
Submitted:
11 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
Background: Sexual dysfunction is the most common side effect encountered by cervical cancer patients during and after treatment, and rehabilitation strategies are needed to improve their quality of life. A variety of rehabilitation strategies have been reported in previous studies, varying by country, race and even continent. However, the common rehabilitation strategies used by cervical cancer survivors in Tanzania and their outcomes are unknown. The study aimed to unfold sexual rehabilitation strategies and outcome practiced by cervical cancer survivors who experienced sexual dysfunction during and after treatment in North-western Tanzania. Methods: Descriptive qualitative study were employed. Phenomenology study design used with a sample of 7 participants and data corrected via in-depth interview guided by 11 questions. Audiotaped and transcribed to get main themes and sub themes through deductive analysis. Results: Most participants reported inability to achieve an orgasm and low libido and dyspareunia after treatment. Most participants were eagerly to have their sexual activity recovered. However, they were not familiar with any rehabilitation strategy after the experience of sexual dysfunction. Even though, some of the participants attempted various interventions, but all were unsatisfactory leading to a significant decline in sexual interest and activity. Conclusion: Cervical cancer survivors are not familiar with any sexual rehabilitation strategies. Health education concerning various sexual rehabilitation strategies should be provided to survivors during and even after treatment.
Keywords:
cervical cancer
; cervical cancer survivors
; rehabilitation
; sexual dysfunction
; sexual rehabilitationtrategies
Introduction
Cervical cancer is a deadly disease associated with poor quality of life (QoL) and continues to lost lives of many women globally, requiring urgent intervention. GLOBOCAN estimates that about more than 600000 new cases of cervical cancer and more than 300000 deaths are reported globally each year (Bray et al., 2018; Vu et al., 2018). Africa, which in 2020 has the highest incidence (117,316 new cases) and highest mortality (76,745 deaths), is projected to increase by 85.6 percent, respectively, in 2040 (Sung et al., 2021). Even though the treatment modalities of cervical cancer is increasing globally, the quality of life among patients during and post-treatment remains poor due to treatment side effects(Sung et al., 2021). There has been increasing discussion in literature review pointing out that addressing specific treatment related side effects as a key approach to improving quality of life among cervical cancer survivors(Fakunle & Maree, 2019).
Health sexual activity is one of the vital entity affecting QoL of adults, regardless of their medical condition. Previous studies have shown that sexual activity is the strongest contributors to the variance of overall QoL in adults, it is one of the most fundamental and complex experiences that is often profoundly affected during cancer treatment. A study conducted in Indonesia by (Afiyanti et al., 2019) shows that sexual related problems are the major problems that affect the quality of life (Afiyanti et al., 2019). Another study conducted in Europe reported that lack of lubrication and a significant decrease in sexual interest and activity after treatment are commonly reported (Lammerink et al., 2012).
Implementing sexual rehabilitation interventions for cervical cancer survivors is crucial for improving their quality of life, especially considering the common treatment side effects reported among African women post-treatment (Fakunle & Maree, 2019; Greenwald & McCorkle, 2008; Zeng et al., 2011). Studies have highlighted the importance of addressing sexual dysfunction in survivors, as sexual activity plays a significant role in enhancing quality of life and overall survival outcomes (Vermeer et al., 2015). In Tanzania, where many cervical cancer patients are diagnosed at advanced stages, interventions targeting sexual-related issues are seen as vital for enhancing both quality of life and overall survival (Khalil et al., 2015).
Implementing sexual rehabilitation interventions to cervical cancer survivors is crucial to improving their quality of life. Sexual activity plays a key role in improving QoL and overall survival outcomes in patients with cervical cancer (Sanchez Varela et al., 2013). Since most cervical cancer patients in Tanzania are diagnosed at an advanced stage, interventions aimed at addressing their sexual related problems including issues such as vaginal dryness, pain during intercourse, and decreased sexual interest (Fakunle & Maree, 2019; Zeng et al., 2011) are considered to contribute significantly to improving their QoL and Overall survival.
Psychological issues like self-image disturbance and reduced marital intimacy are also commonly reported among cervical cancer survivors, emphasizing the need for comprehensive rehabilitation interventions (Lee, 2006). Furthermore, the impact of cervical cancer on survivors' quality of life and sexuality has been studied extensively, with findings indicating that despite improvements in treatments and survival rates, survivors still experience side effects that affect their well-(Afiyanti et al., 2016, 2019). Addressing sexual concerns through nursing care interventions has been shown to be effective in reducing sexual dysfunction among cervical cancer survivors.
Cervical cancer survivors often face challenges related to their quality of life, with sexual dysfunction being a common issue post-treatment. Studies have shown that rehabilitation interventions are crucial to address these challenges and improve the well-being of survivors (Pfaendler et al., 2015). Research indicates that the rehabilitation strategies utilized by survivors can vary based on factors such as age, country, and continent, with a noted gap in research from developing countries like Tanzania (Corkum et al., 2013).
Factors associated with poor quality of life among cervical cancer survivors include depression, anxiety, sleep disorders, and the impact of antineoplastic agents on survivors' well-being (Afiyanti et al., 2019; Osann et al., 2014)
Additionally, cervical cancer survivors are at an increased risk of developing subsequent tobacco-related malignancies compared to survivors of other cancers like breast and colorectal cancer (Underwood et al., 2012). Psychological distress and quality of life in cervical cancer survivors are influenced by various factors such as the type of radiotherapy, disease stage, and self-esteem (Kobayashi et al., 2009). Furthermore, interventions involving counselling and rehabilitation for sexual function are recommended for survivors, especially after radiotherapy (Harding et al., 2014).
Previous studies have shown that cervical cancer survivors use different Poor quality of life is commonly reported in cervical cancer survivors during and after treatment. Treatment related side effects particularly sexual dysfunctions commonly reported in Cervical cancer survivor is attributed as the most cause of the situation, and rehabilitation interventions are needed to improve their quality of life. rehabilitation strategies to try to restore their impaired sexual activity (Afiyanti et al., 2019). Interestingly studies has shown that the rehabilitation strategies used by patients vary by age, country and continent However ,most of the studies come from developed countries and there is no or limited research in developing countries such as Tanzania (Sanchez Varela et al., 2013). Therefore, this study explored sexual rehabilitation strategies practiced by cervical cancer survivors attending clinic at BMC.
Methods and Materials
Study Area
The study was conducted at Bugando Medical Centre, serving the North-western population. BMC is the only hospital in the North-western, which provide cancer screening and treatment. It is situated at Nyamagana District Mwanza Tanzania.
Study Design
This is the descriptive qualitative study employing a phenomenology study design to explore sexual rehabilitation strategies and outcomes among cervical cancer patients who experienced sexual dysfunction during or after treatment.
Study Population
The study population was including all women diagnosed with cervical cancer receiving or completed treatment at the time of data collection, inclusion and exclusion criteria were considered.
Selection Criteria
Women aged 18 years and above, diagnosed with cervical cancer undergoing treatment or have completed treatment and experienced sexual dysfunction. Cervical cancer patients with mental illness and those who are critically sick was excluded from the study.
Sample Size
Sample size depended on a reaching saturation point for the focus group formed and individuals In-depth interview (IDS). The Focus Group Discussion(FGD) was conducted with small group discussion of participants so that the ‘deep, case oriented analysis’ can be attained (around 5-7 participants in homogenous groups) additional interview were conducted as needed to pursue relevant theme as they emerge to allow the unfolding sexual rehabilitation strategies and outcomes(Maxwell, 2012).
Sampling Procedure
Purposive sampling procedure approach were used to explore sexual rehabilitative strategies and outcome.
Data Collection Procedure
Interview and focus group discussion were used to explore information about sexual rehabilitative strategies and outcome among cervical cancer patients via asking questions, listening answers from an individual or group on a structured, semi-structured or unstructured format and using interactive session.
Data analysis and Statistical Analysis
Deductive approach by using research questions to group the data and then look for similarities and differences, also inductive approach by using emergent framework to group the data then look for relationship followed by organizing the data, identifying framework, sorting data into framework, using the framework for descriptive analysis, second order analysis.
Ethical Consideration
Ethical clearance sought from CUHAS Research ethics and review committee(CREC) certificate no. 2207/2021. Permission to conduct this study were sought from Director General of Bugando medical Center(BMC) with ref: AB.286/317/01, informed consent obtained from each participant. Confidentiality was ensured to all participants.
Results
Response Rate
The participant’s expected to respond in this study were 7 the participant who responded to this study was equal to required sample size. Therefore, the response rate was 100%.
Participant’s Demographic Characteristics
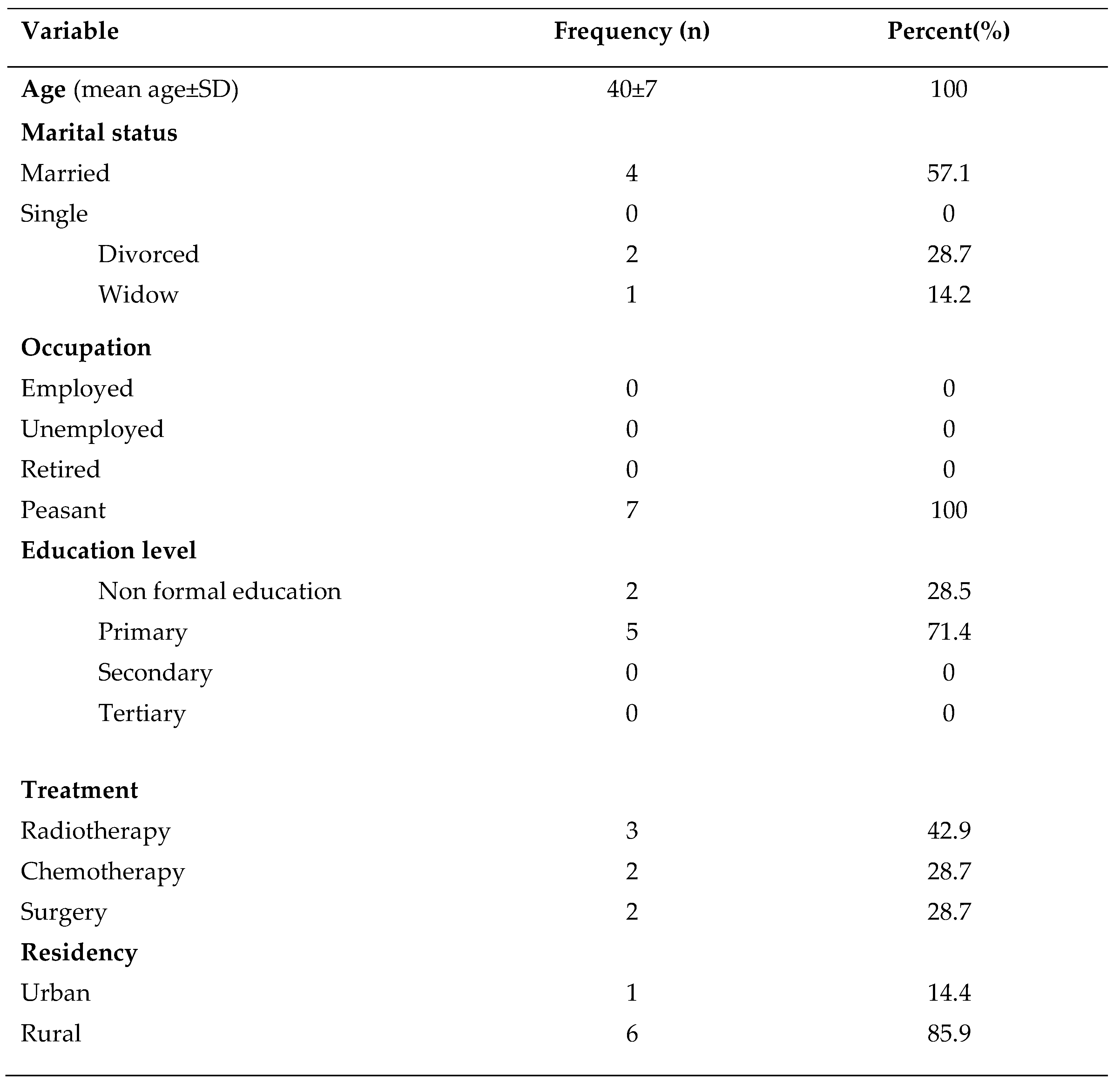
A total of 7 cervical cancer patients were included in the study, where majority of them were from the age groups of 40-55(71.4%), married4(57.1%), peasants 7(100%), from rural areas 6(85.9%), Sukuma in tribes 3(42.9) and divorced 4(57.1%).

Table 1.
Participants’ demographic characteristics.
Main Themes and Sub-Themes
Characterizing Sexual Dysfunction
Decreased libido as a result of relationship duration, age or sexuality having less important and this accompanied with decreased interest in sex since they started their treatment as portrayed by participant 3
‘since I see signs of cervical cancer my libido and sexual interest has dropped’.
Participants started having painful sexual intercourse or mentioned experiencing an anxiety of pain or penetration irrespective of actual experience of pain. Anxiety of pain made participant avoid sexual intercourse due to having feeling of painful sexual intercourse during sexual activity
‘I feel much pain when we are doing sexual intercourse with my partner’.
Some women experience changes in their body that lead to negatively body images or feelings of insecurities a quote from participant ‘I have treated with external radiation but I see some bruises and my skin colour has changed to the site’. Although it was not of the interview guide, 2 participants mentioned human papillomavirus as a cause of disease or as a reason to be fearful resuming sexual intercourse quote from the participant
‘They told me that males are not vulnerable to human papilloma virus but they may carry the virus and transmit to another partner during unprotected sexual intercourse.’
Consequences of Sexual Dysfunction
Sexual violence, participants reported to engage in sexual act without their consent especially when they are in treatment regime for cervical cancer. Patients are forced to do sexual intercourse regards to pain experience during the sexual activity. A quote from participant.
‘My husband forces me to do sexual intercourse even when am sick, kindly I found accepting him for the fear of being betrayed with him if he ends up unsatisfied’
Psychological violence, a course of behaviour performed by husbands of the participants where they insulted verbally with defamation. (Quote from participant 6)
‘my husband has a series of insulting me verbally since I diagnosed with cervical cancer’.
Economic violence, cervical cancer survivors are restricted to access different financial resources like engaging in entrepreneurship activities, a quote from the participant.
‘My husband restricted me to do any business, he told me that my responsibility is to take care of children’s’.
Participants complaining to lack financial support from their partners during the treatment period. The responsibility shifted to their relatives so as to care them. Quote from participant1
‘Only my relatives who are taking care of me and they are paying my treatment cost, my partner told me that he has no money for paying any hospital cost’. Participant 3 ‘My husband told me that only my relatives are responsible for taking care of me during illness’.
Intimate partner violence, both current and former partner being in an intimate relationship with other spouses since diagnosed with cervical cancer because of sexual satisfaction. Patients complained being dismissed as a result of disease. A quote from participants
‘since I diagnosed with cervical cancer my husband divorced me, he left me and he married another partner’. Participant7 ‘what I think my husband is in another intimate relationship but he deceives me that his absence at home is because of searching money’.
Sexual Rehabilitation Strategies
Participants used abstinence from sexual intercourse as one of the commonest rehabilitative method as quoted from participant 5
‘I don’t want to do sexual intercourse now until my doctor confirm to me that am now free from disease’
Majority testified that avoidance from sexual intercourse has poor outcomes after resuming their sexual activity. Others feeling inhibited during sexual intercourse also the use of analgesics such as ibuprofen testified by all cervical cancer patients as a common rehabilitative method during painful intercourse.
Cervical cancer patients used to watch television and gospel songs as a building block for them for sexual their sexual intimacy a quote from participant 3 ‘myself I used to watch TV, listening gospel songs, watching movies and attending to services for worshipping God as a way to resume sexual desire’. However, others reported that if their partner will honour them and take care of them their desire will be retained well as quoted from participant 2
“What I want from my husband is to have sincere love to me, to honour me as his only wife and to take care of me”.
Sexual Rehabilitation Outcomes
Some participant says that sexual intercourse abstinence brought poor outcome to them after resuming to sexual intercourse. Participant 6
‘after I completed six months since from treatments, I started doing sexual intercourse with my partner surprisingly massive bleeding resumed as usual’.
Partners intimate shown a positive response in cervical cancer survivors prognosis where many participants desired a close relationship from their partners’. Participants need to be loved, honoured and given a dignities care from their husband for them to resume in normal sexual functioning and this brought a good outcome.
Discussion
Oncologist has focused their efforts on maximizing the overall survival of cervical cancer patients. Even if there is general acknowledgement that sexual rehabilitative strategies are important aspect of patient care. There is an increasing interest to evaluate and improve sexual rehabilitative strategies and quality of life among cervical cancer survivors.
When comparing the general information of our study participants involving cervical cancer survivors, sample seems to be typical in terms of age with the majority being younger than 50 years. However, the mean age of sample being 40.5 was younger than the mean age of 50 found Similar to our study, the study conducted in the west cape by (du Toit & Kidd, 2015) where larger percentage of women were married and widowed.
In this study provided evidence that the majority of the women (85.7%) were sexually active with low libido during four weeks since they started treatment, this high percentage supported by study conducted by (Tangjitgamol et al., 2007) Other reported that activity decreased during the commencement of treatment. Finding from this study provided further evidence that pain experienced during sexual activity after treatment persisted with high level of pain and low improvement as time going on (Tangjitgamol et al., 2007).
More than 85% of cervical cancer women experienced pain and irritation to the vagina after chemo-radiation similar to the study conducted by Jensen (Gordon et al., 2003). Persistent of pain to the changes in vagina resulting from vaginal bleeding and reduction in lubrication as shown by more than half of cervical cancer survivors similar to other studies. As portrayed in current study satisfaction was least affected to explain the fact that women have a tendency to adapt to sexual relations as they wish to please their partners even if they have little or no desires(Gordon et al., 2003).
Limitation of the Study
Participants’ incorrect information’s may have led to erroneous conclusions.
Conclusions
The sexual rehabilitation needs of cervical cancer survivors during and after treatment remain unmet. Survivors are not familiar with any sexual recovery strategies. Health care providers should inform the patients various sexual rehabilitation strategies during and even after treatment.
Recommendations
All health care providers should provide scientific sexual rehabilitative strategies to all cervical cancer survivors during and after treatment as many participants required approved sexual rehabilitative strategies. Health education should be given to cervical cancer survivors on how to handle sexual experiences and sexual rehabilitative strategies during and after treatment. More studies about sexual rehabilitative strategies should be conducted in North-western Tanzania in order to answer all contradicting questions from the cervical cancer survivors concerning sexual rehabilitative strategies and outcomes.
Funding
No funding.
Conflicts of Interest
Author declares there is no conflict of interest.
Abbreviations
QoL-Quality of Life;.
References
- Afiyanti, Y., Rachmawati, I. N., & Milanti, A. (2016). Evaluating sexual nursing care intervention for reducing sexual dysfunction in Indonesian cervical cancer survivors. Asia-Pacific Journal of Oncology Nursing, 3(3), 266–271. [CrossRef]
- Afiyanti, Y., Wardani, I. Y., & Martha, E. (2019). The Quality of Life of Women with Cervical Cancer in Indonesia: A Cross-Sectional Study. Nurse Media Journal of Nursing, 9(2), 128–140. [CrossRef]
- Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians, 68(6), 394–424. [CrossRef]
- Corkum, M., Hayden, J. A., Kephart, G., Urquhart, R., Schlievert, C., & Porter, G. (2013). Screening for new primary cancers in cancer survivors compared to non-cancer controls: A systematic review and meta-analysis. Journal of Cancer Survivorship, 7(3), 455–463. [CrossRef]
- du Toit, G. C., & Kidd, M. (2015). Prospective quality of life study of South African women undergoing treatment for advanced-stage cervical cancer. Clinical Therapeutics, 37(10), 2324–2331. [CrossRef]
- Fakunle, I. E., & Maree, J. E. (2019). Sexual function in South African women treated for cervical cancer. International Journal of Africa Nursing Sciences, 10, 124–130. [CrossRef]
- Gordon, G. J., Jensen, R. V., Hsiao, L.-L., Gullans, S. R., Blumenstock, J. E., Richards, W. G., Jaklitsch, M. T., Sugarbaker, D. J., & Bueno, R. (2003). Using gene expression ratios to predict outcome among patients with mesothelioma. Journal of the National Cancer Institute, 95(8), 598–605. [CrossRef]
- Greenwald, H. P., & McCorkle, R. (2008). Sexuality and Sexual Function in Long-Term Survivors of Cervical Cancer. Journal of Women’s Health, 17(6), 955–963. [CrossRef]
- Harding, Y., Ooyama, T., Nakamoto, T., Wakayama, A., Kudaka, W., Inamine, M., Nagai, Y., Ueda, S., & Aoki, Y. (2014). Radiotherapy- or Radical Surgery–Induced Female Sexual Morbidity in Stages IB and II Cervical Cancer. International Journal of Gynecologic Cancer, 24(4). [CrossRef]
- Kobayashi, M., Ohno, T., Noguchi, W., Matsuda, A., Matsushima, E., Kato, S., & Tsujii, H. (2009). Psychological Distress and Quality of Life in Cervical Cancer Survivors After Radiotherapy: Do Treatment Modalities, Disease Stage, and Self-esteem Influence Outcomes? International Journal of Gynecologic Cancer, 19(7). [CrossRef]
- Lammerink, E. A. G., de Bock, G. H., Pras, E., Reyners, A. K. L., & Mourits, M. J. E. (2012). Sexual functioning of cervical cancer survivors: A review with a female perspective. Maturitas, 72(4), 296–304. [CrossRef]
- Lee, R. T.-T. (2006). Nurses’ Perceptions of Their Documentation Experiences in a Computerized Nursing Care Planning System. Journal of Clinical Nursing. [CrossRef]
- Maxwell, J. (2012). Qualitative Research Design: An Interactive Approach / J.A. Maxwell.
- Osann, K., Hsieh, S., Nelson, E. L., Monk, B. J., Chase, D., Cella, D., & Wenzel, L. (2014). Factors associated with poor quality of life among cervical cancer survivors: Implications for clinical care and clinical trials. Gynecologic Oncology, 135(2), 266–272. [CrossRef]
- Pfaendler, K. S., Wenzel, L., Mechanic, M. B., & Penner, K. R. (2015). Cervical Cancer Survivorship: Long-term Quality of Life and Social Support. Clinical Therapeutics, 37(1), 39–48. [CrossRef]
- Sanchez Varela, V., Zhou, E. S., & Bober, S. L. (2013). Management of sexual problems in cancer patients and survivors. Current Problems in Cancer, 37(6), 319–352. [CrossRef]
- Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., & Bray, F. (2021). Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians, 71(3), 209–249. [CrossRef]
- Tangjitgamol, S., Manusirivithaya, S., Hanprasertpong, J., Kasemsarn, P., Soonthornthum, T., Leelahakorn, S., Thawaramara, T., & Lapcharoen, O. (2007). Sexual dysfunction in Thai women with early-stage cervical cancer after radical hysterectomy. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 17(5), 1104–1112. [CrossRef]
- Underwood, J. M., Rim, S. H., Fairley, T. L., Tai, E., & Stewart, S. L. (2012). Cervical cancer survivors at increased risk of subsequent tobacco-related malignancies, United States 1992–2008. Cancer Causes & Control, 23(7), 1009–1016. [CrossRef]
- Vu, M., Yu, J., Awolude, O. A., & Chuang, L. (2018). Cervical cancer worldwide. Current Problems in Cancer, 42(5), 457–465. [CrossRef]
- Zeng, Y. C., Li, D., & Loke, A. Y. (2011). Life after cervical cancer: Quality of life among Chinese women. Nursing & Health Sciences, 13(3), 296–302. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



