
Submitted:
17 May 2024
Posted:
20 May 2024
You are already at the latest version
Abstract
: This study aimed to validate the effects of self-compassion-based forest healing therapy as an intervention for reducing stress and promoting coping resources. Therefore, we investigated the effects of self-compassion-based forest healing therapy on stress, self-compassion, and connectedness to nature. A total of 30 participants were divided into an experimental and control group. Two sessions of forest healing meditation activities were held at the Forest of Healing every two weeks between October and November 2023. As a repeated measures experiment, data were collected before the intervention, after the first intervention, and after the second intervention. Perceived stress, positive and negative affect, and salivary cortisol were measured to assess physiological and psychological stress in participants. Connectedness to nature and self-compassion were measured to evaluate stress-coping resources. The results showed that the forest healing program had significant positive effects on stress and emotional states in the experimental group after the intervention. Further, there was a significant incremental effect on connectedness to nature and self-compassion in the experimental group. Therefore, self-compassion meditation-based forest healing therapy is a feasible and efficient approach for facilitating stress management and coping resource building.
Keywords:
natural environment-based interventions
; forest therapy
; stress
; positive affect
; negative affect
; connectedness to nature
; self-compassion
1. Introduction
While less dramatic than major life events or chronic stressors, daily stressors experienced by modern individuals may become chronic if they continue to accumulate without being resolved and are a significant factor for individuals’ long-term adjustment, health, and well-being [1,2]. Particularly, emotional responses to daily stressors have been shown to predict chronic diseases, which are a major public health challenge of the 21st century [1]. However, according to Lazarus and Folkman’s stress transaction model, not all stressors have a detrimental effect on health; stress is activated when an individual perceives their coping resources to be inadequate through an appraisal thereof [3]; this process includes the use of internal and external resources as coping strategies. If an individual exhibits stable responses to stress, such differential responses are known to influence their well-being [4].
According to the 2022 Community Health Survey (CHS) conducted by the Korea Disease Control and Prevention Agency (KDCA), 24.5% of Korean adults mentioned that they have extremely high or high stress in their daily life [5]. One out of every four adults is estimated to face threats to their well-being due to daily stress that overwhelm their personal coping resources and adaptative capability. For example, 63.9% of adults in Korea experienced at least one or more mental health issues, such as depression, stress, and insomnia, in 2022, with stress reported as a major threat to mental health [6]. This suggests that failure to cope with daily stressors may lead to prolonged accumulation of perceived stress and negative emotions, ultimately causing more chronic health conditions and severe mood disorders [1]. Thus, there is a growing need for interventions that offer effective, affordable, and accessible coping resources for daily stress to manage mental health issues in everyday life [7,8].
The natural environment is progressively acknowledged as a vital resource for sustaining and recuperating health in the lives of contemporary individuals, who often experience heightened mental stress [9]. Exposure to nature triggers unconscious autonomic responses characterized by a reduction in physiological arousal, a decrease in negative impact, and an increase in positive impact, thereby alleviating physiological and psychological stress [10,11,12]. Empirical studies on nature-based health interventions consistently demonstrate a reduction in physiological stress markers such as blood pressure, heart rate, and cortisol levels, as well as perceived stress regardless of the nature of participation (active, passive, or virtual [12,13]. Moreover, changes in positive emotional and affective states are consistently associated with psychological recovery from stress [14,15,16]. According to Fredrickson’s broaden-and-build theory of positive emotions, positive affect broadens individuals’ momentary thought-action repertoires, enhances mental flexibility, strengthens meaning-based coping, and motivates engagement in new activities and social relationships [17,18]. Importantly, positive emotions—though transient—act as a preparatory resource that enhances the likelihood of stress coping, thereby contributing to the construction of long-term psychological, physical, and social resources [17]. Thus, the natural environment may be more than just a place for recovery from stress [19,20,21,22,23]. In this perspective, forest healing activities, a classic example of nature-based health interventions, can facilitate the management of daily stress and serve as an intervention to help individuals foster key inner characteristic resources to cope with stressors [19,20,21,22].
Mayer and Frantz characterize the connectedness to nature as both a state and trait reflecting an individual’s emotional bond with the natural world [24]. While exposure to nature often fosters this bond, the absence of attention and inability to cultivate this connectedness can impede the realization of nature’s potential health benefits [25]. Connectedness to nature is known to partially mediate and moderate the association between nature exposure and positive health outcomes [22,26]. Meta-analytical evidence suggests that heightened levels of connectedness to nature are linked to increased happiness and overall well-being [27,28]. Recent findings by Bakir-Demir et al. have shown that a strong connectedness to nature is predictive of reduced perceived stress, facilitated by the reinforcement of adaptive emotion regulation strategies [29]. Hence, connectedness to nature can serve as a valuable coping mechanism that enhances the probability of employing cognitive reappraisal as an adaptive emotion regulation strategy [29].
Conversely, compassion, a concept rooted in Buddhist traditions, has evolved into a significant attribute for mental health and well-being through conceptualization over the processes of secularization and scientification [30,31,32]. Self-compassion represents a compassionate attitude directed inwardly, where one embraces oneself as a focus of care and attention amid experiences of mental, emotional, and physical distress [33]. As defined by Neff, self-compassion entails offering warmth, support, and understanding to oneself during periods of hardship or failure, perceiving one’s suffering as part of the collective human experience, and acknowledging it with balance and mindfulness [33,34]. Elevated levels of self-compassion are associated with enhanced psychological well-being and reduced levels of depression, anxiety, and perceived stress [35,36,37,38,39]. In particular, self-compassion serves as a protective buffer against acute stressors [40] and plays a role in regulating health-promoting behaviors and shaping the process of coping with stress [41,42,43,44,45]. Therefore, this study aims to explore the potential of self-compassion, recognized for facilitating adaptive responses to stressors, as a pivotal element of forest healing activities and facilitating the cultivation of internal resources in tandem with connectedness to nature [44,45].
In a recent study by McEwan et al., the effects of Compassion Mind Training (CMT) (an emotional regulation intervention established in the United Kingdom), forest bathing, and a combined intervention of forest bathing and CMT were compared [46]. All three conditions led to enhancements in indicators related to well-being, connectedness to nature, and compassion, with the interventions showing equivalent effectiveness. Notably, the combined forest bathing and CMT group (change score = 0.84) showed a greater improvement in the connectedness to nature score compared to that of the forest bathing alone (change score = 0.72) and CMT alone (change score = 0.25). Given the findings of McEwan et al.’s study, there may be a synergistic relationship between connectedness to nature and compassion.
Stress management is a crucial aspect of addressing mental health concerns [6]. The need for individuals to develop coping resources is becoming more pressing in the face of challenges associated with managing mental health due to stress. The eight-week Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Self-Compassion (MBSC) programs are recognized as established interventions that promote individual well-being and effective stress management [39,47,48,49,50]. However, access to these programs may be limited for many people due to constraints related to time, resources, and accessibility [51,52]. In Korea, forest resources have been repurposed as public health and welfare assets since the 2000s, offering forest healing as a health and welfare service that is readily accessible and beneficial to the public [53,54]. Forest healing initiatives in Korea are provided for free or at a minimal cost, to enhance public welfare. The number of national and public forests of healing has expanded from five in 2015 to 43 in 2024, with a significant surge in the number of visitors seeking forest healing experiences [55]. In a systematic study on the current state of forest healing in Korea, Park et al. have recommended that programs be tailored to cater to a broad audience rather than focusing on specific groups, as over 90% of forest healing participants engage in programs designed for the general public [56]. Typically, individuals may face challenges in visiting forests of healing regularly; therefore, most of these sites offer single-session programs. Against this backdrop, there is a growing demand for evidence-based interventions that offer brief forest healing activities [56].
We aim to obtain evidence supporting the use of a self-compassion-based forest healing program as a public health intervention by investigating its potential to promote recovery from daily stress and foster connectedness to nature and self-compassion as coping resources. In this regard, we establish the following hypotheses to examine whether a brief forest healing meditation program helps reduce daily stress and cultivates stress-coping resources.
The main hypotheses are: (1) A self-compassion-based forest healing meditation program will progressively improve psychological and physiological stress and affect. (2) A self-compassion-based forest healing meditation program will progressively cultivate connectedness to nature and self-compassion.
2. Materials and Methods
2.1. Participants and Procedure
Participants were recruited from September to early October 2023 by posting notices and banners at the JatHyanggi Green Forest Healing Center in Gyeonggi Province, as well as through recommendations from personal acquaintances. The number of participants in the forest healing program was limited to approximately 15 to ensure the quality of forest healing. The inclusion criteria were middle-aged adults residing in the Seoul metropolitan area who were healthy enough to conduct their daily living, had no impediments to outdoor activities, and were able to complete self-reported questionnaires.
The participants were informed about the aim and procedures of the study and provided informed consent before participating in the experiment. After completing all measurements, the participants in the experimental group were provided with lunch, while those in the control group received gift vouchers worth thirty thousand Korean won. This study was approved by the Institutional Review Board of Chungbuk National University (IRB number: CBNU-202307-HR-0167).
The experiment was conducted for two hours, starting at 10:30 AM on the third week of October 2023 and two weeks later, in the first week of November. Participants in the experimental group arrived at the site one hour before the start of the program using their own transportation and completed the pre-test. After the conclusion of the program at 12:30 PM, they completed the post-test. They revisited two weeks later to participate in the program again and complete the second post-test. Salivary cortisol tests were conducted before and after the experimental treatment, in consideration of the circadian rhythm. The control group maintained their normal daily activities, and the questionnaires and salivary cortisol test were conducted at the same time.
2.2. Study Design
The study was designed as a repeated-measures controlled experiment with a 2×3 mixed study design. Data were collected before the intervention, after the first intervention, and after the second intervention two weeks later. The sample size was determined using the G-Power 3.1.9.7 program based on a set effect size, significance level, and power. With an effect size of 0.25 (medium size in the F-distribution), an α of 0.05, and a 1-β of 0.08, the minimum sample size was calculated as 28. In consideration of potential dropouts and the optimal number of participants for the forest healing program, the sample size was set at 30 in this study [57]. To address group homogeneity, external factors were controlled for by limiting the participants’ area of residence and age, and the gender ratio was adjusted. A total of 30 participants who provided consent were divided into the experimental group (n=15) and control group (n=15) based on the conditions of participation in the experiment. Table 1 shows the experimental study design.
2.3. Experimental Site
The experiment was conducted in Jat-Hyanggi Green Forest in Gapyeong-gun, Gyeonggi-do, which was designated as “Forest of Healing” by the Korea Forest Service in 2017 [58]. JatHyanggi Green Forest is approximately 45km northeast of Seoul, making it a popular destination for urban residents and a suitable location for recruiting study participants among forest visitors (Figure 1) [59]. The forest is equipped with a healing center, forest trails, barrier-free walking paths, meditation spaces, wildflower gardens, and water therapy areas, all designed to utilize environmental elements for health promotion. Situated at an altitude of 450–600 meters on the slopes of Mt. Chukryeong and Mt. Seori, it spans an area of 153 hectares and is home to the largest distribution of pine trees over 90 years old in Korea. The healing center within the forest offers forest healing programs twice daily from March to early December run by forest therapy instructors on-site; the programs are available for reservation on a first-come, first-served basis. This study was conducted with the cooperation of the Healing Forest management organization, and a safe, quiet, and undisturbed walking course suitable for the forest healing meditation program was established in consultation with the on-site forest therapy instructors. The weather was clear during the first program session and cloudy for the second session conducted two weeks later. The average temperature range in Gapyeong-gun during the experiment was between 13.4–18.4ºC.
2.4. Self-Compassion-Based Forest Healing Activities
The self-compassion intervention was modeled after the core meditations and practices of the MBSC program developed by Neff and Germer [49,60,61,62]. The program consists of a series of basic meditation practices aimed at directly training mindfulness and self-compassion in natural environments, targeting general adults with little to no meditation experience (Figure 2).
The meditation practices included movement in the forest (breathing, walking, stretching), staying still, sitting, or lying down and were comprised of affectionate breathing meditation, compassionate movement meditation, mindful walking meditation, and compassion and loving-kindness meditation. Each practice incorporated present-moment awareness with an emphasis on sensory connection with the surrounding natural environment, and participants were guided to connect external sensory experiences to inner experiences. Singing bowls were used to signal the start and end of each activity.
The breathing meditation was guided towards feeling and experiencing the gentle rhythm of the breath, rather than focusing on concentration. The features of nature were linked to loving-kindness. The walking meditation guided participants to notice sensory contact with the natural environment through mindfulness and to fully savor the experience. The movement meditation guided participants to be aware of parts of the body where stress is felt and to allow natural movements to relieve stress.
All practices structurally included guidance on attention and awareness of the body and mind, similar to traditional mindfulness-based meditation training.
The program was facilitated by a researcher registered as a meditation instructor with the Korean Society for Meditation, who has completed leadership courses in MBSR and MBSC programs. The self-compassion meditation training is based on a sense of safety, thus, the author strived to foster a safe environment and atmosphere [63]. Most activities were conducted individually, and participants were encouraged to only engage in minimal conversations during the program.
2.5. Data Measurement
We used a self-report questionnaire to collect demographic factors and the Perceived Stress Scale (PSS), Positive and Negative Affect Schedule (PANAS), Self-Compassion Scale (SCS), and Connection with Nature Scale (CNS) scores. Additionally, salivary cortisol was collected as a physiological indicator of stress levels to measure the stress hormone.
The Korean version of the PSS, developed by Cohen et al. [64] and adapted by Lee Jong-ha et al. [65], was used to measure the degree of stress perceived by participants in their daily lives. This scale is effective in assessing subjective stress perception and interpretation rather than objective stress situations. It consists of two factors: stress factors and stress control factors. Each of the ten items is rated on a five-point Likert scale (0–4). The reliability (Cronbach’s α) of the scale was 0.811 in this study.
The participants’ affective states were measured using the Korean version of the PANAS, developed by Watson et al. [66] and adapted by Park and Lee [67]. This scale consists of two factors, positive affect and negative affect, with higher scores indicating higher negative affect. Each factor contains 10 items for a total of 20 items, and each item is rated on a five-point Likert scale (1–5). The reliability (Cronbach’s α) of the scale was 0.838 in this study.
The participants’ self-compassion was measured using the SCS short form (SCS-SF) developed by Raes et al. [68] and adapted by Park [69]. The SCS measures the degree to which individuals treat themselves with kindness and care when faced with loss, failure, or rejection. Self-compassion consists of six sub-scales: self-kindness, self-judgment, common humanity, isolation, mindfulness, and over-identification. Each of the 12 items is rated on a five-point Likert scale (1–5). The reliability (Cronbach’s α) of the scale was 0.752 in this study.
Connectedness to nature was measured using the scale developed by Mayer and Franz [24] and adapted into Korean by Gim et al. [70]. This scale measures the experiential oneness with the natural world and the participant’s actual affective and experiential connection. Each of the ten items is rated on a five-point Likert scale (1–5). The reliability (Cronbach’s α) of the scale was 0.889 in this study.
As a physiological indicator of stress, cortisol levels were measured by collecting saliva at the same time before and after the program participation. The baseline salivary cortisol was measured between 9:30 AM and 10:00 AM, while post-test salivary cortisol was measured between 12:30 PM and 1:00 PM. As salivary cortisol levels are prone to contamination, participants were restricted from consuming food one hour before saliva collection. Saliva samples were collected by placing a cotton swab under the participant’s tongue to collect approximately 2 ml of saliva, which was then frozen and delivered to the laboratory. Saliva was centrifuged at the laboratory and analyzed using a human cortisol ELISA kit reagent in an ELISA Reader (Biotek Instruments, USA).
2.6. Data Analysis
This study analyzed the effects of a self-compassion-based forest healing meditation program on daily stress management and coping by dividing the participants into the experimental and control groups. Data were analyzed using the SPSS 19.0 Windows version, and statistical significance was set to p < 0.05. Sociodemographic factors were presented as frequency and percentage, and comparisons between the two groups were made using mean and standard deviation and conducting t-tests. The time x group interaction scores for the outcome measures, namely perceived stress, positive and negative affect, self-compassion, connectedness to nature, and cortisol, were analyzed using repeated measures ANOVA. Additionally, changes in the scores within each group were also analyzed using repeated measures ANOVA. Finally, the differences in the mean pre-test and post-test scores of cortisol were analyzed with a paired t-test (SPSS; IBM, Armonk, NY, USA).
Although 30 participants were initially enrolled, two failed to complete the second round of the experiment. Thus, a total of 28 participants were included in the repeated measures analysis.
3. Results
3.1. Participants’ General Characteristics and Comparisons
The participants’ sociodemographic characteristics included gender, age, education level, area of residence, religion, subjective economic status, perceived daily stress, duration of exposure to nature, prior visits to Forest of Healing, prior participation in forest healing programs, prior participation in meditation, and current medication use (Table 3). Most participants were women (93.3%). The majority were aged 50 years or older (n=28, 93.3%), with two aged 40–49 years (6.7%). Education levels included college (n=13, 43.3%), high school (n=12, 40.0%), graduate school (n=4, 13.3%), and middle school (n=1, 3.3%). Twenty (66.7%) participants lived in Gyeonggi-do, while 10 (33.3%) were Seoul residents. Twelve (40.0%) participants had no religion, and 8 (26.7%), 6 (20.0%), and 4 (13.4%) were Catholic, Christian, and Buddhist, respectively.
Regarding subjective economic status, 25 (83.3%), 3 (10.0%), and 2 (6.7%) were middle, low, and high, respectively. The daily stress level was moderate (n=19, 63.3%), high (n=6, 20.0%), or low (n=5, 16.7%). Duration of exposure to nature was ≤ 30 minutes (n=10, 33.3%), 2 hours (n=8, 26.7%), none (n=7, 23.3%), 1 hour (n=4, 13.3%), or ≥ 3 hours (n=1, 3.3%). Of the 30 participants, 21 (70.0%) had never visited a Forest of Healing, and 24 (80.0%) and 20 (66.7%) had never participated in a forest healing program and meditation, respectively.
Table 4 shows the differences in participants’ outcome variables between the two groups at baseline. There were no significant differences in the outcome measures, namely perceived stress (t=1.944, p=0.062), positive and negative affect (t=0.743, p=0.464), self-compassion (t=-0.473, p=0.640), connectedness to nature (t=0.024, p=0.981), and cortisol (t=0.701, p=0.494).
3.2. Perceived Stress
Table 5 shows the results of repeated measures ANOVA for analyzing the differences in the mean perceived stress scores between the experimental (self-compassion based forest therapy program) and control groups. There was a significant time and group interaction effect for perceived stress (F=4.529, p<0.05). The experimental group had significantly reduced perceived stress compared to the control group. There were also significant changes in perceived stress after the intervention compared to the baseline in the experimental group (F=6.213, p<0.01).
Additionally, there was a significant group and time interaction effect (F=4.185, p<0.05) and significant effects in the experimental group (F=3.881, p<0.05) for stressors. For stress moderators, there was no significant group and time interaction effect, but there was a significant change within the experimental group (F=5.143, p<0.05).
3.3. Positive and Negative Affect
Table 6 shows the results of repeated measures ANOVA for analyzing the differences in the mean positive and negative affect scores between the experimental (self-compassion-based forest healing program) and control groups. There was a significant group and time interaction effect for positive and negative affect, confirming that the experimental group had significantly reduced negative affect (F=4.928, p<0.05). In addition, repeated measures ANOVA for within-group changes showed that there were significant changes within the experimental group (F=6.437, p<0.01).
For the factors of positive and negative affect, there was a significant group and time interaction effect for positive affect (F=3.556, p<0.05). While there was no significant group and time interaction effect for negative affect, the experimental group showed significant changes in negative affect (F=5.509, p=0.05).
3.4. Connectedness to Nature
Table 7 shows the results of repeated measures ANOVA for analyzing the differences in the mean connectedness to nature scores between the experimental (self-compassion-based forest healing program) and control groups. There was a significant group and time interaction effect for connectedness to nature (F=3.678, p<0.05). In addition, repeated measures ANOVA for within-group changes showed that there were significant changes within the experimental group (F=6.205, p<0.01).
3.5. Self-Compassion
Table 8 shows the results of repeated measures ANOVA for analyzing the differences in the mean self-compassion scores between the experimental (self-compassion-based forest healing program) and control groups. There was a significant group and time interaction effect for self-compassion (F=4.046, p<0.05). The experimental group showed significantly increased self-compassion over time compared to the control group.
Additionally, the results for each of the six factors of the SCS are as follows. There were significant positive group and time interaction effects for self-judgment (F= 5.154, p<0.05) and common humanity (F=3.692, p<0.05). Within the experimental group, there were significant changes in self-judgment (F=4.764, p<0.05) and common humanity (F=4.029, p<0.05). However, there were no significant between- and within-group effects for self-kindness, isolation, mindfulness, and over-identification.
3.6. Cortisol
Several participants in the experimental group had baseline AM cortisol levels that were outside the normal range (AM cortisol levels were ≤ 1.00 ng, indicating a physiological state of fatigue close to lethargy). Therefore, the data from five participants were excluded from the repeated measures ANOVA for cortisol due to abnormal values, and nine individual data points were excluded from the comparison of pre-test and post-test values.
Table 9 shows the results of repeated measures ANOVA for analyzing the differences in the mean cortisol levels between the experimental (self-compassion-based forest healing program) and control groups. There was no significant group and time interaction effect for cortisol; thus, a paired t-test was performed to analyze the changes in cortisol levels between the pre-test and post-test (Table 10). The experimental group showed a significant reduction in cortisol levels after participating in the program compared to the baseline (t=2.753, p=0.05).
4. Discussion
This study hypothesized and validated the effectiveness of a self-compassion-based forest healing intervention in alleviating daily stress and enhancing coping resources by evaluating the psychological and physiological changes in participants. Participants’ psychological and physiological changes were assessed before the program intervention, after one session of intervention, and after the second session of intervention two weeks later. The results showed that perceived stress, positive and negative affect, connectedness to nature, and self-compassion significantly changed over time in the experimental group compared to the control group. Salivary cortisol was measured as a physiological marker, and it significantly changed within the group after the intervention compared to the baseline. These results indicate that a short-duration (two-hour) self-compassion-based forest healing intervention provided over a two-week interval can serve as an effective resource for managing daily stress and building resources in adults.
Regarding the impact on stress as proposed in the initial hypothesis, the participants in the experimental group exhibited a significant reduction in perceived stress over time compared to the control group following the self-compassion-based forest healing program. For the specific factors of perceived stress, changes in perception of stressors also decreased significantly in comparison to the control group, while stress coping factors increased significantly within the group. Although no changes were observed in salivary cortisol levels between groups, the experimental group showed a significant change in cortisol levels after the intervention compared to the baseline. These findings align with the findings of Kim et al. [71] who investigated the effects of interventions combining forest healing and horticultural activities. In both studies, there were no significant changes in cortisol levels between groups, but there were significant changes within the experimental group after the intervention compared to the baseline. Additionally, positive and negative affect—another indicator of stress relief—was significantly positively changed in the experimental group over time compared to the control group. Specifically, positive affect increased significantly in the experimental groups compared to the control group, while negative affect decreased significantly within the group. These results are in line with the findings of a systematic review by Corazon et al. [14], which highlighted that positive affect plays a crucial role in stress recovery in nature-based interventions.
In summary, the self-compassion-based forest healing meditation activities significantly improved perceived stress and positive affect over time and reduced salivary cortisol, a physiological indicator, thereby supporting Hypothesis 1. Perceived stress is the most consistently evidenced stress-related factor in the literature [13]. Although it is a subjective self-reported health-related parameter, it shows significant overlap between chronic health conditions and physician-based diagnoses, thus providing useful indicators for public health interventions [72].
Regarding the second hypothesis, connectedness to nature and self-compassion, both of which were evaluated as potential resources for coping with stress, were significantly increased incrementally over time in the experimental group compared to the control group. This is consistent with the results of McEwan et al. [46], where a two-hour intervention combining forest bathing and compassion training significantly changed connectedness to nature and self-compassion. In a similar study addressing self-compassion and connectedness with nature based on natural environments, Djernis et al. [52] evaluated the effects of a five-day residential mindfulness training modeled on MBSR in a natural environment. Their results showed no significant increase in stress, self-compassion, and connectedness with nature immediately after the program intervention, but significant changes were observed at the three-month follow-up, suggesting that the effects of the intervention may manifest over time [52].
Meditation is a key element of forest healing interventions and the most widely used mental intervention therapy in Korea [72]. There have been numerous empirical studies on the effects of nature-based meditation intervention activities and programs to address mental health issues and stress [52,74]. However, the impact of forest healing activities that explicitly emphasize self-compassion has not been sufficiently reported. Thus, the psychological and physiological changes revealed in this study can provide a basis for applying self-compassion interventions in forest healing activities aimed at managing everyday stress in adults.
5. Conclusions
This study confirmed that a short self-compassion-based forest therapy program is effective in managing stress and enhancing personal coping resources such as connectedness to nature and self-compassion in modern individuals. Therefore, self-compassion-based forest therapy programs can serve as a valuable and accessible public health intervention for managing mental health problems induced by daily stress in adults. The effectiveness of these interventions can be progressively amplified when participants engage in two-hour sessions at two-week intervals. In the context of today’s society, intermittent visits may be more practical than continuous and long-term visits. Future studies should explore the impact of different visit frequencies on stress management and coping to provide valuable insights for developing targeted health intervention strategies.
This study has a few limitations. First, the pre-test data for the experimental group was collected at the Forest of Healing site, potentially increasing the risk of including the effect of exposure to nature in the pre-test values. Therefore, the timing for pre-test data collection should be carefully considered for an accurate assessment of effects. Second, although a preliminary experiment was conducted after surveying the site’s resources before administering the forest healing intervention, the site’s abundant natural elements could have not been used adequately in practice. Third, the program was executed following a pre-developed instruction manual, but there were adaptations made in response to the field situation. Fourth, some courses were adjusted within the Forest of Healing, which would have caused variations in the natural environment. Fifth, as the group size of 15 participants posed certain limitations in facilitating immersive experiences and ensuring personal space, future studies should consider smaller group sizes.
Author Contributions
Conceptualization, S.-Y.Y. and W.-S.S.; methodology, S.-Y.Y. and W.-S.S.; investigation, S.-Y.Y. and M.-M.L.; data curation, S.-Y.Y.; writing—original draft preparation, S.-Y.Y.; writing—review and editing, S.-Y.Y. and W.-S.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Chungbuk National University (IRB number: CBNU-202307-HR-0167).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
References
- Piazza, J.R.; Charles, S.T.; Sliwinski, M.J.; Mogle, J.; Almeida, D.M. Affective Reactivity to Daily Stressors and Long-Term Risk of Reporting a Chronic Physical Health Condition. Ann. Behav. Med. 2013, 45, 110–120. [CrossRef]
- Almeida, D.M. Resilience and Vulnerability to Daily Stressors Assessed via Diary Methods. Curr. Dir. Psychol. Sci. 2005, 14, 64–68. [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984.
- Cohen, S.; Hamrick, N.M.S.; Rodriguez, M.S.; Feldman, P.J.; Rabin, B.S.; Manuck, S.B. The stability of and intercorrelations among cardiovascular, immune, endocrine, and psychological reactivity. Ann. Behav. Med. 2000, 22, 171–179. [CrossRef]
- Korea Disease Control and Prevention Agency. Community Health Survey. Available online: https://chs.kdca.go.kr/chs/stats/statsMain.do (accessed on 02 March 2024).
- National Center for Mental Health. 2022 National Mental Health Knowledge and Attitude Survey. Available online: https://www.ncmh.go.kr/metalhealth/board/boardView.do?no=9219&fno=106&gubun_no=10&menu_cd=04_02_00_05&bn=newsView&bno=&pageIndex=1&search_item=&search_content=# (accessed on 2 March 2024).
- Beames, J.R.; Kikas, K.; Werner-Seidler, A. Prevention and early intervention of depression in young people: an integrated narrative review of affective awareness and Ecological Momentary Assessment. BMC Psychol. 2021, 9, 113.
- Pretty, J.; Barton, J. Nature-Based Interventions and Mind–Body Interventions: Saving Public Health Costs Whilst Increasing Life Satisfaction and Happiness. Int. J. Environ. Res. Public Heal. 2020, 17, 7769. [CrossRef]
- Townsend, M.; Henderson-Wilson, C.; Ramkissoon, H.; Werasuriya, R. Therapeutic landscapes, restorative environments, place attachment, and well-being. In Oxford Textbook of Nature and Public Health: The Role of Nature in Improving the Health of a Population; Van den Bosch, M.; Bird, W.; Eds.; Oxford University Press: Oxford, UK, 2018; pp. 57-62.
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989.
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [CrossRef]
- Jimenez, M.P.; DeVille, N.V.; Elliott, E.G.; Schiff, J.E.; Wilt, G.E.; Hart, J.E.; James, P. Associations between Nature Exposure and Health: A Review of the Evidence. Int. J. Environ. Res. Public Heal. 2021, 18, 4790. [CrossRef]
- Shuda, Q.; Bougoulias, M.E.; Kass, R. Effect of nature exposure on perceived and physiologic stress: A systematic review. Complement. Ther. Med. 2020, 53, 102514. [CrossRef]
- Corazon, S.S.; Sidenius, U.; Poulsen, D.V.; Gramkow, M.C.; Stigsdotter, U.K. Psycho-Physiological Stress Recovery in Outdoor Nature-Based Interventions: A Systematic Review of the Past Eight Years of Research. Int. J. Environ. Res. Public Heal. 2019, 16, 1711. [CrossRef]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The benefits of nature experience: Improved affect and cognition. Landsc. Urban Plan. 2015, 138, 41–50. [CrossRef]
- Neill, C.; Gerard, J.; Arbuthnott, K.D. Nature contact and mood benefits: contact duration and mood type. J. Posit. Psychol. 2019, 14, 756–767. [CrossRef]
- Fredrickson, B.L. The broaden–and–build theory of positive emotions. Philos. Trans. R. Soc. London B. Biol. Sci. 2004, 359, 1367–1377.
- Conway, A.M.; Tugade, M.M.; Catalino, L.I.; Fredrickson, B.L. The broaden-and-build theory of positive emotions: Form, function and mechanisms. In The Oxford Handbook of Happiness, David, S.A; Boniwell, I.; Conley Ayers, A.; Eds.; Oxford University Press: Oxford, UK, 2013; pp. 17-34.
- McMahan, E.A.; Estes, D. The effect of contact with natural environments on positive and negative affect: A meta-analysis. J. Posit. Psychol. 2015, 10, 507–519. [CrossRef]
- Shanahan, D.F.; Astell–Burt, T.; Barber, E.A.; Brymer, E.; Cox, D.T.C.; Dean, J.; Depledge, M.; Fuller, R.A.; Hartig, T.; Irvine, K.N.; et al. Nature–Based Interventions for Improving Health and Wellbeing: The Purpose, the People and the Outcomes. Sports 2019, 7, 141. [CrossRef]
- Huynh, T.; Torquati, J.C. Examining connection to nature and mindfulness at promoting psychological well-being. J. Environ. Psychol. 2019, 66, 101370. [CrossRef]
- Mayer, F.S.; Frantz, C.M.; Bruehlman-Senecal, E.; Dolliver, K. Why is nature beneficial? The role of connectedness to nature. Environ. Behav. 2009, 41, 607-643.
- Lee, S.H. The realization of the spirit of positive psychology through natural environments: Positive experience. Korean J. Psychol.: General. 2014, 33(1), 51–79.
- Mayer, F.S.; Frantz, C.M. The connectedness to nature scale: A measure of individuals’ feeling in community with nature. J. Environ. Psychol. 2004, 24, 503–515. [CrossRef]
- Mantler, A.; Logan, A.C. Natural environments and mental health. Adv. Integr. Med. 2015, 2, 5–12. [CrossRef]
- Martin, L.; White, M.P.; Hunt, A.; Richardson, M.; Pahl, S.; Burt, J. Nature contact, nature connectedness and associations with health, wellbeing and pro-environmental behaviours. J. Environ. Psychol. 2020, 68, 101389. [CrossRef]
- Capaldi, C.A.; Dopko, R.L.; Zelenski, J.M. The relationship between nature connectedness and happiness: a meta-analysis. Front. Psychol. 2014, 5, 976. [CrossRef]
- Pritchard, A.; Richardson, M.; Sheffield, D.; McEwan, K. The Relationship Between Nature Connectedness and Eudaimonic Well-Being: A Meta-analysis. J. Happiness Stud. 2019, 21, 1145–1167. [CrossRef]
- Bakir-Demir, T.; Berument, S.K.; Akkaya, S. Nature connectedness boosts the bright side of emotion regulation, which in turn reduces stress. J. Environ. Psychol. 2021, 76, 101642. [CrossRef]
- Condon, P.; Makransky, J. Compassion and Skillful Means: Cultural Adaptation, Psychological Science, and Creative Responsiveness. Mindfulness 2022, 1–11. [CrossRef]
- Strauss, C.; Taylor, B.L.; Gu, J.; Kuyken, W.; Baer, R.; Jones, F.; Cavanagh, K. What is compassion and how can we measure it? A review of definitions and measures. Clin. Psychol. Rev. 2016, 47, 15–27. [CrossRef]
- Zessin, U.; Dickhäuser, O.; Garbade, S. The Relationship Between Self-Compassion and Well-Being: A Meta-Analysis. Appl. Psychol. Heal. Well-Being 2015, 7, 340–364. [CrossRef]
- Neff, K.D.; Dahm, K.A. Self-compassion: What it is, what it does, and how it relates to mindfulness. In Handbook of Mindfulness and Self-regulation; Ostafin, B.D.; Robinson, M.D.; Meier, B.P.; Eds.; Springer: New York, NY, 2015; pp. 121-137.
- McGehee, P.; Germer, C.; Neff, K. Core values in mindful self-compassion. In Practitioner’s Guide to Ethics and Mindfulness-based Interventions; Monteiro, L.; Compson, J.F.; Musten, F.; Eds.; Springer: Cham, Switzerland, 2017; 279–293.
- Trembath, D.; Gurm, M.; Scheerer, N.E.; Trevisan, D.A.; Paynter, J.; Bohadana, G.; Roberts, J.; Iarocci, G. Systematic review of factors that may influence the outcomes and generalizability of parent-mediated interventions for young children with autism spectrum disorder. Autism Res. 2019, 12, 1304–1321. [CrossRef]
- Kim, C.; Ko, H. The impact of self-compassion on mental health, sleep, quality of life and life satisfaction among older adults. Geriatr. Nurs. 2018, 39, 623–628. [CrossRef]
- Murfield, J.; Moyle, W.; Jones, C.; O'Donovan, A. Self-Compassion, Health Outcomes, and Family Carers of Older Adults: An Integrative Review. Clin. Gerontol. 2020, 43, 485–498. [CrossRef]
- Han, A.; Kim, T.H. Effects of Self-Compassion Interventions on Reducing Depressive Symptoms, Anxiety, and Stress: A Meta-Analysis. Mindfulness 2023, 14, 1553–1581. [CrossRef]
- Ferrari, M.; Hunt, C.; Harrysunker, A.; Abbott, M.J.; Beath, A.P.; Einstein, D.A. Self-Compassion Interventions and Psychosocial Outcomes: a Meta-Analysis of RCTs. Mindfulness 2019, 10, 1455–1473. [CrossRef]
- Neff, K.D.; Kirkpatrick, K.L.; Rude, S.S. Self-compassion and adaptive psychological functioning. J. Res. Pers. 2007, 41, 139–154. [CrossRef]
- Homan, K.J.; Sirois, F.M. Self-compassion and physical health: Exploring the roles of perceived stress and health-promoting behaviors. Heal. Psychol. Open 2017, 4. [CrossRef]
- Sirois, F.M.; Kitner, R.; Hirsch, J.K. Self-compassion, affect, and health-promoting behaviors. Health Psychol. 2015, 34, 661.
- Rahimi-Ardabili, H.; Reynolds, R.; Vartanian, L.R.; McLeod, L.V.D.; Zwar, N. A Systematic Review of the Efficacy of Interventions that Aim to Increase Self-Compassion on Nutrition Habits, Eating Behaviours, Body Weight and Body Image. Mindfulness 2018, 9, 388–400. [CrossRef]
- Ewert, C.; Vater, A.; Schröder-Abé, M. Self-Compassion and Coping: a Meta-Analysis. Mindfulness 2021, 12, 1063–1077. [CrossRef]
- Chishima, Y.; Mizuno, M.; Sugawara, D.; Miyagawa, Y. The Influence of Self-Compassion on Cognitive Appraisals and Coping with Stressful Events. Mindfulness 2018, 9, 1907–1915. [CrossRef]
- McEwan, K.; Giles, D.; Clarke, F.J.; Kotera, Y.; Evans, G.; Terebenina, O.; Minou, L.; Teeling, C.; Basran, J.; Wood, W.; et al. A Pragmatic Controlled Trial of Forest Bathing Compared with Compassionate Mind Training in the UK: Impacts on Self-Reported Wellbeing and Heart Rate Variability. Sustainability 2021, 13, 1380. [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144-156.
- Kabat-Zinn, J. Full Catastrophe Living, Revised Edition: How to Cope with Stress, Pain and Illness using Mindfulness Meditation; Hachette UK: London, UK, 2013.
- Neff, K.D. Self-Compassion: Theory, Method, Research, and Intervention. Annu. Rev. Psychol. 2023, 74, 193–218. [CrossRef]
- Wilson, A.C.; Mackintosh, K.; Power, K.; Chan, S.W.Y. Effectiveness of Self-Compassion Related Therapies: a Systematic Review and Meta-analysis. Mindfulness 2018, 10, 979–995. [CrossRef]
- Bergen-Cico, D.; Possemato, K.; Cheon, S. Examining the Efficacy of a Brief Mindfulness-Based Stress Reduction (Brief MBSR) Program on Psychological Health. J. Am. Coll. Heal. 2013, 61, 348–360. [CrossRef]
- Djernis, D.; O’toole, M.S.; Fjorback, L.O.; Svenningsen, H.; Mehlsen, M.Y.; Stigsdotter, U.K.; Dahlgaard, J. A Short Mindfulness Retreat for Students to Reduce Stress and Promote Self-Compassion: Pilot Randomised Controlled Trial Exploring Both an Indoor and a Natural Outdoor Retreat Setting. Healthcare 2021, 9, 910. [CrossRef]
- Shin, W.S.; Lee, J. (2020). Forest therapy. In Outdoor Therapies: An Introduction to Practices, Possibilities, and Critical Perspectives; Harper, N.J.; Dobud, W.W.; Eds.; Routledge: New York, NY, pp. 159-172.
- Korea Forest Welfare Institute. Available online: https://www.fowi.or.kr/user/main/main.do (accessed on 24 February 2024).
- Korea Forest Welfare Institute. Available online: https://www.fowi.or.kr/user/contents/contentsView.do?cntntsId=43 (accessed on 24 February 2024).
- Park, S.; Kim, S.; Kim, G.; Choi, Y.; Kim, E.; Paek, D. Evidence-Based Status of Forest Healing Program in South Korea. Int. J. Environ. Res. Public Heal. 2021, 18, 10368. [CrossRef]
- Yeo, S.Y.; Shin, W.S. Perceptions and needs of forest therapy experts regarding forest therapy meditation intervention. J. Life. 2023, 27, 25-39.
- Korea Forest Service. Available online: https://www.forest.go.kr/kfsweb/kfi/kfs/cms/cmsView.do?mn=NKFS_03_06_02_01&cmsId=FC_001570 (accessed on 17 March 2024).
- Gyeonggi Jat Hyanggi Green Forest. Available online: https://forest.gg.go.kr/forest/10311 (accessed on 15 March 2024).
- Neff, K. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude Toward Oneself. Self Identit- 2003, 2, 85–101. [CrossRef]
- Germer, C.; Neff, K. Mindful self-compassion (MSC). In Handbook of Mindfulness-based Programmes: Mindfulness Interventions from Education to Health and Therapy; Ivtzan, I.; Ed.; Routledge: Abingdon, UK, 2019; pp. 357-367.
- Germer, C.K.; Neff, K.D. Self-compassion in clinical practice. J. Clin. Psychol. 2013, 69, 856-867.
- Germer, C.; Germer, C.K.; Neff, K. Teaching the Mindful Self-compassion Program: A Guide for Professionals. Guilford Press, New York, NY, 2019.
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Heal. Soc. Behav. 1983, 24, 385–96. [CrossRef]
- Lee, J.H.; Shin, C.M.; Ko, Y.H.; Im, J.H.; Cho, S.H.; Kim, S.H.; Jung, I.K.; Han, CS. The reliability and validity studies of the Korean Version of the Perceived Stress Scale. Korean J. Psychosom. Med. 2012, 20, 127-134.
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063.
- Park, H.S.; Lee, J.M. A Validation Study of Korean Version of PANAS-Revised. Korean J. Psychol. Gen. 2016, 35, 617. [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [CrossRef]
- Park, I. The Effects of Self-compassion Treatment Using Movie on State Self-compassion, State Anxiety and Emotional Reactions: For College Students with Speech Anxiety. Master’s Thesis, Catholic University of Korea, 2014.
- Gim, W.-S.; Lee, M.-H.; Kim, K.-H. A Validation Study of the Korean Version of the Connectedness to Nature Scale. J. People, Plants, Environ. 2019, 22, 621–628. [CrossRef]
- Kim, H.R.; Oh, W.S.; Kim, J.G.; Shin, W.S. The influence of urban gardening activities on participants’ perceived restorativeness, resilience, sense of community and stress. In Healthcare. 2023, 11, 1664.
- Cohen, S.; Rodriguez, M.S. Pathways linking affective disturbances and physical disorders. Health Psychol. 1995, 14, 374.
- Lee, E.D.; Park, S.J.; Yoo, R.H.; Hong, S.J. Analysis on the activity contents of forest healing programs in Korea. Journal KIFR 2011, 15, 101-109.
- Djernis, D.; Lerstrup, I.; Poulsen, D.; Stigsdotter, U.; Dahlgaard, J.; O’Toole, M. A Systematic Review and Meta-Analysis of Nature-Based Mindfulness: Effects of Moving Mindfulness Training into an Outdoor Natural Setting. Int. J. Environ. Res. Public Health 2019, 16, 3202. [CrossRef]
Figure 1.
Location of Forest of Healing and the management center.

Figure 2.
Reference for forest healing activities.
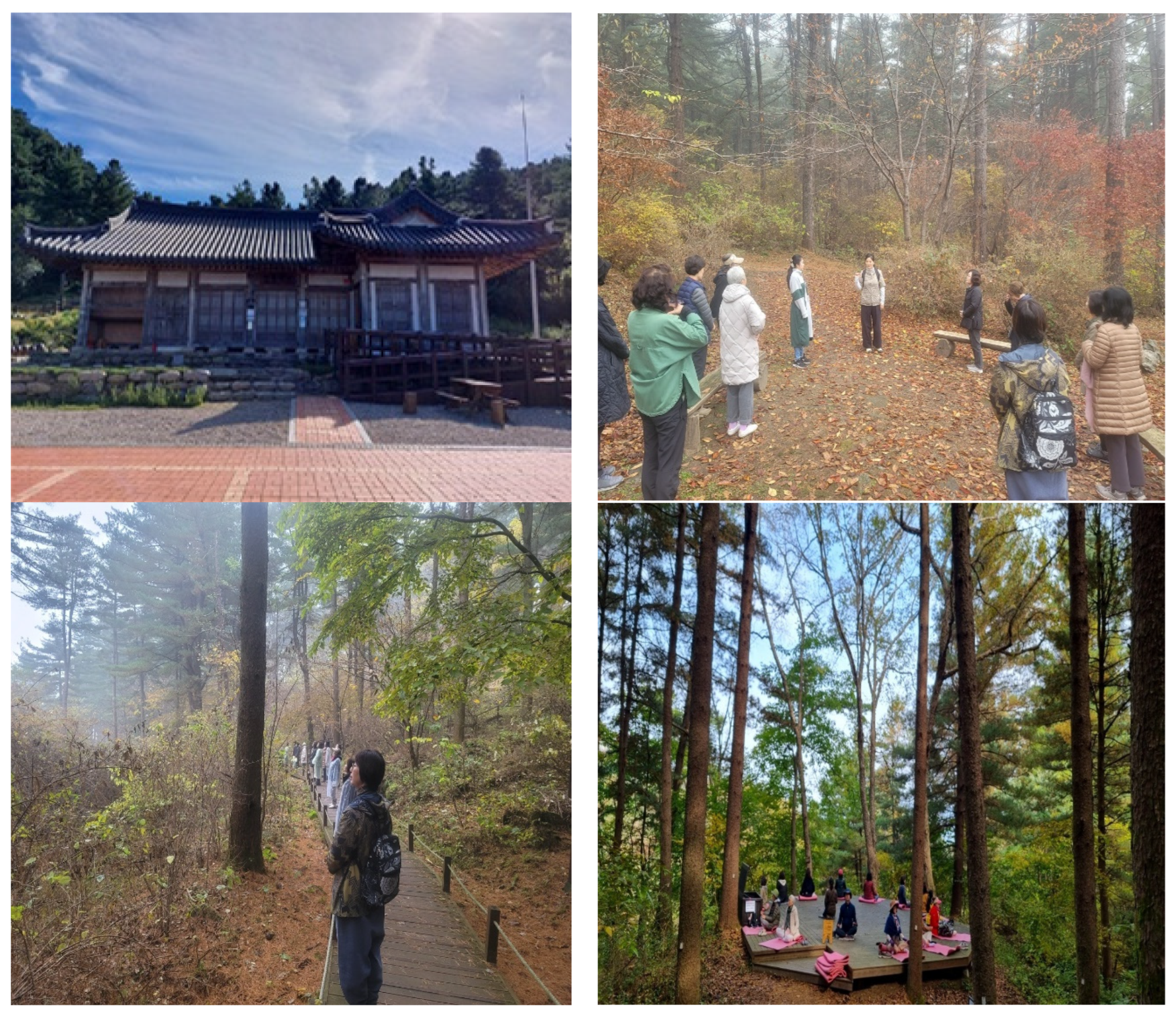

Table 1.
Basic study design for program validation.
| Group | Pre-test | Treatment | 1st post-test | Pre-test | Treatment | 2nd post-test |
|---|---|---|---|---|---|---|
| Experimental group (n=15) | O1 | T1 | O2 | O1-1 | T2 | O3 |
| Control group (n=15) | O1 | O2 | O1-1 | O3 |
O1-1: Only salivary test.
Table 2.
Composition of self-compassion-based forest meditation therapy program.
| Step | Time | Objective | Activities | Description |
|---|---|---|---|---|
| Opening | 10 min | Safety and reliability | Introduction | Greeting the facilitator and participants Present-moment awareness Introduction to the program’s purpose and activities Confirmation of motivation and guidance on participation rules Health and safety check for participants |
| Forest therapy activity | 20 min | Directly experiencing and gently mellowing the body | Compassionate movement meditation | Present-moment awareness Gentle stretching Connecting breath and movement Awareness of body sensations and feelings Checking the state of mind (Excessive effort vs. physical care) |
| 10 min | Walking through the forest trail | Quietly, slowly, freely | ||
| 20 min | Awareness of affective feelings | Affectionate breathing meditation | Comfortable and supportive posture Present-moment awareness Awareness of body and breath sensations Using comforting touch Gently redirecting attention Connection with simply being |
|
| 25 min | Awareness of external senses and internal experiences | Mindful walking meditation | Paying attention to the surrounding environment through external senses Savoring pleasant feelings If discomfort is felt, stop and take deep breaths, provide comforting touch |
|
| 25 min | Connect with loving-kindness and compassion | Compassion meditation. | Comfortable and supportive posture Present-moment awareness Self-contact through internal bodily sensations Connecting with loving-kindness through natural imagery Exchanging loving breaths Providing compassionate phrases Providing compassionate movements |
|
| Wrap-up | 10 | Recognizing the status of mind and body | Active listening | Briefly sharing experiences |
Table 3.
Participants’ general characteristics (N=30).
| Category | Class | Frequency | Percentage (%) |
|---|---|---|---|
| Gender | Men | 2 | 6.7 |
| Women | 28 | 93.3 | |
| Age (years) | 40–49 | 2 | 6.7 |
| 50–59 | 6 | 20.0 | |
| 60–69 | 22 | 73.3 | |
| Education | Middle school or less | 1 | 3.3 |
| High school | 12 | 40.0 | |
| College | 13 | 43.3 | |
| Graduate school or more | 4 | 13.3 | |
| Area of residence | Seoul | 10 | 33.3 |
| Gyeonggi-do Gapyeong (2), Goyang (10), Guri (1), Suwon (1), Anyang (4), Yongin (1), Paju (1) |
20 | 66.7 | |
| Religion | None | 12 | 40.0 |
| Christian | 6 | 20.0 | |
| Buddhist | 4 | 13.3 | |
| Catholic | 8 | 26.7 | |
| Subjective economic status | High | 2 | 6.7 |
| Middle | 25 | 83.3 | |
| Low | 3 | 10.0 | |
| Perceived daily stress | High | 6 | 20.0 |
| Moderate | 19 | 63.3 | |
| Low | 5 | 16.7 | |
| Duration of exposure to nature | None | 7 | 23.3 |
| ≤ 30 minutes | 10 | 33.3 | |
| 1 hour | 4 | 13.3 | |
| 2 hours | 8 | 26.7 | |
| ≥ 3 hours | 1 | 3.3 | |
| Prior visit to a Forest of Healing | No | 21 | 70.0 |
| Yes | 9 | 30.0 | |
| Prior participation in forest healing program | None | 24 | 80.0 |
| 1 time | 2 | 7.7 | |
| ≥ 2 times | 2 | 7.7 | |
| Prior participation in meditation | None | 20 | 66.7 |
| 1–2 times | 5 | 16.7 | |
| ≥ 3 times | 5 | 16.7 | |
| Current medications | None | 17 | 56.7 |
| Yes Hypertension (3), Hyperlipidemia (2), Thyroid (2), Osteoporosis (1), Neurology (1), Insomnia (1), Acute cerebral infarction (1), Lung cancer (1), other (1) |
13 | 43.3 |
Table 4.
Comparison of groups at the baseline.
| Group | N | M(SD) | t (p) | |
|---|---|---|---|---|
| PSS | Experimental Group | 15 | 1.97 (0.44) | 1.944 (0.062) |
| Control Group | 15 | 1.63 (0.51) | ||
| PANAS | Experimental Group | 15 | 2.70 (0.52) | 0.743 (0.464) |
| Control Group | 15 | 2.56 (0.51) | ||
| CNS | Experimental Group | 15 | 3.37 (0.99) | 0.024 (0.981) |
| Control Group | 15 | 3.36 (0.43) | ||
| SCS | Experimental Group | 15 | 3.40 (0.61) | -0.473 (0.640) |
| Control Group | 15 | 3.49 (0.39) | ||
| Cortisol | Experimental Group | 15 | 4.77 (8.57) | 0.701 (0.494) |
| Control Group | 15 | 3.17 (1.88) |
PSS: Perceived Stress Scale. PANAS: Positive and Negative Affect Scale. CNS: Connectedness to Nature Scale. SCS: Self-Compassion Scale.
Table 5.
Changes and differences in perceived stress between groups and within groups.
| Group | Pre-test | Post-test 1 | Post-test 2 | Time | Group x time | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||||
| PSS |
Experimental group (n=13) |
19.15a | 1.34 | 16.69 | 1.30 | 14.84b | 1.26 | F=6.213, p=0.007** | F=4.529, p=0.023* =0.148 |
|
| Control group (n=15) |
16.26 | 1.24 | 15.93 | 1.21 | 16.13 | 1.17 | F=0.104, p=0.820 | |||
| Factors | Stressors | Experimental group |
10.23 | 3.65 | 9.15 | 3.51 | 7.77 | 2.05 | F=3.881, p=0.035* | F=4.185, p=0.029* =0.139 |
| Control group |
7.20 | 3.76 | 7.53 | 3.66 | 7.73 | 3.99 | F=0.425, p=0.567 | |||
| Moderators | Experimental group |
8.92 | 1.66 | 7.54 | 1.80 | 7.08 | 2.36 | F=5.143, p=0.014* | F=.104, p=0.820 |
|
| Control group |
9.07 | 2.89 | 8.40 | 2.29 | 8.40 | 2.64 | F=1.256, p=0.300 | |||
*p<.05, **p<.01. a<b (p<0.05). PSS: Perceived Stress Scale.
Table 6.
Changes and differences of positive and negative affect.
| Group | Pre-test | Post-test 1 | Post-test 2 | Time | Group x time | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||||
| PANAS | ExperimentalGroup | 54.46 | 10.40 | 45.15 | 8.36 | 43.77 | 9.08 | F=6.437, p=0.007** | F=4.928 p=0.011* =0.159 |
|
| Control Group | 51.20 | 10.23 | 49.93 | 10.98 | 51.67 | 7.77 | F=0.424, p=0.659 | |||
| Factors | Positive affect | Experimental Group | 35.00 | 6.92 | 31.15 | 6.97 | 29.85 | 7.24 | F=3.378, p=0.051 | F=3.556 p=0.036* =0.120 |
| Control Group | 32.33 | 6.30 | 33.27 | 7.35 | 33.60 | 6.03 | F=0.385, p=0.684 | |||
| Negative affect | Experimental Group | 19.46a | 9.27 | 14.00b | 4.86 | 13.92 | 4.53 | F=5.509, p=0.024* | F=1.905 p=0.172 |
|
| Control Group | 18.86 | 7.93 | 16.67 | 6.26 | 18.07 | 6.28 | F=0.954, p=0.370 | |||
*p<.05, a<b (p<0.05). PANAS: Positive and Negative Affect Scale.
Table 7.
Changes and differences in connectedness to nature.
| Group | Pre-test | Post-test 1 | Post-test 2 | Time | Group x time | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||||
| Connectedness to nature | Experimental Group | 35.30a | 8.10 | 39.46b | 8.43 | 42.69c | 6.13 | F=6.205 p=0.007** |
F=3.678 p=0.042* =0.124 |
|
| Control Group | 33.60 | 4.36 | 35.13 | 6.05 | 34.93 | 6.24 | F=1.340 p=0.278 |
|||
*p<.05, **p<.01. a<b, a<c (p<0.05).
Table 8.
Changes and differences in self-compassion.
| Group | Pre-test | Post-test 1 | Post-test 2 | Time | Group x time | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |||||
| Self-compassion | ExperimentalGroup | 42.00 | 7.15 | 42.23 | 5.56 | 44.46 | 5.19 | F=1.751, p=0.195 | F=4.046 p=0.023* =0.135 |
|
| Control Group |
41.87 | 4.71 | 41.93 | 4.55 | 40.53 | 4.64 | F=3.171, p=0.057 | |||
| Factors | Self-kindness | Experimental Group | 6.23 | 1.53 | 5.92 | 1.80 | 6.61 | 1.50 | F=0.934, p=0.407 | F=3.005 p=0.058 |
| Control Group |
5.53 | 1.50 | 6.07 | 1.16 | 5.33 | 1.35 | F=2.783, p=0.079 | |||
| Self-judgment | Experimental Group | 8.23a | 1.59 | 9.07b | 1.18 | 9.15 | 1.40 | F=4.764, p=0.043* | F=5.154 p=0.020* =0.165 |
|
| Control Group |
9.07 | 1.16 | 9.13 | 1.30 | 8.86 | 1.64 | F=1.328, p=0.281 | |||
| Common humanity | Experimental Group | 5.92 | 1.12 | 4.92 | 1.66 | 6.00 | 1.22 | F=4.029, p=0.031* | F=3.692 p=0.032* =0.124 |
|
| Control Group |
4.67 | 1.29 | 5.00 | 1.07 | 4.80 | 1.56 | F=0.425, p=0.557 | |||
| Isolation | Experimental Group | 7.69 | 1.49 | 7.92 | 1.80 | 7.54 | 1.71 | F=0.412, p=0.667 | F=0.941, p=0.378 |
|
| Control Group |
8.00 | 1.56 | 7.40 | 1.80 | 7.33 | 2.09 | F=1.441, p=0.255 | |||
| Mindfulness | Experimental Group | 6.53 | 1.45 | 6.23 | 1.74 | 7.30 | 1.49 | F=2.215, p=0.131 | F=1.924, p=0.156 |
|
| Control Group |
6.07 | 1.39 | 6.07 | 1.58 | 5.80 | 2.00 | F=0.199, p=0.820 | |||
| Over-identification | Experimental Group | 7.38 | 1.89 | 8.15 | 1.34 | 7.85 | 1.99 | F=1.295, p=0.292 | F=1.874 p=0.164 |
|
| Control Group |
8.53 | 1.50 | 8.27 | 1.87 | 8.40 | 2.06 | F=0.463, p=0.634 | |||
*p<.05, a<b (p<0.1).
Table 9.
Changes and differences in cortisol.
| Group | Pre-test | Post-test 1 | Post-test 2 | Time | Group x time | ||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||||
| Cortisol | Experimental group(n=8) | 7.86 | 11.09 | 3.60 | 6.91 | 1.29 | 0.50 | F=2.730 p=0.133 |
F=2.897 p=0.089 |
| Control group (n=15) |
3.18 | 1.88 | 2.13 | 1.49 | 1.83 | 0.93 | F=3.048 p=0.086 |
||
5 people with outliers that deviate from the normal morning cortisol levels (pretest) were removed.
Table 10.
Changes in cortisol levels across pre-test and post-test.
| Group | Pre-test | Post-test | t | p | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Cortisol | Experimental group(n=21) | 4.44 | 7.19 | 2.13 | 4.27 | 2.753 | 0.012* |
| Control group (n=15) |
3.18 | 1.87 | 2.13 | 1.49 | 1.444 | 0.171 | |
7 outliers that deviate from the normal morning cortisol levels were removed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



