Submitted:
02 May 2024
Posted:
02 May 2024
You are already at the latest version
Abstract
This study analyzed eye examination data from the 5th Korea National Health and Nutrition Examination Survey to investigate the relationship between cataract prevalence and sunlight exposure among Koreans. Out of 952 individuals from 192 districts surveyed from January to December, statistical analyses using SPSS version 26, including chi-square tests and logistic regression, were conducted. Results: Results showed that the incidence of cataracts was higher in people exposed to sunlight for more than 5 hours. Regarding gender, the incidence of cataracts was higher in female in the 2-5 hours of sunlight exposure group, and in male in the group exposed to sunlight for more than 5 hours. Age significantly increased cataracts after age 45 in both groups. Additionally, the prevalence was higher among college graduates in the 2 to 5 groups, and among elementary school graduates in the more than 5 hours usage group. In urban areas, the cataract prevalence rate was higher in the 2-5-hour usage group, and in rural areas, the cataract prevalence was higher in the more than 5-hour usage group. In conclusion, prolonged sunlight exposure, particularly over 5 hours, correlated with higher cataract prevalence among Koreans, with various demographic factors influencing incidence rates.
Keywords:
Cataracts
; sunlight exposure time
; gender
; age
; education
; residence
1. Introduction
Cataract is one of the visual impairment diseases caused by opacity of the lens of the eye. In addition, cataract is a disease that commonly occurs in middle-aged and elderly adults among eye-related diseases. According to data from the Korea Centers for Disease Control and Prevention in 2012, the prevalence of cataracts in Korea over the age of 65 was 38.8% (male 31.0%, female 44.3%), with females 13% higher than males. Moreover, Korea is showing the fastest aging rate in the world due to the improvement of health and nutrition along with the improvement of income level. It is expected to increase to 13.23 million in 2040 and 17.81 million in 2040 (approximately 40%). Given the rapidly aging population of Korea, the incidence of cataracts is expected to continue to increase in the future.
The mechanism of cataract formation is very complex and has been reported to be related to systemic diseases such as diabetes, as well as ultraviolet rays, heat, hormone abnormalities, and smoking [1]. Among them, ultraviolet (UV) is known to be an important factor in causing cataract both epidemiologically and experimentally [2,3] Ultraviolet rays are divided into UVC (200-290nm), UVB (290-320nm), and UVA (320-400nm) according to their biological properties. It is absorbed by the lens. However, the exact mechanism for the occurrence of cataracts by these ultraviolet rays is still unknown [4,5].
The primary function of the human lens is to focus light undistorted onto the retina. Although the properties of most of the transmitting components of the eye remain constant, the transparency and properties of the lens change throughout life. The lens is clear for the first 3 years of life and then gradually develops yellow pigments (3-hydroxy kynurenine and its glucoside). This is a protective pigment, which absorbs UV radiation and safely dissipates [6]. As long as that pigment is present, no UV-A or UV-B radiation reaches the retina, and in this way, the adult human retina is protected against normal levels of UV radiation [7].
On the other hand, in case of intense acute UV radiation or chronic exposure, cataracts occur in which the lens becomes cloudy. As a result, it affects the clarity of the lens and causes damage to vision and retinal function [8,9]. Until now, it is known that DNA damage accumulation by ultraviolet rays, structure and function of lens epithelial cell membrane, and hydrogen peroxide, superoxide anion, singlet oxygen, hydroxyl radical, etc. Physiological and biochemical changes in the lens due to the generation of reactive oxygen species have been reported to form cataracts [10,11].
It is known that UV rays accelerate skin aging. Likewise, the eye is a transparent tissue exposed to direct light along with the skin, so it is expected that it is related to the aging of the eye, and it is highly likely that light including ultraviolet rays plays a very important role in the occurrence of diseases [12]. The WHO estimates that 20% of global blindness due to cataracts can be attributed to UV exposure. Avoidance of direct sunlight during peak hours of UV-B radiation has been suggested as a strong primary preventive measure for cortical cataracts [13,14]. Sunlight, which contains ultraviolet rays, can increase the risk of developing cataracts if exposed excessively over a long period of time [15]. One study found that male with higher average annual UV levels were 1.36 times more likely to have more severe cortical opacities than male with lower average UV levels [16]. Additionally, a study reported that the risk of cortical cataracts increased by 4.3% for each hour of outdoor activity [17].
Based on these research results, this study attempted to analyze various demographic factors such as gender, age, education level, and region regarding sunlight exposure time and cataract prevalence among Korean adults. The purpose of this is to provide counseling for the elderly and cataract patients, and it is intended to be used as basic data for epidemiological research on the prevalence of cataracts.
2. Materials and Methods
2.1. Subject
In order to confirm the correlation between the prevalence of cataracts and sunlight in Koreans, this study conducted the 5th National Health and Nutrition Survey (2019) among cross-sectional data designed to accurately evaluate the health and nutritional levels of the people conducted by the Korea Centers for Disease Control and Prevention (KCDC). The analysis was conducted using eye examination data (last revised in March). 192 sample districts were extracted and analysis was conducted on 952 subjects (522 men, 430 women) with exposure to sunlight for more than 2 hours to increase accuracy. The target group of the National Health and Nutrition Survey was Korean citizens residing in Korea, and subjects who did not respond to the questionnaire or recorded that they had no disease were excluded from the analysis.
2.2. Research Variables and Weight
In this study, the dependent variable was the incidence of cataracts, and the independent variable was the sunlight exposure time depending on the time of day, which was divided into 2 to 5 hours group and 5 hours or more group. Among the sampled households, all household members were selected for the survey, excluding unsuitable household members (living in other areas, etc.). Therefore, the household response rate was calculated as the percentage of households surveyed that completed the survey. The individual response rate was calculated as the percentage of survey respondents among surveyed households. The final response rate was calculated as the product of the household response rate and the household member response rate.
2.3. Statistical Analysis
In this study, we investigated sociological factors related to sunlight exposure time and cataract prevalence among Korean adults. General characteristics were analyzed, percentages (%) and standard errors (S.E.) were presented in a table, and differences between groups were confirmed using chi-square. For analysis related to age among sociological factors, logistic regression analysis was performed to statistically verify its effect on cataracts. Statistical analysis was performed using SPSS version 26, and p<0.05 was considered statistically significant.
3. Results
In this study, the dependent variable was the incidence of cataracts, and the independent variable was the sunlight exposure time depending on the time of day, which was divided into 2 to 5 hours group and 5 hours or more group. Among the sampled households, all household members were selected for the survey, excluding unsuitable household members (living in other areas, etc.). Therefore, the household response rate was calculated as the percentage of households surveyed that completed the survey. The individual response rate was calculated as the percentage of survey respondents among surveyed households. The final response rate was calculated as the product of the household response rate and the household member response rate.
Table 1 shows the demographic and sociological characteristics of the study subjects as follows. The amount of sunlight was 482 people (50.6%) when it was 2-5 hours, and 470 people (49.4%) when it was more than 5 hours, showing little difference in the proportions of the two groups. As for the gender, 522 (54.8%) were male and 430 (45.2%) were female, and 259 (27.2%) were under the age of 45 and 693 (72.8%) were over the age of 45. As for the educational level, 354 (37.2%) were graduating from elementary school and 136 (14.3%) were graduating from middle school. And there were 268 (28.2%) were graduating from high school and 138 (14.5%) were graduating from college. The residence was 139 people in Gyeonggi Province (14.6%) and 137 in North Gyeong-sang Province (14.4%), 15 in Jeju (1.6%) and 13 in Daejeon (1.4%). The refractive power was 303 people (34.8%) with myopia and 566 people (65.2%) from primitive.
Cross tabulations were calculated to verify differences in cataract incidence rates depending on sunlight exposure time. As a result, in the 2-5-hour group, there were 275 people (57.1%) without cataracts and 207 people (42.9%) with cataracts, and in the group over 5 hours, there were 213 people (45.3%) without cataracts, the number of people with cataracts was 257 (54.7%). As a result of conducting a chi-square test to determine the statistical significance of the difference in cataract incidence rate according to sunlight exposure time, it was found that there was a statistically significant difference (Figure 1, Table 2).
Cross tabulations were calculated to verify differences in cataract incidence rates by gender. As a result, in the 2-5-hour group, there were 225 men (46.7%) and 257 women (53.3%), and in the 5 hour or more group, there were 297 men (63.2%) and 173 women (36.8%) appeared. As a result of conducting a chi-square test to determine the statistical significance of the difference in cataract incidence rates between men and women according to sunlight exposure time, the cataract incidence rate was 6.6% higher in women than men in the 2-5 hour group, and in the group of more than 5 hours, men was 26.4% higher than that of women, and this was statistically significant (Figure 2, Table 3).
To determine the difference in cataract incidence by sunlight exposure and age, across-analysis was conducted by dividing the subjects into groups over 45 years old and under 45 years old.
As a result, in the group exposed to sunlight for 2 to 5 hours, 317 people (65.8%) were over 45 years old, and 165 people (34.2%) were under 45 years old. In the group exposed to sunlight for more than 5 hours, 317 people (65.8%) were over 45 years old. Of these 376 people (80.0%), 94 people (20.0%) were under 45 years of age. A chi-square test was performed to determine whether the cataract incidence rate according to age was statistically significant. As a result, both the 2 to 5 hours of sunlight exposure group and the 5 or more hours of sunlight exposure group showed a statistically significantly higher incidence of cataracts after the age of 45 compared to before the age of 45 (Figure 3, Table 4).
Logistic regression analysis was performed to verify the effect of age on the occurrence of cataracts. As a result, the logistic regression model was found to be statistically significant (Hosmer & Lemeshow Test: x2=8.872, p=.353), and the explanatory power of the regression model was approximately 60.5% (Nagelkerke R2=.605). As a result of testing the significance of the regression coefficient, age (OR=1.173, p<.001) was found to have a significant effect on the incidence of cataracts. It was estimated that age increases by about 1.173 times when it increases by one level (Table 5)
Cross-tabulation analysis was conducted on 896 people (94.1%) out of a total of 952 people, excluding 56 people (5.9%) with missing data, to verify the difference in cataract incidence according to education level.
As a result, in terms of sunlight exposure of 2 to 5 hours, there were 143 (31.4%) elementary school graduates, 72 (15.4%) middle school graduates, 147 (32.3%) high school graduates, and 93(20.4%) university graduates.
And in groups of 5 hours or more, elementary school 211 people (47.8%) graduated from middle school, 64 people (14.5%) graduated from high school, 212 people (27.4%) graduated from high school, and 45 people (10.2%) graduated from university.
As a result of conducting a chi-square test to determine the statistical significance of the cataract incidence rate due to differences in curriculum according to sunlight exposure time, the cataract incidence rate was higher for university graduates than for elementary school graduates in the 2-5 hours group, and in the 5 hours or more group, Graduation from elementary school was higher than graduation from university. This was statistically significant (Figure 4, Table 6).
As shown Figure 5, Cross-tabulation analysis was performed to determine differences in cataract incidence according to sunlight exposure and place of residence. As a result, in the group exposed to sunlight for 2 to 5 hours, there were 52 people (10.8%) in the Seoul area and 63 people (13.1%) in the Busan area. In the group lasting more than 5 hours, 36 people (7.7%) were in the Gangwon region and 85 people (18.1%) were in the Gyeong-Buk region. A chi-square test was performed to determine the incidence of cataracts according to residential area. As a result, in the 2 to 5-hour group, the cataract incidence rate was high in large cities such as Seoul and Busan, and in the 5 hour or more group, the cataract incidence rate was significantly higher in rural areas such as Gangwon and Gyeong-Buk.
4. Discussion
Cataracts can be defined as decreased vision due to light scattering in the lens. Global atmospheric changes, such as stratospheric ozone depletion, are expected to increase ground-level ultraviolet (UVR) levels and adversely affect human health. Epidemiological studies and UVR exposure experiments in animals show a relationship between UVR exposure and induced lens turbidity. Latitude and daylight hours are also associated with cataract incidence [18,19,20]
The notion that human exposure to ultraviolet wavelengths of sunlight is a factor in the development of cataracts has been around for many years (Duke Elder, 1926; Clark, 1935). And for many years, good experimental evidence has been obtained [21,22]. The free radicals produced by UV, oxygen, and ozone present in the external environment cause cell damage, and the lens of the eye is always exposed to these oxidative stresses [23].
The sunlight coming to Earth from the sun consists of electromagnetic waves of various wavelengths. In the vacuum of the upper atmosphere, it consists of 50% infrared, 40% visible, and 10% ultraviolet light, with a total incident energy of approximately 1.4 kW/m2 [24]. UV rays are known to accelerate skin aging. Likewise, because the eyes are transparent tissues that are exposed to direct sunlight along with the skin, it is expected to be related to eye aging, and light including ultraviolet rays is likely to play a very important role in the development of diseases [25].
Tang Y et al. studied the relationship between outdoor activity and age-related cataract risk. In a population-based cross-sectional study of outdoor activity and age-related cataract risk in a rural population from July to September 2012, 883 adults (44.0%) of participants had a diagnosis of cataract [17]
A study by Li X et al. analyzed the correlation between sunlight and cataracts through a meta-analysis and showed that sunlight exposure was associated with a slightly higher risk of cortical cataracts in three types of the cataract [15].
Lawrence et al. examined the relationship between cataract prevalence, altitude, and sunlight hours in a large, national probability sample survey conducted in 105 districts of the Himalayan Kingdom of Nepal from December 1980 to April 1981. Age- and gender-standardized cataract prevalence was 2.7 times higher in areas below 185 m than in areas above 1000 m. Cataract prevalence showed a negative correlation with altitude (r=-0.533, p< 0.0001). However, there was a significant correlation between cataract prevalence and sunlight. A positive correlation was observed between the two (r = 0.563, p < 0.0001). Areas with an average of 12 hours of sunlight had 3.8 times more cataracts than areas with an average of 7 hours of sunlight [26].
In this study's analysis of the difference in cataract prevalence according to sunlight exposure and time, the proportion of subjects without cataracts in the 2-5-hour sunlight exposure group was significantly higher than that of subjects with cataracts. On the other hand, in the 5-hour or longer group, the proportion of subjects with cataracts was significantly higher than the proportion of subjects without cataracts. Therefore, the prevalence of cataracts according to sunlight exposure time in Korea concluded that there is a risk of developing cataracts when exposure to sunlight is more than 5 hours. Although there was a slight lag compared to previous studies, the results were identical, suggesting that sunlight exposure is related to ultraviolet rays. As a result of analyzing the prevalence of cataracts according to sunlight exposure time, the majority of Korean adults had nuclear cataracts (73.2%), followed by cortical cataracts (25.4%) and posterior subcapsular cataracts (1.3%). These results were similar to those studied by Xu L et al [27].
Additionally, our study's analysis of differences in cataract incidence by sunlight exposure and gender showed that, interestingly, men exposed to sunlight for more than 5 hours had a higher incidence of cataracts. However, in the case of women, the incidence of cataracts was higher in the group exposed to sunlight for 2-5 hours, so a temporal difference in the occurrence of cataracts according to gender could be confirmed. This time difference also suggests that women are more vulnerable to sunlight exposure than men when it comes to cataract prevalence. In a study analyzing the prevalence of cataracts in Koreans from 2008 to 2011, the prevalence of cataracts was higher in women (42.3%) than in men (38.9%), and is partially consistent with previous studies that included causes of environmental exposure [28].
Tsai et al.'s analysis of 806 patients diagnosed with age-related cataracts found that women had a higher prevalence of cataracts than men (64.0% vs. 56.1%, p=0.004). This involved nuclear cataracts (38.9%) being the most common type, followed by cortical cataracts (21.9%) and posterior subcapsular cataracts (9.2%) [29].
In CruickshanksK et al.'s study on ultraviolet light exposure and lens opacity (CruickshanksK, et al., 1992), the relationship between sunlight exposure and the UVB (ultraviolet-B) component of light and lens opacity was investigated. The results showed that men with higher average annual UVB light levels were 1.36 times more likely to have more severe cortical opacities than men with lower average annual UVB light levels [30].
The ozone layer present in Earth's atmosphere absorbs most of the light from space. This ozone layer absorbs 100% of ultraviolet C and 90% of ultraviolet B, but ultraviolet A is not absorbed by the ozone layer and enters the Earth's atmosphere. Because the absorption process of ultraviolet rays also occurs in the atmospheric layer, it is known that ultraviolet B and ultraviolet A are transmitted to the actual Earth's surface at a ratio of 1:20 [31].
Human eyes cannot avoid continuous exposure to sunlight and artificial light. The transmission of light through the eye is fundamental to the unique biological functions that direct vision and circadian rhythms. Therefore, the light absorbed by the eye must be positive. However, for those over 40 years of age, exposure to ambient radiation is very dangerous and can lead to vision loss and temporary or permanent blindness. Both UV-A and UV-B cause cataract formation and are not necessary for vision [32].
Of all the important factors in Kanthan's study, as in previous studies, age was the most important risk factor for cataracts, with older age having a significantly higher incidence of geriatric cataracts compared to those aged 40 to 49 years [33]. Senile cataracts are the most common type in adults, beginning between the ages of 45 and 50 [34]. Aging is the most significant risk factor for cataracts because structural and functional changes in the lens can promote the development of cataracts [35].
This result is partially consistent with the results of our study analyzing the difference in cataract incidence by sunlight exposure and age. The results showed that both the group exposed to sunlight for 2 to 5 hours and the group exposed to sunlight for more than 5 hours had a statistically significantly higher incidence of cataracts after the age of 45 compared to before the age of 45.
Various previous research results related to the level of education on cataracts show that Lower education level was associated with cortical cataracts and nuclear cataracts. Educational status may have a dependent relationship with socioeconomic status. However, it has actually been shown to be an independent risk factor for cataracts [36,37]. They also reported that socioeconomic status and educational status may present the possibility of more risk factors associated with common lifestyles that may create risk factors that have not yet been explained [36,37].
The results of our study's analysis of differences in cataract incidence according to sunlight exposure and education level showed that the incidence of cataracts was higher in college graduates than in elementary school graduates when exposed to sunlight for 2 to 5 hours. In the 5 hours or more group, it was confirmed that elementary school graduates had a higher incidence of cataracts than college graduates.
In addition, as a result of analyzing the difference in cataract incidence according to sunlight exposure and place of residence, the cataract incidence rate was significantly higher in large cities such as Seoul and Busan in the 2-5 hours group, and the incidence rate was significantly higher in rural areas such as Gangwon-do and Gyeongbuk in the 5-hour or more group. It was very high. Therefore, it was confirmed that the prevalence of cataracts was higher in large cities despite shorter sunlight exposure times than in rural areas. Meanwhile, a study in Taiwan reported that the prevalence of cataracts was higher in participants living in highly urbanized areas than in participants living in other levels of urbanization [22,38].
Another study also reported that, looking at urbanization of residential areas, the incidence of senile cataracts was significantly higher in people living in highly urbanized areas compared to those in moderately urbanized areas [39].
However, another study reported that the prevalence of cataracts was higher in rural areas than in urban areas in southern India, and that people living in rural areas were more likely to develop cataracts [40].
In this study, we found that Koreans had a higher incidence of cataracts in those exposed to sunlight for more than 5 hours. And the difference according to gender was that when the sunlight exposure time was 2 to 5 hours, the cataract incidence rate was higher in women, and when the sunlight exposure time was more than 5 hours, the cataract incidence rate was higher in men. Additionally, the age-related incidence of cataracts significantly increased after age 45 in both the 2-5 hours and more than 5 hours groups. In terms of education level, the prevalence of cataracts was higher among college graduates in the 2 to 5-hour usage group, and the prevalence of cataracts was higher among elementary school graduates in the more than 5-hour usage group. In urban areas, the prevalence of cataracts was higher in those exposed to sunlight for 2 to 5 hours, and in rural areas, those exposed to sunlight for more than 5 hours. Therefore, Koreans' sunlight exposure time, especially more than 5 hours, was associated with an increased prevalence of cataracts, and various demographic factors affecting the incidence were identified.
5. Conclusions
In our study, we found that Koreans had a higher incidence of cataracts in those exposed to sunlight for more than 5 hours. And the difference according to gender was that when the sunlight exposure time was 2 to 5 hours, the cataract incidence rate was higher in women, and when the sunlight exposure time was more than 5 hours, the cataract incidence rate was higher in men. Additionally, the age-related incidence of cataracts significantly increased after age 45 in both the 2-5 hours and more than 5 hours groups. In terms of education level, the prevalence of cataracts was higher among college graduates in the 2 to 5-hour usage group, and the prevalence of cataracts was higher among elementary school graduates in the more than 5 hour usage group. In urban areas, the prevalence of cataracts was higher in those exposed to sunlight for 2 to 5 hours, and in rural areas, those exposed to sunlight for more than 5 hours. Therefore, Koreans' sunlight exposure time, especially more than 5 hours, was associated with an increased prevalence of cataracts, and various demographic factors affecting the incidence were identified.
Cataracts are the most common disease in ophthalmology, accounting for approximately 50% of blindness worldwide.
Damage to the retina caused by light in daily life is caused by various mechanisms, and damage is particularly likely due to exposure to ultraviolet rays. Understanding trends in cataract prevalence worldwide over the past 30 years and into the future is critical for cataract control in key population groups. Going beyond the current therapeutic approach, the preventive aspect that can reduce the incidence of cataracts should be emphasized in the future. Due to increasingly severe environmental problems, research must be actively conducted to protect eyes from damage related to ultraviolet ray exposure. To achieve this, I believe that research on risk factors related to the development of cataracts is essential. Therefore, we hope that this study will be meaningfully used in the defense role of cataracts in the population.
Author Contributions
Conceptualization, H. J.; validation, H. J.; formal analysis, J. K.; investigation, J. K.; resources, J. K.; data curation, J. K.; writing—original draft preparation, H. J.; writing—review and editing, H. J.; visualization, J. K.; supervision, H. J.; project administration, H. J. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Worgul, B.V.; Merriam, G.R. Jr.; Medvedovsky, C. Cortical cataract development an expression of primary damage to the lensepithelium. Lens Eye Tox Res. 1989, 6, 559-571.
- Taylor, H.R.; West, S.K.; Rosenthal, F.S.; Beatriz, M.S.; Newland, H.S.; Abbdy, F.H.; Emmett, E.A. Effect of ultraviolet radiation on cataract formation. N Engl J Med. 1988, 319, 1429-1433. [CrossRef]
- Zigman, S.; Vaughn, T. Near-ultraviolet light effect on the lenses and retinas of mice. Invest Ophthalmol Vis Sci. 1974, 13, 462-5.
- Spector, A.; Garner, H. Hydrogen peroxide and human cataract. Exp Eye Res. 1981, 33, 673-681.
- Ramachandran, S.; Morris, S.M.; Devamanoharan, P.; Henein, M.; Varma, S.D. Radio-isotopic determination of hydrogen peroxide in aqueous humor and urine. Exp Eye Res. 1991, 53, 503-506 . [CrossRef]
- Dillon, J.; Atherton, S.J.; Time resolved spectroscopic studies on the intact human lens. Photochem Photobiol. 1990, 51, 465–468. [CrossRef]
- Dillon, J. Photophysics and photobiology of the eye. J Photochem PhotobiolB Biol. 1991, 10, 23–40. [CrossRef]
- Roberts, J.E. Ocular phototoxicity. J Photochem Photobiol B Biol. 2001, 64, 136–143.
- Roberts, J.E. Screening for ocular phototoxicity. Int J Toxicol. 2002, 21, 491–500. [CrossRef]
- Spector, A.; Garner, H. Hydrogen peroxide and human cataract. Exp Eye Res. 1981, 33, 673-681.
- Ramachandran, S.; Morris, S.M.; Devamanoharan, P.; Henein, M.; Varma, S.D. Radio-isotopic determination of hydrogen peroxide in aqueous humor and urine. Exp Eye Res. 1991, 53, 503-506. [CrossRef]
- Young, R.W. Solar radiation and age-related macular degeneration. Surv Opht. 1988, 32(4), 252-269. [CrossRef]
- Taylor, H.R. Epidemiology of age-related cataract. Eye. 1999, 13, 445–448. [CrossRef]
- McCarty, C.A.; Taylor, H.R. A review of the epidemiologic evidence linking ultraviolet radiation and cataracts. Dev Ophthalmol. 2002, 35, 21–31.
- Li, X.; Cao, X.; Yu, Y.; Bao, Y. Correlation of Sunlight Exposure and Different Morphological Types of Age-Related Cataract. BioMed Research International, 2021, 12. [CrossRef]
- Cruickshanks, K. J.; Klein, B. E.; Klein, R. Ultraviolet light exposure and lens opacities: the Beaver Dam Eye Study. American journal of public health. 1992, 82, 12, 1658-1662. [CrossRef]
- Tang, Y.; Ji, Y.; Ye, X.; Wang, X.; Cai, L.; Xu, J.; Lu, Y. The association of outdoor activity and age-related cataract in a rural population of Taizhou Eye Study: phase 1 report. PLoS One. 2015, 10, 8 . [CrossRef]
- Hiller, R.; Sperduto, R.D.; Ederer, F. Epidemiologic associations with cataract in the 1971–1972 National Health and Nutrition Examination Survey. Am J Epidemiol. 1983, 118, 239–249. [CrossRef]
- Cruickshanks, K.J.; Klein, B.E.; Klein, R. Ultraviolet light exposure and lens opacities: the Beaver Dam Eye Study. Am J Public Health. 1992, 82, 1658–1662. [CrossRef]
- Dolin, P.J. Assessment of epidemiological evidence that exposure to solar ultraviolet radiation causes cataract. Rev Doc Ophthalmol. 1994, 3(4), 327–337. [CrossRef]
- Duke-Elder, W. S. The pathological action of light upon the eye. Lancet I. 1926, 5365(207), 1250-1255.
- Clark, J. H. The effect of ultraviolet radiation on lens protein in the presence of salts and the relation of radiation to industrial and senile cataract. Am. J. Physiol. 1935, 113, 538. [CrossRef]
- Green, K. Free radicals and aging of anterior segment tissues of the eye: a hypothesis. Ophthalmic Res. 1995, 1, 143-149. [CrossRef]
- Q. Fu, “Solar radiation”. Elsevier Science, 2003, 1859-1863.
- Young, R.W. Solar radiation and age-related macular degeneration. Surv Ophtalmol. 1998, 32(4), 252-269. [CrossRef]
- Brilliant, L.B.; Grasset, N.C.; Pokhrel, R.P.; Kolstad, A.; Lepkowski, J.M.; Brilliant, G.E.; Hawks, W.N.; Pararajasegaram, R. Associations among cataract prevalence, sunlight hours, and altitude in the Himalayas. Am J Epidemiol. 1983, 118(2), 250–264. [CrossRef]
- Xu, L.; Cui, T.; Zhang, S.; Sun, B.; Zheng, Y.; Hu, A.; Li, J.; Ma, K.; Jonas, J.B. Prevalence and risk factors of lens opacities in urban and rural Chinese in Beijing. Ophthalmology. 2006, 113(5), 747-755. [CrossRef]
- Nam, G.E.; Han K.; Ha, S.G. Relationship between socioeconomic and lifestyle factors and cataracts in Koreans: The Korea National Health and Nutrition Examination Survey 2008–2011. Eye. 2015, 29, 913-920. [CrossRef]
- Tsai, S.Y.; Hsu, W.M.; Cheng, C.Y.; Liu, J.H.; Chou, P. Epidemiologic study of age-related cataracts among an elderly Chinese population in Shih-Pai, Taiwan. Ophthalmology. 2003, 110(6), 1089-1095. [CrossRef]
- Cruickshanks, K. J.; Klein, B. E.; Klein, R. Ultraviolet light exposure and lens opacities: the Beaver Dam Eye Study. American journal of public health. 1992, 82(12), 1658-1662. [CrossRef]
- Palm, M.D.; O’Donoghue, M.N. Update on photoprotection. Dermatol. Ther. 2007, 20, 360-376.
- Roberts, J.E. Ultraviolet Radiation as a Risk Factor for Cataract and Macular Degeneration. Eye & Contact Lens: Science & Clinical Practice. 2011, 37(4), 246-249. [CrossRef]
- Kanthan G.L.; Wang J.J.; Roch China E.; Tan AG.; Lee A.; Chia EM.; Mitchell P. Ten-year incidence of age-related cataract and cataract surgery in an older Australian population. The Blue Mountains Eye Study. Ophthalmology. 2008, 115 (5), 808-814.
- Liu YC, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet. 2017, 390(10094), 600-612.
- Budnar P, Tangirala R, Bakthisaran R, Rao CM. Protein aggregation and cataract: role of age-related modifications and mutations in α-crystallins. Biochemistry (Mosc). 2022, 87(3), 225-241. [CrossRef]
- Klein B.; Klein, R.; Lee, K.E.; Meuer, S.M. Socioeconomic and lifestyle factors and the 10-year incidence of age-related cataracts. Am J Ophthalmol. 2003, 136 (3), 506-512. [CrossRef]
- Tyler H. T. R.; Kim, M, H.; Kim, W.C. Cataract subtype risk factors identified from the Korea National Health and Nutrition Examination survey. 2008–2010. BMC Ophthalmol. 2014, 4(14).
- Shih, Y.H.; Chang, H.Y.; Lu, M.I.; Hurng, B.S. Time trend of prevalence of self-reported cataract and its association with prolonged sitting in Taiwan from 2001 and 2013. BMC Ophthalmol. 2014,14,128. [CrossRef]
- WS Yu.; CH Wang.; NW Kuo. Impact of Urbanization and Sunlight Exposure on Cataract Incidence. Appl. Sci. 2021, 11(17), 8137. [CrossRef]
- Raman, R.; Singh, S.; Pardhan, S.; Kulothungan, V.; Swaminathan, G.; Ravichandran, J.S.; Ganesan, S.; Sharma, T. The prevalence and risk factors for cataract in rural and urban. India. Indian J. Ophthalmol. 2019, 67, 477-483. [CrossRef]
Figure 1.
Cataract incidence rates according to sunlight exposure time were divided into two groups.
Figure 1.
Cataract incidence rates according to sunlight exposure time were divided into two groups.
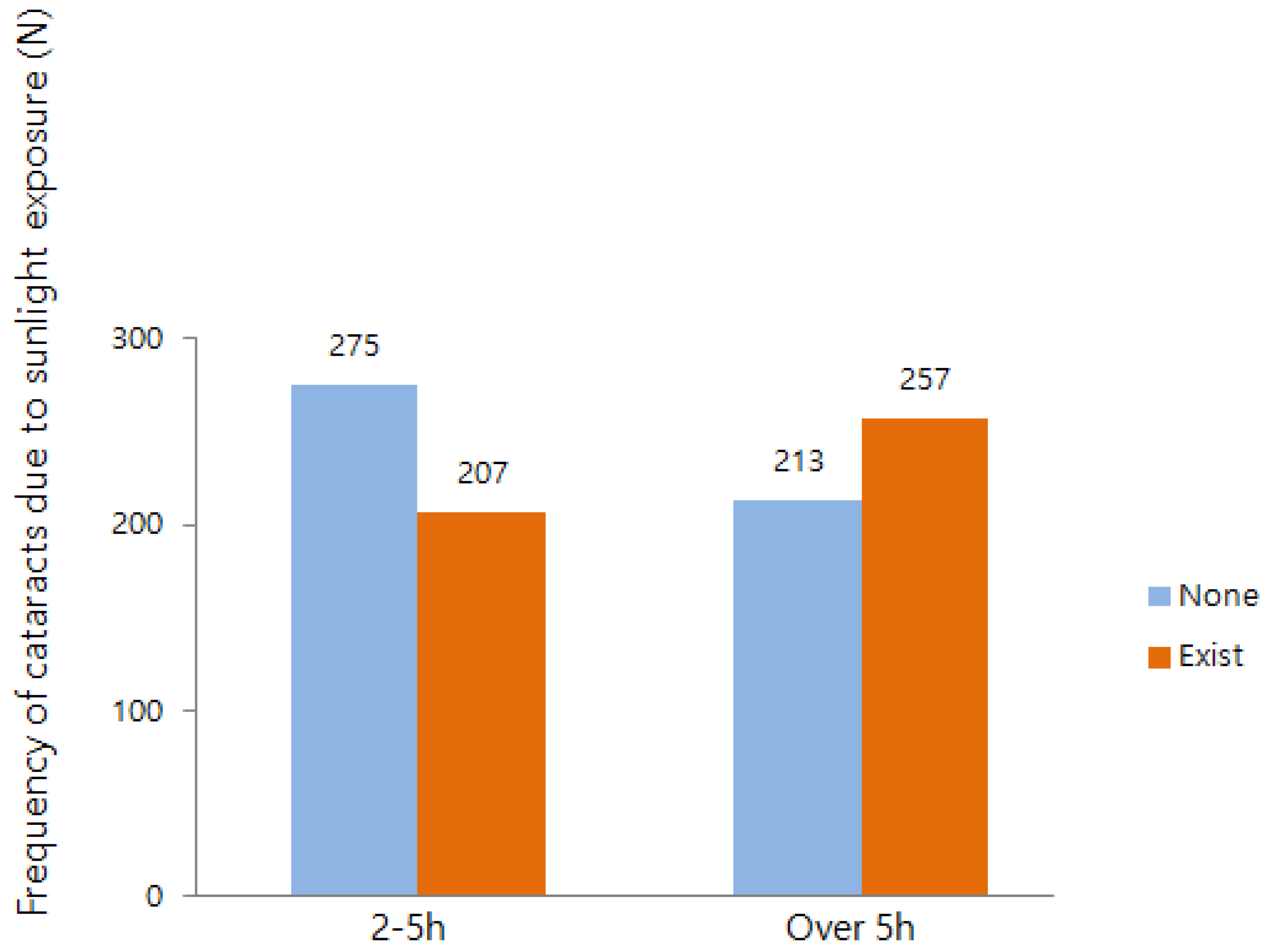
Figure 2.
Cataract incidence rates according to gender were divided into two groups.
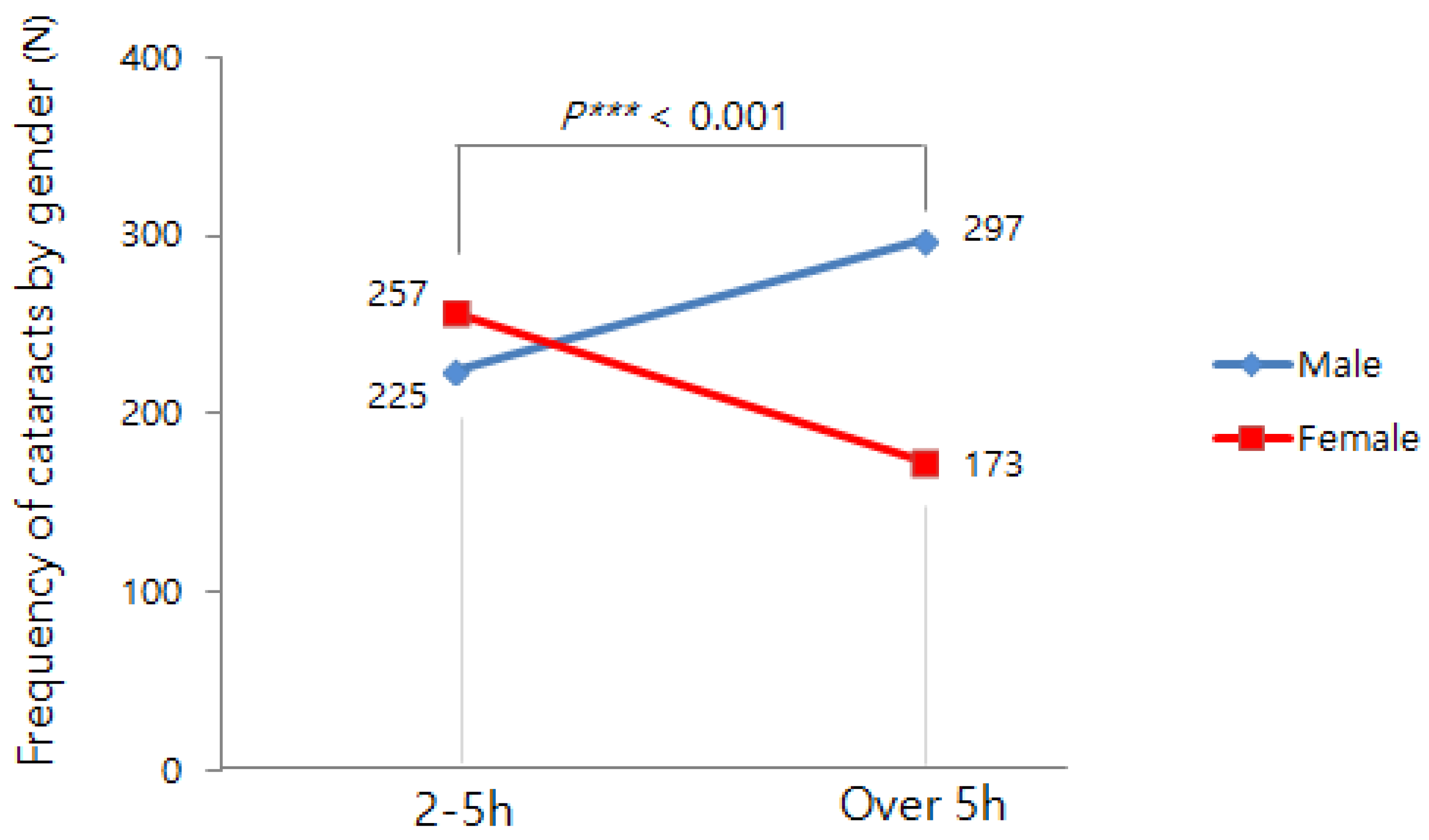
Figure 3.
Cataract incidence rates according to age were divided into two groups.
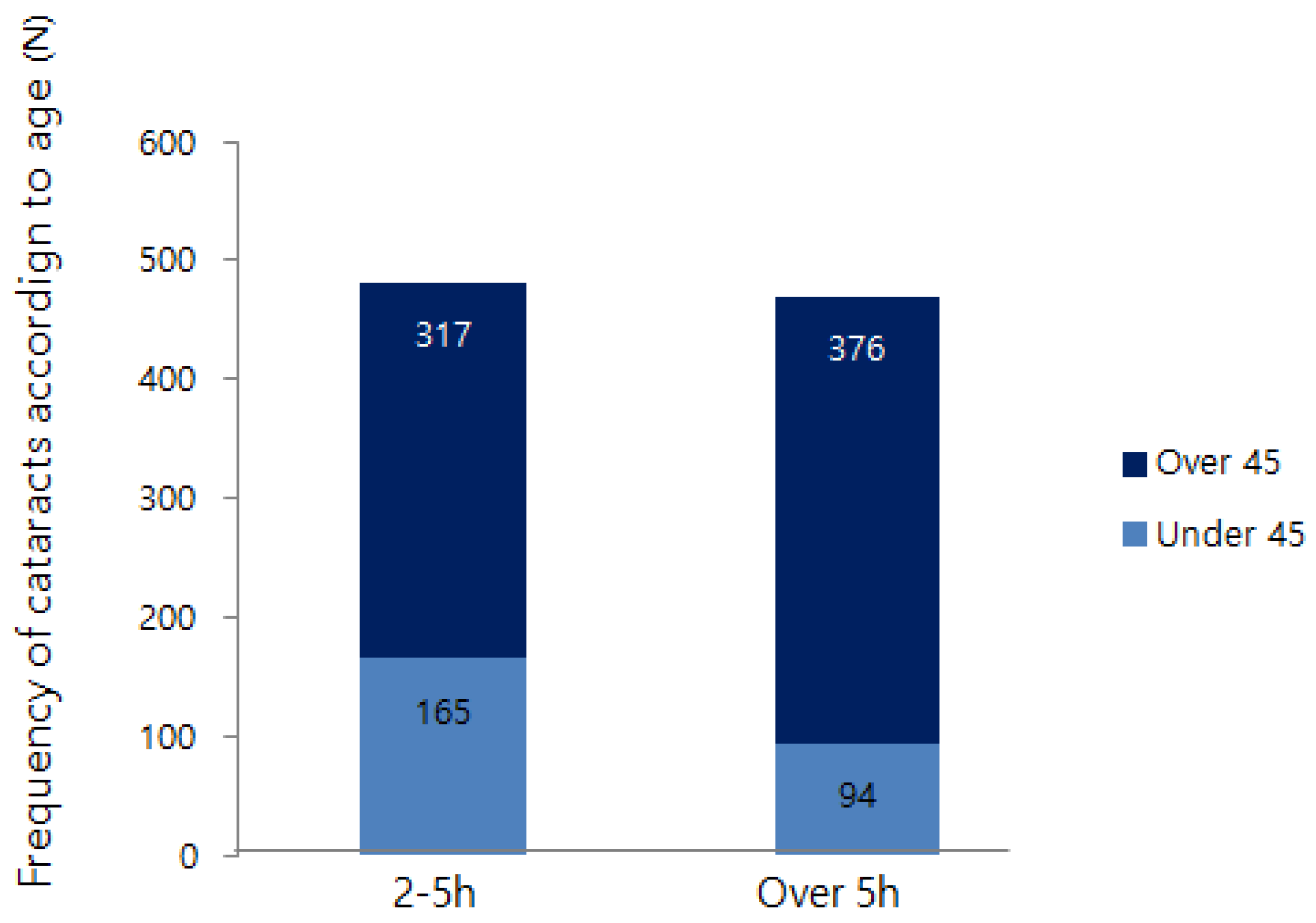
Figure 4.
Cataract incidence rates according to education level were divided into two groups.
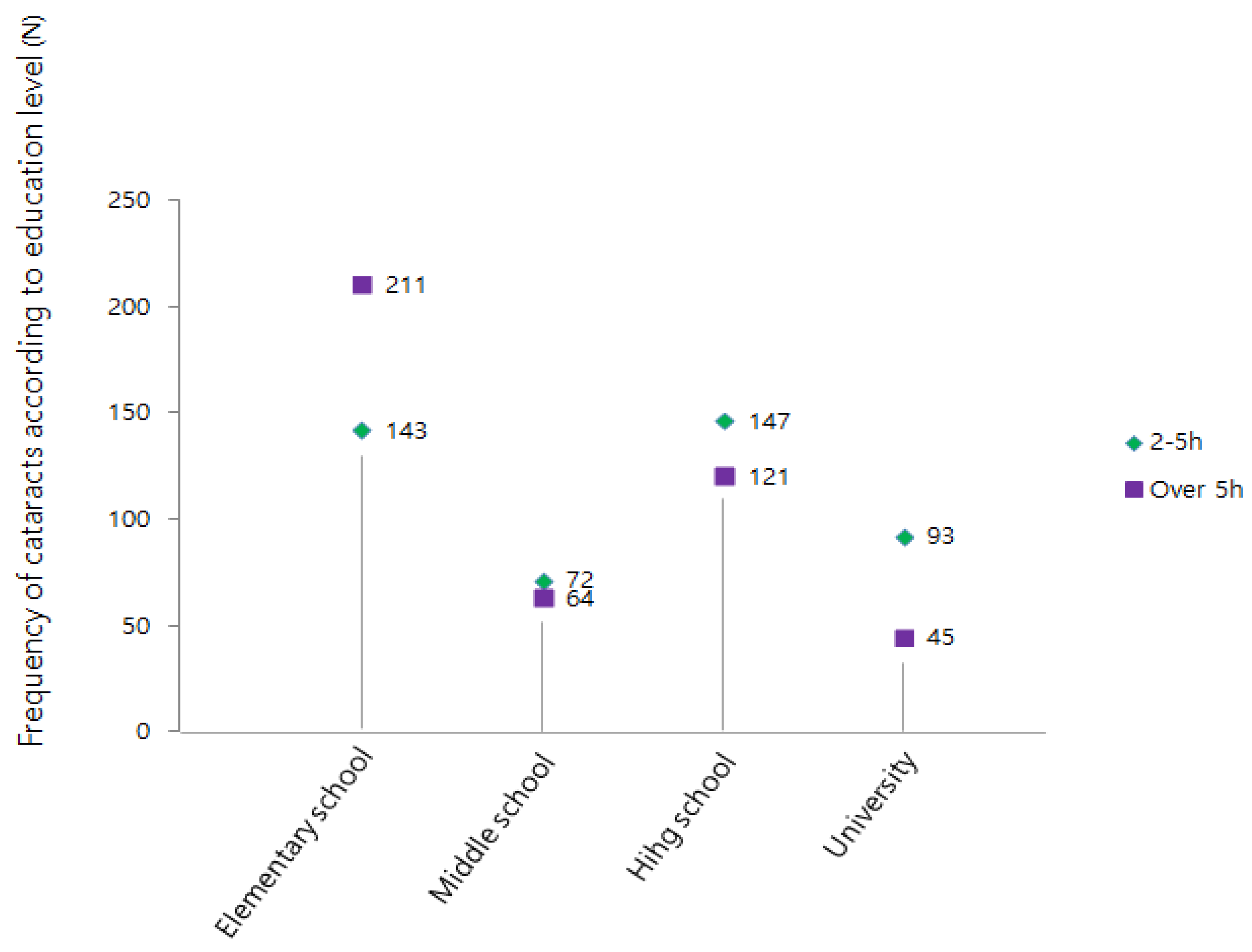
Figure 5.
Cataract incidence rates according to to region of residence were divided into two groups.
Figure 5.
Cataract incidence rates according to to region of residence were divided into two groups.
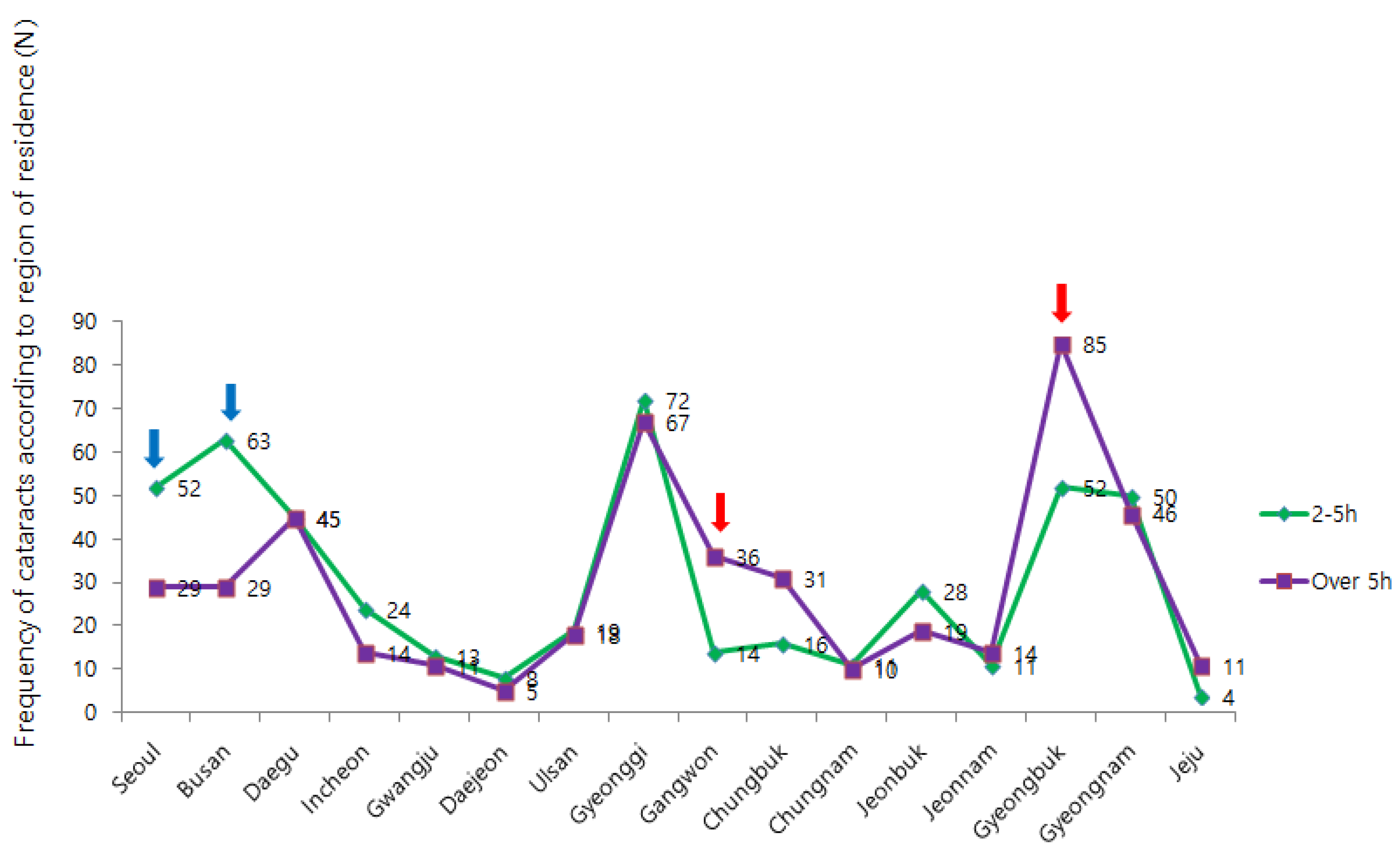

Table 1.
Sociodemographic analysis of study subjects. N= 952.
| Division | Classification | Frequency | Ratio (%) | |
|---|---|---|---|---|
| Sunlight | 2-5-hr | 482 | 50.6 | |
| Over 5-hr | 470 | 49.4 | ||
| Gender | Male | 522 | 54.8 | |
| Female | 430 | 45.2 | ||
| Age | Over 45 | 259 | 27.2 | |
| Under 45 | 693 | 72.8 | ||
| Education Level (n=896) |
Elementary School | 354 | 37.2 | |
| Middle School | 136 | 14.3 | ||
| High School | 268 | 28.2 | ||
| University | 138 | 14.5 | ||
| Residence | Seoul | 81 | 8.5 | |
| Busan | 92 | 9.7 | ||
| Daegu | 90 | 9.5 | ||
| Incheon | 38 | 4.0 | ||
| Gwangju | 24 | 2.5 | ||
| Daejeon | 13 | 1.4 | ||
| Ulsan | 37 | 3.9 | ||
| Gyeonggi | 139 | 14.6 | ||
| Gangwon | 50 | 5.3 | ||
| Chungbuk | 47 | 4.9 | ||
| Chungnam | 21 | 2.2 | ||
| Jeonbuk | 47 | 4.9 | ||
| Jeonnam | 25 | 2.6 | ||
| Gyeongbuk | 137 | 14.4 | ||
| Gyeongnam | 96 | 10.1 | ||
| JeJu | 15 | 1.6 | ||
| Refractive Power (n=869) |
Myopia | 303 | -2.03 D (Std. E. 0.120) | |
| Hyperopia | 566 | 1.31 D (Std. E. 0.042 | ||
Table 2.
Frequency of cataracts due to sunlight exposure.
| Sun Exposure | Total | x2 | p | |||
|---|---|---|---|---|---|---|
| 2-5-hr | Over 5-hr | |||||
| Prevalence of cataract |
Non. | 275(57.1) | 213(45.3) | 488(53.1) | 13.116 | .000*** |
| Exist. | 207(42.9) | 257(54.7) | 464(48.7) | |||
| Total | 482(100) | 470(100) | 952(100) | |||
p*<0.05, p**<0.01, p***<0.001 Unit: Frequency (%).
Table 3.
Frequency of cataracts due to gender.
| Sun Exposure | Total | x 2 | p | |||
|---|---|---|---|---|---|---|
| 2-5-hr | Over 5-hr | |||||
| Prevalence of cataract |
Male | 225(46.7) | 297(63.2) | 522(100) | 26.193 | .000*** |
| Female | 257(53.3) | 173(36.8) | 430(100) | |||
| Total | 482(100) | 470(100) | 952(100) | |||
p*<0.05, p**<0.01, p***<0.001 Unit: Frequency (%).
Table 4.
Frequency of cataracts due to age.
| Sun Exposure | Total | x 2 | p | |||
|---|---|---|---|---|---|---|
| 2-5-hr | Over 5-hr | |||||
| Prevalence of cataract |
Over 45 | 317(65.8) | 376(80.0) | 693(72.8) | 24.339 | .000*** |
| Under 45 | 165(34.2) | 94(20.0) | 259(27.2) | |||
| Total | 482(100) | 470(100) | 952(100) | |||
p*<0.05, p**<0.01, p***<0.001 Unit: Frequency (%).
Table 5.
Increasing age affects the development of cataracts.
| Dependent Variable | Independent Variable | B | S.E. | OR | 95% CI | p |
|---|---|---|---|---|---|---|
| Prevalence | Age | 0.160 | 0.010 | 1.173 | (1.150~1.197) | .000 |
-2LL=743.781, Nagelkerke R2=.605, Hosmer & Lemeshow Test:x2=8.872 (p=.353).
Table 6.
Frequency of cataracts due to education level.
| Sun Exposure | Total | x 2 | p | |||
|---|---|---|---|---|---|---|
| 2-5-hr | Over 5-hr | |||||
| Prevalence of cataract |
Elementary school | 143(31.4) | 211(47.8) | 354(39.5) | 32.540 | .000*** |
| Middle school | 72(15.4) | 64(14.5) | 136(15.2) | |||
| High school | 147(32.3) | 212(27.4) | 268(29.9) | |||
| University | 93(20.4) | 45(10.2) | 138(15.4) | |||
| Total | 455(100) | 441(100) | 896(100) | |||
p*<0.05, p**<0.01, p***<0.001 Unit: Frequency (%).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



