
Submitted:
11 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
Background: Colorectal cancer (CRC) patients experienced multiple chemotoxicity affecting treatment compliance, survival, and quality of life (QOL). Prior research shows clinician-reported chemotoxicity (i.e., grading scales or diagnostic codes) predicts rehospitalization and cancer survival. However, a comprehensive synthesis of clinician-reported chemotoxicity is still lacking. Objectives: We conducted a systematic review and meta-analysis to determine the chemotoxicity's prevalence and risk factors in CRC. Methods: A systematic search from 2009 to 2024 yielded 30 studies for review, with 25 included in the meta-analysis. Results: Pooled prevalences of overall, non-hematological, and hematological moderate-to-severe toxicities were 45.7%, 39.2%, and 25.3%, respectively. The most common clinician-reported chemotoxicities were gastrointestinal (GI) toxicity (22.9%) and neuropathy or neutropenia (17.9%). Significant risk factors at baseline were malnutritional status, frailty, impaired immune or hepato-renal functions, short telomere lengths, low gut lactobacillus levels, age, female sex, aggressive chemotherapy, and low QOL. Age was associated with neutropenia (β: -1.44) and GI toxicity (β:1.85) (Ps 65 y.o.) had higher prevalences of overall (OR: 1.14) and GI (OR: 1.65) toxicities, but a lower prevalence of neutropenia (OR: 0.65) than younger adults (Ps
Keywords:
colorectal cancer
; chemotoxicity
; prevalence
; risk factors
; review
1. Introduction
Colorectal cancer (CRC) is the 4th most common type of cancer and the second leading cause of cancer-related deaths in the United States (U.S.) when men and women are combined [1,2]. By 2030, the number of new CRC cases is expected to reach around 170,968, marking a 17.3% increase from the total cases in 2020. Additionally, CRC is predicted to result in approximately 64,553 deaths, reflecting a 22.2% rise from 2020 [1,2]. CRC is frequently diagnosed in younger (age <50 years old) (average 20% of diagnoses in 2019) as well as in older patients, with nearly half of the cases being diagnosed in individuals who are 70 years old or older [3]. Among CRC patients, colon cancer is a primary diagnosis more than two-thirds of CRC patients are colon cancer patients [1,2]. While surgery is the primary modality of management for CRC in patients with non-metastatic disease (stages I-III), approximately 70% of CRC patients receive chemotherapy (Chemotherapy, primarily 5-fluorouracil [5-FU]-based agents) as the most common, standard adjuvant cancer treatment after undergoing CRC surgery [4,5,6].
Chemotherapy can enhance survival rates in both young-onset and older CRC patients, but it can also cause serious toxicities and exacerbate existing conditions [7]. CRC patients receiving chemotherapy frequently develop chemotoxicity, i.e., the harmful or adverse effects of chemotherapy drugs on healthy cells and tissues in the body and related side effects [7]. These toxicities are measured by both patients and clinicians, with a high incidence of severe events occurring within the first two months of treatment initiation and persisting for months or years [7]. Moreover, patient-reported outcomes highlight the enduring physical and psychosocial symptom distress and functional impairment faced by CRC patients receiving chemotherapy, all of which detrimentally affect health-related quality of life (HRQoL) [8].
Chemotoxicity varies across cancer types due to distinct pathological features and treatment approaches [9]. In CRC, gastrointestinal (GI) toxicity is particularly prevalent, largely because the treatments target tissues within the GI tract [5,10,11,12]. Between 50 and 80% of CRC patients with frequent and severe GI symptoms prior to or during chemotherapy experience persistent GI symptoms for months or even years post-chemotherapy [5,10,11,12]. Chemotherapeutic agents can induce a range of pro-inflammatory responses, leading to histopathological changes in the intestinal lining [13]. This inflammation can manifest as diarrhea, abdominal pain, nausea/vomiting, and bloating [13,14]. Moreover, the combination of surgery and radiation can exacerbate these symptoms [13]. Long-term intestinal injury may result in severe GI tract damage, such as strictures, stenosis with obstruction, fistulas, and bowel perforation, which are linked to systemic health problems like sepsis and malnutrition [15].
These toxicities are significant concerns in CRC, leading to dose reduction, increased mortality or recurrence rates, treatment non-compliance, emergency room visits, and hospitalization [5,12]. Early identification and management are key to allowing treatment to continue as planned or at a lower dose if required [9]. Therefore, when planning chemotherapy, weighing the potential risks against the benefits is crucial [5,12]. Understanding the major types and risk factors of chemotoxicity in CRC is necessary for effective management [16,17,18]. Several risk factors of chemotoxicity have been identified, such as patient and clinical factors (e.g., age, body mass index [BMI], and types and doses of chemotherapy) [7,19]. However, the results of current studies on chemotoxicity in CRC patients [7,16,17,18] have been mixed with several limitations, such as small sample sizes, varied measures, and differences in cancer sites, stages, chemotherapy types, and patient characteristics, which led to no definitive factors associated with chemotoxicity in CRC. These limitations underscore the need for a comprehensive understanding of chemotoxicity, particularly its types and potential risk factors in CRC patients.
Current studies on chemotoxicity in CRC mainly focus on patient-reported outcomes (PROs) [12,14] and cancer treatment outcomes (e.g., response rates, cancer death) [20,21,22]. In previous studies comparing adverse events between PROs versus clinician-reported outcomes (e.g., grading scales, diagnostic codes, or progress notes) in lung cancer [23], and mixed cancer types [24], patients generally reported symptoms earlier and more frequently than clinicians, had a higher incidence and severity of subjective toxicities, and had poor to modest agreement with clinician-reported values [23,24]. Previous studies have demonstrated that PROs were more strongly associated with daily health status (e.g., HRQoL, distress), while clinician-reported chemotoxicity was more strongly associated with future rehospitalization and survival [23,24]. However, the overall prevalence and associated risk factors of chemotoxicity assessed by clinicians remain unsynthesized, leading to inconclusive evidence [16,17,18].
A comprehensive assessment is needed to bridge research gaps and optimize chemotoxicity management in CRC, considering various approaches, including clinician-graded evaluations. To provide up-to-date overall consensus on clinician-reported chemotoxicity, this systematic review and meta-analysis aims to investigate the characteristics of chemotoxicity and quantitatively analyze the pooled prevalence of chemotoxicity (i.e., what types of chemotoxicity) according to clinician-reported assessments and the risk factors that predict their occurrence in CRC patients.
Conceptual Framework. This study's conceptual framework (Figure 1) is based on the Quality Health Outcomes Model [25]. This model incorporates numerous contextual factors that affect healthcare outcomes by proposing dynamic relationships between systems, patient characteristics, interventional components, and outcomes. In our conceptual framework [25], the patient characteristics include socio-demographic data, cancer clinical characteristics, and biomarkers. Examples of interventional components include risk prediction models, targeted chemotoxicity management, support, and coordination of care of patients and caregivers/families. Systemic characteristics encompass the awareness, knowledge, and skills of oncological medical professionals in chemotoxicity assessment, prevention, and management, as well as the clinician- and patient-reported chemotoxicity assessment system. The primary outcome is clinician-reported chemotoxicity (types and their prevalences). Among the four domains in this model, our study specifically investigated the “interventional components,” “patient characteristics,” as risk factors of chemotoxicity, and “primary outcomes: clinician-reported chemotoxicity.” Given the current study's findings, this conceptual framework allows for a comprehensive understanding of the factors influencing chemotoxicity and its potential interventions.
2. Materials and Methods
2.1. Search Strategies and Data Sources
Following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [26], we conducted a systematic review of the literature in order to integrate the findings of quantitative studies. Our review encompassed seven electronic databases: CINAHL, Medline via PubMed, Cochrane Library (Review and CENTRAL), EMBASE, PsycINFO, and Web of Science. The focus of our research was on the symptom experiences of CRC patients after receiving chemotherapy. Through the use of MeSH terms and manual searches, we examined keywords using Boolean operators (AND, OR) to construct the search strategies: ("colorectal cancer" OR “colon cancer” OR “rectal cancer” OR "CRC" OR "colorectal neoplasms" OR "colorectal adenocarcinoma") AND ("chemotherapy" OR "chemotoxicity" OR "chemotherapeutic agents" OR "antineoplastic agents") AND ("risk factors" OR “risk factors” OR "predictive models" OR "prognostic factors" OR "response prediction") AND (“symptom*” OR “adverse event*” “side effect*”). (details in the Supplementary Table 1). Additionally, we identified other relevant studies by reviewing the references cited in the obtained published studies. The full, reproducible search strategies for all included databases are located in Supplementary Table 1.
2.2. Inclusion and Exclusion Criteria
To be included in our review, studies had to meet the following criteria: (a) be published within the last 15 years, from January 2009 to March 2024, to reflect the most up-to-date evidence on a topic; (b) report chemotoxicity reported by clinicians after chemotherapy using quantitative measures; (c) examine patients with CRC receiving chemotherapy as a primary treatment, including but not limited to conventional chemotherapy regimens, targeted therapy, adjuvant or palliative chemotherapy (d) be based on original or experimental data; (e) examine patients who were 18 years or older and had CRC; and (f) be published in English.
Studies were excluded if they: (a) presented only qualitative results; (b) were not published in English; (c) were review papers, editorials, meta-syntheses, theory-based works, dissertations, or case studies; (d) patients-reported symptoms as primary outcomes; (e) reported only cancer survival rates; or (f) included CRC patients receiving radiotherapy or surgery as a primary treatment. We also reviewed and included eligible studies from the references of previous reviews, focusing on nutritional status and chemotoxicity in CRC [27,28]. There were no restrictions regarding the timing of chemotoxicity assessment after chemotherapy, whether during the recovery or long-term survivorship phases. This comprehensive approach ensured that all relevant literature was included in our review.
2.3. Study Selections and Screening
Two authors (CH and SM) independently evaluated the collected articles based on predetermined criteria, including examining titles, abstracts, and full-text articles. Any discrepancies were addressed through discussion.
2.4. Data Extraction and Data Synthesis
Data extraction involved the retrieval of variables from the included studies, such as publication year, study design, country of research, research setting, sample size, participant demographic and cancer-related clinical characteristics, methods of measuring chemotoxicity, risk factors for chemotoxicity, and any impact of chemotoxicity, as well as the primary results and conclusions of the studies. The first author extracted the data using standardized forms, which were then verified by the other authors for accuracy and completeness. Any discrepancies were resolved through consensus-building discussions with a third author. The extracted data was synthesized and presented using narrative descriptions and descriptive statistics.
2.5. Methodological Quality Appraisal
Two authors (CH and SM) evaluated the methodological integrity of each article using the Critical Appraisal Skills Program (CASP) checklists. These checklists — which include 12 questions for observational cohort studies and 11 questions for randomized controlled trials — aim to scrutinize the robustness of the research and the likelihood of bias from the investigator. Each question can be answered with “Yes,” “Can’t tell,” or “No.” However, there is no universally accepted standard for assessing an article’s quality using these checklists. We used a commonly applied arbitrary cut-off in critical appraisal, deeming an article as “high” quality if it satisfied at least 80% of the checklist criteria, “low” quality if it satisfied 50% or less, and “medium” quality if it satisfied more than 50% but less than 80% of the criteria. If the two authors could not agree, a third author provided arbitration (Supplementary Table 2).
2.6. Meta-Analytical and Statistical Methods
2.6.1. Publication bias
We examined funnel plots to visually assess the asymmetry of values of chemotoxicity prevalences (Begg’s test and Egger’s test to test the asymmetry statistically). Heterogeneity was assessed using Q statistics, which measure the squared variance. A p-value of less than 0.05 was considered statistically significant, indicating the presence of heterogeneity[29]. Additionally, I2 statistics were used to assess heterogeneity, with values below 25.0% indicating no heterogeneity and values above 75.0% indicating high or extreme heterogeneity[29]. Results from the random effects model were presented in our study for data with high heterogeneity.
2.6.2. Pooled Estimations.
A meta-analysis was conducted to combine data from multiple studies to obtain more accurate estimations of the prevalence (i.e., pooled prevalence) of chemotoxicity after chemotherapy and the relationships of risk factors with chemotherapy. This approach enhanced the statistical power compared to analyzing individual studies alone [30]. Only studies that provided information on the prevalence (percentage of research participants reporting at least moderate-to-severe toxicity during or after chemotherapy) with/without examining the risk factors of chemotoxicity were included in our meta-analysis. Furthermore, the pooled estimates for prevalence and/or associations between potential risk factors and chemotoxicity were only analyzed if they were present in at least two studies per type of chemotoxicity. The pooled prevalence of chemotoxicity was calculated by extracting proportions from all included studies, using weighted mean and standard errors to establish a 95% confidence interval (CI). Additionally, the pooled association between risk factors and chemotoxicity was determined using adjusted/unadjusted Beta coefficients or Odd Ratios (ORs) in meta-regressions or F statistics in a meta-analysis of variance (ANOVA) tests. Forest plots were utilized to present the pooled mean prevalences of chemotoxicity, and associations of risk factors with chemotoxicity, along with corresponding 95% CIs. Subgroup analyses were conducted per chemotoxicity subgroups (e.g., hematological, non-hematological, and GI toxicity). A two-sided p-value of less than 0.05 was considered statistically significant. For the meta-analysis, the statistical analyses, including funnel and forest plots, were conducted using Comprehensive Meta-Analysis (version 2.2.050; Biostat, Engelwood, NJ). Descriptive statistical analysis was performed using the Statistical Package for the Social Sciences version 23.0 (SPSS, Inc., Chicago, IL).
3. Results
3.1. Search Results and Methodological Quality Evaluation
The search methods resulted in 1,181 articles, excluding duplicates. A review of titles and abstracts narrowed it to 104 relevant studies, with 30 [7,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59] selected for final analysis after assessing full-text articles. Among 30 studies included in this review, 5 studies [37,38,39,43,48] were excluded from meta-analyses due to unavailable chemotoxicity prevalence data or data that was not comparable for inclusion in meta-analyses. Evaluation of the 30 quantitative studies using CASP tools is detailed in Supplementary Table 2. The inter-rater agreement between authors was 95.8%, and no studies were excluded for low quality. The literature search process is illustrated in Figure 2, and details for the 30 studies are provided in Tables 1AB and Supplementary Table 3.
3.2. Study Characteristics
The study characteristics reveal that among the 30 studies examined (Table 1AB), the majority of studies had observational cohort study designs (n = 24 for prospective study design [7,31,32,33,34,36,37,38,39,40,41,42,44,45,46,47,48,51,52,53,54,57,58,59], n = 5 for retrospective study design [35,43,49,55,56], while one study used a randomized control trial (RCT) [50].) Among 24 prospective studies, six studies [31,42,47,51,54,57] used longitudinal follow-up assessing chemotoxicity from baseline to after chemotherapy with multiple time points (at every cycle over 8 cycles [47,54]; at every 3 months over one year [51]; at every cycle over 12 cycles [31]; at weekly over a month [42]; at monthly over 3 months [57]) over the course of chemotherapy. The most common time point to assess chemotherapy was 6 months follow-up [7,35,39,49,50] throughout chemotherapy. None of the studies assessed chemotoxicity longer than 1 year follow-up. Studies were conducted across various countries, predominantly in Europe (studies n = 15 [7,32,33,34,35,36,39,40,41,48,50,51,52,53,54,59]), followed by Asia (studies n = 6 [45,47,49,55,57,58]) and United States (US) (studies n = 4 [37,38,43,44]). The sample sizes ranged from 2,691 [40] to 52 [33], and the sample sizes were between > 100 and < 500 in the majority of studies (n = 16). Among 30 studies, 24 studies [7,31,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,53,55,57] identified significant risk factors of chemotoxicity; 10 studies [31,33,37,39,40,43,46,48,49,50] examined the differences of chemotoxicity by categorical groups (i.e., high, versus low values) of risk factors; 11 studies reported odds ratios [ORs] [34,35,36,38,41,44,45,47,51,53,55,57]; and 2 studies [7,42] reported a Beta coefficient to present the associations of risk factors with chemotoxicity. Two studies found no significant risk factors of chemotoxicity [54,59], and four did not examine chemotoxicity risk factors [32,52,56,58].

Table 1.
A. Characteristics of Studies Included for Meta-Analysis (N = 25).
| Authors(year)/ Country |
Study Design | Cancer types | Samples(N)/F(%)/ Mean Age [range] |
Primary Regimens | Top 2 prevalence of moderate-to-severe chemotoxicity subgroupsa | |
|---|---|---|---|---|---|---|
| Ali et al. (2016) /Canada& France |
PL | CRC/ mixed stages |
138/F50%/62[28–87] | 5-FU | GI (20%)/Neuropathy (13%) | |
| Antonio et al. (2018)/Europe | P | Older Adults CRC/ mixed stages |
193/F32%/80[75–89] | 5-FU | Diarrhea (9.5%)/ Fatigue, Neutropenia (8.1%) |
|
| Aparicio et al (2016)/Europe | P | Older Adults mCRC/IV | 271/F42%/80[75–92] | 5-FU | Neutropenia (22%)/ GI (20.8%) |
|
| Backshall et al. (2011)/Europe | P | mCRC/IV | 52/F35%/79[42–86] | Cape |
Hand-foot-syndrome (11%)/ Diarrhea (9%) |
|
| Barret et al. (2011)/Europe | P | mCRC/IV | 114/F32%/65[22–92] | 5-FU | Neuropathy (85.5%)/ GI (28.7%) |
|
| Beukers et al. (2021)/Europe | R | Older Adults Colon/III | 97/F52%/77[70–85] | 5-FU | Diarrhea (30%)/ Hand-foot syndrome (20%) |
|
| Breton et al. (2021)/Europe | P | mCRC/IV | 2,190/F38%/67[59–75] | 5-FU | Composite GI (15%)/ Neutropenia (13.2%) |
|
| Feliu et al. (2022)/Europe | P | Older Adults CRC/mixed stages | 321/F32%/78[70–90] | 5-FU | Fatigue (12%)/ Diarrhea (10%) |
|
| Folprecht et al. (2008)/Europe | P | CRC/ mixed stages |
2,691/F33%/ 70[18–79] |
5-FU | Neutropenia (28.9%)/ Diarrhea (20.5%) |
|
| Gallois et al. (2019)/Europe | P | Older Adults mCRC/IV | 168/F44%/75[70–92] | 5-FU | Nausea, vomiting (15%)/ Diarrhea (8%) |
|
| Garg et al. (2012)/Australia | PL | CRC/III | 173/F43%/63[54–72] | 5-FU | Neutropenia (55%)/ GI (50.6%, mucositis 12%) |
|
| Hochster et al. (2007)/USA | P | Older Adults CRC/ mixed stages |
55/F47%/81[75–90] | Leucovorin |
GI (35.7%)/ Diarrhea (25%) |
|
| Jung et al. (2015)/S.Korea | P | Colon/III | 229/F59%/61[53–67] | 5-FU | Neutropenia (40%) | |
| Karabulut et al. (2022)/Turkey | P | mCRC/IV | 137/F61%/62[18–83] | 5-FU | Anemia (30%)/ GI (15.5%) |
|
| Li et al. (2021)/China | PL | CRC/no data | 233/F34%/58[28–87] | Cape | Nausea (35%)/Vomiting (35%) | |
| Okada et al. (2017)/Japan | R | mCRC/IV | 108/F56%/65[34–83] | 5-FU | Non-hematological (57%)/ Hematological toxicity (45%) |
|
| Osterlund et al. (2007)/Europe | RCT | mCRC/IV | 150/F49%/60[31–75] | 5-FU | GI (51%)/ Neutropenia (16%) |
|
| Retornaz et al. (2020)/Europe | PL | Older Adults Colon/ mixed stages |
97/F51%/79[70–90] | 5-FU | Fatigue (64%)/ GI (40%) |
|
| Sastre et al. (2012)/Europe | P | Older Adults mCRC/IV | 66/F42%/70[70–86] | 5-FU | Neuropathy (16%)/ Diarrhea (16%) |
|
| Seymour et al. (2011)/Europe | P | mCRC/IV | 440/F41%/74[35–86] | 5-FU | Pain (16%)/Diarrhea (10%) | |
| Stein et al. (2016)/Europe | PL |
mCRC/IV | 1,249/F45%/
74 [21–99] |
Cape |
Pain, Anemia, Diarrhea (12%)/ Nausea (8%) |
|
| Tominga et al.(2016)/Japan | R | CRC/III | 135/F58%/63[58–71] | 5FU/Cape | Neutropenia (52%)/ Anorexia (17%) |
|
| Tsuchihashi et al. (2018)/Japan | R | mCRC/IV | 523/F41%/63[55–85] | Regorafenib, Trifluridine, Tipiracil | Hand-foot-syndrome (20%)/ Anemia (12%) |
|
| Watanabe et al. (2018)/Canada | PL | CRC/III | 371/F49%/64[60–89] | Cape/5-FU | GI (80%)/ Neuropathy (80%) |
|
| Yamada et al. (2013)/Japan | P | mCRC/IV | 512/F36%/63[33–79] | 5-FU/OX | Neutropenia (43%)/ GI (12%) |
|
Note. Cape: Capecitabine; CRC: colorectal cancer; F: female; GI: gastrointestinal; 5-FU: 5-Fluorouracil; mCRC: metastatic CRC; OX: oxaliplatin. Study designs P: prospective study design; PL: Prospective longitudinal design with repeated measures; R: retrospective design; RCT: randomized controlled trials. aToxicities measured by the Common Terminology Criteria for Adverse Events (CTCAE).
Table 1.
B. Characteristics of Studies Not Included for Meta-Analysis (N = 5).
| Authors(year) /Country |
Study Design | Cancer Stages | Samples(N)/ F(%) /Mean Age [range] |
Primary Regimens | Chemotoxicity Measures | Top prevalence of moderate-to-severe chemotoxicity subgroups | |
|---|---|---|---|---|---|---|---|
| Brown et al. (2022)/USA | P | Colon/ II-III |
533/F56%/ 59[47–70] |
5-FU | Physicians’ chart and progress note review, | Discontinuation of chemotherapy (13%) | |
| Cespedes Feliciano et al. (2017)/USA | P | Colon/ II-IV |
533/F55.4%/ 59 [no data] |
5-FU | Physicians’ chart and progress note review and EMR ICD9 Codes | Early discontinuation (36%)/Neuropathy (24.1%) | |
| Decoster et al. (2018)/Europe | P | Older Adults mCRC/ IV |
252/F38%/ 77[69–91] |
5-FU | Physicians’ chart and progress note review | Vascular toxicity (35%)/ GI toxicity (13.6%) |
|
| Grimes, C. (2022)/USA | R | CRC/III | 89/F58%/ 62[no data] |
5-FU. | Physicians’ chart and progress note review | Diarrhea (6.7%)/ Nausea (5.6%) |
|
| Looijaard et al. (2020)/Europe | P | Older Adults Colon/III |
53/F45%/ 71[68–74] |
5-FU | Physicians’ chart and progress note review | Dose reduction/ incompletion (52.8%) |
|
Note. CRC: colorectal cancer; EMR: electronic medical record; F: female; 5-FU: 5-Fluorouracil; GI: gastrointestinal; ICD-9: international classification of diseases, 9th Revision (ICD-9); mCRC: metastasis CRC; PRO-CTCAE: patient-reported outcomes version of the common terminology criteria for adverse events.
3.3. Systematic Review: Prevalence and Risk Factors of Chemotoxicity
We reviewed the selected 30 studies based on the patient characteristics, interventional components, and primary outcomes (clinician-reported chemotoxicity) of the conceptual framework, Quality Health Outcomes Mode (Figure 1) [25].
3.3.1. Patient Characteristics
Among 12,706 samples across 30 studies, most participants were male (56%). Stage IV was the most prevalent, representing an average of 59% of participants, followed by stage III (28% of total samples). The mean age across the 30 studies was 68.4 years old. Age ranged from 58 [47] to 81 years old [44] across 30 studies. Ten studies [7,32,35,39,41,44,48,51,52,59] focused solely on older adults (> 65 years old) with the CRC population. The majority of participants were diagnosed with CRC, followed by colon cancer only (n = 6 [35,37,38,45,48,51]). Additionally, 14 studies were conducted on metastatic CRC (Table 1AB).
3.3.2. Interventional Components
Only Osterlund et al. (2007) [50] conducted an RCT with Lactobacillus intervention in metastatic CRC. Compared to the no-intervention groups, grade 3 or 4 diarrhea incidence was lower in patients treated with Lactobacillus (22% vs 37%, p =0.027). Additionally, these patients experienced less abdominal discomfort, required fewer hospital visits, and had a reduced number of chemotherapy dose reductions due to GI toxicity.
3.3.3. Primary Outcomes.
Clinician-reported chemotoxicity (Prevalence). The primary chemotherapy regimen in CRC was 5-FU-based agents, and the most common chemotoxicity measure was the Cancer Terminology Criteria for Adverse Events (CTCAE) grading scale, used in 25 studies among 30 selected studies. Five studies [37,38,39,43,48] assessed the prevalence of chemotoxicity by reviewing electronic health records (EHR), such as physicians’ charts and progress note reviews, which included the International Classification of Diseases (ICD)-9 codes (study n =1 [38]). The majority of the studies reported GI toxicity as the most prevalent type of moderate-to-severe chemotoxicity, from 12% to as high as 80% in different studies, except for 6 [37,38,45,48,49,56] out of 30 studies (Table 1AB). Diarrhea was a frequently reported symptom of GI toxicity in 11 studies [7,33,35,40,41,43,44,52,53,54,59] , with prevalence rates ranging from 8%[41] to 30% [35] across the studies. The next most frequently reported top-ranked moderate-to-severe chemotoxicity across the studies was neutropenia in 9 studies [32,36,40,42,45,50,55,57,59] with prevalence rates ranging from 8.1% [59] to 55% [42], followed by neuropathy in 5 studies [34,38,52,57], ranging from 13% [31] to 85.5%[34]. Three studies also evaluated chemotoxicity by examining the incidence of chemotherapy discontinuation or dose reduction/incompletion [37,38,48].
Clinician-reported chemotoxicity (Risk factors). Regarding risk factors of chemotoxicity (Table 2), four main categories were identified: nutritional status, geriatric assessment, biomarkers, and demographic/clinical factors. Fourteen studies [7,31,34,37,38,41,43,45,46,47,49,51,55,57] focused on malnutrition. The most common risk factor was low albumin levels [34,41,46,47,49,51,55]), followed by weight loss [7,34,41,46,47], low BMI [37,38,46], and low hemoglobin levels [47,57] before chemotherapy. Body composition, such as low muscle mass, sarcopenia, and high abdominal adiposity [37,38,43,45] were also significant factors. Body composition, including muscle and fat mass, were more sensitive risk factors of chemotoxicity than BMI, body weight, or body surface area. Seven studies [7,35,36,39,44,51,53] included a geriatric assessment, including comprehensive frailty score, physical frailty-grip status, or performance levels, showing that the baseline frailty status is associated with chemotoxicity. Various biomarkers were studied with two major categories: 1) Pro-inflammatory markers, e.g., white blood cell counts (WBC) [7,47,53], C-reactive protein (CRP) [47,51,55], lactate [40]; and 2) Hepato-renal functions [7,36,40,51]. Higher levels of low-density lipoprotein-derived lipids, short telomere length, lack of lactobacillus microbiome, and high carcinogenic antigen (CEA) were also shown to be associated with the risk of chemotoxicity. In demographic/clinical factors, the associations of age with chemotoxicity were inconsistent. Significant associations were found between younger adult age group (<50 years old) and neutropenia [42,47], as well as GI toxicity [42]. On the other hand, older age (> 65 years old) was significantly associated with GI toxicity [44,47] and hematological toxicity [47,57]. Female sex, cancer stages, previous history of aggressive chemotherapy or colorectal surgeries, and baseline HRQoL were also significantly associated with chemotoxicity (Table 2).
Table 2.
Significant Predictorsa of Overall Chemotoxicity (moderate-to-severe).
| Authors(year)b/ Statistical methods |
Nutrition | Geriatric assessments | Biomarkers | Demographic/ Clinical Factors |
|---|---|---|---|---|
| Ali et al.(2016)/ Group comparisons |
Body mass with neuropathy |
|||
| Backshall et al. (2011)/ Group comparisons |
Metabolic lipid panel | |||
| Barret et al. (2011)/ Odds Ratios (ORs) |
Weight loss, low albumin |
|||
| Beukers et al. (2021)/ORs | Comprehensive Frailty | Female sex/ Cancer stages |
||
| Breton et al. (2021)/ORs | Physical Frailty (Performance) |
Alkaline phosphatase (ALP) | Surgical history. Hx of aggressive chemotherapy | |
| Feliu et al. (2022)/ Beta coefficient |
Weight loss | Comprehensive Frailty | Kidney function | |
| Folprecht et al. (2008)/ Group comparisons |
High WBC, ALP, lactate | |||
| Gallois et al. (2019)/ ORs |
Weight loss, low albumin |
|||
| Garg et al. (2012)/ Beta Coefficient |
Short telomere length, high platelet lymphocyte ratio, and low neutrophil count with hematological and GI toxicity. | Younger age with neutropenia and GI toxicity |
||
| Hochster et al. (2007)/ORs | Physical Frailty (Performance) |
CEA, liver panels, creatine | Older age with GI toxicity (diarrhea) | |
| Jung et al. (2015)/ORs | Psoas muscle mass | |||
| Karabulut et al. (2022)/ Group comparisons |
Low BMI, Weight loss, low albumin | |||
| Li et al. (2021)/ORs | Weight loss with hand-foot syndrome, and nausea low Hemoglobin and albumin with hematological toxicity. |
Increased WBC, high CRP with hematological toxicity | Older age with GI and hematological toxicity. Younger age with neutropenia. |
|
| Okada et al. (2017)/ Group comparisons |
Low albumin with hepatotoxicity. | |||
| Osterlund et al. (2007)/ Group comparisons |
Lactobacillus | |||
| Retornaz et al. (2020)/ORs | Low albumin | Physical Frailty (Grip strength, Performance) |
Increased CRP, and ALP | Hx of aggressive chemotherapy |
| Seymour et al. (2011)/ORs | Physical Frailty (Performance) |
Increased WBC | Baseline quality of life | |
| Tominga et al. (2016/ORs |
Low albumin. |
CRP/Albumin ratio. elevated neutrophil to lymphocyte ratio | ||
| Watanabe et al. (2018)/ORs | Low Hemoglobin with hematological toxicity | Increased age & female sex with hematological toxicity | ||
| Studies not included in Meta-Analysis* | ||||
| Brown et al. (2022)/ Group comparisons |
BMI and abdominal adiposity | |||
| Cespedes Feliciano et al. (2017)/ORs | BMI, muscle mass index | |||
| Decoster et al. (2018)*/Group comparisons | Physical Frailty (Performance) |
|||
| Grimes, C. (2022)/Group comparisons | Sarcopenia | |||
| Looijaard et al. (2020)/Group comparisons | Hx of aggressive chemotherapy | |||
Note. Alb: albumin; BMI: body mass index; CEA: carcinoembryonic antigen; CRP: C-reactive protein; GI: gastrointestinal; Hx: history; ORs: odd ratios; USA: United States of America; WBC: white blood cell count. aAssociated with multiple chemotoxicity unless otherwise specified. bWe excluded studies with no significant risk factors (Antonio et al. 2018; Stein et al. 2016), or without examining risk factors of chemotoxicity (Aparicio et al. 2016; Sastre et al. 2012; Tsuchihashi et al. 2018; Yamada et al. 2013). *Studies not included in meta-analysis (n = 5) due to unavailable chemotoxicity prevalence data or data that was not comparable for inclusion in the meta-analyses.
3.4. Meta-Analysis: Prevalence and Risk Factors of Chemotoxicity
Among 30 studies analyzed in this review, 25 were included for meta-analysis when considering consistent chemotoxicity measures (i.e., CTCAE) (Table 1A).
3.4.1. Publication bias (asymmetry and heterogeneity) assessment
Among 25 studies in the meta-analysis, we performed the publication bias assessment, primarily based on the prevalence of overall moderate-to-severe chemotoxicity across 17 studies using the CTCAE grading scale (Asymmetry shown in Figure 3; Heterogeneity shown in Table 3). Then, we also performed a publication bias assessment based on the prevalence of chemotoxicity subgroups by the rank, from the selected 25 studies (Table 4 and Supplementary Figure 1). No asymmetries from Begg’s and Egger’s tests and funnel plots were found in the 25 selected studies included for meta-analysis (Table 3 and Table 4, Figure 3, and Supplementary Figure 1). Overall, high levels of heterogeneity were observed in chemotoxicity prevalence and its subgroups, with I2 > 75%. Consequently, random-effect models were utilized to interpret results (Table 3 and Table 4).
3.4.2. Pooled prevalence of chemotoxicity
Moderate-to-severe chemotoxicity. The prevalence of moderate-to-severe overall chemotoxicity based on the CTCAE grading scale was reported in 17 studies [7,31,32,33,35,36,40,41,42,44,45,47,50,51,53,54,57]. The pooled prevalence of moderate-to-severe overall chemotoxicity was 45.7% (95% CI: 38.2 to 53.2) (Table 3 and Figure 4).
Table 3.
Heterogeneity Tests for Publication Bias Among 17 Studies Included for Meta-Analysis of Prevalence of Overall Chemotoxicity (Moderate-to-Severe).
Table 3.
Heterogeneity Tests for Publication Bias Among 17 Studies Included for Meta-Analysis of Prevalence of Overall Chemotoxicity (Moderate-to-Severe).
| Study Characteristicsa | Sub-variables | Studies n/ Total Sample n |
Pooled Prevalence of Overall Chemotoxicityd% (95% CI) | Test for heterogeneity between studiese | ||
|---|---|---|---|---|---|---|
|
Qdf Between |
I2 (%) Between | p Between | ||||
| Total Studiesa | 17/n=8,819 | 45.7 (38.2 to 53.2) | 112.5416 |
78.14 |
<.001 | |
|
Countryb |
Europe | 12/n=7,793 | 45.4 (36.3 to 55.3) | 154.6511 | 98.32 | <.001 |
| Asia | 2/n=462 | 40.1 (30.8 to 49.8) | 223.531 | 99.41 | .049 | |
| Publication year | 2007-2010 | 3/n=2,896 | 46.1 (23.6 to 29.7) | 158.392 | 95.49 | .012 |
| 2011-2015 | 4/n=894 | 37.0 (26.9 to 47.7) | 133.413 | 98.65 | .005 | |
| 2016-2020 | 6/n=2,294 | 55.9 (33.9 to 76.8) | 148.855 | 95.42 | .044 | |
| 2021-2024 | 4/n=2,735 | 47.5 (39.2 to 55.8) | 133.523 | 88.41 | .043 | |
|
Study designc |
Observational | 16/n=8,669 | 45.5 (37.1 to 53.5) | 140.8915 | 96.89 | .023 |
| Female prevalence | <50.0% | 13/n=8,258 | 47.6 (37.6 to 57.7) | 35.3212 | 91.23 | .010 |
| ≥ 50.0% | 4/n=561 | 46.7 (42.6 to 50.8) | 28.523 | 89.41 | .043 | |
| Sample size | n < 100 | 4/n=301 | 40.5 (22.9 to 59.4) | 158.423 | 78.75 | .044 |
| 100 ≤ n < 500 | 10/n=2,388 | 52.9 (39.6 to 65.9) | 192.529 | 66.49 | .013 | |
| n ≥ 500 | 3/n=6,130 | 38.8 (24.3 to 54.5) | 151.452 | 74.32 | .007 | |
|
Age group (Participants’ age range) |
18 < age < 65 | 11/n=7,916 | 33.4 (22.3 to 39.5) | 185.8910 | 85.65 | .041 |
| 65> Older Adults |
6/n= 903 | 50.1 (27.6 to 69.9) | 133.555 | 86.56 | .035 | |
|
Cancer Types |
Colon only | 4/n= 870 | 47.1 (42.3 to 51.8) | 321.323 | 98.61 | .019 |
| Mixed stages CRC | 5/n=3,196 |
48.8 (32.0 to 65.7) | 139.324 | 88.53 | .043 | |
| Metastatic CRC | 7/n=4,520 | 41.9 (32.9 to 51.4) | 98.496 | 89.65 | .041 | |
Note. CI: confidence intervals; CRC: colorectal cancer; df: degree of freedom; GI: gastrointestinal. a We included only 17 studies reporting overall chemotoxicity prevalence with moderate-to-severe severity using the Common Terminology Criteria for Adverse Events (CTCAE) measure among 25 studies included in the meta-analysis in our study. b We excluded Ali et al., Hochster et al., and Watanabe et al. as these studies are the sole representation of a particular country among a total of 25 selected studies of this study. c We excluded Osterlund et al. (2007) from the RCT study. d Moderate-to-severe toxicity; weighted effect size and standard error were applied, resulting in pooled prevalence and 95% Confidence Intervals (CIs). e p-value <.05 is considered significant for heterogeneity tests.
We also performed the subgroup analyses of the pooled prevalence of moderate-to-severe chemotoxicity by stratifying prevalence according to subgroups of chemotoxicity (e.g., non-hematological, hematological, and others) (Table 4, and funnel plots in Supplementary Figure 2). In moderate-to-severe chemotoxicity subgroups, the pooled prevalences of moderate-to-severe non-hematological and hematological toxicities were 39.2% (33.7 to 44.7) and 25.3% (19.4 to 31.5), respectively. Among moderate-to-severe other chemotoxicity subgroups, abdominal pain was the most frequent (24.3%), followed by GI toxicity (22.9%), neuropathy (17.9%), neutropenia (17.8%), nausea/vomiting (17.8%), and diarrhea (14.1%) (Table 4, and Supplementary Figure 2).
Mild chemotoxicity. Only a few studies reported the prevalence of chemotoxicity with mild severity. Six studies [7,32,50,51,53,55] were included for the pooled prevalence of mild overall chemotoxicity resulting in 61.7% of pooled prevalence. The pooled prevalences of mild non-hematological and hematological toxicities were 50.1% and 22.5%, respectively (Figure 5 and Table 4). Among chemotoxicity subgroups with mild severity (Table 4 and Supplementary Figure 3), diarrhea was the most frequent chemotoxicity (58.9%), followed by hand-foot syndrome (51.7%), anemia (36.5%), and mucositis/stomatitis (28.6%).
Table 4.
Asymmetry and Heterogeneity Tests for Publication Bias: Subgroups of Chemotoxicity.
|
Study Sub-variables |
Studies n/ Total sample n |
Pooled Prevalence by rank (%: 95% CI)a |
Asymmetry tests | Heterogeneity tests between studies |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Begg's test |
Egger's test | |||||||||||
| Kendall's Ƭ | pb | SE | pc |
Qdf Between |
I2 (%) Between |
pb Between |
||||||
| Pooled Prevalence of Moderate-to-Severe Chemotoxicity | ||||||||||||
| Non-Hematological Toxicity | 16/n=6,602 | 39.2 (33.7 to 44.7) | 0.34 | .600 | 4.9 | .943 | 121.6915 | 88.56 | .033 | |||
| Hematological Toxicity | 19/n=6,882 | 25.3 (19.4 to 31.5) | 0.29 | .491 | 2.5 | .423 | 132.6518 | 93.79 | .049 | |||
| Pooled Prevalence of Moderate-to-Severe Chemotoxicity Subgroups | ||||||||||||
| Abdominal pain | 3/n =1,655 | 24.3 (2.01 to 60.1) | 0.33 | .412 | 6.3 | .143 | 56.12 | 99.61 | <.001 | |||
| GI Toxicity | 20/n=9,489 | 22.9 (16.4 to 30.1) | 0.23 | .598 | 2.4. | .892 | 132.5219 | 98.59 | <.001 | |||
| Neuropathy | 9/n=5,382 | 17.9 (4.9 to 36.5) | 0.42 | .394 | 3.2 | .352 | 122.598 | 95.89 | .049 | |||
| Neutropenia | 14/n=8,227 | 17.9 (11.1 to 25.9) | 0.51 | .341 | 5.3 | .422 | 144.6513 | 98.51 | <.001 | |||
| Nausea/Vomiting | 10/n=5,089 | 17.8 (8.5 to 29.6) | 0.41 | .535 | 5.6 | .314 | 69.59 | 98.66 | <.001 | |||
| Diarrhea | 18/n=7,209 | 14.1 (11.1 to 17.4) | 0.31 | .591 | 4.4 | .289 | 144.0117 | 98.11 | <.001 | |||
| Leukocytosis | 2/n=2,287 | 12.9 (0.4 to 38.2) | 0.32 | .542 | 3.4 | .132 | 243.311 | 99.51 | .035 | |||
| Fatigue | 7/n=2,772 | 12.6 (4.6 to 23.7) | 0.38 | .224 | 4.5 | .499 | 132.566 | 99.92 | <.001 | |||
| Anemia | 7/n=2,547 | 10.4 (4.5 to 18.3) | 0.56 | .621 | 3.4 | .289 | 132.556 | 89.61 | <.001 | |||
| Leukopenia | 3/n=4,452 | 10.2 (3.6 to 19.6) | 0.41 | .214 | 5.6 | .512 | 241.952 | 89.52 | .021 | |||
| Mucositis/stomatitis | 7/n=2,608 | 9.5 (2.9to 18.7) | 0.59 | .399 | 6.2 | .526 | 87.46 | 95.41 | .014 | |||
| Hand-Foot-Syndrome | 5/n=700 | 9.0 (1.8 to 20.9) | 0.16 | .841 | 6.5 | .431 | 353.174 | 97.84 | .019 | |||
| Anorexia | 5/n=1,804 | 6.4 (3.7 to 9.6) | 0.41 | .412 | 5.4 | .122 | 101.424 | 99.41 | <.001 | |||
| Coagulation disorders | 2/n=2,757 | 4.9 (4.1 to 5.8) | 0.33 | .312 | 5.5 | .082 | 99.491 | 89.59 | <.001 | |||
| Constipation | 2/n=341 | 3.4 (1.8 to 5.6) | 0.14 | .623 | 5.6 | .412 | 93.041 | 84.23 | .048 | |||
| Pooled Prevalence of Mild Chemotoxicity | ||||||||||||
| Overall Chemotoxicity | 6/n=1,309 | 61.7 (48.0 to 74.6) | 0.54 | .841 | 2.3 | .347 | 122.685 | 95.92 | <.001 | |||
| Non-Hematological Toxicity | 3/n=473 | 50.1(21.1 to 78.9) | 0.55 | .792 | 3.1 | .572 | 134.882 | 92.51 | .002 | |||
| Hematological Toxicity | 4/n=913 | 22.1 (6.6 to 43.5) | 0.41 | .852 | 2.9 | .123 | 156.413 | 85.91 | .024 | |||
| Pooled Prevalence of Mild Chemotoxity Subgroups | ||||||||||||
| Diarrhea | 4/n=956 | 58.9 (28.8 to 85.6) | 0.41 | .312 | 2.4 | .312 | 111.313 | 78.41 | .048 | |||
| Hand-Foot-Syndrome | 2/n=202 | 51.7 (0.4 to 98.8) | 0.52 | .411 | 4.1 | .522 | 198.561 | 88.51 | .009 | |||
| Anemia | 3/n=763 | 36.5 (1.5 to 84.9) | 0.33 | .012 | 2.3 | .731 | 153.662 | 94.55 | .014 | |||
| Mucositis/stomatitis | 3/n=884 | 28.6 (7.2 to 57.0) | 0.28 | .102 | 4.9 | .341 | 142.652 | 93.41 | <.001 | |||
| Neutropenia | 3/n=884 | 25.7 (6.2 to 52.3) | 0.62 | .531 | 5.3 | .512 | 166.242 | 99.79 | <.001 | |||
| Nausea/Vomiting | 3/n=1,572 | 18.3 (0.6 to 52.3) | 0.38 | .512 | 2.5 | .823 | 143.662 | 95.12 | <.001 | |||
| Fatigue | 2/n=492 | 17.1 (0.5 to 63.7) | 0.12 | .312 | 2.4 | .623 | 98.421 | 98.55 | .032 | |||
| Coagulation disorders | 2/n=1,422 | 4.3 (0.7 to 10.7) | 0.52 | .432 | 2.3 | .412 | 102.031 | 85.66 | .045 | |||
Note. CI: confidence intervals; GI: gastrointestinal; df = degree of freedom; SE: standard error. a Weighted effect size and standard error were applied, resulting in pooled estimates and 95% Confidence Intervals (CIs). b p <.05 considered significant publication bias. .
3.4.3. Pooled Associations of Age as a Predictor of Chemotoxicity Prevalence
In our review of significant risk factors for chemotoxicity (Table 2), we identified multiple inconsistencies. These inconsistencies were present in the types of statistical correlations used (e.g., ORs, Beta coefficients, or group comparisons) and in chemotoxicity subgroups (e.g., prevalences of overall toxicity, hematological, non-hematological, GI toxicities, or neutropenia). Given these inconsistencies, age was the only risk factor available for computing pooled associations with the prevalence of chemotoxicity (Table 5AB). In unadjusted meta-regression models (Table 5A), there were significant relationships between age (continuous variables) and chemotoxicity. When all other variables held constant, an increase of 1-year old in age was negatively associated with an average 1.09 change (unstandardized B= -1.09) in the prevalence of moderate-to-severe neutropenia (p = .003), while age was positively associated with an average change of B unites in the prevalence of nausea/vomiting (B = 1.32, p = .028), diarrhea (B = 1.05, p = .012), and GI toxicity (B = 1.02, p =.044). Given the standardized β coefficients in unadjusted models, age was the most significantly associated with GI toxicity (β = 1.97, p = .005), followed by the prevalence of neutropenia (β = -1.78, p =.002). In adjusted meta-regression models (controlling for cancer stages as the most prevalent cancer stage, metastatic status, cancer types, sample size as group variables, and sex as the most prevalent sex group variable), similar results were found, showing a negative association between age and neutropenia, while positive associations were found between age and nausea/vomiting, diarrhea, and GI toxicity prevalences. Given the standardized β coefficients in adjusted models (Table 5A), age was the most significantly associated with the prevalence of GI toxicity (β = 1.85, p = .001), followed by the prevalence of neutropenia (β = -1.44, p =.004). No significant relationship existed between age and overall, non-hematological, and hematological chemotoxicities in unadjusted and adjusted models (Table 5A).
Table 5B presents the results of a meta-ANOVA (F tests) and regressions (ORs) comparing the prevalence of different types of chemotoxicity between two age groups: adults (age > 18 and < 65 years old) and older adults (age > 65 years old). Significant differences existed in the prevalence of overall chemotoxicity, neutropenia, diarrhea, and GI toxicity between adults and older adults. The mean prevalences of overall chemotoxicity, diarrhea, and GI toxicity were higher in the older adult group compared to the adult group, while this was lower in the older adult group compared to the adult group for the prevalence of neutropenia. Compared to adult groups, older adult groups reported higher prevalences of chemotoxicity, with 14% in overall chemotoxicity (OR= 1.14), 27% in diarrhea (OR = 1.27), and 65% in GI toxicity (OR = 1.65). However, they reported a 35% lower prevalence of chemotoxicity in neutropenia (OR = 0.65).
4. Discussion
This study is the first to systematically review clinician-reported chemotoxicity and perform a meta-analysis to compute the pooled prevalence of chemotoxicity and the pooled associations of risk factors of chemotoxicity in CRC patients. Our study has added new information to the comprehensive understanding of the current literature on chemotoxicity in CRC populations. It provides insights into the pooled prevalence and risk factors of clinician-reported chemotoxicity, including its subgroups, to foster a better consensus on this topic. We showed evidence to suggest a significant prevalence of chemotoxicity and several risk factors of chemotoxicity in CRC patients. New findings gathered from the current study include the overall prevalence of chemotoxicity (45.7% for moderate-to-severe levels and 61.7% for mild severity levels), indicating that the problem of chemotoxicity needs to be improved in CRC patients. Our subgroup analyses also provided further details of the prevalences of subgroups of chemotoxicity, showing that non-hematological toxicity was more common compared to hematological toxicity regardless of the severity.
Among subgroups of chemotoxicity, GI-related side effects were prevalent regardless of the severity (e.g., moderate-to-severe toxicity: abdominal pain, composite GI toxicity, nausea/vomiting, diarrhea; mild toxicity: diarrhea, mucositis/stomatitis, nausea/vomiting). This finding was corroborated by the systematic review and meta-analysis of patient-reported outcomes (PROs) in CRC patients, which showed prevalent and severe GI symptoms (mean prevalences 40%) after cancer treatments [14], compared to other cancers (mean GI toxicity prevalence < 5% in breast cancer [60] and < 10% in lung cancer [61]. However, fatigue was less prevalent (12.6%for moderate-to-severe fatigue and 17.1% for mild fatigue), and no psychological distress data was reported by clinicians in our review. Conversely, previous literature [14] reported that fatigue and psychological distress were the most severe and prevalent among CRC patients. The discrepancy between patient-reported toxicities and those assessed by clinicians using the CTCAE can be attributed to several factors. Evidence suggests that clinician-reported adverse events may miss or underreport up to 50% of symptoms that patients experience during treatment [62]. Clinicians might not fully recognize or document all treatment-related adverse events, especially more subjective ones like fatigue, depression, and sleep disturbances [62]. In conclusion, both PROs and clinician-reported chemotoxicity provide valuable and complementary insights. Including both data types in chemotoxicity assessment and management appears to be warranted.
Our study suggests that chemotoxicity assessment and management should consider various subgroups (e.g., non-hematological or hematological) due to differing etiologies [63]. Inconsistencies in risk factor measures and chemotoxicity outcome subgroups (i.e., hematological, GI toxicity, neuropathy, etc.), along with statistical methods, limited our meta-regressions. Despite this, our findings on common chemotoxicity risk factors will aid in identifying high-risk groups and the future development of prediction models or targeted interventions. Referring to our guiding conceptual model (Figure 1, Quality Health Outcomes Model [25]), patients’ clinical characteristics were identified as frequent chemotoxicity risk factors, including malnutrition, frailty, hepato-renal functions, pro-inflammatory status (increased WBC or CRP), previous colorectal surgical histories, cancer stages, chemotherapy doses, and baseline HRQoL in our systematic review. Among interventional components, only Lactobacillus (diet) RCT improved chemotoxicity [50]. Furthermore, our systematic review (Table 2) and meta-analyses (Table 5AB) investigating the common risk factors of chemotoxicity showed consistent results for age: Age was positively associated with composite and individual GI toxicities but negatively with neutropenia. This was consistent with a previous study on 927 older adult patients with mixed cancer types (breast 33%, lung 19%, and colon 10%) [63]. A potential explanation is that an age-related decline in GI function (i.e., leaky gut, slow transition, dysbiosis) can exacerbate the vulnerability of mucosal damage in the gut triggered by CRC pathology per se and chemotherapy [64]. Additionally, certain drugs, such as 5-FU (the primary treatment agent for CRC) or immune checkpoint inhibitors (for metastatic CRC), can have more severe side effects on the GI tract in CRC patients [65]. Our negative associations could be due to the use of lower doses or less aggressive chemotherapy regimens in older adults due to concerns about treatment tolerance and comorbidities [63,66].
In our review, malnutrition status was measured using weight loss, BMI, albumin or hemoglobin levels, and muscle or fat mass. Emphasis was placed on muscle or fat mass as more sensitive chemotoxicity indicators than body weight or BMI. Previous reviews in nutritional status and chemotherapy tolerance (e.g., chemotoxicity, treatment non-compliance, dose reduction, etc.) in CRC [33,34] corroborate our findings, suggesting an association between lean muscle mass and chemotoxicity and the importance of nutritional screening before initiating chemotherapy. This could be because a low lean mass might be associated with frailty, greater comorbidities, and slow drug metabolisms of hydrophilic chemotherapy (such as 5-FU), leading to more incidences of chemotoxicity [40]. On the other hand, a high-fat mass could be involved in poor drug distribution and clearance, impacting the increased degree of toxicity [40]. However, the potential mechanisms for the association between body composition and chemotoxicities remain unclear. Our review identified frailty (performance, cognition, or comprehensive frailty scores) as a predictor of chemotoxicity. This is consistent with a previous review study [14], which found that frailty predicted HRQoL and symptom toxicity. Physical frailty and malnutrition statuses, such as sarcopenia, were closely related. Therefore, further monitoring of chemotoxicity for patients with both frail and malnourished conditions is warranted such as dietary evaluations by a nutritionist.
Increased WBC and CRP significantly predicted chemotoxicity in our study. This could be due to high tumor burden and altered immune responses [67]: High WBC and CRP levels can also indicate a larger tumor burden. Larger tumors may require more aggressive chemotherapy, leading to increased chemotoxicity. Furthermore, both high WBC and CRP levels indicate an activated immune response. Chemotherapeutic agents can cause damage to the immune system, particularly to T cells, and an already activated pro-inflammatory status may exacerbate this damage, leading to worse chemotoxicity triggered by altered immune and inflammatory functions [67].
Anti-inflammatory interventions, such as lifestyle or microbiome modifications, demonstrated the anti-inflammatory effects in cancer patients [68]. Lactobacillus microbiome intervention was the only intervention study in CRC patients to examine the chemotoxicity identified in our study [50]. Microbiome has been associated with multiple symptoms, including GI, psychological distress, dermatological disorders, neuropathy, and hematological complications in many chronic diseases [69]. Therefore, anti-inflammatory or microbiome-targeted interventions can be considered for pre- and post-rehabilitation of chemotherapy for this patient group. Despite several intervention studies, including a geriatric assessment [70], muscle resistance exercise [71], and nutritional [72] interventions aiming to reduce chemotoxicity, none of these studies focused primarily on CRC [70, 72], and examined clinician-reported chemotoxicity [71, 72]. Our review of risk factors of chemotoxicity, based on our conceptual framework – interventional components, also revealed limited interventions for chemotoxicity in CRC. None of the 30 analyzed studies conducted interventions such as predicting and screening for chemotoxicity or implementing physical and psychological interventions to manage chemotoxicity.
Clinical Implications.Our study underscores the need for targeted approaches to prevent and manage chemotoxicity in CRC patients undergoing chemotherapy. Consideration of specific subgroups of chemotoxicity, such as GI toxicity, neuropathy, and neutropenia, is crucial for tailoring interventions effectively. Oncology professionals should explore diverse strategies, such as nutritional, anti-inflammatory, and pain interventions, to address different subgroups of chemotoxicity. Pre-screening for potential risk factors, like age, nutritional status, and frailty, is essential to anticipate and mitigate adverse effects. Rather than relying solely on chronological age, a comprehensive assessment of multiple risk factors (e.g., age-nutritional status-chemotherapy doses and durations) is recommended to guide treatment decisions. Balancing treatment benefits with side effect risks is vital for older patients who may be more vulnerable. Conversely, younger patients may face increased chemotoxicity risks due to aggressive treatment regimens. Early discussions regarding individualized goals of care are paramount for minimizing chemotoxicity and optimizing treatment outcomes.
Future Research.Future research should consider precision medicine approaches to tailor individualized supports mitigating chemotoxicity based on patient characteristics, aiming to minimize chemotoxicity. To achieve this, the primary steps of research will include: Exploring the underlying socio-biological mechanisms of chemotoxicity, including its subgroups; developing chemotoxicity prediction models by considering the most significant risk factors and integrating biomarkers involved in immune and inflammatory systems (e.g., hematological immune parameters, microbiome or metabolomics) to identify at-risk groups; and designing and testing personalized interventions that apply various strategies (e.g., nutrition, anti-inflammatory, social support-focused, or health system changes), primarily targeting common risk factors of overall chemotoxicity, or specific to chemotoxicity subgroups in CRC, and integrating patient preferences into treatment decisions.
Limitations.Although the overall meta-analysis yielded significant findings, several subgroups of chemotoxicity (e.g., coagulation disorders, constipation) were reported in a low number of included studies. The endpoint of measuring chemotoxicity over the course of chemotherapy varied by studies. Thus, longitudinal trajectories of chemotoxicity are unclear. We only conducted meta-regressions with age variables due to inconsistent measures and statistical analyses across studies in other risk factors of chemotoxicity. Other important risk factors could require further investigation of relationships with chemotoxicity. Additionally, there may be clinical factors (e.g., years since cancer diagnosis, doses and duration of cancer treatments, comorbidities) that may moderate the relationships of age with chemotoxicity that were not explored in this study.
5. Conclusions
This study reveals chemotherapy’s impact on chemotoxicity, especially non-hematological and GI toxicity. It highlights the interplay between various factors and chemotoxicity, emphasizing the necessity for personalized strategies considering chemotoxicity risk factors such as malnutrition, frailty, certain immune and inflammatory biomarkers, and patient characteristics like age. Understanding these factors is crucial in predicting the potential harm of chemotoxicity in patients with CRC. While PROs assessments are important, clinician-reported toxicity by considering objective factors can assist in better prevention and management of chemotoxicity. Ongoing research exploring underlying mechanisms of chemotoxicity, including its subgroups and patient-centered prediction and intervention models, is crucial for optimizing patient well-being and treatment success.
Supplementary Materials
The following supporting information (tables and figures) ccan be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, CH, CB, DV.; methodology, CH, SM, TF, DV ; validation, CH, XN, CB, DS, FT, SM.; formal analysis, CH, FT.; investigation, CH, CB, DV.; data curation, CH, FT, SM.; writing—original draft preparation, CH.; writing—review and editing, CH, XN, CB, DS, FT, MK, AN, DA; visualization, CH, FT.; supervision, CB, DV. All authors have read and agreed to the published version of the manuscript.
Funding
The work was original research that had not been published previously. CH: Cancer Research Seed Grant from the Ohio State University College of Nursing and the Ohio State University Comprehensive Cancer Center. CH is also funded by the Oncology Nurse Foundation (ONF) RE03. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Institutional Review Board Statement
This is a systematic review and meta-analysis; thus, the study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
The authors affirm that this systematic review and meta-analysis has been reported in line with the PRISMA guidelines. The extracted data from the published papers supporting this study's findings are available from the corresponding author upon reasonable request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Arnold M, Abnet CC, Neale RE, et al. Global burden of 5 major types of gastrointestinal cancer. Gastroenterol. 2020;159(1):335-349.e15. [CrossRef]
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. [CrossRef]
- Wong MCS, Huang J, Lok V, et al. Differences in incidence and mortality trends of colorectal cancer worldwide based on sex, age, and anatomic location. Clin Gastroenterol Hepatol. 2021;19(5):955-966.e61. [CrossRef]
- Biller LH, Schrag D. Diagnosis and Treatment of Metastatic Colorectal Cancer: A Review. JAMA. 2021;325(7):669-685. [CrossRef]
- Chan GHJ, Chee CE. Making sense of adjuvant chemotherapy in colorectal cancer. J Gastrointest Oncol. 2019;10(6):1183-1192. [CrossRef]
- Chen Y, Cheng CS, Tan HY, Tam CW, Wang N, Feng Y. Efficacy of herbal medicines intervention for colorectal cancer patients with chemotherapy-induced gastrointestinal toxicity: A Systematic review and meta-analysis. Front Oncol. 2021;11:629132. Published 2021 Mar 25. [CrossRef]
- Feliu J, Espinosa E, Basterretxea L, et al. Prediction of chemotoxicity, unplanned hospitalizations and early death in older patients with colorectal cancer treated with chemotherapy. Cancers (Basel). 2021;14(1):127. Published 2021 Dec 28. [CrossRef]
- Rutherford C, Müller F, Faiz N, King MT, White K. Patient-reported outcomes and experiences from the perspective of colorectal cancer survivors: meta-synthesis of qualitative studies. J Patient Rep Outcomes. 2020;4(1):27. Published 2020 Apr 25. [CrossRef]
- Yazbeck V, Alesi E, Myers J, Hackney MH, Cuttino L, Gewirtz DA. An overview of chemotoxicity and radiation toxicity in cancer therapy. Adv Cancer Res. 2022;155:1-27. [CrossRef]
- Tantoy IY, Cataldo JK, Aouizerat BE, Dhruva A, Miaskowski C. A Review of the literature on multiple co-occurring symptoms in patients with colorectal cancer who received chemotherapy alone or chemotherapy with targeted therapies. Cancer Nurs. 2016;39(6):437-445. [CrossRef]
- Shaw RD, Ivatury SJ. Late and long-term symptom management in colorectal cancer survivorship. Dis Colon Rectum. 2021;64(12):1447-1450. [CrossRef]
- Han CJ, Reding KW, Kalady MF, Yung R, Greenlee H, Paskett ED. Factors associated with long-term gastrointestinal symptoms in colorectal cancer survivors in the women's health initiatives (WHI study). PLoS One. 2023;18(5):e0286058. Published 2023. 19 May. [CrossRef]
- Lee CS, Ryan EJ, Doherty GA. Gastro-intestinal toxicity of chemotherapeutics in colorectal cancer: the role of inflammation. World J Gastroenterol. 2014;20(14):3751-3761. [CrossRef]
- Han CJ, Yang GS, Syrjala K. Symptom experiences in colorectal cancer survivors after cancer treatments: a systematic review and meta-analysis. Cancer Nurs. 2020;43(3):E132-E158. [CrossRef]
- Grenon NN, Chan J. Managing toxicities associated with colorectal cancer chemotherapy and targeted therapy: a new guide for nurses. Clin J Oncol Nurs. 2009;13(3):285-296. [CrossRef]
- Magnuson A, Sedrak MS, Gross CP, et al. Development and validation of a risk tool for predicting severe toxicity in older adults receiving chemotherapy for early-stage breast cancer. J Clin Oncol. 2021;39(6):608-618. [CrossRef]
- Schiefen JK, Madsen LT, Dains JE. Instruments That Predict Oncology Treatment Risk in the Senior Population. J Adv Pract Oncol. 2017;8(5):528-533.
- Kurtz DM, Esfahani MS, Scherer F, et al. Dynamic risk profiling using serial tumor biomarkers for personalized outcome prediction. Cell. 2019;178(3):699-713.e19. [CrossRef]
- Ji J, Sun CL, Cohen HJ, Muss HB, Bae M, Sedrak MS. Toxicity risk score and clinical decline after adjuvant chemotherapy in older breast cancer survivors. J Natl Cancer Inst. 2023;115(5):578-585.
- Kotani D, Oki E, Nakamura Y, et al. Molecular residual disease and efficacy of adjuvant chemotherapy in patients with colorectal cancer. Nat Med. 2023;29(1):127-134. [CrossRef]
- Choi CS, Kin K, Cao K, et al. The association of body composition on chemotherapy toxicities in non-metastatic colorectal cancer patients: a systematic review. ANZ J Surg. 2024;94(3):327-334. [CrossRef]
- Lee S, Kang DH, Ahn TS, et al. The Impact of Pre-Chemotherapy Body Composition and Immunonutritional Markers on Chemotherapy Adherence in Stage III Colorectal Cancer Patients. J Clin Med. 2023;12(4):1423. Published 2023 Feb 10. [CrossRef]
- Basch E, Jia X, Heller G, et al. Adverse symptom event reporting by patients vs clinicians: relationships with clinical outcomes. J Natl Cancer Inst. 2009;101(23):1624-1632. [CrossRef]
- Hertz, DL. Concerns regarding use of patient-reported outcomes in biomarker studies of chemotherapy-induced peripheral neuropathy. Pharmacogenomics J. 2019;19(5):411-416. [CrossRef]
- Mitchell PH, Ferketich S, Jennings BM. Quality health outcomes model. American Academy of Nursing Expert Panel on Quality Health Care. Image J Nurs Sch. 1998;30(1):43-46. [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. [CrossRef]
- Beukers K, Voorn MJJ, Trepels R, et al. Associations between outcome variables of nutritional screening methods and systemic treatment tolerance in patients with colorectal cancer: A systematic review. J Geriatr Oncol. 2022;13(8):1092-1102. [CrossRef]
- Drami I, Pring ET, Gould L, et al. Body composition and dose-limiting toxicity in colorectal cancer chemotherapy treatment: A systematic review of the literature. Could Muscle Mass be the New Body Surface Area in Chemotherapy Dosing? Clin Oncol (R Coll Radiol). 2021;33(12):e540-e552. [CrossRef]
- Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Comparison of two methods to detect publication bias in meta-analysis. JAMA. 2006;295(6):676-680. [CrossRef]
- George BJ, Aban IB. An application of meta-analysis based on DerSimonian and Laird method. J Nucl Cardiol. 2016;23(4):690-692. [CrossRef]
- Ali R, Baracos VE, Sawyer MB, et al. Lean body mass as an independent determinant of dose-limiting toxicity and neuropathy in patients with colon cancer treated with FOLFOX regimens. Cancer Med. 2016;5(4):607-616. [CrossRef]
- Aparicio T, Lavau-Denes S, Phelip JM, et al. Randomized phase III trial in elderly patients comparing LV5FU2 with or without irinotecan for first-line treatment of metastatic colorectal cancer (FFCD 2001-02). Ann Oncol. 2016;27(1):121-127. [CrossRef]
- Backshall A, Sharma R, Clarke SJ, Keun HC. Pharmacometabonomic profiling as a predictor of toxicity in patients with inoperable colorectal cancer treated with capecitabine. Clin Cancer Res. 2011;17(9):3019-3028. [CrossRef]
- Barret M, Malka D, Aparicio T, et al. Nutritional status affects treatment tolerability and survival in metastatic colorectal cancer patients: results of an AGEO prospective multicenter study. Oncology. 2011;81(5-6):395-402. [CrossRef]
- Beukers K, Bessems SAM, van de Wouw AJ, et al. Associations between the Geriatric-8 and 4-meter gait speed test and subsequent delivery of adjuvant chemotherapy in older patients with colon cancer. J Geriatr Oncol. 2021;12(8):1166-1172. [CrossRef]
- Breton C, Aparicio T, Le Malicot K, et al. Predictive factors of severe early treatment-related toxicity in patients receiving first-line treatment for metastatic colorectal cancer: Pooled analysis of 2190 patients enrolled in Fédération Francophone de Cancérologie Digestive (FFCD) trials. Eur J Cancer. 2021;153:40-50. [CrossRef]
- Brown JC, Meyerhardt JA, Cespedes Feliciano EM, Cheng E, Caan BJ. The association of abdominal adiposity with premature discontinuation of postoperative chemotherapy in colon cancer. Clin Nutr. 2022;41(7):1600-1604. [CrossRef]
- Cespedes Feliciano EM, Lee VS, Prado CM, et al. Muscle mass at the time of diagnosis of nonmetastatic colon cancer and early discontinuation of chemotherapy, delays, and dose reductions on adjuvant FOLFOX: The C-SCANS study. Cancer. 2017;123(24):4868-4877. [CrossRef]
- Decoster L, Kenis C, Naessens B, et al. Integrating geriatric assessment in the first line chemotherapy treatment in older patients with metastatic colorectal cancer: Results of a prospective observational cohort study (AVAPLUS). J Geriatr Oncol. 2018;9(2):93-101. [CrossRef]
- Folprecht G, Seymour MT, Saltz L, et al. Irinotecan/fluorouracil combination in first-line therapy of older and younger patients with metastatic colorectal cancer: combined analysis of 2,691 patients in randomized controlled trials. J Clin Oncol. 2008;26(9):1443-1451. [CrossRef]
- Gallois C, Artru P, Lièvre A, et al. Evaluation of two nutritional scores' association with systemic treatment toxicity and survival in metastatic colorectal cancer: an AGEO prospective multicentre study. Eur J Cancer. 2019;119:35-43. [CrossRef]
- Garg MB, Lincz LF, Adler K, Scorgie FE, Ackland SP, Sakoff JA. Predicting 5-fluorouracil toxicity in colorectal cancer patients from peripheral blood cell telomere length: a multivariate analysis. Br J Cancer. 2012;107(9):1525-1533. [CrossRef]
- Grimes, C. , Sarcopenia and Tolerance of Chemotherapy in Patients with Stage III Colon Cancer. 2022, Doctoral dissertation, Rush University.
- Hochster HS, Luo W, Popa EC, et al. Phase II study of uracil-tegafur with leucovorin in elderly (> or = 75 years old) patients with colorectal cancer: ECOG 1299. J Clin Oncol. 2007;25(34):5397-5402. [CrossRef]
- Jung HW, Kim JW, Kim JY, et al. Effect of muscle mass on toxicity and survival in patients with colon cancer undergoing adjuvant chemotherapy. Support Care Cancer. 2015;23(3):687-694. [CrossRef]
- Karabulut S, Dogan I, Usul Afsar C, et al. Does nutritional status affect treatment tolerability, chemotherapy response and survival in metastatic gastric cancer patients? Results of a prospective multicenter study in Turkey. J Oncol Pharm Pract. 2022;28(1):127-134. [CrossRef]
- Li M, Chen J, Deng Y, et al. Risk prediction models based on hematological/body parameters for chemotherapy-induced adverse effects in Chinese colorectal cancer patients. Support Care Cancer. 2021;29(12):7931-7947. [CrossRef]
- Looijaard SMLM, Meskers CGM, Slee-Valentijn MS, et al. Computed tomography-based body composition is not consistently associated with outcome in older patients with colorectal cancer. Oncologist. 2020;25(3):e492-e501. [CrossRef]
- Okada S, Yamazaki S, Kaiga T, Funada T, Kochi M, Takayama T. Impact of nutritional status in the era of FOLFOX/FIRI-based chemotherapy. World J Surg Oncol. 2017;15(1):162. Published 2017 Aug 24. [CrossRef]
- Osterlund P, Ruotsalainen T, Korpela R, et al. Lactobacillus supplementation for diarrhoea related to chemotherapy of colorectal cancer: a randomised study. Br J Cancer. 2007;97(8):1028-1034. [CrossRef]
- Retornaz F, Guillem O, Rousseau F, et al. Predicting Chemotherapy Toxicity and Death in Older Adults with Colon Cancer: Results of MOST Study. Oncologist. 2020;25(1):e85-e93. [CrossRef]
- Sastre J, Grávalos C, Rivera F, et al. First-line cetuximab plus capecitabine in elderly patients with advanced colorectal cancer: clinical outcome and subgroup analysis according to KRAS status from a Spanish TTD Group Study. Oncologist. 2012;17(3):339-345. [CrossRef]
- Seymour MT, Thompson LC, Wasan HS, et al. Chemotherapy options in elderly and frail patients with metastatic colorectal cancer (MRC FOCUS2): an open-label, randomised factorial trial. Lancet. 2011;377(9779):1749-1759. [CrossRef]
- Stein A, Quidde J, Schröder JK, et al. Capecitabine in the routine first-line treatment of elderly patients with advanced colorectal cancer--results from a non-interventional observation study. BMC Cancer. 2016;16:82. Published 2016 Feb 10. [CrossRef]
- Tominaga T, Nonaka T, Sumida Y, Hidaka S, Sawai T, Nagayasu T. The C-Reactive Protein to Albumin Ratio as a predictor of severe side effects of adjuvant chemotherapy in Stage III colorectal cancer patients. PLoS One. 2016;11(12):e0167967. Published 2016 Dec 8. [CrossRef]
- Tsuchihashi K, Ito M, Moriwaki T, et al. Role of predictive value of the modified glasgow prognostic score for later-line chemotherapy in patients with metastatic colorectal cancer. Clin Colorectal Cancer. 2018;17(4):e687-e697. [CrossRef]
- Watanabe A, Yang CC, Cheung WY. Association of baseline patient characteristics with adjuvant chemotherapy toxicities in stage III colorectal cancer patients. Med Oncol. 2018;35(10):125. Published 2018 Aug 16. [CrossRef]
- Yamada Y, Takahari D, Matsumoto H, et al. Leucovorin, fluorouracil, and oxaliplatin plus bevacizumab versus S-1 and oxaliplatin plus bevacizumab in patients with metastatic colorectal cancer (SOFT): an open-label, non-inferiority, randomised phase 3 trial [published correction appears in Lancet Oncol. 2014 Jan;15(1):e4]. Lancet Oncol. 2013;14(13):1278-1286. [CrossRef]
- Antonio M, Carmona-Bayonas A, Saldaña J, et al. Factors predicting adherence to a tailored-dose adjuvant treatment on the basis of geriatric assessment in elderly people with colorectal cancer: A prospective study. Clin Colorectal Cancer. 2018;17(1):e59-e68.
- Zanuso V, Fregoni V, Gervaso L. Side effects of adjuvant chemotherapy and their impact on outcome in elderly breast cancer patients: a cohort study. Future Sci OA. 2020;6(9):FSO617. [CrossRef]
- Reck M, Wehler T, Orlandi F, et al. Safety and patient-reported outcomes of atezolizumab plus chemotherapy with or without bevacizumab versus bevacizumab plus chemotherapy in non-small-cell lung cancer. J Clin Oncol. 2020;38(22):2530-2542. [CrossRef]
- Jordan T, Nuamek T, Fornacon-Wood I, et al. A study demonstrating users' preference for the adapted-REQUITE patient-reported outcome questionnaire over PRO-CTCAE® in patients with lung cancer. Front Oncol. 2024;14:1328871. Published 2024 Apr 10. [CrossRef]
- Naeem Tahir, Jerome H. Goldschmidt, Eva Culakova, Marek S. Poniewierski, Debra A. Wolff, David C. Dale, Jeffrey Crawford, Gary H. Lyman. Assessment of Hematologic and non-hematologic toxicity in older cancer patients receiving systemic chemotherapy: Results from a prospective nationwide registry. Blood 2004; 104 (11): 3131. [CrossRef]
- Podolski, AJ. , and Rasim Gucalp. "GI Toxicities from Cancer Therapy." In Geriatric Gastroenterology, pp. 341-379. Cham: Springer International Publishing, 2021.
- Aprile G, Rihawi K, De Carlo E, Sonis ST. Treatment-related gastrointestinal toxicities and advanced colorectal or pancreatic cancer: A critical update. World J Gastroenterol. 2015;21(41):11793-11803. [CrossRef]
- Ba Y, Shi Y, Jiang W, et al. Current management of chemotherapy-induced neutropenia in adults: key points and new challenges: Committee of Neoplastic Supportive-Care (CONS), China Anti-Cancer Association Committee of Clinical Chemotherapy, China Anti-Cancer Association. Cancer Biol Med. 2020;17(4):896-909. [CrossRef]
- Ju M, Gao Z, Gu G, et al. Prognostic value of circulating tumor cells associated with white blood cells in solid cancer: a systematic review and meta-analysis of 1471 patients with solid tumors. BMC Cancer. 2023;23(1):1224. Published 2023 Dec 12. [CrossRef]
- Todoric J, Antonucci L, Karin M. Targeting inflammation in cancer prevention and therapy. Cancer Prev Res (Phila). 2016;9(12):895-905. [CrossRef]
- Vijay A, Valdes AM. Role of the gut microbiome in chronic diseases: a narrative review. Eur J Clin Nutr. 2022;76(4):489-501. [CrossRef]
- Li D, Sun CL, Kim H, et al. Geriatric Assessment-Driven Intervention (GAIN) on chemotherapy-related toxic effects in older adults with cancer: A randomized clinical trial. JAMA Oncol. 2021;7(11):e214158. [CrossRef]
- Caan BJ, Meyerhardt JA, Brown JC, et al. Recruitment strategies and design considerations in a trial of resistance training to prevent dose-limiting toxicities in colon cancer patients undergoing chemotherapy. Contemp Clin Trials. 2021;101:106242. [CrossRef]
- Denise de Lima Bezerra A, Matias de Sousa I, Silva de Souza AP, Miranda de Carvalho AL, Trussardi Fayh AP. Early nutritional intervention does not prevent long-term adverse events in women with breast cancer: A pilot study. Clin Nutr ESPEN. 2023;53:268-273. [CrossRef]
Figure 1.
Conceptual Framework- Quality Health Outcomes Model. Adapted from Mitchell et al. [25].
Figure 1.
Conceptual Framework- Quality Health Outcomes Model. Adapted from Mitchell et al. [25].
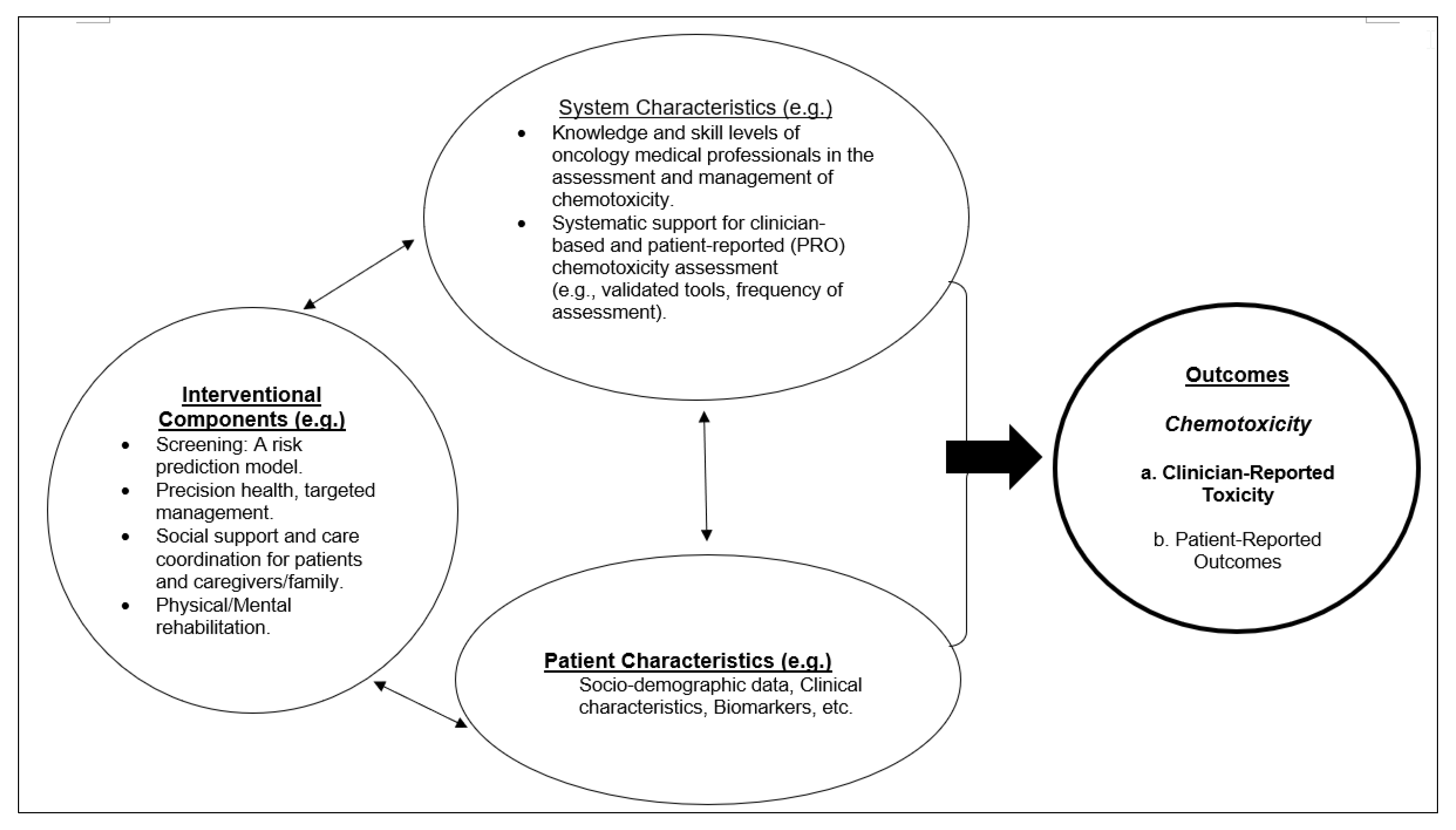
Figure 2.
The PRISMA 2020 Flow Diagram.
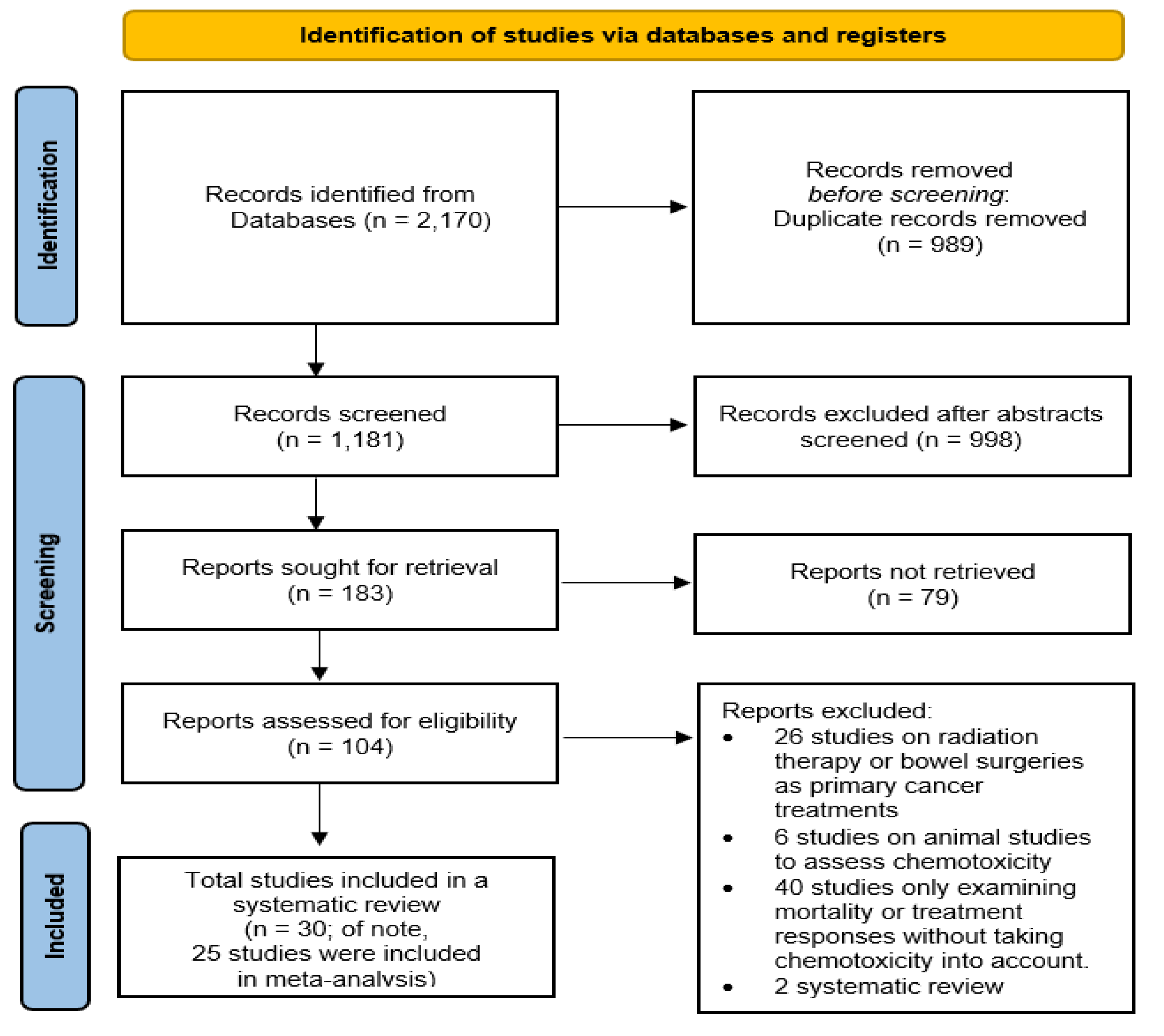
Figure 3.
Funnel Plot Publication Bias (based on the 17 articles, reporting prevalences of overall moderate-to-severe chemotoxicity data).
Figure 3.
Funnel Plot Publication Bias (based on the 17 articles, reporting prevalences of overall moderate-to-severe chemotoxicity data).
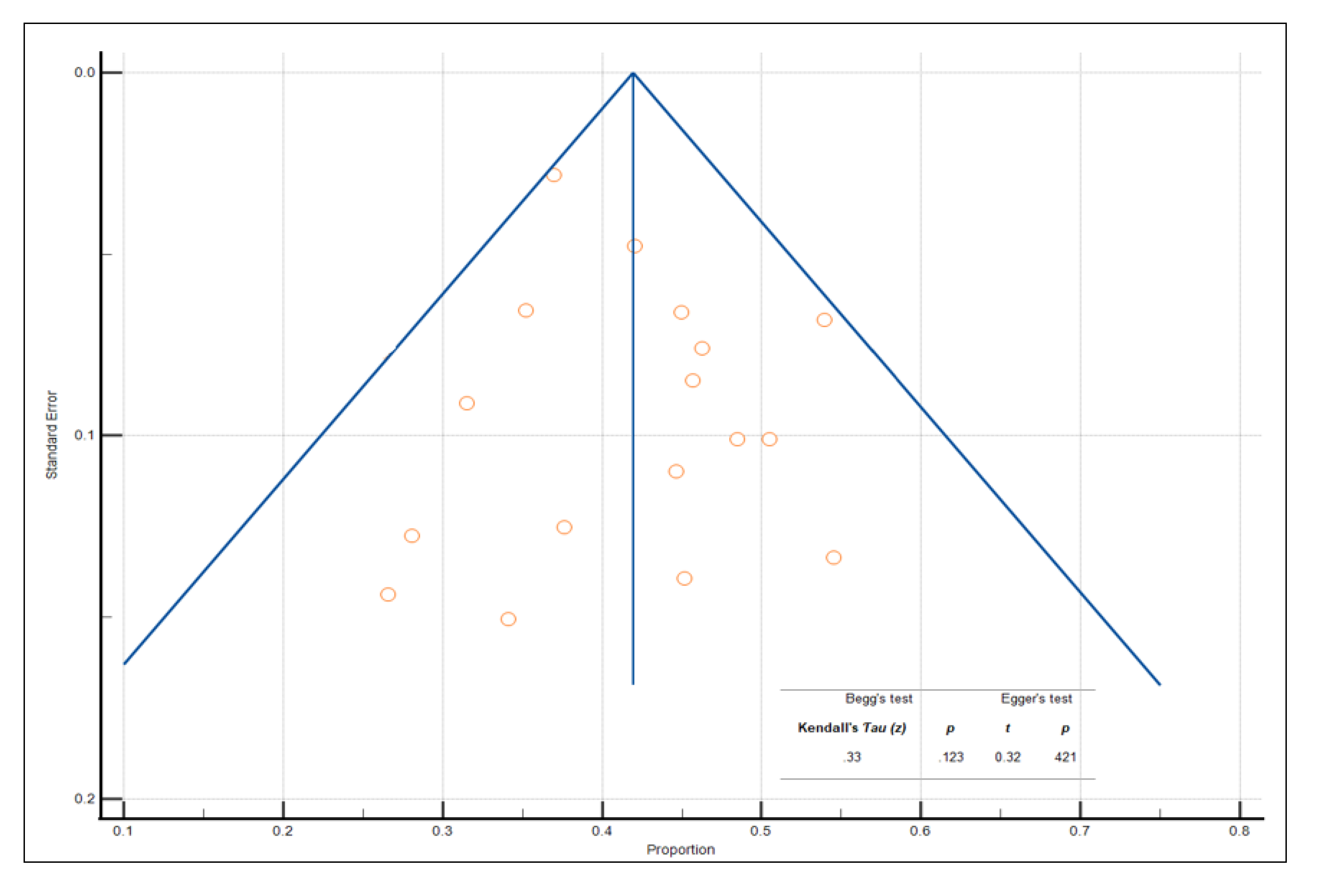
Figure 4.
Forest Plots for Pooled Prevalences of Moderate-to-Severe Chemotoxicity (Overall, Non-Hemaotologcial and Hematological Toxicities).
Figure 4.
Forest Plots for Pooled Prevalences of Moderate-to-Severe Chemotoxicity (Overall, Non-Hemaotologcial and Hematological Toxicities).
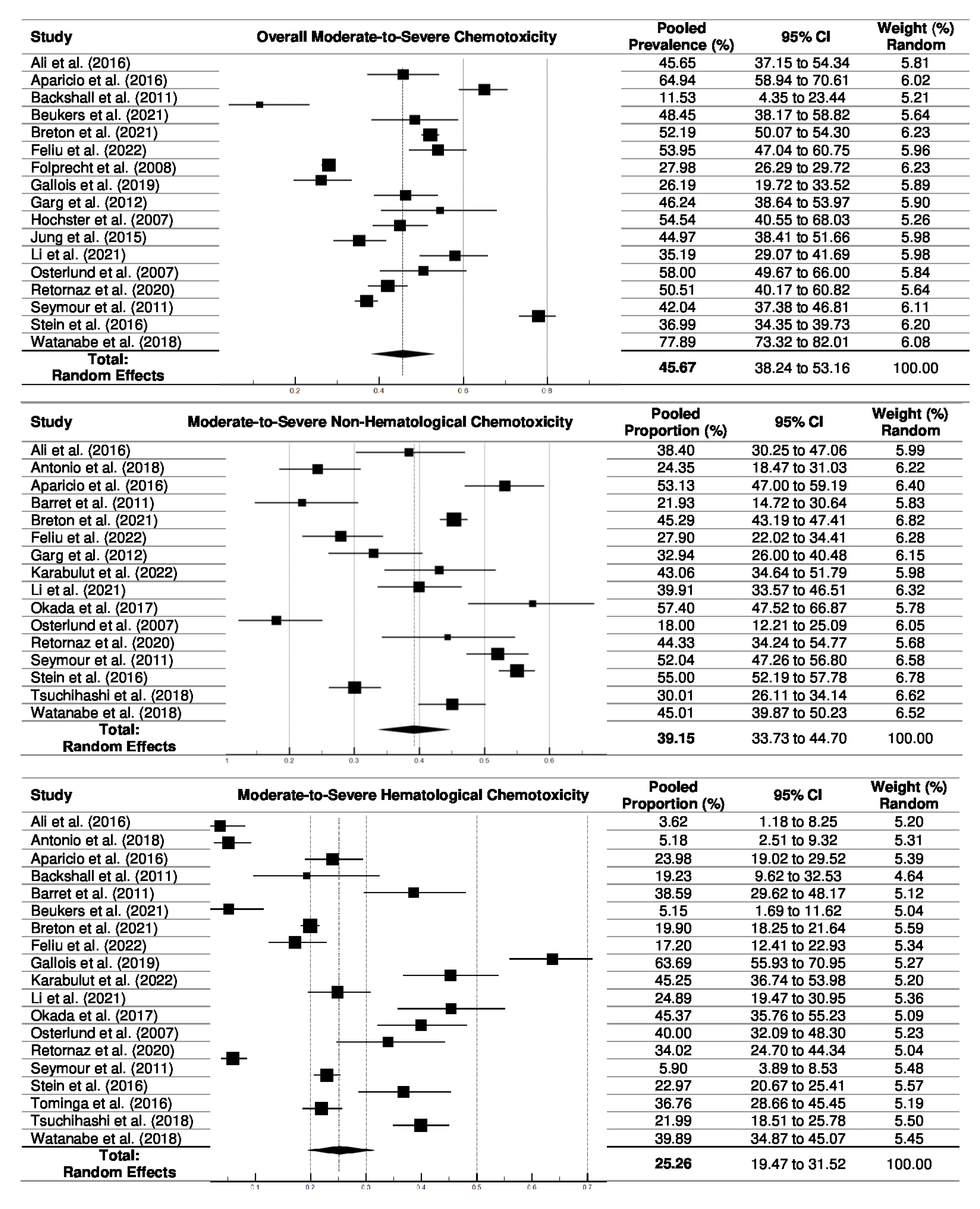
Figure 5.
Forest Plots for Pooled Prevalences of Mild Chemotoxicity (Overall, Non-Hemaotologcial and Hematological Toxicities).
Figure 5.
Forest Plots for Pooled Prevalences of Mild Chemotoxicity (Overall, Non-Hemaotologcial and Hematological Toxicities).
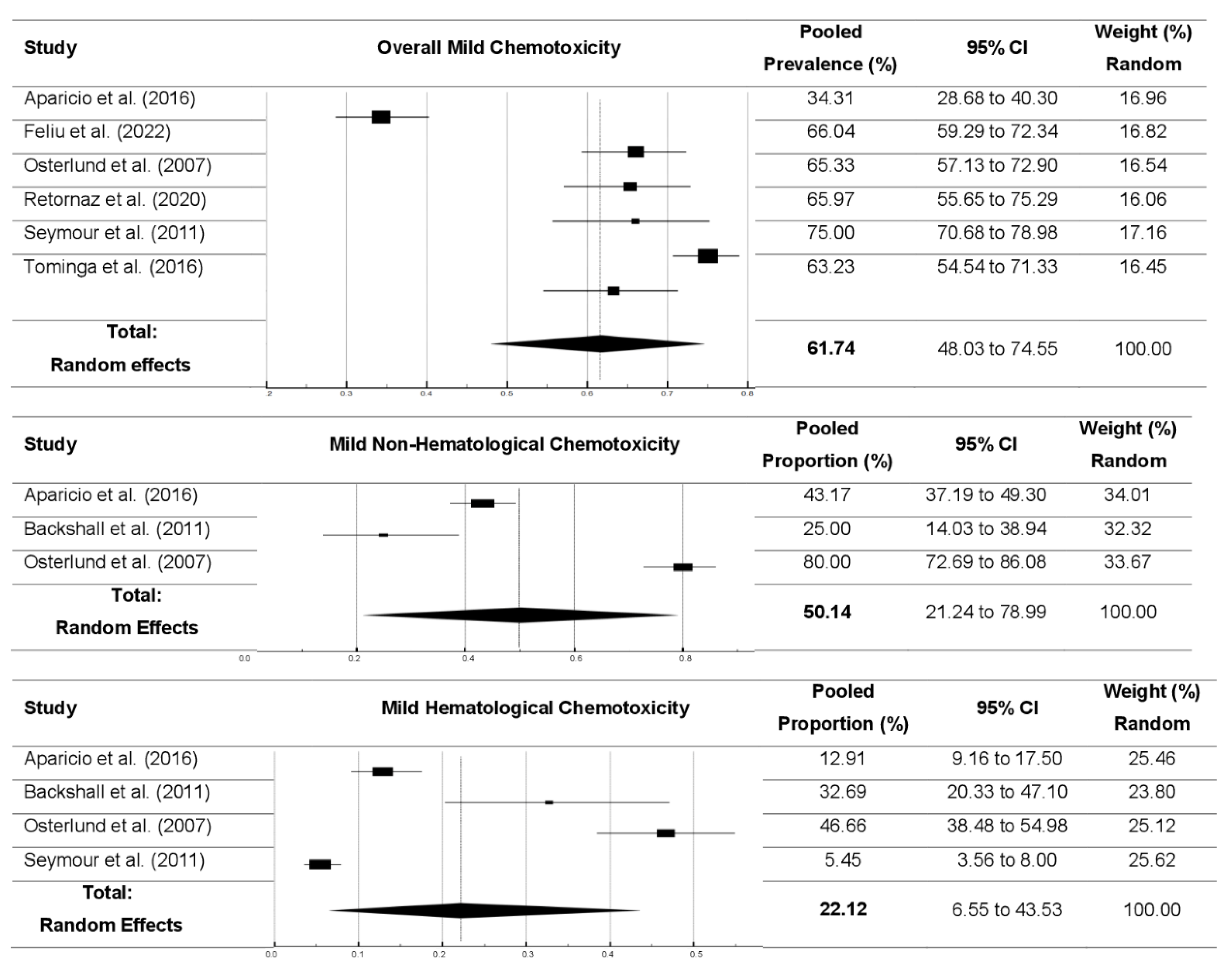
Table 5.
Meta-Analyses: Relationships of Age with Prevalence of Chemotoxicity (moderate-to-severe levels).
Table 5.
Meta-Analyses: Relationships of Age with Prevalence of Chemotoxicity (moderate-to-severe levels).
| A. Meta-Regressiona: Age (continuous variable) and the prevalence of chemotoxicity | ||||||||||||||||||||||
| Unadjusted analyses | Adjusted analysesb | Sample n | ||||||||||||||||||||
| Age (y.o.): predictor | Unstandardizedc B | Standardizedc β | Unstandardizedc B | Standardizedc β | ||||||||||||||||||
| B(SE) | t | pd | β (SE) | t | pd | B (SE) | t | pd | β (SE) | t | pd | |||||||||||
| Overall chemotoxicity | 0.54 (0.49) |
.03 | .512 | 0.62 (0.25) |
.47 | .640 | 0.44 (0.32) |
.01 | .211 | 0.56 (0.33) | .35 | .879 | 8,819 | |||||||||
| Non-Hematological chemotoxicity | 0.40 (0.40) |
.11 | .413 | 0.89 (0.97) |
.35 | .396 | 0.35 (0.29) |
.21 | .314 | 0.93 (0.34) | .12 | .145 | 6,602 | |||||||||
| Hematological chemotoxicity | 0.41 (0.38) |
.09 | .331 | 0.76 (0.51) |
.15 | .574 | 0.51 (0.43) |
.04 | .421 | 1.21 (0.45) | .41 | .652 | 6,882 | |||||||||
| Neutropenia | -1.09 (0.56) |
2.13 | .003 | -1.78 (0.54) |
2.41 | .002 | -1.01 (0.41) |
3.12 | .003 | -1.44 (0.39) | 1.98 | .004 | 8,227 | |||||||||
| Nausea/ Vomiting |
1.32 (0.85) |
3.13 | .028 | 1.72 (0.56) |
3.35 | .001 | 1.14 (0.72) |
2.19 | .012 | 1.65 (0.56) |
3.12 | .001 | 5,089 | |||||||||
| Diarrhea | 1.05 (0.31) |
2.41 | .012 | 1.51 (0.29) |
3.16 | .004 | 1.01 (0.31) |
2.41 | .001 | 1.33 (0.32) | 2.91 | .005 | 7,209 | |||||||||
| GI toxicity | 1.02 (0.44) |
3.01 | .044 | 1.97 (0.43) |
2.11 | .005 | 1.03 (0.35) |
2.98 | <.001 | 1.85 (0.32) | 2.53 | .001 | 9,489 | |||||||||
| B. Age group and the prevalence of chemotoxicity (Meta-ANOVA and Meta-Regression) | ||||||||||||||||||||||
| Meta-Anova | Meta-Regression | |||||||||||||||||||||
| Adult Group (All participants’ age range from > 18 to < 65 years old) |
Older Adult Group (All participants’ age > 65 years old) |
F/pd | Adjusted ORb (95% CI) Ref. adult group |
|||||||||||||||||||
| Mean (SD) | Sample n | Mean (SD) | Sample n | |||||||||||||||||||
| Overall Chemotoxicity | 43.5(5.1) | 7,916 | 49.8 (5.3) | 903 | 4.898, .002 | 1.14 (1.01, 1.56), p =.045 | ||||||||||||||||
| Non-Hematological chemotoxicity | 39.6 (3.8) | 5,476 | 37.4(6.8) | 1,126 | 0.214, .643 | 0.84 (0.75, 1.32), p =.984 | ||||||||||||||||
| Hematological chemotoxicity |
24.3 (4.4) | 5,483 | 22.0 (8.4) | 1,399 | 0.106, .745 | 1.35 (0.85, 1.56), p =.845 | ||||||||||||||||
| Neutropenia | 24.3 (6.9) | 7,396 | 13.7 (4.7) | 831 | 5.382, .002 | 0.65 (0.32, 0.95), p =.031 | ||||||||||||||||
| Nausea/Vomiting | 22.9 (5.2) | 4,498 | 18.3 (7.6) | 591 | 0.045, .831 | 0.98 (0.75, 1.32), p =.652 | ||||||||||||||||
| Diarrhea | 14.2 (2.9) | 6,007 | 16.8 (4.3) | 1,202 | 3.214, .003 | 1.27 (1.05, 1.95), p =.003 | ||||||||||||||||
| GI toxicity | 18.1 (4.2) | 8,472 | 25.9 (4.8) | 1,017 | 2.494, <.001 | 1.65 (1.12, 2.01), p =.026 | ||||||||||||||||
Note. Age: at the time of surveys; GI: gastrointestinal; SD: standard deviation; SE: standard error. a Weighted least squares were applied (i.e., sample size weight adjustment). Types of chemotoxicity were selected only if the number of studies measuring the chemotoxicity was > 10. bAdjusted regression models included prevalent cancer stages, metastatic status, cancer types, sample size (group categories), and sex group variables. c Unstandardized B Coefficient is interpreted as all other variables held constant, an increase of 1-year-old in age is associated with an average change of Beta units in the prevalence of chemotoxicity (moderate-to-severe). The standardized β (Beta) Coefficient is interpreted as, for every one standard deviation increase in age, the outcome variables are expected to increase by β standard deviations, holding other variables constant. dp value of <.05 was considered statistically significant. Significant findings (p <.05) were highlighted in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



