
Submitted:
09 May 2024
Posted:
10 May 2024
You are already at the latest version
Abstract
This cross-sectional, analytical, and observational study aimed to investigate the relationship between Visceral Adiposity Index (VAI) and anthropometric, biochemical, and insulin resistance (IR) parameters in Brazilians at risk of CVD. Biochemical parameters and anthropometric measurements were evaluated. The Pearson test was used to assess the correlation between VAI and anthropometric, biochemical, and IR parameters, with a predefined significance level of 5%. The analyzed sample consisted of 88 men and 72 women, with an average age of 58.78±13.48. VAI revealed noteworthy and positive correlations with all anthropometric parameters assessed (p<0.0001). Furthermore, significant positive associations were noted between VAI and total cholesterol in women (p=0.0064), glycemia in men (p=0.0105), and LDL-c (p<0.01) and triglycerides in both genders (p˂0.0001). A significant negative association was observed between VAI and HDL-c in both genders (p<0.0001). Notably, the correlation between VAI and total cholesterol in men, glycemia in women, and CRP in both genders was not found to be significant. However, a significant relationship between VAI and IR parameters was observed in both sexes (p<0.05). The results obtained from our study suggest that VAI functions as a simple and non-intrusive instrument, demonstrating significant effectiveness in identifying metabolic changes primarily associated with adipose tissue dysfunction, particularly dyslipidemia.
Keywords:
Insulin Resistance
; Visceral Adiposity Index
; Cardiovascular Diseases
; Cardiovascular Risk
; Waist Circumference
; Brazilian Population
1. Introduction
Historically, adipose tissue (AT) was viewed as a passive storage site for lipids. Nowadays it has been recognized as a crucial metabolic organ playing a significant role in regulating various aspects of human homeostasis, including glycemic control, driven by specific hormones known as adipokines. While adipocytes are typically well-controlled in executing their functions accurately, dysregulation of adipose tissue can adversely im-pact human health. This dysregulation not only contributes to obesity but also increases the risk of developing type 2 diabetes mellitus, metabolic syndrome (MetS), and other related complications [1,2].
Cardiovascular diseases (CVD) exert a significant toll on public health systems due to their elevated mortality rates that cause a substantial impact globally. Annually, an estimated 17.9 million people worldwide develop CVD. Consequently, there has been an intensified exploration of risk factors in this context, with obesity emerging as an independent predictor. The prevalence of obesity has reached 650 million in recent years, and it is often coexisting with other conditions such as hypertension, dyslipidemia, and insulin resistance (IR). Additionally, overweight affects 1.9 billion adults globally [3,4].
Considering that obesity significantly contributes to CVD, it is crucial to establish preventive measures and early diagnostic tools for assessing adiposity rates in individuals at risk. Visceral adiposity, characterized by the ectopic accumulation of fat and dysfunctional AT, serves as a key marker. Presently, the visceral adiposity index (VAI) proves valuable as an identification tool for predicting AT dysfunction due to its simplicity and non-invasive nature. As a gender-specific marker that combines anthropometric data and lipid profile, VAI can be widely employed to evaluate the cardiovascular risk associated with dysfunctional adipose tissue accumulation [5,6].
Past research has established a positive association between elevated VAI levels and coronary artery calcium scores, making VAI an independent predictor of risk for coronary atherosclerosis. Furthermore, VAI has been independently correlated with subclinical atherosclerosis in individuals predisposed to diabetes. Additionally, there is a noteworthy connection between elevated VAI scores and the incidence of diabetes and IR. Hypertension can also be predicted as a cardiovascular risk factor in individuals with high VAI indexes [5,7, 8,9]. For this reason, it becomes imperative to thoroughly assess the VAI by considering bio-chemical, anthropometric, and IR parameters.
This comprehensive evaluation is essential for gaining a nuanced understanding of how VAI could potentially be used as a valuable tool to predict CVD.
2. Materials and Methods
2.1. Study Design
This research constituted an analytical observational study employing a cross-sectional design, with the participation of 160 individuals from the University Hospital of the University of Marília, situated in Marília, São Paulo, Brazil. The inclusion criteria comprised individuals seeking routine cardiovascular care consultations at the Cardiology Unit of the University Hospital or those exhibiting active cardiovascular symptoms.
2.2. Study Population
The participants in this study consists of a diverse group of volunteers, adults and elderly individuals of both genders, with age ranging from 20 to 84 years. To ensure the comprehensive collection of relevant data, meticulous attention was given to selecting medical records that contained information on all the essential variables for the study. It is noteworthy that the records of pregnant and lactating women were intentionally excluded to maintain the focus and integrity of the research.
2.3. Anthropometric and Biochemical Analysis
The anthropometric variables collected and analyzed were weight, height, waist circumference (WC), neck circumference (NC), and body mass index (BMI). Anthropometric measurements were taken and recorded by trained professionals using the measurement techniques as preconized by Lohman et al [10] and Gibson [11].
Body mass index values were calculated as the weight in kilograms divided by the square of the height in meters and referenced according to the World Health Organization (WHO) classification as follows: underweight (˂18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2 and obese (≥30 kg/m2) [12]. Waist circumference values were also assessed through WHO classification as follows: low risk (for men ≤93.9 cm and women ≤79.9 cm), an increased risk (for men 94 to 101.9 cm and women 80 to 87.9 cm), and high risk (for men ≥102 cm and women ≥88 cm) [13]. The interpretations of Neck Circumference (NC) values were based on the study by Stabe et al. [14], specifically conducted on the Brazilian population at major risk of developing cardiovascular and metabolic diseases. Notably, the thresholds indicating increased risk were identified as NC > 39.6 cm for men and NC > 36.1 cm for women.
The variables collected for the biochemical analysis were fasting blood glucose levels (FBG), serum high-density lipoprotein cholesterol (HDL-c), serum triglycerides, total cholesterol (TC), serum insulin levels (INS), serum low-density lipoprotein cholesterol levels (LDL-c), and ultra-sensitive C-reactive protein (hs-CRP). Additionally, for a subset of patients, only LDL-c levels were determined using Friedewald’s formula [15]. The Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) was calculated for all included patients using fasting glucose and insulin blood levels [16,17]. All biochemical parameters followed the São Francisco Laboratory protocols at the University of Marília.
2.4. Calculation of VAI
Sex-specific equations were used for calculation of Visceral Adiposity Index for all participants in the study. Essential parameters for this calculation included waist circumference, body mass index, serum triglycerides levels, and serum high-density lipoprotein cholesterol. The VAI formulas incorporated two anthropometric parameters (BMI in kg/m2 and WC in cm) along with two biochemical parameters (TG and HDL-c in mmol/L) [5].
VAIMEN = [WC/{39.68+(1.88*BMI)}]*(TG/ 1.03)*(1.31/HDL-c)
VAIWOMEN = [WC/{36.58+(1.89*BMI)}]*(TG/ 0.81)*(1.52/HDL-c)
2.5. Ethics Approval and Consent to Participate
The University of Marília's Ethics Committee granted approval for all experimental protocols in this study (conducted in Marília, São Paulo, Brazil) under the ethical approval number 2.746.117. The commencement of the study occurred only after obtaining signed free and informed consent forms from all participants, adhering to Resolutions 466/2012 and 510/2016 of the National Health Council. Written informed consent has also been diligently acquired from the patients for the publication of this paper, ensuring that due consideration is given to the ethical principles surrounding confidentiality and privacy. This practice underscores our commitment to respecting the rights and wishes of the individuals involved, emphasizing transparency and responsible communication in the dissemination of research findings. All procedures in the study adhered to the ethical standards outlined in the Institutional Ethics Committee and the Helsinki Declaration of 1975 (revised in 2008).
2.6. Statistical Analysis
The quantitative and continuous variables are presented as mean and standard deviation (SD). To assess the correlation between VAI and various anthropometric, biochemical, and insulin resistance parameters, the Pearson test was employed. Significance was established at 5% (p-value ≤ 0.05). All analyses were conducted using the BioEstat 5.3 program.
3. Results
The baseline characteristics of the participants by gender are presented in Table 1. The study comprised a sample of 160 participants in which 55% (n=88) were men, with an average age of 58.78±13.48 years. The mean values for anthropometric and biochemical parameters were as follows: height (1.65±0.09 m), weight (81.96±19.07 kg), BMI (29.70±6.00 kg/m²), WC (101.18±15.53 cm), NC (38.75±4.45 cm), FBG (105.80±28.54), TC (189.14±44.85 mg/dL), HDL-c (46.24±12.32 mg/dL), LDL-c (172.28±51.88 mg/dL), TG (146.94±73.38 mg/dL), hs-CRP (6.07±24.30 mg/L), and INS (13.91±15.66 µUI/mL).
Figure 1 showcases scatter diagrams illustrating the associations between anthropometric variables and VAI values for both men and women. The diagrams on the left present correlations based on men's parameters, while the right ones represent women's parameters. In both sexes, positive correlations statistically significant were observed be-tween VAI and the anthropometric variables BMI (p < 0.0001), WC (p < 0.0001), and NC (p < 0.0001).
Figure 2 presents scatter diagrams illustrating the correlations between biochemical and VAI values. Similarly, to the data presented in Figure 1, the left diagrams correspond to men's parameters and the right ones correspond to women's parameters. Significant and positive correlations were noted between VAI and TC in women (p=0.0064), FBG in men (p=0.0105), LDL-c in both sexes (p=0.0114 for men and p < 0.0001), and TG in both sexes (p < 0.0001) while a negative and significant correlation was observed between VAI and HDL-c in both men (p < 0.0001) and women (p < 0.0001). These correlations elucidate the raveled relationship between VAI and key biochemical parameters, providing valuable insights regarding the impact of visceral adiposity on lipid profiles and glucose metabolism. The gender-specific analysis offers a fine understanding of how these correlations manifest in both men and women, contributing to a comprehensive interpretation of the study's biochemical findings.
Figure 3 illustrates the association between HOMA-IR, fasting insulin levels, and VAI, in addition to the correlation between VAI and fasting insulin levels. The scatter dia-grams reveal positive and significant correlations between VAI and elevated HOMA-IR levels in both sexes (p=0.0356 in men and p=0.0111 in women). This indicates a close as-sociation, highlighting that VAI is intimately linked to the escalation of IR. These findings underscore the meaningful connection between visceral adiposity, as represented by VAI, and the manifestation of insulin resistance. The gender-specific analysis further enhances our understanding of how these correlations unfold in both men and women.
4. Discussion
While BMI is a widely used to assess and classify obesity globally, its efficacy in accurately predicting body fat percentage is limited by its curvilinear association with body fat in both men and women. Recognizing this limitation, VAI emerges as a gender-specific equation designed to overcome these challenges by providing a more nuanced assessment of fat content. Importantly, VAI evaluates the functionality of AT to offer a more comprehensive understanding of its impact on health. The development of the VAI equation took into consideration populations of both normal and overweight individuals. This inclusive approach enhances the generalizability of the index, making it applicable to a broader spectrum of individuals. This emphasis on diverse populations contributes to the robustness of VAI as a tool for assessing adiposity and underscores its relevance in capturing variations in body composition beyond what BMI can offer [18,19].
Our study reveals that VAI exhibits positive and significant correlations with both biochemical and anthropometric parameters, pointing towards the identification of individuals at increased risk of CVD. These correlations became evident when examining the concurrent influence of VAI with TC in men, FBG in women, LDL-c in both sexes, and TG in both sexes. Significantly, these outcomes are in harmony with observations from other studies, underscoring the strength and reliability of these correlations across varied populations, with a specific focus on the Brazilian population in this instance. The observed correlations underscore the utility of VAI as a comprehensive metric that captures various facets of cardiovascular functionality. This study contributes to the growing body of evidence supporting the relevance of VAI in identifying individuals at risk for cardiovascular complications, emphasizing its potential as a valuable tool to be used in clinical assessments and risk stratification.
Gu et al. [20] conducted an extensive study to explore the relationship between the VAI and prediabetes. The study employed a cross-sectional epidemiological survey, categorizing all participants into four groups based on VAI and WC levels: VAI and WC both within the normal range, increased VAI (postcritical VAI) with normal WC, VAI with increased WC (normal VAI with postcritical WC), and increased VAI with increased WC (both postcritical VAI and WC), respectively. The researchers employed multivariate logistic analysis to analyze the associations between these groups and prediabetes, as well as diabetes. Results indicated that both VAI and WC emerged as independent risk factors for prediabetes. In males, the Odds Ratios (ORs) for prediabetes were 1.641 (95% CI 1.146–2.349), P=0.007, in the increased VAI with normal WC group and 1.454 (95% CI 1.055–2.005), P=0.022, in the normal VAI and increased WC group, both in Model 2. In females, the ORs for prediabetes were 2.305 (95% CI 1.623–3.273), P=0.000, in the increased VAI and normal WC group and 1.997 (95% CI 1.529–2.608), P=0.000, in the normal VAI and increased WC group. Furthermore, the study assessed the accuracy of predictions for prediabetes using Receiver Operating Characteristic (ROC) curve analysis. For men, the area under the curve (AUC) value of VAI was 0.601 (95% CI 0.568–0.634), P=0.000, and for women, it was 0.645 (95% CI 0.618–0.672), P=0.000. Notably, WC exhibited the highest AUC value of 0.605 (95% CI 0.571–0.638), P=0.000, in prediabetes for men and the highest AUC value of 0.673 (95% CI 0.648–0.697), P=0.000, in prediabetes for women. These findings underscore the significance of VAI and WC in predicting prediabetes, with WC demonstrating notable efficacy in both genders.
Pekgor et al. [21] conducted a comprehensive investigation into the positive and significant relationship between HOMA-IR and VAI levels. Their study discussed the exploration of VAI levels in obese patients, both with and without MetS, shedding light on its association with IR. Additionally, the researchers aimed to establish a cutoff value for VAI in identifying patients with MetS. In this study, 92 obese patients, ranging in age from 18 to 65, were included. The levels of HOMA-IR and VAI were meticulously calculated for each participant. Notably, among the 92 patients, 41 (44.6%) with MetS exhibited significantly higher levels of both HOMA-IR and VAI (P < 0.001 for both). The determined cutoff value for VAI in predicting MetS was identified as 2.205. Intriguingly, the prevalence of MetS was 22.2% when VAI was below this threshold, but it surged to 66% when VAI exceeded 2.205. Furthermore, the study unveiled a positive correlation between VAI and HOMA-IR levels. In cases where HOMA-IR was equal to or greater than 2.5, VAI was observed to be higher in 39.1% of individuals, and concurrently, levels of high-density lipoprotein-cholesterol were lower. The established cutoff value for VAI in predicting IR was determined as 2.31. Within this context, the prevalence of IR was 23.4% in patients with VAI below 2.31, contrasting with a notably higher frequency of 55% in individuals with VAI equal to or greater than 2.31. These findings underscore the significance of VAI as a valuable indicator for assessing both MetS and IR in obese patients, providing clinicians with a practical tool for risk stratification and management.
Jafari and colleagues [22] investigated the correlation between IR indices and the 5- and 10-year incidence of CVD. The study included 1888 and 1450 healthy adults aged 15 to 75 years, selected from the 5895 participants of the KERCADR study in 2012. Participants were monitored for five and ten years, and baseline Lipid Accumulation Product (LAP), triglyceride-glucose index (TyG), and VAI were computed. Logistic regression models were employed to evaluate their association with CVD incidence during the specified follow-up periods. Additionally, the predictive accuracy of these indices in predicting CVD development was assessed using the area under the ROC AUC. Over the 5- and 10-year follow-ups, 399 and 476 CVD cases (21.1% and 32.8%) were recorded, respectively. The adjusted odds ratio (AOR, 95% CI) for 5-year CVD risk showed LAP (2.24 [1.44, 3.50]), VAI (1.58 [1.08, 2.33]), and TyG (1.57 [1.02, 2.42]). For 10-year CVD risk, AOR was LAP (1.61 [1.04, 2.49]), TyG (1.57 [1.02, 2.41]), and VAI (1.41 [0.96, 2.09]). In summary, when considering CVD risk prediction, LAP, TyG, and VAI emerged as more effective predictors compared to conventional single risk factors, which demonstrates insulin resistance indexes’ superiority compared to conventional clinical techniques to assess CVD risk.
The presence of the MetS is linked to a twofold rise in cardiovascular outcomes and a 1.5-fold increase in overall mortality. There is a crucial need for research to determine whether the prognostic significance of the MetS surpasses the risk associated with the cumulative impact of its individual components. Additionally, investigations are imperative to unravel the mechanisms through which the metabolic syndrome amplifies the risk of cardiovascular events [23].
In 2021, a cross-sectional observational cohort study in Brazil aimed to evaluate the diagnostic accuracy of eight IR indicators in identifying MetS within the Brazilian population. This study specifically aimed to evaluate the diagnostic accuracy of eight IR indicators in identifying MetS within the Brazilian population. The studied IR indicators included the metabolic score for IR (METS-IR), triglycerides to high-density lipoprotein cholesterol index (TG-HDL-c), TyG, triglyceride glucose index body mass-index (TyG-BMI), triglyceride glucose index-neck circumference (TyG-NC), triglyceride glucose index-neck circumference to height ratio (TyG-NHtR), triglyceride glucose index-waist circumference (TyG-WC), and triglyceride glucose index-waist to height ratio (TyG-WHtR). The research cohort comprised 268 participants, consisting of 152 men and 116 women aged between 53 and 59 years. Among them, 111 individuals were diagnosed with MetS according to the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) criteria. The study findings demonstrated significant diagnostic accuracy across all eight IR indicators. TyG-WC emerged as the leader with the highest AUC value at 0.849 (95% confidence interval [CI]: 0.800–0.889), followed closely by TyG (AUC: 0.837, 95% CI: 0.787–0.879) and TG-HDL-c (AUC: 0.817, 95% CI: 0.765–0.861). Notably, these values underscore the robust discriminatory ability of these indicators in identifying MetS within the Brazilian population. Further analysis revealed that TG-HDL-c exhibited the most elevated diagnostic sensitivity at 90.99%, closely followed by TyG-WC (89.19%) and TyG-NC (84.68%). Conversely, TyG demonstrated the highest diagnostic specificity at 73.89%, followed by TyG-WHtR (72.61%) and TyG-WC (66.88%). These sensitivity and specificity metrics highlight the capacity of these IR indicators to accurately identify individuals with MetS [24]. It is noteworthy that VAI was not included in the scope of this study.
In our study, we observed an insignificance association between VAI values and CRP levels. This contrasts with findings by Ferreira et al. [25], who conducted a cross-sectional population-based study involving 854 adults in Viçosa, Minas Gerais, Brazil. Their investigation incorporated a questionnaire, anthropometric measurements, body composition analysis, and biochemical data collection. The analysis, employing ordinal logistic regression, aimed to identify factors associated with VAI. Interestingly, in the study by Ferreira et al., a positive association between VAI and the increase in the percentage of body fat, uric acid concentration, and ultra-sensitive C-reactive protein in the blood was noted among males. Among females, the factors associated with VAI included an increase in age, NC, elevated serum uric acid concentration, and higher levels of CRP. The divergence in findings between our study and that of Ferreira et al. underscores the complexity of factors influencing VAI associations. Variability in study populations, methodologies, and regional characteristics may contribute to these differences. It is important to highlight that the participants in our study were drawn from the São Paulo state of Brazil, while Ferreira et al.'s study sample originated from Minas Gerais, another Brazilian state. This geographical distinction between the two studies emphasizes the potential existence of regional variability. The diverse demographic, lifestyle, and environmental factors across different Brazilian states could contribute to variations in health-related parameters and, consequently, impact the associations between VAI and biomarkers like CRP. Further research and exploration are essential to gain a comprehensive understanding of the multifaceted relationships between VAI and various regional factors affecting adiposity and inflammation.
With regards lipid assessments, Jabłonowska-Lietz et al [26] conducted an investigation into the potential of VAI as a reliable predictor for lipid abnormalities among 106 obese adults. This diverse study group comprised 72 women and 34 men, with an average age of 39.0 ± 5.9 years, and a mean BMI of 32.6 ± 2.4 kg/m2. These participants were admitted for body weight reduction. The comprehensive evaluation encompassed various anthropometric measures, including body weight (BW), height, WC, hip circumference (HC), BMI, waist-to-hip ratio (WHR), VAI, body adiposity index (BAI), and waist-to-height ratio. Additionally, bioelectrical impedance was used to determine visceral adipose tissue (VAT) levels and body fat percentage (FM%). Serum concentrations of key lipid parameters, including TC, HDL, LDL, TG, glucose, insulin, and HOMA-IR, were also meticulously assessed. The results revealed significant associations between several anthropometric indicators and VAT estimated by bioimpedance. Notably, VAI, WC, and WHR emerged as robustly correlated with glucose and lipid abnormalities in the obese population. Conversely, BAI and BMI exhibited correlations with total FM%. Furthermore, WC, WHR, and VAI demonstrated correlations with total body weight. These findings underscore the potential of VAI, along with specific anthropometric measures, as valuable indicators for predicting lipid disturbances in obese individuals.
Goldani et al. [27] explored the utility of VAI in predicting components of MetS among elderly individuals in Brazil. This cross-sectional study involved 221 elderly participants with a mean age of 70.65 ± 7.34 years, comprising 53.4% females and 46.4% males. The research gathered comprehensive data, including weight, height, WC, FBG, TG, TC, HDL-c, LDL-c, and blood pressure (BP), along with lifestyle information. Anthropometric indicators such as BMI and WHR were calculated. Adiposity measures were then compared with MetS components, and the predictive capability of VAI for MetS component occurrence was assessed. The analysis of associations among biochemical and MetS components revealed direct and significant correlations of BMI, weight, and VAI with blood glucose, HDL-c, and TG (p<0.01). Remarkably, VAI exhibited the strongest correlation with all parameters. In terms of VAI's applicability in determining the relative risk of MetS component occurrence, it emerged as a robust predictor. Specifically, VAI demonstrated good predictive ability for abdominal obesity (OR = 1.27, p<0.001), hyperglycaemia (OR = 1.10, p=0.043), hypertriglyceridemia (OR = 3.64, p<0.001), and low HDL-c (OR = 2.26, p<0.001).
In another Brazilian investigation, researchers explored the use of VAI for predicting components of MetS, focusing on a younger population. Schuster et al. [28] conducted a cross-sectional survey involving 444 individuals, with a mean age of 25.6 ± 6.5, and a predominant representation of 77.7% females. This study delved into the applicability of VAI in forecasting MetS components in young adults. Comprehensive data on weight, height, WC, BF%, FBG, TG, TC, HDL-c, LDL-c, and BP were collected, alongside information on participants' lifestyles. BMI and WHR were also computed. The results revealed correlations between VAI and glucose (r=0.136), HDL-c (r=-0.436), and TG (r=0.825) in females. Among males, VAI correlated with glucose (r=0.258), HDL-c (r=-0.550), TG (r=0.897), and diastolic BP (r=0.290). Elevated VAI was associated with an increased risk of abdominal obesity (OR=1.86), hypertriglyceridemia (OR=30.74), and low HDL-c (OR=3.95). Notably, among obesity indicators, VAI exhibited a larger AUC for increased TG and low HDL-c. The study contributes valuable information for clinical assessments and risk stratification in the context of metabolic health among the younger demographic.
By delving into these various aspects, we can unravel the intricate relationship between VAI and the risk of CVD. Considering its practicality, simplicity, and non-invasive nature, integrating VAI into daily clinical practice holds considerable promise. The incorporation of VAI into routine assessments could offer clinicians a reliable tool to gauge the potential cardiovascular risks associated with adiposity. This approach not only enhances our ability to identify individuals at risk but also lays the foundation for the development of targeted interventions and preventive strategies to mitigate the impact of CVD. Thus, a thorough evaluation of VAI across multiple parameters is essential for maximizing its clinical utility and advancing its integration into everyday healthcare practices.
5. Conclusions and Future Research Directions
In the course of our investigation, the VAI revealed a notable and positive correlation with various biochemical and anthropometric parameters, along with IR, which transform into CVD risk factors when dysregulated. The findings from our sample indicate that VAI serves as a straightforward and non-invasive tool, proving to be exceptionally valuable in detecting metabolic alterations stemming primarily from AT dysfunction, notably dyslipidemia. Given its simplicity and efficacy, VAI should be routinely incorporated into clinical practice, becoming an integral part of cardiovascular risk assessment. Moreover, its continued application in diverse research studies is warranted, contributing to the establishment of a comprehensive cardiovascular routine for patients identified to be at risk for cardiovascular events. This proactive approach holds significant promise in advancing our understanding of the intricate interplay between VAI and various metabolic parameters, ultimately enhancing cardiovascular risk management strategies.
Embark on longitudinal investigations to meticulously track the trajectory of the VAI over an extended timeframe is of extreme importance. This in-depth examination aims to unravel the dynamic evolution of VAI and its profound implications for long-term cardiovascular health. By systematically monitoring VAI trends over an extended period, researchers can glean valuable insights into the progressive changes associated with this adiposity index and discern its potential impact on cardiovascular outcomes. This comprehensive analysis will contribute to a more nuanced understanding of the temporal patterns of VAI, offering critical information for refining risk assessment strategies and guiding personalized interventions in the realm of cardiovascular health.
Researchers must also examine the suitability and dependability of VAI across a broad spectrum of populations, considering variables such as age, ethnicity, geographical location, and regional susceptibilities. Delving into the potential variances in these factors will contribute to a more comprehensive understanding of VAI's generalizability, ensuring its effectiveness across diverse demographic groups.
Scientists must also embark on a thorough exploration of the intricate mechanisms that establish the connection between VAI and inflammation, delving into the molecular pathways and cellular interactions that underlie this association. By unraveling the intricacies of these biological processes, researchers can gain profound insights into the molecular underpinnings of VAI-related inflammation, opening avenues for innovative therapeutic interventions. Within this research framework, it is essential to scrutinize the molecular pathways involved in the inflammatory response triggered by elevated VAI. Investigate the signaling cascades, cytokine profiles, and immune cell activations that contribute to the inflammatory milieu associated with visceral adiposity. This in-depth exploration may lead to the identification of novel therapeutic targets for mitigating cardiovascular risk associated with elevated VAI. By pinpointing specific molecules or cellular processes that play pivotal roles in VAI-induced inflammation, researchers can envision the development of precision-targeted therapies. These interventions may range from pharmacological agents that modulate key inflammatory mediators to lifestyle interventions that address the cellular and molecular drivers of VAI-related inflammation.
Researchers must delve into a comprehensive exploration of the genetic factors that exert influence on the VAI, thereby unraveling the heritability patterns inherent in this index. By scrutinizing the genetic determinants associated with VAI, researchers can uncover valuable insights into the extent to which individual genetic makeup contributes to the susceptibility to cardiovascular risks linked with visceral adiposity. This line of inquiry involves conducting detailed investigations into the hereditary aspects of VAI, aiming to discern the specific genetic variations or polymorphisms that may predispose individuals to alterations in their visceral adiposity levels. The research should encompass large-scale genomic studies, employing advanced techniques such as genome-wide association studies (GWAS). Moreover, this investigation may lead to the identification of gene-environment interactions, shedding light on how lifestyle factors interact with genetic predispositions to influence VAI. Pinpointing these gene-environment interactions is instrumental in developing personalized approaches to cardiovascular risk assessment and management, as it allows for a more nuanced and precocious understanding of individual susceptibility.
Author Contributions
Conceptualization, L.F.L., S.M.B., M.D.B., A.C.A.d.C, M.O., P.C.d.S.B., T.L.M.Z., and K.Q.; methodology, L.F.L., S.M.B., L.A.S., K.P.S., M.D.B., and K.Q.; software, F.C.C., A.P., B.B.C., C.T.C., G.A.A., I.d.N.V., B.L.B., and J.C.A.; validation, L.F.L., S.M.B., R.J.T., C.R.P.D., J.F.d.S.H., M.D.B., and K.Q.; formal analysis, L.F.L., S.M.B., M.D.B., and K.Q.; investigation, L.F.L., F.C.C., A.P., B.B.C., C.T.C., G.A.A., I.d.N.V., J.C.A., S.M.B., L.A.S., K.P.S., M.D.B., and K.Q.; resources, L.F.L. and S.M.B.; data curation, L.F.L., S.M.B., M.D.B., and K.Q.; writing—original draft preparation, L.F.L. and S.M.B.; writing—review and editing, L.F.L., S.M.B., M.D.B., and K.Q.; visualization, L.F.L., S.M.B., M.D.B., and K.Q.; supervision, L.F.L., S.M.B., M.D.B., and K.Q.; project administration, L.F.L., S.M.B., and K.Q.; funding acquisition, L.F.L. and S.M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Unibersity of Marília (protocol code 2.746.117 November 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Harvey, I.; Boudreau, A.; Stephens, J.M. Adipose tissue in health and disease. Open Biol 2020, 10, 200291. [Google Scholar] [CrossRef]
- Lenz, M.; Arts, I.C.W.; Peeters, R.L.M.; de Kok, T.M.; Ertaylan, G. Adipose tissue in health and disease through the lens of its building blocks. Sci Rep 2020, 10, 10433. [Google Scholar] [CrossRef]
- Mottillo, E.P.; Steinberg, G.R. Current and emerging roles of adipose tissue in health and disease. Biochem J 2020, 477, 3645–3647. [Google Scholar] [CrossRef]
- Callaghan, M.A.; Alatorre-Hinojosa, S.; Connors, L.T.; Singh, R.D.; Thompson, J.A. Plasticizers and Cardiovascular Health: Role of Adipose Tissue Dysfunction. Front Pharmacol 2020, 11, 626448. [Google Scholar] [CrossRef]
- Bagyura, Z.; Kiss, L.; Lux, Á.; Csobay-Novák, C.; Jermendy Á, L.; Polgár, L.; Szelid, Z.; Soós, P.; Merkely, B. Association between coronary atherosclerosis and visceral adiposity index. Nutr Metab Cardiovasc Dis 2020, 30, 796–803. [Google Scholar] [CrossRef]
- Bolat, M.S.; Kocamanoglu, F.; Ozbek, M.L.; Buyukalpelli, R.; Asci, R. Can High Visceral Adiposity Index Be a Risk Factor for Sexual Dysfunction in Sexually Active Men? J Sex Med 2020, 17, 1926–1933. [Google Scholar] [CrossRef]
- Yang, J.; Li, H.; Han, L.; Zhang, L.; Zhou, Y. Association between Visceral Adiposity Index and hypertension among Chinese Adults: a nationwide cross-sectional study in the China Health and Nutrition Survey. Blood Press Monit 2020, 25, 271–277. [Google Scholar] [CrossRef]
- Nusrianto, R.; Tahapary, D.L.; Soewondo, P. Visceral adiposity index as a predictor for type 2 diabetes mellitus in Asian population: A systematic review. Diabetes Metab Syndr 2019, 13, 1231–1235. [Google Scholar] [CrossRef]
- Randrianarisoa, E.; Lehn-Stefan, A.; Hieronimus, A.; Rietig, R.; Fritsche, A.; Machann, J.; Balletshofer, B.; Häring, H.U.; Stefan, N.; Rittig, K. Visceral Adiposity Index as an Independent Marker of Subclinical Atherosclerosis in Individuals Prone to Diabetes Mellitus. J Atheroscler Thromb 2019, 26, 821–834. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: 1988.
- Gibson, R.S. Principles of Nutritional Assessment; Oxford University Press: 2005.
- Kurisu, S.; Nitta, K.; Sumimoto, Y.; Ikenaga, H.; Ishibashi, K.; Fukuda, Y.; Kihara, Y. Frontal QRS-T angle and World Health Organization classification for body mass index. Int J Cardiol 2018, 272, 185–188. [Google Scholar] [CrossRef]
- Patry-Parisien, J.; Shields, M.; Bryan, S. Comparison of waist circumference using the World Health Organization and National Institutes of Health protocols. Health Rep 2012, 23, 53–60. [Google Scholar]
- Stabe, C.; Vasques, A.C.; Lima, M.M.; Tambascia, M.A.; Pareja, J.C.; Yamanaka, A.; Geloneze, B. Neck circumference as a simple tool for identifying the metabolic syndrome and insulin resistance: results from the Brazilian Metabolic Syndrome Study. Clin Endocrinol (Oxf) 2013, 78, 874–881. [Google Scholar] [CrossRef]
- Wolska, A.; Remaley, A.T. Measuring LDL-cholesterol: what is the best way to do it? Curr Opin Cardiol 2020, 35, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Mirr, M.; Skrypnik, D.; Bogdański, P.; Owecki, M. Newly proposed insulin resistance indexes called TyG-NC and TyG-NHtR show efficacy in diagnosing the metabolic syndrome. J Endocrinol Invest 2021, 44, 2831–2843. [Google Scholar] [CrossRef] [PubMed]
- So, A.; Sakaguchi, K.; Okada, Y.; Morita, Y.; Yamada, T.; Miura, H.; Otowa-Suematsu, N.; Nakamura, T.; Komada, H.; Hirota, Y.; et al. Relation between HOMA-IR and insulin sensitivity index determined by hyperinsulinemic-euglycemic clamp analysis during treatment with a sodium-glucose cotransporter 2 inhibitor. Endocr J 2020, 67, 501–507. [Google Scholar] [CrossRef]
- Borga, M.; West, J.; Bell, J.D.; Harvey, N.C.; Romu, T.; Heymsfield, S.B.; Dahlqvist Leinhard, O. Advanced body composition assessment: from body mass index to body composition profiling. J Investig Med 2018, 66, 1–9. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C. Visceral Adiposity Index: An Indicator of Adipose Tissue Dysfunction. International Journal of Endocrinology 2014, 2014, 730827. [Google Scholar] [CrossRef]
- Gu, D.; Ding, Y.; Zhao, Y.; Qu, Q. Visceral Adiposity Index was a useful Predictor of Prediabetes. Exp Clin Endocrinol Diabetes 2018, 126, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Pekgor, S.; Duran, C.; Berberoglu, U.; Eryilmaz, M.A. The Role of Visceral Adiposity Index Levels in Predicting the Presence of Metabolic Syndrome and Insulin Resistance in Overweight and Obese Patients. Metab Syndr Relat Disord 2019, 17, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Jafari, A.; Najafipour, H.; Shadkam, M.; Aminizadeh, S. Evaluation of the novel three lipid indices for predicting five- and ten-year incidence of cardiovascular disease: findings from Kerman coronary artery disease risk factors study (KERCADRS). Lipids Health Dis 2023, 22, 169. [Google Scholar] [CrossRef] [PubMed]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed]
- Fornari Laurindo, L.; Minniti, G.; José Tofano, R.; Quesada, K.; Federighi Baisi Chagas, E.; Maria Barbalho, S. Detection of Metabolic Syndrome Using Insulin Resistance Indexes: A Cross-Sectional Observational Cohort Study. Endocrines 2023, 4, 257–268. [Google Scholar] [CrossRef]
- Ferreira, F.G.; Segheto, W.; Da Silva, D.C.G.; Pereira, P.F.; Longo, G.Z. Visceral adiposity index associated with behavioral and inflammatory parameters in adults: a population based study. Nutr Hosp 2018, 35, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Jabłonowska-Lietz, B.; Wrzosek, M.; Włodarczyk, M.; Nowicka, G. New indexes of body fat distribution, visceral adiposity index, body adiposity index, waist-to-height ratio, and metabolic disturbances in the obese. Kardiol Pol 2017, 75, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Goldani, H.; Adami, F.S.; Antunes, M.T.; Rosa, L.H.; Fassina, P.; Quevedo Grave, M.T.; Morelo Dal Bosco, S. APPLICATILITY OF THE VISCERAL ADIPOSITY INDEX (VAI) IN THE PREDICTION OF THE COMPONENTS OF THE METABOLIC SYNDROME IN ELDERLY. Nutr Hosp 2015, 32, 1609–1615. [Google Scholar] [CrossRef] [PubMed]
- Schuster, J.; Vogel, P.; Eckhardt, C.; Morelo, S.D. Applicability of the visceral adiposity index (VAI) in predicting components of metabolic syndrome in young adults. Nutr Hosp 2014, 30, 806–812. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Correlations of VAI with anthropometric parameters in both sexes: (a) NC in men, (b) NC in women, (c) WC in men, (d) WC in women, (e) BMI in men, and (f) BMI in women. NC: neck circumference, WC: waist circumference and BMI: body mass index.
Figure 1.
Correlations of VAI with anthropometric parameters in both sexes: (a) NC in men, (b) NC in women, (c) WC in men, (d) WC in women, (e) BMI in men, and (f) BMI in women. NC: neck circumference, WC: waist circumference and BMI: body mass index.
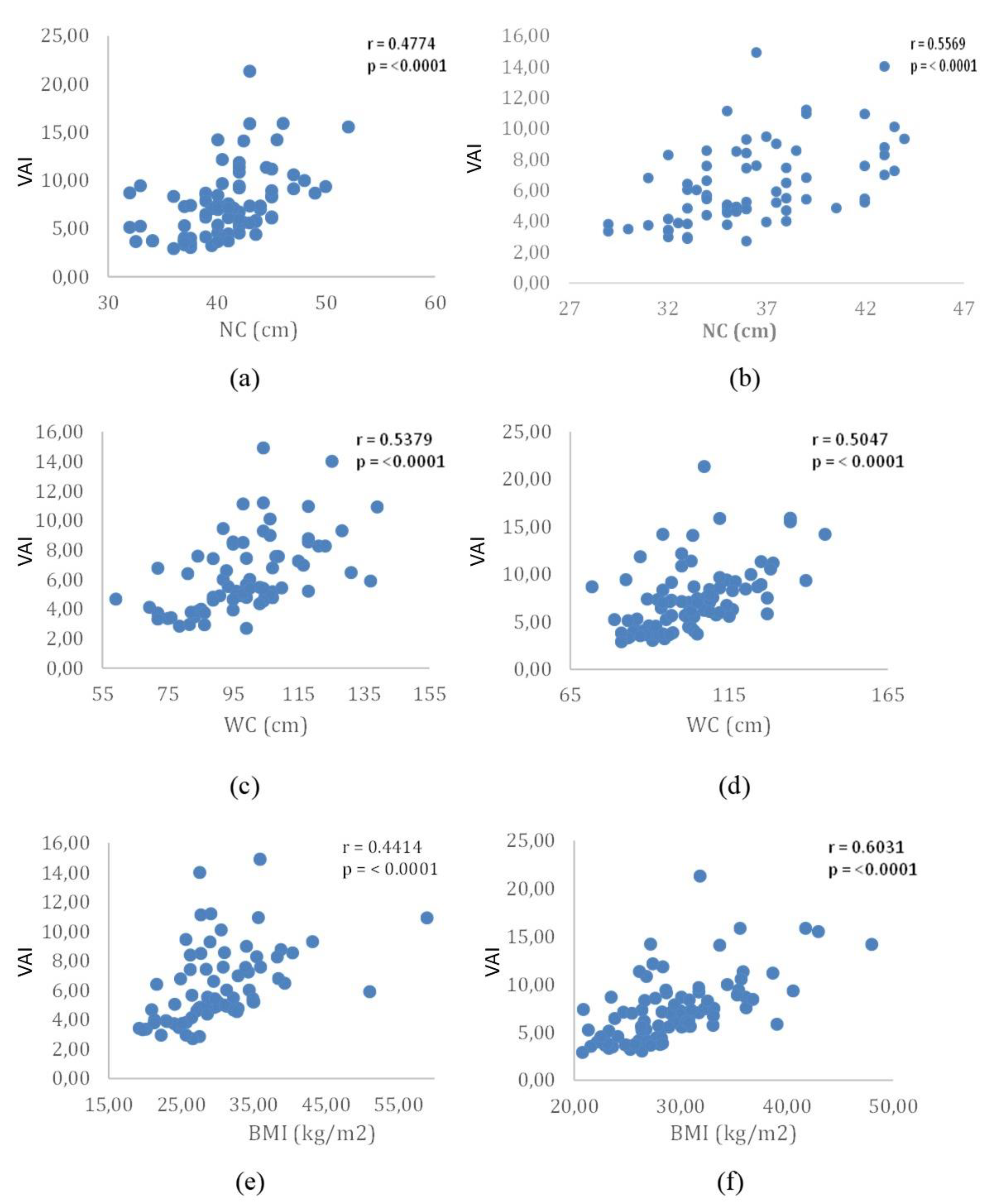
Figure 2.
Correlation of VAI with biochemical parameters in both sexes: (a) FBG in men, (b) FBG in women, (c) TC in men, (d) TC in women, (e ) HDL-c in men, (f) HDL-c in women, (g) LDL-c in men, (h) LDL-c in women, (i) TG in men, (j) TG in women, (k) CRP in men, and (l) CRP in women. FBG: fasting blood glucose, TC: total cholesterol, HDL-c: high-density lipoprotein cholesterol, LDL-c: low density lipoprotein cholesterol, TG: triglycerides and CRP: C reactive protein.
Figure 2.
Correlation of VAI with biochemical parameters in both sexes: (a) FBG in men, (b) FBG in women, (c) TC in men, (d) TC in women, (e ) HDL-c in men, (f) HDL-c in women, (g) LDL-c in men, (h) LDL-c in women, (i) TG in men, (j) TG in women, (k) CRP in men, and (l) CRP in women. FBG: fasting blood glucose, TC: total cholesterol, HDL-c: high-density lipoprotein cholesterol, LDL-c: low density lipoprotein cholesterol, TG: triglycerides and CRP: C reactive protein.
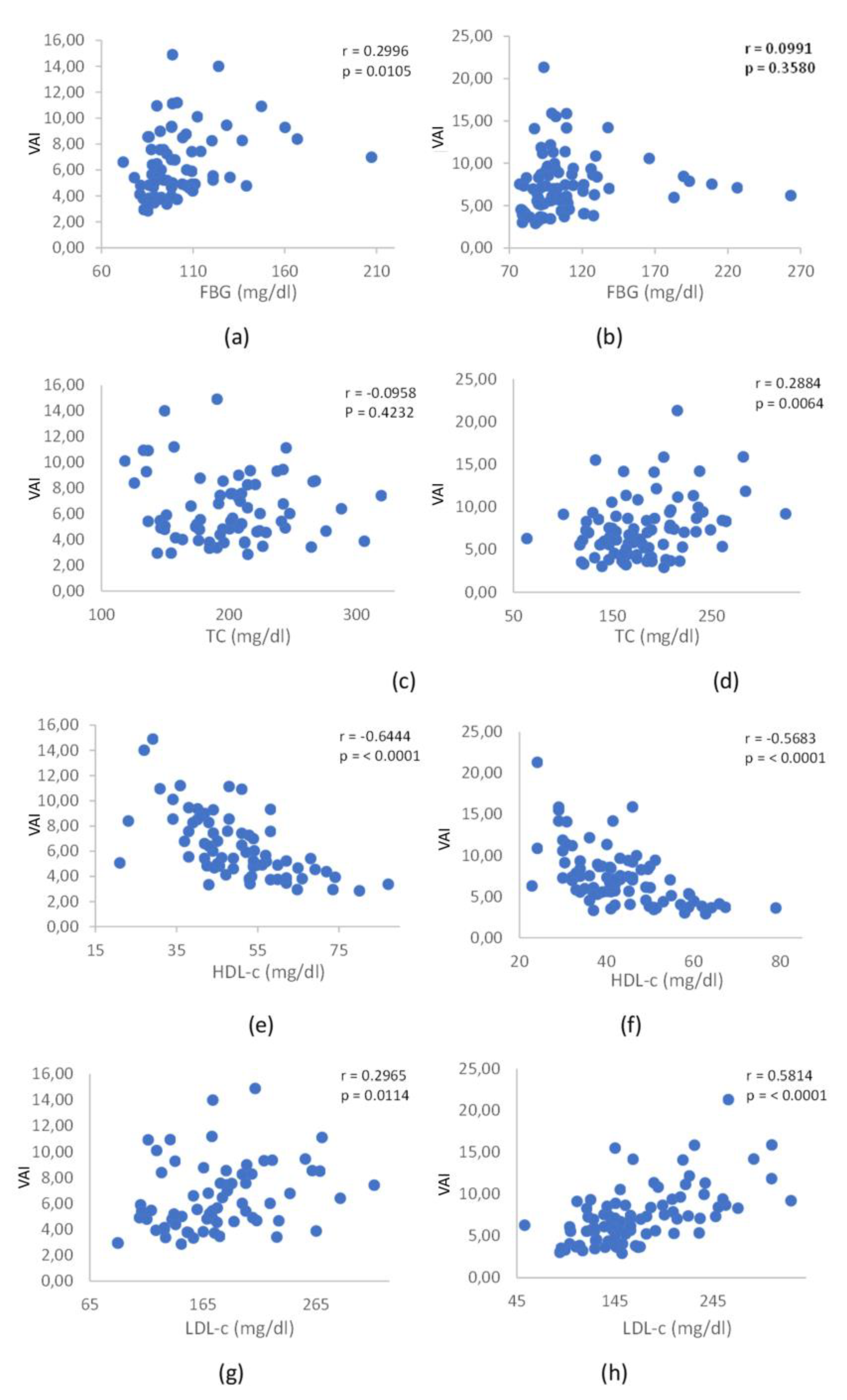
Figure 3.
Correlation of visceral adiposity index with parameters that assess insulin resistance: insulin in fasting men (a), insulin in fasting women (b), HOMA-IR in men (c), and HOMA-IR in women (d). HOMA-IR: homeostatic model assessment for insulin resistance.
Figure 3.
Correlation of visceral adiposity index with parameters that assess insulin resistance: insulin in fasting men (a), insulin in fasting women (b), HOMA-IR in men (c), and HOMA-IR in women (d). HOMA-IR: homeostatic model assessment for insulin resistance.
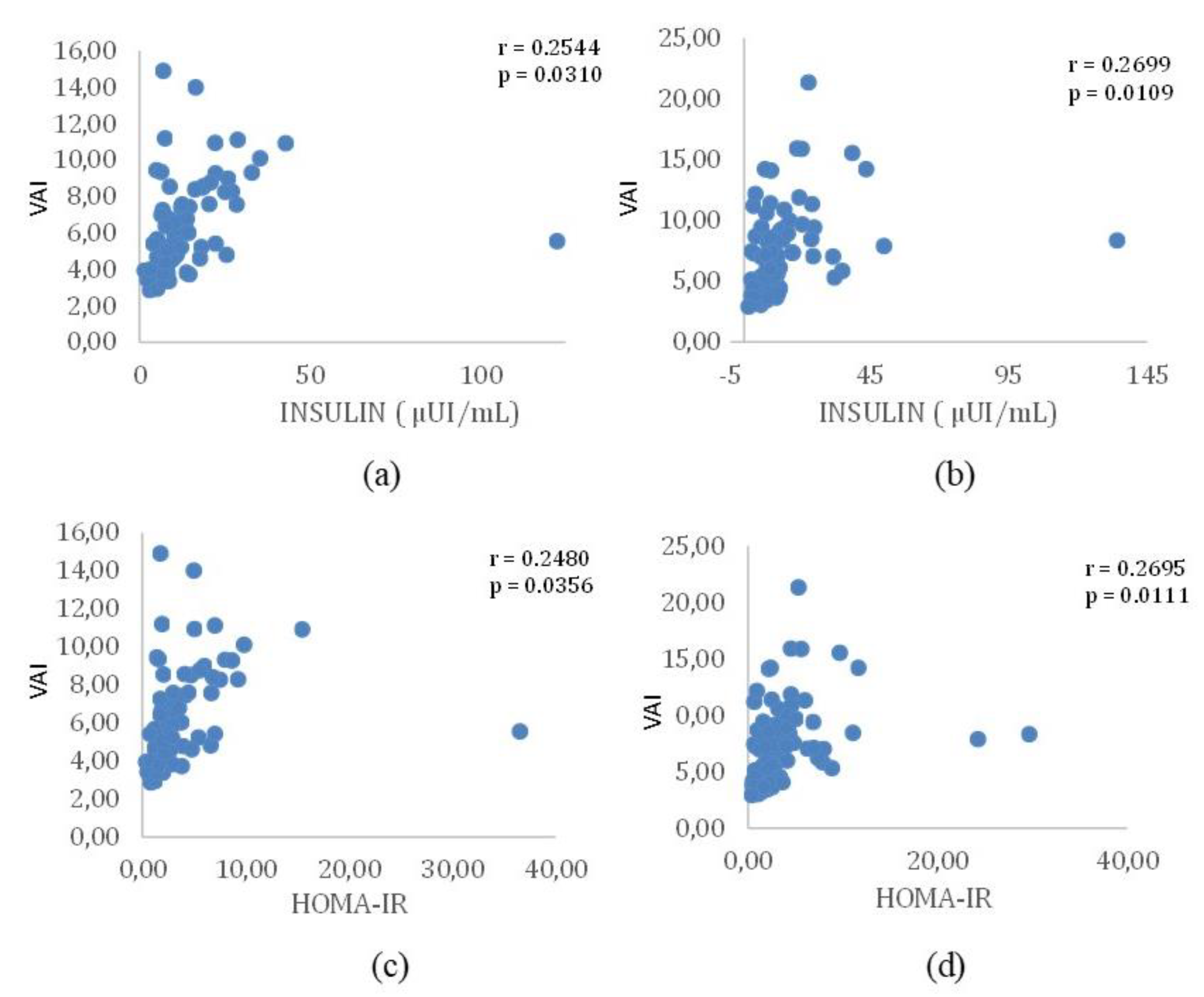

Table 1.
Anthropometric and biochemical parameters of the sample (n=160).
| Parameters | Men (n = 88) | Women (n =72) |
|---|---|---|
| Age | 86.56 ± 17.99 | 59.97 ± 11.89 |
| BMI (kg / m2) | 29.36 ± 5.27 | 30.11 ± 6.80 |
| WC (cm) | 103.26 ± 14.73 | 98.65 ± 16.21 |
| NC (cm) | 40.87 ± 3.91 | 36.20 ± 3.71 |
| FBG (mg /dL) | 108.42 ± 32.77 | 102.61 ± 22.14 |
| INS (μIU / mL) | 13.59 ± 15.93 | 14.33 ± 15.45 |
| TC (mg / dL) | 180.43 ± 44.80 | 199.81 ± 42.85 |
| TG (mg / dL) | 155.08 ± 80.44 | 137.00 ± 62.85 |
| CRP (mg/l) | 7.07 ± 32.51 | 4.87 ± 5.01 |
| HDL-c (mg / dL) | 43.16 ± 11.08 | 50.03 ± 12.80 |
| LDL-c (mg / dL) | 168.28 ± 55.01 | 177.18 ± 47.72 |
| VAI* | 7.37 ± 3.46 | 3.5 ± 3.2 |
| HOMA-IR** | 3.73 ± 4.30 | 3.85 ± 4.74 |
Values are presented as mean ± standard deviation (SD) for continuous variables or number (percentage) for categorical variables.* VAI is a sex-specific mathematical equation based on WC, BMI, TG, and HDL-c levels that indirectly expresses visceral adipose dysfunction associated with cardiometabolic risk.** HOMA -IR is an index to assess insulin resistance based on serum glucose and insulin levels in fasting.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



