Submitted:
08 May 2024
Posted:
09 May 2024
You are already at the latest version
Abstract
Introduction: Caries is a public health problem in Kosovo among children, Caries is a multifactorial microbial disease and connection of this disease with soft drinks and food habits between children and their poor oral health is very strong.
Aim: The aim of present study is to evaluate prevalence of caries among 12 to 16 years old students in municipality of Suhareka and to analyze related risk factors that contribute in occurrence of caries.
Material and methods: To observe parameters of soft drink we used experimental method and a cross-sectional study was carried out among 120 adolescents in “Sadri Duhla” elementary school in Duhel and “7 Marsi” elementary school in city of Suhareka. Oral clinical examination and self administered questionnaire were used to collect information about dental caries and its correlation to soft drinks and food habits. Examination was done between May and October in the year 2023. Impact of soft drink in caries was assessed through DMFT index and frequency of consumption of soft drinks. The data were collected statistically using SPSS version 26 and presented in tables and graphs.
Results: The highest result of DMFT (4.36) with standard deviation 1.23 was noted in the group consuming more than 16 cans per week also the highest score in adolescent compared to frequency of consumed cans per week. Soft drinks found in Kosovo’s mar-kets are acidic with low pH, 93.75% of them had a pH below 4 which are considered erosive and only 6.25% are minimally erosive with a pH > 4, in terms of buffer capacity soft drinks can be ordered like this energy drinks >soda >100% fruit juice > fruit drinks. Improper tooth-brushing, dental visits only in case of pain and not preventive visits were significantly related to dental caries.
Conclusion: The results of the research awarned us for high frequency consumption of soft drinks related to dental caries. It is recommended to be aware of the use of soft drinks, regular visits to the doctor, higher maintenance of oral health by using paste with sufficient fluoride content also brushing teeth 1 hour after consuming acidic food.
Keywords:
DMFT
; soft drinks
; frequency
; adolescents
1. Introduction
On the occurrence of dental caries and enamel degradation, food has the most important nutritional impact. One of main ingredients in food are acids, naturally or added which can be separated by origin into intrinsic and extrinsic factors. These are believed to be among the main causes of dental erosion. Low pH of acidic foods and drinks play an important role in the development of erosion. Poor oral hygiene and continuous consumption of soft drinks lead to tooth disease. In other cases that have been studied, slowly progressed caries may suddenly become rampant. Frequent exposure to erosive acids may lead to dental caries (McIntyre, 1992) Consumption of acidic foods and soft drinks is associated with tooth substance loss which bring erosion as an increasing social problem because it is frequently linked with individuals lifestyle and eating habits [1]. High consumption of soft drinks has been increased through the years in all the world, young generation especially, which leads to the early loos of teeth and this is a serious concern. All these together lead to a lot of researches that has been done and to be also, to find out the exact factors associated with this problem and how to prevent this effect. Consumption of these beverages is increasing and this is coming most of it through the commercials and their refreshing taste, these beverages are presented as source of vitamin, energy booster etc. The major added content to these soft drinks are sugar, fructose syrup, citric acid, phosphoric acid and malic acid [2]. One of most common dangers of dental decay is intake of carbonated drinks, especially in children and adolescents [3,4,5]. External factors as soft drink for the alteration in tooth enamel to occur on other side we have also the intrinsic factors, such as eating disorder, gastric reflux, which can lead to output of gastric content into the oral cavity. This leads to a loss of tooth substance or erosion of the tooth [1].
From available literature and researches, explain to us that are many factors that influence the behavior of enamel when it is exposed to soft drinks. These factors are pH, buffer capacities, acidic species, exposure time, lifestyle carbohydrate intake, calcium and phosphate content [1,6,7]. If not controlled, enamel erosion leads to dentinal hypersensitivity and therefore to pain [8,9].
The consumption of soft drinks causes a reduction in the salivary pH. Known as “critical pH” for enamel dissolution is considered a pH of 5. 5, while for dentin it is 6. 8. Buffering capacity of soft drinks and their pH represent their erosive potential. In previous reports, the initial pH values of some soft drinks and their buffering capacities were determined. The lowest pH indicated to be for carbonated drinks more than fruit juices also. The buffering capacities are in the following order: fruit juices>fruit-based carbonated drinks>non-fruit-based carbonated drinks [10,11]. Many researches has been following information on certain types of foods and beverages with a high level of acidity, such as carbonated drinks, fruit, fruit juices, and other beverages, also the timing of consumption, during main meals or snacks [12].
Soft drinks are largely produced as acidic beverages with an interval of pH between 2. 5 – 4. 0 and consumed worldwide [13]. In the second half of the nineteenth century the first carbonated drinks were produced [14]. Main ingredients of soft drinks are water, sweetener, acidifier, flavorings, carbon dioxide, coloring agents, chemical preservatives (within the legal limits), antioxidants, and foaming agents. [2]. Sugar and fermentable carbohydrates can provide substrate for oral bacteria action in this way it lower the plaque and salivary pH, and as a result of all this we have beginning of tooth demineralization. There is a direct link between the consumption of sugars and dental caries and this has been proven by scientific research [15].
2. AIM
Aim of this research were twofold: (1) to investigate frequency of soft drinks intake and its correlation with DMFT, also the connection between DMFT with food habits and oral health practices, (2) to examine physic-chemical properties of soft drinks present in Kosovo markets.
3. Methodology
A total of 80 beverages were purchased from stores in Suhareka, Prizren, Dragash, Rahovec, categorized (i. e. soda, soft drinks, fruit juices, 100% fruit juices) and assessed for pH, total acidity, °Brix, buffer capacity.
Determination of pH
An HANNA edge® pH meter calibrated was used to measure the pH of each beverage in triplicate immediately after opening at 25°C to give a mean measurement for that drink. After that we determined the erosive potential of each beverage based on relative beverage erosivity zones from studies of apatite solubility in acid.
Determination of °Brix
“Refractometer 30PX”, produced by METTLER TOLEDO was used for determination of °Brix, at temperature around 20°C, measurements were repeated in triplicate for all drinks and average value was taken with standard deviation. Dissolved sugar in the fruit juice is measured in terms of °Brix, Baume or Oechsle. °Brix is the most widely used unit in the food and beverage industry. It indicates the number of dissolved solids in a liquid measured via its specific gravity (SG). One degree °Brix is 1 g of sucrose in 100 g of solution (1 °Brix = 1% sugar).
Determination of Buffer Capacity
Buffering capacity: 100ml of each drink titrated with 1M NaOH added in 0. 2ml increments until 5. 5 and 7 of pH was reached. This was done by mixing the sample until a stable pH reading was obtained after each increment (0. 2ml) of NaOH. This procedure was done from [16] to measure buffer capacity amount. Each titration was done three times in row for all the drinks to check for reproducibility and to give a mean value for that drink.
Participants and Oral Examination Procedure
The second part and the most important of our study represent a cross-sectional study KP (knowledge, practice) involved 120 students participated. Questionnaire and help was given to the participants. Questionnaire was built according to socio-demographic factors, age, gender, consumption of soft beverages, knowledge also oral-health were asked to the participants. A detailed oral-examination was carried out after answer sheets were collected. The examination was done between May and October in the year 2023, by two doctors. This research was confined to the participants between 12 - 16 years old.
During clinical examination of participants being seated in ordinary chair with supply of adequate daylight, supplemented with a torch if required to facilitate the examination. Dental caries was done in accordance with WHO criteria and data recorded on a WHO oral health assessment form. The exam was conducted in the morning to eliminate any errors that may occur in the evening, due to less sunlight different food that could be eaten during day. Between 35 to 40 adolescents were examined during day and also the questionnaire was fulfilled. Next day 20 participants were chosen randomly and re-examined and results were same as previous day, this was done to eliminate any of inter-examiner lability. Detection of dental caries was done tooth by tooth, according to decayed, filled teeth and surfaces (DMFT and DMFS). As a conclusion oral examination has been done in accordance to the WHO criteria [17].
Criteria for diagnosis and coding was done by following conditions as described:
- 0.
- Sound crown: A crown considered to be sound when it doesn’t show evidence of treated or untreated caries. In the absence of positive criteria, a crown with following defects is coded as sound:
- White or chalky spots: When we touch the tooth with probe even it is discoloured or rough spots those aren’t soft
- Stained pits or fissures: in the enamel there isn’t any visual sign of cavities or enamel damage.
- Dark shiny, hard and pitted areas that shows signs of fluorosis.
- Lesions that based on visual examination appear to be due to abrasion.
- 1.
- Decayed Crown: Caries is recorded as present when there was a lesion in pit or fissure wich has an unmistakable cavity. In cases of tooth with a temporary filling a tooth wich is sealed [code 6] will be included in this category. When there is only the root, because the crown has been destroyed by caries is scored as a decayed crown.
- 2.
- Filled crown, with decay: A crown considered filled with decay, when the tooth have one or more permanent restoration but there is also one or more areas that are decayed. Between primary and secondary caries isn’t made any distinction.
- 3.
- Filled Crown, with no decay: When a crown has one or more permanent restoration present but there is no evidence of caries anywhere on the crown.
- 4.
- Missing tooth: It’s used for permanent dentition for the teeth that have been extracted as a result of caries. as a result of caries.
- 5.
- Permanent tooth missing, for different reason: This was used for teeth that considered to be absent for congenitally problems, or that have been extracted due to orthodontic reasons, trauma, any other periodontal disease etc.
- 6.
- Fissure sealant: This code was used for permanent teeth in which on the occlusal surface have been placed a fissure sealant or has been placed a composite material.
- 7.
- Bridge abutment, crown or veneer: This code is used under coronal status and can also be used for crowns.
- 8.
-
Unerupted crown: This code included unerupted permanent teeth without a primary teeth, and for congenitally reasons the tooth is missing or due to traumatic reasons the tooth have been lost.T. Trauma (fracture): A fractured crown is scored when a crown is missing some of its surface.
- 9.
- Not recorded: This classification is used for erupted permanent tooth that for any reason cannot be examined. The following reasons are: severe to moderate hypoplasia, orthodontic bands etc. The surface with dental plaque was evaluated by Quigley and Hein index5 modified6 also findings of bleeding were recorded separately for each of the index teeth (DD 16, 11,26,36,31 and 46). Gingival health status was assessed, data collected by Chi-square test and statistical analysis was performed by using SPSS software.
Statistical Analysis
Me e pershkru procesimin e te dhenave me SPSS
4. Results
Soft Drinks and Its Physico-Chemical Characteristics
pH Measurements
The average pH of each group from soft drinks with their standard deviation was shown in chart below represented in Figure 3. pH of fruit drinks were in range from 2. 74 – 3. 6 with an average of 3. 02, pH of 100% fruit juices were in range from 3. 4 – 4. 1 with an average of 3. 72, pH of drinks classified in soda category were in range from 2. 4 – 3. 2 with an average of 2. 69, pH of energy drinks were in range from 3. 1 – 3. 65 with an average of 3. 54.
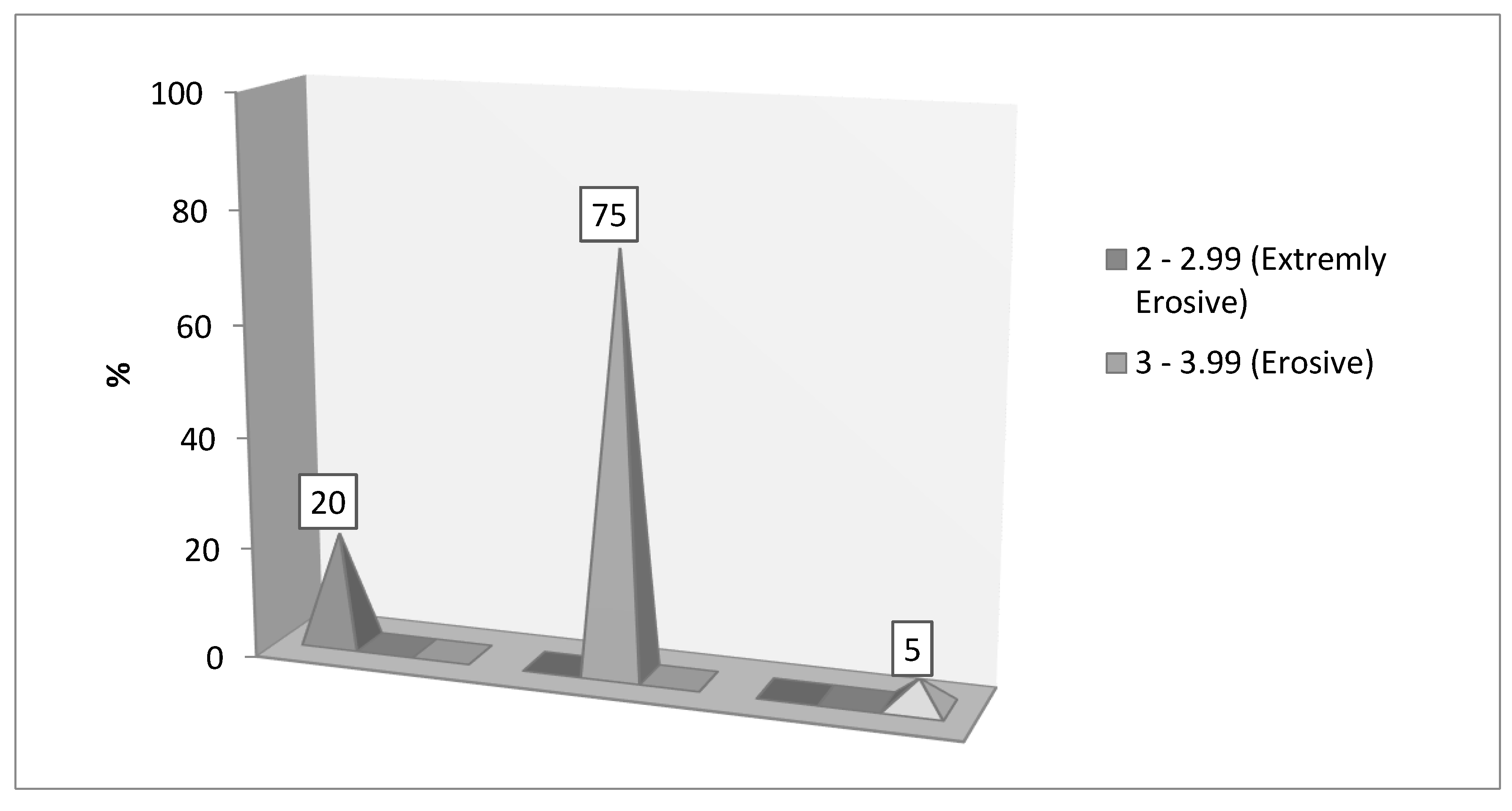
Around (75/80) of beverages had a pH < 4. 0, and (5/80) had a pH ≥ 4. Relative beverage erosive zones based on previous studies of apatite solubility in acid indicated: 20% of the beverages were considered extremely erosive (pH <3. 0); 75% were considered erosive (pH 3. 0 to 3. 99); 5% were considered minimally erosive (pH ≥4. 0). These results are represented in chart below.
Figure 1.
Soft drinks classification in term of erosivity based on apatite solubility in acid.
Brix Measurements
Dissolved sugar in the fruit juice is measured in terms of °Brix, Baume or Oechsle. °Brix is the most widely used unit in the food and beverage industry. It indicates the number of dissolved solids in a liquid measured via its specific gravity (SG). One degree ° Brix is 1 g of sucrose in 100 g of solution (1 °Brix = 1% sugar). Results of °Brix have been shown in the chart below: °Brix of fruit drinks were in range from 8. 9% – 12. 5% with an average of 10. 28%, °Brix of 100% fruit juices were in range from 11. 0% – 14. 5% with an average of 12. 33%, °Brix of beverages classified in soda category were in range from 9. 1% – 13. 2% with an average of 11,2% °Brix of energy drinks were in range from 11% – 11. 5% with an average of 11. 26%.
Buffer Capacity Measurements
The buffering capacity of each beverage was assessed by measuring by adding 1M NaOH in the increments of 0. 2 ml into 100 ml of each drink till the pH arrived to 5. 5 respectively 7. Based on statistical analysis using ANOVA and Fisher's post hoc tests at a P < 0. 05 level of significance, beverages classified at energy drinks category had the highest mean buffering capacity (indicating the strongest potential for erosion of enamel), followed by soda, fruit drinks and 100% fruit juices.
An average of 8. 72 mL of base is required to bring the pH back to the neutral level of pH 7. 0 (Table 1). This indicates that not only are the soda and energy drinks highly acidic but also it is necessary to produce a large amount of alkaline-stimulated saliva to be neutralized when they are in contact with tooth.
Demographic and Oral Health
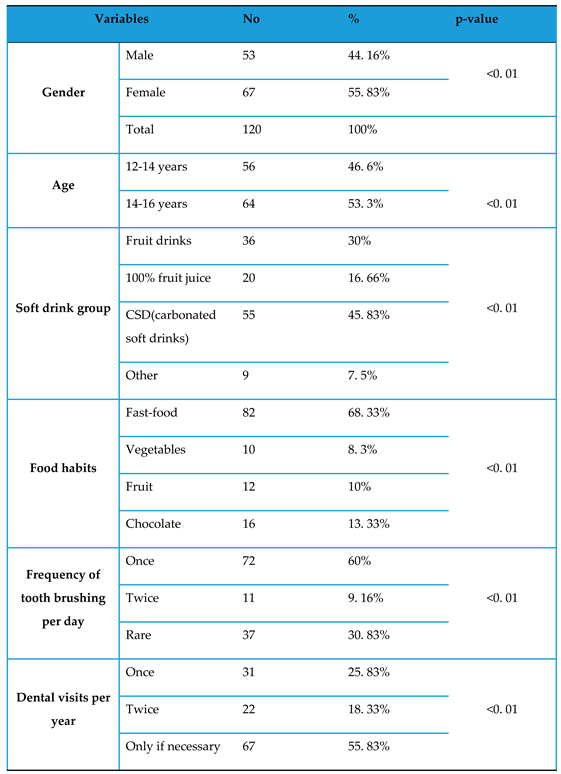
Questionnaire fulfilled by 120 child revealed interesting data. From 120 of them, 53 (44. 16%) were boys and 67 were girls (55. 83%). 56 of participants were between 12-14 years old (46. 6%), and 64 of them were from 14-16 years old (53. 3%). Around 72 of them used to brush teeth only once per day (60%), 11 of them used to brush teeth twice per day (9. 16%), 37 of them brushed teeth rare (30. 83%). As for dental visits 31 of participants used to have once per year(25. 83%), 22 answered they do dental visits twice per year (18. 33%), and 67 stated they finish dental visits only if necessary (55. 83%).
Soft Drinks Frequency and Food Habits
There was a significant difference of DMFT compared to the frequency of consumption of soft drinks. DMFT increased with increase in soft drinks consumption per week. The highest result of DMFT (4. 36) with standard deviation 1. 23 was noted in the group consuming more than 16 cans per week (Table 2).
Soft drinks were distributed into three groups. First was fruit drinks group included still drinks with different types of flavor like: orange, blueberry, forest-fruit, multivitamin etc. Second group included fruit juices with no added sugar, third one included all CSD (carbonated soft drinks). 36 of participants answered they prefer fruit drinks (30%), 20 of them answered 100% fruit juice (16. 66%), 55 of them answered they prefer carbonated soft drinks (45. 83%) and 9 of them did not consumed any of soft drinks, they prefer milk and its products. From 120 child 82 of them prefer fast-food (68. 33%) during meal at school, 16 eat chocolates (13. 33%), 12 prefer fruits (10%), 10 of them preferred vegetables (8. 3%). These results are presented on Table 3.
5. Discussion
Present study in topic of it had to investigate the association between soft drinks and DMFT in adolescents between 12 – 16 years old in Kosovo. Findings suggest that the majority of participants were highly connected with soft drink consumption. Additionally, the highest prevalence of DMFT was found to be associated with high frequency of soft drinks intake also with other various demographic, food habits, oral health factors such as tooth brush frequency, dental visits. Frequency of soft drinks intake was statistically significantly positively correlated with DMFT and this is in accordance with previous researches done by authors [18,19,20,21], researches were done in adolescents 12 years and older, all of them reported a significantly correlation between frequency of soft drink and increase in DMFT. Our first hypothesis has been proven by reported result of DMFT (4. 36) with standard deviation 1. 23 was noted in the group consuming more than 16 cans per week, there is a dose-response relationship between sugars and dental caries, this corresponds to the results in Table 2, where dental caries was higher in people who consumed large amounts of soft drinks compared to those who did not. With an increase of consumption of SD per week the DMFT index was higher to those who consumed less. which is in accordance with the previous findings of the study from [22] author investigated a significant difference by increasing frequency of consumption of carbonated drinks, DMFT increased. Otherwise research done by [23] found that people who did not consume soft drinks had 39% less expression of the DMFT index in relation to those who consumed them on a daily basis, this is also consistent with our results expressed in Table 2, where people who did not consume soft drinks had at least 46. 42% less expression of the DMFT index in relation to those who consumed them weekly. According to [24] sugar and acid content of beverages was the explanation for tooth decay and this is the reason that leads to high pH drops of dental plaque, and it is followed with high dental issues, explanation for that is consumption of sweetened beverages and fruit juice with sugar as me the main ingredient.
Dental caries is associated with frequency consumption of acidic beverages, but properties like pH and titratable acidity of acidic beverages are still under debate. All tested beverages had an acidic pH, below the critical pH level that can lead to enamel loss. Our results from pH measurements are consistent with other authors, for example we determined the pH of beverages around (93. 75 %, 75/80) pH were below 4, and (6. 25% 5/80 had a pH > 4), [25], found that majority (93%, 355/380) of beverages had a pH below 4. 0 and 7% (25/380) had a pH ≥4, [26] found that 88% of all beverages tested had a pH <4, and 12 had a pH ≥ 4. Classifying beverages on apatite solubility in acid indicated that most of the soft drinks on market we can say that >50% are erosive, [25] concluded 54% are erosive, [26] also showed more than 51% were erosive (pH <4). Our study showed that, majority of soft drinks have a pH from 2. 4 to 4. 1 with an average 3. 35, quite close to results from [27] who reported an average of 3. 44 for soft drinks.
Reported amount through researches of sugar founded in soft drinks usually is between 1% and 12% sugar, in form of sucrose, glucose or fructose [2] these results are similarly to our findings expressed in brix degree presented in Table 1. [28] reported the sugar in term of grams for different type of soft drinks found in the market, red bull 39 g/355 ml, coca cola classic 39 g/355 ml, diet coca cola 0 g/355 results are similarly to ours presented in Table 3, where red bull 35. 64 g/330 ml included on energy drink type, cola classic 36. 3 g/330 ml and diet cola 0 g/330 ml both of them were included in soda type.
Our results expressed a mean DMFT value of 3. 9 with a SD of 1. 27, compared to countries in the region where [29] reported in Macedonia a DMFT of 3. 55 with SD of 2. 99 and [30] reported in Albania a DMFT of 4. 9 the results are close to each other, this results express a same situation with a high DMFT prevalence of caries among the adolescents in Balkan.
Other author found that in the permanent dentition, a significant positive correlation was detected between age, soft drinks, sweetened juice, desserts, and DMFT [31], by results expressed in Table 3 there is a positive significant correlation between gender, age, chocolates, fast food and increase of DMFT.
Researches has been reporting apart from its pH value, the ability of an acidic solution to dissolve enamel or dentin depends on its ability to keep pH unaffected by the dissolution of tooth mineral and dilution with saliva (i. e. , buffering capacity). Author reported that energy drinks had the most erosive potential due to their significantly greater buffering capacity as compared to carbonated drinks and fruit juices conclusions from study of [32] are in accordance with ours, reported in Table 1. Where energy drinks had the highest buffer capacity followed by soda, 100% fruit juices and fruit drinks.
Current research presented to us that most of child in Kosovo 72 of them brush their teeth once per day (60%), 11 of them used to brush their teeth twice per day (9. 16%) and 37 brushed their teeth rare (30. 83%). Our results are in accordance with previous research done by [33] observed that rare tooth brushing among 15 years old in Kosovo per day increased level of caries and also [34] reported a correlation between frequency of tooth brushing and caries, better caries status and gingival index was observed with more frequent toothbrushing. [35] also reported that students who had never brushed their teeth or done is so infrequently had scored higher DMFT results opposite to those who brushed their teeth at least once and more. Furthermore contrary to our results, other studies made by [36], observed no correlation between caries and frequency of tooth brushing. This might be related to improper technique of brushing and not enough tooth brushing time and low level of fluoride in toothpaste. As conclusion frequency of tooth brushing is important for oral health and preventing the occurrence of caries, by our findings frequency was positively associated with higher DMFT. Better oral health might be in accordance with regularly dental visits reported [37]. As for dental visits 31 of participants finished dental visits once per year (25. 83%), 22 of participants visit dentist twice per year (18. 33%) and 67 of them used to have dental visits only if necessary (55. 83%) there is a positive significant correlation between this category and DMFT increase, our results are in accordance with previous researches from [33,36] which reported a positive link between dental visits and caries.
6. Conclusion
Our study evidenced soft drinks found in Kosovo markets are acidic with low pH, 93. 75% of them had a pH below 4 which are considered erosive and only 6. 25% are minimally erosive with a pH > 4. Most erosive potential due to their significantly greater buffering capacity was indicated by energy drinks followed by soda, 100% fruit juices and fruit drinks. Soft drinks and its frequency were positively correlated with increase of DMFT. Consumption of fruit and vegetables followed by preventive dental visits with brushing teeth twice was negatively associated with caries. Furthermore the prevalence of dental caries in Kosovo schoolchildren was high, which is in accordance with previous research. Furthermore prevalence of caries in Kosovo compared to countries near is almost the same but still high compared to European countries. We encourage a well-balanced diet with reduction intake of soft drinks, or choosing less erosive ones, and consuming vegetables more often, tooth brushing twice per day with enough content of fluoride (1000-1500 ppm), at least twice per year dental check-up in term of preventive visits and also a strategy for orthodontic treatment in Kosovo it is very important to happen.
References
- Lussi, A.; Schlueter, N.; Rakhmatullina, E.; Ganss, C. Dental Erosion – An Overview with Emphasis on Chemical and Histopathological Aspects. Caries Res. 2011, 45, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Kregiel, D. Health Safety of Soft Drinks: Contents, Containers, and Microorganisms. BioMed Res. Int. 2015, 2015, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Harnack, L.; Stang, J.; Story, M. Soft Drink Consumption Among US Children and Adolescents. J. Am. Diet. Assoc. 1999, 99, 436–41. [Google Scholar] [CrossRef] [PubMed]
- Shenkin, J.D.; Heller, K.E.; Warren, J.J.; Marshall, T.A. Soft drink consumption and caries risk in children and adolescents. Gen Dent. 2003, 51, 30–6. [Google Scholar] [PubMed]
- Tahmassebi, J.; Duggal, M.; Malik-Kotru, G.; Curzon, M. Soft drinks and dental health: A review of the current literature. J. Dent. 2006, 34, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Meurman, J.H.; Gate, J.M.T. Pathogenesis and modifying factors of dental erosion. Eur. J. Oral Sci. 1996, 104, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Ten Gate, J.M.; Imfeld, T. Dental erosion, summary. European J Oral Sciences 1996, 104, 241–4. [Google Scholar] [CrossRef] [PubMed]
- Alcântara, P.M.; Barroso, N.F.F.; Botelho, A.M.; Douglas-De-Oliveira, D.W.; Gonçalves, P.F.; Flecha, O.D. Associated factors to cervical dentin hypersensitivity in adults: a transversal study. BMC Oral Heal. 2018, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Davari, A.; Ataei, E.; Assarzadeh, H. Dentin Hypersensitivity: Etiology, Diagnosis and Treatment; A Literature Review. J. Dent. 2013, 14, 136–145. [Google Scholar]
- Edwards, M.; Creanor, S.L.; Foye, R.H.; Gilmour, W.H. Buffering capacities of soft drinks: the potential influence on dental erosion. J. Oral Rehabilitation 1999, 26, 923–927. [Google Scholar] [CrossRef]
- Owens, B.M. The potential effects of pH and buffering capacity on dental erosion. Gen Dent. 2007, 55, 527–31. [Google Scholar] [PubMed]
- Al-Zwaylif, L.H.; O'Toole, S.; Bernabé, E. Type and timing of dietary acid intake and tooth wear among American adults. J. Public Heal. Dent. 2018, 78, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Azeredo, D.R.; Alvarenga, V.; Sant'Ana, A.S.; Srur, A.U.S. An overview of microorganisms and factors contributing for the microbial stability of carbonated soft drinks. Food Res. Int. 2016, 82, 136–144. [Google Scholar] [CrossRef]
- Matar, M.; Darwish, S.S.; Salma, S.R. Erosive potential of some beverages on the enamel surface of primary molars. IOSR-JDMS. 2021, 20, 43–6. [Google Scholar]
- Touger-Decker, R.; Van Loveren, C. Sugars and dental caries. The American Journal of Clinical Nutrition. 2003, 78, 881S–892S. [Google Scholar] [CrossRef] [PubMed]
- Touyz, L.Z.; Silove, M. Increased acidity in frozen fruit juices and dental implications. ASDC J Dent Child. 1993, 60, 223–5. [Google Scholar]
- World Health Organization, editor. Oral health surveys: basic methods. 4th ed. Geneva: World Health Organization; 1997. 66 p.
- Mello, T.; Antunes, J.; Waldman, E.; Ramos, E.; Relvas, M.; Barros, H. Prevalence and severity of dental caries in schoolchildren of Porto, Portugal. Community Dent Health. 2008, 25, 119–25. [Google Scholar]
- Punitha, V.C.; Amudhan, A.; Sivaprakasam, P.; Rathanaprabu, V. Role of dietary habits and diet in caries occurrence and severity among urban adolescent school children. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. 1), 298–300. [Google Scholar] [CrossRef] [PubMed]
- Skinner, J.; Byun, R.; Blinkhorn, A.; Johnson, G. Sugary drink consumption and dental caries in New South Wales teenagers. Aust. Dent. J. 2015, 60, 169–175. [Google Scholar] [CrossRef]
- Zhang, S.; Chau, A.M.; Lo, E.C.; Chu, C.-H. Dental caries and erosion status of 12-year-old Hong Kong children. BMC Public Heal. 2014, 14, 1–7. [Google Scholar] [CrossRef]
- Damle, S. The Effect of Consumption of Carbonated Beverages on the Oral Health of Children: A Study in Real Life Situation. 11, 40. [CrossRef]
- Hasheminejad, N.; Mohammadi, T.M.; Mahmoodi, M.R.; Barkam, M.; Shahravan, A. The association between beverage consumption pattern and dental problems in Iranian adolescents: a cross sectional study. BMC Oral Heal. 2020, 20, 74. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Rivas-Tumanyan, S.; Morou-Bermúdez, E.; Colon, A.M.; Torres, R.Y.; Elías-Boneta, A.R. Association between Type, Amount, and Pattern of Carbohydrate Consumption with Dental Caries in 12-Year-Olds in Puerto Rico. Caries Res. 2016, 50, 560–570. [Google Scholar] [CrossRef]
- Reddy, A.; Norris, D.F.; Momeni, S.S.; Waldo, B.; Ruby, J.D. The pH of beverages in the United States. J. Am. Dent. Assoc. 2016, 147, 255–63. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.; Islam, S.; Hasan, N.; Al-Khazraji, A.; Maki, H. Erosive Potential of Various Beverages in the United Arab Emirates: pH Assessment. Dubai Med J. 2023, 6, 124–133. [Google Scholar] [CrossRef]
- Chowdhury, C.; Shahnawaz, K.; P, D.K.; Chowdhury, A.; Gootveld, M.; Lynch, E. Highly acidic pH values of carbonated sweet drinks, fruit juices, mineral waters and unregulated fluoride levels in oral care products and drinks in India: a public health concern. Perspect. Public Heal. 2019, 139, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Arhakis, A.; Mavrogiannidou, Z.; Boka, V. An Overview of the Types of Soft Drinks and Their Impact on Oral Health: Review of Literature. World Journal of Dentistry. 2023, 14, 648–54. [Google Scholar] [CrossRef]
- Ambarakova, V.; Panova, O. Dental Caries Experience among 15-years Old Children in the Southeast Region of the Republic of Macedonia. Oral Health and Dental Management. 2015, 14, 336–73. [Google Scholar]
- Laganà, G.; Abazi, Y.; Beshiri Nastasi, E.; Vinjolli, F.; Fabi, F.; Divizia, M.; et al. Oral health conditions in an Albanian adolescent population: an epidemiological study. BMC Oral Health. 2015, 15, 67. [Google Scholar] [CrossRef]
- Mahmoud, S.A.; El Moshy, S.; Rady, D.; Radwan, I.A.; Abbass, M.M.S.; Al Jawaldeh, A. The effect of unhealthy dietary habits on the incidence of dental caries and overweight/obesity among Egyptian school children (A cross-sectional study). Front. Public Heal. 2022, 10, 953545. [Google Scholar] [CrossRef]
- Shenoy, V.U.; Shaikh, S.; Venkatasubramanyam, S.M.; Verma, J.; Chavan, P.; Gawali, S. To evaluate the buffering capacity of various drinks commonly available in India. MGM J. Med Sci. 2020, 7, 56. [Google Scholar] [CrossRef]
- Ferizi, L.; Bimbashi, V.; Kelmendi, J. Dental Caries Prevalence and Oral Health Status among 15-Year- Old Adolescents in Kosovo. Acta Stomatol. Croat. 2022, 56, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.M.; Mani, S.A.; Doss, J.G.; Danaee, M.; Kong, L.Y.L. Pre-schoolers’ tooth brushing behaviour and association with their oral health: a cross sectional study. BMC Oral Health. 2021, 21, 283. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, F.A.; Khabeer, A.; Moheet, I.A.; Khan, S.Q.; Farooq, I.; ArRejaie, A.S. Prevalence of dental caries in primary and permanent teeth and its relation with tooth brushing habits among schoolchildren in Eastern Saudi Arabia. SMJ. 2015, 36, 737–42. [Google Scholar] [CrossRef] [PubMed]
- Mallineni, S.K.; Alassaf, A.; Almulhim, B.; Alghamdi, S. Influence of Tooth Brushing and Previous Dental Visits on Dental Caries Status among Saudi Arabian Children. Children. 2023, 10, 471. [Google Scholar] [CrossRef]
- Thomson, W.M.; Williams, S.M.; Broadbent, J.M.; Poulton, R.; Locker, D. Long-term Dental Visiting Patterns and Adult Oral Health. J Dent Res. 2010, 89, 307–11. [Google Scholar] [CrossRef]

Table 1.
Description of °Brix, pH, buffer capacity and sugar content of beverages available on the market.
Table 1.
Description of °Brix, pH, buffer capacity and sugar content of beverages available on the market.
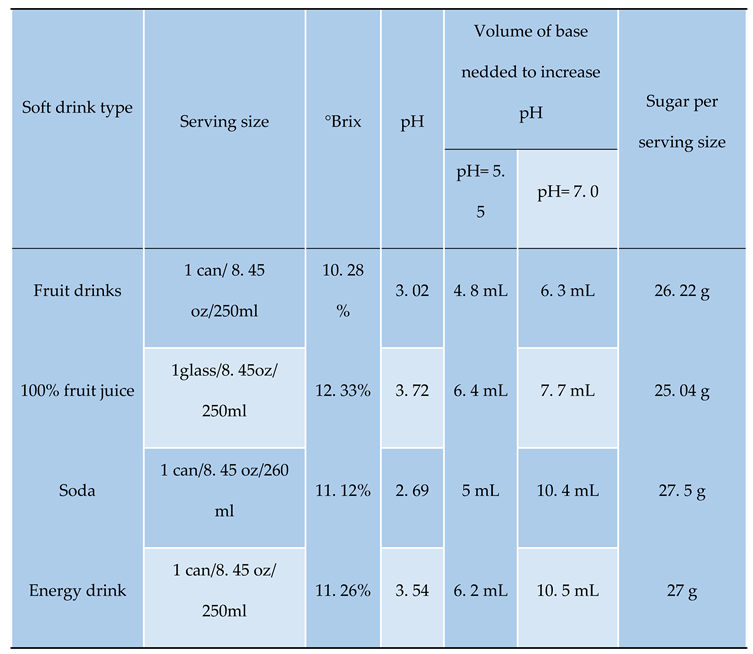 |
Table 2.
Frequency of cans consumed, caries status, index during clinical examination.
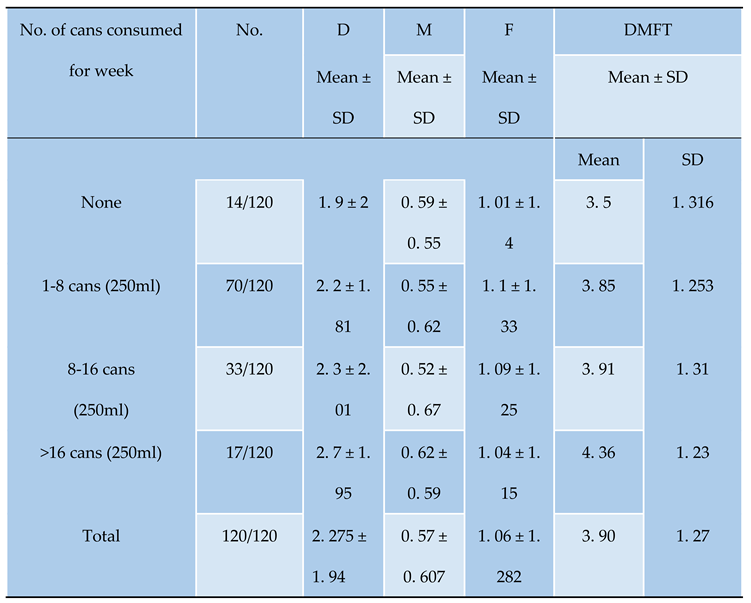 |
Table 3.
DMFT in relation to gender, dietary habits and oral hygiene practices.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



