
Submitted:
11 May 2024
Posted:
13 May 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Cancer patients, susceptible to severe COVID-19 outcomes, exhibit varied vaccine responses, particularly those who are receiving chemotherapy. This prospective cohort study enrolled 115 cancer patients, and data from 91 patients who received two doses of COVID-19 vaccines were analyzed. Blood was drawn at baseline, day 28, and 6 months post-second dose for neutralizing antibody analysis. The primary outcome was seroconversion rate against wild type and Omicron at day 28. Secondary outcomes included seroconversion at 6 months, factors associated with seroconversion, and safety. Of the 157 cancer patients screened, 91 were enrolled, with 45% receiving chemotherapy. Seroconversion rates at day 28 were 77% for the wild type and 62% for Omicron. Chemotherapy did not affect seroconversion (p=0.789 for wild type, p=0.597 for Omicron). Vaccine type positively correlated with seroconversion, with an adjusted ORR of 25.86 (p=0.029) for the wild type and 17.38 (p<0.001) for Omicron with the primary heterologous vaccine. Adverse events were grade 1 in 34.0% and grade 2 in 19.7% of participants. Despite lower seroconversion against Omicron, no difference was noted between chemotherapy and non-chemotherapy groups. COVID-19 vaccinations demonstrated good tolerability. This data underscores vaccine efficacy considerations in cancer patients, informing tailored strategies for this vulnerable population.
Keywords:
COVID-19
; COVID-19 vaccines
; seroconversion rate of neutralizing antibody
; Solid cancer patients
1. Introduction
COVID-19, emerging infectious disease firstly reported in December 2019, is now a global pandemic caused by the SARS-CoV-2 virus. Its entry into host cell triggers an immune response releasing inflammatory cytokines. This excessive inflammation drives high morbidity and mortality [1].
Reports indicate that COVID-19 outcomes are worse with comorbidities [2], particularly in immunocompromised individuals like cancer patients undergoing treatments especially chemotherapy. Cancer patients are more prone to severe infection outcomes, including increased rates of ICU admission, mechanical ventilation, prolonged hospital stays, and mortality [3,4].
Studies on cancer patients have found decreased humoral immunity in post-infection and vaccination. Natural infection led to reduced N-IgG and S-IgG antibody levels especially after recent chemotherapy [5]. However, patients undergoing immunotherapy showed higher antibody levels. Similarly, mRNA-based vaccine studies showed lower seroconversion rates in cancer patients (90-94% after two doses of vaccination) [6,7,8]. with decreased neutralizing antibody levels against COVID variants [9,10]. However, humoral immunities declined over time, making the third booster dose is necessary to maintain adequate level of immunity [11]. Due to poor prognosis of cancer, patients may have a shorter estimated life expectancy particularly in advanced or metastatic diseases. Achieving higher seroconversion rate after two doses of vaccination should be a concern. Data from non-cancer populations showed that heterologous prime-boosted vaccinations generated higher level of neutralizing antibody compared to homologous vaccinations [12]. Further research is needed to elucidate these data in cancer patients.
In this study, our objective is to assess the humoral-mediated immune response in terms of seroconversion rate and percent inhibition of neutralizing antibodies against the wild type and Omicron variant of the SAR-CoV-2 virus in patients with solid cancer who have received two doses of COVID vaccine, comparing chemotherapy and non-chemotherapy groups. Additionally, we aim to investigate factors associated with antibody seroconversion at day 28 after completing vaccination and adverse events following immunization.
2. Materials and Methods
2.1. Study Design and Participants
This observational prospective cohort study was designed to evaluate humoral immunogenicity in terms of surrogate neutralizing antibodies against the wild type and XBB Omicron variants, as well as safety, in patients with solid cancer who received two doses of Sinovac vaccine. However, the protocol allowing for different vaccines combinations was adapted and amended later due to vaccine shortages and uncertain vaccine management of Thailand government. Combinations of vaccines on different platforms were allowed, including mRNA with mRNA boosters, non-mRNA with non-mRNA boosters, and non-mRNA with mRNA boosters. This study included adult solid cancer patients who were 18 years of age or above with confirmed diagnosis of cancer by histology or imaging at any stages and any undergoing treatments, including complete remission disease within 1 year. The patients were required to have estimated life expectancy more than six months. All patients were followed up at medical oncology clinic at Maharaj Nakorn Chiang Mai Hospital, Sriphat Medical Center, Faculty of Medicine, Chiang Mai University and Chiang Mai Klaimor Hospital (Private Hospital). Exclusion criteria included previously diagnosed COVID infection documented by RT-PCR or Antigen test kit (ATK) in the past three months, high-risk epidemiological history within 14 days, for example, close contact with a COVID-19 diagnosis or visiting/living in an outbreak area., receiving prior COVID vaccines, receiving other live attenuated vaccine in the past four weeks or inactivated and subunit vaccine in the past two weeks, known allergy to any vaccine components, has signs and symptoms of active skin infection at injection site, HIV infection, receiving immunosuppressive drug, receiving blood components within three months, pregnancy, uncontrolled medical conditions, and hematologic malignancies. Withdrawal criteria include individuals who cannot follow up after receiving the vaccine and those who do not complete the vaccination program. Patients who completed three doses of the vaccine and those who had COVID infection were also reported. This study was approved by institution Ethics Committee of Faculty of Medicine, Chiang Mai University. All participants were provided and signed informed consent forms.
2.2. Procedure and Materials
2.2.1. Blood and Data Collection
157 patients with solid cancer were screened; 115 patients were enrolled for this study. between August 2021 to February 2022. Data from 91 patients who had completed two doses of vaccination were analyzed for neutralizing antibody levels. Demographic data were obtained, and 6 ml of blood was drawn for baseline analysis from participants on the day of signing informed consent. Each participants received a vaccine as part of their personal vaccination programs provided by government or private hospitals, which included homologous and heterologous vaccine regimens.
Blood was obtained other times at 28 days and 6 months after second dose of vaccination. Third booster doses were allowed. Information on adverse events following immunization was collected during follow up at the oncology clinic. Blood samples from participants were centrifuged and stored as plasma in liquid nitrogen until further used for neutralizing antibody analysis.
2.2.2. Neutralizing Antibody Assay
The surrogate virus neutralization assay kit (MAGLUMI, Shenzhen New Industries Biomedical Engineering Co., Ltd) was used for the wild type neutralizing antibody assay and another neutralizing antibody kit (cPass™, Genscript, XBB variant spike protein) was used for XBB variant neutralizing antibody assay. This method mimics interaction between the host hACE2 receptor and virus biding site using recombinant SAR-CoV2 receptor biding domain (RBD). This assay has shown 100% sensitivity and 100% specificity in clinical samples with confirmed SARS-CoV-2 VNT50 ≥ 20. The assays reported antibody level in IU/mL units (wild type only), percent inhibition, and whether the antibody was detected or undetected. Detected neutralizing antibody is defined as a level of antibody greater than 121.6 IU/mL for wild type and percent inhibition greater than 30% for Omicron variant.
2.3. Outcome
The dual primary outcomes were the seroconversion rates of neutralizing antibodies at 28 days after completing two doses of the vaccine against SAR-CoV2 for both the wild type and XBB Omicron Variants. The secondary outcomes included the percent inhibition of neutralizing antibody, seroconversion rates at 6 months, factors associated with seroconversion of day 28, and adverse events following immunization.
2.4. Statistical Analysis
Based on 90-94% seroconversion rate from previous studies in cancer patients with level of confidence for 95% and a margin of error for 5%, the calculated sample size ranged between 87 and 139. After adjusted for 5% loss follow up rate, the required sample size was 91 to 146 participants. Data will be analyzed as per protocol due to aiming of reflect real world data of vaccine efficacy. Descriptive data were reported using number and percentage, means and standard deviations (SD), as well as medians and interquartile ranges. Chi-Square and Fisher’s Exact test were used to analyze comparisons of baseline characteristics between the chemotherapy and non-chemotherapy groups. The percentage of inhibition and seroconversion rate of neutralizing antibodies were reported as means with 95% confidence intervals and analyzed using repeated-measure mixed models across three time points (baseline, day 28, and month 6) and COVID variants (wild and Omicron variant). Univariate logistic regression analysis was used to identify potential factors associated with seroconversion. Factors with P < 0.1 were further investigated by multivariate logistic regression analysis. Statistical significance in each analysis was defined as P < 0.05. All statistical analyses were performed using STATA/MP software version 17 (StataCorp LLC. College station, TX, USA).
3. Results
3.1. Baseline Characteristics
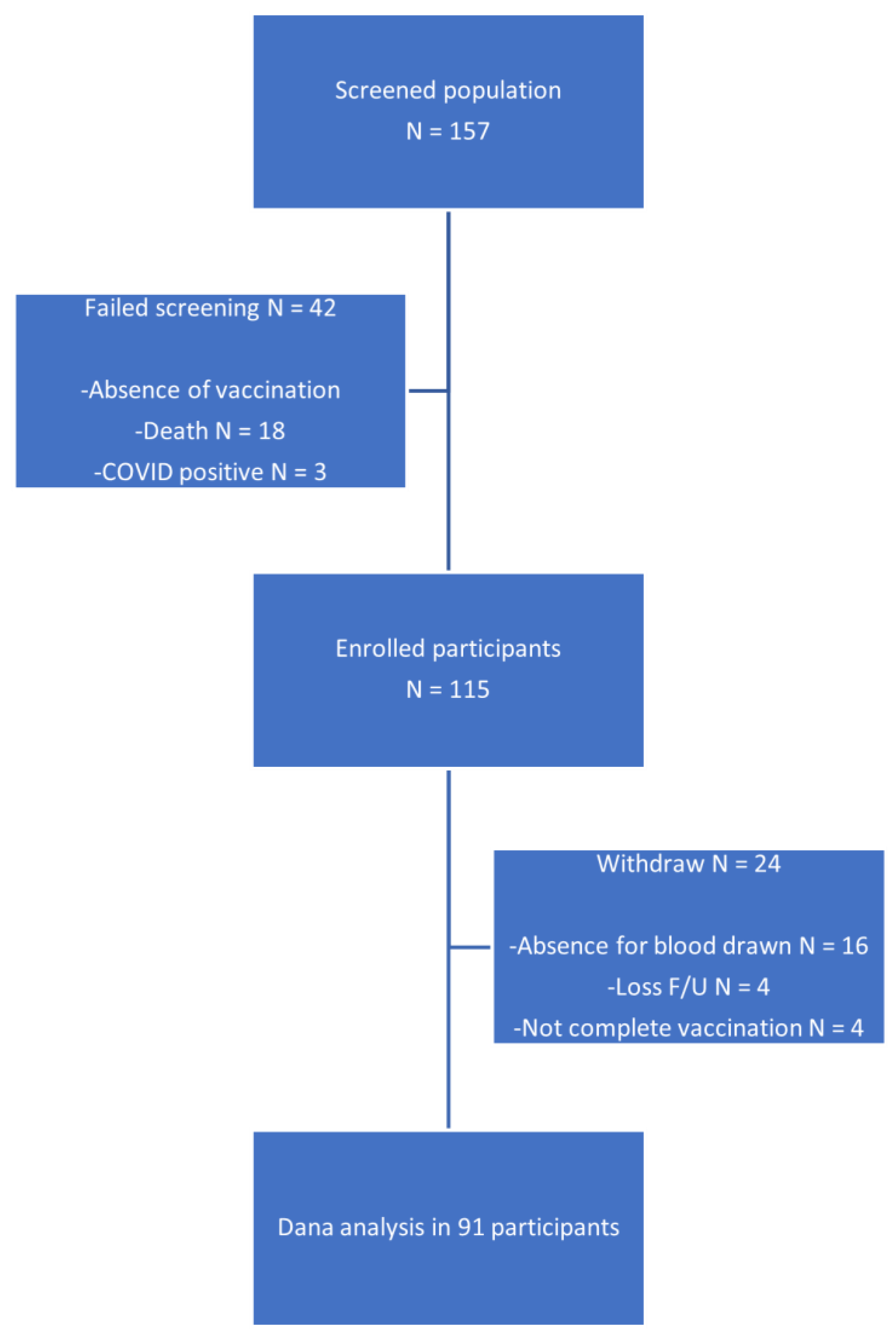
A total of 157 patients with solid cancer, who planned to receive the COVID vaccine, were screened, among them, 115 patients were enrolled for this study. Data from 91 patients who had completed two doses of vaccination were analyzed for neutralizing antibody. The common reasons for failed enrollment were the absence of vaccination (n=21/157, 13.3%) and death before completion of vaccine (n=18/157, 11.4%), including one of them being a COVID related death. Failed screening and participant withdrawal data was reported in the consort diagram. The vaccinations included homologous mRNA-based vaccines (mRNA+mRNA), homologous non-mRNA-based vaccines (non-mRNA+non-mRNA), and heterologous vaccines (non-mRNA+mRNA) in 41 (45%), 31 (34%), and 19 (21%) participants, respectively. Twenty-one of these individuals (23.0%) received a third dose booster vaccine. All patients were then classified into chemotherapy (n=41, 45%) and non-chemotherapy (n=50, 55%) groups for further exploratory analysis, which were not prespecified subgroups.
Baseline demographic and disease characteristics are presented in Table 1. According to an observational-only study, some parameters between groups were not well balanced. In the chemotherapy group, male patients predominated (n=26, 63.4%), while female patients predominated in the non-chemotherapy group (n=31, 62.0%). The mean age and BMI were 60.76 years and 23.44 kg/m², respectively, for all participants. The most common primary cancers were GI cancer (n=21, 51.2%) in the chemotherapy group and breast cancer (n=20, 40.0%) in the non-chemotherapy group. Baseline white blood cell, neutrophil, and lymphocyte counts tended to be lower, and hematologic adverse events during follow-up were more common in the chemotherapy group.
Figure 1.
Consort Diagram.
3.2. Neutralizing Antibody
3.2.1. Seroconversion Rate
Baseline seroconversion rate before vaccination was 0% in all population for both wild type and Omicron variant, affirming seronegative status for COVID in all participants. The seroconversion rate of surrogate neutralizing antibody for wild type COVID at 28 days after completing vaccination in all participants was 77% (95% CI, 67-85%). There was no significant difference in seroconversion between chemotherapy and non-chemotherapy groups (76% vs 78%, p=0.789). Contrary to Omicron variant, seroconversion rate was 62% (95%CI, 51-72%), 59% (95%CI,42-74%), and 64% (95%CI, 49-77%) in all participants, chemotherapy, and non-chemotherapy groups respectively, showing no difference between groups (p=0.597). To compare between variants, the seroconversion rate for the Omicron variant was lower than that for the wild type in both treatment groups (p=0.008 for both chemotherapy and non-chemotherapy groups). Seroconversion rates at 6 months did not differ from day 28 for both variants and were provided in Table 4 and Table 5.
3.2.2. Percent Inhibition
Percent inhibition was below the cutoff level for seroconversion in all participants at baseline. At 28 days after vaccination, the mean percent inhibition for the wild type was 62.25 (95%CI, 55.19-69.30), 61.79 (95%CI, 50.79-72.78), and 62.62 (95%CI, 53.13-72.12) for all participants, chemotherapy, and non-chemotherapy groups respectively (Table 2A and 2B). There was no difference between treatment group (p=0.907). For the Omicron variant, mean percent inhibition was 42.17 (95%CI, 36.90-47.44), 40.09 (95%CI, 32.19-47.99), and 43.87 (95%CI, 36.59-51.16) for all participants, chemotherapy, and non-chemotherapy groups respectively. Again, there was no difference between treatment groups (p=0.476). However, percent inhibition of Omicron variant was lower than that of the wild type (p<0.001 in both treatment groups). Percent inhibitions at 6 months were provided in Table 4 and 5.
3.3. Factors Associated with Seroconversion
The univariate analysis of factors associated with seroconversion of neutralizing antibody for both the wild type and Omicron variant is shown in Table 6. In multivariable analysis, the type of vaccine was the only factor positively correlated with seroconversion. For the wild type COVID variant, the adjusted odd ratios for homologous mRNA vaccine (mRNA+mRNA) and heterologous vaccine (non-mRNA+mRNA) were 14.42 (95%CI 1.99-104.24, p=0.008) and 25.86 (95%CI 1.39-478.06, p=0.029) respectively. For the Omicron variant, the adjusted odd ratios were 8.90 (96%CI 2.93-26.94, p<0.001) and 17.38 (95%CI 2.65-82.66, p<0.001) for homologous mRNA vaccine and heterologous vaccine. Diabetes mellitus (DM) was another potential factor associated with reduced seroconversion for the wild type COVID variant, with an adjusted odds ratio of 0.153 (95% CI0.023-1.022, p=0.053), but no statistical significance was met.

Table 6.
Univariate analysis of factors.
| Factors | Wild Type | Omicron Variant | ||||
|---|---|---|---|---|---|---|
| Seroconversion n (%) | OR (95% CI) |
p-Value | Seroconversion n (%) | OR (95% CI) |
p-Value | |
| Age | ||||||
| <65 yrs | 47 (81.03%) (n=58) |
1.709 (0.63-4.57) | 0.286 | 36 (62.07%) (n=58) |
1.227(0.52-2.88) | 0.638 |
| ≥65 yrs | 25 (71.43%) (n=35) |
ref | - | 20 (57.14%) (n=35) |
ref | - |
| Smoking(yes) | 16 (84.21%) (n=19) |
1.684 (0.44-6.44) | 0.447 | 12 (63.16%) (n=19) |
1.142 (0.40-3.23) | 0.801 |
| BMI | ||||||
| <18.5 (underweight) | 9 (100%) (n=9) |
7.945 (0.425-148.193) | 0.165 (vs bmi≥23) |
8 (88.89%) (n=9) |
3.737 (0.587-23.781) | 0.163 (vs bmi≥23) |
| 5.231 (0.278-98.283) | 0.269 (vs bmi 18.5-22.9) |
4.510 (0.719-28.253) | 0.108 (vs bmi 18.5-22.9) |
|||
| 18.5-22.9 (normal) | 34 (79.07%) (n=43) |
1.518 (0.561-4.106) | 0.410 (vs bmi≥23) |
24 (55.81%) (n=43) |
0.828 (0.345-1.987) | 0.674 (vs bmi≥23) |
| ≥23.0 (overweight) | 27 (71.05%) (n=38) |
ref | - | 23 (60.53%) (n=38) |
ref | - |
| Primary cancer, n (%) | ||||||
| GI | 25 (78.12%) (n=32) |
1.041 (0.372-2.912) | 0.938 | 19 (59.38%) (n=32) |
0.923 (0.386-2.205) | 0.857 |
| HBP | 13 (81.25%) (n=16) |
1.300 (0.333-5.072) | 0.706 | 10 (62.50%) (n=16) |
1.099 (0.362-3.332) | 0.867 |
| Breast | 18/26, 69.23% (n=26) |
0.531 (0.190-1.488) | 0.229 | 14 (53.85%) (n=26) |
0.678 (0.271-1.693) | 0.406 |
| Prostate | 3 (60.00%) (n=5) |
0.407 (0.063-2.614) | 0.344 | 1 (20.00%) (n=5) |
0.147 (0.015-1.374) | 0.093 |
| Others | 13/ (92.86%) (n=14) |
4.406 (0.541-35.850) | 0.166 | 13 (92.86%) (n=14) |
10.340 (1.289-82.925) | 0.028 |
| Metastasis | 36 (81.82%) (n=44) |
1.720 (0.634-4.666) | 0.286 | 28 (63.64%) (n=44) |
1.187 (0.509-2.768) | 0.691 |
| Active cancer treatment | 51 (71.83%) (n=71) |
0.134 (0.016-1.070) | 0.058 | 41 (57.75%) (n=71) |
0.455 (0.149-1.391) | 0.167 |
| Chemo vs non-chemo | 31 (75.61%) (n=41) |
0.874 (0.328-2.432) | 0.788 | 24 (58.54%) (n=41) |
0.794 (0.340-1.854) | 0.594 |
| Targeted vs non-targeted | 11 (57.89%) (n=19) |
0.302 (0.101-0.901) | 0.032 | 10 (52.63%) (n=19) |
0.628 (0.226-1.743) | 0.372 |
| Hormonal vs non-hormonal | 8 (57.14%) (n=14) |
0.322 (0.097-1.070) | 0.064 | 5 (35.71%) (n=14) |
0.283 (0.086-0.931) | 0.038 |
| No active cancer treatment | 19/20, 95.00% (n=20) |
ref | - | 15/20, 75.00% (n=20) |
ref | - |
| Comorbidity | ||||||
| DM | 11 (64.71%) (n=17) |
0.458 (0.145-1.439) | 0.181 | 10 (58.82%) (n=17) |
0.900 (0.308-2.630) | 0.848 |
| HT | 24 (68.57%) (n=35) |
0.464 (0.172-1.246) | 0.128 | 18 (51.43%) (n=35) |
0.529 (0.223-1.253) | 0.148 |
| Other comorbid | 30 (73.175%) (n=41) |
0.665 (0.250-1.767) | 0.414 | 26 (63.41%) (n=41) |
1.213 (0.520-2.825) | 0.654 |
| Vaccine type | ||||||
| mRNA+mRNA | 40 (93.02%) (n=43) |
14.763 (4.062-53.651) | <0.001(vs N+N) | 32 (74.42%) (n=43) |
6.990 (2.545-19.193) | <0.001 (vs N+N) |
| non-mRNA+mRNA | 19 (100.00%) (n=19) |
49.758 (2.765-895.383) | 0.008(vs N+N) | 16 (84.21%) (n=19) |
11.661 (2.940-46.249) | <0.001 (vs N+N) |
| 3.370 (0.165-68.515) | 0.429(vs M+M) | 1.668 (0.438-6.339) | 0.453 (vs M+M) |
|||
| nonRNA+nonRNA | 14 (43.755%) (n=32) |
ref | - | 9 (28.12%) (n=32) |
ref | - |
| Leucopenia | 11 (73.33%) (n=15) |
0.651 (0.167-2.526) | 0.535 | 10 (66.67%) (n=15) |
1.357 (0.400-4.603) | 0.624 |
| Neutropenia | 2 (40.00%) (n=5) |
0.141 (0.020-0.962) | 0.046 | 2 (40.00%) (n=5) |
0.388 (0.060-2.519) | 0.332 |
| Lymphopenia | 14 (70.00%) (n=20) |
0.466 (0.122-1.635) | 0.234 | 12 (60.00%) (n=20) |
0.923 (0.310-2.745) | 0.886 |
Table 7.
Multivariable analysis of factors in the wild type subgroup.
| Factors | Seroconversion, n (%) | Adjusted OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Neutropenia | 2 (40.00%) (n=5) |
0.237 (0.026-2.125) | 0.199 | |
| Diabetes Mellitus | 11 (64.71%) (n=17) |
0.153 (0.023-1.022) | 0.053 | |
| Vaccine type | ||||
| mRNA+mRNA | 40 (93.02%) (n=43) |
14.424 (1.995-104.242) | 0.008 | |
| Non-mRNA + mRNA | 19 (100%) (n=19) |
25.866 (1.399-478.06) | 0.029 | |
Table 8.
Multivariable analysis of factors in the Omicron variant subgroup.
| Factors | Seroconversion, n (%) | Adjusted OR (95% CI) |
p-Value |
|---|---|---|---|
| Cancer type | |||
| Prostate | 1 (20.00%) (n=5) |
0.118 (0.010-1.343) | 0.085 |
| Other cancer | 13 (92.86%) (n=14) |
8.268 (0.813-84.082) | 0.074 |
| Vaccine type | |||
| mRNA+mRNA | 32 (74.42%) (n=43) |
8.900 (2.939-26.949) | <0.001 |
| Non-mRNA + mRNA | 16 (84.21%) (n=19) |
17.380 (3.653-82.669) | <0.001 |
3.4. Safety
Adverse events following immunization occurred in 34.0% and 19.7% in all participants for grade 1 and grade 2, respectively. The most common side effect was pain at the injection site, followed by fever and fatigue. There were no serious events leading to emergency department visits or hospitalizations.
Table 9.
Univariate analysis of factors.
| All Participants (n = 91) | Non-Chemotherapy (n = 50) | Chemotherapy (n = 41) | ||||
|---|---|---|---|---|---|---|
| Grade 1 n (%) |
Grade 2 n (%) |
Grade 1 n (%) |
Grade 2 n (%) |
Grade 1 n (%) |
Grade 2 n (%) |
|
| Any | 31 (34.0%) | 18 (19.7%) | 22 (44.0%) | 8 (16.0%) | 9 (21.9%) | 10 (24.3%) |
| Pain at injection site | 14 (15.3%) | 10 (10.9%) | 11 (22.0%) | 3 (6.0%) | 3 (7.3%) | 7 (17.0%) |
| Fever | 8 (8.7%) | 5 (5.4%) | 5 (10.0%) | 2 (4.0%) | 3 (7.3%) | 3 (7.3%) |
| Fatigue | 4 (4.3%) | 3 (3.2%) | 4 (8.0%) | 3 (6.0%) | 0 | 0 |
| Malaise | 3 (3.2%) | 0 | 1 (2.0%) | 0 | 2 (4.8%) | 0 |
| Diarrhea | 1 (1.0%) | 1 (1.0%) | 1 (2.0%) | 0 | 1 (2.4%) | 1 (2.4%) |
3.5. Clinical Correlation of Seroconversion and COVID Infection
Four participants (n=4/91, 4.39%) were confirmed to have COVID infection after completing vaccinations; additionally, all of them tested negative for seroconversion for both the wild type and Omicron variant. The timing periods of infection ranged from 1 to 11 months after the second dose of the vaccine. Among them, one patient was suffered from severe COVID pneumonia, required mechanical ventilator use and resulting in multiorgan failure leading to death. In contrast, none of the seropositive participants were diagnosed with COVID infection.
4. Discussion
Our study was initially designed during the era of vaccine shortage in Thailand and worldwide. According to government policy at that time, COVID vaccines procurement was disorganized, and access to vaccination relied on personal efforts. Therefore, vaccine combinations with different platforms were expected to be heterogenous unintentionally.
This study was a real-world cohort of patients with solid cancer, showing a very high mortality rate. Apart from cancer itself, these patients were also vulnerable to COVID infection. Eleven percent of participants (n=18) died due to cancer-related problems, including one death from COVID pneumonia, and 3 percent (n=4) were confirmed positive for COVID infection before completing vaccination or blood analysis. Given the grim prognosis of cancer patients, a higher rate of seroconversion to protective antibodies against COVID after two doses vaccination is still a concern, although a third booster dose is crucial to maintain immunity levels.
Neutralizing antibodies can serve as a more predictive tool for assessing protection against COVID infection compared to anti-RBD or anti-S levels, as they can bind to and neutralize the virus, aiding in viral control and clearance [13]. Anti-RBD and anti-S levels are poor predictors of immunity for the wild type and novel variants, as increasing levels of anti-RBD do not necessarily imply the presence of neutralizing antibodies [14]. Data from previous reports may overestimate vaccine efficacy, highlighting the important of defining vaccine efficacy based on neutralizing antibodies. Surrogate neutralization assays offer an alternative effective method that does not require a biosafety level 3 laboratory and exhibit high sensitivity (95-100%) and specificity (99.93%) [15]. The test still performs acceptable after validation for the Omicron variant [16]. Our study revealed lower seroconversion rate of surrogate neutralizing antibody (77% and 62% for wild type and Omicron variants, respectively) compared to previous reports on seroconversion of anti-RBD and anti-S antibodies in patients with solid cancers (90-94%) [6,17] and the healthy population (97-99%) [18]. This result is consistent with a study on pseudo-virus neutralization assay in cancer patients, where detectable neutralization antibodies for the wild type of virus were found in 75-85% of mRNA-based vaccines group [10].
The lower seroconversion of Omicron variant (XBB) in this study was consistent with other reports in both cancer and healthy populations [19,20]. Most Covid vaccines were developed before the era of ongoing novel variants of concerns (VOCs), leading to challenging problems with vaccine effectiveness. In the Capture study, seroconversions of neutralizing antibodies using live virus microneutralization assays were found positive in 83%, 61%, 53% and 54% for the wild type, Alpha, Beta, and Delta variants respectively in patients with cancer [9]. Another study on lung cancer patients receiving mRNA vaccines has shown decreased level of live virus neutralization assay more than 50 folds in Omicron variant compared to the wild type [19]. This finding was in concordance with our study. Additionally, the mean percent inhibition assay also decreased from 62.25 % in the wild type to 42.17 % in the Omicron variant. Thus, these findings suggest limited efficacy of vaccines against variant of concerns.
Active cancer treatments, including chemotherapy, targeted therapy, endocrine therapy, and immunotherapy, have controversial outcomes on seroconversion. Among these, chemotherapy is considered an immunosuppressive agent which might cause leukopenia and lead to infection. This concept has elicited interesting in the potential detrimental effect of chemotherapy on vaccine efficacy. Some studies have shown a reduced humoral immune response in chemotherapy treatment groups [21,22,23]. In a large cohort study in US veterans affairs, patients receiving chemotherapy within 3 months before vaccination had the lowest vaccine effectiveness, which was 57% (95% CI; -23 to 90%) compared with the endocrine therapy and no systemic therapy group (76%, 95% CI; 50 to 91% and 85%, 95% CI; 29 to 100% respectively) [24]. While some studies have revealed no mitigatory effect of chemotherapy on humoral immunity in COVID vaccine [25,26]. Our study showed a lower trend but not statistical significance in both the seroconversion rate and percent inhibition assay in patients receiving chemotherapy three months prior or during vaccination in term of neutralization assay for both wild type and Omicron variant, regardless of leukopenia, neutropenia, and lymphopenia. However, overall effects of systemic treatments in cancer and vaccination on COVID infection outcomes remain unclear and inconsistent [27,28].
The exploratory analysis of factors associated with seroconversion from our study suggested that only the type of the vaccine combinations was related. The primary heterologous vaccine combination yielded the highest seroconversion outcome with an adjusted odds ratio of (ORR) 25.86 (95%CI 1.39-478.06, p=0.029) followed by homologous mRNA vaccines with an adjusted ORR 14.42 (95%CI 1.99-104.24, p=0.008) compared with homologous non-mRNA vaccines for the wild type. This result was similar for Omicron variant, with adjusted odd ratios of 17.38 (95%CI 2.65-82.66, p<0.001) and 8.90 (96%CI 2.93-26.94, p<0.001) for heterologous and homologous mRNA vaccines, respectively. Undoubtedly, booster doses after completing two doses of COVID vaccine generate higher and longer-lasting neutralizing antibody levels [11,29,30], consequently, a third booster vaccine is essential and should be regarded as the standard of care.
However, this study provided a novel report on the more robust immunogenicity of heterologous primary vaccines in patients with cancers, which is coherent with reports on healthy populations [31] and third heterologous prime-boost vaccine [12]. The potential mechanisms include reorientation of B cell responses toward neutralizing sites of expressed epitopes encoded by mRNA vaccines [32] and the accompaniment of cellular and humoral response on different vaccine platforms [33]. Therefore, heterologous vaccine strategy should be encouraged since second booster primary vaccine, particularly in populations that tend to have lower seroconversion rates.
Diabetes was another potential factor contributing to a weaker immune response in wild type COVID, with an adjusted odd ratio of 0.153 (95% CI; 0.023-1.022, p=0.053); however, statistical significance was not met. Diabetes is well-known for its immunosuppressive state. Some systematic reviews in the general population reported inferiority of immune response to COVID vaccine in patients with diabetes particularly in poor controlled glycemic status [34,35]. Diabetes and glycemic control in patients with cancer should be evaluated further about adverse correlations with neutralizing antibodies.
For safety concern, vaccinations were well tolerated in both chemotherapy and non-chemotherapy groups. All participants experienced minor reactions such as pain at injection site, fever, and fatigue which were self-limited or alleviated by over-the-counter drugs. None of them required to seek medical attention or hospitalization.
The strength of our study lies in providing real-world data on COVID-19 vaccine efficacy, specifically in terms of seroconversion of surrogate neutralizing antibodies, in solid cancer patients with and without active cancer treatments, especially chemotherapy in advanced or metastatic diseases. However, there were some limitations in our study. The population size was small due to high mortality rate of cancer, incomplete vaccination and not providing a blood draw in some participants. Secondly, missing information on third booster vaccines during the follow up period resulted in inaccurate analysis of neutralizing antibodies at 6 months. Hence, longevity of antibody cannot be provided in our study. In addition, this study did not include analysis of cellular immunity and memory function of adaptive immune response.
5. Conclusions
The seroconversion rate of neutralizing antibody against Omicron variant was lower compared to wild type in solid cancer patients. However, there was no difference between patients who received chemotherapy and those who did not. COVID vaccinations were well tolerated.
Author Contributions
Conceptualization, B.C., A.T., and P.S.; methodology, B.C., P.S. and A.T.; validation, B.C. and P.S.; formal analysis, B.C., P.S. and A.T.; investigation, B.C. and P.S.; resources, B.C., T.K, T,S., C.C. and N.N.; data curation, B.C. and P.S.; writing—original draft preparation, B.C. and P.S.; writing—review and editing, B.C., P.S., A.T., T.K, T,S., C.C. and N.N.; visualization, B.C.; supervision, B.C.; project administration, B.C. and P.S.; funding acquisition, B.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Faculty of Medicine, Chiang Mai University.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, approved by the Institutional Review Board of Faculty of Medicine, Chiang Mai University (MED-2564-08326, 11 August 2021), and was registered in Thai Clinical Trials Registry (TCTR20230510001).
Informed Consent Statement
All participants were explained about this research and signed in informed consent forms.
Acknowledgments
We would like to extend our sincere gratitude to Watchara Kasinrerk, Witida Laopajon, Nuchjira Takheaw, and Supansa Pata in facilitating laboratory collections and procedures. Their dedication and assistance ensured the smooth execution of our experimental protocols. We also gratefully acknowledge Antika Wongthani for her expert statistical analysis, which significantly contributed to the rigor and interpretation of our study findings. We sincerely thank Chanutchidchanok Jannakorn for her invaluable role in typing and coordinating efforts, which greatly facilitated the organization and execution of this project.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: an overview on cytokine storm and related interventions. Virol J 2022, 19, 92. [Google Scholar] [CrossRef] [PubMed]
- Chenchula, S.; Vidyasagar, K.; Pathan, S.; Sharma, S.; Chavan, M.R.; Bhagavathula, A.S.; Padmavathi, R.; Manjula, M.; Chhabra, M.; Gupta, R.; et al. Global prevalence and effect of comorbidities and smoking status on severity and mortality of COVID-19 in association with age and gender: a systematic review, meta-analysis and meta-regression. Sci Rep 2023, 13, 6415. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Sheng, Y.; Huang, C.; Jin, Y.; Xiong, N.; Jiang, K.; Lu, H.; Liu, J.; Yang, J.; Dong, Y.; et al. Clinical characteristics, outcomes, and risk factors for mortality in patients with cancer and COVID-19 in Hubei, China: a multicentre, retrospective, cohort study. Lancet Oncol 2020, 21, 904–913. [Google Scholar] [CrossRef]
- Salunke, A.A.; Nandy, K.; Pathak, S.K.; Shah, J.; Kamani, M.; Kottakota, V.; Thivari, P.; Pandey, A.; Patel, K.; Rathod, P.; et al. Impact of COVID -19 in cancer patients on severity of disease and fatal outcomes: A systematic review and meta-analysis. Diabetes Metab Syndr 2020, 14, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Yazaki, S.; Yoshida, T.; Kojima, Y.; Yagishita, S.; Nakahama, H.; Okinaka, K.; Matsushita, H.; Shiotsuka, M.; Kobayashi, O.; Iwata, S.; et al. Difference in SARS-CoV-2 Antibody Status Between Patients With Cancer and Health Care Workers During the COVID-19 Pandemic in Japan. JAMA Oncol 2021, 7, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of Seropositivity Following BNT162b2 Messenger RNA Vaccination for SARS-CoV-2 in Patients Undergoing Treatment for Cancer. JAMA Oncol 2021, 7, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Amatu, A.; Pani, A.; Patelli, G.; Gagliardi, O.M.; Loparco, M.; Piscazzi, D.; Cassingena, A.; Tosi, F.; Ghezzi, S.; Campisi, D.; et al. Impaired seroconversion after SARS-CoV-2 mRNA vaccines in patients with solid tumours receiving anticancer treatment. Eur J Cancer 2022, 163, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Limpawittayakul, P.; Sungkasubun, P.; Chaiwiriyawong, W.; Supavavej, A.; Weerasubpong, B.; Siripaibun, J.; Phanthunane, C.; Lamlertthon, W.; Ungtrakul, T.; Tawinprai, K.; et al. Immunogenicity evaluation of ChAdox1 nCov-19 (AZD1222) vaccine in solid cancer patients in Chulabhorn Hospital. Hum Vaccin Immunother 2022, 18, 2104058. [Google Scholar] [CrossRef] [PubMed]
- Fendler, A.; Shepherd, S.T.C.; Au, L.; Wilkinson, K.A.; Wu, M.; Byrne, F.; Cerrone, M.; Schmitt, A.M.; Joharatnam-Hogan, N.; Shum, B.; et al. Adaptive immunity and neutralizing antibodies against SARS-CoV-2 variants of concern following vaccination in patients with cancer: the CAPTURE study. Nat Cancer 2021, 2, 1305–1320. [Google Scholar] [CrossRef]
- Naranbhai, V.; St Denis, K.J.; Lam, E.C.; Ofoman, O.; Garcia-Beltran, W.F.; Mairena, C.B.; Bhan, A.K.; Gainor, J.F.; Balazs, A.B.; Iafrate, A.J. Neutralization breadth of SARS-CoV-2 viral variants following primary series and booster SARS-CoV-2 vaccines in patients with cancer. Cancer Cell 2022, 40, 103–108. [Google Scholar] [CrossRef]
- Furukawa, K.; Tjan, L.H.; Kurahashi, Y.; Sutandhio, S.; Nishimura, M.; Arii, J.; Mori, Y. Assessment of Neutralizing Antibody Response Against SARS-CoV-2 Variants After 2 to 3 Doses of the BNT162b2 mRNA COVID-19 Vaccine. JAMA Netw Open 2022, 5, e2210780. [Google Scholar] [CrossRef] [PubMed]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous Covid-19 Booster Vaccinations. N Engl J Med 2022, 386, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Pang, N.Y.; Pang, A.S.; Chow, V.T.; Wang, D.Y. Understanding neutralising antibodies against SARS-CoV-2 and their implications in clinical practice. Mil Med Res 2021, 8, 47. [Google Scholar] [CrossRef]
- Takheaw, N.; Liwsrisakun, C.; Chaiwong, W.; Laopajon, W.; Pata, S.; Inchai, J.; Duangjit, P.; Pothirat, C.; Bumroongkit, C.; Deesomchok, A.; et al. Correlation Analysis of Anti-SARS-CoV-2 RBD IgG and Neutralizing Antibody against SARS-CoV-2 Omicron Variants after Vaccination. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.; Tiu, C.; Hu, Z.; Chen, V.C.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat Biotechnol 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Santos da Silva, E.; Servais, J.Y.; Kohnen, M.; Arendt, V.; Staub, T.; The Con-Vince, C.; The CoVaLux, C.; Krüger, R.; Fagherazzi, G.; Wilmes, P.; et al. Validation of a SARS-CoV-2 Surrogate Neutralization Test Detecting Neutralizing Antibodies against the Major Variants of Concern. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090. [Google Scholar] [CrossRef]
- Eyre, D.W.; Lumley, S.F.; Wei, J.; Cox, S.; James, T.; Justice, A.; Jesuthasan, G.; O'Donnell, D.; Howarth, A.; Hatch, S.B.; et al. Quantitative SARS-CoV-2 anti-spike responses to Pfizer-BioNTech and Oxford-AstraZeneca vaccines by previous infection status. Clin Microbiol Infect 2021, 27, 1516–e1517. [Google Scholar] [CrossRef]
- Valanparambil, R.M.; Carlisle, J.; Linderman, S.L.; Akthar, A.; Millett, R.L.; Lai, L.; Chang, A.; McCook-Veal, A.A.; Switchenko, J.; Nasti, T.H.; et al. Antibody Response to COVID-19 mRNA Vaccine in Patients With Lung Cancer After Primary Immunization and Booster: Reactivity to the SARS-CoV-2 WT Virus and Omicron Variant. J Clin Oncol 2022, 40, 3808–3816. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.F.; Meng, W.; Chen, L.; Ding, L.; Feng, J.; Perez, J.; Ali, A.; Sun, S.; Liu, Z.; Huang, Y.; et al. Neutralizing antibodies to SARS-CoV-2 variants of concern including Delta and Omicron in subjects receiving mRNA-1273, BNT162b2, and Ad26.COV2.S vaccines. J Med Virol 2022, 94, 5678–5690. [Google Scholar] [CrossRef]
- Felip, E.; Pradenas, E.; Romeo, M.; Marfil, S.; Trinité, B.; Urrea, V.; Hernández, A.; Ballana, E.; Cucurull, M.; Mateu, L.; et al. Impact of chemotherapy and/or immunotherapy on neutralizing antibody response to SARS-CoV-2 mRNA-1237 vaccine in patients with solid tumors. Mol Oncol 2023, 17, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Grinshpun, A.; Rottenberg, Y.; Ben-Dov, I.Z.; Djian, E.; Wolf, D.G.; Kadouri, L. Serologic response to COVID-19 infection and/or vaccine in cancer patients on active treatment. ESMO Open 2021, 6, 100283. [Google Scholar] [CrossRef] [PubMed]
- Lyke, K.E.; Atmar, R.L.; Islas, C.D.; Posavad, C.M.; Szydlo, D.; Paul Chourdhury, R.; Deming, M.E.; Eaton, A.; Jackson, L.A.; Branche, A.R.; et al. Rapid decline in vaccine-boosted neutralizing antibodies against SARS-CoV-2 Omicron variant. Cell Rep Med 2022, 3, 100679. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.T.; La, J.; Branch-Elliman, W.; Huhmann, L.B.; Han, S.S.; Parmigiani, G.; Tuck, D.P.; Brophy, M.T.; Do, N.V.; Lin, A.Y.; et al. Association of COVID-19 Vaccination With SARS-CoV-2 Infection in Patients With Cancer: A US Nationwide Veterans Affairs Study. JAMA Oncol 2022, 8, 281–286. [Google Scholar] [CrossRef]
- De Placido, P.; Pietroluongo, E.; De Angelis, C.; Tafuro, M.; Barraco, C.; Giannatiempo, R.; Buonaiuto, R.; Schettini, F.; Iervolino, A.; Vozzella, E.A.; et al. Safety and immunogenicity of the COVID-19 vaccine BNT162b2 for patients with breast and gynecological cancer on active anticancer therapy: Results of a prospective observational study. Front Oncol 2022, 12, 951026. [Google Scholar] [CrossRef]
- Lau, D.K.; Aresu, M.; Planche, T.; Tran, A.; Lazaro-Alcausi, R.; Duncan, J.; Kidd, S.; Cromarty, S.; Begum, R.; Rana, I.; et al. SARS-CoV-2 Vaccine Immunogenicity in Patients with Gastrointestinal Cancer Receiving Systemic Anti-Cancer Therapy. Oncologist 2023, 28, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: a prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, F.; Angelidakis, G.; Feldman, A.; Ravi, V.; Woodman, E.; Bhatti, M.; Ariza-Heredia, E.; Elhajj, P.; Spallone, A.; Jiang, Y.; Chemaly, R.F. COVID-19 in cancer patients: The impact of vaccination on outcomes early in the pandemic. Cancer Med 2023, 12, 22006–22022. [Google Scholar] [CrossRef]
- Luangdilok, S.; Wanchaijiraboon, P.; Pakvisal, N.; Susiriwatananont, T.; Zungsontiporn, N.; Sriuranpong, V.; Sainamthip, P.; Suntronwong, N.; Vichaiwattana, P.; Wanlapakorn, N.; et al. Immunogenicity after a Third COVID-19 mRNA Booster in Solid Cancer Patients Who Previously Received the Primary Heterologous CoronaVac/ChAdOx1 Vaccine. Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Mondaca, S.; Walbaum, B.; Le Corre, N.; Ferrés, M.; Valdés, A.; Martínez-Valdebenito, C.; Ruiz-Tagle, C.; Macanas-Pirard, P.; Ross, P.; Cisternas, B.; et al. Influence of SARS-CoV-2 mRNA Vaccine Booster among Cancer Patients on Active Treatment Previously Immunized with Inactivated versus mRNA Vaccines: A Prospective Cohort Study. Vaccines (Basel) 2023, 11. [Google Scholar] [CrossRef]
- Chi, W.Y.; Li, Y.D.; Huang, H.C.; Chan, T.E.H.; Chow, S.Y.; Su, J.H.; Ferrall, L.; Hung, C.F.; Wu, T.C. COVID-19 vaccine update: vaccine effectiveness, SARS-CoV-2 variants, boosters, adverse effects, and immune correlates of protection. J Biomed Sci 2022, 29, 82. [Google Scholar] [CrossRef] [PubMed]
- Kaku, C.I.; Champney, E.R.; Normark, J.; Garcia, M.; Johnson, C.E.; Ahlm, C.; Christ, W.; Sakharkar, M.; Ackerman, M.E.; Klingström, J.; et al. Broad anti-SARS-CoV-2 antibody immunity induced by heterologous ChAdOx1/mRNA-1273 vaccination. Science 2022, 375, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Pozzetto, B.; Legros, V.; Djebali, S.; Barateau, V.; Guibert, N.; Villard, M.; Peyrot, L.; Allatif, O.; Fassier, J.B.; Massardier-Pilonchéry, A.; et al. Immunogenicity and efficacy of heterologous ChAdOx1-BNT162b2 vaccination. Nature 2021, 600, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Vasilev, G.; Kabakchieva, P.; Miteva, D.; Batselova, H.; Velikova, T. Effectiveness and safety of COVID-19 vaccines in patients with diabetes as a factor for vaccine hesitancy. World J Diabetes 2022, 13, 738–751. [Google Scholar] [CrossRef]
- He, Y.F.; Ouyang, J.; Hu, X.D.; Wu, N.; Jiang, Z.G.; Bian, N.; Wang, J. Correlation between COVID-19 vaccination and diabetes mellitus: A systematic review. World J Diabetes 2023, 14, 892–918. [Google Scholar] [CrossRef]
Table 1.
Baseline demographic and disease characteristics.
| Characteristics | All (n = 91) |
Non-Chemotherapy (n = 50) |
Chemotherapy (n = 41) |
p-Value |
|---|---|---|---|---|
| Sex, n (%) | ||||
| Male | 45 (49.45%) | 19 (38.00%) | 26 (63.41%) | 0.016 |
| Female | 46 (50.55%) | 31 (62.00%) | 15 (36.59%) | |
| Age, years, mean ± SD | 60.76 ± 11.78 | 59.48 ± 12.16 | 62.48 ± 11.62 | 0.234 |
| BMI, mean ± SD | 23.44 ± 4.48 | 23.21 ± 4.29 (n = 48) | 23.50 ± 4.76 | 0.843 |
| Smoking, n (%) | 19 (20.88%) | 7 (14.00%) | 12 (29.27%) | 0.075 |
| Primary cancer, n (%) | ||||
| GI | 32 (35.16%) | 11 (22.00%) | 21 (51.22%) | 0.004 |
| HBP | 15 (16.58%) | 8 (16.00%) | 7 (17.07%) | 0.891 |
| Breast | 25 (27.47%) | 20 (40.00%) | 5 (12.20%) | 0.003 |
| Prostate | 5 (5.49%) | 2 (4.00%) | 3 (7.32%) | 0.490 |
| GU | 5 (5.49%) | 4 (8.00%) | 1 (2.44%) | 0.247 |
| others | 9 (9.89%) | 5 (10.00%) | 4 (9.76%) | 0.969 |
| Metastatic disease, n (%) | 44 (48.35%) | 17 (34.00%) | 27 (65.85%) | 0.002 |
| Comorbid, n (%) | ||||
| DM | 17 (18.68%) | 9 (18.00%) | 8 (19.51%) | 0.854 |
| HT | 34 (37.46%) | 15 (30.00%) | 19 (46.34%) | 0.109 |
| Other | 40 (43.96%) | 20 (40.00%) | 20 (48.78%) | 0.401 |
| Vaccines, n (%) | ||||
| RNA+RNA | 41 (45.05%) | 21 (42.00%) | 20 (48.78%) | 0.518 |
| nonRNA+RNA | 19 (20.88%) | 12 (24.00%) | 7 (17.07%) | 0.419 |
| nonRNA+nonRNA | 31 (34.07%) | 17 (34.00%) | 14 (34.15%) | 0.988 |
| Third vaccine booster | 21 (23.08%) | 12 (24.00%) | 9 (21.95%) | 0.817 |
| WBC | 6158 (±2461) 5985, 4400, 7280 |
6637 (±2544) 6270, 4730, 7540 |
5679 (±2317) 5040, 4160, 6350 |
0.613 0.085 |
| Neutrophil count | 3557 (±1847) 3085, 2430, 4190 |
3824 (±2034) 3560, 2520, 4190 |
3290 (±1627) 2840, 2300, 4560 |
0.227 0.231 |
| Lymphocyte count | 1853 (±1024) 1720, 1210, 2270 |
2124 (±1227) 1870, 1370, 2570 |
1582 (±689) 1490, 950, 1910 |
0.002 0.057 |
| Hematologic AE during F/U | ||||
| Leukopenia | 15 (24.19%) | 4 (12.9%) | 11 (35.48%) | 0.038 |
| Neutropenia | 5 (8.06%) | 0 | 5 (16.13%) | 0.020 |
| Lymphopenia | 20 (32.26%) | 7 (22.58%) | 13 (41.94%) | 0.103 |
Table 4.
Comparison between chemotherapy and non-chemotherapy group.
| Neutralizing Antibody | Group | Baseline | Day 28 | Month 6 |
p-Value (Month 6 vs Day 28) |
|
|---|---|---|---|---|---|---|
| Percent Inhibition(wild type) | Non-chemotherapy | N | 48 | 50 | 45 | |
| Mean (95% CI) | 6.28 (4.87 – 7.69) | 62.63 (53.13 – 72.12) | 69.73 (59.95 – 79.51) | 0.170 | ||
| Chemotherapy | N | 41 | 41 | 35 | ||
| Mean (95% CI) | 5.24 (4.01 – 6.47) | 61.79 (50.79 – 72.78) | 67.31 (56.17 – 78.44) | 0.254 | ||
| p-Value (chemo vs non-chemo) | 0.907 | 0.791 | ||||
| Total | N | 89 | 91 | 80 | ||
| Mean (95% CI) | 5.80 (4.86 – 6.74) | 62.25 (55.19 – 69.30) | 68.67 (61.48 – 75.86) | 0.074 | ||
| Percent Inhibition(Omicron variant) | Non-chemotherapy | N | 48 | 50 | 45 | |
| Mean (95% CI) | 10.63 (8.72 – 12.54) | 43.87 (36.59 – 51.16) | 52.29 (42.99 – 61.60) | 0.052 | ||
| Chemotherapy | N | 41 | 41 | 35 | ||
| Mean (95% CI) | 7.26 (5.45 – 9.07) | 40.09 (32.19 – 47.99) | 42.88 (32.99 – 52.77) | 0.512 | ||
| p-Value (chemo vs non-chemo) | 0.476 | 0.180 | ||||
| Total | N | 89 | 91 | 80 | ||
| Mean (95% CI) | 9.08 (7.73 – 10.42) | 42.17 (36.90 – 47.44) | 48.18 (41.45 – 54.90) | 0.061 | ||
| Seroconversion(wild type) | Non-chemotherapy | N | 48 | 50 | 45 | |
| Mean (95% CI) | 0 (0 – 0.07) | 0.78 (0.64 – 0.88) | 0.80 (0.65 – 0.90) | 0.778 | ||
| Chemotherapy | N | 41 | 41 | 35 | ||
| Mean (95% CI) | 0 (0 – 0.09) | 0.76 (0.60 – 0.88) | 0.83 (0.66 – 0.93) | 0.236 | ||
| p-Value (chemo vs non-chemo) | 0.789 | 0.743 | ||||
| Total | N | 89 | 91 | 80 | ||
| Mean (95% CI) | 0 (0 – 0.04) | 0.77 (0.67 – 0.85) | 0.81 (0.71 – 0.89) | 0.365 | ||
| Seroconversion(Omicron variant) | Non-chemotherapy | N | 48 | 50 | 45 | |
| Mean (95% CI) | 0 (0 – 0.07) | 0.64 (0.49 – 0.77) | 0.71 (0.56 – 0.84) | 0.316 | ||
| Chemotherapy | N | 41 | 41 | 35 | ||
| Mean (95% CI) | 0 (0 – 0.09) | 0.59 (0.42 – 0.74) | 0.60 (0.42 – 0.76) | 0.875 | ||
| p-Value (chemo vs non-chemo) | 0.597 | 0.311 | ||||
| Total | N | 89 | 91 | 80 | ||
| Mean (95% CI) | 0 (0 – 0.04) | 0.62 (0.51 – 0.72) | 0.66 (0.55 – 0.76) | 0.420 | ||
Table 5.
Comparison between wild type and Omicron variant.
| Strain | Baseline | Day 28 | Month 6 | ||
|---|---|---|---|---|---|
| Percent Inhibition (non-chemotherapy) |
Wild type | N | 48 | 50 | 45 |
| Mean (95% CI) | 6.28 (4.87 – 7.69) | 62.63 (53.13 – 72.12) | 69.73 (59.95 – 79.51) | ||
| Omicron variant | N | 48 | 50 | 45 | |
| Mean (95% CI) | 10.63 (8.72 – 12.54) | 43.87 (36.59 – 51.16) | 52.29 (42.99 – 61.60) | ||
| Wild vs Omicron, p-Value | 0.000 | 0.000 | |||
| Percent Inhibition (chemotherapy) |
Wild type | N | 41 | 41 | 35 |
| Mean (95% CI) | 5.24 (4.01 – 6.47) | 61.79 (50.79 – 72.78) | 67.31 (56.17 – 78.44) | ||
| Omicron variant | N | 41 | 41 | 35 | |
| Mean (95% CI) | 7.26 (5.45 – 9.07) | 40.09 (32.19 – 47.99) | 42.88 (32.99 – 52.77) | ||
| Wild vs Omicron, p-Value | 0.000 | 0.000 | |||
| Seroconversion (non-chemotherapy) |
Wild type | N | 48 | 50 | 45 |
| Mean (95% CI) | 0 (0 – 0.07) | 0.78 (0.64 – 0.88) | 0.80 (0.65 – 0.90) | ||
| Omicron variant | N | 48 | 50 | 45 | |
| Mean (95% CI) | 0 (0 – 0.07) | 0.64 (0.49 – 0.77) | 0.71 (0.56 – 0.84) | ||
| Wild vs Omicron, p-Value | 0.008 | 0.103 | |||
| Seroconversion (chemotherapy |
Wild type | N | 41 | 41 | 35 |
| Mean (95% CI) | 0 (0 – 0.09) | 0.76 (0.60 – 0.88) | 0.83 (0.66 – 0.93) | ||
| Omicron variant | N | 41 | 41 | 35 | |
| Mean (95% CI) | 0 (0 – 0.09) | 0.59 (0.42 – 0.74) | 0.60 (0.42 – 0.76) | ||
| Wild vs Omicron, p-Value | 0.008 | 0.005 | |||
Table 2.
Vaccine regimens.
| Company | Vaccine Platform | |
|---|---|---|
| Non-mRNA vaccines | ||
| AZD1222, ChAdOx1 nCoV-19 | AstraZeneca | Replication-deficient chimpanzee adenoviral vector |
| CoronaVac, SinoVac | Sinovac Biotech | Whole inactivated virus |
| BBIBP-CorV, BIBP vaccine | Sinopharm | Whole inactivated virus |
| mRNA vaccine | ||
| BTN162b2, Comirnaty | Pfizer–BioNTech | nucleoside-modified mRNA |
| mRNA-1273, Spikevax | Moderna | nucleoside-modified mRNA |
Table 3.
Vaccine combinations.
| All (91) | Non-Chemotherapy (50) | Chemotherapy (41) | |
|---|---|---|---|
| mRNA + mRNA | 41 | 21 | 20 |
| Pfizer+ Pfizer | 21 | 8 | 13 |
| Moderna+ Moderna | 19 | 12 | 7 |
| Others | 1 | 1 | 0 |
| Non-mRNA+ mRNA | 19 | 12 | 7 |
| Astrazeneca+Pfizer | 18 | 11 | 7 |
| Others | 1 | 1 | 0 |
| Non-mRNA+ non-mRNA | 31 | 17 | 14 |
| Sinopharm + Sinopharm | 17 | 12 | 5 |
| Sinovac + Astrazeneca | 9 | 4 | 5 |
| Astrzeneca + Astrazeneca | 3 | 0 | 3 |
| Others | 2 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



