
Submitted:
14 May 2024
Posted:
15 May 2024
You are already at the latest version
Abstract
Objective: This study aimed to explore potential interventions or preventive measures to reduce the incidence of falls among the elderly in the Madinah region, and to provide recommendations for healthcare professionals, policymakers, and community stakeholders to enhance fall prevention strategies and improve the overall well-being of the elderly population in this area.
Methods: The study adopted a cross-sectional study design, and was carried out in the Madinah region using convenient physical assignment among of Saudi and non-Saudi local residents aged 65 years and over. Questionnaire surveys were circulated and demographic characteristics were collected, including participants’ fall experience and health status data over the past year, in order to assess the incidence of falls among the elderly population. This design allows for the collection of data at a single point in time, aiming to evaluate the prevalence, risk factors, and consequences of falls among the target population.
Results: A total of 189 participants were recruited to the study, and the data indicated that the prevalence of falls among those aged 65 years and older in the past year was 41.5%. We found that 73% of the participants had experienced falls and post-fall injuries within the past 12 months. There were minimal differences in terms of physical handicapped cases found between those with and without a fall history. Logistic regression analysis revealed a significant link between fall experience and maximum bite force.
Conclusion: There is a high prevalence of falls in the elderly population in the Madinah region. Our study reveals that 50.79% of our elderly participants had experienced more than one fall during the preceding year. Some preventable risk factors were identified in an analysis of their daily routines. The impacts of these risk factors have potential consequences for their healthy lives.
Keywords:
elderly
; prevalence
; public health
; risk factors
; consequent injuries
; fall
Introduction
Falls among the elderly constitute a significant public health issue globally, leading to adverse outcomes such as injuries, hospitalizations, and reduced quality of life. In the Madinah region in Saudi Arabia, where there is a growing elderly population (projected to reach up to 21.8%, i.e., 10 million, by 2050 [1]), falls represent a pressing concern with implications for individual well-being and healthcare resources. Understanding the epidemiology of falls, along with associated risk factors and consequences, is crucial for developing effective prevention and intervention strategies tailored to this population. [2]
Madinah is not as densely populated as other major cities in Saudi Arabia, but it does experience periodic increases in population due to religious pilgrimages. During these times the city can become crowded with pilgrims and tourists, putting infrastructure and services under significant strain. The roads inside the city are well developed and maintained, but due to renovation some places uphill and downhill due to mountain terrains.
The elderly population in Madinah faces unique challenges related to falls, including cultural, environmental, and healthcare system factors. As such, there is a need for comprehensive research to assess the prevalence, risk factors, and consequences of falls among the elderly in this region. By gaining insights into these factors, healthcare professionals, policymakers, and community stakeholders can implement targeted interventions to reduce the burden of falls and improve the overall health outcomes of the region’s elderly population. [3,4,5]
This study aims to address this gap in knowledge by conducting a thorough investigation into falls among the elderly in the Madinah region. Using a cross-sectional study design we will assess the prevalence of falls, examine associated risk factors including demographic, clinical, and environmental variables, and explore the consequences of falls on healthcare utilization and quality of life. Additionally, potential interventions and preventive measures are explored to inform evidence-based strategies for fall prevention tailored to the Madinah context. Ultimately, the findings of this study have the potential to contribute to enhanced public health efforts and better outcomes for elderly individuals in the Madinah region and beyond.
As populations age worldwide, [6] the prevalence of falls among the elderly has become a major public health concern. Falls are a leading cause of injury-related morbidity and mortality among older adults, often resulting in fractures, hospitalizations, and decreased functional independence. In regions with a growing elderly population, such as the Madinah region, understanding the epidemiology of falls and implementing effective prevention strategies is crucial to promote healthy aging and reduce the healthcare burden. Falls among the elderly can result from various risk factors, which may interact and compound each other. These risk factors can include muscle weakness and balance problems, gait and mobility issues, chronic health conditions, medications, vision impairment, environmental hazards, foot problems and improper footwear, cognitive impairment, fear of falling, dehydration and malnutrition, alcohol use, age-related changes, social isolation, and lack of physical activity. [7,8] Identifying and addressing these risk factors through comprehensive fall prevention strategies, including exercise programs, environment modification, medication management, and education, may help to reduce the incidence of falls among the elderly.
Some risk factors that may be associated with an increased risk of falls among elderly participants include demographic factors, health conditions, medication use, environmental hazards, and lifestyle factors. Highlighting the consequences and impact of falls on participants’ health, quality of life, and healthcare utilization will include an analysis of injuries sustained, hospitalizations, functional ability, or psychological impacts. This study also aims to identify any factors or interventions that may be protective against falls, or may be effective in reducing fall risk among the participants. These could include exercise programs, home modifications, medication management, or vision assessments.
The Madinah region, located in the western part of Saudi Arabia, is home to a significant proportion of elderly individuals, with demographic trends indicating a steady increase in the aging population. Factors such as changing lifestyles, urbanization, and advances in healthcare have contributed to longer life expectancy, but have also brought new challenges in managing the health and well-being of the elderly population.
Despite a growing awareness of falls as a critical issue in elderly health, there is a lack of comprehensive research focusing on falls among the elderly specifically in the Madinah region. Existing studies often generalize findings from other regions or countries, overlooking the unique cultural, environmental, and healthcare system factors that may influence the occurrence and consequences of falls in this particular context. [10]
This study seeks to address this gap by conducting a thorough investigation into falls among the elderly in the Madinah region. Using a cross-sectional study design we aim to assess the prevalence of falls and identify associated risk factors, including demographic characteristics, medical history, medication use, and environmental factors. Additionally, we will explore the consequences of falls on healthcare utilization, functional status, and quality of life among elderly individuals in this region. Ultimately, this research has the potential to contribute to the advancement of public health efforts and promote healthy aging in the Madinah region and beyond.
Materials and Methods
A cross-sectional study design is employed to assess the prevalence of falls, along with associated risk factors such as age, gender, comorbidities, medication use, and environmental factors. Additionally, the study will examine the consequences of falls, including injuries sustained, healthcare utilization, and quality of life impact.
Study Design: A cross-sectional study design employed to assess falls among the elderly population (aged 65 years and over) in the Madinah region. This design allows for the collection of data at a single point in time, enabling us to evaluate the prevalence, risk factors, and consequences of falls among the target population.
Study Setting: The study used a data collection form developed for use as a questionnaire in various settings within the Madinah region’s public and private hospitals, including healthcare facilities, community centers, and residential areas where elderly individuals reside.
Participants and Sample Size: The study participants included elderly individuals aged 65 years and above residing in the Madinah region. 189 participants were recruited through convenience sampling from healthcare facilities, community centers, and residential areas.
Data Collection: Data was collected using structured interview questionnaires, taking approximately 10 to 20 minutes depending on the participants’ responses. The structured interview questionnaires were conducted by trained research staff, and gathered information on demographic characteristics, medical history, medication use, mobility status, and fall history. Medical records were reviewed to obtain additional clinical data, including diagnoses, treatments, and healthcare utilization related to falls. Environmental assessments were conducted to identify potential hazards in the living environment that may contribute to falls.
Measures: The primary outcome measure was the prevalence of falls among the elderly population in the Madinah region. Falls were defined as unintentionally coming to rest on the ground, floor, or other lower level. Secondary outcome measures included risk factors associated with falls (e.g., age, gender, comorbidities, medication use, environmental hazards) and consequences of falls (e.g., injuries, hospitalizations, healthcare utilization).
Data Analysis: Descriptive statistics were used to summarize the demographic characteristics of the study population and the prevalence of falls. Bivariate and multivariate analyses were conducted to identify the risk factors associated with falls, and logistic regression analysis was used to determine the odds ratios and 95% confidence intervals for each risk factor. Subgroup analyses were conducted based on age, gender, and other relevant factors. All analyses were performed using the statistical software IBM SPSS 26, and p-values less than 0.05 were considered statistically significant.
Results
Our research team interviewed 189 participants over the period of August 2023 to December 2023. Table 1 shows demographic data about the participants. All the participants were aged 65 or over with an overall mean age of 67.91± 9.06 years; for the male participants the mean was 68.72 ± 9.45 years, while for the females the mean was 66.64± 8.34 years. Males accounted for 54.49% of the participant group, while females accounted for 45.51%; there were slightly more male participants than females.
51.85% of the participants were married and living with their family, 35.45% were either single or widowed, and 12.70% were divorcees. In terms of their financial status, 34.39% were self-employed and 17.46% were government pensioners. 40.21% of the participants reported that they required care or support at home for their daily life needs, while almost 60% reported that they did not have any care needs in daily life. Only 17.46% reported that they were not using any medication, with most of the participants (47.62%) stating that they were using more than four different types of medication daily to help manage chronic diseases. In terms of their smoking habits, 11.11% of the participants were smokers. Walking aids were not used by most of the participants (60.32%), with the rest of the participants using either a walking stick or a wheelchair for daily mobility support.
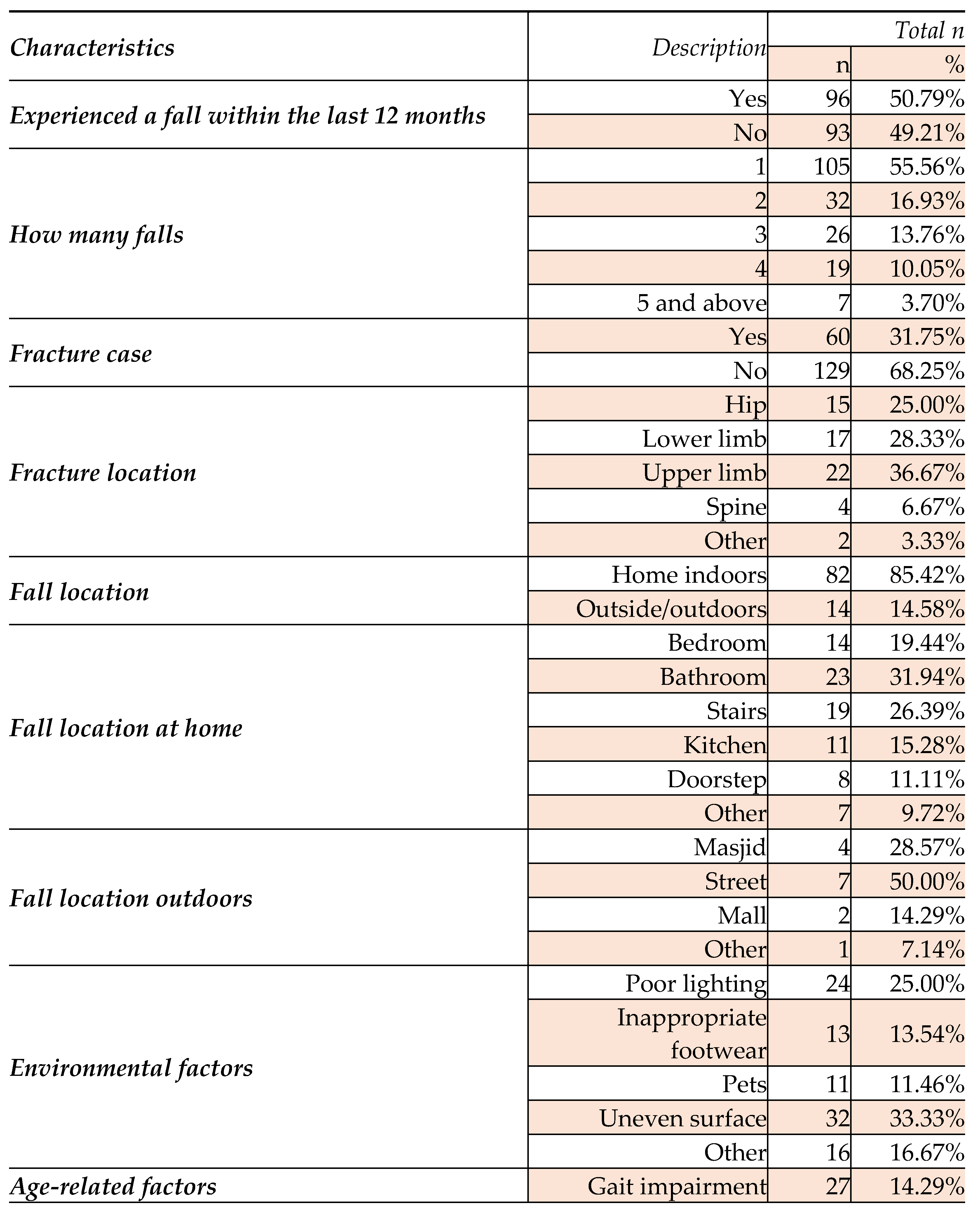
Table 2 shows that 50.79% of the participants had experienced one or more falls during the past year. The percentages of female participants who had fallen either at home or in other places were both higher than for males. Most of the participants had fallen once (55.56%), with 16.93% falling twice, 13.76 % falling three times, 10.05% falling four times and 3.70% experiencing five or more falls.
The table shows that 31.75% of the participants who had fallen had sustained injuries. Upper limb fractures were the most common, reported by 36.67% of those who had sustained an injury as a result of a fall, followed by lower limb and hip fractures (reported by 28.33% and 25.00% respectively).
Most of the participants reported that they recovered with three to six months, but 45% were not able to return their normal life immediately after falling, needing a walking aid, and severe injury was recorded by 3.3% of the participants. Most of the participants were not involved in any physical activities, with only few of them taking part in walking or games.
Regarding the location of the participants’ falls, we classed indoor locations as Home and other locations as Outside the home, i.e. either in the street or at the masjid or mall. Our results indicate that indoor fall cases formed the majority at 85.42%, with only 14.58% of falls occurring in outdoor or public places such as streets, at the masjid or in malls. Most of the falls at home happened in the bathroom (31.94%) or on the stairs (26.39%), with the rest happening in places like kitchens, doorsteps and bedrooms. Many falls occurred in the evening during times of poor lighting periods, and participants mostly fell face down to the ground comparatively back and sides.
There were no significant differences related to age, financial status, smoking, physical activity and marital status in terms of experiencing a fall. Participants who were living in rented places experiencing fall among the participants rather than staying at their own home (OR 1.2). Similarly, those who reported needing help from a caretaker reported significantly more falls than those who did not have a caretaker. Not using any medication was significantly associated with fewer falls (OR 0.52). Moreover, participants who said they used some kind of walking support reported more falls compared with those who did not, and those who used walking frames had a significantly higher risk of falls compared with other users. The stress is also one of the main cause to frequently fall among elderly.
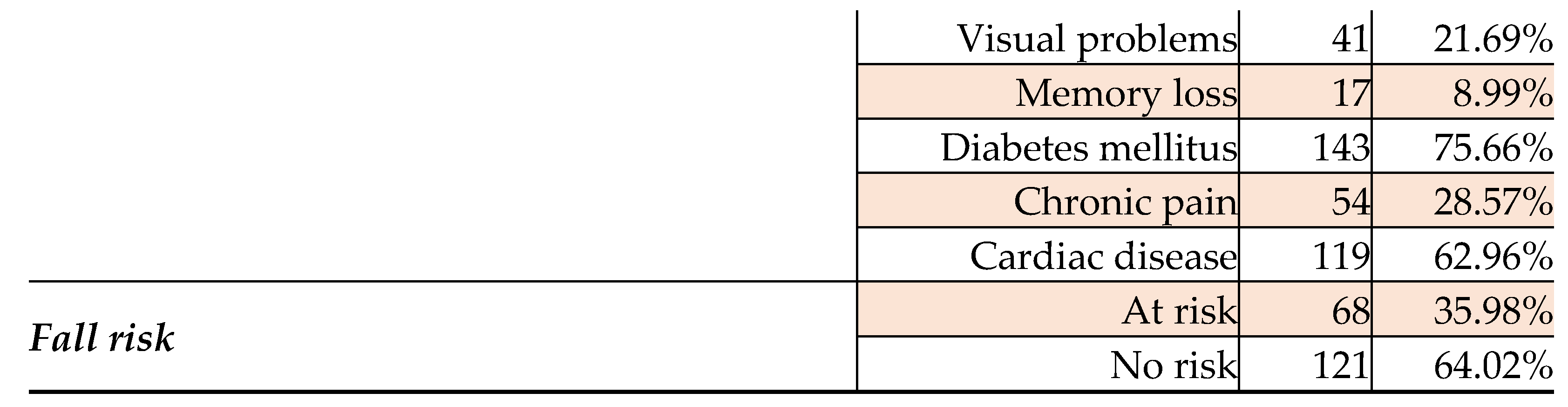
In our study, most of the participants reported one or more comorbidities; heart disease and diabetes mellitus were the most common, at 62.96% and 75.66% respectively. However, other conditions such as hypertension, visual problems, gait impairments, memory loss and chronic pain were also reported, although at lower levels.
Discussion
An increasing prevalence of falls among the elderly is reported worldwide, and has been attributed to various factors. Previous studies have reported wide and diverse risk factors, [10,11] and it was therefore important for us to understand the reasons for falls among elderly people living in the Madinah region in the Kingdom of Saudi Arabia. Our wider program of research addresses and investigates risk factors, morbidity, mortality, hospitalization, and reduced mobility among the elderly. The main aim of this study was to investigate the prevalence of falls, and to identify the risk factors associated with injuries sustained in falls.
Falls among the elderly are a significant global health concern. They can lead to serious injuries, loss of independence, and even death. Many factors contribute to falls in older adults, including age-related changes in vision, balance, and strength, as well as environmental hazards. Prevention strategies often involve exercise programs, home modifications, medication management, and regular vision check-ups. Governments and healthcare systems worldwide are increasingly recognizing the importance of fall prevention initiatives to support a healthy aging population.
Our study reveals that 50.79% of the elderly participants had experienced at least one fall during the previous year, bringing our data within the range of 25% to 50% reported across various studies. A previous study conducted by Alshammari et al. [9] in Riyadh also recorded that most falls occur at home (72.8%), with the most frequent location being the bathroom. [17] The prevalence of falls in the Madinah region was higher than that reported in other countries such as England (28% [11]), Canada (34% [12]), Ecuador (37.4% [13]) and the United States of America (22% [14]). In the Middle East, Egypt recorded a high prevalence of falls among elderly (60.3% [15]), and Qatar recorded 34%. [16]
The mean age of the participants in our study of 67.91 years confirms that we primarily focused on older adults, although there was a relatively wide age range. The slightly higher proportion of male participants may reflect differences in healthcare-seeking behaviors or gender-related risk factors for falls. The fact that the majority of participants were married and living with their families may indicate potential sources of social support and caregiving. However, the significant percentages of single, widowed, or divorced participants also highlights the importance of considering social isolation and support networks in fall prevention efforts.
The majority of falls occurred indoors, with 85.42% happening at home, specifically in locations such as the bedroom, bathroom, stairs, kitchen, and doorstep. A smaller proportion of falls (14.58%) occurred outdoors, in locations including streets, mosques (masjids), and malls. This is similar to the results reported by Almawlawi et al. [15] and Yeong et al., [16] although these studies mentioned that most fall cases occurred on stairs rather than in the bathroom.
Poor lighting, inappropriate footwear, pets, and uneven surfaces were identified as common environmental factors contributing to falls. Similar studies have also reported that falls increase with advancing age, and our study recorded the same. However, gender was not found to be associated with falls in our study. In comparison with other studies, musculoskeletal pain and trips were associated with falls among the elderly in Japan, [19] falls were more common among elderly men than women in Germany, [20] and a Nigerian study [21] found that woman were more likely to fall than men. It is worth noting that the results of some of these studies may be related to unmeasured social, biological, or environmental characteristics.
As noted in Kumar et al.’s [22] study, economic factors must be considered when designing interventions to address fall risk. The reliance on caretakers to meet their daily needs among a significant portion of the participants in our study underscores the presence of functional limitations and healthcare needs. However, our study results also found a high prevalence of medication use for chronic diseases, highlighting the importance of medication management and monitoring any adverse effects related to falls. Various age-related factors, including gait impairment, visual problems, memory loss, diabetes mellitus (DM), chronic pain, and cardiac diseases were reported among the participants. The prevalence of smoking among the participants was also noteworthy, since smoking is associated with various health conditions that may increase fall risk. Additionally, the limited use of walking aids suggests differences in mobility needs and functional abilities among our participants. [24]
A Malaysian study [22,23] suggests that fewer married elderly people (4.9%) experienced injuries after falls at home than widowed or divorced people (8%) or those who were single (8%). That study also found that financial status had no impact on the prevalence of falls among elderly people. A significant proportion of the participants (40.21%) reported needing a caretaker for assistance with daily activities, and the majority of participants did not use any walking support (60.32%), while others used walking sticks, walkers, or wheelchairs; all of these are associated with a greater fall risk in our study, although most studies suggest that walking support protects against falls. Nearly half of our participants (47.62%) reported taking more than four tablets per day, indicating a high prevalence of multiple medication use. Few stress factors were reported in our literature study, but a Korean study [25] suggested that there was a higher fall risk among stressed elderly participants than among those who were not stressed. A small proportion of the participants reported a smoking habit (11.11%).
Overall, our findings provide valuable insights into the prevalence, frequency, consequences, and contributing factors of falls among the study participants. Understanding these factors is essential for developing targeted fall prevention interventions, and for improving the safety and well-being of older adults. These findings also provide valuable insights into the demographic characteristics and health-related behaviors of the study participants, an understanding of which is essential in tailoring interventions to address fall risk and improve the overall well-being of older adults in the Madinah region.
In terms of interventions to decrease fall risk, we note that dimly lit areas can obscure obstacles and increase the risk of trips and falls, especially at night. Those at risk should install brighter light fixtures, add nightlights in hallways and bathrooms, and ensure proper illumination on stairs and in outdoor areas. Wet or polished floors, especially in bathrooms and kitchens, can cause slips and falls, so the use of non-slip mats or rugs is recommended in high-risk areas, along with install grab bars near showers and toilets, and promptly cleaning up spills. Those at risk could also consider using a shower chair or bench for stability.
Uneven or loose floorboards, carpets, or tiles can create tripping hazards; damaged flooring should be replaced, loose rugs should be secured with non-slip pads, and clutter should be removed from walkways. The absence of handrails on stairs or in corridors can lead to loss of balance and falls; we recommend the installation of sturdy handrails on both sides of staircases and along hallways, ensuring they are securely anchored to the wall. Furniture with sharp edges or unstable legs can cause injuries. Furniture should have rounded edges, unstable pieces should be secured, and furniture should be rearranged to create clear pathways. Secure loose cords and wires, and organize belongings to minimize trip hazards. Uneven sidewalks, loose paving stones, and inadequate lighting in outdoor areas can also all pose fall risks.
Elderly people should be encouraged to engage in regular physical activity to improve strength, balance, and flexibility; activities like walking, tai chi, and gentle stretching can be beneficial. Families and caregivers should maintain regular communication with their elderly family members to stay informed about their well-being and any changes in their health or mobility. Emotional support and companionship should be offered to reduce feelings of loneliness and isolation; family members of older adults play a crucial role in supporting their well-being and reducing fall risk.
Conclusion
Mitigating the risk of falls among elderly people should include investigating specific risk factors in more detail, exploring novel interventions, and conducting longitudinal studies to examine long-term outcomes. We emphasize the importance of addressing fall risk factors to improve the health and well-being of older adults, and recommend that future research should explore the relationship between demographic factors and fall risk in more depth, as well as evaluating the effectiveness of targeted interventions for specific subgroups within the wider elderly population.
Offering a demographic profile of our participants provides valuable context for understanding fall risk and designing targeted interventions to prevent falls among older adults. By considering the diverse needs and characteristics of the study population, researchers and healthcare providers can develop comprehensive fall prevention strategies that address the unique challenges faced by older adults.
Funding
No funding was received for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- UNFPA and HelpAge. Ageing in the twenty-first century: A celebration and a challenge. 2012. https://www.unfpa.org/public/home/publications/pid/11584.
- World Health Organization. WHO global report on fall prevention in older age. [Accessed: Jul 2020]. From: www.who.int/ageing/publications/Falls_prevention7March.pdf.
- Oliver D. Development of services for older patients with falls and fractures in England: Successes, failures, lessons and controversies. Arch Gerontol Geriatr. 2009;49:S7–12. [CrossRef]
- Sekaran NK, Choi H, Hayward RA, Langa KM. Fall-associated difficulty with activities of daily living in functionally independent individuals aged 65 to 69 in the United States: A cohort study. J Am Geriatr Soc. 2013;61:96–100. [CrossRef]
- Stel VS, Smit JH, Pluijm SM, Lips P. Consequences of falling in older men and women and risk factors for health service use and functional decline. Age Ageing. 2004;33:58–65. [CrossRef]
- Orces CH. Prevalence and determinants of falls among older adults in Ecuador: An analysis of the SABE I Survey. Curr Gerontol Geriatr Res. 2013;2013. 495468. [CrossRef]
- Janakiraman B, Temesgen MH, Jember G, Gelaw AY, Gebremeskel BF, Ravichandran H, et al. Falls among community-dwelling older adults in Ethiopia: A preliminary cross-sectional study. PLoS One. 2019;14:e0221875. [CrossRef]
- Gale CR, Cooper C, Sayer AA. Prevalence and risk factors for falls in older men and women: The English Longitudinal Study of Ageing. Age Ageing. 2016;45:789–94. [CrossRef]
- Alshammari SA, Alhassan AM, Aldawsari MA, Bazuhair FO, Alotaibi FK, Aldakhil AA, et al. Falls among elderly and its relation with their health problems and surrounding environmental factors in Riyadh. J Fam Community Med. 2018;25:29–34. [CrossRef]
- Gale CR, Cooper C, Aihie Sayer A. Prevalence and risk factors for falls in older men and women: The English Longitudinal Study of Ageing. Age Ageing 2016;45:789–94. [CrossRef]
- Do MT, Chang VC, Kuran N, et al. Fall-related injuries among Canadian seniors, 2005–2013: An analysis of the Canadian Community Health Survey. Health Promot Chronic Dis Prev Can 2015;35:99–108.
- Stevens JA, Ballesteros MF, Mack KA, et al. Gender differences in seeking care for falls in the aged Medicare population. Am J Prev Med 2012;43:59–62. [CrossRef]
- Fang X, Shi J, Song X, et al. Frailty in relation to the risk of falls, fractures, and mortality in older Chinese adults: Results from the Beijing Longitudinal Study of Aging. J Nutr Health Aging 2012;16:903–7. [CrossRef]
- Almawlawi E, Alansari A, Ahmed A. Prevalence and risk factors for falls among the elderly in primary healthcare centers (PHC) in Qatar. Qatar Med J 2011;20:1. [CrossRef]
- Kamel MH, Abdulmajeed AA, Ismail S-S. Risk factors of falls among elderly living in urban Suez, Egypt. Pan Afr Med J 2013;14:26. [CrossRef]
- Mancini C, Williamson D, Binkin N, et al. Epidemiology of falls among the elderly. Ig Sanita Pubbl 2005;61:117–32.
- Yeong UY, Tan SY, Yap JF, et al. Prevalence of falls among community-dwelling elderly and its associated factors: A crosssectional study in Perak, Malaysia. Malays Fam Physician 2016;11:7–14.
- Kitayuguchi J, Kamada M, Okada S, et al. Association between musculoskeletal pain and trips or falls in rural Japanese community-dwelling older adults: A cross-sectional study. Geriatr Gerontol Int 2015;15:54–64. [CrossRef]
- Rapp K, Freiberger E, Todd C, et al. Fall incidence in Germany: Results of two population-based studies, and comparison of retrospective and prospective falls data collection methods. BMC Geriatr 2014;14:105. [CrossRef]
- Bekibele CO, Gureje O. Fall incidence in a population of elderly persons in Nigeria. Gerontology 2010;56:278–83. [CrossRef]
- Kumar A, Carpenter H, Morris R, et al. Which factors are associated with fear of falling in community-dwelling older people? Age Ageing 2014;43:76–84.
- Graafmans WC, Lips P, Wijlhuizen GJ, et al. Daily physical activity and the use of a walking aid in relation to falls in elderly people in a residential care setting. Z Gerontol Geriatr 2003;36:23–8. [CrossRef]
- van Doorn C, Gruber-Baldini AL, Zimmerman S, et al. Dementia as a risk factor for falls and fall injuries among nursing home residents. J Am Geriatr Soc 2003;51:1213–8. [CrossRef]
- Dhargave P, Sendhilkumar R. Prevalence of risk factors for falls among elderly people living in long-term care homes. Journal of Clinical Gerontology and Geriatrics 2016;7:99–103. [CrossRef]
- Choi EJ, Kim SA, Kim NR, et al. Risk factors for falls in older Korean adults: The 2011 Community Health Survey. J Korean Med Sci 2014;29:1482–7. [CrossRef]

Table 1.
Participants’ demographic characteristics, with numbers of respondents and risk factors associated with falls among the elderly.
Table 1.
Participants’ demographic characteristics, with numbers of respondents and risk factors associated with falls among the elderly.
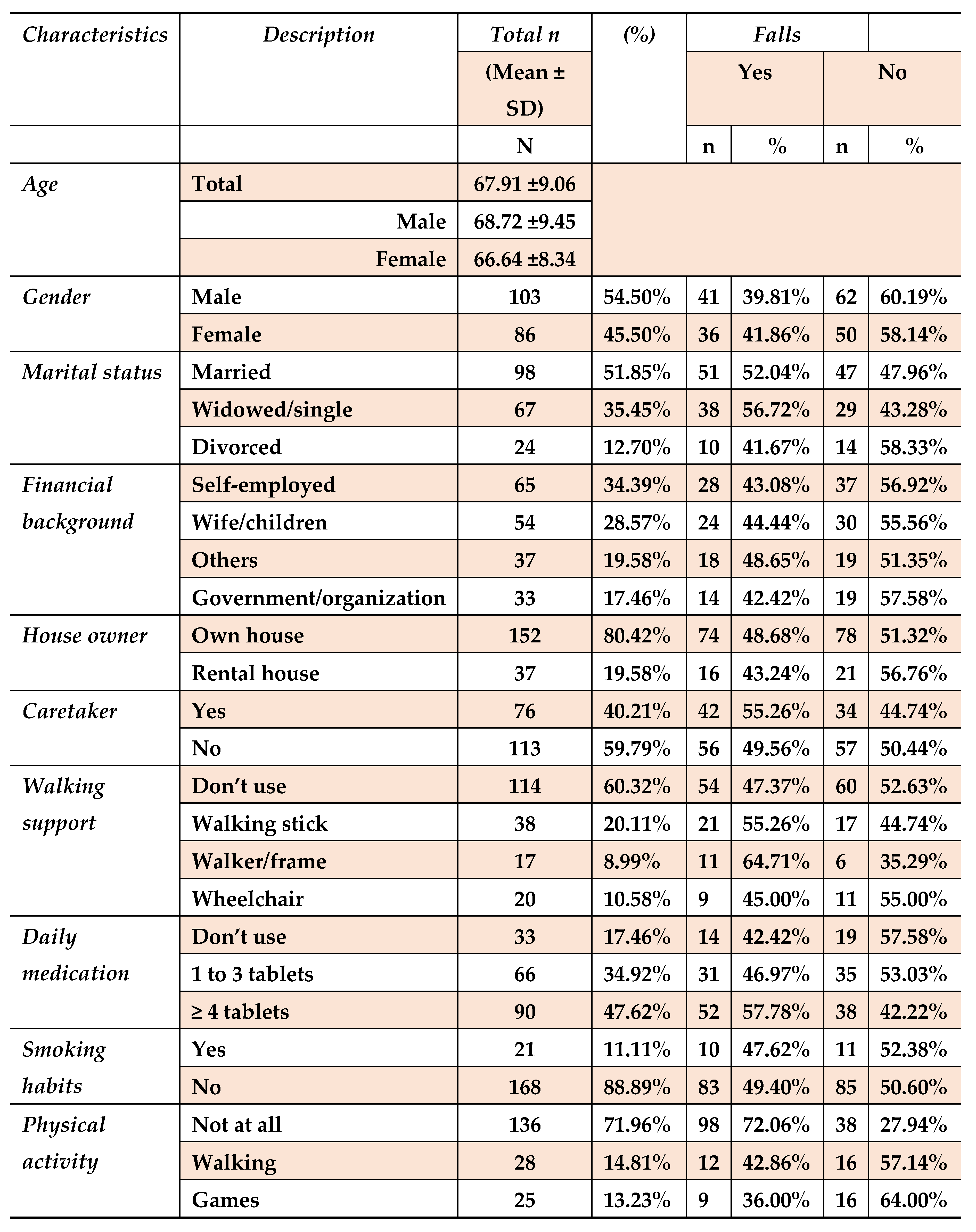
Table 2.
Fall prevalence, location, and risk factors reported by elderly participants.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



