
Submitted:
01 May 2024
Posted:
02 May 2024
You are already at the latest version
Abstract
Patients with Peripheral-artery-disease (PAD) are prone to risks of major-adverse-limb-events (MALE), and major-adverse-cardiovascular-events (MACE). CHA2DS2-VASc is a prognostic score for Atrial fibrillation stroke risk, however, no study exists that evaluated its predictability for MALE and MACE in PAD patients. In this study, patients with PAD were stratified into four risk groups based on CHA2DS2-VASc score. Cox-proportional hazards models,10-fold cross-validation and Receiver operating characteristic (ROC) analyses were utilized to evaluate the predictability of CHA2DS2-VASc for predicting MALE, MACE, and MALE+MACE. Kaplan-Meier analysis estimated the survival-probability of risk-groups. CHA2DS2-VASc was found to be a significant predictor of MACE (hazard ratio (95% confidence interval; P) = 3.47 (0.99 - 12.18; 0.052), 4.12 (1.19 - 14.14; 0.024), and 5.06 (1.48 – 17.28; 0.009), for moderate-, high- and very-high-risk groups, respectively, while for MALE and MALE+MACE significance was achieved only for high-risk group. MACE demonstrated AUC > 0.8, good-discrimination (c-index > 0.8) and good-calibration. However, MALE and MALE+MACE models failed to achieve good performances. Based on all findings, CHA2DS2-VASc could potentially serve as a risk stratification score for predicting MACE in patients with PAD but failed to qualify as a good predictor for MALE.
Keywords:
Peripheral artery disease (PAD)
; modified cumulative risk (MCR) score
; CHA2DS2-VASc
; Major adverse cardiovascular events (MACE)
; Major adverse limb events (MALE)
; percutaneous coronary intervention (PCI)
1. Introduction
Lower extremity peripheral artery disease (PAD) has a high incidence, affecting more than 230 million people globally [1,2]. It is a condition that is characterized by stenosis or occlusion of the arteries, thus reducing flow of blood to the affected limb. People suffering from PAD are at a 10-15 times higher risk of major adverse cardiovascular events (MACE) [3] leading to mortality. It is further associated with extremely higher risks of major adverse limb events (MALE) due to extensive atherosclerosis (3), leading to tragic consequences, such as lower extremity amputation, acute limb ischemia (ALI), and death [4]. Adverse cardiovascular events are defined by events such as component heart failure, non-fatal re-infarction, hospitalization due to cardiovascular conditions, repeat percutaneous coronary intervention (PCI), coronary artery bypass grafting, unscheduled coronary revascularization, and all-cause mortality [5]. MALE comprises major amputations and peripheral re-vascularization with eventual morbidity [6,7].
CHA2DS2-VASc is a cumulative score that is based on predefined criteria where “C” stands for congestive heart failure (CHF), “H” for hypertension (HTN), “A2” for Age >75 (doubled), “D” for Diabetes Mellitus (DM), “S2” for Stroke (doubled), transient ischemic attack or thromboembolism, “V” for Vascular disease, “A” for age range of 65-74 years old, and “Sc” for Sex category (Female), which is a commonly used score for risk stratification of strokes in patients with atrial fibrillation (AF) and is used to assist decision-making regarding anticoagulation therapy for stroke prophylaxis [8,9]. In recent studies CHA2DS2-VASc has been demonstrated to be a predictor of adverse clinical outcomes associated with coronary artery disease, stroke, and other cardiovascular conditions regardless of AF. A study reported that CHA2DS2-VASc score had a high correlation with mortality in PAD patients and may therefore be useful as a predictor for identification of high-risk patients [10]. However, there have been no studies to date to evaluate and validate the predictability of CHA2DS2-VASc for MALE and MACE in PAD patients. This study utilized a modified CHA2DS2-VASc score, for predicting the risk of incidence of MACE, MALE, and MALE+MACE in patients with PAD from Taiwan. A comprehensive analysis was conducted to evaluate the feasibility and efficacy of the predictive ability of CHA2DS2-VASc score for MALE and MACE outcomes in patients with PAD towards. CHA2DS2-VASc has been a score that has been proven to have clinical applicability for stroke risk stratification in AF. Whether it can be used for MALE and MACE risk stratification of patients with PAD who has undergone PCI, is the aim of this study. It is an important research question, that remains to be answered which would contribute important information to the literature.
2. Methods
2.1. Data Description
Demographic data along with medical history (clinical, survival information, laboratory test results, and medications at admission) of 601 Taiwanese subjects with and without PAD were obtained from Taichung Veterans General Hospital. Participants were enrolled from 2015 through 2020, and were followed up until April 2022 with a median follow-up period of 662 days. Patients with the following criteria were excluded from the study: (i) Patients aged <18 and >85 years old, (ii) pregnant women, (iii) patients with any cancer, (iv) patients with any infection (except local wound infection at lower limbs) at the time of recruitment, (v) patients with all extremity artery diseases (except lower extremity artery disease), and (vi) patients with missing information on PAD (Figure 1). Only 503 patients with PAD were included for analyses in this study. Patients were considered to have PAD if they exhibited unhealed wound or gangrene, stenting and clinical presentation, such as ankle brachial index (ABI)<0.9, critical limb ischemia, intermittent claudication, resting pain, trophic changes, previous percutaneous transluminal angioplasty (PTA) or Rutherford classifications 1-6 (Table 1 and Table S1), which is a classification system widely applied for classifying PAD patients.
Other diagnostic, clinical, and environmental factors were available for all PAD patients, defined as follows: smoking history classified as ever- and never-smokers, where ever-smokers were smokers who quit or were current smokers; ≧10 cigarettes a day for at least 1 year without an attempt to quit; with or without hyperlipidemia (HPL), based on a predefined low-density lipoprotein (LDL) cholesterol threshold set by the National Cholesterol Education program (<70 mg/dl for PAD patients; and <55 mg/dl for coronary artery disease (CAD) patients) [11], whether or not on lipid-lowering medications, and/or newly diagnosed patients at the time of hospitalization; history of CAD; history of coronary artery bypass graft (CABG), history of percutaneous cardiac intervention (PCI), history of old myocardial infarction (MI), history of chronic obstructive pulmonary disease (COPD), history of chronic kidney disease (CKD) with a creatinine clearance test threshold value of CCr.: <60ml/min, history of hemodialysis (HD) or peritoneal dialysis (PD), history of atrial fibrillation (AF), history of autoimmune disease, information on blood marker levels, such as glycated hemoglobin (HbA1C), cholesterol, LDL, high-density lipoprotein (HDL) cholesterol, triglyceride (TG), and glucose. Information on medications were also included, such as aspirin (ASA), clopidgrel, cilostazol, pentoxyphilline, warfarin or direct oral anticoagulant (DOAC), angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB), statin, betablocker, calcium channel blockers (CCB), and insulin.
The study has been approved by the institutional review board of Taichung Veterans General Hospital (TCVGH-IRB #: CE21519A). All research was performed in accordance with relevant guidelines/regulations of the ethical committee. It is a retrospective study and therefore patients consent was not required. The IRB committee I &II of Taichung Veterans General Hospital waived the need for the requirement of informed consent. The patient information was de-identified and the authors had no access to the information that could identify individual participants during or after data collection. The data was accessed on July 1, 2022 for this research.
2.2. Endpoints and Events
The baseline time–point of the study was set at the primary intervention for all patients with PAD. The primary intervention consisted of PTA, which involved a balloon insertion followed by its inflation to unclog the artery, thus allowing blood flow in the lower limbs of the patients suffering from PAD. Patients were followed up from primary intervention up until three endpoints: (1) MALE, (2) MACE, and (3) MALE and MACE. MALE was characterized by repeat vascularization or amputation. MACE was characterized by non-fatal stroke, nonfatal myocardial infarction or cardiovascular death. All patients’ information was followed up by telephone, medical chart and clinical visit regarding non-fatal myocardial infarction.
2.3. Statistical Analysis
2.3.1. Modified CHA2DS2-VASc Risk (MCR) Score
First, the traditional CHA2DS2-VASc score of all patients was calculated using the standard criteria by summing up the abnormalities as depicted by the score. The abnormalities were defined based on whether the patients had one or more of the following: CHF defined via chart review; ICD-code diagnosis; and echocardiographic ejection fraction, HTN with a systolic blood pressure ≧ 140mmHg, diastolic blood pressure ≧ 90mmHg or on HTN medication, age ≥75 years, DM with either a prior diagnosis or recorded fasting blood sugar level ≧ 126mg/dl, on anti-DM medication or newly diagnosed at the time of hospitalization, previous stroke, vascular disease defined as having PTA, age 65-74 years, and female gender. In this study, the CHA2DS2-VASc ranged from 0-9 for the study cohort, with very few patients demonstrating scores 0, 1, 2, 3, 7, 8, and 9. Therefore, to avoid bias and obtain a better distribution of risk scores, we used a modified CHA2DS2-VASc score (which, for convenience purposes will be referred to as MCR from here on) that ranged between 3 and 6 by redefining the patients with 3 or less abnormalities as low-risk patients (MCR = 3), and those with 6 or more abnormalities as very high-risk patients (MCR = 6). The two intermediate groups were defined as moderate risk (MCR = 4) and high-risk patients (MCR = 5), respectively (Figure S1). The predictive ability of MCR for events such as MACE, MALE, MALE + MACE were evaluated in this study.
2.3.2. Statistical Analysis Using CHA2DS2-VASc Risk Score as Predictor
Cox-Proportional hazards regression models were fitted with MCR as predictor in this study. Univariate and multivariate adjusted regression analyses were performed for the following outcomes: (i) MALE, (ii) MACE and, (iii) MALE+MACE. Baseline variables such as hyperlipidemia, chronic obstructive pulmonary disease (COPD), chronic kidney disease, cardiac rehabilitation, and atrial fibrillation were selected based on the demographic analysis where only the variants that were significant across groups of event and no-even were used as covariates for the adjusted multivariate models, respectively, for MALE, MACE and MALE+MACE. Cox proportional hazards models [12] were employed using the “Survival” package in R to estimate the hazard ratio and the corresponding 95% confidence intervals (CI) [13]. Kaplan Meier analyses were conducted for all events to estimate the effect of MCR score on the survival probability using the “survival” package in R [13,14].
2.3.3. Model Evaluation
A 10-fold internal cross-validation was performed to conduct model discrimination and model calibration analyses for evaluation of the performances of the proposed models [15,16,17]. As the models were developed with a small hospital based cohort of patients from Taiwanese ancestry, evaluating the model’s performance was necessary to judge its efficacy. Harrell’s c-index for discrimination analysis [16], which evaluates the concordance of predicted and observed survival and calibration analysis, was conducted to compare the observed and predicted events over all study subjects, by a given follow-up time. A random split of all study subjects using a 9:1 ratio for training and testing sets, respectively, was performed for 10 repetitions. We further compared our MCR score-based models with traditional baseline models, but instead of using the MCR score, we utilized the traditional variables, such as CHF, HTN, DM, stroke, vascular disease, age, and sex to predict the outcomes. Average of c-indices across all 10 cross-validations were utilized for evaluating the proposed models’ performances. All of the above were performed for all three outcomes: (i) MALE, (ii) MACE, and (iii) MALE+ MACE. “Survival” package in R was used to conduct all analyses [13]. Furthermore, to evaluate the predictive ability of CHA2DS2-VASc risk score, R-package, “timeROC” was used to conduct receiver operating characteristic (ROC) analysis for MALE, MACE and MALE+MACE at time points of 12 months, 24 months, 36 months and 48 months, respectively and area under curves (AUC) were obtained.
3. Results
3.1. Baseline Demographic and Clinico-Pathologic Variable Analysis
A total of 503 patients from a Taiwanese hospital cohort with PAD were included in this study. Patients with missing information (3 patients) and those without PAD were excluded from the study (Figure 1). Table 1 provides a detailed account of the demographic and clinical characteristics of all patients included in the study analysis. Additionally, a detailed analysis was done using all baseline demographic and clinical variables for PAD patients across the three study endpoints to see if the association of MCR with the incidence of the outcomes was affected by any confounders (Tables S2 and S3). Older PAD patients with MACE had a mean age of 71.75 years, compared with 69.83 years for those with MALE; the mean age of patients with MACE was higher than that of patients without MACE, while the mean age of MALE patients was slightly lower than that of those without MALE. Furthermore, patients demonstrating MACE had a significantly higher proportion of CHF, HTN, and DM when compared to patients without MACE, but the trend was reversed in cases with a MALE event. Hyperlipidemia was observed in a significantly higher number of patients with MACE (P = 0.05) outcomes when compared against those with no event. Smoking (ever) was observed to be correlated in direct proportion to MACE occurrence (46.93% (MACE); 37.83% (no MACE)), but was inversely and proportionally correlated with MALE. Occurrence of other clinical characteristics, such as CAD, CABG, PCI, Old MI, COPD, CKD, and AF was significantly greater in PAD patients with MACE (P<0.0001) in comparison to those without MACE, but the occurrence was low in patients with MALE as compared with their non-MALE counterparts. Autoimmune diseases were less prevalent or absent in patients with MALE and MACE, respectively. Mean ± standard deviation (SD) of all diagnostic blood markers are provided in Table 1; no blood markers were significantly different between MACE and non-MACE, and except for HbA1C (P=0.001) and glucose levels (P=0.02), none showed a significant difference between MALE and non-MALE. Medication usage was also not significantly different among all of the groups with and without events.
3.2. Modified CHA2DS2-VASc Risk (MCR) Score and Its Association with the Three Endpoints: MALE, MACE and MALE+MACE
All patients were stratified based on MCR scores and Table 2 summarizes the baseline characteristics of patients classified according to each of the MCR scores 3, 4, 5, and 6. The mean age of PAD patients increased with higher risk groups (59.14, 67.76, 72.2, and 79.6 years for MCR = 3, 4, 5 and 6, respectively). Increasing numbers of males were observed for groups with higher risks. CHF, HTN, DM, stroke, and vascular diseases all showed a rising trend with higher MCR score. Prevalence of hyperlipidemia and ever-smokers was higher among low-risk groups in comparison to high-risk groups.
Furthermore, for the MCR scores, the proportion of events were explored to understand their associations with MALE, MACE, and MALE + MACE events, as displayed in Figure 2. For MACE patients, a higher number of abnormalities was correlated with a slightly higher proportion of events (3%, 11.3%, 11.43%, and 11.49%); however, it was slightly different for the other two events, MALE (31%, 42.6%, 45%, 33.8%) and MALE+MACE (34%, 49.6%, 50%, 42.6%), where a minimum number of events was observed in PAD patients defined as low-risk (≤3 abnormalities) followed by medium-risk (4 abnormalities) and high-risk (6 abnormalities). Nonetheless, there was a slight dip in the proportion of events for the individuals with the highest number of abnormalities (≥ 6 or more). The corresponding HR and 95%CI are demonstrated via the forest plot in Figure 2
Kaplan-Meier analysis using MCR as the predictor for time-to-event was conducted for all three outcomes, for a maximum follow-up period of 56.5 months (minimum follow-up: 5 days; mean follow-up period: 449 days). Figure 3b shows that for event MACE, the low-risk group (MCR=3) demonstrated the best time-to-event, followed by the moderate-risk, high-risk, and very high-risk groups. Log rank test displayed significance with a P-value of 0.043. For the events MALE (Figure 3a) and MALE +MACE (Figure 3c), MCR was not found to attain significance (P= 0.22 and 0.18, respectively) for inferring time-to-event.
The above findings indicate that MCR could potentially act as a stratification score for identifying PAD patients that could be at a risk of MACE but the results for MALE and MALE+MACE were not encouraging enough.
3.3. Survival Analysis with Modified CHA2DS2-VASc Risk (MCR) Score as Predictor
Univariate and multivariate adjusted Cox proportional hazards regression was performed using MCR score as the predictor for endpoints MALE, MACE, and MALE + MACE. The results are summarized in Table 3.
MCR score was found to be a significant predictor of MACE using the univariate regression analysis with HR (95% CI; P-value) to be 3.47 (0.99 - 12.18; 0.05), 4.12 (1.19 - 14.14; 0.02), and 5.06 (1.48 - 17.28; 0.009) for moderate-risk, high-risk, and very high-risk groups, respectively (Table 3). For the multivariate adjusted regression analysis, significance was only observed with HR (95% CI; P-value) to be 3.72 (0.75 - 18.42) for very high-risk group, while no significance was observed for moderate risk and high risk groups. The c-index values for predicting MACE were 0.61, and 0.825, suggesting a good fit and a good discrimination ability for predicting MACE events.
For the MALE outcome, MCR was a significant predictor only for the high-risk group using both univariate and multivariate regression analysis; univariate (1.55 (1.01 - 2.38; 0.046), and multivariate adjusted (1.82 (1.04 - 3.2; 0.037) (Table 3). There was no significance observed for the moderate-risk and the very high-risk groups. The c-indices were also 0.54, and 0.56, respectively, demonstrating poor discrimination ability. Similarly, for the MALE+MACE outcome, both the univariate and multivariate adjusted regression demonstrated that MCR could significantly predict only the high-risk group (Table 3). Moreover, the c-indices were 0.54, and 0.58, respectively, showing poor discrimination ability.
3.4. Evaluation of MCR as a Legitimate Predictor for MALE, MACE and MALE+MACE
An internal validation was conducted, due to the lack of an independent dataset for validation, using a 10-fold cross-validation process to confirm the predictive performance of the MCR score and to confirm its reproducibility [15]. Also, the MCR-based regression models’ predictions were compared with traditional models that used clinical parameters directly instead of the cumulative score. This was done to determine whether using MCR as the predictor demonstrated any improvement over the traditional methods. Table 4 lists the average and the standard deviations of the c-indices over all 10CVs for all three regression models for MALE, MACE, and MALE+MACE. The results provide evidence that for a given patient pair, MCR can effectively discriminate the occurrence of MACE events, which indicates it to be a good predictor. However, the discrimination power of MCR for MALE and MALE+MACE were not good enough.
Next, calibration analyses were conducted using 10CV for each of the 5 years for all models. The difference between the proportions for the predicted and observed events were averaged and plotted for MCR models in comparison to the traditional model. For MACE, the differences of the proportions between observed and predicted for both MCR and traditional models were ≤5% for the first 2 years, and for the years 3-5 were restricted to <10%, while for both MACE and MALE, the average of differences was quite high (33-49%), except for year 1 (<5%). Figure 4 shows the results of the calibration analysis. Tables S4–S9 further tabulates the detailed calibration results. Results for the univariate models were very similar to those of the multivariate-adjusted models (results not shown).
Further evaluation of the prediction performance of MCR was conducted using ROC analysis for predicting MALE, MACE and MALE+MACE at time points of 12months, 24 months, 36 months and 48 months, respectively (Figure 5). For outcome MACE, the univariate model and the multivariate adjusted model demonstrated a maximum AUC of ~0.66 and ~0.85 for time points 48 months and 12 months, respectively (Figure 5B,E), while for the both outcomes MALE and MALE+MACE the univariate model demonstrated AUCs of <0.6 (Figure 5A,C) for all time points whereas the maximum AUC for multivariate models was ~0.65 for time points >36 months (Figure 5D,F). Based on all of our findings, we can fairly say that CHA2DS2-VASc can be claimed as a good predictor of MACE but doesn’t qualify as a legitimate predictor of MALE and MALE+MACE for patients with PAD.
4. Discussion
Peripheral artery disease is a narrowing of the peripheral arteries that carry blood away from the heart to other parts of the body and is associated with high rates of cardiovascular conditions and high rates of mortality [18]. A higher risk of cardiovascular events, MACE; and limb events, MALE; exist in patients with PAD [4]. Various classification systems utilizing anatomical, clinical, and images have been used for PAD in previous studies [18,19]. Recently, a scoring-based system, CHA2DS2-VASc, has been widely used for effective grading of patients, providing physicians with objective criteria for patient assessment, treatment, and clinical follow-up of PAD and cardiovascular conditions [20]. Classification systems are also important in determining medical, surgical, and percutaneous treatment preferences. This study utilized a modified version of the commonly used CHA2DS2-VASc score, MCR score, and conducted comprehensive analyses to test and confirm its ability to predict the risk of incidence of MACE and MALE in patients suffering from PAD. The most common type of PAD is lower-extremity PAD, in which blood flow is reduced to the legs and feet. Other forms of PAD, such as carotid artery stenosis, mesenteric artery stenosis, and upper-extremity PAD are less common and may require different therapeutic strategies. This study focused on lower-extremity PAD. Two regression models, univariate and multivariate adjusted model, with MCR as predictors were fitted for three outcomes; MALE, MACE, and MALE+MACE. MCR was demonstrated to be a significant predictor of MACE, with an approximate 4-fold, 4-fold, and 5-fold higher risk of MACE events for moderate-risk, high-risk, and very high-risk patients, respectively, compared with the low-risk reference group patients, in this study (Table 3). However, the performance of the MCR was not as convincing, for predicting events, MALE (significant only for the high-risk group) (Table 3) and MALE+MACE (significant only for high-risk group for the multivariate adjusted model) (Table 3). Discriminant analysis and calibration analysis were conducted using a 10-fold cross-validation, and AUC were calculated for predicting the events for different time points. All results indicated CHA2DS2-VASc to be a suitable predictor of MACE in patients with PAD, while demonstrating CHA2DS2-VASc to be not a good predictor of MALE and MALE+MACE.
CHADS2 score has been widely employed since 2001 for predicting risk of stroke in patients with atrial fibrillation (AF), and demonstrated worse stratification performance compared with CHA2DS2-VASc, which works better for identifying truly low-risk patients [21]. This could be justified by the high prevalence rates of peripheral vascular diseases (PVD) among AF patients, which were found to be associated with increased rates of mortality. Therefore, integrating PVD incidence within the risk score improved its risk stratification. Hence, CHA2DS2-VASc was a better score for conducing risk stratification for patients with AF. Although the initial purpose of the scoring system was to predict risk of stroke in AF patients, over time it has increasingly been used for various other stratification purposes. For instance, different studies have used the risk score for different cardiovascular conditions, such as sick sinus syndrome, thromboembolism, and stroke [20,22,23,24]. Other recent studies have demonstrated an association of CHA2DS2-VASc with risk of critical limb ischemia in peripheral arterial occlusive disease patients. Another recent study utilized CHA2DS2-VASc score to predict the risk of mortality in PAD patients with peripheral arteriography. Due to the skewed distribution of CHA2DS2-VASc score in our study cohort, a modified CHA2DS2-VASc risk score, MCR, was utilized in this study, which also demonstrated high predictive ability for MACE in all patients with PAD who underwent PTA, however failed to establish it as a good predictor for MALE.
PTA is a treatment strategy rendered to patients with lower extremity PAD in order to improve their lifestyle-hindering symptoms [23]. All of the patients included in this study demonstrated critical limb ischemia (CLI), and most of them had a long diffuse critical lesion in a leg vessel. The mainstay of treatment for CLI is to re-establish antegrade downstream flow in the leg. Therefore, most of the patients included in this study received revascularization of multi-region vessels. Usually, revascularization of an iliac lesion (common iliac artery + external iliac artery), femoropopliteal lesion (common femoral artery + superficial femoral artery +popliteal), or below-the-knee (BTK) lesion (peroneal + anterior tibial artery + tibioperoneal + posterior tibial artery + dorsalis pedis artery) is conducted concurrently, as it allows longer survival with an increased quality of life compared to patients undergoing primary amputation [25]. Dual antiplatelet therapy (DAPT) was implemented 1-3 months after PTA. The major reason was to cover the period of stent re-endothelialization. All patients with atrial fibrillation were on Warfarin /DOAC (direct oral anticoagulant) and >10 % patients were provided Warfarin/DOAC treatment in both the MALE and non-MALE groups, according to the physician’s judgment which was informed by reference data. This was done to balance the risk of ischemia and bleeding clinically. For identical reasons, anticoagulant management was also implemented in both the MACE group and non-MACE groups.
This study provides valuable insights to the applicability of the MCR for prediction of risk of limb events (MALE) and cardiovascular events (MACE) for PAD patients who underwent PTA, the information of which was missing in literature until now. The results for MALE were not significant and the performance of MCR as a predictor of MALE was not encouraging (low discrimination ability, poor calibration, and low AUC). Possible reasons could be that MALE events occurred in roughly 35% of patients within the first year and was thereafter stable due to wound healing involving multiple factors, such as nutrition status, infection control, and wound debridement. MCR, on the other hand, could successfully predict MACE with a high discrimination ability, and high AUC. MACE outcome in patients included non-fatal stroke, nonfatal myocardial infarction and cardiovascular death, and did not include procedure-related restenosis. Figure 2 shows that that the proportion of patients with MACE rose steadily for higher risk patients (i.e., patients with a higher number of abnormality parameters); while for MALE, there was a drop in the proportion of events for the patients with the highest risk. Clinically, a higher score implies a higher risk of thromboembolism, which would prompt the treating physician to be more aggressive with anticoagulant or antiplatelet drugs [26]. This may explain why the high-risk patients with abnormal parameters greater than or equal to six demonstrated fewer MALEs as the use of anticoagulants can significantly reduce acute limb ischemia in PAD patients after revascularization (voyager study) [27]. Another possible reason could be the higher mortality rate in this group of patients, eventually resulting in relatively lower MALE events.
On comparing traditional models with that of MCR-based regression models, MCR performed similarly or slightly better. Traditional models consist of multiple risk metrics that are associated with known caveats such as low statistical power, extreme higher order interaction terms, low robustness, and collinearity among risk factors [28]. As cumulative scores such as MCR are summed across a number of variables they possess the advantage of being a more stable measure and are more suitable for detecting effects as measurement errors are diminished when scores are summed [29]. This is why MCR is believed to be more robust alternative to traditional models which could be used for risk stratification for MACE of Taiwanese PAD patients who underwent PTA, thereby allowing shared decision making. It is to be noted that CAD is an important comorbidity in PAD patients. A prior study on REACH data set demonstrated that one-third of the patients with CAD also had PAD while almost two-thirds of PAD patients had a coexisting CAD or cerebrovascular disease and the percentage of CAD in PAD patients is logically proportional to the ischemic risk [30]. Therefore, its reasonable that the MACE group had higher burden of CAD than non-MACE group. In addition to medicines, the C part (comorbidities and cardiovascular risk factor management including change of lifestyle) of ABC pathway strategy, which is commonly adopted for A-Fib patients, can also be selected for treating PAD patients with higher ischemic risk, based on risk stratification by MCR.
One of the limitations of this study was the lack of a prospective external cohort to conduct validation of the performance of the MCR for predicting MACE; however, a thorough internal validation was conducted instead. Moreover, we ensured that the analysis of the study cohort took into account the various clinical factors and the complexities associated with all events for PAD patients who underwent PTA. Hence, we believe that the findings could be generalized to specific subgroups of PAD patients. Nevertheless, future studies will be conducted to validate the findings using cohorts of independent external patients. Prognosis for PAD patients could vary based on the distribution of PAD lesions [31]. This study mainly focused on lower extremity PAD. Hence, future studies are needed to clarify the above. There were some other limitations in the data that were analyzed. No information on the number of stents and drug-eluting balloons (DEBs) was available. Also, it was difficult to define the ‘target region’ in CLI patients as concurrent implementation of revascularization of iliac lesion, femoropopliteal lesion, or BTK lesion was conducted. Hence, whether the target region had any effect on the outcome could not be determined.
5. Conclusions
PAD confers an overall higher mortality risk as well as greater risks of coronary and cerebral ischemic events, and thus it is a condition with a high CVD risk. This necessitates strict preventive strategies. The findings of this study indicated that CHA2DS2-VASc could potentially serve as a risk stratification score for outcome MACE for a specific group of patients with lower extremity PAD who underwent PTA, thereby allowing medical practitioners to implement the appropriate therapeutic measures in a timely fashion to prevent worse MACE outcomes. The findings from this study also clearly indicates that CHA2DS2-VASc doesn’t qualify as a good predictor of MALE and therefore cannot be used for risk stratification of MALE for patients with PAD. The negation of the hypothesis for MALE was obtained through extensive evaluation and therefore we believe that it is a valuable scientific information which was absent from the literature related to CHA2DS2-VASc up until now.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1. The distribution of PAD samples based on (a) CHA2DS2-VASc and (b) MCR scores. Table S1. Description of Rutherford classifications. Table S2. Demographic and clinico-pathological characteristics for major adverse limb events (MALE) and major adverse cardiovascular events (MACE). Table S3. Demographic and clinico-pathological characteristics for outcome major adverse limb events (MALE) + major adverse cardiovascular events (MACE). Table S4. Calibration analysis for years 1-5 based on multivariate-adjusted MCR models for MALE. Table S5. Calibration analysis for year 1 - year 5 based on multivariate-adjusted traditional models for MALE. Table S6. Calibration analysis for years 1-5 based on multivariate-adjusted MCR models for MACE. Table S7. Calibration analysis for years 1-5 based on multivariate-adjusted traditional models for MACE. Table S8. Calibration analysis for years 1-5 based on multivariate-adjusted MCR models for MALE + MACE. Table S9. Calibration analysis for years 1-5 based on multivariate-adjusted traditional model for MALE + MACE.
Funding
The author(s) received no specific funding for this work.
Authors Contributions
Y.T.C. and C.S.C. conceptualized the study; Y.T.C. and C.S.C. did the formal analysis; Y.T.C. and C.S.C. did the investigation; Y.T.C. and C.S.C. did the methodology; Y.T.C., F.L.C., and C.S.C. did the project administration; P.H.L. and C.S.C. provided the resources; Y.T.C., P.H.L., and C.S.C. supervised the study; W.C.L. validated the study; Y.T.C. and C.S.C. wrote the original draft; Y.T.C., F.L.C., and C.S.C. wrote, reviewed, and edited the manuscript. All authors reviewed the manuscript.
Institutional Review Board Statement
The study has been approved by the institutional review board (IRB) of Taichung Veterans General Hospital (TCVGH-IRB #: CE21519A). All research was performed in accordance with relevant guidelines/regulations of the ethical committee. It is a retrospective study and therefore consent was not required. The IRB committee I &II of Taichung Veterans General Hospital waived the need for the requirement of informed consent.
Informed Consent Statement
It is a retrospective study and therefore consent was not required. The IRB committee I &II of Taichung Veterans General Hospital waived the need for the requirement of informed consent.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
Not applicable.
Consent for publication
Not applicable.
Conflicts of Interest
The authors have declared that no conflict of interests exist.
Abbreviations
- PAD: peripheral artery disease
- MACE: major adverse cardiovascular events
- MALE: major adverse limb events
- ALI: acute limb ischemia
- PCI: percutaneous coronary intervention
- CHF: congestive heart failure
- HTN: hypertension
- DM: Diabetes Mellitus
- AF: atrial fibrillation
- ABI: ankle brachial index
- HPL: hyperlipidemia
- LDL: low-density lipoprotein
- CAD: coronary artery disease
- CABG: coronary artery bypass graft
- MI: myocardial infarction
- COPD: chronic obstructive pulmonary disease
- CKD: chronic kidney disease
- CCr: creatinine clearance test
- HD: hemodialysis
- PD: peritoneal dialysis
- HDL: high-density lipoprotein
- TG: triglyceride
- ASA: aspirin
- DOAC: direct oral anticoagulant
- ACEI: angiotensin-converting enzyme inhibitors
- ARB: angiotensin receptor blockers
- CCB: calcium channel blockers
- CLI: critical limb ischemia
- BTK: below-the-knee
- DAPT: Dual antiplatelet therapy
References
- Polonsky, T.S.; McDermott, M.M. Lower extremity peripheral artery disease without chronic limb-threatening ischemia: A review. JAMA 2021, 325, 2188–2198. [Google Scholar] [CrossRef] [PubMed]
- Aday, A.W.; Matsushita, K. Epidemiology of peripheral artery disease and polyvascular disease. Circ. Res. 2021, 128, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Shu, J.; Santulli, G. Update on peripheral artery disease: Epidemiology and evidence-based facts. Atherosclerosis 2018, 275, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Szarek, M.; Hess, C.; Patel, M.R.; Jones, W.S.; Berger, J.S.; Baumgartner, I.; Katona, B.; Mahaffey, K.W.; Norgren, L.; Blomster, J. Total Cardiovascular and Limb Events and the Impact of Polyvascular Disease in Chronic Symptomatic Peripheral Artery Disease. J. Am. Heart Assoc. 2022, e025504. [Google Scholar] [CrossRef] [PubMed]
- Tsai, I.; Wang, C.-P.; Lu, Y.-C.; Hung, W.-C.; Wu, C.-C.; Lu, L.-F.; Chung, F.-M.; Hsu, C.-C.; Lee, Y.-J.; Yu, T.-H. The burden of major adverse cardiac events in patients with coronary artery disease. BMC Cardiovasc. Disord. 2017, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, E.M.; Wang, K.; Keo, H.H.; Duval, S.; Smolderen, K.G.; Cohen, D.J.; Steg, G.; Bhatt, D.L.; Hirsch, A.T. Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.S.; Caron, F.; Eikelboom, J.W.; Bosch, J.; Dyal, L.; Aboyans, V.; Abola, M.T.; Branch, K.R.; Keltai, K.; Bhatt, D.L. Major adverse limb events and mortality in patients with peripheral artery disease: The COMPASS trial. J. Am. Coll. Cardiol. 2018, 71, 2306–2315. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J.B.; Torp-Pedersen, C.; Hansen, M.L.; Lip, G.Y. The value of the CHA2DS2-VASc score for refining stroke risk stratification in patients with atrial fibrillation with a CHADS2 score 0–1: A nationwide cohort study. Thromb. Haemost. 2012, 107, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Yalim, Z.; Aldemir, M.; Yalim, S.A. Assessment of the relationship between death and CHA2DS2-VASc score in peripheral artery disease. Int Angiol 2020, 39, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.-S.; Lee, M.; Tang, S.-C.; Huang, P.-H.; Yeh, H.-I.; Hou, C.J.-Y.; Hsieh, I.-C.; Lee, J.-T.; Jeng, J.-S.; Li, Y.-H. 2022 focused update of the 2017 Taiwan lipid guidelines for high risk patients: Coronary artery disease, peripheral artery disease and ischemic stroke. J. Formos. Med. Assoc. 2022, 121, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Klefsjö, B. Proportional hazards model: A review. Reliab. Eng. Syst. Saf. 1994, 44, 177–188. [Google Scholar] [CrossRef]
- Therneau, T.; Lumley, T. R survival package. R Core Team 2013. [Google Scholar]
- Dudley, W.N.; Wickham, R.; Coombs, N. An introduction to survival statistics: Kaplan-Meier analysis. J. Adv. Pract. Oncol. 2016, 7, 91. [Google Scholar] [PubMed]
- Krstajic, D.; Buturovic, L.J.; Leahy, D.E.; Thomas, S. Cross-validation pitfalls when selecting and assessing regression and classification models. J. Cheminformatics 2014, 6, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B. Overall C as a measure of discrimination in survival analysis: Model specific population value and confidence interval estimation. Stat. Med. 2004, 23, 2109–2123. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B.; Nam, B.-H. Evaluation of the performance of survival analysis models: Discrimination and calibration measures. Handb. Stat. 2003, 23, 1–25. [Google Scholar]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of classification systems in peripheral artery disease. In Proceedings of the Seminars in interventional radiology; 2014; pp. 378–388. [Google Scholar]
- Dopheide, J.F.; Ramadani, H.; Adam, L.; Gahl, B.; Papac, L.; Veit, J.; Kaspar, M.; Schindewolf, M.; Baumgartner, I.; Drexel, H. Development of a 3-Dimensional Prognostic Score for Patients With Symptomatic Peripheral Artery Disease: PAD3D Score. Angiology 2020, 71, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.-C.; Su, H.-M.; Lee, W.-H.; Chiu, C.-A.; Chi, N.-Y.; Tsai, W.-C.; Lin, T.-H.; Voon, W.-C.; Lai, W.-T.; Sheu, S.-H. CHA2DS2-VASc Score and Risk of New-Onset Peripheral Arterial Occlusive Disease in Patients without Atrial Fibrillation. Acta Cardiol. Sin. 2021, 37, 261. [Google Scholar] [PubMed]
- Chen, J.-Y.; Zhang, A.-D.; Lu, H.-Y.; Guo, J.; Wang, F.-F.; Li, Z.-C. CHADS2 versus CHA2DS2-VASc score in assessing the stroke and thromboembolism risk stratification in patients with atrial fibrillation: A systematic review and meta-analysis. J. Geriatr. Cardiol. JGC 2013, 10, 258. [Google Scholar] [PubMed]
- Chao, T.-F.; Liu, C.-J.; Tuan, T.-C.; Chen, S.-J.; Wang, K.-L.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Chen, T.-J. Comparisons of CHADS2 and CHA2DS2-VASc scores for stroke risk stratification in atrial fibrillation: Which scoring system should be used for Asians? Heart Rhythm 2016, 13, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Kim, B.-S.; Shin, J.-H.; Kim, W.; Kook, H.; Park, H.-C.; Park, M.; Park, S.; Lim, Y.-H. Influence of concomitant percutaneous transluminal angioplasty with percutaneous coronary intervention on clinical outcomes of stable lower extremity artery diseases. Sci. Rep. 2022, 12, 1–11. [Google Scholar]
- Svendsen, J.H.; Nielsen, J.C.; Darkner, S.; Jensen, G.V.H.; Mortensen, L.S.; Andersen, H.R.; Investigators, D. CHADS2 and CHA2DS2-VASc score to assess risk of stroke and death in patients paced for sick sinus syndrome. Heart 2013, 99, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R.; Group, T.I.W. Inter-society consensus for the management of peripheral arterial disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.-H.; Wu, L.-S.; Chang, S.-H.; Lee, H.-F.; Liu, J.-R.; See, L.-C.; Yeh, Y.-H.; Kuo, C.-T. Young male patients with atrial fibrillation and CHA2DS2-VASc score of 1 may not need anticoagulants: A nationwide population-based study. PLoS ONE 2016, 11, e0151485. [Google Scholar] [CrossRef] [PubMed]
- Capell, W.H.; Bonaca, M.P.; Nehler, M.R.; Chen, E.; Kittelson, J.M.; Anand, S.S.; Berkowitz, S.D.; Debus, E.S.; Fanelli, F.; Haskell, L. Rationale and design for the Vascular Outcomes study of ASA along with rivaroxaban in endovascular or surgical limb revascularization for peripheral artery disease (VOYAGER PAD). Am. Heart J. 2018, 199, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Li, D.; Whipple, S.S. Cumulative risk and child development. Psychol. Bull. 2013, 139, 1342. [Google Scholar] [CrossRef] [PubMed]
- Flouri, E.; Tzavidis, N.; Kallis, C. Area and family effects on the psychopathology of the Millennium Cohort Study children and their older siblings. J. Child Psychol. Psychiatry 2010, 51, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Smolderen, K.; Wang, K.; De Pouvourville, G.; Brüggenjürgen, B.; Röther, J.; Zeymer, U.; Parhofer, K.; Steg, P.; Bhatt, D.; Magnuson, E. Two-year vascular hospitalisation rates and associated costs in patients at risk of atherothrombosis in France and Germany: Highest burden for peripheral arterial disease. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Desormais, I.; Lacroix, P.; Salazar, J.; Criqui, M.H.; Laskar, M. The general prognosis of patients with peripheral arterial disease differs according to the disease localization. J. Am. Coll. Cardiol. 2010, 55, 898–903. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Exclusion criteria and inclusion of subjects for analyses.
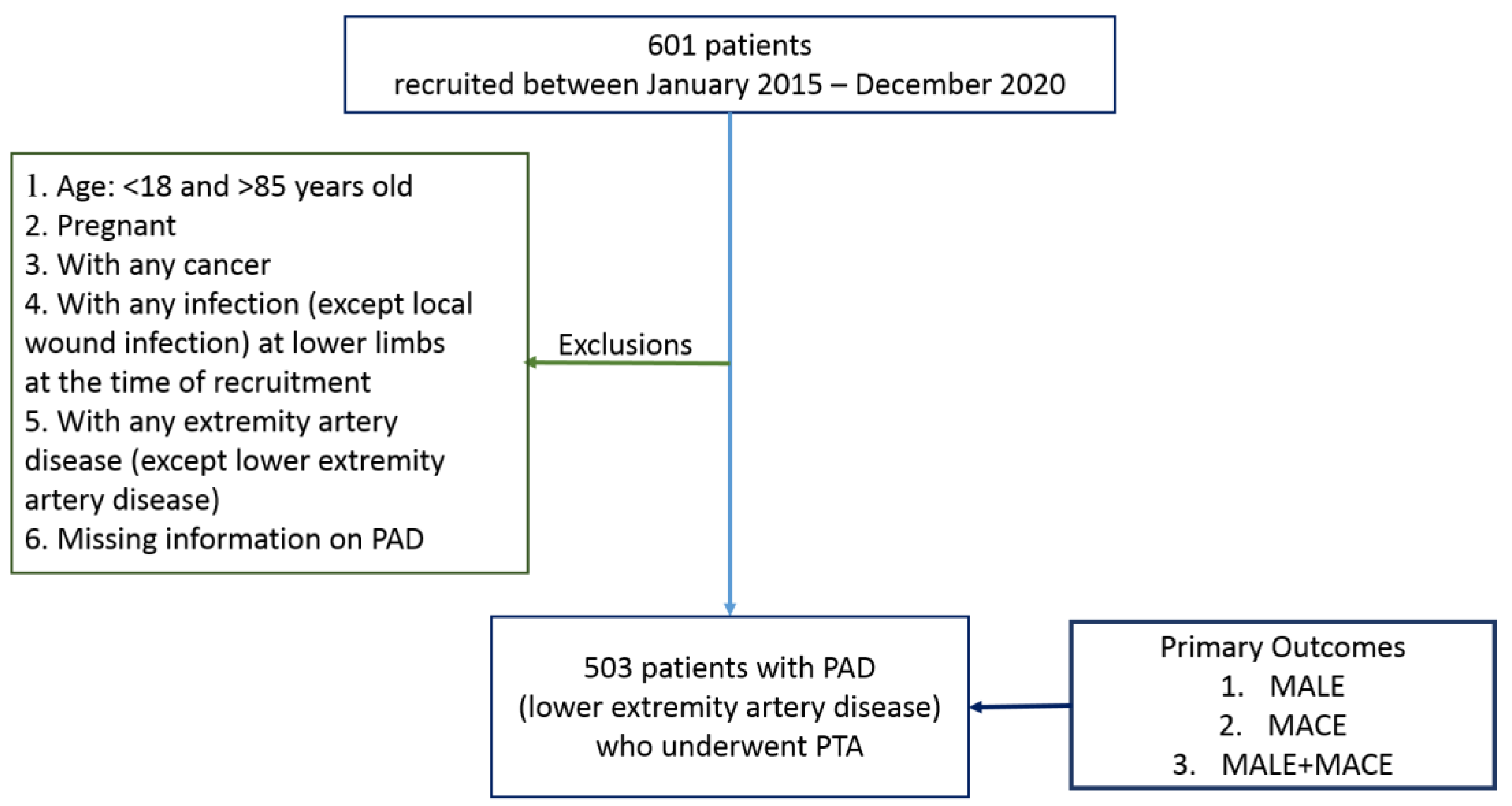
Figure 2.
Event rates for each of three outcomes MALE, MACE, and MALE+MACE, for study subjects classified into four risk groups based on MCR risk parameters (low-risk, moderate-risk, high-risk and very high-risk) (N = 503). MALE: major adverse limb events; MACE: major adverse cardiovascular events.
Figure 2.
Event rates for each of three outcomes MALE, MACE, and MALE+MACE, for study subjects classified into four risk groups based on MCR risk parameters (low-risk, moderate-risk, high-risk and very high-risk) (N = 503). MALE: major adverse limb events; MACE: major adverse cardiovascular events.
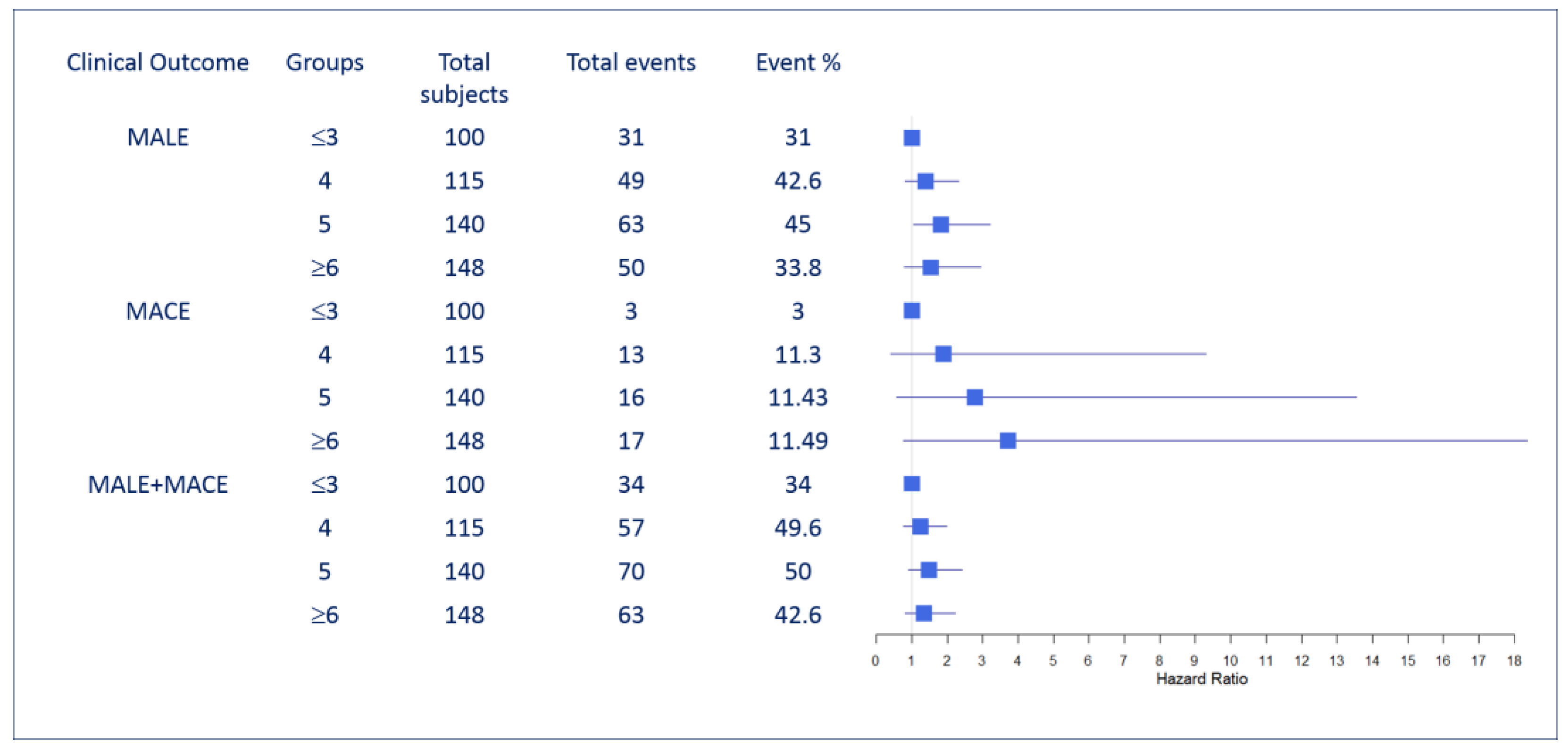
Figure 3.
Kaplan-Meier plots to compare the survival probability of subjects (N = 503) with MCR score (low-risk, moderate-risk, high-risk, very high-risk). P-values indicate whether significant differences exist among the different groups: (A) MALE, (B) MACE, and (C) MALE+MACE. MALE: major adverse limb events; MACE: major adverse cardiovascular events.
Figure 3.
Kaplan-Meier plots to compare the survival probability of subjects (N = 503) with MCR score (low-risk, moderate-risk, high-risk, very high-risk). P-values indicate whether significant differences exist among the different groups: (A) MALE, (B) MACE, and (C) MALE+MACE. MALE: major adverse limb events; MACE: major adverse cardiovascular events.
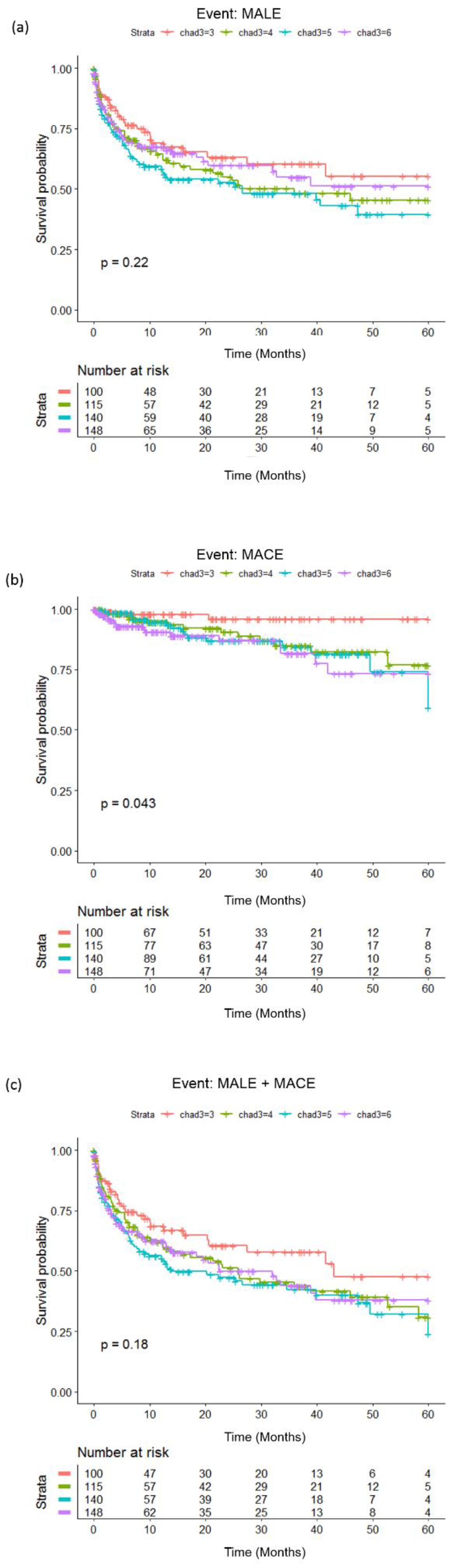
Figure 4.
Calibration plots for the events (A) MALE, (B) MACE and, (C) MALE+MACE showing the difference between observed and predicted survival probability for proposed MCR-based prognostic models (with MCR score) and the traditional model (only traditional variables without MCR score). Calibration for each of the models was conducted using 10-fold cross-validation (CV) and each bar shows an average of the probability difference over 10 models for each CV.
Figure 4.
Calibration plots for the events (A) MALE, (B) MACE and, (C) MALE+MACE showing the difference between observed and predicted survival probability for proposed MCR-based prognostic models (with MCR score) and the traditional model (only traditional variables without MCR score). Calibration for each of the models was conducted using 10-fold cross-validation (CV) and each bar shows an average of the probability difference over 10 models for each CV.
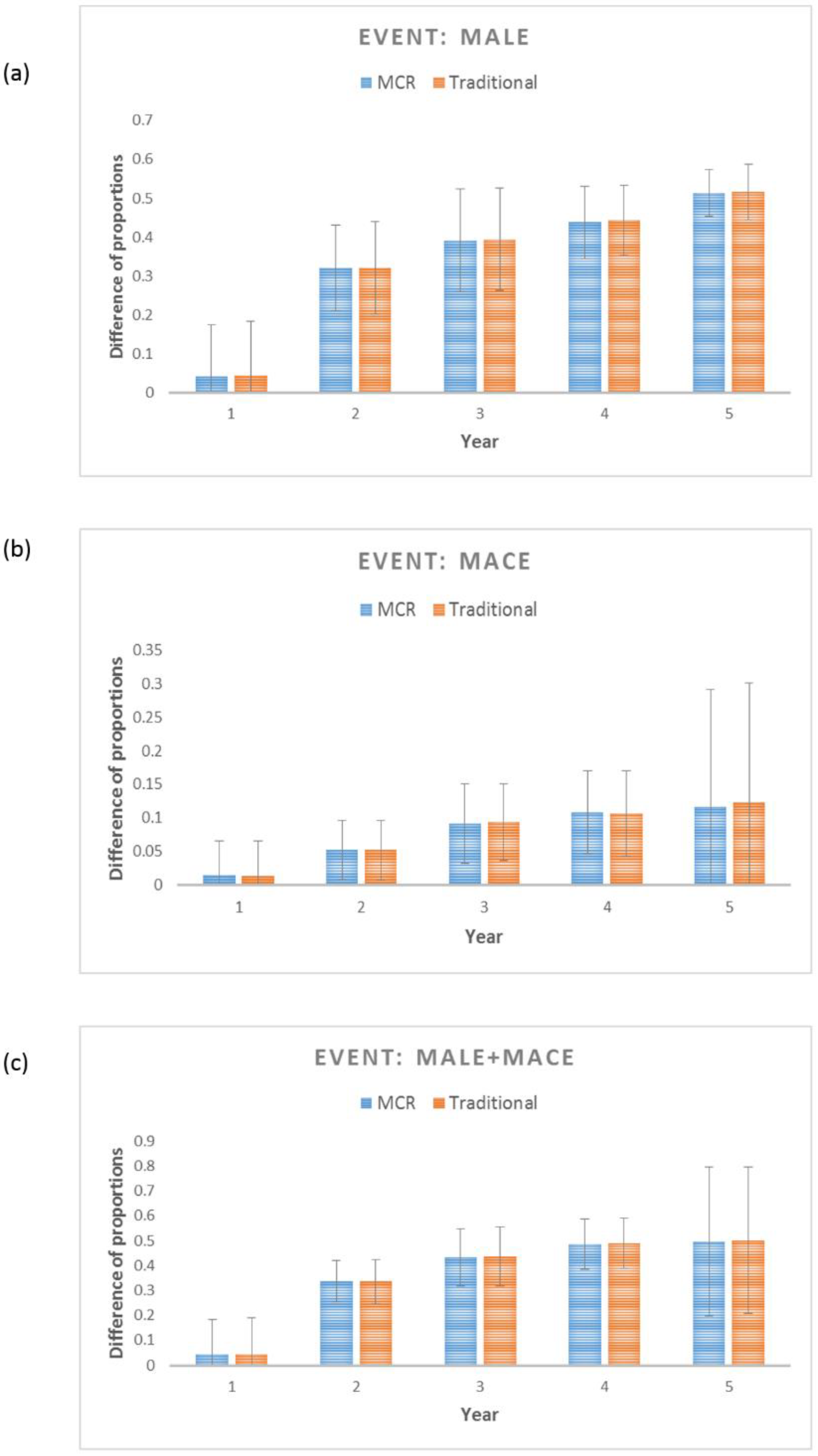
Figure 5.
ROC plots for 12 months, 24 months, 36 months and 48 months using univariate models, and multivariate adjusted models with CHA2DS2-VASc as predictor. (A) - (C): Univariate models for MALE, MACE and MALE+MACE respectively. (D) - (F): Multivariate adjusted models for MALE, MACE and MALE+MACE.
Figure 5.
ROC plots for 12 months, 24 months, 36 months and 48 months using univariate models, and multivariate adjusted models with CHA2DS2-VASc as predictor. (A) - (C): Univariate models for MALE, MACE and MALE+MACE respectively. (D) - (F): Multivariate adjusted models for MALE, MACE and MALE+MACE.
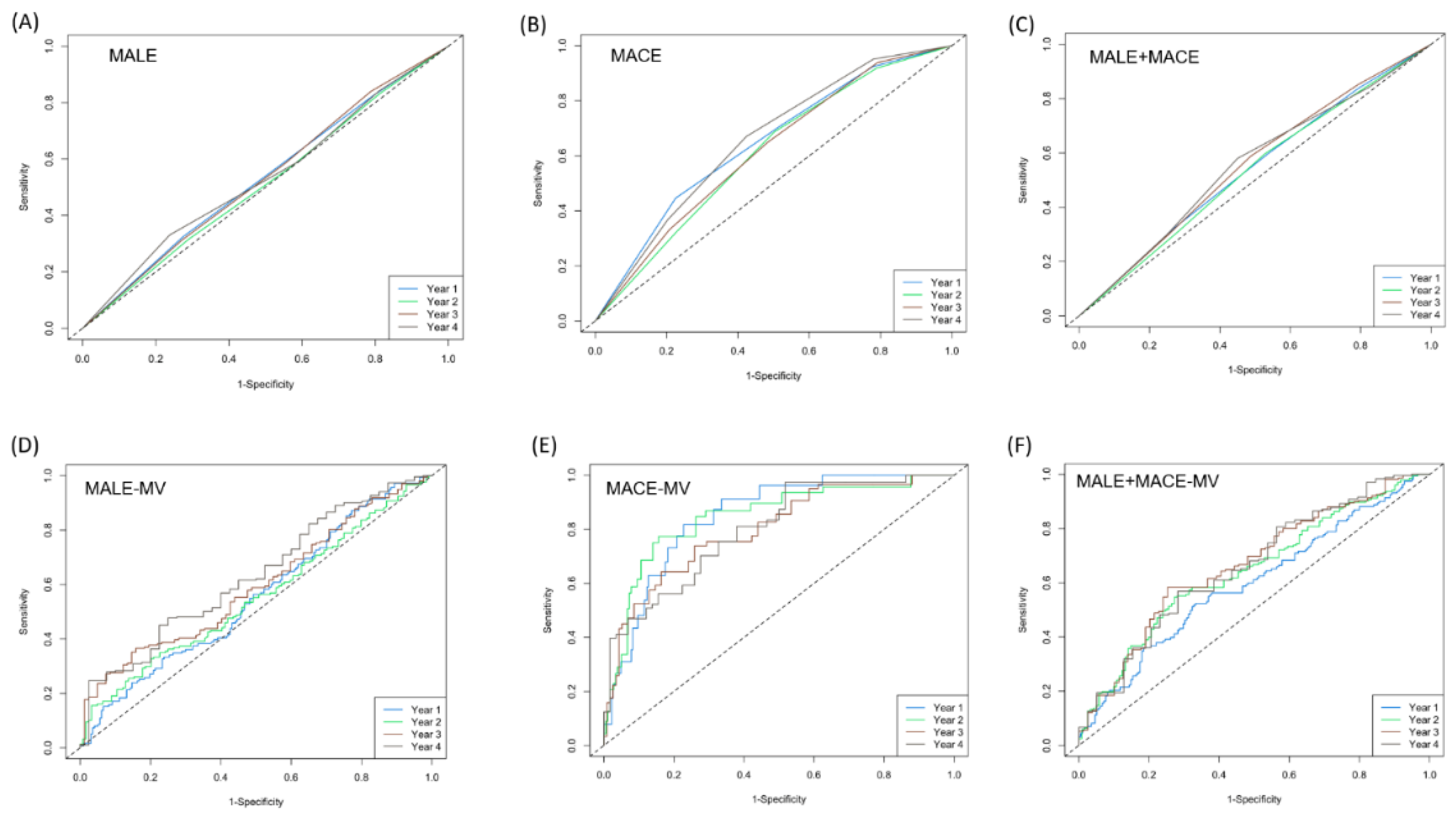

Table 1.
Characteristics of patients with peripheral artery disease.
| Characteristics (units) |
Measurement N=503 |
| Age (years) | 70.77 ± 12.39 |
| Sex = Male | 326 (64.81) |
| = Female | 177 (35.19) |
| BMI (Kg/m2) | 23.97 ± 3.91 |
| CHF (C) | 238 (47.32) |
| HTN | 403 (86.68) |
| DM | 376 (74.75) |
| Stroke (S)/TIA | 91 (18.09) |
| Vascular Disease | 503 (100) |
| HPL | 241 (47.91) |
| SMK | 195 (38.77) |
| CAD | 263 (52.29) |
| CABG | 53 (10.54) |
| PCI | 239 (47.51) |
| Old MI | 79 (15.71) |
| COPD | 21 (4.17) |
| CKD | 319 (63.42) |
| HD/PD | 181 (35.98) |
| Cr (mg/dL) | 3.26 ± 3.04 |
| Af | 120 (23.86) |
| Imd | 21 (4.03) |
| HbA1C (%) | 7.32 ± 1.86 |
| Cholesterol (mg/dL) | 149.65 ± 39.42 |
| LDL (mg/dL) | 83.37 ± 33.35 |
| HDL (mg/dL) | 42.94 ± 15.21 |
| TG (mg/dL) | 130.87 ± 83.79 |
| Glu (mg/dL) | 145.60 ± 69.49 |
| TG/HDL | 3.69 ± 3.86 |
| ASA | 385 (76.54) |
| clopidgrel | 427 (84.89) |
| cilostazol | 301 (59.84) |
| pentoxyphilline | 1 9 (0.19) |
| direct oral anticoagulant (DOAC) | 73 (14.51) |
| ACEIARB | 220 (43.74) |
| statin | 283 (56.26) |
| Betablocker | 189 (37.57) |
| CCB | 201 (39.96) |
| Insulin | 106 (21.07) |
| Rutherford =1 | 0 (0) |
| Rutherford = 2 | 0 (0) |
| Rutherford = 3 | 0 (0) |
| Rutherford = 4 | 130 (25.84) |
| Rutherford = 5 | 316 (62.82) |
| Rutherford = 6 | 57 (11.33) |
| Target vessel CIA | 41 (8.15) |
| Target vessel EIA | 45 (8.95) |
| Target vessel CFA | 27 (5.37) |
| Target vessel SFA | 285 (56.66) |
| Target vessel ATA | 248 (49.30) |
| Target vessel Popliteal | 107 (21.27) |
| Target vessel Peroneal artery | 96 (19.09) |
| Target vessel Tibiofibular TP trunk | 64 (12.72) |
| Target vessel PTA | 196 (38.97) |
| Target vessel DPA | 15 (2.98) |
| Target vessel Plantar artery | 23 (4.57) |
All measures are depicted as mean ± standard or n (%). BMI: body mass index; CHF (C): HTN: hypertension; DM: diabetes mellitus; Stroke (S)/TIA; HPL: hyperlipidemia; SMK: smoking status; CAD: coronary artery disease; CABG: Coronary Artery Bypass Graft; PCI: Percutaneous coronary intervention; MI: myocardial infarction; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease; HD/PD: hemodialysis/peritoneal dialysis; Cr: creatinine; Af: atrial fibrillation; Imd: immune-related disease; HbA1C: hemoglobin A1C, LDL: low-density lipoprotein; HDL: high-density lipoprotein; TG: triglyceride; Glu: glucose; ASA: Acetylsalicylic acid; ACEIARB: Angiotensin-Converting Enzyme Inhibitor (ACEI)/Angiotensin Receptor Blocker (ARB); CCB: Calcium channel blockers; Rutherford: Rutherford classification; CIA: common iliac artery; EIA: external iliac artery; CFA: common femoral artery; SFA: superficial femoral artery; ATA: anterior tibial artery; Tibiofibular TP (tibioperoneal) trunk; PTA: posterior tibial artery; DPA: dorsalis pedis artery.
Table 2.
Characteristics of 503 PAD patients (N = 503) divided into risk groups based on n.
| Variables | score =3 (N = 100) |
score = 4 (N= 115) |
score = 5 (N = 140) |
score = 6 (N = 148) |
P value |
|---|---|---|---|---|---|
| Age | 59.14 ± 12.07 | 67.76 ± 11.06 | 72.2 ± 10.54 | 79.60 ± 6.800 | <0.0001* |
| Sex (Male) | 86 (86) | 93 (80.87) | 84 (60) | 63 (42.57) | <0.0001* |
| BMI | 23.96 ± 3.85 | 24.48 ± 4.414 | 23.59 ± 3.503 | 23.93 ± 3.881 | 0.341 |
| CHF (C) | 13 (13) | 50 (43.48) | 67 (47.86) | 108 (72.97) | <0.0001* |
| HTN | 52 (52) | 101 (87.82) | 136 (97.14) | 147 (99.32) | <0.0001* |
| DM | 44 (44) | 89 (77.39) | 107 (76.43) | 136 (91.89) | <0.0001* |
| Stroke (S)/TIA | 3 (3) | 7 (6.09) | 28 (20) | 53 (35.81) | <0.0001* |
| Vascular Disease | 100 (100) | 115 (100) | 140 (100) | 148 (100) | 1 |
| Hyperlipidemia | 36 (36) | 51 (44.53) | 69 (49.28) | 85 (57.43) | 0.008* |
| SMK (smoking) | 63 (63) | 60 (52.17) | 44 (31.43) | 28 (18.92) | <0.0001* |
| Coronary Artery disease | 28 (28) | 60 (52.17) | 85 (60.71) | 90 (60.81) | <0.0001* |
| Coronary Artery Bypass Graft (CABG) | 3 (3) | 15 (13.04) | 15 (10.71) | 20 (13.51) | 0.022* |
| PCI (Percutaneous coronary intervention) | 22 (22) | 57 (49.57) | 77 (55) | 83 (56.08) | <0.0001* |
| Old MI (myocardial infarction) | 5 (5) | 19 (16.52) | 26 (18.57) | 29 (19.59) | 0.004* |
| COPD | 2 (2) | 2 (1.74) | 9 (6.43) | 8 (5.4) | 0.168 |
| CKD | 35 (35) | 70 (60.87) | 109 (77.86) | 105 (70.95) | <0.0001* |
| HD/PD | 25 (25) | 42 (36.52) | 55 (39.29) | 59 (39.86) | 0.069 |
| Cr (cardiac rehabilitation) score | 2.65 ± 3.24 | 3.493 ± 3.569 | 3.536 ± 2.898 | 3.226 ± 2.553 | 0.136 |
| Af (atrial fibrillation) | 10 (10) | 19 (16.52) | 40 (28.47) | 51 (34.46) | <0.0001* |
| Imd (Immune related disease) | 10 (10) | 3 (2.61) | 4 (2.86) | 4 (2.70) | 0.033* |
| HbA1C | 7.013 ± 1.928 | 7.675 ± 2.129 | 7.285 ± 1.600 | 7.298 ± 1.799 | 0.072 |
| Cholesterol | 163.65 ± 40.72 | 149.50 ± 42.07 | 147.81 ± 40.29 | 142.05 ± 32.99 | 0.0003* |
| LDL | 93 ± 34.675 | 82.03 ± 32.08 | 83.22 ± 36.68 | 78.01 ± 28.69 | 0.006* |
| HDL | 43.76 ± 18.288 | 43.02 ± 16.36 | 41.53 ± 12.31 | 43.770 ± 14.486 | 0.542 |
| TG | 147.31 ± 99.34 | 131.71 ± 93.15 | 129.2 ± 72.41 | 120.67 ± 73.13 | 0.106 |
| Glu | 135.29 ± 65.37 | 154.71 ± 80.44 | 147.75 ± 68.83 | 143.44 ± 63.002 | 0.216 |
| Medications | |||||
| ASA | 79 (79) | 88 (76.52) | 111 (79.29) | 107 (72.30) | 0.504 |
| clopidgrel | 76 (79) | 97 (84.35) | 124 (88.57) | 130 (87.84) | 0.0428 |
| cilostazol | 62 (62) | 77 (66.96) | 79 (56.43) | 83 (56.08) | 0.242 |
| pentoxyphilline | 0 (0) | 0 (0) | 0 (0) | 1 (0.67) | 1 |
| direct oral anticoagulant (DOAC) | 15 (15) | 11 (9.56) | 24 (17.14) | 23 (15.54) | 0.349 |
| ACEIARB | 35 (35) | 54 (46.96) | 67 (47.86) | 64 (43.24) | 0.204 |
| statin | 57 (57) | 63 (54.78) | 81 (57.86) | 82 (55.41) | 0.958 |
| Betablocker | 22 (22) | 48 (41.74) | 58 (41.43) | 61 (41.22) | 0.003* |
| CCB | 37 (37) | 43 (37.39) | 66 (47.14) | 55 (37.16) | 0.251 |
| Insulin | 13 (13) | 26 (22.61) | 28 (20) | 39 (26.35) | 0.076 |
| Rutherford classification | |||||
| 1 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 |
| 2 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 |
| 3 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 |
| 4 | 36 (36) | 28 (24.34) | 34 (24.29) | 32 (21.62) | 0.079 |
| 5 | 55 (55) | 72 (62.61) | 86 (61.43) | 103 (69.59) | 0.129 |
| 6 | 9 (9) | 15 (13.04) | 20 (14.29) | 13 (8.78) | 0.394 |
| Target vessel | |||||
| CIA | 8 (8) | 11 (9.56) | 15 (10.71) | 7 (4.73) | 0.249 |
| EIA | 11 (11) | 11 (9.56) | 13 (9.29) | 10 (6.76) | 0.677 |
| CFA | 10 (10) | 4 (3.48) | 8 (5.71) | 5 (3.38) | 0.128 |
| SFA | 42 (42) | 59 (51.30) | 86 (61.43) | 98 (66.22) | 0.0007* |
| ATA | 49 (49) | 62 (53.91) | 70 (50) | 67 (45.27) | 0.581 |
| Popliteal | 19 (19) | 19 (16.52) | 33 (23.57) | 36 (24.32) | 0.375 |
| Peroneal artery | 12 (12) | 22 (19.13) | 27 (19.29) | 35 (23.65) | 0.147 |
| Tibiofibular TP trunk | 9 (9) | 6 (5.21) | 23 (16.43) | 26 (17.57) | 0.005* |
| PTA | 44 (44) | 46 (40) | 50 (35.71) | 56 (37.84) | 0.613 |
| DPA | 4 (4) | 4 (3.48) | 3 (2.14) | 4 (2.70) | 0.825 |
| Plantar artery | 2 (2) | 8 (6.96) | 8 (5.71) | 5 (3.38) | 0.269 |
Number of abnormal parameters (≤3, 4, 5, and ≥6). BMI: body mass index; CHF: chronic heart failure; HTN: hypertension; DM: diabetes mellitus; TIA: Transient ischemic attack; HPL: hyperlipidemia; SMK: smoking status; CAD: coronary artery disease; CABG: Coronary Artery Bypass Graft; PCI: Percutaneous coronary intervention; MI: myocardial infarction; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease; HD/PD: hemodialysis/peritoneal dialysis; Cr: creatinine; Af: atrial fibrillation; Imd: immune-related disease; HbA1C: hemoglobin A1C, LDL: low-density lipoprotein; HDL: high-density lipoprotein; TG: triglyceride; Glu: glucose.
Table 3.
Performance of MCR score as a predictor of MACE using 503 patients with peripheral artery disease.
Table 3.
Performance of MCR score as a predictor of MACE using 503 patients with peripheral artery disease.
| Events | Low risk (N = 100) |
Moderate risk (N= 115) |
High Risk (N = 140) |
Very high risk (N = 148) |
|---|---|---|---|---|
| Major adverse cardiovascularevents (MACE) | ||||
| #MACE (%) | 3(3) | 13 (11.30) | 16 (11.43) | 17 (11.49) |
| Crude HR (95% CI) | 1 | 3.47 (0.99 - 12.18) | 4.12 (1.19 - 14.14) | 5.06 (1.48 - 17.28) |
| P-value | 0.052* | 0.024* | 0.009* | |
| Multivariate adjusted HR (95% CI) | 1 | 1.89 (0.39 - 9.31) | 2.78 (0.57 - 13.55) | 3.72 (0.75 - 18.42) |
| P-value | 0.21 | 0.13 | 0.049* | |
| Major adverse limb events (MALE) | ||||
| # MALE (%) | 31 (31) | 49 (42.60) | 63 (45) | 50 (33.78) |
| Crude HR (95% CI) | 1 | 1.33 (0.85 - 2.09) | 1.55 (1.01 - 2.38) | 1.21 (0.77 - 1.89) |
| P-value | 0.213 | 0.046* | 0.398 | |
| Multivariate adjusted HR (95%CI) | 1 | 1.38 (0.81 - 2.33) | 1.82 (1.04 - 3.2) | 1.53 (0.79 - 2.94) |
| P-value | 0.23 | 0.037* | 0.202 | |
|
Major adverse limb and cardiac events (MALE + MACE) |
||||
| #MALE + MACE (%) | 34 (34) | 57 (49.57) | 70 (50) | 63 (42.57) |
| Crude HR (95% CI) | 1 | 1.37 (0.89 - 2.09) | 1.58 (1.05 - 2.37) | 1.41 (0.93 - 2.14) |
| P-value | 0.145 | 0.029* | 0.107 | |
| Multivariate adjusted HR (95%CI) | 1 | 1.24 (0.77 - 1.98) | 1.48 (0.91 - 2.41) | 1.34 (0.81 - 2.22) |
| P-value | 0.18 | 0.04* | 0.09 |
Multivariate model adjusted by factors that were found significant in Tables S2 and S3 for MACE, MALE and MALE+MACE. Multivariate adjusted MACE model was adjusted by hyperlipidemia, coronary Artery Bypass Graft, chronic obstructive pulmonary disease; chronic kidney disease; creatinine; atrial fibrillation; immune-related disease; hemoglobin, old myocardial Infarction. Multivariate adjusted MALE model was adjusted by HbA1C and Glu. Multivariate adjusted MALE + MACE model was adjusted by hyperlipidemia, Percutaneous coronary intervention, creatinine, hemoglobin A1C, glucose.
Table 4.
Average and standard deviation of c-indices from 10-fold cross-validation.
| MALE | MACE | MALE+MACE | ||||
| Avg. C-Index | Std. Dev. C-Index | Avg. C-Index | Std. Dev. C-Index | Avg. C-Index | Std. Dev. C-Index | |
| Crude MCR model | 0.54 | 0.009 | 0.63 | 0.02 | 0.54 | 0.009 |
| Multivariate-adjusted MCR model | 0.57 | 0.009 | 0.81 | 0.014 | 0.56 | 0.009 |
| Traditional model | 0.55 | 0.01 | 0.81 | 0.01 | 0.54 | 0.007 |
MCR: modified cumulative risk; MALE: major adverse limb events; MACE: major adverse cardiovascular events. Multivariate model adjusted by hyperlipidemia, smoking status, chronic obstructive pulmonary disease; chronic kidney disease; hemodialysis/peritoneal dialysis; creatinine; atrial fibrillation; immune-related disease; hemoglobin, cholesterol, low-density lipoprotein, high-density lipoprotein, triglyceride and glucose levels.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



