
Submitted:
11 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
Some evidence supports the influence of the implant macro-design and primary stability. Additionally, tactile perception can be used to assess implant stability when placing the implant. This research aimed to quantify the primary and secondary stability of three implant systems with two different macro geometries (cylindrical and conical) determined through the insertion torque and the implant stability quotient (ISQ) at the moment of implant placement as a function of implant-related factors (length, width, dental arch, and implant location in the arch), intraoperative factors (bone density determined subjectively by the clinician's tactile perception), and patient-related factors (age, gender and bone density determined objectively in the cone beam computed tomography (CBCT). Methods: 102 implants of three implant systems with two different macro geometries (conical and cylindrical) were placed in 53 patients. The insertion torque, the ISQ at the implant placement (ISQ0), and bone quality according to the clinician's tactile sensation were recorded on the day of the surgery. After a three-month healing period, the ISQ was re-evaluated (ISQ3). Results: Cylindrical implants exhibited significantly higher insertion torque and ISQ at the moment of the surgery and after three months than conical implants. Cylindrical implants also showed significantly lower indices of tactile evaluation of bone quality during the implant placement surgery. However, no differences were demonstrated in the bone density measured objectively in the CBCT. (4) Conclusions: The cylindrical implants achieved the highest values for primary stability (Ncm and ISQ) and secondary stability (ISQ after three months). Insertion torque was the variable that most influenced ISQ on the day of the surgery. Implant location (incisors-canines, bicuspids-molars) and the implant macro geometry were the variables that most influenced the secondary stability (ISQ at three months).
Keywords:
Dental implants
; bone density
; macro-design
; implant stability
; computerized tomography
; bone quality
1. Introduction
Dental implants are an option that provides satisfactory and esthetic results when treating edentulous areas or performing immediate implantology [1,2,3]. Consolidated technologies such as cone beam computed tomography (CBCT), specific planning software, and non-invasive tools for evaluating the primary and secondary stability of the implant (e.g., resonance frequency analysis, RFA) provide the means for clinicians to reach a correct diagnosis and treatment plan [4,5,6].
Research has demonstrated that implant stability, bone volume, and quality determination can contribute to dental implant surgery success [7, 8]. Primary impact stability is one of the areas that has received the most attention since failure rates have been observed to decrease when insertion torque increases [9, 10] because of a reduction of implant micromotion [11]. Primary stability is also influenced by bone quality, the macro geometry of the implant, and the drilling sequence used to prepare the implant bed [12,13,14]. Evaluating bone density before dental implant surgery enables the clinician to optimize the drilling sequence and select the best implant design (conical or cylindrical; self-tapping or non-self-tapping) to achieve optimal primary stability [11, 15].
Several classification systems have been established for evaluating bone density. Lekholm and Zarb [16] divided bone density into four types: from the more compact type I bone to type IV, which is low-density trabecular bone surrounded by a thin layer of cortical bone. Misch [17] classified bone density according to the surgeon’s tactile sensation from D1 – with a hardness analogous to oak or maple wood – to D4, approximately as hard as styrofoam [17]. Objective methods have also been developed to quantitatively assess bone density through the Hounsfield scale (Hounsfield units, HU)[18, 19]. Bone density ranges between 100 and 1900 HU, while soft tissues are close to or below 0 HU [18].
There appears to be evidence that primary and secondary stability is influenced by bone quality, implant macro geometry, and implant dimensions (diameter and length). Therefore, the present study was designed to analyze how bone quality, measured through Hounsfield Unit estimations, and the clinician’s tactile perception during implant placement (who categorized the bone from D1 to D4, according to the Misch [17] classification scheme) affected the primary and secondary implant stability of three implant systems with two different macro geometries (cylindrical and conical).
This clinical study aimed to compare the primary and secondary stability, determined through the insertion torque and the ISQ at the moment of implant placement and after three months, of two different implant macro geometries (cylindrical and conical) as a function of patient-related factors (gender, age, and bone quality determined objectively in the CBCT), implant-related factors (width, length, dental arch, and implant location in the arch), and intraoperative factors (bone quality determined by the clinician’s tactile sensation during implant placement). In addition, it was also aimed to determine the correlation (overall and within each macro geometry) between the patient-related, implant-related, and intraoperative variables. The null hypothesis was that no variable could predict the implant stability.
2. Materials and Methods
2.1. Study Design
In this prospective study, patients requiring implant surgery were consecutively recruited from December 2019 to September 2022. The trial protocol was registered on ClinicalTrials.gov (NCT05670340) and developed under the Declaration of Helsinki on medical research involving human subjects, as revised in 2013. Sample size calculation determined a subsample size of 31 implants to achieve a power of 80% and a level of significance of 5% (two-sided) for detecting a true difference in means between implant groups of 5 ISQ units, assuming a pooled standard deviation of 7 ISQ units for the day of surgery, and expected means between 70 and 75 ISQ among distinct implant subgroups.
The patients included in this study were partially or completely edentulous with healed bone crests. Exclusion criteria comprised patients with previous chemotherapy or radiotherapy history, with any medical compromise (metabolic bone disorder and/or uncontrolled diabetes), and under bisphosphonates treatment. Similarly, to provide standardization of bone maturation, patients who had recent tooth extraction at the implant sites (<3 months) or those treated with bone augmentation procedures were also excluded [20].
A preoperative CBCT scan was performed on all the patients, which was initially used for implant planning and evaluation of the bone quality at the expected implant site. Three types of implants with two different macro-designs were used. The Nobel Active® implant (Nobel Biocare AB, Gothenburg, Sweden) is a conical implant with a reverse neck, micro-threads in the coronal portion, a variable thread design (changing from a V-thread in the coronal portion to buttress threads in the apical portion), and a 1.2 mm thread pitch at the implant apex and body. The Nobel Parallel® implant (Nobel Biocare AB, Gothenburg, Sweden) is cylindrical with a conical apex and V-thread design. It has a thread pitch of 0.6 mm for implants with diameters of 3.75 mm and 4.3 mm and 0.8 mm for implants with a 5 mm diameter, meaning that it has a more significant number of threads. Finally, the 3i T3® implant (ZimVie, USA) is a conical implant with no micro-threads in the most coronal portion, a V-thread design, and a thread pitch of 0.8 mm. The implants were distributed randomly among patients using closed envelopes as the randomization method.
2.2. Preoperative Radiographic Assessment
A CBCT scan assessed each patient’s mandible and maxilla preoperative. Invivo™ 6 dental software was used for CBCT 3D scan image visualization and implant planning. This software enabled the surgeon to select the length and diameter of the implants placed in the patients. For the densitometric analysis, BTI Scan software (BTI Biotechnology Institute) was used to evaluate the averaged bone density (in HU) of the implant area and 0.5 mm all-around of the bone to be occupied by the planned implant. The BTI scan uses an algorithm that traduces bone density through the gray scales in HU, as depicted in Figure 1. The surgeon was blinded to the bone density-related assessment before and during the implant surgery.
2.3. Surgical Protocol
All implants were placed by an experienced surgeon (NQ) and then left for transmucosal healing, following a one-stage surgical procedure protocol. The surgeries were performed under local anesthesia, using articaine 2% mg/ml with epinephrine 1:100, 000. After applying the local anesthesia, mucoperiosteal flaps were elevated to expose the bone crest. The osteotomies were conducted following the manufacturers’ instructions for each type of implant and bone quality, so the last step of the drilling sequence varied depending on the clinician’s tactile evaluation of bone density while preparing the implant bed because he was blinded regarding the bone density assessed by CBCT.
When the surgeon perceived a hardness analogous to styrofoam (soft bone), undersized bone bed preparation was conducted. In contrast, the entire drilling sequence, including screw tap drills, was completed when the surgeon’s tactile evaluation indicated that there was bone with a hardness analogous to oak or maple wood (hard bone).
The surgeon placed the implants sequentially once the needed drilling protocol had been performed. Sixty-five conical implants (32 3i T3 implants and 33 Nobel Active implants) and thirty-seven cylindrical implants (37 Nobel Parallel implants) were placed in 53 patients (Figure 2). The surgeon subjectively recorded bone density during bed preparation while drilling into one of four bone-quality groups (D1-D4), following the Misch classification system [17]. The primary stability of each implant type was recorded with a manual torque wrench using the maximum insertion torque value (Ncm), rounded to the nearest 5 Ncm, obtained at the end of implant insertion into the recipient site. The values of implant stability quotient (ISQ) were also recorded (ISQ0). The Smartpeg® was placed in direct contact with the implant, and three consecutive measurements were taken (vestibular, interproximal, and lingual/palatal) to obtain a mean value (Figure 2). After the primary stability assessment, healing abutments were placed, and the flap was sutured with 5/0 simple sutures. After three months of osseointegration, secondary stability was again recorded using resonance frequency analysis (ISQ3).
2.4. Statistical Analysis
The normal distribution of data collected was assessed through the Saphiro-Wilks statistic. Measured insertion torque, implant stability quotient at the moment of implant insertion (ISQ0), and after three months (ISQ3) failed to follow a normal distribution, so non-parametric statistics were used. In the statistical description of the sample, the mean and standard deviation were used for describing the objectively measured bone density, and the median and the interquartile range for the insertion torque, and the implant stability quotient (at implant placement and after three months) quantitative variables. The absolute frequency and percentage in categories were used for describing the nominal variables. Although some implants were placed in the same patients, all were considered independent because they were objectively or subjectively individually characterized during data collection. Collected data was considered paired when comparing the implant stability quotient measured at the implant insertion and after three months. Depending on the normal distribution assessment, Pearson’s or Spearman’s correlation coefficient, and parametric tests (Student’s t-test) or non-parametric tests (Mann-Whitney (M-W) test) were used to compare the effect on the studied variables (insertion torque, ISQ0, and ISQ3) of the implant-related factors (implant macro geometry (cylindrical or conical), implant location (incisor-canine, bicuspids-molars), dental arch (mandible or maxilla) implant dimensions (diameter and length)), intraoperative variable (bone density, and bone quality determined by clinician’s tactile sensation), and patient’s-related factors (gender (male, female), and age (>55,<55)). Then, significant predictors for the ISQ0 and ISQ3 were identified through a stepwise linear regression analysis. Finally, a stepwise linear regression analysis was performed using ISQ0 and ISQ3 as dependent variables and the significant predictors previously identified. SPSS 27 statistical software (SPSS Statistics, version 27, IBM Corp) was used. Significance was set at p-values ≤ 0.05.
3. Results
Fifty-three patients (22 women and 31 men, with a mean age of 56.6 years ± 10.1) were included in this study (Table 1). One hundred-two implants were placed (43 in the mandible and 59 in the maxilla). Sixty-five conical implants (32 3i T3 implants (31.4%), 33 Nobel Active implants (32.4%)), and thirty-seven cylindrical implants (37 Nobel Parallel implants(36.3%)) were placed in 53 patients. The implants were also grouped according to their location in the arch: the incisor-canine group included 36 implants (21 conical and 15 cylindrical implants), and the bicuspid-molar group included 66 implants (44 conical and 22 cylindrical implants). The distribution of the implants of the study according to length and diameter is also shown in Table 1. The distribution, correlation, and analysis of the insertion torque, ISQ0, ISQ3, clinician’s tactile bone quality assessment, and bone density, together with their relationship for each studied macro geometry, are shown in Table 2 and Table 3.
Without dividing the data by implant macro geometry group (n=102 implants), a significant relationship was found between the clinician’s tactile bone quality assessment and the bone density, insertion torque, and ISQ values on the day of the surgery (Table 2, Figure 3). An indirect significant correlation was found between the clinician’s tactile bone quality assessment, the insertion torque values (rho=-0.425; p<0.001), and ISQ values on the day of the surgery (rho=-0.245; P=0.013). In other words, higher insertion torque and ISQ values were recorded when the clinician perceived the bone as hard (D1-type bone). Additionally, a significant inverse association was identified between the clinician’s tactile bone quality assessment and the bone density (in HU) (r=-0.273; P=0.005). In contrast, no statistical significance was revealed between the clinician’s tactile bone quality assessment and ISQ after 3 months (rho=--0.035; p=0.728). When analyzing the relationship between the clinician’s tactile bone quality assessment and the various patient-related and intraoperative variables in each of the implant macro geometry groups, an indirect significant association was found for the conical implants group in the insertion torque (rho=-0.403; p<0.001) and the bone density (r=-3.73; p=0.002). The cylindrical implants group also displayed an indirect significant association with the insertion torque (rho=-0.366; p=0.026) but not for the bone density (r=0.062; p=0.716).
When analyzing the association between insertion torque and ISQ, a strong positive correlation was identified in the conical implant group (rho=0.554; P<0.001) but not with the cylindrical implants (rho=0.214; p=0.203). Mann-Whitney test revealed that the cylindrical implant group displayed a significantly higher insertion torque than the conical implants (U=748; p<0.001). (Table 3)
Cylindrical implants showed a significantly higher ISQ on the day of the surgery (U=766.50; p=0.0002) and after three months (U==689.50; p<0.001). The clinician’s tactile sensation revealed a significantly softer bone when using conical implants (CHI2=22.2; p=0.001). However, bone density did not confirm the difference in bone density when using cylindrical or conical implants (t=1.481; p=0.142).
Descriptive data and the comparison of the patient-related and intraoperative variables in the distinct implant locations (the incisor-canine and bicuspid-molar regions) are summarized in Table 4. No significant differences were found when comparing the insertion torque, the ISQ on the day of the surgery (Figure 4), and the clinician’s tactile evaluation of bone density according to the implant location. In contrast, ISQ values recorded after three months were significantly higher in the bicuspid-molars area in the cylindric implants group (U=88.50; p=0.002) (Figure 5). Significant higher bone density was found in the incisors-canine area on conical and cylindrical implants (t=3.00; p=0.005 and t=3.99; p<0.001, respectively).
When studying the effect of arch location (maxilla or mandible) (Table 5), significantly higher ISQ values on the day of the surgery and greater bone density were demonstrated on the mandible when using conical implants (U<0286; p=0.005, and t=-2.578; p=0.012, respectively). It is also remarkable that insertion torque was higher in the maxilla when using conical implants (U=315; p=0.010), and that the ISQ recorded on the day of the surgery and after three months, and the bone density was higher in the maxilla when using cylindrical implants (U=131; p<0.001, U=202; p=0.006, and t=2.314; p=0.024, respectively).
Table 6 and Table 7 display descriptive data and the effect of the implant diameter (standard and wide) and the implant width (standard and long) for the various preoperative and intraoperative variables, respectively. Higher insertion torque and denser bone were detected for standard-width conical implants compared to wide implants (U=126; p=0.006, and t=3.454; p<0.001, respectively). Lower tactile bone quality indices were assessed for standard-width conical implants (CHI2=20.93; p<0.001). Higher insertion torque and ISQ on the day of the surgery and after three months were assessed for standard-width cylindrical implants., in comparison to conical implants (U=665; p=0.008, U=667; p=0.009, and U=537; p<0.001, respectively). (Table 6)
When cylindrical and conical implants were compared according to implant length (standard or long), no significant differences were identified (P>0.05) in any of the variables examined. However, significantly higher insertion torque and ISQ on the day of the surgery and after three months were assessed with long implants when using cylindrical implants (U=218; p=0.036, U=194.50; p=0.012, and U=201.50; p=0.018, respectively). The same effect was found in the ISQ after three months with standard-length implants (U=151.50; p=0.012).
ISQ on the day of the surgery (ISQ0) and after 3 months (ISQ3) were considered the dependent variables in the linear regression analysis. Implant-related factors (implant macro geometry, length, width, dental arch, and implant location in the arch), intraoperative factors (bone density determined subjectively by the clinician’s tactile perception, ISQ0, and insertion torque), and patient-related factors (age, gender, and bone density determined objectively in the cone beam computed tomography (CBCT)) were firstly assessed as independent variables. Still, only significant predictors were considered in the final linear regression analysis. The predictor variables used in the ISQ measured on the day of the surgery (ISQ0) linear regression analysis were insertion torque, length, and implant macro-design. For the ISQ measured after three months of osseointegration (ISQ3), predictors were location, implant macro-design, and age. (Table 8).
The primary stability linear regression model studied with the ISQ0 as the dependent variable resulted in very significant (F=12.589; p<0.001), although it only predicted 27.8% of the results for ISQ on the day of the surgery, according to the coefficient of determination (R2). Therefore, as a baseline, an average ISQ of 74.8 ± 7.79 is obtained on the day of the surgery at the incisor-canine area, and for each applied extra Ncm in the insertion torque, between 0.147 and 0.4 ISQ units are gained. Using longer implants results in a gain of 0.05-5.239 ISQ units, and utilizing conical-shaped implants results in a loss of 0.35-5.269 ISQ units. (Table 7)
The secondary stability linear regression model, assessed with the ISQ after three months (ISQ3), depended mainly on the location of the implant in the arch (incisor-canines, bicuspid-molars), the implant macro-design (cylindrical, conical), and the age of the patient (≤55, >55). According to the significant regression model (F=7.258; p<0.001), which only predicts 18.2% of the results of the measured ISQ3 values, the average ISQ after three months at the incisor-canine area, 76.67 ± 7.13, will increase by 1.35-6.66 units when the implant is placed more posteriorly (bicuspids and molars), and 0.11-5.21 units in older patients. If conical-shaped implants are used, ISQ3 will decrease by 1.375-6.660. (Table 7)
4. Discussion
Many factors can affect the success of implant therapy, but patient-related factors and implant-related factors are perhaps the two most important variables to consider [21, 22]. Achieving primary stability in implant surgery is one of the many desired outcomes for clinicians [23, 24], and it is reported to depend mainly on bone density and implant macro geometry [25]. Research relating to insertion torque and implant success is becoming increasingly frequent. Barone et al. [26], in a randomized clinical trial lasting 12 months, evaluated the influence of insertion torque and peri-implant bone stability. Their results showed that implants placed with a high insertion torque (≥ 50 Ncm) showed greater peri-implant bone remodeling and greater recession of the buccal soft tissues. Following this trend, Marconcini et al. [27] observed similar results in terms of bone resorption (less marginal bone loss and less facial soft tissue recession) and implant success. They obtained a success rate of 98.2% in implants placed at a regular insertion torque (<50 Ncm) and 91.3% in implants placed at a high insertion torque (≥50 Ncm).
The present study’s first overall correlation analysis – i.e., before the data was divided into implant macro-geometry groups – showed a significant association between the tactile evaluation of bone density during the preparation of the osteotomy and the insertion torque, ISQ on the day of the surgery, and bone-density values attained with the CBCT. However, when the correlation analysis was conducted for each group of implants, the conical-shaped implants had an inversed significant correlation with the insertion torque and the bone density, and the cylindrical-shaped implants only for the insertion torque, as mentioned earlier (Table 2). Several studies have analyzed the correlation between the surgeon’s tactile sensation and variables such as insertion torque, ISQ, and bone density values derived from CBCT [7, 28–30]. Fernandes Triches et al. [30] identified a moderate, negative association between insertion torque and the bone type selected through tactile evaluation. The present study found a negative association between insertion torque and tactile sensation for conical (rho=-0.403; P<0.001) and parallel implants (rho=-366; p=0.026). These differences may be influenced by the macro-geometry of the implants since no prior studies have been found comparing all these variables and implant macro-designs.
The present study significantly demonstrated that cylindrical implants provided higher primary stability values (insertion torque and ISQ values) than conical implants. In contrast, Waechter et al. [31] showed that conical and cylindrical implants of the same length but different diameters placed in the posterior region of the mandible produced similar results for primary stability. Likewise, authors such as Cochran et al. [32] and Sakoh et al. [33] found no significant differences between the primary stability of conical and cylindrical implants. However, some studies have recorded higher levels of primary stability for conical implants. [25, 34, 35]. Further, several of the studies mentioned above were in vitro [33], animal-model [31, 34], or retrospective clinical studies [7], and each study used different macro-designs (conical, cylindrical, and hybrid implants, with different thread designs and pitches, with or without micro-spirals in the coronal portion), which makes it challenging to draw any conclusions on this issue.
Another possible reason for the higher primary stability values for cylindrical implants was the type of surgical procedure performed during the osteotomy. Most clinicians perform some drilling strategy depending on the perceived bone quality to achieve adequate primary stability. Thread-forming drills might be used whenever implants are placed in hard bone (Lekholm and Zarb type I and II) and underdrill the implant bed whenever soft bone is felt (Lekholm and Zarb type III and IV). [36, 37]. However, new bone preparation techniques, such as Osseodensification, are emerging, with significant results compared to the conventional technique. [37, 38]
Another notable finding was that the significantly lower ISQ obtained at the moment of the surgery for the conical implants was maintained at the ISQ after three months, which may imply that the implant’s macro-geometry (thread design) may play a role in both primary and secondary stability.
Despite subjective tactile evaluation of bone quality assessed softer bone when placing the conical implants, such differences did not correspond with the objective bone density assessment, which may indicate that implant macro-geometry may play a role in the tactile perception during implant placement.
This study also explored other factors, such as implant location in the arch (incisors-canines, bicuspid-molars) and whether implants were placed in the maxilla or mandible. Our results show that the more posterior the implant location, the lower the bone density. The values for mean bone density according to implant location within the arch observed in the present study (Table 4) were similar to those reported by Fuster-Torres et al.[7] These authors obtained a mean value of 684 ± 131 HU in the anterior region and 568.5 ± 170 HU in the posterior region. Therefore, in line with the results reported by Turkyilmaz et al. [39] in 2007, the highest values for bone density (HU) are found in the anterior region, and the lowest values (HU) occur in the posterior region.
This study found no statistically significant differences between implants placed in the maxilla or mandible regarding primary stability, secondary stability, or bone density (Table 5), in contrast to other researchers [7, 28, 39]. This study also found that implant length (Table 7) did not significantly affect primary stability, secondary stability, or bone density. However, implant diameter was found to have significant effects (Table 6) on insertion torque and bone density variables. Wide-diameter implants achieved significantly lower insertion torque than implants with a standard diameter. There are likely to be two main reasons for these results. Firstly, most implants (63.6%) were placed in the maxilla, where bone density is expected to be lower (reduced HU). Secondly, all the wide implants were placed in the molar region, where the mean bone density was the lowest.
In contrast, Farronato et al. [40] reported that a wider implant diameter was associated with greater insertion torque. However, this was an in vitro study in which bone density would be difficult to control, given the challenge of reproducing human bone’s macroscopic and microscopic characteristics in models. In a clinical study using a similar methodology, Da Rocha Ferreira et al. [41] compared cylindrical (Nobel Parallel) and conical (Nobel Active) implants and found no significant differences relating to implant diameter and insertion torque (P=0.57). However, they did find that implant diameter had a significant effect (P=0.04) on ISQ on the day of the surgery. While the present research did not identify significant differences (P=0.162) related to implant diameter and ISQ on the day of the surgery, lower ISQ scores were achieved for wide implants compared to standard-diameter implants. These results support those presented by Da Rocha Ferreira et al. [40]. In the present research, a linear regression analysis showed that the implant macro-design, the length, and the insertion torque were the most influential ISQ at the moment of implant placement predictors. Location, implant macro-design, and age of the patients were the most significant predictors for the ISQ after three months of healing.
Moreover, this study showed that although some implant macro-designs are specifically designed to achieve high primary stability values on the day of the surgery, after 3 months of osseointegration, some implant designs achieved greater secondary stability (Table 2). Clinicians should know that the implant design, site, and diameter would modulate the primary and secondary stability of implants placed in healed sites. The secondary stability also depends on other surface conditions of the implants, such as surface topography or roughness. [42,43,44].
One limitation of the present study was the relatively small sample of wide-diameter implants (n=11), specifically for the cylindrical group, with only one implant. 4.5 diameter was the limit for considering an implant standard or wide. Cylindrical implants used in this study had a standard width of 4.3 mm, so most of the implants placed were considered standard in this study, but they were used in many cases as wide clinically.
5. Conclusions
Bearing the limitations mentioned above in mind, the present study enables us to establish that:
- On healed bone crests, higher values for primary stability (insertion torque and ISQ points) will be achieved with standard diameter implants (Ø≤4.5).
- After implant osseointegration (three months), cylindrical implants yielded higher ISQ values than conical implants. Further research is needed to assess factors that affect secondary stability.
- ISQ values after three months will be lower in implants placed in the incisor-canine region than those placed in the bicuspid-molar region.
- Insertion torque is the variable that most influences ISQ on the day of the surgery, and the implant location and macro-design in the arch have the most significant effect on ISQ after three months.
Author Contributions
Conceptualization, resources, N.Q.-L. and JM; methodology, N.Q.-L., JM, and S.M.-M.; software, S.M.-M.; validation N.Q.-L., M.I.S.-J., C.G.-P., O.F.-A, and J.F.-F.; writing—original draft preparation, N.Q.-L., O.F.-A, and JM; writing (review and editing), N.Q.-L., C.G.-P., J.F.-F., I.S.-B. and JM; data interpretation, C.G.-P., R.A.-O. and M.I.S.-J.; all statistical analyses, N.Q.-L., O.F.-A and JM All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the University of Salamanca (protocol code 473, Jun 22, 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The study was conducted within the Research Group “Avances en Salud Oral” (Advances in Oral Health) of the University of Salamanca. https://avancessaludoral.usal.es (accessed on Nov 23 2021).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| CBCT | Cone Beam Computed Tomography. |
| HU | Hounsfield Units. |
| DICOM | Digital Imaging and Communication in Medicine |
| IT | insertion torque |
| ISQ | implant stability quotient |
Appendix B
Figure 1.
CBCT image used for implant planning, and image of bone-density evaluation (in HU) using BTI Scan software. The purple bar chart shows the bone density inside the implant, and the green bar chart shows the bone density 0.5 mm outside the implant.
Figure 2.
Implant placement and measurement of implant stability quotient (ISQ).
Figure 3.
Bar chart representing medians of insertion torque (N*cm), implant stability quotient at the moment of the surgery, and after three months. Confidence intervals were set at p=0.05.
Figure 4.
Bar chart representing medians of implant stability quotient at the moment of the surgery according to macro-design and location. Confidence intervals were set at p=0.05.
Figure 5.
Bar chart representing medians of implant stability after three months according to macro-design and location. Confidence intervals were set at p=0.05.
References
- Gamborena, I.; Sasaki, Y.; Blatz, M.-B. Predictable immediate implant placement and restoration in the esthetic zone. J. Esthet. Restor. Dent. 2021, 33, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.-J.; Singh, M.; Weber, H.-P.; Gallucci, G.-O. Success criteria in implant dentistry: a systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Carosi, P.; Lorenzi, C.; Laureti, M.; Ferrigno, N.; Arcuri, C. Short Dental Implants (≤ 6 mm) to Rehabilitate Severe Mandibular Atrophy: A Systematic Review. Int. J. Oral. Maxillofac. Implants. 2021, 36, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.-M.; Scarfe, W.-C.; Vaughn, V.-M.; Jacobs, R. Cone beam computed tomography in implant dentistry: a systematic review focusing on guidelines, indications, and radiation dose risks. Int. J. Oral. Maxillofac. Implants. 2014, 29, 55–77. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.-M. Cone beam computed tomography in implant dentistry: recommendations for clinical use. BMC. Oral. Health. 2018; 18, 88. [Google Scholar] [CrossRef]
- Marquezan, M.; Osório, A.; Sant’Anna, E.; Souza, M.-M.; Maia, L. Does bone mineral density influence the primary stability of dental implants? A systematic review. Clin. Oral. Implants. Res. 2012, 23, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Fuster-Torres, M.-Á.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Relationships between bone density values from cone beam computed tomography, maximum insertion torque, and resonance frequency analysis at implant placement: a pilot study. Int. J. Oral. Maxillofac. Implants. 2011, 26, 1051–1056. [Google Scholar] [PubMed]
- Turkyilmaz, I.; Aksoy, U.; McGlumphy, E.-A. Two alternative surgical techniques for enhancing primary implant stability in the posterior maxilla: a clinical study including bone density, insertion torque, and resonance frequency analysis data. Clin. Implant. Dent. Relat. Res. 2008, 10, 231–237. [Google Scholar] [CrossRef]
- Ottoni, J.-M.; Oliveira, Z.-F.; Mansini, R.; Cabral, A.-M. Correlation between placement torque and survival of single-tooth implants. Int. J. Oral. Maxillofac. Implants. 2005, 20, 769–776. [Google Scholar]
- Lages, F.-S.; Douglas-de Oliveira, D.-W.; Costa, F.-O. Relationship between implant stability measurements obtained by insertion torque and resonance frequency analysis: A systematic review. Clin. Implant. Dent. Relat. Res. 2018, 20, 26–33. [Google Scholar] [CrossRef]
- Trisi, P.; Perfetti, G.; Baldoni, E.; Berardi, D.; Colagiovanni, M.; Scogna, G. Implant micromotion is related to peak insertion torque and bone density. Clin. Oral. Implants. Res. 2009, 20, 467–471. [Google Scholar] [CrossRef]
- Mikic, M.; Vlahovic, Z.; Stevanović, M.; Arsic, Z.; Mladenovic, R. The Importance of Correlation between CBCT Analysis of Bone Density and Primary Stability When Choosing the Design of Dental Implants-Ex Vivo Study. Tomography. 2022; 8, 1293–1306. [Google Scholar] [CrossRef]
- Falco, A.; Berardini, M.; Trisi, P. Correlation Between Implant Geometry, Implant Surface, Insertion Torque, and Primary Stability: In Vitro Biomechanical Analysis. Int. J. Oral. Maxillofac. Implants. 2018, 33, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Barone, S.; Attanasio, F.; Salviati, M.; Cerra, M.G.; Calabria, E.; Bennardo, F.; Giudice, A. Effect of Implant Macro-Design and Magnetodynamic Surgical Preparation on Primary Implant Stability: An In Vitro Investigation. Dent. J. 2023, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Pevida, E.; Cherro, R.; Camps-Font, O.; Piqué, N. Effects of Drilling Protocol and Bone Density on the Stability of Implants According to Different Macrogeometries of the Implant Used: Results of an In Vitro Study. Int. J. Oral. Maxillofac. Implants. 2020, 35, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Lekholm, U.; Zarb, G.-A. Patient selection and preparation. In: Brånemark P-I, Zarb GA, AlbrektssonT, eds. Tissue Integrated Prostheses. Osseointegration in Clinical Dentistry. Chicago, IL: Quintessence Publishing Co.; 1985, 199-209.
- Misch, C.-E. Density of bone: effect on surgical approach, and healing. In: Misch CE, ed. Contemporary Implant Dentistry. St. Louis: Mosby-Year Book, 1999; 371–384. [Google Scholar]
- Todisco, M.; Trisi, P. Bone mineral density and bone histomorphometry are statistically related. Int. J. Oral. Maxillofac. Implants. 2005, 20, 898–904. [Google Scholar] [PubMed]
- Sennerby, L.; Andersson, P.; Pagliani, L.; Giani, C.; Moretti, G.; Molinari, M.; Motroni, A. Evaluation of a Novel Cone Beam Computed Tomography Scanner for Bone Density Examinations in Preoperative 3D Reconstructions and Correlation with Primary Implant Stability. Clin. Implant. Dent. Relat. Res. 2015, 17, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.J.; Prihoda, T.J.; Mealey, B.L.; Lasho, D.J.; Noujeim, M.; Huynh-Ba, G. Evaluation of Healing at Molar Extraction Sites With and Without Ridge Preservation: A Randomized Controlled Clinical Trial. J. periodontol. 2017, 88, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.-R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors Influencing Early Dental Implant Failures. J. Dent. Res. 2016, 95, 995–1002. [Google Scholar] [CrossRef]
- Chatzopoulos, G.-S.; Wolff, L.-F. Retrospective analysis of 50, 333 implants on implant failure and associated patient-related factors [published online ahead of print, 2023 Jul 10]. J. Stomatol. Oral. Maxillofac. Surg. 2023, 101555. [Google Scholar] [CrossRef]
- Griggs, J.-A. Dental Implants. Dent. Clin. North. Am. 2017; 61, 857–871. [Google Scholar] [CrossRef]
- Heimes, D.; Becker, P.; Pabst, A. How does dental implant macrogeometry affect primary implant stability? A narrative review. Int. J. Implant. Dent. 2023, 9, 20. [Google Scholar] [CrossRef]
- Torroella-Saura, G.; Mareque-Bueno, J.; Cabratosa-Termes, J.; Hernández-Alfaro, F.; Ferrés-Padró, E.; Calvo-Guirado, J.-L. Effect of implant design in immediate loading. A randomized, controlled, split-mouth, prospective clinical trial. 2015; 26, 240–244. [Google Scholar] [CrossRef]
- Barone, A.; Alfonsi, F.; Derchi, G.; Tonelli, P.; Toti, P.; Marchionni, S.; Covani, U. The Effect of Insertion Torque on the Clinical Outcome of Single Implants: A Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2016, 18, 588–600. [Google Scholar] [CrossRef]
- Marconcini, S.; Giammarinaro, E.; Toti, P.; Alfonsi, F.; Covani, U.; Barone, A. Longitudinal analysis on the effect of insertion torque on delayed single implants: A 3-year randomized clinical study. Clin. Implant. Dent. Relat. Res. 2018, 20, 322–332. [Google Scholar] [CrossRef]
- Makary, C.; Rebaudi, A.; Mokbel, N.; Naaman, N. Peak insertion torque correlated to histologically and clinically evaluated bone density. Implant. Dent. 2011, 20, 182–191. [Google Scholar] [CrossRef]
- Aksoy, U.; Eratalay, K.; Tözüm, T.-F. The possible association among bone density values, resonance frequency measurements, tactile sense, and histomorphometric evaluations of dental implant osteotomy sites: a preliminary study. Implant. Dent. 2009, 18, 316–325. [Google Scholar] [CrossRef]
- Triches, D.-F.; Alonso, F.-R.; Mezzomo, L.-A. Relation between insertion torque and tactile, visual, and rescaled gray value measures of bone quality: a cross-sectional clinical study with short implants. Int. J. Implant. Dent. 2019, 5, 9. [Google Scholar] [CrossRef]
- Waechter, J.; Madruga, M.-M.; Carmo Filho, L.-C.-D.; Leite, F.-R.-M.; Schinestsck, A.-R.; Faot, F. Comparison between tapered and cylindrical implants in the posterior regions of the mandible: A prospective, randomized, split-mouth clinical trial focusing on implant stability changes during early healing. Clin. Implant. Dent. Relat. Res. 2017, 19, 733–741. [Google Scholar] [CrossRef]
- Cochran, D.; Stavropoulos, A.; Obrecht, M.; Pippenger, B.; Dard, M. A Comparison of Tapered and Nontapered Implants in the Minipig. Int. J. Oral. Maxillofac. Implants. 2016, 31, 1341–1347. [Google Scholar] [CrossRef]
- Sakoh, J.; Wahlmann, U.; Stender, E.; Nat, R.; Al-Nawas, B.; Wagner, W. Primary stability of a conical implant and a hybrid, cylindric screw-type implant in vitro. Int. J. Oral. Maxillofac. Implants. 2006, 21, 560–566. [Google Scholar]
- O’Sullivan, D.; Sennerby, L.; Meredith, N. Influence of implant taper on the primary and secondary stability of osseointegrated titanium implants. Clin. Oral. Implants. Res. 2004, 15, 474–480. [Google Scholar] [CrossRef]
- Toyoshima, T.; Wagner, W.; Klein, M.-O.; Stender, E.; Wieland, M.; Al-Nawas, B. Primary stability of a hybrid self-tapping implant compared to a cylindrical non-self-tapping implant with respect to drilling protocols in an ex vivo model. Clin. Implant. Dent. Relat. Res. 2011, 13, 71–78. [Google Scholar] [CrossRef]
- Stacchi, C.; Troiano, G.; Montaruli, G.; Mozzati, M.; Lamazza, L.; Antonelli, A.; Giudice, A.; Lombardi, T. . Changes in implant sability using different site preparation techniques: Osseodensification drills versus piezoelectric surgery. A multi-center prospective randomized controlled clinical trial. Clin. Implant. Dent. Relat. Res. 2023, 25, 133–140. [Google Scholar] [CrossRef]
- Althobaiti, A.K.; Ashour, A.W.; Halteet, F.A.; Alghamdi, S.I.; AboShetaih, M.M.; Al-Hayazi, A.M.; Saaduddin, A.M. A Comparative Assessment of Primary Implant Stability Using Osseodensification vs. Conventional Drilling Methods: A Systematic Review. Cureus. 2023, 15, e46841. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, N.; Perrotti, V.; Caponio, V.C.A.; Matsubara, V.H.; Patalwala, D.; Quaranta, A. Comparison of heat production and bone architecture changes in the implant site preparation with compressive osteotomes, osseodensification technique, piezoelectric devices, and standard drills: an ex vivo study on porcine ribs. Odontolog. 2023, 111, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Turkyilmaz, I.; Tumer, C.; Ozbek, E.-N.; Tözüm, T.-F. Relations between the bone density values from computerized tomography, and implant stability parameters: a clinical study of 230 regular platform implants. J. Clin. Periodontol. 2007, 34, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Farronato, D.; Manfredini, M.; Stocchero, M.; Caccia, M.; Azzi, L.; Farronato, M. Influence of Bone Quality, Drilling Protocol, Implant Diameter/Length on Primary Stability: An In Vitro Comparative Study on Insertion Torque and Resonance Frequency Analysis. J. Oral. Implantol. 2020, 46, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Da Rocha-Ferreira, J.-J.; Machado, L.-F.-M. Insertion Torque Value and Implant Stability Quotient: Separate Evaluation and Correlation for Different Clinical Parameters. Int. J. Oral. Maxillofac. Implants. 2022, 37, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Raghavendra, S.; Wood, M.-C.; Taylor, T.-D. Early wound healing around endosseous implants: a review of the literature. Int. J. Oral. Maxillofac. Implants. 2005, 20, 425–431. [Google Scholar]
- Gursoytrak, B.; Ataoglu, H. Use of resonance frequency analysis to evaluate the effects of surface properties on the stability of different implants. Clin Oral Implants Res. 2020, 31, 239–245. [Google Scholar] [CrossRef]
- Neugebauer, J.; Weinländer, M.; Lekovic, V.; von Berg, K.-H.; Zoeller, J.-E. Mechanical stability of immediately loaded implants with various surfaces and designs: a pilot study in dogs. Int. J. Oral. Maxillofac. Implants. 2009; 24, 1083–1092. [Google Scholar]
Figure 1.
CBCT image used for implant planning, and image of bone-density evaluation (in HU) using BTI Scan software. The purple bar chart shows the bone density inside the implant, and the green bar chart shows the bone density 0.5 mm outside the implant.
Figure 1.
CBCT image used for implant planning, and image of bone-density evaluation (in HU) using BTI Scan software. The purple bar chart shows the bone density inside the implant, and the green bar chart shows the bone density 0.5 mm outside the implant.
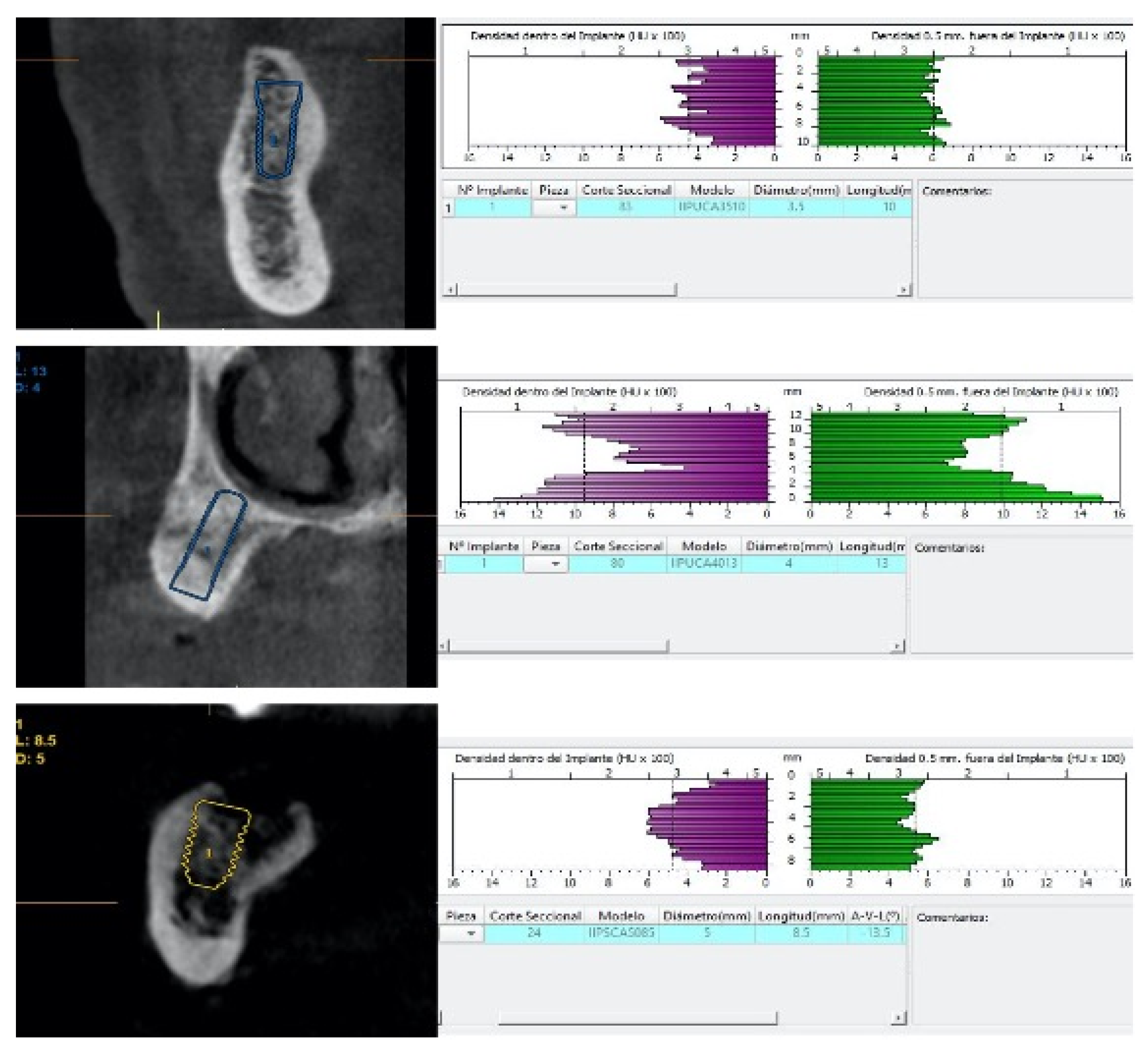
Figure 2.
Implant placement and measurement of implant stability quotient (ISQ).
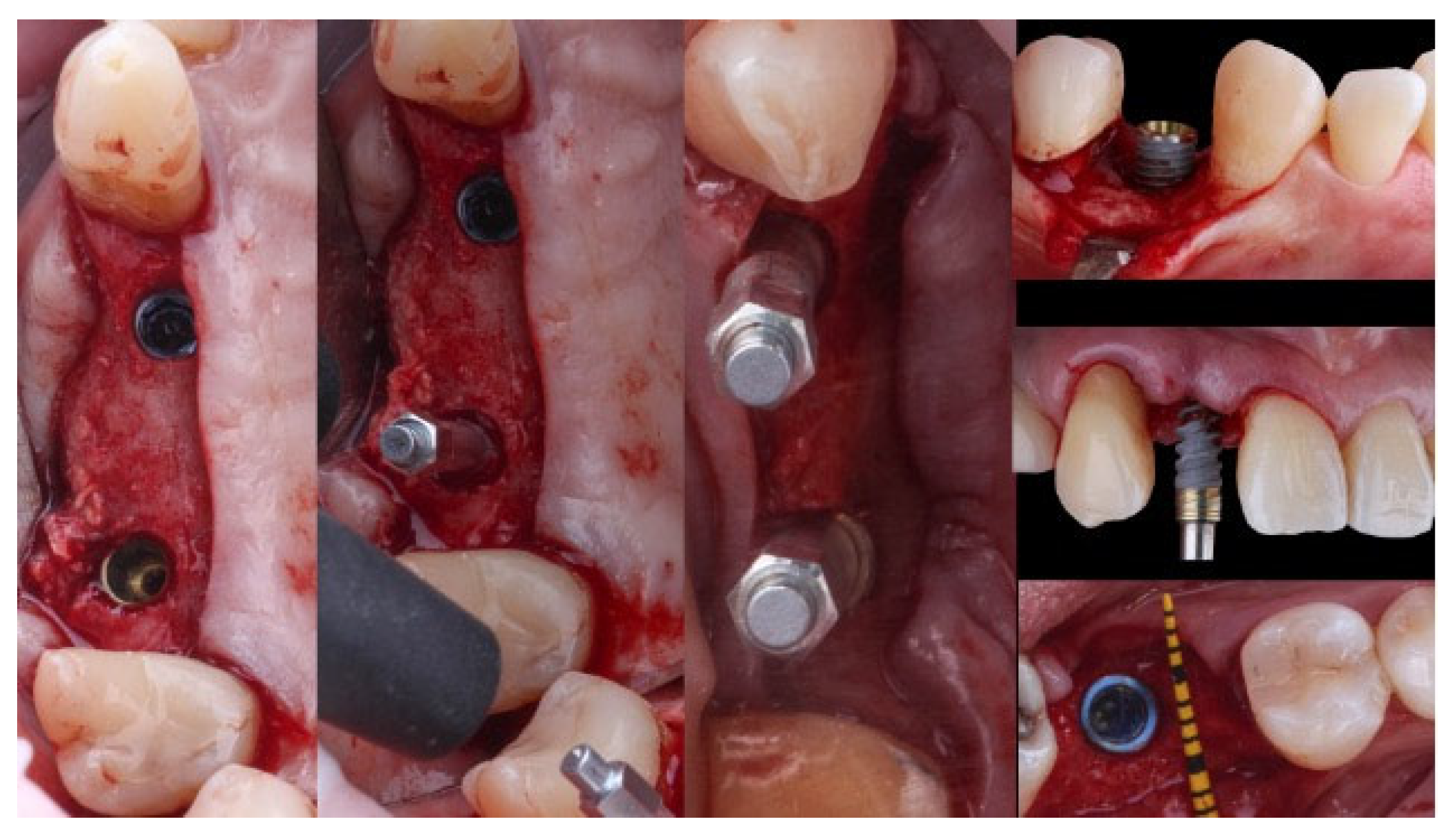
Figure 3.
Bar chart representing medians of insertion torque (N*cm), implant stability quotient at the moment of the surgery, and after three months depending on the implant macro design. Confidence intervals were set at p=0.05.
Figure 3.
Bar chart representing medians of insertion torque (N*cm), implant stability quotient at the moment of the surgery, and after three months depending on the implant macro design. Confidence intervals were set at p=0.05.
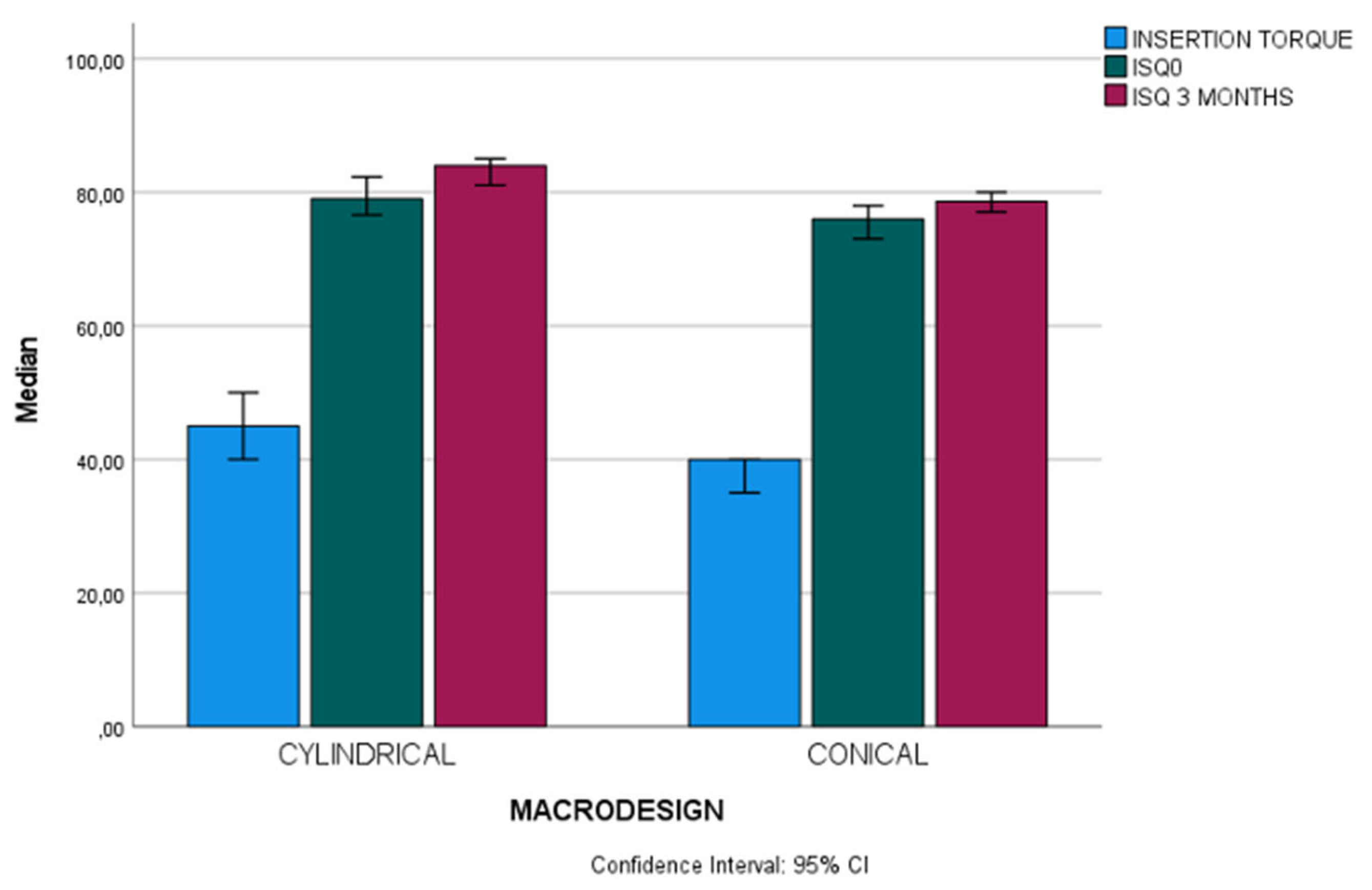
Figure 4.
Bar chart representing medians of implant stability quotient at the moment of the surgery according to macro-design and location. Confidence intervals were set at p=0.05.
Figure 4.
Bar chart representing medians of implant stability quotient at the moment of the surgery according to macro-design and location. Confidence intervals were set at p=0.05.
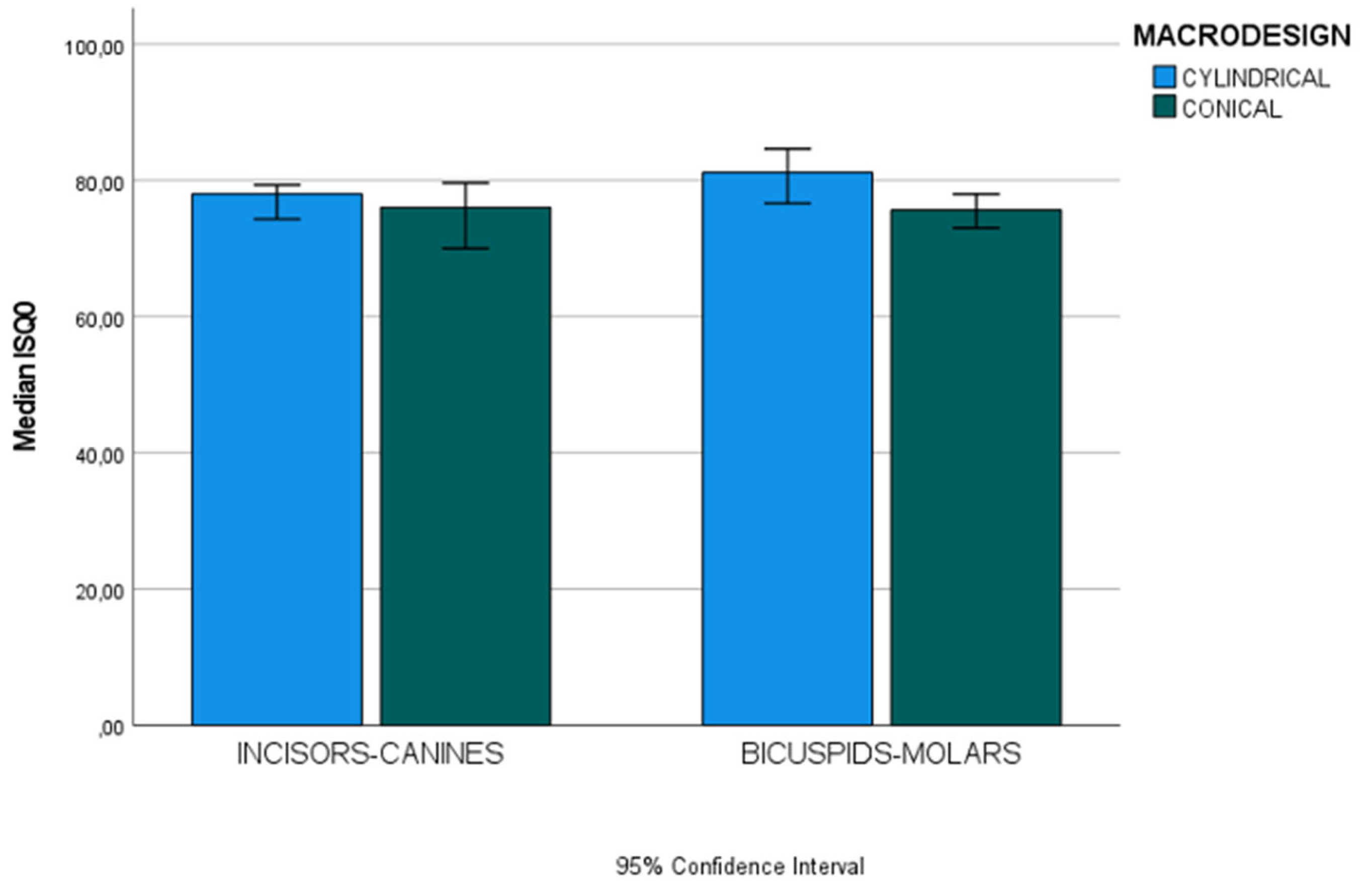
Figure 5.
Bar chart representing medians of implant stability after three months according to macro-design and location. Confidence intervals were set at p=0.05.
Figure 5.
Bar chart representing medians of implant stability after three months according to macro-design and location. Confidence intervals were set at p=0.05.
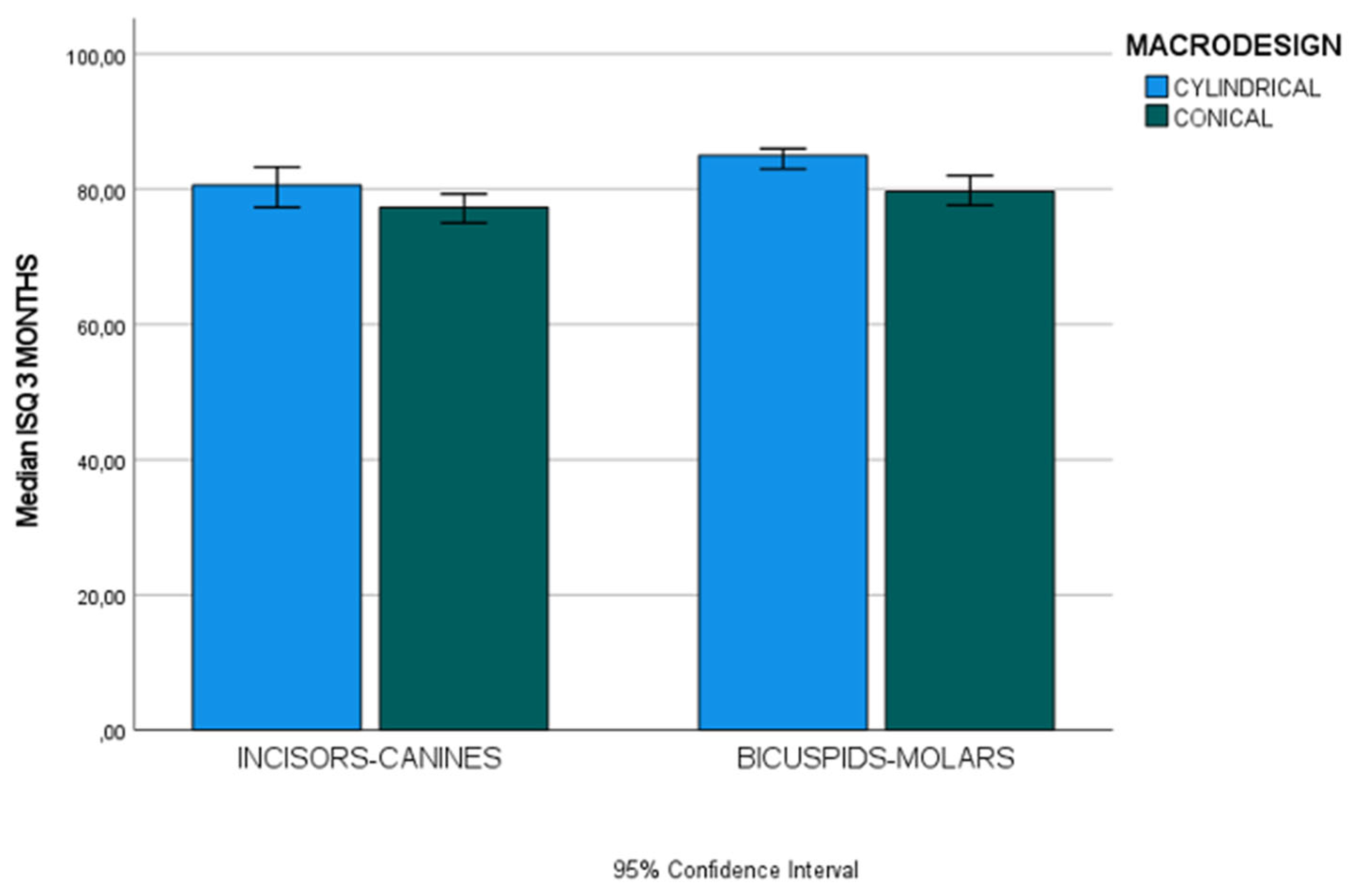

Table 1.
Baseline demographic and clinical data of patients and implants (n=53 patients, n=102 implants).
Table 1.
Baseline demographic and clinical data of patients and implants (n=53 patients, n=102 implants).
| Patient Related-Variables (n=53) | Groups | n (%) | |||
| Gender | Women | 22 (41.1%) | |||
| Men | 31 (58, 5%) | ||||
| Age (years) | ≤ 55 years | 27 (50.9%) | |||
| >55 years | 26 (49.1%) | ||||
| Average age in years (mean ± sd) | 56.6 ±10.1 | ||||
| Dental Arch | Mandible | 43 (42.2%) | |||
| Maxilla | 59 (57.8%) | ||||
| Implant location in the arch | Incisors-Canines | 36 (35.3%) | |||
| Bicuspids-Molars | 66 (64.7%) | ||||
| Implant-Related Variables (n=102) | |||||
| IMPLANT MACRO-DESIGN | Conical | Cylindrical | |||
| VARIABLES | n | % | n | % | |
| Macrogeometry design | 65 | 63.7% | 37 | 36.3% | |
| Location in the arch | Incisors-Canines | 21 | 20.59% | 15 | 14.70% |
| Bicuspids-Molars | 44 | 43.14% | 22 | 21.57% | |
| Implant Diameter | Standard (<4.5 mm) | 55 | 53.92% | 36 | 35.29% |
| Wide (≥4.5 mm) | 10 | 9.80% | 1 | 0.98% | |
| Implant Length | Standard (≤10 mm) | 30 | 29.41% | 18 | 17.65% |
| Long (>10 mm) | 35 | 34.31% | 19 | 18.63% | |
Table 2.
Pearson or Spearman correlation coefficient (r) between the patient-related and intraoperative variables of stability and bone density in the two types of macro geometries implants (n=102 implants).
Table 2.
Pearson or Spearman correlation coefficient (r) between the patient-related and intraoperative variables of stability and bone density in the two types of macro geometries implants (n=102 implants).
| Groups (n) ESTIMATIONS OF INITIAL STABILITY |
Insertion Torque (Ncm) |
ISQ Day of Surgery (ISQ units) |
ISQ 3 Months (ISQ units) |
Tactile evaluation of bone quality (D1-D4 Range) |
Bone Density (HU) |
||||||||
| Rho- r- |
p- value | Rho- r- |
p-value | Rho- r- |
p-value | Rho- r- |
p-value | Rho- r- |
p-value | ||||
| Insertion Torque (Ncm) |
Cylindrical (n=37) | 1 | 0.214 | 0.203 | 0.033 | 0.845 | -0.366 | 0.026 | -0.036 | 0.832 | |||
| Conical (n=65) | 1 | 0.554 | <0.001* | 0.237 | 0.057 | -0.403 | <0.001* | 0.358 | 0.003* | ||||
| Total (n=102) | 1 | 0.497 | <0.001* | 0.258 | 0.009* | -0.425 | <0.001* | 0.294 | 0.003* | ||||
| ISQ Day of Surgery (ISQ units) |
Cylindrical (n=37) | 0.214 | 0.203 | 1 | 0.429 | 0.008* | 0.132 | 0.438 | -0.245 | 0.144 | |||
| Conical (n=65) | 0.554 | <0.001* | 1 | 0.310 | 0.012 | -0.236 | 0.059 | -0.030 | 0.812 | ||||
| Total (n=102) | 0.497 | <0.001* | 1 | 0.417 | <0.001* | 0.245 | 0.013* | -0.038 | 0.705 | ||||
| ISQ 3 Months (ISQ units) |
Cylindrical (n=37) | 0.033 | 0.845 | 0.429 | 0.008* | 1 | 0.076 | 0.656 | -0.332 | 0.045* | |||
| Conical (n=65) | 0.237 | 0.057 | 0.310 | 0.012* | 1 | -0.041 | 0.745 | -0.016 | 0.902 | ||||
| Total (n=102) | 0.258 | 0.009* | 0.417 | <0.001* | 1 | -0.035 | 0.728 | -0.068 | 0.496 | ||||
| Tactile evaluation of bone quality (D1-D4 Range) |
Cylindrical (n=37) | -0.366 | 0.026* | -0.132 | 0.438 | 0.076 | 0.656 | 1 | 0.062 | 0.716 | |||
| Conical (n=65) | -0.403 | <0.001* | -0.236 | 0.059 | 0.041 | 0.745 | 1 | -0.373 | 0.002* | ||||
| Total (n=102) | -0.425 | <0.001* | -0.245 | 0.013* | -0.035 | 0.728 | 1 | 0.273 | 0.005* | ||||
| Bone Density (HU) |
Cylindrical (n=37) | -0.036 | 0.832 | -0.245 | 0.144 | -0.332 | 0.045* | 0.062 | 0.716 | 1 | |||
| Conical (n=65) | 0.358 | 0.003* | -0.030 | 0.812 | -0.016 | 0.902 | -0.373 | 0.002* | 1 | ||||
| Total (n=102) | 0.294 | 0.003* | -0.038 | 0.705 | -0.068 | 0.496 | -0.273 | 0.005 | 1 | ||||
* Statistically significant differences after Spearman or Pearson coefficient. Coefficients above r=0.40 are highlighted in light grey.
Table 3.
Student-t test (t-test), Mann-Whitney test (U M-W test), or Pearson’s Chi-Square test between the patient-related and intraoperative variables of stability and bone density in the three types of implants (n=102 implants).
Table 3.
Student-t test (t-test), Mann-Whitney test (U M-W test), or Pearson’s Chi-Square test between the patient-related and intraoperative variables of stability and bone density in the three types of implants (n=102 implants).
| Groups (n) ESTIMATIONS OF INITIAL STABILITY |
Mean ± sd Median (IR) n (%) |
Range | U T CHI2 |
p-value | |
| Insertion Torque (Ncm) |
Cylindrical (n=37) | 45 (10) | 20-55 | U 748 | 0.001* |
| Conical (n=65) | 40 (15) | 15-70 | |||
| Total (n=102) | 40 (15) | 15-70 | |||
| ISQ Day of Surgery (ISQ units) |
Cylindrical (n=37) | 79 (8, 95) | 61, 60-88 | U 766.50 | 0.002* |
| Conical (n=65) | 76 (10.35) | 44.60-83 | |||
| Total (n=102) | 77.5 (8.40) | 44.60-83 | |||
| ISQ 3 Months (ISQ units) |
Cylindrical (n=37) | 84 (6.65) | 53.30-89 | U 689.50 | <0.001* |
| Conical (n=65) | 78.60 (6.65) | 55.30-86.60 | |||
| Total (n=102) | 80 (7.95) | 53.30-89 | |||
| Tactile evaluation of bone quality (D1-D4 Range) |
Cylindrical (n=37) | 36 (35.29%) | CHI2 22.2 | 0.001* | |
| Conical (n=65) | 66 (64, 71%) | ||||
| Total (n=102) | 102 (100%) | ||||
| Bone Density (HU) |
Cylindrical (n=37) | 696.62±158.95 | 375-950 | T 1.481 | 0.142 |
| Conical (n=65) | 642.50±205.94 | 225-1100 | |||
| Total (n=102) | 662.13±191.21 | 225-1100 |
* Statistically significant differences after t-test, M-W, or Pearson’s CHI square tests (P < .05).
Table 4.
Effect of the implant location in the arch (incisors-canines, bicuspids-) on the patient-related and intraoperative variables of stability and bone density, according to Student’s t-test, M-W non-parametric test or Pearson’s Chi-Square test (n=102 implants).
Table 4.
Effect of the implant location in the arch (incisors-canines, bicuspids-) on the patient-related and intraoperative variables of stability and bone density, according to Student’s t-test, M-W non-parametric test or Pearson’s Chi-Square test (n=102 implants).
| Groups (n) | Cylindrical Mean±sd Median (IR) n(%) |
Conical Mean±sd Median (IR) n(%) |
U t CHI2 |
p-value | |
| Insertion Torque (Ncm) |
Incisors-Canine (n=36) | 45(5) | 40 (15) | U 99.50 | 0.058 |
| Bicuspids-Molars (n=66) | 45 (11.5) | 35 (15) | U 303 | 0.013* | |
| U (p-value) | 130 (0.267) | 340.5 (0.085) | |||
| ISQ Day of Surgery (ISQ units) |
Incisors-Canine (n=36) | 78 (23.40) | 76 (9.95) | U 136.50 | 0.500 |
| Bicuspids-Molars (n=66) | 81.15 (8.50) | 75.65 (11.90) | U 240.50 | <0.001* | |
| U (p-value) | 108 (0.08) | 452.50 (0.894) | |||
| ISQ 3 Months (ISQ units) |
Incisors-Canine (n=36) | 80.60 (6) | 77.30 (4.85) | U 105 | 0.092 |
| Bicuspids-Molars (n=66) | 85 (3) | 79.65 (6.92) | U 215 | <0.001* | |
| U (p-value) | 68.50 (0.002*) | 330.50 (0.065) | |||
| Tactile evaluation of bone quality (D1-D4 Range) |
Incisors-Canine (n=36) | 15 (14.70%) | 21 (20.59%) | CHI2 2.176 | 0.537 |
| Bicuspids-Molars (n=66) | 22 (21.57%) | 44 (20.59%) | CHI2 7.986 | 0.092 | |
| CHI2 (p-value) | 2.256 (0.689) | 4.340 (0.362) | |||
| Bone Density (HU) |
Incisors-Canine (n=36) | 782.50±124.89 | 775.59±170.59 | t 0.133 | 0.895 |
| Bicuspids-Molars (n=66) | 638.06±155.09 | 578.98±191.85 | t 1.253 | 0.215 | |
| t (p-value) | 3.00 (0.005*) | 3.99 (<0.001*) |
Table 5.
Effect of the arch (maxilla or mandible) on the patient-related and intraoperative variables of stability and bone density, according to the Student’s t-test, Mann-Whitney’s non-parametric test, or Pearson CHI square test (n=102 implants).
Table 5.
Effect of the arch (maxilla or mandible) on the patient-related and intraoperative variables of stability and bone density, according to the Student’s t-test, Mann-Whitney’s non-parametric test, or Pearson CHI square test (n=102 implants).
| Groups (n) | Cylindrical Mean±sd Median (IR) n(%) |
Conical Mean±sd Median (IR) n(%) |
U t CHI2 |
p-value | |
| Insertion Torque (Ncm) |
Maxilla (n=59) | 45 (11.25) | 35 (12.50) | U 215.5 | 0.010* |
| Mandible (n=43) | 50 (10) | 42.50 (20) | U 157 | 0.078 | |
| U (p-value) | 144 (0.401) | 427.5 (0.375) | |||
| ISQ Day of Surgery (ISQ units) |
Maxilla (n=59) | 80.80 (7.28) | 73.30 (11.15) | U 131 | <0.001* |
| Mandible (n=43) | 77 (7) | 78.50 (17.40) | U 215 | 0.759 | |
| U (p-value) | 101.50 (0.34) | 286 (0.005*) | |||
| ISQ 3 Months (ISQ units) |
Maxilla (n=59) | 85 (7.78) | 77.60 (5.65) | U 202.50 | 0.006* |
| Mandible (n=43) | 83 (6.60) | 79.50 (8.97) | U 153 | 0.066 | |
| U (p-value) | 161 (0.760) | 399 (0.206) | |||
| Tactile evaluation of bone quality (D1-D4 Range) |
Maxilla (n=59) | 18 (17.64%) | 41 (40.20%) | CHI2 4.450 | 0.349 |
| Mandible (n=43) | 19 (18.63%) | 24 (23.53%) | CHI2 9.855 | 0.079 | |
| CHI2 (p-value) | 2.835 (0.586) | 3.057 (0.547) | |||
| Bone Density (HU) |
Maxilla (n=59) | 709.03±148.08 | 594.21±185.95 | t 2.314 | 0.024* |
| Mandible (n=43) | 684.87±171.82 | 725±215.91 | t 2.869 | 0.512 | |
| t (p-value) | 0.457 (0.651) | -2.578 (0.012*) |
Table 6.
Effect of implant diameter on the patient-related and intraoperative variables of stability and bone density, according to the Student’s t-test, Mann-Whitney’s non-parametric test, or Pearson CHI square test (n=102 implants).
Table 6.
Effect of implant diameter on the patient-related and intraoperative variables of stability and bone density, according to the Student’s t-test, Mann-Whitney’s non-parametric test, or Pearson CHI square test (n=102 implants).
| Groups (n) | Cylindrical Mean±sd Median (IR) n(%) |
Conical Mean±sd Median (IR) n(%) |
U t CHI2 |
p-value | |
| Insertion Torque (Ncm) |
Standard (<4.5 Ø;)(n=91) |
45 (10) | 40 (10) | U 665, 50 | 0.008* |
| Wide (≥4.5 Ø;)(n=11) |
35 | 27.5 (18.75) | |||
| U (p-value) | 126.5 (0.006*) | ||||
| ISQ Day of Surgery (ISQ units) |
Standard (<4.5 Ø;)(n=91) |
78.80 (8.92) | 76.3 (8.10) | U 667 | 0.009* |
| Wide (≥4.5 Ø;)(n=11) |
82.30 | 68.95 (15.20) | |||
| U (p-value) | 264 (0.841) | ||||
| ISQ 3 Months (ISQ units) |
Standard (<4.5 Ø;)(n=91) |
84(5.90) | 79 (6) | U 537.50 | <0.001* |
| Wide (≥4.5 Ø;)(n=11) |
77.00 | 76.80 (9.17) | |||
| U (p-value) | 264 (0.841) | ||||
| Tactile evaluation of bone quality (D1-D4 Range) |
Standard (<4.5 Ø;)(n=91) |
36 (35.29%) | 55 (53.92%) | CHI2 6, 046 | 0.196 |
| Wide (≥4.5 Ø;)(n=11) |
1 (0.98%) | 10 (9.80%) | |||
| CHI2 (p-value) | 20.93 (<0.001*) | ||||
| Bone Density (HU) |
Standard (<4.5 Ø;)(n=91) |
697.57±161.10 | 677.27±195.49 | t 0.518 | 0.606 |
| Wide (≥4.5 Ø;)(n=11) |
662.50 | 451.25±155.73 | |||
| t (p-value) | 3.454 (<0.001*) |
Table 7.
Effect of implant length on the patient-related and intraoperative variables of stability and bone density, according to the Student’s t-test, Mann-Whitney’s non-parametric test, or Pearson CHI square test (n=102 implants).
Table 7.
Effect of implant length on the patient-related and intraoperative variables of stability and bone density, according to the Student’s t-test, Mann-Whitney’s non-parametric test, or Pearson CHI square test (n=102 implants).
| Groups (n) | Cylindrical Mean±sd Median (IR) n(%) |
Conical Mean±sd Median (IR) n(%) |
U t CHI2 |
p-value | |
| Insertion Torque (Ncm) |
Standard (≤10 mm)(n=48) |
47.50 (11.25) | 37.50 (20) | U 154.50 | 0.13 |
| Long (>10 mm)(n=54) |
45 (10) | 40 (15) | U 218.50 | 0.036* | |
| U (p-value) | 169 (0.950) | 441.50 (0.266) | |||
| ISQ Day of Surgery (ISQ units) |
Standard (≤10 mm)(n=48) |
78 (11.85) | 73.80 (38.40) | U 182 | 0.061 |
| Long (>10 mm)(n=54) |
79 (9) | 77 (25) | U 194.50 | 0.012* | |
| U (p-value) | 132 (0.235) | 412.50 (0.138) | |||
| ISQ 3 Months (ISQ units) |
Standard (≤10 mm)(n=48) |
84.50 (5.10) | 78.80 (9) | U 151.50 | 0.012* |
| Long (>10 mm)(n=54) |
81.30 (7) | 78.60 (5.30) | U 201.50 | 0.018* | |
| U (p-value) | 130.50 (0.216) | 500.50 (0.747) | |||
| Tactile evaluation of bone quality (D1-D4 Range) |
Standard (≤10 mm)(n=48) |
18 (17.65%) | 30 (29.41%) | CHI2 9.719 | 0.021* |
| Long (>10 mm)(n=54) |
19 (18.63%) | 35 (34.31%) | CHI2 2.746 | 0.601 | |
| CHI2 (p-value) | 2.835 (0.586) | 8.954 (0.062) | |||
| Bone Density (HU) |
Standard (≤10 mm)(n=48) |
663.19±166.58 | 645.83±217.66 | t 0.291 | 0.773 |
| Long (>10 mm)(n=54) |
728.29±148.83 | 639.64±198.51 | t 1.852 | 0.070 | |
| t (p-value) | -1.255 (0.218) | 0.120 (0.905) |
Table 8.
Linear regression model between the stability and bone-density variables.
| Dependent Variables | Independent Variables | β | Error | p-value | Lower CI 95% |
Upper CI 95% |
|
| Primary Stability | |||||||
| ISQ day of the surgeryA | Macrodesign | -0.200 | 1.410 | 0.028 | -5.948 | -0.350 | |
| Length | 0.175 | 1.315 | 0.046 | 0.049 | 5.269 | ||
| Insertion Torque | 0.387 | 0.064 | <0.001 | 0.147 | 0.400 | ||
| Secondary Stability | |||||||
| ISQ 3 monthsB | Location | 0.274 | 1.338 | 0.003 | 1.349 | 6.660 | |
| Macrodesign | -0.277 | 1.333 | 0.003 | -6.667 | -1.375 | ||
| Age | 0.190 | 1.284 | 0.041 | 0.112 | 5.208 | ||
A: Coefficient of determination R2=0.278 F=12.589; P<0.001, B: Coefficient of determination R2=0.182 F=7.258; P<0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



