analogue Scales (VAS), nor major changes in the gut microbiota composition [90].
Probiotic supplementation has been shown potential in lowering systemic inflammation among both patients with acute infection and Long COVID-19 syndrome [91]. To date, interventions with probiotics conducted in COVID-19 patients, including strains Lacticasseibacillus rhamnosus, Lactiplantacillus plantarum, Lactobacillus salivarius, Lactobacillus acidophilus, Pediococcus acidilactici, Bifdobacterium bifdum, Live Bifidobacterium longum, Bifdobacterium longum subsp, Pediococcus acidilactici, Streptococcus thermophilus have been associated with positive health outcomes including to lowered systemic inflammation and reduction in serum CRP; as well as improvement in respiratory symptoms, particularly cough and shortness of breath, however with no obvious effect on fever, headache and weakness [69]. For example, clinical intervention with commercial probiotic (SLAB51), known as Sivomixx800® (Ormendes, Switzerland) consisting of Streptococcus thermophilus DSM 32245®, Bifidobacterium lactis DSM 32246®, Bifidobacterium lactis DSM 32247®, Lactobacillus acidophilus DSM 32241®, Lactobacillus helveticus DSM 32242®, Lactobacillus paracasei DSM 32243®, Lactobacillus plantarum DSM 32244®, and Lactobacillus brevis DSM 27961® have been shown to significantly lower the proportion of Long COVID patients reporting fatigue on FAS scale compared to individuals without the treatment after 21 days (3 weeks) of treatment. This effect was further attributed to favorable changes in the key metabolites related with glucose metabolism among patients receiving oral bacteriotherapy, who had significantly increased concentrations of serum Arginine, Asparagine, Lactate; and lower levels of 3-Hydroxyisobutirate, than controls [92]. Similarly, treatment with probiotic consortium of eight live and freeze-dried strains of Streptococcus thermophilus BT01; B. breve BB02, B. animalis subsp. lactis BL03, B. animalis subsp. lactis BI04, L. acidophilus BA05, L. plantarum BP06, L paracasei BP07, and L. helveticus BD08 (VSL#3®) after 28 days (4 weeks) significantly reduced fatigue scores on the Chalder Fatigue Scale (CFS) in Long COVID patients compared to placebo; which were maintained for 4 weeks post-intervention [93]. Furthermore, combining probiotic strains into formulations of multi-ingredient preparations also including bioactive components been efficient in reducing inflammation in respiratory infections [94] has been proposed as efficient strategy in management of Long COVID-19 symptoms. For example, a multi-enzyme formulation (ImmunoSEB) consisting of probiotic (ProbioSEB CSC3), containing blend of Bacillus coagulans LBSC (DSM 17654), Bacillus subtilis PLSSC (ATCC SD 7280) and Bacillus clausii 088AE (MCC 0538) strains along with Peptizyme SP, inclduing enteric coated serratiopeptidase, bromelain, amylase, lysozyme, peptidase, catalase, papain, glucoamylase and lactoferrin significantly reduced a total as well as physical and mental fatigue scores in give patients with COVID-19 compared to placebo. In addition, this supplement was well tolerated with no adverse events reported. In addition, after initial 14 of supplementation, these patients with mild-to-moderate disease severity reported health benefits demonstrated as reduced systemic inflammation determined as reduced CRP levels (by 77% in the treatment and by 56% for placebo, respectively), enhanced recovery was achieved on day 10 of the intervention, compared to placebo [84]. Similar benefits were also observed with use of symbiotic combining probiotic strains of Lactobacillus plantarum, Lactobacillus rhamnosus, Lactobacillus bulgaricus, Lactococcus lactis and Lactobacillus paracasei with prebiotic inulin fibre, and a phytochemical-rich whole food blend of Citrus Sinensis fruit, Chamomile (Matricaria recutita L. flower), Curcuma Longa, Pomegranate (Punica granatum L.) and resveratrol extracted from Polygonum cuspidatum root, which after 4 weeks resulted in almost two-fold reduction in the mean fatigue scores and a double improvement on the overall wellbeing scores on the Subjective Well-being Score compared to placebo [95].
Furthermore, a recent thus small study conducted in females co-diagnosed with fibromyalgia and ME/CFS have shown to be effective in reducing levels of perceived fatigue thus the impact of fibromyalgia on these patients, compared to baseline after synbiotic (Synbiotic, Gasteel Plus® (Heel España S.A.U.), supplementation, which formulation based on probiotics, e.g., Bifidobacterium lactis CBP-001010, Lactobacillus rhamnosus CNCM I-4036, and Bifidobacterium longum ES1, combined with prebiotic, fructooligosaccharides (200 mg), and micronutrients, including zinc, (1.5mg), selenium (8.25g) and vitamin D (0.75g) [96]. In addition, a pilot study investigating the effectiveness of multi-component preparation, “OMNi-BiOTiC®STRESS Repair 9” (Institute AllergoSan, Graz, Austria) consisting of probiotics e.g., Lactobacillus casei W56, Lactobacillus acidophilus W22, Lactobacillus paracasei W20, Bifidobacterium lactis W51, Lactobacillus salivarius W24, Lactococcus lactis W19, Bifidobacterium lactis W52, Lactobacillus plantarum W62 and Bifidobacterium bifidum W23; prebiotic fructooligosaccharides (FOS), such as inulin, enzymes (amylases), and selected micronutrients, including potassium chloride, vitamin B2 (riboflavin 5′-sodium phosphate), vitamin B6 (pyridoxine hydrochloride), manganese sulfate and vitamin B12 (cyanocobalamin) have been shown to be effective in improving fatigue, mood, and quality of life in both the probiotic and placebo groups, however with greater improvements reported in the probiotic group after 6 months of treatment [97]. Although results of these studies suggest that bacteriotherapy in management of Long COVID is promising, the low number of trails, often varying in the duration of the treatment, as well as tested formulation of the supplement (probiotic strains used and dose; presence of other bioactives, e.g., vitamins, minerals, phytonutrients) provided not sufficient evidence to use microbial preparations in the clinical care of patients with post-viral syndromes.
The reported benefits of improved immunity, energy metabolism, respiratory functions and psychiatric wellbeing suggest that probiotic supplementation has potential to improve the management of ME/CFS and Long COVID. Although the results of conducted trials may suggest that supplementation with single as well as multi-strain probiotics may have potential benefits for reducing fatigue and inflammation in ME/CFS and Long COVID patients, only few studies using the preparations of Bifidobacteria and Lactobacillus demonstrated their good efficiency in reducing inflammatory markers, and their effects on the fatigue scoring scales remains inconsistent, thereby indicating that the need for further exploration into the interplay between probiotics bacteria and fatigue, as well as inflammation in ME/CFS and Long COVID.
3.2. Effects of Probiotics on Psychiatric Symptoms (Psychobiotics)
Psychobiotics, as selected probiotic strains and their preparations, which ingested in sufficient amounts may have positive impact on mental health, including reduced symptoms of depression, anxiety as well as chronic stress, as well as improved sleep quality [98]; attributed to the ability to modulate the gut-brain axis [99], and/or production of neuroactive bioactives, such as γ-aminobutyric acid (GABA) and serotonin [100]. Although many probiotics were proposed as potential psychotropic agents, including Streptococcus thermophilus, Bifidobacterium animalis, Bifidobacterium bifidum, Bifidobacterium longum, Streptococcus thermophiles, Lactobacillus bulgaricus, Lactococcus lactis, Lactobacillus acidophilus, Lactobacillus plantarum, Lactobacillus reuteri, Lactobacillus paracasei, Lactobacillus helveticus, Lactobacillus rhamnosus, Bacillus coagulans, Clostridium butyricum, and others [100,101] depending on the acquired neuropsychiatric condition [101] their effectiveness may vary. In context of post viral syndromes, such as ME/CFS and Long COVID patients, specific strains of Lactobacillus and Bifidobacterium have gained interest, as beside their immuno-modulatory effects, they may also be relevant to reduce risk factors associated with these conditions and fatigue, including low quality/disturbed sleep, depression and chronic stress. Although none of the psychobiotics formulation were exclusively tested in ME/CFS and Long COVID patients, there is growing evidence indicating that use of probiotic strains might be beneficial for managing stress and anxiety [100] frequently reported by these patients. For example, psychobiotics metabolites acting as neurotransmitters and neurochemicals, can influence the brain-gut axis and modulate the stress response via the hypothalamic–pituitary–adrenal (HPA) axis. Stress, proposed as the factor linked with fatigue induction, can cause neuroendocrine deregulation resulting from the activation of the HPA axis and stimulation of glucocorticoid production, which has been characterized as increased cortisol level and secretion of pro-inflammatory cytokines. The chronic activation of the HPA axis can also significantly affect the gut microbiota composition, which have been linked to presence of mental and physical illnesses. Therefore, use of microbial preparations, such as psychobiotics aiming to restore gut homeostasis and normalize HPA axis hyperactivity, due to may help to relieve negative consequences of chronic stress [100,101], implicated in ME/CFS as well as long COVID patients.
To date, studies have shown that psychobiotics can help in reducing depressive symptoms and potentially can be used as supportive therapy in Major Depressive Disorder (MDD). For example, Clostridium butyricum (CBM588) supplementation along with the prescribed antidepressants significantly reduced (e.g., ≥ 50% reduction) a total HAMD-17 score in Hamilton rating scale for depression and Beck depression inventory (BDI) scores in patients with treatment-resistant MDD compared to placebo [102]. Similar benefits were reported in management of Generalized Anxiety Disorder (GAD) and anxiety-like symptoms with multi-strain preparations including L. heleveticus Rosell-52 and B. longum Rosell-175 [103]; Bifidobacterium longom, Bifidobacterium bifidum, Bifidobacterium lactis and Lactobacillus acidophilus [104]; as well as multi-strain consortium of L. acidophilus LA5 and B. lactis BB12 [105], which significantly reduced the intensity of anxiety symptoms and improved overall mental health outcomes. Additional benefits attributed to psychobiotics formulation consisting of Lactobacillus fermentum LF16, L. rhamnosus LR06, L. plantarum LP01, and Bifidobacterium longum BL04; Lactobacillus acidophilus, Lactobacillus casei and Bifidobacterium bifidum; Lactobacillus helveticus R0052, Bifidobacterium longum R0175, as well as Lactobacillus plantarum 299v have been shown to significantly improve mood, by reducing depressive and anger feelings [106,107], as well as reduce the response to stress on HPA axis [108] observed as reduced salivary cortisol levels [110] all together leading to improved sleep. In particularly, supplementation of Lactobacillus paracasei HII01 in fatigued participants after 12 weeks have been shown to significantly reduce salivary cortisol level compared to baseline [110], what may suggest potential benefits also for fatigue reduction among the patients with post-viral syndromes.
While the use of psychobiotics to modify the gut microbiome has been shown to improve anxiety [103,104] and depression symptoms [102,106,111], as well as improve mental well-being upon chronic stress [105,109] with additional benefits for sleep quality [107] the direct application of probiotic strains with psychobiotic properties may have potential to reduce psychiatric symptoms in ME/CFS and Long COVID patients, owing to the reported gut dysbiosis along with aberrant immune responses. For example, overlapping psychiatric symptoms between MDD, ME/CFS and Long COVID, suggest that treatments with certain psychobiotic strains among ME/CFS, such as Lactobacillus casei strain Shirota may help to reduce anxiety [88]; while preparations consisting of Lactobacillus rhamnosus combined with Lactobacillus casei (Ramnoselle) and Lactobacillus casei combined with Bifidobacterium lactis (Cytogenex) significantly improved capability of these individuals to respond to stressful situations, which has been demonstrated as increased levels of urinary free cortisol (2.4x times), a stress hormone; and DHEA-S (1.4x), an indicator of psychological illness and stress [112]. As ME/CFS patients usually demonstrate low levels of these hormones [113], the reported increase to normal values may improve individual ability to cope with stressful events, further confirmed as significantly improved mood scores and reduced perception of fatigue on the (BDI-I and BDI-II) tests [82]. Significant reduction in anxiety among ME/CFS patients, reported after probiotic supplementation with L. paracasei spp. paracasei F19, L. acidophilus NCFB 1748, and B. lactis Bb12 strains also improved their neurocognitive functioning [90].
The available studies from Long COVID cohorts investigating effect on probiotic supplementation on mental health indices are limited, as the majority of them focused on management of respiratory or GI symptoms (NCT04420676; NCT04813718) after acute infection; and/or improving immunity (NCT04922918; NCT04734886) [114]. To date, the clinical trial dedicated to psychiatric sequelae investigating the probiotic formulation (VSL#3®) containing eight freeze-dried strains, e.g., Streptococcus thermophilus BT01; B. breve BB02, B. animalis subsp. lactis BL03, B. animalis subsp. lactis BI04, L. acidophilus BA05, L. plantarum BP06, L paracasei BP07, and L. helveticus BD08 after 28 days (4 weeks), has failed to improve the performance and somatization symptoms, as well as psychiatric (e.g., anxiety, depression) outcomes; nevertheless the significant improvement on fatigue scoring may indicate that certain strains may still benefit patients despite limited effectiveness on modulating the gut-brain axis [93]. Furthermore, other studies focused on the dietary supplementation aiming to target mental health outcomes in Long COVID patients, involved preparations combining probiotic strains with other bioactives with antioxidant and anti-inflammatory properties, such as prebiotic fibres of fructooligosaccharides (FOS), which added with probiotic mixture consisting of L. casei, L. acidophilus, L. bulgaricus, L. rhamnosus, Bacillus breve, B. longum, Streptococcus thermophilus has been shown to significantly decreased depressive symptoms in moderately depressed patients compared placebo [111]. Consequently, evidence obtained from Long COVID patients although limited by low number of studies, indicated that interventions with functional microbial preparations, like “OMNi-BiOTiC® STRESS Repair 9”, combining 9 probiotic strains e.g., Lactobacillus casei W56, Lactobacillus acidophilus W22, Lactobacillus paracasei W20, Bifidobacterium lactis W51, Lactobacillus salivarius W24, Lactococcus lactis W19, Bifidobacterium lactis W52, Lactobacillus plantarum W62 and Bifidobacterium bifidum W23; with prebiotic FOS and enzymes (e.g., amylases), minerals (magnesium sulfate, manganese sulfate) and vitamins (vitamin B2, vitamin B6,vitamin B12) improved symptoms of depression and improved perceived emotional wellbeing self-assessed among 44.3% (n=27) of study participants over the course of 6 months [97]. Interestingly, benefits of using symbiotics were also reported in small, thus recent study conducted in women with fibromyalgia co-diagnosed with ME/CFS, who after 4 weeks of synbiotic intake (Synbiotic, Gasteel Plus® (Heel España S.A.U.), containing probiotic strains of Bifidobacterium lactis CBP-001010, Lactobacillus rhamnosus CNCM I-4036, and Bifidobacterium longum ES1, combined with prebiotic, FOS (200 mg), and micronutrients, including zinc, (1.5mg), selenium (8.25g) and vitamin D (0.75g) had significantly reduced anxiety, when compared with the baseline scores followed by improvements in pain perception and sleep quality [96].
Given the reported associations between the alerted gut microbiome composition and the reported psychiatric complications in ME/CFS and Long COVID-19 [115] the use of psychbiotics through modulating the gut-brain axis may serve as potential adjunct treatment to improve mental health outcomes in the patients with post viral syndromes [116], while also reduce stress, regulate mood and improve their cognitive functioning (Berding et al., 2023). Although these benefits seem to be attributed to the immunomodulatory properties of the microbial metabolities (e.g., SCFAs) [117], the limited number of studies investigating effects of the psychobiotics and their products on the neurotransmitters and neurotrophic factors implicated in the central nervous system function [116] indicate a need for the exploration, before the use of probiotics will be incorporated in the clinical practice.
3.3. Effects of Probiotics on Gastrointestinal Symptoms in ME/CFS and Long COVID
The presence of certain gut dysbiosis reported in both ME/CFS and long COVID patients suggest that use of microbial-based preparations due to positive effects on gut microbiota composition may be an efficient strategy in the management of GI symptoms in these individuals. Despite still limited number of studies, the evidence from ME/CFS cohorts with GI complains suggest that certain probiotic strains, especially Lactobacilli spp., Bifidobacteria spp., and/or their combination, can positively impact the gut microbiota function while promoting intestinal homeostasis, also strengthen mucosal barrier, normalize the cytokine profile within the gut [3,45,90]. Noteworthy, an anti-inflammatory effect of probiotics by leading to reduced production of pro-inflammatory mediators, such as CRP, TNF-α, and IL-6, may have therapeutic potential for ME/CFS with comorbid IBS [45], leading to reduced IBS-like symptoms in these patients, while improving the quality of life and psychological symptoms [118]. For example, supplementation with symbiotic formulation (Synbiotic, Gasteel Plus® (Heel España S.A.U.), containing probiotic strains of Bifidobacterium lactis CBP-001010, Lactobacillus rhamnosus CNCM I-4036, and Bifidobacterium longum ES1, in addition to prebiotic, fructooligosaccharides (200 mg), and zinc (1.5mg), selenium (8.25g) and vitamin D (0.75g) resulted in better scoring of GI health indices among females co-diagnosed with fibromyalgia and ME/CFS, compared to the scores reported at the baseline; nevertheless these improvements remained not significant [96].
Similarly to ME/CFS, use of probiotic aiming to restore gut homeostasis has been a subject of interest, as 22% of individuals with COVID diagnosis may experience certain GI distress, of which loss of appetite, dyspepsia, IBS-like and abdominal pain seem to be the most common [119]. In addition, the observed associations between changes in the composition of gut microbiome, disease severity and inflammation among Long COVID patients [120,121] suggested that interventions using microbial preparations may help to reduce GI complaints among Long COVID patients and improve their recovery from the disease. To date, most the studies conducted on COVID survivors have shown that probiotic supplementation can improve the overall symptoms, inflammatory response, and time of hospitalization, with some also indicating for beneficial effects on intestinal microbiota characterized by reduced GI symptoms e.g., reduced duration of diarrhea, abdominal pain, nausea, vomiting [69]. For example, supplementation of multi-strain preparation, including Streptococcus thermophilus DSM 32345, L. acidophilus DSM 32241, L. helveticus DSM 32242, Lacticaseibacillus paracasei DSM 32243, L. plantarum DSM 32244, LeviL. brevis DSM 27961, B. lactis DSM 32246, and B. lactis DSM 32247 for 7 days resulted in the reduction in diarrhea and severity of other symptoms accompanying infection (e.g., fever, asthenia, headache, myalgia, and dyspnea) followed by 8-fold reduced risk of respiratory failure among hospitalized patients with COVID-19 [122]. Although use of probiotics might be beneficial for acute COVID infection, the studies assessing their efficacy in Long COVID are limited. Nevertheless, an intervention with symbiotic consisting of lactobacillus strains (e.g., Lactobacillus plantarum, Lactobacillus rhamnosus, Lactobacillus bulgaricus, Lactococcus lactis and Lactobacillus paracasei) and prebiotic inulin after 30 days lead to significant improvements in the gut health and reduced of GI symptoms (e.g., mild increased bloating and diarrhea), especially in older patients with more severe course of the disease. In addition, these patients also reported significantly improved symptoms of fatigue, indigestion and cough [46]. Similar benefits were shown after use of a multi-strain probiotic preparation, “OMNi-BiOTiC® STRESS Repair 9”, providing 9 bacterial strains, including Lactobacillus casei W56, Lactobacillus acidophilus W22, Lactobacillus paracasei W20, Bifidobacterium lactis W51, Lactobacillus salivarius W24, Lactococcus lactis W19, Bifidobacterium lactis W52, Lactobacillus plantarum W62 and Bifidobacterium bifidum W23; along prebiotic fructooligosaccharides (FOS), enzymes (amylases); minerals (magnesium sulfate, manganese sulfate) and vitamins (vitamin B2, vitamin B6,vitamin B12), which after 3 months led to subjective improvement of GI health, including enhanced digestion, reduced diarrhea, constipation, flatulence and abdominal pain [97]. Finally, a phase 3 clinical trial evaluating the efficacy of probiotic formula (VSL#3®) containing 8 strains of Lactic acid bacteria and Bifidobacteria (e.g., Streptococcus thermophilus BT01; B. breve BB02, B. animalis subsp. lactis BL03, B. animalis subsp. lactis BI04, L. acidophilus BA05, L. plantarum BP06, L paracasei BP07, and L. helveticus BD08) have been shown to be effective in ameliorating GI symptoms determined on Structured Assessment of Gastrointestinal Symptoms Scale (SAGIS) compared to placebo; nevertheless, with limited effects on acid regurgitation, nausea, vomiting, constipation, epigastric pain and IBS-like symptoms [93].
In summary, research to date indicate that probiotics, especially lactobacillus, may be beneficial in reducing GI symptoms in patients with ME/CFS and Long COVID [2; 123]. The immunoregulatory properties of probiotics may help to restore perturbed composition of gut microbiota and dysbiosis, which could reduce symptom severity, which was linked to the reduced abundance of butyrate producing bacteria [41]. Consequently, use of live strains of F. prausnitzii and B. pullicaecorum, as potent butyrate producers by increasing SCFAs (e.g., butyrate) levels due to its potent immunoregulatory and anti-inflammatory properties may have to restore gut homeostasis after excessive inflammation and also by strengthening intestinal barrier may prevent a leaky gut syndrome linked IBS-like symptoms [124] resultant from with increased inflammatory response/immune activation due to leakage of proinflammatory endotoxins and pathogens into circulation [125]. In addition, the psychobiotic and anti-inflammatory properties of certain strains may help to reduce GI symptoms resulting from psychological distress resultant from the stress-induced gut dysbiosis and activation of the HPA axis [126]. Although this effects still need to be confirmed in patients affected by post-viral syndromes, supplementation of L. heleveticus Rosell-52 and B. longum Rosell-175 can reduce stress-induced GI discomfort among healthy populations [103]. Furthermore, probiotics have been proposed as a promising intervention for improving the health of patients with post-infectious fatigue, many of whom report GI symptoms such as abdominal pain, constipation/diarrhea, or bloating; nevertheless to confirm these effects further studies are needed, as to date the low number of these studies along with the overall poor quality of data, do not allow to fully understand their role and effectiveness in managing GI symptoms in ME/CFS patients [2].
4. Future Directions
The use of microbial preparations in the management of post-viral syndromes, such as ME/CFS and Long COVID is an area of ongoing research, owing to the several studies indicating for a role of gut dysbiosis, as well as shared in both conditions neuropsychiatric and GI symptoms.
Reported association between low levels of butyrate, as well as reduced abundance of SCFAs producing bacteria in expense of gut pathogens with persisting GI and neurological symptoms in these individuals, highlighted the need for novel strategies for microbiome-tailored disease prevention and treatment. The increased interest and research activity initiated during COVID-19 pandemic, based on the certain similarity observed in pathophysiology of both post-viral syndromes, in particularly in the gut microbiome, may accelerate the progress in developing evidence-based therapeutic options for ME/CFS [13] such as use of microbial preparations.
To date, despite limited evidence, clinical trials to date conducted in the ME/CFS and Long COVID cohorts demonstrated that certain microbial preparations by restoring intestinal homeostasis, regulating gut-brain axis and decreasing inflammation may play a role in the management of ME/CFS and long COVID symptoms and possibly increase quality of life of patients. Whereas certain lactobacilli and bifidobacterial strains have been found to be effective in reducing inflammation and fatigue, their effect on the neurological and psychiatric symptoms remains inconsistent, what might be attributable to varying methodology of the conduced trials and low number of the studies. Nevertheless, the emerging strategy of combining muti-strain probiotics with other functional ingredients previously implicated with anti-inflammatory and anti-oxidative properties, such as prebiotic fibres, vitamins and minerals as well as other bioactive blends are promising approach which may offer significant advantages for not only reducing fatigue, but also increasing wellbeing of patients with post-viral syndromes. Among these strategies, formulations combining potent antioxidants and enzymes, such as peptidase, bromelain, amylase, lysozyme, peptidase, catalase, papain, glucoamylase and lactoferrin; as well as vitamins and minerals implicated in energy metabolism antioxidant defenses and immunity, including zinc, selenium, vitamin D, vitamin B2 (riboflavin 5′-sodium phosphate), vitamin B6 (pyridoxine hydrochloride), manganese sulfate and vitamin B12 (cyanocobalamin) may help to reduce the severity of fatigue and depression, while increasing energy levels, also improve mood, sleep and overall quality of life. Furthermore, combining probiotics with a phytochemical-rich whole plant foods, such as Citrus Sinensis fruit, Chamomile (Matricaria recutita L. flower), Curcuma Longa and Pomegranate (Punica granatum L.), as source of naturally derived prebiotic fibres, antioxidants and micronutrients, may provide synergistic benefits of promoting gut health and microbial activities, related to production of microbial metabolites, which acting systemically can lead to improvement in overall well-being and enhance recovery. It would be interesting to assess the effectiveness of other microbial-based preparations, which include postbiotics, such as microbial cells, their fractions and bioactive metabolites, such as organic acids, bacteriocins, and enzymes. While using a live probiotic strain have been tested and acknowledged for their health benefits, especially in the context of immunity, gut and brain health, postbiotics, as nonviable or inactive probiotics and their metabolic by-products, may offer the significant advantage of providing all the benefits, thereby offering potentially safer and more suitable approach for individuals with chronic inflammatory conditions and/or compromised immunity.
Although further research is needed to fully understand how postbiotics can be beneficial for ME/CFS and Long COVID-19 and patients, the current evidence suggests that they could be a promising area of study for improving the health of these individuals. In particular, the use of microbial metabolites known short chain fatty acids (SCFAs), including acetate, propionate and butyrate, due to its immuno-modulatory properties was suggested to be effective in reducing severity symptoms of COVID-19, which might be also extended for ME/CFS, in particularly for modulating gut-brain axis and strengthening intestinal barriers [125]. For example, supplementation of butyrate, in comparison with other SCFAs, acetate and propionate, may be the most advantageous due to its proven immunomodulatory effects, e.g., increase secretion of mucins and defensins, promoting antiviral defenses, by inducing expression of interferon-gamma and granzyme B, as well as reducing systemic inflammation [125] thus possibly reducing psychiatric and fatigue symptoms. Despite these strategies can be promising there is emerging need for further studies, which would include controlled clinical trials to determine optimal formulation, doses and treatment durations which would allow to achieve the most prominent improvements in health determinants of patients with post-viral syndromes, while minimize potential adverse effects.
5. Conclusions
The use of microbial preparations based on immunomodulatory probiotic strains with demonstrated benefits for gut and brain, might be a promising strategy in the management of comorbidities linked with post-viral syndromes, including ME/CFS and COVID-19.
To date, evidence supported potential of probiotic to improve the overall symptoms, in particular inflammation and GI symptoms in Long COVID [69]; whereas in ME/CFS, the usefulness of probiotic interventions still needs to be determined due to the low-quality of available studies [2] although some benefits for relief from IBS [118] and anxiety [88] have been reported. In addition, given the role of immune dysregulation in neuroinflammation along with increased intestinal permeability may also influence the communication via the gut-brain axis, possibly leading to development of psychiatric symptoms reported in ME/CFS and Long COVID [2]. Implications of the gut dysbiosis in etiologies of both ME/CFS and long COVID, suggest that interventions focused on restoring gut balance may help to reduce symptom severity, especially those common in other chronic and inflammatory diseases, including depression [127], anxiety [127], IBD [128], IBS [129] insomnia and sleep disturbances [130] also comorbid conditions among ME/CFS patients [131]. Therefore, use of microbial-based interventions, which health benefits have been proved for certain probiotic strains, including reduced inflammation and enhanced resistance against infection, as well as improvement in GI and psychiatric function, may indicate that interventions targeting gut microbiome balance can bring benefit for individuals suffering from the post-viral conditions, attributable to decrease virus-induced intestinal inflammation, decreasing severity of the disease and improving their recovery time [41]. Although these implications are promising, reliable research evidence on the impact of probiotics for these individuals should be developed. These future studies are needed to clearly define mechanisms on how probiotics can aid management of ME/CFS and Long COVID pathophysiology; and if including microbial preparations in the current clinical guidelines might be beneficial, whenever given alone or in combination with other compounds, including CoQ10 and selenium (Se) [132] and CoQ10 and lipoic acid [133].
Finally, focusing on the manipulation of the microbiome followed by other areas highlighted to be of the most therapeutic value including energy metabolism, chronic inflammation, fluctuating neuroinflammation and management of the response to stress [13] could provide holistic background supporting the most promising probiotic interaction in the care offered for patients suffering from post-viral syndromes.
Author Contributions
JMJ conceptualized the article, wrote the manuscript, and designed the tables/figures. JC-M contributed to the revision of the manuscript. All authors have read and approved the final manuscript.
Funding
This research was funded by the National Institute of Health Carlos III (Madrid, Spain) within the framework of the Strategic Action Plan on Health (Grant number: PI19/00629) and co-funded by the European Union (European Regional Development Fund – ERDF 2014-2020): “A way to build Europe”. Vall d’Hebron Research Institute (VHIR) is member of the CERCA programme (Generalitat de Catalunya, Barcelona, Spain).
Data Availability Statement
N/A.
Acknowledgments
N/A.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Germain A, Barupal DK, Levine SM, Hanson MR. Comprehensive Circulatory Metabolomics in ME/CFS Reveals Disrupted Metabolism of Acyl Lipids and Steroids. Metabolites. 2020 Jan 14;10(1):34. [CrossRef] [PubMed]
- König RS, Albrich WC, Kahlert CR, Bahr LS, Löber U, Vernazza P, Scheibenbogen C, Forslund SK. The Gut Microbiome in Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Front Immunol. 2022 Jan 3;12:628741. Erratum in: Front Immunol. 2022 Mar 30;13:878196. [CrossRef] [PubMed]
- Lakhan SE, Kirchgessner A. Gut inflammation in chronic fatigue syndrome. Nutr Metab (Lond). 2010 Oct 12;7:79. [CrossRef] [PubMed]
- Mirin AA, Dimmock ME, Jason LA. Research update: The relation between ME/CFS disease burden and research funding in the USA. Work. 2020;66(2):277-282. [CrossRef] [PubMed]
- Sandler CX, Lloyd AR. Chronic fatigue syndrome: progress and possibilities. Med J Aust. 2020 May;212(9):428-433. [CrossRef] [PubMed]
- Jason LA, McManimen S, Sunnquist M, Brown A, Newton JL, Strand EB. Examining the institute of medicine’s recommendations regarding chronic fatigue syndrome: Clinical versus research criteria. Journal of neurology and psychology. 2015;2015(Suppl 2).
- Barry PW, Kelley K, Tan T, Finlay I. NICE guideline on ME/CFS: robust advice based on a thorough review of the evidence. Journal of Neurology, Neurosurgery & Psychiatry. 2024 Feb 28.
- Devasahayam A, Lawn T, Murphy M, White PD. Alternative diagnoses to chronic fatigue syndrome in referrals to a specialist service: service evaluation survey. JRSM Short Rep. 2012 Jan;3(1):4. [CrossRef] [PubMed]
- Carfì A, Bernabei R, Landi F; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA. 2020 Aug 11;324(6):603-605. [CrossRef] [PubMed]
- Komaroff AL, Lipkin WI. ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature. Front Med (Lausanne). 2023 Jun 2;10:1187163. [CrossRef] [PubMed]
- Wong TL, Weitzer DJ. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)-A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina (Kaunas). 2021 Apr 26;57(5):418. [CrossRef] [PubMed]
- White PD, Thomas JM, Amess J, Crawford DH, Grover SA, Kangro HO, Clare AW. Incidence, risk and prognosis of acute and chronic fatigue syndromes and psychiatric disorders after glandular fever. The British Journal of Psychiatry. 1998 Dec;173(6):475-81.
- Tate WP, Walker MO, Peppercorn K, Blair AL, Edgar CD. Towards a better understanding of the complexities of myalgic encephalomyelitis/chronic fatigue syndrome and long COVID. International Journal of Molecular Sciences. 2023 Mar 7;24(6):5124.
- Mandarano AH, Maya J, Giloteaux L, Peterson DL, Maynard M, Gottschalk CG, Hanson MR. Myalgic encephalomyelitis/chronic fatigue syndrome patients exhibit altered T cell metabolism and cytokine associations. The Journal of clinical investigation. 2020 Mar 2;130(3):1491-505.
- Wang EY, Mao T, Klein J, Dai Y, Huck JD, Jaycox JR, Liu F, Zhou T, Israelow B, Wong P, Coppi A. Diverse functional autoantibodies in patients with COVID-19. Nature. 2021 Jul 8;595(7866):283-8.
- Ryabkova VA, Gavrilova NY, Poletaeva AA, Pukhalenko AI, Koshkina IA, Churilov LP, Shoenfeld Y. Autoantibody correlation signatures in fibromyalgia and myalgic encephalomyelitis/chronic fatigue syndrome: association with symptom severity. Biomedicines. 2023 Jan 18;11(2):257.
- Sotzny F, Blanco J, Capelli E, Castro-Marrero J, Steiner S, Murovska M, Scheibenbogen C. Myalgic encephalomyelitis/chronic fatigue syndrome–evidence for an autoimmune disease. Autoimmunity reviews. 2018 Jun 1;17(6):601-9.
- Maksoud R, Magawa C, Eaton-Fitch N, Thapaliya K, Marshall-Gradisnik S. Biomarkers for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): a systematic review. BMC medicine. 2023 ;21(1):189. 24 May.
- Patarca, R. Cytokines and chronic fatigue syndrome. Annals of the New York Academy of Sciences. 2001 Mar;933(1):185-200.
- Low RN, Low RJ, Akrami A. A review of cytokine-based pathophysiology of Long COVID symptoms. Frontiers in Medicine. 2023 Mar 31;10:1011936.
- Montoya JG, Holmes TH, Anderson JN, Maecker HT, Rosenberg-Hasson Y, Valencia IJ, Chu L, Younger JW, Tato CM, Davis MM. Cytokine signature associated with disease severity in chronic fatigue syndrome patients. Proceedings of the National Academy of Sciences. 2017 Aug 22;114(34):E7150-8.
- Missailidis D, Annesley SJ, Fisher PR. Pathological mechanisms underlying myalgic encephalomyelitis/chronic fatigue syndrome. Diagnostics. 2019 Jul 20;9(3):80.
- Hatziagelaki E, Adamaki M, Tsilioni I, Dimitriadis G, Theoharides TC. Myalgic encephalomyelitis/chronic fatigue syndrome—metabolic disease or disturbed homeostasis due to focal inflammation in the hypothalamus?. Journal of Pharmacology and Experimental Therapeutics. 2018 Oct 1;367(1):155-67.
- Al-Hakeim HK, Al-Rubaye HT, Al-Hadrawi DS, Almulla AF, Maes M. Long-COVID post-viral chronic fatigue and affective symptoms are associated with oxidative damage, lowered antioxidant defenses and inflammation: a proof of concept and mechanism study. Molecular Psychiatry. 2023 Feb;28(2):564-78.
- Walker MO, Hall KH, Peppercorn K, Tate WP. The significance of oxidative stress in the pathophysiology of Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medical Research Archives. 2022 Sep 20;10(9).
- Stufano A, Isgrò C, Palese LL, Caretta P, De Maria L, Lovreglio P, Sardanelli AM. Oxidative Damage and Post-COVID Syndrome: A Cross-Sectional Study in a Cohort of Italian Workers. International Journal of Molecular Sciences. 2023 Apr 18;24(8):7445.
- Tahaghoghi-Hajghorbani S, Zafari P, Masoumi E, Rajabinejad M, Jafari-Shakib R, Hasani B, Rafiei A. The role of dysregulated immune responses in COVID-19 pathogenesis. Virus research. 2020 Dec 1;290:198197.
- Giamarellos-Bourboulis EJ, Netea MG, Rovina N, Akinosoglou K, Antoniadou A, Antonakos N, Damoraki G, Gkavogianni T, Adami ME, Katsaounou P, Ntaganou M. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell host & microbe. 2020 Jun 10;27(6):992-1000.
- Paul BD, Lemle MD, Komaroff AL, Snyder SH. Redox imbalance links COVID-19 and myalgic encephalomyelitis/chronic fatigue syndrome. Proceedings of the National Academy of Sciences. 2021 Aug 24;118(34):e2024358118.
- Tanaka S, Kuratsune H, Hidaka Y, Hakariya Y, Tatsumi KI, Takano T, Kanakura Y, Amino N. Autoantibodies against muscarinic cholinergic receptor in chronic fatigue syndrome. International journal of molecular medicine. 2003 Aug 1;12(2):225-30.
- Freitag H, Szklarski M, Lorenz S, Sotzny F, Bauer S, Philippe A, Kedor C, Grabowski P, Lange T, Riemekasten G, Heidecke H. Autoantibodies to vasoregulative G-protein-coupled receptors correlate with symptom severity, autonomic dysfunction and disability in myalgic encephalomyelitis/chronic fatigue syndrome. Journal of Clinical Medicine. 2021 Aug 19;10(16):3675.
- Maes M, Twisk FN, Johnson C. Myalgic encephalomyelitis (ME), chronic fatigue syndrome (CFS), and chronic fatigue (CF) are distinguished accurately: results of supervised learning techniques applied on clinical and inflammatory data. Psychiatry research. 2012 Dec 30;200(2-3):754-60.
- Yamamoto S, Ouchi Y, Nakatsuka D, Tahara T, Mizuno K, Tajima S, Onoe H, Yoshikawa E, Tsukada H, Iwase M, Yamaguti K. Reduction of [11C](+) 3-MPB binding in brain of chronic fatigue syndrome with serum autoantibody against muscarinic cholinergic receptor. PloS one. 2012 Dec 11;7(12):e51515.
- Fischer DB, William AH, Strauss AC, Unger ER, Jason LA, Marshall Jr GD, Dimitrakoff JD. Chronic fatigue syndrome: the current status and future potentials of emerging biomarkers. Fatigue: biomedicine, health & behavior. 2014 Apr 3;2(2):93-109.
- Patil S, Choudhari S, Raka V, Narkar S, Dahiphale J, Gondhali G. Neurological and systemic manifestations in Long covid: Underestimated sequel of covid’s pandora. World Journal of Advanced Pharmaceutical and Medical Research. 2023;4(01):042-52.
- Uhde M, Indart AC, Green PH, Yolken RH, Cook DB, Shukla SK, Vernon SD, Alaedini A. Suppressed immune and metabolic responses to intestinal damage-associated microbial translocation in myalgic encephalomyelitis/chronic fatigue syndrome. Brain, Behavior, & Immunity-Health. 2023 Jul 1;30:100627.
- Cliff JM, King EC, Lee JS, Sepúlveda N, Wolf AS, Kingdon C, Bowman E, Dockrell HM, Nacul L, Lacerda E, Riley EM. Cellular immune function in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Frontiers in immunology. 2019 Apr 16;10:422277.
- Keller J, Gomez R, Williams G, Lembke A, Lazzeroni L, Murphy GM, Schatzberg AF. HPA axis in major depression: cortisol, clinical symptomatology and genetic variation predict cognition. Molecular psychiatry. 2017 Apr;22(4):527-36.
- Meierovics A, Yankelevich WJ, Cowley SC. MAIT cells are critical for optimal mucosal immune responses during in vivo pulmonary bacterial infection. Proceedings of the National Academy of Sciences. 2013 Aug 13;110(33):E3119-28.
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nature Reviews Microbiology. 2023 Mar;21(3):133-46.
- Guo C, Che X, Briese T, Ranjan A, Allicock O, Yates RA, Cheng A, March D, Hornig M, Komaroff AL, Levine S. Deficient butyrate-producing capacity in the gut microbiome is associated with bacterial network disturbances and fatigue symptoms in ME/CFS. Cell host & microbe. 2023 Feb 8;31(2):288-304.
- Mendes de Almeida V, Engel DF, Ricci MF, Cruz CS, Lopes ÍS, Alves DA, d’Auriol M, Magalhães J, Machado EC, Rocha VM, Carvalho TG. Gut microbiota from patients with COVID-19 cause alterations in mice that resemble post-COVID symptoms. Gut Microbes. 2023 Dec 18;15(2):2249146.
- Nijs J, Crombez G, Meeus M, Knoop H, Van Damme S, Van Cauwenbergh D, Bleijenberg G. Pain in patients with chronic fatigue syndrome: time for specific pain treatment?. Pain physician. 2012;15(5):E677-86.
- Koc HC, Xiao J, Liu W, Li Y, Chen G. Long COVID and its Management. International Journal of Biological Sciences. 2022;18(12):4768.
- Varesi A, Deumer US, Ananth S, Ricevuti G. The emerging role of gut microbiota in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): current evidence and potential therapeutic applications. Journal of Clinical Medicine. 2021 Oct 29;10(21):5077.
- Thomas N, Gurvich C, Huang K, Gooley PR, Armstrong CW. The underlying sex differences in neuroendocrine adaptations relevant to myalgic encephalomyelitis chronic fatigue syndrome. Frontiers in neuroendocrinology. 2022 Jul 1;66:100995.
- Aron-Wisnewsky J, Clément K. The gut microbiome, diet, and links to cardiometabolic and chronic disorders. Nature Reviews Nephrology. 2016 Mar;12(3):169-81.
- Lazar V, Ditu LM, Pircalabioru GG, Picu A, Petcu L, Cucu N, Chifiriuc MC. Gut microbiota, host organism, and diet trialogue in diabetes and obesity. Frontiers in nutrition. 2019 Mar 13;6:21.
- Fujimura KE, Slusher NA, Cabana MD, Lynch SV. Role of the gut microbiota in defining human health. Expert review of anti-infective therapy. 2010 Apr 1;8(4):435-54.
- Iacob S, Iacob DG, Luminos LM. Intestinal microbiota as a host defense mechanism to infectious threats. Frontiers in Microbiology. 2019 Jan 23;9:426119.
- Kho ZY, Lal SK. The human gut microbiome–a potential controller of wellness and disease. Frontiers in microbiology. 2018 Aug 14;9:356589.
- DeGruttola AK, Low D, Mizoguchi A, Mizoguchi E. Current understanding of dysbiosis in disease in human and animal models. Inflammatory bowel diseases. 2016 ;22(5):1137-50. 1 May.
- Tisza BB, Iván G, Keczeli V, Kóró M, Szántóri P, Varga ZG, Müller H, Pribéli O, Szabó Z, Verzár Z, Gyuró MS. A Review of Possible Supplements to Relieve the Symptoms of Fatigue after COVID-19.
- Shukla SK, Cook D, Meyer J, Vernon SD, Le T, Clevidence D, Robertson CE, Schrodi SJ, Yale S, Frank DN. Changes in gut and plasma microbiome following exercise challenge in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). PloS one. 2015 Dec 18;10(12):e0145453.
- Navaneetharaja N, Griffiths V, Wileman T, Carding SR. A role for the intestinal microbiota and virome in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)?. Journal of clinical medicine. 2016 Jun 6;5(6):55.
- Nagy-Szakal D, Williams BL, Mishra N, Che X, Lee B, Bateman L, Klimas NG, Komaroff AL, Levine S, Montoya JG, Peterson DL. Fecal metagenomic profiles in subgroups of patients with myalgic encephalomyelitis/chronic fatigue syndrome. Microbiome. 2017 Dec;5:1-7.
- Guo C, Yi B, Wu J, Lu J. The microbiome in post-acute infection syndrome (PAIS). Comput Struct Biotechnol J. 2023 Aug 5;21:3904-3911. [CrossRef] [PubMed]
- Silva CF, Motta JM, Teixeira FC, Gomes AM, Vilanova E, Kozlowski EO, Borsig L, Pavão MS. Non-anticoagulant heparan sulfate from the ascidian phallusia nigra prevents colon carcinoma metastasis in mice by disrupting platelet-tumor cell interaction. Cancers. 2020 May 26;12(6):1353.
- Estaki M, Pither J, Baumeister P, Little JP, Gill SK, Ghosh S, Ahmadi-Vand Z, Marsden KR, Gibson DL. Cardiorespiratory fitness as a predictor of intestinal microbial diversity and distinct metagenomic functions. Microbiome. 2016 Dec;4:1-3.
- Giloteaux L, Goodrich JK, Walters WA, Levine SM, Ley RE, Hanson MR. Reduced diversity and altered composition of the gut microbiome in individuals with myalgic encephalomyelitis/chronic fatigue syndrome. Microbiome. 2016 Dec;4:1-2.
- Dumas A, Bernard L, Poquet Y, Lugo-Villarino G, Neyrolles O. The role of the lung microbiota and the gut–lung axis in respiratory infectious diseases. Cellular microbiology. 2018 Dec;20(12):e12966.
- Budden KF, Gellatly SL, Wood DL, Cooper MA, Morrison M, Hugenholtz P, Hansbro PM. Emerging pathogenic links between microbiota and the gut–lung axis. Nature Reviews Microbiology. 2017 Jan;15(1):55-63.
- Wang RX, Zhou M, Ma HL, Qiao YB, Li QS. The role of chronic inflammation in various diseases and anti-inflammatory therapies containing natural products. ChemMedChem. 2021 May 18;16(10):1576-92.
- Binda C, Lopetuso LR, Rizzatti G, Gibiino G, Cennamo V, Gasbarrini A. Actinobacteria: a relevant minority for the maintenance of gut homeostasis. Digestive and Liver Disease. 2018 May 1;50(5):421-8.
- Simpson CA, Diaz-Arteche C, Eliby D, Schwartz OS, Simmons JG, Cowan CS. The gut microbiota in anxiety and depression–A systematic review. Clinical psychology review. 2021 Feb 1;83:101943.
- Alenazy MF, Aljohar HI, Alruwaili AR, Daghestani MH, Alonazi MA, Labban RS, El-Ansary AK, Balto HA. Gut microbiota dynamics in relation to long-COVID-19 syndrome: role of probiotics to combat psychiatric complications. Metabolites. 2022 Sep 27;12(10):912.
- Yeoh YK, Zuo T, Lui GC, Zhang F, Liu Q, Li AY, Chung AC, Cheung CP, Tso EY, Fung KS, Chan V. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut. 2021 Apr 1;70(4):698-706.
- Chen J, Hall S, Vitetta L. Altered gut microbial metabolites could mediate the effects of risk factors in Covid-19. Reviews in Medical Virology. 2021 Sep;31(5):1-3.
- Tian Y, Ran H, Wen X, Fu G, Zhou X, Liu R, Pan T. Probiotics improve symptoms of patients with COVID-19 through gut-lung axis: a systematic review and meta-analysis. Front Nutr. 2023 May 22;10:1179432. [CrossRef] [PubMed]
- Ferreira C, Viana SD, Reis F. Gut microbiota dysbiosis–immune hyperresponse–inflammation triad in coronavirus disease 2019 (COVID-19): Impact of pharmacological and nutraceutical approaches. Microorganisms. 2020 Oct 1;8(10):1514.
- Zuo T, Wu X, Wen W, Lan P. Gut microbiome alterations in COVID-19. Genomics, proteomics & bioinformatics. 2021 Oct 1;19(5):679-88.
- Liu Q, Mak JW, Su Q, Yeoh YK, Lui GC, Ng SS, Zhang F, Li AY, Lu W, Hui DS, Chan PK. Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut. 2022 Mar 1;71(3):544-52.
- Zhang D, Zhou Y, Ma Y, Chen P, Tang J, Yang B, Li H, Liang M, Xue Y, Liu Y, Zhang J. Gut microbiota dysbiosis correlates with long COVID-19 at one-year after discharge. Journal of Korean Medical Science. 2023 Apr 4;38(15).
- Alenazy MF, Aljohar HI, Alruwaili AR, Daghestani MH, Alonazi MA, Labban RS, El-Ansary AK, Balto HA. Gut Microbiota Dynamics in Relation to Long-COVID-19 Syndrome: Role of Probiotics to Combat Psychiatric Complications. Metabolites. 2022 Sep 27;12(10):912. [CrossRef] [PubMed]
- Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, Morelli L, Canani RB, Flint HJ, Salminen S, Calder PC. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nature reviews Gastroenterology & hepatology. 2014.
- Shahbazi R, Yasavoli-Sharahi H, Alsadi N, Ismail N, Matar C. Probiotics in treatment of viral respiratory infections and neuroinflammatory disorders. Molecules. 2020 Oct 22;25(21):4891.
- Sandionigi A, De Giani A, Tursi F, Michelotti A, Cestone E, Giardina S, Zampolli J, Di Gennaro P. Effectiveness of multistrain probiotic formulation on common infectious disease symptoms and gut microbiota modulation in flu-vaccinated healthy elderly subjects. BioMed Research International. 2022 Jan 27;2022.
- Farzi A, Fröhlich EE, Holzer P. Gut microbiota and the neuroendocrine system. Neurotherapeutics. 2018 Jan 1;15(1):5-22.
- Buglione-Corbett R, Deligiannidis KM, Leung K, Zhang N, Lee M, Rosal MC, Moore Simas TA. Expression of inflammatory markers in women with perinatal depressive symptoms. Archives of women's mental health. 2018 Dec;21:671-9.
- Aziz T, Naveed M. Integrated genome based evaluation of safety and probiotic characteristics of Lactiplantibacillus plantarum YW11 isolated from Tibetan kefir. Frontiers in Microbiology. 2023 Apr 20;14:1157615.
- Rao AV, Bested AC, Beaulne TM, Katzman MA, Iorio C, Berardi JM, Logan AC. A randomized, double-blind, placebo-controlled pilot study of a probiotic in emotional symptoms of chronic fatigue syndrome. Gut pathogens. 2009 Dec;1:1-6.
- Venturini L, Bacchi S, Capelli E, Lorusso L, Ricevuti G, Cusa C. Modification of immunological parameters, oxidative stress markers, mood symptoms, and well-being status in CFS patients after probiotic intake: observations from a pilot study. Oxidative medicine and cellular longevity. 2019 Nov 23;2019.
- Williamson CB, Burns CM, Gossard CM, Pizano JM, Dolan KE, Finley HJ, Gasta MG, Parker EC, Lipski EA. Probiotics and disease: A comprehensive summary—Part 3, Cardiometabolic disease and fatigue syndromes. Integrative Medicine: A Clinician's Journal. 2017 Feb;16(1):30.
- Rathi A, Jadhav SB, Shah N. A randomized controlled trial of the efficacy of systemic enzymes and probiotics in the resolution of post-COVID fatigue. Medicines. 2021 Aug 30;8(9):47.
- Xu L, Yang CS, Liu Y, Zhang X. Effective regulation of gut microbiota with probiotics and prebiotics may prevent or alleviate COVID-19 through the gut-lung axis. Frontiers in Pharmacology. 2022 Apr 25;13:895193.
- Sohail A, Cheema HA, Mithani MS, Shahid A, Nawaz A, Hermis AH, Chinnam S, Nashwan AJ, Cherrez-Ojeda I, Awan RU, Ahmad S. Probiotics for the prevention and treatment of COVID-19: a rapid systematic review and meta-analysis. Frontiers in Nutrition. 2023;10.
- Jason LA, Natelson BH, Bonilla H, Sherif ZA, Vernon SD, Gutierrez MV, O’Brien L, Taylor E. What Long COVID investigators can learn from four decades of ME/CFS research. Brain Behavior and Immunity Integrative. 2023 Dec 1; 4: 100022.Jason LA, Natelson BH, Bonilla H, Sherif ZA, Vernon SD, Gutierrez MV, O’Brien L, Taylor E. What Long COVID investigators can learn from four decades of ME/CFS research. Brain Behavior and Immunity Integrative. 2023 Dec 1;4:100022. [Google Scholar]
- Roman P, Estévez AF, Miras A, Sánchez-Labraca N, Cañadas F, Vivas AB, Cardona D. A pilot randomized controlled trial to explore cognitive and emotional effects of probiotics in fibromyalgia. Scientific reports. 2018 Jul 19;8(1):10965.
- Groeger D, O’Mahony L, Murphy EF, Bourke JF, Dinan TG, Kiely B, Shanahan F, Quigley EM. Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut microbes. 2013 Jul 12;4(4):325-39.
- Sullivan Å, Nord CE, Evengård B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutrition journal. 2009 Jan 26;8(1):4.
- Tomkinson S, Triscott C, Schenk E, Foey A. The potential of probiotics as ingestible adjuvants and immune modulators for antiviral immunity and management of SARS-CoV-2 infection and COVID-19. Pathogens. 2023 Jul 11;12(7):928.
- Santinelli L, Laghi L, Innocenti GP, Pinacchio C, Vassalini P, Celani L, Lazzaro A, Borrazzo C, Marazzato M, Tarsitani L, Koukopoulos AE. Oral bacteriotherapy reduces the occurrence of chronic fatigue in COVID-19 patients. Frontiers in nutrition. 2022 Jan 12;8:1139.
- Caprioli F, Marinoni B, Rimondi A, Bottaro F, Ciafardini C, Amoroso C, Muia M, Caridi B, Noviello D, Bandera A, Gori A. The Role of VSL# 3 in the Treatment of Fatigue and Other Symptoms in Long Covid-19 Syndrome: a Randomized, Double-blind, Placebo-controlled Pilot Study (DELong# 3). medRxiv. 2023:2023-06.
- Khokhlova E, Colom J, Simon A, Mazhar S, García-Lainez G, Llopis S, Gonzalez N, Enrique-López M, Álvarez B, Martorell P, Tortajada M. Immunomodulatory and antioxidant properties of a novel potential probiotic Bacillus clausii CSI08. Microorganisms. 2023 Jan 18;11(2):240.
- Thomas R, Williams M, Aldous J, Yanagisawa Y, Kumar R, Forsyth R, Chater A. A randomised, double-blind, placebo-controlled trial evaluating concentrated phytochemical-rich nutritional capsule in addition to a probiotic capsule on clinical outcomes among individuals with COVID-19—the UK Phyto-V study. COVID. 2022 Mar 22;2(4):433-49.
- Hinchado MD, Quero-Calero CD, Otero E, Gálvez I, Ortega E. Synbiotic Supplementation Improves Quality of Life and Inmunoneuroendocrine Response in Patients with Fibromyalgia: Influence of Codiagnosis with Chronic Fatigue Syndrome. Nutrients. 2023 Mar 25;15(7):1591.
- Obermoser K, Brigo N, Schroll A, Monfort-Lanzas P, Gostner JM, Engl S, Geisler S, Knoll M, Schennach H, Weiss G, Fuchs D. Positive effects of probiotic therapy in patients with post-infectious fatigue. Metabolites. 2023 May 8;13(5):639.
- Ross, K. Psychobiotics: Are they the future intervention for managing depression and anxiety? A literature review. Explore. 2023 Sep 1;19(5):669-80.
- Warda AK, Rea K, Fitzgerald P, Hueston C, Gonzalez-Tortuero E, Dinan TG, Hill C. Heat-killed lactobacilli alter both microbiota composition and behaviour. Behavioural Brain Research. 2019 Apr 19;362:213-23.
- Zielińska D, Karbowiak M, Brzezicka A. The Role of Psychobiotics to Ensure Mental Health during the COVID-19 Pandemic—A Current State of Knowledge. International Journal of Environmental Research and Public Health. 2022 Sep 3;19(17):11022.
- Sharma R, Gupta D, Mehrotra R, Mago P. Psychobiotics: The next-generation probiotics for the brain. Current microbiology. 2021 Feb;78:449-63.
- Miyaoka T, Kanayama M, Wake R, Hashioka S, Hayashida M, Nagahama M, Okazaki S, Yamashita S, Miura S, Miki H, Matsuda H. Clostridium butyricum MIYAIRI 588 as adjunctive therapy for treatment-resistant major depressive disorder: a prospective open-label trial. Clinical neuropharmacology. 2018 Sep 1;41(5):151-5.
- Diop L, Guillou S, Durand H. Probiotic food supplement reduces stress-induced gastrointestinal symptoms in volunteers: a double-blind, placebo-controlled, randomized trial. Nutrition research. 2008 Jan 1;28(1):1-5.
- Eskandarzadeh S, Effatpanah M, Khosravi-Darani K, Askari R, Hosseini AF, Reisian M, Jazayeri S. Efficacy of a multispecies probiotic as adjunctive therapy in generalized anxiety disorder: a double blind, randomized, placebo-controlled trial. Nutritional Neuroscience. 2021 Feb 1;24(2):102-8.
- Mohammadi AA, Jazayeri S, Khosravi-Darani K, Solati Z, Mohammadpour N, Asemi Z, Adab Z, Djalali M, Tehrani-Doost M, Hosseini M, Eghtesadi S. The effects of probiotics on mental health and hypothalamic–pituitary–adrenal axis: A randomized, double-blind, placebo-controlled trial in petrochemical workers. Nutritional neuroscience. 2016 Nov 8;19(9):387-95.
- Akkasheh G, Kashani-Poor Z, Tajabadi-Ebrahimi M, Jafari P, Akbari H, Taghizadeh M, Memarzadeh MR, Asemi Z, Esmaillzadeh A. Clinical and metabolic response to probiotic administration in patients with major depressive disorder: a randomized, double-blind, placebo-controlled trial. Nutrition. 2016 Mar 1;32(3):315-20.
- Marotta A, Sarno E, Del Casale A, Pane M, Mogna L, Amoruso A, Felis GE, Fiorio M. Effects of probiotics on cognitive reactivity, mood, and sleep quality. Frontiers in psychiatry. 2019 Mar 27;10:427235.
- Ait-Belgnaoui A, Colom A, Braniste V, Ramalho L, Marrot A, Cartier C, Houdeau E, Theodorou V, Tompkins T. Probiotic gut effect prevents the chronic psychological stress-induced brain activity abnormality in mice. Neurogastroenterology & Motility. 2014 Apr;26(4):510-20.
- Andersson H, Tullberg C, Ahrné S, Hamberg K, Lazou Ahrén I, Molin G, Sonesson M, Håkansson Å. Oral administration of Lactobacillus plantarum 299v reduces cortisol levels in human saliva during examination induced stress: a randomized, double-blind controlled trial. International journal of microbiology. 2016 Oct;2016.
- Lalitsuradej E, Sirilun S, Sittiprapaporn P, Sivamaruthi BS, Pintha K, Tantipaiboonwong P, Khongtan S, Fukngoen P, Peerajan S, Chaiyasut C. The effects of synbiotics administration on stress-related parameters in thai subjects—a preliminary study. Foods. 2022 Mar 6;11(5):759.
- Ghorbani Z, Nazari S, Etesam F, Nourimajd S, Ahmadpanah M, Jahromi SR. The effect of synbiotic as an adjuvant therapy to fluoxetine in moderate depression: a randomized multicenter trial. Archives of neuroscience. 2018 Apr 30;5(2).
- Lennartsson AK, Theorell T, Kushnir MM, Bergquist J, Jonsdottir IH. Perceived stress at work is associated with attenuated DHEA-S response during acute psychosocial stress. Psychoneuroendocrinology. 2013 Sep 1;38(9):1650-7.
- Morris G, Anderson G, Maes M. Hypothalamic-pituitary-adrenal hypofunction in myalgic encephalomyelitis (ME)/chronic fatigue syndrome (CFS) as a consequence of activated immune-inflammatory and oxidative and nitrosative pathways. Molecular neurobiology. 2017 Nov;54:6806-19.
- Lau HC, Ng SC, Yu J. Targeting the Gut Microbiota in Coronavirus Disease 2019: Hype or Hope? Gastroenterology. 2022 Jan;162(1):9-16. [CrossRef] [PubMed]
- Alenazy MF, Aljohar HI, Alruwaili AR, Daghestani MH, Alonazi MA, Labban RS, El-Ansary AK, Balto HA. Gut Microbiota Dynamics in Relation to Long-COVID-19 Syndrome: Role of Probiotics to Combat Psychiatric Complications. Metabolites. 2022 Sep 27;12(10):912. [CrossRef] [PubMed]
- Thye AY, Law JW, Tan LT, Pusparajah P, Ser HL, Thurairajasingam S, Letchumanan V, Lee LH. Psychological Symptoms in COVID-19 Patients: Insights into Pathophysiology and Risk Factors of Long COVID-19. Biology (Basel). 2022 Jan 2;11(1):61. [CrossRef] [PubMed]
- Del Toro-Barbosa M, Hurtado-Romero A, Garcia-Amezquita LE, García-Cayuela T. Psychobiotics: mechanisms of action, evaluation methods and effectiveness in applications with food products. Nutrients. 2020 Dec 19;12(12):3896.
- Corbitt M, Campagnolo N, Staines D, Marshall-Gradisnik S. A systematic review of probiotic interventions for gastrointestinal symptoms and irritable bowel syndrome in chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). Probiotics and antimicrobial proteins. 2018 Sep;10:466-77.
- Choudhury A, Tariq R, Jena A, Vesely EK, Singh S, Khanna S, Sharma V. Gastrointestinal manifestations of long COVID: A systematic review and meta-analysis. Therap Adv Gastroenterol. 2022 Aug 19;15:17562848221118403. [CrossRef] [PubMed]
- Chakraborty C, Sharma AR, Bhattacharya M, Dhama K, Lee SS. Altered gut microbiota patterns in COVID-19: Markers for inflammation and disease severity. World J Gastroenterol. 2022 Jul 7;28(25):2802-2822. [CrossRef] [PubMed]
- Lymberopoulos E, Gentili GI, Budhdeo S, Sharma N. COVID-19 severity is associated with population-level gut microbiome variations. Front Cell Infect Microbiol. 2022 Aug 23;12:963338. [CrossRef] [PubMed]
- d'Ettorre G, Ceccarelli G, Marazzato M, Campagna G, Pinacchio C, Alessandri F, Ruberto F, Rossi G, Celani L, Scagnolari C, Mastropietro C. Challenges in the management of SARS-CoV2 infection: the role of oral bacteriotherapy as complementary therapeutic strategy to avoid the progression of COVID-19. Frontiers in medicine. 2020 Jul 7;7:389.
- Sfera A, Osorio C, Hazan S, Kozlakidis Z, Maldonado JC, Zapata-Martín del Campo CM, Anton JJ, Rahman L, Andronescu CV, Nicolson GL. Long COVID and the Neuroendocrinology of Microbial Translocation Outside the GI Tract: Some Treatment Strategies. Endocrines. 2022 Nov 7;3(4).
- Geirnaert A, Calatayud M, Grootaert C, Laukens D, Devriese S, Smagghe G, De Vos M, Boon N, Van de Wiele T. Butyrate-producing bacteria supplemented in vitro to Crohn’s disease patient microbiota increased butyrate production and enhanced intestinal epithelial barrier integrity. Scientific reports. 2017 Sep 13;7(1):11450.
- Homayouni-Rad A, Soleimani RA, Khani N. Can postbiotics prevent or improve SARS-CoV-2?. Current Nutrition & Food Science. 2023 Oct 1;19(8):756-7.
- Johnson D, Thurairajasingam S, Letchumanan V, Chan KG, Lee LH. Exploring the role and potential of probiotics in the field of mental health: Major depressive disorder. Nutrients. 2021 ;13(5):1728. 20 May.
- El Dib R, Periyasamy AG, de Barros JL, França CG, Senefonte FL, Vesentini G, Alves MG, da Silva Rodrigues JV, Gomaa H, Júnior JR, Costa LF. Probiotics for the treatment of depression and anxiety: A systematic review and meta-analysis of randomized controlled trials. Clinical nutrition ESPEN. 2021 Oct 1;45:75-90.
- Zhou J, Li M, Chen Q, Li X, Chen L, Dong Z, Zhu W, Yang Y, Liu Z, Chen Q. Programmable probiotics modulate inflammation and gut microbiota for inflammatory bowel disease treatment after effective oral delivery. Nature Communications. 2022 Jun 14;13(1):3432.
- Kumar LS, Pugalenthi LS, Ahmad M, Reddy S, Barkhane Z, Elmadi J. Probiotics in irritable bowel syndrome: a review of their therapeutic role. Cureus. 2022 Apr 18;14(4).
- Haarhuis JE, Kardinaal A, Kortman GA. Probiotics, prebiotics and postbiotics for better sleep quality: A narrative review. Beneficial Microbes. 2022 Aug 3;13(3):169-82.
- Castro-Marrero J, Faro M, Aliste L, Sáez-Francàs N, Calvo N, Martínez-Martínez A, de Sevilla TF, Alegre J. Comorbidity in chronic fatigue syndrome/myalgic encephalomyelitis: a nationwide population-based cohort study. Psychosomatics. 2017 Sep 1;58(5):533-43.
- Castro-Marrero J, Domingo JC, Cordobilla B, Ferrer R, Giralt M, Sanmartín-Sentañes R, Alegre-Martín J. Does coenzyme Q10 plus selenium supplementation ameliorate clinical outcomes by modulating oxidative stress and inflammation in individuals with myalgic encephalomyelitis/chronic fatigue syndrome?
- Barletta MA, Marino G, Spagnolo B, Bianchi FP, Falappone PC, Spagnolo L, Gatti P. Coenzyme Q10+ alpha lipoic acid for chronic COVID syndrome. Clinical and Experimental Medicine. 2023 Jul;23(3):667-78.

Table 1.
A summary of studies investigating use of microbial-based preparations for management of symptoms in ME/CFS and Long COVID.
Table 1.
A summary of studies investigating use of microbial-based preparations for management of symptoms in ME/CFS and Long COVID.
| Participants (n) | Intervention (dose) |
Duration | Outcomes | References | |
|---|---|---|---|---|---|
| ME/CFS patients (n=83) |
Single probiotic: Lactobacillus casei Shirota |
8 weeks | Reduced anxiety scores, Changed the faecal composition |
[88] | |
| ME/CFS patients (n=83) |
Single probiotic: Bifidobacterium infantis 35624 |
8 weeks | Reduced inflammatory biomarkers (CRP, IL-6) | [88] | |
| ME/CFS patients (n=9) |
Probiotic protocol: Enterelle (given in week 1, 4-8): Saccharomyces cerevisiae sub. Boilardii MTCC-5375, Saccharomyces cerevisiae sub. Boilardii SP92, Enterococcus faecium UBEF41, Lactobacillus acidophilus LA14 Bifiselle (given in week 2): Bifidobacterium lactis BL04, Bifidobacterium breve BB03, Bifidobacterium bifidum BB06, Bifidobacterium longum BL05 Citogenex (given in week 4-8): Saccharomyces spp extract titrated in 1-3 beta glucans, Vitamin C, Lactobacillus casei LC11, Bifidobacterium lactis BL04, Lactobacillus acidophilus LA14 Ramnoselle (given in week 3, 4-8): Lactobacillus acidophilus LA14, Lactobacillus rhamnosus LR32, Lactobacillus rhamnosus HN001 |
2 caps/a day Each strain > 1 × 109 CFU |
8 weeks | Reduction of fatigue on the Chadler’s scale, Improvement of physical and mental conditions, Overall increase in the quality of life on the SF-36 score, Improvement of mood on PCS score, Reduced depression symptoms on BDI-I and II scores Reduced inflammation (CRP); Improvement in immune defense (increase in IgM, reduction in CD4/CD8 ratio); Inconsistent effects on oxidative status |
[82] |
| ME/CFS (n=15) |
Multistrain probiotic: Lactobacillus F19 Lactobacillus acidophilus NCFB 1748 Bifidobacterium lactis Bb12 |
× 108 CFU/ml | weeks | Improvement in neurocognitive functions measured as the VAS mean, Inconsistent effects fatigue, mental and physical health, No major changes in GI microbiota |
[90] |
| Hospitalized COVID-19 patients (n=24) |
Multistrain probiotic (SLAB51; Sivomixx800®): Streptococcus thermophilus DSM 32245®, Bifidobacterium lactis DSM 32246®, Bifidobacterium lactis DSM 32247®, Lactobacillus acidophilus DSM 32241®, Lactobacillus helveticus DSM 32242®, Lactobacillus paracasei DSM 32243®, Lactobacillus plantarum DSM 32244®, Lactobacillus brevis DSM 27961® |
3 equal doses of a total of 2.400 × 1011 CFU billion bacteria per day | 23 days | Reduced fatigue on FAS score, Minor changes in metabolomic profile - increased levels of arginine, asparagine, lactate, and decreased levels of 3-Hydroxyisobutyrate following probiotic intake, |
[92] |
| Long COVID patients (19) |
Multistrain probiotic (VSL#3®): Streptococcus thermophilus BT01, Bifidobacterium breve BB02, Bifidobacterium animalis subsp. lactis BL03, Bifidobacterium animalis subsp. lactis BI04, Lactobacillus acidophilus BA05, Lactobacillus plantarum BP06, Lactobacillus paracasei BP07, Lactobacillus helveticus BD08 |
2 shashets a day, A total of 4.5 × 1011 CFU per sachet | 4 weeks | Reduced fatigue (Chalder Fatigue Scale), Significant improvement on physical functioning on SF-36 scale, Reduction in GI symptoms on SAGIS score), No significant difference in specific symptoms of acid regurgitation, nausea and vomiting, constipation, epigastric pain and IBS symptoms vs placebo, No effects on psychiatric symptoms of anxiety, depression, performance and somatization symptoms on SCL-12 scale, |
[93] |
| Fatigue subjects (9) |
Single probiòtic: Lactobacillus paracasei HII01 |
4 × 1010 CFU/g | 12 weeks | Decreased salivary levels of cortisol, No effects on DHEA-S concentration, Decreased ratio cortisol: DHEA-S, |
[110] |
| Hospitalized COVID patients (28) |
Multistrain probiotic (Sivomixx®): Streptococcus thermophilus DSM 32345, Lactobacillus acidophilus DSM 32241, Lactobacillus helveticus DSM 32242, Lacticaseibacillus paracasei DSM 32243, Lactobacillus plantarum DSM 32244, Lactobacillus brevis DSM 27961, Bifidobacterium lactis DSM 32246, Bifidobacterium lactis DSM 32247 |
2.5 × 1010 CFU/a day | 1 week | Amelioration of in diarrhea within 3-7 days, Reduction in other symptoms, including fever, asthenia, headache, myalgia, and dyspnea within 2 days, Improvement in respiratory function – 8-fold reduced risk of respiratory failure, |
[122] |
| Multi-ingredient microbial preparations | |||||
| Long COVID patients (100) |
ImmunoSEB formulation: Probiotics - ProbioSEB CSC3: Bacillus coagulans LBSC (DSM 17654), Bacillus subtilis PLSSC (ATCC SD 7280), Bacillus clausii 088AE (MCC 0538) Bioactives: Peptizyme SP: enteric coated serratiopeptidase, bromelain, amylase, lysozyme, peptidase, catalase, papain, glucoamylase, lactoferrin |
4 capsules a day: One capasule: ImmunoSEB: 500g/capsule + ProbioSEB CSC3: 5 × 1010 CFU/capsule |
2 weeks | Significant reduction of fatigue determined by by the CFQ-11 score (87% of patients were fatigue free in the end of interevention), Significant reduction in all individual measures of physical fatigue (tiredness, need to rest, drowsiness, ability to do things, energy level, muscle strength and feeling of weakness), Significant reduction in mental fatigue (concentration, focus and memory), No adverse events reported, including nausea, vomiting or diarrhea at any stage of study |
[84] |
| Long COVID patients (126) | Phytochemical-rich concentrated food capsule: Probiotic: Lactobacillus plantarum, Lactobacillus rhamnosus, Lactobacillus bulgaricus, Lactococcus lactis Lactobacillus paracasei Prebiotic: Inulin fibre Bioactives: Citrus Sinensis fruit, Chamomile (Matricaria recutita L. flower), Curcuma Longa, Pomegranate (Punica granatum L.), Resveratrol (Polygonum cuspidatum root) |
1 capsule given twice a day Probiotic: 10 × 1010 CFU/total in capsule Prebiotic: 200mg/capsule Phytochemical-rich whole food capsule (PC): Citrus Sinensis fruit: 400 mg, inc. 70 mg of bioflavonoids, Chamomile (Matricaria recutita L. flower): 1000 mg, Curcuma Longa: 23.8mg of curcuminoid, Pomegranate (Punica granatum L.): 1000mg, incl. 10mg ellagic acid, Polygonum cuspidatum root: 100 mg of resveratrol |
2 weeks | 2-fold reduction in fatigue measured on the Chalder Fatigue Scale vs placebo, Reduction in other symtoms associated with infection, including cough, Improved overall well-being measured on SWB score, |
[95] |
| Fibromyalgia (FM) patients co-diagnosed with ME/CFS (15) | Synbiotic (Gasteel Plus®) formulation: Probiotics: Bifidobacterium lactis CBP-001010, Lactobacillus rhamnosus CNCM I-4036 Bifidobacterium longum ES1 Prebiotic: Fructooligosaccharides Bioactives: Zinc, Selenium, Vitamin D |
Each synbiotic bar (300mg): Probiotic: 1 × 109 CFU/total in bar Prebiotic: 200mg/bar Bioactives: Zinc: 1.5mg Selenium: 8.25mg Vitamin D: 0.75g |
2 weeks | No changes in the objective perception of activity/sedentarism and sleep, Significant improvements in depression, stress, anxiety and fatigue in FM patients, Significant improvement in anxiety and fatigue in FM patients with ME/CFS, Reduced inflammation (decrease in IL-8, increse in IL-10) among FM patients, Increased ratio of cortisol/DHEA in all participants, Overall no significant benefits for improved pain, sleep quality and gastrointestinal health of the participants. |
[96] |
| Long COVID patients (70) | OMNi-BiOTiC®STRESS Repair 9” formulation: Probiotics: Lactobacillus casei W56, Lactobacillus acidophilus W22, Lactobacillus paracasei W20, Bifidobacterium lactis W51, Lactobacillus salivarius W24, Lactococcus lactis W19, Bifidobacterium lactis W52, Lactobacillus plantarum W62, Bifidobacterium bifidum W23 Prebiotic: Fructooligosaccharides, inulin Bioactives: Enzymes (amylases), Potassium chloride, Manganese sulfate, Vitamin B2 , Vitamin B6 , Vitamin B12 |
Each sachet: 3g Probiotic: 7.5 × 109 CFU/total in sachet Prebiotic: N/A Bioactives: Enzymes (amylases), Potassium chloride, Manganese sulfate, Vitamin B2 Vitamin B6 Vitamin B12 |
24 weeks | Significant reduction in the fatigue on the FSS score vs placebo, Significant improvement in the severity of depression, Significant improvement in the quality of life, including physical functioning and general Health. Improvement of digestion and reduction of GI complaints. No effect on immune parameters. |
[97] |
CFU, Colony Forming Unit; n, number of participants.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



