
Submitted:
13 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
Objectives. To show the superiority of eccentric versus concentric strengthening in terms of improving quadriceps strength in knee osteoarthritis (OA). A randomized controlled study was conducted to perform 12 sessions of either eccentric or concentric isokinetic muscle strengthening over 6 weeks Methods. We recruited males and females, aged between 40 and 70 years, with predominantly unilateral femorotibial OA. Exclusion criteria were having a prosthesis, inflammatory arthritis or flare-up of OA, symptomatic patellofemoral OA, cardio-vascular or pulmonary disease that could be a contraindication to the study treatment, and any pathology that could cause muscle weakness. The primary endpoint was the between-group difference in change in maximum concentric isokinetic knee extension peak torque (PT) at 60°/s on the OA side at 6 weeks. Secondary endpoints were between-group difference in change in concentric hamstring PT at 60°/s; eccentric quadriceps and hamstring PT at 30°/s; 10 m and 200 m walking speeds; pain and functional status (WOMAC score) at 6 weeks and 6 months. Results. The sample consisted of 11 females and 27 males, with a mean age of 57.7 ±7.52 years and a body mass index (BMI) of 25.95 ±3.93 kg/m². Quadriceps strength increased more at 6 weeks in the concentric than the eccentric group with no statistical difference. There was a rate of 25% major adverse events in the eccentric group. Conclusion. Eccentric training resulted in a smaller improvement in quadriceps strength than concentric training and was associated with a high risk of muscle injury, particularly to the hamstring muscles.
Keywords:
osteoarthritis
; knee
; eccentric
; concentric
; rehabilitation
1. Introduction
Osteoarthritis (OA) affects an estimated 10 million people, 4.6 million of whom have symptomatic OA [1]. This figure is expected to increase with the ageing of the population [2]. Osteoarthritis has an undeniable impact on functional capacity, which places it among the leading causes of disability in Western societies [3]. The knee is the second most frequent symptomatic OA site, with the medial femorotibial compartment affected in more than 2/3 of cases [4,5]. This is associated with a loss of lower limb muscle strength, particularly of the quadriceps muscle. This muscle weakness is not only a cause of pain and instability, but also contributes to the disease progression [6]. The degree of quadriceps muscle strength loss also appears to correlate with the intensity of pain and the extent of the functional disability [7,8,9]. Conversely, people with higher levels of strength have less pain and less functional disability [10]. The value of physical exercise and muscle strengthening in OA has been demonstrated [3,11].
Isokinetic devices provide reliable, reproducible, and validated measurements of force in a dynamic configuration, which is more functional than measurements obtained during isometric contractions. They can also be used to provide precise training programs. Isokinetic training producing contractions at a constant speed, using a dynamometer whose resistance is self-adapted to the force developed by the individual [9]. Several studies have demonstrated the benefits of isokinetic strengthening in the management of knee OA [10,11,12,13,14]. In addition to its effectiveness in improving muscle strength and function, eccentric isokinetic training has advantages over concentric training in terms of cardiovascular tolerance [15]. However, studies of good methodological quality comparing isokinetic rehabilitation to other validated rehabilitation techniques are relatively rare, making it impossible to draw definitive conclusions regarding the most effective methods [16]. Eccentric (ECC) muscle performance, particularly of the quadriceps, plays an essential role in activities of daily living such as walking and descending stairs. The gain in muscular strength after ECC training is reported to be greater than after concentric (CONC) training [17], with a lower energy cost [18,19,20]. In addition, isokinetic dynamometers can be adapted to the motor performance and tolerance of the person, thus limiting the occurrence of injury in people with impaired physical capacities [21].
The main aim of this study was to show the superiority of 12 sessions of ECC exercise over 12 sessions of CONC exercise in improving quadriceps muscle strength in people with femorotibial OA. The secondary objectives were to evaluate isokinetic muscle strengthening in ECC mode, pain reduction and functional improvement in the parameters of walking (maximum speed over 10 and 200 meters), functional status of the patient using the Western Ontario and MacMaster Universities osteoarthritis index [22] and the adherence..
2. Materials and Methods
Design
We conducted a randomized controlled trial. Participants were randomly allocated to 1 of 2 groups (ECC or CONC training) in a 1:1 ratio. The randomization list was generated by block randomization and performed automatically using Stata software by an independent statistician after verification of eligibility and signing of informed consent. The study was approved by the CPP SUD EST VI (No 2011-A00894-37) ethical committee, and all participants provided written consent for participation. The study was registered on clinical trials CT NCT01586130. The results are reported in accordance with the CONSORT guidelines for non-pharmacological trials.
Participants
Participants were recruited from Clermont-Ferrand University Hospital Rehabilitation Medicine department. Outpatient followed in consultation for knee OA were included. The inclusion criteria were males and females aged between 40 and 75 years with unilateral, medial, femorotibial OA of moderate radiological stage (graded 1-3 according to the Kellgren and Lawrence classification), with no contraindications to the training protocols evaluated. Exclusion criteria were having a prosthetic knee, inflammatory arthritis, or flare-up of OA, symptomatic patellofemoral OA, cardio-vascular or pulmonary disease that could contraindicate performance of the training protocols, and any pathology that could cause muscle weakness.
During the inclusion visit, participants underwent a general clinical examination, an electrocardiogram, and additional examinations in case of cardiac abnormality (stress test and cardiological assessment). Baseline outcomes were also measured (see Outcomes section below). The initial maximal moment of force was measured using the Cybex HumacNorm® isokinetic dynamometer. Patients will familiarize themselves with testing procedures by performing three consecutive warmup trials for each muscle group and speed. During tests the subjects will perform five maximal continuous flexion-extension repetitions of both legs at each angular velocity: A 1-minute rest will be allowed between each contraction speed.A 5-minute rest will be allowed between legs. The best repetition among 5 will be kept.
This measurement was used to determine the initial training intensity.
Interventions
The interventions were performed by a team of physiotherapists from the Clermont-Ferrand University hospital who were not blinded to group allocation.
The interventions consisted of 12 sessions of quadriceps and hamstring muscle strengthening of the OA knee using the Cybex HumacNorm® isokinetic dynamometer. The exercises were either exclusively eccentric (intervention group) or exclusively concentric (control group). Sessions were performed twice per week over 6 weeks and had to be at least 48 hours apart.
Each session began with a warm-up on a static bike for 5 minutes at low rate and low load.. The concentric group performed 3 sets of 10 repetitions of extension/flexion at adapted effort at a speed of 60°/s, for a total of 30 repetitions. The eccentric group performed 3 sets of 10 repetitions of extension/flexion at a speed of 30°/s for a total of 30 repetitions. Each repetition was followed by a 20s rest and 1 mn between sets.
The intensity was increased progressively over the sessions. The 1st session was performed at 60% of the initial maximal moment of force, and the intensity was increased by 10% at each session, up to the 6th session if tolerated. In the event of fatigue or muscle pain during a session, the intensity was set at the level of the previous session. We therefore chose to quantitatively progress the exercises by asking participants to develop maximal torque with no pain at each repetition.
Participants were instructed to develop a maximum force torque without pain on each repetition and visual on the PC screen and standardized verbal feedback were provided to increase motivation.
Outcomes
Outcomes were measured at baseline, 6 weeks (short-term assessment, directly at the end of the training sessions) and at 6 months (medium-term assessment). The same physician who was blinded to group allocation performed all the assessments.
The primary endpoint was the change in concentric isokinetic knee extension peak torque (PT) at 60°/s on the OA side from baseline to 6 weeks.
Secondary endpoints were change in: concentric hamstring PT at 60°/s; eccentric quadriceps and hamstring PT at 30°/s; 10m and 200m walking speeds; pain (VAS rating); and WOMAC score from baseline to 6 weeks and baseline to 6 months.
Pain were assessed using a visual analogue scale (VAS) from 0 to 100 before and after each session.
Adherence was measured by the number of sessions performed (maximum 12).
The WOMAC osteoarthritis index, a self-rated questionnaire validated for lower limb OA, was used to grade the impact of the OA on the person’s health status. The index is composed of 24 items grouped into 3 dimensions: pain (A), stiffness (B) and functional capacity (C).
Statistics
The sample size estimation was estimated for a 15% greater increase in the muscle strength of the quadriceps of the OA knee in the ECC group than the CONC group, with an SD of 20%, according to the results of Huang et al [10] and Tuzun et al [11] for concentric training. Therefore, for a two-sided type I error of 5% and a statistical power at 90%, 40 participants were required per group. The rate of losses to follow-up for the primary endpoint after treatment was considered negligible [11]. The high number of major adverse events motivated the promotor of study to carry out an interim analysis to decide if the study should be continued.
The continuous variables are expressed by mean and SD or median and interquartile range, according to the normality of their distribution (verified using the Shapiro-Wilk test). The primary analysis was conducted by intention-to-treat with the last observation carried forward imputation approach for missing data (because the primary outcome was not measured or because the person stopped the study due to an adverse event). A per-protocol analysis was also carried out for participants with no missing data for the primary endpoint at 6 weeks. Between-group comparisons of change in the quadriceps and hamstring PT at 6 weeks and 6 months and disability at 6 weeks and 6 months were performed with the Student t test or the Mann-Whitney test if the assumptions for the t test were not met. The homoscedasticity was analyzed using the Fisher-Snedecor test. The results were expressed using effect-sizes and 95% CI. Between-group comparisons of categorical variables were performed with the Chi-squared or Fisher’s exact test. Multivariate analysis was conducted to adjust the post-intervention results on the WOMAC score and the initial maximal moment of force assessed at inclusion. All statistical analyses were performed using Stata software (version 15, StataCorp, College Station US) for a two-sided type I error at 5%. Because of the potential for type 1 error due to multiple comparisons, findings from the secondary endpoint analyses were considered as exploratory.
Ethics
Participant consent was obtained in writing and the study was approved by the CPP SUD EST VI (No 2011-A00894-37). The study has been registered on clinical trials CT NCT01586130.
3. Results
3.1. Sample
Forty people were included between February 2012 and August 2014. Two withdrew consent before randomization, therefore 38 were randomly allocated to the ECC or CONC groups. (Figure 1) Demographics and baseline data did not differ between groups. (Table 1) The sample consisted of 11 females and 27 males, with a mean age of 57.7 (7.52) years and a body mass index (BMI) of 25.95 (3.93) kg/m².
3.2. Adverse Events and Adherence
Four major adverse events that justified withdrawal of the participant from the training program occurred; all 5 were in the ECC group. Four occurred during the muscle strengthening sessions and 1 at the 6-week assessment. The rate of adverse events in the ECC group was thus 26.3%. In contrast, no adverse events occurred in the CONC group (p=0.046). In total, 13/15 (86%) of participants in the CONC group and 13/17 (76.5%) in the ECC group (p=0.66) completed all sessions.
3.3. Primary Outcome
At 6-weeks, the change in concentric knee extension PT was greater in the CONC than the ECC group, although the difference was not significant (CONC: +28 Nm/kg; 95% CI, -17 to 55; ECC 10 Nm/kg; -100 to 52) (p=0.34, ES = 0.32; -0.32 to 0.96) (Table 2). The per-protocol analysis confirmed these findings with p=0.97 (ES = 0.14; -0.58 to 0.85) (CONC 37 Nm/kg; 95% CI -3 to 66; ECC 20 Nm/kg; 10 to 61]. Concentric quadriceps PT was significantly higher in the CONC group (p=0.04, ES = 0.67; 95% CI 0.01 to 1.32). Multivariate analysis confirmed the findings (p=0.04).
3.4. Secondary Outcomes
None of the secondary outcomes differed between groups at 6 weeks or 6 months (Table 3).
4. Discussion
This randomized controlled trial did not find a short-term (6 weeks) superiority of ECC muscle training over CONC training on concentric quadriceps muscle strength in people with knee OA, in contrast with our hypothesis. Furthermore, tolerance of the ECC contraction mode was very poor. A high proportion (12.5%) of major adverse events occurred, which justified the withdrawal of the participants concerned and resulted in premature cessation of the study at the half of the inclusions.
Unmasking revealed that these events occurred exclusively in the ECC group. Four events occurred during the muscle strengthening sessions and the fifth occurred during the 6-week evaluation. Four hamstring muscle lesions occurred: a stage 3 myoaponeurotic lesion of the biceps femoris according to the classification of Rodineau and Durey [23] and 3 elongation-type lesions. The fifth adverse event was an intolerance of eccentric work which occurred progressively across the sessions and prevented continuation. In contrast, no such major adverse events occurred in the CONC group. In addition, hamstring strength reduced by around 20% at 12 weeks and 6 months following the ECC training. Therefore, the main result of this study is that maximum eccentric hamstring contraction strengthening training comports a risk of injury in people with knee OA.
Preventive measures had been put in place to limit muscle injuries. Exercise, particularly eccentric, are known to cause delayed onset muscle soreness (DOMS) [24]. DOMS generally occurs 8 hours after the end of the exercise and includes a combination of pain, stiffness, loss of active mobility and reduction in strength. The peak of the symptomatology is normally reached at 48 hours and then gradually fades over a week. Therefore, if DOMS occurred during the first training sessions, especially in this sample of non-athletic individuals, it was expected to disappear as the sessions progressed [25]. In addition, a minimum delay of 48 hours between training sessions and 1 week between the last training session and the second evaluation was observed to minimize the impact of DOMS on performance. Furthermore, the exercises were progressed over the sessions by increasing the number of repetitions, as is more often the case in recent studies on the subject [10]. The Cybex Humac Norm® dynamometer did not allow an exercise intensity to be set relative to the moment of maximum force.
The short- and medium-term analyses showed that both CONC and ECC contraction modes improved quadriceps strength, in line with the data in the literature [26]. The beneficial effect of concentric strengthening on quadriceps muscle strength had already been shown [26]. Strength also increased on the non-trained side. This "cross effect" phenomenon of muscle strengthening is well known and is in line with the data in the literature [27,28,29].
Regarding the self-evaluation of function using the WOMAC questionnaire, there was no statistically significant difference between the two groups. The participants included in this study had early-stage OA; therefore, the impact and change in functional level was not very marked. With regards to pain intensity at inclusion, there was no between group difference. VAS pain ratings are relatively reliable and reproducible, it is therefore unlikely that the initial maximal strength evaluation was affected by pain.
Limitations
With regards to the primary outcome, we chose to evaluate concentric, rather than eccentric, strength before and after the strengthening protocol because of its preferential and validated use as a measure of muscle strength and good reproducibility of results at a slow speed of 60°/s. Although muscles more often work eccentrically during activities of daily living, such as walking, which is particularly impaired in OA, we did not evaluate eccentric strength because it is less reproducible and there are fewer data in the literature on this subject [10,11].
To avoid an evaluation bias related to this choice of primary endpoint, a statistical cross-tabulation analysis was performed. This analysis measured change in concentric strength if the participant was randomized to the CONC group and in eccentric strength if the participant was randomized to the ECC group. These results also supported the superiority of concentric training at both the short- and medium-term assessments.
As the study was based on an intervention using a medical device, double blinding was not possible: the participant and physiotherapist had to be aware of the type of strengthening performed. However, the evaluator was blinded to group allocation. Participants in both groups were instructed not to discuss their rehabilitation sessions during the evaluations.
The interest of dynamic work in ECC mode in this population should not be excluded in this pathology. Indeed, the occurrence of these injuries is most probably related to the maximal character of the muscle contraction. In the future, it would be interesting to analyze the effectiveness of ECC strengthening protocols that are qualitatively adjustable, and thus avoid this type of maximal contraction.
5. Conclusions
Eccentric muscle strengthening using maximal isokinetic contractions is deleterious in people with knee OA. Muscle strength increased less with eccentric than concentric training and eccentric training was associated with a high risk of muscle injury in this sample, particularly for the hamstring muscles. The occurrence of adverse events in the eccentric training group led to the premature termination of this study. However, dynamic, concentric muscle strengthening is of value in people with knee OA, since it allows significant improvements in strength and function in both the short- and medium-term.
Author Contributions
C Lanhers (CL), B Pereira (BP), JB Lechauve (JBL), L Dobija (LD), S Girold (SG), R Richard (RR), E Coudeyre (EC) conceived the study. Drafting of the original protocol. CL, BP, RR, EC. Coordination of the study.RR, EC. Acquisition of data. CL, EC. Design of the statistical analysis plan. BP, RR, EC. Design of the study and collection JBL, LD, SG, RR, EC. Analysis and interpretation of the data CL, BP, EC. Writing the manuscript CL, BP, EC. All authors read and approved the manuscript.
Funding
this study was funded by the DGOS (Direction Générale de l’Offre de Soins) for the PHCR-I 2011 COUDEYRE (Projet Hospitalier de recherche Clinique Inter-régional). The funders were not involved in the study design or data collection, management, analysis, or interpretation.
Institutional Review Board Statement
This work was supported by the University Hospital of Clermont-Ferrand for logistical aspects drci@chu-clermontferrand.fr.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets analysed during the current study and statistical code are available from the corresponding author on reasonable request, as is the full protocol.
Acknowledgments
Drs M Giustiniani and AG Jégu.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
2017 CONSORT checklist of information to include when reporting a randomized trial assessing nonpharmacologic treatments (NPTs)*. Modifications of the extension appear in italics and blue.

| Section/Topic Item | Checklist item no. | CONSORT item | Extension for NPT trials |
| Title and abstract | |||
| 1a | Identification as a randomized trial in the title | P1 | |
| 1b | Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) | p 2-3 | |
| Introduction | |||
| Background and objectives | 2a | Scientific background and explanation of rationale | p 4 |
| 2b | Specific objectives or hypotheses | p 5 | |
| Methods | |||
| Trial design | 3a | Description of trial design (such as parallel, factorial) including allocation ratio |
p 5 When applicable, how care providers were allocated to each trial group NA |
| 3b | Important changes to methods after trial commencement (such as eligibility criteria), with reasons | NA | |
| Participants | 4a | Eligibility criteria for participants | p 5 |
| 4b | Settings and locations where the data were collected | p 5 | |
| Interventions† | 5 | The interventions for each group with sufficient details to allow replication, including how and when they were actually administered |
Precise details of both the experimental treatment and comparator p 6 + protocol publication doi: 10.1186/1745-6215-15-106. |
| 5a |
Description of the different components of the interventions and, when applicable, description of the procedure for tailoring the interventions to individual participants. p 6 + protocol publication doi: 10.1186/s12906-018-2339-x.. |
||
| 5b |
Details of whether and how the interventions were standardized. p 7 |
||
| 5c. |
Details of whether and how adherence of care providers to the protocol was assessed or enhanced P 7 |
||
| 5d | Details of whether and how adherence of participants to interventions was assessed or enhanced p 7 adherence to physical exercise | ||
| Outcomes | 6a | Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed | p 7 |
| 6b | Any changes to trial outcomes after the trial commenced, with reasons | NA | |
| Sample size | 7a | How sample size was determined |
P 7 -8 When applicable, details of whether and how the clustering by care providers or centers was addressed p7 |
| 7b | When applicable, explanation of any interim analyses and stopping guidelines | P 9 | |
| Randomization: | |||
| - Sequence generation | 8a | Method used to generate the random allocation sequence | P 7 |
| 8b | Type of randomization; details of any restriction (such as blocking and block size) | P7 | |
| - Allocation concealment mechanism | 9 | Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned | P 9 |
| - Implementation | 10 | Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions | P 9 |
| Blinding | 11a | If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how |
P7 If done, who was blinded after assignment to interventions (e.g., participants, care providers, those administering co-interventions, those assessing outcomes) and how |
| 11b | If relevant, description of the similarity of interventions | P7 | |
| 11c | P7 | ||
| Statistical methods | 12a | Statistical methods used to compare groups for primary and secondary outcomes |
P 8 When applicable, details of whether and how the clustering by care providers or centers was addressed P 8 |
| 12b | Methods for additional analyses, such as subgroup analyses and adjusted analyses |
NA |
|
| Results | |||
| Participant flow (a diagram is strongly recommended) | 13a | For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analyzed for the primary outcome |
P 9 The number of care providers or centers performing the intervention in each group and the number of patients treated by each care provider or in each center P 17 and diagram flow |
| 13b | For each group, losses and exclusions after randomization, together with reasons | P 9 and diagram flow | |
| 13c |
For each group, the delay between randomization and the initiation of the intervention NA immediate allocation due to time period |
||
| new | Details of the experimental treatment and comparator as they were implemented NA | ||
| Recruitment | 14a | Dates defining the periods of recruitment and follow-up | P 9 |
| 14b | Why the trial ended or was stopped | P 10 | |
| Baseline data | 15 | A table showing baseline demographic and clinical characteristics for each group |
P 18 When applicable, a description of care providers (case volume, qualification, expertise, etc.) and centers (volume) in each group. NA |
| Numbers analyzed | 16 | For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups | P 9+ flow chat P17 |
| Outcomes and estimation | 17a | For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval) | |
| 17b | For binary outcomes, presentation of both absolute and relative effect sizes is recommended | ||
| Ancillary analyses | 18 | Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre-specified from exploratory | NA |
| Harms | 19 | All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) | P9 |
| Discussion | |||
| Limitations | 20 | Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses |
P 10-11 In addition, take into account the choice of the comparator, lack of or partial blinding, and unequal expertise of care providers or centers in each group NA |
| Generalizability | 21 | Generalizability (external validity, applicability) of the trial findings |
Generalizability (external validity) of the trial findings according to the intervention, comparators, patients, and care providers and centers involved in the trial P 11 |
| Interpretation | 22 | Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence | P 12 |
| Other information | |||
| Registration | 23 | Registration number and name of trial registry | P5 |
| Protocol | 24 | Where the full trial protocol can be accessed, if available | Protocol published doi: 10.1186/1745-6215-15-106... |
| Funding | 25 | Sources of funding and other support (such as supply of drugs), role of funders | P21 |
*Additions or modifications to the 2010 CONSORT checklist. CONSORT = Consolidated Standards of Reporting Trials. †The items 5, 5a, 5b, 5c, 5d are consistent with the Template for Intervention Description and Replication (TIDieR) checklist.
Appendix B

The TIDieR (Template for Intervention Description and Replication) Checklist*:
Information to include when describing an intervention and the location of the information
| Item number | Item | Where located ** | |
| Primary paper (page or appendix number) |
Other † (details) | ||
| BRIEF NAME | |||
| 1. | Provide the name or a phrase that describes the intervention. | Line 93 | ______________ |
| WHY | |||
| 2. | Describe any rationale, theory, or goal of the elements essential to the intervention. | Line 42 | _____________ |
| WHAT | |||
| 3. | Materials: Describe any physical or informational materials used in the intervention, including those provided to participants or used in intervention delivery or in training of intervention providers. Provide information on where the materials can be accessed (e.g. online appendix, URL). | Line 36 |
_____________ |
| 4. | Procedures: Describe each of the procedures, activities, and/or processes used in the intervention, including any enabling or support activities. | Line 96 | _____________ |
| WHO PROVIDED | |||
| 5. | For each category of intervention provider (e.g. psychologist, nursing assistant), describe their expertise, background and any specific training given. | Line 94 | _____________ |
| HOW | |||
| 6. | Describe the modes of delivery (e.g. face-to-face or by some other mechanism, such as internet or telephone) of the intervention and whether it was provided individually or in a group. | Line 94 | _____________ |
| WHERE | |||
| 7. | Describe the type(s) of location(s) where the intervention occurred, including any necessary infrastructure or relevant features. | Line 94 | _____________ |
| WHEN and HOW MUCH | |||
| 8. | Describe the number of times the intervention was delivered and over what period of time including the number of sessions, their schedule, and their duration, intensity or dose. | Line 96 | _____________ |
| TAILORING | |||
| 9. | If the intervention was planned to be personalised, titrated or adapted, then describe what, why, when, and how. | NA | _____________ |
| MODIFICATIONS | |||
| 10.ǂ | If the intervention was modified during the course of the study, describe the changes (what, why, when, and how). | NA | _____________ |
| HOW WELL | |||
| 11. | Planned: If intervention adherence or fidelity was assessed, describe how and by whom, and if any strategies were used to maintain or improve fidelity, describe them. | Line 122 | _____________ |
| 12.ǂ | Actual: If intervention adherence or fidelity was assessed, describe the extent to which the intervention was delivered as planned. | Line 122 | _____________ |
| ** Authors - use N/A if an item is not applicable for the intervention being described. Reviewers – use ‘?’ if information about the element is not reported/not sufficiently reported. † If the information is not provided in the primary paper, give details of where this information is available. This may include locations such as a published protocol or other published papers (provide citation details) or a website (provide the URL). ǂ If completing the TIDieR checklist for a protocol, these items are not relevant to the protocol and cannot be described until the study is complete. * We strongly recommend using this checklist in conjunction with the TIDieR guide (see BMJ 2014;348:g1687) which contains an explanation and elaboration for each item. * The focus of TIDieR is on reporting details of the intervention elements (and where relevant, comparison elements) of a study. Other elements and methodological features of studies are covered by other reporting statements and checklists and have not been duplicated as part of the TIDieR checklist. When a randomised trial is being reported, the TIDieR checklist should be used in conjunction with the CONSORT statement (see www.consort-statement.org) as an extension of Item 5 of the CONSORT 2010 Statement. When a clinical trial protocol is being reported, the TIDieR checklist should be used in conjunction with the SPIRIT statement as an extension of Item 11 of the SPIRIT 2013 Statement (see www.spirit-statement.org). For alternate study designs, TIDieR can be used in conjunction with the appropriate checklist for that study design (see www.equator-network.org). | |||
References
- Le Pen C. et al. Financial cost of osteoarthritis in France. The "COART" France study. Joint Bone Spine 2005 Dec; 72(6):567-70.
- Guillemin F, Rat AC, Mazieres B, et al. Prevalence of symptomatic hip and knee osteoarthritis: a two-phase population-based Survey. Osteoarthritis and Cartilage 2011; Nov;19(11):1314-22. [CrossRef]
- Fautrel B, Hilliquin P, Rozenberg S et al. Impact of osteoarthritis: results of a nationwide survey of 10,000 patients consulting for OA. Joint Bone Spine. 2005 May;72(3):235-40. [CrossRef]
- Bannuru RR, Osani MC, Vaysbrot EE et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019 Nov;27(11):1578-1589. [CrossRef]
- Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019 Apr 27;393(10182):1745-1759. [CrossRef]
- Hurley MV, Newham DJ. The influence of arthrogenous muscle inhibition on quadriceps réhabilitation of patients with early unilatéral osteoarthritic knees. Br J Rheumatol 1993; 32: 127-131.
- Slemenda C, Heilman DK, Brandt KD et al. Reduced quadriceps strength relative to body weight: a risk factor for knee osteoarthritis in women? Arthritis Rheum. 1998 Nov;41(11):1951-9. [CrossRef]
- O'Reilly SC et al. Quadriceps weakness in knee osteoarthritis: the effect on pain and disability. Ann Rheum Dis. 1998 Oct;57(10):588-94. [CrossRef]
- Critères de suivi en rééducation et d'orientation en ambulatoire ou en soins de suite ou de réadaptation après ligamentoplastie du croisé antérieur du genou. Recommandation de bonne pratique. Haute Autorité de Santé. Avril 2008, Paris. (has-sante.fr).
- Huang MH, Lin YS et al. A comparison of various therapeutic exercises on the functional status of patients with knee osteoarthritis. Semin Arthritis Rheum. 2003 Jun;32(6):398-406. [CrossRef]
- Tuzun et al. Effectiveness of two physical therapy programmes in the treatment of knee osteoarthritis. The Pain Clinic 2004; 16(4): 379-387.
- Gür H et al. Concentric versus combined concentric-eccentric isokinetic training: effects on functional capacity and symptoms in patients with osteoarthrosis of the knee. Arch Phys Med Rehabil. 2002 Mar;83(3):308-16. [CrossRef]
- Maurer BT et al. Osteoarthritis of the knee: isokinetic quadriceps exercise versus an educational intervention. Arch Phys Med Rehabil. 1999 Oct;80(10):1293-9. [CrossRef]
- Eyigor S et al. A comparison of muscle training methods in patients with knee osteoarthritis. Clin Rheumatol. 2004 Apr;23(2):109-15. [CrossRef]
- Elliot J. Assessing muscle strength isokinetically. JAMA 1978; 240: 2408-2410.
- Anaes, Service d’évaluation des technologies, service évaluation économique: Les appareils d’isocinétisme en évaluation et en rééducation musculaire. Février 2001. (has-sante.fr).
- Higbie EJ, et al. Effects of concentric and eccentric training on muscle strength, cross-sectional area, and neural activation. J Appl Physiol (1985). 1996 nov;81(5):2173-81. [CrossRef]
- Lastayo PC et al. Chronic eccentric exercise: improvements in muscle strength can occur with little demand for oxygen. Am J Physiol. 1999 Feb;276(2):R611-5. [CrossRef]
- Stanish WD et al. Eccentric exercise in chronic tendinitis. Clin Orthop Relat Res. 1986 Jul;(208):65-8.
- Vallejo AF et al. Cardiopulmonary responses to eccentric and concentric resistance exercise in older adults. Age Ageing. 2006 May;35(3):291-7. [CrossRef]
- Coudeyre E et al. Isokinetic muscle strengthening for knee osteoarthritis: A systematic review of randomized controlled trials with meta-analysis. Ann Phys Rehabil Med. 2016 Jun;59(3):207-215. [CrossRef]
- Jegu AG et al. Effect of eccentric isokinetic strengthening in the rehabilitation of patients with knee osteoarthritis: Isogo, a randomized trial. Trials. 2014 Apr 2;15:106. [CrossRef]
- Rodineau J. Evaluation clinique des lésions musculaires récentes et essai de classification. Sport Med 1997; 73 : 287-90.
- Proske U, Morgan DL. Muscle damage from eccentric exercise: mechanism, mechanical signs, adaptation and clinical applications. J Physiol. 2001 Dec 1;537(Pt 2):333-45. [CrossRef]
- McHugh MP. Recent advances in the understanding of the repeated bout effect: the protective effect against muscle damage from a single bout of eccentric exercise. Scand J Med Sci Sports. 2003 Apr;13(2):88-97. [CrossRef]
- Roig M, O'Brien K, Kirk G, et al. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: a systematic review with meta-analysis. Br J Sports Med. 2009 Aug;43(8):556-68. [CrossRef]
- Lange AK, et al. Strength training for treatment of osteoarthritis of the knee: a systematic review. Arthritis Rheum. 2008 Oct 15;59(10):1488-94. [CrossRef]
- an Baar ME et al. The effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a randomized clinical trial. J Rheumatol. 1998 Dec;25(12):2432-9.
- Rochcongar P. Evaluation isocinétique des extenseurs et fléchisseurs du genou en médecine du sport: revue de la littérature [Isokinetic thigh muscle strength in sports: a review]. Ann Readapt Med Phys. 2004 Aug;47(6):274-81. French. [CrossRef]
Figure 1.
Flow Chart.
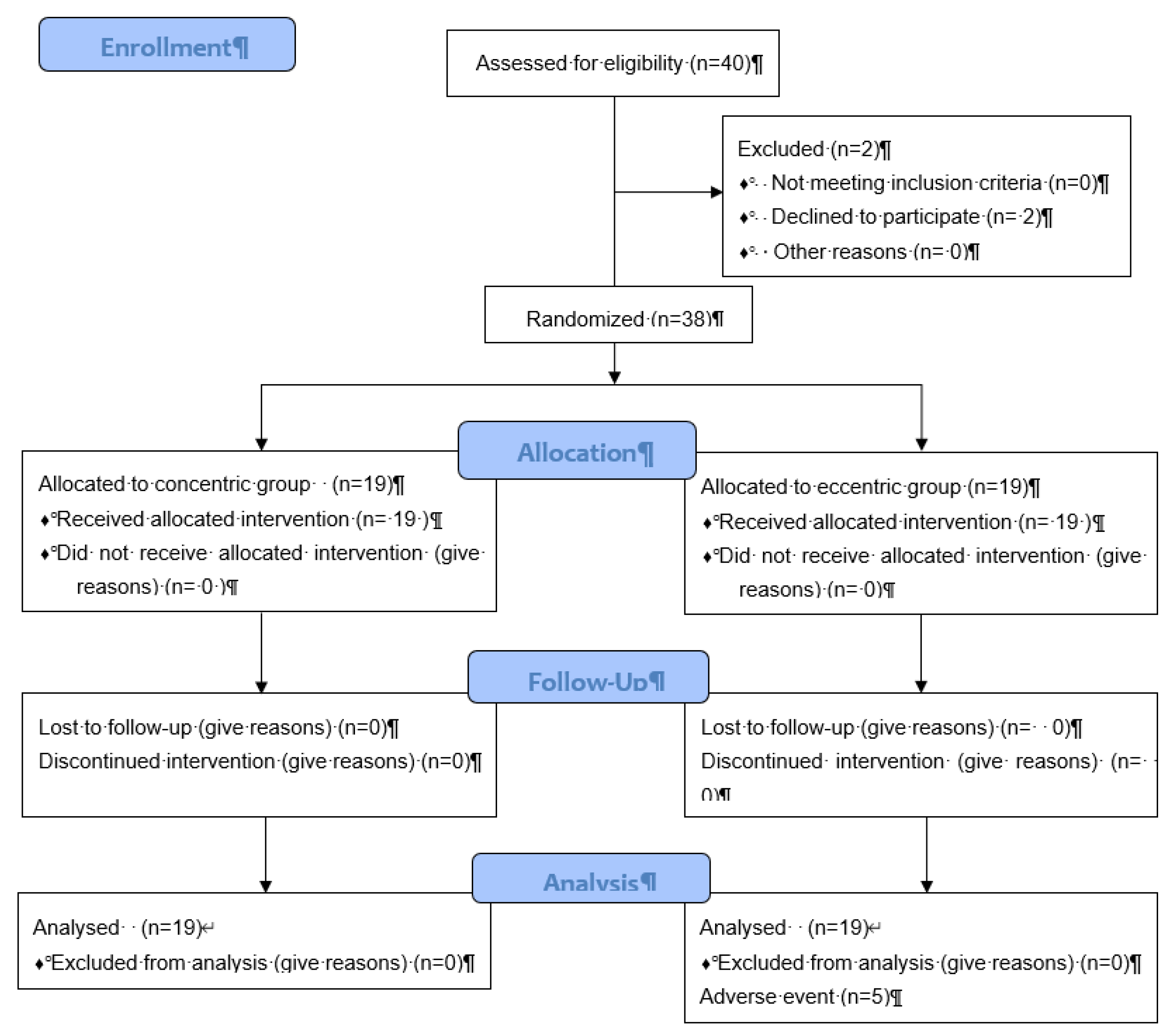
Table 1.
Baseline sample characteristics.
| Concentric Group (n=19) |
Eccentric Group (n=19) |
Total (N=38) |
|
|---|---|---|---|
| Sex (male) | 13 (68.4) | 14 (73.7) | 27 (71.1) |
| Age (years) | 55.9 ± 7.3 | 59.7 ± 7.6 | 57.8 ± 7.6 |
| BMI (kg/m²) | 25.2 ± 3.9 | 26.3 ± 3.9 | 25.8 ± 3.9 |
| Kellgren-Lauwrence score = 1 | 6 (31.6) | 5 (26.3) | 11 (29.0) |
| Kellgren-Lauwrence score = 2+3 | 11 (57.9) | 13 (68.4) | 24 (63.2) |
|
Knee flexion (injured) Knee extension (injured) |
136.6 ± 6.5 -2.5 ± 3.5 |
132.6 ± 7.4 -3.8 ± 4.4 |
134.6 ± 7.1 -3.2 ± 4.0 |
|
Knee flexion (healthy) Knee extension (healthy) |
140.8 ± 7.2 -0.5 ± 1.4 |
139.2 ± 5.2 -0.6 ± 2.3 |
140.0 ± 6.2 -0.6 ± 1.9 |
| VAS pain (OA) (/100) | 25.3 ± 17.1 | 35.5 ± 26.6 | 30.5 ± 22.8 |
| VAS pain (non-OA) (/100) | 12.9 ± 9.6 | 11.7 ± 19.2 | 12.3 ± 15.1 |
| PT OA knee (Nm/kg): | |||
| Quadriceps concentric | 1.29 ± 0.47 | 1.07 ± 0.44 | 1.18 ± 0.46 |
| Harmstring concentric | 0.84 ± 0.32 | 0.76 ± 0.29 | 0.80 ± 0.31 |
| Quadriceps excentric | 2.04 ± 0.66 | 1.81 ± 0.70 | 1.92 ± 0.69 |
| Harmstring excentric | 1.38 ± 0.49 | 1.29 ± 0.61 | 1.33 ± 0.54 |
| PT non-OA knee (Nm/kg): | |||
| Quadriceps concentric | 1.37± 0.44 | 1.22 ± 0.43 | 1.29 ± 0.44 |
| Harmstring concentric | 0.89 ± 0.25 | 0.82 ± 0.28 | 0.85 ± 0.26 |
| Quadriceps excentric | 2.22 ± 0.76 | 2.03 ± 0.77 | 2.12 ± 0.76 |
| Harmstring excentric | 1.29 ± 0.35 | 1.25 ± 0.50 | 1.27 ± 0.42 |
| WOMAC A pain (/20) | 5.2 ± 2.6 | 6.8 ± 3.6 | 6.0 ± 3.2 |
| WOMAC B disability (/68) | 13.7 ± 8.7 | 22.7 ± 13.1 | 18.2 ± 11.9 |
| WOMAC C stiffness (/8) | 2.7 ± 1.5 | 3.8 ± 1.9 | 3.3 ± 1.8 |
| 10m walk speed (m/s) | 1.97 ± 0.19 | 1.90 ± 0.28 | 1.93 ± 0.24 |
| 200m walk speed (s) | 112.9 ± 17.3 | 119.7 ± 15.8 | 116.3 ± 16.7 |
BMI: Body Mass Index; VAS: visual analog scale; PT: peak torque (Nm/Kg); WOMAC. Data are mean ± SD.
Table 2.
Change (%) in quadriceps and harmstring peak torque at 6 weeks and 6 months.
| 6 weeks | 6 months | |||||
|---|---|---|---|---|---|---|
| Concentric group | Eccentric Group |
p-value | Concentric group |
Eccentric Group |
p- value |
|
| Concentric OA knee | ||||||
|
Quadriceps (primary endpoint) |
28 [-17 to 55] | 10 [-100 to 52] | 0.34 | 23 [-99 to 74] | 16 [-100 to 74] | 0.74 |
| Harmstring | 14 [-12 to 44] | -1 [-100 to 24] | 0.21 | -13 [-99 to 36] | -3 [-100 to 29] | 0.96 |
| Ratio Harmstring/Quadriceps | -10 [-26 to 3] | -13 [-100 to 0] | 0.42 | -39 [-99 to -16] | -47 [-100 to -11] | 0.96 |
| Eccentric OA knee | ||||||
| Quadriceps | 0 [-24 to 30] | 0 [-100 to 22] | 0.65 | -12 [-99 to 6] | -1 [-100 to 38] | 0.59 |
| Harmstring | -17 [-45 to 0] | -13 [-100 to 13] | 0.99 | -40 [-99 to 16] | -40 [-100 to 20] | 0.85 |
| Ratio Harmstring/Quadriceps | -8 [-39 to 2] | -20 [-100 to 0] | 0.39 | -35 [-99 to 12] | -32 [-100 to 0] | 0.83 |
| Concentric-eccentric OA knee | ||||||
| Quadriceps | 28 [-17 to 55] | 0 [-100 to 22] | 0.04 | 23 [-99 to 74] | -1 [-100 to 38] | 0.22 |
| Harmstring | 14 [-12 to 44] | -13 [-100 to 13] | 0.04 | -13 [-99 to 36] | -40 [-100 to 20] | 0.42 |
| Ratio Harmstring/Quadriceps | -10 [-26 to 3] | -20 [-100 to 0] | 0.24 | -39 [-99 to -16] | -32 [-100 to 0] | 0.94 |
Data are expressed as median [IQR].
Table 3.
Change (%) in range of motion and disability at 6 weeks and 6 months.
| 6 weeks | 6 months | ||||||
|---|---|---|---|---|---|---|---|
| Concentric group |
Eccentric group |
p- value |
Concentric group | Eccentric group |
p-value | ||
| Flexion OA knee (°) | 0 [-4 to 0.7] | 0 [-100 to 2] | 0.79 | 0 [-4 to 1] | 0 [-100 to 2] | 0.54 | |
| Extension OA knee (°) | 0 [-71 to 0] | -42 [-100 to -13] | 0.34 | -21 [-85 to 0] | -75 [-100 to -33] | 0.28 | |
| VAS OA knee (/100) | -17 [-75 to 0] | -41 [-100 to -17] | 0.31 | -40 [-100 to 0] | -76 [-100 to -33] | 0.44 | |
| WOMAC A pain (/20) | -10 [-50 to 0] | -29 [-100 to 0] | 0.30 | -12 [-50 to 0] | -29 [-100 to 0] | 0.43 | |
| WOMAC B disability (/68) | -8 [-29 to 6] | -38 [-100 to 0] | 0.12 | 0 [-22 to 25] | -20 [-100 to 0] | 0.11 | |
| WOMAC C stiffness (/8) | -20 [-33 to 0] | -25 [-100 to 0] | 0.35 | -50 [-75 to 0] | -20 [-100 to 0] | 0.87 | |
| 10 m walk speed (m/s) | 0 [-7 to 5] | -2 [-100 to 4] | 0.32 | 0 [-16 to 3] | -6 [-100 to 2] | 0.54 | |
| 200m walk speed (s) | -3 [-8 to 0] | -5 [-100 to -1] | 0.56 | -6 [-13 to -1] | 0 [-100 to 7] | 0.15 | |
Data are expressed as median [IQR].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



