
Submitted:
01 May 2024
Posted:
02 May 2024
You are already at the latest version
Abstract
The prevalence of autism has been increasing at an alarming rate. Even accounting for the expansion of autism spectrum disorder diagnostic (ASD) criteria throughout the 1990’s, there has been an over 300% increase in ASD prevalence since the year 2000. The often debilitating personal, familial, and societal sequelae of autism are generally believed to be lifelong. However, there have been several encouraging case reports demonstrating reversal of autism diagnoses with a therapeutic focus on addressing the environmental and modifiable lifestyle factors believed to be largely underlying the condition. This case report describes the reversal of autism among dizygotic, female twin toddlers and provides a review of related literature describing associations between modifiable lifestyle factors, environmental exposures, and various clinical approaches to treating autism. The twins were diagnosed with Level 3 severity ASD “requiring very substantial support” at approximately 20 months of age following concerns of limited verbal and non-verbal communication, repetitive behaviors, rigidity around transitions, and extensive gastrointestinal symptoms, among other common symptoms. A parent-driven, multidisciplinary, therapeutic intervention involving a variety of licensed clinicians focusing primarily on addressing environmental and modifiable lifestyle factors was personalized to each of the twin’s symptoms, labs, and other outcome measures. Dramatic improvements were noted within several months in most domains of the twins’ symptoms, which was manifested in reductions of Autism Treatment Evaluation Checklist (ATEC) scores from 76 to 32 in one of the twins and from 43 to 4 in the other twin. The improvement in symptoms and ATEC scores has remained relatively stable for six months at last assessment. While prospective studies are required, this case offers further encouraging evidence of ASD reversal through a personalized, multidisciplinary approach focusing predominantly on addressing environmental and lifestyle risk factors.
Keywords:
autism spectrum disorders (ASD)
; dizygotic twins
; total allostatic load
; functional medicine
; environmental medicine
; lifestyle medicine
; root-cause medicine
Introduction
Autism diagnoses were exceptionally rare prior to the latter decades of the twentieth century. In the early 1990s, the prevalence of autism among children in the United States was still estimated to be just 1 in 2,000 [1]. Even after the autism spectrum disorders (ASD) diagnostic criteria were subsequently expanded throughout the 1990’s, CDC data suggested that only 1 in 150 children had an ASD diagnosis in 2000 [2,3,4,5,6] The most recent data from the CDC revealed that 1 in 36 children had an ASD diagnosis in 2020, representing an over 300% increase in the past twenty years utilizing similar diagnostic criteria.
The prevalence of ASD among twins has not been studied as extensively. However, limited studies among twin pairs with at least one ASD diagnosis suggest that monozygotic twins are considerably more likely to share a diagnosis (58% concordance) than dizygotic twins (21% concordance). ASD studies among twins have also revealed interesting implications regarding comparative genetic versus environmental influences on ASD diagnosis. A study of over 200 pairs of twins in whom there was an autism diagnosis revealed that environmental and lifestyle factors were a far greater contributor to ASD diagnosis than heritability, accounting for 58% versus 38% of the variance, respectively[7].
ASD can present as a collection of health issues and comorbidities[8,9] not limited to neurodevelopmental, language, or social challenges, nor necessarily tied to genetic factors[10,11,12,13,14,15]. Comorbidities include immune dysregulation,[16,17,18,19,20,21,22,23] gastrointestinal issues such as diarrhea, constipation, and dysbiosis, mitochondrial dysfunction[24,25,26,27], poor detoxification[28], inflammation[29], food sensitivities, evidence of environmental toxicants[30,31,32,33,34,35,36,37,38,39,40,41,42], retained reflexes[43,44] and other structural or functional challenges.
Specific modifiable environmental and lifestyle risk factors for ASD include exposure to environmental toxicants[45,46,47], poor diet[29,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63], disruption of the gut microbiota[64,65,66,67,68,69,70,71,72,73,74], excessive exposure to non-native electromagnetic fields (EMFs)[75,76,77,78,79,80,81,82,83,84], and accumulation of heavy metals. There are limited FDA-approved pharmacological options at present to treat ASD. Accordingly, there have been a number of non-pharmacological interventions tailored to address underlying environmental and lifestyle risk factors that have demonstrated improvements in ASD symptoms[85,86]. These include dietary interventions[48,62] such as gluten and casein free[87,88,89,90,91,92,93,94,95], GAPS, specific carbohydrate diet[48], low glutamate,[96,97,98,99,100,101] and ketogenic[102,103,104,105,106,107,108,109,110,111]. Targeted dietary supplements such as vitamin D [112,113], methylfolate[114,115], and carnitine[116,117], vitamin B12 and other micronutrient supplementation[51,118], mitochondrial support, or supplements thought to be relevant to a child’s functional genomic situation. Addressing other modifiable lifestyle factors and environmental interventions, such as more time in nature, reduction in exposure to artificial light, and improving indoor air quality have demonstrated promise. Therapeutic interventions addressing a child’s physical structure and function such as cranial osteopathy[119,120], retained reflex integration[121,122,123], physical therapy[124,125,126], occupational therapy have also been associated with improved outcomes among ASD patients. While reversal of ASD diagnosis is relatively rare, there have been documented cases in the literature[127,128,129] of complete recovery with multi-modal intervention. One such case achieved reversal of ASD diagnosis through a combination of dietary modifications, probiotics and micronutrient supplementation, and antimicrobials that were personalized to the child’s risk factors, clinical presentation, and a variety of labs.
Patient Information
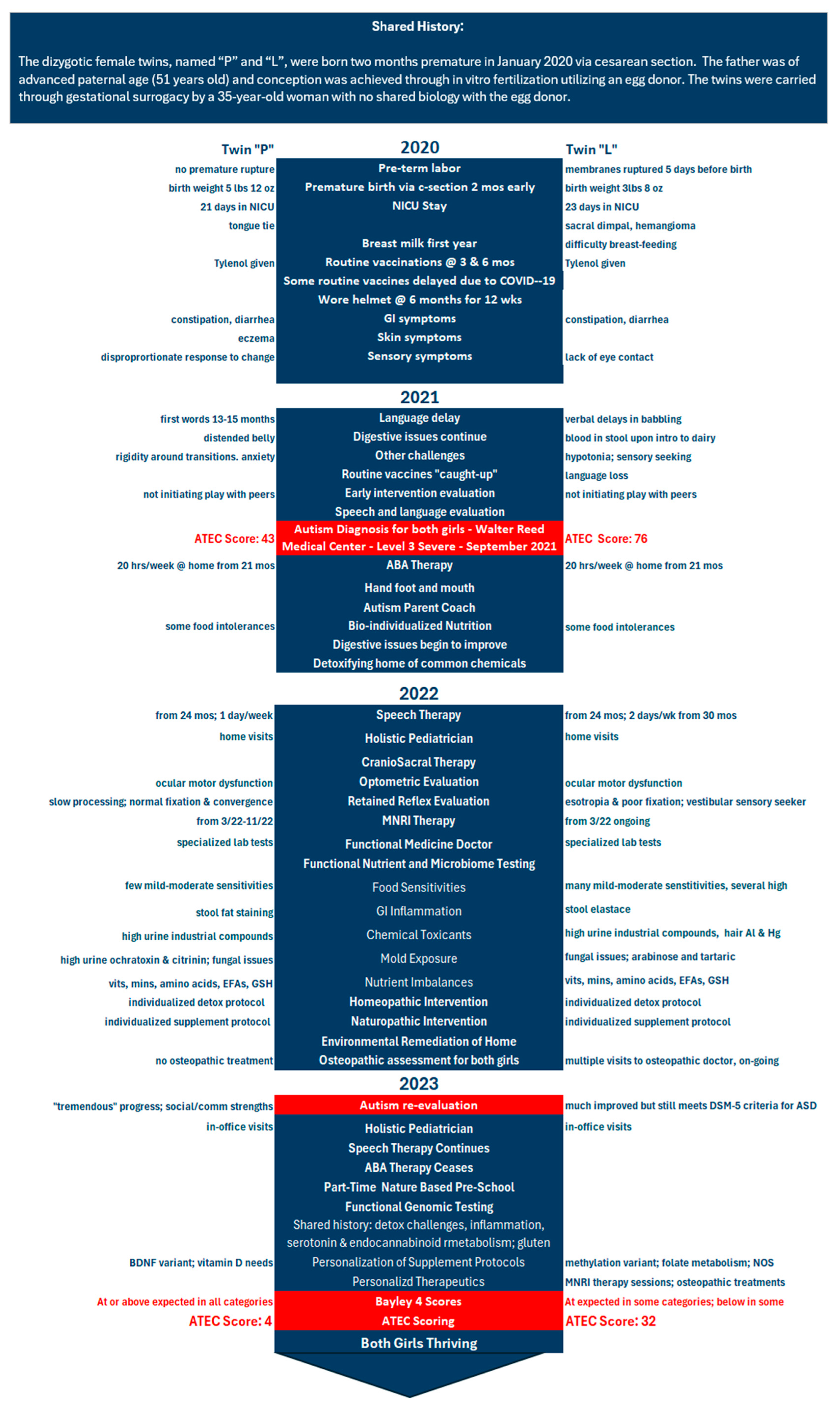
A timeline providing shared history of the patients, diagnoses, treatments, and changes in symptoms and other outcomes over time is provided in Figure 1.
Family History, Conception, and Gestation
The father was of advanced paternal age (51 years old) and conception was achieved through in vitro fertilization utilizing an egg donor. The fetuses were carried through gestational surrogacy by a 35-year-old woman with no shared biology with the egg donor.
Birth and First Year of Life
The dizygotic female twins, named “P” and “L”, were born two months premature in January 2020 via cesarean section. L experienced premature rupture 5 days before delivery. P was 5 lbs, 12 ounces at birth and spent 21 days in neonatal intensive care unit. L was 3lbs, 8 ounces at birth and spent 23 days in neonatal intensive care unit. The twins received routine vaccinations at 3 and 6 months, and then no further vaccination until 14 months of age due largely to the Covid-19 pandemic. Acetaminophen was administered prior to and following vaccines.
Primary Concerns and Symptoms of the Patients
Parental Concerns Prior to Autism Diagnosis – First Year of Life
In P, parents noticed stool symptoms, including occasional diarrhea, constipation, eczema, and a disproportionate response/protest to change or stimuli. In L, parents noticed stool symptoms, including constipation and diarrhea, inconsistent eye contact, babbling communication, and difficulty breast feeding. Hypotonia was observed, but motor milestones were met. There were no issues with eating and sleeping reported. Both twins received breast milk for 12 months via a combination of pumped milk from gestational carrier and induced lactation from mother.
Parental Concerns Prior to Autism Diagnosis – One Year Old until Diagnosis
At 12 months, the twins ceased drinking breast milk and cow dairy/milk was introduced. In L, parents reported cow dairy intolerance (white stool, blood in stool, and vomit upon exposure), constipation and diarrhea, hypotonia, lack of eye contact, sensory seeking, and language delay. In P, parents reported constipation and diarrhea, repetitive behavior/stims, rigidity around transitions, anxiety, and language delay. In March 2021, the twins received a series of “catch up” vaccines that had been delayed due to the Covid-19 pandemic. The parents noticed worsening of some symptoms after this round of vaccinations, including significant language loss for L. In July 2021, a Strong Start Early Intervention eval was conducted. It was noticed that L was communicating only in single words at that time.
Autism Spectrum Disorders Diagnoses
In light of the concerns described above, an ASD evaluation was conducted at Walter Reed National Medical Center in September 2021. Both twins met the DSM-5 Autism Spectrum Disorders diagnosis at Walter Reed National Military Center with Level 3 severity “requiring very substantial support” at approximately 20 months of age. A pediatrician and other specialists noted that L had no language or imaginative play, she had retained reflexes (including Moro reflex[132,133,134]) and on eye exam showed esotropia and poor fixation. P showed ocular motor dysfunction with slow visual spatial processing.
According to a subsequent assessment at Children’s National Hospital - Division of Neuropsychology, L had difficulty in both domains of autism – social communication (she had reduced verbal and non-verbal communication) and repetitive and restrictive patterns of behaviors and interests (she demonstrated stereotyped movements, cv language and jargon, repetitive play actions and sensory seeking behaviors) and met the DSM-5 criteria for Autism Spectrum Disorders with language impairment.
Other Symptoms and Diagnostic Testing
Evaluation by an early intervention professional in December 2021 revealed that the twins typically played independently of each other in their home and were not initiating interactions with peers.
Multiple out-of-pocket specialty lab tests, including buccal swabs for functional genomic profile (IntellxxDNA)[135], urine organic acid[136] tests and testing for organic compounds and metabolites (Mosaic Diagnostics and Genova Diagnostics), hair analysis[137] for metals and minerals (Mosaic Diagnostics), blood analysis for nutritional (vitamin and mineral) status (Genova Diagnostics)[138] and IgG-mediated food sensitivities[139] (Mosaic Diagnostics), stool studies[140] for pathogens and GI health (Mosaic Diagnostics), and urine analysis for mycotoxins[141] (Mosaic Diagnostics) were conducted in the first year after the twin’s official autism diagnosis from March of 2022 with repeat testing in 2023. Findings of these tests in both twins included biomarkers[142,143,144,145,146,147,148,149,150,151,152,153,154,155] associated with mild gastrointestinal inflammation (one child with low elastase and the other with significant fat staining, though plentiful lactobacillus and bifidobacteria and unremarkable secretory IGAs),fatty acid imbalances (high omega 6:3 ratio), nutrient deficits (minerals tested below the 50th percentile, and both twins were relatively low in vitamins C, B12, and B3, alpha lipoic acid, glutathione) with signs of mold exposure (highly elevated urinary ochratoxin and citrinin), fungal issues (elevated arabinose for both girls, and elevated tartaric acid for L), signs of bacterial overgrowth (elevated hippuric acid for P and dihydroxyphenylpropionic acid for L), metal excretion (high aluminum in both girls), sensitivities to common foods, and urinary excretion of toxic compounds and their metabolites (some >100th percentile, glyphosate at or above 75th percentile for both twins).
L and P were both diagnosed with ocular motor dysfunction in Spring 2022.
Therapeutic Interventions
The twins’ parents were able to work with an autism parent coach[156] who initially oriented them to the diagnosis and helped provide them with perspective and confidence. The parents were motivated to address the “total allostatic load” of stressors that is believed to underlie many chronic conditions. The total allostatic load model suggests that chronic exposure to physical, mental, or environmental stressors leads to persistent release of primary mediators (e.g., inflammatory cytokines, cortisol) that disrupt physiological function and can lead to chronic disease[157,158]. Numerous systematic reviews have revealed that total allostatic load is associated with increased risk of chronic disease across the lifespan, including in childhood[159,160]. The parents were exposed to this concept by reading popular books on the topic of total allostatic load and autism[158], listening to autism-focused audio materials[156] provided by their coach and subsequently taking the Child Health Inventory for Resilience and Prevention (CHIRP) survey of the Documenting Hope Project, a comprehensive assessment of total allostatic load among children[161]. Parents who complete CHIRP receive a comprehensive report that identifies stressors contributing to the total allostatic load in the child’s health history and can be shared with health providers or used to identify areas of concern.
In addition to completing the CHIRP survey and receiving the report, the twins’ mother also utilized additional resources through Epidemic Answers, including free webinars offered by different experts on the topic of autism and a parent forum called Healing Together[162], which provides a “road map” of steps designed to change the trajectory of complex chronic health conditions, such as autism.
Alongside Applied Behavior Analysis (ABA, which is typically recommended for new ASD diagnoses), beginning at 22 months and ending at 33 months, and speech therapy starting at 24 months, the twins’ parents implemented a rigorous diet and nutrition intervention around the time of diagnosis. They eliminated sources of glutamate in the children’s diet following the Reduced Excitatory Inflammatory Diet[163]. The twins were also put on a strictly gluten-free, casein-free diet that was low in sugar and had no exposure to artificial colors, dyes, or ultra-processed foods. An emphasis was placed on consuming organic, unprocessed, freshly prepared and home-cooked food from local sources, when possible. The family also consulted with a dietician for guidance around these dietary interventions.
A number of dietary supplements, including omega-3 fatty acids, a multivitamin, vitamin D, carnitine, 5-methyltetrahydrofolate, and bio-individualized homeopathic remedies were taken by both girls. A combination of labs and genomic information were utilized to inform dietary supplementation.
The family consulted a naturopathic doctor who guided them in some DNA-targeted precision medicine using the IntellxxDNA genomics tool[135]. There were some common findings, such as impaired serotonin metabolism, and a recommendation that the girls be fed a diet rich in tryptophan to upregulate serotonin production, as well as consume foods rich in vitamins B12, B6 and folate. Both twins had several genetic variants which may increase their risk of systemic inflammation. The mother was advised to feed the children foods that are high in betaine and choline, as well as to supplement with lion’s mane mushroom and resolvins. However, each girl also had needs that were independent of the other. P had variants that may increase her need for vitamin D. L had several variants that may increase the risk of neuroinflammation, oxidative stress, and compromised detoxification. Advice was provided to support glutathione production.
Trans-disciplinary referrals and specialized therapies helped the parents access complementary structural and functional supports for their twins. The girls had the most sessions of any intervention during the time of this reporting with an occupational therapist who focused on the specialized technique of neuro-sensory motor reflex integration[164,165,166,167] to support the integration process of primary motor reflex patterns and encourage nervous system regulation. This technique is believed to help reengage inhibited neural pathways or facilitate the activation of alternate neural pathways.
Information about the importance of addressing potential load of environmental toxicants on the children from the autism parent coach and independent reading, lead the family to evaluate their home for air quality, mold and moisture risk, and to put supports in place that included opening windows for better cross-ventilation.
In October of 2022, a Building Biology Environmental Consultant[168] was invited to evaluate the twins’ home. The environmental consultant tested the home’s indoor air quality, evaluated possible signs of moisture intrusion, and other potential sources of toxicants. Air tests for mold were reported to be “very clean”. However, the family was encouraged to further evaluate several areas of the home in which a thermal imagining camera and/or a moisture meter suggested the possibility of water damage. A window in the twins’ bedroom was one area designated for further evaluation.
At the recommendation of the developmental optometrist, both girls were taken for evaluation by a cranial osteopath. The family decided to pursue osteopathic care for L and not for L visited an osteopath at regular intervals in 2023 and saw notable benefits, including overall disposition and communication.
Patient Outcomes
The Autism Treatment Evaluation Checklist (ATEC) is a 77-item instrument that is sensitive to change and is utilized to evaluate ASD treatment effectiveness, with lower scores indicating improvement in symptoms[169,170].
L’s ATEC scores improved dramatically, from 76 in March 2022 to 32 in October 2023, and then remained relatively stable at 34 in March 2024. P’s ATEC scores also improved dramatically, from 43 in March 2022 to 4 in October 2023, remaining stable at 4 in March 2024.
In addition to the twins’ improved ATEC scores, there were numerous other behavioral and social improvements noted after implementation of the interventions. L and P’s eye contact, language, attention had all improved noticeably by Fall 2022. This was accompanied by participation in a toddler play group three days per week and ultimately attending pre-school three days per week in Fall 2023. The pediatrician noted that P had undergone “a kind of miracle”.
The twins seemed to tolerate the interventions well, as indicated by their reduced ATEC scores, pre-school success, and other outcomes. There were no adverse events noted.
Please see Figure 1 for a timeline of the twins’ birth, symptoms, diagnosis, treatment strategy, and outcomes on the following page.
Discussion
This case revealed a reversal of the Level 3 Autism Spectrum Disorder diagnoses among dizygotic toddler twin girls that was achieved primarily through environmental and lifestyle modifications over a two-year period. The twins’ dramatic improvements and diagnoses reversal has persisted for over six months with no signs of regression. While there are numerous factors underlying these improvements, the motivation of the twins’ parents to implement environmental and lifestyle modifications was particularly notable. This included both independent, parent-led intervention as well as the guidance and therapeutic intervention of numerous practitioners (e.g. coach, physician, dietitian, occupational therapist, optometrist). Many of these practitioners commented on how the family-wide commitment to and excellent compliance with the total load-oriented interventions, the parents’ exceptional communication with practitioners, and their positive attitude all seemed to influence the positive outcomes noted in this case.
These findings and other published cases of ASD reversal are encouraging[127,128,129], as the ongoing dramatic increase in the prevalence of ASD presents challenges to the lifelong health and wellbeing of both those affected and to society more generally. For instance, the economic impact of ASD is deeply concerning and generally unappreciated at this point in time. Published projections estimate that that even if the future prevalence of ASD remained unchanged over the next decade, there would be approximately 1 million new cases, thereby resulting in an additional $4 trillion of lifelong social costs in the United States. Furthermore, if the current rate of increase in prevalence continues, costs could reach nearly $15 trillion of lifelong costs by 2029[171]. Thus, while ABA and current standard of care can be important contributors to the management of ASD symptoms for some children[172,173,174], many with ASD do not respond and there has been a need for personalization[175]. Investigation into other more personalized, root-cause oriented therapeutic approaches such as those described in this case are warranted.
There are several key strengths of this report. First, the meticulous documentation of diagnoses, tracking of ATEC scores over time, and detailed behavioral reports from the parents and a variety of practitioners helped rigorously establish the twins’ improvement and diagnosis reversal noted in this case. The extensive documentation allowed for the construction of a detailed timeline (Figure 1) including diagnoses, interventions, and changes in key outcomes and other symptoms over time. In addition, while there are a variety of ASD assessments in the published literature, including the Childhood Autism Rating Scale, Autism Diagnostic Interview – Revised, and the Autism Diagnostic Observation Schedule, the ATEC is more sensitive to change with intervention than the majority of these instruments, which are generally better-suited to diagnosis and measurement of ASD stability[170]. Another strength of this case report of dizygotic twins is the clear environmental and lifestyle influences on ASD that these findings help establish, building upon previous studies revealing the comparatively greater impact of these types of factors than genetics[7].
There are also several limitations that are worthy of mention. First, while effective at reversing ASD diagnoses, the comprehensive approach that was employed in this case may not yet be widely generalizable. For instance, the cost of the healthy lifestyle modifications and out-of-pocket costs of care of the numerous practitioners and laboratory assessments in this case would be financially prohibitive to many families. Access to healthy foods and the types of practitioners contributing to this therapeutic approach may also be limited for many families. A second limitation of any comprehensive treatment approach is the lack of clear evidence of the isolated effects of each of the modalities that were employed. However, it has become increasingly clear that ASD treatment is not one-size-fits-all and that personalized, multi-modality treatment approaches to help address the total load of stressors are likely required to achieve optimal outcomes.
Conclusion
The dramatic improvement and reversal of ASD diagnoses among these fraternal twins demonstrates the potential of a comprehensive treatment approach including both conventional therapies (e.g., ABA) and a wide variety of environmental and lifestyle modifications facilitated by a multi-disciplinary team of practitioners addressing the total load of stressors of modern living. The commitment and leadership of well-informed parents or guardians is an essential component to the effective personalization that appears necessary for the feasibility of such improvements. Future prospective studies are warranted to confirm these findings.
Patient Perspective
“Having fraternal twin daughters diagnosed with Autism Spectrum Disorder at 20 months has given us a profound appreciation of the highly individual presentation of Autism. Despite sharing similar genes and identical conception, gestation, birth experience, and post-natal factors - as well as benefitting from consistent nurture, home environment and family dynamics - each daughter presented an ASD diagnosis entirely uniquely. Early in our navigation, we adopted a ‘total load’ theory, understanding that there was not one ’single' factor that catalyzed their diagnosis but the combined assault of many injuries. In accepting the very complex presentation of ASD, we also understood that there would be no singular ‘cure' for it either. Conventional statistics have stacked the odds against the ability to recover a child from an ASD diagnosis. Our approach was therefore focused on following a nonconventional, holistic understanding of each daughter’s bio individual needs, exploring root cause and designing customized support. We began by choosing to pursue functional, integrative support centered around the foundational principles of diet, environment, and lifestyle. We vetted therapies that would deliver support in a naturalistic setting - primarily our home. We chose practitioners who were aligned in our belief in our daughters’ intrinsic ability to heal given the right support. We assembled a team that welcomed our engagement and worked cooperatively with each other. We committed to being highly involved in all the interventions we explored, educating ourselves and advocating for what we felt was best for our children. Finally, we were strategic in focusing on sequence, using labs and other evaluation tools to measure progress, and harnessing the power of innovation to map genes and address cellular health. We explored modalities both new and old, while operating from a place of patience and curiosity. Most importantly, in our experience as parents has been the desire to create and maintain a profound and loving bond with each of our daughters - and to remain parents, not practitioners. Through this approach, we have witnessed the radical recovery of one daughter - who presents today as a joyful, engaging, spirited, extremely bright 4-year-old. We remain steadfast in our support for our other daughter whose progress has also consistently amazed us and has reminded us that recovery is possible at each person’s individual pace.”
Author Contributions
Conceptualization, C.R.D, J.N., E.L., H.T.R.; methodology, C.R.D.; investigation, C.R.D., J.N., E.L., H.T.R; data curation, J.N., H.T.R., S.M. M.R.H.; writing—original draft preparation, C.R.D.; writing—review and editing, J.N., E.L., H.T.R, S.M.; visualization, S.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This case report did not require ethical approval.
Informed Consent Statement
Written informed consent was obtained from the twins’ parents to publish this case report.
Data Availability Statement
Data presented in this case report are available from the corresponding author upon reasonable request. The data are not publicly available to preserve family privacy.
Acknowledgments
The authors would like to acknowledge the twins’ parents and the practitioners and health coaches for their essential contributions to this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tanguay, P.E. Pervasive Developmental Disorders: A 10-Year Review. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1079–1095. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Li, Y.; Liu, B.; Chen, Q.; Xing, X.; Xu, G.; Yang, W. Prevalence of Autism Spectrum Disorder Among Children and Adolescents in the United States From 2019 to 2020. JAMA Pediatr. 2022, 176, 943–945. [Google Scholar] [CrossRef]
- Maenner, M.J. , et al. , Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States 2020, MMWR Surveill Summ 2023, 72, 1–14. [Google Scholar] [PubMed]
- Waterhouse, L. Autism Overflows: Increasing Prevalence and Proliferating Theories. Neuropsychol. Rev. 2008, 18, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Zablotsky, B.; I Black, L.; Blumberg, S.J. Estimated Prevalence of Children With Diagnosed Developmental Disabilities in the United States, 2014-2016. . 2017, 1–8. [Google Scholar]
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A.; Danielson, M.L.; Bitsko, R.H.; Blumberg, S.J.; Kogan, M.D.; Boyle, C.A. Prevalence and Trends of Developmental Disabilities among Children in the United States: 2009–2017. Pediatrics 2019, 144, e20190811. [Google Scholar] [CrossRef] [PubMed]
- Hallmayer, J.; Cleveland, S.; Torres, A.; Phillips, J.; Cohen, B.; Torigoe, T.; Miller, J.; Fedele, A.; Collins, J.; Smith, K.; et al. Genetic Heritability and Shared Environmental Factors Among Twin Pairs With Autism. Arch. Gen. Psychiatry 2011, 68, 1095–1102. [Google Scholar] [CrossRef]
- M. , C.-K. The review of most frequently occurring medical disorders related to aetiology of autism and the methods of treatment. Acta Neurobiol. Exp. 2010, 70, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Liao, T.-C.; Lien, Y.-T.; Wang, S.; Huang, S.-L.; Chen, C.-Y. Comorbidity of Atopic Disorders with Autism Spectrum Disorder and Attention Deficit/Hyperactivity Disorder. J. Pediatr. 2016, 171, 248–255. [Google Scholar] [CrossRef]
- Currenti, S.A. Understanding and Determining the Etiology of Autism. Cell. Mol. Neurobiol. 2009, 30, 161–171. [Google Scholar] [CrossRef]
- Deth, R.; Muratore, C.; Benzecry, J.; Power-Charnitsky, V.-A.; Waly, M. How environmental and genetic factors combine to cause autism: A redox/methylation hypothesis. NeuroToxicology 2008, 29, 190–201. [Google Scholar] [CrossRef] [PubMed]
- D. A., G.; J.K., K.; M.R., G. The biological basis of autism spectrum disorders: Understanding causation and treatment by clinical geneticists. Acta Neurobiol. Exp. 2010, 70, 209–226. [Google Scholar] [CrossRef] [PubMed]
- Herbert, M.; Russo, J.; Yang, S.; Roohi, J.; Blaxill, M.; Kahler, S.; Cremer, L.; Hatchwell, E. Autism and environmental genomics. NeuroToxicology 2006, 27, 671–684. [Google Scholar] [CrossRef]
- Li, Y.; Qiu, S.; Shi, J.; Guo, Y.; Li, Z.; Cheng, Y.; Liu, Y. Association between MTHFR C677T/A1298C and susceptibility to autism spectrum disorders: a meta-analysis. BMC Pediatr. 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.; Cassel, S.; Sutterwala, F. Role of the NLRP3 Inflammasome in Vaccine Responses. J. Allergy Clin. Immunol. 2012, 129, AB162. [Google Scholar] [CrossRef]
- Ashwood, P.; Krakowiak, P.; Hertz-Picciotto, I.; Hansen, R.; Pessah, I.; Van de Water, J. Elevated plasma cytokines in autism spectrum disorders provide evidence of immune dysfunction and are associated with impaired behavioral outcome. Brain, Behav. Immun. 2011, 25, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Ashwood, P.; Wills, S.; Van de Water, J. The immune response in autism: a new frontier for autism research. J. Leukoc. Biol. 2006, 80, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Atladóttir, H.Ó.; Pedersen, M.G.; Thorsen, P.; Mortensen, P.B.; Deleuran, B.; Eaton, W.W.; Parner, E.T.; Sutton, R.M.; Niles, D.; Nysaether, J.; et al. Association of Family History of Autoimmune Diseases and Autism Spectrum Disorders. Pediatrics 2009, 124, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Jyonouchi, H.; Geng, L.; Cushing-Ruby, A.; Quraishi, H. Impact of innate immunity in a subset of children with autism spectrum disorders: a case control study. J. Neuroinflammation 2008, 5, 52–52. [Google Scholar] [CrossRef]
- Blaylock, R.; Strunecka, A.; Patocka, J.; Strunecky, O. Immunoexcitotoxicity as the central mechanism of etiopathology and treatment of autism spectrum disorders: A possible role of fluoride and aluminum. Surg. Neurol. Int. 2018, 9, 74. [Google Scholar] [CrossRef]
- Theoharides, T.C. , Is a subtype of autism an allergy of the brain? Clin Ther 2013, 35, 584–591. [Google Scholar] [CrossRef]
- Vojdani, A. and Lambert, A Gut Feeling for Immune Dysregulation & Neuroinflammation in Autism The Autism File, 2009(31).
- Vuillermot, S.; Luan, W.; Meyer, U.; Eyles, D. Vitamin D treatment during pregnancy prevents autism-related phenotypes in a mouse model of maternal immune activation. Mol. Autism 2017, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- E Frye, R.; DeLaTorre, R.; Taylor, H.; Slattery, J.; Melnyk, S.; Chowdhury, N.; James, S.J. Redox metabolism abnormalities in autistic children associated with mitochondrial disease. Transl. Psychiatry 2013, 3, e273–e273. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, L.; Papaleo, V.; Porcelli, V.; Scarcia, P.; Gaita, L.; Sacco, R.; Hager, J.; Rousseau, F.; Curatolo, P.; Manzi, B.; et al. Altered calcium homeostasis in autism-spectrum disorders: evidence from biochemical and genetic studies of the mitochondrial aspartate/glutamate carrier AGC1. Mol. Psychiatry 2008, 15, 38–52. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, L. and A.M. Persico, Mitochondrial dysfunction in autism spectrum disorders: cause or effect? Biochim Biophys Acta 2010, 1797(6-7): 1130-7.
- Pastural. ; Ritchie, S.; Lu, Y.; Jin, W.; Kavianpour, A.; Su-Myat, K.K.; Heath, D.; Wood, P.L.; Fisk, M.; Goodenowe, D.B. Novel plasma phospholipid biomarkers of autism: Mitochondrial dysfunction as a putative causative mechanism. Prostaglandins, Leukot. Essent. Fat. Acids 2009, 81, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Alabdali, A.; Al-Ayadhi, L.; El-Ansary, A. A key role for an impaired detoxification mechanism in the etiology and severity of autism spectrum disorders. Behav. Brain Funct. 2014, 10, 14–14. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, M.L.; Vargas, D.D. Effectiveness of nutritional interventions on behavioral symptomatology of autism spectrum disorder: a systematic review. Nutr. Hosp. 2022, 39, 1378–1388. [Google Scholar] [CrossRef]
- Adams, J.B.; Romdalvik, J.; Ramanujam, V.M.S.; Legator, M.S. Mercury, Lead, and Zinc in Baby Teeth of Children with Autism Versus Controls. J. Toxicol. Environ. Heal. Part A 2007, 70, 1046–1051. [Google Scholar] [CrossRef] [PubMed]
- Büsselberg, D. Calcium channels as target sites of heavy metals. Toxicol. Lett. 1995, 82-83, 255–261. [Google Scholar] [CrossRef]
- Grandjean, P.; Landrigan, P.J. Developmental neurotoxicity of industrial chemicals: A silent pandemic. Lancet 2006, 368, 2167–2178. [Google Scholar] [CrossRef]
- Hertz-Picciotto, I.; Park, H.; Dostal, M.; Kocan, A.; Trnovec, T.; Sram, R. Prenatal Exposures to Persistent and Non-Persistent Organic Compounds and Effects on Immune System Development. Basic Clin. Pharmacol. Toxicol. 2008, 102, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Hertz-Picciotto, I.; Sass, J.B.; Engel, S.; Bennett, D.H.; Bradman, A.; Eskenazi, B.; Lanphear, B.; Whyatt, R. Organophosphate exposures during pregnancy and child neurodevelopment: Recommendations for essential policy reforms. PLOS Med. 2018, 15, e1002671. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.S.; Blaxill, M.F.; Haley, B.E. Reduced Levels of Mercury in First Baby Haircuts of Autistic Children. Int. J. Toxicol. 2003, 22, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Ivanovski, I.; Ivanovski, A.; Nikolić, D.; Ivanovski, P. Aluminium in brain tissue in autism. J. Trace Elements Med. Biol. 2018, 51, 138–140. [Google Scholar] [CrossRef]
- Jafari, M. , et al. Pediatric Health Medicine and Therapeutics 2020, 11. [Google Scholar]
- Kern, J.K.; Geier, D.A.; Adams, J.B.; Geier, M.R. A biomarker of mercury body-burden correlated with diagnostic domain specific clinical symptoms of autism spectrum disorder. BioMetals 2010, 23, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Palmer, R.F.; Blanchard, S.; Wood, R. Proximity to point sources of environmental mercury release as a predictor of autism prevalence. Heal. Place 2009, 15, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Tomljenovic, L. and C. A. Shaw, Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? J Inorg Biochem 2011, 105, 1489–1499. [Google Scholar]
- Windham, G.C.; Zhang, L.; Gunier, R.; Croen, L.A.; Grether, J.K. Autism Spectrum Disorders in Relation to Distribution of Hazardous Air Pollutants in the San Francisco Bay Area. Environ. Heal. Perspect. 2006, 114, 1438–1444. [Google Scholar] [CrossRef]
- Mold, M.; Umar, D.; King, A.; Exley, C. Aluminium in brain tissue in autism. J. Trace Elements Med. Biol. 2018, 46, 76–82. [Google Scholar] [CrossRef]
- Grigg, T.M.; Fox-Turnbull, W.; Culpan, I. Retained primitive reflexes: Perceptions of parents who have used Rhythmic Movement Training with their children. J. Child Heal. Care 2018, 22, 406–418. [Google Scholar] [CrossRef] [PubMed]
- C., G. C., G., Integration exercise programme for children with learning difficulties who have preserved vestigial primitive reflexes. Acta Neuropsychologica 2017, 15(3).
- Blaylock, R.L. A possible central mechanism in autism spectrum disorders, part 1. . 2008, 14, 46–53. [Google Scholar]
- Blaylock, R.L. A possible central mechanism in autism spectrum disorders, part 3: the role of excitotoxin food additives and the synergistic effects of other environmental toxins. . 2009, 15, 56–60. [Google Scholar] [PubMed]
- Blaylock, R.L. , A possible central mechanism in autism spectrum disorders, part 2: immunoexcitotoxicity. Altern Ther Health Med 2009, 15, 60–67. [Google Scholar] [PubMed]
- S. , A., et al., Specific Carbohydrate Diet (SCD/GAPS) and Dietary Supplements for Children with Autistic Spectrum Disorder. Proceedings of the Latvian Academy of Sciences Section B Natural Exact and Applied Sciences 2021, 75, 417–425.
- Adams, J.B.; Audhya, T.; McDonough-Means, S.; Rubin, R.A.; Quig, D.; Geis, E.; Gehn, E.; Loresto, M.; Mitchell, J.; Atwood, S.; et al. Effect of a vitamin/mineral supplement on children and adults with autism. BMC Pediatr. 2011, 11, 111. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Johansen, L.J.; Powell, L.D.; Quig, D.; Rubin, R.A. Gastrointestinal flora and gastrointestinal status in children with autism–Comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011, 11, 22. [Google Scholar] [CrossRef]
- Adams, J.B.; Kirby, J.; Audhya, T.; Whiteley, P.; Bain, J. Vitamin/mineral/micronutrient supplement for autism spectrum disorders: a research survey. BMC Pediatr. 2022, 22, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B. , et al., Comprehensive Nutritional and Dietary Intervention for Autism Spectrum Disorder-A Randomized, Controlled 12-Month Trial. Nutrients 2018, 10(3).
- Cekici, H.; Sanlier, N. Current nutritional approaches in managing autism spectrum disorder: A review. Nutr. Neurosci. 2017, 22, 145–155. [Google Scholar] [CrossRef]
- Cheng, N.; Rho, J.M.; Masino, S.A. Metabolic Dysfunction Underlying Autism Spectrum Disorder and Potential Treatment Approaches. Front. Mol. Neurosci. 2017, 10, 34. [Google Scholar] [CrossRef]
- Chistol, L.T.; Bandini, L.G.; Must, A.; Phillips, S.; Cermak, S.A.; Curtin, C. Sensory Sensitivity and Food Selectivity in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 48, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Critchfield, J.W.; van Hemert, S.; Ash, M.; Mulder, L.; Ashwood, P. The Potential Role of Probiotics in the Management of Childhood Autism Spectrum Disorders. Gastroenterol. Res. Pr. 2011, 2011, 1–8. [Google Scholar] [CrossRef]
- Hartman, R.E. and D. Patel, Dietary Approaches to the Management of Autism Spectrum Disorders. Adv Neurobiol 2020, 24, 547–571. [Google Scholar]
- Herbert, M.R. and J. A. Buckley, Autism and dietary therapy: case report and review of the literature. J Child Neurol 2013, 28, 975–982. [Google Scholar] [PubMed]
- Karhu, E.; Zukerman, R.; Eshraghi, R.S.; Mittal, J.; Deth, R.C.; Castejon, A.M.; Trivedi, M.; Mittal, R.; Eshraghi, A.A. Nutritional interventions for autism spectrum disorder. Nutr. Rev. 2020, 78, 515–531. [Google Scholar] [CrossRef]
- Knivsberg, A.; Reichelt, K.; Høien, T.; Nødland, M. A Randomised, Controlled Study of Dietary Intervention in Autistic Syndromes. Nutr. Neurosci. 2002, 5, 251–261. [Google Scholar] [CrossRef]
- V. , L., et al., Elimination diets' efficacy and mechanisms in attention deficit hyperactivity disorder and autism spectrum disorder. Eur Child Adolesc Psychiatry. 2017, 26, 1067–1079.
- Matthews, J.S.; Adams, J.B. Ratings of the Effectiveness of 13 Therapeutic Diets for Autism Spectrum Disorder: Results of a National Survey. J. Pers. Med. 2023, 13, 1448. [Google Scholar] [CrossRef]
- Yu, Y.; Huang, J.; Chen, X.; Fu, J.; Wang, X.; Pu, L.; Gu, C.; Cai, C. Efficacy and Safety of Diet Therapies in Children With Autism Spectrum Disorder: A Systematic Literature Review and Meta-Analysis. Front. Neurol. 2022, 13, 844117. [Google Scholar] [CrossRef]
- D'Eufemia, P.; Celli, M.; Finocchiaro, R.; Pacifico, L.; Viozzi, L.; Zaccagnini, M.; Cardi, E.; Giardini, O. Abnormal intestinal permeability in children with autism. Acta Paediatr. 1996, 85, 1076–1079. [Google Scholar] [CrossRef]
- de Magistris, L. , et al. , Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives. J Pediatr Gastroenterol Nutr 2010, 51, 418–424. [Google Scholar] [PubMed]
- Erickson, C.A.; Stigler, K.A.; Corkins, M.R.; Posey, D.J.; Fitzgerald, J.F.; McDougle, C.J. Gastrointestinal Factors in Autistic Disorder: A Critical Review. J. Autism Dev. Disord. 2005, 35, 713–727. [Google Scholar] [CrossRef] [PubMed]
- Horvath, K.; Perman, J.A. Autistic disorder and gastrointestinal disease. Curr. Opin. Pediatr. 2002, 14, 583–587. [Google Scholar] [CrossRef]
- Horvath, K.; Papadimitriou, J.C.; Rabsztyn, A.; Drachenberg, C.; Tildon, J. Gastrointestinal abnormalities in children with autistic disorder. J. Pediatr. 1999, 135, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Heijtz, R.D.; Wang, S.; Anuar, F.; Qian, Y.; Björkholm, B.; Samuelsson, A.; Hibberd, M.L.; Forssberg, H.; Pettersson, S. Normal gut microbiota modulates brain development and behavior. Proc. Natl. Acad. Sci. USA 2011, 108, 3047–3052. [Google Scholar] [CrossRef] [PubMed]
- Jyonouchi, H.; Geng, L.; Ruby, A.; Zimmerman-Bier, B. Dysregulated Innate Immune Responses in Young Children with Autism Spectrum Disorders: Their Relationship to Gastrointestinal Symptoms and Dietary Intervention. Neuropsychobiology 2005, 51, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Bjorklund, G. , et al. , Gastrointestinal alterations in autism spectrum disorder: What do we know? Neurosci Biobehav Rev 2020, 118, 111–120. [Google Scholar] [PubMed]
- Buie, T.; Campbell, D.B.; Fuchs, G.J., 3rd; Furuta, G.T.; Levy, J.; Vandewater, J.; Whitaker, A.H.; Atkins, D.; Bauman, M.L.; Beaudet, A.L.; et al. Evaluation, Diagnosis, and Treatment of Gastrointestinal Disorders in Individuals With ASDs: A Consensus Report. Pediatrics 2010, 125 (Suppl. 1), S1–S18. [Google Scholar] [CrossRef]
- Buie, T.; Fuchs, G.J., III; Furuta, G.T.; Kooros, K.; Levy, J.; Lewis, J.D.; Wershil, B.K.; Winter, H. Recommendations for Evaluation and Treatment of Common Gastrointestinal Problems in Children With ASDs. Pediatrics 2010, 125 (Suppl. 1), S19–S29. [Google Scholar] [CrossRef]
- Wasilewska, J.J.; Klukowski, M. Gastrointestinal symptoms and autism spectrum disorder: links and risks – a possible new overlap syndrome. Pediatr. Heal. Med. Ther. 2015, ume 6, 153–166. [Google Scholar] [CrossRef]
- Dasdag, S.; Akdag, M.Z.; Erdal, M.E.; Erdal, N.; Ay, O.I.; Ay, M.E.; Yilmaz, S.G.; Tasdelen, B.; Yegin, K. Effects of 2.4 GHz radiofrequency radiation emitted from Wi-Fi equipment on microRNA expression in brain tissue. Int. J. Radiat. Biol. 2015, 91, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Aldad, T.S.; Gan, G.; Gao, X.-B.; Taylor, H.S. Fetal Radiofrequency Radiation Exposure From 800-1900 Mhz-Rated Cellular Telephones Affects Neurodevelopment and Behavior in Mice. Sci. Rep. 2012, 2, 312. [Google Scholar] [CrossRef] [PubMed]
- GL, C. and M. TJ, Wireless radiation in the aetiology and treatment of autism: clinical observations and mechanisms. Journal of the Australasian College of Nutritional and Environmental Medicine, 2007.
- Herbert, M.R.; Sage, C. Autism and EMF? Plausibility of a pathophysiological link – Part I. Pathophysiology 2013, 20, 191–209. [Google Scholar] [CrossRef] [PubMed]
- Herbert, M.R.; Sage, C. Autism and EMF? Plausibility of a pathophysiological link part II. Pathophysiology 2013, 20, 211–234. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.C. A possible association between fetal/neonatal exposure to radiofrequency electromagnetic radiation and the increased incidence of Autism Spectrum Disorders (ASD). Med Hypotheses 2004, 62, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Pall, M.L. The Autism Epidemic Is Caused by EMFs, Acting via Calcium Channels and Chemicals Acting via NMDA-Rs: Downstream Effects Cause Autism in Autism One 2015.
- Pall, M.L. Microwave frequency electromagnetic fields (EMFs) produce widespread neuropsychiatric effects including depression. J. Chem. Neuroanat. 2016, 75, 43–51. [Google Scholar] [CrossRef]
- Pall, M.L. Wi-Fi is an important threat to human health. Environ. Res. 2018, 164, 405–416. [Google Scholar] [CrossRef]
- Thornton, I.M. Out of time: A possible link between mirror neurons, autism and electromagnetic radiation. Med Hypotheses 2006, 67, 378–382. [Google Scholar] [CrossRef]
- Mazzone, L.; Dooling, S.W.; Volpe, E.; Uljarević, M.; Waters, J.L.; Sabatini, A.; Arturi, L.; Abate, R.; Riccioni, A.; Siracusano, M.; et al. Precision microbial intervention improves social behavior but not autism severity: A pilot double-blind randomized placebo-controlled trial. Cell Host Microbe 2024, 32, 106–116. [Google Scholar] [CrossRef]
- Pearson, D.A.; Hendren, R.L.; Heil, M.F.; McIntyre, W.R.; Raines, S.R. Pancreatic Replacement Therapy for Maladaptive Behaviors in Preschool Children With Autism Spectrum Disorder. JAMA Netw. Open 2023, 6, e2344136–e2344136. [Google Scholar] [CrossRef]
- Ghalichi, F.; Ghaemmaghami, J.; Malek, A.; Ostadrahimi, A. Effect of gluten free diet on gastrointestinal and behavioral indices for children with autism spectrum disorders: a randomized clinical trial. World J. Pediatr. 2016, 12, 436–442. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Sanders, D.S.; Grünewald, R.A.; Woodroofe, N.; Boscolo, S.; Aeschlimann, D. Gluten sensitivity: from gut to brain. Lancet Neurol. 2010, 9, 318–330. [Google Scholar] [CrossRef]
- Hsu, C.-L.; Lin, C.-Y.; Chen, C.-L.; Wang, C.-M.; Wong, M.-K. The effects of a gluten and casein-free diet in children with autism: a case report. . 2009, 32, 459–65. [Google Scholar]
- Lionetti, E.; Leonardi, S.; Franzonello, C.; Mancardi, M.; Ruggieri, M.; Catassi, C. Gluten Psychosis: Confirmation of a New Clinical Entity. Nutrients 2015, 7, 5532–5539. [Google Scholar] [CrossRef]
- Madra, M.; Ringel, R.; Margolis, K.G. Gastrointestinal Issues and Autism Spectrum Disorder. Psychiatr. Clin. North Am. 2021, 44, 69–81. [Google Scholar] [CrossRef]
- Marí-Bauset, S.; Llopis-González, A.; Zazpe, I.; Marí-Sanchis, A.; Suárez-Varela, M.M. Nutritional Impact of a Gluten-Free Casein-Free Diet in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 46, 673–684. [Google Scholar] [CrossRef]
- Piwowarczyk, A.; Horvath, A.; Pisula, E.; Kawa, R.; Szajewska, H. Gluten-Free Diet in Children with Autism Spectrum Disorders: A Randomized, Controlled, Single-Blinded Trial. J. Autism Dev. Disord. 2019, 50, 482–490. [Google Scholar] [CrossRef]
- Quan, L.; Xu, X.; Cui, Y.; Han, H.; Hendren, R.L.; Zhao, L.; You, X. A systematic review and meta-analysis of the benefits of a gluten-free diet and/or casein-free diet for children with autism spectrum disorder. Nutr. Rev. 2021, 80, 1237–1246. [Google Scholar] [CrossRef]
- Whiteley, P.; Haracopos, D.; Knivsberg, A.-M.; Reichelt, K.L.; Parlar, S.; Jacobsen, J.; Seim, A.; Pedersen, L.; Schondel, M.; Shattock, P. The ScanBrit randomised, controlled, single-blind study of a gluten- and casein-free dietary intervention for children with autism spectrum disorders. Nutr. Neurosci. 2010, 13, 87–100. [Google Scholar] [CrossRef]
- Blaylock, R.L.; Strunecka, A. Immune-Glutamatergic Dysfunction as a Central Mechanism of the Autism Spectrum Disorders. Curr. Med. Chem. 2009, 16, 157–170. [Google Scholar] [CrossRef]
- Ghanizadeh, A. Increased Glutamate and Homocysteine and Decreased Glutamine Levels in Autism: A Review and Strategies for Future Studies of Amino Acids in Autism. Dis. Markers 2013, 35, 281–286. [Google Scholar] [CrossRef]
- Brown, M.S. , et al. , Increased glutamate concentration in the auditory cortex of persons with autism and first-degree relatives: a (1)H-MRS study. Autism Res 2013, 6, 1–10. [Google Scholar]
- Choudhury, P.R.; Lahiri, S.; Rajamma, U. Glutamate mediated signaling in the pathophysiology of autism spectrum disorders. Pharmacol. Biochem. Behav. 2012, 100, 841–849. [Google Scholar] [CrossRef]
- Tzang, R.-F.; Chang, C.-H.; Chang, Y.-C.; Lane, H.-Y. Autism Associated With Anti-NMDAR Encephalitis: Glutamate-Related Therapy. Front. Psychiatry 2019, 10, 440. [Google Scholar] [CrossRef]
- Watkins, J.C. and D.E. Jane, The glutamate story. Br J Pharmacol 2006, 147 Suppl 1(Suppl 1): S100-8.
- Dyńka, D.; Kowalcze, K.; Paziewska, A. The Role of Ketogenic Diet in the Treatment of Neurological Diseases. Nutrients 2022, 14, 5003. [Google Scholar] [CrossRef]
- El-Rashidy, O.; El-Baz, F.; El-Gendy, Y.; Khalaf, R.; Reda, D.; Saad, K. Ketogenic diet versus gluten free casein free diet in autistic children: a case-control study. Metab. Brain Dis. 2017, 32, 1935–1941. [Google Scholar] [CrossRef]
- Gough, S.M.; Casella, A.; Ortega, K.J.; Hackam, A.S. Neuroprotection by the Ketogenic Diet: Evidence and Controversies. Front. Nutr. 2021, 8. [Google Scholar] [CrossRef]
- Lee, R.W.Y.; Corley, M.J.; Pang, A.; Arakaki, G.; Abbott, L.; Nishimoto, M.; Miyamoto, R.; Lee, E.; Yamamoto, S.; Maunakea, A.K.; et al. A modified ketogenic gluten-free diet with MCT improves behavior in children with autism spectrum disorder. Physiol. Behav. 2018, 188, 205–211. [Google Scholar] [CrossRef]
- Li, Q.; Liang, J.; Fu, N.; Han, Y.; Qin, J. A Ketogenic Diet and the Treatment of Autism Spectrum Disorder. Front. Pediatr. 2021, 9. [Google Scholar] [CrossRef]
- Mu, C.; Corley, M.J.; Lee, R.W.Y.; Wong, M.; Pang, A.; Arakaki, G.; Miyamoto, R.; Rho, J.M.; Mickiewicz, B.; Dowlatabadi, R.; et al. Metabolic Framework for the Improvement of Autism Spectrum Disorders by a Modified Ketogenic Diet: A Pilot Study. J. Proteome Res. 2020, 19, 382–390. [Google Scholar] [CrossRef]
- Olivito, I. , et al. , Ketogenic diet ameliorates autism spectrum disorders-like behaviors via reduced inflammatory factors and microbiota remodeling in BTBR T(+) Itpr3(tf)/J mice. Exp Neurol 2023, 366, 114432. [Google Scholar]
- Stafstrom, C.E.; Rho, J.M. The Ketogenic Diet as a Treatment Paradigm for Diverse Neurological Disorders. Front. Pharmacol. 2012, 3, 59. [Google Scholar] [CrossRef]
- Smith, J.; Rho, J.M.; Teskey, G.C. Ketogenic diet restores aberrant cortical motor maps and excitation-to-inhibition imbalance in the BTBR mouse model of autism spectrum disorder. Behav. Brain Res. 2016, 304, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, D.; Kasperek, K.; Rękawek, P.; Piątkowska-Chmiel, I. The Therapeutic Role of Ketogenic Diet in Neurological Disorders. Nutrients 2022, 14, 1952. [Google Scholar] [CrossRef]
- Wu, D.-M.; Wen, X.; Han, X.-R.; Wang, S.; Wang, Y.-J.; Shen, M.; Fan, S.-H.; Zhuang, J.; Li, M.-Q.; Hu, B.; et al. Relationship Between Neonatal Vitamin D at Birth and Risk of Autism Spectrum Disorders: the NBSIB Study. J. Bone Miner. Res. 2017, 33, 458–466. [Google Scholar] [CrossRef]
- Patrick, R. and B. N. Ames, Vitamin D hormone regulates serotonin synthesis. Part 1: relevance for autism. FASEB J 2014, 28, 2398–2413. [Google Scholar]
- Rossignol, D.A.; Frye, R.E. Cerebral Folate Deficiency, Folate Receptor Alpha Autoantibodies and Leucovorin (Folinic Acid) Treatment in Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 1141. [Google Scholar] [CrossRef]
- Frye, R.E.; Rossignol, D.A.; Scahill, L.; McDougle, C.J.; Huberman, H.; Quadros, E.V. Treatment of Folate Metabolism Abnormalities in Autism Spectrum Disorder. Semin. Pediatr. Neurol. 2020, 35, 100835–100835. [Google Scholar] [CrossRef] [PubMed]
- Demarquoy, C.; Demarquoy, J. Autism and carnitine: A possible link. World J. Biol. Chem. 2019, 10, 7–16. [Google Scholar] [CrossRef]
- Malaguarnera, M. and O. Cauli, Effects of l-Carnitine in Patients with Autism Spectrum Disorders: Review of Clinical Studies. Molecules 2019, 24(23).
- Rossignol, D.A.; Frye, R.E. The Effectiveness of Cobalamin (B12) Treatment for Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 784. [Google Scholar] [CrossRef]
- Bramati-Castellarin, I.; Patel, V.B.; Drysdale, I.P. Repeat-measures longitudinal study evaluating behavioural and gastrointestinal symptoms in children with autism before, during and after visceral osteopathic technique (VOT). J. Bodyw. Mov. Ther. 2016, 20, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Wolf, K.; Widjaja, F.; O'Keefe, W.; Chen, Y.; Breard, M.; Parenteau, C.; Keys, J.; Riemer, R.; Hendren, R.L. Osteopathic manipulative treatment for autism spectrum disorder: Three case reports. Int. J. Osteopat. Med. 2024, 51. [Google Scholar] [CrossRef]
- Masgutova, S.; Masgutov, D.; Lieske, T. Effects of MNRI Visual Reflex Neuro-Training on Visual and Academic Skills of Children with Autism. Int. J. Sch. Cogn. Psychol. 2018, 05, 1–15. [Google Scholar] [CrossRef]
- Katarzyna Novak1*, P.S. , Wojciech Sobaniec1, Nelli Akhmatova2, and Patty Shackleford3, Evaluation of the Therapeutic Effect of MNRI Reflex Neuromodulation on Children Diagnosed with Autism Based on Reflex Assessments, QEEG Analysis and ATEC Questionnaire. Journal of Neurology and Neurobiology 2020, 6(2).
- Sk, M.; Nk, A.; L, S.; P, S.; Ea, A. Neurosensorimotor Reflex Integration for Autism: a New TherapyModality Paradigm. J. Pediatr. Neurol. Disord. 2016, 2. [Google Scholar] [CrossRef]
- Ruggeri, A.; Dancel, A.; Johnson, R.; Sargent, B. The effect of motor and physical activity intervention on motor outcomes of children with autism spectrum disorder: A systematic review. Autism 2019, 24, 544–568. [Google Scholar] [CrossRef] [PubMed]
- Y, L. , et al., The Effects of Physical Activity Interventions in Children with Autism Spectrum Disorder: a Systematic Review and Network Meta-analysis. Rev J Autism Dev Disord, 2023.
- Atun-Einy, O.; Lotan, M.; Harel, Y.; Shavit, E.; Burstein, S.; Kempner, G. Physical Therapy for Young Children Diagnosed with Autism Spectrum Disorders–Clinical Frameworks Model in an Israeli Setting. Front. Pediatr. 2013, 1, 19. [Google Scholar] [CrossRef] [PubMed]
- O'Hara, N.H.; Szakacs, G.M. The recovery of a child with autism spectrum disorder through biomedical interventions. . 2008, 14, 42–4. [Google Scholar] [PubMed]
- Graz, M.B.; Monnier, M.; Tschudin, L.v.L.; Truttmann, A.C. Normal neurodevelopmental outcome despite severe and early extensive encephalomalacia: plasticity, repair or magic? Dev. Med. Child Neurol. 2013, 55, 868–869. [Google Scholar] [CrossRef]
- Fein, D.; Barton, M.; Eigsti, I.; Kelley, E.; Naigles, L.; Schultz, R.T.; Stevens, M.; Helt, M.; Orinstein, A.; Rosenthal, M.; et al. Optimal outcome in individuals with a history of autism. J. Child Psychol. Psychiatry 2013, 54, 195–205. [Google Scholar] [CrossRef]
- Riley DS, B.M. , Kienle GS, Aronson JK, von Schoen-Angerer T, Tugwell P, Kiene H, Helfand M, Altman DG, Sox H, Werthmann PG, Moher D, Rison RA, Shamseer L, Koch CA, Sun GH, Hanaway P, Sudak NL, Kaszkin-Bettag M, Carpenter JE, Gagnier JJ, CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol 2017, 89, 218–235. [Google Scholar]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development. Glob. Adv. Heal. Med. 2013, 2, 38–43. [Google Scholar] [CrossRef]
- Matuszkiewicz, M.; Gałkowski, T. Developmental Language Disorder and Uninhibited Primitive Reflexes in Young Children. J. Speech, Lang. Hear. Res. 2021, 64, 935–948. [Google Scholar] [CrossRef]
- Hessl, D.; Libero, L.; Schneider, A.; Kerns, C.; Winder-Patel, B.; Heath, B.; Lee, J.; Coleman, C.; Sharma, N.; Solomon, M.; et al. Fear Potentiated Startle in Children With Autism Spectrum Disorder: Association With Anxiety Symptoms and Amygdala Volume. Autism Res. 2020, 14, 450–463. [Google Scholar] [CrossRef]
- Ebishima, K.; Takahashi, H.; Stickley, A.; Nakahachi, T.; Sumiyoshi, T.; Kamio, Y. Relationship of the Acoustic Startle Response and Its Modulation to Adaptive and Maladaptive Behaviors in Typically Developing Children and Those With Autism Spectrum Disorders: A Pilot Study. Front. Hum. Neurosci. 2019, 13, 5. [Google Scholar] [CrossRef]
- IntellxxDNA. Available from: https://intellxxdna.com/.
- Organic Acids Test (OAT). [cited 2024 ]; Available from: https://mosaicdx.com/test/organic-acids-test/. 28 March.
- Metals – Toxic + Nutrient Elements – Hair. [cited 2024 ]; Available from: https://mosaicdx.com/test/metals-hair-test/. 28 March.
- NutrEval: A Comprehensive Profile for Identifying Nutritional Deficiencies and Indufficiencies. [cited 2024 ]; Available from: https://www.gdx.net/products/nutreval. 28 March.
- IgG Food MAP with Candida + Yeast. [cited 2024 ]; Available from: https://mosaicdx.com/test/igg-food-map/. 28 March.
- Comprehensive Stool Analysis. [cited 2024 ]; Available from: https://mosaicdx.com/test/comprehensive-stool-analysis/. 28 March.
- MycoTOX Profile. [cited 2024 ]; Available from: https://mosaicdx.com/test/mycotox-profile/. 28 March.
- Bradstreet, J.J.; Smith, S.; Baral, M.; A Rossignol, D. Biomarker-guided interventions of clinically relevant conditions associated with autism spectrum disorders and attention deficit hyperactivity disorder. . 2010, 15, 15–32. [Google Scholar]
- Alabdali, A.; Al-Ayadhi, L.; El-Ansary, A. Association of social and cognitive impairment and biomarkers in autism spectrum disorders. J. Neuroinflammation 2014, 11, 4–4. [Google Scholar] [CrossRef]
- Goldani, A.A. , et al. , Biomarkers in autism. Front Psychiatry 2014, 5, 100. [Google Scholar]
- Ruggeri, B.; Sarkans, U.; Schumann, G.; Persico, A.M. Biomarkers in autism spectrum disorder: the old and the new. Psychopharmacology 2013, 231, 1201–1216. [Google Scholar] [CrossRef]
- Ranjbar, A.; Rashedi, V.; Rezaei, M. Comparison of urinary oxidative biomarkers in Iranian children with autism. Res. Dev. Disabil. 2014, 35, 2751–2755. [Google Scholar] [CrossRef] [PubMed]
- Kałużna-Czaplińska, J.; Żurawicz, E.; Struck, W.; Markuszewski, M. Identification of organic acids as potential biomarkers in the urine of autistic children using gas chromatography/mass spectrometry. J. Chromatogr. B 2014, 966, 70–76. [Google Scholar] [CrossRef] [PubMed]
- James, S.J.; Cutler, P.; Melnyk, S.; Jernigan, S.; Janak, L.; Gaylor, D.W.; Neubrander, J.A. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am. J. Clin. Nutr. 2004, 80, 1611–1617. [Google Scholar] [CrossRef] [PubMed]
- Howsmon, D.P.; Vargason, T.; Rubin, R.A.; Delhey, L.; Tippett, M.; Rose, S.; Bennuri, S.C.; Slattery, J.C.; Melnyk, S.; James, S.J.; et al. Multivariate techniques enable a biochemical classification of children with autism spectrum disorder versus typically-developing peers: A comparison and validation study. Bioeng. Transl. Med. 2018, 3, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Frustaci, A.; Neri, M.; Cesario, A.; Adams, J.B.; Domenici, E.; Bernardina, B.D.; Bonassi, S. Oxidative stress-related biomarkers in autism: Systematic review and meta-analyses. Free. Radic. Biol. Med. 2012, 52, 2128–2141. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-O.; Wang, J.-L.; Bjørklund, G.; Zhao, W.-N.; Yin, C.-H. Serum copper and zinc levels in individuals with autism spectrum disorders. NeuroReport 2014, 25, 1216–1220. [Google Scholar] [CrossRef] [PubMed]
- Ratajczak, H.V. Theoretical aspects of autism: biomarkers—a review. J. Immunotoxicol. 2010, 8, 80–94. [Google Scholar] [CrossRef] [PubMed]
- Kordulewska, N.K.; Kostyra, E.; Piskorz-Ogórek, K.; Moszyńska, M.; Cieślińska, A.; Fiedorowicz, E.; Jarmołowska, B. Serum cytokine levels in children with spectrum autism disorder: Differences in pro- and anti-inflammatory balance. J. Neuroimmunol. 2019, 337, 577066. [Google Scholar] [CrossRef] [PubMed]
- El-Ansary, A.; Al-Ayadhi, L. Lipid mediators in plasma of autism spectrum disorders. Lipids Heal. Dis. 2012, 11, 160–160. [Google Scholar] [CrossRef]
- Brown, C.M.; Austin, D.W.; Busija, L. Observable essential fatty acid deficiency markers and autism spectrum disorder. . 2014, 22, 21–6. [Google Scholar] [PubMed]
- Autism Parenting Secrets. 2024 [cited 2024 ]; Available from: https://autismparentingsecrets.com/. 28 March.
- McEwen, B.S. Stress, Adaptation, and Disease: Allostasis and Allostatic Load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef]
- Lemer, P.S. , Outsmarting Autism, Updated and Expanded. 2019: North Atlantic Books.
- Condon, E.M. Chronic Stress in Children and Adolescents: A Review of Biomarkers for Use in Pediatric Research. Biol. Res. Nurs. 2018, 20, 473–496. [Google Scholar] [CrossRef]
- Li, J.; Yu, Y.; Yuan, J.; Liu, D.; Fang, J.; Wu, P.; Zhou, Y.; Wang, Y.; Sun, Y. Association between early life adversity and allostatic load in girls with precocious puberty. Psychoneuroendocrinology 2023, 152, 106101. [Google Scholar] [CrossRef]
- CHIRP Study [cited 2024]; Available from: https://documentinghope.com/chirp-study/. 28 March.
- Healing Together. [cited 2024 ]; Available from: https://healing.documentinghope.com/welcome/. 28 March.
- Unblind my Mind. 2024 [cited 2024 ]; Available from: https://unblindmymind.org/. 28 March.
- C. , B., et al., The Effect of the MNRI Method on Neurotransmitter Biomarkers of Individuals with Neurodevelopmental Disorders. Neuroscience and Medicine 2019, 10, 292–321.
- S, M. , Reflex Integration Disorder as a New Treatment Paradigm for Children with Autism. Svetlana Masgutova Educational Institute® for Neuro-Sensory-Motor and Reflex Integration, 2015.
- T., D. T., D., et al., Physiological Markers and Reflex Pattern Progression in Individuals with Neurodevelopmental Deficits Utilizing the MNRI Method. Neuroscience & Medicine 2019, 10(1).
- S, M. , et al., Progress with Neurosensorimotor Reflex Integration for Children with Autism Spectrum Disorder. Journal of Neurology and Psychology 2016, 4(2).
- Building Biology Environmental Consultant™ (BBEC). 2024 [cited 2024 ]; Available from: https://buildingbiologyinstitute.org/certifications/building-biology-environmental-consultant-bbec/. 28 March.
- Edelson, S. and B. Rimland. Autism Treatment Evaluation Checklist (ATEC). 1999; Available from: https://www.autism.org/autism-treatment-evaluation-checklist/.
- Magiati, I. , et al. , Is the Autism Treatment Evaluation Checklist a useful tool for monitoring progress in children with autism spectrum disorders? J Intellect Disabil Res 2011, 55, 302–312. [Google Scholar]
- Caker, J. et al, The lifetime social cost of autism: 1990–2029. Research in Autism Spectrum Disorders, 2020.
- Fernandes, F.D. & C. A. Amato, Applied behavior analysis and autism spectrum disorders: literature review. Codas 2013, 25, 289–296. [Google Scholar]
- Roane, H.S.; Fisher, W.W.; Carr, J.E. Applied Behavior Analysis as Treatment for Autism Spectrum Disorder. J. Pediatr. 2016, 175, 27–32. [Google Scholar] [CrossRef]
- Mesleh, A.G.; Abdulla, S.A.; El-Agnaf, O. Paving the Way toward Personalized Medicine: Current Advances and Challenges in Multi-OMICS Approach in Autism Spectrum Disorder for Biomarkers Discovery and Patient Stratification. J. Pers. Med. 2021, 11, 41. [Google Scholar] [CrossRef]
- Leaf, J.B.; Cihon, J.H.; Leaf, R.; McEachin, J.; Liu, N.; Russell, N.; Unumb, L.; Shapiro, S.; Khosrowshahi, D. Concerns About ABA-Based Intervention: An Evaluation and Recommendations. J. Autism Dev. Disord. 2021, 52, 2838–2853. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



