
Submitted:
02 May 2024
Posted:
06 May 2024
You are already at the latest version
Abstract
Background: Malnutrition commonly affects patients with oral squamous cell carcinoma (OSCC), which contributes to worsening prognosis. Moreover, specific strategies for diagnosing and managing malnutrition in OSCC are lacking. Methods: This retrospective study included 52 consecutive patients with OSCC who underwent surgery at the University Hospital of Palermo (I) from Jan 2020 to May 2023. In-hospital nutritional support was provided by a dedicated team. The patients were compared with a historical control group of 11 patients. The nutritional treatment consisted of standard oral (ON) or artificial nutrition (AN). Traditional measurements, including bioimpedance-derived body composition and volumetric reconstruction of the posterior paraspinal muscles at the C3 level based on magnetic resonance imaging (MRI-C3), were obtained in 16 patients to investigate sarcopenia. Results: The patients were categorized according to TNM stage: groups A (TNM stages I-III) and B (IVa-IVc). The prevalence of group A patients was 59.6% in the case group and 90.9% in the control group (P
Keywords:
Oral cancer
; malnutrition
; artificial nutrition
; bioimpedance analysis
1. Introduction
Head and neck malignant tumors represent approximately 3% of all malignant tumors in Italy [1]. Similar to what has been observed in the European Union, in Italy, the annual incidence of head and neck cancers is 18/100.000 inhabitants; about 93% of these cancers are epithelial tumors, and 90% are malignant squamous cell carcinomas [2]. Malnutrition is characterized by the depletion of energy, protein reserves, and other nutrients in the body, compromising health and leading to increased morbidity and mortality [3]. Malnutrition is frequently associated with head–neck malignant tumors and is a challenging condition that often requires invasive nutrition [4]. Tumors are the chronic condition with the highest incidence of malnutrition, affecting quality of life, healthcare costs, and survival, often preventing the possibility of drug or surgical treatment [5]. Squamous cell carcinomas of the oral cavity (OSCC) rank as the second most common type of malignancy associated with malnutrition, following malignancies of the gastrointestinal tract [6]. This is due not only to the stage of the tumor but also to dysphagic symptoms that occur even before diagnosis, radiation therapy that may result in xerostomia, and subsequent resection surgeries that lead to functional alterations in mastication and swallowing [7]. Therefore, early comprehensive nutritional assessments and rigorous monitoring programs are recommended for specific oncological patients including those with head and neck tumors [8,9,10,11]. Patients with OSCC may require invasive nutritional support such as nutrition via percutaneous endoscopic gastrostomy (PEG) or nasogastric tube (NG tube) even post-hospitalization, posing a considerable challenge for management in outpatient or community settings. Globally, malnutrition related to oncological diagnosis remains largely unrecognized, underestimated, and inadequately addressed in clinical practice [12]; hence, the early diagnosis of malnutrition is a current challenge [13]. For this purpose, suitable methods for measuring the amount of lean body mass are necessary. The bioimpedance analysis (BIA) is a frequently used method due to low cost, safety, high feasibility by non-specialized operators, and repeatability [14]. However, BIA accuracy may be often compromised in hospitalized patients due to altered fluid distribution or fluid infusions [15]. Imaging techniques, such as magnetic resonance (MR) or computed tomography (CT) imaging, are powerful tools for investigating muscle and adipose tissue; however, these methods are still confined to research settings due to their costs and complexity of use [16].
Therefore, we investigated the prevalence of malnutrition and retrospectively compared the effect of ON and AN treatment on survival in a cohort of patients with OSCC. Moreover, in a subgroup of patients, we preliminary evaluated the MRI volumetric reconstruction of posterior paraspinal muscles at the level of the third cervical vertebra as a possible specific measure of the fat-free mass (MRI-C3).
2. Materials and Methods
2.1. Selection of Patients
Patients who underwent surgery for OSCC at the Unit of Plastic Surgery of the University Hospital Policlinico “P. Giaccone” in Palermo (Italy) between January 2020 and May 2023, were retrospectively identified and included in this study. Briefly, starting in January 2020, a dedicated team of doctors and dieticians of the Unit of Clinical Nutrition, Obesity, and Metabolic Diseases offered specific nutritional support during hospitalization. Patients were classified according to the most recent definition of TNM stage [17]. Upon discharge, nutritional assistance was taken care of by the local health services. Data collected were retrospectively compared with data retrieved from clinical records of a control group that consisted of patients surgically treated for OSCC analog oncological conditions between January and December 2019 in the same unit of surgery in the absence of a dedicated nutritional team. Moreover, MRI exams of those patients who were evaluated before and 3-12 months after surgery at the radiology unit of the same hospital were collected. All patients provided written consent for the use of their data for scientific purposes. Detailed medical history, anthropometric measurements, and laboratory data were recorded. After surgery, radiation or chemoradiation therapy was added as adjuvant treatment for high-risk patients. Systemic therapy could be used in cases of locoregional recurrence or distant metastases.
Information concerning survival was obtained from medical records or by phone contact with patients or their caregivers.
2.2. Measurements
Anthropometric data such as height, body weight, body mass index (BMI, body weight (kg)/height2 (m2)), and mid-arm and calf circumferences (cm) were obtained. The Mini Nutritional Assessment (MNA) score for the screening of malnutrition was recorded. An MNA total score of <17 was indicative of malnutrition and a score of 17–23 was indicative of risk of malnutrition [18].
Body composition (fat mass, FM; fat-free mass, FFM) was determined when permitted by clinical conditions using bioelectrical impedance analysis (BIA; BIA-101 Anniversary, Akern; Florence, Italy) and according to the manufacturer's equations [19]. Briefly, patients were evaluated in the morning after an overnight fast, in the supine position, and body resistance (R, Ohm), reactance (Xc, Ohm), and phase angle [PA degrees= arctan (Xc/R) × (180/π)] were measured. In some cases, BIA could not be performed due to compromised general clinical conditions, concomitant venous treatments, or difficulties in applying electrodes due to the presence of vein catheters. Images and reports of MRI were retrospectively analyzed. Briefly, T1 sequences with and without fat saturation and i.v. gadolinium, T2, and STIR sequences on the axial and coronal planes with a maximum slice thickness of 4 mm were acquired using a 1.5T and 3T MRI device (Ingenia 3.0 T, Philips Healthcare, Best, The Netherlands; Achieva 1.5 T Philips Healthcare, Best, The Netherlands). Volumetric evaluation of paravertebral space muscles was performed using segmentation of 5 slices at the C3 vertebra level on axial T2 images with "3D-slicer" software [20]. Muscle strength was measured as hand-grip strength using a hydraulic hand dynamometer (JAMAR SH5001; Saehan; Republic of Korea). Patients performed the test while sitting (if possible) and were requested to perform a maximal isometric contraction. Three tests were repeated at intervals of 15-20 seconds with each hand, and the average value (kg) of the three tests was used for the analysis [21]. Each patient underwent routine blood tests during hospitalization using standard methods. The following serum parameters at first measurement were recorded for the purposes of the study: glucose, creatinine, albumin, total proteins, total cholesterol, white blood cells, hemoglobin, lymphocytes, iron, ferritin, folic acid, vitamin B12, vitamin D, sodium, potassium, magnesium, and phosphorus.
2.3. Dietary Assessment and Support
Daily energy requirements of hospitalized patients following surgery were estimated as 30 kcal/kg body weight/day monitoring body weight and adjusting intake as required, and protein intake was 1.2 g/kg body weight/day [12,22]. On the basis of nutritional assessment, individualized nutritional support was prescribed, including dietary plans, oral supplements, enteral or parenteral nutrition, or combination strategy. The choice of the type of support was tailored to a single patient's characteristics, needs, overall clinical features, and self-feed ability following current guidelines [12].
2.4. Statistical Analysis
Patients were categorized based on TNM staging (stage A: I, II, and III; stage B: IVa, IVb, and IVc) and nutritional practices at discharge (oral nutrition, ON; artificial nutrition AN). Data are presented as means ± SD for continuous variables and as percentages for categorical variables. Student’s t-test or Pearson's chi-square test was applied to compare between-group differences. Kaplan–Meier survival curves were constructed and outcome differences were evaluated using the log-rank test. Multivariate Cox regression stepwise analysis was applied to determine the independent factors associated with mortality. Hazard ratios with 95% confidence intervals were presented. Simple linear correlation analysis with calculation of r coefficients investigated the association between variables. A P-value of < 0.05 was considered statistically significant. All statistical analyses were performed using Systat (Windows version 13.0; San Jose, CA USA).
3. Results
A total of 52 cases and 11 controls were selected. The participant selection flowchart is shown in Figure 1.
The two groups were not comparable; in fact, the control group included a higher prevalence (85.7% vs. 59.6%) of less severe cases (TNM I-III) with higher survival rates at follow-up than the case group (80.5% vs. 27.3%). Given the limited number of cases, all patients were included in a unique group. Physical, clinical, and nutritional characteristics of patients are reported in Table 1 and Table 2.
The mortality rate was significantly higher in the group with severe TNM stage (Table 1) and in patients on artificial nutrition (Table 2). The Kaplan–Meier survival analysis demonstrated that TNM I-III (Figure 2) and ON (Figure 3) had a higher survival probability that progressively reduced through the TNM stage and the modality of nutrition in different combinations from TNM I-III+ON to TNM IV+AN (Figure 4).
Cox proportional hazard regression (stepwise) analysis including TNM stage A vs. B, nutrition ON vs. AN, serum creatinine <0.7 g/dl, BMI <18.0 kg/m2, and age <70 years as categorical variables demonstrated an independent effect (χ2= 20.8; P< 0.001) on the outcome of death according to TNM stage (IV vs. I-III; P< 0.05; HR, 3.67; 95% CI, 1.05-12.9) and nutrition modality (AN vs. ON; P< 0.05; HR, 4.98; 95% CI, 1.07-23.2). The change in MRI_C3 (Δ MRI_C3) 3-12 months after surgery was obtained in a subsample of 16 patients; the results showed that MRI_C3 increased significantly in ON-treated patients and decreased in patients receiving AN treatment (Table 2); moreover, MRI_C3 was not significantly different between patients with TNM I-III and TNM IV (1803 ± 7201 mm3 vs. -148 ± 8863 mm3; P= 0.64). The MRI_C3 before surgery was significantly correlated with the FFM-kg (r= 0.73; P< 0.05), BIA resistance (r= -0.87; P< 0.005), and reactance (r= -0.78; P< 0.05); the change in MRI_C3 was correlated with the FFM-kg (r= 0.87; P< 0.005) (Figure 5).
4. Discussion
This study agrees with previous investigations demonstrating that OSCC patients often develop malnutrition even before surgical treatment, a condition that may reduce the possibilities of effective therapy [23]. In fact, we observed a high prevalence of malnutrition or risk of malnutrition in the TNM B group and, following surgery, invasive nutrition was prescribed in the majority of these patients (86.4%). However, in patients with a lower stage of the disease (TNM A group), we also observed a high prevalence of malnutrition, which suggests that patients with OSCC experience difficulties in consuming food independently from the stage of the disease. The diagnosis of malnutrition is challenging in patients with OSCC and we confirm [22] that many traditional indicators of malnutrition, such as BMI, fat mass, fat-free mass index, MNA, hemoglobin, creatinine, or hand-grip test, may not be adequate in this particular cancer (Table 1). On the other hand, measurements such as bioelectrical reactance and phase angle or serum proteins and albumins were significantly altered in the TNM B group with respect to the TNM A group. On account of the difficulties in obtaining the traditional measures indicative of malnutrition in all patients [15], new diagnostic tools need to be defined for use in people with head–neck tumors that are also in support of the BIA method, which may present some limitations in admitted patients [15]. In fact, patients undergoing surgery for OSCC often require complex reconstructive procedures, including skin and muscle grafts taken from the limbs, with consequent difficulty in positioning electrodes. The BIA measurements may also be altered due to the presence of localized edema of the neck and upper limbs consequent to lymphadenectomy [24]. Currently, computed tomography (CT) and DEXA techniques are reference methods but rarely accessible. In particular, the CT is the gold standard method for assessing muscle mass through the muscle mass index calculated from the L3 vertebra [25]; however, its application is also limited by the exposure to large amounts of X-rays since in many patients the CT of the abdomen is not requested for staging the disease or for follow-up purposes. Ultrasound has the intrinsic limitation of being an operator-dependent technique with low reproducibility. Recently, Fernandez-Jimenez et al. [26] found that different ultrasound measurements of the quadriceps rectus femoris muscles were associated with malnutrition in patients with head–neck cancer, but the predictive value of the probability of survival was rather low. Interestingly, it was recently proposed to evaluate the cross-sectional area of the neck muscles at C3 as a marker of sarcopenia [27,28,29]. In the present study, we tried to develop an alternative technique using MRI to measure the volume of paravertebral muscles at that level. This approach may present some considerable advantages. In fact, an MRI of the neck is always available in these patients, even at follow-up. Furthermore, the paravertebral muscles are used in any case and are not expected to be altered by potential confounding factors such as atrophy secondary to muscular inactivity, as it may occur for muscles of the lumbar region or lower limbs of patients forced into inactivity in bed or in an armchair. In previous studies [28; 29], all areas of the muscles of the neck were segmented as a single slice at the level of the C3 vertebra. However, patients with OSCC typically undergo radical or modified radical neck dissection, which includes sternocleidomastoid muscle removal in the most advanced stages. Therefore, we excluded sternocleidomastoid muscle segmentation generating a widely applicable MRI system for investigating differences during follow-up. To the best of our knowledge, this is the first study to focus exclusively on the paraspinal muscles, which are usually preserved by surgery and are less affected by reduced physical activity or bedridden syndrome. Indeed, the ergonomics of neck muscles is to be considered. In fact, in the upright position, the head is balanced and moves on the neck, with the gravity vector largely parallel to the neck. In the clinostat position, as during bed rest, the gravitational forces are predominantly perpendicular to the neck, which means that greater muscle strength is required to lift and move the head [30], implying a surplus of exercise for this muscle compartment that may contribute to preserving it more than other muscles. Moreover, we segmented the MRI images of the paraspinal muscles of the neck in five slices at the C3 vertebra level and calculated the muscle volume. Therefore, moving from bi-dimensional to three-dimensional segmentation is expected to improve accuracy [30; 31]. Interestingly, in the small subsample of patients who also had BIA values available (Figure 5), highly significant correlations were observed between the volume of paravertebral muscles at C3 and the values of resistance and fat-free mass. We obtained MRI_C3 measurements in only 16 patients and observed that, before surgery, those who underwent AN treatment had significantly lower values than patients receiving ON treatment, thus suggesting a higher prevalence of sarcopenia (Table 2).
The diagnosis of malnutrition is of great importance in patients with OSCC as it may affect the survival and the adoption of the most appropriate nutritional strategies. As expected, the TNM stage significantly influenced the probability of survival (Figure 2); however, surprisingly, the AN treatment was independently associated with a lower probability of survival than the ON (Table 2, Figure 3 and Figure 4). This result may indicate that AN treatment is associated with a more advanced stage of the disease but also that patients receiving AN have a higher prevalence of malnutrition as the BMI or phase angle value would suggest [32] (Table 2). We cannot exclude that the nutritional follow-up of patients receiving AN treatment would have requested special attention following discharge. In fact, the MRI_C3 3-12 months after surgery increased in patients receiving ON treatment but reduced in those receiving AN, suggesting that malnutrition worsened in the latter group after surgery. Managing oncologic patients is challenging during hospitalization and likely even more so after discharge [11]. Nutrition home management in oncological patients, especially for invasive nutrition, is strongly influenced by territorial healthcare organizations and the socioeconomic status of patients. For specific oncological patients, such as those with head and neck cancers, the importance of structuring comprehensive nutritional assessments and rigorous monitoring programs is emphasized [11]. Our results contribute to highlighting these serious nutritional problems and the need for dedicated professionals to care for them during hospitalization and after discharge [12].
In the present study, males and females were equally affected by OSCC; this result is in agreement with the current progressive reversal of epidemiological trends, probably due to the increasing habit of smoking in women [33]. However, two-thirds of patients receiving the artificial nutrition treatment were female, suggesting a higher prevalence of malnutrition and more severe cases in women; this gender difference remains to be investigated.
This study has intrinsic limitations. First, the aim of this study was to organize a longitudinal retrospective case–control study; however, we could not obtain an adequate control group. This aspect is mainly due to the fact that the unit of surgery where patients were enrolled treated less serious cases in the past and subsequently opened up to more complex cases; therefore, we could not obtain a real historical control group. However, the probability of organizing a real case–control intervention study is low since prospective, longitudinal studies are basically unethical, and retrospective studies have low probabilities of recruiting a real control group as evidenced in this study. Another limitation was the absence of data at follow-up apart from those concerning survival. This fact suggests the need for a more stringent collaboration between hospital and territorial systems of assistance, which is a matter that is not easy to implement given the particular gravity of the disease that in many instances requests long-term institutionalizations even far from the place of care. Finally, this was a monocentric study with a limited number of cases and fragmented data; in future studies, an adequate network between different centers is required in order to collect and share data that may contribute to a better understanding of the specific role of nutritional factors and the implementation of strategies of treatment.
5. Conclusions
This study demonstrates that malnutrition is almost invariably associated with oral OSCC, often precedes surgical treatment, requires AN treatment in a high percentage of cases, and that the latter is independently and unfavorably associated with survival. The MRI measurement of the volume of paraspinal muscles at the C3 level is a promising technique for diagnosing and monitoring sarcopenia. There is a need for teams dedicated to the nutritional management of patients with OSCC, as this condition may influence patient prognosis and quality of life.
Author Contributions
Conceptualization, P.B., S.B., A.C., and A.L.; methodology, P.B., S.B., C.R., and A.L.; software, P.B., and G.Z.; formal analysis, P.B., and S.B.; investigation, P.B., C.R., C.B., E.F., R.C., P.C., M.L., S.C. and G.Z.; resources, S.B., A.L., A.C.; data curation, P.B., C.R., C.B., A.L. and S.B.; writing—original draft preparation, P.B., C.R., S.B., A.L.; writing—review and editing, P.B., C.B., S.B., A.C., and A.L.; supervision, A.L., A.C., and S.B.; project administration, S.B., and CR; funding acquisition, S.B.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not require ethical approval given its retrospective nature. This study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects upon admission to the hospital to utilize their demographic and clinical data for data analysis finalized for clinical research.
Data Availability Statement
We had no authorization from patients to share their clinical data.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- International Agency for Research on Cancer. World Health Organization. Global cancer observatory. URL:https://gco.iarc.fr/ (10/04/2024).
- Istituto Superiore di Sanità, Sistema Nazionale Linee Guida, aprile 2022. URL: https://www.iss.it/documents/20126/8403839/LG493-AIOM-Head-and-neck (10/04/2024).
- Cederholm T, Jensen GL, Correia MITD, Gonzalez MC, Fukushima R, Higashiguchi T, et al., GLIM Core Leadership Committee; GLIM Working Group. GLIM criteria for the diagnosis of malnutrition - a consensus report from the global clinical nutrition community. Clin Nutr. 2019; 38:1e9. [CrossRef]
- Ravasco P, Monteiro-Grillo I, Marques Vidal P, Camilo ME. Impact of nutrition on outcome: a prospective randomized controlled trial in patients with head and neck cancer undergoing radiotherapy. Head Neck 2005; 27(8):659-68. [CrossRef]
- Matsui R, Rifu K, Watanabe J, Inaki N, Fukunaga T. Impact of malnutrition as defined by the GLIM criteria on treatment outcomes in patients with cancer: A systematic review and meta-analysis. Clin Nutr. 2023; 42(5):615-624. [CrossRef]
- Pressoir M, Desné S, Berchery D, Rossignol G, Poiree B, Meslier M, Traversier S, Vittot M, Simon M, Gekiere JP, Meuric J, Serot F, Falewee MN, Rodrigues I, Senesse P, Vasson MP, Chelle F, Maget B, Antoun S, Bachmann P. Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br J Cancer 2010; 102(6):966-71. [CrossRef]
- Martinovic D, Tokic D, Puizina Mladinic E, Usljebrka M, Kadic S, Lesin A, Vilovic M, Lupi-Ferandin S, Ercegovic S, Kumric M, Bukic J, Bozic J. Nutritional Management of Patients with Head and Neck Cancer-A Comprehensive Review. Nutrients 2023; 15(8):1864. [CrossRef]
- Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, Fearon K, Hütterer E, Isenring E, Kaasa S, Krznaric Z, Laird B, Larsson M, Laviano A, Mühlebach S, Muscaritoli M, Oldervoll L, Ravasco P, Solheim T, Strasser F, de van der Schueren M, Preiser JC. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017; 36(1):11-48. [CrossRef]
- Arends J, Baracos V, Bertz H, Bozzetti F, Calder PC, Deutz NEP, Erickson N, Laviano A, Lisanti MP, Lobo DN, McMillan DC, Muscaritoli M, Ockenga J, Pirlich M, Strasser F, de van der Schueren M, Van Gossum A, Vaupel P, Weimann A. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017; 36(5):1187-1196. [CrossRef]
- Caccialanza R, Cotogni P, Cereda E, Bossi P, Aprile G, Delrio P, Gnagnarella P, Mascheroni A, Monge T, Corradi E, Grieco M, Riso S, De Lorenzo F, Traclò F, Iannelli E, Beretta GD, Zanetti M, Cinieri S, Zagonel V, Pedrazzoli P. Nutritional Support in Cancer patients: update of the Italian Intersociety Working Group practical recommendations. J Cancer 2022;13(9):2705-2716. [CrossRef]
- Langius JA, Zandbergen MC, Eerenstein SE, van Tulder MW, Leemans CR, Kramer MH, Weijs PJ. Effect of nutritional interventions on nutritional status, quality of life and mortality in patients with head and neck cancer receiving (chemo)radiotherapy: a systematic review. Clin Nutr. 2013; 32:671-8. [CrossRef]
- Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, Hütterer E, Isenring E, Kaasa S, Krznaric Z, Laird B, Larsson M, Laviano A, Mühlebach S, Oldervoll L, Ravasco P, Solheim TS, Strasser F, de van der Schueren M, Preiser JC, Bischoff SC. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr. 2021; 40(5):2898-2913. [CrossRef]
- Hegazi R, Miller A, Sauer A. Evolution of the diagnosis of malnutrition in adults: a primer for clinicians. Front Nutr. 2024; 6;11:1169538. [CrossRef]
- Di Sebastiano, K.M., Mourtzakis M. A critical evaluation of body composition modalities used to assess adipose and skeletal muscle tissue in cancer. Appl Physiol Nutr Metab 2012; 37:811–821. [CrossRef]
- de Bree R, Meerkerk CDA, Halmos GB, Mäkitie AA, Homma A, Rodrigo JP, López F, Takes RP, Vermorken JB, Ferlito A. Measurement of sarcopenia in head and neck cancer patients and its association with frailty. Front Oncol. 2022; 12;12:884988. [CrossRef]
- Kuriyan, R. Body composition techniques. Indian J Med Res. 2018; 148(5):648-658. [CrossRef]
- Brierley JD, Gospodarowicz MK, Wittekind C, editors. The TNM classification of malignant tumors. 8. Wiley 2017.
- Guigoz Y, Vellas B, Garry PJ. Mini Nutritional Assessment: a practical assessment tool for grading the nutritional state of elderly patients. Facts Res Gerontol 1994: 12–13.
- Buscemi S, Blunda G, Maneri R et al. Bioelectrical characteristics of type 1 and type 2 diabetic subjects with reference to body water compartments. Acta Diabetol. 1998; 35: 220–223. [CrossRef]
- Fedorov A, Beichel R, Kalpathy-Cramer J, Finet J, Fillion-Robin J-C, Pujol S, Bauer C, Jennings D, Fennessy F.M, Sonka M, Buatti J, Aylward S.R, Miller J.V, Pieper S, Kikinis R.3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn Reson Imaging 2012; 30:1323-41. [CrossRef]
- Reddon JR, Stefanyk WO, Gill DM, Renney C. Hand dynamometer: effects of trials and sessions. Percept Mot Skills. 1985; 61:1195-8.
- Talwar B, Donnelly R, Skelly R, Donaldson M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. 2016; 130(S2):S32-S40. [CrossRef]
- Wendrich AW, Swartz JE, Bril SI, Wegner I, de Graeff A, Smid EJ, de Bree R, Pothen AJ. Low skeletal muscle mass is a predictive factor for chemotherapy dose-limiting toxicity in patients with locally advanced head and neck cancer. Oral Oncol. 2017; 71:26-33. [CrossRef]
- Buscemi S, Blunda G, Maneri R, Verga S. Bioelectrical characteristics of type 1 and type 2 diabetic subjects with reference to body water compartments. Acta Diabetol. 1998; 35:220. [CrossRef]
- Prado CM, Lieffers JR, McCargar LJ, Reiman T, Sawyer MB, Martin L, Baracos VE. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 2008; 9:629-35.
- Fernández-Jiménez R, García-Rey S, Roque-Cuéllar MC, Fernández-Soto ML, García-Olivares M, Novo-Rodríguez M, González-Pacheco M, Prior-Sánchez I, Carmona-Llanos A, Muñoz-Jiménez C, Zarco-Rodríguez FP, Miguel-Luengo L, Boughanem H, García-Luna PP, García-Almeida JM. Ultrasound Muscle Evaluation for Predicting the Prognosis of Patients with Head and Neck Cancer: A Large-Scale and Multicenter Prospective Study. Nutrients. 2024; 16:387. [CrossRef]
- Swartz JE, Pothen AJ, Wegner I, Smid EJ, Swart KM, de Bree R, Leenen LP, Grolman W. Feasibility of using head and neck CT imaging to assess skeletal muscle mass in head and neck cancer patients. Oral Oncol. 2016; 62:28-33. [CrossRef]
- Bril SI, van Beers MA, Chargi N, Carrillo Minulina N, Smid EJ, Dankbaar JW, de Bree R. Skeletal muscle mass at C3 is a strong predictor for skeletal muscle mass at L3 in sarcopenic and non-sarcopenic patients with head and neck cancer. Oral Oncol. 2021; 122:105558. [CrossRef]
- Zwart AT, Becker JN, Lamers MJ, Dierckx RAJO, de Bock GH, Halmos GB, van der Hoorn A. Skeletal muscle mass and sarcopenia can be determined with 1.5-T and 3-T neck MRI scans, in the event that no neck CT scan is performed. Eur Radiol. 2021; 31:4053-4062.
- Belavý DL, Miokovic T, Armbrecht G, Felsenberg D. Hypertrophy in the cervical muscles and thoracic discs in bed rest? J Appl Physiol 2013; 115:586-96.
- Comelli A, Bignardi S, Stefano A, Russo G, Sabini MG, Ippolito M, Yezzi A. Development of a new fully three-dimensional methodology for tumours delineation in functional images. Comput. Biol. Med. 2020; 120:103701. [CrossRef]
- Buscemi S, Batsis JA, Parrinello G, Massenti FM, Rosafio G, Sciascia V, Costa F, Pollina Addario S, Mendola S, Barile AM, Maniaci V, Rini N, Caimi G. Nutritional predictors of mortality after discharge in elderly patients on a medical ward. Eur. J. Clin Invest. 2016; 46:609-18. [CrossRef]
- Van Dijk BA, Gatta G, Capocaccia R, Pierannunzio D, Strojan P, Licitra L; RARECARE Working Group. Rare cancers of the head and neck area in Europe. Eur. J. Cancer. 2012; 48:783-96. [CrossRef]
Figure 1.
Flowchart of participant selection (ON: oral nutrition; AN: artificial nutrition; and stage: TNM stage).
Figure 1.
Flowchart of participant selection (ON: oral nutrition; AN: artificial nutrition; and stage: TNM stage).
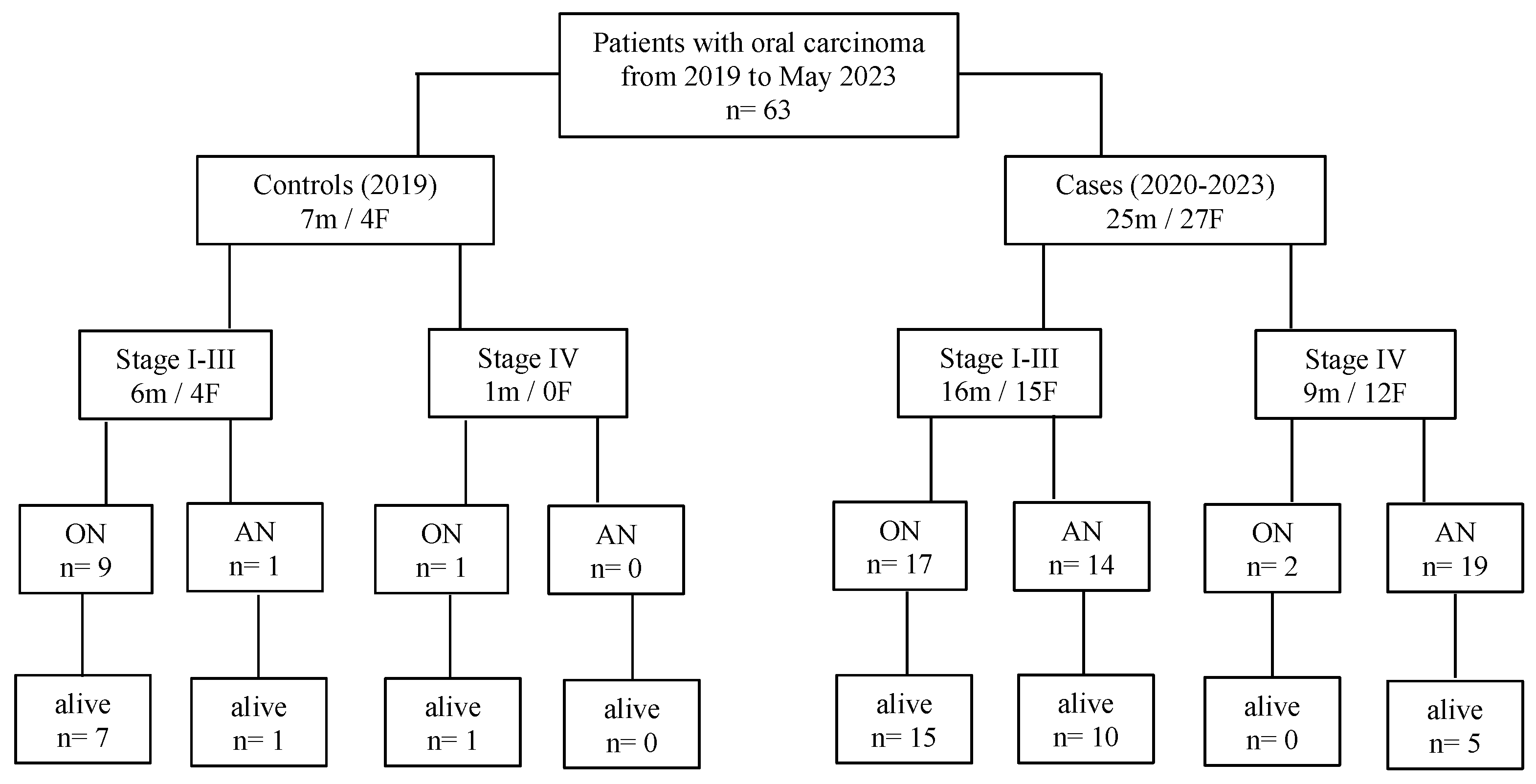
Figure 2.
Kaplan–Meier survival probability curves according to the TNM stage of the disease in 63 patients after surgery for squamous cell carcinomas of the oral cavity.
Figure 2.
Kaplan–Meier survival probability curves according to the TNM stage of the disease in 63 patients after surgery for squamous cell carcinomas of the oral cavity.
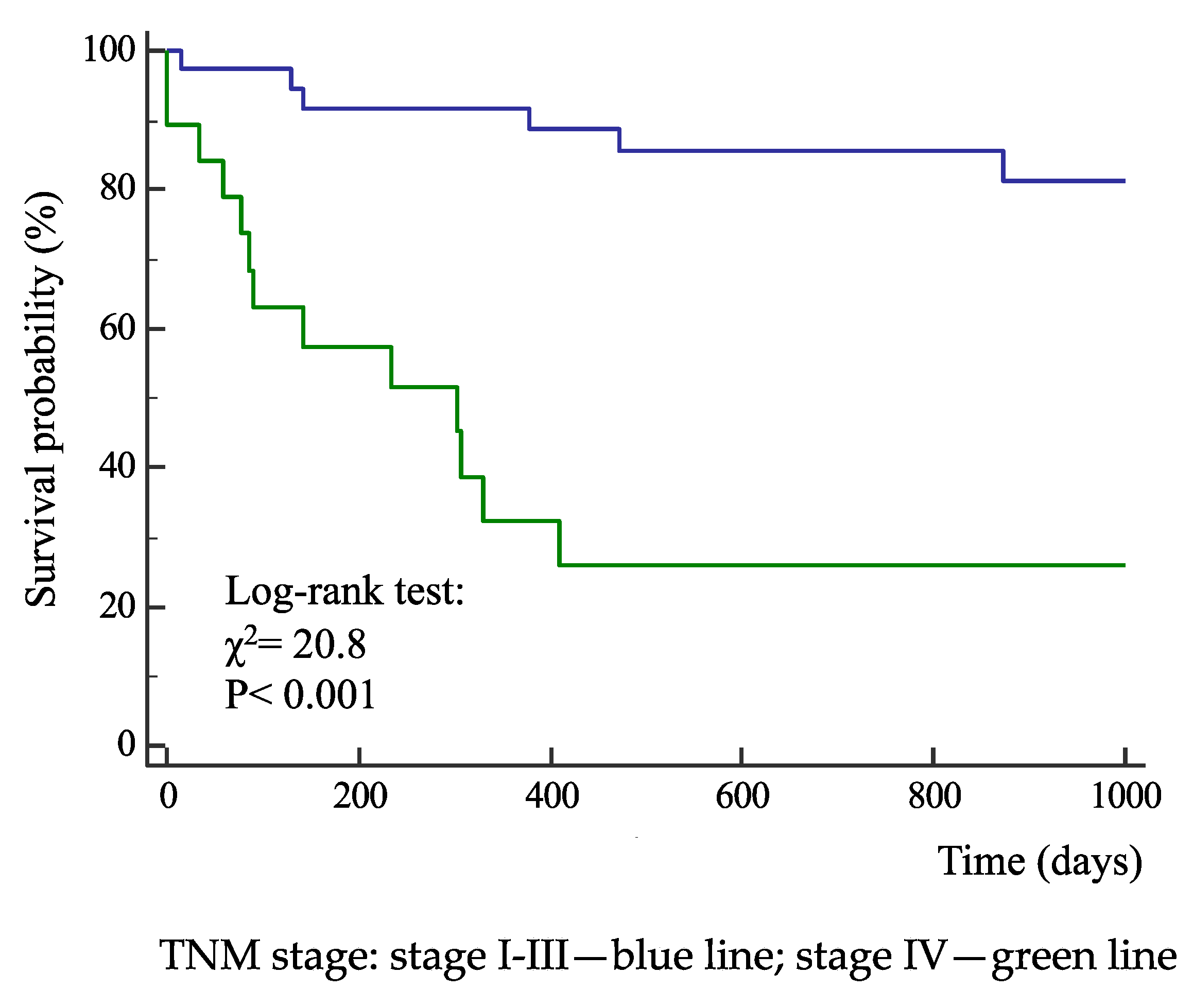
Figure 3.
Kaplan–Meier survival probability curves according to nutrition type (ON: oral nutrition; AN: artificial nutrition) in 63 patients after surgery for squamous cell carcinomas of the oral cavity.
Figure 3.
Kaplan–Meier survival probability curves according to nutrition type (ON: oral nutrition; AN: artificial nutrition) in 63 patients after surgery for squamous cell carcinomas of the oral cavity.
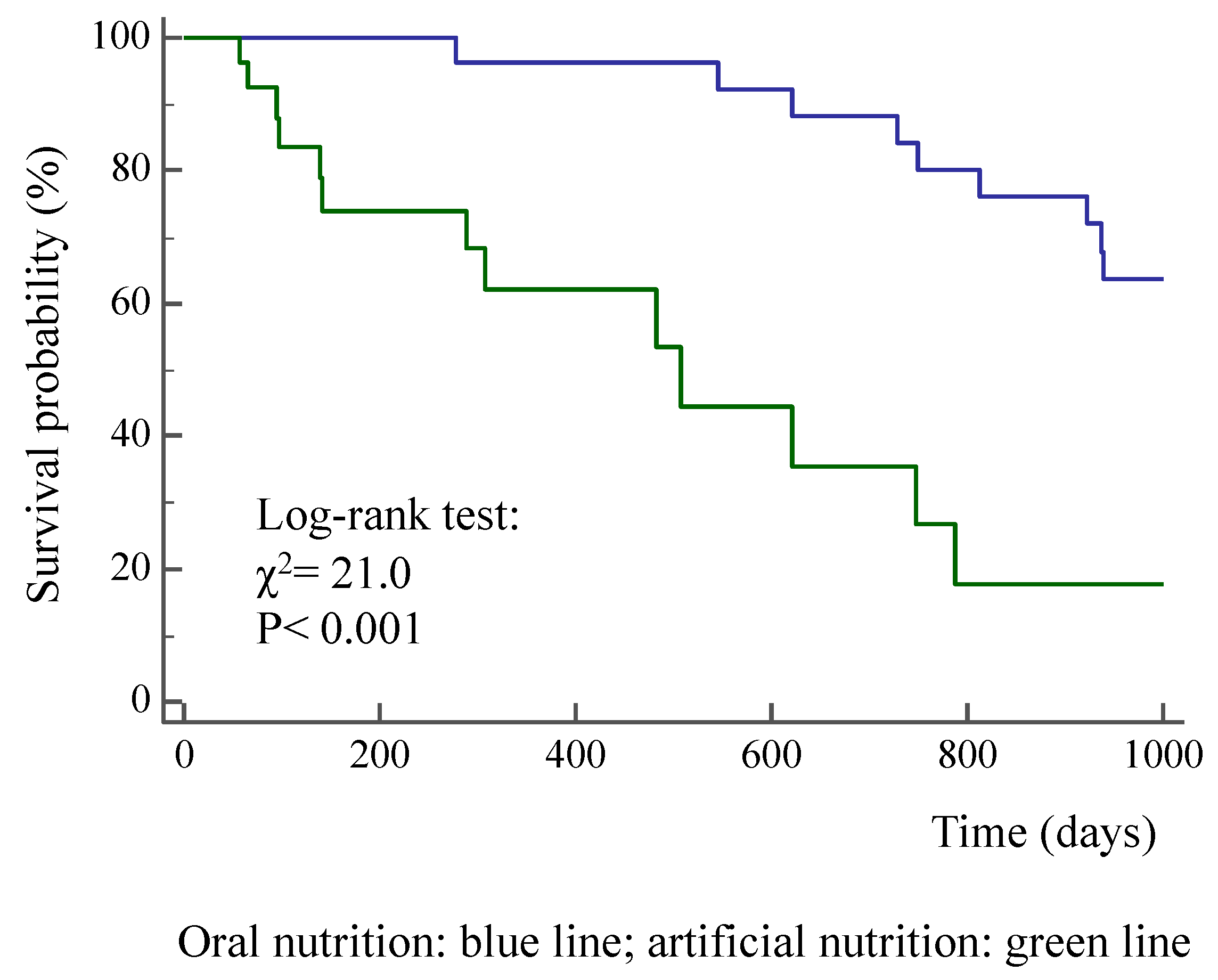
Figure 4.
Kaplan–Meier survival probability curves of the participants classified according to TNM stage and nutrition type (ON: oral nutrition; AN: artificial nutrition) in 63 patients after surgery for squamous cell carcinomas of the oral cavity.
Figure 4.
Kaplan–Meier survival probability curves of the participants classified according to TNM stage and nutrition type (ON: oral nutrition; AN: artificial nutrition) in 63 patients after surgery for squamous cell carcinomas of the oral cavity.
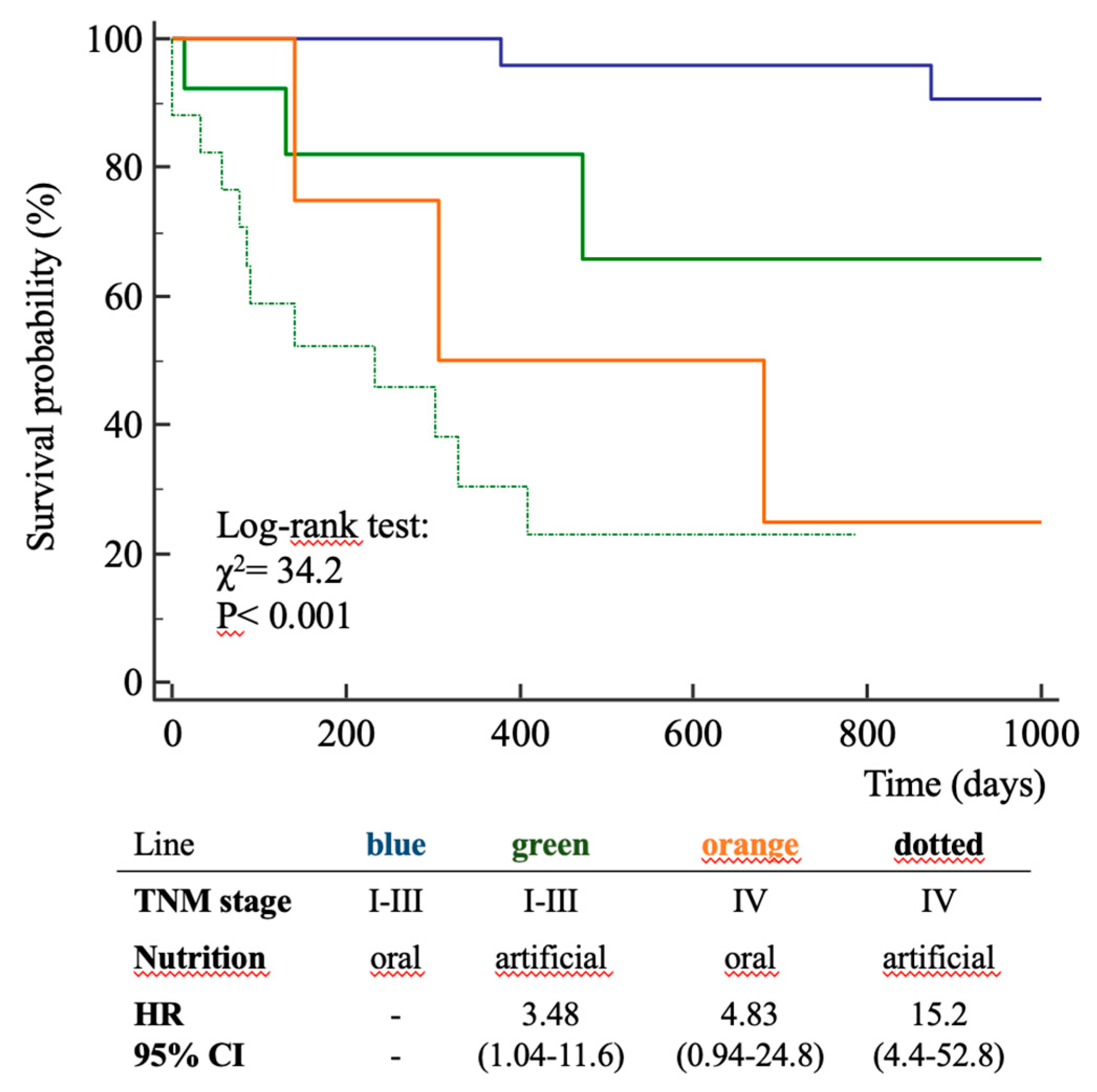
Figure 5.
An example case of a 65-year-old male patient undergoing head–neck MRI before (A) and 8 months after (B) surgical intervention for right hemiglossectomy due to OSCC of the tongue. Volumetric reconstructions and measurement of the volume of the posterior neck muscles at C3 level, in 5 slices, before (C) and after (D) intervention demonstrating a volumetric reduction (23.5982 cm3 vs. 22.7835 cm3). Linear regression analysis of cases with volumetric reconstruction of paravertebral muscle volume and bioelectrical resistance (E), fat-free mass (F), and change in paravertebral muscle volume and fat-free mass (G).
Figure 5.
An example case of a 65-year-old male patient undergoing head–neck MRI before (A) and 8 months after (B) surgical intervention for right hemiglossectomy due to OSCC of the tongue. Volumetric reconstructions and measurement of the volume of the posterior neck muscles at C3 level, in 5 slices, before (C) and after (D) intervention demonstrating a volumetric reduction (23.5982 cm3 vs. 22.7835 cm3). Linear regression analysis of cases with volumetric reconstruction of paravertebral muscle volume and bioelectrical resistance (E), fat-free mass (F), and change in paravertebral muscle volume and fat-free mass (G).
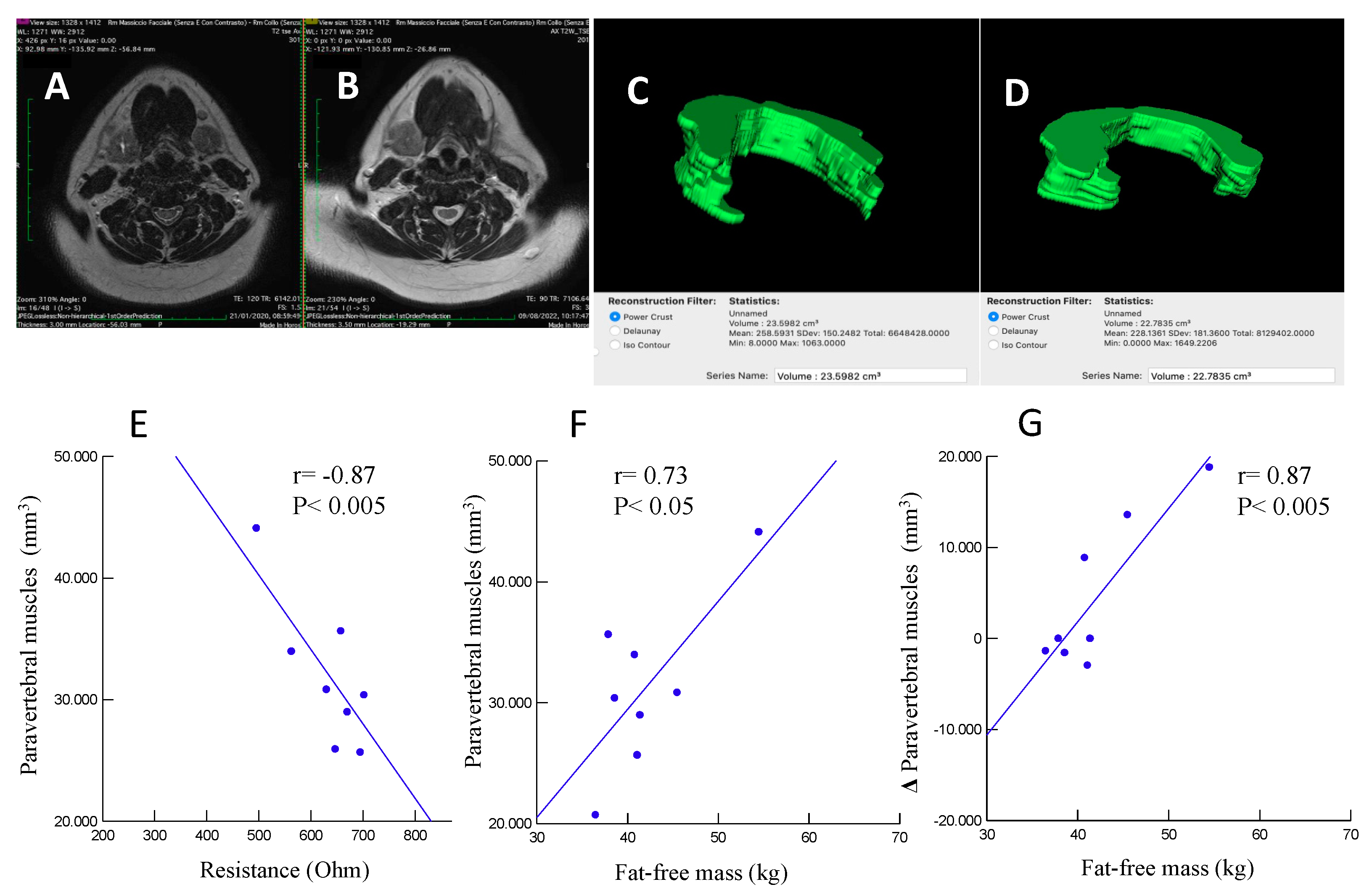

Table 1.
Physical, clinical, and nutritional characteristics of the cohort of patients with oral squamous cell carcinoma according to TNM stage.
Table 1.
Physical, clinical, and nutritional characteristics of the cohort of patients with oral squamous cell carcinoma according to TNM stage.
| Oral Cancer Stage | |||
|---|---|---|---|
| I-III n= 41 |
IV n= 22 |
Pa | |
| Males (%) | 53.7 | 45.5 | 0.54 |
| Age (years) | 65 ± 17 | 64 ± 11 | 0.85 |
| Actual survival from surgery (days) | 764 ± 465 | 317 ± 360 | < 0.001 |
| All-cause death (%) | 19.5 | 72.7 | < 0.001 |
| Nutrition (%): | |||
| oral | 63.4 | 13.6 | |
| artificial | 36.6 | 86.4 | < 0.001 |
| Body weight (kg) | 68.0 ± 17.5 | 60.3 ± 13.2 | 0.07 |
| Body mass index (kg/m2) | 25.3 ± 5.4 | 22.2 ± 5.8 | 0.06 |
| Bioimpedance analysis: | n=11 | n= 12 | |
| resistance (Ohm) | 641 ± 114 | 544 ± 142 | 0.08 |
| reactance (Ohm) | 65 ± 21 | 44 ± 16 | < 0.01 |
| phase angle (°) | 5.7 ± 1.1 | 4.5 ± 0.9 | < 0.01 |
| fat mass (%) | 26.6 ± 10.3 | 17.5 ± 10.2 | 0.06 |
| fat-free mass (kg) | 44.2 ± 8.7 | 45.6 ± 8.4 | 0.70 |
| fat-free mass index (kg/m2) | 16.8 ± 2.3 | 16.8 ± 3.2 | 0.98 |
| Hand-grip test (kg): | n=12 | n= 14 | |
| right | 21.3 ± 9.7 | 23.3 ± 11.4 | 0.64 |
| left | 20.2 ± 10.2 | 21.1 ± 10.1 | 0.82 |
| Mini Nutritional Assessment: | |||
| risk of malnutrition | 47.1 | 38.9 | |
| malnutrition | 52.9 | 61.1 | 0.54 |
| Serum concentration of: | |||
| proteins (g/dl) | 6.1 ± 1.0 | 5.4 ± 0.8 | < 0.005 |
| albumin (g/dl) | 3.8 ± 0.6 | 3.3 ± 0.7 | < 0.01 |
| hemoglobin (g/dl) | 11.0 ± 2.3 | 10.2 ± 2.2 | 0.25 |
| creatinine (mg/dl) | 0.74 ± 0.24 | 0.69 ± 0.42 | 0.61 |
| Mean ± SD; aunpaired Student’s t-test or χ2 when appropriate. | |||
Table 2.
Physical, clinical, and nutritional characteristics of the cohort of patients with oral squamous cell carcinoma according to modality of nutrition.
Table 2.
Physical, clinical, and nutritional characteristics of the cohort of patients with oral squamous cell carcinoma according to modality of nutrition.
| Nutrition | |||
|---|---|---|---|
| Oral n= 29 |
Artificial n= 34 |
Pa | |
| Males (%) | 65.5 | 38.2 | < 0.05 |
| Age (years) | ± | ± | |
| Actual survival from surgery (days) | 994 ± 353 | 289 ± 299 | < 0.001 |
| All-cause death (%) | 20.7 | 52.9 | < 0.01 |
| TNM stage I-III (%) | 89.7 | 44.4 | < 0.001 |
| Body mass index (kg/m2) | 26.4 ± 5.7 | 22.5 ± 5.1 | < 0.01 |
| Bioimpedance analysis: | n= 6 | n= 17 | |
| phase angle (°) | 5.9 ± 0.9 | 4.8 ± 1.1 | < 0.05 |
| fat-free mass index (kg/m2) | 17.4 ± 2.5 | 16.6 ± 2.8 | 0.53 |
| MRI_C3 (mm3): | n= | n= | |
| before surgery | 35586 ± 5063 | 28728 ± 6151 | < 0.05 |
| after (3-12 months) surgery | 44822 ± 10685 | 26088 ± 5123 | < 0.001 |
| Δ MRI_C3 | 9236 ± 7313 | -2640 ± 4184 | < 0.001 |
| Serum creatinine (mg/dl) | 0.79 ± 0.23 | 0.67 ± 0.35 | 0.14 |
| Mean ± SD; aunpaired Student’s t-test or χ2 when appropriate. MRI_C3, volumetric magnetic resonance imaging of posterior paravertebral muscles at the C3 level. | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



