
Submitted:
13 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
Background: Fingertip injuries with volar pulp tissue defects are challenging to manage due to the complex anatomy and critical role of the fingertip in sensory and motor functions. Traditional surgical approaches are associated with donor site morbidity, prolonged immobilization, and suboptimal functional outcomes. This study aimed to evaluate the efficacy of a conservative treatment protocol using artificial dermis and semi-occlusive dressing for these injuries.
Methods: A single-center, prospective study was conducted on 31 patients with fingertip injuries involving volar pulp defects. The treatment protocol involved wound debridement, application of artificial dermis (Pelnac®), and semi-occlusive dressing (IV3000®). Outcomes were assessed using subjective questionnaires and objective measures, including fingerprint regeneration, sensory function, pain, and cosmetic appearance. The impact of injury characteristics on outcomes and treatment duration was evaluated. Complications were recorded, and patient satisfaction was assessed.
Results: The mean treatment duration was 45.29 days (SD=17.53), with no significant differences based on injury characteristics. Complications were minimal, with only one case (3.22%) directly attributable to the treatment. Fingerprint regeneration was considerable (mean score=2.58, SD=0.67), with slightly better scores in bone-exposed injuries. Sensory disturbances were minimal, with no significant differences across injury types. Post-treatment pain was low (mean=0.45, SD=0.67), and cosmetic satisfaction was high (mean=4.09, SD=0.94). Overall patient satisfaction was high (mean=4.41, SD=0.67), regardless of injury severity.
Discussion: This study demonstrates the efficacy of a conservative approach using artificial dermis and semi-occlusive dressing for fingertip injuries with volar pulp defects. The treatment protocol achieved favorable outcomes in tissue regeneration, sensory recovery, pain management, and cosmetic appearance while minimizing complications and morbidity associated with traditional surgical interventions. The high patient satisfaction across all injury types highlights the patient-centered nature of this approach.
Conclusions: The conservative treatment protocol using artificial dermis and semi-occlusive dressing is a promising strategy for managing fingertip injuries with volar pulp defects. This approach harnesses the body's regenerative potential, minimizes surgical morbidity, and achieves excellent functional and aesthetic outcomes. Further research is needed to optimize treatment protocols and investigate long-term outcomes.
Keywords:
Artificial dermis
; Fingertip
; Fingerprint
; Pelnac
; Reconstruction
; Regeneration
; Semi-occlusive
; Volar
1. Introduction
Fingertip injuries, particularly those involving volar pulp tissue defects, present a significant challenge in hand surgery due to the complex anatomy and the critical role of the fingertip in sensory and motor functions [1]. The volar pulp, with its rich neurovascular network and specialized sensory receptors, is essential for fine touch sensation, grip stability, and precise manipulation [2]. Injuries to this region can lead to significant functional impairment, sensory disturbances, and cosmetic disfigurement, ultimately impacting the patient's quality of life [3].
Traditional surgical approaches for the management of fingertip injuries with volar pulp defects include local flaps, skin grafts, and free tissue transfers [4]. While these techniques aim to restore the soft tissue envelope and preserve finger length, they are associated with several drawbacks, such as donor site morbidity, prolonged immobilization, and the need for multiple surgeries [5]. Moreover, these surgical interventions may not adequately restore the intricate sensory and biomechanical properties of the native pulp tissue, leading to suboptimal functional outcomes [6].
In recent years, there has been a growing interest in conservative treatment approaches that harness the body's inherent regenerative potential to promote the regeneration of functional pulp tissue [7]. The use of artificial dermal substitutes, such as Pelnac® (Gunze Limited, Kyoto, Japan), has shown promising results in the management of various soft tissue defects, including burns, chronic wounds, and traumatic injuries [8,9]. These biomaterials provide a three-dimensional scaffold that mimics the natural extracellular matrix, facilitating cell migration, proliferation, and differentiation [10]. When combined with a semi-occlusive dressing, such as IV3000® (Smith & Nephew, Hull, UK), which maintains a moist wound environment and allows for gas exchange, artificial dermal substitutes have the potential to promote the regeneration of vascularized and innervated pulp tissue [11].
Despite the increasing utilization of artificial dermal substitutes in clinical practice, there is limited evidence regarding their efficacy in the management of fingertip injuries with volar pulp defects. Previous studies have primarily focused on the use of artificial dermis for the coverage of fingertip amputations or dorsal skin defects [10,12,13]. Moreover, the optimal treatment protocol, the impact of injury characteristics on outcomes, and the long-term functional and aesthetic results remain poorly understood.
To address these knowledge gaps, we conducted a prospective study to evaluate the efficacy of a conservative treatment protocol employing artificial dermis (Pelnac®) and a semi-occlusive dressing (IV3000®) in the management of fingertip injuries with volar pulp tissue defects. We hypothesized that this approach would promote the regeneration of functional pulp tissue, minimize complications, and achieve high patient satisfaction, while avoiding the morbidity associated with traditional surgical interventions.
The primary objectives of this study were to:
- I.
- Assess the regeneration of volar pulp tissue, including the restoration of fingerprint pattern, sensory function, and cosmetic appearance.
- II.
- Evaluate the impact of injury characteristics, such as bone or tendon exposure, on treatment outcomes and duration.
- III.
- Investigate the incidence of complications and patient-reported outcomes, including pain, sensory disturbances, and overall satisfaction.
- IV.
- Compare the treatment duration and outcomes with those reported in previous studies utilizing artificial dermis for fingertip reconstruction.
By providing a comprehensive evaluation of this conservative treatment approach, we aim to contribute to the growing body of evidence supporting the use of artificial dermal substitutes in the management of challenging fingertip injuries. The insights gained from this study may inform clinical decision-making, guide future research efforts, and ultimately lead to the development of novel, patient-centered treatment strategies that optimize functional and aesthetic outcomes while minimizing the burden of surgical intervention.
2. Materials and Methods
A single-center, prospective study was conducted at our institution, which was approved by the Institutional Review Board (IRB) of the Catholic Kwandong University International St. Mary's Hospital (Approval No. 19연IRB069, Registration No. IS19EISE0072). The study was performed in strict adherence to ethical guidelines. The study period was from December 2019 to December 2022, focusing on patients presenting with volar pulp tissue defects of the fingertip (Figure 1).
To ensure robust statistical power, a power analysis was conducted prior to patient recruitment. The analysis determined that a minimum of 30 patients was necessary to adequately power the study, assuming an alpha of 0.05, a power of 0.80, and an effect size of 0.5. This sample size was chosen to ensure that the study results would be statistically significant and replicable in similar clinical settings. Written informed consent was obtained from all participants involved in this study.
Inclusion Criteria:
Patients were eligible for the study if they:
- Presented with Volar Pulp Tissue Defects: Exclusively patients with volar pulp tissue defects were considered, excluding those with isolated nail bed defects to ensure a homogeneous patient population for relevant clinical evaluations.
- Consented and Understood the Study Procedures: This study included only patients who provided informed consent after receiving a detailed explanation of the study procedures. This explanation emphasized the potentially extended treatment duration compared to traditional flap surgeries, the avoidance of prolonged hospitalization, and the reduced surgical morbidity. The study population consisted of patients who expressed a preference for less invasive treatments, as they wished to avoid surgeries that might require inpatient stays and could be associated with donor site morbidity. These patients prioritized a rapid return to daily life after undergoing a simple procedure, even if it meant a slightly longer overall treatment duration.
- Were Unsuitable for Immediate Replantation: Inclusion extended to patients exhibiting signs such as a ribbon sign, making them unsuitable for immediate replantation but ideal candidates for alternative therapeutic strategies explored in this study.
Exclusion Criteria:
Patients were excluded if they required immediate surgical interventions such as flap surgery or replantation, had a history of previous surgery or injury to the affected finger, or had any underlying conditions that could impair wound healing. This exclusion ensured that the study outcomes were not confounded by factors that traditionally affect wound healing and recovery.
Treatment Protocol
All patients underwent wound debridement, irrigation, and hemostasis under digital nerve block in the operating room. The artificial dermis (Pelnac®, Gunze Limited, Kyoto, Japan), a bilayer membrane composed of an outer silicone layer and an inner collagen sponge layer with a thickness of 3 mm, was soaked in saline, trimmed to cover the defect, and secured with 4-0 nylon sutures (Figure 2). A semi-occlusive dressing (IV3000®, Smith & Nephew, UK), a transparent, waterproof, and breathable polyurethane film dressing, was then applied over the artificial dermis. For patients with excessive oozing, the dressing was changed the following day at the outpatient clinic. In other cases, the first dressing change was performed five days post-operation.
During dressing changes, the finger was soaked in saline for 15 minutes to minimize damage to the Pelnac® during IV3000® removal. The wound and surrounding area were gently irrigated with saline to prevent infection, and a new IV3000® dressing was applied. This process was repeated at five-day intervals until complete epithelialization was achieved, which was defined as the complete coverage of the wound with epithelial tissue without any remaining raw surface. The duration from the initial application of the artificial dermis to complete wound healing was recorded.
Outcome Measures
After complete wound healing, patients were asked to complete a subjective questionnaire assessing the following outcomes:
- I.
- Cosmetic satisfaction: rated on a scale from 1 to 5, with higher scores indicating greater satisfaction with the appearance of the treated finger.
- II.
- Sensory impairment: rated on a scale from 0 to 5, with lower scores indicating less sensory loss.
- III.
- Sensory hypersensitivity: rated on a scale from 0 to 5, with lower scores indicating less discomfort or abnormal sensations.
- IV.
- Pain: assessed using a visual analog scale (VAS) ranging from 0 to 5, with lower scores indicating less or no pain.
- V.
- Overall satisfaction: rated on a scale from 1 to 5, with higher scores indicating greater satisfaction with all aspects of the treatment and recovery process.
To objectively evaluate the pulp tissue reconstruction, the degree of fingerprint regeneration was assessed on a scale from 0 to 3, with higher scores indicating better regeneration. The outcome assessments were performed by two independent, trained assessors who were blinded to the patients' treatment allocation. The assessors underwent a calibration exercise to ensure consistency and reliability in their evaluations.
Complications, including hook nail deformity and onychomycosis, were recorded throughout the study period. The outcome assessments and follow-up visits were conducted at 1, 3, and 6 months post-treatment.
Statistical Analysis
The Shapiro-Wilk test was employed to verify the normality of the data distribution. Treatment duration, which followed a normal distribution, was described using means and standard deviations and analyzed using independent samples t-tests to compare:
- I.
- Patients with and without bone exposure.
- II.
- Patients with and without tendon exposure.
- III.
- Patients with both bone and tendon exposure versus those with neither.
Non-normally distributed variables, including fingerprint regeneration scores, cosmetic satisfaction, sensory impairment, sensory hypersensitivity, pain, and overall satisfaction, were described using medians and interquartile ranges. These variables were compared using the Mann-Whitney U test, a non-parametric test, across different patient groups:
- I.
- Patients with versus without bone exposure.
- II.
- Patients with versus without tendon exposure.
- III.
- Patients with both bone and tendon exposure versus those with neither.
Statistical significance was established at a p-value of less than 0.05. All statistical analyses were performed using IBM SPSS Statistics 29.0.2.0 (IBM Corp., Armonk, NY, USA).
3. Results
3.1. Participant Demographics and Injury Characteristics
A total of 31 patients with fingertip injuries were included in this study, conducted between January 2017 and December 2021. The study cohort consisted of 25 males (80.6%) and 6 females (19.4%), with a mean age of 43.29 years (range, 18-72 years). The distribution of the affected fingers was as follows: thumb (n=3, 8.57%), index finger (n=13, 37.14%), middle finger (n=6, 17.14%), ring finger (n=8, 22.85%), and little finger (n=5, 14.28%). Three patients had injuries on two fingers, resulting in a total of 35 injured fingers. The baseline characteristics of the participants, including comorbidities and risk factors, are presented in Table 1.
Key finding: The study population was predominantly male, and the index finger was the most commonly injured.
3.2. Treatment Protocol and Healing Duration
Among the 31 patients, 9 (29.03%) had soft tissue injuries without bone exposure, while 22 (70.97%) had injuries with bone exposure (Figure 3). The mean treatment duration for all patients was 45.29 days (SD=17.53)
Subgroup analyses revealed no statistically significant differences in treatment duration:
- A.
- Bone exposure: 44.11 days (SD=10.48) without exposure vs. 45.77 days (SD=19.91) with exposure (p=0.131)
- B.
- Tendon exposure: 41.71 days (SD=15.67) without exposure vs. 52.80 days (SD=19.65) with exposure (p=0.512)
- C.
- Combined exposure: 43.63 (SD=11.09) with no exposure at all vs. 53.33 days (SD=20.76) with both bone and tendon exposure (p=0.143)
Key finding: The mean treatment duration was 45.29 days (SD=17.53), with no significant differences based on bone or tendon exposure, although cases with tendon exposure required a slightly longer treatment duration compared to those with bone exposure.
3.3. Complications and Clinical Outcomes
Complications were reported in 9 patients (29.03%), including hook nail deformity (n=6, 19.35%), scar contracture (n=1, 3.22%), onychomycosis (n=1, 3.22%), and nail splitting (n=1, 3.22%). However, after excluding hook nail deformity (a consequence of shortened bone), scar contracture (inevitable due to lesion location), and onychomycosis (presumed to be pre-existing), only one complication (3.22%) of nail splitting (Figure 4) was suspected to be directly related to the treatment (Table 2).
Key finding: The treatment demonstrated a low complication rate, with only one case (3.22%) of nail splitting directly attributable to the procedures used in this study.
3.4. Fingerprint Regeneration
The mean fingerprint regeneration score was 2.58 (SD=0.67) on a scale from 0 to 3, suggesting significant restoration of the fingerprint pattern in most patients.
Subgroup analyses revealed no statistically significant differences in fingerprint regeneration scores:
- A.
- Bone exposure: 2.44 (SD=0.88) without exposure vs. 2.63 (SD=0.58) with exposure (p=0.781) (Figure 5)
- B.
- Tendon exposure: 2.57 (SD=0.67) without exposure vs. 2.60 (SD=0.69) with exposure (p=0.917)
- C.
- Combined exposure: 2.37 (SD=0.91) with no exposure at all vs. 2.55 (SD=0.72) with both bone and tendon exposure (p=0.815)
Interestingly, cases with either tendon or bone exposure showed slightly better fingerprint regeneration scores compared to those without exposure, with the best results observed in cases with bone exposure but without tendon exposure (mean score=2.69).
Key finding: Fingerprint regeneration was considerable (mean score=2.58, SD=0.67) across all patients, with no statistically significant differences based on bone or tendon exposure. Notably, cases with bone exposure demonstrated slightly better regeneration scores compared to those without exposure, although this difference was not statistically significant.
3.5. Sensory Assessment
3.5.1. Hypoesthesia
The mean hypoesthesia score for all 31 patients was 0.09 (SD=0.39), indicating minimal sensory deficits.
Subgroup analyses revealed no statistically significant differences in hypoesthesia scores:
- A.
- Bone exposure: 0.22 (SD=0.66) without exposure vs. 0.04 (SD=0.21) with exposure
- B.
- Tendon exposure: 0.09 (SD=0.43) without exposure vs. 0.10 (SD=0.31) with exposure
- C.
- Combined exposure: 0.25 (SD=0.70) with no exposure at all vs. 0.11 (SD=0.33) with both bone and tendon exposure (p=0.963)
Key finding: Hypoesthesia was minimal (mean=0.09, SD=0.39), with no significant differences across various injury types, suggesting the treatment's effectiveness in preserving sensory function regardless of the presence of bone or tendon exposure.
3.5.2. Hyperesthesia
The mean hyperesthesia score for all 31 patients was 0.25 (SD=0.57), indicating minimal sensory disturbances.
Subgroup analyses revealed no statistically significant differences in hyperesthesia scores:
- A.
- Bone exposure: 0.11 (SD=0.33) without exposure vs. 0.31 (SD=0.64) with exposure
- B.
- Tendon exposure: 0.28 (SD=0.64) without exposure vs. 0.20 (SD=0.42) with exposure
- C.
- Combined exposure: 0.12 (SD=0.35) with no exposure at all vs. 0.22 (SD=0.44) with both bone and tendon exposure (p=0.743)
Key finding: Hyperesthesia was minimal (mean=0.25, SD=0.57), with no significant differences across various injury types, suggesting the treatment's effectiveness in maintaining normal sensory function regardless of the presence of bone or tendon exposure.
3.6. Pain Assessment
The mean pain score for all 31 patients was 0.45 (SD=0.67), indicating minimal post-treatment pain. Pain was assessed using a visual analog scale (VAS) ranging from 0 to 5, with lower scores representing less or no pain.
Subgroup analyses revealed no statistically significant differences in pain scores:
- A.
- Bone exposure: 0.44 (SD=0.52) without exposure vs. 0.45 (SD=0.73) with exposure (p=0.781)
- B.
- Tendon exposure: 0.38 (SD=0.58) without exposure vs. 0.60 (SD=0.84) with exposure (p=0.633)
- C.
- Combined exposure: 0.37 (SD=0.51) with neither bone nor tendon exposure vs. 0.55 (SD=0.88) with both exposures (p=0.743)
Key finding: Post-treatment pain was minimal (mean=0.45, SD=0.67), with no significant differences across various injury types, suggesting the treatment's effectiveness in pain management regardless of the presence of bone or tendon exposure.
3.7. Cosmetic Assessment
The mean cosmetic satisfaction score for all 31 patients was 4.09 (SD=0.94), indicating high satisfaction with the cosmetic outcomes.
Subgroup analyses revealed no statistically significant differences in cosmetic satisfaction scores:
- A.
- Bone exposure: 4.22 (SD=0.97) without exposure vs. 4.04 (SD=0.95) with exposure (p=0.654)
- B.
- Tendon exposure: 4.14 (SD=0.91) without exposure vs. 4.00 (SD=1.05) with exposure (p=0.787)
- C.
- Combined exposure: 4.12 (SD=0.99) with neither bone nor tendon exposure vs. 3.88 (SD=1.05) with both exposures (p=0.673)
Key finding: Cosmetic satisfaction was high (mean=4.09, SD=0.94), with no significant differences across various injury types, suggesting the treatment's effectiveness in achieving satisfactory cosmetic outcomes regardless of the presence of bone or tendon exposure.
3.8. Overall Satisfaction
The mean overall satisfaction score for all 31 patients was 4.41 (SD=0.67), indicating high satisfaction with the treatment outcomes.
Subgroup analyses revealed no statistically significant differences in satisfaction scores:
- A.
- Bone exposure: 4.66 (SD=0.70) without exposure vs. 4.31 (SD=0.64) with exposure (p=0.174)
- B.
- Tendon exposure: 4.47 (SD=0.67) without exposure vs. 4.30 (SD=0.67) with exposure (p=0.492)
- C.
- Combined exposure: 4.62 (SD=0.74) with neither bone nor tendon exposure vs. 4.22 (SD=0.66) with both exposures (p=0.236)
Key finding: Overall treatment satisfaction was high (mean=4.41, SD=0.67), with no significant differences across various injury types, suggesting the treatment's effectiveness regardless of the presence of bone or tendon exposure (Table 3).
3.9. Statistical Analysis
The Shapiro-Wilk test was used to assess the normality of the data. Only the treatment duration followed a normal distribution. Therefore, independent samples t-tests were used for the analysis of treatment duration, while non-parametric Mann-Whitney U tests were used for the other variables.
It is important to note that not all tests yielded statistically significant results. Some comparisons between groups did not reach the predetermined significance level (p < 0.05), indicating that the observed differences could be due to chance. However, the use of appropriate statistical tests based on the data distribution ensures the validity of the analyses and helps to minimize the risk of Type I errors (false positives).
The interpretation of non-significant results should be done cautiously, considering factors such as sample size, effect size, and clinical relevance. The absence of statistical significance does not necessarily imply a lack of clinical importance. This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
4. Discussion
This prospective study provides compelling evidence for the efficacy of a conservative treatment protocol employing artificial dermis (Pelnac®) and semi-occlusive dressing (IV3000®) in the management of fingertip injuries with volar pulp tissue defects. The findings underscore the potential of this approach to achieve favorable clinical outcomes while minimizing surgical morbidity and hospitalization, paving the way for a paradigm shift in the treatment of these challenging injuries.
One of the most striking findings of this study is the consistently high overall satisfaction scores across all injury types and exposure groups, underscoring the treatment protocol's ability to meet patient expectations and achieve favorable outcomes, regardless of the injury's severity or complexity. This can be attributed to the minimally invasive nature of the treatment, which avoids the morbidity and potential complications associated with traditional surgical interventions, while still providing adequate functional and cosmetic outcomes [14]. Furthermore, the conservative approach aligns with the growing emphasis on patient-centered care, prioritizing patient comfort, autonomy, and quality of life considerations in the treatment decision-making process [15].
The study cohort exhibited substantial fingerprint regeneration, a crucial aspect of functional and aesthetic restoration. Interestingly, patients with bone-exposed injuries demonstrated slightly better fingerprint regeneration scores compared to those without bone exposure. This phenomenon could be attributed to the complex interplay between the injury microenvironment and the body's inherent regenerative mechanisms. When the bone is exposed, the periosteum and bone marrow cells, which possess inherent regenerative capabilities, can contribute to the formation of new tissue [16]. Additionally, the inflammatory response triggered by bone exposure may stimulate the recruitment of mesenchymal stem cells and the release of growth factors, further enhancing the regenerative process [16]. The artificial dermis likely serves as a conducive scaffold, facilitating cell migration, proliferation, and differentiation, ultimately promoting the organized regeneration of the pulp tissue architecture [17,18].
The intriguing dichotomy observed in the sensory assessments, with the bone-exposed injury group experiencing less sensory loss (hypoesthesia) but higher levels of hypersensitivity (hyperesthesia), warrants further exploration. This observation may be elucidated by the complex interplay between nerve regeneration, scar tissue formation, and the depth of the injury. While bone exposure may facilitate better nerve regeneration and preservation of sensory function by providing a conducive environment for axonal growth and guidance [19], it may also increase the risk of hypersensitivity due to the exposure of deeper nerve structures and the formation of neuroma or entrapment neuropathies [20]. Additionally, the regeneration of nerve fibers may not necessarily follow the original anatomical pathways, leading to aberrant connections and altered sensory perception [20]. Further research is needed to elucidate the molecular and cellular mechanisms underlying this phenomenon, which could potentially inform novel therapeutic strategies to optimize sensory recovery.
The consistently low pain levels across all subgroups suggest that the treatment protocol effectively managed pain, regardless of the injury severity or location. This could be attributed to the anti-inflammatory properties of the artificial dermis, which may modulate the inflammatory microenvironment and reduce nociceptor activation [21]. Furthermore, the protective barrier provided by the semi-occlusive dressing may have minimized further tissue damage and nociceptor stimulation, contributing to effective pain management [22].
The high overall cosmetic satisfaction, even in patients with bone-exposed injuries, highlights the treatment protocol's ability to achieve favorable aesthetic outcomes. This could be attributed to the natural regeneration of the pulp tissue and the minimization of scar formation, as the artificial dermis serves as a scaffold for cell migration and tissue ingrowth, promoting a more organized and physiological healing process [10]. Additionally, the semi-occlusive dressing may have facilitated a moist wound healing environment, reducing the risk of excessive scarring and promoting better cosmetic outcomes [23].
A notable difference between the current study and previous studies utilizing artificial dermis for fingertip reconstruction is the treatment duration (Table 4). In the present study, the mean treatment duration was 45.29 days (SD=17.53), which is slightly longer than 34.0 ± 4.9 days reported by Namgoong et al. [24]. Interestingly, Wang et al. [25] also used Pelnac® for fingertip defects with bone exposure, but their treatment duration was shorter, ranging from 28 to 42 days. This difference in treatment duration may be attributed to the unique combination of the artificial dermis (Pelnac®) and the semi-occlusive dressing (IV3000®) used in this study, which likely influences the complex regenerative processes occurring within the wound bed.
The semi-occlusive dressing used in this study helps maintain a moist wound environment, which is crucial for the optimal function of the artificial dermis scaffold and the regenerative processes taking place within the wound [23,26]. This moist environment may slow down the initial stages of wound healing, such as inflammation and proliferation, as the artificial dermis gradually integrates into the wound bed and supports the growth of new tissue [27]. As a result, the use of a semi-occlusive dressing in conjunction with the artificial dermis may prolong the treatment duration compared to using artificial dermis alone.
However, the prolonged treatment duration may be counterbalanced by the potential for improved quality of the regenerated pulp tissue. The combination of artificial dermis and semi-occlusive dressing creates a favorable environment for the regeneration of a well-vascularized and innervated pulp, which may result in better long-term functional and aesthetic outcomes compared to wounds treated with artificial dermis alone. The semi-occlusive dressing helps maintain the optimal moisture balance required for the artificial dermis to function as a scaffold, promoting the organized growth of blood vessels, nerves, and soft tissue [28].
In essence, the slightly longer treatment duration observed in the current study may be a trade-off for the potential benefits of using a semi-occlusive dressing with the artificial dermis. This combination may create an environment more conducive to the regeneration of a pulp structure closely resembling the original fingertip tissue. Further research is needed to elucidate the specific mechanisms by which semi-occlusive dressings influence the regenerative process in the presence of an artificial dermis and to optimize their use in fingertip reconstruction.
The unique properties of the artificial dermis and semi-occlusive dressing, particularly the IV3000, play a crucial role in the wound healing process by maintaining a moist environment that is essential for tissue regeneration. However, the permeability characteristics of IV3000 are pivotal, as they must balance moisture retention with adequate gas exchange and exudate management. Inadequate permeability can lead to excessive fluid loss or exudate accumulation, which may hinder healing and extend the treatment duration.
This consideration brings to light the importance of evaluating and optimizing the properties of wound dressings in the context of fingertip injuries. Comparative studies focusing on different dermal substitutes and dressing materials are needed to identify the most effective combinations that minimize treatment time while maximizing regenerative outcomes.
Furthermore, the potential of combining artificial dermal substitutes with regenerative therapies like growth factors or stem cell treatments should be explored in large-scale, randomized controlled trials. These studies could provide insights into the synergistic effects of these combinations, enhancing the overall effectiveness of conservative treatment protocols.
Despite its promising results, this study's limitations. First, the absence of a control group prevents a direct comparison between our conservative treatment protocol and traditional surgical methods, which could provide more definitive conclusions about relative efficacy and outcomes. This design limitation could influence the robustness of the findings and their applicability in broader clinical practice. Secondly, the relatively short follow-up period limits our ability to assess long-term outcomes such as durability of the regenerated tissue, recurrence of complications, and long-term functional and sensory recovery. Longer-term follow-up would provide more comprehensive data on the stability and effectiveness of the treatment over time. Lastly, it is important to acknowledge that while the treatment protocol was effective in promoting tissue regeneration and improving functional outcomes, it did not facilitate elongation of bone in cases with bone-exposed injuries. This aspect remains a significant challenge and underscores the need for treatment strategies that can also address bone loss to provide a more holistic approach to fingertip reconstruction.
These limitations suggest that while the study contributes valuable insights into the conservative management of fingertip injuries, further research with more rigorous experimental designs, including control groups and extended follow-up periods, is necessary to enhance the evidence base supporting the use of artificial dermis and semi-occlusive dressing in this context. including its single-center design and small sample size, must be acknowledged. These factors limit the generalizability of the findings and underscore the need for more extensive research to verify the long-term effects and efficacy of this treatment approach comprehensively.
5. Conclusions
This study tested the hypothesis that a conservative treatment protocol using artificial dermis (Pelnac®) combined with a semi-occlusive dressing (IV3000®) could effectively manage fingertip injuries with volar pulp defects. The findings confirm that this treatment approach significantly enhances tissue regeneration, sensory function, and cosmetic outcomes, while reducing the morbidity associated with traditional surgical interventions.
Author Contributions
Conceptualization, D Kang.; methodology, D Kang; formal analysis, D Kang; investigation, D Kang; resources, D Kang; data curation, D Kang; writing—original draft preparation, D Kang; writing—review and editing, D Kang; visualization, D Kang; supervision, D Kang; All authors have read and agreed to the published version of the manuscript. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
This single-center, prospective study was approved by the Institutional Review Board of the Catholic Kwandong University International St. Mary's Hospital (IRB No. 19연IRB069, Registration No. IS19EISE0072). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are not publicly available due to privacy and ethical restrictions, as the research involves sensitive patient information.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Zeng, Q. Reverse Homodigital Artery Island Flap With Palmar Cutaneous Branches of the Proper Digital Nerve for Repairing of Finger Pulp Defect and Sensory Reconstruction: Is It Deserving? Annals of Plastic Surgery 2023, 91, 789. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.-C.; Wen, C.; Wang, Z. Volar Neurovascular Advancement Flap With an All Neural Branch–preserving Technique. Techniques in Hand & Upper Extremity Surgery 2021, 25, 63–68. [Google Scholar]
- Ryang, S.-R.; Jang, M.-G.; Kuk-Chol Kim, S.-G. Clinical Study on Reconstruction of Soft Tissue Defects of the Digits by Volar Flaps. Journal of Orthopaedics and Sports Medicine 2020, 2, 10–17. [Google Scholar] [CrossRef]
- Faderani, R.; et al. The free Thenar flap for thumb pulp reconstruction: A case report. Microsurgery 2023, 43, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Martin-Playa, P.; Foo, A. Approach to fingertip injuries. Clinics in plastic surgery 2019, 46, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; et al. Reconstruction of Finger Pulp Defects. In Atlas of Finger Reconstruction: Techniques and Cases; Springer Nature Singapore: Singapore, 2023; pp. 225–244. [Google Scholar]
- Balagué, N.; L'Huillier, A.G. Regenerative healing ability of the digit tip. Journal of the American Academy of Dermatology 2023, 88, e185–e186. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; et al. Clinical application of artificial dermis and autologous skin in repairing skin and soft tissue defects of hands and feet with bone exposure injuries. Evidence-based Complementary and Alternative Medicine: eCAM, 2021. 2021.
- Kashimura, T.; et al. Selection of artificial dermis for shortening treatment period: Integra versus Pelnac. Plastic and Reconstructive Surgery–Global Open 2021, 9, e3599. [Google Scholar] [CrossRef] [PubMed]
- Salih, A.M.; Mustafa, S.O. The Use of Acellular Dermal Matrix for the Closure of Skin Defects. AMJ (Advanced Medical Journal) 2023, 8, 94–101. [Google Scholar] [CrossRef]
- Cheang, C.J.Y.; et al. IV3000 semi-occlusive dressing use in simple and complex fingertip injuries: efficacy and affordability. Journal of Wound Care 2022, 31, 340–347. [Google Scholar] [CrossRef]
- Wang, J.; et al. Long-term follow-up of one-stage artificial dermis reconstruction surgery for fingertip defects with exposed phalanx. Hand Surgery and Rehabilitation 2022, 41, 353–361. [Google Scholar] [CrossRef]
- Namgoong, S.; et al. Potential of tissue-engineered and artificial dermis grafts for fingertip reconstruction. Plastic and Reconstructive Surgery 2020, 146, 1082–1095. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, W.A.; et al. Which factors are associated with satisfaction with treatment results in patients with hand and wrist conditions? A large cohort analysis. Clinical Orthopaedics and Related Research® 2022, 480, 1287–1301. [Google Scholar] [PubMed]
- Hutchison, A.-M.; et al. Functional outcome and patient satisfaction with a ‘self-care’protocol for minimally displaced distal radius fractures: a service evaluation. Bone & Joint Open 2022, 3, 726–732. [Google Scholar]
- Zhu, J.; Xiong, J.; Ji, W. A systematic review of bone marrow stromal cells and periosteum-derived cells for bone regeneration. Tissue Engineering Part B: Reviews 2023, 29, 103–122. [Google Scholar] [CrossRef] [PubMed]
- Lou, X.; et al. One-stage Pelnac Reconstruction in Full-thickness Skin Defects with Bone or Tendon Exposure. Plast Reconstr Surg Glob Open 2018, 6, e1709. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, A.M.; Al-Chalabi, M.M.M.; Sulaiman, W.A.W. Integra: An Alternative Option for Reconstruction of Extensive Finger Defects With Exposed Bones. Cureus 2021, 13, e16223. [Google Scholar] [CrossRef] [PubMed]
- Neto, E.; et al. Sensory neurons sprouting is dependent on osteoclast-derived extracellular vesicles involving the activation of epidermal growth factor receptors. BioRxiv 2018, 259218. [Google Scholar]
- Leitão, L.; et al. Osteoblasts are inherently programmed to repel sensory innervation. Bone research 2020, 8, 20. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.Z.; et al. The clinical application effects of artificial dermis scaffold and autologous split-thickness skin composite grafts combined with vacuum-assisted closure in refractory wounds. International Wound Journal 2023, 20, 2113–2120. [Google Scholar] [CrossRef]
- Pastor, T.; et al. Semi-occlusive dressing therapy versus surgical treatment in fingertip amputation injuries: a clinical study. European Journal of Trauma and Emergency Surgery 2023, 49, 1441–1447. [Google Scholar] [CrossRef]
- Schultz, J.; et al. Semi-occlusive management of fingertip injuries with finger caps: A randomized controlled trial in children and adults. Medicine 2022, 101, e29324. [Google Scholar] [CrossRef] [PubMed]
- Namgoong, S.; et al. Potential of Tissue-Engineered and Artificial Dermis Grafts for Fingertip Reconstruction. Plast Reconstr Surg 2020, 146, 1082–1095. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; et al. Long-term follow-up of one-stage artificial dermis reconstruction surgery for fingertip defects with exposed phalanx. Hand Surg Rehabil 2022, 41, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Hoigne, D.; et al. Semi-occlusive dressing for the treatment of fingertip amputations with exposed bone: quantity and quality of soft-tissue regeneration. J Hand Surg Eur Vol 2014, 39, 505–9. [Google Scholar] [CrossRef] [PubMed]
- Junker, J.P.; et al. Clinical impact upon wound healing and inflammation in moist, wet, and dry environments. Advances in wound care 2013, 2, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Hubert, J.; et al. Prospective Outcomes of Semi-occlusive Dressings Versus Non-occlusive Dressings Over Donor Sites for Split Thickness Skin Grafting. Plastic and Reconstructive Surgery–Global Open 2022, 10, 152. [Google Scholar] [CrossRef]
Figure 1.
The flow diagram of the study.
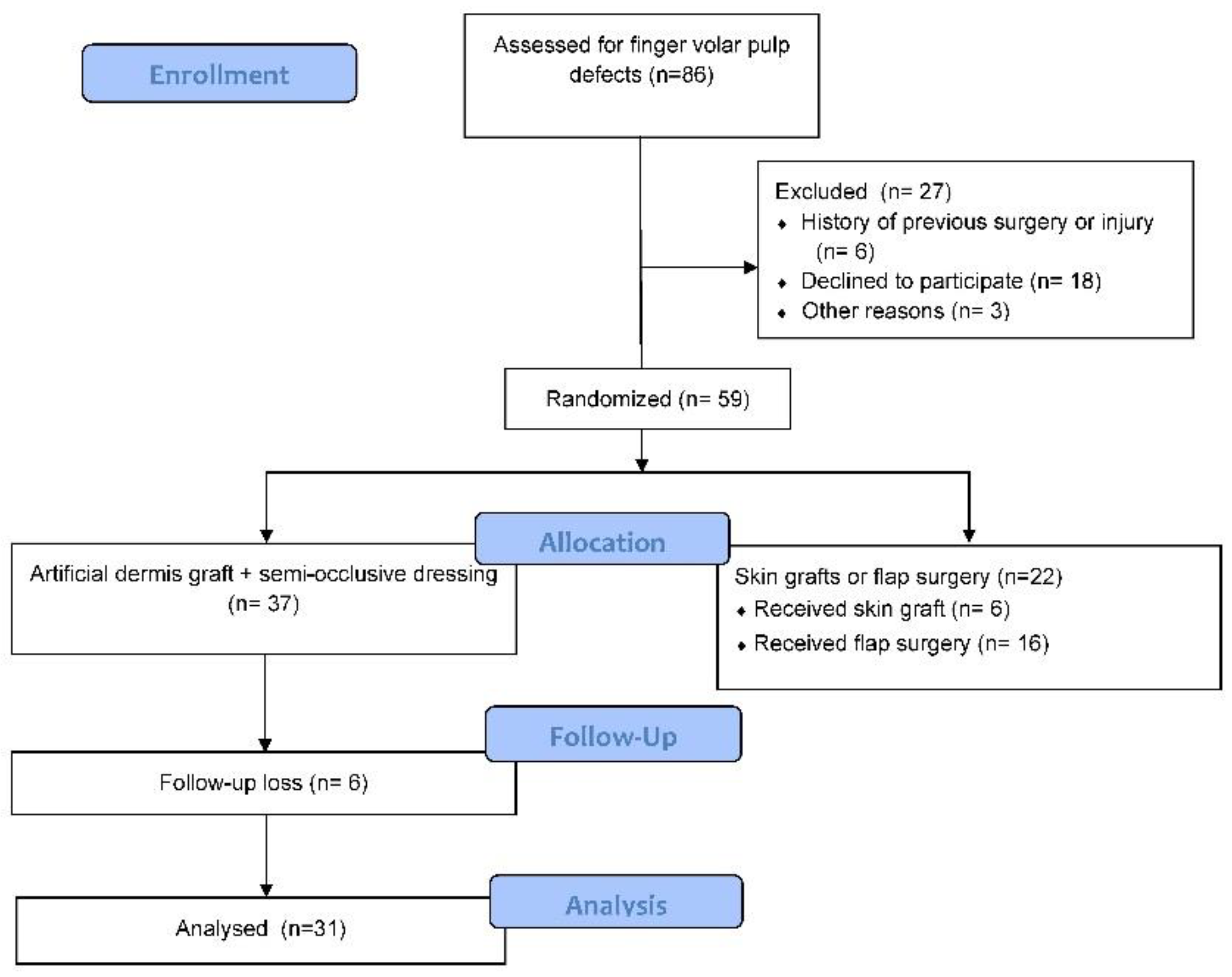
Figure 2.
Application of artificial dermis and semi-occlusive dressing for fingertip injury. (A) Preoperative view of a middle finger pulp injury. (B) Intraoperative view showing the application of artificial dermis (Pelnac®) to the defect, followed by a semi-occlusive dressing (IV3000®).
Figure 2.
Application of artificial dermis and semi-occlusive dressing for fingertip injury. (A) Preoperative view of a middle finger pulp injury. (B) Intraoperative view showing the application of artificial dermis (Pelnac®) to the defect, followed by a semi-occlusive dressing (IV3000®).

Figure 3.
Treatment progression and outcomes following artificial dermis application and semi-occlusive dressing for a fingertip injury. (A) Preoperative view of the right index fingertip injury with distal phalanx and soft tissue defect. (B) Immediate postoperative view after debridement and application of artificial dermis. (C) Five weeks post-treatment, showing the regeneration of pulp tissue and early restoration of the fingerprint pattern under the semi-occlusive dressing. (D) Seven weeks post-treatment, demonstrating complete wound healing with well-formed fingerprint ridges, restored sensation, minimal pain, and satisfactory cosmetic appearance.
Figure 3.
Treatment progression and outcomes following artificial dermis application and semi-occlusive dressing for a fingertip injury. (A) Preoperative view of the right index fingertip injury with distal phalanx and soft tissue defect. (B) Immediate postoperative view after debridement and application of artificial dermis. (C) Five weeks post-treatment, showing the regeneration of pulp tissue and early restoration of the fingerprint pattern under the semi-occlusive dressing. (D) Seven weeks post-treatment, demonstrating complete wound healing with well-formed fingerprint ridges, restored sensation, minimal pain, and satisfactory cosmetic appearance.
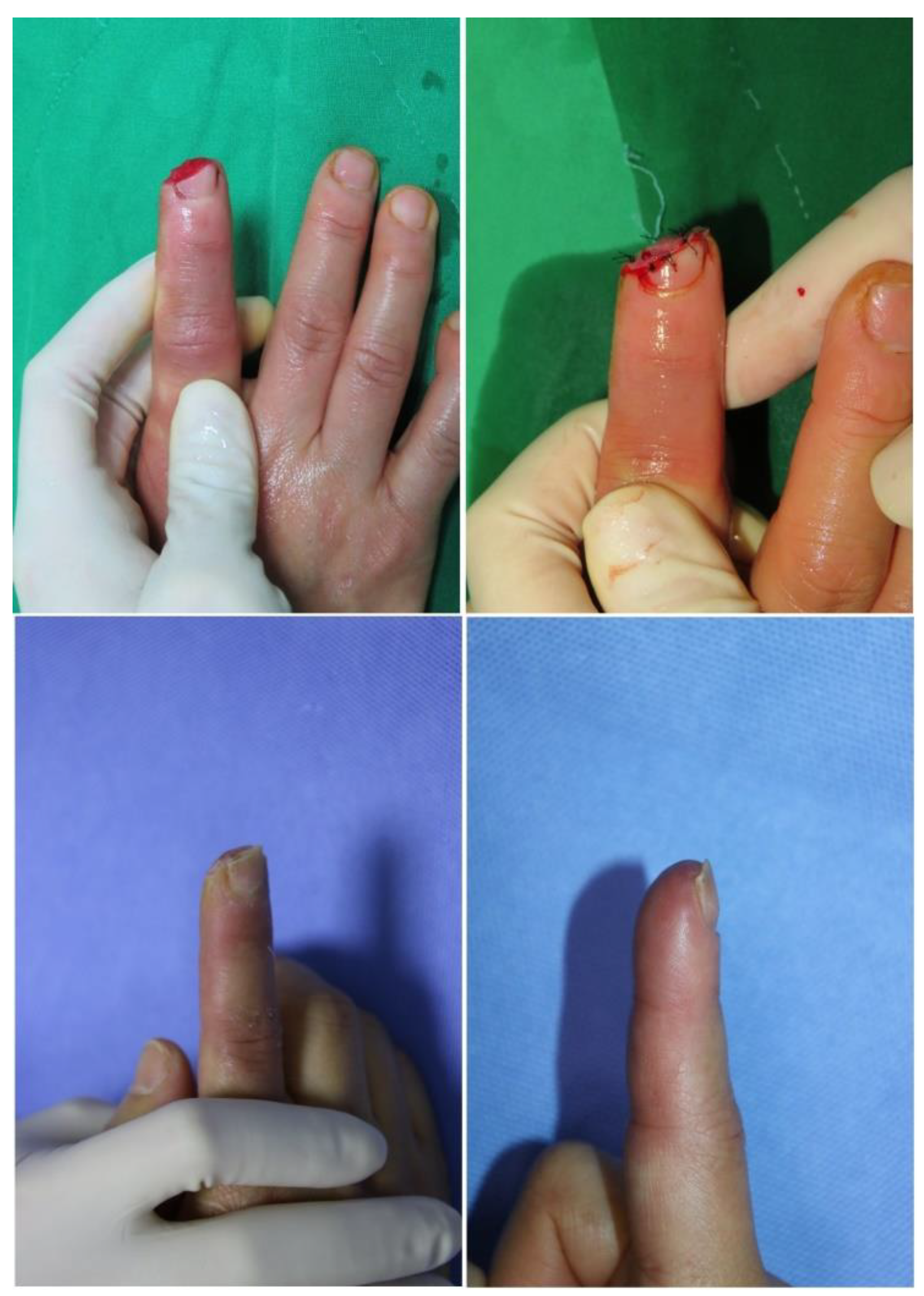
Figure 4.
Reconstruction of a thumb tip defect using artificial dermis application and semi-occlusive dressing, resulting in nail splitting. (A, B) Preoperative pictures showing a soft tissue defect of the right thumb side wall with tendon and bone exposure. (C) Appearance after artificial dermis grafting. (D) Follow-up photograph 7 weeks after the treatment, demonstrating good healing of the defect site but with observable nail splitting.
Figure 4.
Reconstruction of a thumb tip defect using artificial dermis application and semi-occlusive dressing, resulting in nail splitting. (A, B) Preoperative pictures showing a soft tissue defect of the right thumb side wall with tendon and bone exposure. (C) Appearance after artificial dermis grafting. (D) Follow-up photograph 7 weeks after the treatment, demonstrating good healing of the defect site but with observable nail splitting.

Figure 5.
Clinical progression of fingertip regeneration following treatment with artificial dermis and semi-occlusive dressing, demonstrating variability in outcomes. (A) Preoperative view of severe injuries to the left ring and little fingers with complete soft tissue loss and exposed distal phalanges. (B) Four weeks post-treatment, showing significant granulation tissue formation and coverage of the exposed bone. (C) Seven weeks post-treatment, demonstrating slower progression of wound healing, with no exposed bone and partial restoration of the fingerprint ridges. However, trophic changes in the nail bed are evident due to the shortened distal phalanges. (D) Ten weeks post-treatment, revealing complete wound healing with residual scarring on the ring finger and near-complete regeneration of the fingerprint on the little finger. Hook nail deformities are present in both fingers as a consequence of the shortened distal phalanges, which could not be lengthened by the treatment protocol.
Figure 5.
Clinical progression of fingertip regeneration following treatment with artificial dermis and semi-occlusive dressing, demonstrating variability in outcomes. (A) Preoperative view of severe injuries to the left ring and little fingers with complete soft tissue loss and exposed distal phalanges. (B) Four weeks post-treatment, showing significant granulation tissue formation and coverage of the exposed bone. (C) Seven weeks post-treatment, demonstrating slower progression of wound healing, with no exposed bone and partial restoration of the fingerprint ridges. However, trophic changes in the nail bed are evident due to the shortened distal phalanges. (D) Ten weeks post-treatment, revealing complete wound healing with residual scarring on the ring finger and near-complete regeneration of the fingerprint on the little finger. Hook nail deformities are present in both fingers as a consequence of the shortened distal phalanges, which could not be lengthened by the treatment protocol.


Table 1.
Participant Demographics and Injury Characteristics.
| Characteristic | Total (N=31) | Bone Exposure | No Bone Exposure | Tendon Exposure | No Tendon Exposure |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 25 (80.6%) | 17 | 8 | 8 | 17 |
| Female | 6 (19.4%) | 5 | 1 | 2 | 4 |
| Age (years) | |||||
| Mean ± SD | 43.29 ± 15.00 | 43.11 ± 17.22 | 43.36 ± 14.44 | 40.50 ± 14.73 | 44.61 ± 15.30 |
| Affected Fingers | |||||
| Thumb | 3 (9.7%) | 2 | 1 | 3 | 0 |
| Index | 13 (41.9%) | 8 | 5 | 8 | 4 |
| Middle | 6 (19.4%) | 4 | 2 | 4 | 2 |
| Ring | 8 (25.8%) | 6 | 2 | 4 | 4 |
| Little | 5 (16.1%) | 3 | 2 | 3 | 2 |
Table 2.
Complications and their management.
| Complication | No. of patients (%) | Management |
|---|---|---|
| Hook nail deformity | 6 (19.35%) | Observation and patient education |
| Scar contracture | 1 (3.22%) | Steroid injection and Silicone gel ointment |
| Onychomycosis | 1 (3.22%) | Antifungal medication |
| Nail splitting | 1 (3.22%) | Observation and patient education |
Table 3.
Subgroup analysis of outcome measures based on injury characteristics.
| Outcome measure | Bone exposure | Tendon exposure | Combined exposure |
|---|---|---|---|
| Treatment duration (days) | 44.11 ± 10.48 (without) vs. 45.77 ± 19.91 (with) (p=0.131) | 41.71 ± 15.67 (without) vs. 52.80 ± 19.65 (with) (p=0.512) | 43.63 ± 11.09 (neither) vs. 53.33 ± 20.76 (both) (p=0.143) |
| Fingerprint regeneration score† | 2.44 ± 0.88 (without) vs. 2.63 ± 0.58 (with) (p=0.781) | 2.57 ± 0.67 (without) vs. 2.60 ± 0.69 (with) (p=0.917) | 2.37 ± 0.91 (neither) vs. 2.55 ± 0.72 (both) (p=0.815) |
| Hypoesthesia score§ | 0.22 ± 0.66 (without) vs. 0.04 ± 0.21 (with) (p=0.426) | 0.09 ± 0.43 (without) vs. 0.10 ± 0.31 (with) (p=0.968) | 0.25 ± 0.70 (neither) vs. 0.11 ± 0.33 (both) (p=0.963) |
| Hyperesthesia score§ | 0.11 ± 0.33 (without) vs. 0.31 ± 0.64 (with) (p=0.382) | 0.28 ± 0.64 (without) vs. 0.20 ± 0.42 (with) (p=0.702) | 0.12 ± 0.35 (neither) vs. 0.22 ± 0.44 (both) (p=0.743) |
| Pain score(VAS)§ | 0.44 ± 0.52 (without) vs. 0.45 ± 0.73 (with) (p=0.781) | 0.38 ± 0.58 (without) vs. 0.60 ± 0.84 (with) (p=0.633) | 0.37 ± 0.51 (neither) vs. 0.55 ± 0.88 (both) (p=0.743) |
| Cosmetic satisfaction score¶ | 4.22 ± 0.97 (without) vs. 4.04 ± 0.95 (with) (p=0.654) | 4.14 ± 0.91 (without) vs. 4.00 ± 1.05 (with) (p=0.787) | 4.12 ± 0.99 (neither) vs. 3.88 ± 1.05 (both) (p=0.673) |
| Overall satisfaction score¶ | 4.66 ± 0.70 (without) vs. 4.31 ± 0.64 (with) (p=0.174) | 4.47 ± 0.67 (without) vs. 4.30 ± 0.67 (with) (p=0.492) | 4.62 ± 0.74 (neither) vs. 4.22 ± 0.66 (both) (p=0.236) |
*Data presented as without exposure vs. with exposure, p>0.05 for all comparisons (independent samples t-test). †Assessed on a scale from 0 to 3, with higher scores indicating better regeneration. ‡Data presented as without exposure vs. with exposure, p>0.05 for all comparisons (Mann-Whitney U test). §Rated on a scale from 0 to 5, with lower scores indicating less sensory loss, discomfort or pain. ¶Rated on a scale from 1 to 5, with higher scores indicating greater satisfaction.
Table 4.
Comparison of treatment duration with previous studies utilizing artificial dermis for fingertip reconstruction.
Table 4.
Comparison of treatment duration with previous studies utilizing artificial dermis for fingertip reconstruction.
| Study | Sample Size | Injury Type | Method | Treatment Duration (days) | Key Outcomes |
|---|---|---|---|---|---|
| Current Study | 31 | Volar pulp defects with bone and/or tendon exposure | Pelnac® | 45.29 ± 17.53 | High patient satisfaction, good sensory recovery, and cosmetic outcomes |
| Wang et al., 2022 | 24 | Fingertip defects with bone exposure | Pelnac® | 28 ~ 42 | Improves appearance and function, and decreases the need for stump trimming in amputated fingers. |
| Namgoong et al., 2020 | 23 | Fingertip defects with bone exposure | Tissue-engineered artificial dermis | 34.0 ± 4.9 | Superior functional and aesthetic outcome compared to artificial dermis graft |
| Hoigné et al., 2014 | 19 | Fingertip amputations(Ishikawa zones II – III) | OpSite® Flexifix® dressing | 21 ~ 56 | Good sensory recovery and cosmetic outcomes |
| Boudard et al., 2019 | 19 | Fingertip amputations (M & D* zone I - III) | Tegaderm® dressing | 30.1 ± 7 | Good functional and cosmetic outcomes |
| Mennen & Wiese, 1993 | 200 | Various fingertip injuries | OpSite® dressing | 20-30 | Good functional and cosmetic outcomes, low complication rate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



