
Submitted:
10 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
This report elucidates the first surgical correction of an infundibular muscular ventricular septal defect (VSD) in a one-year-old Ragdoll cat via cardiac arrest using cardiopulmonary bypass, a method that is rarely used in feline cardiac surgery. VSDs can lead to congestive heart failure and pulmonary hypertension, particularly in patients with large shunts. This case involved a VSD that was atypically located and classified under the Soto classification instead of the standard Kirklin classification. Detailed echocardiography revealed that the defect required intervention owing to left heart and main pulmonary artery enlargement. Despite the VSD being located on the contralateral side, as anticipated in the preoperative examinations, the choice of median sternotomy allowed for successful closure of the defect. Conversely, the insertion of two cannulas into the ascending aorta resulted in damage to the adjacent thoracic duct, causing transient chylothorax, which resolved with conservative treatment. Cardiac arrest induced by a cardioplegic solution facilitated the surgical procedure, although it has led to anemia in cats. However, on postoperative day 490, the patient exhibited only minor residual shunting with normalized heart size, and remained healthy. This technique appears to be a viable treatment option for congenital heart disease in cats.
Keywords:
cat
; congenital heart disease
; feline cardiac surgery
; surgical correction
; ventricular septal defect
1. Introduction
Ventricular septal defect (VSD) is a congenital heart disease characterized by an unclosed ventricular septum leading to left-to-right shunting, which can result in congestive left heart failure and pulmonary hypertension in patients with large defects and significant shunt volumes. The prevalence of congenital heart disease in mixed-breed cats is 0.14%, indicating that such conditions are uncommon in cats [1]. However, clinical studies focusing exclusively on cats with congenital heart disease have shown that 50% of these cases are due to VSD, making it the most common congenital heart disease in cats [2]. In cats, VSD predominantly presents as either the membranous or perimembranous type, accounting for approximately 79% of cases. Other types include the supracristal type at approximately 13% and the atrioventricular canal and muscular types at approximately 4% each [3]. These classifications are commonly referred to as the Kirklin classification and are widely used in veterinary medicine [4]. While VSD alone rarely presents any clinical signs, among 27 cats with VSD, six exhibited respiratory symptoms, three of whom developed congestive left heart failure [3]. Typically, medical management such as diuretic therapy is implemented; however, palliative surgical treatments such as pulmonary artery banding to restrict blood flow have also been reported [5]. In humans, cases of VSD with pulmonary hypertension or other clinical symptoms are treated with catheter intervention or direct closure under cardiopulmonary bypass during cardiac arrest [6]. To the best of our knowledge, no surgical treatment for feline VSD have been reported. This report presents a case that did not fall under the Kirklin classification, was diagnosed as an infundibular muscular VSD according to the Soto classification [7], and underwent surgical correction under cardiopulmonary bypass.
2. Case Description
A 3-month-old female Ragdoll cat weighing 1.98 kg (body condition score [BCS]: 4/9) was presented for consultation. No apparent cardiogenic clinical signs were observed; however, a heart murmur was observed before acquisition. During vaccination, cardiac enlargement was noted at a referral hospital, leading to further examination at the Azabu University Veterinary Teaching Hospital. The heart murmur was most pronounced at the right cardiac apex, with an audible grade 5/6 systolic murmur. The body temperature was 38.2 °C, heart rate was 138 bpm, and respiratory rate was 48 breaths/min. Chest radiography indicated a vertebral heart size of 9.0 vertebrae (v), which is within the normal range for a kitten (median 9.5 v; range: 7.7–10.8 v) [8]; however, an enlarged pulmonary artery shadow was noted. Electrocardiography revealed increased R waves, but the electrical axis was +80 °with a normal sinus rhythm (180 bpm), and no arrhythmias were observed. Transthoracic echocardiography (TTE) was performed using an ultrasound unit (Vivid E9; GE Healthcare Co., Ltd., Tokyo, Japan) equipped with 6–12 MHz phased-array transducers. TTE identified a defect just below the aortic valve in the right parasternal left ventricular outflow tract view. Additionally, at the level of the aortic valve in the right parasternal short-axis view, the defect was located between the pulmonary artery outflow tract and tricuspid valve, leading to a diagnosis of a combination of Type 2 and Type 3 VSD according to the Kirklin classification. The VSD flow was 4.97 m/s. The left atrial diameter was 1.45 cm, enlarged compared with the normal value for a 2 kg kitten (0.96 cm; range: 0.82–1.13 cm) [8]. The left ventricular end-diastolic diameter was 1.94 cm, which was larger than the normal value of 1.25 cm (range: 1.04–1.49 cm) [8]. The pulmonary artery was significantly dilated, and the pulmonary-to-systemic blood flow ratio (Qp:Qs) [9] calculated using Doppler imaging was 2.45. The owner expressed interest in surgical treatment for the patient and visited our hospital, but decided to wait for the kitten to grow up because of its small size.
On day 383, the cat weighed 4.44 kg (BCS: 4/9). Echocardiography revealed that the VSD had a minor axis of 1.2 mm and major axis of 8.1 mm (Figure 1) with a VSD/Ao ratio of 95.3%. Color Doppler imaging in the right parasternal short-axis view at the level of the aortic valve revealed a shunt flow at the 12 o’clock position (Figure 1B). The LA/Ao ratio was 1.69 (1.43/0.85 cm; normal range < 1.5 [10]), which was considerably enlarged, and the left ventricular internal diameter in diastole (LVIDd) was 1.8 cm, at the upper limit of the normal range for an adult cat weighing 4.5 kg (1.8 cm, range: 1.27–1.98 cm [11]).
Significant enlargement of the pulmonary artery was evident (main pulmonary artery-to-aorta diameter ratio 1.29 (11.0/8.5 mm); normal value in dogs < 1.0 [12] (Figure 2). Although no tricuspid or pulmonary valve regurgitation and no evident signs of pulmonary hypertension (PH) were noted [12,13], the pulmonary to systemic blood flow ratio calculated by using Doppler was 2.96. Given the enlargement of the left side of the heart, surgical intervention was deemed necessary, and the cat underwent surgical correction under cardiopulmonary bypass. Pre-anesthesia included subcutaneous administration of atropine (0.025 mg/kg; Atropine Sulfate; NIPRO ES PHARMA Co., Ltd., Osaka, Japan), followed by intravenous administration of cefazolin (20 mg/kg, with additional doses every 2 h during surgery; Cefazolin Sodium for Injection, Nichi-Iko Pharmaceutical Co., Ltd., Toyama, Japan ), and slow intravenous injection of dexamethasone (0.2 mg/kg; dexamethasone injection A; Nippon Zenyaku Kogyo Co., Ltd., Fukushima, Japan). The cat was oxygenated with 100% oxygen for 5 min and received an intravenous injection of fentanyl (2 μg/kg; Fentanyl injection 0.5 mg; Janssen Pharmaceutical K.K., Tokyo, Japan). Subsequently, alfaxalone (5 mg/kg; Alfaxan multidose; Meiji Animal Health Co., Ltd., Kumamoto, Japan) was administered intravenously, and anesthesia was maintained with isoflurane (1–2%; Isoflurane; Mylan Pharma Co., Ltd., Osaka, Japan). During surgery, a continuous rate infusion (CRI) of fentanyl (5 μg/kg/h) was administered for pain management. Rocuronium bromide (0.3 mg/kg; Eslax intravenous; MSD K.K., Tokyo, Japan) was administered intravenously to halt respiration, with additional doses of 0.1 mg/kg administered every 40 min as needed. If the blood pressure dropped during surgery, isoflurane was discontinued, and anesthesia was maintained with a CRI of alfaxalone (5–8 mg/kg/h).
After anesthesia, the cat was positioned in dorsal recumbency. Arterial pressure was measured invasively after exposing the femoral artery and vein via cutdown. A median sternotomy was performed, followed by a median pericardiotomy, and the pericardium was retracted to either side to create a pericardial tent. At this stage, palpation of the thrill caused by the VSD revealed a defect in the right ventricular outflow tract, and the VSD was approached by incising the pulmonary artery.
The periaortic adipose tissue was removed to expose the aorta for the placement of a perfusion cannula distally and a myocardial protection solution root cannula proximally. Before inserting the perfusion cannula, double purse-string sutures were placed using non-absorbable monofilament 6-0 polyvinylidene fluoride sutures (Asflex; Konoseisakusyo Co., Ltd., Tokyo, Japan). Similarly, a single purse-string suture was used to secure the root cannula. For venous drainage, the cranial vena cava, azygos vein, and caudal vena cava were dissected, and taping was performed on the cranial and caudal vena cava using an expanded polytetrafluoroethylene suture (CV-0; ethylene oxide gas before surgery). A purse-string suture with 6-0 polyvinylidene fluoride was placed before the venous drainage cannula was inserted. A purse-string suture of the same material was used to vent the left atrial appendage. During cardiac incision, carbon dioxide was infused into the thoracic cavity to prevent air embolism.
Subsequently, heparin (heparin sodium injection; NIPRO ES PHARMA Co., Ltd., Osaka, Japan) was administered intravenously at a dose of 200 IU/kg, and an activated coagulation time (ACT) exceeding 300 s was confirmed. An 8 Fr arterial perfusion cannula (DLP™ One-Piece Pediatric Arterial Cannula, MEDTRONIC JAPAN CO., LTD., Tokyo, Japan) and a 16 G root cannula (DLP™ Pediatric Aortic Root Cannulae, MEDTRONIC JAPAN CO., LTD., Tokyo, Japan) were then inserted and secured with tourniquets. An 8 Fr curved venous return cannula was inserted into the cranial vena cava and a 10 Fr straight venous return cannula (Flexmate, Senko Medical Instrument MFG. Co. Ltd., Tokyo, Japan) was placed in the caudal vena cava, inserted distal to the taped ePTFE sutures, and secured with a tourniquet. A vent cannula was placed in the left atrium and secured using a tourniquet.
Partial bypass perfusion was initiated, followed by cross-clamping of the aorta. Myocardial protection solution (Miotector coronary vascular injection, Kyowa Criticare Co., Ltd., Kanagawa, Japan) was slowly administered via a root cannula at 34 ml/kg (150 ml) to achieve cardiac arrest and transition to total bypass perfusion. After 30 min, an additional dose of 15 ml/kg (65 ml) was administered, totaling 215 ml. Initially, the plan was to tape the azygos vein together with the cranial vena cava. However, owing to the distance, a suction cannula was inserted through the right atrial incision to perform suction venous drainage from the blood perfused from the azygos vein.
After cardiac arrest was induced, the main pulmonary artery was incised, and the pulmonary valve was incised to the right ventricle at the commissure to expose the ventricular septum. This revealed an elliptical defect surrounded by muscular tissue, measuring 9 mm in length and approximately 2–3 mm in width (Figure 3A). The full extent of the defect was visualized by inserting a right-angle clamp into the defect and pulling it towards the operator. The rim of the defect was sutured using six double-armed sutures with polypropylene pledgets (Oval-M; Matsudaika Inc., Tokyo, Japan). A patch (Nippon Becton Dickinson Company, Ltd., Tokyo, Japan) was used to close the defect, which was tailored to fit the size of the hole. Double-armed needles previously sewn into the rim were then threaded through the circular patch in sequence, and closure was completed once it was confirmed that no blood had leaked from the left ventricle (Figure 3). Subsequently, blood was evacuated from the left atrial vent cannula, and the pulmonary artery and right ventricle were continuously sutured using 6-0 polyvinylidene fluoride sutures. The right atrium was similarly sutured continuously, and upon release of the aortic cross-clamp, spontaneous beating of heart resumed. Partial cardiopulmonary bypass continued until the patient was rewarmed to 36.5 °C. The total aortic cross-clamp time was 56 min and cardiopulmonary bypass duration was 105 min. Subsequently, a chest drain was placed and the chest was closed in the standard manner. Postoperative pain was managed with fentanyl (2 microg/kg/h) administration continuously for 24 h.
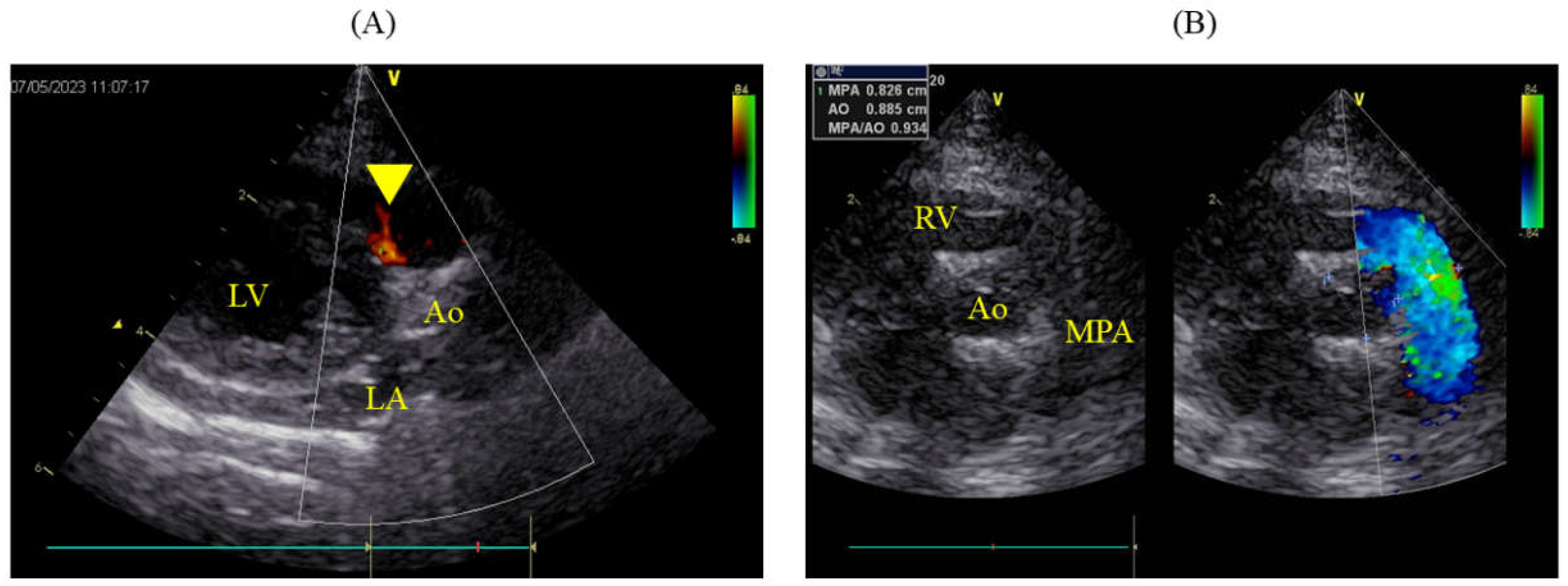
The packed cell volume (PCV) decreased to 15.7% postoperatively, necessitating a transfusion of 49 ml of blood, after which the PCV on the following day was 24.3%. Urine output immediately post-surgery was maintained at 2 ml/kg/hr but subsequently decreased, and by the second postoperative day, azotemia was observed (blood urea nitrogen, BUN: 78.5 mg/dL; creatinine, Cre: 3.6 mg/dL). Blood potassium level remained normal at 4.03 mmol/L. Continuous fluid therapy resulted in normalization by postoperative day 12 (BUN: 26.0 mg/dL; Cre: 1.2 mg/dL). However, by postoperative day 7, the pleural effusion had turned milky, requiring approximately 100 ml/day to be drained. The triglyceride (TG) and total cholesterol (T-Chol) levels in the pleural fluid were 60.0 mg/dL, with serum levels at TG 59.0 mg/dL and T-Chol 183.0 mg/dL. From postoperative day 8, oral administration of rutin 500 mg three times daily was initiated. A contrast-enhanced CT scan under anesthesia was performed on the postoperative day 12. The thoracic duct was highlighted using an iodinated contrast (iohexol 300 mg/ml; Fuji Pharma Co., Ltd., Tokyo, Japan) injected subcutaneously at 1.8 ml/kg around the anus, followed by 5 min of massage. This revealed significant collateral development in the anterior chest and leakage of the contrast agent into the pleural cavity. No thrombi or embolic material was found in the cranial vena cava. The milky effusion gradually decreased and resolved by postoperative day 15, allowing removal of the chest drain on the following day and discharge on postoperative day 17. Antithrombotic therapy was not implemented in this case. On the postoperative day 490, the patient remained asymptomatic and lively, with no recurrence of the chylothorax. Echocardiography showed slight residual shunting from the VSD (Figure 4A), but the pulmonary artery had returned to normal (MPA: Ao 0.93; 8.3/8.9 mm), and both LA/Ao and LVIDd were within normal ranges at 1.41 (1.25/0.89 cm) and 1.18 cm, respectively (Figure 4B).
4. Discussion
We encountered a cat with an infundibular muscular VSD classified according to the Soto classification, and surgically closed the defect using total bypass perfusion via a median sternotomy approach with a heart-lung machine. To the best of our knowledge, there are no prior reports of the surgical closure of VSD in cats, nor are there any reports specifically detailing infundibular muscular VSD. Additionally, while cardiac surgeries in cats using cardiopulmonary bypass, including left atrial-to-atrial septal defects, have been reported, these were conducted via an intercostal approach and involved partial bypass perfusion without cardiac arrest induced by cardioplegia [14,15].
Initially, the cat was diagnosed with the most common type of VSD in felines, perimembranous VSD, via echocardiographic examination. However, upon opening the chest and palpating the heart, the thrill observed in the pulmonary outflow tract led to a diagnosis of infundibular muscular VSD. In felines, VSDs are generally classified according to the Kirklin classification, where Type 1 VSDs are supracristal, Type 2 are either membranous or perimembranous, and Types 3 and 4 are atrioventricular canal and muscular VSDs, respectively, with 79% diagnosed as membranous or perimembranous [3].
However, in this case, the VSD was located in the outflow septum and surrounded entirely by muscular tissue, making it difficult to classify using the Kirklin classification. The Soto classification, commonly used in humans, categorizes VSDs into four types: (1) infundibular defects situated in the infundibular septum, often part of which abuts the semilunar valves; (2) membranous defects centered around the membranous septum and extending to areas near the atrioventricular or aortic valves; (3) defects between the membranous part and the inflow tract, similar to those seen in atrioventricular septal defects; and (4) muscular defects, where the surrounding tissue of the defect is entirely muscular [7]. Furthermore, muscular defects are sub-classified based on their location: infundibular, inflow tract, and trabecular septums.
According to the Kirklin classification, a Type 1 defect located above the crista supraventricularis corresponds to an infundibular defect according to the Soto classification, where the aortic valve may deviate. In the Kirklin classification, Type 1 defects are located above the crista supraventricularis and correspond to infundibular defects in the Soto classification. These defects are large and occur directly below the pulmonary valve, potentially causing deviations in the aortic valve. However, in the present case, although the defect was near the crista supraventricularis, it was not an infundibular defect because of its distance from the pulmonary artery. Consequently, it was ultimately classified as a muscular defect according to the Soto classification and diagnosed as an infundibular muscular VSD. This type of defect is advantageous for suturing because unlike perimembranous VSDs, it does not have a nearby conduction system.
In the case of membranous defects, color Doppler imaging using the clock-face method typically reveals a defect between the 10 and 11 o’clock positions. Conversely, a defect under the aortic valve (subaortic VSD) appears between the 11 and 1 o’clock positions, and in the Kirklin classification, a Type 1 defect is seen between the 1 and 2 o’clock positions [16]. In the present case, the absence of a defect directly beneath the pulmonary artery and the shunt flow originating from the 12 o’clock direction suggested that it was unlikely to be an infundibular or membranous defect. Thus, a preoperative diagnosis of infundibular muscular VSD may have been possible.
Additionally, there was a slight discrepancy between the measurements of VSD size by using color Doppler imaging and those obtained visually during surgery. This discrepancy could be attributed not only to the difference between the beating heart and the heart relaxed by cardioplegia but also to the elliptical shape of the defect. Studies on humans have reported that three-dimensional (3D) echocardiography can measure the size and location of defects more accurately than that measured using two-dimensional echocardiography [17].
Henceforth, particularly in cats undergoing closure procedures, it would be beneficial to use preoperative 3D echocardiography to better understand the size and location of defects. Additionally, the Soto classification appears to be more appropriate for categorizing VSDs, especially when traditional methods such as the Kirklin classification encounter limitations owing to anatomical variations specific to felines.
Shunt volume in VSD is determined by the size of the defect, pulmonary vascular resistance, and systemic vascular resistance, with severity typically assessed by the Qp:Qs. When Qp:Qs is less than 1.5, between 1.5 and 2.5, and greater than 2.5, the VSD is defined as small (restrictive), moderate (moderately restrictive), or large (nonrestrictive), respectively, correlating with the VSD: Ao ratio [3]. A higher Qp:Qs ratio is associated with pulmonary hypertension (PH) and heart failure; in this case, both high Qp:Qs and high VSD: Ao ratio were noted, along with significant dilation of the main pulmonary artery. When Qp:Qs is < 1.5, it is advisable to monitor the patient’s condition without any intervention. However, if Qp:Qs exceeds 2.5 and there are clinical signs such as cardiac enlargement or indicators suggestive of PH, aggressive therapeutic intervention is warranted [3].
Surgical correction using a cardiopulmonary bypass is less common in cats than in dogs. In dogs, it is common to establish a cardiopulmonary bypass by inserting a perfusion cannula into the common carotid artery; however, in cats, this artery is too narrow to accommodate the necessary equipment. Additionally, cats have a smaller blood volume, which complicates securing sufficient blood for transfusion, and leads to anemia due to blood dilution during cardiopulmonary bypass.
In cats, surgical corrections for conditions such as Cor Triatriatum Sinister (CTS) and atrial septal defect (ASD) have been reported, utilizing intercostal approaches without the use of cardioplegia, thereby avoiding blood dilution [14,15]. In ASD repair, a 5 Fr feeding tube is used as a substitute for a perfusion cannula and inserted into the common carotid artery [15]. For the CTS, an 8 Fr perfusion cannula was inserted into the descending aorta [14]. In our case, because a median sternotomy approach was used, we were able to insert an appropriately sized perfusion cannula into the ascending aorta without difficulty, maintaining cerebral circulation due to the direction of blood flow. For venous drainage, the ASD cases involved the insertion of 8 Fr straight-type cannulas into both the cranial and caudal vena cava [15], whereas in CTS, a 16 Fr cannula was inserted into the right atrium [14]. In this case, we chose a curved venous return cannula for the cranial vena cava to facilitate insertion at the tip of the cannula.
Unlike the previous two cases, the use of cardioplegia in this case provided a stable field for surgery, making the procedure easier. However, 215 ml of cardioplegia was administered, which resulted in postoperative anemia. Transient renal impairment observed in this case may have been associated with anemia [18]. Given that hypothermia during cardiopulmonary bypass can reduce heart rate, surgery under pulsatile conditions might have been possible [15,19]. Furthermore, although not explored in cats, techniques such as electrically induced ventricular fibrillation have been reported in dogs [20]. In cats, where the donor blood supply is often insufficient, future considerations may need to include using less or avoiding cardioplegia altogether.
In veterinary medicine, open-heart surgery typically involves intercostal thoracotomy approach. The right intercostal approach is appropriate for treating common membranous VSDs in cats. This allows the insertion of venous drainage cannulae into both the cranial and caudal vena cava, enabling VSD closure through an incision in the right atrium or ventricle. However, in this case, an infundibular muscular VSD was diagnosed after thoracotomy at the left ventricular outflow tract. Such a diagnosis would likely have resulted in an unsuccessful outcome with the right intercostal approach, justifying the use of a median sternotomy approach to prepare for unforeseen circumstances.
Additionally, the patient exhibited transient chylothorax postoperatively, which resolved with conservative treatment. Chylothorax is a rare complication in humans following thoracotomy, primarily caused by thoracic duct damage, with no significant difference in incidence between the intercostal and median sternotomy approaches [21]. In cats, the thoracic duct runs along the left side of the aorta and drains into the venous system [22]. The possibility of thoracic duct damage cannot be excluded in this case because the ascending aorta was dissected to insert perfusion and root cannulas using the median sternotomy approach. Thus, careful handling of major vessels is necessary when performing a median sternotomy.
Postoperative chylothorax can also be associated with elevated central venous pressure during surgery [23]. In this case, the central venous pressure might have increased due to taping of the cranial vena cava, potentially contributing to thoracic duct damage. However, similar to other cases in cats in which chylothorax does not necessitate surgery unless the thoracic duct is severed, this condition improved with the administration of rutin and regular drainage from a chest drain [24]. Therefore, conservative treatment and observation over 1–2 weeks are suitable for managing postoperative chylothorax following open-heart surgery.
5. Conclusions
This is the first reported instance of encountering an infundibular muscular VSD in a cat and closing it surgically using the cardiopulmonary bypass approach. Although the use of cardioplegia to achieve cardiac arrest during cardiopulmonary bypass in cats facilitates surgical manipulation, it may lead to postoperative anemia due to blood dilution. Transient chylothorax can also occur. Albeit improvements made to this approach, median sternotomy for open heart surgery in cats appears to be a viable option for treating congenital heart disease.
Author Contributions
Conceptualization, T.A.; methodology, T.A., H.S., N.F. and T.M.; validation, T.M.; formal analysis, T.A.; investigation, T.A., T.T., Y.J. and K.I.; data curation, T.A., T.T., K.I. and Y.J.; writing—original draft preparation, T.A.; writing—review and editing, T.M.; visualization, T.A.; supervision, H.S., N.F. and T.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the retrospective nature of the study, with minor modifications to the procedure routinely performed at our hospital.
Informed Consent Statement
Informed consent was obtained from the owner of the patient.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Schrope, D.P. Prevalence of congenital heart disease in 76,301 mixed-breed dogs and 57,025 mixed-breed cats. J Vet Cardiol 2015, 17, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Tidholm, A.; Ljungvall, I.; Michal, J.; Häggström, J.; Höglund, K. Congenital heart defects in cats: A retrospective study of 162 cats (1996–2013). J Vet Cardiol 2015, 17, S215–S219. [Google Scholar] [CrossRef] [PubMed]
- Bomassi, E.; Misbach, C.; Tissier, R.; Gouni, V.; Trehiou-Sechi, E.; Petit, A.M.; Desmyter, A.; Damoiseaux, C.; Pouchelon, J.L.; Chetboul, V. Signalment, clinical features, echocardiographic findings, and outcome of dogs and cats with ventricular septal defects: 109 cases (1992–2013). J Am Vet Med Assoc 2015, 247, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Santamaria, H.; Soto, B.; Ceballos, R.; Bargeron, L.M.; Coghlan, H.C.; Kirklin, J.W. Angiographic differentiation of types of ventricular septal defects. AJR Am J Roentgenol 1983, 141, 273–281. [Google Scholar] [CrossRef]
- Sutherland, B.J.; Pierce, K.V.; Gagnon, A.L.; Scansen, B.A.; Orton, E.C. Dilatable pulmonary artery banding for ventricular septal defect: surgical technique and case report of three cats. J Vet Cardiol 2019, 25, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Lozier, J.S.; Sati, M.; Cheifetz, I.M.; Bocks, M.L. Update on percutaneous and perventricular device closure of congenital ventricular septal defect. Expert Rev Cardiovasc Ther 2023, 21, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Soto, B.; Becker, A.E.; Moulaert, A.J.; Lie, J.T.; Anderson, R.H. Classification of ventricular septal defects. Br Heart J 1980, 43, 332–343. [Google Scholar] [CrossRef] [PubMed]
- Gunther-Harrington, C.T.; Sharpe, A.N.; Vernau, K.M.; Ueda, Y.; Montgomery, E.A.; Surmick, J.D.; Fernandez, N.; Ontiveros, E.; Walker, A.L.; Stern, J.A. Reference intervals for radiographic, echocardiographic and N-terminal pro B-type natriuretic peptide values in healthy kittens. J Feline Med Surg 2021, 23, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Serres, F.; Chetboul, V.; Tissier, R.; Gouni, V.; Desmyter, A.; Sampedrano, C.C.; Pouchelon, J.L. Quantification of pulmonary to systemic flow ratio by a Doppler echocardiographic method in the normal dog: repeatability, reproducibility, and reference ranges. J Vet Cardiol 2009, 11, 23–29. [Google Scholar] [CrossRef]
- Abbott, J.A.; MacLean, H.N. Two-dimensional echocardiographic assessment of the feline left atrium. J Vet Intern Med 2006, 20, 111–119. [Google Scholar] [CrossRef]
- Häggström, J.; Andersson, Å.O.; Falk, T.; Nilsfors, L.; OIsson, U.; Kresken, J.G.; Höglund, K.; Rishniw, M.; Tidholm, A.; Ljungvall, I. Effect of body weight on echocardiographic measurements in 19,866 pure-bred cats with or without heart disease. J Vet Intern Med 2016, 30, 1601–1611. [Google Scholar] [CrossRef] [PubMed]
- Reinero, C.; Visser, L.C.; Kellihan, H.B.; Masseau, I.; Rozanski, E.; Clercx, C.; Williams, K.; Abbott, J.; Borgarelli, M.; Scansen, B.A. ACVIM consensus statement guidelines for the diagnosis, classification, treatment, and monitoring of pulmonary hypertension in dogs. J Vet Intern Med 2020, 34, 549–573. [Google Scholar] [CrossRef]
- Rolph, K.E.; Cavanaugh, S.M. Feline pulmonary hypertension: are we overlooking an important comorbidity? J Feline Med Surg 2022, 24, e636–e646. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, N.; Gouni, V.; Behr, L.; Trehiou-Sechi, E.; Petit, A.; Misbach, C.; Raillard, M.; Retortillo, J.L.; Pouchelon, J.L.; Pierrel, A.; et al. Surgical treatment of cor triatriatum sinister in a cat under cardiopulmonary bypass. Vet Surg 2015, 44, 964–969. [Google Scholar] [CrossRef] [PubMed]
- Uechi, M.; Harada, K.; Mizukoshi, T.; Mizuno, T.; Mizuno, M.; Ebisawa, T.; Ohta, Y. Surgical closure of an atrial septal defect using cardiopulmonary bypass in a cat. Vet Surg 2011, 40, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.R.; Nemeth, M.; Flamm, S.D.; Sung, C.; Stainback, R.F. Supracristal ventricular septal defect. Tex Heart Inst J 2006, 33, 96–97. [Google Scholar] [PubMed]
- Kardon, R.E.; Cao, Q.L.; Masani, N.; Sugeng, L.; Supran, S.; Warner, K.G.; Pandian, N.G.; Marx, G.R. New insights and observations in three-dimensional echocardiographic visualization of ventricular septal defects: experimental and clinical studies. Circulation 1998, 98, 1307–1314. [Google Scholar] [CrossRef]
- Nangaku, M.; Eckardt, K.U. Pathogenesis of renal anemia. Semin Nephrol 2006, 26, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, R.W. Some effects of hypothermia on the cardiovascular system and Ecg of cats. Proc Soc Exp Biol Med 1964, 115, 1–4. [Google Scholar] [CrossRef]
- Kugelberg, J. Electrical induction of ventricular fibrillation in the human heart. A study of excitability levels with alternating current of different frequencies. Scand J Thorac Cardiovasc Surg 1976, 10, 237–240. [Google Scholar] [CrossRef]
- Wu, J.M.; Yao, C.T.; Kan, C.D.; Yeh, C.N.; Yang, Y.R.; Wang, J.N. Postoperative chylothorax: differences between patients who received median sternotomy or lateral thoracotomy for congenital heart disease. J Card Surg 2006, 21, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Lee, H.; Lee, N.; Choi, M.; Kim, J.; Chang, D.; Choi, M.; Yoon, J. Ultrasound-guided mesenteric lymph node iohexol injection for thoracic duct computed tomographic lymphography in cats. Vet Radiol Ultrasound 2011, 52, 302–305. [Google Scholar] [CrossRef] [PubMed]
- McBride, M.E.; Drass, J.C.; Berkenbosch, J.W.; Wilson, W.R.; Tobias, J.D. Hypogammaglobulinemia complicating chylothorax after cardiac surgery in two infants. J Cardiothorac Vasc Anesth 2001, 15, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.S.; Cohn, L.A.; Jordan, R.C. Use of rutin for medical management of idiopathic chylothorax in four cats. J Am Vet Med Assoc 1999, 215, 345–348. [Google Scholar] [CrossRef]
Figure 1.
Echocardiographic findings. (A) Right parasternal long-axis view of the LV outflow tract showing a VSD directly below the aortic valve (yellow arrow-head). (B) Right parasternal short-axis view at the level of the aortic valve using color flow Doppler, where the largest diameter of the VSD is observed during diastole. The left-to-right shunt from the VSD is at 12 o’clock direction, located between the TV and pulmonary valve (yellow arrow). LA: left atrium; LV: left ventricle; Ao: aorta; RA: right atrium; TV: tricuspid valve; RV: right ventricle; VSD, ventricular septal defect.
Figure 1.
Echocardiographic findings. (A) Right parasternal long-axis view of the LV outflow tract showing a VSD directly below the aortic valve (yellow arrow-head). (B) Right parasternal short-axis view at the level of the aortic valve using color flow Doppler, where the largest diameter of the VSD is observed during diastole. The left-to-right shunt from the VSD is at 12 o’clock direction, located between the TV and pulmonary valve (yellow arrow). LA: left atrium; LV: left ventricle; Ao: aorta; RA: right atrium; TV: tricuspid valve; RV: right ventricle; VSD, ventricular septal defect.
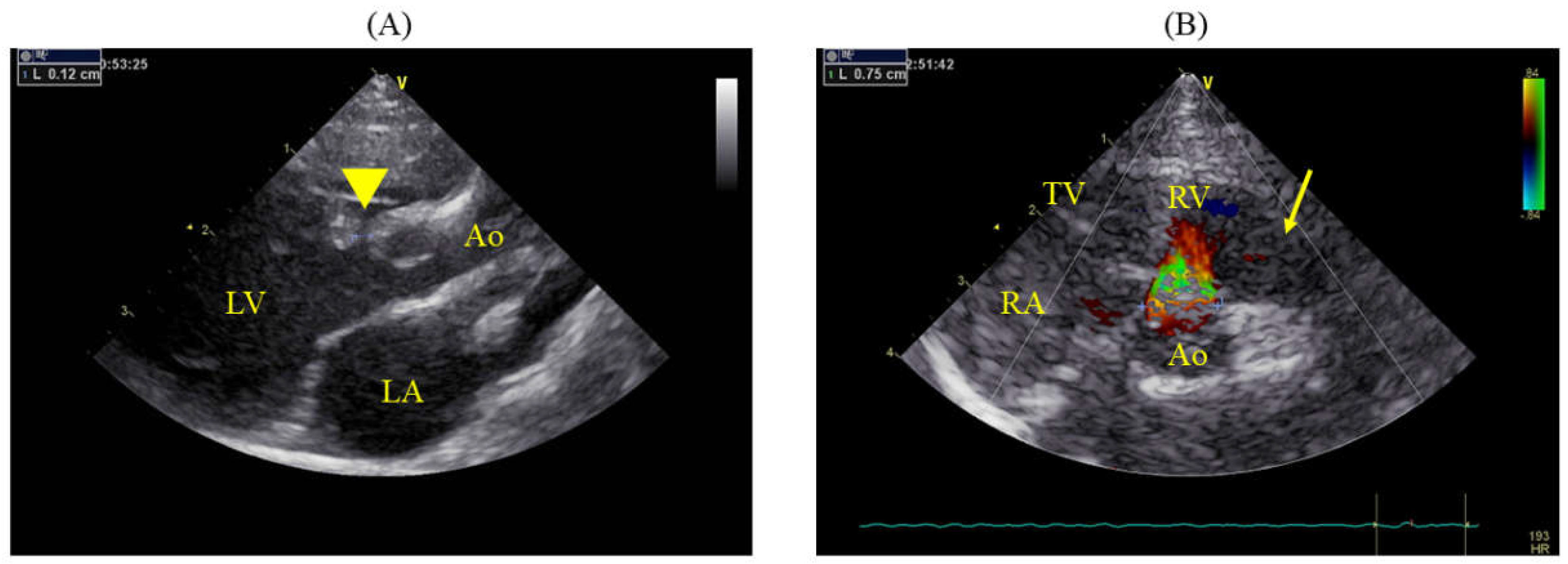
Figure 2.
Right parasternal short-axis view at the level of the aortic valve showing significant dilation of the MPA. The diameter of the aorta is 8.5 mm, and that of MPA is 11.0 mm, indicating an MPA:Ao ratio of 1.29. Ao: aorta; MPA: main pulmonary artery; RV: right ventricle.
Figure 2.
Right parasternal short-axis view at the level of the aortic valve showing significant dilation of the MPA. The diameter of the aorta is 8.5 mm, and that of MPA is 11.0 mm, indicating an MPA:Ao ratio of 1.29. Ao: aorta; MPA: main pulmonary artery; RV: right ventricle.
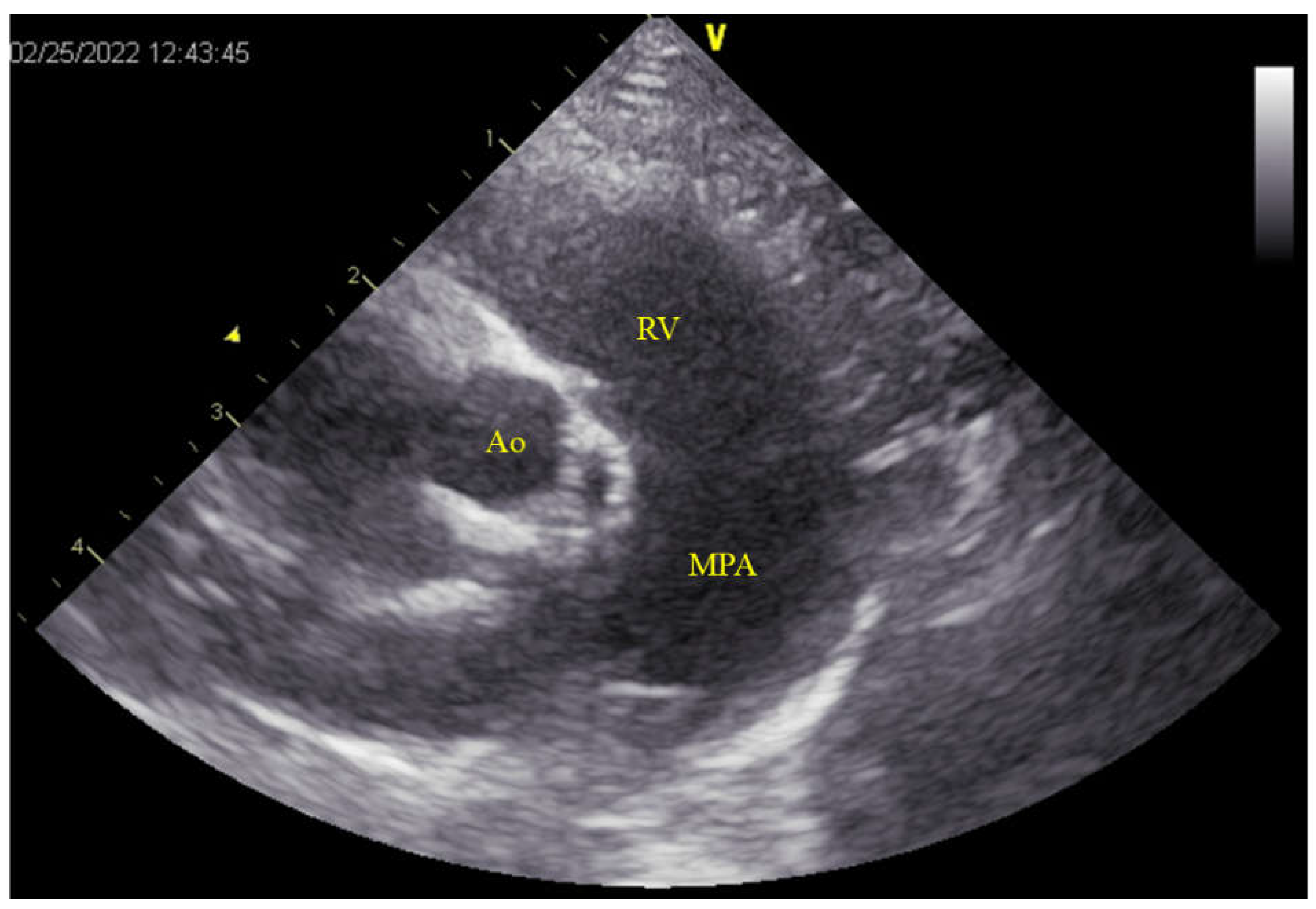
Figure 3.
Intraoperative findings of the VSD. (A) The MPA is incised, and an incision from the commissure of the PV to the RV reveals a VSD measuring 9 mm in length and 2–3 mm in width (yellow arrow-head). The defect is observed on the RV side of the PV. (B) The VSD is closed by using a patch (yellow arrow). MPA: main pulmonary artery; PV: pulmonary valve; RV: right ventricle; VSD: ventricular septal defect.
Figure 3.
Intraoperative findings of the VSD. (A) The MPA is incised, and an incision from the commissure of the PV to the RV reveals a VSD measuring 9 mm in length and 2–3 mm in width (yellow arrow-head). The defect is observed on the RV side of the PV. (B) The VSD is closed by using a patch (yellow arrow). MPA: main pulmonary artery; PV: pulmonary valve; RV: right ventricle; VSD: ventricular septal defect.
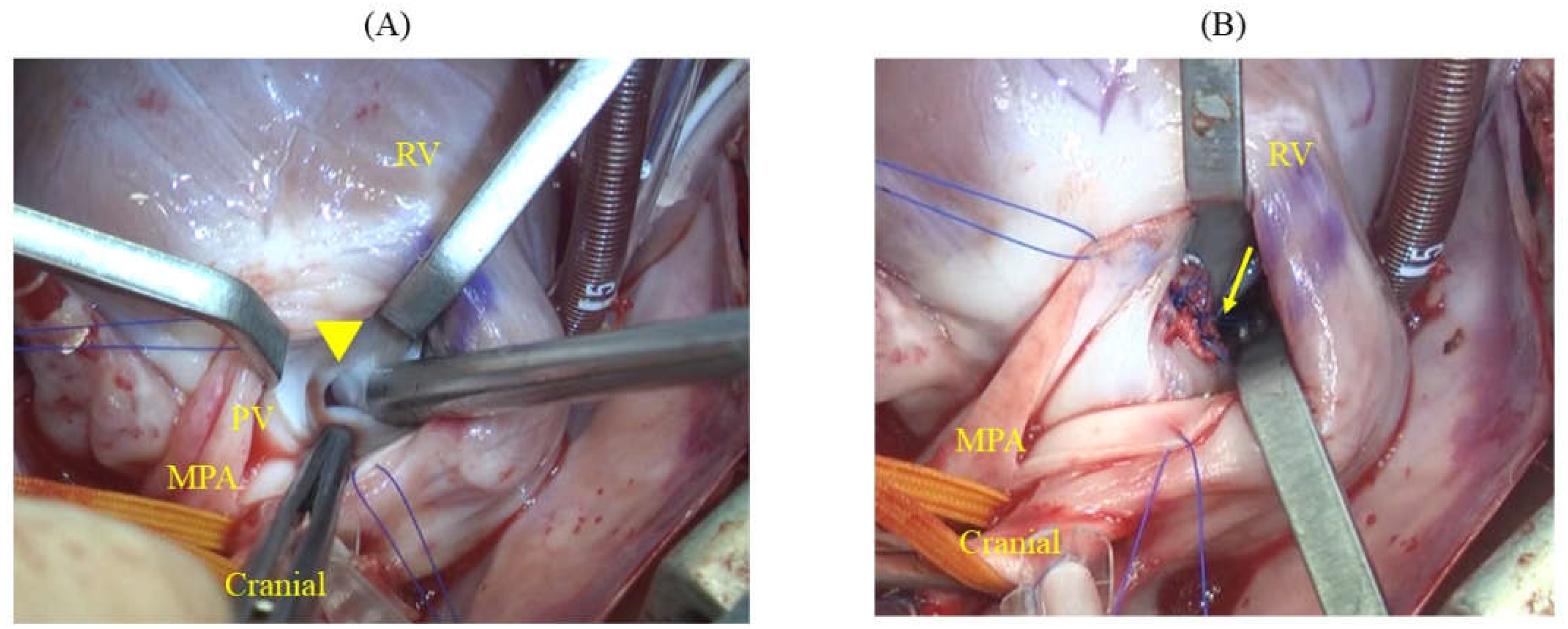
Figure 4.
Echocardiographic findings 490 days post-operation. (A) Right parasternal long-axis view of the LV outflow tract, where color flow Doppler is slightly adjusted to confirm residual shunting, showing minor residual shunting (yellow arrow-head). (B) Simultaneous right parasternal short-axis view at the level of the aortic valve indicating the diameters of the aorta at 8.9 mm and MPA at 8.3 mm, with an MPA:Ao ratio of 0.93. LA: left atrium; LV: left ventricle; Ao: aorta; MPA: main pulmonary artery; RV: right ventricle.
Figure 4.
Echocardiographic findings 490 days post-operation. (A) Right parasternal long-axis view of the LV outflow tract, where color flow Doppler is slightly adjusted to confirm residual shunting, showing minor residual shunting (yellow arrow-head). (B) Simultaneous right parasternal short-axis view at the level of the aortic valve indicating the diameters of the aorta at 8.9 mm and MPA at 8.3 mm, with an MPA:Ao ratio of 0.93. LA: left atrium; LV: left ventricle; Ao: aorta; MPA: main pulmonary artery; RV: right ventricle.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



