Submitted:
08 May 2024
Posted:
08 May 2024
You are already at the latest version
Abstract
Recovery between physical efforts is essential for optimal performance in sports. Dietary supplements like cannabidiol (CBD) have been proposed to facilitate recovery and performance optimization. This systematic review aimed to: a) systematize the scientific evidence on CBD for recovery, b) associate CBD's biomedical properties with those required for optimal fatigue recovery, and c) recommend a future research agenda. Searches across databases identified 70 relevant studies from 1990-2022, including 38.6% preclinical, 31.4% clinical trials, and 30.0% reviews/meta-analyses across various populations like mice, rats, epileptics, and athletes. CBD demonstrated potentially beneficial properties for athlete recovery such as anti-inflammatory, neuroprotective, anxiolytic, and analgesic effects with doses ranging from 5-600mg administered orally, intravenously, and via other routes. However, rigorous confirmatory research specifically in athlete populations is lacking. While CBD appears promising for facilitating recovery and performance optimization, further randomized placebo-controlled trials are needed to test the acute and chronic effects of different CBD dosing regimens in athletes. Future research should focus on elucidating CBD's physiological mechanisms of action as they relate to post-exercise recovery, as well as its comparative effectiveness versus conventional medications and therapies. Advancing our understanding of CBD's role in athlete recovery could provide new therapeutic strategies to optimize recovery and performance.
Keywords:
recovery
; cannabidiol
; anti-inflammatory
; dietary supplements
; sport
1. Introduction
Nowadays, recovery between physical efforts is essential to achieve optimal performance in sports. The increase in the number, frequency, and intensity of competitions has resulted in relatively little time between efforts[1], which increases the relevance of planning and implementing effective and accessible recovery strategies.[2] Physical exertion causes a series of structural and functional alterations that must be controlled, monitored, and counteracted to achieve a rapid return to homeostasis.[3] In this sense, depending on the exercise dose, myositis occurs by releasing cytokines (e.g., IL-1, IL-6, TNFα) that trigger inflammatory responses[4] and lead to an effective but relatively slow recovery process. Sports practice can also cause drowsiness, swelling, pain, and weakness for hours or even days.[5] So, these aspects can be largely mitigated with the use of certain recovery measures.
Thanks to scientific and technological advances, the level of performance among elite athletes is very similar, which suggests the need to seek new alternatives to improve performance.[6] For recovery effects to achieve optimal performance different ergogenic supplements have been used as dietary supplements[7], antioxidants[8], and more recently, organic foods such as ginseng and beetroot.[9] One of these proposed new aids is cannabidiol (CBD), a phytocannabinoid grouped among the cannabinoids found in the cannabis sativa plant and also obtained from hemp.[10]
CBD can be administered in the form of oral solutions, oral capsules, buccal aerosol, and drops, among other presentations, and the dose can vary depending on the desired effect.[11] Unlike Δ9-tetrahydrocannabinol (THC) is one of the compounds in the cannabis sativa plant, CBD lacks psychotomimetic and psychotropic effects, and there is no evidence of dependence or abuse, and it has a fairly favorable safety and tolerability profile.[12] Although somnolence, diarrhea, and an variances on body temperature are among the reported side effects, these are mild and infrequent.[13] The common concentration of CBD in hemp oils is 12-18% (often higher due to enrichment procedures) [14]; CBD has been administered for medical purposes at doses of 1-50 mg/kg/d[15], 200-300 mg/d for six months[16] y 1200-1500 mg/d for four weeks[17] without significant adverse effects.
In all international sports leagues and organizations, tetrahydrocannabinol (THC) and its metabolites, such as 11-COOH-THC, are prohibited both in and out of competition, with an acceptable threshold of 11-COOH-THC in urine ranging from >15 to 150 ng/ml.[18] However, isolated cannabidiol (CBD) is not included in the World Anti-Doping Agency's (WADA) Prohibited List, and it was recently removed from the list.[18] This reflects a growing social acceptance of CBD and cannabis use for recreational and medicinal purposes, although not all of its biological effects are fully understood.[19] Nevertheless, it is important to note that CBD products may contain traces of THC, so athletes should be cautious when consuming these products to avoid potential anti-doping rule violations.[20] In this regard, a recent systematic review on cannabis use in sports suggested that 25% of athletes reported having consumed cannabis in the last 12 months.[18]
Preclinical and clinical evidence suggests that CBD could provide a positive effect on the treatment of chronic pain, spasticity, and sleep quality[21], and has a potential role in managing mood disorders.[22] CBD intake has presented multiple benefits at the immune level, including anti-inflammatory and immunosuppressive effects[19], both crucial for the recovery of sports injuries and the effects of fatigue caused by the daily physical load that athletes are exposed to.[23,24] The supposed effects of CBD include, among others, analgesic, antioxidant, anxiolytic, anti-inflammatory, cytotoxic, and anticonvulsant, which are mediated by signaling mechanisms that include cannabinoid receptors, protein-coupled receptors, and serotonin receptors.[25]
The mechanism of action of CBD in the body could be explained by the endocannabinoid system, among other body systems that participate in it. This endocannabinoid system participates globally in maintaining homeostasis in the human body and is involved in a variety of regulatory functions such as chronic inflammation and regulation of the immune system.[14] The body has its own endogenous cannabinoids and there are strong hypotheses that endocannabinoids could mediate some central and peripheral effects of exercise.[26] Previous research indicated that endocannabinoids could have an influence on skeletal muscle, adipose tissue, liver, immune system and redox state[27], increasing anti-inflammatory and immunosuppressive responses[27], reducing pain[28] and improving sleep and anxiety scores when consuming CBD.[29]
The evidence regarding the use of cannabinoids and CBD in sports is relatively scarce due to a gap in research that lasted for decades that led to a lack of research, reducing the potential benefits of CBD.[30] With the recent legal opening for the medicinal prescription of cannabinoids, as well as an allocation for recreational use with greater popular acceptance, studies have begun to emerge. Although the publication rate on CBD worldwide is relatively low due to some administrative processes regarding the local pharmaceutical institution[31], scientists' interest has increased significantly, implying the need to direct efforts based on the evidence gathered to date.
In sports, recently published narrative reviews on the effect of cannabidiol and its relationship with performance[32] and recovery[33] suggest that CBD possesses anti-inflammatory, neuroprotective, and analgesic effects, and also promotes the healing of traumatic skeletal injuries. Additionally, early-stage clinical studies suggest that CBD may have anxiolytic effects, and some evidence points to an improvement in sleep.[32,33] Based on this evidence, and understanding the need to orient future research on CBD and sports recovery, this systematic review aims to: a) systematize the first and second-level scientific evidence related to the study of CBD, b) associate the biomedical properties attributed to CBD with those required for optimal fatigue recovery, and c) recommend a future research agenda related to the role of CBD in recovery.
2. Materials and Methods
2.1. Study Design
This study followed an integrative systematic review methodology to synthesize and critically analyze the diverse literature related to the use of cannabidiol (CBD) in sports recovery following the Preferred Reporting Guidelines for Systematic Reviews and Meta-Analysis (PRISMA).[34] Integrative systematic reviews facilitate the combination and synthesis of different types of evidence, including empirical studies, theoretical literature, and methodological contributions.[35] The key feature of this approach is the possibility of incorporating a wide range of relevant data to build a comprehensive understanding of the research topic.[36]
This integrative systematic methodology was consider appropriate given the emergent and multidisciplinary nature of the research topic, which spans domains such as sports science, exercise physiology, pharmacology, and medicine.[37] The comprehensive and rigorous synthesis of diverse evidence, including both empirical and non-empirical sources, aligns with the overarching purpose of providing a holistic understanding of CBD's efficacy and mechanisms in the context of sports recovery. The protocol for this integrative systematic review was registered in PROSPERO (ID: 479815) to ensure transparency and minimize potential bias.
2.2. Eligibility Criteria
To identify relevant studies in the use of cannabidiol (CBD) for sports recovery, this systematic review used a structured set of eligibility criteria following the PICOS (Population, Intervention, Comparator, Outcomes, Study design) framework.[34] Additionally, studies were excluded following this criteria: (1) if the article was not written in English; (2) if the full-text was not available, (3) if the type of document was doctoral thesis, books or book chapters, conference papers, patents or low-quality articles with a severe lack of information (number and characteristics of participants, design, methodology, CBD dose, etc.). The eligibility criteria were shown in Table 1.
2.3. Search Strategy and Article Management Process
The search strategy for this integrative systematic review was designed to capture a comprehensive body of literature related to the use of cannabidiol (CBD) in sports recovery. An initial exploratory search was conducted to identify relevant keywords, controlled vocabulary terms, and subject headings across different disciplines related to the topics of CBD, sports, exercise, recovery, fatigue, and performance. The search terms were selected or adapted based on the Medical Subject Headings (MeSH) descriptor data from the National Library of Medicine. Once this initial identification of relevant descriptors was made, the words chosen for the formal search were: "(cannabidiol OR CBD) AND (sports OR exercise OR physical activity) AND (recovery of function OR fatigue OR sports performance OR injury OR inflammation OR muscle fatigue)."
Then, the formal search was then performed on November 30th, 2023 by two independent reviewers in three electronic databases: PubMed (MEDLINE), Scopus (EMBASE) and Web of Science (Web of Science Core Collection, MEDLINE, Current Contents Connect, Derwent Innovations Index, KCI-Korean Journal Database, Russian Science Citation Index and Scielo Citation Index). Additionally, the reference lists of included studies were manually screened to identify any potentially relevant publications that may have been missed in the initial search, All references were extracted and imported into an open-source research tool (5.0.64, Zotero, CA, United States) to subsequently systematize the studies (Excel, Microsoft, CA, United States). All duplicates found among the databases were identified and eliminated.
2.4. Study Selection
The selection of studies for inclusion was guided by the predetermined eligibility criteria outlined previously, considering empirical data, theoretical perspectives, or literature reviews related to the use of CBD in the context of sports, exercise, recovery, fatigue, or performance. Firstly, the title and abstract screening was conducted independently by two reviewers. Any disagreements that arose during this initial screening phase were resolved through discussion between the two reviewers.
The articles that passed the title and abstract screening then underwent a full-text assessment for final eligibility. During this stage, the full manuscripts were reviewed to ensure the studies met all of the inclusion criteria. Only those studies that were deemed eligible based on the full-text review were selected for data extraction and synthesis. The PRISMA flow of the integrative review can be analyzed in Figure 1.
2.5. Study Quality Assessment
For assessing the preclinical animal studies, the ARRIVE guidelines have been used.[39] The selected studies obtained moderate to high methodological quality. Most of them clearly report the study objectives, animal characteristics, experimental procedures, and statistical analyses. However, some studies not include important aspects such as randomization, blinding, and sample size calculations, which are important to ensure internal validity and minimize bias. Additionally, most of them recommended replicating and extending their findings in the future, suggesting more robust preclinical evidence.
The clinical studies involving human participants were assessed using the Cochrane Risk of Bias 2 (RoB 2) tool.[40] The risk of bias across the studies was generally low to moderate. Most studies demonstrated appropriate randomization, blinding, and handling of missing data. Instead, some studies had concerns that could introduce potential sources of bias like the selection of the reported results and the overall study design. It is necessary to conduct larger, well-designed, and adequately powered clinical trials to further establish the efficacy and safety of cannabidiol (CBD) in various medical conditions.
The studies under review and meta-analysis were assessed using the AMSTAR checklist.[41] The methodological quality of these studies was found to be moderate to high. The authors of the reviews provided a comprehensive search strategy, clearly defined the inclusion criteria and conducted a thorough quality assessment of the included studies. However, certain reviews did not mention details on the rationale for excluded studies, the evaluation of publication bias, and the exploration of potential sources of heterogeneity. These areas should be improved in future review-level evidence to enhance the reliability and robustness of the conclusions.
In summary, the analysis of the study methods across the preclinical, clinical, and review-level evidence indicates that the overall quality is acceptable, with some opportunities for development. Improving the methodological rigor, specifically in areas such as randomization, blinding, and sample size calculations, will help enhance the validity and reproducibility of the findings. In addition, more well-designed, large-scale clinical trials and comprehensive systematic reviews are needed to elucidate the therapeutic potential of cannabidiol (CBD) and its fundamental mechanisms of action.
2.6. Data Extraction
The data extraction process involved compiling key information from the included studies into a standardized spreadsheet. Two independent reviewers extracted the following data elements:
- a)
- Authors and year of publication: The full citation details, including the year the study was published.
- b)
- Main aim: The primary objective or research question addressed by the study.
- c)
-
Methodology:
- c.1)
- Subjects: The participant characteristics, such as species (human, animal), population (athletes, healthy individuals), age, sex, etc.
- c.2)
- Study design: The type of study design (e.g. randomized controlled trial, observational, systematic review).
- c.3)
- CBD supplement: Details on the CBD intervention, including the formulation (oral, topical, etc.), dosage, and administration protocol (frequency, timing).
- d)
- Main results (CBD effects): The key findings and conclusions related to the effects of CBD, such as impact on recovery, performance, inflammation, pain, sleep, etc.
- e)
- Recommendations for future research: Any suggestions or directions for further study proposed by the authors.
The reviewers worked independently to extract this information, with any discrepancies resolved through discussion and consensus. This systematic data collection process ensured comprehensive and accurate extraction of the relevant study details.
3. Results
3.1. Search, Selection and Inclusion of Publications
1761 articles were identified from the Web of Science (n = 630), PubMed (n = 728) and Science Direct (n = 403) database search. In the screening phase, 1322 articles were deleted due to the year of publication, the title of the article or abstract. From the remaining 439 papers in the eligibility phase, they were exported to a reference manager (Zotero), and any duplicates (76 articles) were eliminated automatically. Finally, 363 articles arrived at the last phase, where 288 did not fulfill the inclusion criteria and 5 had methodological doubts, so 293 articles were removed. At the end of the screening procedure, 70 articles remained for the systematic review related to the study topic that were included in Table 2, indicating authors and year of publication, main aim, methodology (subjects, study design and CBD supplement, including periodization and dose characteristics), main results (CBD effects) and recommendations for future research.
3.2. Type of Study, Subjects and Clinical Evidence of CBD
Regarding the type of study, preclinical studies represent 38.57% (n=27), clinical studies represent 31.43% (n=22), and reviews and meta-analyses represent 30.00% (n=21). Various populations were evaluated during the studies, such as mice (26%), rats (37%), epileptics (16%), men (8%), women (9%), girls (2%), and rugby players (2%). Respect to clinical evidence, 22% of selected studies reporting its beneficial effect during the pathology treatment, 17% on anxiety, 17% on anti-inflammatory characteristics, 11% exploring its effects on sleep, and 6% on muscle recovery in athletes.
3.3. Effects of CBD, doses and Administration Methods
The effects of CBD are varied, among which 39% refer to studies with anti-inflammatory effects, 22% on disorders (fibrosis, asthma, chronic pain), another 22% are studies on muscular recovery and as a therapeutic agent and 17% on studies about the benefits as a neuroprotector. The doses used were 5-10mg (21%), 20-30mg (43%), 300-600mg (36%), other doses used in a smaller percentage were 60mg, 0.005-5mg, 50mg, 150mg, and 120mg. Additionally, CBD was administered mixed in a medium such as oil in 6%, orally in 33%, intravenously in 40%, aerosol, intracerebroventricular, subcutaneous, and intraperitoneal in 7%, and with a plug in a single dose (n=1, 0.01%).

Table 2.
Summary of first and second-level scientific evidence related to the biomedical properties of cannabidiol.
Table 2.
Summary of first and second-level scientific evidence related to the biomedical properties of cannabidiol.
| # | Authors | Aim | Methodology | Main results (CBD effects) |
Recommendations for future research |
|---|---|---|---|---|---|
| Preclinic research (animals) (n= 27) | |||||
| 1 | Zieba et al. (2019) [42] | Effect of CBD on anxiety-related behavior | n = 72 mice with acute administration of CBD at 5-20 mg/kg versus control | Better adaptation to the new anxiolytic environment | Clarify the relationship between CBD and pre-pulse inhibition. |
| 2 | Schleicher et al. (2019) [43] |
Effect of CBD on behavioral profile, motor performance, anxiety, and memory | Acute administration of CBD in mice at 20 mg/kg for six months versus control | Non-negative effects | Optimal treatment strategies. |
| 3 | Myers et al. (2019) [44] | Effects of CBD on cognition | n = 335 mice Acute CBD intake at 3-10 mg/kg, chronic at 5-20 mg/kg |
Anxiolytic | More suitable animal models. |
| 4 | Iannotti et al. (2019) [45] | Effect of cannabinoids (CBD) on inflammation, functional autophagy, and improvement of muscle function | Mice, muscular dystrophies Chronic intake of CBD at 60 mg/kg, three times per week for two weeks |
Improved structural and functional muscle enhancement and recovery | Replication and extension of findings. |
| 5 | Santiago et al. (2019) [46] | Effects of CBD on neuroplasticity, inflammation, and cognitive function | Diabetic rats Chronic CBD at 10 mg/kg, once a day for 30 days. |
Reduction of blood glucose levels, cognitive enhancer, reduction of neurodegeneration and inflammation, and attenuation of decreased levels of BDNF (neuroprotective) | Effects of low-high dose ratio of THC and CBD administration. |
| 6 | Casey et al. (2017) [47] | Effects of cannabinoids on neuropathic pain | Mice, chronic constriction injury 0.01-0.015 mg/g |
Potential in the treatment of neuropathic pain Anti-allodynic properties |
Confirm results. |
| 7 | Hayakawa et al. (2007) [48] | Effects of CBD as a neuroprotective agent. | Mouse, cerebral ischemia Dissolved at 1% |
Neuroprotection through an anti-inflammatory mechanism of the CB1 receptor | Confirm chronic effects of CBD administration on cerebral ischemia. |
| 8 | Mori et al. (2017) [49] | Effects of CBD on functional recovery after cerebral ischemic injury | Mice, bilateral common carotid artery occlusion Short-term 10 mg/kg CBD before and after the event |
Prevention of anxiety-like behavior, memory impairments, and despair-like behavior | Clarify the relationship between CBD and pre-pulse inhibition. |
| 9 | Murillo-Rodríguez et al. (2018) [50] | Effects of CBD on neurochemicals related to wakefulness | Rats, microdialysis surgeries Intravenous dose of 5-30 mg/kg |
Increases acetylcholine levels in a brain region related to wakefulness control. | Clarification of how CBD induces improvement in neurobiological processes involving acetylcholine. |
| 10 | García-Baños et al. (2021) [51] |
Effects of CBD demonstrating that Phytocannabinoid could attenuate alcohol-induced cognitive deficits | n = 6 rats. CBD (20 mg/kg ip). 10 ml alcohol or water | Counteract neuroinflammatory-induced cognitive impairments with PLAE treatment with CBD. | Further studies evaluating dose-dependent positive or adverse effects of CBD. |
| 11 | Mukhopadhyay et al. (2011) [52] | Effects of cannabidiol (CBD) on myocardial dysfunction, inflammation, oxidative/nutrient stress, cell death, and interrelated signaling pathways | Mice. Dose of 50 mg/kg dissolved in 100 ml citrate buffer pH 4.5 for 5 consecutive days. | Did not alter glucose levels. Improved myocardial dysfunction. | CBD as a potential therapeutic in the treatment of diabetic cardiovascular conditions and oxidative stress. |
| 12 | Gregorio et al. (2019) [53] | Determining whether acute CBD administration modulates DRN 5-HT neuronal activity and effect of repeated treatment with low doses of CBD on mechanical allodynia | Rats. Acute increasing intravenous doses of CBD (0.1-1.0 mg/kg). Repeated treatment with CBD (5 mg/kg/day, subcutaneously) | Repeated CBD treatment could prevent mechanical allodynia and anxiety-like behavior. | Repeating with low doses of CBD induces analgesia and reduces anxiety. |
| 13 | Bis-Humbert et al. (2021) [54] | Comparing the antidepressant-like response induced by cannabidiol | Rats. 3, 10, and 30 mg/kg | Decreased body weight. Improved despair-like behavior. Did not modulate anxiety-like behavior. | Support the idea that cannabidiol exerts antidepressant and anxiolytic effects. |
| 14 | Borys et al. (1979) [55] | Effects in mice of both acute and subacute CBD treatment on sleep time | Rats. 120 mg/kg | Significant increases in sleep. | Inhibitory action of CBD is still unknown. |
| 15 | Peres et al. (2016) [56] | CBD treatment would attenuate motor and cognitive impairments | Rats. 0.5 or 5 mg/kg | CBD improves motor and cognitive impairments. | Include CBD in the pharmacotherapy of Parkinson's disease. |
| 16 | Vuolo et al. (2015) [57] | Effects of CBD on inflammatory parameters (evaluated by cytokine levels) in an asthma model. | Rats. Dose of 5 mg/kg. | Significantly reduced cytokine levels, exhibiting anti-inflammatory effects. | Beneficial effect of CBD in an animal model of asthma. |
| 17 | Wheal et al. (2014) [58] | CBD effect decreases insulitis, inflammation, neuropathic pain, and myocardial dysfunction in preclinical models | Rats. Dose of 10 mg. | Relaxing | Improves the ability of arteries to relax through increased production of vasodilatory products. |
| 18 | Hammell et al. (2016) [59] | Cannabidiol (CBD) attenuates inflammation and pain without side effects | Rats. | Reduced joint inflammation. | Effective doses for reduce inflammation. |
| 19 | Belardo et al. (2019) [60] | Effects of CBD on neurological dysfunctions associated with TBI | Dose of 0.6 to 6.2 mg/day. | Restored behavioral alterations and partially normalized cortical biochemical changes. | CBD as a pharmacological tool to improve neurological dysfunctions caused by trauma. |
| 20 | Ceprián et al. (2017) [61] | Protective effect of CBD in a neonatal rat model of AIS. | Dissolved in hemp seed oil and tocopherol. CBD (30 μl, 10% oil). | Improved neurobehavioral function in terms of strength, hemiparesis, coordination, and sensorimotor performance. | CBD administration following middle cerebral artery occlusion (MCAO). |
| 21 | Costa et al. (2004a) [62] | Anti-inflammatory and anti-hyperalgesic effects of cannabidiol | Rats. Dose of 5 mg/kg intraperitoneally. | Anti-hyperalgesic effect. | Beneficial effect on two inflammation symptoms. |
| 22 | Costa et al. (2004b) [63] | Anti-hyperalgesic effect of CBD | Rats. Oral dose (5-40 mg/kg). | Anti-hyperalgesic effect. | The potential involvement of transient receptor potential vanilloid type 1 receptor. Could be a molecular target of anti-hyperalgesic action. |
| 23 | Costa et al. (2007) [64] | Therapeutic potential in neuropathic pain. | Rats. Oral dose of 10 mg kg-1 (5 ml kg-1). | Anti-inflammatory and immunomodulatory effects. | Therapeutic use for pain. |
| 24 | Ignatowska-Jankowska et al. (2011) [65] | Effects of repeated CBD administration on body weight gain in rats | Rats. at doses of 2.5 and 5 mg/kg/day | Ability to modulate weight gain. | Further investigation into the regulation of body weight. |
| 25 | Murillo-Rodríguez, et al. (2006) [66] | Effects of CBD on sleep | Rats. Doses of 10mg/5mg intracerebroventricularly | Modulates wakefulness. | Addressing vanilloid receptors. |
| 26 | Schiavon et al. (2014) [67] | Cannabidiol, one of the main non-psychoactive components | Mice. Doses of 3, 10, and 30 mg/kg | Protective effect of CBD on neuronal death. | The mechanisms underlying the neuroprotective effects of CBD. |
| 27 | Wang et al. (2017) [68] | Effects of CBD on alcohol-induced chronic and compulsive feeding-induced liver injury. | Mice. Doses: ethanol (5 g/kg body weight) and 5 or 10 mg/kg/day of CBD. | Antioxidant, cytoprotective, and anti-inflammatory properties. Attenuates chronic liver injury and ethanol-induced steatosis. | Therapeutic potential in liver diseases associated with inflammation, oxidative stress, metabolic dysregulation, and steatosis. |
| Clinical studies in humans (n=19) | |||||
| 28 | Zuardi et al. (1993a) [69] | Explore the effect of CBD and aspirin in stressful situations. | n = 40 (♂ = 18, ♀ = 22), CBD single healthy doce at 300 mg dissolved in corn oil (100 mg / ml) | Anxiolytic | Realize confirmatory analysis of results |
| 29 | Zuardi et al. (1993b) [70] | Explore the effects of CBD on plasma prolactin, growth hormone, and cortisol. | n = 11, healthy Single dose of CBD at 300 mg and 400 mg |
Sedative and anti-inflammatory | Realize confirmatory analysis of results |
| 30 | Martin et al. (2019) [71] | Long-term effects of CBD on cognitive function. | n = 27, epilepsy Annual CBD intake of 36,5 mg / kg / día |
No effects on cognitive function | Realize new studies with Randomized, placebo-controlled, and larger samples. |
| 31 | Allendorfer et al. (2019) [72] | Effects of CBD oral solution on attention. | n = 22 epilepsy 25 mg / kg / d for at least 2 weeks |
No effect on mood | Controlled trials and examination of long-term effects, follow-ups after treatment. |
| 32 | Santos et al. (2021) [73] | Reduce tremors in patients with ET. | n=19 ET patients. Oral dose of CBD (300 mg). | A single dose had no effect on upper limb tremors | Chronic treatment with CBD. |
| 33 | Kasper et al. (2020) [74] | Prevalence of CBD use in professional rugby league and union players. | n=517 rugby players. Survey. | CBD use showed improvement in recovery/pain (80%) and sleep (78%), and 68% of players reported a perceived benefit | Need to explore claims regarding pain and sleep. |
| 34 | Cochrane-Snyman et al. (2021) [75] | Effect of CBD oil on perceived muscle pain, inflammation, and strength performance. | n=13 men Dose: 150 mg. |
They did not support that supplementation with CBD oil would have an effect on muscle damage and inflammation after an ECC protocol. | Investigate broader ranges of CBD dosage and scheduling in trained and untrained men and women. |
| 35 | Neubauer et al. (2018) [76] | Evaluate the effectiveness of complementary therapy with CBD. | Patients with epilepsy. Dose of less than 8 mg/kg/day. | Less intense seizures, shorter seizure duration, shorter recovery time, and other positive side effects of CB treatment. | Potential benefits as adjunctive therapy. |
| 36 | Lopez et al. (2020) [77] | Effects of a CBD oil extract on stress resilience, perceived recovery, mood, affect, and body composition. | 65 men and women. Dose of 60 mg. | Improved HDL cholesterol, supported psychometric measures of sleep, stress response, and perceived vitality. | Supplementary use. |
| 37 | Hatchett et al. (2020) [78] | Determine the influence of cannabidiol oil in attenuating delayed onset muscle soreness. | N=23. Dose of 16.67 mg. | Muscle recovery | Investigate the role of CBD dosage level, nutrition, sleep, exercise type, and other factors on CBD's ability to attenuate exercise-induced muscle damage effects and aid in the recovery process. |
| 38 | Sahinovic et al. (2022) [79] | Effects of acute CBD treatment on physiological and psychological responses to aerobic exercise | n=9, trained males (57.4±4 ml/kg/min) CBD (300 mg) vs Placebo 1.5h before exercise |
CBD appeared to increase VO2, ratings of pleasure and blood lactate compared to placebo. | Larger studies are required to confirm and better understand these preliminary findings. |
| 39 | Alhamoruni et al. (2012) [80] | Determine if cannabinoids modulate increased permeability associated with inflammation in vitro. | Dose of 10 ng · mL -1. | Recovery of increased permeability | Locally produced endocannabinoids, acting through CB1 receptors, play a role in mediating changes in permeability with inflammation. |
| 40 | Arndt and de Wit (2017) [81] | Effects of CBD on responses to negative emotional stimuli as a model for its potential anxiety-reducing effects. | n=38. Oral CBD 300, 600, and 900 mg. |
CBD did not produce detectable subjective effects or alterations in mood or anxiety. | Further research on the behavioral and neural mechanisms of CBD and |
| 41 | Bergamaschi et al. (2011) [82] | Effects of a simulated public speaking test. | N=24 CBD dose of 600 mg |
Reduced anxiety, cognitive impairment, and discomfort in speech performance, and decreased anticipatory speech alertness. | More research to determine the precise mechanisms of action of CBD in different anxiety disorders. |
| 42 | Birnbaum et al. (2019) [83] | Evaluate the pharmacokinetics of an oral cannabidiol capsule with and without food. | n=8. Dose of 99% pure CBD capsules on an empty stomach as well as under fed conditions. | More precise pharmacokinetic parameters | Use of CBD capsules |
| 43 | Jadoon et al. (2017) [84] | Investigate if CBD reduces blood pressure in humans. | n=9. Dose of 600 mg. | Reduces resting blood pressure and attenuates blood pressure increase during stress | Research to establish if CBD has a role in the treatment of cardiovascular disorders. |
| 44 | Kraft et al. (2008) [85] | Effects of oral cannabis extract in two different human models of acute inflammatory pain and hyperalgesia. | n=18 women. Oral capsule administration. | Hyperalgesic | Future clinical studies in patients with chronic pain |
| 45 | Linares et al. (2018) [86] | Effect of a clinically anxiolytic dose of CBD on the sleep-wake cycle. | n=27. Dose of 300 mg. | Does not interfere with the sleep cycle | Address the effects of CBD on the sleep-wake cycle in patient populations |
| 46 | Masataka (2019) [87] | Evaluate the efficacy of CBD treatment for adolescents with social anxiety disorder. | n=17. Dose of 300 mg. | Reduced anxiety | Useful option for treating social anxiety. |
| 47 | Shannon and Opila-Lehman (2016) [88] | Evidence that CBD is effective as a safe alternative treatment to traditional psychiatric medications for reducing anxiety and insomnia. | n=1, 10-year-old girl. CBD supplements (25 mg) at bedtime, and 6 mg to 12 mg of sublingual CBD spray administered during the day |
Reduces anxiety and improves sleep | Study long-term effects. |
| 48 | Isenmann et al. (2021) [89] | Effect of CBD after resistance training on performance and muscle damage | n=21 CBD after exercise (60mg on 250 mL water) vs Placebo |
Small significant effects on muscle damage and recovery after 72 h in CBD group vs Placebo | More data are required for clearer statements concerning potential pro-regenerative effects of CBD |
| 49 | Crossland et al. (2022) [90] | Determine that CBD is effective to reduce inflammation and enhances performance for strenuous eccentric exercise | 27 female (18-26 years-old) Isolate CBD (5 mg/kg; 3 times -2h, 0h and +10h) vs Placebo |
No effect for inflammation, muscle damage and subjective fatigue | Study of varying CBD supplements to determine if other phytochemicals in cannabis plant prove effective for recovery |
| Reviews and meta-analysis (n=21) | |||||
| 50 | McCartney et al. (2020) [32] | Present preliminary preclinical laboratory animal data in humans, non-athletes. | Narrative review | Anti-inflammatory Neuroprotector Analgesic Anxyolitic |
Rigorous and controlled studies in humans |
| 51 | Burggren et al. (2019) [91] | Review the effects of CBD on brain structure, function, and cognition. | Literature review | Insufficient evidence | Short and long-term consequences Effect in older adults Efficacy and safety of existing products |
| 52 | Burstein (2015) [30] | Review the effects of CBD on inflammation. | Literature review | Anti-inflammatory Decrease of secondary inflammatory effects |
Human trials with clinical application Advantages of CBD over other cannabinoids Synthetic analogs with greater potency than CBD |
| 53 | Hill et al. (2012) [92] | Effects of phyto-cannabinoids (CBD) in preclinical models of central nervous system disease. | Literature review | Neuroprotective anticonvulsant (modulates immune cell activity and limits oxidative stress) |
Long-term, double-blind, placebo-controlled trials are needed. Participants with different affective disorders. |
| 54 | Booz (2011) [93] | Effects of CBD on inflammation and oxidative stress. | Narrative review | Anti-inflammatory Antioxidant |
More details are needed on how CBD targets inflammatory signaling. Test studies on the therapeutic utility of CBD. |
| 55 | Lorenzetti et al. (2016) [94] | Recent findings from human structural neuroimaging research. | Systematic review | CBD protects against these harmful effects in the hippocampus, prefrontal cortex, amygdala, and cerebellum. | Urgent development of consensus-based guidelines to quantify cannabis consumption and exposure in human studies. |
| 56 | Rojas-Valverde (2021) [33] | Explore the potential role of CBD in sports recovery. | Narrative review | CBD has anti-inflammatory, antioxidant, anxiolytic properties, and improves sleep quality. | Specific investigations are required to determine if cannabis can provide indirect benefits to athletes. |
| 57 | Kramer et al. (2020) [95] | Effects of chronic cannabis consumption on physiological parameters of sports performance. | Systematic review | It did not have a significant effect on athletic performance. Resting heart rate was the only physiological measure that differed. | Specific investigations are required to determine if cannabis can provide indirect benefits to athletes. |
| 58 | Singh and Neary (2020) [96] | Neuroprotective effects of cannabinoids, specifically the phytocannabinoid CBD, after a traumatic brain injury (TBI). | Systematic review | Enhancing neuroprotection by reducing inflammation. | Influence the blood-brain barrier, brain-derived neurotrophic factors, cognitive ability, brain vasculature, cardiovascular physiology, and neurogenesis. |
| 59 | Reillo (2019) [97] | Examine sport-related traumatic brain injury and the preventive and therapeutic use of cannabidiol among athletes. | Systematic review | Efficacy of preventive and therapeutic administration of cannabidiol (CBD) in head injuries. | Recommended as a preventive and therapeutic intervention in the treatment of traumatic brain injury. |
| 60 | Fine and Rosenfeld (2013) [98] | Link the endocannabinoid system and phytocannabinoids to their potentially therapeutic role in chronic pain management. | Systematic review | Analgesic for chronic pain. | Administered orally. |
| 61 | Sholler et al. (2020) [99] | Synthesize the efficacy of CBD as a therapeutic agent. | Systematic review | Efficacy of CBD as a therapeutic for various medical conditions, including epilepsy, anxiety, pain/inflammation, schizophrenia, and substance use disorders. | Rigorous and controlled evidence of the therapeutic efficacy of CBD is lacking. |
| 62 | Lowin et al. (2019) [100] | General effects of cannabinoids on inflammation. | Systematic review | Anti-inflammatory effects. | Targeting the right receptors in the right place. |
| 63 | Stanley et al. (2013) [101] | Establish whether the cardiovascular system is a potential therapeutic target for CBD. | Systematic review | CBD reduces the cardiovascular response to stress models. | More evidence of the positive role of CBD in the heart. |
| 64 | Bruni et al. (2018) [102] | Synergistic effect in pain treatment. | Systematic review | Therapeutic, anti-inflammatory. | Further assessment of nanotechnology systems. |
| 65 | Zurier and Burstein (2016) [103] | Ability to facilitate inflammation resolution. | Systematic review | Anti-inflammatory Reduction of fibrosis |
Cannabinoids becoming safe and effective anti-inflammatory medications. |
| 66 | Vuolo et al. (2019) [104] | CBD in respiratory pathways remodeling. | Systematic review | Anti-inflammatory Reduction of asthma |
More details on airway remodeling. |
| 67 | Crippa et al.(2011) [105] | Investigate generalized social anxiety disorder (GSAD) using functional neuroimaging. | Preliminary report | Reduction of anxiety | Effects on activity in the limbic and paralimbic areas of the brain. |
| 68 | Huestis et al. (2011) [106] | Support the status of cannabis regarding the Prohibited List. | Systematic review | Positive effect on performance | Further research on the development of tolerance after long-term frequent exposure. |
| 69 | Lattanzi et al. (2018) [107] | Efficacy and safety of CBD as an adjunctive treatment in patients with epilepsy. | Systematic review and metanalysis | Reduction of seizures frequency | Does not produce euphoric or intrusive side effects. |
| 70 | Ware et al. (2018) [108] | Identify and highlight challenges in interpreting information regarding elite athletic performance and identify important areas of research that need to be addressed. | Literature review | Promising effect for the treatment of chronic pain. | There is no evidence that cannabis consumption is a performance-enhancing drug. |
4. Discussion
4.1. Preclinic Research (Animals)
Despite the relatively popular use of cannabinoids in humans, most of the actual evidence on the effects of CBD on physiological and psychological effects focuses on animals, especially pigs, mice, and rats. The lack of clinical trials could be due to national and international restrictions on access to cannabinoids, including CBD, and strict control of their use for research purposes. Other limitations are rigorous procedures for trial approval by government drug agencies. Therefore, preclinical studies have been conducted to determine the safe initial dose and assess the potential toxicity of CBD before testing it in humans.
Some preliminary studies have found some benefits of CBD consumption in both physiological and cognitive functions. Recent evidence suggested a reduction in anxiety and better adaptation to new environments when CBD is prescribed in mice.[42,44] In contrast, other studies suggest no benefits on anxiety in response to CBD administration but not found negative effects.[43] Novel studies have suggested a neuroprotective consequence of CBD administration leading to a decrease in attenuation in BNDF levels related to the reduction of neuroinflammation[46], and some neuroprotection after a stroke event[48], stimulating neurogenesis and promoting dendritic restructuring in the hippocampus.[49] CBD also showed potential in the treatment of central and peripheral neuropathic pain[47] and some increases in acetylcholine in the brain after its administration were reported.[50] In addition, it was found to exert antidepressant and anxiolytic effects at the cognitive level, with only positive and beneficial evidence for functional recovery and anti-inflammatory symptoms.[50]
Regarding muscle function and anti-inflammatory effects of CBD administration in animals, a revealing study found that CBD intake could lead to structural and functional improvement of muscles, suggesting muscular recovery.[45] This study explained that CBD could promote the differentiation of myoblast cells into myotubes by increasing Ca2+, preventing locomotor activity loss related to the reduction of proinflammatory markers in tissue and plasma and restoration of autophagy. The results of this main study on the anti-inflammatory effects of CBD are supported by additional evidence, recognizing its use as a potential new treatment in the inflammatory response and reduction of chronic pain.[46] Hammell et al.[59] and Vuolo et al.[57] also found a positive relation of CBD with anti-inflammatory parameters (reduction of cytokine levels). Other studies have found the benefits of CBD consumption regarding sleep disorders in animals, showing that it can prolong sleep time and avoid excessive drowsiness.[46,55,66]
The notable physiological differences between animals and humans notwithstanding, these results indicate promising potential for CBD to improve muscular recovery. The data suggest CBD may modulate inflammation and thereby accelerate healing stages like inflammation, proliferation, and regeneration following tissue damage. While extrapolation to healthy humans or athletes is premature, the results merit further research on CBD's utility in recovery from muscular injury in both animals and humans.
Exercise-induced fatigue and damage in humans trigger physiological and psychological cascades. Extensive research, including studies, guidelines, reviews, and meta-analyses, has examined exercise fatigue to elucidate the central and peripheral mechanisms disrupting bodily function.[2] Common delayed-onset symptoms like sleepiness, swelling, pain, and weakness often persist hours or days post-exertion.[5] This review synthesizes human evidence on CBD’s potential to improve recovery. Elucidating CBD’s effects on inflammation, sleep, pain, and other cognitive and psychological outcomes in healthy and pathological populations could inform future applied research on CBD in sports science and medicine.
4.2. Noninflammatory and Antioxidant Effects in Humans
Eccentric exercise can induce sarcolemma damage by altering muscle cell membrane permeability and the basement membrane, enabling Ca++ influx that disrupts muscle fiber electrochemical gradients. If sarcolemma damage is modest, ATPase pumps can restore Ca++ homeostasis and reverse the damage. However, Ca++ overload initiates degradation of structural and contractile proteins, eliciting an inflammatory cascade involving macrophage and phagocyte activation within 2-6 hours post-injury, persisting for days.[30,109]
A single 300mg CBD dose alters human glucocorticoid levels including the key inflammatory regulator cortisol[70], that is considered as one of the main homeostatic regulators of the inflammatory response to injury.[110] A recent narrative review proposed CBD's anti-inflammatory effects in humans could benefit athletic performance[32], potentially by interacting with inflammation-modulating receptors (e.g., CB1, CB2, A2A) and attenuating pro-inflammatory cytokines including IL-1, TNFα, thus suppressing hyperactive immune responses and associated tissue damage.[30,92,93] There is also evidence suggesting the potential of CBD to promote the release of arachidonic acid, leading to greater healing capacity as a result of central regulation of growth signals mediated by pro-resolving substances such as lipoxin A4 and 15d-PGJ2.[30]
CBD may confer neuroprotection by reducing inflammation, protecting the brain and heart, and attenuating cardiovascular responses.[30] As CBD resolves chronic inflammation via phytocannabinoids, it could have therapeutic efficacy in conditions like epilepsy and Parkinson's disease.[30] It is also known that many human diseases due to tissue and organ damage are underpinned by the interaction between inflammation and oxidative stress.[111] In this sense, in sports, the hypothesis is raised that this CBD related to inhibitions of oxidative stress and neuroinflammation could have some therapeutic potential in sports research.
4.3. Pain and Discomfort in Humans
In sports, changes in muscle structure in response to damage can cause pain. Maximum pain is experienced 2-3 days after exercise as a result of prostaglandins produced by monocytes, which sensitize afferent nerve endings in the muscles and cause a sensation of discomfort felt as fatigue and tension (nociceptive pain). Swelling causes pain, and after intense exercise, maximum swelling typically occurs five days after exertion due to increased muscle pressure as a result of inflammation (inflammatory pain).[112] Both pain and swelling can cause a reduction in muscle shortening capacity, limitations in mobility and range of motion, decreased sleep quality, reduced muscle strength, and other reductions in neuromechanical function; that is why research on effective and efficient recovery methods is crucial in sports.[113,114]
The delayed onset of muscle pain due to damage from physical activity, as well as the management of chronic pain, are part of the therapeutic benefits of using CBD in sports performance, also improving sleep and therefore mood.[113,114] They can also include the potential of reducing resting blood pressure as a potential that improves athlete performance and regulation of body weight by CB2 receptors.[113,114]
Currently, there is very limited evidence about the ingestion of CBD and its sedative effect. In this sense, 300-400 mg of CBD seems to have sedative effects in humans due to apparently acting directly on the central nervous system[70], supported by the idea that CBD has a beneficial action on edema and hyperalgesia.[30,115] In this sense, in many countries, drugs such as Sativex, THC, and CBD are approved for the treatment of both central and peripheral neuropathic pain, which is associated with microglial activation and subsequent proinflammatory cytokine cascades such as IL-6, IL-1β, and TNFα; this supports the idea of using CBD as an anti-nociceptive agent.[93] This effect, along with other neuroprotective qualities, was also found in a recent systematic review of the outcome of CBD ingestion concerning its potential use as a substance to enhance sports performance.[32]
4.4. Sleep Quality
Sleep disorders are relatively common among athletes when recovering from fatigue injuries. Athletes are recommended to sleep for 7 to 10 hours per night, and the usual duration of sleep is less than 8 hours per night, increasing the risk of injury. The duration of sleep, but not sleep quality, appears to have an impact on performance.[116]
Sleep and pain have a reciprocal relationship, with greater pain resulting in greater sleep disturbance, as well as poor sleep quality and higher levels of pain. Some strategies such as mindfulness, self-hypnosis, meditation, and stress or anxiety reduction techniques show significant potential for sleep improvement.[113] Additionally, other psychological factors may potentially influence sleep, such as overtraining, which often occurs when intensified training and competition are accompanied by insufficient recovery.[116]
Some natural alternatives have been proposed, such as infusions, hot showers, tea consumption, and the use of oil as sleep and anxiety improvement strategies.[117] Based on these effective benefits, some team sports athletes have widely used CBD for sleep, pain relief, and recovery, and its consumption increases with age.[74] Endocannabinoid system stimulation may modulate sleep disorders in aging, being very promising evidence for sports while some elements of this system modulate the sleep-wake cycle.[118]
4.5. Cognitive and Psychological Effects
Regarding the effect on cognition and mood, there is evidence suggesting the absence of benefits after prolonged use of CBD in humans.[71,72] On the other hand, a single administration of 300 mg of CBD has been reported to have an anxiolytic effect in healthy humans.[69] Specifically in sports, athletes, due to their competitive nature, tend to exhibit exaggerated behaviors. This can lead to states of high anxiety and even in some situations can trigger states of depression. In this sense, CBD could have anxiolytic and antidepressant actions through the activation of 5-HT1A receptors, but more evidence is needed to consider these conclusions strong enough.[93]
Preliminary studies show that CBD protects against neuroanatomical alterations.[93] This is significant as emotional stimuli can be determinants in sports performance, such as anxiety[93], and they are reduced with the useful use of cannabidiol on the limbic and paralimbic areas of the brain.[93] Finally, the potential use of CBD in sports performance as an anxiolytic substance has been explored, with authors linking the possible effect on exercise with previous clinical and preclinical studies in animals, healthy populations, and patients with underlying pathologies.[32]
4.6. Study Limitations
Due to the lack of research in sports medicine and science, the main limitation is the struggle to extrapolate the benefits found in animals, healthy humans, and patients with pathologies to potential applications in sports science. There is a need for new evidence in humans considering the lack of available information, knowing an exact dosage, and relatively common methodological flaws in accessible research.
The relatively low rate of publications analyzing the effects of CBD on variables related to recovery led to a large amount of duplicated information among databases. The way some studies approach the descriptors cannabinoids, CBD, cannabis, and THC generates confusion, due to some flaws in the presentation of methodology, which make interpretation of results difficult. As a result of the different approaches of studies and methodological differences, it was difficult to systematize information.
Although CBD has been shown to have a series of properties that may suggest its potential use in athletes, there are current conditions of sale and commercialization that require caution in its consumption. Poor manufacturing, THC present in CBD products and lack of product labeling and analytical reports could cause serious health problems and violations of doping regulations. In addition, the large doses of CBD used in the reviewed studies are not readily available to athletes without prescription.
5. Conclusions
CBD appears to have anti-inflammatory, neuroprotective, analgesic, anxiolytic, and potentially performance-enhancing properties in athletes, but further scientific evidence is necessary to confirm these effects. Confirmatory analyses using randomized placebo-controlled trials to test the acute and chronic effects of different dosing regimens are needed. These studies should consider fundamental aspects of sports, such as the variety of biological and situational conditions that contribute to fatigue, the characteristics of each discipline during training and competition, as well as individual athlete peculiarities, tolerance and response to CBD intake, and the combined effect of CBD administration with other physical and nutritional aids.
5.1. Practical Applications and Future Research
Given the relatively common use of cannabis and CBD among athletes, there is a clear need to improve scientific understanding of the effects of CBD use on athlete recovery and performance. More scientific advances are needed, mainly the execution of experimental trials, which allow for a greater understanding of both positive and negative critical results for the ultimate benefit of athlete recovery and performance.
New randomized placebo-controlled studies should consider different etiologies of fatigue and damage, individualities and disciplines, needs and special characteristics. Other potential research areas include: (1) optimal dosing based on physical and physiological load, (2) the efficacy concerning the timing of CBD administration (before, during, or after training/competition), (3) the chronic versus the acute effects of CBD, (4) the cumulative responses with other recovery strategies, or (5) the differences in tolerance and efficacy by sex, professional level, fitness level, and other individual conditions. More information is needed on understanding CBD's inflammatory signaling in recovery process. Also, the effectiveness of CBD versus conventional medication should be evaluated.
The resulting evidence could provide new clinical guidance for prescribing CBD during the athlete's recovery process and other potential applications. The possible therapeutic benefits of CBD administration have been minimized for years, but the actual scenario could facilitate increased knowledge about this natural compound and its effects. Moreover, a clearer and global policy for the use of cannabis in sports should be considered.
Author Contributions
Conceptualization, C.E.V.-G. and D.R.-V.; methodology, B.S.-U. and C.A.-M.; software, C.E.V.-G. and C.D.G.-C.; validation, C.D.G.-C., C.A.-M. and D.R.-V.; formal analysis, C.D.G.-C. and B.S.-U.; investigation, C.E.V.-G. and D.R.-V.; resources, B.S.-U. and C.A.-M.; data curation, C.D.G.-C. and B.S.-U.; writing—original draft preparation, C.E.V.-G. and C.D.G.-C.; writing—review and editing, B.S.-U., C.A.-M. and D.R.-V.; visualization, B.S.-U. and C.A.-M.; supervision, D.R.-V.; project administration, B.S.-U. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rojas-Valverde, D.; Gutiérrez-Vargas, R.; Rodríguez-Montero, A.; Pereira, L.A.; Loturco, I.; Martín-Rodríguez, S. Reduced Muscle Contractile Function in Elite Young Soccer Players after a Short-Congested Fixture Period. Proc. Inst. Mech. Eng. Part P J. Sports Eng. Technol. 2018, 175433711881795. [CrossRef]
- Martínez-Guardado, I.; Rojas-Valverde, D.; Gutiérrez-Vargas, R.; Ugalde Ramírez, A.; Gutiérrez-Vargas, J.C.; Sánchez-Ureña, B. Intermittent Pneumatic Compression and Cold Water Immersion Effects on Physiological and Perceptual Recovery During Multi-Sports International Championship. J. Funct. Morphol. Kinesiol. 2020, 5, 45. [CrossRef]
- Ament, W.; Verkerke, G.J. Exercise and Fatigue. Sports Med. Auckl. NZ 2009, 39, 389–422. [CrossRef]
- Metsios, G.S.; Moe, R.H.; Kitas, G.D. Exercise and Inflammation. Best Pract. Res. Clin. Rheumatol. 2020, 101504. [CrossRef]
- Kreher, J.B.; Schwartz, J.B. Overtraining Syndrome: A Practical Guide. Sports Health Multidiscip. Approach 2012, 4, 128–138. [CrossRef]
- Haugen, T.; Seiler, S.; Sandbakk, Ø.; Tønnessen, E. The Training and Development of Elite Sprint Performance: An Integration of Scientific and Best Practice Literature. Sports Med. - Open 2019, 5, 44. [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [CrossRef]
- Merry, T.L.; Ristow, M. Do Antioxidant Supplements Interfere with Skeletal Muscle Adaptation to Exercise Training? J. Physiol. 2016, 594, 5135–5147. [CrossRef]
- Rojas-Valverde, D.; Montoya-Rodríguez, J.; Azofeifa-Mora, C.; Sanchez-Urena, B. Effectiveness of Beetroot Juice Derived Nitrates Supplementation on Fatigue Resistance during Repeated-Sprints: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2020, 1–12. [CrossRef]
- Campos, A.C.; Moreira, F.A.; Gomes, F.V.; Del Bel, E.A.; Guimarães, F.S. Multiple Mechanisms Involved in the Large-Spectrum Therapeutic Potential of Cannabidiol in Psychiatric Disorders. Philos. Trans. R. Soc. B Biol. Sci. 2012, 367, 3364–3378. [CrossRef]
- Lim, S.Y.; Sharan, S.; Woo, S. Model-Based Analysis of Cannabidiol Dose-Exposure Relationship and Bioavailability. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 291–300. [CrossRef]
- WHO Cannabidiol (CBD): World Health Organisation Expert Committe on Drug Dependence. Thyrty-Ninth Meet. 2017.
- Stout, S.M.; Cimino, N.M. Exogenous Cannabinoids as Substrates, Inhibitors, and Inducers of Human Drug Metabolizing Enzymes: A Systematic Review. Drug Metab. Rev. 2014, 46, 86–95. [CrossRef]
- VanDolah, H.J.; Bauer, B.A.; Mauck, K.F. Clinicians’ Guide to Cannabidiol and Hemp Oils. Mayo Clin. Proc. 2019, 94, 1840–1851. [CrossRef]
- Millar, S.A.; Stone, N.L.; Bellman, Z.D.; Yates, A.S.; England, T.J.; O’Sullivan, S.E. A Systematic Review of Cannabidiol Dosing in Clinical Populations. Br. J. Clin. Pharmacol. 2019, 85, 1888–1900. [CrossRef]
- Cunha, J.M.; Carlini, E.A.; Pereira, A.E.; Ramos, O.L.; Pimentel, C.; Gagliardi, R.; Sanvito, W.L.; Lander, N.; Mechoulam, R. Chronic Administration of Cannabidiol to Healthy Volunteers and Epileptic Patients. Pharmacology 1980, 21, 175–185. [CrossRef]
- Zuardi, A.; Crippa, J.; Dursun, S.; Morais, S.; Vilela, J.; Sanches, R.; Hallak, J. Cannabidiol Was Ineffective for Manic Episode of Bipolar Affective Disorder. J. Psychopharmacol. Oxf. Engl. 2010, 24, 135–137. [CrossRef]
- Docter, S.; Khan, M.; Gohal, C.; Ravi, B.; Bhandari, M.; Gandhi, R.; Leroux, T. Cannabis Use and Sport: A Systematic Review. Sports Health 2020, 12, 189–199. [CrossRef]
- Nichols, J.M.; Kaplan, B.L.F. Immune Responses Regulated by Cannabidiol. Cannabis Cannabinoid Res. 2019, 5, 12–31. [CrossRef]
- Huestis, M.A.; Solimini, R.; Pichini, S.; Pacifici, R.; Carlier, J.; Busardò, F.P. Cannabidiol Adverse Effects and Toxicity. Curr. Neuropharmacol. 2019, 17, 974–989. [CrossRef]
- Whiting, P.F.; Wolff, R.F.; Deshpande, S.; Nisio, M.D.; Duffy, S.; Hernandez, A.V.; Keurentjes, J.C.; Lang, S.; Misso, K.; Ryder, S.; et al. Cannabinoids for Medical Use: A Systematic Review and Meta-Analysis. JAMA 2015, 313, 2456–2473. [CrossRef]
- Pinto, J.V.; Saraf, G.; Frysch, C.; Vigo, D.; Keramatian, K.; Chakrabarty, T.; Lam, R.W.; Kauer-Sant’Anna, M.; Yatham, L.N. Cannabidiol as a Treatment for Mood Disorders: A Systematic Review. Can. J. Psychiatry 2020, 65, 213–227. [CrossRef]
- Higgins, T.R.; Greene, D.A.; Baker, M.K. Effects of Cold Water Immersion and Contrast Water Therapy for Recovery From Team Sport: A Systematic Review and Meta-Analysis. J. Strength Cond. Res. 2017, 31, 1443–1460. [CrossRef]
- Rojas-Valverde, D.; Sánchez-Ureña, B.; Crowe, J.; Timón, R.; Olcina, G.J. Exertional Rhabdomyolysis and Acute Kidney Injury in Endurance Sports: A Systematic Review. Eur. J. Sport Sci. 2020, 0, 1–28. [CrossRef]
- McPartland, J.M.; Duncan, M.; Marzo, V.D.; Pertwee, R.G. Are Cannabidiol and Δ9-Tetrahydrocannabivarin Negative Modulators of the Endocannabinoid System? A Systematic Review. Br. J. Pharmacol. 2015, 172, 737–753. [CrossRef]
- Carek, P.J.; Laibstain, S.E.; Carek, S.M. Exercise for the Treatment of Depression and Anxiety. Int. J. Psychiatry Med. 2011, 41, 15–28. [CrossRef]
- Tantimonaco, M.; Ceci, R.; Sabatini, S.; Catani, M.V.; Rossi, A.; Gasperi, V.; Maccarrone, M. Physical Activity and the Endocannabinoid System: An Overview. Cell. Mol. Life Sci. 2014, 71, 2681–2698. [CrossRef]
- Cuñetti, L.; Manzo, L.; Peyraube, R.; Arnaiz, J.; Curi, L.; Orihuela, S. Chronic Pain Treatment With Cannabidiol in Kidney Transplant Patients in Uruguay. Transplant. Proc. 2018, 50, 461–464. [CrossRef]
- Shannon, S.; Lewis, N.; Lee, H.; Hughes, S. Cannabidiol in Anxiety and Sleep: A Large Case Series. Perm. J. 2019, 23. [CrossRef]
- Burstein, S. Cannabidiol (CBD) and Its Analogs: A Review of Their Effects on Inflammation. Bioorg. Med. Chem. 2015, 23, 1377–1385. [CrossRef]
- Zarrabi, A.J.; Frediani, J.K.; Levy, J.M. The State of Cannabis Research Legislation in 2020. N. Engl. J. Med. 2020, 382, 1876–1877. [CrossRef]
- McCartney, D.; Benson, M.J.; Desbrow, B.; Irwin, C.; Suraev, A.; McGregor, I.S. Cannabidiol and Sports Performance: A Narrative Review of Relevant Evidence and Recommendations for Future Research. Sports Med. - Open 2020, 6, 27. [CrossRef]
- Rojas-Valverde, D. Potential Role of Cannabidiol (CBD) on Sport Recovery: A Narrative Review. Front. Physiol. 2021, 12. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906.
- Whittemore, R.; Knafl, K. The Integrative Review: Updated Methodology. J. Adv. Nurs. 2005, 52, 546–553. [CrossRef]
- A Step-by-Step Guide to Conducting an Integrative Review; Toronto, C.E., Remington, R., Eds.; Springer International Publishing: Cham, 2020; ISBN 978-3-030-37503-4.
- Souza, M.T. de; Silva, M.D. da; Carvalho, R. de Integrative Review: What Is It? How to Do It? Einstein São Paulo 2010, 8, 102–106.
- Medina, J.M.; McKeon, P.O.; Hertel, J. Rating the Levels of Evidence in Sports-Medicine Research. Int. J. Athl. Ther. Train. 2006, 11, 38–41. [CrossRef]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. BMC Vet. Res. 2020, 16, 242. [CrossRef]
- Crocker, T.F.; Lam, N.; Jordão, M.; Brundle, C.; Prescott, M.; Forster, A.; Ensor, J.; Gladman, J.; Clegg, A. Risk-of-Bias Assessment Using Cochrane’s Revised Tool for Randomized Trials (RoB 2) Was Useful but Challenging and Resource-Intensive: Observations from a Systematic Review. J. Clin. Epidemiol. 2023, 161, 39–45. [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [CrossRef]
- Zieba, J.; Sinclair, D.; Sebree, T.; Bonn-Miller, M.; Gutterman, D.; Siegel, S.; Karl, T. Cannabidiol (CBD) Reduces Anxiety-Related Behavior in Mice via an FMRP-Independent Mechanism. Pharmacol. Biochem. Behav. 2019, 181, 93–100. [CrossRef]
- Schleicher, E.M.; Ott, F.W.; Mueller, M.; Silcher, B.; Sichler, M.E.; Loew, M.J.; Wagner, J.M.; Bouter, Y. Prolonged Cannabidiol Treatment Lacks on Detrimental Effects on Memory, Motor Performance and Anxiety in C57BL/6J Mice. Front. Behav. Neurosci. 2019, 13, 94. [CrossRef]
- Myers, A.M.; Siegele, P.B.; Foss, J.D.; Tuma, R.F.; Ward, S.J. Single and Combined Effects of Plant-Derived and Synthetic Cannabinoids on Cognition and Cannabinoid-Associated Withdrawal Signs in Mice. Br. J. Pharmacol. 2019, 176, 1552–1567. [CrossRef]
- Iannotti, F.A.; Pagano, E.; Moriello, A.S.; Alvino, F.G.; Sorrentino, N.C.; D’Orsi, L.; Gazzerro, E.; Capasso, R.; De Leonibus, E.; De Petrocellis, L.; et al. Effects of Non-Euphoric Plant Cannabinoids on Muscle Quality and Performance of Dystrophic Mdx Mice. Br. J. Pharmacol. 2019, 176, 1568–1584. [CrossRef]
- Santiago, A.N.; Mori, M.A.; Guimaraes, F.S.; Milani, H.; Weffort de Oliveira, R.M. Effects of Cannabidiol on Diabetes Outcomes and Chronic Cerebral Hypoperfusion Comorbidities in Middle-Aged Rats. Neurotox. Res. 2019, 35, 463–474. [CrossRef]
- Casey, S.L.; Atwal, N.; Vaughan, C.W. Cannabis Constituent Synergy in a Mouse Neuropathic Pain Model. Pain 2017, 158, 2452–2460. [CrossRef]
- Hayakawa, K.; Mishima, K.; Nozako, M.; Hazekawa, M.; Irie, K.; Fujioka, M.; Orito, K.; Abe, K.; Hasebe, N.; Egashira, N.; et al. Delayed Treatment with Cannabidiol Has a Cerebroprotective Action via a Cannabinoid Receptor-Independent Myeloperoxidase-Inhibiting Mechanism. J. Neurochem. 2007, 102, 1488–1496. [CrossRef]
- Mori, M.A.; Meyer, E.; Soares, L.M.; Milani, H.; Guimarães, F.S.; de Oliveira, R.M.W. Cannabidiol Reduces Neuroinflammation and Promotes Neuroplasticity and Functional Recovery after Brain Ischemia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2017, 75, 94–105. [CrossRef]
- Murillo-Rodríguez, E.; Arankowsky-Sandoval, G.; Rocha, N.B.; Peniche-Amante, R.; Veras, A.B.; Machado, S.; Budde, H. Systemic Injections of Cannabidiol Enhance Acetylcholine Levels from Basal Forebrain in Rats. Neurochem. Res. 2018, 43, 1511–1518. [CrossRef]
- García-Baos, A.; Puig-Reyne, X.; García-Algar, Ó.; Valverde, O. Cannabidiol Attenuates Cognitive Deficits and Neuroinflammation Induced by Early Alcohol Exposure in a Mice Model. Biomed. Pharmacother. Biomedecine Pharmacother. 2021, 141, 111813. [CrossRef]
- Mukhopadhyay, P.; Rajesh, M.; Horváth, B. Cannabidiol Protects against Hepatic Ischemia/Reperfusion Injury by Attenuating Inflammatory Signaling and Response, Oxidative/Nitrative Stress, and Cell Death. Free Radic Biol Med 2011, 50.
- Gregorio, D.; McLaughlin, R.; Posa, L. Cannabidiol Modulates Serotonergic Transmission and Reverses Both Allodynia and Anxiety-like Behavior in a Model of Neuropathic Pain. Pain. 2019, 160.
- Bis-Humbert, C.; García-Cabrerizo, R.; García-Fuster, M.J. Antidepressant-like Effects of Cannabidiol in a Rat Model of Early-Life Stress with or without Adolescent Cocaine Exposure. Pharmacol. Rep. 2021. [CrossRef]
- Borys, H.K.; Ingall, G.B.; Karler, R. Development of Tolerance to the Prolongation of Hexobarbitone Sleeping Time Caused by Cannabidiol. Br. J. Pharmacol. 1979, 67, 93–101.
- Peres, F.F.; Levin, R.; Suiama, M.A.; Diana, M.C.; Gouvêa, D.A.; Almeida, V.; Santos, C.M.; Lungato, L.; Zuardi, A.W.; Hallak, J.E.C.; et al. Cannabidiol Prevents Motor and Cognitive Impairments Induced by Reserpine in Rats. Front. Pharmacol. 2016, 7, 343. [CrossRef]
- Vuolo, F.; Petronilho, F.; Sonai, B.; Ritter, C.; Hallak, J.E.C.; Zuardi, A.W.; Crippa, J.A.; Dal-Pizzol, F. Evaluation of Serum Cytokines Levels and the Role of Cannabidiol Treatment in Animal Model of Asthma. Mediators Inflamm. 2015, 2015, 538670. [CrossRef]
- Wheal, A.J.; Cipriano, M.; Fowler, C.J.; Randall, M.D.; O’Sullivan, S.E. Cannabidiol Improves Vasorelaxation in Zucker Diabetic Fatty Rats through Cyclooxygenase Activation. J. Pharmacol. Exp. Ther. 2014, 351, 457–466. [CrossRef]
- Hammell, D.C.; Zhang, L.P.; Ma, F.; Abshire, S.M.; McIlwrath, S.L.; Stinchcomb, A.L.; Westlund, K.N. Transdermal Cannabidiol Reduces Inflammation and Pain-Related Behaviours in a Rat Model of Arthritis. Eur. J. Pain Lond. Engl. 2016, 20, 936–948. [CrossRef]
- Belardo, C.; Iannotta, M.; Boccella, S.; Rubino, R.C.; Ricciardi, F.; Infantino, R.; Pieretti, G.; Stella, L.; Paino, S.; Marabese, I.; et al. Oral Cannabidiol Prevents Allodynia and Neurological Dysfunctions in a Mouse Model of Mild Traumatic Brain Injury. Front. Pharmacol. 2019, 10, 352. [CrossRef]
- Ceprián, M.; Jiménez-Sánchez, L.; Vargas, C.; Barata, L.; Hind, W.; Martínez-Orgado, J. Cannabidiol Reduces Brain Damage and Improves Functional Recovery in a Neonatal Rat Model of Arterial Ischemic Stroke. Neuropharmacology 2017, 116, 151–159. [CrossRef]
- Costa, B.; Colleoni, M.; Conti, S. Oral Anti-Inflammatory Activity of Cannabidiol, a Non-Psychoactive Constituent of Cannabis, in Acute Carrageenan-Induced Inflammation in the Rat Paw. Naunyn. Schmiedebergs Arch. Pharmacol. 2004, 369, 294–299. [CrossRef]
- Costa, B.; Giagnoni, G.; Franke, C.; Trovato, A.; Colleoni, M. Vanilloid TRPV1 Receptor Mediates the Antihyperalgesic Effect of the Nonpsychoactive Cannabinoid, Cannabidiol, in a Rat Model of Acute Inflammation. Br. J. Pharmacol. 2004, 143, 247–250. [CrossRef]
- Costa, B.; Trovato, A.; Comelli, F.; Giagnoni, G.; Colleoni, M. The Non-Psychoactive Cannabis Constituent Cannabidiol Is an Orally Effective Therapeutic Agent in Rat Chronic Inflammatory and Neuropathic Pain. Eur. J. Pharmacol. 2007, 556, 75–83. [CrossRef]
- Ignatowska-Jankowska, B.; Jankowski, M.M.; Swiergiel, A.H. Cannabidiol Decreases Body Weight Gain in Rats: Involvement of CB2 Receptors. Neurosci. Lett. 2011, 490, 82–84. [CrossRef]
- Murillo-Rodríguez, E.; Millán-Aldaco, D.; Palomero-Rivero, M.; Mechoulam, R.; Drucker-Colín, R. Cannabidiol, a Constituent of Cannabis Sativa, Modulates Sleep in Rats. FEBS Lett 2006, 580.
- Schiavon, A.P.; Soares, L.M.; Bonato, J.M.; Milani, H.; Guimarães, F.S.; Weffort de Oliveira, R.M. Protective Effects of Cannabidiol against Hippocampal Cell Death and Cognitive Impairment Induced by Bilateral Common Carotid Artery Occlusion in Mice. Neurotox. Res. 2014, 26, 307–316. [CrossRef]
- Wang, Y.; Mukhopadhyay, P.; Cao, Z.; Wang, H.; Feng, D.; Haskó, G.; Mechoulam, R.; Gao, B.; Pacher, P. Cannabidiol Attenuates Alcohol-Induced Liver Steatosis, Metabolic Dysregulation, Inflammation and Neutrophil-Mediated Injury. Sci. Rep. 2017, 7, 12064. [CrossRef]
- Zuardi, A.; Cosme, R.; Graeff, F.; Guimaraes, F. Effects of Ipsapirone and Cannabidiol on Human Experimental Anxiety. J. Psychopharmacol. (Oxf.) 1993, 7, 82–88. [CrossRef]
- Zuardi, A.W.; Guimarães, F.S.; Moreira, A.C. Effect of Cannabidiol on Plasma Prolactin, Growth Hormone and Cortisol in Human Volunteers. Braz. J. Med. Biol. Res. Rev. Bras. Pesqui. Medicas E Biol. 1993, 26, 213–217.
- Martin, R.C.; Gaston, T.E.; Thompson, M.; Ampah, S.B.; Cutter, G.; Bebin, E.M.; Szaflarski, J.P. Cognitive Functioning Following Long-Term Cannabidiol Use in Adults with Treatment-Resistant Epilepsy. Epilepsy Behav. 2019, 97, 105–110. [CrossRef]
- Allendorfer, J.B.; Nenert, R.; Bebin, E.M.; Gaston, T.E.; Grayson, L.E.; Hernando, K.A.; Houston, J.T.; Hansen, B.; Szaflarski, J.P. fMRI Study of Cannabidiol-Induced Changes in Attention Control in Treatment-Resistant Epilepsy. Epilepsy Behav. 2019, 96, 114–121. [CrossRef]
- Santos de Alencar, S.; Crippa, J.A.S.; Brito, M.C.M.; Pimentel, Â.V.; Cecilio Hallak, J.E.; Tumas, V. A Single Oral Dose of Cannabidiol Did Not Reduce Upper Limb Tremor in Patients with Essential Tremor. Parkinsonism Relat. Disord. 2021, 83, 37–40. [CrossRef]
- Kasper, A.M.; Sparks, S.A.; Hooks, M.; Skeer, M.; Webb, B.; Nia, H.; Morton, J.P.; Close, G.L. High Prevalence of Cannabidiol Use Within Male Professional Rugby Union and League Players: A Quest for Pain Relief and Enhanced Recovery. Int. J. Sport Nutr. Exerc. Metab. 2020, 1–8. [CrossRef]
- Cochrane-Snyman, K.C.; Cruz, C.; Morales, J.; Coles, M. The Effects of Cannabidiol Oil on Noninvasive Measures of Muscle Damage in Men. Med. Sci. Sports Exerc. 2021, 53, 1460–1472. [CrossRef]
- Neubauer, D.; Perković Benedik, M.; Osredkar, D. Cannabidiol for Treatment of Refractory Childhood Epilepsies: Experience from a Single Tertiary Epilepsy Center in Slovenia. Epilepsy Behav. EB 2018, 81, 79–85. [CrossRef]
- Lopez, H.L.; Cesareo, K.R.; Raub, B.; Kedia, A.W.; Sandrock, J.E.; Kerksick, C.M.; Ziegenfuss, T.N. Effects of Hemp Extract on Markers of Wellness, Stress Resilience, Recovery and Clinical Biomarkers of Safety in Overweight, But Otherwise Healthy Subjects. J. Diet. Suppl. 2020, 17, 561–586. [CrossRef]
- Hatchett, A.; Armstrong, K.; Hughes, B.; Parr, B. The Influence Cannabidiol on Delayed Onset of Muscle Soreness. Int. J. Phys. Educ. Sports Health 2020, 89–94.
- Sahinovic, A.; Irwin, C.; Doohan, P.T.; Kevin, R.C.; Cox, A.J.; Lau, N.S.; Desbrow, B.; Johnson, N.A.; Sabag, A.; Hislop, M.; et al. Effects of Cannabidiol on Exercise Physiology and Bioenergetics: A Randomised Controlled Pilot Trial. Sports Med. - Open 2022, 8, 27. [CrossRef]
- Alhamoruni, A.; Wright, K.L.; Larvin, M.; O’Sullivan, S.E. Cannabinoids Mediate Opposing Effects on Inflammation-Induced Intestinal Permeability. Br. J. Pharmacol. 2012, 165, 2598–2610. [CrossRef]
- Arndt, D.L.; de Wit, H. Cannabidiol Does Not Dampen Responses to Emotional Stimuli in Healthy Adults. Cannabis Cannabinoid Res. 2017, 2, 105–113. [CrossRef]
- Bergamaschi, M.M.; Queiroz, R.H.C.; Chagas, M.H.N.; de Oliveira, D.C.G.; De Martinis, B.S.; Kapczinski, F.; Quevedo, J.; Roesler, R.; Schröder, N.; Nardi, A.E.; et al. Cannabidiol Reduces the Anxiety Induced by Simulated Public Speaking in Treatment-Naïve Social Phobia Patients. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2011, 36, 1219–1226. [CrossRef]
- Birnbaum, A.K.; Karanam, A.; Marino, S.E.; Barkley, C.M.; Remmel, R.P.; Roslawski, M.; Gramling-Aden, M.; Leppik, I.E. Food Effect on Pharmacokinetics of Cannabidiol Oral Capsules in Adult Patients with Refractory Epilepsy. Epilepsia 2019, 60, 1586–1592. [CrossRef]
- Jadoon, K.A.; Tan, G.D.; O’Sullivan, S.E. A Single Dose of Cannabidiol Reduces Blood Pressure in Healthy Volunteers in a Randomized Crossover Study. JCI Insight 2017, 2, e93760, 93760. [CrossRef]
- Kraft, B.; Frickey, N.A.; Kaufmann, R.M.; Reif, M.; Frey, R.; Gustorff, B.; Kress, H.G. Lack of Analgesia by Oral Standardized Cannabis Extract on Acute Inflammatory Pain and Hyperalgesia in Volunteers. Anesthesiology 2008, 109, 101–110. [CrossRef]
- Linares, I.M.P.; Guimaraes, F.S.; Eckeli, A.; Crippa, A.C.S.; Zuardi, A.W.; Souza, J.D.S.; Hallak, J.E.; Crippa, J.A.S. No Acute Effects of Cannabidiol on the Sleep-Wake Cycle of Healthy Subjects: A Randomized, Double-Blind, Placebo-Controlled, Crossover Study. Front. Pharmacol. 2018, 9, 315. [CrossRef]
- Masataka, N. Anxiolytic Effects of Repeated Cannabidiol Treatment in Teenagers With Social Anxiety Disorders. Front. Psychol. 2019, 10, 2466. [CrossRef]
- Shannon, S.; Opila-Lehman, J. Effectiveness of Cannabidiol Oil for Pediatric Anxiety and Insomnia as Part of Posttraumatic Stress Disorder: A Case Report. Perm. J. 2016, 20, 16–005. [CrossRef]
- Isenmann, E.; Veit, S.; Starke, L.; Flenker, U.; Diel, P. Effects of Cannabidiol Supplementation on Skeletal Muscle Regeneration after Intensive Resistance Training. Nutrients 2021, 13, 3028. [CrossRef]
- Crossland, B.W.; Rigby, B.R.; Duplanty, A.A.; King, G.A.; Juma, S.; Levine, N.A.; Clark, C.E.; Ramirez, K.P.; Varone, N.L. Acute Supplementation with Cannabidiol Does Not Attenuate Inflammation or Improve Measures of Performance Following Strenuous Exercise. Healthcare 2022, 10, 1133. [CrossRef]
- Burggren, A.C.; Shirazi, A.; Ginder, N.; London, E.D. Cannabis Effects on Brain Structure, Function, and Cognition: Considerations for Medical Uses of Cannabis and Its Derivatives. Am. J. Drug Alcohol Abuse 2019, 45, 563–579. [CrossRef]
- Hill, A.J.; Williams, C.M.; Whalley, B.J.; Stephens, G.J. Phytocannabinoids as Novel Therapeutic Agents in CNS Disorders. Pharmacol. Ther. 2012, 133, 79–97. [CrossRef]
- Booz, G.W. Cannabidiol as an Emergent Therapeutic Strategy for Lessening the Impact of Inflammation on Oxidative Stress. Free Radic. Biol. Med. 2011, 51, 1054–1061. [CrossRef]
- Lorenzetti, V.; Solowij, N.; Yücel, M. The Role of Cannabinoids in Neuroanatomic Alterations in Cannabis Users. Biol. Psychiatry 2016, 79, e17-31. [CrossRef]
- Kramer, A.; Sinclair, J.; Sharpe, L.; Sarris, J. Chronic Cannabis Consumption and Physical Exercise Performance in Healthy Adults: A Systematic Review. J. Cannabis Res. 2020, 2, 34. [CrossRef]
- Singh, J.; Neary, J.P. Neuroprotection Following Concussion: The Potential Role for Cannabidiol. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2020, 47, 289–300. [CrossRef]
- Reillo, M.R. Cannabidiol (CBD) in the Management of Sports-Related Traumatic Brain Injury: Research and Efficacy. Sports Inj. Med. 2019, 3. [CrossRef]
- Fine, P.G.; Rosenfeld, M.J. The Endocannabinoid System, Cannabinoids, and Pain. Rambam Maimonides Med. J. 2013, 4, e0022. [CrossRef]
- Sholler, D.J.; Schoene, L.; Spindle, T.R. Therapeutic Efficacy of Cannabidiol (CBD): A Review of the Evidence from Clinical Trials and Human Laboratory Studies. Curr. Addict. Rep. 2020, 7, 405–412. [CrossRef]
- Lowin, T.; Schneider, M.; Pongratz, G. Joints for Joints: Cannabinoids in the Treatment of Rheumatoid Arthritis. Curr. Opin. Rheumatol. 2019, 31, 271–278. [CrossRef]
- Stanley, C.P.; Hind, W.H.; O’Sullivan, S.E. Is the Cardiovascular System a Therapeutic Target for Cannabidiol? Br. J. Clin. Pharmacol. 2013, 75, 313–322. [CrossRef]
- Bruni, N.; Della Pepa, C.; Oliaro-Bosso, S.; Pessione, E.; Gastaldi, D.; Dosio, F. Cannabinoid Delivery Systems for Pain and Inflammation Treatment. Mol. Basel Switz. 2018, 23, 2478. [CrossRef]
- Zurier, R.B.; Burstein, S.H. Cannabinoids, Inflammation, and Fibrosis. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2016, 30, 3682–3689. [CrossRef]
- Vuolo, F.; Abreu, S.C.; Michels, M.; Xisto, D.G.; Blanco, N.G.; Hallak, J.E.; Zuardi, A.W.; Crippa, J.A.; Reis, C.; Bahl, M.; et al. Cannabidiol Reduces Airway Inflammation and Fibrosis in Experimental Allergic Asthma. Eur. J. Pharmacol. 2019, 843, 251–259. [CrossRef]
- Crippa, J.A.S.; Derenusson, G.N.; Ferrari, T.B.; Wichert-Ana, L.; Duran, F.L.S.; Martin-Santos, R.; Simões, M.V.; Bhattacharyya, S.; Fusar-Poli, P.; Atakan, Z.; et al. Neural Basis of Anxiolytic Effects of Cannabidiol (CBD) in Generalized Social Anxiety Disorder: A Preliminary Report. J. Psychopharmacol. Oxf. Engl. 2011, 25, 121–130. [CrossRef]
- Huestis, M.A.; Mazzoni, I.; Rabin, O. Cannabis in Sport: Anti-Doping Perspective. Sports Med. Auckl. NZ 2011, 41, 949–966. [CrossRef]
- Lattanzi, S.; Brigo, F.; Trinka, E.; Zaccara, G.; Cagnetti, C.; Del Giovane, C.; Silvestrini, M. Efficacy and Safety of Cannabidiol in Epilepsy: A Systematic Review and Meta-Analysis. Drugs 2018, 78, 1791–1804. [CrossRef]
- Ware, M.; Jensen, D.; Barrette, A.; Vernec, A.; Derman, W. Cannabis and the Health and Performance of the Elite Athlete. Clin J Sport Med 2018, 28.
- Armstrong, R.; Warren, G.; Warren, J. Mechanisms of Exercise-Induced Muscle-Fiber Injury. Sports Med. 1991, 12, 184–207. [CrossRef]
- Yeager, M.P.; Pioli, P.A.; Guyre, P.M. Cortisol Exerts Bi-Phasic Regulation of Inflammation in Humans. Dose-Response 2010, 9, 332–347. [CrossRef]
- Gamelin, F.-X.; Cuvelier, G.; Mendes, A.; Aucouturier, J.; Berthoin, S.; Di Marzo, V.; Heyman, E. Cannabidiol in Sport: Ergogenic or Else? Pharmacol. Res. 2020, 156, 104764. [CrossRef]
- Clarkson, P.; Nosaka, K.; Braun, B. Muscle Function After Exercise-Induced Muscle Damage and Rapid Adaptation. Med. Sci. Sports Exerc. 1992, 24, 512–520.
- Hainline, B.; Derman, W.; Vernec, A.; Budgett, R.; Deie, M.; Dvorak, J.; Harle, C.; Herring, S.A.; McNamee, M.; Meeuwisse, W.; et al. International Olympic Committee Consensus Statement on Pain Management in Elite Athletes. Br. J. Sports Med. 2017, 51, 1245–1258. [CrossRef]
- Rudroff, T.; Sosnoff, J. Cannabidiol to Improve Mobility in People with Multiple Sclerosis. Front. Neurol. 2018, 9. [CrossRef]
- Hill, K.P.; Palastro, M.D.; Johnson, B.; Ditre, J.W. Cannabis and Pain: A Clinical Review. Cannabis Cannabinoid Res. 2017, 2, 96–104. [CrossRef]
- Fox, J.L.; Scanlan, A.T.; Stanton, R.; Sargent, C. Insufficient Sleep in Young Athletes? Causes, Consequences, and Potential Treatments. Sports Med. 2020, 50, 461–470. [CrossRef]
- Verma, K.; Singh, D.; Srivastava, A. The Impact of Complementary and Alternative Medicine on Insomnia: A Systematic Review. Cureus 2022, 14, e28425. [CrossRef]
- Murillo-Rodríguez, E.; Budde, H.; Veras, A.B.; Rocha, N.B.; Telles-Correia, D.; Monteiro, D.; Cid, L.; Yamamoto, T.; Machado, S.; Torterolo, P. The Endocannabinoid System May Modulate Sleep Disorders in Aging. Curr. Neuropharmacol. 2020, 18, 97–108. [CrossRef]
Figure 1.
Flowchart of article identification, selection, and exclusion.
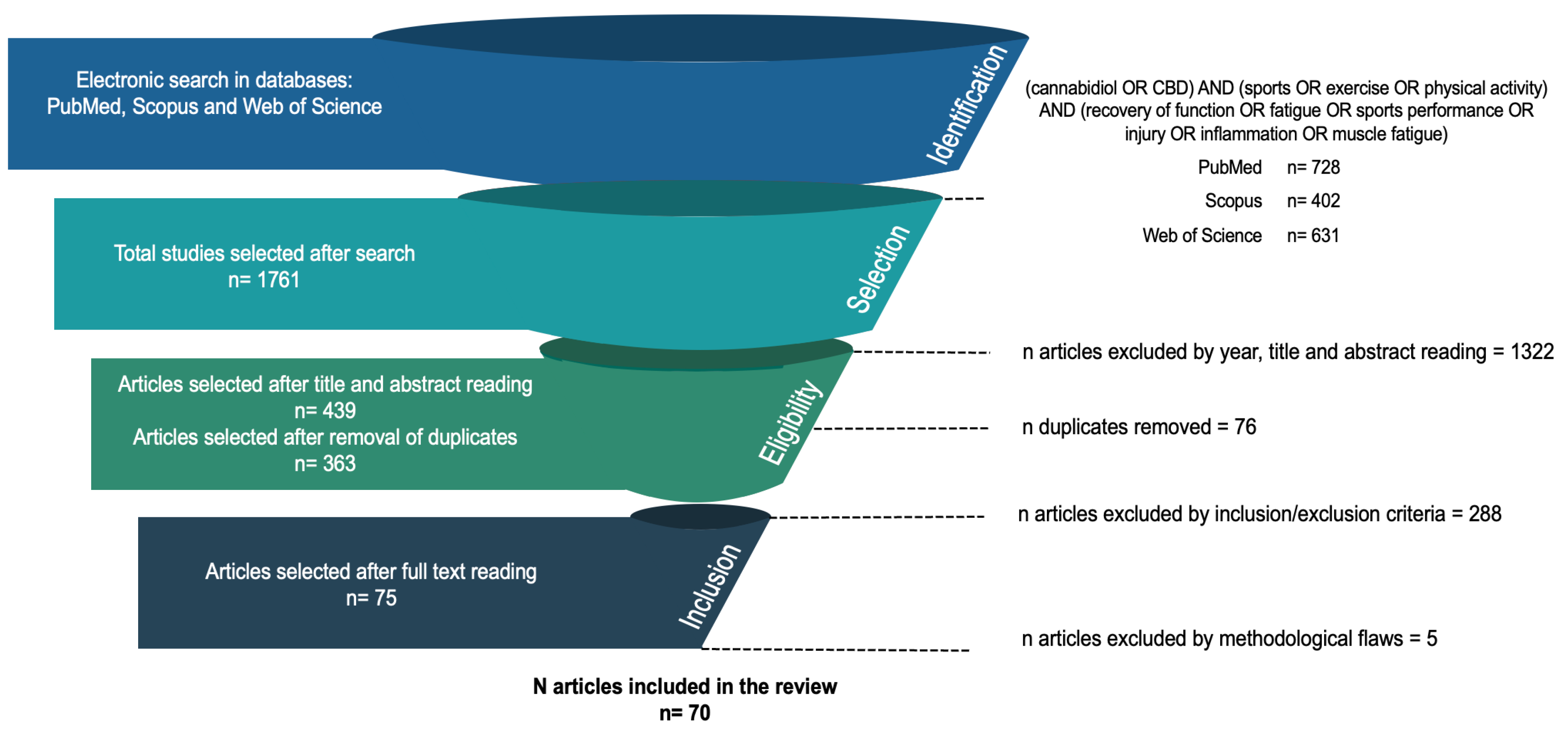
Table 1.
Eligibility criteria.
| PICOS | Inclusion criteria | Exclusion criteria |
| Population | Studies involving humans (e.g. athletes and healthy individuals), as well as animal models (e.g. mice, rats). | Studies that not involve humans or animals. |
| Intervention/ Exposure |
Examining the use of CDB in any formulation (e.g. oral, topical) or dosage as primary intervention. | Not examining the use of CBD as primary intervention. |
| Comparator | Studies with a placebo or control group were included, as well as those without a comparator. | None. |
| Outcomes | Studies reporting outcomes related to sports/exercise recovery, physical performance, and/or physiological effects of CBD (e.g. inflammation, pain, sleep, cognition). | Studies that report only the psychoactive effects of CBD. |
| Study design | Scientific evidence classified as a first and second level were incorporated[38], that Included experimental (randomized trials, non-randomized trials), observational (cohort, case-control), and systematic reviews/meta-analyses. | Studies were non-empirical or lacked sufficient methodological details. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



