
Submitted:
14 May 2024
Posted:
16 May 2024
You are already at the latest version
Abstract
Microbicides, topical antiseptic agents, and a revolutionary advance in HIV prevention aim to prevent the entry of infectious agents into the human body, thus stopping the sexual transmission of HIV and other sexually transmitted diseases. Microbicides represent the promise of a new age in preventive measures against one of the world's most pressing health challenges. In addition to their direct antiviral effects during HIV transmission, microbicides also influence vaginal mucosal immunity. This article reviews microbicides by presenting different drug classifications and highlighting significant representatives from each group. It also explains their mechanisms of action and presents information about vaginal mucosal immune responses, emphasizing the critical role they play in responding to HIV during sexual transmission. For each chemical compound, the article provides a brief overview of relevant preclinical and clinical research, emphasizing their potential as microbicides.The article offers insights into the multifaceted impact of microbicides, which signify a pivotal step forward in the pursuit of effective and accessible pre-exposure prophylaxis (PrEP).
Keywords:
HIV
; AIDS
; mucosal immunity
; microbicides
; pre-exposure prophylaxis
1. Introduction
Based on the latest data of 2022, the number of people currently suffering from the human immunodeficiency virus (HIV) has reached the mark of 39 million worldwide. Despite the measures taken to prevent the spread of HIV, more than million people are being annually infected. Ever since acquired immunodeficiency syndrome (AIDS) was first clinically observed, it remains one of the main problems which humanity has faced. In 2022, approximately 630,000 people died from AIDS-related illnesses. Moreover, mortality rates are remarkably higher for young adults in developing countries reaching the highest numbers in sub-Saharan Africa [1,2].
Currently, 86% out of all HIV infected people know their HIV status and only 89% of them receive treatment. Considering the bleak statistics, detaining the spread of HIV and increasing the life expectancy should be the main intention. This, in turn, can be obtained through raising public awareness of HIV prevention methods, increasing the effectiveness and universal availability of both HIV diagnostics and active antiretroviral therapy [1,2,3,4,5].
Some studies indicate that the prophylaxis of HIV infection generated substantial economic benefits compared to those of therapy. Preventive measures can be implemented on different levels, including condom usage, voluntary medical male circumcision (VMMC) and pre-exposure prophylaxis (PrEP). Additionally, microbicides can be considered potential drugs used to combat the spread of HIV infection [6,7,8,9].
This review involves the description of some microbicides’ action mechanisms, which can help us understand their evidence base, entering a new era of HIV prophylaxis.
2. Materials and Methods
In this review, we collected information about mucosal immunity and microbicides from different groups. The aim was to describe the current state of microbicide research, highlight new drugs for PrEP (pre-exposure prophylaxis), and show where they are in clinical development and how effective their use is. We used a nonsystematic approach to search for information over a long period of time, starting with the earliest groups of microbicides and progressing to new prospective drugs that are undergoing preclinical and clinical trials. To do this, we used databases such as PubMed, Google Scholar, RePORTER and registers such as ClinicalTrials. We searched by keywords such as “HIV”, “microbicide”, “prophylaxis” and by product name. We selected randomized controlled trials and projects for this review using different combinations of these keywords. Inclusion criteria included up-to-date clinical and randomized controlled trials on different groups of microbicides used for topical immunoprophylaxis. We excluded review articles based on clinical trials, the ones that contained off topic data.
We outlined the main findings from the articles regarding the effectiveness of existing and newly developed microbicides for the most vulnerable populations. We categorized microbicides according to their mechanisms of action and the stage of development they currently exist at. The efficacy of each microbicide was compared with each other, as well as a placebo. Based on this information, we can identify the most promising areas for developing new microbicides and their potential uses.
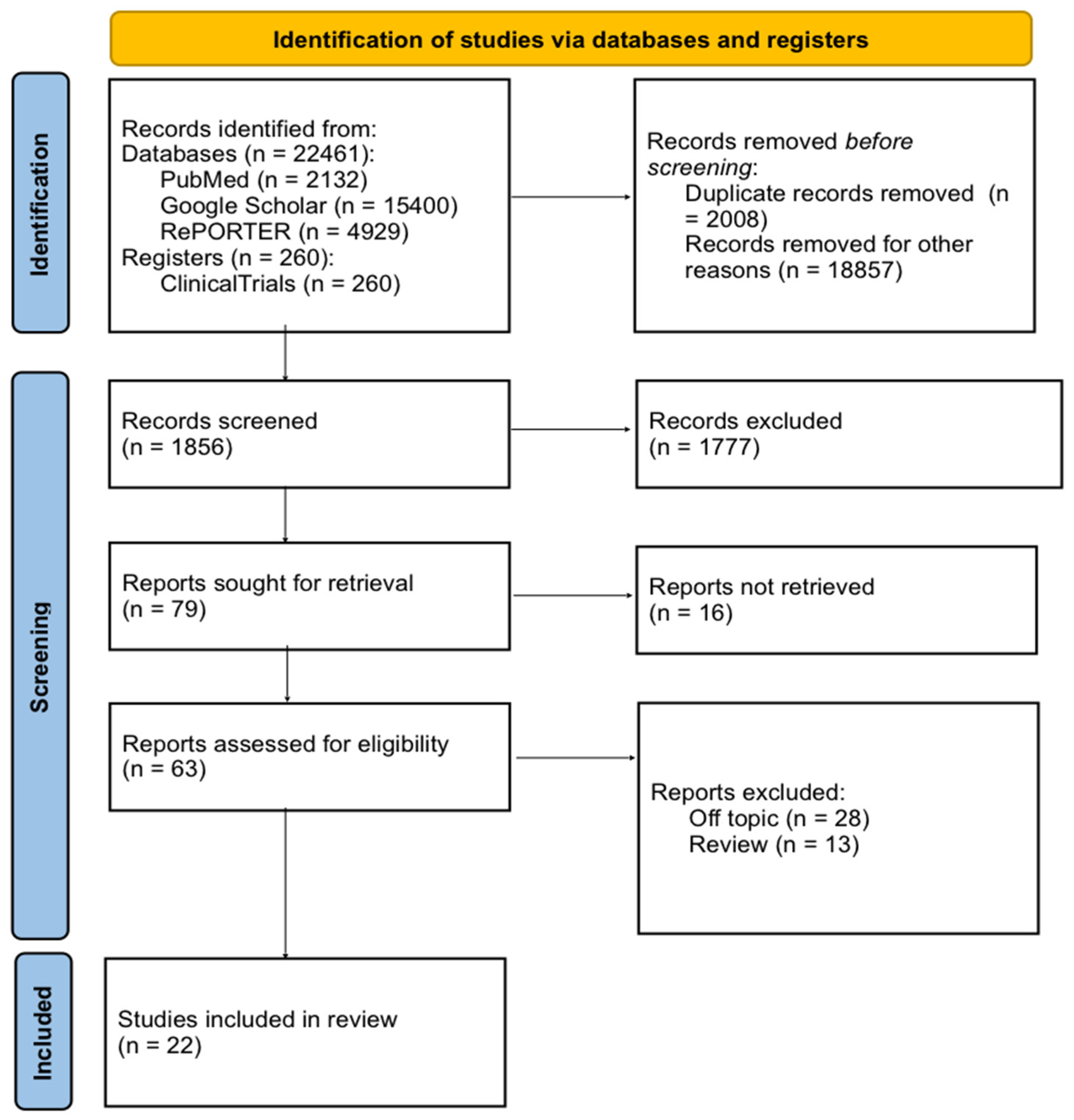
Figure 1.
PRISMA flow diagram illustrating searches of databases and registers.
3. Local Immune Response and Mucous Membranes
Most pathogens enter the body through mucous membranes, usually during ingestion, inhalation, or sexual contact, thus, overcoming not only the physical barrier, but also the immune response, organised by the mucosa-associated lymphoid tissue (MALT). In order to better understand the mechanisms of mucosal protection, let’s take a closer look at the anatomy of the female reproductive tract (FRT). The lower FRT is covered by a thick, stratified squamous epithelium. In contrast, the upper FRT is lined with simple columnar epithelium. The transformation area between two tissues contains numerous CD4+ T cells and antigen-presenting cells [10,11]. Most of the ways in which HIV enters the lower FRT involve the breach of the mucosal surface during sexual activity, ulceration caused by other sexually transmitted infections, and the direct infection of CD4+ T cells or macrophages within the epithelium. It is noteworthy that studies suggest anal intercourse to be a more significant risk factor for HIV-1 acquisition than vaginal intercourse [12]. This is explained by the presence of highly susceptible to HIV CD4+ T-cells in the distal gastrointestinal tract and their rapid depletion after the infection, so it makes sense why diarrhoea and wasting syndromes are some of the most common manifestations of the disease [13].
The process of overcoming the mucosal barrier by HIV infection includes several steps. Firstly, the selection of the virus’s genotype occurs, therefore, not all virions will be able to penetrate through the mucous membranes. For instance, B cells upon activation by mucosal dendritic cells switch the class to IgA, which can capture and inactivate viral particles that are not associated with cells [14]. Unfortunately, HIV possesses various ways of suppressing the first line of the mucosal defence. One hypothesis of an impaired humoral response relates to the impact of HIV-1 Nef on B-cell signalling and the inhibition of immunoglobulin class switching. This proposed mechanism involves the creation of actin-driven cellular conduits, that allows Nef to transit from infected macrophages and dendritic cells to uninfected germinal center B cells and accumulate there, which leads to to diminished expression of activation-induced cytidine deaminase, an essential enzyme for class switching. This process is thought to interfere with the normal functioning of B cells and their ability to mount an effective immune response [15,16] (Figure 2).
After transmission of HIV to CD4+ cells,the next step of virus selection develops, where the main role belongs to CD8+ cells, which must recognize infected cells and destroy them through the release of cytotoxic substances. However, upon close examination, it has been observed that gastrointestinal CD8+ T cells have notably lower levels of perforin and granzyme B compared to their counterparts in the blood [17]. Furthermore, two crucial transcription factors, whose expression is required for perforin expression and cytotoxicity, T-bet and Eomesodermin, are weakly expressed by rectal CD8+ T cells. Additionally, the HIV protein Nef limits detection of infected cells by cytotoxic T lymphocytes through the selective downregulation of both HLA-A and HLA-B expression, reducing the presentation of viral epitopes on the cell surface [18]. Restriction of cytotoxic response might prove beneficial to the host by limiting mucosal T-cell depletion and tissue damage. On the other hand, the inability to completely eliminate HIV-infected cells results in the failure of the second step of the virus selection [19].
4. Microbicides
Microbicides represent a potential intervention strategy for preventing HIV transmission. When applied in the vagina or rectum, these medications work to inhibit the penetration of infectious agents affecting the components of mucosal immunity.
Almost three decades ago, the concept of a topical microbicide to protect against HIV was proposed. This idea was driven by the goal of providing women with protection they can control as the majority of prevention methods available to females are subject to the control of their male partners [20]. Along with effective vaccines, microbicides (topical preexposure prophylaxis (PrEP)) and oral PrEP have the potential to accomplish this goal. Both can also serve to protect both men and women from HIV transmission during unprotected anal intercourse [21].
Modern microbicides can be divided into fast-acting drugs, designed to be applied within 1 hour before or after coitus, and drugs used to deliver the active component over a prolonged period of time. The first type includes various forms: gels, creams, ointments, lotions, tablets, aerosols, rinses and application films. These types of microbicides offer the benefit of easy application but their disadvantage is the brief duration of the active component’s effectiveness due to its rapid removal from the epithelial surface. Prolonged drugs include microbicides in forms of contraceptive sponges, intravaginal rings (IVR), uterine (cervical) caps, or enclosed in vaginal or rectal suppositories. They maintain the virucidal concentration of the active component over a greater period of time but also require mechanical installation, for which gynaecological intervention can be used [21,22].
The following groups of microbicides can be distinguished: surfactants or membrane disruptors; vaginal milieu protectors; anionic polymers; dendrimers; carbohydrate-binding proteins; HIV replication inhibitors (reverse transcriptase inhibitors).
Multi-purpose prevention technologies (MPTs) deserve special attention - these are means that provide a combination of HIV prevention, a number of sexually transmitted diseases and contraception.
For the most part, and this is evident from the research currently underway, these are advanced microbicides. Often this is a hormonal drug that acts as a contraceptive and an antiretroviral drug. Among the MPTs being developed, it is worth noting the presence of an implant form, which is injected subcutaneously and gradually releases the active substance.
4.1. Surfactants/Membrane Disruptors
Surfactants were among the first compounds to undergo clinical evaluation as topical microbicides. Well-known representatives of the first generation include nonoxynol-9 (N-9), a mixture of cetyl betaine and myristamine oxide (1.0% C31G; SAVVY) and sodium lauryl sulfate (SLS). Their action mechanism is non-specific and involves disruption of cellular and microbial membranes, which offers contraceptive activity against a wide range of pathogens. However, this could also be potentially toxic to host cells, leading to the destruction of the epithelium, vaginal irritation, inflammation, tissue infiltration by host immune cells, and alterations in vaginal flora, consequently increasing the risk of HIV infection.
The first microbicide formally tested for its efficacy in preventing HIV transmission was N-9. Phase II efficacy trial with COL-1492, a N-9 vaginal gel in female sex workers revealed that applying it more than three times per working day doubled the risk of HIV infection compared to placebo users [23]. Another phase III clinical trial represented that the use of N-9 vaginal film did not reduce the rate of new HIV infection [24]. Both of these results lead to the conclusion that it can no longer be regarded as an effective method for preventing HIV.
C31G, showing broad anti-infective activity against many bacterial and viral STD pathogens, was tested in different safety trials and was advanced to phase III clinical trial in Africa (Ghana and Nigeria) [25,26]. The Nigerian trial with SAVVY vaginal gel represented no significant differences among participants receiving SAVVY compared with those receiving placebo [27].
Sodium lauryl sulfate (SLS) was represented as a potent inhibitor of the infectivity of several enveloped (HIV-1, Herpes simplex viruses, Semliki Forest virus) and nonenveloped (papillomaviruses, reovirus, rotavirus and poliovirus) viruses because of its protein denaturing potency [28]. It was designed to function like an “invisible condom”, able to coat the vaginal wall in liquid form at room temperature and subsequently transition into a gel at body temperature. Although the results of a phase II study of 200 women in Cameroon have been pending, the interest in development of surfactants, indicating a narrow margin between effectiveness and safety, has waned.
4.2. Vaginal Milieu Protectors
Vaginal milieu protectors, another broad group of microbicides, function to preserve the acidic environment within the vaginal canal at a pH level of 4, which was shown to inactivate HIV [29]. The microbicides of this category either directly acidify or enhance the production of lactobacilli. They also serve as spermicides because the presence of semen neutralises the baseline acidity of the vagina, thereby facilitating the penetration of the virus.
Carbopol 974P (BufferGel) is one of the modern representatives of microbicides and a polymer of acrylic acid that can significantly reduce the acidity of the vaginal environment. This, in turn, demonstrates virucidal activity against HIV, as confirmed through in-vitro testing [30]. According to clinical studies conducted on female volunteers in India, Thailand, Malawi, and Zimbabwe BufferGel was proved to be safe and well tolerated by the cervicovaginal epithelium. Notably, there was a reported decrease in the prevalence of bacterial vaginosis after the first week of product use [31]. In 2009, the US National Institute of Allergy and Infectious Diseases (NIAID) discovered that repeated use of Buffer Gel led to the suppression of innate immunity. This finding prevented the product from entering the pharmaceutical market.
The Novel Intravaginal Ring as a Non-Hormonal MPT from the Population Council, whose active ingredients are copper, zinc, lactate, is also designed to optimise vaginal health and protect against STIs by increasing vaginal lactic acid concentrations. Copper IVR (Cu-IVR) from the University of California, which has a similar mechanism of action but does not offer protection against HIV, is also at an early preclinical stage. These drugs are also spermicides (inhibit sperm motility).
Additionally, in the early 21st century, attempts were made by doctors to employ lactobacilli as microbicides for stabilising vaginal pH—a remedy historically used for managing different dysbioses. However, due to the brief duration of therapeutic effects and the extended time required for lactobacilli colonies to flourish, research on microbicides based on non-genetically modified Lactobacillus sp. was subsequently discontinued.
4.3. Entry Inhibitors
The group of microbicides based on anionic polymers and dendrimers includes substances such as carrageenans, naphthalene sulfonate polymers, cellulose sulfate, nanosized dendrimers and humic acids. Action mechanism of this group involves the inhibition of viral fusion by binding to HIV surface proteins or to receptors and co-receptors of target cells.
One of the first microbicides of this group were carrageenans, a family of linear sulfated polysaccharides derived from a seaweed extract. Carrageenans are similar in structure to heparan sulfate, which is used by many microorganisms as a biochemical receptor for initial attachment to the cell membrane. Thus, carrageenans act as decoy receptors for virus fusion [22]. However, a phase III study carried out on female volunteers in South Africa from 2004 to 2007 indicated that while Carraguard gel was deemed safe for over a 2-year period of use, the occurrence of new HIV infections was comparable in both the Carraguard and placebo groups. Thus, the study did not demonstrate a statistically significant impact of carrageenans on the sexual transmission of HIV infection [32].
Other polyanionic microbicides are naphthalene sulfonate polymers PIC 024-4 and PRO 2000. PRO 2000 competes with the V3 loop of gp120 HIV-1 envelope in binding with the target cell receptor CD4 [33]. Clinical trials of PRO 2000 vaginal gel conducted on female volunteers from South Africa, Tanzania, Uganda and Zambia showed the safety of the drug, however, its effectiveness was not proven.
SPL7013 (or VivaGel® or astodrimer sodium), belonging to macromolecules with a tree-like and regularly branching structure (dendrimers) is of great interest as it is the only medication that does not contain antiretroviral (ARV) agents but yet demonstrates excellent anti-HIV potential. This medication, which initially showed its effectiveness in treating bacterial vaginosis, has already completed phase 3 clinical trials (NCT01577537), and has been registered and approved for use in more than 55 countries. In addition, the company began producing a lubricated condom and a nasal spray with the same active ingredient, which provides a moisturizing and protective barrier against respiratory viruses [34].
In the future, developments based on dendrimer-like substances, such as humic acids found ubiquitously in nature, hold promise. These substances are hyperbranched polyelectrolytes, characterized by a network of polydisperse aromatic and aliphatic structures highly substituted by carboxyl and hydroxyl groups. Humic acids, known for their low toxicity and antioxidant activity, have synthetic analogs like HS-1500 (oxyhumate), obtained through hydroquinone polymerization. Research has shown their ability to inhibit HIV in MT-2 cells [35], with effective concentrations ranging from 50-300 ng/ml and a semi-toxic concentration of 600 µg/ml.
HS-1500’s proposed mechanism involves blocking the binding of the V3 loop of gp120 to the CD4 receptor on target cells. Studies by G.K. Joone et al. demonstrated that HS-1500 enhances the proliferative effect of phytohemagglutinin on lymphocytes from HIV-infected patients [36]. This stimulative effect was also observed when administering HS-1500 to HIV-positive patients at a dose of 4 g/day for 2 weeks. The observed proliferation stimulation correlated with increased production of interleukin (IL) 2 and expression of IL-2 receptors, along with a decrease in the amount of IL-10 under the influence of HS-1500.
Another promising group may be polysaccharide-binding substances, whose representatives belong to natural peptides. The most prominent representatives are cyanovirin-N (CVN), a lectin compound derived from the cyanobacterium Nostoc ellipsosporum, and griffithsin (GRFT), derived from the red algae Griffithsia. Their mechanism of action involves the prevention of viral-host cell fusion by mannose residues on the surface of the virion. The effectiveness of these proteins against HIV infection when administered rectally and vaginally has been proven in preclinical studies [37]. The Population Council has begun to develop a vaginal insert based on this substance and 2 studies are currently at the preclinical testing stage. For the purposes of this study, GRFT has been genetically modified to produce a more stable compound less prone to oxidation, called Q-GRFT. It will be safe and suitable for use by women of any age, as well as pregnant and lactating women [38].
Peptide microbicides are promising, as it is possible to integrate the gene encoding this peptide into any microorganism. At the U.S. National Institutes of Health (NIH), research is being conducted on the potential colonisation of women’s vaginal microbiota with Lactobacillus jensenii, bacteria containing an embedded gene producing cyanovirin-N protein. Thus, this kind of microbicide will have multiple mechanisms of action: the ability to bind mannose residues on the virion surface and restore the normal vaginal flora.
4.4. HIV Replication Inhibitors
The mechanism of action of this group involves binding to the HIV-1 Reverse Transcriptase (RT) enzyme, which is responsible for the conversion of viral RNA into Proviral DNA, making viral replication impossible. One of the main distinguishing features of HIV replication inhibitors is that their active substances have already demonstrated efficacy in HIV Therapeutics. There are Nucleoside RT Inhibitors (NRTIs), or Nucleotide RT Inhibitors, which mimic endogenous nucleotides and halt the elongation of the viral DNA chain within the target cell, and Non-Nucleoside RT Inhibitors (NNRTIs), which in turn disrupt the binding of the substrate to the active site of the enzyme and have been demonstrated to bind irreversibly to RT [39]. The most famous representative of the NNRTI class is Dapivirine. Due to its irreversible binding and lipophilic properties, it may be active against both Cell-Free and Cell-Associated HIV. A vaginal gel based on dapivirine has demonstrated the ability to prevent HIV infection in humanised mice during preclinical trials [40]. The lead NRTI, in turn, is tenofovir, an adenosine monophosphate analogue. Tenofovir is converted into the active metabolite tenofovir diphosphate, which competes with deoxycytidine 5’-triphosphate for HIV-1 reverse transcriptase. It was formulated as a 1.0% vaginal gel as a microbicide composition.
Clinical trials conducted by the Centre for the AIDS Programme of Research in South Africa (CAPRISA) in July 2010 showed that tenofovir gel was 39% effective [41]. The results of third phase (FACTS-001) clinical trials indicated that peri-coital tenofovir did not prevent HIV-1 acquisition among young women at risk for HIV infection in South Africa. Microbicides from this group play a crucial role in drugs designed for pre-exposure prophylaxis, which are currently undergoing both clinical and preclinical trials.
4.4.1. Clinical Trials of Topical and oral Pre-Exposure Prophylaxis (PrEP)
In introducing drugs designed for topical pre-exposure prophylaxis (PrEP) currently undergoing clinical trials, it is essential to highlight the diverse intravaginal rings (IVRS) as notable candidates in this emerging landscape. IVRS containing only tenofovir (TFV) or TFV plus levonorgestrel (LNG), which is a contraceptive hormone, have undergone several Phase I trials conducted by CONRAD in 2016 (NCT02235662) and 2019 (NCT03279120), respectively, and have successfully met all performance benchmarks.Currently, the NCT03255915 study of intravenous administration (TDF-FTC pod-IVR) is ongoing, but participants have not been recruited yet. A Phase-IIa trial conducted in Kenya (NCT03762382) showed that TFV/LNG and TFV-containing IVRS did not adversely affect the genital microbiota and are therefore safe to use [42].
Another type of IVRS includes those containing dapivirine, an NNRTI (non-nucleoside reverse transcriptase inhibitor), which are in their final stages of development. The completed Phase 3b trial by the Microbicide Trials Network (MTN 043) affirms the safety of monthly DPV (dapivirine)-containing IVRS, particularly when used by breastfeeding women. It is worth noting that DPV IVRs have been approved by the South African Health Products Regulatory Agency (SAHPRA), for women, in March 2022. This was immediately followed by an official WHO recommendation being issued. IVRs containing DPV/LNG, which are released over a period of 90 days, underwent Phase I trials, resulting in encouraging outcomes, supporting further development of the DPV/ LNG IVR. Additionally, it is worth noting fast-dissolving inserts that are applicable for both vaginal and rectal use. They incorporate tenofovir alafenamide (TAF), a tenofovir prodrug, and elvitegravir (EVG), which is an HIV-1 integrase strand transfer inhibitor. The latter prevents the integration of HIV-1 DNA into the host DNA, thereby blocking the formation of the HIV-1 provirus [20,42,43]
These inserts have shown positive results in non-human primates, whether they are inserted vaginally hours before or after exposure to SHIV (simian human immunodeficiency virus). Additionally, in phase I trials (CONRAD 146 and MTN-039), the inserts were assessed for safety, pharmacokinetics, and pharmacodynamics. CONRAD 146 was a completed study that evaluated the TAF/EVG vaginal insert, while MTN-039 was a study focused on the rectal administration of the same and its results are expected soon. Additionally, a placebo version of this insert was assessed in two global studies: the Quatro study comparing four vaginal forms in African women and the MTN-035 (DESIRE) study comparing three rectal forms. The next step involves bringing this drug to a comprehensive multi-dose safety and pharmacokinetic study [44].
It is necessary to mention the means being developed for HIV monoprophylaxis. For example, MK-8527, a new nucleoside reverse transcriptase translocation inhibitor is being developed by Merck. This drug will be used as a once-weekly drug for treatment and as a monthly drug for PrEP. Merck had hoped that islatravir could be developed as a weekly or monthly antiretroviral, but at the higher doses needed for long-acting dosing, islatravir caused loss of lymphocytes. Currently, there are 2 trials of the drug underway. These are the MK-8527 Single-Dose Trial in HIV-1 Infected Participants (MK-8527-004) under registration number NCT05494736, taking place in Romania and South Africa, and the Safety and Pharmacokinetic Study of Oral MK-8527 QM in Participants at Low-Risk for HIV-1 Infection (MK-8527-007) under registration number NCT06045507, currently recruiting in Israel and the USA.
The first study evaluated the safety, tolerability, pharmacokinetics, and antiretroviral activity of MK-8527 in participants who had not previously received antiretroviral therapy with HIV-1 infection. The second study is a double-blind, placebo-controlled study designed to assess the safety, tolerability, and pharmacokinetics of oral MK-8527 taken once a month in participants at low risk of HIV-1 infection.
It is important to remember PrEp drugs that have been approved by the Food and Drug Administration (FDA). There are two combined drugs from Gilead: Truvada and Descovy. Descovy contains two different medicines: emtricitabine and tenofovir alafenamide. Truvada contains two different active ingredients: emtricitabine and tenofovir disoproxil fumarate. Both are used for HIV PrEP to reduce the risk of HIV infection in adults and adolescents who weigh at least 77 lb (35 kg), are HIV negative, and are at risk of getting HIV. However, the Descovy drug for PrEP is not approved for use in females at risk of infection through vaginal sex, as this use has not been studied in clinical trials [45,46].
The company ViiV Healthcare is introducing Cabotegravir in two forms - tablets and long-acting injections. Cabotegravir oral tablet (brand name: Vocabria) is used both for the short-term treatment of HIV infection in adults and adolescents 12 years of age and older who weigh at least 77 lb (35 kg) and for short-term PrEP to reduce the risk of HIV infection in adults and adolescents who weigh at least 77 lb (35 kg), are HIV negative, and are at risk of getting HIV. Long-acting injectable cabotegravir (brand name: Apretude) is used for HIV PrEP to reduce the risk of HIV infection in adults and adolescents who weigh at least 77 lb (35 kg), are HIV negative, and are at risk of getting HIV [47].
Gilead Sciences presents Lenacapavir, approved by the FDA under the brand name Sunlenca for HIV treatment. Belonging to a group of capsid inhibitors, Lenacapavir can interfere with the HIV capsid, which protects the virus’s genetic material and replication enzymes. This interference leads to disruption at various stages of the viral life cycle, preventing HIV multiplication and reducing viral load. Lenacapavir is also under investigation as a preventive measure in ongoing studies (NCT04994509 in South Africa and Uganda, and NCT04925752 in the United States, Brazil, Puerto Rico, and South Africa), with Phase 3 results pending [48]. Ongoing clinical trials are shown in Table 1.
4.4.2. Drugs in Preclinical and Early Clinical Phases
There are quite a few combined drugs undergoing preclinical and early-stage clinical development that hold potential for progressing into subsequent phases of clinical trials. We would have an easier time categorising these drugs according to their hormonal classification. Drugs of the hormonal type typically consist of a hormonal contraceptive (LNG, EE, Etonogestrel or Norelgestromin), combined with various antiretroviral drugs such as DPV, TDF, TFV or Cabotegravir and Islatravir. As mentioned earlier, these combinations serve to prevent ovulation and inhibit replication of HIV.
Another example of potential hormonal drugs involves combining contraceptive hormones with the stable analog of non-anti-retroviral anti-HIV lectins, QGRFT, which binds to the HIV envelope glycoprotein and prevents entry into target cells. Non-hormonal microbicides composed of various components primarily aim to bind or inactivate sperm, thereby preventing not only pregnancy but also transmission of HIV. Some are based on combinations of monoclonal antibodies like mAb 2C7, which mediates the killing of Neisseria gonorrhoeae or agglutinating sperm antibodies, with antiretroviral drugs, specifically TDF. Others are represented by IVR containing a fully human antibody (HCA) that has the ability to agglutinate sperm incorporated into a sustained release delivery system effectively preventing both pregnancy and transmission of HIV, but monoclonal antibodies are not the only option for future PrEP. There are other combinations of drugs like QGRFT with organic acids formulated into fast dissolving inserts that lower vaginal pH in presence of semen rendering it inactive. Other possible drugs for rendering semen infertile without harming other cells are combinations of polyphenylene and carboxymethylene (PPCM). PPCM causes premature acrosome loss in sperm and inhibits hyaluronidase, preventing sperm from fertilising an ovum [52].
Except for new combinations with a familiar delivery system, certain products have been introduced using an innovative one. This involves incorporating TFV / EFV nanoparticles (NPs) into a polymer film base (TFV / EFV NPs - in - film), enabling higher concentrations of both drugs in the genitals compared to their delivery in a liquid carrier [53]. The discussed combined microbicides, featuring groundbreaking innovations, have promising prospects. Notably, these formulations are at various stages in clinical trials, ranging from early to advanced phases and are nearing commercial viability. A significant number of candidates are undergoing clinical investigation, highlighting the potential of microbicides for future preventive applications.
As these products progress through research phases, it becomes increasingly clear that microbicides have the potential to play a critical role in preventive healthcare strategies [20,54,55,56,57]. Summary chapters are available in Table 2 and Table 3. The chemical structures of the mentioned microbicides are presented in Table 4.
5. Discussion
Microbicides play a crucial role in the fight against HIV/AIDS by providing an additional prevention tool, particularly for populations facing barriers to other existing methods such as condoms or oral PrEP. The urgent need for microbicides targeting HIV, particularly those designed for vaginal application, stems from several critical factors that underline the ongoing global efforts to curb the spread of HIV/AIDS. Globally, women bear a disproportionate burden of HIV infection, especially in sub-Saharan Africa where they account for a majority of new infections. Biological factors, such as the higher susceptibility of vaginal tissues to HIV transmission compared to penile tissues, contribute to this disparity. Vaginal microbicides offer a targeted approach to address this vulnerability by providing a protective barrier at the site of transmission, potentially reducing the risk of HIV acquisition among women. While significant progress has been made in HIV prevention, existing strategies such as condoms and oral PrEP have limitations that underscore the need for additional options. Condoms require partner cooperation and may not be consistently used, while oral PrEP may be inaccessible or unsuitable for some individuals. Vaginal microbicides offer a complementary approach that can be used discreetly and independently, filling critical gaps in the prevention toolkit and bolstering overall HIV prevention efforts.
6. Conclusion
In conclusion, the field of microbicides holds great promise for the ongoing fight against HIV infection. Recently discovered, these compounds offer a fertile ground for potential breakthroughs with numerous unexplored and unsynthesized forms. We have examined diverse classes of microbicide, dissecting their benefits and drawbacks. Our focus has narrowed down to the most promising groups of preventive agents, exploring their evolution through different phases of clinical trials. Microbicides with their multifaceted nature move from early research into the verge of being available. Within clinical trials, the extensive interest in them become apparent, revealing the nuanced promise that these agents hold for preventing HIV. Despite challenges such as optimising efficacy and distributing widely, the documented progress indicates a hopeful trajectory. Ongoing exploration and synthesis of microbicide fuel optimism for innovative solutions in HIV prevention. This field is an exciting frontier for further research and development in the global battle against HIV/AIDS.
Author Contributions
Conceptualization, Y.V.Z., V.O.P. and M.Y.S.; writing-original draft preparation, Y.V.Z., V.O.P., M.Y.S., S.O.V.; writing—review and editing, Y.V.Z., V.O.P., M.Y.S., S.O.V., E. Al-khaleefa, K.R.P., N.Y.F., D.V.S., R.V.P., O.V.M., A.A.B., N.N.Z.; visualization, M.Y.S., Y.V.Z.; supervision, Y.V.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- UNAIDS data 2023. Available online: https://www.unaids.org/en/resources/documents/2023/2023_unaids_data (accessed on 14 May 2024).
- WHO HIV data and statistics. Available online: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics (accessed on 14 May 2024).
- Frolova, O.P.; Butylchenko, O.V.; Gadzhieva, P.G.; Timofeeva, M.Y.; Basangova, V.A.; Petrova, V.O.; Fadeeva, I.A.; Kashutina, M.I.; Zabroda, N.N.; Basov, A.A.; et al. Medical Care for Tuberculosis-HIV-Coinfected Patients in Russia with Respect to a Changeable Patients’ Structure. Trop. Med. Infect. Dis. 2022, 7, 86. [Google Scholar] [CrossRef]
- Moskaleychik, F.F.; Laga, V.Y.; Delgado, E.; Vega, Y.; Fernandez-Garcia, A.; Kornilaeva, G.V.; Pronin, A.Y.; Zhernov, Y.V.; Thomson, M.M.; Bobkova, M.R.; et al. Rapid spread of the HIV-1 circular recombinant CRF02-AG in Russia and neighboring countries. Vopr Virusol. 2015, 60, 14–19. (In Russian) [Google Scholar] [PubMed]
- Karamov, E.; Epremyan, K.; Siniavin, A.; Zhernov, Y.; Cuevas, M.T.; Delgado, E.; Sanchez-Martinez, M.; Carrera, C.; Kornilaeva, G.; Turgiev, A.; et al. HIV-1 Genetic Diversity in Recently Diagnosed Infections in Moscow: Predominance of AFSU, Frequent Branching in Clusters, and Circulation of the Iberian Subtype G Variant. AIDS Res. Hum. Retroviruses 2018, 34, 629–634. [Google Scholar] [CrossRef]
- Zhernov, Y.V.; Kremb, S.; Helfer, M.; Schindler, M.; Harir, M.; Mueller, C.; Hertkorn, N.; Avvakumova, N.P.; Konstantinov, A.I.; Brack-Werner, R.; et al. Supramolecular combinations of humic polyanions as potent microbicides with polymodal anti-HIV-activities. New J. Chem. 2016, 41, 212–224. [Google Scholar] [CrossRef]
- Zhernov, Y. Natural humic substances interfere with multiple stages of the replication cycle of human immunodeficiency virus. J. Allergy Clin. Immunol. 2018, 141, AB233–AB233. [Google Scholar] [CrossRef]
- Zhernov, Y.V.; Khaitov, M.R. Microbicides for topical immunoprevention of HIV infection. Bull. Sib. Med. 2019, 18, 49–59. [Google Scholar] [CrossRef]
- Zhernov, Y.V.; Konstantinov, A.I.; Zherebker, A.; Nikolaev, E.; Orlov, A.; Savinykh, M.I.; Kornilaeva, G.V.; Karamov, E.V.; Perminova, I.V. Antiviral activity of natural humic substances and shilajit materials against HIV-1: Relation to structure. Environ. Res. 2020, 193, 110312–110312. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, A. Antiviral immune responses in the genital tract: clues for vaccines. Nat. Rev. Immunol. 2010, 10, 699–711. [Google Scholar] [CrossRef] [PubMed]
- Pudney, J.; Quayle, A.J.; Anderson, D.J. Immunological Microenvironments in the Human Vagina and Cervix: Mediators of Cellular Immunity Are Concentrated in the Cervical Transformation Zone1. Biol. Reprod. 2005, 73, 1253–1263. [Google Scholar] [CrossRef]
- Chenine, A.L.; Siddappa, N.B.; Kramer, V.G.; Sciaranghella, G.; Rasmussen, R.A.; Lee, S.J.; Santosuosso, M.; Poznansky, M.C.; Velu, V.; Amara, R.R.; et al. Relative Transmissibility of an R5 Clade C Simian-Human Immunodeficiency Virus Across Different Mucosae in Macaques Parallels the Relative Risks of Sexual HIV-1 Transmission in Humans via Different Routes. J. Infect. Dis. 2010, 201, 1155–1163. [Google Scholar] [CrossRef]
- Veazey, R.S.; DeMaria, M.; Chalifoux, L.V.; Shvetz, D.E.; Pauley, D.R.; Knight, H.L.; Rosenzweig, M.; Johnson, R.P.; Desrosiers, R.C.; Lackner, A.A. Gastrointestinal Tract as a Major Site of CD4 + T Cell Depletion and Viral Replication in SIV Infection. Science 1998, 280, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Moretti, S.; Cafaro, A.; Tripiciano, A.; Picconi, O.; Butto, S.; Ensoli, F.; Sgadari, C.; Monini, P.; Ensoli, B. HIV therapeutic vaccines aimed at intensifying combination antiretroviral therapy. Expert Rev. Vaccines 2020, 19, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Qiao, X.; He, B.; Chiu, A.; Knowles, D.M.; Chadburn, A.; Cerutti, A. Human immunodeficiency virus 1 Nef suppresses CD40-dependent immunoglobulin class switching in bystander B cells. Nat. Immunol. 2006, 7, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; A Santini, P.; Sullivan, J.S.; He, B.; Shan, M.; Ball, S.C.; Dyer, W.B.; Ketas, T.J.; Chadburn, A.; Cohen-Gould, L.; et al. HIV-1 evades virus-specific IgG2 and IgA responses by targeting systemic and intestinal B cells via long-range intercellular conduits. Nat. Immunol. 2009, 10, 1008–1017. [Google Scholar] [CrossRef] [PubMed]
- Shacklett, B.L.; Cox, C.A.; Quigley, M.F.; Kreis, C.; Stollman, N.H.; Jacobson, M.A.; Andersson, J.; Sandberg, J.K.; Nixon, D.F. Abundant Expression of Granzyme A, but Not Perforin, in Granules of CD8+ T Cells in GALT: Implications for Immune Control of HIV-1 Infection. J. Immunol. 2004, 173, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Shacklett, B.L. Mucosal Immunity in HIV/SIV Infection: T Cells, B Cells and Beyond. Curr. Immunol. Rev. 2019, 15, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Kiniry, B.; Ganesh, A.; Critchfield, J.; Hunt, P.; Hecht, F.; Somsouk, M.; Deeks, S.; Shacklett, B. Predominance of weakly cytotoxic, T-betLowEomesNeg CD8+ T-cells in human gastrointestinal mucosa: implications for HIV infection. Mucosal Immunol. 2016, 10, 1008–1020. [Google Scholar] [CrossRef] [PubMed]
- Baeten, J.M.; Hendrix, C.W.; Hillier, S.L. Topical Microbicides in HIV Prevention: State of the Promise. Annu. Rev. Med. 2020, 71, 361–377. [Google Scholar] [CrossRef] [PubMed]
- Shattock, R.J.; Rosenberg, Z. Microbicides: Topical Prevention against HIV. Cold Spring Harb. Perspect. Med. 2011, 2, a007385–a007385. [Google Scholar] [CrossRef]
- Zhernov, Y.V.; Khaitov, M.R. Microbicides for topical immunoprevention of HIV infection. Bull. Sib. Med. 2019, 18, 49–59. [Google Scholar] [CrossRef]
- Van Damme, L.; Ramjee, G.; Alary, M.; Vuylsteke, B.; Chandeying, V.; Rees, H.; Sirivongrangson, P.; Tshibaka, L.M.; Ettiègne-Traoré, V.; Uaheowitchai, C.; et al. Effectiveness of COL-1492, a nonoxynol-9 vaginal gel, on HIV-1 transmission in female sex workers: a randomised controlled trial. Lancet 2002, 360, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Roddy, R.E.; Zekeng, L.; Ryan, K.A.; Tamoufe, U.; Weir, S.S.; Wong, E.L. A controlled trial of nonoxynol-9 film to reduce male-to-female transmission of sexually transmitted diseases. N Engl J Med. 1998, 339, 504–10. [Google Scholar] [CrossRef]
- Bax, R.; Douville, K.; McCormick, D.; Rosenberg, M.; Higgins, J.; Bowden, M. Microbicides—evaluating multiple formulations of C31G. Contraception 2002, 66, 365–368. [Google Scholar] [CrossRef]
- Ballagh, S.; Baker, J.; Henry, D.; Archer, D. Safety of single daily use for one week of C31G HEC gel in women. Contraception 2002, 66, 369–375. [Google Scholar] [CrossRef]
- Feldblum, P.J.; Adeiga, A.; Bakare, R.; Wevill, S.; Lendvay, A.; Obadaki, F.; Olayemi, M.O.; Wang, L.; Nanda, K.; Rountree, W. SAVVY Vaginal Gel (C31G) for Prevention of HIV Infection: A Randomized Controlled Trial in Nigeria. PLOS ONE 2008, 3, e1474. [Google Scholar] [CrossRef] [PubMed]
- Piret, J.; Desormeaux, A.; Bergeron, M.G. Sodium Lauryl Sulfate, a Microbicide Effective Against Enveloped and Nonenveloped Viruses. Curr. Drug Targets 2002, 3, 17–30. [Google Scholar] [CrossRef] [PubMed]
- O'Connor, T.J.; Kinchington, D.; O Kangro, H.; Jeffries, D.J. The Activity of Candidate Virucidal Agents, Low pH and Genital Secretions against HIV-1 In Vitro. Int. J. STD AIDS 1995, 6, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Ongradi, J.; Ceccherini-Nelli, L.; Pistello, M.; Specter, S.; Bendinelli, M. Acid Sensitivity of Cell-Free and Cell-Associated HIV-1: Clinical Implications. AIDS Res. Hum. Retroviruses 1990, 6, 1433–1436. [Google Scholar] [CrossRef] [PubMed]
- van de Wijgert, J.; Fullem, A.; Kelly, C.; Mehendale, S.; Rugpao, S.; Kumwenda, N.; Chirenje, Z.; Joshi, S.; Taha, T.; Padian, N.; et al. Phase 1 Trial of the Topical Microbicide BufferGel: Safety Results From Four International Sites. Am. J. Ther. 2001, 26, 21–27. [Google Scholar] [CrossRef]
- van de Wijgert, J.H.H.M.; Braunstein, S.L.; Morar, N.S.; E Jones, H.; Madurai, L.; Strickfaden, T.T.E.; Moodley, M.; Aboobaker, J.; Ndlovu, G.; Ferguson, T.M.; et al. Carraguard Vaginal Gel Safety in HIV-Positive Women and Men in South Africa. Am. J. Ther. 2007, 46, 538–546. [Google Scholar] [CrossRef]
- Fletcher, P.S.; Wallace, G.S.; Mesquita, P.M.; Shattock, R.J. Candidate polyanion microbicides inhibit HIV-1 infection and dissemination pathways in human cervical explants. Retrovirology 2006, 3, 46–46. [Google Scholar] [CrossRef] [PubMed]
- Rupp, R.E.; Rosenthal, S.L.; Stanberry, L.R. VivaGel™ (SPL7013 Gel): A candidate dendrimer – microbicide for the prevention of HIV and HSV infection. Int. J. Nanomed. 2007, 2, 561–566. [Google Scholar]
- Schneider, J.; Weis, R.; Männer, C.; Kary, B.; Werner, A.; Seubert, B.J.; Riede, U.N. Inhibition of HIV-1 in Cell Culture by Synthetic Humate Analogues Derived from Hydroquinone: Mechanism of Inhibition. Virology 1996, 218, 389–395. [Google Scholar] [CrossRef]
- Jooné, G.K.; Dekker, J.; van Rensburg, C.E.J. Investigation of the Immunostimulatory Properties of Oxihumate. Z. Naturforsch C. 2003, 58, 263–267. [Google Scholar] [CrossRef] [PubMed]
- O'Keefe, B.R.; Vojdani, F.; Buffa, V.; Shattock, R.J.; Montefiori, D.C.; Bakke, J.; Mirsalis, J.; D'Andrea, A.-L.; Hume, S.D.; Bratcher, B.; et al. Scaleable manufacture of HIV-1 entry inhibitor griffithsin and validation of its safety and efficacy as a topical microbicide component. Proc. Natl. Acad. Sci. 2009, 106, 6099–6104. [Google Scholar] [CrossRef] [PubMed]
- Griffithsin-based Rectal Microbicide for PREvention of Viral ENTry (PREVENT). Available online: https://clinicaltrials.gov/study/NCT04032717 (accessed on 14 May 2024).
- Garg, A.B.; Nuttall, J.; Romano, J. The Future of HIV Microbicides: Challenges and Opportunities. Antivir. Chem. Chemother. 2009, 19, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Di Fabio, S.; Van Roey, J.; Giannini, G.; Mooter, G.v.D.; Spada, M.; Binelli, A.; Pirillo, M.F.; Germinario, E.; Belardelli, F.; de Bethune, M.-P.; et al. Inhibition of vaginal transmission of HIV-1 in hu-SCID mice by the non-nucleoside reverse transcriptase inhibitor TMC120 in a gel formulation. AIDS 2003, 17, 1597–1604. [Google Scholar] [CrossRef]
- Karim, Q.A.; Karim, S.S.A.; Frohlich, J.A.; Grobler, A.C.; Baxter, C.; Mansoor, L.E.; Kharsany, A.B.M.; Sibeko, S.; Mlisana, K.P.; Omar, Z.; et al. Effectiveness and Safety of Tenofovir Gel, an Antiretroviral Microbicide, for the Prevention of HIV Infection in Women. Science 2010, 329, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Dabee, S.; Mudhune, V.; McLellan-Lemal, E.; Peacock, S.; O’connor, S.; Njoroge, B.; Nyagol, B.; Thurman, A.R.; Ouma, E.; Ridzon, R.; et al. Genital microbiota of women using a 90 day tenofovir or tenofovir and levonorgestrel intravaginal ring in a placebo controlled randomized safety trial in Kenya. Sci. Rep. 2022, 12, 1–13. [Google Scholar] [CrossRef]
- Drug Database: Dapivirine. Available online: https://clinicalinfo.hiv.gov/en/drugs/dapivirine/patient (accessed on 14 May 2024).
- Drug Database: Tenofovir-Based Microbicides. Available online: https://clinicalinfo.hiv.gov/en/drugs/tenofovir-based-microbicides/patient (accessed on 14 May 2024).
- Drug Database: Emtricitabine / Tenofovir Disoproxil Fumarate. Available online: https://clinicalinfo.hiv.gov/en/drugs/emtricitabine-tenofovir-disoproxil-fumarate/patient (accessed on 14 May 2024).
- Drug Database: Emtricitabine / Tenofovir Alafenamide. Available online: https://clinicalinfo.hiv.gov/en/drugs/emtricitabine-tenofovir-alafenamide/patient (accessed on 14 May 2024).
- Drug Database: Cabotegravir. Available online: https://clinicalinfo.hiv.gov/en/drugs/cabotegravir-1/patient (accessed on 14 May 2024).
- Drug Database: Lenacapavir (HIV prevention). Available online: https://clinicalinfo.hiv.gov/en/drugs/lenacapavir-hiv-prevention (accessed on 14 May 2024).
- PK, Safety Study of 90-Day Use of Vaginal Rings Containing Dapivirine and Levonorgestrel. Available online: https://clinicaltrials.gov/study/NCT05041699 (accessed on 14 May 2024).
- Dapivirine-Contraceptive Ring. Available online: https://www.ipmglobal.org/our-work/our-products/dapivirine-contraceptive-ring (accessed on 14 May 2024).
- A Study of MK-8527 in Human Immunodeficiency Type 1 Virus (HIV-1) Infected Participants (MK-8527-002). Available online: https://clinicaltrials.gov/study/NCT03615183 (accessed on 14 May 2024).
- North, B.B.; Weitzel, M.B.; Waller, D.P.; Birch, W.X.; Feathergill, K.A.; Birch, L.A.; De Jonge, C.J.; Prins, G.S. Evaluation of the novel vaginal contraceptive agent PPCM in preclinical studies using sperm hyaluronan binding and acrosome status assays. Andrology 2021, 10, 367–376. [Google Scholar] [CrossRef]
- Cunha-Reis, C.; Machado, A.; Barreiros, L.; Araújo, F.; Nunes, R.; Seabra, V.; Ferreira, D.; Segundo, M.A.; Sarmento, B.; das Neves, J. Nanoparticles-in-film for the combined vaginal delivery of anti-HIV microbicide drugs. J. Control. Release 2016, 243, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Young, I.C.; Benhabbour, S.R. Multipurpose Prevention Technologies: Oral, Parenteral, and Vaginal Dosage Forms for Prevention of HIV/STIs and Unplanned Pregnancy. Polymers 2021, 13, 2450. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Garcia, M.; Patel, M.V.; Wira, C.R. Innate and adaptive anti-HIV immune responses in the female reproductive tract. J. Reprod. Immunol. 2013, 97, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.; Baxi, K.; Sawarkar, S.; Sarmento, B.; das Neves, J. Vaginal multipurpose prevention technologies: promising approaches for enhancing women’s sexual and reproductive health. Expert Opin. Drug Deliv. 2020, 17, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Maier, I.; Schiestl, R.H.; Kontaxis, G. Cyanovirin-N Binds Viral Envelope Proteins at the Low-Affinity Carbohydrate Binding Site without Direct Virus Neutralization Ability. Molecules 2021, 26, 3621. [Google Scholar] [CrossRef] [PubMed]
- Rupp, R.E.; Rosenthal, S.L.; Stanberry, L.R. VivaGel™ (SPL7013 Gel): A candidate dendrimer – microbicide for the prevention of HIV and HSV infection. Int. J. Nanomed. 2007, 2, 561–566. [Google Scholar]
- Thurman, A.R.; Ouattara, L.A.; Yousefieh, N.; Anderson, P.L.; Bushman, L.R.; Fang, X.; Hanif, H.; Clark, M.; Singh, O.; Doncel, G.F. A phase I study to assess safety, pharmacokinetics, and pharmacodynamics of a vaginal insert containing tenofovir alafenamide and elvitegravir. Front. Cell. Infect. Microbiol. 2023, 13, 1130101. [Google Scholar] [CrossRef]
- Dual Prevention Pill. Available online: https://www.prepwatch.org/products/dual-prevention-pill/ (accessed on 14 May 2024).
- An Etonogestrel/Ethinyl Estradiol/QGriffithsin (ETG/EE/QGRFT) IVR to Prevent Pregnancy and HIV. Available online: https://reporter.nih.gov/project-details/10138979 (accessed on 14 May 2024).
- Innovative 3D Printed Intravaginal Rings: Reengineering Multipurpose Intravaginal Rings for Prevention of HIV, STIs and Unintended Pregnancy. Available online: https://reporter.nih.gov/project-details/9761451 (accessed on 14 May 2024).
- Novel Intravaginal Ring as a Non-Hormonal Contraceptive – Population Council. Available online: https://popcouncil.org/project/novel-intravaginal-ring-as-a-non-hormonal-contraceptive/ (accessed on 14 May 2024).
- Next Generation Multipurpose Intravaginal Ring Technology Using Innovative CLIP 3D Printing. Available online: https://reporter.nih.gov/search/1z4GeTVlh0mC6fnWYAk0lw/project-details/10063935 (accessed on 14 May 2024).
- Gonorrhea and HIV prevention with intravaginal ring drug delivery. Available online: https://reporter.nih.gov/search/VIBGcRE-3kWMKyipADFpXw/project-details/10137883 (accessed on 14 May 2024).
- Next Generation Multipurpose Prevention Technology: An Intravaginal Ring for HIV Prevention and Nonhormonal Contraception. Available online: https://reporter.nih.gov/search/qZ_a5xi4M0SzX0laS07Tjw/project-details/10158504 (accessed on 14 May 2024).
- Capsule-intravaginal ring for sustained release of antibodies for non-hormonal contraception and vaginal protection against HIV. Available online: https://reporter.nih.gov/project-details/9799170 (accessed on 14 May 2024).
- Non-ARV/Non-Hormonal Multi-Purpose Vaginal Ring | MATRIX. Available online: https://www.matrix4prevention.org/products/non-arvnon-hormonal-multi-purpose-vaginal-ring (accessed on 14 May 2024).
- Novel pre-coital, non-hormonal multipurpose prevention technology (MPT). Available online: https://reporter.nih.gov/project-details/10395456 (accessed on 14 May 2024).
- Griffithsin Fast Dissolving Vaginal Insert | MATRIX. Available online: https://www.matrix4prevention.org/products/griffithsin-fast-dissolving-vaginal-insert (accessed on 14 May 2024).
- Long Acting Film Technology for Contraception and HIV Prevention (LATCH). Available online: https://reporter.nih.gov/project-details/10085198 (accessed on 14 May 2024).
- Extended Release Dapivirine Vaginal Film with Levonorgestrel | MATRIX. Available online: https://www.matrix4prevention.org/products/extended-release-dapivirine-vaginal-film-levonorgestrel (accessed on 14 May 2024).
- Cunha-Reis, C.; Machado, A.; Barreiros, L.; Araújo, F.; Nunes, R.; Seabra, V.; Ferreira, D.; Segundo, M.A.; Sarmento, B.; das Neves, J. Nanoparticles-in-film for the combined vaginal delivery of anti-HIV microbicide drugs. J. Control. Release 2016, 243, 43–53. [Google Scholar] [CrossRef]
- Cabotegravir Pellet Implant with Levonorgestrel. Available online: https://www.conrad.org/ (accessed on 14 May 2024).
- Long-acting multi prevention implant for 2-year contraception and HIV PrEP. Available online: https://reporter.nih.gov/search/t0FXMGGdiE622_eUszaw7g/project-details/10619811 (accessed on 14 May 2024).
- Ultra-Long-Acting Polymeric Injectable Multi-Purpose Prevention Technology for Contraception and HIV Prevention. Available online: https://reporter.nih.gov/search/WcUn8fWZy0KhTneo0yrZJQ/project-details/10258079 (accessed on 14 May 2024).
- Continuing Preclinical Development of PPCM Vaginal Contraceptive MPT to IND. Available online: https://reporter.nih.gov/project-details/9889971 (accessed on 14 May 2024).
- Copper Intravaginal Contraception. Available online: https://reporter.nih.gov/project-details/10018526 (accessed on 14 May 2024).
Figure 2.
In the first step of selection, the virus genotype is chosen. B cells switch the class to IgA, capturing and neutralising viral particles not linked to cells. On the other hand, HIV’s Nef protein impedes the immunoglobulin class switching process, limiting the effectiveness of humoral immunity. Second step involves selection of HIV particles associated with cells. CD8+ cells identify infected CD4+ cells and eliminate them by releasing cytotoxic substances.
Figure 2.
In the first step of selection, the virus genotype is chosen. B cells switch the class to IgA, capturing and neutralising viral particles not linked to cells. On the other hand, HIV’s Nef protein impedes the immunoglobulin class switching process, limiting the effectiveness of humoral immunity. Second step involves selection of HIV particles associated with cells. CD8+ cells identify infected CD4+ cells and eliminate them by releasing cytotoxic substances.
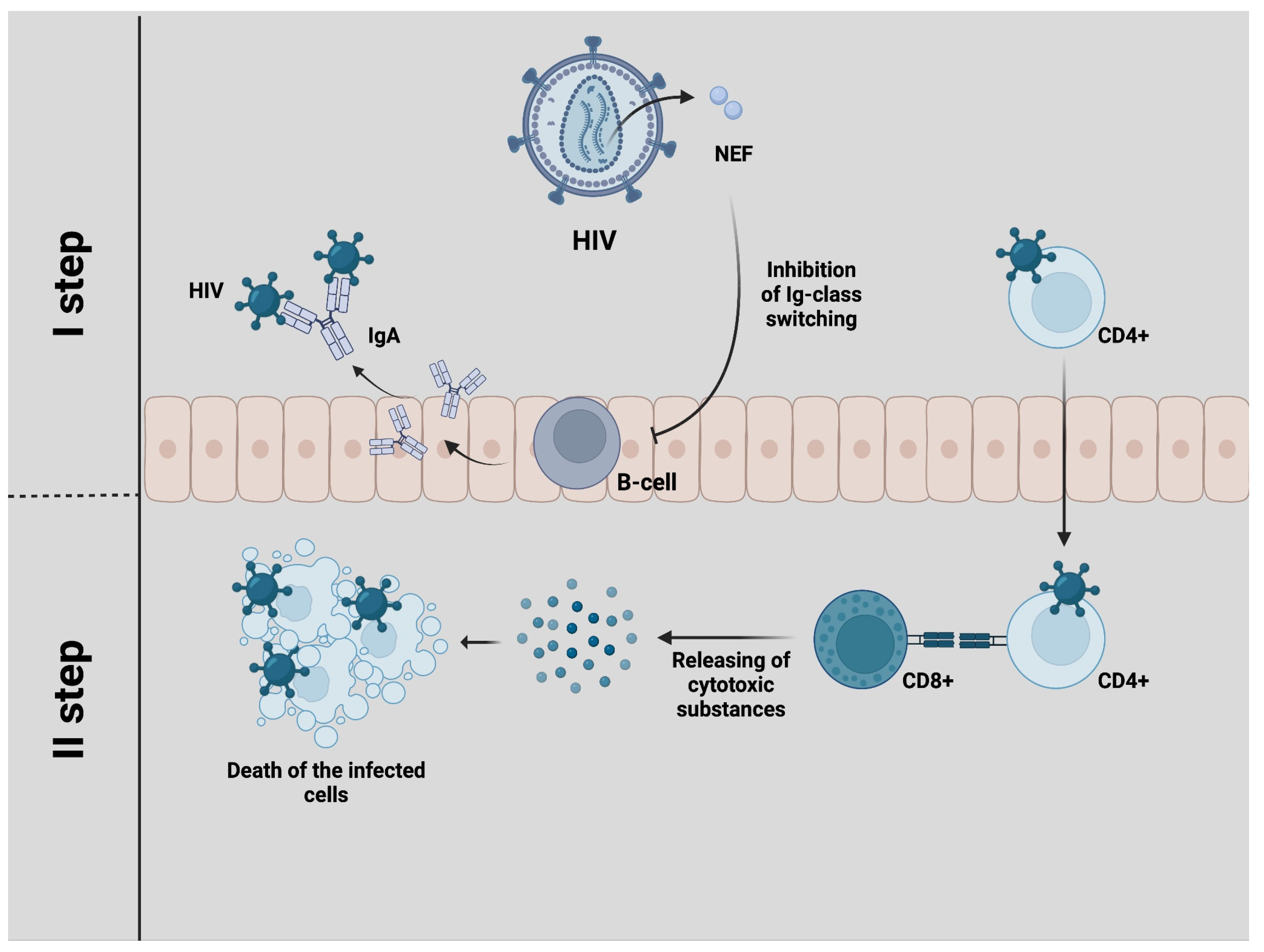

Table 1.
Clinical trials of pre-exposure prophylaxis currently under way.
| Product Name | Delivery method | Product developer | Active ingredients | Hormonal type | Useful links | Registration number |
|---|---|---|---|---|---|---|
| Dapivirine + Levonorgestrel IVR | Intravaginal Ring (IVR) | International Partnership for Microbicides | Dapivirine Levonorgestrel | Hormonal | [49,50] | NCT05041699 |
| MK-8527 | Oral tablet | Merck | MK-8527 new nucleoside reverse transcriptase translocation inhibitor | Non-hormonal | [51] | NCT05494736 NCT06045507 |
| Lenacapavir | Injectables (Subcutaneus) | Gilead | Lenacapavir- capsid inhibitor in combination with other antiretrovirals | Non-hormonal | [48] | NCT04994509 NCT04925752 |
Table 2.
Antiretroviral drugs at the preclinical and early clinical stages and their mechanisms of action.
Table 2.
Antiretroviral drugs at the preclinical and early clinical stages and their mechanisms of action.
| Product developer | Active Ingredients | Hormonal type | Mechanism of Action (Meaning) |
|---|---|---|---|
| Population Council, Oak Crest Institute of Science | Etonogestrel Ethinyl Estradiol QGRFT |
Hormonal | Ovulation inhibition (pregnancy); binding to HIV envelope glycoproteins to prevent entry of HIV into target cells (QGRFT) |
| University of North Carolina, Chapel Hill | Dapivirine Levonorgestrel Pritelivir |
Hormonal | Antiretroviral drug + hormonal contraceptive |
| Auritec Pharmaceuticals | Acyclovir Dolutegravir Etonogestrel Ethinyl Estradiol Rilpivirine |
Hormonal | Antiretroviral drug + hormonal contraceptive |
| University of North Carolina, Chapel Hill | Etonogestrel Ethinyl Estradiol Islatravir (EFdA) |
Hormonal | Antiretroviral drug + hormonal contraceptive |
| MassBiologics Oak Crest Institute of Science Planet Biotechnology, Inc. University of Massachusetts |
Monoclonal Antibodies Tenofovir Disoproxil Fumarate (TDF) |
Non-Contraceptive | mAb 2C7 mediates complement-dependent killing of Neisseria gonorrhoeae. TDF is NRTI targeting HIV infection. |
| Oak Crest Institute of Science, Univ. of North Carolina, Chapel Hill |
Monoclonal Antibodies Tenofovir Disoproxil Fumarate (TDF) |
Non-Hormonal | Nucleoside analogue reverse transcriptase inhibitor (NRTI) and sperm agglutinating antibody |
| MUCCOMMUNE LLC | HCA Monoclonal Antibodies VRC01 + N6 |
Non-Hormonal | viral neutralisation (sustained release of antibodies for non-hormonal contraception and HIV prevention) |
| Population Council | QGRFT Organic acids |
Non-Hormonal | The selected organic acids will lower vaginal pH (pH = 3.5-4.5) in the presence of semen. The low pH inactivates sperm and bacteria. When inserted into the vagina, the FDI dissolves into a viscous gel delivering the active agents throughout the vaginal lumen to prevent sperm penetration. QGRFT is a potent non-antiretroviral (ARV) inhibitor of HIV. QGRFT binds to HIV envelope glycoproteins and prevents entry of HIV into target cells. |
| Magee-Women’s Research Inst. & Fndn., University of Pittsburgh | 4′-Ethynyl-2-fluoro-2′-deoxyadenosine (EFdA) 4′-Ethynyl-2-fluoro-2′-deoxyadenosine prodrug (EFdA-P) Progestin |
Hormonal | Nucleoside reverse transcriptase translocation inhibitor and progestin hormonal contraceptive |
| Magee-Women’s Research Inst. & Fndn., University of Pittsburgh | Dapivirine Levonorgestrel |
Hormonal | Antiretroviral drug + hormonal contraceptive |
| Inst. For Research & Innovation in Health (i3S), University of Porto |
Efavirenz (EFV) Tenofovir (TFV) |
Non-Contraceptive | Short-term (on-demand) protective film that dissolves on contact with vaginal fluids to deliver combination antiviral compounds |
| Research Triangle International (RTI) | Unspecified | Hormonal | nucleoside reverse transcriptase inhibitor; ovulation suppression |
| PATH Queen’s University Belfast |
Norelgestromin ARV candidates under review |
Hormonal | ARV + Progestin |
| CONRAD | Cabotegravir Levonorgestrel |
Hormonal | Integrase strand-transfer inhibitor; progestin |
| University of North Carolina, Chapel Hill | Hormonal Contraceptive Antiretroviral (ARV) |
Hormonal | Antiretroviral drug + hormonal contraceptive |
| Yaso Therapeutics | Polyphenylene Carboxymethylene (PPCM) | Non-Hormonal | PPCM prevents viral binding and fusion to a host cell by attaching to and blocking key viral binding sites. It has been demonstrated that PPCM binds gB on HSV-2 and gp120 on HIV. PPCM has also shown promise against Ebola virus in vitro and gonorrhoea, in vitro and in mice. PPCM renders sperm infertile without damaging other cells. |
Table 3.
Antiretroviral drugs at the preclinical and early clinical stages.
| Product Name | Indications | Clinical Phase | Product Developer | Active ingredients | Hormonal type | Useful links |
|---|---|---|---|---|---|---|
| Intravaginal ring (IVR) | ||||||
| 90-day Pod-type Etonogestrel/Ethinyl Estradiol/QGriffithsin (EEQ) | HIV, Pregnancy | Preclinical – Early (Pre1) | Population Council, Oak Crest Institute of Science | Etonogestrel Ethinyl Estradiol QGRFT |
Hormonal | [61] |
| Dapivirine + Pritelivir + Levonorgestrel 3D Printed IVR | HIV, Pregnancy, HSV-2 | Preclinical – Early (Pre1) | University of North Carolina, Chapel Hill | Dapivirine Levonorgestrel Pritelivir |
Hormonal | [62] |
| Novel Intravaginal Ring as a Non-Hormonal Contraceptive Multipurpose Prevention Technology (MPT) | Bacterial Vaginosis (BV) Chlamydia Gonorrhea HIV HSV-2 Pregnancy |
Pre-formulation, pre-Phase 1, Non-clinical | Population Council Queen’s University Belfast Weill Cornell Medical College |
Copper Zinc Lactide |
Non-Hormonal | [63] |
| Islatravir (EFdA) + Etonogestrel/Ethinyl Estradiol 3D Printed IVR | HIV Pregnancy |
Preclinical – Early (Pre1) | University of North Carolina, Chapel Hill | Etonogestrel Ethinyl Estradiol Islatravir (EFdA) |
Hormonal | [64] |
| IVR. mAb | ||||||
| mAb 2C7 + TDF IVR | HIV, Gonorrhea | Preclinical – Advanced (Pre2) | MassBiologics Oak Crest Institute of Science Planet Biotechnology, Inc. University of Massachusetts |
Monoclonal Antibodies Tenofovir Disoproxil Fumarate (TDF) |
Non-Contraceptive | [65] |
| Novel mAb contraceptive + Tenofovir Disoproxil Fumarate (TDF) IVR | HIV, Pregnancy | Preclinical – Early (Pre1) | Oak Crest Institute of Science, Univ. of North Carolina, Chapel Hill |
Monoclonal Antibodies Tenofovir Disoproxil Fumarate (TDF) |
Non-Hormonal | [66] |
| Human Contraceptive Antibody (HCA) + VRC01 + N6 IVR | HIV, Pregnancy | Preclinical – Advanced (Pre2) | MUCCOMMUNE LLC | HCA Monoclonal Antibodies VRC01 + N6 |
Non-Hormonal | [67] |
| Non-ARV/Non-Hormonal Multi-Purpose Vaginal Ring | HIV HPV HSV-1 HSV-2 Pregnancy |
Pre-formulation | Oak Crest Institute of Science | Unspecified | Non-Hormonal | [68] |
| Fast- dissolving inserts (FDIs) (Vaginal) | ||||||
| Non-hormonal Contraceptive Multipurpose Prevention Technology (MPT) Containing Q-Griffithsin (QGRFT) | Bacterial Vaginosis (BV) Chlamydia Gonorrhea HIV HSV-2 Pregnancy |
Preclinical – Early (Pre1) | Population Council | QGRFT Organic acids |
Non- Hormonal | [69] |
| Griffithsin (GRFT) Fast-Dissolving Insert (FDI) | HIV HPV HSV-1 HSV-2 |
Pre-formulation | Population Council | Unspecified | Non-Contraceptive | [70] |
| Films (Vaginal) | ||||||
| EFdA-P + Progestin Intravaginal Film | HIV, Pregnancy | Early Preclinical | Magee-Women’s Research Inst. & Fndn., University of Pittsburgh | 4′-Ethynyl-2-fluoro-2′-deoxyadenosine (EFdA) 4′-Ethynyl-2-fluoro-2′-deoxyadenosine prodrug (EFdA-P) Progestin |
Hormonal | [71] |
| Dapivirine/Levonorgestrel Extended-Release Monthly Film | HIV, Pregnancy | Early Preclinical | Magee-Women’s Research Inst. & Fndn., University of Pittsburgh | Dapivirine Levonorgestrel |
Hormonal | [72] |
| Tenofovir (TFV)/Efavirenz (EFV) Nanoparticles-in-film | HIV, HSV-1, HSV-2 | Advanced Preclinical | Inst. For Research & Innovation in Health (i3S), University of Porto |
Efavirenz (EFV) Tenofovir (TFV) |
Non-Contraceptive | [73] |
| Implants | ||||||
| Cabotegravir Pellet Implant with Levonorgestrel | HIV, Pregnancy | Early Preclinical | CONRAD | Cabotegravir Levonorgestrel |
Hormonal | [74] |
| Long-acting refillable nanofluidic implant (NanoMPI)- SC | HIV, Pregnancy | Early Preclinical | University of Washington Methodist Hospital Research Institute (HMRI) |
Etonogestrel Islatravir (EFdA) |
Hormonal | [75] |
| Injectables (Subcutaneus) | ||||||
| Cabotegravir/Levonorgestrel Long-Acting MPT Injectable | HIV Pregnancy |
Advanced Preclinical | CONRAD | Cabotegravir Levonorgestrel |
Hormonal | [74] |
| Injectable In-situ Forming Implants | ||||||
| Ultra-Long-Acting MPT In-situ Forming Implant (ISFI) | HIV Pregnancy |
Early Preclinical | University of North Carolina, Chapel Hill | Hormonal Contraceptive Antiretroviral (ARV) |
Hormonal | [76] |
| Gels (Vaginal / Rectal) | ||||||
| Yaso-GEL | HIV, Pregnancy, HSV-2, HPV, Gonorrhea | Advanced Preclinical | Yaso Therapeutics | Polyphenylene Carboxymethylene (PPCM) | Non-Hormonal | [77] |
| Oral Tablet | ||||||
| Dual Prevention Pill (DPP) Regimen | HIV Pregnancy |
Preclinical – Early (Pre1) | Population Council Medicines360 |
Emtricitabine (FTC) Ethinyl Estradiol (EE) Levonorgestrel Tenofovir Alafenamide (TAF) |
Hormonal | [60] |
| Intravaginal Rings (Non-HIV) | ||||||
| Copper Intravaginal Ring (Cu-IVR) | Pregnancy, HSV-2, Zika virus | Early Preclinical | University of California, Davis | Copper | Non-Hormonal | [78] |
Table 4.
The chemical structure of microbicides.
 |
 |
| Nonoxynol-9 (C33H60O10) | C31G (C30H64N2O3) |
 |
 |
| Sodium lauryl sulfate (C12H25SO4Na) | Carbopol 974P ( [C3H4O2]n) |
 |
 |
| Ϳ-Carrageenans ([C12H16O15S2 2-]n) | Naftalane sulfonate polymers ([C11H9NaSO4]n) |
 |
 |
| Dapivirine (C20H19N5) | Tenofovir (C9H14N5O4P) |
 |
 |
| Levonorgestrel (C21H28O2) | Tenofovir alafenamide (C21H29N6O5P) |
 |
 |
| Elvitegravir (C23H23ClFNO5) | Emtricibatine (C8H10FN3O3S) |
 |
 |
| Tenofovir disoproxil fumarate (C23H34N5O14P) | Cabotegravir (C19H17F2N3O5) |
 | |
| Islatravir (C12H12FN5O3) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



