
Submitted:
09 May 2024
Posted:
09 May 2024
You are already at the latest version
Abstract
Maternal diet plays a significant role in the fatty acid composition of breast milk. Natural trans fatty acids (TFAs) are generated through the biohydrogenation of unsaturated fatty acids (FAs) in the rumen of animals by bacterial isomerases and are consequently found in milk, dairy products, and meat from ruminant animals. Dietary products such as milk and meat are the primary sources of natural TFAs for humans, derived from rumen fermentations. These peculiar fatty acids hold nutritional significance as they not only lack the detrimental effects on endothelium characteristic of industrially produced trans fat, but also exhibit anti-inflammatory properties. The relationship between the presence in breast milk of eight fatty acids (including natural TFAs trans-vaccenic and conjugated linoleic acid) and maternal diet has been explored, and their abundance has been compared to that of infant formulas. Two cohorts of lactating women participated in this study, originating from a Spanish region adhered to the Southern European Atlantic Diet or Atlantic Diet. While the consumption of conventional meat or dairy products does not seem to increase the abundance of trans fatty acids in breast milk, trans-vaccenic and oleic acid are among the most distinctive features of breast milk fat in mothers consuming naturally improved dairy products, with an improved fatty acid profile. The most significant differences between natural breastfeeding and formula feeding lie in natural trans fatty acids, since formula are notably deficient, while overfortified in alpha-linolenic acid in comparison to breast milk.
Keywords:
Breast milk
; Human milk
; SEAD
; Atlantic diet
; Trans-vaccenic acid
; Trans fatty acid
1. Introduction
Breastfeeding is a biological process that protects the neonate from malnutrition or even infectious diseases. Health benefits of breastfeeding for mother and baby are substantial and widely recognized worldwide. Human milk has been described as the gold standard of infant nutrition and serves as a valuable reference for establishing optimal nutrient intakes for infants who are unable to exclusively breastfeed [1]. For this reason, the composition of infant formulas should closely resemble that of breast milk [2]. The fatty acids (FA) found in breast milk have been attributed to two distinct origins: (a) the release of fatty acids from external sources and (b) the de novo synthesis of fatty acids in the liver or mammary tissue. In this sense, a previous study by Barreiro et al. has underscored the significant impact of maternal diet on the fatty acid composition of breast milk[3].
Trans fatty acids (TFA) such as elaidic acid (trans-9-C18:1) are typical of industrially hydrogenated vegetable fats and often present in large quantities in commercial foods such as margarines and cakes [4]. They promote the endothelial dysfunction and appear to negatively affect health by increasing the risk of diseases of the circulatory system and type 2 diabetes [5]. These TFA can also have a harmful effect on the development of babies, leading to lower levels of certain fatty acids (FA) important for normal brain and vision development such as arachidonic acid (AA) and docosahexaenoic acid (DHA) [6].
Another type of TFA can be naturally found in some foods. For example, natural TFAs are generated by biohydrogenation of unsaturated FAs in the rumen of animals by bacterial isomerases and are therefore found in milk, dairy products, and meat of these ruminant animals. Dominant TFA from natural food sources are trans-vaccenic acid (TVA) (trans-C18:1 n-7), trans-palmitoleic acid (TPA), also known as trans-C16:1 n-7 or trans-9 C16:1 and conjugated linoleic acid (CLA) (main isomer—rumenic acid, C18:2 n9c, n11t). These natural TFAs have nutritional significance. Not only they do not seem to have this dysfunctional effect on the endothelium but also exhibit anti-inflammatory properties [7]. In 2023 [8], it was reported that one of those natural TFA, dietary TVA, could promote cytotoxic and tumor infiltrating functions of effector CD8+ T cells, leading to greater antitumor immunity in vivo. In this article [8]through a comprehensive evaluation of this nutrient derived from the diet. progress is made in the identification and understanding of the mechanistic links between diet and human physiology and pathology. Also, TPA has been recognized in prior epidemiological prospective studies as a biomarker indicative of metabolic health [9,10].
Dietary products such as milk and meat are the main sources of trans fatty acids for humans, derived from rumen fermentations. Intake of these fatty acids is exclusively ensured by ruminant-derived foods as milk and dairy products and meat [11]. TVA is the major trans-C18:1 isomer in ruminant dairy fat [12]. Guillocheau et al. findings suggest that endogenous 16:1 t9 TPA is not exclusively derived, as it has been previously assumed, from the diet, but it may also be produced by partial β-oxidation of dietary TVA [11]. In particular, the dietary pattern of northern Portugal and Galicia (northwest Spain), known as Southern European Atlantic Diet (SEAD) or Atlantic Diet (AD), is characterized by high consumption of milk and dairy products and moderate consumption of meat [13,14,15].
The FA secreted in human milk have different origins: de novo synthesis in the breast and maternal diet or body stores [16]. Additionally, FA from maternal diet can interact directly or indirectly with some transcription factors that would eventually produce changes in the composition of milk [7]. The scientific community agrees that the human body cannot synthesize trans fatty acids (TFA), although some studies indicate that vaccenic acid can be converted to rumenic acid by Δ9-desaturase in the maternal gland during lactation [17]. Therefore. the trans fatty acid composition of breast milk will be predominantly affected by maternal diet [18].
Higher levels of the ruminal CLA isomer and its precursor TVA in breast milk correlate with lower rates of atopic manifestations in children. Perhaps because these natural TFAs modulate immune function in the human body by reducing the production of pro-inflammatory mediators [19,20].
In previous studies with Galician lactating women, it was found that many of them adhere to the Atlantic diet and factors such as maternal diet and prolonged lactation influence the lipid profile of human milk [21,22].
In the present work we will discuss the relationship between the presence of natural eight FA (including natural TFA TVA and CLA), the adherence of Galician mothers to the healthy dietary pattern SEAD, the consumption of milk and dairy products (conventional or from improved production) and bovine meat, in addition to other factors such as the duration of lactation. A comparison of breast milk with FA levels found in infant formulas available in the Spanish market is also included.
2. Materials and Methods
2.1. Samples
This is an observational cross-sectional design study, involving lactating mothers residing in the northwest of Spain (Galicia). The population in this region is adhered to a dietary pattern known as the SEAD, characterized by frequent consumption of milk, dairy products, and beef [13].
- Cohort 1
Milk sampling, and data collection were carried out using convenience sampling in collaboration with the midwifery service and a local breastfeeding association. The study was registered on ClinicalTrials.gov under the identification number NCT03245697, Ethical approval for this study was granted by the Clinical Research Ethics Committee of Galicia (approval code 2016/280), and it adhered to the principles of the 1975 Declaration of Helsinki, revised in 1983. Informed written consent was obtained from all participants. Mothers collected human milk samples at home, extracting approximately 25 ml of milk manually or using a breast pump before breastfeeding the child. The samples were collected in sterile plastic tubes, stored between 3 and 5 °C and delivered to the laboratory within 12 hours where they were preserved at-24ºC. All samples were collected before the first morning feed or two hours after the last session when the child breastfed at night [12]. Breast milk samples from 93 lactating women were utilized. Mothers were interviewed and preselected based on the following exclusion criteria: mothers with acute or chronic illnesses, those with metabolic disorders, gestation of less than 36 weeks, and substance abuse (drugs or alcohol). All babies were healthy and growing well. Lactating women were surveyed for personal data, including age, medications, tobacco use, anthropometric data (body weight, height, and BMI), childbirth (delivery date, natural or cesarean section, and gender), and breastfeeding (duration in months after childbirth). Additionally, mothers were queried about their dietary habits (dairies and bovine meat foods). Furthermore, the 9-item brief questionnaire (SEAD) was used to assess adherence to the diet [15,23]. None of the mothers were taking dietary supplements like vitamins, iron, or fish oil at the time of sample collection.
- Cohort 2
The study incorporated breast milk samples from 16 mothers who consumed dairy products from improved milk, as part of a project approved by the Clinical Research Ethics Committee of Galicia (approval code 2010/027). The samples were collected from these women once month between 1 and 5 months postpartum, resulting in a total of 66 milk samples from the 16 participants, with colostrum being excluded. The volunteers collected the milk via manual extraction, and the samples were stored at −24°C until further analysis. Throughout lactation, the mothers consumed an average of 3 daily servings of milk, yoghurt, and butter from a premium brand of UHT milk produced in Galicia called UNICLA. The diet of UNICLA dairy cattle includes a significant amount of flax seeds, which is a source of unsaturated fatty acids such as omega-3. and selenized yeast, as a source of organic selenium [24]. An overview of UNICLA® milk composition and differential comparison to conventional milk can be found in the literature [25]
Each participant underwent a face-to-face interview and exclusion criteria were applied, including restrictions on diet, food intolerances, vegetarian or vegan diets, and non-consumption of major food groups outlined in the SEAD (fruits and vegetables, meat. eggs, milk and dairy products, fish, or cereals). The participating mothers were in good health, with no history of alcohol or substance abuse, non-smokers, and had no obstetric complications during pregnancy or delivery. None of the mothers were taking dietary supplements like vitamins, iron, or fish oil at the time of sample collection.
- Infant formula
Twenty-three infant formulas were collected in different commercial areas and pharmacies of Spain, including 5 first-stage formulas (intended for babies from 0 to 6 months of age), 13 follow-on infant formulas (intended for babies from 6 months on), and 5 growing-up milks (intended for young children), Samples were stored in the dark at −24 °C until analysis. The powdered formulas were reconstituted in water to obtain liquid formulas, following the manufacturer’s instructions, prior analysis.
2.2. Fatty Acid Determination
The qualitative and quantitative determination of the fatty acid composition of breast milk was conducted using the method described by Sanjulián et al. [26]. Fatty acid methyl esters were extracted with n-hexane and analyzed using a gas chromatography system (Agilent Technologies 6850) equipped with a flame ionization detector (GC-FID) in Palo Alto, CA, USA.
2.3. Statistics
GraphPad® Prism 10 version 10.2.2 (GraphPad Software, LCC, Dotmatics, UK) was used for statistical analysis and graphical representation. Unpaired Test t was used to determine the differences in fatty acids between lactation time, BMI, gender of infant, milk consumption, meat consumption and adherence to Atlantic diet. This test was also used to determine the differences in fatty acids between the two mother cohorts. One-way anova with pos-hoc Dunnet test was used to compare the differences between the mother cohort that intake naturally enriched in ruminal trans FA products and the other cohort of mothers and the infant formulas fatty acids. A p value <0.05 was used to consider the differences as statistically significant. Two principal component analysis (PCA) using a standardize method were carried out. One between the two cohorts and other including the cohorts and formula was performed.
3. Results and Discussion
3.1. Samples Data
3.1.1. TFA, Diet and Lactation Characteristics
- Cohort 1
A cohort of lactating women belonging to a cross-sectional observational study designed to investigate the composition of breast milk of lactating mothers residing in the northwest of Spain (Galicia) has been studied. Ninety-two lactating women, aged between 26 and 46, were recruited and they generously donated milk samples. The samples were collected between 1 and 59 months postpartum. [14,24]. All of mothers and children were healthy, only 9 women (12%) underwent a C-section delivery and 60% were primiparous. Data on gestation and on maternal and newborn characteristics are provided in Table 1. Continuous data are expressed as mean and standard deviation (SD). and categorical variables are expressed as percentages.
- Cohort 2
Sixteen lactating women, aged between 26 and 35, were recruited and they generously donated milk samples. The samples were collected between 1 and 5 months postpartum, with 13 women providing samples at month 4 and only 3 at month 5.
The mothers of cohort 2 consumed at least 3 servings a day of a type of premium milk produced in Galicia, UNICLA®.
3.1.2. TFA across Samples
A total of eight fatty acids were analyzed in all the samples, including oleic acid (OA), linoleic acid (LA), alfa-linolenic acid (ALA), arachidonic acid (AA), eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), trans-vaccenic acid (TVA) and CLA (cis-9,trans-11 CLA and trans-10,cis-12 CLA isomers). Table 2 displays the mean level of each fatty acid across different groups of samples, including lactation time (LT), body mass index (BMI), newborn sex, SEAD score, milk and meat consumption, naturally enriched in ruminal trans FA dairy products consumption, and infant formulas (FSF, FOF, GUF).
- Cohort 1
In the production of breast milk, some compounds, such as CLA or TVA, partly come from the mother's diet, while others are produced by the mother's body. Dietary products from ruminants (milk and meat) are the main sources of natural trans fatty acids for human consumers [26]. Several studies have examined the effect of CLA supplementation on the presence of natural trans FAs in breast milk, but little is known about their short-term transfer. Recent data suggest that concentrations of CLA and TVA in breast milk can be influenced by diet. It is recommended that the source of these FAs in the diet of breastfeeding women be natural products rather than dietary supplements [27,28]. Analysis of data from cohort 1 showed that, the FA fraction remained constant across groups, except for OA, the most abundant FA, for which significant differences were found based on maternal BMI (p=0.0210) and among women consuming more than 3 servings of meat per week (p=0.0157). Other authors have found a relationship between OA content and the nutritional status of mothers, specifically with undernutrition status. Although statistical tests did not find significant differences (p > 0.05) between the levels of oleic acid in breastfeeding mothers with chronic energy deficiency and those with normal nutritional status, in the study by Muhrifan [29] lower levels were found in women with chronic energy deficiency. However, the consumption of conventional meat or dairy does not appear to influence a higher abundance of trans fatty acids in breast milk.
- Cohort 1 versus cohort 2
The milk consumed by Cohort 2 is distinguished by its improved nutritional composition. achieved by modifying the cow's diet by incorporating high-quality forages and improving digestibility, instead of artificially altering the final product. The main components of the diet of dairy cows in Galicia consist of grass and corn silage, which farmers harvest and store and supply to livestock throughout the year, along with forage produced by Feiraco S.L. (cooperative of stockbreeders) as a supplement to improve the nutritional profile of the milk, the composition of the forage was modified. The objective was to provide a balanced and sufficient ration to dairy cattle, reproducing the fatty acid profile of spring pastures.
The type of cow milk production can affect its composition, which has been extensively studied in the case of lipid composition. Several studies have shown that cow milk from animals fed pasture or raised according to organic production guidelines [27,28,29] has higher contents of natural trans fatty acids than conventional milk. The hypothesis that the amount of CLA and TVA in breastfeeding women's milk could be increased by increasing the dietary amount of organic ruminant products has been studied in the Koala cohort [30]. In the milk of these mothers, the contents of CLA and its main precursor TVA increased when transitioning from a conventional diet to a moderately organic and strictly organic one. In the study by Simões-Wüst et al. [31], it was also demonstrated that the content of rumenic acid was higher in the breast milk of women who consumed a type of organic dairy product called biodynamic, compared to those consuming conventional or organic dairy products other than biodynamic, which was intermediate. Biodynamic organic farms consider, in addition to organic production guidelines, cosmic rhythms, which they believe result in improvements in plant and livestock production (http://www.demeter.net/). In the case of TVA, a profile comparable to that of CLA was found. Since TVA can be converted into rumenic acid in humans [32,33], it seems logical that their values are parallel. Again, the highest level of TVA was detected to a greater extent in the milk of women who consumed biodynamic dairy products, followed by the group of women who consumed other organic dairy products and the group of conventional dairy products. Although these differences were not statistically significant, the authors argue that the physiological importance of these apparently moderate differences should not be underestimated. In fact, in the studied cohort, an inverse correlation was already demonstrated between the levels of CLA in the milk of participating women and a pathological condition in their children (atopic diseases and eczema) [34].
In our cohort 1, samples were categorized into two groups based on lactation time (LT), as infants typically begin complementary feeding at 6 months. The early lactation group (< 6 months) was used for comparison with samples from cohort 2, which included mothers up to 5 months of lactation. The unpaired t-test results showed significant differences in the content of some fatty acids evaluated: The content of OA (p<0,0001), TVA (p<0,0001), and CLA (p<0,0055) is significantly higher in samples from cohort 2. This is consistent with the previous research findings explain above, that have linked the consumption of organic dairy products to an increase in the levels of these fatty acids in breast milk [30,31].
Principal component analysis (PCA) using a standardize method was carried out including the two cohorts. In Figure 1 a score scatter plot shows the existence of cohort-dependent features in the fatty acid profiles, as milk samples from woman who consumed CLA-enriched dairy products, cohort 2, are plotted relatively far from milk from cohort 1 subjects. In this sense, the loading plot shows that, TVA and OA, are among the most distinctive features of breast milk fat in cohort 2. Conversely, cohort 1 samples are scored lower for these two fatty acids.
- Breast milk versus infant formula
In a previous study by our research group [35], no significant differences were found in the fatty acid composition of formulas from different categories or stages, except for those enriched or fortified with specific fatty acids. In the same study, it was observed that during the first 6 months of lactation, breast milk had less oleic acid, being slightly more saturated than monounsaturated, and containing more LA, ALA, AA, and DHA than in the subsequent months of lactation (> 6 months). It is during the first months of life when the baby requires a greater amount of these fatty acids due to neuronal and retinal development.
The fatty acid composition of milk formulas marketed in Spain and human milk from the two cohorts of mothers, were compared using one-way ANOVA with post-hoc Dunnett test. For this test, only samples < 6 months of lactation were considered. Figure 2 shows the plots for each of the fatty acids studied.
The presence of OA is higher in all infant formulas, but the difference was not significant. ALA is a fatty acid with a significantly higher presence in all infant formulas studied than in maternal milk. In contrast, the content of AA is lower in infant formulas than in maternal milk. AA has very different biological functions compared to DHA, for example, functions in the vasculature and specific aspects of immunity. DHA suppresses concentrations of arachidonic acid in the membrane and its function. An infant formula with DHA and without arachidonic acid is at risk of cardiovascular and cerebrovascular morbidity and even mortality due to the suppression of favorable oxylipin derivatives of AA [36]. The differences were not significant for DHA and EPA; however, in all three types of formulas, the amount was lower than in the two cohorts of breast milk. However, the greatest differences between natural and formula feeding are in natural trans fatty acids, which are clearly deficient in all infant formulas analyzed in this study.
Author Contributions
Conceptualization. C.F. and P.R.; methodology. R.B., L.S., L.GA and P.R.; formal analysis. C.F..; data curation. A.L.; writing—original draft preparation. C.F.; writing—review and editing. P.R. and A.L.; funding acquisition. A.C., I.M. All authors have read and agreed to the published version of the manuscript. Please turn to the CRediT taxonomy for the term explanation.
Funding
The authors thank Xunta de Galicia and European Regional Development Funds (FEDER), consolidation grant ED431C 2022/14, for covering the costs of the analyses.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on reasonable request.
Acknowledgments
Authors acknowledge the support given by Feiraco Sociedade Cooperativa Galega, through the donation of dairy products for cohort 2.
Conflicts of Interest
Ismael Martínez is member of Feiraco Sociedade Cooperativa Galega. The funder had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
References
- Hennet, T.; Borsig, L. Breastfed at Tiffany’s. Trends Biochem Sci 2016, 41, 508–518. [Google Scholar] [CrossRef]
- Grote, V.; Verduci, E.; Scaglioni, S.; Vecchi, F.; Contarini, G.; Giovannini, M.; Koletzko, B.; Agostoni, C. Breast Milk Composition and Infant Nutrient Intakes during the First 12 Months of Life. Eur J Clin Nutr 2016, 70. [Google Scholar] [CrossRef]
- Barreiro, R.; Díaz-Bao, M.; Cepeda, A.; Regal, P.; Fente, C.A. Fatty Acid Composition of Breast Milk in Galicia (NW Spain): A Cross-Country Comparison. Prostaglandins Leukot Essent Fatty Acids 2018, 135, 102–114. [Google Scholar] [CrossRef]
- Craig-Schmidt, M.C. World-Wide Consumption of Trans Fatty Acids. Atheroscler Suppl 2006, 7. [Google Scholar] [CrossRef]
- Ganguly, R.; Pierce, G.N. The Toxicity of Dietary Trans Fats. Food and Chemical Toxicology 2015, 78, 170–176. [Google Scholar] [CrossRef]
- Mennitti, L. V; Oliveira, J.L.; Morais, C.A.; Estadella, D.; Oyama, L.M.; do Nascimento, C.M.O.; Pisani, L.P. Type of Fatty Acids in Maternal Diets during Pregnancy and/or Lactation and Metabolic Consequences of the Offspring. J Nutr Biochem 2015, 26, 99–111. [Google Scholar] [CrossRef]
- Valenzuela, C.A.; Baker, E.J.; De Souza, C.O.; Miles, E.A.; Calder, P.C. Differential Effects of Ruminant and Industrial 18-Carbon Trans-Monounsaturated Fatty Acids (Trans Vaccenic and Elaidic) on the Inflammatory Responses of an Endothelial Cell Line. Molecules 2021, 26, 5834. [Google Scholar] [CrossRef]
- Fan, H.; Xia, S.; Xiang, J.; Li, Y.; Ross, M.O.; Lim, S.A.; Yang, F.; Tu, J.; Xie, L.; Dougherty, U. Trans-Vaccenic Acid Reprograms CD8+ T Cells and Anti-Tumour Immunity. Nature 2023, 1–10. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Cao, H.; King, I.B.; Lemaitre, R.N.; Song, X.; Siscovick, D.S.; Hotamisligil, G.S. Trans-Palmitoleic Acid, Metabolic Risk Factors, and New-Onset Diabetes in US Adults: A Cohort Study. Ann Intern Med 2010, 153, 790–799. [Google Scholar] [CrossRef]
- Imamura, F.; Fretts, A.; Marklund, M.; Ardisson Korat, A. V; Yang, W.-S.; Lankinen, M.; Qureshi, W.; Helmer, C.; Chen, T.-A.; Wong, K. Fatty Acid Biomarkers of Dairy Fat Consumption and Incidence of Type 2 Diabetes: A Pooled Analysis of Prospective Cohort Studies. PLoS Med 2018, 15, e1002670. [Google Scholar] [CrossRef]
- Guillocheau, E.; Penhoat, C.; Drouin, G.; Godet, A.; Catheline, D.; Legrand, P.; Rioux, V. Current Intakes of Trans-Palmitoleic (Trans-C16: 1 n-7) and Trans-Vaccenic (Trans-C18: 1 n-7) Acids in France Are Exclusively Ensured by Ruminant Milk and Ruminant Meat: A Market Basket Investigation. Food Chem X 2020, 5, 100081. [Google Scholar] [CrossRef]
- Wolff, R.L. Content and Distribution of Trans-18: 1 Acids in Ruminant Milk and Meat Fats. Their Importance in European Diets and Their Effect on Human Milk. J Am Oil Chem Soc 1995, 72, 259–272. [Google Scholar] [CrossRef]
- Varela, G.; Moreiras, O.; Ansón, R. Consumo de Alimentos En Galicia-La Dieta Atlántica. Madrid, Spain: Fundación Española de Nutrición 2004. [Google Scholar]
- Oliveira, A.; Lopes, C.; Rodríguez-Artalejo, F. Adherence to the Southern European Atlantic Diet and Occurrence of Nonfatal Acute Myocardial Infarction. Am J Clin Nutr 2010, 92, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Guallar-Castillón, P.; Oliveira, A.; Lopes, C.; López-García, E.; Rodríguez-Artalejo, F. The Southern European Atlantic Diet Is Associated with Lower Concentrations of Markers of Coronary Risk. Atherosclerosis 2013, 226, 502–509. [Google Scholar] [CrossRef]
- Nasser, R.; Stephen, A.M.; Goh, Y.K.; Clandinin, M.T. The Effect of a Controlled Manipulation of Maternal Dietary Fat Intake on Medium and Long Chain Fatty Acids in Human Breast Milk in Saskatoon, Canada. Int Breastfeed J 2010, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mosley, E.E.; McGuire, M.K.; Williams, J.E.; McGuire, M.A. Cis-9, Trans-11 Conjugated Linoleic Acid Is Synthesized from Vaccenic Acid in Lactating Women. J Nutr 2006, 136, 2297–2301. [Google Scholar] [CrossRef]
- Aumeistere, L.; Beluško, A.; Ciproviča, I.; Zavadska, D. Trans Fatty Acids in Human Milk in Latvia: Association with Dietary Habits during the Lactation Period. Nutrients 2021, 13, 2967. [Google Scholar] [CrossRef]
- Thijs, C.; Müller, A.; Rist, L.; Kummeling, I.; Snijders, B.E.P.; Huber, M.; Van Ree, R.; Simões-Wüst, A.P.; Dagnelie, P.C.; Van Den Brandt, P.A. Fatty Acids in Breast Milk and Development of Atopic Eczema and Allergic Sensitisation in Infancy. Allergy 2011, 66, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Chisaguano, A.M.; Montes, R.; Castellote, A.I.; Morales, E.; Júlvez, J.; Vioque, J.; Sunyer, J.; López-Sabater, M.C. Elaidic, Vaccenic, and Rumenic Acid Status during Pregnancy: Association with Maternal Plasmatic LC-PUFAs and Atopic Manifestations in Infants. Pediatr Res 2014, 76, 470–476. [Google Scholar] [CrossRef]
- Sánchez, C.; Fente, C.; Barreiro, R.; López-Racamonde, O.; Cepeda, A.; Regal, P. Association between Breast Milk Mineral Content and Maternal Adherence to Healthy Dietary Patterns in Spain: A Transversal Study. Foods 2020, 9, 659. [Google Scholar] [CrossRef]
- Barreiro, R.; Regal, P.; López-Racamonde, O.; Cepeda, A.; Fente, C. Evolution of Breast Milk Fatty Acids in Spanish Mothers after One Year of Uninterrupted Lactation. Prostaglandins Leukot Essent Fatty Acids 2020, 159, 102141. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Martín, C.; Garcia-Ortiz, L.; Rodriguez-Sanchez, E.; Martin-Cantera, C.; Soriano-Cano, A.; Arietaleanizbeaskoa, M.S.; Magdalena-Belio, J.F.; Menendez-Suarez, M.; Maderuelo-Fernandez, J.A.; Lugones-Sanchez, C. The Relationship of the Atlantic Diet with Cardiovascular Risk Factors and Markers of Arterial Stiffness in Adults without Cardiovascular Disease. Nutrients 2019, 11, 742. [Google Scholar] [CrossRef] [PubMed]
- Roibás, L.; Martínez, I.; Goris, A.; Barreiro, R.; Hospido, A. An Analysis on How Switching to a More Balanced and Naturally Improved Milk Would Affect Consumer Health and the Environment. Science of the Total Environment 2016, 566, 685–697. [Google Scholar] [CrossRef] [PubMed]
- Guadarrama-Flores, B.; Matencio, A.; Navarro-Orcajada, S.; Martínez-Lede, I.; Conesa, I.; Vidal-Sánchez, F.J.; García-Carmona, F.; López-Nicolás, J.M. Development If Healthy Milk and Yogurt Products for Reducing Metabolic Diseases Using Cyclodextrin and Omega-3 Fatty Acids from Fish Oil. Food Funct 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Sanjulián, L.; Lamas, A.; Barreiro, R.; Cepeda, A.; Fente, C.A.; Regal, P. Bacterial Diversity of Breast Milk in Healthy Spanish Women: Evolution from Birth to Five Years Postpartum. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Jahreis, G.; Pritsche, J.; Steinhart, H. Conjugated Linoleic Acid in Milk Fat: High Variation Depending on Production System. Nutrition Research 1997, 17. [Google Scholar] [CrossRef]
- Bergamo, P.; Fedele, E.; Iannibelli, L.; Marzillo, G. Fat-Soluble Vitamin Contents and Fatty Acid Composition in Organic and Conventional Italian Dairy Products. Food Chem 2003, 82. [Google Scholar] [CrossRef]
- van Wijlen, R.P.J.; Colombani, P.C. Grass-Based Ruminant Production Methods and Human Bioconversion of Vaccenic Acid with Estimations of Maximal Dietary Intake of Conjugated Linoleic Acids. Int Dairy J 2010, 20, 433–448. [Google Scholar] [CrossRef]
- Rist, L.; Mueller, A.; Barthel, C.; Snijders, B.; Jansen, M.; Simões-Wüst, A.P.; Huber, M.; Kummeling, I.; von Mandach, U.; Steinhart, H.; et al. Influence of Organic Diet on the Amount of Conjugated Linoleic Acids in Breast Milk of Lactating Women in the Netherlands. British Journal of Nutrition 2007, 97. [Google Scholar] [CrossRef]
- Simões-Wüst, A.P.; Rist, L.; Mueller, A.; Huber, M.; Steinhart, H.; Thijs, C. Consumption of Dairy Products of Biodynamic Origin Is Correlated with Increased Contents of Rumenic and Trans-Vaccenic Acid in the Breast Milk of Lactating Women. Organic Agriculture 2011, 1. [Google Scholar] [CrossRef]
- Turpeinen, A.M.; Mutanen, M.; Aro, A.; Salminen, I.; Basu, S.; Palmquist, D.L.; Griinari, J.M. Bioconversion of Vaccenic Acid to Conjugated Linoleic Acid in Humans. American Journal of Clinical Nutrition 2002, 76. [Google Scholar] [CrossRef] [PubMed]
- Mosley, E.E.; McGuire, M.K.; Williams, J.E.; McGuire, M.A. Cis-9, Trans-11 Conjugated Linoleic Acid Is Synthesized from Vaccenic Acid in Lactating Women. J Nutr 2006, 136, 2297–2301. [Google Scholar] [CrossRef] [PubMed]
- Thijs, C.; Müller, A.; Rist, L.; Kummeling, I.; Snijders, B.E.P.; Huber, M.; Van Ree, R.; Simões-Wüst, A.P.; Dagnelie, P.C.; Van Den Brandt, P.A. Fatty Acids in Breast Milk and Development of Atopic Eczema and Allergic Sensitisation in Infancy. Allergy 2011, 66, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Barreiro, R.; Regal, P.; López-Racamonde, O.; Cepeda, A.; Fente, C.A. Comparison of the Fatty Acid Profile of Spanish Infant Formulas and Galician Women Breast Milk. J Physiol Biochem 2018, 74. [Google Scholar] [CrossRef]
- Crawford, M.A.; Wang, Y.; Forsyth, S.; Brenna, J.T. The European Food Safety Authority Recommendation for Polyunsaturated Fatty Acid Composition of Infant Formula Overrules Breast Milk, Puts Infants at Risk, and Should Be Revised. Prostaglandins Leukot Essent Fatty Acids 2015, 102, 1–3. [Google Scholar] [CrossRef]
Figure 1.
PCA score scatter plot (A) and loading plot (B) of fatty acid profiles of breast milk from cohorts 1 and 2.
Figure 1.
PCA score scatter plot (A) and loading plot (B) of fatty acid profiles of breast milk from cohorts 1 and 2.
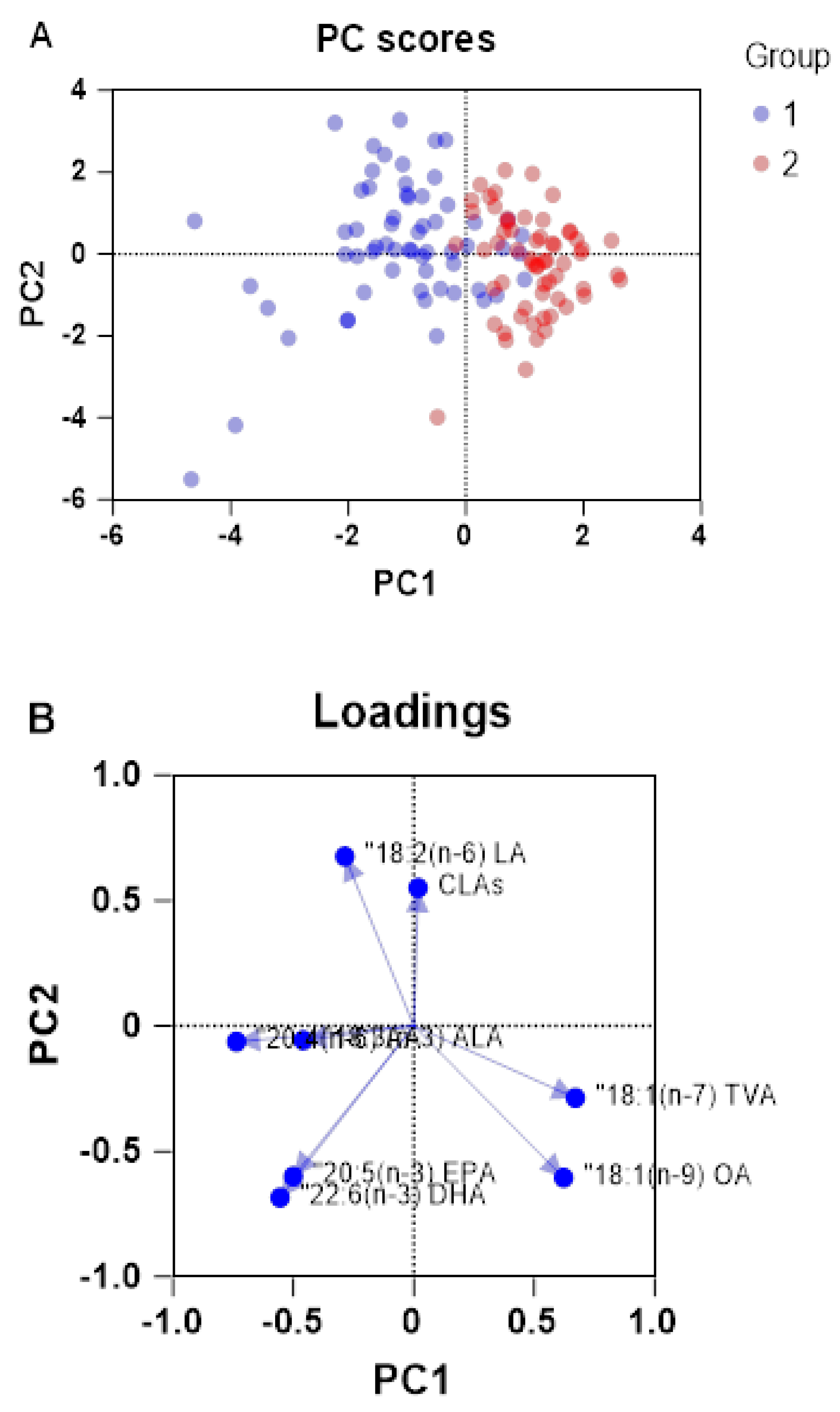
Figure 2.
Box plots showing the abundance of OA (a), LA (b), ALA (c), AA (d), EPA (e), DHA (f), TVA (g), and CLA(h) fatty acids in breast milk samples from cohorts 1 and 2 (C1 < 6 months, C2) and in infant formula (first stage, FSF, follow-on, FOF, and growing up, GUF, formula). Significant differences between groups are highlighted with * (p<0.05), ** (p<0.01), *** (p<0.001) or **** (p<0.05).
Figure 2.
Box plots showing the abundance of OA (a), LA (b), ALA (c), AA (d), EPA (e), DHA (f), TVA (g), and CLA(h) fatty acids in breast milk samples from cohorts 1 and 2 (C1 < 6 months, C2) and in infant formula (first stage, FSF, follow-on, FOF, and growing up, GUF, formula). Significant differences between groups are highlighted with * (p<0.05), ** (p<0.01), *** (p<0.001) or **** (p<0.05).
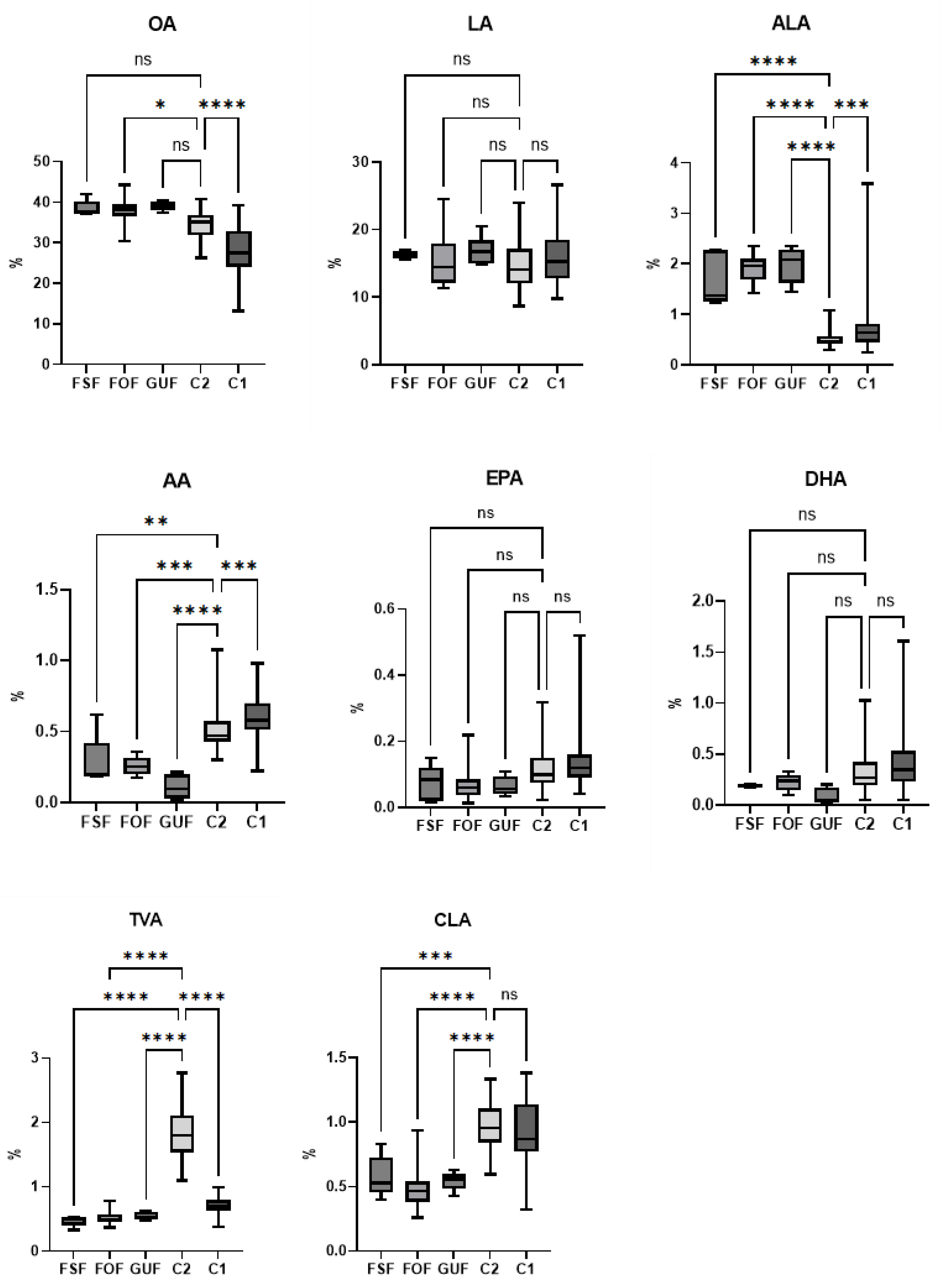

Table 1.
Pregnancy and maternal characteristics. continuous and categorical variables (n=92).
| Maternal Data | Mean | Median | SD | Min | Max |
|---|---|---|---|---|---|
| Pregnancy Time (weeks) | 39.77 | 40.00 | 1.34 | 36.00 | 42.29 |
| Maternal Age (years) | 35.43 | 35.00 | 4.06 | 26.00 | 46.00 |
| Maternal BMI (kg/m2) | 24.47 | 24.36 | 3.83 | 17.85 | 35.03 |
| Lactating time (months) | 7.77 | 3.00 | 11.12 | 0.5 | 58.97 |
| AD adherence (score) | 3.80 | 4.00 | 1.48 | 0.00 | 7.00 |
| Time lactation | 7.77 | 3.00 | 11.12 | 0.5 | 58.97 |
| Infant gender: n♂(%)/n♀(%) | 43 (46.73)/49 (53.26) | C-section delivery (%) | 11.96 | Parity number 1st child (%) | 60.87 |
Table 2.
Oleic acid (OA), linoleic acid (LA), α-Linolenic acid (ALA), arachidonic acid (AA), eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), trans-vaccenic acid (TVA), and conjugated linoleic acid (CLA, sum of cis-9,trans-11 CLA and trans-10,cis-12 CLA isomers), presented as mean, standard deviation and range across different groups of breast milk samples and infant formula (first stage, FSF, follow-on, FOF, and growing-up, GUF). Variables considered are lactating time (LT, months), body mass index (BMI), newborn sex (0=boy, 1= girl), SEAD adherence (score), milk and meat consumption (servings per week), naturally enriched dairy products consumption (cohort 1: no, cohort 2: yes)..
Table 2.
Oleic acid (OA), linoleic acid (LA), α-Linolenic acid (ALA), arachidonic acid (AA), eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), trans-vaccenic acid (TVA), and conjugated linoleic acid (CLA, sum of cis-9,trans-11 CLA and trans-10,cis-12 CLA isomers), presented as mean, standard deviation and range across different groups of breast milk samples and infant formula (first stage, FSF, follow-on, FOF, and growing-up, GUF). Variables considered are lactating time (LT, months), body mass index (BMI), newborn sex (0=boy, 1= girl), SEAD adherence (score), milk and meat consumption (servings per week), naturally enriched dairy products consumption (cohort 1: no, cohort 2: yes)..
| Cohort 1 | Cohort 2 | Infant formula | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fatty acid (%wt/wt of total fatty acids) | LT < 6 | LT≥ 6 | BMI< 25 | BMI≥ 25 | Infant 0 | Infant 1 | SEAD <5 | SEAD ≥5 | Milk <3 | Milk ≥3 | Meat <3 | Meat ≥3 | LT<6 | FSF | FOF | GUF | |
| n= 67 | n= 26 | n= 47 | n= 46 | n= 41 | n= 52 | n= 64 | n= 29 | n= 39 | n= 41 | n= 63 | n= 18 | n= 16 | n= 5 | n= 13 | n= 5 | ||
| 18:1(n-9) OA | Mean | 28.35* | 29.38 | 30.02 | 27.34 | 30.12 | 27.47 | 28.17 | 29.67 | 28.41 | 29.49 | 27.74 | 31.88 | 34.49* | 38.49 | 38.06* | 39.07 |
| SD | 5.87 | 8.37 | 6.85 | 6.20 | 6.81 | 6.30 | 6.86 | 6.05 | 6.96 | 6.00 | 6.20 | 6.58 | 3.22 | 2.06 | 3.44 | 1.18 | |
| Min | 13.11 | 14.52 | 14.52 | 13.11 | 19.76 | 13.11 | 13.11 | 20.03 | 13.11 | 20.15 | 13.11 | 22.50 | 26.21 | 37.10 | 36.45 | 37.32 | |
| Max | 39.28 | 43.19 | 42.57 | 43.19 | 43.19 | 41.58 | 43.19 | 42.11 | 42.11 | 43.19 | 43.19 | 42.11 | 40.67 | 42.04 | 44.20 | 40.43 | |
| 18:2(n-6) LA | Mean | 15.96 | 15.78 | 15.63 | 16.18 | 15.68 | 16.10 | 15.84 | 16.08 | 16.64 | 15.23 | 16.50 | 14.53 | 14.60 | 16.26 | 15.64 | 16.96 |
| SD | 3.84 | 4.17 | 4.13 | 3.73 | 4.03 | 3.85 | 3.77 | 4.27 | 4.10 | 3.85 | 3.99 | 2.44 | 3.41 | 0.58 | 3.91 | 2.32 | |
| Min | 9.75 | 8.73 | 8.73 | 9.42 | 8.73 | 9.75 | 8.73 | 9.42 | 9.42 | 8.73 | 8.73 | 9.42 | 8.66 | 15.50 | 11.54 | 14.90 | |
| Max | 26.64 | 23.86 | 26.64 | 24.80 | 24.80 | 26.64 | 24.80 | 26.64 | 26.64 | 22.68 | 26.64 | 19.62 | 23.97 | 16.94 | 24.53 | 20.51 | |
| 18:3(n-3) ALA | Mean | 0.75* | 0.91 | 0.91 | 0.68 | 0.66 | 0.89 | 0.83 | 0.70 | 0.94 | 0.71 | 0.79 | 0.70 | 0.50* | 1.69* | 1.88* | 1.98* |
| SD | 0.49 | 0.75 | 0.74 | 0.33 | 0.29 | 0.71 | 0.66 | 0.31 | 0.69 | 0.37 | 0.52 | 0.29 | 0.13 | 0.54 | 0.28 | 0.36 | |
| Min | 0.25 | 0.31 | 0.31 | 0.25 | 0.25 | 0.31 | 0.31 | 0.25 | 0.31 | 0.25 | 0.25 | 0.40 | 0.30 | 1.23 | 1.69 | 1.45 | |
| Max | 3.59 | 4.12 | 4.12 | 1.69 | 1.55 | 4.12 | 4.12 | 1.54 | 4.12 | 1.67 | 3.59 | 1.54 | 1.08 | 2.27 | 2.35 | 2.35 | |
| 20:4(n-6) AA | Mean | 0.60* | 0.60 | 0.58 | 0.61 | 0.59 | 0.60 | 0.59 | 0.61 | 0.58 | 0.60 | 0.59 | 0.56 | 0.45* | 0.28* | 0.26* | 0.11* |
| SD | 0.14 | 0.19 | 0.16 | 0.16 | 0.16 | 0.15 | 0.16 | 0.15 | 0.15 | 0.18 | 0.15 | 0.15 | 0.11 | 0.19 | 0.07 | 0.09 | |
| Min | 0.22 | 0.30 | 0.30 | 0.22 | 0.22 | 0.31 | 0.30 | 0.22 | 0.30 | 0.22 | 0.22 | 0.35 | 0.28 | 0.18 | 0.28 | 0.02 | |
| Max | 0.98 | 1.00 | 0.98 | 1.00 | 1.00 | 0.98 | 1.00 | 0.98 | 1.00 | 0.98 | 1.00 | 0.88 | 0.72 | 0.62 | 0.36 | 0.21 | |
| 20:5(n-3) EPA | Mean | 0.14 | 0.12 | 0.15 | 0.13 | 0.12 | 0.15 | 0.14 | 0.13 | 0.14 | 0.15 | 0.14 | 0.10 | 0.11 | 0.07 | 0.07 | 0.06 |
| SD | 0.09 | 0.08 | 0.09 | 0.09 | 0.08 | 0.09 | 0.09 | 0.09 | 0.07 | 0.12 | 0.08 | 0.05 | 0.06 | 0.05 | 0.05 | 0.03 | |
| Min | 0.04 | 0.05 | 0.06 | 0.04 | 0.04 | 0.05 | 0.05 | 0.04 | 0.05 | 0.04 | 0.04 | 0.05 | 0.02 | 0.02 | 0.01 | 0.03 | |
| Max | 0.52 | 0.35 | 0.51 | 0.52 | 0.52 | 0.51 | 0.52 | 0.51 | 0.35 | 0.52 | 0.52 | 0.29 | 0.32 | 0.15 | 0.22 | 0.11 | |
| 22:6(n-3) DHA | Mean | 0.42 | 0.50 | 0.48 | 0.40 | 0.39 | 0.48 | 0.44 | 0.43 | 0.44 | 0.47 | 0.41 | 0.37 | 0.32 | 0.21 | 0.22 | 0.09 |
| SD | 0.32 | 0.30 | 0.33 | 0.29 | 0.27 | 0.34 | 0.30 | 0.34 | 0.28 | 0.37 | 0.29 | 0.24 | 0.18 | 0.05 | 0.08 | 0.08 | |
| Min | 0.05 | 0.17 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.18 | 0.28 | 0.01 | |
| Max | 1.61 | 1.23 | 1.61 | 1.41 | 1.41 | 1.61 | 1.41 | 1.61 | 1.23 | 1.61 | 1.41 | 0.96 | 1.03 | 0.30 | 0.33 | 0.20 | |
| 18:1(n-7) TVA | Mean | 0.71* | 0.69 | 0.70 | 0.71 | 0.70 | 0.71 | 0.71 | 0.70 | 0.69 | 0.75 | 0.70 | 0.72 | 1.84* | 0.47* | 0.53* | 0.54* |
| SD | 0.13 | 0.13 | 0.12 | 0.13 | 0.14 | 0.12 | 0.12 | 0.14 | 0.12 | 0.15 | 0.12 | 0.14 | 0.41 | 0.08 | 0.11 | 0.06 | |
| Min | 0.38 | 0.41 | 0.43 | 0.38 | 0.38 | 0.42 | 0.42 | 0.38 | 0.41 | 0.38 | 0.38 | 0.41 | 1.10 | 0.33 | 0.45 | 0.48 | |
| Max | 0.99 | 0.87 | 0.99 | 0.94 | 0.95 | 0.99 | 0.95 | 0.99 | 0.94 | 0.99 | 0.95 | 0.94 | 2.77 | 0.53 | 0.79 | 0.63 | |
| CLAs | Mean | 0.93 | 0.86 | 0.89 | 0.93 | 0.88 | 0.93 | 0.93 | 0.85 | 0.96 | 0.85 | 0.94 | 0.85 | 0.97* | 0.58* | 0.50* | 0.54* |
| SD | 0.23 | 0.30 | 0.26 | 0.24 | 0.26 | 0.24 | 0.25 | 0.24 | 0.26 | 0.25 | 0.26 | 0.23 | 0.19 | 0.16 | 0.19 | 0.07 | |
| Min | 0.32 | 0.50 | 0.41 | 0.32 | 0.32 | 0.59 | 0.41 | 0.32 | 0.41 | 0.32 | 0.32 | 0.57 | 0.60 | 0.40 | 0.42 | 0.43 | |
| Max | 1.38 | 1.42 | 1.42 | 1.38 | 1.42 | 1.38 | 1.42 | 1.31 | 1.42 | 1.29 | 1.42 | 1.33 | 1.33 | 0.83 | 0.94 | 0.63 | |
n=number of samples; numbers in bold indicate significant differences (p<0.05) between two groups of comparison in cohort 1; significant differences between cohort 2 and cohort 1 (LT < 6), and between cohort 2 and different formulas, are highlighted with an asterisk.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



