
Submitted:
15 May 2024
Posted:
15 May 2024
You are already at the latest version
Abstract
Medicinal activities carried out within hospitals lead to a high consumption of antibiotics and subsequently result in a high excretion rate of antibiotic residues. These antibiotics consumed in human medicine are not fully absorbed by the body and are often discharged into the environment as biological waste from infected human patients. The significant water consumption in hospitals and the pharmaceutical impact on wastewater from healthcare facilities facilitate the emergence and spread of antibiotic-resistant bacteria and antibiotic-resistant genes in the environment. Hospital effluents could be doubly involved in the dissemination of antibiotic molecules and multidrug-resistant bacteria in various ecosystems. The objective of this study is to characterize hospital effluents by assessing antibiotic concentrations and the diversity of antibiotic-resistant bacteria in these hospital wastewaters and within the environment (aquatic environments; rivers), as well as to inventory the bacteria present and those carrying antibiotic resistance in both hospital wastewater and the environment.
Keywords:
hospital effluents
; antibiotic resistance
; bacteria
; environment Introduction
Introduction
The effluents generated by hospital activities can pose a potential danger both to humans and the environment due to the nature and quantity of specific substances and microorganisms they carry (pharmaceutical residues, chemicals, and multidrug-resistant pathogenic bacteria). These effluents are discharged into the municipal sewer system without prior treatment, similar to conventional urban wastewater [1].
On average, in healthcare facilities, the antibiotic consumption of a hospitalized patient is about ten times higher than the average consumption per capita in households [2]. Furthermore, the significant use of antibiotics in hospitals exerts selective pressure that promotes the emergence of multidrug-resistant bacteria, including extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL-EB) [3]. These multidrug-resistant bacteria are then eliminated in wastewater as antibiotic-resistant fecal bacteria (ARFB) and liquid waste [2,4,5]. In developing countries, wastewater treatment before discharge into the environment presents a major challenge due to a lack of resources, unplanned urbanization, and limited industrialization [6].
It is in this context that communal and hospital wastewater plays a key role in the dissemination of antibiotic-resistant bacteria (ARB), such as ESBL-EB [3,4,5,6,7]. Hospital effluents contribute to the animals, etc.) [8]. Multidrug-resistant microorganisms carried in these contaminated waters can induce the transfer and dissemination of antibiotic resistance genes (ARGs) to other bacteria, especially pathogenic bacteria, posing a significant health risk to surrounding populations [9,10]. This is a global public health problem, highlighting the importance of a literature review on antibioticresistant bacteria (ARB) isolated from hospital wastewater. This literature review will consist of drawing up a list of antibiotic residues and bacteria carrying antibiotic resistance, present both in hospital wastewater and in the environment.
Materials and Methods
Relevant articles on the subject were searched in Google Scholar, PubMed, and CrossRef databases. Articles or other scientific publications primarily addressing the following keywords were considered: “antibiotic residues in hospital sewage “, “bacterial resistance to antibiotics in hospital wastewater”, “hospital wastewater risks for human health”, “hospital wastewater risks for the environment”, and “ESBL in hospital effluents” (Figure 1). The documents included in this study were published between 2002 and 2022. To obtain articles more easily for this study, each keyword was directly associated with the name of a country. The objective was to identify recent trends in the microbiology (bacteriology) of hospital wastewater, and its risks to human health, and aquatic ecosystems.
Hospital Waste Disposal
Hospitals are significant consumers of water. While the per capita daily water consumption in domestic settings ranges from 150 to 200 litres, the average water consumption in hospitals has increased from 400 to 1200 litres per day, and the production of liquid waste is estimated at 1 cubic meter per day per active bed [27,28,29]. Additionally, special waters used by the hospital, such as distilled water for irrigation, wound cleaning, tissue rinsing, or surgical equipment humidification, add to this water consumption [30]. The quantity of wastewater discharged by hospitals is estimated at 1000 litres per day in America [27,31,32].
In Africa, the situation regarding the disposal and treatment of liquid waste is dire [18]. Liquid waste generated by hospitals is continuously discharged into natural water reservoirs without any prior treatment, leading to the vulnerability of local flora and fauna in these natural environments [33,34].
Antibiotics and Antibiotic-Resistant Bacteria in Hospital Wastewater
Origins of Antibiotics Found in Wastewater
Medical activities carried out within hospitals generally lead to high antibiotic consumption and a high excretion rate of antibiotic residues [10,11,76]. This consumption is believed to be the main source of antibiotic resistance in some patients and the environment, but it is difficult to assess [12,13]. Indeed, after ingestion, antibiotics undergo chemical modifications, and the resulting metabolites can be more or less toxic and may also have different, even antagonistic properties compared to the initial medication [14]. Most of these antibiotics consumed in human and veterinary medicine are not fully absorbed by the body and are often released into the environment as biological waste (blood, urine, pus, etc.) from infected human and animal patients [15,16,17,18].
Furthermore, the portion of unused medications eliminated through wastewater discharge points can constitute a potential source of ecosystem pollution [19,20].
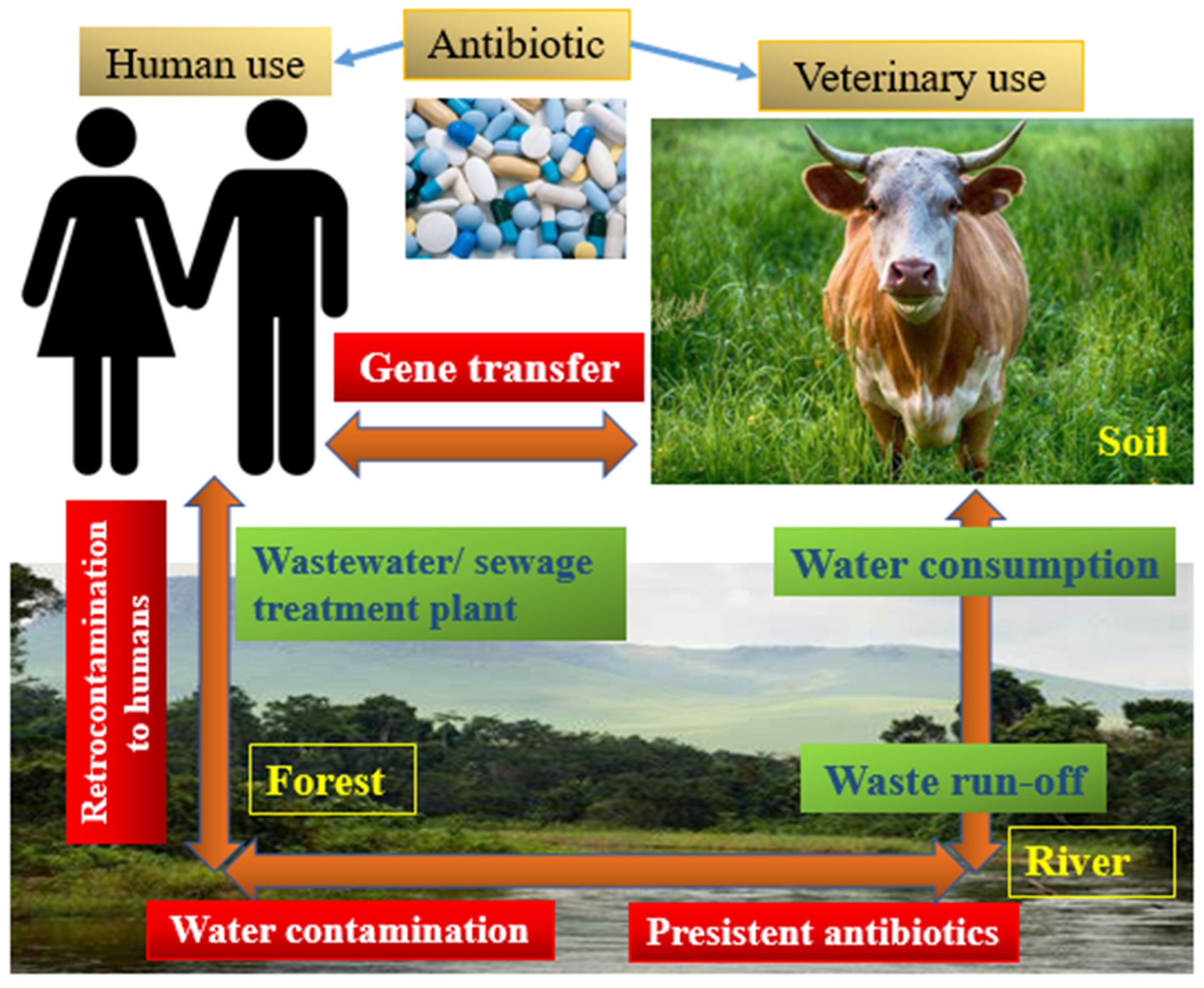
Additionally, healthcare facilities’ discharges present a unique situation due to the number of patients treated, and the quantity and variety of drugs used, including anticancer drugs, anaesthetics, antibiotics, diagnostic products, contrast agents, or radioactive materials [21,22]. In the external environment of hospitals, the quantitative and qualitative evolution of antibiotic and microorganism contamination occurs according to the gradient of anthropogenic activities [23,24,25] (Figure 2 and Figure 3).
Antibiotics in Hospital Wastewater and Their Dissemination in the Environment
Antibiotics are essential drugs used to combat bacterial infections in both human and veterinary medicine [113]. The intensive use of antibiotics in both of these medical fields has two serious consequences for environmental impact: the presence of residues of active molecules and the increase in the selection of resistant bacteria. The most commonly used antibiotic families in hospitals are betalactams (penicillin and cephalosporins), sulfonamides, tetracyclines (doxycycline, oxytetracycline), quinolones/fluoroquinolones (nalidixic acid, ciprofloxacin, ofloxacin, etc.) [71,72]. Antibiotics prescribed in human and veterinary medicine, along with antimicrobial resistance bacteria (AMRB), are released into the environment through urine and faeces [25]. Four antibiotics have been detected and quantified, with three of them regularly found in hospital effluents. These include amoxicillin (0.066 ± 0.08 μg/l), erythromycin (0.04 ± 0.0 μg/l), sulfamethoxazole + trimethoprim (0.06 ± 0.21 / 0.08 ± 0.006 μg/l), and metronidazole (0.02 ± 0.0 μg/l). Amoxicillin and sulfamethoxazole were detected and quantified at both points, while erythromycin and metronidazole were only found at the “G” Point of Bamako Teaching Hospital [73]. Treated effluents from wastewater treatment plants (WWTPs) and soil runoff or leaching are the main sources of water and sediment contamination [114].

Table 1.
Average concentrations measured in urban effluents (UWw) and hospital effluents (HWw) for commonly found pharmaceutical compounds [74].
Table 1.
Average concentrations measured in urban effluents (UWw) and hospital effluents (HWw) for commonly found pharmaceutical compounds [74].
| Antibiotics | Concentration in HWw (µg L-1) | Concentration in UWw (µg L-1) |
| Ciprofloxacin | 0,03-125 | 0,01-5,88 |
| Clarithromycin | 0,2-3 | 0,1-4,8 |
| Coprofloxacin | 0,85-2 | |
| Doxycycline | 0,1-6,7 | |
| Erythromycin | 27-83 | 0,04-2,7 |
| Lincomycin | 0,3-2 | |
| Metronidazole | 0,1-90 | |
| Norfloxacin | 0,029-44 | 0,01-0,96 |
| Ofloxacin | 0,353-35,5 | 0,01-31,70 |
| Oxytetracycline | 0,01-3,75 | |
| Penicillin G | 0,85-5,2 | 0,03 |
| Sulfamethoxazole | 0,04-83 | 0,01-6,0 |
| Tetracycline | 0,01-4,2 | 0,01-1,30 |
| Trimethoprim | 0,01-15 | 0,02-7,90 |
Quantification of Antibiotic Residues Encountered in Samples from Certain Rivers Worldwide
In the study conducted by Dong Li et al. in China, the resistance rate to doxycycline (DOX) has consistently been the lowest (1.5% to 83.1%) among tetracyclines (1.5% to 95.2%) in the three water samples from the Xiao River. The resistance prevalence rate was lower for cefotaxime (CTX) (1.5% to 71.2%) than for ampicillin (AMP) (24.6% to 93.1%), both of which are beta-lactams [56].
According to a study conducted on irrigation water samples in Burkina Faso, the antibiogram showed that non-typhoid Salmonella was resistant to tetracycline (66.67%, 38/57), followed by ampicillin (66.67%, 38/57), amoxicillin + clavulanic acid, and amoxicillin (30%, 17/57) [75]. A Gabones study highlighted among the 35 coliforms found in 27 samples of river and stream waters, resistance to antibiotics for ampicillin (91%, 32/35), cefotaxime (3%, 1/35), and cotrimoxazole (9%, 3/35). No resistance was detected against ciprofloxacin, imipenem, meropenem, and ertapenem in these waters [64].
The concentrations of antibiotic residues found in wastewater range from nanograms per litre to micrograms per litre [77]. In rivers, the range of antibiotic concentrations varies from a few nanograms to a few tens of nanograms per litre [78]. Among the main sources of surface water contamination, domestic effluents are primarily mentioned, as well as hospital effluents, and pharmaceutical manufacturing and packaging facilities [79].
Table 2.
Minimum Inhibitory Concentration (MIC) of 12 antibiotics on bacterial isolates isolated from WW, WTP, and RW [37].
Table 2.
Minimum Inhibitory Concentration (MIC) of 12 antibiotics on bacterial isolates isolated from WW, WTP, and RW [37].
| Activity against the Isolates | ||||
|---|---|---|---|---|
| Antibiotics | Resistance Prevalence (%) | MIC (mg L-1) | ||
| Rank | 50% | 90% | ||
| Ampicillin (AMP) | 100 | 64 to ≥ 1024 | 1024 | 1024 |
| Amoxicillin (AMO) | 100 | 1 to ≥ 1024 | 1024 | 1024 |
| Streptomycin Sulfate (STR) | 92.3 | 1 to ≥ 1024 | 128 | 52 |
| Trimethoprim (TRI) | 98 | 8 to ≥ 1024 | 1024 | 1024 |
| Chloramphenicol (CHL) | 100 | 256 to ≥ 1024 | 1024 | 1024 |
| Sulfonamide (SUL) | 100 | 512 ≥ 1024 | 1024 | 1024 |
| Tetracycline (OXY) | 90.6 | 2 to ≥ 512 | 128 | 256 |
| Oxytetracycline (OXY) | 90.6 | 1 to ≥ 1024 | 256 | 512 |
| Nalidixic Acid (NAL) | 73.6 | 1 to ≥ 1024 | 512 | 1024 |
| Erythromycin (ERY) | 92.5 | 4 to ≥ 1024 | 128 | 512 |
| Spiramycin (SPIRA) | 90.6 | 2 to ≥ 1024 | 512 | 1024 |
| Kanamycin (KAN) | 54.7 | 1 to ≥ 1024 | 128 | 1024 |
WW, wastewater effluent; WTP, wastewater treatment plant; RW, river water; 50%, MIC50; 90%, MIC90. MICs for each antibiotic for all isolates tested in WW, WTP, and RW, representing the MICs required for the inhibition of 50% and 90% of bacterial strains, respectively.
Bacteria Found in Hospital
Wastewater Wastewater typically contains 107 to 108 bacterial organisms per litre, with a concentration of pathogenic bacteria on the order of 104 organisms per litre [35]. The most common bacteria found in hospital wastewater can be those originating from biological waste (faeces, urine, surgical instruments, etc.) of hospitalized patients (Acinetobacter spp., Klebsiella pneumoniae, Proteus mirabilis, Enterobacter spp., Bacillus spp., Salmonella spp., Shigella spp., and Staphylococcus aureus, among others), or bacteria responsible for nosocomial infections (Escherichia coli, Staphylococcus spp., Streptococcus spp., Pseudomonas spp., etc.). Pathogenic bacteria such as Salmonella, especially Salmonella typhi and paratyphi species, are generally more prevalent in hospital-origin urban wastewater and can be harmful to human health while potentially harbouring antibiotic resistance genes (ARGs) [36,37]. The concentrations of identified bacteria are 10 times higher in hospital effluents than in community wastewater [16,37,38].
| Pathogenic species | Load of bacteria detected in 100 ml water effluent | Estimated minimal infecting Dosis |
|---|---|---|
| Campylobacter spp. | 104-105 | 1.103 |
| Clostridium perfringens | 6.104-8.104 | 103-105 spores |
| Escherichia coli | 104-107 | 106-107 ; 10-102 |
| Entérocoques intestinaux | 4.7.103-108 | 60-102 |
| Salmonella spp. | 0.2-8.103 | 104-1010 |
| Vibrio spp. | ND | 1.106 |
| Shigella spp. | 0.1-103 | 10-104 |
Haut du formulaire; NA = not applicable.
Bacteria Isolated in Community Wastewater and Rivers
In developing countries, poverty and a lack of awareness about health risks lead populations to use wastewater as their primary choice for irrigating vegetable gardens [58]. These practices expose vegetable growers to health risks and also lead to the introduction of various contaminants from these waters into the food chain [59]. In most African countries, there are numerous issues related to the quantity and quality of hospital wastewater. In Burkina Faso, Somda et al. reported that hospital wastewater was responsible for the contamination of certain lettuces and other garden products, as they were contaminated with certain antibiotics and bacteria (Salmonella paratyphi B and Salmonella spp.) generated by hospital activities, and these various impacts were identified in the surrounding water bodies [60]. Furthermore, it has been reported in some countries like Benin, Morocco, and Kenya, that hospital wastewater is discharged into community septic tanks due to inappropriate drainage systems [61,62,63].
In Gabon, studies conducted by Jonas Ehrhardt et al. [64] and Yala et al. [65] have shown a high population of enterobacteria in the rivers bordering certain provinces of Gabon. In the first study, they were able to isolate Citrobacter freundii (25.9%, 7/27), Enterobacter spp (25.9%, 7/27), Escherichia coli (3.7%, 1/27), Klebsiella pneumoniae (22.2%, 6/27), Kluyvera ascorbata (3.7%, 1/27), Leclercia adecarboxylata (3.7%, 1/27), Pantoea dispersa (3.7%, 1/27), Serratia marcescens (37%, 10/27), and Yokenella regensburgei (3.7%, 1/27). This corresponds to an overall contamination rate of 13.5% by coliforms. Additionally, a strain of Klebsiella pneumoniae producing extended-spectrum beta-lactamase (ESBL) was found in one of the collected samples [64] (Table 3). In the second study, the authors were able to isolate the following enterobacteria: Enterobacter sakazakii (9.67%, 3/31), Escherichia coli (6.45%, 2/31), Enterobacter cloacae (3.2%, 1/31), Klebsiella ozaenae (3.2%, 1/31), and Klebsiella pneumoniae (3.2%, 1/31) [65].
Table 4.
Transmission of pathogenic bacteria between household effluents and environmental effluents.
Table 4.
Transmission of pathogenic bacteria between household effluents and environmental effluents.
| country | Source | Host (s) | Reference |
|---|---|---|---|
| Benin | Urban wastewater | Eschérichia coli, | [66] |
| RC | Household Wastewater |
Escherichia coli, Salmonella spp., Shigella spp., Klebsiella spp., Enterobacter aerogenes, Enterobacter cloacae , Arizona spp., Proteus spp. |
[67] |
| Gabon | River |
Citrobacter freundii, Enterobacter sp, Escherichia coli, Klebsiella pneumoniae, Kluyvera ascorbata, Leclercia adecarboxylata, Pantoea dispersa; Serratia marcescens; and Yokenella regensburgei, Salmonella enterica |
[64] |
| Tunisia | Urban wastewater | Escherichia coli, Salmonella spp. | [68] |
| Ethiopia | Hospital sewage | Klebsiella spp., P. aeruginosa | [69] |
| DRC | River | Escherichia coli | [70] |
RC: Republic of Congo, DRC: Democratic Republic of Congo.
In estuarine environments or rivers, antibiotic-resistant bacteria and the most stable drug molecules settle in the mudflats [23]. The sediments then become an environment in which subinhibitory concentrations of antibiotic molecules (or their metabolites) can be reached. Potential transfer of resistance genes to native species, followed by retrotransfer to pathogenic strains for humans, is possible, although the probability is low [25].
The Bacteria Isolated from Both Hospital Effluents and Rivers
The number of microorganisms can multiply by a thousand in river waters after urban waste discharge and stagnant waters provide a favourable environment for the development of bacterial biofilms conducive to the contamination of numerous ecosystems [41,42,43]. However, antibioticresistant bacteria naturally exist in many water sources, even in geographical areas without significant antibiotic selection pressure [44,117].
Table 5.
List of Bacteria found in hospital wastewater and some rivers in Africa.
| Species | Country | Water source | Reference |
|---|---|---|---|
| Pseudomonas aeruginosa, salmonella spp. | Ivory Coast | Hospital sewage | [38] |
| Escherichia coli | DRC | Hospital sewage, river | [45] |
| Klebsiella spp. | South Africa | Hospital sewage | [46] |
| Salmonella spp., Pseudomonas spp, and Escherichia coli | Burkina Faso | Hospital sewage | [47] |
|
Klebsiella pneumoniae, Aeromonas spp. and Escherichia coli |
Benin | Hospital sewage | [48] |
| Escherichia coli, Enterococcus faecium, Enterobacter cloacae and Pseudomonas aeruginosa, Acinetobacter townrii | Benin & Burkina Faso | Hospital sewage | [49] |
| E. coli, Klebsiella spp., Salmonella spp, Shigella spp., Citrobacter spp.; Bacillus spp., Proteus spp. | Ethiopia | Hospital sewage | [50] |
|
Klebsiella spp., Pseudomonas spp., E. coli, Citrobacter spp., |
Ethiopia | Hospital sewage | [51] |
DRC: Democratic Republic of Congo.
Antibiotic-Resistant Bacteria Found in Rivers Surrounding Hospitals
Microbial pollutants can also serve as indicators of water quality [52]. Untreated effluents generated by hospital activities can significantly contribute to the spread of microbial pollutants in the environment, particularly multidrug-resistant bacteria (MDR) originating from patient pathological products [53,54]. MDR from effluents primarily stem from either colonized patient biological fluids [15,16] or horizontal transfer of resistance genes between multidrug-resistant infectious strains and environmental strains [55].
In China, a study by Zhang L et al. (2020) demonstrated that the most frequently identified bacteria in the river water receiving hospital effluents were E. coli (37.9%, 25/66), followed by K. pneumoniae (16.7%, 11/66) and Acinetobacter spp. (16.7%, 11/66), but the resistant strains identified in the effluent samples were dominated by Pseudomonas spp. (29.4%, 5/17), Acinetobacter spp. (29.4%, 5/17), and E. coli (23.5%, 4/17). In another study, researchers characterized bacterial populations in surface waters (Xiao River) receiving effluents from an oxytetracycline (OTC) production plant. In upstream river water, only Stenotrophomonas maltophilia isolates showed a significantly higher prevalence of resistance compared to Pseudomonas fragi, Pseudomonas fluorescens, Bacillus cereus, and Pseudomonas putida (paired Wilcoxon test, all ‘p’ values were < 0.009) [56].
In France, the multidisciplinary FLASH project (Fate of Antibiotics, Gene and Antibiotic- Resistant Bacteria Fluxes in Surface Hydrosystems) aimed to study the relationship between antibiotic prescription (both veterinary and human use), antibiotic resistance, and antibiotic molecules in water on the scale of a rural hydrological continuum and a hospital continuum discharging into a Seine tributary (the Risle). The study’s results show the presence of antibioticresistant strains of E. coli and Enterococcus spp. circulating in these waters. This antibiotic resistance selection pressure results from both medical prescriptions in human clinics and veterinary clinics [23].
Antibiotic-Resistant Bacteria (Gram-Negative Bacilli) in Water
Compared with Enterobacterales, few published reports have documented the isolation of class A carbapenemase-producing glucose-non-fermenting Gram-negative bacteria (GNB) from aqueous ecosystems, KPC (Klebsiella pneumoniae carbapenemase), KPC-2-, GES variants (for Guiana extended spectrum). The GES-5 enzyme has been detected in K. pneumoniae isolated from stream water [60] , in R. ornithinolytica and Citrobacter sp. Recovered from river water [57,59], in Enterobacter spp. isolates obtained from seawater [25,48], in Citrobacter spp., E. coli, K. pneumoniae, K. oxytoca and E. cloacae obtained from hospital sewage [53,61,62], in E. cloacae complex, in K. pneumoniae and in R. ornithinolytica isolated from wastewater treatment plants (WWTPs) [53,57,63], and GES-16 producing Acinetobacter spp. and Aeromonas spp. isolates were recovered from WWTPs, hospital sewage, and river and seawater samples in the USA, Brazil and China [118,119,120,122,123,125]. In addition, the GES-31 carbapenemase was first described in an Aeromonas punctata isolate recovered from a Brazilian river [121] de Araujo et al. and Xu et al. have reported the isolation of KPC-2-producing Aeromonas hydrophila from rivers in Brazil and China, respectively [121,127]. Recently, KPC-2-producing A. hydrophilia and Aeromonas caviae were recovered from river water and WWTP effluents [124,126].
Characterization of ESBLs in Wastewater
Numerous studies have found significant quantities of bacteria producing extended-spectrum beta-lactamases (ESBL-producing E. coli) in community and hospital effluents, as well as in bathing waters, with more ESBL-producing E. coli in hospital wastewater than in community wastewater [3]. This can be explained, in part, by a higher frequency and density of carriage among hospitalized patients compared to healthy community carriers [82]. On the other hand, the high consumption of antibiotics in hospitals leads to their elimination in the form of compounds that are still active in wastewater. These compounds exert a selection pressure that favours resistant bacteria, including extended spectrum β-lactamases (ESBLs) [93]. These enzymes that hydrolyze broad-spectrum penicillins and cephalosporins were initially derived from narrow-spectrum plasmidic penicillinases and were mainly found in hospital strains of Klebsiella pneumoniae [80,81] and Klebsiella oxytoca [37].
Table 6.
Bacteria capable of producing ESBLs encountered in effluents (Hospitals and rivers).
| Country | Source | Host | ESBLs | Reference |
| Ghana | River waters | Escherichia coli | P, E. coli | [83] |
| South Africa | Sewage | Escherichia coli | P, E. coli | [84] |
| Burkina Faso | Sewage | Klebsiella oxytoca, Serratia spp, Citrobacter spp, | P, Klebsiella oxytoca | [85] |
| Cameroun | Well water | E. Coli, Salmonella spp, P. aeroginosa, Klebsiella pneumoniae et Bulkholderia cepaceae | P, E. coli | [86] |
| Ivory Coast | Hospital sewage | E. coli, K. pneumoniae, P. aeruginosa et Acinetobacter baumanii | P, Acinetobacter baumanii | [115] |
| Nigeria | Hospital sewage | E. coli, Klebsiella pneumoniae, E. coli, K. pneumoniae | P, E. coli & K. pneumoniae | [87] |
| Ethiopia | Sewage |
E.coli, Salmonella, Klebsiella pneumonia, Enterobacter aerogenes, Citrobacter, Klebsiella oxytoca and Enterobacter cloacae, |
P, K. pneumonia & E. coli | [88] |
P: Positive at ESBL.
Characterization of Antibiotic Resistance Genes in Bacteria Isolated from Wastewater
In South Africa, for Fadare F. T et al., among the 31 bacterial species isolated in this study, genes encoding for beta-lactamases were detected in 20 species (64.5%, 20/31), while resistance genes to other antibiotic families were detected in 27 species (87.1%, 27/31). The most commonly detected beta-lactam resistance genes belonged to the blaCTX-M group (including groups 1, 2, and 3), which were detected in isolates at a rate of 51.6% (16/31) [18]. In China, on the other hand, other authors were able to determine (66.3%, 69/104) the blaCTX-M-type gene in water samples [7]. In the same study by Fadare F. T, they showed that the most frequently detected resistance genes to other antibiotic families were CatII (79.2%, 19/24) (acting against Phenicol), followed by the tetA gene (46.7%, 14/30) (against Tetracyclines). The frequencies of other non-beta-lactam genes include sulI and sulII (35.5%, 11/31) (against Sulfamides), tetB (23.3%, 7/30), aadA (12.9%, 4/31) (against Aminoglycosides), tetC (10%, 3/30), and tetD (3.3%, 1/30) [18].
The Fate of Hospital Antibiotics in Natural Environments
The danger of pharmaceutical substances in the environment lies in the fact that they can behave from a physico-chemical perspective like substances secreted by the host organism, thus retaining their effectiveness [89]. They can also substitute for molecules or bind to specific receptors within the recipient organism. Furthermore, these substances may follow the path of bioaccumulation of antibiotics in organisms and affect ecosystem functioning [90].
Also, the low concentrations of drugs and their metabolites, generally lower than those encountered in therapy, do not allow for an accurate estimation of the actual presence of these substances in the environment [116].
Fecal bacteria and chemical contaminants associated with suspended matter in the water column settle in the mudflats, and sediment accumulation zones [92]. In these sediments, it has been shown that antibiotics persist for more than 30 years, at concentrations reaching 32 mg/kg for quinolones, 15 mg/kg for sulfamides, and 20 mg/kg for nalidixic acid [92]. The risk associated with certain antibiotics such as doxycycline, oxytetracycline, and levofloxacin lies in their elimination by the organism in an active form (bioactive molecules), potentially dangerous for the environment [91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116].
Risk of Contaminated Water in Aquatic Animals
Aquatic environments constitute important reservoirs of antibiotic-resistance genes. They also serve as a vehicle through which antibiotic-resistance genes (ARGs) or antibiotic-resistant bacteria (ARB) can be disseminated from one ecosystem to another [100]. The effects of these anthropogenic inputs on the bacterial flora of the aquatic environment are still poorly understood. However, the genomes of aquatic bacteria are particularly rich in mobile genetic elements involved in the selection and dissemination of resistance genes [101]. For example, qnrA and qnrS, plasmidic resistance genes to quinolones, have been mobilized from the genomes of Shewanella algae and Vibrio splendidus [102].
The bioaccumulation of antibiotics in wild fish species has been observed by Valdés et al. [103]. Erythromycin was the most commonly observed antibiotic in the crustacean Fenneropenaeus penicillatus at the adult stage, at concentrations ranging from 2,498 to 15,090 ng/g-1 [104]. When the aquatic environment receives inputs from animal or anthropogenic sources, the number and type of bacteria present can render the water unfit for human and animal use [105,106].
Consequences of Contamination Related to Hospital Wastewater
Most diseases resulting from contact with wastewater are caused by pathogenic germs such as bacteria. These pathogens can cause severe illnesses, especially in particularly vulnerable groups (children, the elderly, and individuals with weakened immune systems), and workers in contact with such waters, such as sewage workers and wastewater treatment plant employees [91].
Consuming Untreated Water Can Lead to Waterborne Illnesses
Therefore, water, vital for existence, can also be a source of water-related diseases [107]. According to the World Health Organization (WHO), 361,000 children under the age of 5 die each year from diarrheal diseases due to inadequate access to clean water and sanitation [108]. Human health is seriously affected by water-related diseases, as well as by pollution from chemical discharges into water from various human activities. According to UNICEF, 60% of child mortality worldwide is due to infectious or parasitic diseases, mostly related to water pollution [109,110,111]. Moreover, if measures are not taken to combat antibiotic resistance, it is estimated that by 2050, antibiotic-resistant bacteria could be responsible for the deaths of 10 million people annually worldwide, including 390,000 people in Europe. Global economic losses would amount to 100.000 billion euros [112].
Conclusions
This review has demonstrated the potential relationship between hospital effluents and environmental contamination by antibiotic-resistant bacteria. Therefore, it is essential to consider the entire chain of the issue to study prevention measures effectively. The genetic diversity of naturally occurring bacteria in the environment makes them a natural reservoir of resistance genes. The spread of antibiotic-resistant bacteria and their genes in hospital wastewater could, in turn, worsen their presence in the environment. Further studies are needed to assess the impact of antibiotic-resistant bacteria and their genes in watercourses. Ensuring the good quality of water before discharge helps maintain a minimally or non-polluted environment while ensuring the health of the population.
Funding
This research received no external funding.
References
- Darsy, Coralie, Lescure, Irène, Payot, Véronique, G Rouland. Effluents des établissements hospitaliers: teneur en microorganismes pathogènes, risques sanitaires, procédures particulières d’épuration et de gestion des boues. Mémoire. Office international de l’eau, service national d’information et de documentation sur l’eau, 2002, p 3. Available online: https: // http://greeqs.free.fr/siteeqs/eau/textes/nonregl/aut-02-02a.pdf (accessed on 25 june 2023).
- Julien Passerat, Fatima Tamtam, Barbara Le Bot, Joëlle Eurin, Marc Chevreuil et Pierre Servais. Rejets hospitaliers d’antibiotiques et de bactéries fécales antibiorésistantes dans les rivières du bassin de la Seine. Eur. J. Water Qual. 2010; 26.41, 1–13. [CrossRef]
- Bréchet, C., Hocquet, D., et Bertrand, X. Eaux usées et Escherichia coli producteur de β-lactamases à spectre étendu. J Anti-infect, 2015; 17 (2), 53-59. [CrossRef]
- Kolpin, Dana W., Skopec, Mary, Meyer, Michael T., et al. Urban contribution of pharmaceuticals and other organic wastewater contaminants to streams during differing flow conditions. Sci. Total Environ, 2004; 328, 1-3, 119-130. [CrossRef]
- Watkinson, A. J., Murby, E. J., Costanzo, S. D. Removal of antibiotics in conventional and advanced wastewater treatment: implications for environmental discharge and wastewater recycling. Water Res, 2007; 41, (18), 4164-4176. [CrossRef]
- Mbog, Mbog S., Nguidjoe, Evrard Marcel, Djocgoue, Pierre F., et al. Évaluation de la gestion des déchets liquides hospitaliers du Centre Hospitalier Universitaire de Yaoundé I (CHU): cas des eaux usées. Sci. Nat. Appl, 2019; 38, 2.
- Luhua Zhang, Xinyue Ma, Li Luo, Nan Hu, Jiayao Duan, Zhongjian Tang, Rujie Zhong and Ying LI. The Prevalence and Characterization of Extended-Spectrum -Lactamase- and Carbapenemase-Producing Bacteria from Hospital Sewage, Treated Effluents and Receiving Rivers. Int. J. Environ. Res. Public Health 2020; 17, 1183. [CrossRef]
- Parveau P, Bactéries multi résistantes dans l’environnement : recherche dans les effluents de la ville de TOULOUSE, Université de Limoges, France. 2011; p 55. Available online: https:// https://scholar.google.fr/scholar?hl=fr&as_sdt=0%2C5&q=Parveau+P%2C+Bact%C3%A9ries (accessed on 25 April 2023).
- Julia Baudart and Nathalie Paniel. Sources et devenir des micro-organismes pathogènes dans les environnements aquatiques Sources and fate of pathogenic microorganisms in aquatic environments. Rev Fran des Lab, 2014; 459, 29-39. [CrossRef]
- Peralta, Denisse Archundia. Etude du devenir et de l’impact des antibiotiques à l’échelle d’un bassin versant: application au bassin versant du Katari (Bolivie). Diss. Université Grenoble Alpes, 2016.
- Orias Frédéric et Perrodin, Yves. Characterisation of the ecotoxicity of hospital effluents: a review. Sci. Total Environ, 2013; 454, 250-276. [CrossRef]
- Silva B, Costa F, Neves IC, Tavares T. Psychiatric Pharmaceuticals as Emerging Contaminants in Wastewater. Springer International Publishing; 2015. Available online: https:// link.springer.com/book/10.1007/978-3-319-20493-2.
- Chamkal N., Lhlou I., Bandadi L., Ounine K. Hospital Antibiotics Usage: Environmental Hazard and Promotion of Antibiotic Resistant Bacteria. Ann Ig, 2022; 34 (3): 266-278. [CrossRef]
- Haguenoer Jean-Marie. Does Pharmaceutical Waste and Drug Residue Pose a Risk to Public Health? Sante Publique, 2010; 22 (3), 325-342.
- Akoua-Koffi, C., Guessennd, N., Gbonon, V., et al. La méticillino-résistance de Staphylococcus aureus isolés à Abidjan (1998–2001): un nouveau problème en milieu hospitalier. Méd Mal Infect, 2004, 34 (3), 132-136. [CrossRef]
- Guessennd, N., Bremont, S., Gbonon, V., et al. Résistance aux quinolones de type qnr chez les entérobactéries productrices de bêta-lactamases à spectre élargi à Abidjan en Côte d’Ivoire. Pathol. Biol. 2008; 56, (7-8), 439-446. [CrossRef]
- Lamprecht C, Romanis M, Huisamen N, Carinus A, Schoeman N, Sigge Go, et al. Escherichia coli with virulence factors and multidrug resistance in the Plankenburg River. S Afr J Sci, 2014; 110: 1–6. [CrossRef]
- Fadare Ft, Okoh Anthony Ifeanyi, Distribution and molecular characterization of ESBL, pAmpC β-lactamases, and non-β-lactam encoding genes in Enterobacteriaceae isolated from hospital wastewater in Eastern Cape Province, South Africa, Plos One, 2021; 16 (7), e0254753. [CrossRef]
- Corvaisier, N. Les substances médicamenteuses rejetées dans les eaux urbaines. Ecole Nationale du Génie Rural des Eaux et des Forets. Centre de Montpellier-Février, France, 2000.
- Davies, Julian et Davies, Dorothy. Origins and evolution of antibiotic resistance. Microbiol. Mol. Biol. Rev., 2010; 74 (3), 417-433. [CrossRef]
- Garric, Jeanne et Ferrari, Benoît. Les substances pharmaceutiques dans les milieux aquatiques. Niveaux d’exposition et effet biologique: que savons-nous?. Rev. Sci. Eau, 2005; 18 (3), 307-330. [CrossRef]
- Heberer Thomas. Occurrence, fate, and removal of pharmaceutical residues in the aquatic environment: a review of recent research data. Toxicol. lett, 2002; 131, (1-2), 5-17. [CrossRef]
- Mater, Nicolas, Geret, Florence, Castillo, Luis, et al. In vitro tests aiding ecological risk assessment of ciprofloxacin, tamoxifen and cyclophosphamide in range of concentrations released in hospital wastewater and surface water. Environ. Int., 2014; 63, 191-200. [CrossRef]
- Oberlé K, Capdeville Mj, Berthe T, Budzinski H, Petit F. Evidence for a complex relationship between antibiotics and antibiotic-resistant Escherichia coli: from medical center patients to a receiving environment. Environ Sci Technol, 2012; 46: 1859-68.ORIAS. [CrossRef]
- Berthe T, Ratajczak M, Clermont O, Denamur E, Petit F. Evidence for coexistence of distinct Escherichia coli populations in various aquatic environments and their survival in estuary eater. Appl Environ Microbiol, 2013; 79: 4684-93. [CrossRef]
- Fabienne Petit. L’antibiorésistance dans les environnements aquatiques: une problématique d’écologie microbienne et de santé publique, Environ Risque Sante, 2018; 17 (1), 40-46.
- Kingsley Ehi Ebomah and Anthony Ifeanyi Okoh. An African perspective on the prevalence, fate and effects of carbapenem resistance genes in hospital effluents and wastewater treatment plant (WWTP) final effluents: A critical review. Heliyon 6, 2020; e03899. [CrossRef]
- Emmanuel, Evens, Perrodin, Yves, Keck, Gérard, Blanchard, J. M., & Vermande, P. Effects of hospital wastewater on aquatic ecosystem. In: Proceedings of the XXVIII Congreso Interamericano de Ingenieria Sanitaria y Ambiental. Cancun, México. 2002. 27-31.
- Ngankem Ngankem Ii, Aurelien Flavien. Evaluation de la gestion des déchets biomédicaux liquides dans les centres hospitaliers universitaires du Point G et Gabriel Touré. Thèse de doctorat. Université des Sciences des Techniques et des Technologies de BAMAKO, Mali. 2014. Available online: https://bibliosante.ml/handle/123456789/736 (accessed on 25 April 2023).
- Akin, Beril Salman, et al. Contaminant properties of hospital clinical laboratory wastewater: a physiochemical and microbiological assessment. J. Environ, 2016, 7 (5), 635. [CrossRef]
- Al-Ajlouni, Kholoud, Shakhatreh, Saleh, Al-Ibraheem, N., Jawarneh, M. Evaluation of wastewater discharge from hospitals in Amman–Jordan. J Basic Appl Sci, 2013, 13 (4), 44-50.
- Mahvi, A. H., Ghanbarian, M., Nasseri, S., et al. Mineralization and discoloration of textile wastewater by TiO2 nanoparticles. Desalination, 2009; 239 (1-3), 309-316. [CrossRef]
- Ibeh, I. N. and Omoruyi, M. I. Seasonal Dynamics in the physiochemical parameters of hospital effluent from a university teaching hospital based in Southern Nigeria. Asian J. Sci. Res, 2011; 1 (1), 7.
- Qadouri Asmaa, Mouhir Latifa, Belkadi MS. Application d’une méthode d’étude quantitative et qualitative des rejets liquides hospitaliers au niveau de la Région de Marrakech Tensift El Haouz, Maroc. Eur Sci. J, 2016; 12 (32), 110-130. [CrossRef]
- Koutchika, Olga, SALOU, Souwébatou, et DEGBEY, Comlan Cyriaque. Gestion des déchets biomédicaux liquides dans les maternités des formations sanitaires publiques de la commune de Sème-Podji. EPAC/CAP/UAC, 2019.
- Benneni Halima, Bouarissa Besma. Epuration des eaux usées, analyse et synthèse des données scientifiques. Cas de la station d’épuration des eaux de la wilaya de Bordj Bou Arreridj: Prospection, évaluation du rendement épuratif. Diss. Mémoire de Master. 2020. m596. pdf (univ-bba.dz) Available online: (accessed on 15 March 2023).
- Hocquet Didier, Muller Allison, et Bertrand, Xavier. What happens in hospitals does not stay in hospitals: antibiotic-resistant bacteria in hospital wastewater systems. J. Hosp. Infect, 2016; 93 (4), 395-402.
- Amarachukwu Obayiuwana, Adeniyi Ogunjobi, Min Yang and Mark Ibekwe. Characterization of bacterial communities and their antibiotic resistance profiles in wastewaters obtained from pharmaceutical facilities in Lagos and Ogun States, Nigeria. Int. J. Environ. Res. Public Health, 2018, 15 (7), 1365. [CrossRef]
- Placide, Sadia Sahi, Ollo, Kambiré, Quand-Même, Gnamba Corneil, et al. Mineralization of Wastewater from the Teaching Hospital of Treichville by a Combination of Biological Treatment and Advanced Oxidation Processes. Asian J Chem Sci, 2021, 10 (2): 1-10. [CrossRef]
- Derolez Valérie. Méthode de caractérisation de la fragilité microbiologique des zones conchylicoles. Rapport ENSP, 2003. Available online: https: // https://documentation.ehesp.fr/memoires/2003/igs/derolez.pdf (accessed on 25 April 2023).
- World Health Organization. Guidelines for safe recreational water environments: Coastal and fresh waters. Vol. 1. World Health Organization, 2003.
- Gotkowska-Płachta, A. The prevalence of virulent and multidrug-resistant enterococci in river water and in treated and untreated municipal and hospital wastewater. Int. J. Environ. Res. Public Health, 2021; 18 (2), 563. [CrossRef]
- Rouquet, R. M. La légionellose: la bactérie et les données épidémiologiques. Lett. pneumol, 2005; 8 (1), 17-20.
- Walia, S., Murleedharn, C., Band, J., Kanwar, M., & Kumar, A. Quantitation of antibiotic resistance genes pollution in hospital waste water effluent and Urban Clinton River Water, Michigan, USA. Curr. Med. Res. Pract, 2016; 6 (4), 149-151. [CrossRef]
- Lévi Yves. Inquiétudes sur la présence d’antibiotiques et de bactéries antibiorésistantes dans les eaux. Environ. Risques Santé, 2006; 5 (4), 261-265.
- Laffite, Amandine, Kilunga, Pitchouna I., Kayembe, John M., et al. Hospital effluents are one of several sources of metal, antibiotic resistance genes, and bacterial markers disseminated in Sub-Saharan urban rivers. Front. Microbiol, 2016; 7, 1128. [CrossRef]
- King Tlb, Schmidt S, Essack Sy. Antibiotic resistant Klebsiella spp. from a hospital, hospital effluents and wastewater treatment plants in the uMgungundlovu District, KwaZulu-Natal, South Africa. Sci Total Environ, 2020; 712: 135550. [CrossRef]
- Ouedraogo, Ganamé Abasse, Kone, Souleymane, Ouedraogo, Arouna, et al. Ecotoxicity of hospital wastewaters and their impact on bacterial multi-drug resistance: a review. Jlife Sci. Biomed, 2021; 11 (4), 58- 71. [CrossRef]
- Koudokpon, H., Dougnon, V., Lougbegnon, C., Agbankpe, A. J., Avodagbe, G., Saidou, S., ... & Baba- Moussa, L. Emergence of Multidrug-resistance Bacteria Isolated of Drinking Water, Groundwater and Hospital Wastewater in Southern Benin: Antibiotic Resistance Profile and Resistomes Determination. Res Sq. 2021. [CrossRef]
- Markkanen, Melina A., Haukka, Kaisa, Pärnänen, Katariina MM, et al. Metagenomic analysis of the abundance and composition of antibiotic resistance genes in hospital wastewater in Benin, Burkina Faso, and Finland. Msphere, 2023; 8, 1, e00538-22. [CrossRef]
- Fekadu, Sintayehu, Merid, Yared, Beyene, Hunachew, et al. Assessment of antibiotic-and disinfectantresistant bacteria in hospital wastewater, south Ethiopia: a cross-sectional study. J. Infect. Dev. Ctries, 2015; 9, (2), 149-156. [CrossRef]
- Moges, Feleke, Endris, Mengistu, Belyhun, Yeshambel, et al. Isolation and characterization of multiple drug resistance bacterial pathogens from waste water in hospital and non-hospital environments, Northwest Ethiopia. BMC Res. Notes, 2014; 7, 1-6. [CrossRef]
- Radhakrishna L, Nagarajan P. Isolation and Preliminary Characterization of Bacterial from Liquid Hospital Wastes. Int J Pharmtech Res, 2015; 8 (2), 308–314.
- Dhafer Mmas, Georgette Nn, Amandine L, Jean-Paul O, Crispin M, John P. Ecotoxicology and Environmental Safety Hospital wastewaters: A reservoir and source of clinically relevant bacteria and antibiotic resistant genes dissemination in urban river under tropical conditions. Ecotoxicol. Environ. Saf. 2020; 200, 9.
- Jyothirmai Vk, Sharmila Smr, Arun S. Degradation of ciprofloxacin using fenton process and its effect on biodegradability. Rasayan J. Chem, 2020; 13 (4), 2274–2280.
- Thomas, Kevin V., Dye, Christian, Schlabach, Martin, Langford, K. H. Source to sink tracking of selected human pharmaceuticals from two Oslo city hospitals and a wastewater treatment works. J Environ Monitor, 2007; 9 (12), 1410-1418. [CrossRef]
- Dong Li, Tao Yu, Yu Zhang, Min Yang, Zhen Li, Miaomiao Liu, and Rong Qi. Antibiotic Resistance Characteristics of Environmental Bacteria from an Oxytetracycline Production Wastewater Treatment Plant and the Receiving River. Appl. Environ. Microbiol. 2010; 76 (11), 3444–3451. [CrossRef]
- Petit F, Denamur E, Clermont O, et al. Fate of antibiotic and antibiotic-resistant fecal bacteria in water and sediments from the contamination source to the estuary: impact and/or resilience? In: Marine productivity: perturbation and resilience of socio-ecosystem. Springer Verlag, 2014. Available online: hps://link.springer.com/chapter/10.1007/978-3-319-13878-7_9 (accessed on 25 May 2023).
- Kapepula L, Ndikumanat, Dieu-Donné M, Alconero Pl, Tamungang Neb, Tarimo I, Bruggen Bvd. Qualitative and quantitative analysis of the pollutant load of effluents discharged Northwestern of Lake Tanganyika, in the Democratic Republic of Congo. Afr. J. Environ. Sci. Technol. 2020; 14, 11, 361–373. [CrossRef]
- Dubois-Brissonnet F, Guillier L. Les maladies microbiennes d’origine alimentaire. Cah. de Nutr. Diet. 2020; 55 (1), 30–38. [CrossRef]
- Siourimè, Somda Namwin, Isidore, Bonkoungou Ouindgueta Juste, Oumar, Traoré, et al. Serotyping and antimicrobial drug resistance of Salmonella isolated from lettuce and human diarrhea samples in Burkina Faso. Afr J Infect Dis, 2017; 11 (2), 24-30. [CrossRef]
- K’oreje Kold, Vergeynst D, Ombaka P, De Wispelaere M, Okoth Ch, Langenhove Kv. Chemosphere Occurrence patterns of pharmaceutical residues in wastewater, surface water and groundwater of Nairobi and Kisumu city, Kenya. Elsevier (Chemosphere). 2016; 149 (238–244), 7. [CrossRef]
- Asmaa Qlm, Said B. M. Application d’une méthode d’étude quantitative et qualitative des rejets liquides hospitaliers au niveau de la Région de Marrakech Tensift El Haouz, Maroc. Eur. Sci. J. 2016 ; 12 (32), 110–130. [CrossRef]
- Elias A, Kanhounnon Sa, Gbèdodé W, Boni Cc, Dogbè Ca, Koumolou L, Bonou B, Fiogbe Ed, Aléodjrodo Pe. Physicochemical and microbiological characterization of effluents from the “Centre Hospitalier Universitaire de la Mère et d e l’Enfant Lagune (CHU-MEL)” discharged in the Cotonou lagoon in Benin. Int. J. Biol. Chem. Sci. 2018; 12 (1991–8631), 1955–1964. [CrossRef]
- Ehrhardt, Jonas, Alabi, Abraham S., Kremsner, Peter G., Rabsch, W., Becker, K., Foguim, F. T.. Bacterial contamination of water samples in Gabon, 2013. J Microbiol, Immunol Infect, 2017; 50 (5), 718-722. [CrossRef]
- Yala, Jean-Fabrice, Souza, Alain, Lebamba, JudicaëL, et al. Etude préliminaire de l’évaluation des paramètres physico-chimiques, détection et dénombrement des coliformes totaux et fécaux dans quelques lacs de la ville de Franceville [Preliminary study of the evaluation of physicochemical parameters, detection and enumeration of total and faecal coliforms in some lakes of the town of Franceville (Gabon). Int. J. Innov Appl. Stud, 2017; 20 (3), 963-974. [CrossRef]
- Mathieu Hounsou, Euloge K. Agbossou, Bernard Ahamide et Irenikatche Akponikpe, Qaulité bactériologique de l’eau du bassin de l’Ouémé: cas de coliformes totaux et fécaux dans les retenues d’eau de l’Okpara, de Djougou et de Savalou au Bénin. Int. J. Chem. Sci, 2010, 4 (2), 377-390.
- Moyen, Rachel, Ngoulou, Tarcisse Baloki, Nguimbi, Etienne, et al. Antibiotic Resistance Phenotypes of Enterobacteriaceae Isolated from Household Wastewater in Brazzaville, Republic of Congo. Adv. Microbiol, 2021; 11 (1), 27-36. [CrossRef]
- Salem, Imen Ben, Ouardani, Imen, Hassine, Mouna, et al. Bacteriological and physico-chemical assessment of wastewater in different region of Tunisia: impact on human health. BMC Res Notes, 2011; 4 (1), 1-11. [CrossRef]
- Asfaw, Tsegahun, Negash, Letemichael, Kahsay, Amlsha, et al. Antibiotic resistant bacteria from treated and untreated hospital wastewater at Ayder Referral Hospital, Mekelle, North Ethiopia. Adv. Microbiol, 2017, 7 (12), 871-886. [CrossRef]
- Tshibanda, Joseph B., Devarajan, Naresh, Birane, Niane, et al. Microbiological and physicochemical characterization of water and sediment of an urban river: N’Djili River, Kinshasa, Democratic Republic of the Congo. Sustain. Water Qual. Ecol, 2014; 3, 47-54. [CrossRef]
- Touati A, Benallaoua S, Kecha M Et Idres N. Etude des phénotypes de résistance aux β-lactamines des souches d’entérobactéries isolées, en milieu hospitalier : cas de l’hôpital d’Amizouk (W. Bejaia). Sci. Technol, 2003; 19: 92-7.
- Alexy Radka, Kümpel Tina, Kümmerer Klaus. Assessment of degradation of 18 antibiotics in the closed bottle test. Chemosphere. 2004; 57, (6), 505-51. [CrossRef]
- Aminata Maiga, Nathalie Aya Nguessend, Oumar Agaly Dicko, Modibo Fofana, Ibrahim Izetiégouma Maiga, Koumba Soumahoro Man Agbo, Mireille Dosso. Les résidus d’antibiotiques dans les effluents hospitaliers de BAMAKO (MALI), Mali medical, 2018; 33 (3).
- Boillot, Clotilde. Évaluation des risques écotoxicologiques liés aux rejets d’effluents hospitaliers dans les milieux aquatiques. Contribution à l’amélioration de la phase «caractérisation des effets». Diss. INSA de Lyon. 2008. Thèse de doctorat. 2008. Available online:https://www.bing.com/search?q=Billau+Pascal%2C+2008.+Estimation+des+dangers+de+d%C3%A9 chets+ (accessed on 2 May 2023).
- Somda, Namwin Siourime, Isidore Juste O. Bonkoungou, Bissoume Sambe-Ba, Moustapha Soungalo Drabo, Abdoul Aziz Wane, Hagr’etou Sawadogo-Lingani, Aly Savadogo. Diversity and antimicrobial drug resistance of non-typhoid Salmonella serotypes isolated in lettuce, irrigation water and clinical samples in Burkina Faso. J. Agric. Food Res; 2021; 5; , 100-167. [CrossRef]
- Frédéric, Orias and Yves, Perrodin. Pharmaceuticals in hospital wastewater: their ecotoxicity and contribution to the environmental hazard of the effluent. Chemosphere, 2014, 115, 31-39. [CrossRef]
- Lévi Yves. Contamination des eaux par les résidus de médicaments et stratégies de prévention Contamination of waters by drug residues and prevention strategies. Elsevier, 2020; 59; 18-23.
- Kolpin, Dana W., Furlong, Edward T., Meyer, Michael T., et al. Pharmaceuticals, hormones, and other organic wastewater contaminants in US streams, 1999− 2000: A national reconnaissance. Environ Sci. Technol., 2002; 36 (6), 1202-1211. [CrossRef]
- Besse, Jean-Philippe et Garric, Jeanne. Médicaments à usage humain : risque d’exposition et effets sur les milieux récepteurs. Proposition d’une liste de médicaments à usage humain à surveiller dans les eaux de surface continentales. irstea. 2007, pp.260. ⟨hal-02590157.
- Abdoul-Salam Ouedraogo. Prévalence, circulation et caractérisation des bactéries multirésistantes au Burkina Faso. Université Montpellier, France, 2016Ladjal, Salima, and Amira Baghdadi. Mécanismes de résistance aux β-lactamines chez Escherichia coli au niveau des hôpitaux algériens. Thèse de doctorat. Universite Mohamed Boudiaf-M’sila, Algérie, 2021.
- Ruppé, E., Lixandru, B., Cojocaru, R., Büke, Ç., Paramythiotou, E., Angebault, C., ... & Andremont, A. Relative fecal abundance of extended-spectrum-β-lactamase-producing Escherichia coli strains and their occurrence in urinary tract infections in women. Antimicrobial agents and chemotherapy. 2013; 57 (9), 4512-4517. [CrossRef]
- Banu, Regina Ama, Alvarez, Jorge Matheu, REID, Anthony J., et al. Extended Spectrum Beta-Lactamase Escherichia coli in river waters collected from two cities in Ghana, 2018–2020. Trop. Med. Infect, 2021, 6 (2), 105. [CrossRef]
- Gumede, S. N., Abia, A. L., Amoako, D. G., & Essack, S. Y. Analysis of wastewater reveals the spread of diverse extended-spectrum β-lactamase-producing E. coli strains in uMgungundlovu District, South Africa. Antibiotics. 2021; 10 (7), 860. [CrossRef]
- Soré, Souleymane, Sawadogo, Yacouba, Bonkoungou, Juste Isidore, et al. Detection, identification and characterization of extended-spectrum beta-lactamases producing Enterobacteriaceae in wastewater and salads marketed in Ouagadougou, Burkina Faso. Int J. Biol. Chem. Sci. 2020; 14 (8), 2746-2757. [CrossRef]
- Viban, Tangwa Bernard, Herman, Okah-Nnane Ndode, Layu, Tangwa Clotilda, et al. Risk factors contributing to microbiological contamination of boreholes and hand dug wells water in the Vina Division, Adamawa, Cameroon. Adv. Microbiol, 2021; 11 (2), 90-108. [CrossRef]
- Atta, H. I., Idris, S. M., Gulumbe, B. H., et al. Detection of extended spectrum beta-lactamase genes in strains of Escherichia coli and Klebsiella pneumoniae isolated from recreational water and tertiary hospital waste water in Zaria, Nigeria. Int. J. Environ Health Res, 2022, 32 (9), 2074-2082. [CrossRef]
- Tesfaye, Hemen, Alemayehu, Haile, Desta, Adey F., et al. Antimicrobial susceptibility profile of selected Enterobacteriaceae in wastewater samples from health facilities, abattoir, downstream rivers and a WWTP in Addis Ababa, Ethiopia. Antimicrob. Resist. Infect. Control, 2019; 8 (1), 1-11. [CrossRef]
- Khaled Hassine and Ridha Hamza. Les Risques Lies Aux Eléments Biologiques Et Minéraux Des Eaux Usées Urbaines. Institut d’Aménagement et d’Urbanisme de la Région Ile de France. 2004. Available online: https:// http://193.95.84.5/revue_sante_pub/3-4.pdf (accessed on 25 April 2022).
- Puckowski, Alan, Mioduszewska, Katarzyna, Łukaszewicz, Paulina, et al. Bioaccumulation and analytics of pharmaceutical residues in the environment: A review. J. Pharm. Biomed. Anal, 2016; 127, 232-255. [CrossRef]
- Bilal, M., Ashraf, S. S., Barceló, D., & Iqbal, H. M. Biocatalytic degradation/redefining “removal” fate of pharmaceutically active compounds and antibiotics in the aquatic environment. Sci. Total Environ, 2019, 691, 1190-1211. [CrossRef]
- Tamtam F, Le Bot B, Dinh T, et al. A 50-year record of quinolone and sulphonamide antimicrobial agents in Seine River sediments. J Soils Sed, 2011; 11: 852-9. [CrossRef]
- Coutu S, Rossi L, Barry DA, Rudaz S, Vernaz N. Temporal variability of antibiotics fluxes in wastewater and contribution from hospitals. PLoS One, 2013;8:e53592. [CrossRef]
- Montezzi LF, Campana EH, Correa LL, et al. Occurrence of carbapenemase-producing bacteria in coastal recreational waters. Int J Antimicrob Agents 2015;45: 174–7. [CrossRef]
- Paschoal RP , Campana EH , Correa LL , et al. Concentration and variety of carbapenemase producers in recreational coastal waters showing distinct levels of pollution. Antimicrob Agents Chemother 2017;61:e01963 -17. [CrossRef]
- Gomi R, Matsuda T, Yamamoto M, et al. Characteristics of carbapenemase-producing Enterobacteriaceae in wastewater revealed by genomic analysis. Antimicrob Agents Chemother 2018;62:e02501 -17. [CrossRef]
- Mathys DA, Mollenkopf DF, Feicht SM, et al. Carbapenemase-producing Enterobacteriaceae and Aeromonas spp. present in wastewater treatment plant effluent and nearby surface waters in the US. PLoS One, 2019;14:e0218650. [CrossRef]
- Teixeira P, Tacao M, Pureza L, et al. Occurrence of carbapenemase-producing Enterobacteriaceae in a Portuguese river: bla NDM , bla KPC and bla GES among the detected genes. Environ Pollut 2020;260: 113913.
- Manageiro V, Ferreira E, Canica M, et al. GES-5 among the β-lactamases detected in ubiquitous bacteria isolated from aquatic environment samples. FEMS Microbiol Lett 2014;351: 64–9. [CrossRef]
- Sivalingam, Periyasamy, Poté, John, et Prabakar, Kandasamy. Environmental prevalence of carbapenem resistance Enterobacteriaceae (CRE) in a tropical ecosystem in India: human health perspectives and future directives. Pathogens, 2019; 8 (4), 174. [CrossRef]
- Jean Lesne, Sandrine Baron. La résistance bactérienne aux antibiotiques : stratégies de lutte One Health ou Global Health et normes sociales de comportement individuel. Environ. Risques Santé. 2022; 4 ; 4 (21), 303-309. [CrossRef]
- Briet, Arnaud. “Étude de la flore bactérienne et de sa résistance aux antibiotiques des produits de la pêche et de l’aquaculture.” Université du Littoral Côte d’Opale, 2018. Thèse de doctorat. 2018. Available online: https: //scholar. google.com /scholar?hl =fr&as_sdt =0%2C5&q= Briet+Arnaud.+%22%C3%89tude+de+la+flore+bact%C3%A9rienne+et+de+ (accessed on 2 May 2023).
- Valdés, F., Camiloti, P. R., Rodriguez, R. P., Delforno, T. P., Carrillo-Reyes, J., Zaiat, M., & Jeison, D. Sulfideoxidizing bacteria establishment in an innovative microaerobic reactor with an internal silicone membrane for sulfur recovery from wastewater. Biodegradation. 2016; 27, 119-130. [CrossRef]
- Peralta, Denisse Archundia. Etude du devenir et de l’impact des antibiotiques à l’échelle d’un bassin versant: application au bassin versant du Katari (Bolivie). Université Grenoble Alpes, France. 2016. Available online: https://theses.hal.science/tel-01530466/ (accessed on 20 May 2023).
- Hébert, Serge et Légaré, Stéphane. Suivi de la qualité de l’eau des rivières et des petits cours d’eau. 2000. Available online: https:// belsp.uqtr.ca/id/eprint/1288/ (accessed on 2 April 2023).
- Ivanowsky A. Ouvrages d’assainissement des eaux et qualité du milieu récepteur en zone urbaine. Cas de rejets dans la Marque à Villeneuve d’Ascq. Thèse de Doctorat. Université de Lille 1, France, 2016; p 229. Available online: https:// hal.science/tel-01581755/ (accessed on 25 April 2021).
- Ndahama, Henri, Cishibanji, Pierre Batumike, Mashimago, Jean Jacques Bagalwa, et al. Inventaire de la Biodiversité Aquatique du Bassin du Lac Kivu: Cas Spécifique des Poissons de la Rivière Nyabarongo RD Congo [Inventory of the Biodiversity of Kivu Lake Bassin: Specific Case of Nyabarongo River Fishes]. Int J Innovat Appl Stud, 2014; 7 (4), 1298.
- World Health Organization, et al. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. WHO, 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/255874/97892415?sequence=1 (accessed on 25 February2023).
- Some Ysc, Soro Td, Ouedraogo S. Étude de la prévalence des maladies liées à l’eau et influences des facteurs environnementaux dans l’arrondissement de Nomgr-Masson: cas du quartier Tanghin (Ouagadougou-Burkina Faso). Int J. Biol. Chem. Sci., 2014; 8: 289–303. [CrossRef]
- Rouamba J, Nikiema E, Rouamba S, et al. Accès à l’eau potable et risques sanitaires en zone périphérique d’Ouagadougou, Burkina Faso. Rev Épidémiol Santé Publique, 2016; 64: S211. [CrossRef]
- Benkaddour Batoul. Contribution à l’étude de la contamination des eaux et des sédiments de l’Oued Chéliff (Algérie). Thèse de doctorat. Université de Perpignan; Université Abdelhamid Ibn Badis Mostaganem (Mostaganem, Algérie), 2018. Available online: Benkaddour Batoul. Contribution à l’étude Abdelhamid -Google Scholar (accessed on 25 April 2020).
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. In Review on Antimicrobial Resistance; Chaired by Jim O’Neill, December 2014; Wellcome Trust: London, UK, 2016.
- Singer, R. S., Finch, R., Wegener, H. C., Bywater, R., Walters, J., & Lipsitch, M. Antibiotic resistance—the interplay between antibiotic use in animals and human beings. The Lancet infectious diseases, 2003; 3 (1), 47-51. [CrossRef]
- Ouattara, N. K., Passerat, J., & Servais, P. Faecal contamination of water and sediment in the rivers of the Scheldt drainage network. Environ. Monit. Assess, 2011; 183, 243-257. [CrossRef]
- Guessennd, N. K., Ouattara, M. B., Ouattara, N. D., Nevry, R. K., Gbanon, V., Tiekoura, K. B., ... & Ger, B. M. R. Étude des bactéries multirésistantes des effluents hospitaliers d’un centre hospitalier et universitaire (CHU) de la ville d’Abidjan (Côte d’Ivoire). J. Appl. Biosci, 2013, 69, 5456-5464. [CrossRef]
- Hernando, M. D., Mezcua, M., Fernández-Alba, A. R., & Barceló, D. Environmental risk assessment of pharmaceutical residues in wastewater effluents, surface waters and sediments. Talanta, 2006, 69 (2), 334-342. [CrossRef]
- Zineb Cherak, Lotfi Loucif, Abdelhamid Moussi, Jean-Marc Rolain, Carbapenemase producing Gramnegative bacteria in aquatic environments: a review. J. Glob. Antimicrob. Resist, 2021, 25, 287–309. Montezzi LF, Campana EH, Correa LL, et al. Occurrence of carbapenemase- producing bacteria in coastal recreational waters. Int J Antimicrob Agents, 2015; 45:174–7.
- Weingarten RA, Johnson RC, Conlan S, et al. Genomic analysis of hospital plumbing reveals diverse reservoir of bacterial plasmids conferring carbapenem resistance. mBio, 2018;9:e02011 -17. [CrossRef]
- Picao RC, Cardoso JP, Campana EH, et al. The route of antimicrobial resistance from the hospital effluent to the environment: focus on the occurrence of KPC-producing Aeromonas spp. and Enterobacteriaceae in sewage. Diagn Microbiol Infect Dis 2013;76:80–5. [CrossRef]
- de Araujo CF, Silva DM, Carneiro MT, et al. Detection of carbapenemase genes in aquatic environments in Rio de Janeiro, Brazil. Antimicrob Agents Chemother 2016; 60:4380–3. [CrossRef]
- Yang F, Mao D, Zhou H, et al. Prevalence and fate of carbapenemase genes in a wastewater treatment plant in Northern China. PLoS One 2016; 11:e0156383. [CrossRef]
- Paschoal RP, Campana EH, Correa LL, et al. Concentration and variety of carbapenemase producers in recreational coastal waters showing distinct levels of pollution. Antimicrob Agents Chemother 2017; 61:e01963 -17. [CrossRef]
- Mathys DA, Mollenkopf DF, Feicht SM, et al. Carbapenemase-producing Enterobacteriaceae and Aeromonas spp. present in wastewater treatment plant effluent and nearby surface waters in the US. PLoS One 2019;14:e0218650. [CrossRef]
- Mathers AJ, Vegesana K, German Mesner I, et al. Intensive care unit wastewater interventions to prevent transmission of multispecies Klebsiella pneumonia carbapenemase-producing organisms. Clin Infect Dis 2018;67:171–8. [CrossRef]
- Sekizuka T, Inamine Y, Segawa T, et al. Potential KPC-2 carbapenemase reservoir of environmental Aeromonas hydrophila and Aeromonas caviae isolates from the effluent of an urban wastewater treatment plant in Japan. Environ Microbiol Rep 2019;11:589–97. [CrossRef]
- Xu H, Wang X, Yu X, et al. First detection and genomics analysis of KPC-2-producing Citrobacter isolates from river sediments. Environ Pollut 2018;235:931–7. [CrossRef]
Figure 1.
Flowchart of the process for selecting included studies.
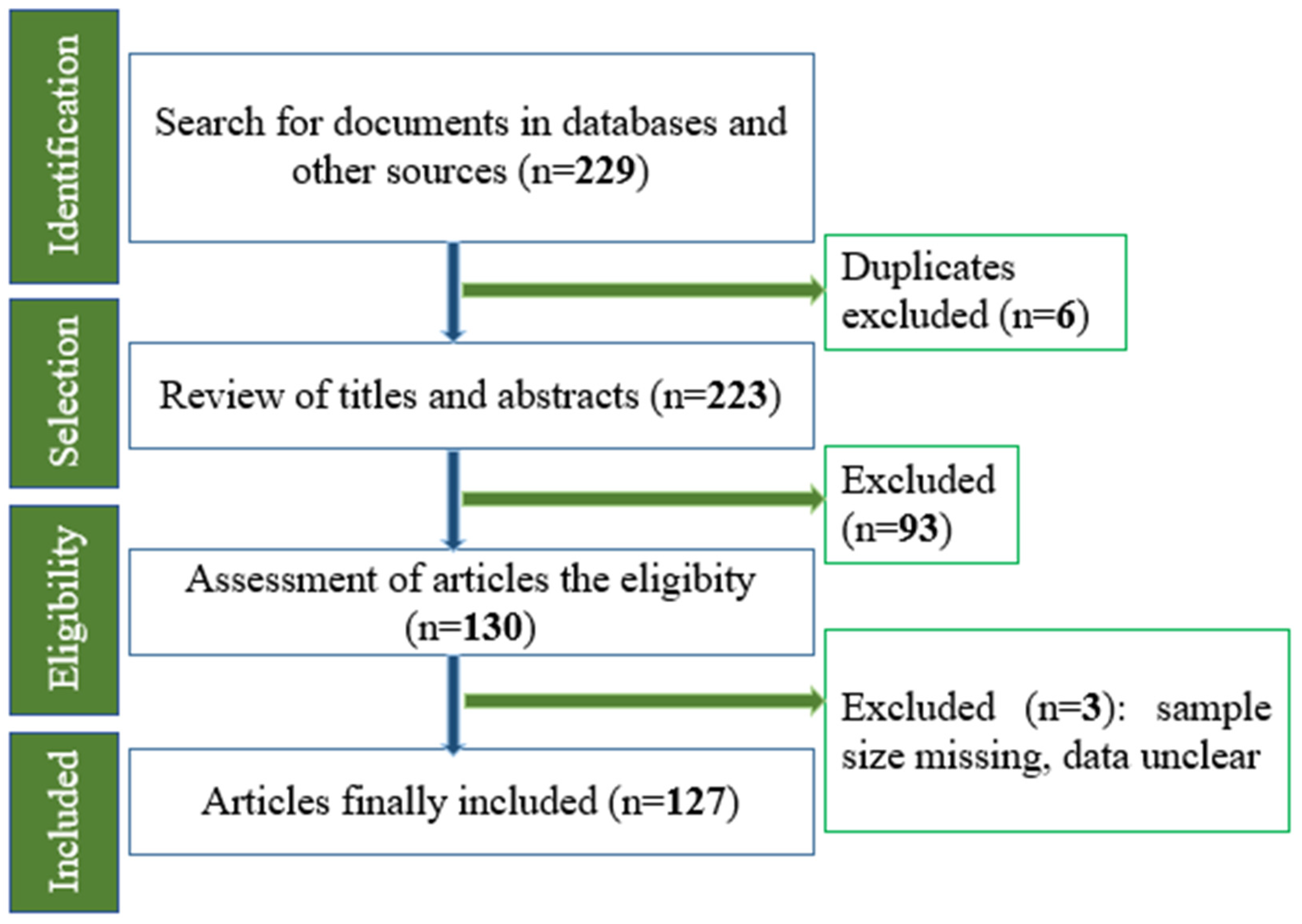
Figure 2.
Schematic diagram illustrating the process of spread of antibiotic-resistant bacteria. [26].
Figure 2.
Schematic diagram illustrating the process of spread of antibiotic-resistant bacteria. [26].
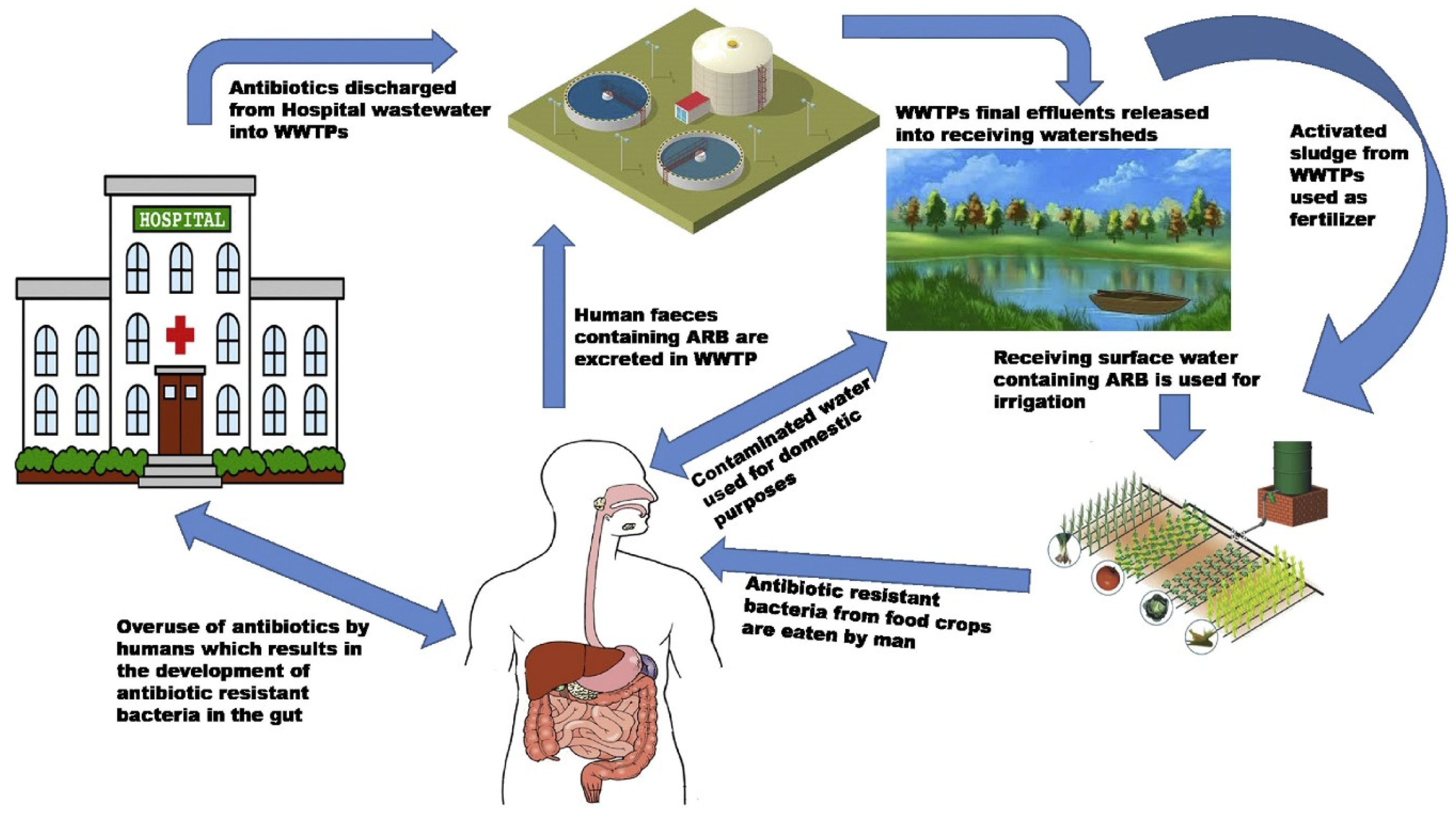
Figure 3.
Circulation of antibiotic-resistant microorganisms and antibiotics within the four major ecosystems: humans and animals undergoing antibiotic treatment, soil, and water.
Figure 3.
Circulation of antibiotic-resistant microorganisms and antibiotics within the four major ecosystems: humans and animals undergoing antibiotic treatment, soil, and water.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



