
Submitted:
08 May 2024
Posted:
09 May 2024
You are already at the latest version
Abstract
Background: Many clinical conditions are affected by meteorological factors and climate changes. Psychiatric disorders are large contributors to the global disease burden, but the literature on the impact of climate changes on mental health is limited. The aim of this study is to investigate the correlation between rising temperatures and admissions for acute exacerbations of psychiatric disorders.
Methods: Data were collected for summer months of years 2013 to 2022. Mean monthly tempera-tures were obtained from the meteorological station of the Department of Physics of the Universi-ty of Turin. Data on patients admitted to the acute psychiatric unit of San Luigi Gonzaga Univer-sity Hospital (Turin, Italy) were extracted from the hospital registry. Linear regression analyses were used to investigate the correlation between temperature and number of admissions.
Results: A total of 1600 admissions to our psychiatric ward were recorded. Mean monthly temper-ature and monthly number of admissions were directly correlated (P = 0.0020). The correlation between temperature and admissions was significant for the subgroup of admissions due to Bipo-lar Disorders (BD) (P=0.0011), but not for Schizophrenia (P=0.6070) (SCZ) or Major Depressive Disorder (MDD) (P=0.0588).
Conclusions: These results confirm the impact of meteorological factors on mental disorders, and in particular on the course of BD. This provides new insights into etiopathological mechanisms and can contribute to improved follow up and relapse prevention.
Keywords:
Global warming
; Temperature
; Mental health
; Major depressive disorder
; Bipolar disorder
; Schizophrenia
1. Introduction
In recent years, global climate has been facing drastic changes, largely induced by human activities. New peaks of global temperature have been reached in recent years, and scientists predict a progressive and unavoidable worsening in the years to come [1]. Last year has been the warmest solar year on record [2], and the 6th July 2023 has been the warmest day ever recorded, with a global average of 17.08°C [3]. Anthropogenic climate change is making extreme climatic events such as heat waves, floods and draughts more common [4,5], and is altering seasonal patterns [6].
The impact of temperature and hence of climate change on morbidity has been studied for over a decade, with a clear focus on cardiovascular disease, endocrine and metabolic disorders, and other conditions related to physical health and infective disorders [7]. Seasonal patterns have been observed in the gut microbiota of patients living with inflammatory bowel diseases [8] as well as in symptoms of multiple sclerosis [9], and temperature extremes have been associated with mortality due to respiratory disorders [10]. Many authors have specifically highlighted the impact of human-driven climate changes on morbidity. Available data suggest that rising temperatures lead to increased cardiovascular mortality through increased blood pressure and viscosity, increased heart rate, and endothelial damage [11]. Extreme weather events have been shown to increase morbidity and mortality in patients living with diabetes [12]. The impact of pollution, greenhouse gases and climatic changes on reproductive health has also been explored, with reports showing damaging effects of climate change on fertility and pregnancy outcomes [13].
Mental disorders are among the leading causes of disease burden worldwide, and their impact in terms of prevalence and disability has been increasing in the last 30 years [14], but little attention has been paid on the effects of climate change on mental health. Psychiatric conditions can lead to suicidal ideation and self-harm [15], as well as psychomotor agitation [16], which often lead to presentation to emergency departments and admission, whose rates are also increasing [17].
There is a tight interconnection between mental health and climate, specifically in terms of season cycles, light exposure and temperature. Many authors have reported seasonal patterns in the course of psychiatric disorders, with rises in admissions, involuntary admissions and suicidal ideation in spring/summer [18]. Some reports have also suggested that different diagnostic groups face peaks in admissions in different times of the year, with exacerbations of Bipolar Disorder (BD) in summer, Schizophrenia (SCZ) in winter and Major Depressive Disorder (MDD) in early winter [19,20]. Nevertheless, available data support the notion that seasonal patterns are particularly characteristic of bipolar spectrum disorders [21]. Also light-dark cycles are of high relevance for mental health conditions, especially for mood disorders. Data suggest that photoperiod and sunlight exposure are directly correlated with the rate of admission for manic or hypomanic episodes [22,23]. Daylight exposure also influences sleep patterns, which play a crucial role in mental disorders. Sleep disruption is a symptom of many psychiatric conditions, and modulation of light exposure and sleep has therapeutic applications [24]. Bright light therapy and sleep deprivation therapy, indeed, have proven efficacy in seasonal affective disorder [25], as well as in unipolar and bipolar depression and act through normalisation of sleep patterns as well as a plethora of biological mechanisms at the cellular level [26,27,28]. Literature concerning the relationship between temperature and mental health is also present, but results are not univocal. Few papers have described direct correlations of maximum and mean ambient temperatures with emergency presentations for psychiatric disorders [23,29], with involuntary admissions [30] and even with mortality in psychiatric patients [31]. On the other hand, some authors found small or non-significant impact of meteorological patterns on admission rates [32,33,34]. In a recent review, authors gathered data on the association between admissions for schizophrenia and temperature. Despite most of the included studies reported an association between higher temperature and admission rates for schizophrenia, studies are heterogeneous and often contradicting, and further research in the matter has been advocated [35].
Despite the burden of psychiatric disorders, their known interconnection with environmental and climatic factors, and gaps in the understanding of the mechanisms underlying such interconnection, research on the impact of climatic changes on mental health is scarce and its generalizability is hindered by geographical factors. Air pollution, high temperatures, draughts and extreme precipitation events have been associated to an increased suicide risk [36], and one large American study on nearly 2 million observations suggested an impact of multi-yearly rises in temperatures on mental health issues. Nevertheless, the results of the latter study were drawn from data that are more than 10 years-old now, and authors could not differentiate acute from chronic mental issues, nor could identify the impact of climatic changes on different diagnostic groups [37]. In 2018, a systematic review identified 35 studies assessing the impact of temperature on mental health outcomes, but only 2 were conducted in Mediterranean Europe, and none investigated the effects of the rise in temperature observed in the last decades [38]. Therefore, further research efforts are necessary to confirm the putative impact of global warming on mental health.
The aim of this study is to contribute to the body of literature concerning the effects of climate change on psychiatric disorders. We intend to do this by analysing the correlation between mean monthly temperatures and admissions to our acute psychiatric inpatient unit during summer months over a 10-year period.
2. Materials and Methods
Study Design
The present study is a descriptive, cross-sectional study. Data on mean monthly temperatures and on admissions to our clinic were collected retrospectively for summer months of 10 years. The study included data from all patients admitted during the observation period to the acute psychiatric unit of San Luigi Gonzaga University Hospital in Orbassano, Turin, Italy. The total observation period was of 40 months, i.e. the months from June to September of years 2013 to 2022.
Data Extraction
Temperature: Data on daily temperatures for the observation period were downloaded from online registries of measurements from the meteorological station of the Department of Physics of the University of Turin. Mean monthly temperatures were computed for statistical analyses.
Admissions: Anonymised data regarding socio-demographic (i.e. age and gender) and clinical (i.e. main diagnosis at discharge, date, duration and compulsoriness of admission) characteristics were extracted from hospital registries. Diagnoses at discharge in our hospital registry are encoded according to ICD-9 classification. For the present study diagnoses were divided into four mutually exclusive groups: Schizophrenia and related disorders; Bipolar and related disorders; Major Depressive disorder; other. “Other” diagnoses included personality disorders, obsessive-compulsive disorder, substance use disorder, eating disorders and neurocognitive disorders. For the analyses, the total number of admissions and the number of admissions for each diagnostic group were computed for each month.
Statistical Analyses
All statistical analyses were carried out on GraphPad Prism 8. The value of statistical significance was set at p <0.05. Shapiro-Wilk test was used to test normality of distribution for continuous variables. Independent T test was used to compare means of independent measures between two groups. One-way ANOVA was used when comparing means between more than two groups. For the analysis of correlation between two continuous variables (e.g. temperature and number of admissions) we performed linear regression analyses and computed Pearson correlation coefficients (R2).
3. Results
3.1. Sample Characteristics and DESCRIPTIVE statistics
A total of 1600 admissions to our psychiatric ward were recorded over the observation period. The mean number of admissions per month was 40 (±9.89). The mean (±Standard Deviation (SD)) age of the sample was 45.74 (±15.51) years; 722 of patients (45.13%) were females; the mean duration of hospitalization was 9.99 (±8.95) days; the rate of involuntary admission was 7.38% (N = 118).
Concerning the main diagnosis, 556 (34.75%) patients had Bipolar and related disorders, 325 (20.31%) had Schizophrenia and related disorders, 231 (14.44%) had Major Depressive Disorders and 488 (30.50%) had other diagnoses. (Table 1) The mean temperature throughout the observation period was 22.24°C (±2.34). Figure 1 shows the trend in mean summer temperature (left Y axis) and in total number of admissions for each summer (right Y axis). (Figure 1)
3.2. Total Number of Admissions According to Month
3.3. Temperature and Number of Admissions
We performed linear regression analysis setting mean monthly temperature as the independent variable and monthly number of admissions as the dependent variable. The regression coefficient was 1.998 (95% Confidence Interval (CI) 0.7785 to 3.218, P = 0.0020), and Pearson correlation coefficient (R2) was 0.2245. (Figure 3)
3.4. Temperature and Number of Admissions According to Diagnosis
Linear regression analysis was performed between mean monthly temperature and number of admissions according to each diagnostic group. The regression coefficient was 0.1231 (95% CI -0.3576 to 0.6039, P = 0.6070) for admissions of patients with schizophrenia and related disorders, 1.410 (95% CI 0.6052 to 2.215, P = 0.0011, R2 = 0.2487) for bipolar related disorders, 0.3033 (95% CI -0.01183 to 0.6184, P = 0.0588) for major depressive disorder. (Figure 4)
3.5. Temperature and Involuntary Admissions
No significant correlation was found performing linear regression analysis between temperature and monthly number of involuntary admission (Y = -0.01314*X + 3.242;P = 0.9284; R2 = 0.0002151). (Figure 5A)
3.6. Temperature and Length of Stay
No significant correlation was found performing linear regression analysis between mean monthly temperature and length of hospitalisation (Y = -0.06038*X + 11.62; P = 0.6739; R2 = 0.004709). (Figure 5B)
4. Discussion
In recent years, anthropogenic climate changes have become increasingly evident. Extreme climatic events such as heavy precipitations, floods, prolonged draughts and heat waves are becoming more common [4], and global temperatures are rising [2]. The impact of rising temperatures and adverse meteorological events on health is also increasingly considered [7,39]. Despite the available knowledge on the interconnection between mental health and climatic conditions [20,32,40], few authors have investigated the impact of climatic changes on psychiatric disorders. Indeed our comprehension of this impact is hampered by paucity of data, contradictory results and poor generalizability due to limited geographical diffusion of these investigations [38].
To our knowledge this is the first study explicitly examining the impact of rising temperatures on mental health outcomes in Mediterranean Europe throughout a long period of observation. A recent systematic review on 35 studies [38] identified 2 previous analyses of the correlation between temperature and admissions in Spain, but they either focused on admissions for dementia [41], or they considered a short time span [42]. In both cases, analyses were conducted on data that are now older than 15 years, and the rising trend in temperatures was not taken into consideration.
The present study investigated the correlation between mean monthly temperatures in summer months and admissions to our acute psychiatric unit in Turin, Italy. Our data show an oscillating but overall increasing trend in mean summer temperatures in Turin throughout the observation period, paralleled by the trend in admissions to our inpatient unit. A relevant background consideration is that this suggests that the variations in the number of admissions are not merely due to a secular drift, which might be explained by confounding factors such as overall increased prevalence of psychiatric conditions or increased efficiency in inpatient turnover. Moreover, the similarity in the evolution of summer temperature and summer admissions, together with the non-significant difference in total number of admissions for each month of any year, suggests that the observed correlations are not due to the potential confounding effect of seasonal patterns of psychiatric disorders. Our analyses yielded a significant correlation between the mean monthly temperature and the number of admissions to our psychiatric inpatient unit. This is in line with previous reports [29], and highlights the importance of considering mental health outcomes when discussing the adverse effects of global warming. Contrary to what Jahan and colleagues reported [35], we found no association between temperature and admissions when looking into the sample of patients with SCZ. It has to be noted that Jahan and colleagues stressed the heterogeneity of results on the matter, and suggested themselves further research in order to confirm or dismiss the notion that the course of SCZ is influenced by temperature. On the other hand, our results confirmed the impact of temperature on the course of BD, as suggested by other pieces of literature [23], but not of MDD. Peaks in depressive episodes have been associated, in previous reports, to winter seasons [19] and, therefore, are likely to be less influenced by high ambient temperature.
In our opinion, implications of the presented results stretch beyond epidemiological considerations. The relationship between increasing temperature and rising number of admissions might shed a light on pathophysiological mechanisms contributing to onset or exacerbation of major psychiatric disorders and in particular BD. Exposure to high temperatures leads to protein misfolding and induction of heat-shock proteins through heat shock factors [39], which can induce changes in protein expression and potentially activate pro-inflammatory processes. Moreover, heat per se can induce accumulation of reactive oxygen species and, most of all, alterations in blood brain barrier permeability [39]. Inflammation [43], oxidative stress [44], and blood brain barrier leakiness [45] have all been extensively associated with BD etiopathogenesis and course.
Understanding the relationship between temperature and exacerbations of BD can also inform patient monitoring. The disease course of BD is influenced by a number of circadian cycles such as melatonin peaks, cortisol levels, body temperature, sleep-wake alternation and chronotype [40]. It is undoubtedly relevant to know a patient sleep habits, and to consider exposure to melatonin or cortisol in order to adequately approach a clinical picture. Similarly, if the negative impact of rising temperatures on BD is confirmed, this should be taken into account when managing an exacerbation of the disorder. Knowledge of underlying mechanisms can allow correct interpretation of patient’s history and most of all can facilitate accurate follow up. As public health resources are lacking in many areas of the globe, and those assigned to mental health are consistently inferior to the demand [46], finding ways to make resource allocation more efficient is becoming increasingly crucial. The possibility to reasonably predict which patients are more likely to experience a disease recrudescence depending on season and temperature trend can, therefore, become a precious asset for psychiatrists.
The results presented and the discussed implications have to be pondered in light of the limitations of our study. The observational cross-sectional design of our study limits the inference of causal relationships between the exposure (i.e. higher temperatures) and the putative effect (i.e. admissions). Nevertheless, studies on weather variables, especially those considering historical measurements on long periods of time, can only be observational in design. Our observation period was limited to summer months, while taking into consideration the whole year might be more explicative of the true effect of temperature on psychiatric presentations. We decided to only consider summer months in order to minimise the potential confounding effect of seasonality, and because the effects of global warming are more evident in summer months [2]. We opted for a monthly resolution of our measurements, which limited our data points to 40. While this allows to observe the effects of the exposure even if lagged in time, narrower time windows (e.g. weekly) might help to improve significance and validity of results. Our data on admissions suffer from a ceiling effect imposed by the maximum number of beds in our inpatient unit. The number of presentations to the emergency departments for psychiatric complaints would represent a more sensible parameter and would work around the ceiling bias. On the other hand, admissions were preferred for this study in order to increase specificity for severe exacerbations of psychiatric disorders, i.e. those that require admission.
5. Conclusions
This paper describes a direct correlation between mean monthly temperature in summer and number of admissions to an acute psychiatric inpatient unit in Italy. If corroborated by other studies, this notion would be of utmost relevance in view of the human-induced climate changes that we have been observing, and could contribute to further understanding of pathophysiological mechanisms, to more accurate follow up and to improvements in relapse prevention.
Author Contributions
Conceptualization, Nicola Rizzo Pesci, Giuseppe Maina and Gianluca Rosso; Formal analysis, Nicola Rizzo Pesci and Elena Teobaldi; Investigation, Nicola Rizzo Pesci and Elena Teobaldi; Methodology, Nicola Rizzo Pesci, Giuseppe Maina and Gianluca Rosso; Supervision, Gianluca Rosso; Writing – original draft, Nicola Rizzo Pesci; Writing – review & editing, Elena Teobaldi, Giuseppe Maina and Gianluca Rosso. All authors will be informed about each step of manuscript processing including submission, revision, revision reminder, etc. via emails from our system or assigned Assistant Editor.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2013.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting the findings of the present study are available upon request.
Conflicts of Interest
The authors have no competing interests to disclose that are relevant for this article.
References
- Baronetti A, Dubreuil V, Provenzale A, Fratianni S. Future droughts in northern Italy: high-resolution projections using EURO-CORDEX and MED-CORDEX ensembles. Clim Change [Internet]. 2022 [cited 2024 Feb 22];172(22). [CrossRef]
- Global Climate Highlights 2023 | Copernicus [Internet]. [cited 2024 Feb 22]. Available from: https://climate.copernicus.eu/global-climate-highlights-2023.
- July 2023 is set to be the hottest month on record. 2023.
- Alifu H, Hirabayashi Y, Imada Y, Shiogama H. Enhancement of river flooding due to global warming. Sci Rep [Internet]. 2022 [cited 2024 Feb 22];12:20687. [CrossRef]
- Christidis N, Mitchell D, Stott PA. Rapidly increasing likelihood of exceeding 50 °C in parts of the Mediterranean and the Middle East due to human influence. npj Clim Atmos Sci [Internet]. 2023 [cited 2024 Feb 22];6(45). [CrossRef]
- Hajek OL, Knapp AK. Shifting seasonal patterns of water availability: ecosystem responses to an unappreciated dimension of climate change. New Phytol. 2022 Jan 1;233(1):119–25. [CrossRef]
- Ye X, Wolff R, Yu W, Vaneckova P, Pan X, Tong S. Ambient Temperature and Morbidity: A Review of Epidemiological Evidence. Environ Health Perspect [Internet]. 2012 [cited 2024 Feb 19];120(1):19. Available from: /pmc/articles/PMC3261930/. [CrossRef]
- Tani M, Shinzaki S, Asakura A, Tashiro T, Amano T, Otake-Kasamoto Y, et al. Seasonal variations in gut microbiota and disease course in patients with inflammatory bowel disease. PLoS One [Internet]. 2023 Apr 1 [cited 2024 Feb 23];18(4):e0283880. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0283880.
- Celius EG, Grothe M, Gross S, Süße M, Strauss S, Penner IK. The Seasonal Fluctuation of Fatigue in Multiple Sclerosis. Front Neurol | www.frontiersin.org [Internet]. 2022 [cited 2024 Feb 23];1:900792. Available from: www.frontiersin.org.
- Jahan S, Cauchi JP, Galdies C, England K, Wraith D. The adverse effect of ambient temperature on respiratory deaths in a high population density area: the case of Malta. Respir Res [Internet]. 2020 [cited 2024 Feb 23];23:299. [CrossRef]
- Gostimirovic M, Novakovic R, Rajkovic J, Djokic V, Terzic D, Putnik S, et al. The influence of climate change on human cardiovascular function. Arch Environ Occup Health. 2020 Oct 2;75(7):406–14.
- Zilbermint M. Diabetes and climate change. J Community Hosp Intern Med Perspect [Internet]. 2020 Sep 2 [cited 2024 Feb 26];10(5):409. Available from: /pmc/articles/PMC7671730/.
- Segal TR, Giudice LC. Systematic review of climate change effects on reproductive health. Fertil Steril [Internet]. 2022 Aug 1 [cited 2024 Feb 23];118(2):215–23. Available from: http://www.fertstert.org/article/S0015028222003831/fulltext.
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet Psychiatry. 2022 Feb 1;9(2):137–50. [CrossRef]
- Barratt H, Rojas-García A, Clarke K, Moore A, Whittington C, Stockton S, et al. Epidemiology of Mental Health Attendances at Emergency Departments: Systematic Review and Meta-Analysis. PLoS One [Internet]. 2016 Apr 1 [cited 2024 Feb 22];11(4). Available from: https://pubmed-ncbi-nlm-nih-gov.bibliopass.unito.it/27120350/.
- Sacchetti E, Valsecchi P, Tamussi E, Paulli L, Morigi R, Vita A. Psychomotor agitation in subjects hospitalized for an acute exacerbation of Schizophrenia. Psychiatry Res. 2018 Dec 1;270:357–64. [CrossRef]
- Weiss AJ, Barrett ML, Heslin KC, Stocks C. Trends in Emergency Department Visits Involving Mental and Substance Use Disorders, 2006–2013. Healthc Cost Util Proj Stat Briefs [Internet]. 2016 [cited 2024 Feb 22]; Available from: https://www-ncbi-nlm-nih-gov.bibliopass.unito.it/books/NBK409512/.
- Aguglia A, Moncalvo M, Solia F, Maina G. Involuntary admissions in Italy: the impact of seasonality. Int J Psychiatry Clin Pract [Internet]. 2017 Oct 1 [cited 2024 Feb 19];20(4):232–8. Available from: https://iris.unito.it/handle/2318/1634552.
- Asimakopoulos LO, Koureta A, Benetou V, Lagiou P, Samoli E. Investigating the association between temperature and hospital admissions for major psychiatric diseases: A study in Greece. J Psychiatr Res. 2021 Dec 1;144:278–84. [CrossRef]
- Lee HC, Tsai SY, Lin HC. Seasonal variations in bipolar disorder admissions and the association with climate: A population-based study. J Affect Disord. 2007 Jan 1;97(1–3):61–9. [CrossRef]
- Aguglia A, Cuomo A, Amerio A, Bolognesi S, Di Salvo G, Fusar-Poli L, et al. A new approach for seasonal pattern: is it related to bipolarity dimension? Findings from an Italian multicenter study. Int J Psychiatry Clin Pract [Internet]. 2021 [cited 2024 Feb 23];25(1):73–81. Available from: https://www-tandfonline-com.bibliopass.unito.it/doi/abs/10.1080/13651501.2020.1862235.
- Aguglia A, Borsotti A, Maina G. Bipolar disorders: is there an influence of seasonality or photoperiod? Brazilian J Psychiatry [Internet]. 2018 Jan 1 [cited 2024 Feb 19];40(1):6. Available from: /pmc/articles/PMC6899423/.
- Aguglia A, Serafini G, Escelsior A, Canepa G, Amore M, Maina G. Maximum Temperature and Solar Radiation as Predictors of Bipolar Patient Admission in an Emergency Psychiatric Ward. Int J Environ Res Public Heal 2019, Vol 16, Page 1140 [Internet]. 2019 Mar 29 [cited 2024 Feb 19];16(7):1140. Available from: https://www.mdpi.com/1660-4601/16/7/1140/htm.
- Suzuki M, Dallaspezia S, Locatelli C, Uchiyama M, Colombo C, Benedetti F. Does early response predict subsequent remission in bipolar depression treated with repeated sleep deprivation combined with light therapy and lithium? J Affect Disord. 2018 Mar 15;229:371–6. [CrossRef]
- Pjrek E, Friedrich ME, Cambioli L, Dold M, Jäger F, Komorowski A, et al. The Efficacy of Light Therapy in the Treatment of Seasonal Affective Disorder: A Meta-Analysis of Randomized Controlled Trials. Psychother Psychosom [Internet]. 2020 Jan 14 [cited 2024 Feb 23];89(1):17–24. [CrossRef]
- Sarzetto A, Cavallini MC, Fregna L, Pacchioni F, Attanasio F, Barbini B, et al. Sleep architecture modifications after double chronotherapy: A case series of bipolar depressed inpatients. Psychiatry Res. 2022 Oct 1;316:114781. [CrossRef]
- Benedetti F, Dallaspezia S, Melloni EMT, Lorenzi C, Zanardi R, Barbini B, et al. Effective Antidepressant Chronotherapeutics (Sleep Deprivation and Light Therapy) Normalize the IL-1β:IL-1ra Ratio in Bipolar Depression. Front Physiol [Internet]. 2021 Sep 1 [cited 2024 Feb 19];12:740686. Available from: www.frontiersin.org.
- Fountoulakis KN, Yatham LN, Grunze H, Vieta E, Young AH, Blier P, et al. The CINP Guidelines on the Definition and Evidence-Based Interventions for Treatment-Resistant Bipolar Disorder. Int J Neuropsychopharmacol [Internet]. 2020 [cited 2024 Feb 23];23(4):230–56. Available from: https://academic.oup.com/ijnp/article/23/4/230/5658435.
- Niu L, Girma B, Liu B, Schinasi LH, Clougherty JE, Sheffield P. Temperature and mental health–related emergency department and hospital encounters among children, adolescents and young adults. Epidemiol Psychiatr Sci [Internet]. 2023 Apr 17 [cited 2024 Feb 19];32. Available from: /pmc/articles/PMC10130844/.
- Aguglia A, Serafini G, Escelsior A, Amore M, Maina G. What is the role of meteorological variables on involuntary admission in psychiatric ward? An Italian cross-sectional study. Environ Res. 2020 Jan 1;180:108800. [CrossRef]
- Page LA, Hajat S, Sari Kovats R, Howard LM. Temperature-related deaths in people with psychosis, dementia and substance misuse. Br J Psychiatry [Internet]. 2012 Jun [cited 2024 Feb 19];200(6):485–90. Available from: https://www-cambridge-org.bibliopass.unito.it/core/journals/the-british-journal-of-psychiatry/article/temperaturerelated-deaths-in-people-with-psychosis-dementia-and-substance-misuse/77BB0669DFD55C4A717B25DFA0E6EAAC.
- McWilliams S, Kinsella A, O’Callaghan E. The effects of daily weather variables on psychosis admissions to psychiatric hospitals. Int J Biometeorol [Internet]. 2013 Jul 2 [cited 2024 Feb 19];57(4):497–508. Available from: https://link-springer-com.bibliopass.unito.it/article/10.1007/s00484-012-0575-1.
- Tupinier Martin F, Boudreault J, Campagna C, Lavigne É, Gamache P, Tandonnet M, et al. The relationship between hot temperatures and hospital admissions for psychosis in adults diagnosed with schizophrenia: A case-crossover study in Quebec, Canada. Environ Res [Internet]. 2024 Apr 1 [cited 2024 Feb 19];246:118225. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0013935124001294.
- Qiu X, Wei Y, Weisskopf M, Spiro A, Shi L, Castro E, et al. Air pollution, climate conditions and risk of hospital admissions for psychotic disorders in U.S. residents. Environ Res. 2023 Jan 1;216:114636. [CrossRef]
- Jahan S, Wraith D, Dunne MP, Naish S, McLean D. Seasonality and schizophrenia: a comprehensive overview of the seasonal pattern of hospital admissions and potential drivers. Int J Biometeorol [Internet]. 2020 Aug 1 [cited 2024 Feb 23];64(8):1423–32. [CrossRef]
- Dumont C, Haase E, Dolber T, Lewis J, Coverdale J. Climate Change and Risk of Completed Suicide. J Nerv Ment Dis [Internet]. 2020 Jul 1 [cited 2024 Feb 23];208(7):559–65. Available from: https://journals.lww.com/jonmd/fulltext/2020/07000/climate_change_and_risk_of_completed_suicide.6.aspx.
- Obradovich N, Migliorini R, Paulus MP, Rahwan I. Empirical evidence of mental health risks posed by climate change. Proc Natl Acad Sci U S A [Internet]. 2018 Oct 23 [cited 2024 Feb 26];115(43):10953–8. Available from: /pmc/articles/PMC6205461/.
- Thompson R, Hornigold R, Page L, Waite T. Associations between high ambient temperatures and heat waves with mental health outcomes: a systematic review. Public Health. 2018 Aug 1;161:171–91. [CrossRef]
- Oosthuizen J, Hime NJ, Bi P, Mathieson A, Natur S, Damri O, et al. The Effect of Global Warming on Complex Disorders (Mental Disorders, Primary Hypertension, and Type 2 Diabetes). 2022 [cited 2024 Feb 23]. [CrossRef]
- Abreu T, Bragança M. The bipolarity of light and dark: A review on Bipolar Disorder and circadian cycles. J Affect Disord. 2015 Oct 1;185:219–29. [CrossRef]
- Linares C, Culqui D, Carmona R, Ortiz C, Díaz J. Short-term association between environmental factors and hospital admissions due to dementia in Madrid. Environ Res. 2017 Jan 1;152:214–20. [CrossRef]
- García FM, Boada SS i, Collsamata AX, Joaquim IG, Pérez YA, Tricio OG, et al. Meteorological factors and psychiatric emergencies. Actas Españolas Psiquiatr [Internet]. 2009 Jan 1 [cited 2024 Apr 7];37(1):34–41. Available from: https://actaspsiquiatria.es/index.php/actas/article/view/822.
- Saccaro LF, Crokaert J, Perroud N, Piguet C. Structural and functional MRI correlates of inflammation in bipolar disorder: A systematic review. J Affect Disord. 2023 Mar 15;325:83–92. [CrossRef]
- Valvassori SS, Bavaresco D V., Feier G, Cechinel-Recco K, Steckert A V., Varela RB, et al. Increased oxidative stress in the mitochondria isolated from lymphocytes of bipolar disorder patients during depressive episodes. Psychiatry Res. 2018 Jun 1;264:192–201. [CrossRef]
- Kamintsky L, Cairns KA, Veksler R, Bowen C, Beyea SD, Friedman A, et al. Blood-brain barrier imaging as a potential biomarker for bipolar disorder progression. NeuroImage Clin. 2020 Jan 1;26:102049. [CrossRef]
- McAllister MS, Olagunju AT. Revisiting the unmet mental health needs in Canada: Can PAs be part of the solution? J Am Acad Physician Assist [Internet]. 2023 Dec 1 [cited 2024 Feb 27];36(12):42–5. Available from: https://journals.lww.com/jaapa/fulltext/2023/12000/revisiting_the_unmet_mental_health_needs_in.11.aspx.
Figure 1.
Trends in mean summer temperatures and total number of admissions per summer.
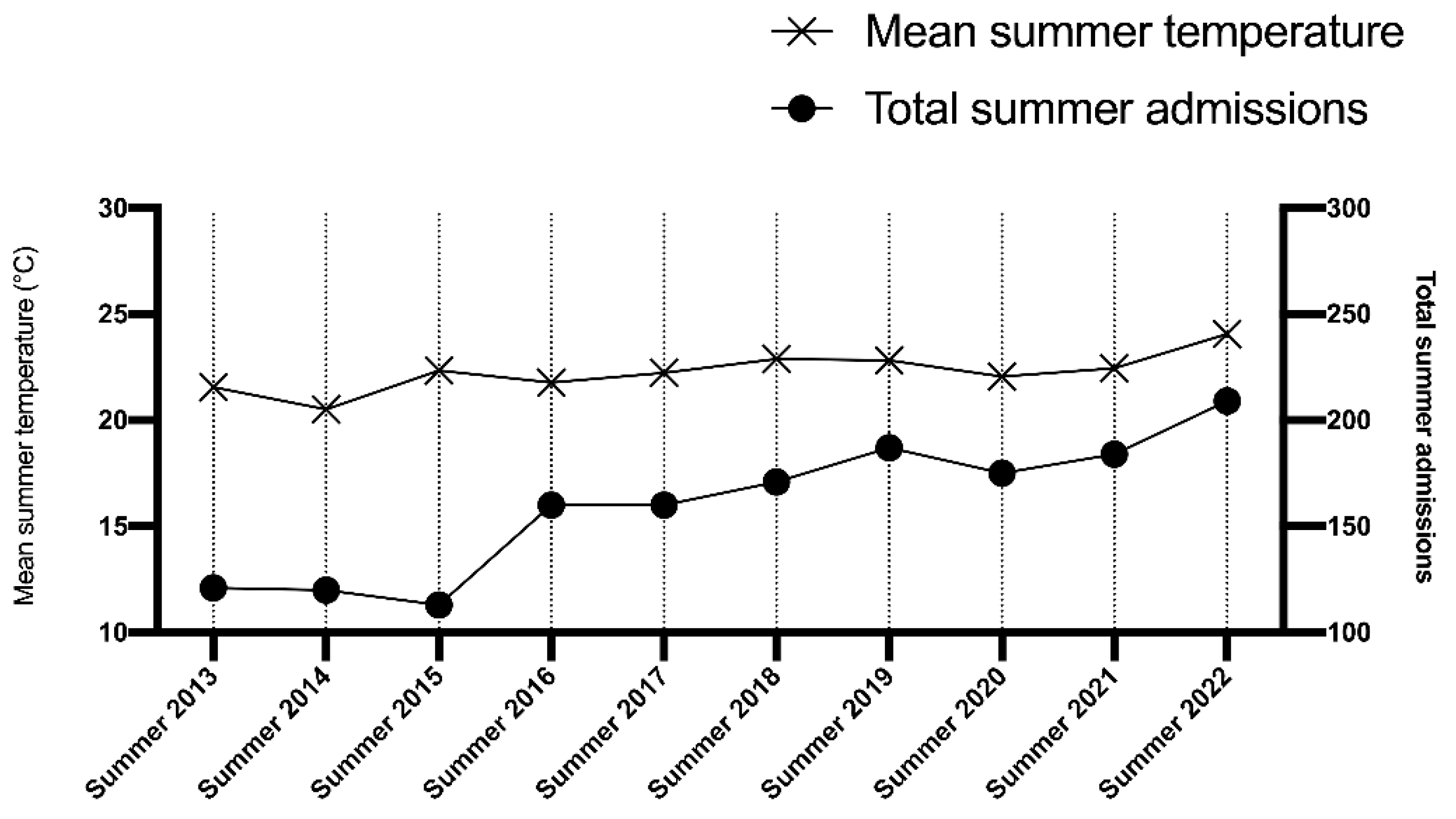
Figure 2.
Comparison of total number of admissions for each month of any year.
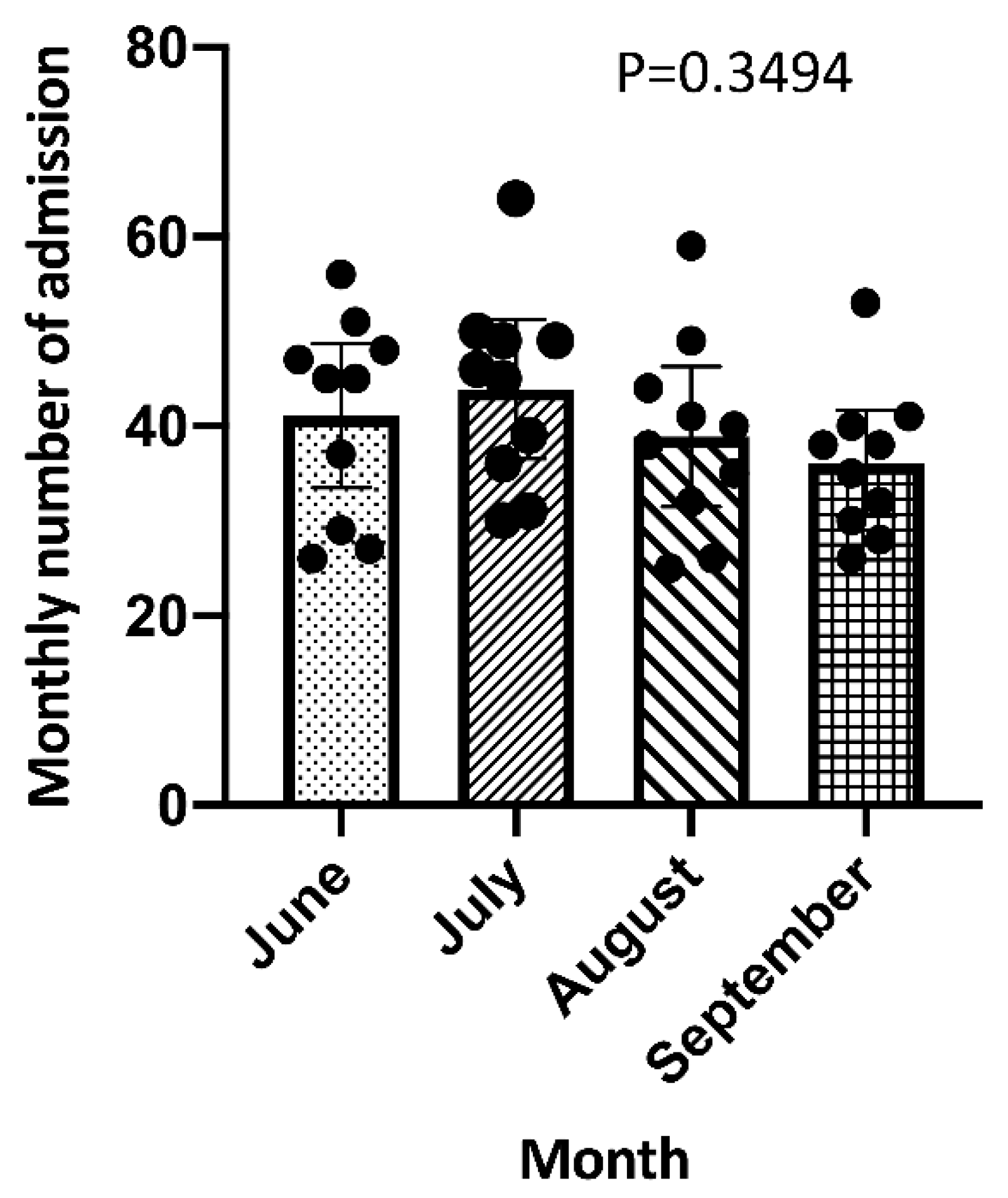
Figure 3.
Linear regression analysis between mean monthly temperature and monthly number of admissions.
Figure 3.
Linear regression analysis between mean monthly temperature and monthly number of admissions.
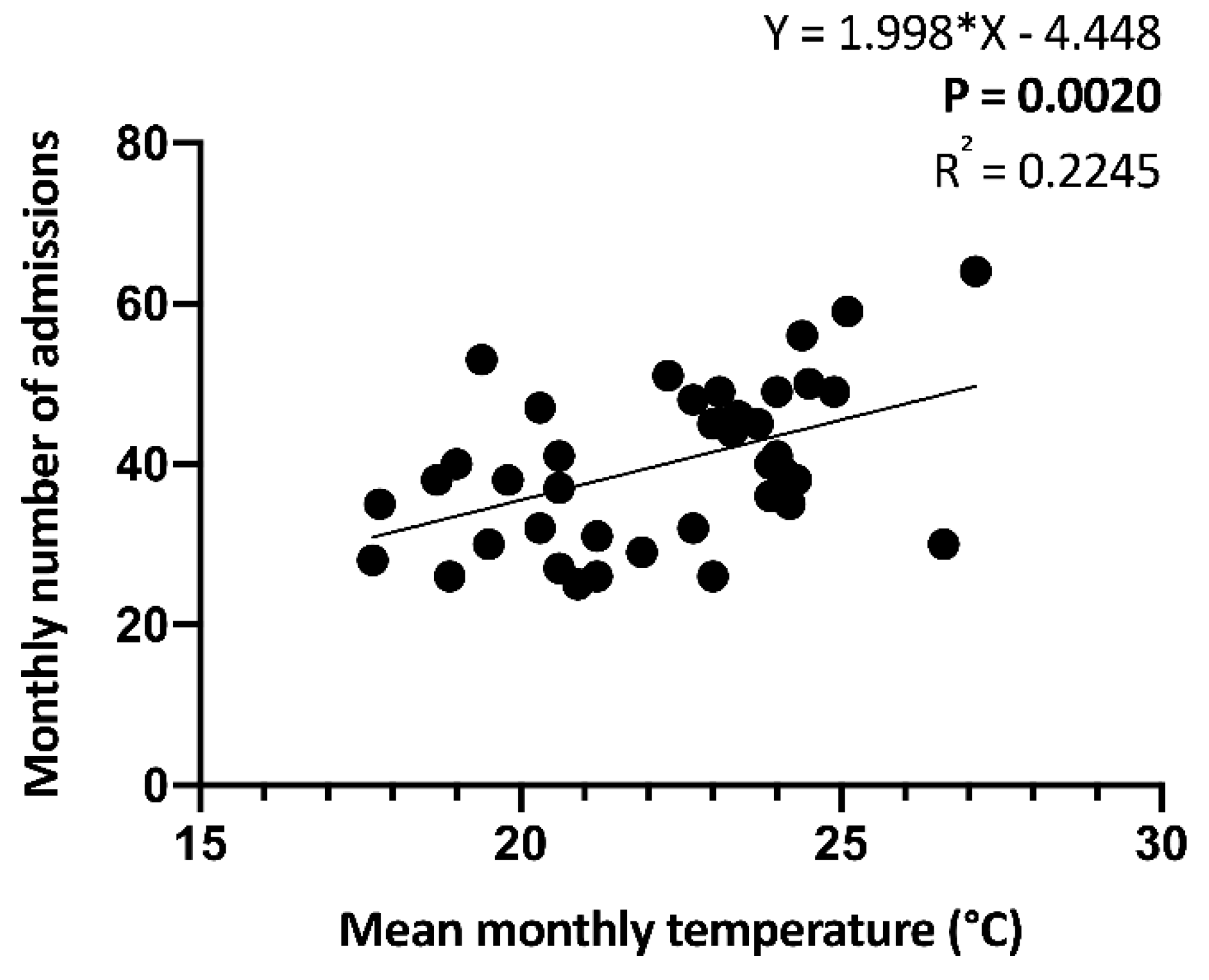
Figure 4.
Linear regression analyses between mean monthly temperature and monthly number of admissions for Schizophrenia (A), Bipolar Disorder (B) and Major Depressive Disorder (C).
Figure 4.
Linear regression analyses between mean monthly temperature and monthly number of admissions for Schizophrenia (A), Bipolar Disorder (B) and Major Depressive Disorder (C).
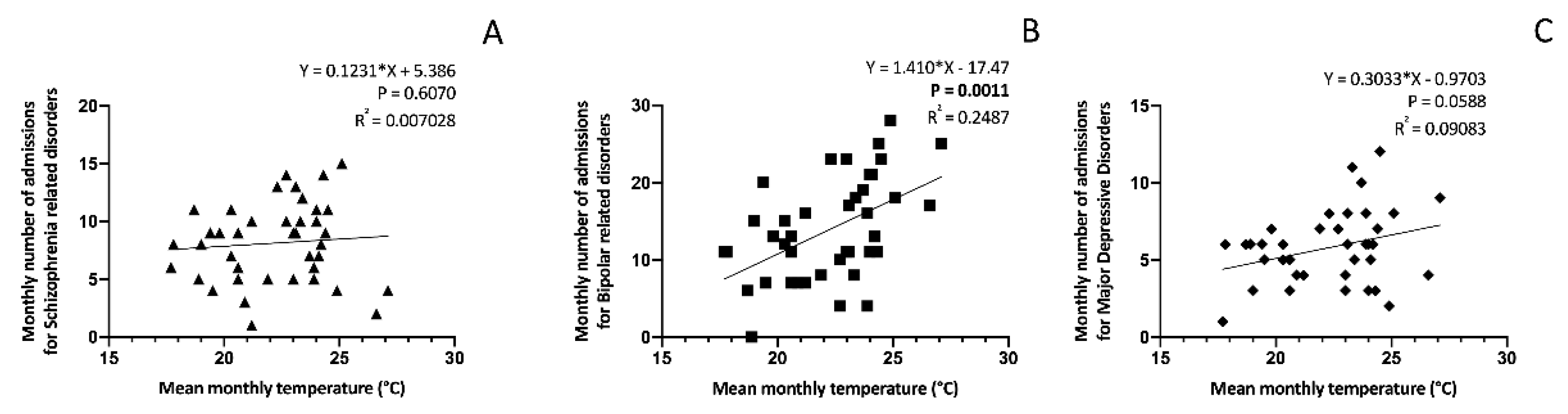
Figure 5.
Linear regression analysis between mean monthly temperature and monthly number of involuntary admissions (A) and mean duration of admission (B).
Figure 5.
Linear regression analysis between mean monthly temperature and monthly number of involuntary admissions (A) and mean duration of admission (B).
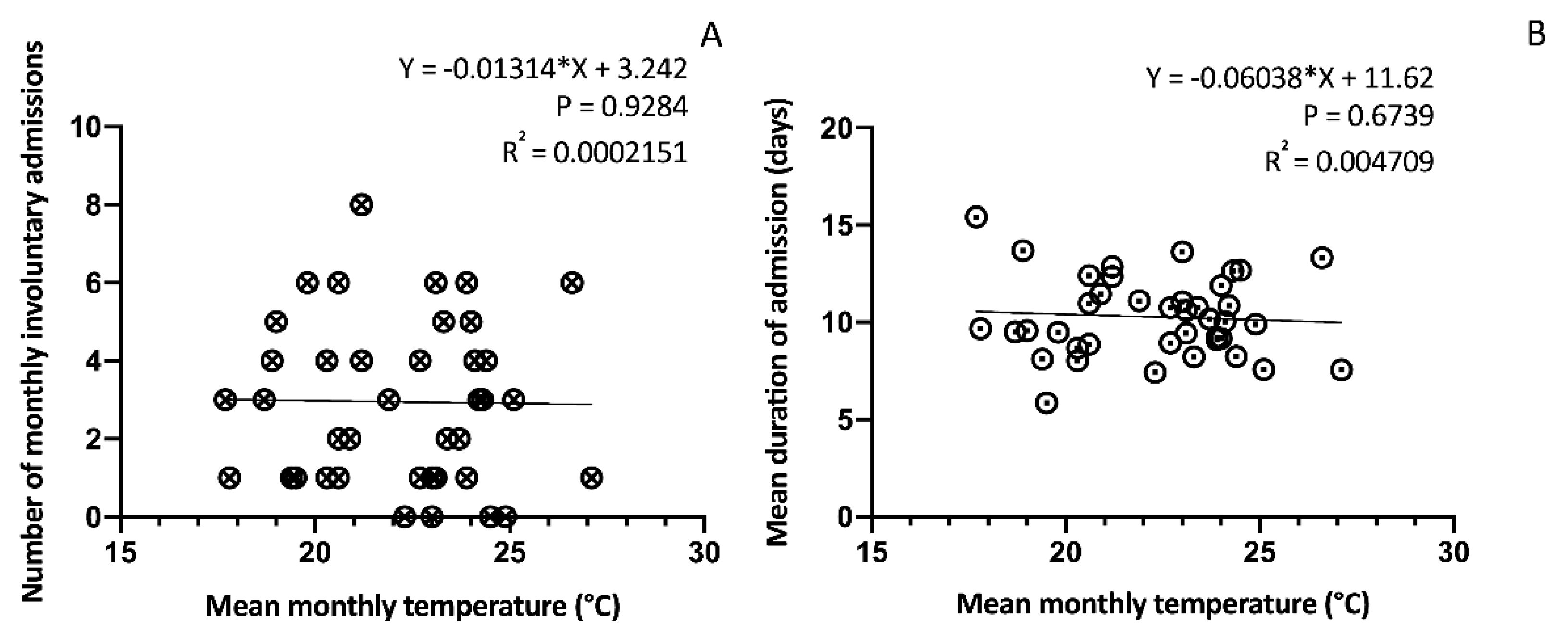

Table 1.
Socio-demographic and clinical characteristics of the sample.
| Total number of admissions | 1600 |
| Age, mean (+/-SD) | 45.74 (+/-15.51) years |
| Gender, n(%) |
878 (54.87) 722 (45.13) |
| Male Female | |
| Main diagnosis, n(%) |
556 (34.75) 231 (14.44) 325 (20.31) |
| BD MDD SCZ | |
| Type of admission, n (%) |
1482 (92.62) 118 (7.38) |
| Voluntary Involuntary | |
| Duration of admission, mean (+/- SD) | 9.99 (+/-8.95) days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



