
Submitted:
17 May 2024
Posted:
20 May 2024
You are already at the latest version
Abstract
The quantity, makeup, and distribution of bodily fluids have a significant impact on the cognitive and physiological health of individuals. The knowledge of an individual on the recommended daily Total Water Intake (TWI) by the World Health Organization (WHO) and the European Food Safety Authority (EFSA) influences the practice of Adequate Water Intake (AWI). To sufficiently measure the knowledge of hydration, it is expedient to develop and validate a scale to adequately measure knowledge of the recommended daily Total Water Intake (TWI). Hence, this study aims to develop an 11-items scale to measure the Knowledge of hydration (KH-11) and evaluate its psychometric properties among foreign student at Óbuda University, Hungary. The novelty of this study is the development of an 11-item scale to measure the knowledge of hydration among students at Óbuda University, Hungary.
Keywords:
Adequate Water Intake (AWI)
; Health
; Hydration
; Knowledge
; Total Water Intake (TWI)
; Water
1. Introduction
Maintaining fluid and electrolyte balance is known as homeostasis, which is crucial for healthy functioning of the human body [1]. Salt and water overload, hypervolemia, and dehydration have all been linked to adverse outcomes of the human body and how it stays healthy [2]. Water balance of the human body is maintained by regulating its intake (by adopting Adequate Water Intake (AWI) [3]) with its loss [4]; thus, an essential component of life [5]. It is a component of all living cells and extracellular fluids [6]. Epidemiological studies have since revealed that humans can only survive for some days without drinking water [7,8,9]. Hence, water is considered as one of the most vital nutrients required for cellular homeostasis and life. Water makes up between 55% – 75% of an adult's body weight, thereby contributing to regular functioning of the human organs (and the entire human body) [10]. The quantity, makeup, and distribution of bodily fluids have a significant impact on cell activity. It also serves as a solvent, releasing a variety of solutes for use by cells, and it is the medium required for all processes [11]. The physiological functions of digestion, absorption, and elimination all require water to function by a conscious practice of the recommended Total Water Intake (TWI) [12]. A few years ago, the World Health Organization (WHO) [13] has agreed with the European Food Safety Authority (EFSA) [14] concerning the relevance of water to human health as regards the recommended daily Total Water Intake (TWI) with similar measurement of total fluids intake in Liters (L). As for WHO, daily Total Water Intake (TWI) is 2.9L for an adult male and 2.2L for an adult female who lives a sedentary lifestyle, while those who live an active lifestyle is 4.5L for an adult male and 4.5L for an adult female [15]. While for EFSA, daily Total Water Intake (TWI) for an adult female is 1.6L and the adult male can take 2.0L [16]. It is said that if any of these recommendations are not adopted, then the human body will suffer from water deprivation.
Water deprivation occurs when the balance between daily Total Water Intake (TWI) [14,15] and loss is disrupted; thus causes a state of dehydration in the human body [17,18] which may lead to mild/chronic illness [5]. Dehydration can be defined as a decrease in daily Total Water Intake (TWI) content due to fluid loss, reduction in fluid intake, or even both [19]. Dehydration could occur if a person loses as little as 3% of their body weight due to water loss. However, water loss of more than 5% of the total body fluid would probably lead to mild dehydration while severe dehydration occurs when there’s 9% – 10% loss of the total body fluid [5]. The lack of adequate daily Total Water Intake (TWI) has been revealed to contribute to body weight loss, deteriorating memory, and reduced concentration/focus [19]. According to many research studies which have proven to find specific medical evidence that shows the association between dehydration (as a result of inadequate water intake and some leading complications/risk factors such as lack physical effort, exposure to harsh climatic conditions (i.e. heat and humidity), inadequate water intake, and other factors connected to lifestyle [20]) and some chronic diseases/disorders [21,22]. Just to mention a few of these chronic diseases/disorders; they are kidney stones, heart disease, stroke, cystitis, bowel and colon cancer, stomach ulcer, constipation, excess weight and obesity, diarrheal, digestive disorder, high and low blood pressure, acid-alkaline imbalance, premature aging, skin disorder (e.g. eczema), and energy loss (e.g. fatigue, dizziness, restlessness, etc.) [5].
The WHO guideline for Total Water Intake (TWI) is based on a comprehensive review of scientific literature, including studies on water balance, hydration status, and health outcomes. It takes into consideration recommendations from other reputable sources, such as the National Academies of Sciences, Engineering, and Medicine, and the European Food Safety Authority [30]. Even though Total Water Intake (TWI) is said to vary by gender, individual water requirements may also vary depending on factors such as climate, physical activity level, and health status [30].
2. Study Motivation
Public awareness of dehydration is not widely assessed. A study conducted a hydration assessment in 2017 among university students in Southern Nigeria, the authors reported a 46.4% dehydration rate while 59% had inadequate water intake. The study further revealed that the likelihood of coffee intake for dehydration was higher among the study participants [20]. In 2011, some Chinese scholars also carried out a study on the knowledge of dehydration during summer in four cities and they reported that only 28.4% knew about dehydration [23]. Another study assessed dehydration status among university club athletes in Europe and found that dehydration was common (40%) among Karateka, female netball players, army officer cadets, and golfers [24]. A systematic review has reported that there is a major gap in knowledge and measurement of fluid intake and hydration status [10]. A link has been established between knowledge and healthy behavior [25,26], implying that the knowledge of people on daily Total Water Intake (TWI) will influence the practice of Adequate Water Intake (AWI) [27]. Therefore, to understand the knowledge of water intake among any population, the development of scales to adequately measure water intake is required. Although some studies have attempted to assess knowledge of dehydration among diverse populations, there is lack of clarity on the validity and reliability of the measurement of dehydration. Albeit, after a holistic review there is paucity of information on scale development for measurement of water intake among foreign university students in Hungary. Hence, this study aims to develop a scale (Knowledge of Hydration 11 items (KH-11)) and evaluate its psychometric properties among foreign student in Óbuda University, Hungary on the practice of Total Water Intake (TWI) by WHO or EFSA.
3. Methods
3.1. Study Design
An online cross-sectional study was conducted to assess the perception, knowledge, and practice of water intake among the foreign students of John von Neumann Faculty of Informatics, Óbuda University, Hungary for 3 months in 2019. The study population were international (foreign) students at Óbuda University. The survey link was shared among students of John von Neumann Faculty of Informatics only and shared on the University’ dormitory Facebook page for the specified students to access easily.
3.2. Sample Size
After the distribution of the survey for a period of 3 months, a total of 395 foreign students filled out the survey but not all participants were included in this study after data processing. However, only 323 foreign students were included in this study.
3.3. Instrument – Knowledge of Hydration 11 Items Scale (KH-11)
The KH-11 scale of 11 items was developed for the assessment of knowledge of water intake among the students. However, the whole survey contained 21 questions (which includes questions to capture the participants’ demographic characteristics, knowledge and perception about hydration, and dehydration status). In this study, we have extracted 11-knowledge-based questions on hydration to estimate the validity. The scale consists of 3 subscales: 1. Importance of water intake for staying hydrated [1-item]; 2. Recommendation of Total Water Intake (TWI) and source (Personal recommendation and recommendation according to the European Food Safety (EFSA) and the World Health Organization (WHO) [4-items]); 3. Knowledge of the benefits of Adequate Water Intake (AWI) [6 items].
The information in Table 1 below captured the questions for each item, options, the scores, and the scoring guide.
According to the table above, the sum of all the items resulted in a total of 80 possible scores. The KH-11 scale has good reliability having a Cronbach’s alpha of 80%. The subscale had an acceptable internal consistency as Cronbach’s alpha for the subscales ranged from 74.5% to 80.8%.
3.4. Data Collection
An electronic version of the survey which comprises the participants’ demographics, the knowledge of hydration scale, and other related questions was set up on Survey planet survey website. The electronic survey was administered by sending the survey link to the study population through Óbuda University’ Facebook page.
3.5. Data Analysis
The data were analyzed with IBM SPSS Statistics version 26. Descriptive statistics were analyzed presented in frequencies and percentages. We determined the internal consistency and reliability of the scales and the subscales using Cronbach’s alpha. The Cronbach alpha acceptability threshold of 70% or higher was adopted for this study [28]. Also, intraclass correlation and chi-square were estimated and presented. Factor analysis was done to examine the structure of the factors for KH-11 and the rotated component matrix was presented. We categorized the knowledge score into three groups (<50% score = poor knowledge, 50% – 70% = intermediate knowledge and 71% – 100% = adequate knowledge). This is to be able to analyze and present the level of knowledge of hydration among the study participants.
3.6. Ethical Consideration
The fore page of the electronic survey presented adequate information about the study and participants were informed that participation in the study is voluntary and no experiment needed to be performed. Hence, ethnical approval for this research was not required. All tenets of Helsinki’s declaration were ensured in this study. Data was downloaded on a personal computer which is password-protected and only accessible to the researchers (authors of this study).
4. Results
4.1. Demographic Characteristics of the Study Participants
The results in Table 2 below presented the demographic characteristics of the study participants. More of the participants were aged 25 to 34 years 144 (44.6%), while 41.2% of them were aged 18 to 24 years. Similarly, over half of 182 (56.4%) of the participants were males and 141 (43.6%) were females. The majority 157 (48.6%) of the students originated from Africa, 118 (36.5%) from Europe, and 48 (14.9%) from Asia. All 323 (100.0%) of the participants reside in Hungary when this study was conducted.
4.2. Distribution, Characteristics, Internal Consistency, Reliability, and Homogeneity of the KH-11
The distribution and characteristics of the KH-11 were presented in Table 3 below (and Table 1 in the supplementary material). The KH-11 score ranges from 0 (very low knowledge) to 72 (very high knowledge). The mean score was 55.2±11.61. The distribution of the knowledge score is skewed to the left. Also, the results showed that the KH-11 had an overall good reliability with a Cronbach’s alpha value of 0.80. The items had an acceptable level of consistency with the item Cronbach’s alpha value ranging from 0.75 to 0.81. All the items demonstrated sufficient independence from each other as Pearson’s correlation within factors was positive and ranged from 0.02 to 0.74.
4.3. Participants’ Knowledge about Hydration
As presented in Table 4 below, the total score for the scale is 72 and the mean score for the KH-11 was 55.2±11.61SD. Also, the mean score for Subscale 1. (Importance of water intake for staying hydrated [1-item]) was 0.9±0.07. Subscale 2. (Recommendation of Total Water Intake (TWI) [4-items]) had a mean score of 6.3±3.60 and Subscale 3. (Knowledge of the benefits of Total Water Intake (TWI) [6-items]) had a mean score of 47.9±11.17.
4.4. Factor Analysis Results
The results in Table 5 below show the factor loading for KH-11. The results also revealed an excellent factor loading for the subscales. For instance, all items (6-itmes) measure the knowledge of the benefits of Total Water Intake (TWI) loaded on factor 1 with a factor loading >0.5. Similarly, for 4-items loaded on the second subscale (Recommendation of Total Water Intake (TWI) and source), the factor loading was >0.9. Only one item was loaded on the third subscale (Importance of water intake for staying hydrated) with a factor loading >0.9. Overall, the model yielded an acceptable fit (χ2 = 3259.4, P = 0.000).
As shown in the table below, the items demonstrated a high level and positive concordance (0.770). Also, the two-way mixed effect model revealed a good model for KH-11 with an average intraclass correlation of 0.80 at a 95% confidence interval (CI), where P-value = 0.000 (see Table 6 below).
4.5. Knowledge of Hydration among Foreign Students of Óbuda University, Hungary
The result captured in Figure 1 presents the pattern of knowledge of hydration among the study participants. The majority (66.3%) of the participants had adequate knowledge, while 24.4% had intermediate knowledge and 9.3% had poor knowledge of hydration.
5. Discussion
We developed and conducted the psychometric analysis of a scale for assessment of the Knowledge of Hydration (KH-11) among foreign students at Óbuda University, Hungary. The mean score was 55.2±11.61, indicating a relatively high level of knowledge among the study population. However, the distribution of the knowledge scores was skewed to the left, suggesting that some participants may have lower levels of knowledge. The reliability of the KH-11 was assessed using Cronbach's alpha, a measure of internal consistency. The overall reliability of the KH-11 was good, with a Cronbach's alpha value of 0.80, indicating that the items in the questionnaire were consistent in measuring the same construct of knowledge about the topic. Furthermore, the item-level consistency of the KH-11 was also evaluated using item Cronbach's alpha values, which ranged from 0.75 to 0.81, indicating an acceptable level of consistency among the items. This suggests that the items in the KH-11 were reliable in measuring the knowledge of the participants. In addition, the Pearson's correlation within factors, which assesses the independence of items within each factor, was positive and ranged from 0.02 to 0.74, indicating that the items were sufficiently independent from each other. This suggests that the items in the KH-11 were measuring different aspects of knowledge and were not overly correlated, supporting the construct validity of the questionnaire. Hence, the scale KH-11 has a recommended reliability and consistency. Conventionally, a Cronbach’s alpha value >70% is acceptable [29]. Compared to the Cronbach value found in this study, some validated scales had a lower value. For instance, the psychometric properties developed for a brief generic cancer knowledge for patients reported a lower Cronbach’s alpha value of 0.68 [30]. Although, another study on psychometric properties of the dementia knowledge assessment among home care workers in Taiwan reported a Cronbach’s alpha slightly higher than the value we found in our study [31]. However, the value found in this study still falls within the acceptable threshold. Factors leading to a low Cronbach’s alpha value include fewer items in the scale and weakness of the set of items to measure the construct of interest [29].
The factor loadings for the KH-11 questionnaire were generally remarkable, suggesting that the items in the questionnaire effectively measured the underlying constructs of knowledge related to Total Water Intake (TWI) and its benefits, recommendations, and importance for staying hydrated. Specifically, all six items measuring the knowledge of the benefits of TWI loaded on factor 1 with factor loadings greater than 0.5, indicating a strong association between these items and the underlying construct of knowledge about the benefits of TWI. Similarly, the four items measuring recommendations of TWI and its sources loaded on the second subscale with factor loadings greater than 0.9, indicating a very strong association between these items and the underlying construct of knowledge about recommendations and sources of TWI. Only one item was loaded on the third subscale, measuring the importance of water intake for staying hydrated, with a factor loading greater than 0.9, indicating a high association between this item and the underlying construct of knowledge about the importance of water intake for staying hydrated. Furthermore, the overall model fit was acceptable, with a chi-square value of 3259.4 and a p-value of 0.000, indicating that the model adequately explained the observed data. The high concordance value of 0.770 among the items also indicates a high level of consistency in the responses, suggesting that the KH-11 questionnaire is reliable in measuring knowledge about water intake. Additionally, the two-way mixed effect model revealed a good model for KH-11 with an average intraclass correlation of 0.80 at a 95% confidence interval, with a p-value of 0.000, indicating that the KH-11 questionnaire has good reliability and consistency across different raters or measurements.
The use of our study instrument captured that the participants had a good knowledge of hydration with a mean score of 55.2±11.17 SD out of a total score of 72. Relative to other studies carried out in a different context that reported a seemingly high level of knowledge on hydration [19]. The disparity is likely caused by the construct of the instrument used for measuring the referenced study. Our study developed and validated a scale for the assessment of knowledge in the light of the study context.
Factor analysis was used to examine the psychometric properties of the KH-11. The result determined a three-factor structure for the scale. The items optimally loaded on the three subscales (Subscale 1. Knowledge of the benefits of Total Water Intake (TWI); Subscale 2. Recommendation of daily Total Water Intake (TWI) and source; and subscale 3. Importance of water intake for staying hydrated). This optimal factor loading with an acceptable score ranging from 0.5 to 0.9, the model fit, and the intraclass correlation implies construct validity for the KH-11 scale. The novelty of this study is the development of an 11-item scale to measure the knowledge of hydration among students at Óbuda University, Hungary. Other studies developed scales to measure an outcome different from the outcome of interest in this study. Many of the studies also reported optimal results similar to this study [32]. The similarity in the findings could be linked to the use of the same methods of developing the scales and the method of analysis.
The mean score for the KH-11 questionnaire was 55.2±11.61SD, out of a total possible score of 72. This suggests that, on average, the participants had a moderate level of knowledge about water intake as assessed by the KH-11 questionnaire. Furthermore, the mean scores for the three subscales of the KH-11 questionnaire were also reported. Subscale 1, which measures the importance of water intake for staying hydrated with only 1 item, had a mean score of 0.9±0.07, indicating a high level of knowledge on this specific aspect. Subscale 2, which measures recommendations of Total Water Intake (TWI) with 4 items, had a mean score of 6.3±3.60, indicating a moderate level of knowledge on this aspect. Subscale 3, which measures the knowledge of the benefits of TWI with 6 items, had a mean score of 47.9±11.17, indicating a moderate level of knowledge on this aspect as well.
In furtherance, we categorized the knowledge score into three groups (< 50% score = poor knowledge, 50% – 70% = intermediate knowledge and 71% – 100%= adequate knowledge) to determine the level of knowledge of water intake among the students. The result showed that the majority (66.3%) of the students had good knowledge, while 24.4% had intermediate knowledge and 9.3% had poor knowledge of hydration. The rate of good knowledge reported in this study was quite higher compared to a similar study carried out in 2014 among adults in the United Kingdom, France, and Spain – the study from which we have adopted the survey questions [33]. Another study conducted in 2022 found a 51% rate of adequate knowledge of hydration among medical university students in UAE who correctly recognized the importance of water [34]. This prevalence is also lower compared to our findings. Similarly, Lee et al reported a rate of 28% prevalence of adequate water intake in 2016 [35]. The disparity in this finding could be a spatial distribution of the participants in the different studies. Also, the level of intervention towards improvement of wellbeing varied across countries [36,37]. In the same vein, there is a possible time difference in the findings, the pattern seems to increase over time. Factors such as context, population, and robust methodology of the current study play a key role in the disparities between this study and the other studies being compared. However, our study revealed a slightly higher prevalence of knowledge about hydration among students.
6. Conclusion
The KH-11 scales had a significant amount of acceptable reliability and consistency. Also, the items were optimally loaded on a three-factor structure for the scale which implies construct validity. Also, the use of this instrument captured that the participants had a good knowledge of hydration with a mean score of 55.2±11.17SD. The prevalence of adequate level of knowledge of hydration was 66.3% in this study. This is low. This study suggests a need for further education and intervention to improve knowledge about hydration among the foreign students, which can have important implications for their overall health and well-being. Overall, the results of the study indicate that the KH-11 is a reliable and valid measure of knowledge about the topic under investigation, with good overall reliability and acceptable item-level consistency. However, the skewed distribution of knowledge scores suggests that some participants may have lower levels of knowledge, which may warrant further investigation or intervention to improve knowledge in those individuals.
7. Recommendation
We recommend the use of this scale for future research in the context in which the scale was developed. Although, this study revealed an appreciable level of knowledge of hydration, but intervention should be made to improve knowledge to 100% among the students of John von Neumann Faculty of Informatics at Óbuda University, Hungary. Hence, we have considered the need to begin a campaign to include the entire students (foreign and local-Hungarian) of the university: Hydration Campaign at Óbuda University.
8. Study Limitations and Future Work
Due to unavailability of adequate resources, we could only reach out to a fraction of the students of Óbuda University during the survey distribution. Furthermore, the use of hydration biomarkers was not implemented to diagnose hydration status in this study. However, this does not erode the significance of this paper, as probabilistic samples were drawn from the target population. In order to correct the shortcomings of unavailability of sufficient data for this study, we are currently organizing hydration campaign among the (foreign and local) PhD students of Óbuda University to create more awareness about hydration, assess the knowledge of the students about hydration, and also assess their knowledge using the second survey to estimate if there is an improvement on the knowledge about hydration after taking the first survey.
Author Contributions
Conceptualization of research: M.O.O. and M.K.; methodology: M.O.O., O.D.E., and M.K.; software: M.O.O. and O.D.E.; formal analysis: M.O.O. and O.D.E.; investigation: M.O.O.; resources: M.O.O. and M.K.; data curation: M.O.O.; writing—original draft preparation: M.O.O., O.D.E., and M.V.; writing—review and editing: M.O.O., O.D.E., M.V., and M.K.; visualization: M.O.O., O.D.E., M.V., and M.K.; supervision: M.K.; project administration: M.O.O. and M.K.; funding acquisition: M.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Ministry of Innovation and Technology NRDI Office within the framework of the Infocommunications and Information Technologies National Laboratory. The authors hereby thank the Eötvös Loránd Research Network Secretariat under grant agreement no. ELKH KÖ-40/2020 (Development of cyber-medical systems based on AI and hybrid cloud methods, the GINOP-2.2.1-15-2017-00073 “Telemedicina alapú ellátási formák fenntartható megvalósítását támogató keretrendszer kialakítása és tesztelése” project, and the 2019-1.3.1-KK-2019-00007, In-novációs szolgáltató bázis létrehozása diagnosztikai, terápiás és kutatási célú kiberorvosi rend-szerek fejlesztésére” project for their financial support.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Participants provided consent by clicking the “accept to participate” button after reading the informed consent on the first page of the online survey. To assure the privacy and confidentiality of the participants, all participants voluntarily participated in this study and no identifying information was captured. Since data were collected online, the study has no/minimal risk to the health of the participants, their environment, or their relatives.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The hydration and dehydration data collected during this project and processed for this research publication are available upon request. Data are contained within the article.
Acknowledgments
This research was supported by the Ministry of Innovation and Technology NRDI Office within the framework of the Infocommunications and Information Technologies National Laboratory. The authors hereby thank the Eötvös Loránd Research Network Secretariat under grant agreement no. ELKH KÖ-40/2020 (Development of cyber-medical systems based on AI and hybrid cloud methods, the GINOP-2.2.1-15-2017-00073 “Telemedicina alapú ellátási formák fenntartható megvalósítását támogató keretrendszer kialakítása és tesztelése” project, and the 2019-1.3.1-KK-2019-00007, Innovációs szolgáltató bázis létrehozása diagnosztikai, terápiás és kutatási célú kiberorvosi rendszerek fejlesztésére” project for their financial support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- S. M. Adler and J. G. Verbalis, “Disorders of Body Water Homeostasis in Critical Illness,” Endocrinology and Metabolism Clinics of North America, vol. 35, no. 4, pp. 873–894, Dec. 2006. [CrossRef]
- M. El-Sharkawy et al., “Hydration and outcome in older patients admitted to hospital (The HOOP prospective cohort study),” Age Ageing, vol. 44, no. 6, pp. 943–947, Nov. 2015. [CrossRef]
- Malisova et al., “Water Intake and Hydration Indices in Healthy European Adults: The European Hydration Research Study (EHRS),” Nutrients, vol. 8, no. 4, p. 204, Apr. 2016. [CrossRef]
- D. Sladek and A. K. Johnson, “Integration of thermal and osmotic regulation of water homeostasis: The role of TRPV channels,” Am J Physiol Regul Integr Comp Physiol, vol. 305, no. 7, pp. R669-678, Oct. 2013. [CrossRef]
- M. Omone, M. Kozlovszky, T. Ferenci, and I. G. Inalegwu, “Hydration Assessment Among Foreign University Students,” in 2019 IEEE 19th International Symposium on Computational Intelligence and Informatics and 7th IEEE International Conference on Recent Achievements in Mechatronics, Automation, Computer Sciences and Robotics (CINTI-MACRo), Nov. 2019, pp. 000161–000168. [CrossRef]
- T. Szádeczky, “Water 4.0 in Hungary: Prospects and Cybersecurity Concerns,” ACTA POLYTECH HUNG, vol. 20, no. 7, pp. 211–230, 2023. [CrossRef]
- V. Agrawal, M. Agarwal, S. R. Joshi, and A. K. Ghosh, “Hyponatremia and hypernatremia: Disorders of water balance,” J Assoc Physicians India, vol. 56, pp. 956–964, Dec. 2008.
- J. D. Akers, R. A. Cornett, J. S. Savla, K. P. Davy, and B. M. Davy, “Daily Self-Monitoring of Body Weight, Step Count, Fruit/Vegetable Intake, and Water Consumption: A Feasible and Effective Long-Term Weight Loss Maintenance Approach,” Journal of the Academy of Nutrition and Dietetics, vol. 112, no. 5, pp. 685-692.e2, May 2012. [CrossRef]
- L. E. Armstrong et al., “Bioimpedance spectroscopy technique: Intra-, extracellular, and total body water:,” Medicine & Science in Sports & Exercise, vol. 29, no. 12, pp. 1657–1663, Dec. 1997. [CrossRef]
- B. M. Popkin, K. E. D’Anci, and I. H. Rosenberg, “Water, hydration, and health: Nutrition Reviews©, Vol. 68, No. 8,” Nutrition Reviews, vol. 68, no. 8, pp. 439–458, Aug. 2010. [CrossRef]
- S. N. Boilesen, S. Tahan, F. C. Dias, L. C. F. L. Melli, and M. B. de Morais, “Water and fluid intake in the prevention and treatment of functional constipation in children and adolescents: Is there evidence?,” Jornal de Pediatria, vol. 93, no. 4, pp. 320–327, Jul. 2017. [CrossRef]
- S. Balaghi, E. Faramarzi, R. Mahdavi, and J. Ghaemmaghami, “Fluids Intake and Beverage Consumption Pattern among University Students,” Health Promot Perspect, vol. 1, no. 1, pp. 54–61, 2011. [CrossRef]
- W. H. O. S. D. and H. E. Cluster, Nutrients in drinking water. World Health Organization, 2005. Accessed: Oct. 11, 2019. [Online]. Available: https://apps.who.int/iris/handle/10665/43403.
- “Scientific Opinion on Dietary Reference Values for water,” EFSA Journal, vol. 8, no. 3, p. 1459, 2010. [CrossRef]
- W. H. O. Water and S. and H. Team, Guidelines for drinking-water quality. Vol. 1, Recommendations. World Health Organization, 2004. Accessed: Oct. 11, 2019. [Online]. Available: https://apps.who.int/iris/handle/10665/42852.
- “Dietary reference values for water | European Food Safety Authority.” https://www.efsa.europa.eu/en/efsajournal/pub/1459 (accessed Oct. 01, 2019).
- B. Bothorel, M. Follenius, R. Gissinger, and V. Candas, “Physiological effects of dehydration and rehydration with water and acidic or neutral carbohydrate electrolyte solutions,” Europ. J. Appl. Physiol., vol. 60, no. 3, pp. 209–216, 1990. [CrossRef]
- S. N. Cheuvront and R. W. Kenefick, “Dehydration: Physiology, Assessment, and Performance Effects,” in Comprehensive Physiology, R. Terjung, Ed., Hoboken, NJ, USA: John Wiley & Sons, Inc., 2014, pp. 257–285. [CrossRef]
- N. A. Shaheen, A. A. Alqahtani, H. Assiri, R. Alkhodair, and M. A. Hussein, “Public knowledge of dehydration and fluid intake practices: Variation by participants’ characteristics,” BMC Public Health, vol. 18, no. 1, p. 1346, Dec. 2018. [CrossRef]
- C. E. Ekpenyong and I.-A. M. Akpan, “High prevalence and associated risk factors of dehydration among college students: Implications for health and academic performance,” International Journal Of Community Medicine And Public Health, vol. 4, no. 4, pp. 1043–1055, Mar. 2017. [CrossRef]
- Prüss-Ustün et al., “Burden of disease from inadequate water, sanitation and hygiene in low- and middle-income settings: A retrospective analysis of data from 145 countries,” Trop Med Int Health, vol. 19, no. 8, pp. 894–905, Aug. 2014. [CrossRef]
- J.-H. Kim, H.-K. Cheong, and B.-H. Jeon, “Burden of Disease Attributable to Inadequate Drinking Water, Sanitation, and Hygiene in Korea,” J Korean Med Sci, vol. 33, no. 46, Oct. 2018. [CrossRef]
- Q. Zhang et al., “[Water intake of adults in four cities of China in summer],” Zhonghua Yu Fang Yi Xue Za Zhi, vol. 45, no. 8, pp. 677–682, Aug. 2011.
- P. J. Magee, A. M. Gallagher, and J. M. McCormack, “High Prevalence of Dehydration and Inadequate Nutritional Knowledge Among University and Club Level Athletes,” Int J Sport Nutr Exerc Metab, vol. 27, no. 2, pp. 158–168, Apr. 2017. [CrossRef]
- Y. Bilan, K. Chudy-Laskowska, E. Szczygieł, and T. Piecuch, “People’s Behavior, in the Context of Living Standards Changes and Sustainable Development, Exemplified by the Carpathian Euroregion,” ACTA POLYTECH HUNG, vol. 18, no. 2, pp. 105–125, 2021. [CrossRef]
- M. Garai-Fodor, “Food Consumption Patterns, in a Values-based Approach, for Generation Z,” ACTA POLYTECH HUNG, vol. 18, no. 11, pp. 117–134, 2021. [CrossRef]
- D. S. Kenkel, “Health Behavior, Health Knowledge, and Schooling,” Journal of Political Economy, vol. 99, no. 2, pp. 287–305, 1991.
- F. Hayes and J. J. Coutts, “Use Omega Rather than Cronbach’s Alpha for Estimating Reliability. But…,” Communication Methods and Measures, vol. 14, no. 1, pp. 1–24, Jan. 2020. [CrossRef]
- G. O. Boateng, T. B. Neilands, E. A. Frongillo, H. R. Melgar-Quiñonez, and S. L. Young, “Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer,” Frontiers in Public Health, vol. 6, 2018, Accessed: Feb. 11, 2023. [Online]. Available: https://www.frontiersin.org/articles/10.3389/fpubh.2018.00149.
- E. Ziegler, J. Klein, and C. Kofahl, “Do members of cancer peer support groups know more about cancer than non-members? Results from a cross-sectional study in Germany,” Support Care Cancer, vol. 31, no. 1, p. 7, Dec. 2022. [CrossRef]
- H.-C. Sung, H.-F. Su, H.-M. Wang, M. Koo, and R. Y. Lo, “Psychometric properties of the dementia knowledge assessment scale-traditional Chinese among home care workers in Taiwan,” BMC Psychiatry, vol. 21, p. 515, Oct. 2021. [CrossRef]
- J. Klein, C. Kofahl, and E. Ziegler, “Development and psychometric properties of a brief generic cancer knowledge scale for patients (BCKS-10),” Cancer Causes Control, vol. 33, no. 9, pp. 1173–1179, Sep. 2022. [CrossRef]
- M. A. F. Rosemary Tyrwhitt-Drake Rafael Urrialde de Andrés,-, “Knowledge and perceptions of hydration: A survey among adults in the United Kingdom, France and,” REVISTA ESPAÑOLA DE NUTRICION COMUNITARIA, no. 4, pp. 128–136, Sep. 2014. [CrossRef]
- R. Abdulsalam, A. Alsadah, M. Alkhuboli, D. Muala, A. Hussein, and A. B. Elmoselhi, “Hydration status assessment and impinging factors among university students in the UAE”.
- K. W. Lee, D. Shin, and W. O. Song, “Total Water Intake from Beverages and Foods Is Associated with Energy Intake and Eating Behaviors in Korean Adults,” Nutrients, vol. 8, no. 10, p. 617, Oct. 2016. [CrossRef]
- K. Ruggeri, E. Garcia-Garzon, Á. Maguire, S. Matz, and F. A. Huppert, “Well-being is more than happiness and life satisfaction: A multidimensional analysis of 21 countries,” Health and Quality of Life Outcomes, vol. 18, no. 1, p. 192, Jun. 2020. [CrossRef]
- “Interventions to improve the mental health or mental well-being of migrants and ethnic minority groups in Europe: A scoping review | Cambridge Prisms: Global Mental Health | Cambridge Core.” https://www.cambridge.org/core/journals/global-mental-health/article/interventions-to-improve-the-mental-health-or-mental-wellbeing-of-migrants-and-ethnic-minority-groups-in-europe-a-scoping-review/08FC1FB10DEC9E0E69EE43728E136D19 (accessed Aug. 14, 2023).
Figure 1.
Knowledge of Hydration among Foreign Students of Óbuda University, Hungary.
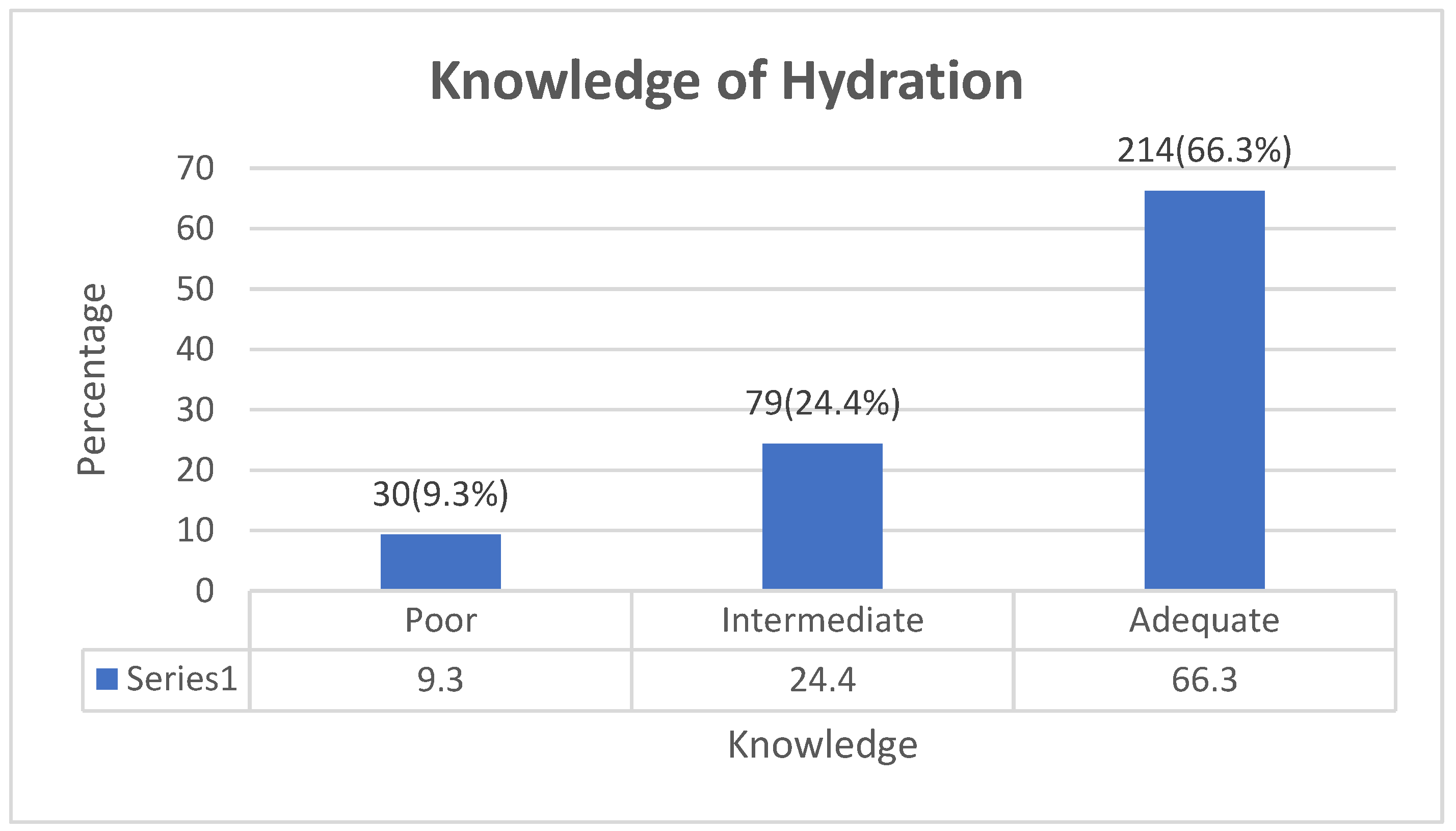

Table 1.
Knowledge of Hydration 11 items scale (KH-11) Survey Questions.
| SN | Questions – KH-11 | Options and Scores |
|---|---|---|
| 1 | Do you think drinking water is important to help stay properly hydrated? | Yes = 1 No = 0 |
| 2 | What do you think is the recommended daily Total Water Intake (TWI) (in Liters per day)? Please, answer for both males and females. | Male = 2.5 = 2 Female = 2.0 = 2 Else = 0 |
| 3 | According to the European Food Safety Authority (EFSA) or World Health Organization (WHO), what do you think is the recommended daily Total Water Intake (TWI) (in Liters per day)? Please, answer for both males and females. | Male = 2.5 =2 Female = 2.0 = 2 Else = 0 |
| 4 | The daily recommended water intake has to come from which of the following? | [Food moisture only] = 0, [Beverages of all kinds only] = 0, [Water only] = 0 [All of the Above = 4] = 1 |
| 5 | According to the European Food Safety Authority (EFSA) or World Health Organization (WHO), the daily recommended Total Water Intake (TWI) has to come from which of the following? | [Food moisture only] = 0, [Beverages of all kinds only] = 0, [Water only] = 0 [All of the Above = 4] = 1 |
| 6 | Please carefully read each of the following statements about hydration during different moments in your life. Decide by using a scale of 1 - 10 (note: the scale increases from 1 to 10) Each of the 6 items has a score ranging from 1 – 10 summed up to 60 possible score |
|
| 11 items, the total possible score is 72. High scores imply good knowledge | ||
Table 2.
Demographic Characteristics of the Participants.
| Variables | Frequency (n=323) | Percent (%) |
|---|---|---|
| Age Group | ||
| Between 18 - 24 | 133 | 41.2 |
| Between 25 - 34 | 144 | 44.6 |
| Between 35 – 44 | 28 | 8.7 |
| Between 45 – 54 | 12 | 3.7 |
| Between 55 – 65 | 6 | 1.9 |
| Gender | ||
| Female | 141 | 43.6 |
| Male | 182 | 56.4 |
| Continent of Origin | ||
| Africa | 157 | 48.6 |
| Asia | 48 | 14.9 |
| Europe | 118 | 36.5 |
| Place of Residence | ||
| Hungary | 323 | 100.0 |
Table 3.
The Distribution and Characteristics of the KH-11.
| Mean (SD) | No of items | Cronbach's Alpha | Shapiro-Wilk | P-value |
|---|---|---|---|---|
| 55.2(11.61) | 11 | 0.80 | 0.89 | 0.000 |
Table 4.
Knowledge about Hydration.
| Subscales | Mean (SD) | Total possible score |
|---|---|---|
| Subscale 1: Importance of water intake for staying hydrated [1-item]. | 0.9 (0.07) | 1 |
| Subscale 2: Recommendation of Total Water Intake (TWI) and source (Personal recommendation and recommendation according to the European Food Safety (EFSA) and the World Health Organization (WHO) [4-items]. | 6.3(3.60) | 11 |
| Subscale 3: Knowledge of the benefits of Total Water Intake (TWI) [6-items]. | 47.9 (11.17) | 60 |
| Total | 55.2 (11.61) | 72 |
Table 5.
Factor Analysis Results for KH-11.
| Items | Factors | Chi-square | P- Value | ||
| 1 | 2 | 3 | 3259.4 | 0.000 | |
| Do you think drinking water is important to help stay properly hydrated? | 0.97 | ||||
| What do you think is the recommended daily Total Water Intake (TWI) (in Liters per day)? | 0.91 | ||||
| According to the European Food Safety Authority (EFSA) or World Health Organization (WHO), what do you think is the recommended daily Total Water Intake (TWI) (in Liters per day)? | 0.91 | ||||
| The daily recommended Total Water Intake (TWI) has to come from which of the following? | 0.91 | ||||
| According to the European Food Safety Authority (EFSA) or World Health Organization (WHO), the daily recommended Total Water Intake (TWI) has to come from which of the following? | 0.91 | ||||
| Please carefully read each of the following statements about hydration during different moments in your life | |||||
| In an adult, drinking a lot of water is a good way to cleanse the body. | 0.86 | ||||
| At school and work, adequate hydration is important for proper brain performance and productivity. | 0.89 | ||||
| During the day everyone should drink at least 2.0 Liters of water. | 0.86 | ||||
| Staying hydrated can be influenced by some factors (such as Exercise Intensity and Duration, Temperature and Humidity, etc.). | 0.84 | ||||
| Due to age, the sensation of thirst can be reduced. | 0.51 | ||||
| Increased water intake contributes to living a healthy life. | 0.87 | ||||
| Kendal Tau coefficient of concordance | 0.77 | ||||
Rotated Component Matrix.Factor 1: Knowledge of the benefits of Adequate Water Intake (AWI). Factor 2: Recommendation of Adequate Water Intake (AWI) and source. Factor 3: Importance of water intake for staying hydrated.
Table 6.
Two-way Mixed Effect Model for KH-11.
| Intraclass Correlation | 95% CI | F Test | |||
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | P-value | |||
| Average Measures | 0.80 | 0.767 | 0.827 | 4.952 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



