
Submitted:
29 April 2024
Posted:
01 May 2024
You are already at the latest version
Abstract
Degenerative disc disease (DDD) is a pervasive condition that limits quality of life and burdens economies. Traditional pharmacological treatments aimed at slowing degeneration are ineffective in the long-term. Orthobiologics, regenerative agents derived from the patient’s own tissue, are a promising emerging therapy for degenerative disc disease. This review first outlines the pathophysiology of degenerative disc disease, highlighting the limitations of existing treatments and explores the orthobiologic tools for treating degenerative disc disease (platelet-rich plasma, mesenchymal stem cells). Their history in regenerative medicine is outlined, demonstrating how in vitro evidence informed preclinical animal studies on their efficacy in treating degenerative disc disease. Finally, clinical trials utilizing these treatment options are reviewed and directions for future research are outlined. Although the current clinical evidence available is limited to propagate their routine clinical usage the field holds immense potential in the management of DDD. There is room for these treatments to be optimized for effective consistent clinical outcomes in DDD.
Keywords:
disc disease
; orthobiologics
; inflammation
; orthopedics
; regenerative medicine
1. Introduction
Degenerative disc diseases (DDDs) encompass a wide and heterogeneous set of health conditions which can affect all musculoskeletal and nervous tissues along the spine [1]. DDDs are frequently associated with pain syndromes, radiculopathy, spondylosis, spondylolisthesis, stenosis, fractures, tumors, and osteoporosis [1]. DDD is linked to significant pain and disability, generating major socioeconomic given its high global prevalence [2]. Patients often present pseudoradicular pain, mostly due to degenerative processes involving intervertebral discs (IVDs), facet joints and soft tissues [3]. Pseudoradicular pain can also have less common causes such as infections, non-infectious inflammation, metabolic syndrome and tumors [3]. The most obvious and common cause of radicular pain is likely compression of the nerve roots which can arise from numerous intrinsic and extrinsic factors as well. This type of pain can also be accompanied by degenerative processes, infections, and secondary problems including other diseases and injuries involving anatomical sites along the spine [4].
Many conventional management strategies have been studied and proposed for DDDs. For instance, physical therapy and non-steroidal anti-inflammatory drugs (NSAIDs) are common conservative treatments [5]. However, it must be emphasized that although NSAIDs and corticosteroids can effectively target pain, chronic use of these medications risks complications such as peptic ulcer disease, acute renal failure, and stroke/myocardial infarction [6,7]. In more severe injuries such as lumbar disc herniation, for example, these conventional management strategies may not suffice, ultimately forcing the patient to seek alleviation from orthopedic surgeons. Similarly, other alternatives such as intradiscal electrothermal treatments are not always effective. Arthrodesis is often recommended for discogenic back pain but there is still some controversy in the literature [5].
Given the shortcomings of traditional therapies, the demand for novel solutions for DDD has motivated the medical community to contribute to the expansion of medical biotechnology. Continuous research has promoted significant growth in the regenerative medicine market with the emergence of orthobiologics; derivates of endogenous molecules, cells or tissues applied to injured tissue to prompt regeneration [8]. Some of the most popular contemporary orthobiologic alternatives commercially available are autologous solutions such as platelet-rich plasma (PRP), bone marrow-derived products and adipose tissue derivatives [8]. These materials trigger a wide set of biological responses that contribute to the amelioration of regeneration in areas where standard tissue healing is disrupted or difficult to achieve [9]. Although the biological mechanisms are complex, the aforementioned products share many similarities, especially in virtue of autocrine and paracrine signaling via release of several bioactive molecules [8,9,10,11].
DDDs are challenging and often present a multifactorial nature; therefore, physicians must be able to thoroughly evaluate the patient to correctly identify the root source of the problem. Physical examination and medical imaging methods are indispensable in order to avoid misdiagnosis. Delays between initial symptoms, correct diagnosis and onset of treatment is also another important factor that must be avoided in order to achieve successful clinical outcomes [4].
The objective of this manuscript is to explain DDD pathophysiology and review the potential of the orthobiologics platelet-rich plasma, mesenchymal stem cells and an orthobiologic adjunct material (hyaluronic acid) in the treatment of this spinal condition according to what has been documented in the literature.
2. Etiopathogenesis
The degenerative alterations and abnormalities that affect the spine involve bony structures and the IVD. In addition to age-related changes, these alterations may also be linked to traumatic, metabolic, toxic, vascular, infectious and genetic factors [12,13]. However, there is also a significant incidence of chronic overload and sequelae of acute traumatic spine injuries [12]. Abnormal physical stress, even if not sufficient to cause fracture, can still harm bone and disc if maintained for a large amount of time [12]. At the cervical level, the distribution of axial load is normally responsible for degenerative alterations of C5-6 and C6-7 vertebrae in most cases; in the lumbosacral tract the most frequently affected sites are L4-5 and L5-S1 since these levels suffer the highest dynamic and static loads [14].
The IVD structurally consists of a fibrocartilaginous annulus fibrosus (AF) encasing a gel-like matrix termed the nucleus pulposus (NP). The NP matrix is maintained through proteoglycan and type II collagen synthesis by NP cells (NPCs). The interaction between these two extracellular matrix components imbues the NP matrix with hydroscopic properties which is crucial for IVDs to be able to absorb compressive shocks during movement [15]. Any damage to the endplates due to these cyclic compressive loads marks the beginning of the cascade of degenerative disc disease as shown in Figure 1.
However, these same cells also produce matrix metalloproteinases which degrade the NP ECM. The presence of anabolic signals such as IGF-1, TGF and bFGF promotes ECM deposition [16], whereas various inflammatory cytokines (typically secreted following tissue injury promote ECM degradation [8,9,17,18,19,20]. Therefore, if the cellular microenvironment shifts IVD cells to a catabolic state, degradation of the NP matrix will begin [21].
2.1. Age
Aging gradually increases the production of collagen, favoring collagen I production over collagen II production, which makes the IVD gradually more fibrous [22]. The anatomical demarcation between the nucleus pulposus and the annulus fibrosus becomes significantly diminished as these two regions merge [13]. The increase in collagen and collagen-proteoglycan binding reduces the availability of proteoglycan polar groups and therefore their capability to bind to water [23]. Consequently, desiccation renders the nucleus pulposus more solid and granular, increasing the risk of cracks and injuries not only to itself but to adjacent structures as well [22]. Senescence of IVD cells also has a fair share of culpability in these pathological developments as it significantly reduces their ability to proliferate [24]. Additionally, senescent cells also contribute to degenerative progression by means of decreased anabolism and/or increased catabolic activity, reducing the tissue’s ability to compensate for net loss [24,25].
2.2. Genetics
Certain genetic factors are also partially responsible for DDDs in some cases, even more so in comparison to environmental factors. For instance, polymorphisms in the promoter region of the MMP-3 gene can accelerate degenerative alterations in the lumbar tract in elderly populations [26]. Similarly, patients with Trp2 and Trp3 variants in type IX collagen are also more susceptible to lumbar disorders because this mutation generates an unstable triple helix that is less resistant to mechanical stress [27]. Interestingly, variations in pro-inflammatory mediator genes are also at play in DDDs. A study shows that IL-1αT889 and IL-1βT3954, pathological alleles of the interleukin-1 gene, have been associated with disc bulging [28].
2.3. Nutrition
IVD cells obtain their nutrients from blood vessels in the peripheral soft tissue structures, relying on nutrient diffusion from capillaries across the cartilaginous endplate and disc matrix to the cells [29]. Insufficient or disrupted blood supply to these structures could be the main causative factor underpinning pathological progression [30]. Reduced delivery of nutrients leads to cell death and, ultimately, increases in oxidative stress markers [29,30]. Low oxygen levels and the acidic pH resulting from anaerobic metabolism impair the synthesis of proteoglycans and other proteins [29]. Furthermore, poor metabolic health also plays a significant role in cell nutrition, as is the case with that metabolic syndrome, which is known to disrupt standard cell activity [31].
2.4. Mechanobiology
Mechanical overload is frequently associated with spine conditions, especially when it comes to disorders affecting the lumbar discs [32]. The discs are structures designed to sustain and disperse mechanical forces. In fact, loading is a key component in human biology as physical stimuli trigger many developmental processes including the regulation of matrix turnover [33]. Conversely, excessive loading harms these structures not only via physical damage but also by reducing gene expression of anabolic proteins, favoring a catabolic shift and inflammation [34].
Sudden and severe compressive forces can lead to fractures of the vertebral endplate, causing multiple problems. Although callus formation is a natural healing response, it can occlude blood vessels in the endplate and block the delivery of nutrients and oxygen for cells, disrupting the maintenance of extracellular matrix [35]. Over time, damage to the endplate gradually leads to depressurization of the nucleus pulposus, applying more stress to the annulus fibrosus [36]. Consequently, this structure is no longer braced by the nucleus pulposus, generating greater interlaminar shear stress, delamination and, ultimately, tearing of the annulus fibrosus [36]. The resulting bone marrow lesions are dense with newly formed nerve endings which are exposed to the inflammatory microenvironment and inadequately braced compressive forces (Figure 1). These newly-proliferated nerves are thought to be a major source of pain [37]. Destruction of cartilage from an endplate fracture, in turn, triggers an inflammatory response mediated by IL-1β, with the subsequent production of catabolic enzymes that attack matrix proteins [38]. Lastly, the matrix becomes vulnerable not only to unfavorable pH but to blood in the vertebral bodies as well, increasing the risk of an equivocal immunogenic response [39,40].
3. Orthobiologic Solutions
3.1. Platelet-Rich Plasma
Platelet-rich plasma is an orthobiologic derived from the patient’s own blood and has been researched in clinical settings for nearly 40 years [41]. Its preparation methods are diverse, however all aim to concentrate the platelet count within the patient’s plasma sample before delivering it to the site of desired tissue regeneration [42]. Given the role of platelets in secreting growth factors and promoting regeneration of damaged tissue, PRP has many predicted functions at the degenerating disc. Additionally, PRP’s orthobiologic nature ensures that it will be non-immunogenic and carry no risk of disease transmission in comparison to xenobiologic or allobiologic treatments [43]. Given its long history and relatively non-invasive preparation protocol in comparison to bone marrow aspirates, an array of preclinical and clinical research has examined the effectiveness of PRP in treating DDD.
PRP application to cultured cells of the intervertebral disc, including NPCs and annular fibrosis cells (AFCs), has been investigated to provide preclinical evidence for its efficacy in treating DDD. Cultured NPCs from porcine and rabbit NPCs treated with PRP resulted in an increase in cell proliferation, proteoglycan synthesis [44] and increased transcription of extracellular matrix genes [45] respectively. In a model of immortalized human NPCs, LPS-induced inflammation was reversed by PRP administration [46]. These results mirror the anti-inflammatory effects seen from PRP administration to cultured human NPCs following IL-1β and TNF-α-induced inflammation.
The influence of PRP on NPC proliferation and differentiation is unclear. In one study, human NPCs derived from healthy donors and cultured with PRP display increased proliferation and the expression of chondrogenic genes [47]. This study also demonstrated a synergistic effect between PRP and 1 ng/mL of TGF-1β [47]. The findings of Mietsch et al. (2013) instead find that TGF-1β alone induces chondrogenesis on human NPCs more strongly than PRP. Mietsch and colleagues (2013) ultimately suggest that this discrepancy is due to other differences present within the cell media. While both studies demonstrated an induction of anabolism by PRP, other environmental variables likely determined whether this anabolic programming resulted in the mutually exclusive processes of cellular differentiation (i.e., chondrogenesis) or proliferation [49].
PRP administration to cultured AFCs has also been examined. Pirvu et al. (2014) reported an increase in ECM synthesis and cellular proliferation following PRP administration to bovine AFCs. Complementary results were also generated in Hondke and colleagues’ (2020) study of cultured human AFCs. Specifically, they found that PRP increased cell proliferation and ECM synthesis in AFCs. Lastly, when porcine AFCs also increase their cellular proliferation and ECM synthesis in response to PRP exposure [44]. Taken together, these studies demonstrate that PRP plasma also promotes anabolism in AFCs in vitro. In summary, PRP administration shifts cultured NPCs and AFCs to an anabolic, anti-inflammatory state ideal for regenerating the cellular and extracellular environment of the degenerating intervertebral disc.
Given these promising in vitro findings, it is not surprising that many studies have progressed to assessing the efficacy of PRP in reversing DDD using preclinical animal models. The first of such studies was performed by Nagae and colleagues (2007) on nucleotomised rabbits. PRP treatment alone demonstrated no difference to control groups, however, when combined with a hydrogel scaffold, PRP treatment increased proteoglycan presence at the AF and halted further disc degeneration [52]. Using the same treatment combinations on a larger sample of nucleotomised rabbits revealed similar findings; only combined PRP impregnated into gelatin hydrogel microspheres increased proteoglycan gene transcript and decreased apoptosis [53]. These early experiments supported the notion that PRP administration needed to be appropriately scaffolded to allow for its facilitation of regeneration to occur in situ.
In contrast, a study examining the anatomical integrity of needle-punctured rat IVDs showed that PRP injection alone protected from further anatomical degradation, an effect that was amplified the earlier the PRP was supplied post-injury [54]. Additionally, Pirvu et al. (2014) also examined PRP injection in three bovine IVDs with an AF defect. Following PRP injection, matrix synthesis increased at the defect site, however this study lacked statistical power to detect significant differences between treatment groups.
These contrasting results again point to the synergistic nature of PRP treatment when combined with other agents. For example, Wang and colleagues’ analysis of treatments for needle-punctured rabbit IVDs showed only minor structural regeneration in PRP-treated groups, however groups treated with combined PRP and bone marrow-derived mesenchymal stem cells had far superior disc regeneration when assessed histologically and by MRI [55]. In summary, PRP is an effective orthobiologic agent that reprograms degenerating IVD cells to an anabolic, anti-inflammatory state. Its effectiveness is also increased when paired with an appropriate scaffold or additional orthobiologic agent. A number of clinical trials (Table 1) have therefore examined lone PRP, or PRP combinations as a treatment for human DDD.
3.2. Mesenchymal Stem Cells
The previous interventions discussed rely on shifting pre-existing IVD cells into an anabolic state to facilitate disc regeneration. However, multipotent stem cells can also be delivered to the site of degeneration with the hope that they will differentiate and replenish the intervertebral disc population. The potential of MSCs as a DDD therapeutic was first demonstrated in in vitro experiments. MSCs, when co-cultured with NPCs extracted from degenerating discs, promotes MSC differentiation into chondrogenic cells with NPC phenotypes, whilst also promoting ECM production [80,81]. MSCs also initiate anti-inflammatory, anti-apoptotic cues within the IVD microenvironment (reviewed by Esquijarosa Hechavarria & Richard, 2022).
In addition to their regenerative potential (Figure 2), another therapeutic advantage of MSCs is the relative ease with which autologous MSCs can be sourced. Harvesting autologous IVD cells directly has limited therapeutic potential [83] and potentially further damages the vertebral column. In contrast, autologous or allogenic MSCs can be sourced from a variety of non-vertebral tissues, including bone marrow [8], adipose tissue and umbilical cord blood [84,85].
ECM Extracellular Matrix, IVD Intervertebral Disc
MSCs regenerated damaged IVDs through three mechanisms. Firstly, MSCs may directly differentiate into IVD cells, including AFCs [86] and NPCs [87], thus replenishing the cellular population. MSCs also alter the cellular microenvironment of existing IVD cells. Paracrine signaling following the release of growth factors and ECM components can shift IVD cells to an anabolic state [88]. Lastly, MSCs may also release immunomodulatory mediators to blunt destructive immune responses to the compromised IVD microenvironment [89].
While MSCs are highly effective in vitro, their ability to survive in situ is limited. The hypoxic, acidic environment of the degenerating disc [29] is often fatal for implanted MSCs [90,91]. Therefore, emerging research has examined strategies to differentiate MSCs prior to their implantation. For example, preconditioning MSCs with a hypoxic culture environment promotes their expression of NPC phenotypes [87,92]. Alternatively, hydrogels, including those composed of hyaluronic acid, can alter the cellular environment of MSCs, prompting their differentiation into NPCs [93,94]. There are a plethora of additional pre-conditioning strategies for MSCs which are currently being examined for their effectiveness in DDD; a comprehensive review of all of these strategies has been recently published by Ohnishi et al. (2023). MSCs therefore represent a diverse variety of orthobiologic treatments for DDD.
3.3. Adjunct Materials - Hyaluronic Acid
Importantly, the efficacy of orthobiologics is heavily influenced by adjunct materials that accompany their injection at the degenerating disc. This section will illustrate thew importance of adjunct materials by reviewing the use of hyaluronic acid (HA) in DDD. HA is an unsulfated glycosaminoglycan constituting a major component of the extracellular matrix [96]. Its hydroscopic properties, like other glycosaminoglycans, allow it to facilitate shock absorption within the intervertebral discs. Additionally, large HA fragments also function to inhibit neighboring extracellular receptors that induce inflammatory or nociceptive cascades [97]. Lastly, hydrogels have been widely developed from HA scaffolds, allowing for more customisable mechanical properties. Often, these HA hydrogels can be used as a vehicle to deliver other orthobiologic agents to the joint site [98]. HA is therefore a promising regenerative material for the treatment of degenerative disc disease.
In vitro studies have shown that HA has significant influence over cultured NPC function. Firstly, Alini et al. demonstrated that a matrix of type I collagen and HA supplied stimulated the production of proteoglycans in both NPCs and AFCs. When HA is administered to cultured NPCs derived from human degenerating discs it stimulates mitophagy which has downstream protective effects against apoptosis and degradation of the ECM [99]. Similar ECM-protective effects of HA were demonstrated in a separate study examining the application of a HA hydrogel with fibroblast growth factor in both human and bovine NPCs [100]. Importantly, these regenerative effects are concentration dependent in a non-linear manner; Gansau and Buckley [101] found that very high concentrations of HA would suppress rather than enhance collagen production in bovine chondrocytes Isa et al. [102] stimulated cultured bovine NPCs with IL-1β to model the inflammatory conditions of disc degeneration. Cells that were supplied with a HA hydrogel again downregulated their expression of pro-inflammatory signals whilst also downregulating the production of neurotrophins, potentially providing a molecular basis for the analgesic function of HA.
HA has also been tested in many preclinical models of degenerative disc disease. Firstly, Isa et al. [103] expanded on their previous in vitro findings and demonstrated that HA alleviates pain in a rat model of disc degeneration. These behavioural findings were supported by a concurrent decrease in cFOS expression in the left dorsal horn of the spinal cord of HA-treated rats. Finally, a comparative proteomic analysis mirrored in vitro findings, demonstrated an anti-inflammatory shift in protein expression induced by HA exposure. The hydroscopic properties of HA hydrogels also demonstrated regeneration potential in a rabbit model of disc degermation; intrarticular injection with a HA hydrogel increased disc height and water absorption and overall decreased the severity of degermation as scored through MRI [104]. Similar findings were observed using a different HA hydrogel to treat a murine model of DDD [93] Interestingly, a similar in vivo study on the goat degenerating disc demonstrated no advantage to injecting BMP-2/7 through a HA hydrogel when compared to BMP-2/7 injection alone [105]. In a study of explanted injured murine discs, HA hydrogels decreased the expression of IGFBP3, IFNa and caspase 3, whilst upregulating the key ECM components HAPLN1 and aggrecan [106].
To summarise, hyaluronic acid could acts as a key delivery vehicle for orthobiologics in the treatment of degenerative disc disease. Its FDA approval for the treatment of knee osteoarthritis [107] has led to extensive investigations of its efficacy in other joints, including the intervertebral discs. In vitro research on NPCs and explanted disc tissue consistently demonstrates HA’s potential to attenuate inflammation, regenerate the ECM and reduce pain reception. Preclinical animal models utilizing HA hydrogels are also effective in regenerating the degenerating disc, however the specific contribution of HA to this regeneration is hard to characterize given that it is often used in combination with other growth factors or other orthobiologics. All studies however demonstrated an excellent safety profile for intradiscal HA injection.
4. Clinical Evidence
Published scholarly literature, as well as clinical trial repositories (ClinicalTrials.gov and EudraCT) were searched to identify completed clinical trials evaluating the use of the preceding orthobiologic tools in the treatment of DDD. The results of the 19 clinical trials analysed are briefly summarized in Table 1. For an overview of ongoing clinical trials on cell-based therapies for DDD, refer to the review by Binch et al. [108], and Table 2.
5. Future Directions
Overall, current clinical data suggests that orthobiologic treatments, such as intradiscal PRP, HA or MSC injection, have the potential to outperform conventional therapies. All studies demonstrated a sustained reduction in reported pain. Given that a majority of these studies only included patients who did not respond to conventional DDD therapies, these results are even more promising. However, as others have concluded [109], the current clinical data cannot be used to recommend orthobiologic treatment for DDD without further research.
Firstly, most of these clinical studies are prospective in nature and lack control groups. These controls are important, as illustrated by Zielinski et al.’s (2022) study which found that most patients receiving PRP injection reported a decrease in pain at follow-up, but that this pain reduction was not significantly different than patients in the control group who received a sham injection. Additionally, the sample sizes of these trials are often very low which limits the statistical power of this research. Lastly, very few studies [67] make direct comparisons between orthobiologic treatments, which means that clinicians cannot currently discern which orthobiologic treatment is best suited for their patient/s. Future research should not be aimed at demonstrating the potential of orthobiologics in DDD, but rather aimed at demonstrating which combination of orthobiologics and treatment methods produce the most favourable outcomes.
The sheer number of potential therapeutic strategies, combining cellular therapies with scaffolds, makes this a daunting task [110]. This is further exacerbated by the long-standing inconsistencies present in preclinical animal models of DDD and orthobiologic treatments [108,111,112]. In order to navigate these issues, in vitro studies should first be performed to compare and assay confounding variables (e.g., stem-cell type, culturing conditions, presence or absence of growth factors). Then, culturing conditions which yield the most regenerative phenotype can be used to plan preclinical animal experiments. In doing so, clinical trials can be reserved for pre-optimised orthobiologic therapies.
Author Contributions
CO: GS and JR wrote the manuscript; BO and BR proposed the research subtopics; RT and IR were responsible for navigating the literature and sharing the relevant studies that were included in this review; DJ formatted the citations and compiled the references; AN revised and formatted the body of the manuscript verifying spelling, punctuation and grammatical errors; MJ and PE created figures and tables. As the supervisor, JL was responsible for reviewing and approving all the modifications made to the manuscript, from draft to final version.
Funding
This research received no external funding.
Data Availability Statement
The authors have no acknowledgements to declare.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Alshami, A.M. Prevalence of Spinal Disorders and Their Relationships with Age and Gender. SMJ 2015, 36, 725–730. [Google Scholar] [CrossRef]
- Coenen, P.; Smith, A.; Paananen, M.; O’Sullivan, P.; Beales, D.; Straker, L. Trajectories of Low Back Pain From Adolescence to Young Adulthood: LBP Trajectories in Early Life. Arthritis Care & Research 2017, 69, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Van Boxem, K.; Van Zundert, J.; Patijn, J.; van Kleef, M. Pseudoradicular and Radicular Low-Back Pain: How to Diagnose Clinically? Pain 2008, 135, 311–312. [Google Scholar] [CrossRef]
- Raciborski, F.; Gasik, R.; Kłak, A. Disorders of the Spine. A Major Health and Social Problem. Reumatologia 2016, 54, 196–200. [Google Scholar] [CrossRef]
- Madigan, L.; Vaccaro, A.R.; Spector, L.R.; Milam, R.A. Management of Symptomatic Lumbar Degenerative Disk Disease. J Am Acad Orthop Surg 2009, 17, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Marcum, Z.A.; Hanlon, J.T. Recognizing the Risks of Chronic Nonsteroidal Anti-Inflammatory Drug Use in Older Adults. Annals of Long-Term Care.
- Setti, T.; Arab, M.G.L.; Santos, G.S.; Alkass, N.; Andrade, M.A.P.; Lana, J.F.S.D. The Protective Role of Glutathione in Osteoarthritis. Journal of Clinical Orthopaedics and Trauma 2020. [Google Scholar] [CrossRef] [PubMed]
- Lana, J.F.; da Fonseca, L.F.; Azzini, G.; Santos, G.; Braga, M.; Cardoso Junior, A.M.; Murrell, W.D.; Gobbi, A.; Purita, J.; de Andrade, M.A.P. Bone Marrow Aspirate Matrix: A Convenient Ally in Regenerative Medicine. International Journal of Molecular Sciences 2021. [Google Scholar] [CrossRef] [PubMed]
- Ramires, L.C.; Jeyaraman, M.; Muthu, S.; Shankar A, N.; Santos, G.S.; da Fonseca, L.F.; Lana, J.F.; Rajendran, R.L.; Gangadaran, P.; Jogalekar, M.P.; et al. Application of Orthobiologics in Achilles Tendinopathy: A Review. Life 2022, 12, 399. [Google Scholar] [CrossRef]
- Caplan, A.I.; Dennis, J.E. Mesenchymal Stem Cells as Trophic Mediators. Journal of Cellular Biochemistry 2006, 98, 1076–1084. [Google Scholar] [CrossRef]
- Squillaro, T.; Peluso, G.; Galderisi, U. Clinical Trials With Mesenchymal Stem Cells: An Update. Cell Transplant 2016, 25, 829–848. [Google Scholar] [CrossRef]
- Gallucci, M.; Limbucci, N.; Paonessa, A.; Splendiani, A. Degenerative Disease of the Spine. Neuroimaging Clin N Am 2007, 17, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Hadjipavlou, A.G.; Tzermiadianos, M.N.; Bogduk, N.; Zindrick, M.R. The Pathophysiology of Disc Degeneration. The Journal of Bone and Joint Surgery. British volume, 1261. [Google Scholar] [CrossRef]
- Gallucci, M.; Puglielli, E.; Splendiani, A.; Pistoia, F.; Spacca, G. Degenerative Disorders of the Spine. Eur Radiol 2005, 15, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.R.; Matsui, Y.; Wu, J.-J. Collagen Polymorphisms of the Intervertebral Disc. Biochemical Society Transactions 2002, 30, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Seki, S.; Kawaguchi, Y.; Chiba, K.; Mikami, Y.; Kizawa, H.; Oya, T.; Mio, F.; Mori, M.; Miyamoto, Y.; Masuda, I.; et al. A Functional SNP in CILP, Encoding Cartilage Intermediate Layer Protein, Is Associated with Susceptibility to Lumbar Disc Disease. Nat Genet 2005, 37, 607–612. [Google Scholar] [CrossRef]
- Lana, J.F.; Macedo, A.; Ingrao, I.L.G.; Huber, S.C.; Santos, G.S.; Santana, M.H.A. Leukocyte-Rich PRP for Knee Osteoarthritis: Current Concepts. Journal of Clinical Orthopaedics and Trauma 2019. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.J.; Ferreira, J.R.; Cunha, C.; Corte-Real, J.V.; Bessa-Gonçalves, M.; Barbosa, M.A.; Santos, S.G.; Gonçalves, R.M. Macrophages Down-Regulate Gene Expression of Intervertebral Disc Degenerative Markers Under a Pro-Inflammatory Microenvironment. Front Immunol 2019, 10, 1508. [Google Scholar] [CrossRef]
- Zhu, P.; Li, J.; Fujino, M.; Zhuang, J.; Li, X.-K. Development and Treatments of Inflammatory Cells and Cytokines in Spinal Cord Ischemia-Reperfusion Injury. Mediators Inflamm 2013, 2013, 701970. [Google Scholar] [CrossRef]
- Hellenbrand, D.J.; Quinn, C.M.; Piper, Z.J.; Morehouse, C.N.; Fixel, J.A.; Hanna, A.S. Inflammation after Spinal Cord Injury: A Review of the Critical Timeline of Signaling Cues and Cellular Infiltration. Journal of Neuroinflammation 2021, 18, 284. [Google Scholar] [CrossRef]
- Tokuhara, C.K.; Santesso, M.R.; Oliveira, G.S.N. de; Ventura, T.M. da S.; Doyama, J.T.; Zambuzzi, W.F.; Oliveira, R.C. de Updating the Role of Matrix Metalloproteinases in Mineralized Tissue and Related Diseases. J Appl Oral Sci 2019, 27, e20180596. [Google Scholar] [CrossRef]
- Haefeli, M.; Kalberer, F.; Saegesser, D.; Nerlich, A.G.; Boos, N.; Paesold, G. The Course of Macroscopic Degeneration in the Human Lumbar Intervertebral Disc. Spine 2006, 31, 1522–1531. [Google Scholar] [CrossRef]
- Iozzo, R.V.; Schaefer, L. Proteoglycan Form and Function: A Comprehensive Nomenclature of Proteoglycans. Matrix Biol 2015, 42, 11–55. [Google Scholar] [CrossRef]
- Roberts, S.; Evans, E.H.; Kletsas, D.; Jaffray, D.C.; Eisenstein, S.M. Senescence in Human Intervertebral Discs. Eur Spine J 2006, 15, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Gruber, H.E.; Ingram, J.A.; Norton, H.J.; Hanley, E.N.J. Senescence in Cells of the Aging and Degenerating Intervertebral Disc: Immunolocalization of Senescence-Associated β-Galactosidase in Human and Sand Rat Discs. Spine 2007, 32, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Haro, H.; Wakabayashi, Y.; Kawa-uchi, T.; Komori, H.; Shinomiya, K. The Association of Degeneration of the Intervertebral Disc with 5a/6a Polymorphism in the Promoter of the Human Matrix Metalloproteinase-3 Gene. The Journal of Bone and Joint Surgery. British volume. [CrossRef]
- Persikov, A.V.; Ramshaw, J.A.M.; Brodsky, B. Collagen Model Peptides: Sequence Dependence of Triple-Helix Stability. Biopolymers 2000, 55, 436–450. [Google Scholar] [CrossRef]
- Solovieva, S.; Kouhia, S.; Leino-Arjas, P.; Ala-Kokko, L.; Luoma, K.; Raininko, R.; Saarela, J.; Riihimäki, H. Interleukin 1 Polymorphisms and Intervertebral Disc Degeneration. Epidemiology 2004, 15, 626–633. [Google Scholar] [CrossRef]
- De Geer, C.M. Intervertebral Disk Nutrients and Transport Mechanisms in Relation to Disk Degeneration: A Narrative Literature Review. J Chiropr Med 2018, 17, 97–105. [Google Scholar] [CrossRef]
- Grunhagen, T.; Wilde, G.; Soukane, D.M.; Shirazi-Adl, S.A.; Urban, J.P.G. Nutrient Supply and Intervertebral Disc Metabolism. J Bone Joint Surg Am 2006, 88 Suppl 2, 30–35. [Google Scholar] [CrossRef]
- Azzini, G.O.M.; Santos, G.S.; Visoni, S.B.C.; Azzini, V.O.M.; Santos, R.G. dos; Huber, S.C.; Lana, J.F. Metabolic Syndrome and Subchondral Bone Alterations: The Rise of Osteoarthritis – A Review. Journal of Clinical Orthopaedics and Trauma 2020. [Google Scholar] [CrossRef] [PubMed]
- Stokes, I.A.F.; Iatridis, J.C. Mechanical Conditions That Accelerate Intervertebral Disc Degeneration: Overload Versus Immobilization. Spine (Phila Pa 1976) 2004, 29, 2724–2732. [Google Scholar] [CrossRef]
- Chan, S.C.W.; Ferguson, S.J.; Gantenbein-Ritter, B. The Effects of Dynamic Loading on the Intervertebral Disc. Eur Spine J 2011, 20, 1796–1812. [Google Scholar] [CrossRef] [PubMed]
- Neidlinger-Wilke, C.; Würtz, K.; Urban, J.P.G.; Börm, W.; Arand, M.; Ignatius, A.; Wilke, H.-J.; Claes, L.E. Regulation of Gene Expression in Intervertebral Disc Cells by Low and High Hydrostatic Pressure. Eur Spine J 2006, 15, 372–378. [Google Scholar] [CrossRef]
- Benneker, L.M.; Heini, P.F.; Alini, M.; Anderson, S.E.; Ito, K. 2004 Young Investigator Award Winner: Vertebral Endplate Marrow Contact Channel Occlusions and Intervertebral Disc Degeneration. Spine 2005, 30, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Rade, M.; Määttä, J.H.; Freidin, M.B.; Airaksinen, O.; Karppinen, J.; Williams, F.M. Vertebral Endplate Defect as Initiating Factor in Intervertebral Disc Degeneration; Strong Association between Endplate Defect and Disc Degeneration in the General Population. Spine (Phila Pa 1976) 2018, 43, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Lotz, J.C.; Fields, A.J.; Liebenberg, E.C. The Role of the Vertebral End Plate in Low Back Pain. Global Spine J 2013, 3, 153–164. [Google Scholar] [CrossRef]
- Tang, P.; Zhu, R.; Ji, W.-P.; Wang, J.-Y.; Chen, S.; Fan, S.-W.; Hu, Z.-J. The NLRP3/Caspase-1/Interleukin-1β Axis Is Active in Human Lumbar Cartilaginous Endplate Degeneration. Clin Orthop Relat Res 2016, 474, 1818–1826. [Google Scholar] [CrossRef]
- Marjoram, T. The Endplate and Trabecular Bone in Lumbar Degenerative Disc Disease: A Narrative Review. SN Compr. Clin. Med. 2020, 2, 332–337. [Google Scholar] [CrossRef]
- Fields, A.J.; Ballatori, A.; Liebenberg, E.C.; Lotz, J.C. Contribution of the Endplates to Disc Degeneration. Curr Mol Biol Rep 2018, 4, 151–160. [Google Scholar] [CrossRef]
- Ferrari, M.; Zia, S.; Valbonesi, M.; Henriquet, F.; Venere, G.; Spagnolo, S.; Grasso, M.A.; Panzani, I. A New Technique for Hemodilution, Preparation of Autologous Platelet-Rich Plasma and Intraoperative Blood Salvage in Cardiac Surgery. Int J Artif Organs 1987, 10, 47–50. [Google Scholar] [CrossRef]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Stojanovic, P. Platelet Rich Plasma: A Short Overview of Certain Bioactive Components. Open Med (Wars) 2016, 11, 242–247. [Google Scholar] [CrossRef]
- Dos Santos, R.G.; Santos, G.S.; Alkass, N.; Chiesa, T.L.; Azzini, G.O.; da Fonseca, L.F.; Dos Santos, A.F.; Rodrigues, B.L.; Mosaner, T.; Lana, J.F. The Regenerative Mechanisms of Platelet-Rich Plasma: A Review. Cytokine 2021, 144, 155560. [Google Scholar] [CrossRef]
- Akeda, K.; An, H.S.; Okuma, M.; Attawia, M.; Miyamoto, K.; Thonar, E.J.-M.A.; Lenz, M.E.; Sah, R.L.; Masuda, K. Platelet-Rich Plasma Stimulates Porcine Articular Chondrocyte Proliferation and Matrix Biosynthesis. Osteoarthritis Cartilage 2006, 14, 1272–1280. [Google Scholar] [CrossRef]
- Yang, H.; Yuan, C.; Wu, C.; Qian, J.; Shi, Q.; Li, X.; Zhu, X.; Zou, J. The Role of TGF-Β1/Smad2/3 Pathway in Platelet-Rich Plasma in Retarding Intervertebral Disc Degeneration. J Cell Mol Med 2016, 20, 1542–1549. [Google Scholar] [CrossRef]
- Liu, M.-C.; Chen, W.-H.; Wu, L.-C.; Hsu, W.-C.; Lo, W.-C.; Yeh, S.-D.; Wang, M.-F.; Zeng, R.; Deng, W.-P. Establishment of a Promising Human Nucleus Pulposus Cell Line for Intervertebral Disc Tissue Engineering. Tissue Eng Part C Methods 2014, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-H.; Lo, W.-C.; Lee, J.-J.; Su, C.-H.; Lin, C.-T.; Liu, H.-Y.; Lin, T.-W.; Lin, W.-C.; Huang, T.-Y.; Deng, W.-P. Tissue-Engineered Intervertebral Disc and Chondrogenesis Using Human Nucleus Pulposus Regulated through TGF-Β1 in Platelet-Rich Plasma. Journal of Cellular Physiology 2006, 209, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Mietsch, A.; Neidlinger-Wilke, C.; Schrezenmeier, H.; Mauer, U.M.; Friemert, B.; Wilke, H.-J.; Ignatius, A. Evaluation of Platelet-Rich Plasma and Hydrostatic Pressure Regarding Cell Differentiation in Nucleus Pulposus Tissue Engineering. Journal of Tissue Engineering and Regenerative Medicine 2013, 7, 244–252. [Google Scholar] [CrossRef]
- Drengk, A.; Zapf, A.; Stürmer, E.K.; Stürmer, K.M.; Frosch, K.-H. Influence of Platelet-Rich Plasma on Chondrogenic Differentiation and Proliferation of Chondrocytes and Mesenchymal Stem Cells. Cells Tissues Organs 2009, 189, 317–326. [Google Scholar] [CrossRef]
- Pirvu, T.N.; Schroeder, J.E.; Peroglio, M.; Verrier, S.; Kaplan, L.; Richards, R.G.; Alini, M.; Grad, S. Platelet-Rich Plasma Induces Annulus Fibrosus Cell Proliferation and Matrix Production. Eur Spine J 2014, 23, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Hondke, S.; Cabraja, M.; Krüger, J.P.; Stich, S.; Hartwig, T.; Sittinger, M.; Endres, M. Proliferation, Migration, and ECM Formation Potential of Human Annulus Fibrosus Cells Is Independent of Degeneration Status. Cartilage 2020, 11, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Nagae, M.; Ikeda, T.; Mikami, Y.; Hase, H.; Ozawa, H.; Matsuda, K.-I.; Sakamoto, H.; Tabata, Y.; Kawata, M.; Kubo, T. Intervertebral Disc Regeneration Using Platelet-Rich Plasma and Biodegradable Gelatin Hydrogel Microspheres. Tissue Eng 2007, 13, 147–158. [Google Scholar] [CrossRef]
- Sawamura, K.; Ikeda, T.; Nagae, M.; Okamoto, S.; Mikami, Y.; Hase, H.; Ikoma, K.; Yamada, T.; Sakamoto, H.; Matsuda, K.; et al. Characterization of in Vivo Effects of Platelet-Rich Plasma and Biodegradable Gelatin Hydrogel Microspheres on Degenerated Intervertebral Discs. Tissue Eng Part A 2009, 15, 3719–3727. [Google Scholar] [CrossRef]
- Gullung, G.B.; Woodall, J.W.; Tucci, M.A.; James, J.; Black, D.A.; McGuire, R.A. Platelet-Rich Plasma Effects on Degenerative Disc Disease: Analysis of Histology and Imaging in an Animal Model. Evid Based Spine Care J 2011, 2, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-Z.; JIN, J.-Y.; GUO, Y.-D.; MA, L.-Y.; CHANG, Q.; PENG, X.-G.; GUO, F.-F.; ZHANG, H.-X.; HU, X.-F.; WANG, C. Intervertebral Disc Regeneration Using Platelet-Rich Plasma-Containing Bone Marrow-Derived Mesenchymal Stem Cells: A Preliminary Investigation. Mol Med Rep 2016, 13, 3475–3481. [Google Scholar] [CrossRef]
- Noriega, D.C.; Ardura, F.; Hernández-Ramajo, R.; Martín-Ferrero, M.Á.; Sánchez-Lite, I.; Toribio, B.; Alberca, M.; García, V.; Moraleda, J.M.; Sánchez, A.; et al. Intervertebral Disc Repair by Allogeneic Mesenchymal Bone Marrow Cells: A Randomized Controlled Trial. Transplantation 2017, 101, 1945–1951. [Google Scholar] [CrossRef]
- Pettine, K.A.; Suzuki, R.K.; Sand, T.T.; Murphy, M.B. Autologous Bone Marrow Concentrate Intradiscal Injection for the Treatment of Degenerative Disc Disease with Three-Year Follow-Up. Int Orthop 2017, 41, 2097–2103. [Google Scholar] [CrossRef] [PubMed]
- Pettine, K.; Suzuki, R.; Sand, T.; Murphy, M. Treatment of Discogenic Back Pain with Autologous Bone Marrow Concentrate Injection with Minimum Two Year Follow-Up. Int Orthop 2016, 40, 135–140. [Google Scholar] [CrossRef]
- Pettine, K.A.; Murphy, M.B.; Suzuki, R.K.; Sand, T.T. Percutaneous Injection of Autologous Bone Marrow Concentrate Cells Significantly Reduces Lumbar Discogenic Pain through 12 Months. Stem Cells 2015, 33, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Orozco, L.; Soler, R.; Morera, C.; Alberca, M.; Sánchez, A.; García-Sancho, J. Intervertebral Disc Repair by Autologous Mesenchymal Bone Marrow Cells: A Pilot Study. Transplantation 2011, 92, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Haufe, S.M.W.; Mork, A.R. Intradiscal Injection of Hematopoietic Stem Cells in an Attempt to Rejuvenate the Intervertebral Discs. Stem Cells Dev 2006, 15, 136–137. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Ueda, Y.; Miyazaki, K.; Koizumi, M.; Takakura, Y. Disc Regeneration Therapy Using Marrow Mesenchymal Cell Transplantation: A Report of Two Case Studies. Spine 2010, 35, E475. [Google Scholar] [CrossRef]
- Elabd, C.; Centeno, C.J.; Schultz, J.R.; Lutz, G.; Ichim, T.; Silva, F.J. Intra-Discal Injection of Autologous, Hypoxic Cultured Bone Marrow-Derived Mesenchymal Stem Cells in Five Patients with Chronic Lower Back Pain: A Long-Term Safety and Feasibility Study. Journal of Translational Medicine 2016, 14, 253. [Google Scholar] [CrossRef]
- Centeno, C.; Markle, J.; Dodson, E.; Stemper, I.; Williams, C.J.; Hyzy, M.; Ichim, T.; Freeman, M. Treatment of Lumbar Degenerative Disc Disease-Associated Radicular Pain with Culture-Expanded Autologous Mesenchymal Stem Cells: A Pilot Study on Safety and Efficacy. J Transl Med 2017, 15, 197. [Google Scholar] [CrossRef]
- Blanco, J.F.; Villarón, E.M.; Pescador, D.; da Casa, C.; Gómez, V.; Redondo, A.M.; López-Villar, O.; López-Parra, M.; Muntión, S.; Sánchez-Guijo, F. Autologous Mesenchymal Stromal Cells Embedded in Tricalcium Phosphate for Posterolateral Spinal Fusion: Results of a Prospective Phase I/II Clinical Trial with Long-Term Follow-Up. Stem Cell Res Ther 2019, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Ruiz, V.; Blanco, J.F.; Villarón, E.M.; Fidalgo, H.; López-Parra, M.; Sánchez-Guijo, F. Autologous Mesenchymal Stem Cell Transplantation for Spinal Fusion: 10 Years Follow-up of a Phase I/II Clinical Trial. Stem Cell Research & Therapy 2023, 14, 78. [Google Scholar] [CrossRef]
- Navani, A.; Ambach, M.; Calodney, A.; Rosenthal, R.; Li, G.; Mahoney, C.B.; Everts, P.A. The Safety and Effectiveness of Orthobiologic Injections for Discogenic Chronic Low Back Pain: A Multicenter Prospective, Crossover, Randomized Controlled Trial with 12 Months Follow-Up. Pain Physician 2024, 27, E65–E77. [Google Scholar]
- Pang, X.; Yang, H.; Peng, B. Human Umbilical Cord Mesenchymal Stem Cell Transplantation for the Treatment of Chronic Discogenic Low Back Pain. Pain Physician 2014, 17, 525–530. [Google Scholar] [CrossRef]
- Comella, K.; Silbert, R.; Parlo, M. Effects of the Intradiscal Implantation of Stromal Vascular Fraction plus Platelet Rich Plasma in Patients with Degenerative Disc Disease. Journal of Translational Medicine 2017, 15, 12. [Google Scholar] [CrossRef]
- Kumar, H.; Ha, D.-H.; Lee, E.-J.; Park, J.H.; Shim, J.H.; Ahn, T.-K.; Kim, K.-T.; Ropper, A.E.; Sohn, S.; Kim, C.-H.; et al. Safety and Tolerability of Intradiscal Implantation of Combined Autologous Adipose-Derived Mesenchymal Stem Cells and Hyaluronic Acid in Patients with Chronic Discogenic Low Back Pain: 1-Year Follow-up of a Phase I Study. Stem Cell Res Ther 2017, 8, 262. [Google Scholar] [CrossRef]
- Tuakli-Wosornu, Y.A.; Terry, A.; Boachie-Adjei, K.; Harrison, J.R.; Gribbin, C.K.; LaSalle, E.E.; Nguyen, J.T.; Solomon, J.L.; Lutz, G.E. Lumbar Intradiskal Platelet-Rich Plasma (PRP) Injections: A Prospective, Double-Blind, Randomized Controlled Study. PM&R 2016, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Levi, D.; Horn, S.; Tyszko, S.; Levin, J.; Hecht-Leavitt, C.; Walko, E. Intradiscal Platelet-Rich Plasma Injection for Chronic Discogenic Low Back Pain: Preliminary Results from a Prospective Trial. Pain Medicine 2016, 17, 1010–1022. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, M.A.; Evans, N.E.; Bae, H.; Kamrava, E.; Calodney, A.; Remley, K.; Benyamin, R.; Franc, D.; Peterson, M.R.; Lovine, J.; et al. Safety and Efficacy of Platelet Rich Plasma for Treatment of Lumbar Discogenic Pain: A Prospective, Multicenter, Randomized, Double-Blind Study. Pain Physician 2022, 25, 29–34. [Google Scholar] [PubMed]
- Goyal, T.; Paswan, A.K.; Jain, D.; Verma, N.; Dubey, R.K. Comparative Evaluation of Efficacy of Percutaneous Intradiscal Radiofrequency Ablation and Platelet Rich Plasma Injection for Discogenic Low Back Pain: A Prospective Randomized Trial. J. Musculoskelet. Res. 2022, 25, 2250009. [Google Scholar] [CrossRef]
- Akeda, K.; Ohishi, K.; Takegami, N.; Sudo, T.; Yamada, J.; Fujiwara, T.; Niimi, R.; Matsumoto, T.; Nishimura, Y.; Ogura, T.; et al. Platelet-Rich Plasma Releasate versus Corticosteroid for the Treatment of Discogenic Low Back Pain: A Double-Blind Randomized Controlled Trial. Journal of Clinical Medicine 2022, 11, 304. [Google Scholar] [CrossRef] [PubMed]
- Akeda, K.; Fujiwara, T.; Takegami, N.; Yamada, J.; Sudo, A. Retrospective Analysis of Factors Associated with the Treatment Outcomes of Intradiscal Platelet-Rich Plasma-Releasate Injection Therapy for Patients with Discogenic Low Back Pain. Medicina 2023, 59, 640. [Google Scholar] [CrossRef] [PubMed]
- Bodor, M.; Toy, A.; Aufiero, D. Disc Regeneration with Platelets and Growth Factors. In Platelet-Rich Plasma: Regenerative Medicine: Sports Medicine, Orthopedic, and Recovery of Musculoskeletal Injuries; Lana, J.F.S.D., Andrade Santana, M.H., Dias Belangero, W., Malheiros Luzo, A.C., Eds.; Lecture Notes in Bioengineering; Springer: Berlin, Heidelberg, 2014; ISBN 978-3-642-40117-6. [Google Scholar]
- Navani, A.; Hames, A. Platelet-Rich Plasma Injections for Lumbar Discogenic Pain: A Preliminary Assessment of Structural and Functional Changes. Techniques in Regional Anesthesia and Pain Management 2015, 19, 38–44. [Google Scholar] [CrossRef]
- Akeda, K.; Ohishi, K.; Masuda, K.; Bae, W.C.; Takegami, N.; Yamada, J.; Nakamura, T.; Sakakibara, T.; Kasai, Y.; Sudo, A. Intradiscal Injection of Autologous Platelet-Rich Plasma Releasate to Treat Discogenic Low Back Pain: A Preliminary Clinical Trial. Asian Spine J 2017, 11, 380–389. [Google Scholar] [CrossRef]
- Strassburg, S.; Richardson, S.M.; Freemont, A.J.; Hoyland, J.A. Co-Culture Induces Mesenchymal Stem Cell Differentiation and Modulation of the Degenerate Human Nucleus Pulposus Cell Phenotype. Regenerative Medicine 2010, 5, 701–711. [Google Scholar] [CrossRef]
- Svanvik, T.; Barreto Henriksson, H.; Karlsson, C.; Hagman, M.; Lindahl, A.; Brisby, H. Human Disk Cells from Degenerated Disks and Mesenchymal Stem Cells in Co-Culture Result in Increased Matrix Production. Cells Tissues Organs 2009, 191, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Esquijarosa Hechavarria, M.; Richard, S.A. Edifying the Focal Factors Influencing Mesenchymal Stem Cells by the Microenvironment of Intervertebral Disc Degeneration in Low Back Pain. Pain Research and Management 2022, 2022, e6235400. [Google Scholar] [CrossRef]
- Mochida, J.; Sakai, D.; Nakamura, Y.; Watanabe, T.; Yamamoto, Y.; Kato, S. Intervertebral Disc Repair with Activated Nucleus Pulposus Cell Transplantation: A Three-Year, Prospective Clinical Study of Its Safety. Eur Cell Mater 2015, 29, 202–212. [Google Scholar] [CrossRef]
- Ekram, S.; Khalid, S.; Bashir, I.; Salim, A.; Khan, I. Human Umbilical Cord-Derived Mesenchymal Stem Cells and Their Chondroprogenitor Derivatives Reduced Pain and Inflammation Signaling and Promote Regeneration in a Rat Intervertebral Disc Degeneration Model. Mol Cell Biochem 2021, 476, 3191–3205. [Google Scholar] [CrossRef]
- Huang, H.; Liu, X.; Wang, J.; Suo, M.; Zhang, J.; Sun, T.; Zhang, W.; Li, Z. Umbilical Cord Mesenchymal Stem Cells for Regenerative Treatment of Intervertebral Disc Degeneration. Front Cell Dev Biol 2023, 11, 1215698. [Google Scholar] [CrossRef]
- See, E.Y.-S.; Toh, S.L.; Goh, J.C.H. Simulated Intervertebral Disc-like Assembly Using Bone Marrow-Derived Mesenchymal Stem Cell Sheets and Silk Scaffolds for Annulus Fibrosus Regeneration. Journal of Tissue Engineering and Regenerative Medicine 2012, 6, 528–535. [Google Scholar] [CrossRef]
- Risbud, M.V.; Albert, T.J.; Guttapalli, A.; Vresilovic, E.J.; Hillibrand, A.S.; Vaccaro, A.R.; Shapiro, I.M. Differentiation of Mesenchymal Stem Cells Towards a Nucleus Pulposus-like Phenotype In Vitro: Implications for Cell-Based Transplantation Therapy. Spine 2004, 29, 2627. [Google Scholar] [CrossRef]
- Shim, E.-K.; Lee, J.-S.; Kim, D.-E.; Kim, S.K.; Jung, B.-J.; Choi, E.-Y.; Kim, C.-S. Autogenous Mesenchymal Stem Cells from the Vertebral Body Enhance Intervertebral Disc Regeneration via Paracrine Interaction: An in Vitro Pilot Study. Cell Transplant 2016, 25, 1819–1832. [Google Scholar] [CrossRef]
- Teixeira, G.Q.; Pereira, C.L.; Ferreira, J.R.; Maia, A.F.; Gomez-Lazaro, M.; Barbosa, M.A.; Neidlinger-Wilke, C.; Goncalves, R.M. Immunomodulation of Human Mesenchymal Stem/Stromal Cells in Intervertebral Disc Degeneration: Insights From a Proinflammatory/Degenerative: Ex Vivo: Model. Spine 2018, 43, E673. [Google Scholar] [CrossRef]
- Liang, C.; Li, H.; Tao, Y.; Zhou, X.; Li, F.; Chen, G.; Chen, Q. Responses of Human Adipose-Derived Mesenchymal Stem Cells to Chemical Microenvironment of the Intervertebral Disc. Journal of Translational Medicine 2012, 10, 49. [Google Scholar] [CrossRef]
- Merceron, C.; Mangiavini, L.; Robling, A.; Wilson, T.L.; Giaccia, A.J.; Shapiro, I.M.; Schipani, E.; Risbud, M.V. Loss of HIF-1α in the Notochord Results in Cell Death and Complete Disappearance of the Nucleus Pulposus. PLOS ONE 2014, 9, e110768. [Google Scholar] [CrossRef]
- Stoyanov, J.V.; Gantenbein-Ritter, B.; Bertolo, A.; Aebli, N.; Baur, M.; Alini, M.; Grad, S. Role of Hypoxia and Growth and Differentiation Factor-5 on Differentiation of Human Mesenchymal Stem Cells towards Intervertebral Nucleus Pulposus-like Cells. Eur Cell Mater 2011, 21, 533–547. [Google Scholar] [CrossRef]
- Chen, P.; Ning, L.; Qiu, P.; Mo, J.; Mei, S.; Xia, C.; Zhang, J.; Lin, X.; Fan, S. Photo-Crosslinked Gelatin-Hyaluronic Acid Methacrylate Hydrogel-Committed Nucleus Pulposus-like Differentiation of Adipose Stromal Cells for Intervertebral Disc Repair. Journal of Tissue Engineering and Regenerative Medicine 2019, 13, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Vadalà, G.; Russo, F.; Musumeci, M.; D’Este, M.; Cattani, C.; Catanzaro, G.; Tirindelli, M.C.; Lazzari, L.; Alini, M.; Giordano, R.; et al. Clinically Relevant Hydrogel-Based on Hyaluronic Acid and Platelet Rich Plasma as a Carrier for Mesenchymal Stem Cells: Rheological and Biological Characterization. J Orthop Res 2017, 35, 2109–2116. [Google Scholar] [CrossRef]
- Ohnishi, T.; Homan, K.; Fukushima, A.; Ukeba, D.; Iwasaki, N.; Sudo, H. A Review: Methodologies to Promote the Differentiation of Mesenchymal Stem Cells for the Regeneration of Intervertebral Disc Cells Following Intervertebral Disc Degeneration. Cells 2023, 12, 2161. [Google Scholar] [CrossRef]
- Toole, B.P. Hyaluronan: From Extracellular Glue to Pericellular Cue. Nat Rev Cancer 2004, 4, 528–539. [Google Scholar] [CrossRef]
- Altman, R.; Bedi, A.; Manjoo, A.; Niazi, F.; Shaw, P.; Mease, P. Anti-Inflammatory Effects of Intra-Articular Hyaluronic Acid: A Systematic Review. CARTILAGE 2019, 10, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Stergar, J.; Gradisnik, L.; Velnar, T.; Maver, U. Intervertebral Disc Tissue Engineering: A Brief Review. Bosn J Basic Med Sci 2019, 19, 130–137. [Google Scholar] [CrossRef]
- Zhang, F.; Wang, S.; Gao, M.; Li, B.; He, Z.; Tang, T.; Zhu, Z.; Liu, S.; Zhou, Z. Hyaluronic Acid Ameliorates Intervertebral Disc Degeneration via Promoting Mitophagy Activation. Front Bioeng Biotechnol 2022, 10, 1057429. [Google Scholar] [CrossRef] [PubMed]
- Häckel, S.; Zolfaghar, M.; Du, J.; Hoppe, S.; Benneker, L.M.; Garstka, N.; Peroglio, M.; Alini, M.; Grad, S.; Yayon, A.; et al. Fibrin-Hyaluronic Acid Hydrogel (RegenoGel) with Fibroblast Growth Factor-18 for In Vitro 3D Culture of Human and Bovine Nucleus Pulposus Cells. Int J Mol Sci 2019, 20, 5036. [Google Scholar] [CrossRef]
- Gansau, J.; Buckley, C.T. Incorporation of Collagen and Hyaluronic Acid to Enhance the Bioactivity of Fibrin-Based Hydrogels for Nucleus Pulposus Regeneration. J Funct Biomater 2018, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Isa, I.L.M.; Srivastava, A.; Tiernan, D.; Owens, P.; Rooney, P.; Dockery, P.; Pandit, A. Hyaluronic Acid Based Hydrogels Attenuate Inflammatory Receptors and Neurotrophins in Interleukin-1β Induced Inflammation Model of Nucleus Pulposus Cells. Biomacromolecules 2015, 16, 1714–1725. [Google Scholar] [CrossRef] [PubMed]
- Mohd Isa, I.L.; Abbah, S.A.; Kilcoyne, M.; Sakai, D.; Dockery, P.; Finn, D.P.; Pandit, A. Implantation of Hyaluronic Acid Hydrogel Prevents the Pain Phenotype in a Rat Model of Intervertebral Disc Injury. Sci Adv 2018, 4, eaaq0597. [Google Scholar] [CrossRef]
- Watanabe, A.; Mainil-Varlet, P.; Decambron, A.; Aschinger, C.; Schiavinato, A. Efficacy of HYADD®4-G Single Intra-Discal Injections in a Rabbit Model of Intervertebral Disc Degeneration. Biomed Mater Eng 2019, 30, 403–417. [Google Scholar] [CrossRef]
- Peeters, M.; Detiger, S.E.L.; Karfeld-Sulzer, L.S.; Smit, T.H.; Yayon, A.; Weber, F.E.; Helder, M.N. BMP-2 and BMP-2/7 Heterodimers Conjugated to a Fibrin/Hyaluronic Acid Hydrogel in a Large Animal Model of Mild Intervertebral Disc Degeneration. Biores Open Access 2015, 4, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Kazezian, Z.; Sakai, D.; Pandit, A. Hyaluronic Acid Microgels Modulate Inflammation and Key Matrix Molecules toward a Regenerative Signature in the Injured Annulus Fibrosus. Advanced Biosystems 2017, 1, 1700077. [Google Scholar] [CrossRef]
- Food and Drug Administration Intent To Consider the Appropriate Classification of Hyaluronic Acid Intra-Articular Products Intended for the Treatment of Pain in Osteoarthritis of the Knee Based on Scientific Evidence Available online:. Available online: https://www.federalregister.gov/documents/2018/12/18/2018-27351/intent-to-consider-the-appropriate-classification-of-hyaluronic-acid-intra-articular-products (accessed on 14 February 2024).
- Binch, A.L.A.; Fitzgerald, J.C.; Growney, E.A.; Barry, F. Cell-Based Strategies for IVD Repair: Clinical Progress and Translational Obstacles. Nat Rev Rheumatol 2021, 17, 158–175. [Google Scholar] [CrossRef] [PubMed]
- Maloney, J.; Strand, N.; Wie, C.; Pew, S.; Dawodu, A.; Dunn, T.; Johnson, B.; Eells, A.; Viswanath, O.; Freeman, J.; et al. Current Review of Regenerative Medicine Therapies for Spine-Related Pain. Curr Pain Headache Rep 2023. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Dong, H.; Xia, Q.; Wang, Y.; Zhu, L.; Hu, Z.; Xia, J.; Mao, Q.; Weng, Z.; Yi, J.; et al. A New Strategy for Intervertebral Disc Regeneration: The Synergistic Potential of Mesenchymal Stem Cells and Their Extracellular Vesicles with Hydrogel Scaffolds. Biomedicine & Pharmacotherapy 2024, 172, 116238. [Google Scholar] [CrossRef]
- Sakai, D.; Andersson, G.B.J. Stem Cell Therapy for Intervertebral Disc Regeneration: Obstacles and Solutions. Nat Rev Rheumatol 2015, 11, 243–256. [Google Scholar] [CrossRef]
- Thorpe, A.A.; Bach, F.C.; Tryfonidou, M.A.; Le Maitre, C.L.; Mwale, F.; Diwan, A.D.; Ito, K. Leaping the Hurdles in Developing Regenerative Treatments for the Intervertebral Disc from Preclinical to Clinical. JOR Spine 2018, 1, e1027. [Google Scholar] [CrossRef]
Figure 1.
Pathophysiology of internal disc disruption secondary to vertebral end plate injury leading to disc degeneration.
Figure 1.
Pathophysiology of internal disc disruption secondary to vertebral end plate injury leading to disc degeneration.
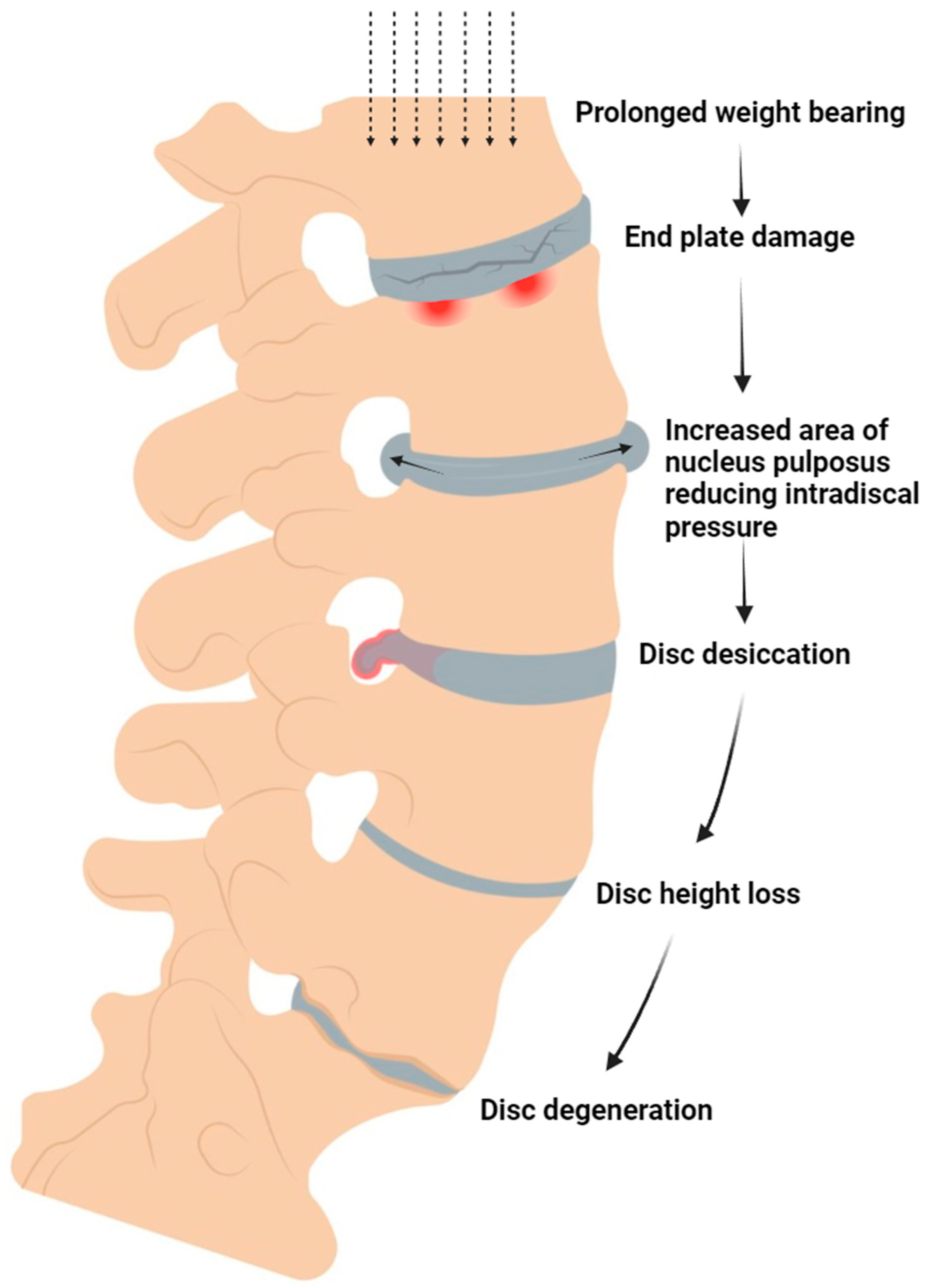
Figure 2.
Mechanism of action of transplanted MSCs in the context of degenerative IVDD.
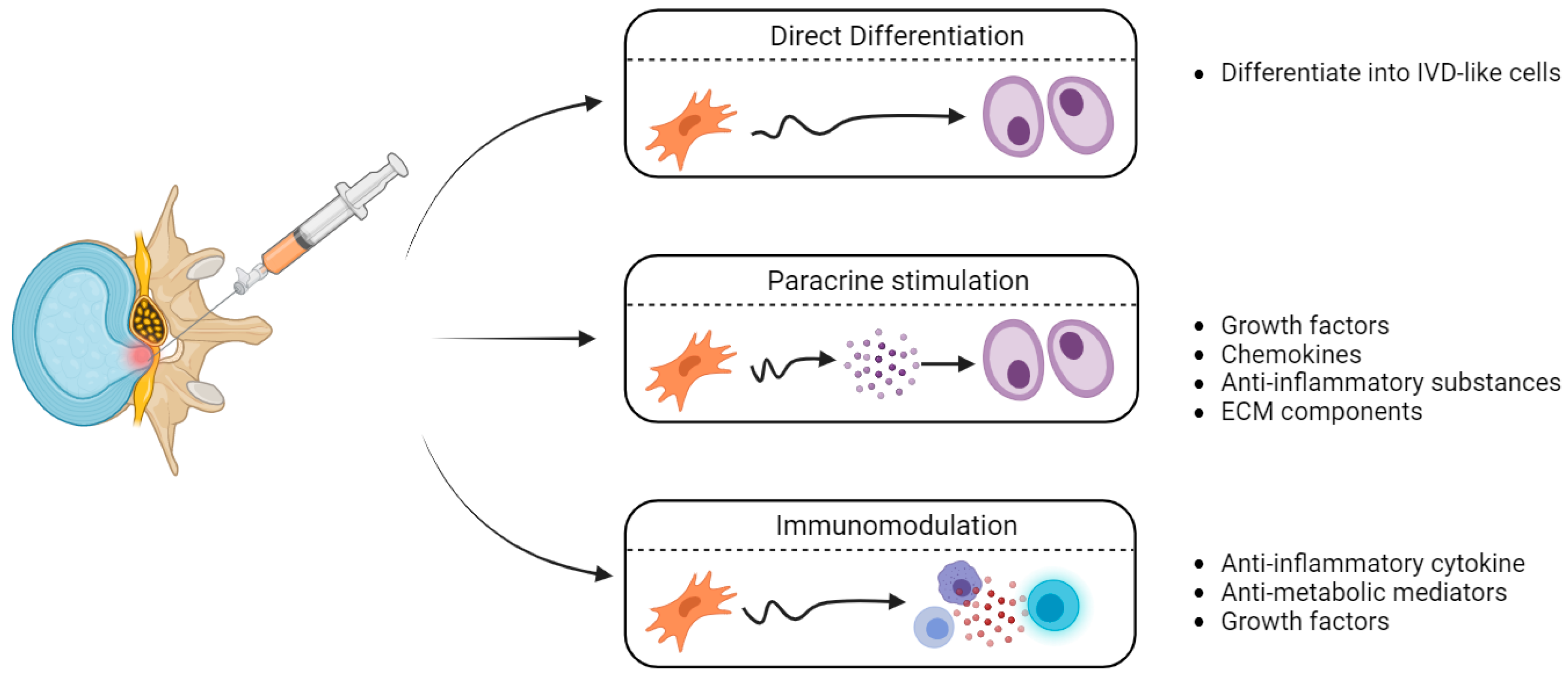

Table 1.
Published Clinical Trials examining the effectiveness of intradiscal orthobiologic injections for degenerative disc disease. (BMMSC = bone marrow-derived MSCs, AMSC = adipose-derived MSCs, UCMSC = umbilical-cord-derived MSCs, PRP = platelet-rich plasma, HA = hyaluronic acid).
Table 1.
Published Clinical Trials examining the effectiveness of intradiscal orthobiologic injections for degenerative disc disease. (BMMSC = bone marrow-derived MSCs, AMSC = adipose-derived MSCs, UCMSC = umbilical-cord-derived MSCs, PRP = platelet-rich plasma, HA = hyaluronic acid).
| Treatment | First author, year | Total participant number | Trial design | Outcome |
|---|---|---|---|---|
| BMMSC | [56] | 24 | Randomized controlled trial – single intradiscal injection of BMMSCs or sham injection (unspecified anesthetic) | Reduced pain and degeneration at 12 months follow-upFeasibility and safety confirmed |
| BMMSC | [57,58,59] | 26 | Prospective, open-label nonrandomized trial – intradiscal injection of BMMSCs at one IVD (n=13) or two adjacent IVDs (n=13). | Reduced pain at 1,2 and 3 years follow up |
| BMMSC | [60] | 10 | Single treatment group – single intradiscal injection of BMMSCs | Feasibility and safety confirmed. Reduced pain and disability at 3 months. IVD water content increased at 12 months |
| BMMSC | [61] | 10 | Single treatment group – single intradiscal injections of BMMSCs followed by 2 weeks of hyperbaric oxygen therapy | No pain reduction at 12 months follow up |
| BMMSC | [62] | 2 | Single treatment group – single intradiscal injection of collagen scaffold soaked in BMMSCs | Reduced pain and vacuum phenomenon (gas in IVD) at 24 months follow-up |
| BMMSC | [63] | 5 | Single treatment group – single intradiscal injection of hypoxic-cultured BMMSCs. | No adverse outcomes. Improved mobility and strength reported for 4 patients at 4-6 year follow-up |
| BMMSC | [64] | 33 | Single treatment group – single intradiscal injection of BMMSCs. | Safety confirmed. Pain reduction at 3-6 years follow-up. 85% of the 20 patients who underwent post-treatment MRI also had reduced disc bulge size |
| BMMSC | [65,66] | 11 | Single treatment group – single lumbar intradiscal injection of BMMSCs embedded in tricalcium pohosphate | Reduced pain and disability at 5 and 10 years follow-up. All imaged patients demonstrated lumbar fusion. |
| BMMSC & PRP | [67] | 40 | Multicenter randomized controlled trial – single intradiscal injection of BMMSCs, PRP or saline (placebo control) | PRP reduced pain and improved function at 1 year follow-up when compared to placebo. BMAC reduced pain and improved function at 1 year follow-up when compared to placebo. No significant differences between PRP and BMMSC treatments were detected. |
| UCMSC | [68] | 2 | Single treatment group – single injection of UCMSCs | No severe adverse events following treatment. Reduced pain at 24 months follow-up |
| AMSC | [69] | 15 | Single treatment group – single injection of AMSCs | No severe adverse events following treatment. Reduced pain and disability at 12 months follow-up |
| AMSC & HA | [70] | 10 | Single treatment group – single injection of AMSCs combined with a HA derivative | No severe adverse events following treatment. Reduced pain at 1 year follow-up. Three patients demonstrated increased IVD water content in 1 year follow-up MRI. |
| PRP | [71] | 47 | Double-blind, randomized controlled trial. Single intradiscal injection of PRP (n=29) or contrast agent (placebo control; n=18). | Statistically significant pain reduction at 8 weeks follow-up for PRP treatment group when compared with placebo group. |
| PRP | [72] | 22 | Single treatment group – intradiscal injection of PRP in two IVDs (n=10), three IVDs (n=2) or five IVDs (n=1). | Reduced pain and disability at 6 months follow-up. |
| PRP | [73] | 26 | Double-blind, randomized controlled trial. Single intradiscal injection of PRP (n=18) or saline (placebo control; n=8) | No significant differences in pain or disability reduction seen between PRP and placebo groups. |
| PRP | [74] | 48 | Double-blind, randomized controlled trial. Single intradiscal injection of PRP Percutaneous intradiscal radiofrequency ablation | Statistically significant reduction in pain and disability at 3 and 6 months follow-up, however no statistically significant difference in pain/disability reduction between PRP and radiofrequency ablation groups. |
| PRP | [75,76] | 16 | Double-blind, randomized controlled trial. Single intradiscal injection of PRP releasate (n=9) or betamethasone sodium phosphate (a corticosteroid; n=7). 15 patients also received an additional, optional PRP injection 8 weeks after treatment. | Significant improvement in disability and walking ability in PRP releasate group when compared to corticosteroid group at 26 weeks follow-up. Both treatment groups had significant reduction in pain, however no significant differences in pain reduction between groups were detected. |
| PRP | [77] | 5 | Single treatment group – single intradiscal injection of PRP | Gradual pain and disability reduction up to and including at 1 year follow-up |
| PRP | [78] | 6 | Single treatment group – single intradiscal injection of PRP | Pain reduction at approximately monthly follow-ups for 6 months for all patients. 6-months post MRI demonstrated structural improvements in disc anatomy for some patients. |
| PRP | [79] | 14 | Single treatment group – single intradiscal injection of PRP releasate | No adverse effects observed following treatment. Statistically significant pain reduction at 1 and 6-month follow-ups. No significant differences detected in follow-up MRI T2 quantification. |
Table 2.
Ongoing Clinical Trials examining the effectiveness of orthobiologic treatments for degenerative disc disease not previously listed by Binch et al. (2021) [108]. (BMMSC = bone marrow-derived MSCs, AMSC = adipose-derived MSCs, UCMSC = umbilical-cord-derived MSCs, PRP = platelet-rich plasma).
Table 2.
Ongoing Clinical Trials examining the effectiveness of orthobiologic treatments for degenerative disc disease not previously listed by Binch et al. (2021) [108]. (BMMSC = bone marrow-derived MSCs, AMSC = adipose-derived MSCs, UCMSC = umbilical-cord-derived MSCs, PRP = platelet-rich plasma).
| Treatment | ClinicalTrials.gov ID | Total participant number | Protocol | Trial Status at March, 2024 |
|---|---|---|---|---|
| PRP | NCT05287867 | 42 (28 treatment, 14 sham control) | Single-blind, randomized, placebo-controlled study. 2 treatments, 4 weeks apart of intradiscal PRP (or sham injection) | Actively recruiting |
| PRP | NCT04816747 | 50 (estimated) | Single group assignment, single intradiscal PRP injection | Not yet recruiting |
| PRP | NCT02983747 | 112 (estimated) | Randomised controlled trial (PRP intradiscal injection compared to thrice weekly oral NSAID (loxoprofen)) | Recruiting |
| UCMSC | NCT04414592 | 20 (estimated) | Single group assignment, single intradiscal UCMSCs injection | Status unknown |
| AMSC | NCT05011474 | 4 (estimated) | Single group assignment (AMSC intradiscal injection enriched with the ECM protein matrilin-3) | Status unknown |
| BMMSC | NCT05066334 | 52 (estimated) | Randomized controlled trial (intradiscal injection of BMMSCs vs sham control of local anesthesia) | Status unknown |
| BMMSC | NCT04759105 | 48 | Randomized control trial (intradiscal injection of BMMSCs vs sham control of local anesthesia) | Active, not recruiting |
| BMMSC | NCT04042844 | 99 (estimated) | Double-blind, randomized controlled trial (intradiscal injection of BMMSC vs saline) | Actively recruiting |
| BMMSC | NCT04735185 | 106 (estimated) | Randomized controlled trial of single intradiscal injection (intradiscal injection of BMMSCs, methylprednisolone or local anesthethic (bupivacaine) control) | Suspended (awaiting sponsor and FDA feedback) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



