
Submitted:
09 May 2024
Posted:
09 May 2024
You are already at the latest version
Abstract
Anxiety disorders affect patient quality of life (QoL). This study aimed to examine the associations between improved QoL and reduced clinical symptoms and Korean medicine (KM) in patients with anxiety disorders. Medical records of patients with anxiety who were treated with KM (acupuncture, Anxiety disorders affect patient quality of life (QoL). This study aimed to examine the associations between improved QoL and reduced clinical symptoms and Korean medicine (KM) in patients with anxiety disorders. Medical records of patients with anxiety who were treated with KM (ac-upuncture, psychotherapy, Chuna therapy, aromatherapy, or herbal medicine) for at least 4 weeks were retrospectively analyzed. Clinical, QoL, and cost outcomes were measured at baseline and at 4 and 12 weeks (Anxiety: State-Trait Anxiety Inventory[STAI X-1(state), X-2(trait)], Beck Anxiety Inventory[BAI]; anger: State-Trait Anger Expression Inventory State[STAXI-S(state), T(trait)], Anger Expression Inventory[AXI-K-I(anger-in), AXI-K-O(anger-out), AXI-K-C(anger-control); depression: Beck Depression Inventory-II[BDI II], QoL: QoL-related instruments Euro Quality of Life 5 Dimensions utility score[EQ-5D], Euro QoL Visual Analog Scale[EQ-VAS]). The quali-ty-adjusted life years (QALYs) and average cost-effectiveness ratio of KM for anxiety were esti-mated. The medical records for 67 patients were evaluated. KM treatments were found to be as-sociated with decreased anxiety (STAI X-1; STAI X-2; BAI, p
Keywords:
anxiety disorder
; cost analysis
; Korean medicine
; quality of life
; retrospective study
1. Introduction
Anxiety is defined as a ‘persistent feeling of dread, apprehension, and impending disaster or tension and uneasiness’ [1]. Anxiety disorders are the most common type of mental disorder and include generalized anxiety disorder (GAD), panic disorder (PD), phobias, obsessive-compulsive disorder, and posttraumatic stress disorder (PTSD) due to general medical conditions [2]. These disorders are associated with considerable distress, impaired functioning, and increased risk of suicide [3]. Over 301 million people worldwide, representing approximately 3.9% of the world’s population, were estimated to be affected by anxiety disorders, accounting for the largest proportion of all mental diseases (31.1%) in 2019 [4,5].
While various pharmacological and psychological therapies exist for anxiety disorders, patients with these conditions often opt for the use of complementary and alternative medicine (CAM) to decrease or avoid medication use, alleviate physical and psychological symptoms, and improve quality of life (QoL) [6]. Moreover, CAM can help with areas of mental health that are difficult to address using WM [7,8]. In Korea, a unique dual medical system exists in which both WM and Korean medicine (KM) are available to patients with anxiety disorders [9]. KM uses a symptom-based approach that identifies specific etiologies and symptoms rather than prioritizing the naming of specific diseases or diagnoses, and it utilizes various treatments such as herbal medicines, acupuncture, moxibustion, and physical therapies [10]. These categories are specific to KM and may not directly correspond to the classifications of CAM therapies used in other countries [8,11,12,13]. While psychotropic drugs are widely used to treat anxiety disorders, patients often seek KM to reduce their dependence on such medications to replace pharmacotherapy altogether and avoid adverse drug reactions [6].
In KM clinics, anxiety is typically diagnosed through self-evaluation, counseling, and anxiety questionnaires such as the State-Trait Anxiety Inventory (STAI) and Beck Anxiety Inventory (BAI), as well as instrumental examinations such as heart rate variability (HRV) measurement and neurofeedback [6]. The goal of anxiety treatment in KM is not only to stabilize the mind and alleviate symptoms but also to regulate body function and maintain internal energy balance [14]. To achieve this, acupuncture and herbal medicine are commonly used following the treatment principles of regulating the balance between yin and yang as well as regulating the states of Qi and blood [14]. Psychotherapy, moxibustion, cupping therapy, electroacupuncture, and other techniques may also be used [6,14]. Furthermore, anxiety, depression, and anger are interrelated not only in their co-occurrence but also in their underlying mechanisms and treatment approaches [15,16,17,18]. When measuring the effectiveness of anxiety treatment, multiple dimensions such as depression, anger, and QoL are often examined along with anxiety symptoms [15,16,19]. In addition, previous studies of KM therapy have only examined the effectiveness of specific KM treatments for anxiety disorders, so there is no research on the overall effectiveness of KM therapy for anxiety disorders [20,21]. Thus, it is necessary to examine how symptoms of anger or depression improve when anxiety symptoms get better with KM treatment in patients with anxiety.
The present study aimed to investigate the effect of KM treatment regimens (acupuncture, KM psychotherapy, Chuna therapy, aromatherapy, and herbal medicine) on patients with anxiety disorders. We scrutinized medical records from KM clinics and evaluated the clinical, QoL, and cost-effectiveness outcomes of KM treatment currently being employed for patients with anxiety.
2. Materials and Methods
2.1. Study Design
A retrospective case series study design was adopted to evaluate the clinical outcomes, QoL outcomes, and costs of KM treatments. We reviewed medical records of patients with anxiety who visited one of two neuropsychiatric Korean medicine (NKM) clinics in Seoul. The study was carried out in accordance with the Code of Ethics of the World Medical Association; however, informed consent was not required due to the retrospective nature of the study.
2.2. Study Population
The study population included patients who first visited one of the two NKM clinics between December 1, 2017, and June 30, 2020. All patients were aged 20 years or older at their first visit and had been diagnosed with social anxiety disorder (SAD), PD, PTSD, or GAD according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Demographic data, clinical and QoL outcomes, and expenditures for each treatment of patients who received treatment for more than 4 weeks were extracted from the medical records.
2.3. Korean Medicine Intervention for anxiety
The diagnostic process in KM involves personality tests, psychiatric history-taking, and HRV measurements upon initial examination by a KM physician. Among the treatment items in the KM regimen for anxiety disorders, acupuncture, KM psychotherapy, family therapy, aromatherapy, and Chuna therapy were provided weekly. All treatments were covered by the National Health Insurance Service (NHIS) except for herbal medicine and aromatherapy which needed to be fully paid for by the patient. Herbal medicine, such as Ondamtang or Gwibitang, was usually prescribed for a 1-month supply with daily administration and provided to all patients once a diagnosis was made based on the test results. From weeks 5 to 12, the previous treatment methods other than herbal medicine were provided weekly to patients who visited the clinic; for those requiring continuous herbal treatment, additional herbal medicine was administered.
2.4. Outcome Measurement Variables
In the NKM clinics, patients with anxiety were assessed at treatment initiation at check-up points typically occurring at 4 and 12 weeks after treatment initiation. Five domains of anxiety-related scales were examined: (1) Anxiety: STAI axis1 (State, STAI X-1), STAI axis2 (Trait, STAI X-2) [22], and BAI [23]; (2) Anger: State-Trait Anger Expression Inventory State Anger (STAXI-S), State-Trait Anger Expression Inventory Trait Anger (STAXI-T) [24], Anger Expression Inventory Anger-In (AXI-K-I), Anger Expression Inventory Anger-Out (AXI-K-O), and Anger Expression Inventory Anger-Control (AXI-K-C) [25]; (3) Depression: Beck Depression Inventory-II (BDI II) [26]; (4) Optimism: The revised Life Orientation Test (LOT-R) [27]; and (5) Satisfaction: The Satisfaction with Life Scale (SWLS), The Life Satisfaction Expectancy Scale (LSES), and The Life Satisfaction Motivation Scale (LSMS) [28]. A detailed description of the above is provided in Table S1. In addition, we employed the two QoL-related instruments Euro Quality of Life 5 Dimensions utility score (EQ-5D) and Euro QoL Visual Analog Scale (EQ-VAS). The score ranges and their clinical implications are shown in Figure S1. The instruments were completed by surveying patients by a clinical psychologist at the NKM who was familiar with the patients and their disorders.
To evaluate the cost-effectiveness of KM treatment, quality-adjusted life years (QALY) were calculated based on the change in utility scores measured using the EQ-5D. It was assumed that the utility status observed 12 weeks after treatment initiation would persist for 40 weeks based on the experience of one of the researchers, who is a Korean medicine neuropsychiatric specialist (KMNPS). Medical costs for the treatment of anxiety disorders were exclusively examined and analyzed using a micro-costing approach based on medical charts and billing statements, and the average cost-effectiveness ratio (ACER) of NKM services for patients with anxiety disorders was calculated based on the QALY and estimated costs.
2.5. Statistical Analysis
A descriptive analysis of the patients’ baseline clinical characteristics was performed. Continuous variables are presented as the mean ± standard deviation (SD) after testing for normal distribution. Categorical variables are expressed as the number of patients and percentages. The t-test was used to evaluate changes between baseline and after 4 weeks of treatment. To visualize the underlying relational structures among outcome measurement scales, we utilized a multidimensional scaling technique [29]. A distance matrix was computed using the Euclidean distance, and k-means clustering was performed. A correlation analysis was then conducted to determine the strength of the relationship between scales. In all cases, statistical significance was set at p<0.05.
Medical expenses are reported as means with SD. Costs were adjusted to the South Korean won (KRW) in 2020 using the healthcare component of the customer price index from the Korean Statistical Information Service, and the exchange rate from US dollar to KRW in 2020 (1 USD = 1,086.3 KRW) was used. All analyses were performed using R 4.0.2.
3. Results
3.1. Demographic Characteristics and Clinical Outcomes in Patients
Of the 106 patients who visited the NKM clinics during the observation period, 67 who were treated for 4 weeks or longer were considered for analysis. The flow chart for patient selection is shown in Figure S2. The mean age of the included patients at the first visit was 33.2 ± 10.7 years, and 42 (62.7%) were female patients. Patients with GAD accounted for 44.8% (n=30), followed by those with PD (33.8%, n=26), SAD (13.4%, n=9), and PTSD (3%, n=2) (Table S2). Male and female patients did not significantly differ in age, clinical scores, or QoL-related scores, except for BDI II and EQ-5D scores.
Table 1 shows the changes in clinical outcomes between baseline and week 4 of the treatment. Anxiety levels were at baseline severe considering the STAI X-1 (59.24 ± 9.55) and BAI (28.15 ± 12.74) scores or moderate according to the STAI X-2 (57.33 ± 9.98; refer to Figure S1 for the scores and their clinical implications). Patients were found to have severe depression (BDI II, 25.78 ± 12.04) at baseline whereas anger-related scores were relatively low. LOT-R scores were at a low level (11.81 ± 4.04) indicating a low level of optimism, expectancy, or outlook on life. Regarding life satisfaction, at baseline the participants showed a high level of motivation toward achieving life satisfaction (LSMS, 30.24 ± 3.97), while the level of satisfaction regarding their future life expectations was moderate (LSES, 21.63 ± 7.15). However, the level of satisfaction with their current situation was low (SWLS, 15.31 ± 5.89). The QoL scores were close to optimal, with an EQ-VAS score of approximately 50 and EQ-5D score of approximately 0.75.
Most of the six anxiety-related domains showed positive improvements after 4 weeks of treatment, with the exception of the factor anger control (AXI-K-C) in the anger dimension. The greatest statistically significant improvement was found for anxiety levels by 22.5,14.6, and 9.6% in terms of BAI, STAI X-1, and STAI X-2 scores, respectively, from baseline. Further improvements were observed for depression (BDI II, 11.4%, p<0.001), life satisfaction (LSES, 6.2%, p=0.003), and QoL (EQ-5D, 8.4%, p<0.001; EQ-VAS, 11.9%, p<0.001). Of the five anger-related dimensions, both internal (5.0%) and external (3.0%) anger expression showed significant improvement (p=0.012 and 0.047, respectively).
Improvements in clinical outcomes were found in both men and women with similar patterns (Table S3). Regarding anger, an improvement of 5.5% (p=0.022) was observed in how men expressed their anger (AXI-K-O), whereas women showed a significant enhancement in managing their suppressed anger (AXI-K-I) with a 5.6% increase (p=0.046). The results also showed that men had a statistically significant improvement in the LSES (7.9%, p=0.019; Table S3).
3.2. Relationships between Anxiety-Relevant Measurement Scales
Figure 1 presents the interrelationship values among outcome measurement scales for anxiety disorders. Anxiety indicators demonstrated greater correlations (ρ=0.43–0.75) with one another and strong relationships with anger and depression indicators such as STAXI-T (ρ=0.51–0.56) and BDI II (ρ=0.44–0.57). QoL indicators (EQ-5D and EQ-VAS) had a low or moderate correlation with anxiety parameters. For example, EQ-VAS scores had the strongest correlations with STAI X-I (ρ=-0.29) and BAI (ρ=-0.22) scores for anxiety and STAXI-S (ρ=-0.23) score for anger among all examined parameters. The QoL variables showed a greater level of similarity with the measures of anger expression (AXI-K-O) and anger control (AXI-K-C), according to the results of the multidimensional scaling analysis (Supplementary Figure S3). Likewise, life satisfaction parameters (SWLS, LSES, and LSMS) were similar to those of optimism (LOT-R; Figure S3).
Only correlation coefficients ≥0.4 are indicated in the plot.
3.3. Costs of Traditional Korean Medicine Treatment for Patients with Anxiety
During the 4 weeks of treatment, patients visited KM clinics approximately five times (mean, 5.1; range, 2–9). When the observation period was expanded to 12 weeks (36 patients), the mean number of visits was 11.2 (range, 4–22). The medical costs incurred for the treatment of anxiety disorders in KM clinics can be divided into diagnostic and treatment categories (Figure 2). The diagnostic cost is a one-off cost incurred at the initial visit, and each item in the treatment cost is an average cost over the course of 4 or 8 weeks (Table S4). In 4 weeks, the medical costs amounted to 1,790,222 KRW (1,360 USD). Over the subsequent 8 weeks, the costs were decreased to 521,108 KRW (396 USD), representing a reduction of approximately 29% compared to the initial four-week period, as the relatively expensive herbal decoction prescription was given only to patients who required it after the 4 weeks of treatment (Figure 2). Assuming that the improvement in QoL resulting from 12 weeks of treatment was sustained for the following 40 weeks for a 1-year period, the ACER value was estimated to be 24,629,000 KRW/QALY (22,673 USD/QALY; Table 2).
The diagnostic cost is the one-time expense incurred during the initial visit, while each item of treatment cost represents the average cost over a four-week or eight-week period. 1 USD = 1,086.3 KRW (2020).
ACER, average cost-effectiveness ratio; EQ-5D, Euro Quality of Life 5 Dimensions utility score; KM, Korean medicine; KRW, South Korean won; QALY, quality-adjusted life year.
This result was based on bootstrapping analysis. The cost obtained from the medical records was the treatment cost for a period of 12 weeks. 1 USD = 1,086.3 KRW (2020).
4. Discussion
Our results demonstrated the KM approach to be effective in enhancing clinical outcomes and QoL in patients with anxiety disorders in real-world clinical settings. In our analysis of the results of the effects of KM (acupuncture, KM psychotherapy, Chuna therapy, aromatherapy, and herbal medicine) for over 4 weeks, there were improvements not only in anxiety but also in depression and anger, along with an increase in the QoL. It was also calculated that 24,629,000 KRW was needed to improve 1 QALY over a 12-week period.
Among previous studies, only two previous randomized controlled trials (RCTs) have shown that KM modalities such as acupuncture and herbal medicine had a positive impact on both the clinical outcomes and the QoL in patients with anxiety [20,21]. A meta-analysis that included 20 RCTs showed that acupuncture was more effective than conventional treatments in reducing anxiety symptoms, with a standard mean effect size of -0.41 (p<0.0001) [21]. Herbal medicine, Gamisoyo-San, for 8 weeks showed a significant 12% increase (p=0.021) in the QoL (WHOQOL-BREF scores) compared with the placebo-treated control group in patients diagnosed with GAD in Korea [20]. However, KM typically refers to treatment care that provides and applies several types of treatments such as acupuncture and herbal medicines in entirety and does not provide only a single therapy in the field.
Therefore, to understand the actual value of KM for anxiety disorders, the outcomes need to be examined in on-site practice rather than in an experimental setting that compares treatment arms confined to single or dual remedies. Two herbal medicines, Gami-ondam-tang and Gami-guibi-tang were provided and incorporated in the 4-week KM treatment course in the present study. While the effectiveness was not driven only by the contribution of herbal medicine, the percentage improvement of QoL (8.4% (p<0.001) on the EQ-5D and 12% (p<0.001) on the EQ-VAS) was similar to the results for Gamisoyo-San in the aforementioned study [20].
Recent research has recognized the effectiveness of holistic approaches in the treatment of mental disorders [30,31,32]. Holistic therapy considers the patient’s physical, mental, and spiritual health on the whole rather than focusing on symptoms. This type of medicine combines natural and alternative therapies to provide powerful healing benefits with fewer side effects compared with conventional treatment [33]. Holistic approaches have been shown to reduce anxiety and depressive symptoms in adolescents and mothers, who are more likely to experience anxiety disorders [30,31]. Therefore, holistic therapy is thought to effectively alter several anxiety-related indicators such as QoL not only in patients with mild symptoms but also in those with sociopsychological vulnerabilities [34]. Furthermore, the Korean Medicine Clinical Practice Guidelines recommends conducting screening tests at the first visits of patients with anxiety disorders and providing KM treatments utilizing herbal medicine, acupuncture, and KM psychotherapy based on the patient's pattern or disease progression [35]. KM offers a holistic approach to health and well-being, recognizing the importance of balance and harmony in maintaining well-being rather than viewing the body as a collection of separate parts to be treated separately [36,37]. By integrating the various modalities of herbal medicine, acupuncture, aromatherapy, and psychotherapy, it is possible to holistically improve a patient’s QoL.
Our research revealed that the treatment of anxiety resulted in improvements not only in anxiety symptoms but also in those of anger and depression. Anxiety disorders generally precede the onset of depressive disorders, and anxiety and depression often develop together [38,39]. Changes in neural circuits— specifically in the prefrontal-limbic pathways that govern emotional regulation— are a shared feature of both anxiety and depressive disorders [40]. Anger and anxiety, both stress-related emotions, often coexist due to shared psychological mechanisms, such as intolerance of uncertainty or anxiety sensitivity and reactions to perceived threats [41]. As reported in the Netherlands Study of Depression and Anxiety, 67% of patients with a primary diagnosis of depression also had concurrent anxiety disorders. Similarly, 63% of patients with primary anxiety disorder are also affected by depression [42]. As approximately one-third (29–32%) of patients with anxiety disorders experience anger attacks [43], anxiety, anger, and depression are not only interrelated but also influence QoL and life satisfaction [15,17,44]. Therefore, when measuring the effectiveness of anxiety treatment, it is crucial to evaluate these associated conditions of anxiety. In our study, a significant improvement in the clinical symptoms common to anxiety and depressive disorders was observed, which shows that KM treatment was generally effective in addressing mental health conditions in patients. This improvement also has an overall impact on QoL, which can be interpreted as a positive factor for economic evaluation indicators. However, when we evaluated changes in anger expression (AXI-K), we found that anger suppression (AXI-K-I) and anger expression (AXI-K-O) were decreased after 4 weeks of treatment, while anger control (AXI-K-C) did not change significantly between the beginning and end of the treatment. This suggests that the treatment had a positive effect on anger suppression and anger expression, which are simpler and emotion-driven aspects of anger but did not yield significant changes in anger control, a more complex aspect that involves social skills. This treatment process may have limitations that prevent it from fundamentally addressing anger arising from the overall difficulty of living with anxiety. In addition, the correlation with QoL indicators was higher for anger than for anxiety, suggesting that anger acts as an extended secondary emotional problem of anxiety and has a negative impact on one’s overall life.
While KM has been considered to bring greater clinical and holistic benefits, especially for individuals with mental illness, its usage remains relatively low in Korea. In our comparison of the utilization of KM and WM in patients diagnosed with anxiety from the 2013 National Health Insurance Service sample cohort of Korea, of the 7,811 patients with anxiety, only 2% (n=151) visited KM clinic. The limited use of KM for anxiety care could be attributed to two main factors. First, KM clinics specializing in neuropsychiatry are not prevalent; in 2022, only 24 out of 15,095 KM clinics in Korea were specialized in KM neuropsychiatry. Moreover, the active KM medicine doctors having a board-certified specialty in neuropsychiatry (with the title KMNPS) are relatively few (n=300, about 1.25% of KM doctors) [45]; additionally, several items of KM treatments such as herbal medicine or aromatherapy are not covered by National Health Insurance scheme and need to be paid for out-of-pocket. In this study, the average out-of-pocket cost was 76% of the total cost over 4 weeks, which could prevent low-income or elderly patients from the access to KM service.
Despite its significance, our study has some limitations. First, because it was an case series study with no comparison group, our results may overestimate the effect of KM on anxiety disorders. Nevertheless, the estimates from real-world data are meaningful by reflecting the actual clinical practice. Second, the treatment regimen given in this study was not precisely defined due to variations in regimen (duration of treatment, type of herbal medicine, etc.) across patients. As aforementioned, KM was transferred to each patient in a customized and personalized regimen according to patient symptoms. Thus, it is difficult to formulate a universal treatment regimen that could be offered to any patient with an anxiety disorder in the context of KM. Third, while this study is the first to provide ACER values for KM treatment in real-world settings for patients with anxiety disorders, an incremental cost-effectiveness ratio value could not be estimated in the present study. Future comparative studies with antidepressants and anti-anxiety medications traditionally used to treat anxiety disorders may complete the cost-effectiveness of KM. Finally, a relatively short period of 12 weeks was observed to estimate QALYs in the present study. Thus, further studies are needed to investigate long-term clinical and QoL outcomes as long as the cost-effectiveness of KM compared to conventional treatments for anxiety disorder.
5. Conclusions
Our retrospective case series study demonstrates that KM, which includes acupuncture, herbal medicine, and psychotherapy, can effectively treat patients with anxiety disorders, leading to significant improvements in both clinical symptoms and QoL. Furthermore, our cost analysis revealed that KM may be a cost-effective treatment option for individuals with anxiety disorders. In light of the findings, policymakers may wish to expand the insurance benefits to KM therapies such as herbal medicine or aromatherapy to improve the efficiency of treatment and health outcomes in patients with anxiety disorders.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Figure S1: Psychological and health-related quality of life measures; Figure S2: Flowchart of the study; Table S1: Detailed description of anxiety-related scales; Table S2: Detailed description of anxiety-related scales; Table S3: The difference of outcomes for post treatment of 4 weeks between males and female; Table S4: The unit or cost of Korean Medicine for patients for 4 weeks and 12 weeks (KRW).
Author Contributions
Conceptualization, S.-Y.L.; methodology, S.-Y.L.; validation, S.-I.L. and J.-E.L.; formal analysis, S.-I.L. and J.-E.L.; investigation data curation, J.-H.Y. writing—original draft preparation, S.-Y.L. and J.-E.L.; writing—review and editing visualization, G.-W.K. and E.C.; supervision, E.C.; project administration, G.-W.K.; funding acquisition, G.-W.K. and E.C. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Traditional Korean Medicine R&D Project, Ministry of Health & Welfare, Republic of Korea [Grant number: HB16C0021] and by grants from the Korean Institute of Oriental Medicine [Grant number: KSN20224113].
Institutional Review Board Statement
This study was approved by the Institutional Review Board of Sookmyung Women's University (SMWU-2009-HR-081).
Informed Consent Statement
Owing to the retrospective study, the need for patient consent was waived by the IRB.
Data Availability Statement
The data that support the findings of this study are available within the article.
Acknowledgments
We would like to thank Editage (www.editage.co.kr) for English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV; Washington, DC: 1994; Volume 4.
- Bandelow, B.; Michaelis, S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin Neurosci 2015, 17, 327–335. [Google Scholar] [CrossRef]
- Nepon, J.; Belik, S.L.; Bolton, J.; Sareen, J. The relationship between anxiety disorders and suicide attempts: Findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety 2010, 27, 791–798. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Dattani S; Rodés-Guirao L; Ritchie H; M, R. Mental Health. Available online: https://ourworldindata.org/mental-health (accessed on May 8).
- Seo, S.I.; Choi, S.Y.; Kim, E.J.; Koo, B.S.; Hyo, W.J.; Lee, G.H.; Kim, G.W. Patterns of Integrative Korean Medicine Practice for Anxiety Disorders: A Survey among Korean Medicine Doctors (KMDs) in Korea. Evid Based Complement Alternat Med 2020, 2020, 3140764. [Google Scholar] [CrossRef] [PubMed]
- Unützer, J.; Klap, R.; Sturm, R.; Young, A.S.; Marmon, T.; Shatkin, J.; Wells, K.B. Mental disorders and the use of alternative medicine: Results from a national survey. Am J Psychiatry 2000, 157, 1851–1857. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Soukup, J.; Davis, R.B.; Foster, D.F.; Wilkey, S.A.; Van Rompay, M.I.; Eisenberg, D.M. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry 2001, 158, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Shih, C.C.; Cheng, H.C.; Kwon, S.H.; Kim, H.M.; Lim, B.M. A comparative study of the traditional medicine systems of South Korea and Taiwan: Focus on administration, education and license. Integr Med Res 2021, 10, 100685. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Koo, M.S. Modern psychiatric understanding of the psychopathology of psychosis in oriental medicine. J Korean Neuropsychiatric Assoc 2010, 508–515. [Google Scholar]
- Herman, P.M.; Poindexter, B.L.; Witt, C.M.; Eisenberg, D.M. Are complementary therapies and integrative care cost-effective? A systematic review of economic evaluations. BMJ open 2012, 2, e001046. [Google Scholar] [CrossRef]
- Natioanl Center for Complementary and Integrative Health. Complementary, Alternative, or Integrative Health: What’s In a Name? Available online: https://www.nccih.nih.gov/health/complementary-alternative-or-integrative-health-whats-in-a-name (accessed on May 9).
- Leichsenring, F.; Steinert, C.; Rabung, S.; Ioannidis, J.P.A. The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: An umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry 2022, 21, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kang, M.J.; Lim, J.H.; Seong, W.Y. A review study in treatment for anxiety disorder in traditional chinese medicine. J Orient Neuropsychiatry 2012, 23, 1–12. [Google Scholar] [CrossRef]
- Brenes, G.A. Anxiety, depression, and quality of life in primary care patients. Prim Care Companion J Clin Psychiatry 2007, 9, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Reheiser, E.C. Assessment of emotions: Anxiety, anger, depression, and curiosity. Appl Psychol Health Well Being 2009, 1, 271–302. [Google Scholar] [CrossRef]
- Wilmer, M.T.; Anderson, K.; Reynolds, M. Correlates of quality of life in anxiety disorders: Review of recent research. Curr Psychiatry Rep 2021, 23, 77. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, G.M. The overlap between anxiety, depression, and obsessive-compulsive disorder. Dialogues Clin Neurosci 2015, 17, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Deschênes, S.S.; Dugas, M.J.; Fracalanza, K.; Koerner, N. The role of anger in generalized anxiety disorder. Cogn Behav Ther 2012, 41, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Park, D.M.; Kim, S.H.; Park, Y.C.; Kang, W.C.; Lee, S.R.; Jung, I.C. The comparative clinical study of efficacy of Gamisoyo-San (Jiaweixiaoyaosan) on generalized anxiety disorder according to differently manufactured preparations: Multicenter, randomized, double blind, placebo controlled trial. J Ethnopharmacol. 2014, 158, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.Y.; Yang, N.B.; Huang, F.F.; Ren, S.; Li, Z.J. Effectiveness of acupuncture on anxiety disorder: A systematic review and meta-analysis of randomised controlled trials. Annals of general psychiatry 2021, 20, 9. [Google Scholar] [CrossRef] [PubMed]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). Br J Clin Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J Consult Clin Psychol. 1988, 56, 893. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D. State-Trait anger expression inventory. The Corsini encyclopedia of psychology 2010, 1–1. [Google Scholar] [CrossRef]
- Chon, K.K.; Hahn, D.W.; Lee, C.H.; Spielberger, C.D. Korean adaptation of the state-trait anger expression inventory: Anger and blood pressure. The Korean journal of health psychology 1997, 2, 60–78. [Google Scholar]
- Arnau, R.C.; Meagher, M.W.; Norris, M.P.; Bramson, R. Psychometric evaluation of the Beck Depression Inventory-II with primary care medical patients. Health Psychol. 2001, 20, 112. [Google Scholar] [CrossRef] [PubMed]
- Bastianello, M.R.; Pacico, J.C.; Hutz, C.S. Optimism, self-esteem and personality: Adaptation and validation of the Brazilian version of the Revised Life Orientation Test (LOT-R). Psico-USF 2014, 19, 523–531. [Google Scholar] [CrossRef]
- Kim, J.H. The relationship between life satisfaction/life satisfaction expectancy and stress/well-being: An application of motivational states theory. The Korean Journal of Health Psychology 2007, 12, 325–345. [Google Scholar] [CrossRef]
- Jarow, J.P.; LaVange, L.; Woodcock, J. Multidimensional evidence generation and FDA regulatory decision making: Defining and using “real-world” data. JAMA 2017, 318, 703–704. [Google Scholar] [CrossRef] [PubMed]
- Ainur, S.; Herawati, L.; Widyawati, M.N. The benefits of holistic therapy for psychological disorders in postpartum mother: A systematic review. STRADA Jurnal Ilmiah Kesehatan 2020, 9, 1708–1717. [Google Scholar] [CrossRef]
- Rentala, S.; Lau, B.H.P.; Aladakatti, R.; Thimmajja, S.G. Effectiveness of holistic group health promotion program on educational stress, anxiety, and depression among adolescent girls–A pilot study. J Family Med Prim Care 2019, 8, 1082–1089. [Google Scholar] [CrossRef] [PubMed]
- Becker, B.J. A holistic approach to anxiety and stress. Am J Psychoanal 1976, 36, 139–146. [Google Scholar] [CrossRef]
- Papathanasiou, I.; Sklavou, M.; Kourkouta, L. Holistic nursing care: Theories and perspectives. Am J Nurs Sci 2013, 2, 1–5. [Google Scholar] [CrossRef]
- National Center for Mental Health. National Mental Health Survey 2021. Available online: https://mhs.ncmh.go.kr/front/en/infographic.do?category=1&%20category_en%20=%20The%20Survey%20of%20Mental%20disorder%20in%20Korea%202021 (accessed on August 8).
- National Institute for Korean Medicine Development. Manual for developing Evidence-based Clinical Practice Guideline of Korean Medicine. Available online: https://nikom.or.kr/board/boardFile/download/24/23541/28224.do (accessed on August 8).
- Yin, C.S.; Ko, S.G. Introduction to the history and current status of evidence-based Korean medicine: A unique integrated system of allopathic and holistic medicine. Evid Based Complement Alternat Med 2014, 2014, 740515. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Pham, D.D. Sasang constitutional medicine as a holistic tailored medicine. Evid Based Complement Alternat Med 2009, 6, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Wang, P.S. The descriptive epidemiology of commonly occurring mental disorders in the United States. Annu. Rev. Public Health 2008, 29, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Dunner, D.L. Management of anxiety disorders: The added challenge of comorbidity. Depress Anxiety 2001, 13, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Etkin, A.; Schatzberg, A.F. Common abnormalities and disorder-specific compensation during implicit regulation of emotional processing in generalized anxiety and major depressive disorders. Am J Psychiatry 2011, 168, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.S.; Schmidt, N.B. The role of anxiety sensitivity in anger symptomatology: Results from a randomized controlled trial. J Anxiety Disord 2021, 83, 102462. [Google Scholar] [CrossRef]
- Lamers, F.; van Oppen, P.; Comijs, H.C.; Smit, J.H.; Spinhoven, P.; van Balkom, A.J.; Nolen, W.A.; Zitman, F.G.; Beekman, A.T.; Penninx, B.W. Comorbidity patterns of anxiety and depressive disorders in a large cohort study: The Netherlands Study of Depression and Anxiety (NESDA). J Clin Psychiatry 2011, 72, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Gould, R.A.; Ball, S.; Kaspi, S.P.; Otto, M.W.; Pollack, M.H.; Shekhar, A.; Fava, M. Prevalence and correlates of anger attacks: A two site study. J Affect Disord 1996, 39, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Mamani-Benito, O.; Esteban, R.F.C.; Castillo-Blanco, R.; Caycho-Rodriguez, T.; Tito-Betancur, M.; Farfán-Solís, R. Anxiety and depression as predictors of life satisfaction during pre-professional health internships in COVID-19 times: The mediating role of psychological well-being. Heliyon 2022, 8, e11025. [Google Scholar] [CrossRef] [PubMed]
- Health Insurance Review & Assessment Service. Healthcare bigdata Hub. Available online: https://opendata.hira.or.kr/op/opc/olapHumanResourceStatInfoTab1.do (accessed on May 4).
Figure 1.
Correlation plot for the improvement in measurement scores over 4 weeks.
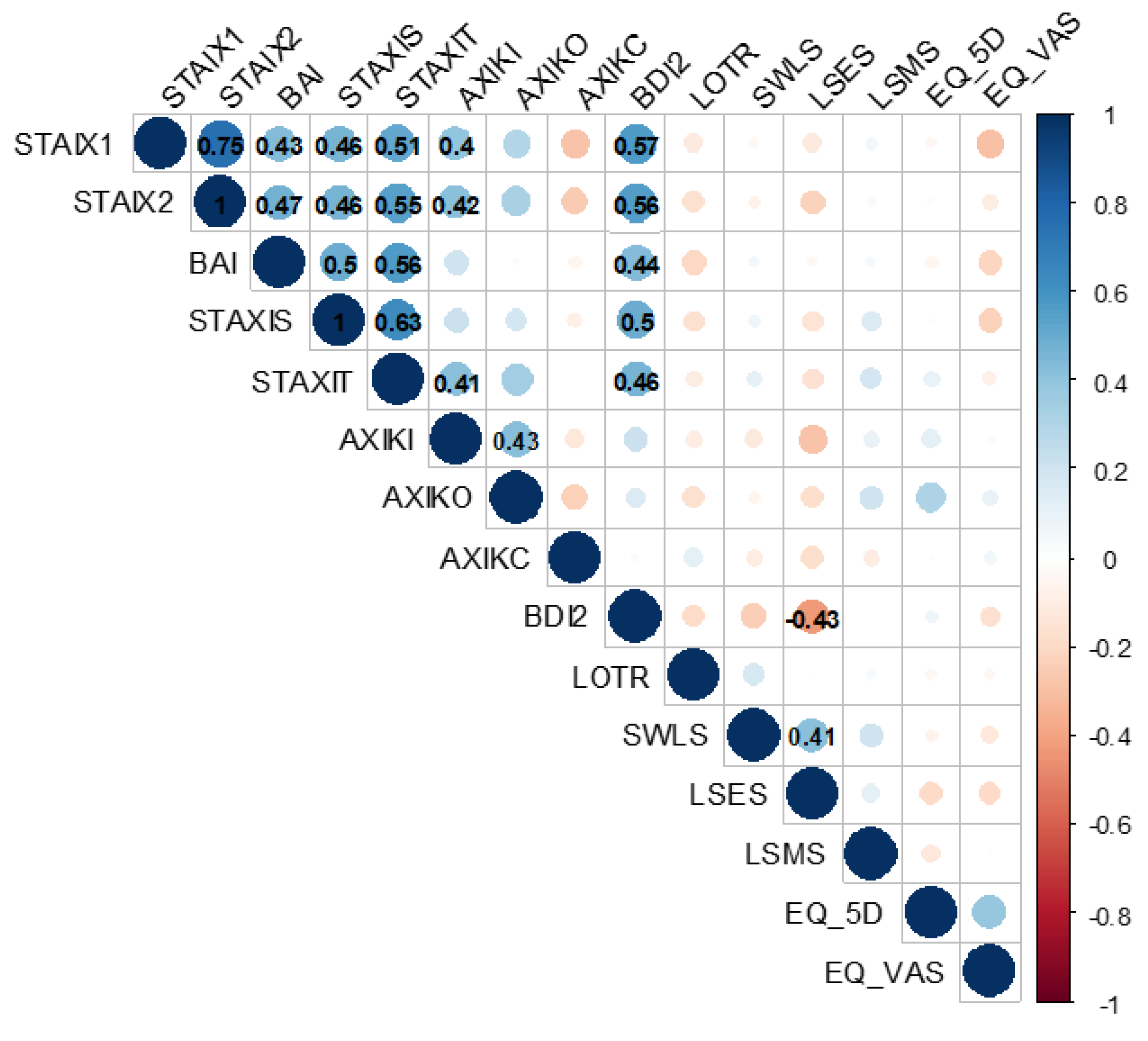
Figure 2.
Average cost by Korean medicine treatment item in patients with anxiety disorders for 4 and 12 weeks.
Figure 2.
Average cost by Korean medicine treatment item in patients with anxiety disorders for 4 and 12 weeks.
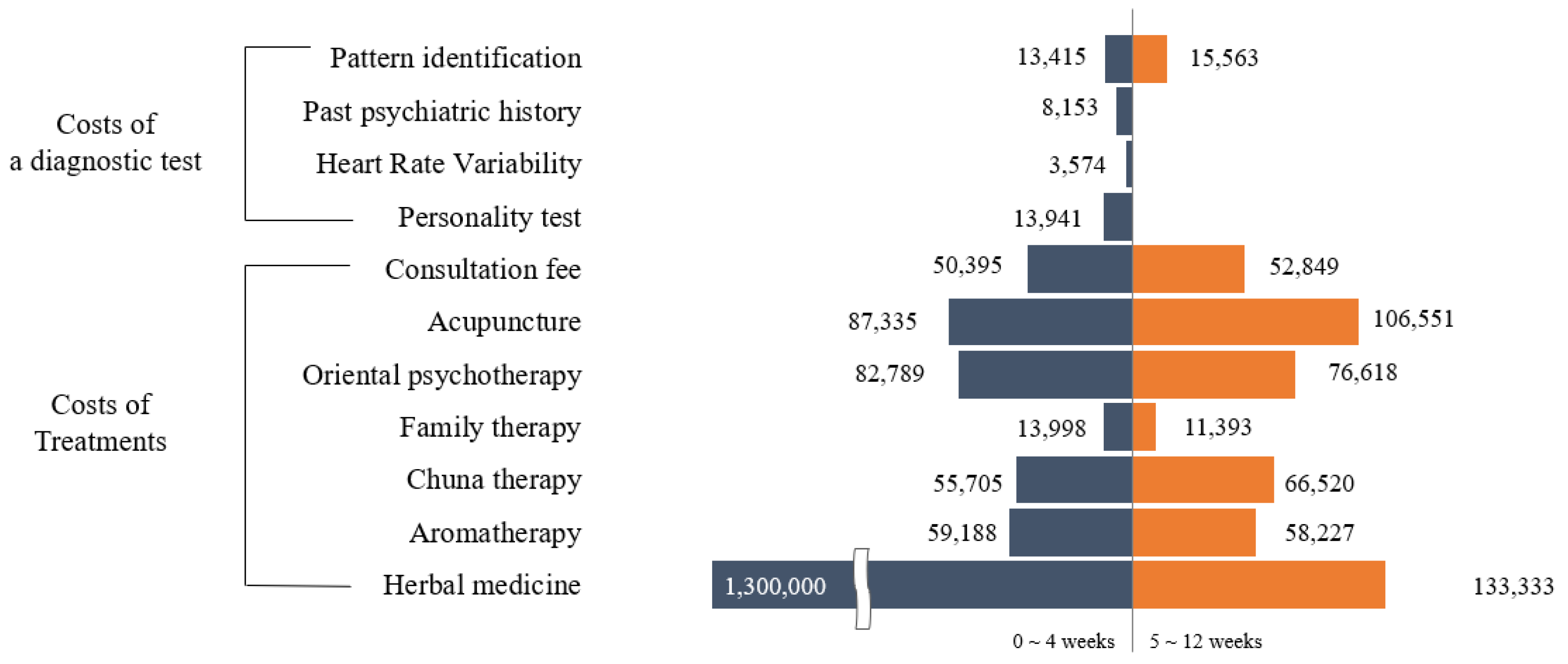

Table 1.
Changes in clinical outcomes over 4 weeks in patients with anxiety disorder (n=67).
| Range |
Baseline mean (SD) |
After 4 weeks mean (SD) | Improvement from baseline (%) | p-value | |
| Anxiety | |||||
| STAI X-1# | 20–80 | 59.24 (9.55) | 50.48 (12.67) | 14.6 | <0.001*** |
| STAI X-2# | 20–80 | 57.33 (9.98) | 51.57 (11.77) | 9.6 | <0.001*** |
| BAI# | 0–63 | 28.15 (12.74) | 18.72 (13.47) | 22.5 | <0.001*** |
| Anger | |||||
| STAXI-S# | 10–40 | 16.39 (7.28) | 15.33 (7.43) | 3.5 | 0.135 |
| STAXI-T# | 10–40 | 20.30 (7.22) | 19.48 (6.79) | 2.7 | 0.237 |
| AXI-K-I# | 8–32 | 18.22 (5.29) | 17.01 (5.28) | 5.0 | 0.012*** |
| AXI-K-O# | 8–32 | 14.31 (5.17) | 13.58 (5.48) | 3.0 | 0.047*** |
| AXI-K-C | 8–32 | 21.70 (5.12) | 21.61 (4.78) | -0.4 | 0.817 |
| Depression | |||||
| BDI II # | 0–63 | 25.78 (12.04) | 18.6 (13.8) | 11.4 | <0.001*** |
| Optimism | |||||
| LOT-R | 6–30 | 11.81 (4.04) | 12.63 (3.70) | 3.4 | 0.016*** |
| Satisfaction | |||||
| LSMS | 5–35 | 30.24 (3.97) | 30.25 (4.20) | 0.1 | 0.975 |
| SWLS | 5–35 | 15.31 (5.89) | 15.58 (5.72) | 0.9 | 0.556 |
| LSES | 5–35 | 21.63 (7.15) | 23.48 (7.32) | 6.2 | 0.003*** |
| Quality of life | |||||
| EQ-5D | 0–1 | 0.75 (0.17) | 0.83 (0.14) | 8.4 | <0.001*** |
| EQ-VAS | 0–100 | 49.54 (22.96) | 61.39 (21.11) | 11.9 | <0.001*** |
AXI-K-C, Anger Expression Inventory Anger-Control; AXI-K-I, Anger Expression Inventory Anger-In; AXI-K-O, Anger Expression Inventory Anger-Out; BAI, Beck Anxiety Inventory; BDI II, Beck Depression Inventory-II; EQ-VAS, EuroQoL Visual Analog Scale; EQ-5D, Euro Quality of Life 5 Dimensions utility score; LOT-R, The Revised Life Orientation Test; LSES, The Life Satisfaction Expectancy Scale; LSMS, The Life Satisfaction Motivation Scale; PD, panic disorder; SD, standard deviation; STAI, State-Trait Anxiety Inventory, axis1 (X-1, State), axis2 (X-2, Trait); STAXI-S, State-Trait Anger Expression Inventory State Anger; STAXI-T, State-Trait Anger Expression Inventory Trait Anger; SWLS, The Satisfaction with Life Scale.# A lower score indicates a higher degree of symptoms. *** p<0.05.
Table 2.
Average cost-effectiveness ratio of Korean medicine for patients with anxiety.
| Medical expenditure | Quality of life | QALY | ACER (KRW/QALY) | |
|---|---|---|---|---|
| Insured | Paid by patients | ΔEQ-5D | ||
| 679,000 | 1,632,000 | 0.10 | 0.0938 | 24,629,000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



