
Submitted:
17 May 2024
Posted:
17 May 2024
You are already at the latest version
Abstract
There is evidence that the tendency to adopt a particular pattern of causal inference, known as attributional style, is likely to be associated with specific pattern of psychopathology among youth. This study aims to assess preliminary psychometric properties of the Italian Children’s Attributional Style Questionnaire-Revised (CASQ-R) and to explore the presence of any subgroups of children and early adolescents from the general population who might exhibit internally homogeneous and externally heterogeneous attributional styles, through cluster analyses, delving also potential sociodemographic and clinical differences among the identified clusters of attributional styles. A sample of 337 children was recruited and their attributional styles and depressive symptoms were analyzed. Four distinct clusters emerged using the six CASQ-R subscales in a multivariate finite mixture model. In particular, high levels of depressive symptoms were reported by children showing high scores in all the negative attributional subscales (globality, internality and stability) and medium scores in all the positive attributional subscales. Conversely, low levels of depressive symptoms were reported by children showing medium-to-high scores in the positive attributional subscales and low-to-medium scores in the negative attributional subscales. The identified clusters shed light on distinct patterns associated with depressive symptoms, offering potential insights for targeted interventions.
Keywords:
attributional styles
; depressive symptoms
; children and early adolescents
; Children’s Attributional Style Questionnaire-Revised
; cluster analysis
1. Introduction
The tendency to adopt a particular pattern of causal inferences has been referred to as one’s attributional style or explanatory style [1]. Attributional style is conceptualised along three dimensions: internal–external, global–specific, and stable–unstable [2]. The internal–external dimension refers to whether the explanation for an event is grounded in the physical, behavioural, or cognitive characteristics of the self (i.e., internal) or arises as a consequence of someone or something outside the self (i.e., external). The stable–unstable dimension refers to whether the explanation for an event has enduring (i.e., stable) or ephemeral effects (i.e., unstable). Lastly, the global–specific dimension refers to whether the event is viewed as having ubiquitous effects and generalised to much of the individual’s life (i.e., global) or has more limited effects and influences only particular facets of the individual’s life (i.e., specific).
Considerable evidence underscores the importance of attributional style in human functioning and wellbeing. Research conducted in adult populations demonstrated a significant association between attributional style and health outcomes [3], occupational outcomes [4], athletic performance [5], and many other relevant measures of functioning [6]. Notably, these findings extend to adolescents. For instance, Dweck and colleagues have persuasively argued that the attributions made by youth after academic and social task failures constitute a critical determinant of their subsequent responses to those tasks [7,8]. That is, how youth explain or attribute these events serves as a predictive factor for their future explanations or attributions of similar occurrences. Along the same lines, research conducted on children identified a connection between attributional style and both social and academic performance [9,10,11,12,13]. Moreover, children attributing their social failures to internal and stable factors (i.e., a lack of ability) are more likely to withdraw from social interactions and are less liked by peers [14].
In a psychopathological framework, internal, stable, and global attributions for the causes of negative events have demonstrated significant implications for depressive symptomatology in children and adolescents [15,16,17,18]. Moreover, existing literature suggests that children with anxiety disorders tend to exhibit higher negative attributions (internal, global, stable) for adverse events compared to normal controls (for a review see [19,20,21]). A perceived lack of control over life events is described as a key risk factor for both anxiety and depression, directly related to hopeless attributional style (i.e., attributional style characterised by a sense of uncontrollability, uncertainty, and unpredictability regarding future occurrences of events).
If the association between attributional style and internalizing symptoms has been ascertained by several meta-analyses [22,23], the direction of this link is still to be clarified. Most of the existing longitudinal studies considered attributional style as the predictor, but this does not exclude the possibility that internalizing symptoms predict a specific attributional style. In support of this claim, an experimental study conducted by Lo and colleagues [24] showed that depressive symptoms were able to predict negative attributional style among college students. More recently, another study demonstrated that, after controlling for depressive symptoms, positive attributions for good events were predicted by low levels of social anxiety in 337 Italian children [25].
Another possibility, that has not been tested yet, is that a bidirectional link exists between attributional style and internalizing symptoms.
Finally, it is possible that attributional style acts as a mediator between specific individual features and internalizing symptoms. Support to this latter possibility comes from a recent study conducted by Luo and Wu [26], who showed that a depressogenic attributional style significantly mediated the relationship between self-discrepancies and anxiety.
Overall, beyond the nature and the direction of the link between attributional style and adaptive/maladaptive functioning, early identification of dysfunctional attributional style seems to be particularly important, as potentially lifelong consequences can be prevented or mitigated through timely interventions.
The main measure of attributional style in children is the Children’s Attributional Style Questionnaire [2] (CASQ), which aligns with the reformulation of the learned helplessness model of depression in children [27], and is constituted by 48 items. Several studies have consistently demonstrated that children making more internal-stable-global attributions for negative events and more external-unstable-specific attributions for positive events, as measured by CASQ, tend to report higher levels of depressive symptoms compared to their peers with the reverse attributional style [28].
In the last years, a revised version of the CASQ has been developed, constituted by 24 items. The fact that children have a limited attention span, and that the CASQ is often used in larger test batteries, have led to the development of a shortened version [29]. The 24 items of the CASQ revised [30] (CASQ-R) were selected based on psychometric analyses (i.e., positive corrected item-total correlations and internal consistency reliability) conducted on the answers of 449 elementary school children who completed the original CASQ [31,32]. The psychometric properties of CASQ-R were examined on 1,086 children aged 9 to 12 years old, with equal representation of boys and girls, and of African American and Caucasian children. Approximately one half (n = 475) of the youths also completed the CASQ-R six months later. Results revealed that although the CASQ-R was somewhat less reliable than the original CASQ, with moderate internal consistency reliability and fair test-retest reliability, it demonstrated equivalent criterion-related validity with self-reported depressive symptoms. A following study [33] using a sample of 621 adolescents (184 males and 437 females), aged 11–18 years, indicated an adequate model fit for a one-factor solution for negative event items and a two-factor solution for positive event items. Reliability estimates for these factors were low but acceptable in the former, and lower than recommended guidelines in the latter.
Nonetheless, to date, the CASQ-R is the most widely used measure of youth attributions. Since the CASQ-R has never been studied in Italian children, this study aims at assessing preliminary psychometric properties of the Italian CASQ-R, to determine whether this shortened scale is a reliable and valid substitute for the original CASQ with Italian-speaking children. Furthermore, to delve deeper into the investigation of attributional styles within the general population of Italian-speaking children, we conducted a clustering analysis using the CASQ-R scores. This approach allowed us to explore the presence of any subgroups of children who might exhibit internally homogeneous and externally heterogeneous attributional styles. Finally, we tested the mean differences in the target sociodemographic and clinical variables across the identified clusters.
2. Method
2.1. Participants
A sample of 368 children and early adolescents attending primary and middle schools located in three medium-to-big cities in Northern Italy was recruited for this research project. After receiving a complete description of the study, 89% of parents and children/early adolescents agreed to participate through a signed informed consent, this leading to an effective study sample of 337 subjects. Children and early adolescents affected by severe neurological/psychiatric disorders were excluded from the study.
2.2. Procedure
The current research used pre-existing data gathered through a project focused on exploring the connection between sociocognitive understanding and depressive symptoms.
The participants filled in self-reports questionnaires and performed verbal ability and sociocognitive understanding tasks in class during school time in one 50-minute collective session.
2.3. Measures
Attributional style. The Children’s Attributional Style Questionnaire-Revised [29] (CASQ-R) consists of 24 double-choice items that address both positive (12 items) and negative (12 items) outcomes. Among the 12 positive events, 2 items focus on the internal-external dimension, 7 items evaluate the stable-unstable dimension, and 3 items pertain to the global-specific dimension. Similarly, for the 12 negative events, 3 items address the internal-external dimension, 6 items assess the stable-unstable dimension, and 3 items pertain to the global-specific dimension. Positive, negative, and overall (positive composite minus negative composite) scores can be derived. A lower positive composite score, along with a higher negative composite score, and a lower overall composite score indicate a more depressive attributional style. The child’s endorsed causal attributions are scored in a manner akin to the approach employed in the original CASQ.
Depressive symptoms. Depressive symptoms were measured through the Child Depression Inventory [34,35] (CDI). The CDI comprises 27 items, each containing three self-report statements rated on a severity scale from 0 to 2, where 2 indicates a severe manifestation of a depressive symptom, and 0 signifies the absence of that symptom. The child is directed to fill out the CDI based on their emotions over the past two weeks. The overall score ranges from 0 to 54. In the current study, the internal consistency of the CDI was found to be satisfactory (Cronbach’s α = .82).
2.4. Data Analyses
Statistical analyses were carried out using SPSS 27[36], and R version 4.2.2 statistical software [37] with the additional “mclust” version 5 package for mixture modelling [38]. An alpha level of 0.05 (two-tailed) was adopted as the criterion for statistical significance.
2.4.1. Descriptive Statistics
Firstly, the descriptive statistics and frequency analyses of gender, age, and class attendance were performed for all participants to delineate the main characteristics of the children involved in the study. The mean values of the CASQ-R subscales were as follows: CASQ-R positive = 7.35 (± 1.92), CASQ-R negative = 4.12 (± 1.91), and CASQ-R total = 3.23 (± 2.98), whereas the mean value of the CDI total score was 10.84 (± 6.27).
2.4.2. Between-Group Comparisons
Between-group comparisons were run to exclude the potential influence of confounding variables, like age and gender, on depressive symptoms and attributional styles. In particular, age cohorts were arbitrarily created splitting the entire sample in two using 12 years old as age cut-off, so that children aged below 11 years old were named younger children, whereas those aged above 12 years old were named older children.
2.4.3. Psychometric Properties of CASQ-R
Psychometric properties of the CASQ-R, namely internal consistency through Kuder-Richardson reliability coefficient (KR20) and criterion-related validity through the comparison with CDI scores, were carried out in accordance with Thompson and colleagues[29].
2.4.4. Clusters Estimation
Afterward, a cluster analysis (i.e., an unsupervised machine learning model), was performed to identify potential subgroups of participants sharing common characteristics, considering the six CASQ-R subscales (i.e., Negative Globality, Negative Internality, Negative Stability, Positive Globality, Positive Internality, and Positive Stability). Finite mixture models (FMM) estimating solutions of two or more clusters were compared using the Bayesian information criterion (BIC), with the best model having a BIC value closer to 0 [38]. Each subject was then assigned to their highest probability cluster. Each cluster characteristics were analysed by estimating its parameters (subgroup mean and standard deviation) for the CASQ-R scores.
2.4.5. Clusters Characteristics
Non-parametric between-clusters comparisons were carried out, considering, respectively, the six CASQ-R subscales, age, and depressive symptoms as dependent variables. Lastly, a Pearson’s chi-squared test was performed considering cluster membership and gender, for testing any associations between the two variables.
3. Results
3.1. Descriptive Statistics
The sample is composed of 337 children (11.29 ± 1.76 years old, 169 females and 168 males) attending the third (N = 87) and fifth (N = 73) year of primary school, and the second year (N = 177) of middle school.
3.2. Between-Group Comparisons
T-test for independent samples revealed that no gender differences exist in the assessed sample with regard to positive attributional style (t(323) = 1.35, p = .09, d = 1.92), negative attributional style (t(323) = .517, p = .30, d = 1.91), and overall attributional style (t(323) = .534, p = .29, d = 2.99), whereas significant gender differences emerged on depressive symptomatology (t(335) = -2.33, p = .01, d = 6.24) with higher depressive symptoms displayed by females (11.63 ± 6.22) compared to males (10.04 ± 6.25).
Similarly, t-test for independent samples among the younger (˂11 years old) and older (˃12 years old) cohort revealed no age differences regarding all the study variables (positive attributional style: t(309) = .126, p = .450, d = 1.90; negative attributional style: t(309) = .277, p = .39, d = 1.92; overall attributional style; t(309) = -.098, p = .461, d = 2.97; and depressive symptomatology: t(321) = 1.27, p = .10, d = 6.32).
3.3. Psychometric Properties of CASQ-R
Internal consistency of CASQ-R. The internal consistency of CASQ-R was calculated on a sample of 325 subjects using the Kuder-Richardson reliability coefficient (KR20), which is the statistical equivalent of Cronbach’s Alpha in case of dichotomous items (usually scored as 0 or 1), for the positive (α = .370) and negative (α = .352) composite scores, as well as for the single CASQ-R subscales, namely positive internality (α = .200), positive stability (α = .207), positive globality (α = .173), negative internality (α = .260), negative stability (α = .272), and negative globality (α = .099).
Criterion-related validity of the CASQ-R. Pearson’s bivariate correlations run on the entire sample outlined that CASQ-R positive (r = -.328, p < .001), negative (r =.249, p < .001), and overall (r = -.371, p < .001) composite scores correlated significantly and in the predicted directions with children’s score on CDI. Specifically, lower scores on the positive (i.e., a more depressive attributional style for positive events) and overall (i.e., more internal-stable-global attributions for negative events and more external-unstable-specific attributions for positive events) composite scores were associated with higher levels of depressive symptoms in children; whereas higher scores on the negative composite score (i.e., a depressive attributional style for negative events) were related to heightened self-reported symptoms of depression. Criterion-related validity of CASQ-R was also performed separately by gender and age categories and, as Table 1 and Table 2 show, the same correlational patterns emerged with no differences noted among males and females, as well as among younger and older children.
Cluster estimation. The six CASQ-R subscales (i.e., Negative Globality, Negative Internality, Negative Stability, Positive Globality, Positive Internality, and Positive Stability) were considered jointly in a multivariate FMM. The BIC value (-5284.253) suggested the presence of four clusters with diagonal distribution, variable volume, and equal shape. The clusters’ estimated results are summarized in Figure 1 and Table 3.
Cluster characteristics. Non-parametric between-clusters comparisons outlined that the six CASQ-R subscales were significantly different among the four clusters. Results are shown in Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7.
The first cluster is characterized by low levels of positive globality, positive internality, and positive stability attributional style, medium levels of negative globality attributional style, and high levels of negative internality attributional style.
The second cluster is characterized by low levels of negative globality attributional style and medium levels of negative internality, negative stability, positive globality, positive internality, and positive stability attributional style.
The third cluster is characterized by medium levels of positive globality, positive internality, and positive stability attributional style, and high levels of negative globality, negative internality and negative stability attributional style.
The fourth cluster is characterized by low levels of negative internality and negative stability attributional style, medium levels of negative globality attributional style, and high levels of positive globality, positive internality, and positive stability attributional style.
Likewise, between-clusters comparisons highlighted that depressive symptoms are significantly different among the four clusters. Specifically, low levels of depressive symptoms were encountered in the second and fourth clusters, medium levels of depressive symptoms in the first cluster and high levels in the third cluster (See Figure 8).
Lastly, no significant between-cluster differences emerged considering age and gender.
4. Discussion
The present research aimed at evaluating the psychometric properties of the Italian CASQ-R and at exploring the presence of any subgroups of children and early adolescents of the general population who might exhibit internally homogeneous and externally heterogeneous attributional styles. Moreover, we aimed at investigating potential sociodemographic and clinical differences among the identified clusters of attributional styles.
Overall, the internal consistency of the CASQ-R composite scores was very low in the present study. Nonetheless, existing literature concerning both CASQ and CASQ-R (both original version and translations) most of times reported mediocre values [29,33,39,40,41,42,43,44].
Criterion-related validity of the CASQ-R yielded good results, in that positive/negative/overall composite scores of the CASQ-R significantly correlated with depressive symptoms scores in a coherent fashion (i.e., depressive symptoms were positively associated with negative CASQ-R and negatively associated with positive/overall CASQ-R). This result is in line with past literature [2,29] and further extends the significant link between attributional style and depressive symptoms to Italian children of the general populations.
Moreover, in this study, neither age nor gender differences emerged for CASQ-R composite scores, coherently with the results obtained in previous studies conducted on subjects of a similar age [29]. Nonetheless, we believe that gender should still be investigated in future research, as it could be an important factor especially when considering attributions interacting with depressive symptoms and/or anxiety [45,46,47,48,49,50,51]. Similarly, age is to be taken into account when the comparison is between very different age groups, since people become increasingly selective in engaging cognitive resources and they can develop expert social knowledge across time [52,53].
The overall low internal consistency found in the present research warranted further statistical analyses based on clustering. Specifically, four distinct clusters emerged using the six CASQ-R subscales in a multivariate finite mixture model. Such clusters presented peculiar levels of positive/negative, internal/external, stable/unstable attributions. More interestingly, the four clusters revealed different associations with depressive symptoms scores, so that high levels of depressive symptoms were reported by children showing high scores in all the negative attributional subscales (globality, internality and stability) and medium scores in all the positive attributional subscales. Conversely, low levels of depressive symptoms were reported by children showing medium-to-high scores in the positive attributional subscales and low-to-medium scores in the negative attributional subscales. Our results are not directly comparable with those of other research, as no previous study used cluster analysis to look at attributional styles. Nonetheless, the features of the distinct clusters are definitely in line with the large amount of literature that has accumulated on the attributional styles that typically characterize depressed subjects [22,23,54,55]. Notably, neither gender nor age differences were found comparing the four clusters emerged in our study.
Overall, the interesting groupings of subjects that emerged in our study could guide interventions aimed at reducing depressive symptoms starting from the school context by acting on attributional styles in children and adolescents. Such interventions could build on Dweck’s work conducted within the framework of the cognitive theories of depression, which focuses on the cognitive restructuring of attributions[56]. More recently, children's beliefs/mindsets about the stability of self-concepts such as intelligence and personality received growing attention. Therefore, promising interventions could also target children’s mindset, with potential beneficial effects on wellbeing [57,58].
Despite our study offers valuable insights, it is essential to acknowledge certain limitations. First, the generalizability of our findings to a broader population may be constrained due to the regional focus on Northern Italy. Secondly, the cross-sectional design of our study limits our ability to establish causation, and future research employing longitudinal approaches could provide a more nuanced understanding of the phenomenon. Specifically, research should better address the independent and interactive relationships among attributional styles, life events, coping and depressive symptomatology [59,60].
In summary, our study investigated attributional styles and depressive symptoms in a sample of Italian children using the CASQ-R; our findings contribute to the understanding of attributional styles in the Italian context. The identified clusters shed light on distinct patterns associated with depressive symptoms, offering potential insights for targeted interventions. Future research should employ longitudinal designs, diverse measurement methods, and broader participant inclusion to strengthen causal inferences and enhance generalizability. Additionally, evaluating the effectiveness of interventions targeting attributional styles could further inform preventive strategies for depressive symptoms in children.
Author Contributions
S.S. and M.C. conceptualized the work and laid out the manuscript's structural framework. S.S. wrote the introduction. S.G., L.G. and S.D.F. carried out the statistical analyses and wrote the method and results’ sections of the manuscript. M.C. contributed to the critical discussion of the main findings. B.F. carefully revised the entire manuscript providing crucial insights for the article's conclusions. All authors approved the final version of the manuscript.
Funding
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
the authors would like to thank Prof. Nadine Kaslow of the Emory University for having granted us permission to translate the original version of the scale she devised and for allowing us to validate it on an Italian sample; and Prof. Anna Ogliari of the Vita Salute San Raffaele University of Milan for having facilitated an initial contact with the author of the scale. Finally, the authors would like to thank all the children and their families for their valuable participation, which enabled the completion of this study.
Conflicts of Interest
All authors declared that there are no conflicts of interest.
References
- 1. Buchanan GM, Seligman MEP. Explanatory style. 1995.
- 2. Seligman MEP, Kaslow NJ, Alloy LB, Peterson C, Tanenbaum RL, Abramson LY. Attributional style and depressive symptoms among children. Journal of Abnormal Psychology. [CrossRef]
- 3. Rasmussen HN, Scheier MF, Greenhouse JB. Optimism and physical health: A meta-analytic review. Annals of Behavioral Medicine. [CrossRef]
- 4. Mark G, Smith, AP. Effects of occupational stress, job characteristics, coping, and attributional style on the mental health and job satisfaction of university employees. Anxiety, Stress & Coping. [CrossRef]
- Gordon, RA. Attributional style and athletic performance: Strategic optimism and defensive pessimism. Psychology of Sport and Exercise. [CrossRef]
- 6. Cheng H, Furnham A. Attributional style and personality as predictors of happiness and mental health. Journal of Happiness Studies. [CrossRef]
- 7. Dweck CS, Chiu CY, Hong YY. Implicit theories and their role in judgments and reactions: A word from two perspectives. Psychological Inquiry. [CrossRef]
- 8. Dweck CS, Leggett EL. A social-cognitive approach to motivation and personality. Psychological Review. [CrossRef]
- 9. Anderman EM, Anderman LH, Griesinger T. The relation of present and possible academic selves during early adolescence to grade point average and achievement goals. The Elementary School Journal.
- 10. Bickett LR, Milich R, Brown RT. Attributional styles of aggressive boys and their mothers. Journal of Abnormal Child Psychology. [CrossRef]
- Houston, DM. Revisiting the relationship between attributional style and academic performance. Journal of Applied Social Psychology. [CrossRef]
- 12. McQuade JD, Hoza B, Murray-Close D, Waschbusch DA, Owens JS. Changes in self-perceptions in children with ADHD: A longitudinal study of depressive symptoms and attributional style. Behavior Therapy. [CrossRef]
- 13. Rodríguez-Naranjo C, Cano A. Development and validation of an attributional style questionnaire for adolescents. Psychological Assessment. [CrossRef]
- 14. Erdley CA, Loomis CC, Cain KM, Dumas-Hines F. Relations among children's social goals, implicit personality theories, and responses to social failure. Developmental Psychology. [CrossRef]
- 15. Abela JR, Sarin S. Cognitive vulnerability to hopelessness depression: A chain is only as strong as its weakest link. Cognitive Therapy and Research. [CrossRef]
- Muris, P. , Schmidt, H., Lambrichs, R., & Meesters, C. (2001). Protective and vulnerability factors of depression in normal adolescents. ( 39(5), 555–565. [CrossRef] [PubMed]
- Nolen-Hoeksema S, Morrow J, Fredrickson BL. Response styles and the duration of episodes of depressed mood. Journal of Abnormal Psychology 1993; 102(1): 20-28. [CrossRef]
- 18. Voelz ZR, Haeffel GJ, Joiner JTE, Wagner KD. Reducing hopelessness: the interation of enhancing and depressogenic attributional styles for positive and negative life events among youth psychiatric inpatients. Behaviour Research and Therapy, 1183. [CrossRef]
- 19. Bell-Dolan D, Wessler AE. Attributional style of anxious children: Extensions from cognitive theory and research on adult anxiety. Journal of Anxiety Disorders. [CrossRef]
- 20. Schleider JL, Vélez CE, Krause ED, Gillham J. Perceived psychological control and anxiety in early adolescents: The mediating role of attributional style. Cognitive Therapy and Research. [CrossRef]
- 21. Caffo E, Forresi B, Strik Lievers L. Impact, psychological sequelae and management of trauma affecting children and adolescents. Current Opinion in Psychiatry. [CrossRef]
- 22. Joiner JTE, Wagner KD. Attributional style and depression in children and adolescents: A meta-analytic review. Clinical Psychology Review. [CrossRef]
- 23. Sweeney PD, Anderson K, Bailey S. Attributional style in depression: a meta-analytic review. Journal of Personality and Social Psychology. [CrossRef]
- 24. Lo CS, Ho SM, Hollon SD. The effects of rumination and depressive symptoms on the prediction of negative attributional style among college students. Cognitive Therapy and Research. [CrossRef]
- 25. Scaini S, Caputi M, Ogliari A, Oppo A. The relationship among attributional style, mentalization, and five anxiety phenotypes in school-age children. Journal of Research in Childhood Education. [CrossRef]
- 26. Luo Y, Wu Y. The Relationship Between Self/Value Discrepancies and Anxiety: The Mediation Effect of Depressogenic Attributional Style. Journal of Rational-Emotive & Cognitive-Behavior Therapy. [CrossRef]
- 27. Abramson LY, Seligman ME, Teasdale JD. Learned helplessness in humans: critique and reformulation. Journal of Abnormal Psychology. [CrossRef]
- 28. Gladstone TR, Kaslow NJ. Depression and attributions in children and adolescents: A meta-analytic review. Journal of Abnormal Child Psychology. [CrossRef]
- Thompson M, Kaslow NJ, Weiss B, Nolen-Hoeksema S. Children's Attributional Style Questionnaire—Revised: Psychometric examination. Psychological Assessment 1998; 10(2): 166-170. [CrossRef]
- 30. Kaslow NJ, Nolen-Hoeksema S. Children’s Attributional Style Questionnaire—Revised. 1991.
- 31. Nolen-Hoeksema S, Girgus JS, Seligman ME. Learned helplessness in children: a longitudinal study of depression, achievement, and explanatory style. Journal of Personality and Social Psychology. [CrossRef]
- Nolen-Hoeksema S, Girgus JS, Seligman ME. Predictors and consequences of childhood depressive symptoms: a 5-year longitudinal study. Journal of Abnormal Psychology 1992; 101(3): 405-422. [CrossRef]
- 33. Lewis SP, Waschbusch DA, Sellers DP, Leblanc M, Kelley ML. Factor structure of the Children’s Attributional Style Questionnaire–Revised. Canadian Journal of Behavioural Science/Revue, 1: sciences du comportement 2014; 46(2), 2014. [CrossRef]
- Kovacs, M. Children’s depression inventory. Toronto Ontario; 1985.
- 35. Camuffo M, Cerutti R, Lucarelli L, Mayer R. Children’s Depression Inventory, 1988.
- IBM Corp. IBM SPSS Statistics for Windows (Version 27.0) [Computer software]. IBM Corp; 2020.
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; 2022. URL https://www.R-project.org/.
- 38. Scrucca L, Fop M, Murphy TB, Raftery AE. mclust 5: clustering, classification and density estimation using Gaussian finite mixture models. The R Journal.
- 39. Ciarrochi J, Heaven PCL, Davies F. The impact of hope, self-esteem, and attributional style on adolescents’ school grades and emotional well-being: A longitudinal study. Journal of Research in Personality, 1178. [CrossRef]
- Cunningham, EG. Psychometric properties of the children’s attributional style questionnaire. Psychological Reports. [CrossRef]
- 41. Roberts CM, Kane R, Bishop B, Cross D, Fenton J, Hart B. The prevention of anxiety and depression in children from disadvantaged schools. Behaviour Research and Therapy. [CrossRef]
- 42. Salama-Younes M, Zadeh HM, Cunningham E. A Preliminary Validation of a French Version of the Children’s Attributional Style Questionnaire. International Journal of Psychology.
- 43. Sheikh HI, Hayden EP, Singh SM, Dougherty LR, Olino TM, Durbin C, … Klein DN. An examination of the association between the 5-HTT promoter region polymorphism and depressogenic attributional styles in childhood. Personality and Individual Differences. [CrossRef]
- 44. Waschbusch DA, Sellers DP, LeBlanc MM, Kelley ML. Helpless attributions and depression in adolescents: The roles of anxiety, event valence, and demographics. Journal of Adolescence. [CrossRef]
- Bar-Tal, D. Attribution analysis of achievement-related behaviour. Review of Educational Research. [CrossRef]
- Beyer, S. Gender differences in causal attributions by college students of performance on course examinations. Current Psychology. [CrossRef]
- 47. Dweck CS, Goetz TE, Strauss NL. Sex differences in learned helplessness: IV. An experimental and naturalistic study of failure generalization and its mediators. Journal of Personality and Social Psychology. [CrossRef]
- 48. Dweck CS, Mangels JA, Good C. Do high-achieving female students underperform in private? The implications of threatening environments on intellectual Processing. Journal of Educational Psychology. [CrossRef]
- 49. Nelson LJ, Cooper J. Gender differences in children’s reactions to success and failure with computers. Computers in Human Behavior. [CrossRef]
- Nolen-Hoeksema S, Girgus JS, Seligman MEP. Sex differences in depression and Explanatory style in children. Journal of Youth and Adolescence 1991; 20: 233-245. [CrossRef]
- 51. Yeo LS, Tan K. Attributional style and self-efficacy in Singaporean adolescents. Journal of Psychologists and Counsellors in Schools. [CrossRef]
- Blanchard-Fields, F. Causal attributions across the adult life span: The influence of social schemas, life context, and domain specificity. Applied Cognitive Psychology. [CrossRef]
- Hess, TM. Adaptive aspects of social cognitive functioning in adulthood: age–related goal and knowledge influences. Social Cognition. [CrossRef]
- 54. Abramson LY, Metalsky GI, Alloy LB. Hopelessness depression: A theory-based subtype of depression. Psychological Review. [CrossRef]
- 55. Wang J, Wang X, McWhinnie CM, Xiao, J. Depressogenic Attributional Style and Depressive Symptoms in Chinese University Students: The Role of Rumination and Distraction. Journal of Rational-Emotive & Cognitive-Behavior Therapy. [CrossRef]
- Dweck, CS. Motivational processes affecting learning. American Psychologist, 1040. [Google Scholar] [CrossRef]
- 57. Alatorre AI, DePaola RV, Haeffel GJ. Academic achievement and depressive symptoms: Are fixed mindsets distinct from negative attributional style? Learning and Individual Differences. [CrossRef]
- 58. Jiang X, Mueller CE, Paley N. A Systematic Review of Growth Mindset Interventions Targeting Youth Social–Emotional Outcomes. School Psychology Review. [CrossRef]
- 59. Bruder-Mattson SF, Hovanitz CA. Coping and attributional styles as predictors of depression. Journal of Clinical Psychology. [CrossRef]
- 60. Rueger SY, George R. Indirect effects of attributional style for positive events on depressive symptoms through self-esteem during early adolescence. Journal of Youth and Adolescence. [CrossRef]
Figure 1.
Clustering results on the CASQ-R subscales.

Figure 2.
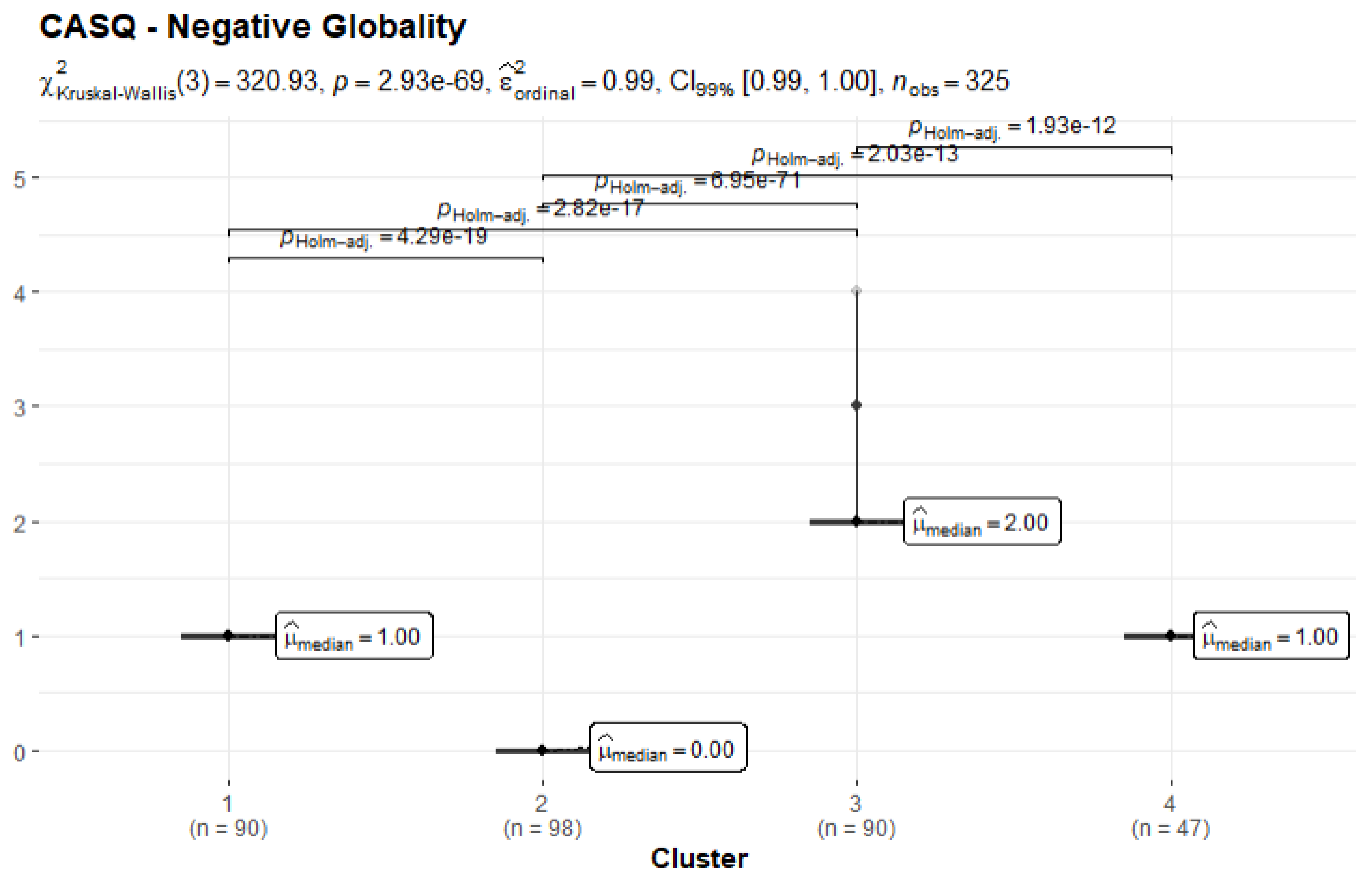
Figure 3.
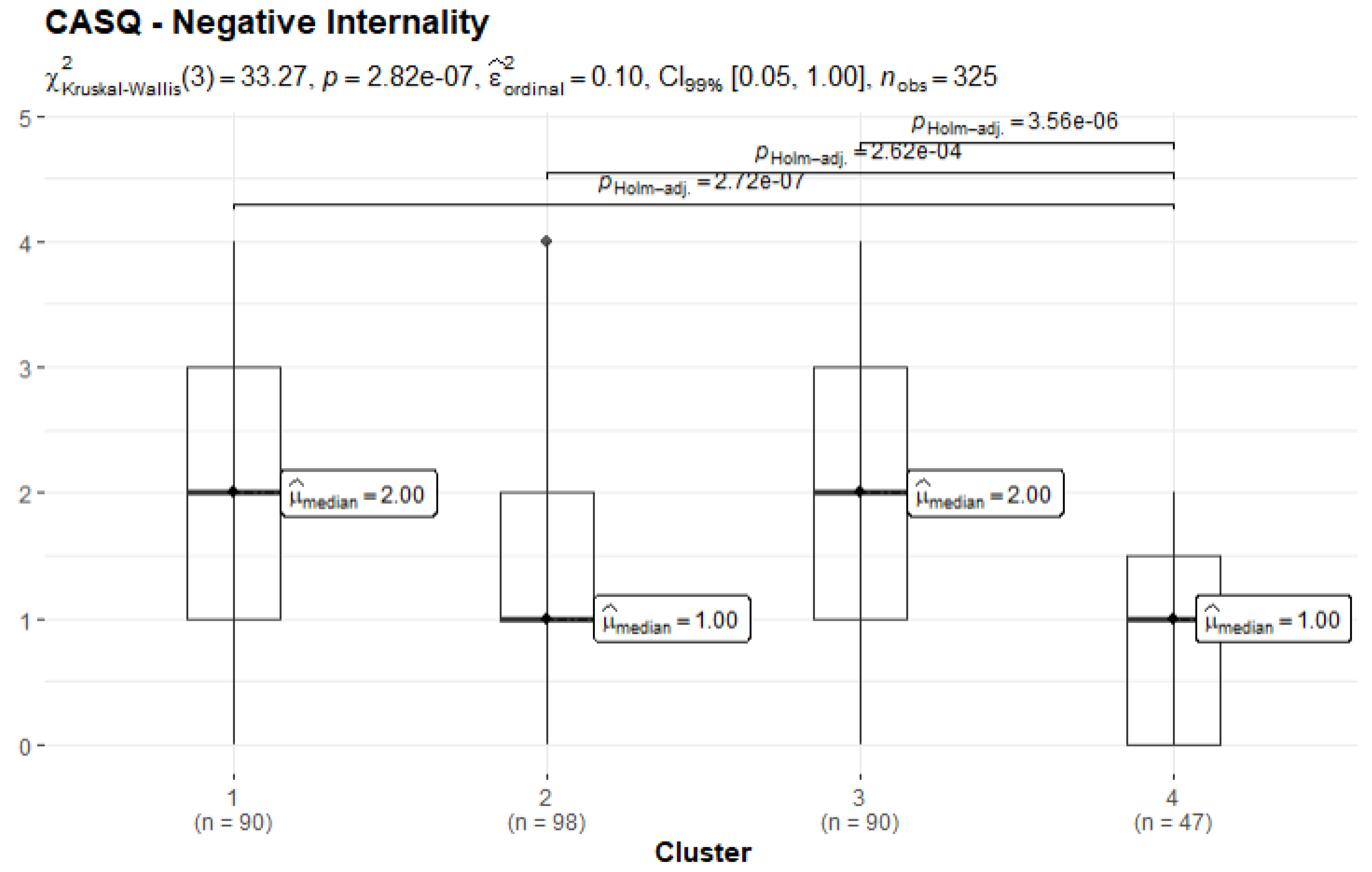
Figure 4.
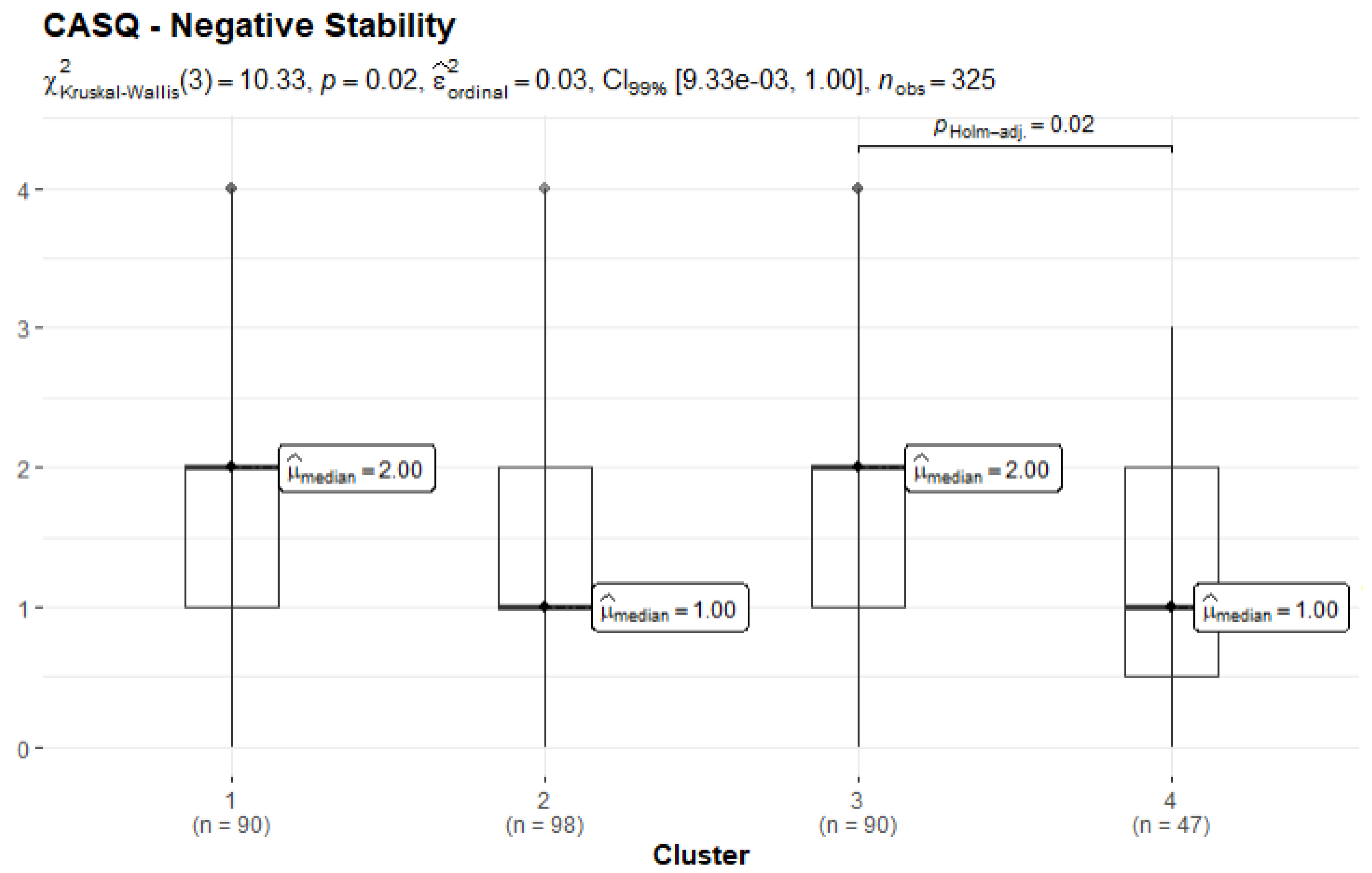
Figure 5.
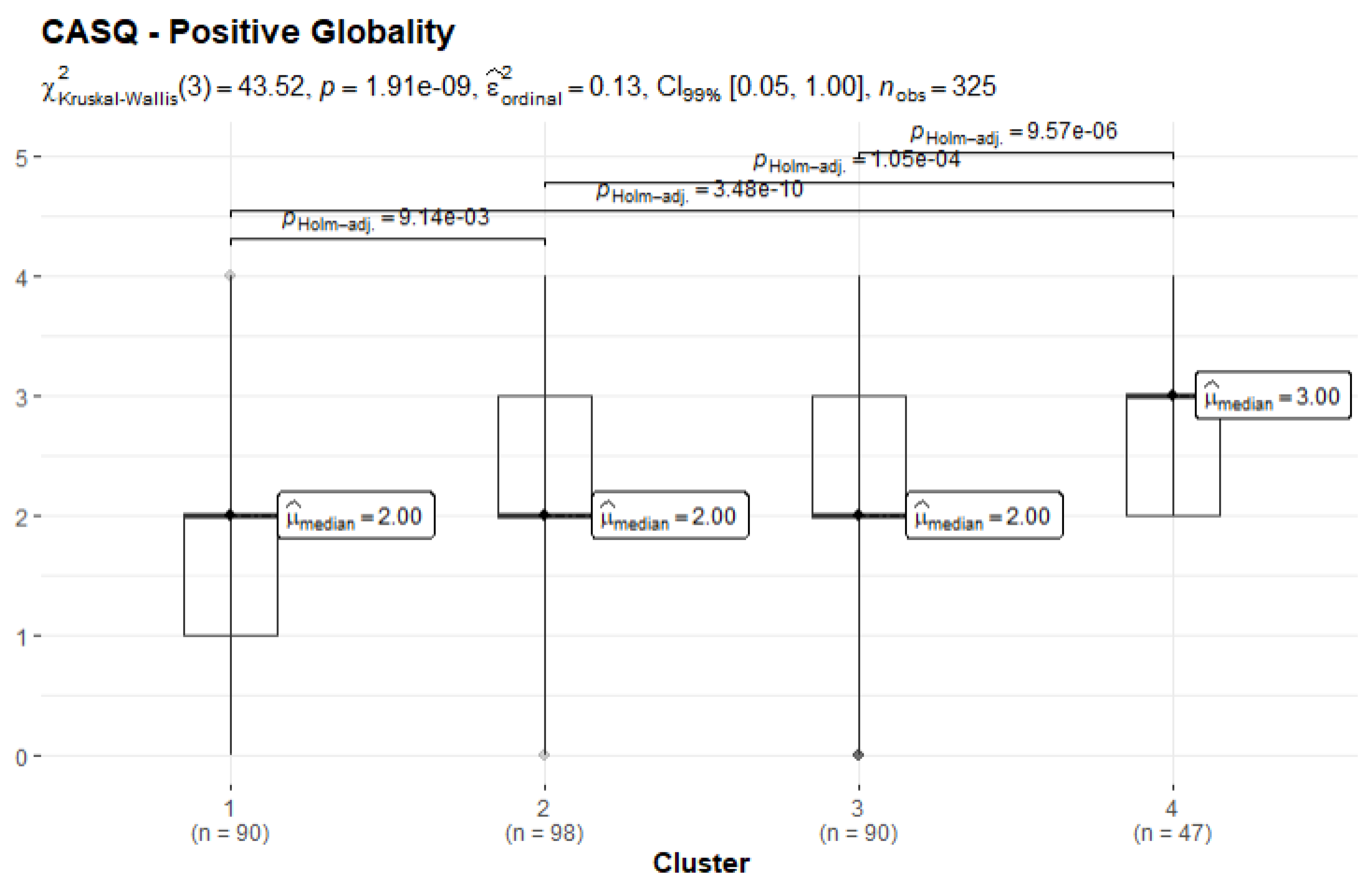
Figure 6.
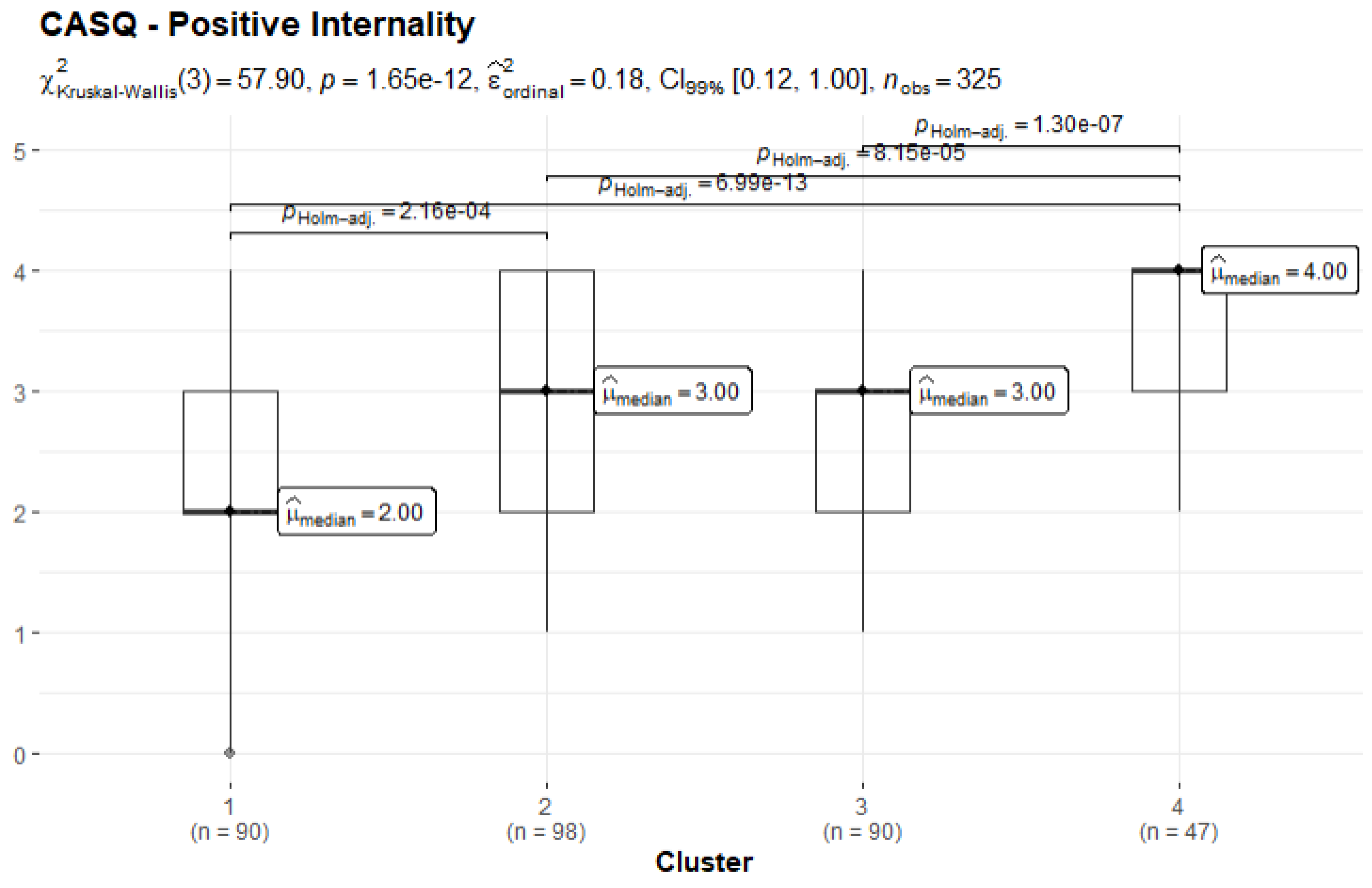
Figure 7.
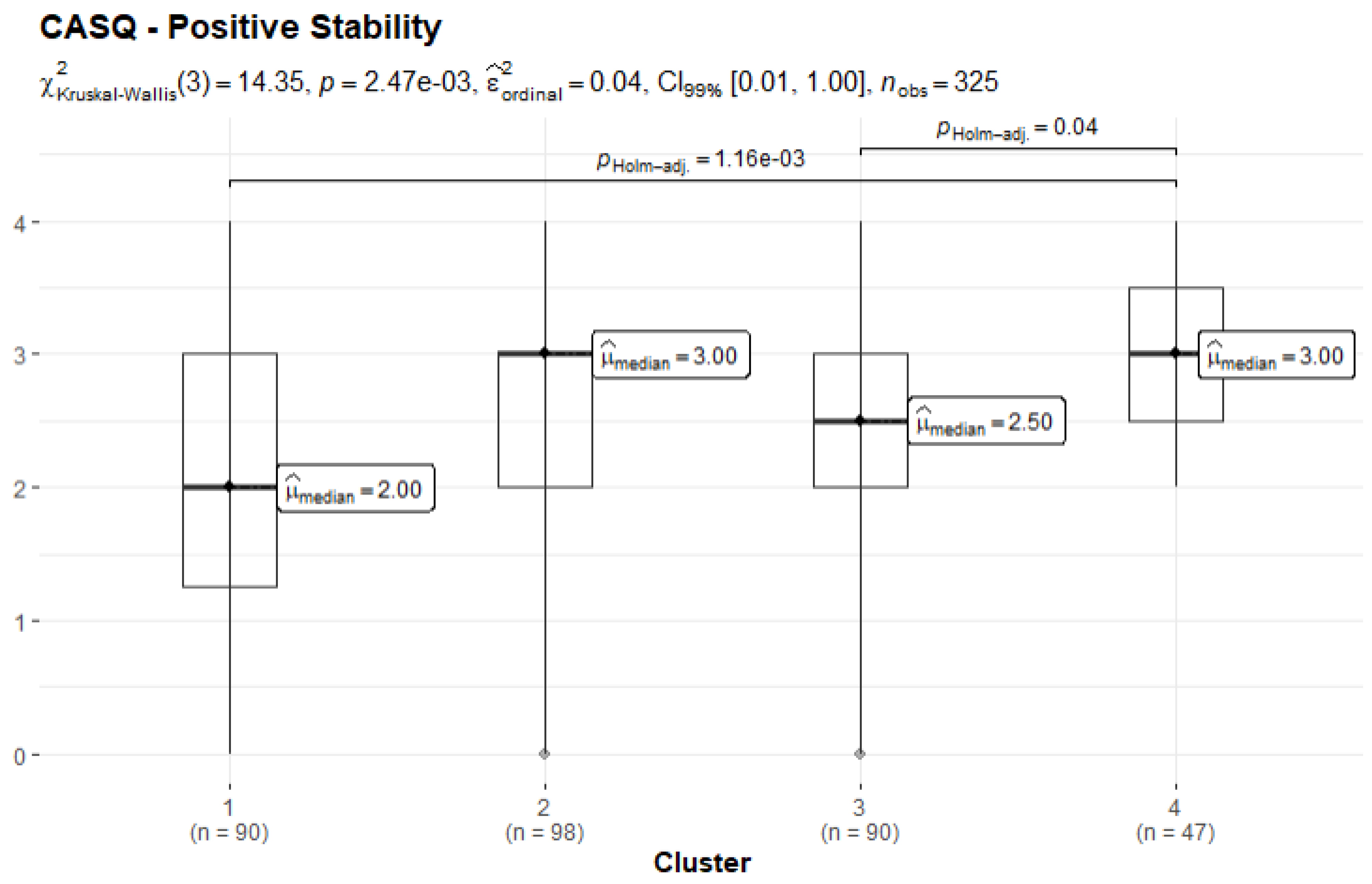
Figure 8.
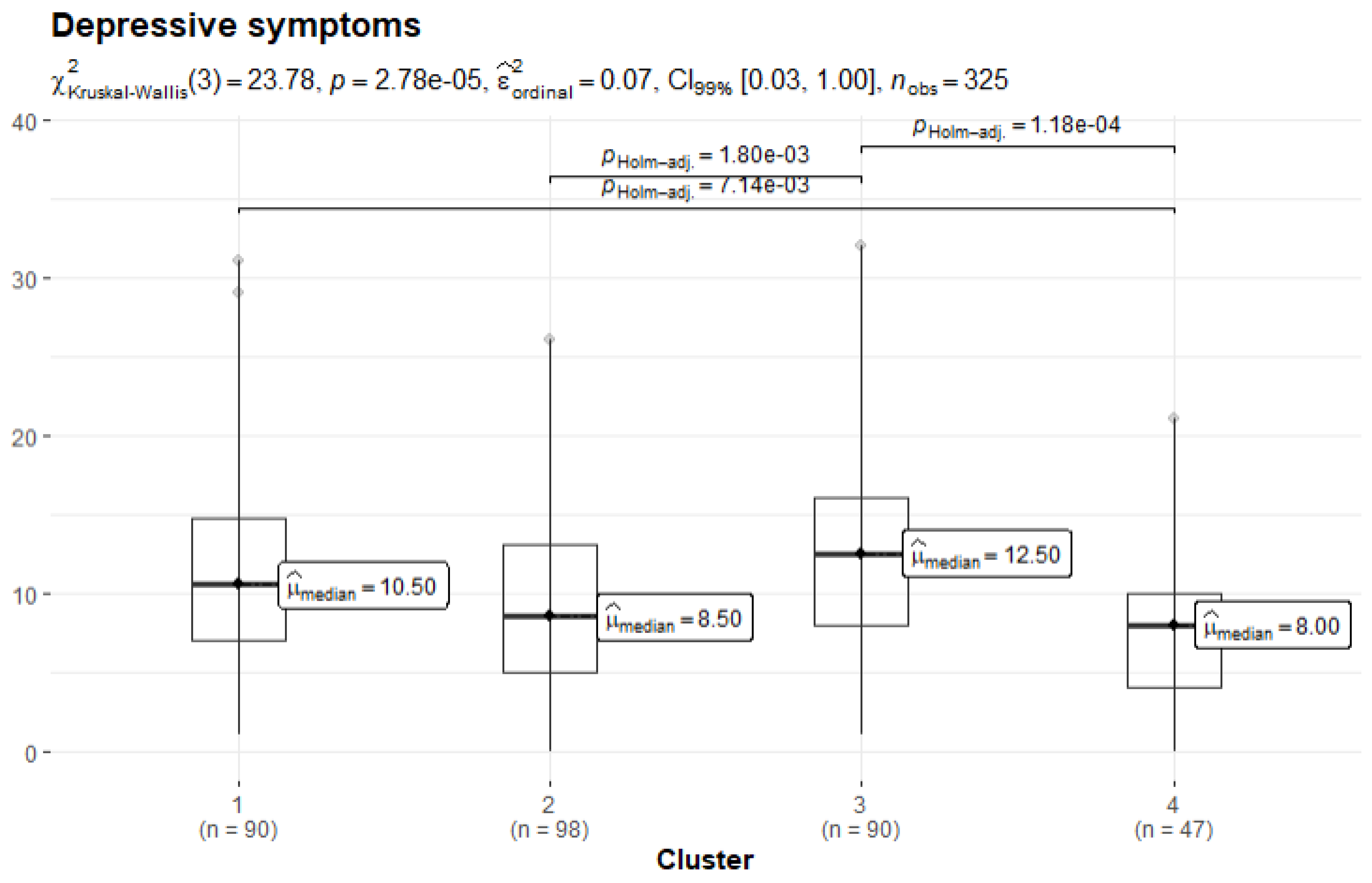

Table 1.
Pearson’s bivariate correlations among the study variables. Note that correlation coefficients depicted in bold are referred to the female sample, whereas the non-bold coefficients are referred to the sample of males.
Table 1.
Pearson’s bivariate correlations among the study variables. Note that correlation coefficients depicted in bold are referred to the female sample, whereas the non-bold coefficients are referred to the sample of males.
| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| 1. CDI total | - | -.314*** | .339*** | -.408*** |
| 2. CASQ-R positive | -.331*** | - | -.280*** | .803*** |
| 3. CASQ-R negative | .167* | -.139 | - | -.797*** |
| 4. CASQ-R total | -.330*** | .753*** | -.756*** | - |
Note. Significance levels * p < .05, *** p < .001; M: males; F: females; CDI: Children Depression Inventory; CASQ-R positive: positive composite score of the Children’s Attributional Style Questionnaire – Revised; CASQ-R negative: negative composite score of the Children’s Attributional Style Questionnaire – Revised; CASQ-R total: overall composite score of the Children’s Attributional Style Questionnaire – Revised.
Table 2.
Pearson’s bivariate correlations among the study variables in younger (˂11 years old, coefficients depicted in non-bold) and older (˃12 years old, coefficients depicted in bold) children.
Table 2.
Pearson’s bivariate correlations among the study variables in younger (˂11 years old, coefficients depicted in non-bold) and older (˃12 years old, coefficients depicted in bold) children.
| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| 1. CDI total | - | -.329*** | .233** | -.366*** |
| 2. CASQ-R positive | -.337*** | - | -.173* | .753*** |
| 3. CASQ-R negative | .266*** | -.243** | - | -.779*** |
| 4. CASQ-R total | -.383*** | .796*** | -.781*** | - |
Note. Significance levels * p < .05, ** p < .01; *** p < .001; Y: younger than 11 years old; O: older than 12 years old; CDI: Children Depression Inventory; CASQ-R positive: positive composite score of the Children’s Attributional Style Questionnaire – Revised; CASQ-R negative: negative composite score of the Children’s Attributional Style Questionnaire – Revised; CASQ-R total: overall composite score of the Children’s Attributional Style Questionnaire – Revised.
Table 3.
Cluster characteristics.
| Cluster | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Number of subjects (%) | 90 (27%) | 98 (30%) | 90 (27%) | 47 (16%) |
| m ± sd | m ± sd | m ± sd | m ± sd | |
| CASQ-R Negative Globality | 1.00±0.13 | 0.00±0.13 | 2.16±0.21 | 1.00±0.10 |
| CASQ-R Negative Internality | 1.91±0.97 | 1.64±0.97 | 1.80±1.52 | 0.91±0.76 |
| CASQ-R Negative Stability | 1.58±0.98 | 1.35±0.97 | 1.66±1.54 | 1.07±0.76 |
| CASQ-R Positive Globality | 1.80±0.81 | 2.21±0.81 | 2.08±1.27 | 2.83±0.63 |
| CASQ-R Positive Internality | 2.23±0.84 | 2.78±0.83 | 2.52±1.31 | 3.36±0.65 |
| CASQ-R Positive Stability | 2.26±0.96 | 2.60±0.96 | 2.51±1.50 | 2.99±0.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



