
Submitted:
29 April 2024
Posted:
01 May 2024
You are already at the latest version
Abstract
Graves' disease (GD) is an autoimmune disorder in which Thyrotropin Receptor Antibodies (TRAb) continuously stimulate thyroid receptors, leading to excessive production of thyroid hormones. TRAb also affect the orbital tissues, causing Graves' ophthalmopathy. Treatment to control Graves' disease consists of antithyroid drugs, radioiodine and thyroidectomy, and through such treatments, TRAb is reduced and the disease is alleviated. The mechanism by which TRAb, which play a critical role in the pathogenesis of Graves’ disease, decreases after GD treatment is still unknown. This paper presents a theoretical mechanism of how GD patients maintain a vicious cycle and how GD treatment can reduce the TRAb levels and breaks the cycle using stress-based ideas.
Keywords:
Graves' disease
; hyperthyroidism
; Graves' ophthalmopathy
; antithyroid drugs
; stress
1. Introduction
Graves' disease is an autoimmune disorder in which thyrotropin receptor antibodies (TRAb) appear for some reason, which stimulate the thyroid stimulating hormone (TSH) receptors on the surface of thyroid follicular cells, generally creating a state of hyperthyroidism. It suggests that TRAb suppress TSH secretion independently of thyroid hormone (TH) levels even in treated euthyroid Graves' disease patients [1,2]and interfere with the binding of TSH to thyroid receptors [3]. Additionally, in untreated GD patients, TRAb maintains high TH levels independent of negative feedback, which lowers TSH that is controlled by that feedback. Therebefore, it seems that in GD patients, TH synthesis and secretion are entirely controlled by TRAB before treatment. It also suggests that TRAb are independent risk factors for graves’ ophthalmopathy [4]. The key to treating Graves' hyperthyroidism is to restore TH levels to normal, reduce TRAb levels, and normalize TSH levels. Since TRAb level at the end of drug treatment is reported to be closely related to a high likelihood of relapse or entering into a sustained remission [5], therefore lowering TRAb levels will be a crucial role in the treatment of GD.
2. Materials and Methods
Antithyroid Drugs
Antithyroid drugs (ATD) belong to the class of thionamides (carbimazole (in the UK), methimazole and propylthiouracil (in the US)) and have been used to treat thyrotoxicosis since the 1940s. A recent meta-analysis including 6 studies with ATD duration of > 24 months in adults with GD documented a remission rate of 57% [6].However the mechanisms of action of ATD are not completely understood, in particular, how the drugs lower TRAb levels, which causes GD, only knowing that the action of these drugs is to inhibit TH synthesis [7]. There was once a hypothesis that ATD directly lower TRAb levels by immunosuppressive effect [8]. However, the hypothesis is unconvincing for the following reasons. 1) In addition to thyroid hormone synthesis inhibitors, TRAb can also be reduced by thyroidectomy or radioiodine treatment [9,10] 2) No difference in remission rates between low and high-dose ATD regimens [11] 3) Although it is a case report, administration of large and sudden doses of methimazole increased TRAb [12] Therefore, rather than saying that these agents have a direct immunosuppressive effect, it seems more reasonable to think that they reduce TH levels and that the reduced TH lowers TRAb indirectly through some mediators [13,14,15].
Vicious Cycle in GD Patients
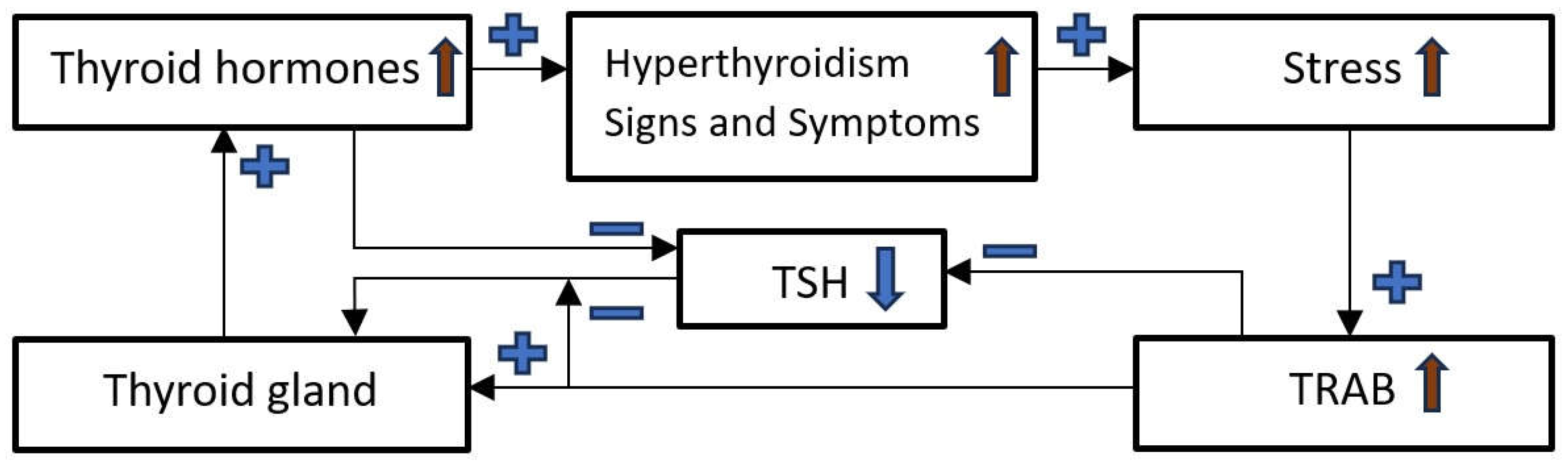
Hyperthyroidism signs and symptoms: Nervousness, anxiety, irritability, increased heat sensitivity, difficulty sleeping, mood swings, feeling tired all the time, palpitations, weight loss, muscle weakness, altered menstrual rhythm, eye problems, such as redness, dryness or vision problems, trembling hands and legs, increased intestinal transit, warm skin and excessive sweating etc. [16]. The above symptoms and signs of hyperthyroidism themselves act as emotional and physical stress in GD patients. Additionally, GD patients react more sensitively to external stress, for example, they may become easily irritated or have severe heart palpitations due to exposure to mild heat or a minor argument with a colleague. Furthermore, some experimental studies showed an elevated oxidative stress during hyperthyroidism [17]. In several studies, stress is known to act as a trigger for the onset and recurrence of autoimmune diseases, including GD, as well as to create and maintain their vicious cycles by altering the cytokine profile released [18,19].
Figure 1.
Vicious cycle in GD patients.
Breaking the Vicious Cycle
Regardless of treatment modality, restoration of euthyroidism is accompanied by improvement in the quality of life and psychological symptoms in GD patients [21] as well as alleviating systemic oxidative stress [17,22]. Such improvement in stress resulting from treatments will reduce TRAb levels and break the vicious cycle of GD.
Through a logical interpretation of the results of various related studies, it is highly likely that the improvement or cure of GD can be achieved by alleviating stress related to the signs and symptoms of GD by lowering the excess TH level regardless of the treatments methods.
3. Discussion
Anti-thyroid drugs, the main treatment for the disease, were developed about 80 years ago, but the exact mechanism is still unknown. There is little evidence that the drugs directly reduce levels of TRAb, which causes the disease. This paper describes a possible mechanism for how GD can be alleviated and cured. What drug therapy, radioiodine and thyroidectomy have in common is to restore elevated thyroid hormones to normal levels. Several studies have shown that restoration of normal levels of TH reduces mental, physical and oxidative stress which are associated with a decrease in autoimmune antibody levels. In that context, drugs such as benzodiazepines, which reduce patients' mental stress, or supplements with antioxidant effects such as selenium may be helpful [23,24,25].GD is easier to treat and cure than other autoimmune diseases, such as rheumatoid arthritis. The reason may be that it is easier to break the vicious cycle mediated by stress than other autoimmune diseases. Elevated TH level is associated with stress, and alleviating that stress can be achieved simply by lowering TH levels with any treatment.
However, a phenomenon is observed that contradicts the claim in this paper. This paper says that TRAb level decreases when the high TH level recovers to normal, but it is observed that after radioiodine treatment TRAb temporarily increases and that transient increase in TRAb is associated with the deterioration and the onset of the grave´s ophthalmopathy [26]. The exact cause for that is not yet clear, but the following reasons are possible:
1. Radioiodine treatment itself causes oxidative stress [29] which may increase TRAb.
2. Due to the high incidence of transient hypothyroidism during the first 3 months following radioiodine treatment [30]. Several studies observed that TRAb increased even more in the patients who transitioned to hypothyroidism [31,32]. Hypothyroidism is also related to increasing oxidative stress which led to TRAb increase [33].
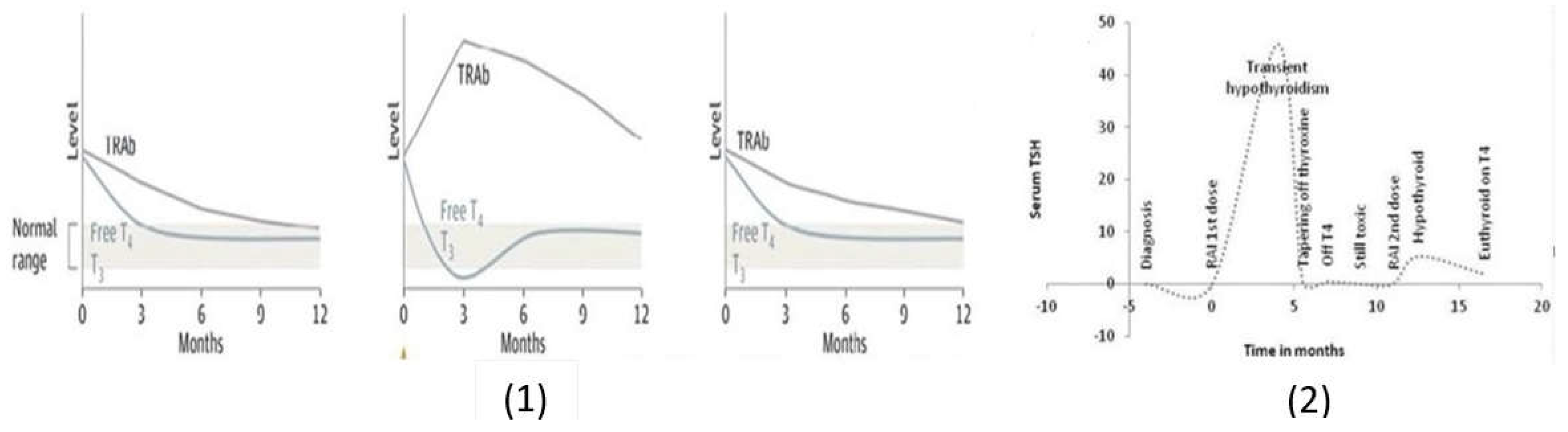
3. Due to the sudden decrease in TH level. As observed in the article (Figure 2-(1)) [27], radioiodine treatment reduces TH level more rapidly than other treatments, as a result that TRAb level may temporarily increase as a rebounding effect to the sudden decrease in TH level. The simultaneous increase of TSH and TRAb immediately after treatment can support this thought (Figure 2-(1)) [28]. Levothyroxine replacement during this time will slow the rate of decrease in TH levels and prevent transient hypothyroidism, slowing down the TRAb increase rate, and consequently helping to prevent RAI-induced ophthalmopathy [34].
(1). Change in TH and TRAb levels after anti-thyroid drug(left), radioiodine (middle), total thyroidectomy (right) [27]
(2). Change in TSH level by radioiodine therapy for GD patients [28].
Although there have been numerous papers on GD so far, there are still very few papers on the mechanism by which the disease is cured. Understanding the mechanism will help treat the disease more effectively and develop new drugs to treat the disease. This paper explains the mechanism of GD treatments with this logical chain relationship: "elevated TH level -> worsening of stress -> high TRAb level -> maintain elevated TH level-> vicious cycle-> treatment -> normalization of TH level -> relief of stress -> reduction of TRAb -> alleviation of disease" However, we cannot rule out the possibility that TH reduction itself causes a decrease in TRAB levels, which is the main cause of the disease, by mediators other than stress. Nevertheless, it appears that stress is the main mediator of maintaining the vicious cycle of GD and its curing.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, S.S.; methodology, S.S and J.M.V.L..; formal analysis, S.S., J.M.A.L and J.M.V.L.; investigation, S.S.; resources, S.S.; data curation, S.S and J.M.V.L..; writing—original draft preparation, S.S..; writing—review and editing, J.M.A.L. and J.M.V.L..; supervision, J.M.A.L. and J.M.V.L..; project administration, J.M.V.L.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Brokken, L. J. , Wiersinga, W. M., & Prummel, M. F. (2003). Thyrotropin receptor autoantibodies are associated with continued thyrotropin suppression in treated euthyroid Graves’ disease patients. The Journal of Clinical Endocrinology & Metabolism, 88(9), 4135-4138.
- Chung, Y. J. , Lee, B. W., Kim, J. Y., Jung, J. H., Min, Y. K., Lee, M. S.,... & Chung, J. H. (2006). Continued suppression of serum TSH level may be attributed to TSH receptor antibody activity as well as the severity of thyrotoxicosis and the time to recovery of thyroid hormone in treated euthyroid Graves' patients. Thyroid, 16(12), 1251-1257.
- Barbesino, G. , & Tomer, Y. (2013). Clinical utility of TSH receptor antibodies. The Journal of Clinical Endocrinology & Metabolism, 98(6), 2247-2255.
- Eckstein, A. K. , Plicht, M., Lax, H., Neuhäuser, M., Mann, K., Lederbogen, S.,... & Morgenthaler, N. G. (2006). Thyrotropin receptor autoantibodies are independent risk factors for Graves’ ophthalmopathy and help to predict severity and outcome of the disease. The Journal of Clinical Endocrinology & Metabolism, 91(9), 3464-3470.
- Orgiazzi, J. , & Madec, A. M. (2002). Reduction of the risk of relapse after withdrawal of medical therapy for Graves' disease. Thyroid, 12(10), 849-853.
- Abdi, H. , Amouzegar, A., & Azizi, F. (2019). Antithyroid drugs. Iranian journal of pharmaceutical research: IJPR, 18(Suppl1), 1.
- Burch, H. B. , & Cooper, D. S. (2018). Antithyroid drug therapy: 70 years later. European Journal of Endocrinology, 179(5), R261-R274.
- Tötterman, T. H. , Karlsson, F. A., Bengtsson, M., & Mendel-Hartvig, I. B. (1987). Induction of circulating activated suppressor-like T cells by methimazole therapy for Graves' disease. New England Journal of Medicine, 316(1), 15-22.
- Laurberg, P. , Wallin, G., Tallstedt, L., Abraham-Nordling, M., Lundell, G., & Tørring, O. (2008). TSH-receptor autoimmunity in Graves' disease after therapy with anti-thyroid drugs, surgery, or radioiodine: a 5-year prospective randomized study. European Journal of Endocrinology, 158(1), 69-75.
- Törring, O. , Tallstedt, L., Wallin, G., Lundell, G., Ljunggren, J. G., Taube, A.,... & Hamberger, B. (1996). Graves' hyperthyroidism: treatment with antithyroid drugs, surgery, or radioiodine--a prospective, randomized study. Thyroid Study Group. The Journal of Clinical Endocrinology & Metabolism, 81(8), 2986-2993.
- Reinwein, D. , Benker, G., Lazarus, J. H., & Alexander, W. D. (1993). A prospective randomized trial of antithyroid drug dose in Graves' disease therapy. European Multicenter Study Group on Antithyroid Drug Treatment. The Journal of Clinical Endocrinology & Metabolism, 76(6), 1516-1521.
- Lewandowski, K. C. , Marcinkowska, M., Skowrońska-Jóźwiak, E., Makarewicz, J., & Lewiński, A. (2008). New onset Graves' disease as a cause of an adrenal crisis in an individual with panhypopituitarism: brief report. Thyroid Research, 1, 1-5.
- Volpe, R. (1994). Evidence that the immunosuppressive effects of antithyroid drugs are mediated through actions on the thyroid cell, modulating thyrocyte-immunocyte signaling: a review. Thyroid, 4(2), 217-223.
- Kocjan, T. , Wraber, B., Kocijančič, A., & Hojker, S. (2004). Methimazole upregulates T-cell-derived cytokines without improving the existing Th1/Th2 imbalance in Graves’ disease. Journal of Endocrinological Investigation, 27, 302-307.
- Wenzel, K. W. , & Lente J. R. (1984). Similar effects of thionamide drugs and perchlorate on thyroid-stimulating immunoglobulins in Graves' disease: evidence against an immunosuppressive action of thionamide drugs. The Journal of Clinical Endocrinology & Metabolism, 58(1), 62-69.
- Stern, R. A. , Robinson, B., Thorner, A. R., Arruda, J. E., Prohaska, M. L., & Prange Jr, A. J. (1996). A survey study of neuropsychiatric complaints in patients with Graves' disease. Journal of Neuropsychiatry and Clinical Neurosciences, 8(2), 181-185.
- Bianchi, G. , Solaroli, E., Zaccheroni, V. A. A., Grossi, G., Bargossi, A. M., Melchionda, N., & Marchesini, G. (1999). Oxidative stress and anti-oxidant metabolites in patients with hyperthyroidism: effect of treatment. Hormone and Metabolic Research, 31(11), 620-624.
- Stojanovich, L., & Marisavljevich, D. (2008). Stress as a trigger of autoimmune disease. Autoimmunity Reviews, 7(3), 209-213.
- Sharif, K. , Watad, A., Coplan, L., Lichtbroun, B., Krosser, A., Lichtbroun, M.,... & Shoenfeld, Y. (2018). The role of stress in the mosaic of autoimmunity: an overlooked association. Autoimmunity Reviews, 17(10), 967-983.
- Vita, R. , Lapa, D., Trimarchi, F., & Benvenga, S. (2015). Stress triggers the onset and the recurrences of hyperthyroidism in patients with Graves’ disease. Endocrine, 48, 254-263.
- Gulseren, S. , Gulseren, L., Hekimsoy, Z., Cetinay, P., Ozen, C., & Tokatlioglu, B. (2006). Depression, anxiety, health-related quality of life, and disability in patients with overt and subclinical thyroid dysfunction. Archives of medical research, 37(1), 133-139.
- Larsen, C. B. , Riis, K. R., Winther, K. H., Larsen, E. L., Ellervik, C., Hegedüs, L.,... & Bonnema, S. J. (2021). Treatment of hyperthyroidism reduces systemic oxidative stress, as measured by markers of RNA and DNA damage. The Journal of Clinical Endocrinology & Metabolism, 106(7), e2512-e2520.
- Vita, R. , Lapa, D., Vita, G., Trimarchi, F., & Benvenga, S. (2009). A patient with stress-related onset and exacerbations of Graves’ disease. Nature Clinical Practice Endocrinology & Metabolism, 5(1), 55-61.
- Benvenga, S. (1996). Benzodiazepine and remission of Graves' disease. Thyroid, 6(6), 659-660.
- Wang, L. , Wang, B., Chen, S. R., Hou, X., Wang, X. F., Zhao, S. H.,... & Wang, Y. G. (2016). Effect of selenium supplementation on recurrent hyperthyroidism caused by Graves’ disease: a prospective pilot study. Hormone and Metabolic Research, 48(09), 559-564.
- Shahida, B. , Tsoumani, K., Planck, T., Modhukur, V., Asp, P., Sundlöv, A.,... & Lantz, M. (2022). Increased risk of Graves´ ophthalmopathy in patients with increasing TRAb after radioiodine treatment and the impact of CTLA4 on TRAb titres. Endocrine, 75(3), 856-864.
- Burch, H. B. , & Cooper, D. S. (2015). Management of Graves disease: a review. JAMA, 314(23), 2544-2554.
- Sheehan, M. T. , & Doi, S. A. (2016). Transient hypothyroidism after radioiodine for Graves’ disease: challenges in interpreting thyroid function tests. Clinical Medicine & Research, 14(1), 40-45.
- Abalovich, M. , Llesuy, S., Gutierrez, S., & Repetto, M. (2003). Peripheral parameters of oxidative stress in Graves’ disease: the effects of methimazole and 131 iodine treatments. Clinical Endocrinology, 59(3), 321-327.
- Stan, M. N. , Durski, J. M., Brito, J. P., Bhagra, S., Thapa, P., & Bahn, R. S. (2013). Cohort Study on Radioactive Iodine–Induced Hypothyroidism: Implications for Graves' Ophthalmopathy and Optimal Timing for Thyroid Hormone Assessment. Thyroid, 23(5), 620-625.
- Perros, P. , Kendall-Taylor, P., Neoh, C., Frewin, S., & Dickinson, J. (2005). A prospective study of the effects of radioiodine therapy for hyperthyroidism in patients with minimally active Graves’ ophthalmopathy. The Journal of Clinical Endocrinology & Metabolism, 90(9), 5321-5323.
- Aizawa, Y. , Yoshida, K., Kaise, N., Fukazawa, H., Kiso, Y., Sayama, N.,... & Abe, K. (1997). The development of transient hypothyroidism after iodine-131 treatment in hyperthyroid patients with Graves' disease: prevalence, mechanism and prognosis. Clinical Endocrinology, 46(1), 1-5.
- Chakrabarti, S. K., Ghosh, S., Banerjee, S., Mukherjee, S., & Chowdhury, S. (2016). Oxidative stress in hypothyroid patients and the role of antioxidant supplementation. Indian Journal of Endocrinology and Metabolism, 20(5), 674-678.
- Tallstedt, L. , Lundell, G., Blomgren, H., & Bring, J. (1994). Does early administration of thyroxine reduce the development of Graves' ophthalmopathy after radioiodine treatment? European Journal of Endocrinology, 130(5), 494-497.
Figure 2.
Drug-mediated changes in TH and TSH levels.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



