
Submitted:
18 May 2024
Posted:
20 May 2024
You are already at the latest version
Abstract
Pulmonary hypertension (PH) is a severe and chronic disease characterized by increased pulmonary vascular resistance and remodeling often precipitating right-sided heart dysfunction and death. Although the condition is progressive and incurable, current therapies for the disease focus on multiple different drugs and general supportive therapies to manage symptoms and prolong survival, ranging from medications more specific to pulmonary arterial hypertension (PAH) to exercise training. Moreover, there are multiple studies exploring novel experimental drugs and therapies including unique neurostimulation, to help better manage the disease. Here we provide a narrative review focusing on current PH treatments that target multiple underlying biochemical mechanisms, including but not limited to imbalances in vasoconstrictor-vasodilator and autonomic nervous system function, inflammation, and bone morphogenic protein (BMP) signaling. We also focus on the potential of novel therapies for managing PH, focusing on multiple types of neu-rostimulation including acupuncture. Lastly, we also touch upon the disease’s different subgroups, clinical presentations and prognosis, diagnostics, demographics, and cost.
Keywords:
pulmonary hypertension (PH)
; pulmonary arterial hypertension (PAH)
; chronic thromboembolic pulmonary hypertension (CTEPH)
; cardiac dysfunction
; neurostimulation and electroacupuncture
; vascular remodeling
; alveolar hypoxia
1. Introduction
Pulmonary hypertension (PH) is a progressive, incurable clinical condition defined hemodynamically by a mean pulmonary arterial pressure (mPAP) ≥ 20 mmHg at rest as measured by right heart catheterization (RHC) [1,2]. In accordance with guidelines of the European Society of Cardiology and European Respiratory Society, PH is generally classified into five etiological groups: pulmonary arterial hypertension (PAH; Group 1), PH due to left heart disease (PH-LHD; Group 2), PH due to lung disease or hypoxia (Group 3), PH due to chronic thromboembolic disease (CTEPH) or other pulmonary artery obstructions (Group 4), and PH with unclear or multifactorial mechanisms (Group 5) [1]. There are multiple subtypes within each group as listed below in Table 1. In this paper, we focus particularly on the broader groups, including Group 1 and Group 3.
PH patients may also be categorized into different groups based on their functional class (FC): the World Health Organization (WHO) for instance separates PH patients into FC I (least severe) through IV (most severe) based on limitations and symptoms that arise during physical activity (dyspnea, fatigue, chest pain, syncope), as well as comfort at rest [1]. Defining the functional classes is important in determining initial treatment plans and defining goals in stages, for both the patient and physician. For instance, the goal to contain symptoms at FC I or II can be used for the treatment of PH [1,3]. As such, a better survival rate is observed in patients who improves from a more severe to a less severe FC compared to those remaining at the same FC [4,5].
This review article will explore how the different groups of PH are treated, particularly exploring standard and novel neurostimulation therapies for the disease and the mechanisms they target. Diagnosis, cost, and demographics of the disease will also be mentioned.
2. Diagnosis
Diagnosis and classification of PH relies on mPAP, but also other hemodynamic measures such as Pulmonary Arterial Wedge Pressure (PAWP; mmHg units) to measure pulmonary vein and left-sided heart pressure, and Pulmonary Vascular Resistance (PVR; Wood units) to measure pulmonary arterial resistance and narrowing. For instance, a PAWP of ≤ 15 mmHg is generally necessary for a diagnosis of pre-capillary PH, including PAH [1,2]. Medications such as riociguat, epoprostenol, and sildenafil have been shown to significantly decrease mPAP in patients [6,7].
There are other numerous diagnostic techniques in addition to hemodynamic measures that could be used when assessing for PH. For instance, an electrocardiogram (ECG) could provide evidence for right atrial dilation, right ventricular hypertrophy and strain, right axis deviation, P pulmonale, right bundle branch block, and a prolonged QTc interval; while RHC is still necessary for a definitive diagnosis and ECG can still provide a probability estimate for PH [7,8,9]. Other complications associated with the disease include arrythmias, for which rhythm-control therapy is helpful in survival [1].
Depending on the subtype of PH, chest radiography can also be used to assess for similar results, including right atrial enlargement, dilated pulmonary arteries, calcifications, and aneurysms [1,7,10]. Pulmonary function tests and arterial blood gas analysis can help distinguish between groups such as idiopathic PAH and PH associated with lung disease by measuring parameters such as total lung capacity and forced expiratory volume, while ventilation/perfusion scintigraphy and pulmonary angiography can be used in diagnosing CTEPH [1]. Other tests include but are not limited to blood tests for brain natriuretic peptide, transthoracic doppler-echocardiography, exercise tests, and abdominal ultrasound for portal hypertension [1]. Typically, PAH is diagnosed only after excluding other groups of PH as defined in Table 1 [1,11].
Those with PH typically present with symptoms not entirely specific to the disease but important for physicians to suspect and initiate prompt action for therapy and referral. For instance, a cardinal feature of PH is progressive exercise dyspnea, while other symptoms are fatigue, tachycardia, and syncope upon exertion. On physical examination, patients may also display lower extremity edema, dilated jugular veins, and ascites. Additional symptoms observed in PH patients are augmented heart sounds, such as a pronounced pulmonary component in the second heart sound, cyanosis, and exertional and nocturnal hypoxia. Moreover, mental stress due to sleep problems, anxiety, and depression have been reported in patients with PH, in which case adequate psychosocial support and medications could be used [1,12,13].
3. Demographics and Cost
Older patients over the age of 65 have an estimated PH prevalence of 10%, and those with comorbidities such as aortic stenosis or heart failure (HF) with preserved ejection fraction (HFpEF) have a higher prevalence of PH ranging from around 30-90% depending upon how it is evaluated [14,15,16,17]. Despite scanty evidence, studies do suggest that those with residence in economically developing nations, poor healthcare access, low annual income, higher risk of diseases such as tuberculosis and human immunodeficiency virus (HIV) infection, and low health literacy have a higher prevalence of PH and worse FC and are less likely to receive adequate diagnosis and treatment [18,19,20,21,22,23]. Through mechanisms such as inflammation and vascular injury, COVID-19 cohorts are associated with higher prevalence of PH, in part due to the high prevalence of pre-existing PH with lung and heart comorbidities in COVID-19 patients [24,25,26]. On the other hand, a few studies suggest that COVID-19 could precipitate elevated pulmonary arterial pressure observed in PH [27,28].
Multiple studies report that PH-LHD is the most common type of PH, followed by PH due to lung disease and/or hypoxia [1,14]. However, regardless of the specific group, current trends indicate that the prevalence of PH is rising. Consequently, it is necessary to understand and tackle certain risk factors associated with PH, such as disease prevention and healthcare equity programs, along with finding novel therapies [1,18].
PH also imposes a large cost on the patient, their caregivers, and the broader economy. For instance, in the United States (US) alone, PAH-specific drugs can often cost anywhere between $5,000 to $250,000 annually, which is evidently compounded for those on combination therapies or in worse FCs. Similar costs have also been reported in other countries [29,30,31,32,33]. Combined with costs for instance in hospitalizations, medical devices, diagnostics, supportive therapies, screenings, and transplants, annual healthcare costs hundreds of millions of dollars [29,30,31,34,35,36,37]. Moreover, studies report patients with PH more often have their work and income affected by the disease, including being unable to work at all, taking extended sick and disability leave, or considering early retirement. Similarly, caregivers of these patients often have their own work and income affected and experience exhaustion leading to an indirect annual cost of thousands of dollars and tens of millions of dollars nationally [29,34,38,39,40,41].
4. Mechanisms and Treatments
Vasoconstriction of the pulmonary arteries with potential involvement of pulmonary vein and capillaries contributes to an elevated mPAP. Histologically, PH shows pathological vascular remodeling and vascular lesions [7,42]. Multiple studies report vascular thickening of the capillaries and hypertrophy of the arterial vessel intima, media, and adventitia in models of PAH such as PH due to left heart disease and PH on account of hypoxia [43,44,45,46]. Fibroblast migration to these layers, increased production of matrix proteins, endothelial cell proliferation, and neovascularization [43,44,45,46]. Moreover, lesions could form from pathological endothelial cell thickening and increase the chance of surgical risk, especially in CTEPH [7,47,48].
Hypoxia, infection and inflammation, shear stress, genetics, vasodilator-vasoconstrictor imbalances, and dysautonomia contribute to or are results of such vascular pathology. Treatments addressing these mechanisms are discussed below.
4.1. PAH-Specific Drugs and Vasoconstrictor-Vasodilator Imbalances
PH has long been associated with increased production of vasoconstrictors, such as endothelin-1 (ET-1), and decreased production of vasodilators, such as nitric oxide (NO), prostacyclin, and calcitonin gene-related peptide (CGRP).
ET-1 is overexpressed in both the plasma and lungs of PH patients in multiple different groups and positively correlates with severity of symptoms [49,50,51,52]. ET-1 activates two G-coupled protein receptor subtypes, endothelin receptor A (ETA) and endothelin receptor B (ETB). ETA receptors typically dominate over ETB receptors in the pulmonary vasculature and activation of the former leads to vasoconstriction while the latter induces vasodilator release [52,53,54]. ET-1 promotes intracellular calcium release through the phospholipase C (PLC)/inositol triphosphate pathway causing smooth muscle contraction. Diacylglycerols produced by PLC activation further potentiates smooth muscle contraction [54,55]. Furthermore, ET-1 can induce transcription of genes to promote smooth muscle cell growth and proliferation by the extracellular signal-regulated kinase (ERK) or sodium/hydrogen pump [53,56,57,58].
In accordance with these mechanisms, multiple current drugs aim to block ETA activation that help manage symptoms in PAH patients. Such antagonists include drugs such as bosentan, ambrisentan, and macitentan. Bosentan and macitentan target both ETA and ETB receptors while ambrisentan is selective towards endothelin A receptors. Although there are side effects associated with these medications, including liver dysfunction and thrombocytopenia, these drugs are effective in improving mortality and morbidity rates, WHO defined FC, and exercise capacity as measured by the six-minute walk distance (6-MWD) test, as well as hemodynamic parameters such as PVR and mPAP [59,60,61,62]. However, these drugs are more specific to PAH and have minimal effect on improving symptoms such as exercise capacity in other groups of PH patients [1,63,64,65,66].
Activation of ETB receptors on endothelial cells promotes vasodilator release through an increase in intracellular calcium via the PLC pathway. Calcium activates endothelial nitric oxide synthase (eNOS) leading to NO production and diffusion to vascular smooth muscle cells, soluble guanylate cyclase (sGC) activation, cyclic guanosine monophosphate (cGMP) generation, and smooth muscle relaxation and vasodilation [56]. However, in PH patients, there is reduced lung expression of eNOS, and increased expression of the enzyme that degrades cGMP, phosphodiesterase 5 (PDE5) [67,68,69].
Drugs tackling these pathways are similarly more specific for PAH. For instance, PDE5 inhibitors (PDE5i) include tadalafil and sildenafil, which target the NO pathway by acting as reversible competitive inhibitors of PDE5 to improve hemodynamic values and functional status in PAH [70,71]. There are also sGC stimulators including riociguat, which has been used to help treat those affected by both PAH and CTEPH. For instance, riociguat targets the NO pathway by increasing the sensitivity of sGC to NO and directly stimulating the sGC enzyme independently of NO. Riociguat also helps increase exercise, improve FC, and hemodynamic parameters in these patients [6,72].
Prostacyclin synthase expression is reduced in the lungs of PH patients. Prostacyclin is a potent vasodilator and may be used to correct vasoconstrictor-vasodilator imbalances through cyclic adenosine monophosphate-mediated vasodilation [73]. Prostacyclin analogues used to treat PAH include epoprostenol, iloprost, and Treprostinil. They are typically administered differently from the oral medications listed above and utilized in patients with more severe symptoms. For instance, epoprostenol is administered intravenously and is better for those in more severe FC compared to other therapies [74,75]. Treprostinil is similar but can also be administered subcutaneously or inhaled, while iloprost is typically inhaled. Selexipag is yet another prostacyclin receptor agonist and can be orally available. For many PAH patients, a combination of a PDE5i and endothelin receptor antagonist is used as a standard of care for both mild and more severe cases of PH [3].
Detected mainly in sensory C and Aδ fibers, CGRP a potent vasodilator, has also been found to be reduced in the plasma and lungs of rats affected by PH. Administration of CGRP is also reported to reduce hypertension in the lungs with vascular resistance and remodeling in animal models by suppression of ET-1 release. CGRP ligands activating the CLR/RAMP1 receptor leads to activation of multiple signaling pathways that in turn regulate not only intracellular energy metabolic patterns but also induce inflammatory factors by mitochondrial damage that are also involved in the development PAH. CGRP promotes anti-inflammatory effect by inhibiting the cGAS-STING-NFκB pathway [76,77,78,79]. The clinical use of CGRP is yet to be investigated and studies are warranted to discover the translational effectiveness in subjects with PH.
4.2. Hypoxia and Oxygen Therapies
Hypoxia is known to be a contributing factor to PH through multiple mechanisms. Studies report that hypoxic conditions trigger mechanisms such as mitochondria-mediated reactive oxygen species (ROS) production, ROS-mediated modification of protein channels, and nitrogen species-mediated inactivation of enzymes in the NO pathway that ultimately result in a calcium influx into smooth muscle cells, triggering depolarization and vasoconstriction [80,81].
There is also growing evidence that intrapulmonary oxygen sensors can play a role in the pathogenesis of PH. Studies show that sensors in the alveolar and bronchiole endothelium by sensory pulmonary neuroendocrine cells (PNECs) detect low oxygen levels. They seem to interact with peripheral nerves such as pulmonary axon reflexes and intrapulmonary ganglion that in the presence of hypoxia influence vascular function such as vascular remodeling in PH [82,83]. PNECs are situated next to pulmonary vessels and influence multiple neurotransmitters including CGRP and potent vasoconstrictor serotonin (5-HT) promoting epithelial and fibroblast proliferation [82,84]. Indeed, hyperplasia of PNECs is seen in PH, and hypoxia is a known trigger of 5-HT release from PNECs [85,86]. Serotonin has long been suggested to play a role in PH pathogenesis [84,87,88]. Exactly how PNECs contribute to the vasoconstrictor-vasodilator imbalances are involved in the pathogenesis of PH, perhaps via hypoxia-mediated pathways, is unclear and pleading for future studies.
Hypoxia has been reported to reduce eNOS transcription in pulmonary endothelial cells, but reports are conflicting as some report normal or even increased levels of eNOS [89,90,91]. It has been suggested that eNOS transcription is increased especially early in hypoxia via hypoxia-inducible factor 1 (HIF-1)- and 2 (HIF-2)-mediated binding to the eNOS promoter, and that this could cause high production of uncoupled eNOS and consequently high production of ROS. ROS reacts with and reduces the bioavailability of NO, contributing to vasoconstriction and triggering endothelial dysfunction [90,92,93]. Arginase, an enzyme that competes with eNOS for the substrate arginine, is elevated in animal models and humans with PH. Moreover, arginine transport into endothelial cells is reduced under hypoxic conditions [91,94]. Hypoxia also increases ET-1 expression through HIF-1 complex-mediated binding to the transcription site for ET-1 [95]. HIF-1 may also be involved in pathways controlling platelet adhesion to endothelial cell walls in the pathogenesis of CTEPH, extracellular matrix remodeling in the pathogenesis of PAH, and endothelial cell migration and proliferation [96,97]. Hypoxia may also trigger fibroblast migration and proliferation through complex signaling pathways involving protein kinase B (Akt), as well as vascular remodeling through HIF-mediated increases in activin, a ligand associated with PH [98,99,100].
Medications targeting these pathways have not yet been established in PH patients. However, inhibitors of the HIF-2 pathway have been shown to improve symptoms such as right heart function and pulmonary remodeling in rat models of PH [101,102]. At the same time, numerous studies have reported similar results with HIF-1 inhibitors in rat [103,104,105,106,107].
In each group of PH, oxygen therapy can be supplemented to maintain pulmonary and systemic oxygen levels when pO2 is low, but it is typically reserved for those with low levels of oxygen saturation during exercise or sleep. It is reported that oxygen therapy does not have a significant clinical or survival benefit in the prognosis of those with PH [1,108]. Regardless, some studies have reported that oxygen may induce pulmonary vasodilation and improve exercise function in patients affected by multiple types of PH; oxygen therapy is recommended if there’s symptomatic benefit [1,109].
4.3. Genetics and Signaling Pathways
Imbalances in proliferative and anti-proliferative signaling via the transforming growth factor-β (TGF-β) receptor is also associated with PH. Mutations in BMP receptor type II (BMPR2), a subtype of TGF-β receptor, is the most common heritable form of PAH and is associated with increased intima, smooth muscle, and adventitia thickening in pulmonary arteries through complex signaling pathways [45]. However, mutations in other genes are likely involved in PH, since not all of those with BMPR2 mutations develop the PH phenotype.
BMPR2 signaling is highly complex and controls multiple signaling pathways. First, BMPR2 downstream targets include BMP4 and BMP7 in vascular smooth muscle cells, which help repress the secretion of ET-1 [110,111]. Moreover, ET-1 downregulates BMPR2 expression, hence reduction in BMPR2 results in excessive vasoconstriction [110,111]. Immunologically, BMPR2 deficiency is associated with increased cytokine production through alterations to superoxide dismutase (SOD) activity and increased production of ROS, as well as increased lymphocyte, neutrophil, monocyte, and macrophage activity and migration [112,113,114]. This is understandable given that BMPR2 receptor activation on macrophages inhibit macrophage activation and upregulation of adhesive membrane proteins [112,113,114]. From a metabolic standpoint, BMPR2 loss is associated with mitochondrial dysfunction in endothelial cells and cardiomyocytes by shifting away from glucose and fatty acid oxidation respectively; these changes are thought to predispose PH clinical symptoms such as endothelial inflammation and right ventricular failure [115,116]. From a viral standpoint, it’s been reported that human immunodeficiency virus (HIV) infection can lead to miRNA-mediated downregulation of BMPR2 expression [117].
More pertinently, impaired BMPR2 activity may result in impaired regulation of activin, a pro-proliferative ligand that reduces BMP activity and promotes myogenic proliferation and remodeling [118,119]. Accordingly, sotatercept, an activin signaling inhibitor, has been shown to improve clinical outcomes for PAH patients [120,121]. Etanercept has also been shown to target the BMPR2 pathway by inhibiting the cytokine tumor necrosis factor-alpha (TNFα), the overexpression of which is found in PAH patients and leads to downregulation of BMPR2 mRNA in rat models [122,123]. Targeted delivery of exosomes to replace defective BMPR2 has also been explored [124].
Other pathways are also implicated within the pathogenesis of PH. For instance, studies indicate that SRT2104, an activator of Sirtuin 1 (SIRT1), can mediate the restoration of tuberous sclerosis complex 2 (TSC2), a growth suppressor protein on smooth muscle cells that is decreased in PAH [125].
4.4. Inflammation
Inflammation is a crucial factor in the pathogenesis of PH, especially in those with infection or connective tissue diseases. For instance, lymphocytes, dendritic cells, mast cells, macrophages, and proliferating endothelial cells are found in vascular lesions [126,127,128,129]. Patients with PH show higher serum cytokines including multiple interleukins (IL), TNFα, and chemokines [122,130,131].
Multiple cytokines and pathways contribute to PH pathogenesis. For instance, studies show that hypoxia increases lung production of IL-1β, which activates receptors on smooth muscle cell and triggers proliferation [132]. Moreover, IL-6 activates signal transducer and activator of transcription 3 (STAT3), which causes the increase of certain miRNAs that degrade BMPR2 mRNA leading to vasoconstriction [133]. Studies have shown that Il-6 can increase endothelial growth factor receptors and matrix metalloproteinases that promote smooth muscle proliferation and endothelial-mesenchymal transition seen in PH [134,135]. IL-6 and other cytokines such as IL-8 and IL-10 appear to be a predictor for survival perhaps more so than certain clinical tests or hemodynamic parameters, signifying its importance in PH pathogenesis [122,136]. Other interleukins, such as IL-8 and IL-13, act through pathways that promote endothelial cell proliferation and arginase upregulation, respectively [137,138]. The mechanisms related to increased lymphocyte activity and consequent cytokine production is less clear in PH. Studies have reported that such patients may have dysregulated regulatory T-cell function which could predispose high immune system reactivity [139,140]. A considerable proportion of PH patients have circulating autoantibodies [141,142], which precipitate endothelial cell damage and further PH pathogenesis. Infections such as HIV or COVID-19 are also associated with damage to the vascular endothelia, cytokine storms, increased inflammation, and PH pathogenesis. COVID-19 is reported to potentiate intense platelet activation, which might contribute to thrombosis seen in different groups of PH patients [143,144].
All PAH-specific drugs have limited anti-inflammatory effects while prostacyclins are even stronger mediators of immune activity [145]. Immunosuppressive drugs such as dexamethasone, mycophenolate mofetil, cyclosporine, tacrolimus and etanercept have been shown to attenuate endothelial cell dysfunction and hemodynamic parameters in animal models. These preclinical findings warrant further translational and clinical investigation [146]. Rituximab, which promotes B-cell depletion, and anakinra, which acts as a IL-1 receptor antagonist, both have shown clinical benefit in PAH patients but will need more clinical trials to establish safety and efficacy [147,148].
4.5. General Therapies
Most PAH-specific drugs are not recommended for those with PH-LHD or PH with associated lung disease or hypoxia, as evidence suggest a lack of clinical improvement and potentially adverse outcomes [1]. However, riociguat is approved for helping those with CTEPH, and macitentan is reported to benefit CTEPH patients [1,149]. Moreover, diuretics are considered as a general supportive therapy in multiple groups of PH to relieve pulmonary congestion and right-sided heart failure [1].
In CTEPH, pulmonary thromboendarterectomy (PEA) is typically the treatment of choice and is potentially curative; percutaneous balloon pulmonary angioplasty (BPA) can also be utilized if PEA is ineffective or unfeasible due to surgery risk [1]. Lifelong anticoagulation is recommended in all patients with CTEPH and often including Vitamin K antagonists and Factor Xa inhibitors like rivaroxaban. Generally, Vitamin K antagonists are preferred for those with antiphospholipid syndrome [1,150]. Using anticoagulation treatment in PAH is unclear. To prevent thrombosis, few studies show that anticoagulation therapies such as warfarin may alleviate idiopathic PAH, but others report no significant advantage by anticoagulation in idiopathic PAH patients [1,151,152].
Other general therapies include managed exercise training improving hemodynamics, oxygen uptake, and quality of life in patients affected by PH [153,154]. Limiting salt and water consumption to reduce volume overload and hypertension as well as correcting iron deficiency, often seen in PH, are recommended [1]. Women are also often strongly advised against pregnancy, as pregnancy is associated with higher maternal mortality rates in those affected by PH [1]. Routine vaccinations to prevent infections such as influenza and pneumococcal pneumonia are recommended as a general safety measure [1].
Management of PH patients in Group 2 and Group 3 often focus on addressing the underlying issue with numerous therapies, which focus on problems such as heart failure, valvulopathy, or obstructive or restrictive lung diseases. Currently, lung transplants are the only potentially curative treatment for PH associated with chronic lung disease, and such transplants can also be used for patients in other PH groups who are unresponsive to medications and in a high FC [1].
4.6. Autonomic Nervous System Imbalance, Therapies, and Neurostimulation
There is also increasing evidence for a role of autonomic nervous system in PH. Studies have suggested both increased sympathetic activity and decreased parasympathetic activity in PH patients [155,156].
4.6.1. Multiple Pharmacological Therapies Have Been Tested to Assess the Role of the Autonomic System in the Pathogenesis of PH
The heart selectively downregulates expression of beta-1 (β1) receptors and increases expression of beta-2 (β2) receptors in patients with PH [157]. Accordingly, the beta-blocker carvedilol has been shown to improve heart rate and RV function in rat models of PH, inhibit smooth muscle cell proliferation in vitro, and show some benefit in controlling heart rate in PH patients [158,159,160]. Moreover, nebivolol, a β1 antagonist and β2 agonist, has been shown to significantly ameliorate PVR and pulmonary vascular remodeling in rat models of PH, as well as improve exercise capacity in PH patients [161,162]. Other similar drugs, such as bisoprolol and arotinolol, both have been shown to improve RV function by preventing RV hypertrophy and improving RV contractility in animal models of PH [163,164]. However, more extensive clinical trials with beta-blockers have shown a lack of efficacy in patients with PH related to function and remodeling, although some drugs such as nebivolol have not yet been widely tested [1,165,166,167,168,169]. With regards to the parasympathetic nervous system, the acetylcholinesterase inhibitor pyridostigmine has been reported to attenuate right-sided heart dysfunction and pulmonary remodeling in rat models of PH [156,170].
4.6.2. Non-Pharmacological Therapies: Sympathetic Activity Modulation and Stimulation of Vagal Nerve or Somatosensory Nerves
Non-pharmacological PH therapies such as sympathetic modulation and neurostimulation of the parasympathetic nerves are under investigation. Sympathetic modulation has been pursued with various methods such as sympathetic ganglion block, renal sympathetic denervation, and pulmonary artery denervation (PADN), which are accomplished by multiple techniques such as radiofrequency ablation or high-energy ultrasound [170,171,172,173]. Numerous studies with animal models of PH have reported that reducing sympathetic activity attenuates pulmonary vascular remodeling, reducing hemodynamic parameters including right ventricular pressure and mPAP, and reducing pulmonary wall thickness [170,174,175,176,177,178,179,180,181]. Sympathetic modulation leads to increased NO signaling, an altered expression of genes that are related to inflammation and vasoconstriction, and downregulation of the activity of the renin-angiotensin-aldosterone system [170,174,175,176]. Pertinently, denervation of the pulmonary artery reduces mPAP, PVR, and resulted in an improvement in exercise capacity and cardiac function in patients with PAH [172,182,183,184]. Other studies suggest that denervation of the pulmonary artery could have similar benefits in those with residual CTEPH [185,186], but more studies are warranted to assess PADN’s effectiveness relative to other medical therapies [1].
Vagal nerve stimulation may be helpful for patients with PH. For instance, chronic vagal nerve stimulation (VNS) prolongs survival, reduces dysautonomia and inflammation, and improves right heart function and hemodynamic parameters in rats with PH. Studies have also reported that neurostimulation helps to preserve right ventricular function in rats with significant right ventricular overload [187,188].
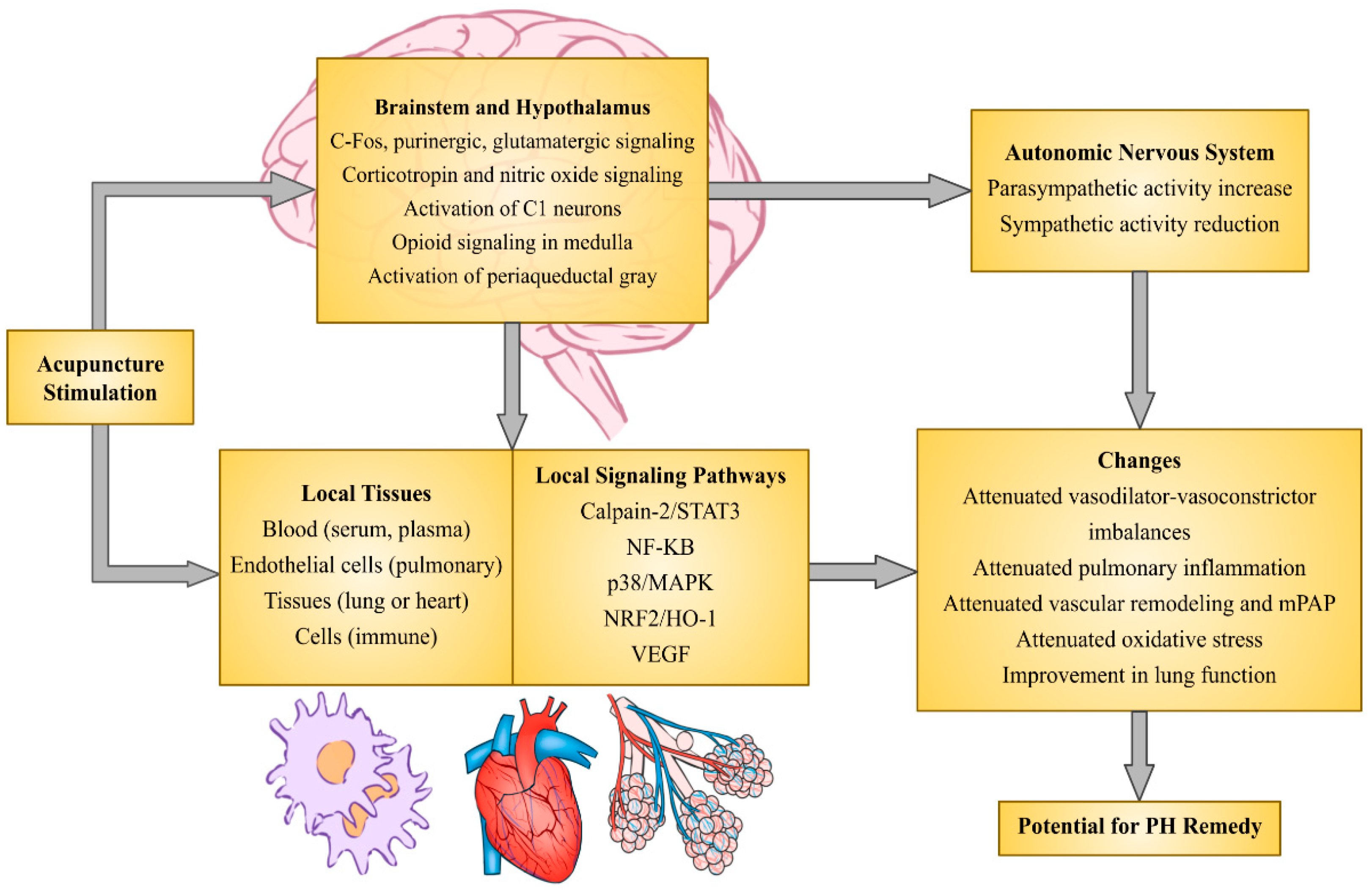
Manual acupuncture (MA) and electroacupuncture (EA) stimulating somatosensory nerves ameliorate PH symptoms and related risk factors. Relevant studies are described in the following paragraphs and listed in Table 2. The reported mechanisms are diagrammed in Figure 1. Electrically stimulating acupuncture needles overlying specific nerves (acupoints) appears to ameliorate elevated mPAP, vascular remodeling, and right ventricular hypertrophy in rat models of hypoxia-induced PH by normalizing ET-1 and eNOS imbalances [189]. A number of studies indicate that acupuncture regulates ET-1-NO imbalances not only in the heart and serum but also in lungs in animal models with hypertension and asthma. These findings are also observed in patients with hypertension [190,191,192,193,194]. Previous studies show acupuncture’s role in improving lung and pulmonary function, exercise capacity and endurance, efficiency of oxygen uptake, oxygen saturation, and quality of life in patients with chronic obstructive pulmonary disease (COPD) [195,196,197,198,199,200,201]. Notably, acupuncture improves ejection fraction and regulation of pathological ventricular enlargement in subjects with heart failure, both in preclinical and clinical studies [202,203,204,205]. In this respect, acupuncture could potentially benefit patients with PH, including those with comorbidities such as chronic lung diseases by improving pulmonary function and attenuating vascular remodeling.
Sympathetic activity is elevated in patients with PH [155]. In the subset of patients with COPD and chronic high-altitude exposure, PH is mediated by hypoxia-inducible factor signaling as detailed above [206,207]. The underlying mechanism typically associated with inflammation leads to consequent remodeling of the pulmonary vasculature. Moreover, hypoxia can contribute to PH by not only triggering oxygen chemoreceptors within the carotid body, but also increasing their sensitivity to low oxygen levels, predisposing patients to increased sympathetic activity [208,209,210,211,212]. Hypoxia also contributes to cellular changes centrally by increasing purinergic or glutamatergic signaling pathways in the NTS, rostral ventro-lateral medulla (rVLM), and paraventricular nucleus (PVN), which lead to increased sympathetic tone and may also contribute to PH [213,214,215]. In this regard, multiple studies have reported that EA can dampen elevated sympathetic responses, especially in several rat models of cardiac events including heart failure or myocardial infarction [204,216,217,218].

Table 2.
Studies Supporting a Role of Acupuncture in the Pathologies of PH.
| Reference | Model | Technique | Findings Relevant to PH |
|---|---|---|---|
| [189] | Pre-clinical Hypoxic-induced PH |
EA | mPAP ↓, RV size ↓ Pathological pulmonary remodeling ↓ Serum/lung eNOS ↑, serum/lung ET-1 ↓ |
| [190,246] | Pre-clinical Hypertension |
EA Non-EA |
Sympathetic activity (e.g. via NOS pathways) ↓ Serum norepinephrine ↓ Serum interleukins/C-reactive protein ↓ Serum ET-1 ↓, myocardial eNOS ↑ |
| [193,194] | Clinical Hypertension |
Non-EA + EECP | Serum NO ↑, serum ET-1 ↓ |
| [195,196,197,198,199,200,201] | Clinical COPD (i.e. Group 3) |
EA Non-EA |
Oxygen utilization/efficiency ↑, dyspnea ↓, exercise capacity ↑ |
| [203,248–252,261,264] | Pre-clinical Systemic inflammation |
EA Non-EA |
Serum/lung TNF-α, interleukins ↓ Parasympathetic (vagus) outflow ↑ Ejection fraction ↑ |
| [204] | Pre-clinical Heart failure (i.e. Group 2) |
EA | Sympathetic outflow ↓ Heart function ↑ (i.e. left ventricle ejection fraction ↑, left ventricle size ↓ |
| [216–218,220,221,227–230,240,241,243] | Pre-clinical Sympathetically stressed |
EA | Sympathetic outflow ↓ (i.e. via central opioid, CRH pathways) Serum CRH, cortisol, norepinephrine, adrenaline |
| [257] | Clinical Post-surgery secondary to lung cancer |
EA | PaO2/FiO2 ↑ SOD activity ↑ Length of hospital stay ↓ |
| [247] | Clinical Systemic sclerosis (i.e. Group 5) |
EA | Plasma ET-1 ↓ |
| [258,262,263] | Pre-clinical Lung injury |
EA | Lung SOD activity ↑ Serum/lung cytokines ↓ PaO2 ↑ Lung injury score ↓ |
| [260,267] | Pre-clinical COPD |
EA | Pathological pulmonary remodeling ↓ Lung cytokines ↓ Lung function (i.e. expiratory volume) ↑ |
| PH = pulmonary hypertension; EA = electroacupuncture; ET-1 = endothelin-1, NO = nitric oxide, eNOS = endothelial nitric oxide synthase; EECP = enhanced external counterpulsation; COPD = chronic obstructive pulmonary disease; CRH = corticotropin-releasing hormone; PaO2/FiO2 = arterial oxygen pressure/fraction of inspired oxygen; SOD = superoxide dismutase | |||
A frequently examined somatic nerve in modulating sympathetic tone is the median nerve. EA-mediated reduction in sympathetic activity involves activation of the median nerves including the C-fibers and thinly myelinated Aδ-fibers underlying the acupoints P5-6 located near the wrist [217,219,220]. Stimulation of these fibers during EA activates specific cardiovascular regions in the brain that processes the convergence from the somatosensory fibers and input from elevated sympathetic activity. The underlying mechanisms and pathways range from specific neurotransmitter systems to neurocircuitry in the hypothalamus and midbrain. Central regions also involved in the actions of EA in reducing sympathetic activity are the medulla and spinal cord. The central actions of EA lead to increases in opioid expression and signaling through specific opioid receptor subtypes in the rVLM, which then reduces sympathetic efferent activity [216,219,221]. Additionally, EA’s modulation of sympathetic activity involves glutamatergic neurons associated with the reciprocal excitatory pathways between the arcuate nucleus (ARC) and the midbrain ventrolateral periaqueductal gray (vlPAG) [218,222].
Hypoxia alters neurotransmitter signaling leading to increased sympathetic tone. It is conceivable that sympathetic overactivity in PH is driven by increased glutamatergic signaling in the rVLM [134,223,224,225]. Chronic intermittent hypoxia, a form of hypobaric hypoxia, leading to PH changes the signaling in the rVLM and heightens sympathetic tone [83,226]. Accordingly, EA inhibits glutamatergic transmission in the rVLM through opioid mechanisms and decreases sympathetic outflow [227]. Studies have demonstrated that EA reduces GABA release in the vlPAG, which disinhibits vlPAG neurons, and in turn suppresses sympathetic neuronal activity in the rVLM through a serotonergic-mediated pathway [228,229,230]. Additionally, EA activates opioidergic neurons in the ARC that monosynaptically project to the rVLM likely reducing elevated activity of the pre-sympathetic neurons [230].
Electroacupuncture also reduces sympathetic activity through other central pathways. For instance, hyperactivity of sympathetic neurons within the hypothalamic PVN and their ensuing connections with the rVLM is implicated in multiple diseases, including in models of hypoxia-induced PH [231,232,233,234]. Elevated levels of corticotropin-releasing hormone (CRH) synthesis and neuronal activity contribute to this sympathetic overactivity, including in disease models of PH [231,232]. Moreover, CRH neurons observed in the PVN and NTS are activated during acute hypoxic conditions leading to increased sympathetic outflow [235,236,237,238,239]. Although studies have not been done in PH models, EA has been shown to reduce corticotropin-releasing hormone (CRH) signaling in the rVLM and PVN in animal models of stress, cardiovascular disease, and multiple other sympathoexcitatory related conditions [240,241,242,243]. Reductions in other nitric oxide synthases, including neuronal nitric oxide synthases (nNOS), in the PVN and other areas such as the lung exposed to hypoxia, promote hypoxia-induced PH and are associated with increased sympathetic activity [244,245]. However, the mechanisms associated with EA effect in PH are less clear although study has shown that EA decreases nNOS levels in the hypothalamus in a rat model of hypertension [246]. Hence, exploration of sympathoinhibition by EA in attenuating PH is important.
Figure 1.
Potential mechanisms of acupuncture-mediated neurostimulation for pulmonary hypertension (PH).
Figure 1.
Potential mechanisms of acupuncture-mediated neurostimulation for pulmonary hypertension (PH).
Acupuncture may ameliorate PH through actions within the lungs. For instance, EA reduces serum levels of the vasoconstrictor ET-1 in patients with systemic sclerosis and hypertension, which similarly might reduce PH [190,194,247]. As mentioned above, a preclinical study has demonstrated acupuncture stimulating specific nerves reverses hypoxia-induced pulmonary hypertension by attenuating elevated mean pulmonary arterial pressure, right ventricular hypertrophy, and pulmonary vascular remodeling [189]. With this regard, EA decreased ET-1 that was elevated by hypoxia [189].
Mounting evidence shows that neurostimulation techniques such as acupuncture through the autonomic nervous system may also reduce inflammation and ameliorate symptoms of PH. For instance, multiple studies report that both MA and EA at varying acupoints help reduce serum cytokines – including TNFα, IL-1β, and IL-6 – in rat models of endotoxin-mediated inflammation partially or primarily through the activation of vagal efferents [203,248,249,250,251,252]. Acupuncture has been shown to influence the stimulation of the vagal-adrenal axis by activation of the vagus nerve, dopamine release from the adrenal gland, and suppression of systemic inflammation [250,251], referred to as the cholinergic-anti-inflammatory pathway (CAP) [203,253,254]. The central mechanisms underlying acupuncture’s activation of this reflex are complex. Acupuncture input in the brain influences central processing leading to increased vagal activity, including upregulation of c-Fos, glutamatergic and purinergic signaling in the nucleus tract solitarus (NTS) and broader dorsal vagal complex (DVC) [248,250,255,256]. The neuronal activities in the DVC and the nucleus ambiguus facilitate the parasympathetic outflow and activity of vagal efferents leading to anti-inflammation.
Acupuncture improves pulmonary function and regulates oxidative stress and inflammation. For instance, EA increases SOD activity both within the circulation and lung tissue to improve pulmonary lung function [257,258,259]. Other studies have demonstrated that EA affects multiple signaling pathways to reduce inflammation, pulmonary vascular remodeling, and oxidative stress in animal models. For example, studies have shown acupuncture-mediated actions such as inhibition of calpain-2 and STAT3 pathways in cardiomyocytes, activation of local cannabinoid receptors and inhibition of toll-like receptor 4 (TLR4)-NF-κB signaling in peripheral immune cells or lung tissue, regulation of p38 phosphorylation, MAPK, and caspase-3 pathways in lung tissue, upregulation of acetylcholine receptor signaling, modulation of the nuclear factor erythroid 2-related factor (Nrf2)/heme oxygenase-1 (HO-1) pathway, and reduction in pathways leading to angiogenesis, such as those involving vascular endothelial growth factor (VEGF) [203,252,258,260,261,262,263,264]. There is also evidence that acupuncture reduces the expression of genes related to oxidative stress and inflammation as well, limiting ROS and cytokine production, albeit in animal models with varying conditions like inflammation and ischemia-induced hypoxia [261,265,266]. Other studies indicate that acupuncture could also mediate immune cell migration in lung tissue [267,268].
The non-adrenergic, non-cholinergic neuropeptide CGRP has a protective role in vascular tone and is important in the development of PH as evidenced by a reduction in plasma of rats with PH. Interestingly, the oxygen sensors pulmonary neuroendocrine cells synthesize CGRP while there is insufficient CGRP available to maintain normal vascular tone in PH. Other studies have shown that CGRP in left ventricle plasma is reduced significantly in pulmonary hypertensive rats with elevated mPAP, right ventricular hypertrophy, and pulmonary vascular remodeling [269,270]. Depletion of CGRP with capsaicin exacerbates PH [270]. Transfer of the CGRP gene with adenoviral vector decreases hypobaric chamber-induced pulmonary hypertension in mice [271]. Although it is unclear if EA increases CGRP in subjects with PH, a previous study has shown that EA increases CGRP expression in spinally injured rats [272].
Acupuncture impacts muscle activity, which could benefit patients with PH and COPD. Application of acupuncture results in more efficient and effective oxygen uptake as measured by oxygen saturation, which ameliorates PH and the hypoxic condition [195,198]. Moreover, other studies suggest that acupuncture suppresses electromyogram (EMG) activity of the muscles undergoing repeated contraction. Thus, muscles that are hyper-activated in patients with COPD could be similarly suppressed by acupuncture to relax the muscles while gaining strength and increase motility of the muscle cage at a lesser cost of energy expenditure [201,273]. Acupuncture could relieve PH in addition to COPD by alleviating chronic repeated muscle contraction.
Acupuncture has been reported to help treat multiple other diseases. Clinically, it is often used to help manage multiple types of pain, especially chronic pain [274]. However, there are also studies suggesting that acupuncture could be beneficial in managing symptoms in diabetes [275,276], depression and sleep disorders [277,278], hypertension, cardiovascular problems, and other conditions listed above. A considerable number of the studies listed are pre-clinical and hence more investigations are needed to establish acupuncture’s efficacy in patients. Most notably, there is a real potential in acupuncture’s role in helping to manage symptoms in those with PH, given that each of the conditions above are either common comorbidities for or a result of the disease PH [1].
5. Conclusion
Pulmonary hypertension is a complex disease that affects millions of people globally. While many studies have revealed multiple pharmacological treatments alleviating suffering and a number of mechanisms associated with the disease, further investigations would be beneficial in exploring complementary non-pharmacological treatments. Moreover, given that PH is on the rise, more research is needed to offer preventive and potential curative treatments for PH.
Funding
The authors S. Tjen-A-Looi and S. Malik are NCCIH RO1 AT011306 award recipients.
References
- Humbert, M., Kovacs, G., Hoeper, M. M., Badagliacca, R., Berger, R. M. F., Brida, M., Carlsen, J., Coats, A. J. S., Escribano-Subias, P., Ferrari, P., Ferreira, D. S., Ghofrani, H. A., Giannakoulas, G., Kiely, D. G., Mayer, E., Meszaros, G., Nagavci, B., Olsson, K. M., Pepke-Zaba, J., Quint, J. K., … ESC/ERS Scientific Document Group (2022). 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. European heart journal, 43(38), 3618–3731. [CrossRef]
- Simonneau, G., Montani, D., Celermajer, D. S., Denton, C. P., Gatzoulis, M. A., Krowka, M., Williams, P. G., & Souza, R. (2019). Haemodynamic definitions and updated clinical classification of pulmonary hypertension. The European respiratory journal, 53(1), 1801913.
- Hoeper, M. M., Ghofrani, H. A., Grünig, E., Klose, H., Olschewski, H., & Rosenkranz, S. (2017). Pulmonary Hypertension. Deutsches Arzteblatt international, 114(5), 73–84. [CrossRef]
- Barst, R. J., Chung, L., Zamanian, R. T., Turner, M., & McGoon, M. D. (2013). Functional class improvement and 3-year survival outcomes in patients with pulmonary arterial hypertension in the REVEAL Registry. Chest, 144(1), 160–168. [CrossRef]
- Sitbon, O., Humbert, M., Nunes, H., Parent, F., Garcia, G., Hervé, P., Rainisio, M., & Simonneau, G. (2002). Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. Journal of the American College of Cardiology, 40(4), 780–788. [CrossRef]
- Ghofrani, H. A., Galiè, N., Grimminger, F., Grünig, E., Humbert, M., Jing, Z. C., Keogh, A. M., Langleben, D., Kilama, M. O., Fritsch, A., Neuser, D., Rubin, L. J., & PATENT-1 Study Group (2013). Riociguat for the treatment of pulmonary arterial hypertension. The New England journal of medicine, 369(4), 330–340. [CrossRef]
- Montani, D., Günther, S., Dorfmüller, P., Perros, F., Girerd, B., Garcia, G., Jaïs, X., Savale, L., Artaud-Macari, E., Price, L. C., Humbert, M., Simonneau, G., & Sitbon, O. (2013). Pulmonary arterial hypertension. Orphanet journal of rare diseases, 8, 97. [CrossRef]
- Rich, S., Dantzker, D. R., Ayres, S. M., Bergofsky, E. H., Brundage, B. H., Detre, K. M., Fishman, A. P., Goldring, R. M., Groves, B. M., & Koerner, S. K. (1987). Primary pulmonary hypertension. A national prospective study. Annals of internal medicine, 107(2), 216–223. [CrossRef]
- Henkens, I. R., Mouchaers, K. T., Vonk-Noordegraaf, A., Boonstra, A., Swenne, C. A., Maan, A. C., Man, S. C., Twisk, J. W., van der Wall, E. E., Schalij, M. J., & Vliegen, H. W. (2008). Improved ECG detection of presence and severity of right ventricular pressure load validated with cardiac magnetic resonance imaging. American journal of physiology. Heart and circulatory physiology, 294(5), H2150–H2157. [CrossRef]
- Diller, G. P., & Gatzoulis, M. A. (2007). Pulmonary vascular disease in adults with congenital heart disease. Circulation, 115(8), 1039–1050. [CrossRef]
- McLaughlin, V. V., Archer, S. L., Badesch, D. B., Barst, R. J., Farber, H. W., Lindner, J. R., Mathier, M. A., McGoon, M. D., Park, M. H., Rosenson, R. S., Rubin, L. J., Tapson, V. F., Varga, J., American College of Cardiology Foundation Task Force on Expert Consensus Documents, American Heart Association, American College of Chest Physicians, American Thoracic Society, Inc, & Pulmonary Hypertension Association (2009). ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. Journal of the American College of Cardiology, 53(17), 1573–1619. [CrossRef]
- Pfeuffer, E., Krannich, H., Halank, M., Wilkens, H., Kolb, P., Jany, B., & Held, M. (2017). Anxiety, Depression, and Health-Related QOL in Patients Diagnosed with PAH or CTEPH. Lung, 195(6), 759–768. [CrossRef]
- Harzheim, D., Klose, H., Pinado, F. P., Ehlken, N., Nagel, C., Fischer, C., Ghofrani, A., Rosenkranz, S., Seyfarth, H. J., Halank, M., Mayer, E., Grünig, E., & Guth, S. (2013). Anxiety and depression disorders in patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. Respiratory research, 14(1), 104. [CrossRef]
- Hoeper, M. M., Humbert, M., Souza, R., Idrees, M., Kawut, S. M., Sliwa-Hahnle, K., Jing, Z. C., & Gibbs, J. S. (2016). A global view of pulmonary hypertension. The Lancet. Respiratory medicine, 4(4), 306–322. [CrossRef]
- Zlotnick, D. M., Ouellette, M. L., Malenka, D. J., DeSimone, J. P., Leavitt, B. J., Helm, R. E., Olmstead, E. M., Costa, S. P., DiScipio, A. W., Likosky, D. S., Schmoker, J. D., Quinn, R. D., Sisto, D., Klemperer, J. D., Sardella, G. L., Baribeau, Y. R., Frumiento, C., Brown, J. R., O'Rourke, D. J., & Northern New England Cardiovascular Disease Study Group (2013). Effect of preoperative pulmonary hypertension on outcomes in patients with severe aortic stenosis following surgical aortic valve replacement. The American journal of cardiology, 112(10), 1635–1640. [CrossRef]
- Tichelbäcker, T., Dumitrescu, D., Gerhardt, F., Stern, D., Wissmüller, M., Adam, M., Schmidt, T., Frerker, C., Pfister, R., Halbach, M., Baldus, S., & Rosenkranz, S. (2019). Pulmonary hypertension and valvular heart disease. Pulmonale Hypertonie und Herzklappenerkrankungen. Herz, 44(6), 491–501. [CrossRef]
- Ovchinnikov, A., Potekhina, A., Belyavskiy, E., & Ageev, F. (2022). Heart Failure with Preserved Ejection Fraction and Pulmonary Hypertension: Focus on Phosphodiesterase Inhibitors. Pharmaceuticals (Basel, Switzerland), 15(8), 1024. [CrossRef]
- Mocumbi, A., Humbert, M., Saxena, A., Jing, Z. C., Sliwa, K., Thienemann, F., Archer, S. L., & Stewart, S. (2024). Pulmonary hypertension. Nature reviews. Disease primers, 10(1), 1. [CrossRef]
- Thienemann, F., Dzudie, A., Mocumbi, A. O., Blauwet, L., Sani, M. U., Karaye, K. M., Ogah, O. S., Mbanze, I., Mbakwem, A., Udo, P., Tibazarwa, K., Damasceno, A., Keates, A. K., Stewart, S., & Sliwa, K. (2016). The causes, treatment, and outcome of pulmonary hypertension in Africa: Insights from the Pan African Pulmonary Hypertension Cohort (PAPUCO) Registry. International journal of cardiology, 221, 205–211. [CrossRef]
- Katoto, P. D. M. C., Mukasa, S. L., Sani, M. U., Karaye, K. M., Mbanze, I., Damasceno, A., Mocumbi, A. O., Dzudie, A., Sliwa, K., & Thienemann, F. (2023). HIV status and survival of patients with pulmonary hypertension due to left heart disease: the Pan African Pulmonary Hypertension Cohort. Scientific reports, 13(1), 9790. [CrossRef]
- Schikowski, E. M., Swabe, G., Chan, S. Y., & Magnani, J. W. (2022). Association between income and likelihood of right heart catheterization in individuals with pulmonary hypertension: A US claims database analysis. Pulmonary circulation, 12(3), e12132. [CrossRef]
- Harikrishnan, S., Mani, A., G, S., M, A., Menon, J., G, R., Kumar, R. K., Koshy, A. G., Attacheril, T. V., George, R., Punnose, E., Ashraf, S. M., Sr, A., Cholakkal, M., Jeemon, P., Joseph, S., Govindan, U., Joseph, J., Eapen, K., Sreedharan, M., … Venugopal, K. (2022). Pulmonary Hypertension Registry of Kerala, India (PRO-KERALA): One-year outcomes. Indian heart journal, 74(1), 34–39. [CrossRef]
- Talwar, A., Sahni, S., Talwar, A., Kohn, N., & Klinger, J. R. (2016). Socioeconomic status affects pulmonary hypertension disease severity at time of first evaluation. Pulmonary circulation, 6(2), 191–195. [CrossRef]
- Caravita, S., Baratto, C., Di Marco, F., Calabrese, A., Balestrieri, G., Russo, F., Faini, A., Soranna, D., Perego, G. B., Badano, L. P., Grazioli, L., Lorini, F. L., Parati, G., & Senni, M. (2020). Haemodynamic characteristics of COVID-19 patients with acute respiratory distress syndrome requiring mechanical ventilation. An invasive assessment using right heart catheterization. European journal of heart failure, 22(12), 2228–2237. [CrossRef]
- Pagnesi, M., Baldetti, L., Beneduce, A., Calvo, F., Gramegna, M., Pazzanese, V., Ingallina, G., Napolano, A., Finazzi, R., Ruggeri, A., Ajello, S., Melisurgo, G., Camici, P. G., Scarpellini, P., Tresoldi, M., Landoni, G., Ciceri, F., Scandroglio, A. M., Agricola, E., & Cappelletti, A. M. (2020). Pulmonary hypertension and right ventricular involvement in hospitalised patients with COVID-19. Heart (British Cardiac Society), 106(17), 1324–1331. [CrossRef]
- Charif, F., Dakroub, F., Bou Akl, I., Kularatne, M., & Montani, D. (2023). Pulmonary arterial hypertension and COVID-19: Piecing the puzzle. Respiratory medicine and research, 84, 101053. [CrossRef]
- Tudoran, C., Tudoran, M., Lazureanu, V. E., Marinescu, A. R., Pop, G. N., Pescariu, A. S., Enache, A., & Cut, T. G. (2021). Evidence of Pulmonary Hypertension after SARS-CoV-2 Infection in Subjects without Previous Significant Cardiovascular Pathology. Journal of clinical medicine, 10(2), 199. [CrossRef]
- Khan, A. W., Ullah, I., Khan, K. S., Tahir, M. J., Masyeni, S., & Harapan, H. (2021). Pulmonary arterial hypertension post COVID-19: A sequala of SARS-CoV-2 infection?. Respiratory medicine case reports, 33, 101429. [CrossRef]
- Zozaya, N., Abdalla, F., Casado Moreno, I., Crespo-Diz, C., Ramírez Gallardo, A. M., Rueda Soriano, J., Alcalá Galán, M., & Hidalgo-Vega, Á. (2022). The economic burden of pulmonary arterial hypertension in Spain. BMC pulmonary medicine, 22(1), 105. [CrossRef]
- Burger, C. D., Ghandour, M., Padmanabhan Menon, D., Helmi, H., & Benza, R. L. (2017). Early intervention in the management of pulmonary arterial hypertension: clinical and economic outcomes. ClinicoEconomics and outcomes research : CEOR, 9, 731–739. [CrossRef]
- Bergot, E., De Leotoing, L., Bendjenana, H., Tournier, C., Vainchtock, A., Nachbaur, G., & Humbert, M. (2019). Hospital burden of pulmonary arterial hypertension in France. PloS one, 14(9), e0221211. [CrossRef]
- Selexipag (Uptravi) for pulmonary arterial hypertension. (2016). The Medical letter on drugs and therapeutics, 58(1488), 21–23.
- Sikirica, M., Iorga, S. R., Bancroft, T., & Potash, J. (2014). The economic burden of pulmonary arterial hypertension (PAH) in the US on payers and patients. BMC health services research, 14, 676. [CrossRef]
- Ogbomo, A., Tsang, Y., Mallampati, R., & Panjabi, S. (2022). The direct and indirect health care costs associated with pulmonary arterial hypertension among commercially insured patients in the United States. Journal of managed care & specialty pharmacy, 28(6), 608–616. [CrossRef]
- Sherif, A. A., Gilvaz, V. J., Abraham, S., Saji, A. M., Mathew, D., Isath, A., Rajendran, A., Contreras, J., Lanier, G. M., & Reginato, A. M. (2024). Systemic sclerosis is associated with increased in-patient mortality in patients hospitalized for heart failure. ESC heart failure, 10.1002/ehf2.14457. Advance online publication. [CrossRef]
- Said, Q., Martin, B. C., Joish, V. N., Kreilick, C., & Mathai, S. C. (2012). The cost to managed care of managing pulmonary hypertension. Journal of medical economics, 15(3), 500–508. [CrossRef]
- Weiss, T., Near, A. M., Zhao, X., Ramey, D. R., Banerji, T., Xie, H., & Nathan, S. D. (2023). Healthcare resource utilization in patients with pulmonary hypertension associated with chronic obstructive pulmonary disease (PH-COPD): a real-world data analysis. BMC pulmonary medicine, 23(1), 455. [CrossRef]
- Delcroix, M., & Howard, L. (2015). Pulmonary arterial hypertension: the burden of disease and impact on quality of life. European respiratory review : an official journal of the European Respiratory Society, 24(138), 621–629. [CrossRef]
- Fuge, J., Park, D. H., von Lengerke, T., Richter, M. J., Gall, H., Ghofrani, H. A., Kamp, J. C., Hoeper, M. M., & Olsson, K. M. (2022). Impact of Pulmonary Arterial Hypertension on Employment, Work Productivity, and Quality of Life - Results of a Cross-Sectional Multi-Center Study. Frontiers in psychiatry, 12, 781532. [CrossRef]
- Runheim, H., Kjellström, B., Beaudet, A., Ivarsson, B., Husberg, M., Pillai, N., Levin, L. Å., & Bernfort, L. (2023). Societal costs associated with pulmonary arterial hypertension: A study utilizing linked national registries. Pulmonary circulation, 13(1), e12190. [CrossRef]
- Kjellström, B., Runheim, H., Beaudet, A., Husberg, M., Ivarsson, B., Pillai, N., Levin, L. Å., & Bernfort, L. (2023). Societal costs associated to chronic thromboembolic pulmonary hypertension: A study utilizing linked national registries. Pulmonary circulation, 13(2), e12254. [CrossRef]
- Tuder, R. M., Abman, S. H., Braun, T., Capron, F., Stevens, T., Thistlethwaite, P. A., & Haworth, S. G. (2009). Development and pathology of pulmonary hypertension. Journal of the American College of Cardiology, 54(1 Suppl), S3–S9. [CrossRef]
- Stenmark, K. R., Gerasimovskaya, E., Nemenoff, R. A., & Das, M. (2002). Hypoxic activation of adventitial fibroblasts: role in vascular remodeling. Chest, 122(6 Suppl), 326S–334S. [CrossRef]
- Davie, N. J., Crossno, J. T., Jr, Frid, M. G., Hofmeister, S. E., Reeves, J. T., Hyde, D. M., Carpenter, T. C., Brunetti, J. A., McNiece, I. K., & Stenmark, K. R. (2004). Hypoxia-induced pulmonary artery adventitial remodeling and neovascularization: contribution of progenitor cells. American journal of physiology. Lung cellular and molecular physiology, 286(4), L668–L678. [CrossRef]
- Stacher, E., Graham, B. B., Hunt, J. M., Gandjeva, A., Groshong, S. D., McLaughlin, V. V., Jessup, M., Grizzle, W. E., Aldred, M. A., Cool, C. D., & Tuder, R. M. (2012). Modern age pathology of pulmonary arterial hypertension. American journal of respiratory and critical care medicine, 186(3), 261–272. [CrossRef]
- Chazova, I., Loyd, J. E., Zhdanov, V. S., Newman, J. H., Belenkov, Y., & Meyrick, B. (1995). Pulmonary artery adventitial changes and venous involvement in primary pulmonary hypertension. The American journal of pathology, 146(2), 389–397.
- Tuder R. M. (2017). Pulmonary vascular remodeling in pulmonary hypertension. Cell and tissue research, 367(3), 643–649. [CrossRef]
- Delcroix, M., Torbicki, A., Gopalan, D., Sitbon, O., Klok, F. A., Lang, I., Jenkins, D., Kim, N. H., Humbert, M., Jais, X., Vonk Noordegraaf, A., Pepke-Zaba, J., Brénot, P., Dorfmuller, P., Fadel, E., Ghofrani, H. A., Hoeper, M. M., Jansa, P., Madani, M., Matsubara, H., … Simonneau, G. (2021). ERS statement on chronic thromboembolic pulmonary hypertension. The European respiratory journal, 57(6), 2002828. [CrossRef]
- Giaid, A., Yanagisawa, M., Langleben, D., Michel, R. P., Levy, R., Shennib, H., Kimura, S., Masaki, T., Duguid, W. P., & Stewart, D. J. (1993). Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. The New England journal of medicine, 328(24), 1732–1739. [CrossRef]
- Reesink, H. J., Meijer, R. C., Lutter, R., Boomsma, F., Jansen, H. M., Kloek, J. J., & Bresser, P. (2006). Hemodynamic and clinical correlates of endothelin-1 in chronic thromboembolic pulmonary hypertension. Circulation journal : official journal of the Japanese Circulation Society, 70(8), 1058–1063. [CrossRef]
- Goerre, S., Wenk, M., Bärtsch, P., Lüscher, T. F., Niroomand, F., Hohenhaus, E., Oelz, O., & Reinhart, W. H. (1995). Endothelin-1 in pulmonary hypertension associated with high-altitude exposure. Circulation, 91(2), 359–364.
- Cacoub, P., Dorent, R., Nataf, P., Carayon, A., Riquet, M., Noe, E., Piette, J. C., Godeau, P., & Gandjbakhch, I. (1997). Endothelin-1 in the lungs of patients with pulmonary hypertension. Cardiovascular research, 33(1), 196–200. [CrossRef]
- Liu, R., Yuan, T., Wang, R., Gong, D., Wang, S., Du, G., & Fang, L. (2023). Insights into Endothelin Receptors in Pulmonary Hypertension. International journal of molecular sciences, 24(12), 10206. [CrossRef]
- Brewster, L. M., Garcia, V. P., Levy, M. V., Stockelman, K. A., Goulding, A., DeSouza, N. M., Greiner, J. J., Hijmans, J. G., & DeSouza, C. A. (2020). Endothelin-1-induced endothelial microvesicles impair endothelial cell function. Journal of applied physiology (Bethesda, Md. : 1985), 128(6), 1497–1505. [CrossRef]
- Marsden, P. A., Danthuluri, N. R., Brenner, B. M., Ballermann, B. J., & Brock, T. A. (1989). Endothelin action on vascular smooth muscle involves inositol trisphosphate and calcium mobilization. Biochemical and biophysical research communications, 158(1), 86–93. [CrossRef]
- Zhang, Y. M., Wang, K. Q., Zhou, G. M., Zuo, J., & Ge, J. B. (2003). Endothelin-1 promoted proliferation of vascular smooth muscle cell through pathway of extracellular signal-regulated kinase and cyclin D1. Acta pharmacologica Sinica, 24(6), 563–568.
- Douglas, S. A., & Ohlstein, E. H. (1997). Signal transduction mechanisms mediating the vascular actions of endothelin. Journal of vascular research, 34(3), 152–164. [CrossRef]
- Simonson, M. S., Wann, S., Mené, P., Dubyak, G. R., Kester, M., Nakazato, Y., Sedor, J. R., & Dunn, M. J. (1989). Endothelin stimulates phospholipase C, Na+/H+ exchange, c-fos expression, and mitogenesis in rat mesangial cells. The Journal of clinical investigation, 83(2), 708–712. [CrossRef]
- Rubin, L. J., Badesch, D. B., Barst, R. J., Galie, N., Black, C. M., Keogh, A., Pulido, T., Frost, A., Roux, S., Leconte, I., Landzberg, M., & Simonneau, G. (2002). Bosentan therapy for pulmonary arterial hypertension. The New England journal of medicine, 346(12), 896–903. [CrossRef]
- Galiè, N., Rubin, L.j, Hoeper, M., Jansa, P., Al-Hiti, H., Meyer, G., Chiossi, E., Kusic-Pajic, A., & Simonneau, G. (2008). Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet (London, England), 371(9630), 2093–2100. [CrossRef]
- Pulido, T., Adzerikho, I., Channick, R. N., Delcroix, M., Galiè, N., Ghofrani, H. A., Jansa, P., Jing, Z. C., Le Brun, F. O., Mehta, S., Mittelholzer, C. M., Perchenet, L., Sastry, B. K., Sitbon, O., Souza, R., Torbicki, A., Zeng, X., Rubin, L. J., Simonneau, G., & SERAPHIN Investigators (2013). Macitentan and morbidity and mortality in pulmonary arterial hypertension. The New England journal of medicine, 369(9), 809–818. [CrossRef]
- Galiè, N., Olschewski, H., Oudiz, R. J., Torres, F., Frost, A., Ghofrani, H. A., Badesch, D. B., McGoon, M. D., McLaughlin, V. V., Roecker, E. B., Gerber, M. J., Dufton, C., Wiens, B. L., Rubin, L. J., & Ambrisentan in Pulmonary Arterial Hypertension, Randomized, Double-Blind, Placebo-Controlled, Multicenter, Efficacy Studies (ARIES) Group (2008). Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation, 117(23), 3010–3019. [CrossRef]
- Koller, B., Steringer-Mascherbauer, R., Ebner, C. H., Weber, T., Ammer, M., Eichinger, J., Pretsch, I., Herold, M., Schwaiger, J., Ulmer, H., & Grander, W. (2017). Pilot Study of Endothelin Receptor Blockade in Heart Failure with Diastolic Dysfunction and Pulmonary Hypertension (BADDHY-Trial). Heart, lung & circulation, 26(5), 433–441. [CrossRef]
- Vachiéry, J. L., Delcroix, M., Al-Hiti, H., Efficace, M., Hutyra, M., Lack, G., Papadakis, K., & Rubin, L. J. (2018). Macitentan in pulmonary hypertension due to left ventricular dysfunction. The European respiratory journal, 51(2), 1701886. [CrossRef]
- Packer, M., McMurray, J. J. V., Krum, H., Kiowski, W., Massie, B. M., Caspi, A., Pratt, C. M., Petrie, M. C., DeMets, D., Kobrin, I., Roux, S., Swedberg, K., & ENABLE Investigators and Committees (2017). Long-Term Effect of Endothelin Receptor Antagonism With Bosentan on the Morbidity and Mortality of Patients With Severe Chronic Heart Failure: Primary Results of the ENABLE Trials. JACC. Heart failure, 5(5), 317–326. [CrossRef]
- Park, J., Song, J. H., Park, D. A., Lee, J. S., Lee, S. D., & Oh, Y. M. (2013). Systematic review and meta-analysis of pulmonary hypertension specific therapy for exercise capacity in chronic obstructive pulmonary disease. Journal of Korean medical science, 28(8), 1200–1206. [CrossRef]
- Giaid, A., & Saleh, D. (1995). Reduced expression of endothelial nitric oxide synthase in the lungs of patients with pulmonary hypertension. The New England journal of medicine, 333(4), 214–221. [CrossRef]
- Nagendran, J., Archer, S. L., Soliman, D., Gurtu, V., Moudgil, R., Haromy, A., St Aubin, C., Webster, L., Rebeyka, I. M., Ross, D. B., Light, P. E., Dyck, J. R., & Michelakis, E. D. (2007). Phosphodiesterase type 5 is highly expressed in the hypertrophied human right ventricle, and acute inhibition of phosphodiesterase type 5 improves contractility. Circulation, 116(3), 238–248. [CrossRef]
- Wharton, J., Strange, J. W., Møller, G. M., Growcott, E. J., Ren, X., Franklyn, A. P., Phillips, S. C., & Wilkins, M. R. (2005). Antiproliferative effects of phosphodiesterase type 5 inhibition in human pulmonary artery cells. American journal of respiratory and critical care medicine, 172(1), 105–113. [CrossRef]
- Galiè, N., Ghofrani, H. A., Torbicki, A., Barst, R. J., Rubin, L. J., Badesch, D., Fleming, T., Parpia, T., Burgess, G., Branzi, A., Grimminger, F., Kurzyna, M., Simonneau, G., & Sildenafil Use in Pulmonary Arterial Hypertension (SUPER) Study Group (2005). Sildenafil citrate therapy for pulmonary arterial hypertension. The New England journal of medicine, 353(20), 2148–2157. [CrossRef]
- Galiè, N., Brundage, B. H., Ghofrani, H. A., Oudiz, R. J., Simonneau, G., Safdar, Z., Shapiro, S., White, R. J., Chan, M., Beardsworth, A., Frumkin, L., Barst, R. J., & Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) Study Group (2009). Tadalafil therapy for pulmonary arterial hypertension. Circulation, 119(22), 2894–2903. [CrossRef]
- Ghofrani, H. A., D'Armini, A. M., Grimminger, F., Hoeper, M. M., Jansa, P., Kim, N. H., Mayer, E., Simonneau, G., Wilkins, M. R., Fritsch, A., Neuser, D., Weimann, G., Wang, C., & CHEST-1 Study Group (2013). Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. The New England journal of medicine, 369(4), 319–329. [CrossRef]
- Tuder, R. M., Cool, C. D., Geraci, M. W., Wang, J., Abman, S. H., Wright, L., Badesch, D., & Voelkel, N. F. (1999). Prostacyclin synthase expression is decreased in lungs from patients with severe pulmonary hypertension. American journal of respiratory and critical care medicine, 159(6), 1925–1932. [CrossRef]
- Barst, R. J., Rubin, L. J., Long, W. A., McGoon, M. D., Rich, S., Badesch, D. B., Groves, B. M., Tapson, V. F., Bourge, R. C., Brundage, B. H., Koerner, S. K., Langleben, D., Keller, C. A., Murali, S., Uretsky, B. F., Clayton, L. M., Jöbsis, M. M., Blackburn, S. D., Shortino, D., Crow, J. W., … Primary Pulmonary Hypertension Study Group (1996). A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The New England journal of medicine, 334(5), 296–301. [CrossRef]
- Badesch, D. B., Tapson, V. F., McGoon, M. D., Brundage, B. H., Rubin, L. J., Wigley, F. M., Rich, S., Barst, R. J., Barrett, P. S., Kral, K. M., Jöbsis, M. M., Loyd, J. E., Murali, S., Frost, A., Girgis, R., Bourge, R. C., Ralph, D. D., Elliott, C. G., Hill, N. S., Langleben, D., … Medsger, T. A., Jr (2000). Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Annals of internal medicine, 132(6), 425–434. [CrossRef]
- Tjen-A-Looi, S., Ekman, R., Lippton, H., Cary, J., & Keith, I. (1992). CGRP and somatostatin modulate chronic hypoxic pulmonary hypertension. The American journal of physiology, 263(3 Pt 2), H681–H690. [CrossRef]
- Keith, I. M., & Ekman, R. (1992). Dynamic aspects of regulatory lung peptides in chronic hypoxic pulmonary hypertension. Experimental lung research, 18(2), 205–224. [CrossRef]
- Champion, H. C., Bivalacqua, T. J., Lambert, D. G., McNamara, D. B., & Kadowitz, P. J. (1999). The influence of candesartan and PD123319 on responses to angiotensin II in the hindquarters vascular bed of the rat. Journal of the American Society of Nephrology : JASN, 10 Suppl 11, S95–S97.
- Yan, X., Huang, J., Zeng, Y., Zhong, X., Fu, Y., Xiao, H., Wang, X., Lian, H., Luo, H., Li, D., & Guo, R. (2024). CGRP attenuates pulmonary vascular remodeling by inhibiting the cGAS-STING-NFκB pathway in pulmonary arterial hypertension. Biochemical pharmacology, 222, 116093. [CrossRef]
- Sylvester, J. T., Shimoda, L. A., Aaronson, P. I., & Ward, J. P. (2012). Hypoxic pulmonary vasoconstriction. Physiological reviews, 92(1), 367–520. [CrossRef]
- Rawat, M., Lakshminrusimha, S., & Vento, M. (2022). Pulmonary hypertension and oxidative stress: Where is the link?. Seminars in fetal & neonatal medicine, 27(4), 101347. [CrossRef]
- Tjen-A-Looi, S.C., Fu, LW., Nguyen, A.T., Gong, Y., Malik, S. (2022). Autonomic Function and Electroacupuncture. In: Xia, Y. (eds) Advanced Acupuncture Research: From Bench to Bedside. Springer, Cham. [CrossRef]
- Tjen-A-Looi, S., Kraiczi, H., Ekman, R., & Keith, I. M. (1998). Sensory CGRP depletion by capsaicin exacerbates hypoxia-induced pulmonary hypertension in rats. Regulatory peptides, 74(1), 1–10. [CrossRef]
- Johnson, D. E., & Georgieff, M. K. (1989). Pulmonary neuroendocrine cells. Their secretory products and their potential roles in health and chronic lung disease in infancy. The American review of respiratory disease, 140(6), 1807–1812. [CrossRef]
- Heath, D., Yacoub, M., Gosney, J. R., Madden, B., Caslin, A. W., & Smith, P. (1990). Pulmonary endocrine cells in hypertensive pulmonary vascular disease. Histopathology, 16(1), 21–28. [CrossRef]
- Fu, X. W., Nurse, C. A., Wong, V., & Cutz, E. (2002). Hypoxia-induced secretion of serotonin from intact pulmonary neuroepithelial bodies in neonatal rabbit. The Journal of physiology, 539(Pt 2), 503–510. [CrossRef]
- Eddahibi, S., Raffestin, B., Hamon, M., & Adnot, S. (2002). Is the serotonin transporter involved in the pathogenesis of pulmonary hypertension?. The Journal of laboratory and clinical medicine, 139(4), 194–201. [CrossRef]
- Chambers, C. D., Hernandez-Diaz, S., Van Marter, L. J., Werler, M. M., Louik, C., Jones, K. L., & Mitchell, A. A. (2006). Selective serotonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. The New England journal of medicine, 354(6), 579–587. [CrossRef]
- McQuillan, L. P., Leung, G. K., Marsden, P. A., Kostyk, S. K., & Kourembanas, S. (1994). Hypoxia inhibits expression of eNOS via transcriptional and posttranscriptional mechanisms. The American journal of physiology, 267(5 Pt 2), H1921–H1927. [CrossRef]
- Kalinowski, L., Janaszak-Jasiecka, A., Siekierzycka, A., Bartoszewska, S., Woźniak, M., Lejnowski, D., Collawn, J. F., & Bartoszewski, R. (2016). Posttranscriptional and transcriptional regulation of endothelial nitric-oxide synthase during hypoxia: the role of microRNAs. Cellular & molecular biology letters, 21, 16. [CrossRef]
- Xu, W., Kaneko, F. T., Zheng, S., Comhair, S. A., Janocha, A. J., Goggans, T., Thunnissen, F. B., Farver, C., Hazen, S. L., Jennings, C., Dweik, R. A., Arroliga, A. C., & Erzurum, S. C. (2004). Increased arginase II and decreased NO synthesis in endothelial cells of patients with pulmonary arterial hypertension. FASEB journal : official publication of the Federation of American Societies for Experimental Biology, 18(14), 1746–1748. [CrossRef]
- Jaitovich, A., & Jourd'heuil, D. (2017). A Brief Overview of Nitric Oxide and Reactive Oxygen Species Signaling in Hypoxia-Induced Pulmonary Hypertension. Advances in experimental medicine and biology, 967, 71–81. [CrossRef]
- Zhao, Y. Y., Zhao, Y. D., Mirza, M. K., Huang, J. H., Potula, H. H., Vogel, S. M., Brovkovych, V., Yuan, J. X., Wharton, J., & Malik, A. B. (2009). Persistent eNOS activation secondary to caveolin-1 deficiency induces pulmonary hypertension in mice and humans through PKG nitration. The Journal of clinical investigation, 119(7), 2009–2018. [CrossRef]
- Block, E. R., Herrera, H., & Couch, M. (1995). Hypoxia inhibits L-arginine uptake by pulmonary artery endothelial cells. The American journal of physiology, 269(5 Pt 1), L574–L580. [CrossRef]
- Yamashita, K., Discher, D. J., Hu, J., Bishopric, N. H., & Webster, K. A. (2001). Molecular regulation of the endothelin-1 gene by hypoxia. Contributions of hypoxia-inducible factor-1, activator protein-1, GATA-2, AND p300/CBP. The Journal of biological chemistry, 276(16), 12645–12653. [CrossRef]
- Tuder, R. M., Chacon, M., Alger, L., Wang, J., Taraseviciene-Stewart, L., Kasahara, Y., Cool, C. D., Bishop, A. E., Geraci, M., Semenza, G. L., Yacoub, M., Polak, J. M., & Voelkel, N. F. (2001). Expression of angiogenesis-related molecules in plexiform lesions in severe pulmonary hypertension: evidence for a process of disordered angiogenesis. The Journal of pathology, 195(3), 367–374. [CrossRef]
- Alba, G. A., Samokhin, A. O., Wang, R. S., Zhang, Y. Y., Wertheim, B. M., Arons, E., Greenfield, E. A., Lundberg Slingsby, M. H., Ceglowski, J. R., Haley, K. J., Bowman, F. P., Yu, Y. R., Haney, J. C., Eng, G., Mitchell, R. N., Sheets, A., Vargas, S. O., Seo, S., Channick, R. N., Leary, P. J., … Maron, B. A. (2021). NEDD9 Is a Novel and Modifiable Mediator of Platelet-Endothelial Adhesion in the Pulmonary Circulation. American journal of respiratory and critical care medicine, 203(12), 1533–1545. [CrossRef]
- Chai, X., Sun, D., Han, Q., Yi, L., Wu, Y., & Liu, X. (2018). Hypoxia induces pulmonary arterial fibroblast proliferation, migration, differentiation and vascular remodeling via the PI3K/Akt/p70S6K signaling pathway. International journal of molecular medicine, 41(5), 2461–2472. [CrossRef]
- Ryanto, G. R. T., Ikeda, K., Miyagawa, K., Tu, L., Guignabert, C., Humbert, M., Fujiyama, T., Yanagisawa, M., Hirata, K. I., & Emoto, N. (2021). An endothelial activin A-bone morphogenetic protein receptor type 2 link is overdriven in pulmonary hypertension. Nature communications, 12(1), 1720. [CrossRef]
- Merfeld-Clauss, S., Lu, H., Wu, X., March, K. L., & Traktuev, D. O. (2018). Hypoxia-induced activin A diminishes endothelial cell vasculogenic activity. Journal of cellular and molecular medicine, 22(1), 173–184. [CrossRef]
- Macias, D., Moore, S., Crosby, A., Southwood, M., Du, X., Tan, H., Xie, S., Vassallo, A., Wood, A. J. T., Wallace, E. M., & Cowburn, A. S. (2021). Targeting HIF2α-ARNT hetero-dimerisation as a novel therapeutic strategy for pulmonary arterial hypertension. The European respiratory journal, 57(3), 1902061. [CrossRef]
- Dai, Z., Zhu, M. M., Peng, Y., Machireddy, N., Evans, C. E., Machado, R., Zhang, X., & Zhao, Y. Y. (2018). Therapeutic Targeting of Vascular Remodeling and Right Heart Failure in Pulmonary Arterial Hypertension with a HIF-2α Inhibitor. American journal of respiratory and critical care medicine, 198(11), 1423–1434. [CrossRef]
- Chen, T., Zhou, Q., Tang, H., Bozkanat, M., Yuan, J. X., Raj, J. U., & Zhou, G. (2016). miR-17/20 Controls Prolyl Hydroxylase 2 (PHD2)/Hypoxia-Inducible Factor 1 (HIF1) to Regulate Pulmonary Artery Smooth Muscle Cell Proliferation. Journal of the American Heart Association, 5(12), e004510. [CrossRef]
- Docherty, C. K., Nilsen, M., & MacLean, M. R. (2019). Influence of 2-Methoxyestradiol and Sex on Hypoxia-Induced Pulmonary Hypertension and Hypoxia-Inducible Factor-1-α. Journal of the American Heart Association, 8(5), e011628. [CrossRef]
- Jiang, Y., Zhou, Y., Peng, G., Liu, N., Tian, H., Pan, D., Liu, L., Yang, X., Li, C., Li, W., Chen, L., Ran, P., & Dai, A. (2018). Topotecan prevents hypoxia-induced pulmonary arterial hypertension and inhibits hypoxia-inducible factor-1α and TRPC channels. The international journal of biochemistry & cell biology, 104, 161–170. [CrossRef]
- Cheng, C. C., Chi, P. L., Shen, M. C., Shu, C. W., Wann, S. R., Liu, C. P., Tseng, C. J., & Huang, W. C. (2019). Caffeic Acid Phenethyl Ester Rescues Pulmonary Arterial Hypertension through the Inhibition of AKT/ERK-Dependent PDGF/HIF-1α In Vitro and In Vivo. International journal of molecular sciences, 20(6), 1468. [CrossRef]
- Luo, Y., Teng, X., Zhang, L., Chen, J., Liu, Z., Chen, X., Zhao, S., Yang, S., Feng, J., & Yan, X. (2019). CD146-HIF-1α hypoxic reprogramming drives vascular remodeling and pulmonary arterial hypertension. Nature communications, 10(1), 3551. [CrossRef]
- Sandoval, J., Aguirre, J. S., Pulido, T., Martinez-Guerra, M. L., Santos, E., Alvarado, P., Rosas, M., & Bautista, E. (2001). Nocturnal oxygen therapy in patients with the Eisenmenger syndrome. American journal of respiratory and critical care medicine, 164(9), 1682–1687. [CrossRef]
- Green, S., & Stuart, D. (2021). Oxygen and pulmonary arterial hypertension: effects, mechanisms, and therapeutic benefits. European journal of preventive cardiology, 28(1), 127–136. [CrossRef]
- Din, S., Sarathchandra, P., Yacoub, M. H., & Chester, A. H. (2009). Interaction between bone morphogenetic proteins and endothelin-1 in human pulmonary artery smooth muscle. Vascular pharmacology, 51(5-6), 344–349. [CrossRef]
- Maruyama, H., Dewachter, C., Belhaj, A., Rondelet, B., Sakai, S., Remmelink, M., Vachiery, J. L., Naeije, R., & Dewachter, L. (2015). Endothelin-Bone morphogenetic protein type 2 receptor interaction induces pulmonary artery smooth muscle cell hyperplasia in pulmonary arterial hypertension. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation, 34(3), 468–478. [CrossRef]
- Soon, E., Crosby, A., Southwood, M., Yang, P., Tajsic, T., Toshner, M., Appleby, S., Shanahan, C. M., Bloch, K. D., Pepke-Zaba, J., Upton, P., & Morrell, N. W. (2015). Bone morphogenetic protein receptor type II deficiency and increased inflammatory cytokine production. A gateway to pulmonary arterial hypertension. American journal of respiratory and critical care medicine, 192(7), 859–872. [CrossRef]
- Talati, M., West, J., Zaynagetdinov, R., Hong, C. C., Han, W., Blackwell, T., Robinson, L., Blackwell, T. S., & Lane, K. (2014). BMP pathway regulation of and by macrophages. PloS one, 9(4), e94119. [CrossRef]
- Kim, C. W., Song, H., Kumar, S., Nam, D., Kwon, H. S., Chang, K. H., Son, D. J., Kang, D. W., Brodie, S. A., Weiss, D., Vega, J. D., Alberts-Grill, N., Griendling, K., Taylor, W. R., & Jo, H. (2013). Anti-inflammatory and antiatherogenic role of BMP receptor II in endothelial cells. Arteriosclerosis, thrombosis, and vascular biology, 33(6), 1350–1359. [CrossRef]
- Diebold, I., Hennigs, J. K., Miyagawa, K., Li, C. G., Nickel, N. P., Kaschwich, M., Cao, A., Wang, L., Reddy, S., Chen, P. I., Nakahira, K., Alcazar, M. A., Hopper, R. K., Ji, L., Feldman, B. J., & Rabinovitch, M. (2015). BMPR2 preserves mitochondrial function and DNA during reoxygenation to promote endothelial cell survival and reverse pulmonary hypertension. Cell metabolism, 21(4), 596–608. [CrossRef]
- Sutendra, G., & Michelakis, E. D. (2014). The metabolic basis of pulmonary arterial hypertension. Cell metabolism, 19(4), 558–573. [CrossRef]
- Palakeel, J. J., Ali, M., Chaduvula, P., Chhabra, S., Lamsal Lamichhane, S., Ramesh, V., Opara, C. O., Khan, F. Y., Kabiraj, G., Kauser, H., & Mostafa, J. A. (2022). An Outlook on the Etiopathogenesis of Pulmonary Hypertension in HIV. Cureus, 14(7), e27390. [CrossRef]
- Ryanto, G. R. T., Musthafa, A., Hara, T., & Emoto, N. (2023). Inactivating the Uninhibited: The Tale of Activins and Inhibins in Pulmonary Arterial Hypertension. International journal of molecular sciences, 24(4), 3332. [CrossRef]
- Olsen, O. E., Sankar, M., Elsaadi, S., Hella, H., Buene, G., Darvekar, S. R., Misund, K., Katagiri, T., Knaus, P., & Holien, T. (2018). BMPR2 inhibits activin and BMP signaling via wild-type ALK2. Journal of cell science, 131(11), jcs213512. [CrossRef]
- Humbert, M., McLaughlin, V., Gibbs, J. S. R., Gomberg-Maitland, M., Hoeper, M. M., Preston, I. R., Souza, R., Waxman, A., Escribano Subias, P., Feldman, J., Meyer, G., Montani, D., Olsson, K. M., Manimaran, S., Barnes, J., Linde, P. G., de Oliveira Pena, J., Badesch, D. B., & PULSAR Trial Investigators (2021). Sotatercept for the Treatment of Pulmonary Arterial Hypertension. The New England journal of medicine, 384(13), 1204–1215. [CrossRef]
- Hoeper, M. M., Badesch, D. B., Ghofrani, H. A., Gibbs, J. S. R., Gomberg-Maitland, M., McLaughlin, V. V., Preston, I. R., Souza, R., Waxman, A. B., Grünig, E., Kopeć, G., Meyer, G., Olsson, K. M., Rosenkranz, S., Xu, Y., Miller, B., Fowler, M., Butler, J., Koglin, J., de Oliveira Pena, J., … STELLAR Trial Investigators (2023). Phase 3 Trial of Sotatercept for Treatment of Pulmonary Arterial Hypertension. The New England journal of medicine, 388(16), 1478–1490. [CrossRef]
- Soon, E., Holmes, A. M., Treacy, C. M., Doughty, N. J., Southgate, L., Machado, R. D., Trembath, R. C., Jennings, S., Barker, L., Nicklin, P., Walker, C., Budd, D. C., Pepke-Zaba, J., & Morrell, N. W. (2010). Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension. Circulation, 122(9), 920–927. [CrossRef]
- Hurst, L. A., Dunmore, B. J., Long, L., Crosby, A., Al-Lamki, R., Deighton, J., Southwood, M., Yang, X., Nikolic, M. Z., Herrera, B., Inman, G. J., Bradley, J. R., Rana, A. A., Upton, P. D., & Morrell, N. W. (2017). TNFα drives pulmonary arterial hypertension by suppressing the BMP type-II receptor and altering NOTCH signaling. Nature communications, 8, 14079. [CrossRef]
- Aliotta, J. M., Pereira, M., Wen, S., Dooner, M. S., Del Tatto, M., Papa, E., Goldberg, L. R., Baird, G. L., Ventetuolo, C. E., Quesenberry, P. J., & Klinger, J. R. (2016). Exosomes induce and reverse monocrotaline-induced pulmonary hypertension in mice. Cardiovascular research, 110(3), 319–330. [CrossRef]
- Shen, Y., Goncharov, D. A., Pena, A., Baust, J., Chavez Barragan, A., Ray, A., Rode, A., Bachman, T. N., Chang, B., Jiang, L., Dieffenbach, P., Fredenburgh, L. E., Rojas, M., DeLisser, H., Mora, A. L., Kudryashova, T. V., & Goncharova, E. A. (2022). Cross-talk between TSC2 and the extracellular matrix controls pulmonary vascular proliferation and pulmonary hypertension. Science signaling, 15(763), eabn2743. [CrossRef]
- Tuder, R. M., Marecki, J. C., Richter, A., Fijalkowska, I., & Flores, S. (2007). Pathology of pulmonary hypertension. Clinics in chest medicine, 28(1), 23–vii. [CrossRef]
- Heath, D., & Yacoub, M. (1991). Lung mast cells in plexogenic pulmonary arteriopathy. Journal of clinical pathology, 44(12), 1003–1006. [CrossRef]
- Perros, F., Dorfmüller, P., Souza, R., Durand-Gasselin, I., Mussot, S., Mazmanian, M., Hervé, P., Emilie, D., Simonneau, G., & Humbert, M. (2007). Dendritic cell recruitment in lesions of human and experimental pulmonary hypertension. The European respiratory journal, 29(3), 462–468. [CrossRef]
- Tuder, R. M., Groves, B., Badesch, D. B., & Voelkel, N. F. (1994). Exuberant endothelial cell growth and elements of inflammation are present in plexiform lesions of pulmonary hypertension. The American journal of pathology, 144(2), 275–285.
- Humbert, M., Monti, G., Brenot, F., Sitbon, O., Portier, A., Grangeot-Keros, L., Duroux, P., Galanaud, P., Simonneau, G., & Emilie, D. (1995). Increased interleukin-1 and interleukin-6 serum concentrations in severe primary pulmonary hypertension. American journal of respiratory and critical care medicine, 151(5), 1628–1631. [CrossRef]
- Smolders, V. F. E. D., Lodder, K., Rodríguez, C., Tura-Ceide, O., Barberà, J. A., Jukema, J. W., Quax, P. H. A., Goumans, M. J., & Kurakula, K. (2021). The Inflammatory Profile of CTEPH-Derived Endothelial Cells Is a Possible Driver of Disease Progression. Cells, 10(4), 737. [CrossRef]
- Parpaleix, A., Amsellem, V., Houssaini, A., Abid, S., Breau, M., Marcos, E., Sawaki, D., Delcroix, M., Quarck, R., Maillard, A., Couillin, I., Ryffel, B., & Adnot, S. (2016). Role of interleukin-1 receptor 1/MyD88 signalling in the development and progression of pulmonary hypertension. The European respiratory journal, 48(2), 470–483. [CrossRef]
- Brock, M., Trenkmann, M., Gay, R. E., Michel, B. A., Gay, S., Fischler, M., Ulrich, S., Speich, R., & Huber, L. C. (2009). Interleukin-6 modulates the expression of the bone morphogenic protein receptor type II through a novel STAT3-microRNA cluster 17/92 pathway. Circulation research, 104(10), 1184–1191. [CrossRef]
- Steiner, M. K., Syrkina, O. L., Kolliputi, N., Mark, E. J., Hales, C. A., & Waxman, A. B. (2009). Interleukin-6 overexpression induces pulmonary hypertension. Circulation research, 104(2), 236–244. [CrossRef]
- Coll-Bonfill, N., Musri, M. M., Ivo, V., Barberà, J. A., & Tura-Ceide, O. (2015). Transdifferentiation of endothelial cells to smooth muscle cells play an important role in vascular remodelling. American journal of stem cells, 4(1), 13–21.
- Selimovic, N., Bergh, C. H., Andersson, B., Sakiniene, E., Carlsten, H., & Rundqvist, B. (2009). Growth factors and interleukin-6 across the lung circulation in pulmonary hypertension. The European respiratory journal, 34(3), 662–668. [CrossRef]
- Li, A., Varney, M. L., Valasek, J., Godfrey, M., Dave, B. J., & Singh, R. K. (2005). Autocrine role of interleukin-8 in induction of endothelial cell proliferation, survival, migration and MMP-2 production and angiogenesis. Angiogenesis, 8(1), 63–71. [CrossRef]
- Zimmermann, N., King, N. E., Laporte, J., Yang, M., Mishra, A., Pope, S. M., Muntel, E. E., Witte, D. P., Pegg, A. A., Foster, P. S., Hamid, Q., & Rothenberg, M. E. (2003). Dissection of experimental asthma with DNA microarray analysis identifies arginase in asthma pathogenesis. The Journal of clinical investigation, 111(12), 1863–1874. [CrossRef]
- Tamosiuniene, R., Tian, W., Dhillon, G., Wang, L., Sung, Y. K., Gera, L., Patterson, A. J., Agrawal, R., Rabinovitch, M., Ambler, K., Long, C. S., Voelkel, N. F., & Nicolls, M. R. (2011). Regulatory T cells limit vascular endothelial injury and prevent pulmonary hypertension. Circulation research, 109(8), 867–879. [CrossRef]
- Huertas, A., Tu, L., Gambaryan, N., Girerd, B., Perros, F., Montani, D., Fabre, D., Fadel, E., Eddahibi, S., Cohen-Kaminsky, S., Guignabert, C., & Humbert, M. (2012). Leptin and regulatory T-lymphocytes in idiopathic pulmonary arterial hypertension. The European respiratory journal, 40(4), 895–904. [CrossRef]
- Becker, M. O., Kill, A., Kutsche, M., Guenther, J., Rose, A., Tabeling, C., Witzenrath, M., Kühl, A. A., Heidecke, H., Ghofrani, H. A., Tiede, H., Schermuly, R. T., Nickel, N., Hoeper, M. M., Lukitsch, I., Gollasch, M., Kuebler, W. M., Bock, S., Burmester, G. R., Dragun, D., … Riemekasten, G. (2014). Vascular receptor autoantibodies in pulmonary arterial hypertension associated with systemic sclerosis. American journal of respiratory and critical care medicine, 190(7), 808–817. [CrossRef]
- Isern, R. A., Yaneva, M., Weiner, E., Parke, A., Rothfield, N., Dantzker, D., Rich, S., & Arnett, F. C. (1992). Autoantibodies in patients with primary pulmonary hypertension: association with anti-Ku. The American journal of medicine, 93(3), 307–312. [CrossRef]
- Zaid, Y., Puhm, F., Allaeys, I., Naya, A., Oudghiri, M., Khalki, L., Limami, Y., Zaid, N., Sadki, K., Ben El Haj, R., Mahir, W., Belayachi, L., Belefquih, B., Benouda, A., Cheikh, A., Langlois, M. A., Cherrah, Y., Flamand, L., Guessous, F., & Boilard, E. (2020). Platelets Can Associate with SARS-Cov-2 RNA and Are Hyperactivated in COVID-19. Circulation research, 127(11), 1404–1418. Advance online publication. [CrossRef]
- Connors, J. M., & Levy, J. H. (2020). COVID-19 and its implications for thrombosis and anticoagulation. Blood, 135(23), 2033–2040. [CrossRef]
- Voelkel, N. F., Tamosiuniene, R., & Nicolls, M. R. (2016). Challenges and opportunities in treating inflammation associated with pulmonary hypertension. Expert review of cardiovascular therapy, 14(8), 939–951. [CrossRef]
- Meloche, J., Renard, S., Provencher, S., & Bonnet, S. (2013). Anti-inflammatory and immunosuppressive agents in PAH. Handbook of experimental pharmacology, 218, 437–476. [CrossRef]
- Zamanian, R. T., Badesch, D., Chung, L., Domsic, R. T., Medsger, T., Pinckney, A., Keyes-Elstein, L., D'Aveta, C., Spychala, M., White, R. J., Hassoun, P. M., Torres, F., Sweatt, A. J., Molitor, J. A., Khanna, D., Maecker, H., Welch, B., Goldmuntz, E., & Nicolls, M. R. (2021). Safety and Efficacy of B-Cell Depletion with Rituximab for the Treatment of Systemic Sclerosis-associated Pulmonary Arterial Hypertension: A Multicenter, Double-Blind, Randomized, Placebo-controlled Trial. American journal of respiratory and critical care medicine, 204(2), 209–221. [CrossRef]
- Trankle, C. R., Canada, J. M., Kadariya, D., Markley, R., De Chazal, H. M., Pinson, J., Fox, A., Van Tassell, B. W., Abbate, A., & Grinnan, D. (2019). IL-1 Blockade Reduces Inflammation in Pulmonary Arterial Hypertension and Right Ventricular Failure: A Single-Arm, Open-Label, Phase IB/II Pilot Study. American journal of respiratory and critical care medicine, 199(3), 381–384. [CrossRef]
- Ghofrani, H. A., Simonneau, G., D'Armini, A. M., Fedullo, P., Howard, L. S., Jaïs, X., Jenkins, D. P., Jing, Z. C., Madani, M. M., Martin, N., Mayer, E., Papadakis, K., Richard, D., Kim, N. H., & MERIT study investigators (2024). Macitentan for the treatment of inoperable chronic thromboembolic pulmonary hypertension (MERIT-1): results from the multicentre, phase 2, randomised, double-blind, placebo-controlled study. The Lancet. Respiratory medicine, 12(4), e21–e30. [CrossRef]
- Ordi-Ros, J., Sáez-Comet, L., Pérez-Conesa, M., Vidal, X., Riera-Mestre, A., Castro-Salomó, A., Cuquet-Pedragosa, J., Ortiz-Santamaria, V., Mauri-Plana, M., Solé, C., & Cortés-Hernández, J. (2019). Rivaroxaban Versus Vitamin K Antagonist in Antiphospholipid Syndrome: A Randomized Noninferiority Trial. Annals of internal medicine, 171(10), 685–694. [CrossRef]
- Frank, H., Mlczoch, J., Huber, K., Schuster, E., Gurtner, H. P., & Kneussl, M. (1997). The effect of anticoagulant therapy in primary and anorectic drug-induced pulmonary hypertension. Chest, 112(3), 714–721. [CrossRef]
- Preston, I. R., Roberts, K. E., Miller, D. P., Sen, G. P., Selej, M., Benton, W. W., Hill, N. S., & Farber, H. W. (2015). Effect of Warfarin Treatment on Survival of Patients With Pulmonary Arterial Hypertension (PAH) in the Registry to Evaluate Early and Long-Term PAH Disease Management (REVEAL). Circulation, 132(25), 2403–2411. [CrossRef]
- Ehlken, N., Lichtblau, M., Klose, H., Weidenhammer, J., Fischer, C., Nechwatal, R., Uiker, S., Halank, M., Olsson, K., Seeger, W., Gall, H., Rosenkranz, S., Wilkens, H., Mertens, D., Seyfarth, H. J., Opitz, C., Ulrich, S., Egenlauf, B., & Grünig, E. (2016). Exercise training improves peak oxygen consumption and haemodynamics in patients with severe pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: a prospective, randomized, controlled trial. European heart journal, 37(1), 35–44. [CrossRef]
- Pandey, A., Garg, S., Khunger, M., Garg, S., Kumbhani, D. J., Chin, K. M., & Berry, J. D. (2015). Efficacy and Safety of Exercise Training in Chronic Pulmonary Hypertension: Systematic Review and Meta-Analysis. Circulation. Heart failure, 8(6), 1032–1043. [CrossRef]
- Velez-Roa, S., Ciarka, A., Najem, B., Vachiery, J. L., Naeije, R., & van de Borne, P. (2004). Increased sympathetic nerve activity in pulmonary artery hypertension. Circulation, 110(10), 1308–1312. [CrossRef]
- da Silva Gonçalves Bós, D., Van Der Bruggen, C. E. E., Kurakula, K., Sun, X. Q., Casali, K. R., Casali, A. G., Rol, N., Szulcek, R., Dos Remedios, C., Guignabert, C., Tu, L., Dorfmüller, P., Humbert, M., Wijnker, P. J. M., Kuster, D. W. D., van der Velden, J., Goumans, M. J., Bogaard, H. J., Vonk-Noordegraaf, A., de Man, F. S., … Handoko, M. L. (2018). Contribution of Impaired Parasympathetic Activity to Right Ventricular Dysfunction and Pulmonary Vascular Remodeling in Pulmonary Arterial Hypertension. Circulation, 137(9), 910–924. [CrossRef]
- Bristow, M. R., Ginsburg, R., Umans, V., Fowler, M., Minobe, W., Rasmussen, R., Zera, P., Menlove, R., Shah, P., & Jamieson, S. (1986). Beta 1- and beta 2-adrenergic-receptor subpopulations in nonfailing and failing human ventricular myocardium: coupling of both receptor subtypes to muscle contraction and selective beta 1-receptor down-regulation in heart failure. Circulation research, 59(3), 297–309. [CrossRef]
- Patel, M. K., Chan, P., Betteridge, L. J., Schachter, M., & Sever, P. S. (1995). Inhibition of human vascular smooth muscle cell proliferation by the novel multiple-action antihypertensive agent carvedilol. Journal of cardiovascular pharmacology, 25(4), 652–657. [CrossRef]
- Farha, S., Saygin, D., Park, M. M., Cheong, H. I., Asosingh, K., Comhair, S. A., Stephens, O. R., Roach, E. C., Sharp, J., Highland, K. B., DiFilippo, F. P., Neumann, D. R., Tang, W. H. W., & Erzurum, S. C. (2017). Pulmonary arterial hypertension treatment with carvedilol for heart failure: a randomized controlled trial. JCI insight, 2(16), e95240. [CrossRef]
- Bogaard, H. J., Natarajan, R., Mizuno, S., Abbate, A., Chang, P. J., Chau, V. Q., Hoke, N. N., Kraskauskas, D., Kasper, M., Salloum, F. N., & Voelkel, N. F. (2010). Adrenergic receptor blockade reverses right heart remodeling and dysfunction in pulmonary hypertensive rats. American journal of respiratory and critical care medicine, 182(5), 652–660. [CrossRef]
- Perros, F., Ranchoux, B., Izikki, M., Bentebbal, S., Happé, C., Antigny, F., Jourdon, P., Dorfmüller, P., Lecerf, F., Fadel, E., Simonneau, G., Humbert, M., Bogaard, H. J., & Eddahibi, S. (2015). Nebivolol for improving endothelial dysfunction, pulmonary vascular remodeling, and right heart function in pulmonary hypertension. Journal of the American College of Cardiology, 65(7), 668–680. [CrossRef]
- Kamp, O., Metra, M., Bugatti, S., Bettari, L., Dei Cas, A., Petrini, N., & Dei Cas, L. (2010). Nebivolol: haemodynamic effects and clinical significance of combined beta-blockade and nitric oxide release. Drugs, 70(1), 41–56. [CrossRef]
- Ishikawa, M., Sato, N., Asai, K., Takano, T., & Mizuno, K. (2009). Effects of a pure alpha/beta-adrenergic receptor blocker on monocrotaline-induced pulmonary arterial hypertension with right ventricular hypertrophy in rats. Circulation journal : official journal of the Japanese Circulation Society, 73(12), 2337–2341. [CrossRef]
- de Man, F. S., Handoko, M. L., van Ballegoij, J. J., Schalij, I., Bogaards, S. J., Postmus, P. E., van der Velden, J., Westerhof, N., Paulus, W. J., & Vonk-Noordegraaf, A. (2012). Bisoprolol delays progression towards right heart failure in experimental pulmonary hypertension. Circulation. Heart failure, 5(1), 97–105. [CrossRef]
- van Campen, J. S., de Boer, K., van de Veerdonk, M. C., van der Bruggen, C. E., Allaart, C. P., Raijmakers, P. G., Heymans, M. W., Marcus, J. T., Harms, H. J., Handoko, M. L., de Man, F. S., Vonk Noordegraaf, A., & Bogaard, H. J. (2016). Bisoprolol in idiopathic pulmonary arterial hypertension: an explorative study. The European respiratory journal, 48(3), 787–796. [CrossRef]
- Moretti, C., Grosso Marra, W., D'Ascenzo, F., Omedè, P., Cannillo, M., Libertucci, D., Fusaro, E., Meynet, I., Giordana, F., Salera, D., Annone, U., Chen, S. L., Marra, S., & Gaita, F. (2015). Beta blocker for patients with pulmonary arterial hypertension: A single center experience. International journal of cardiology, 184, 528–532. [CrossRef]
- Provencher, S., Herve, P., Jais, X., Lebrec, D., Humbert, M., Simonneau, G., & Sitbon, O. (2006). Deleterious effects of beta-blockers on exercise capacity and hemodynamics in patients with portopulmonary hypertension. Gastroenterology, 130(1), 120–126. [CrossRef]
- So, P. P., Davies, R. A., Chandy, G., Stewart, D., Beanlands, R. S., Haddad, H., Pugliese, C., & Mielniczuk, L. M. (2012). Usefulness of beta-blocker therapy and outcomes in patients with pulmonary arterial hypertension. The American journal of cardiology, 109(10), 1504–1509. [CrossRef]
- Martyniuk, T. V., Konosova, I. D., & Chazova, I. E. (2012). Terapevticheskii arkhiv, 84(12), 49–53.
- Karpov, A. A., Vachrushev, N. S., Shilenko, L. A., Smirnov, S. S., Bunenkov, N. S., Butskih, M. G., Chervaev, A. A., Vaulina, D. D., Ivkin, D. Y., Moiseeva, O. M., & Galagudza, M. M. (2023). Sympathetic Denervation and Pharmacological Stimulation of Parasympathetic Nervous System Prevent Pulmonary Vascular Bed Remodeling in Rat Model of Chronic Thromboembolic Pulmonary Hypertension. Journal of cardiovascular development and disease, 10(2), 40. [CrossRef]
- Xu, W., Wang, D. Y., Chen, Z. Y., Gao, Q., Zou, Y. L., Sun, D. H., Zhang, S., Zhao, X. B., Gong, Y. T., Zhang, Y., Zhang, D. X., & Li, Y. (2023). Noninvasive Stereotactic Radiotherapy for PADN in an Acute Canine Model of Pulmonary Arterial Hypertension. JACC. Basic to translational science, 9(2), 244–256. [CrossRef]
- Chen, S. L., Zhang, F. F., Xu, J., Xie, D. J., Zhou, L., Nguyen, T., & Stone, G. W. (2013). Pulmonary artery denervation to treat pulmonary arterial hypertension: the single-center, prospective, first-in-man PADN-1 study (first-in-man pulmonary artery denervation for treatment of pulmonary artery hypertension). Journal of the American College of Cardiology, 62(12), 1092–1100. [CrossRef]
- Rothman, A. M. K., Vachiery, J. L., Howard, L. S., Mikhail, G. W., Lang, I. M., Jonas, M., Kiely, D. G., Shav, D., Shabtay, O., Avriel, A., Lewis, G. D., Rosenzweig, E. B., Kirtane, A. J., Kim, N. H., Mahmud, E., McLaughlain, V. V., Chetcuti, S., Leon, M. B., Ben-Yehuda, O., & Rubin, L. J. (2020). Intravascular Ultrasound Pulmonary Artery Denervation to Treat Pulmonary Arterial Hypertension (TROPHY1): Multicenter, Early Feasibility Study. JACC. Cardiovascular interventions, 13(8), 989–999. [CrossRef]
- Liu, C., Jiang, X. M., Zhang, J., Li, B., Li, J., Xie, D. J., & Hu, Z. Y. (2016). Pulmonary artery denervation improves pulmonary arterial hypertension induced right ventricular dysfunction by modulating the local renin-angiotensin-aldosterone system. BMC cardiovascular disorders, 16(1), 192. [CrossRef]
- Na, S., Kim, O. S., Ryoo, S., Kweon, T. D., Choi, Y. S., Shim, H. S., & Oh, Y. J. (2014). Cervical ganglion block attenuates the progression of pulmonary hypertension via nitric oxide and arginase pathways. Hypertension (Dallas, Tex. : 1979), 63(2), 309–315. [CrossRef]
- Zhou, L., Zhang, J., Jiang, X. M., Xie, D. J., Wang, J. S., Li, L., Li, B., Wang, Z. M., Rothman, A. M. K., Lawrie, A., & Chen, S. L. (2015). Pulmonary Artery Denervation Attenuates Pulmonary Arterial Remodeling in Dogs with Pulmonary Arterial Hypertension Induced by Dehydrogenized Monocrotaline. JACC. Cardiovascular interventions, 8(15), 2013–2023. [CrossRef]
- Chen, S. L., Zhang, Y. J., Zhou, L., Xie, D. J., Zhang, F. F., Jia, H. B., Wong, S. S., & Kwan, T. W. (2013). Percutaneous pulmonary artery denervation completely abolishes experimental pulmonary arterial hypertension in vivo. EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology, 9(2), 269–276. [CrossRef]
- Rothman, A. M., Arnold, N. D., Chang, W., Watson, O., Swift, A. J., Condliffe, R., Elliot, C. A., Kiely, D. G., Suvarna, S. K., Gunn, J., & Lawrie, A. (2015). Pulmonary artery denervation reduces pulmonary artery pressure and induces histological changes in an acute porcine model of pulmonary hypertension. Circulation. Cardiovascular interventions, 8(11), e002569. [CrossRef]
- da Silva Gonçalves Bos, D., Happé, C., Schalij, I., Pijacka, W., Paton, J. F. R., Guignabert, C., Tu, L., Thuillet, R., Bogaard, H. J., van Rossum, A. C., Vonk-Noordegraaf, A., de Man, F. S., & Handoko, M. L. (2017). Renal Denervation Reduces Pulmonary Vascular Remodeling and Right Ventricular Diastolic Stiffness in Experimental Pulmonary Hypertension. JACC. Basic to translational science, 2(1), 22–35. [CrossRef]
- Qingyan, Z., Xuejun, J., Yanhong, T., Zixuan, D., Xiaozhan, W., Xule, W., Zongwen, G., Wei, H., Shengbo, Y., & Congxin, H. (2015). Beneficial Effects of Renal Denervation on Pulmonary Vascular Remodeling in Experimental Pulmonary Artery Hypertension. Revista espanola de cardiologia (English ed.), 68(7), 562–570. [CrossRef]
- Huang, Y., Liu, Y. W., Pan, H. Z., Zhang, X. L., Li, J., Xiang, L., Meng, J., Wang, P. H., Yang, J., Jing, Z. C., & Zhang, H. (2019). Transthoracic Pulmonary Artery Denervation for Pulmonary Arterial Hypertension. Arteriosclerosis, thrombosis, and vascular biology, 39(4), 704–718. [CrossRef]
- Chen, S. L., Zhang, H., Xie, D. J., Zhang, J., Zhou, L., Rothman, A. M., & Stone, G. W. (2015). Hemodynamic, functional, and clinical responses to pulmonary artery denervation in patients with pulmonary arterial hypertension of different causes: phase II results from the Pulmonary Artery Denervation-1 study. Circulation. Cardiovascular interventions, 8(11), e002837. [CrossRef]
- Zhang, H., Wei, Y., Zhang, C., Yang, Z., Kan, J., Gu, H., Fan, F., Gu, H., Wang, Q., Xie, D., Zhang, G., Guo, X., Yin, Y., Jin, B., Zhou, H., Yang, Z., Wang, Z., Xin, Y., Zhang, C., Meng, L., … Chen, S. L. (2022). Pulmonary Artery Denervation for Pulmonary Arterial Hypertension: A Sham-Controlled Randomized PADN-CFDA Trial. JACC. Cardiovascular interventions, 15(23), 2412–2423. [CrossRef]
- Rothman, A. M. K., Vachiery, J. L., Howard, L. S., Mikhail, G. W., Lang, I. M., Jonas, M., Kiely, D. G., Shav, D., Shabtay, O., Avriel, A., Lewis, G. D., Rosenzweig, E. B., Kirtane, A. J., Kim, N. H., Mahmud, E., McLaughlain, V. V., Chetcuti, S., Leon, M. B., Ben-Yehuda, O., & Rubin, L. J. (2020). Intravascular Ultrasound Pulmonary Artery Denervation to Treat Pulmonary Arterial Hypertension (TROPHY1): Multicenter, Early Feasibility Study. JACC. Cardiovascular interventions, 13(8), 989–999. [CrossRef]
- Zhang, H., Zhang, J., Chen, M., Xie, D. J., Kan, J., Yu, W., Li, X. B., Xu, T., Gu, Y., Dong, J., Gu, H., Han, Y., & Chen, S. L. (2019). Pulmonary Artery Denervation Significantly Increases 6-Min Walk Distance for Patients With Combined Pre- and Post-Capillary Pulmonary Hypertension Associated With Left Heart Failure: The PADN-5 Study. JACC. Cardiovascular interventions, 12(3), 274–284. [CrossRef]
- Romanov, A., Cherniavskiy, A., Novikova, N., Edemskiy, A., Ponomarev, D., Shabanov, V., Losik, D., Elesin, D., Stenin, I., Mikheenko, I., Zhizhov, R., Kretov, E., Pokushalov, E., Po, S. S., Martynyuk, T. V., & Steinberg, J. S. (2020). Pulmonary Artery Denervation for Patients With Residual Pulmonary Hypertension After Pulmonary Endarterectomy. Journal of the American College of Cardiology, 76(8), 916–926. [CrossRef]
- Yoshida, K., Saku, K., Kamada, K., Abe, K., Tanaka-Ishikawa, M., Tohyama, T., Nishikawa, T., Kishi, T., Sunagawa, K., & Tsutsui, H. (2018). Electrical Vagal Nerve Stimulation Ameliorates Pulmonary Vascular Remodeling and Improves Survival in Rats With Severe Pulmonary Arterial Hypertension. JACC. Basic to translational science, 3(5), 657–671. [CrossRef]
- Yoshida, K., Saku, K., Jan Bogaard, H., Abe, K., Sunagawa, K., & Tsutsui, H. (2022). Vagal nerve stimulation preserves right ventricular function in a rat model of right ventricular pressure overload. Pulmonary circulation, 12(4), e12154. [CrossRef]
- Pan, P., Zhang, X., Qian, H., Shi, W., Wang, J., Bo, Y., & Li, W. (2010). Effects of electro-acupuncture on endothelium-derived endothelin-1 and endothelial nitric oxide synthase of rats with hypoxia-induced pulmonary hypertension. Experimental biology and medicine (Maywood, N.J.), 235(5), 642–648. [CrossRef]
- Xin, J. J., Gao, J. H., Liu, Q., Zhao, Y. X., Zhou, C., & Yu, X. C. (2022). Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 42(6), 647–653. [CrossRef]
- Shi, Y. R., Yi, W., Qiao, Y., Zhuo, S. Y., Zhang, Q., Yang, X. J., Liang, T., & Ling, X. (2023). Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 43(8), 937–943. [CrossRef]
- Qiao, Y., Liang, Y., Zhuo, S., Yang, X., Liang, T., Ling, X., Zhang, Q., Shi, Y., & Yi, W. (2024). Effect and mechanism of acupuncture on airway smooth muscle relaxation during acute asthma attack in rats. 针刺松弛哮喘急性发作大鼠气道平滑肌的作用机制. Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 44(3), 295–302. [CrossRef]
- Lin, M., Wang, X., Ye, B., Zhang, J., Lin, S., Xu, Y., Zhou, J., Liu, S., Zhou, S., Guan, X., Jin, Y., & Wang, L. (2023). External counterpulsation stimulation combined with acupuncture for vascular endothelial function in patients with hypertension: A randomized pilot trial. Clinical and experimental hypertension (New York, N.Y. : 1993), 45(1), 2181355. [CrossRef]
- Jiang X. (2003). Effects of magnetic needle acupuncture on blood pressure and plasma ET-1 level in the patient of hypertension. Journal of traditional Chinese medicine = Chung i tsa chih ying wen pan, 23(4), 290–291.
- Maekura, T., Miki, K., Miki, M., Kitada, S., & Maekura, R. (2019). Clinical Effects Of Acupuncture On The Pathophysiological Mechanism Of Chronic Obstructive Pulmonary Disease During Exercise. International journal of chronic obstructive pulmonary disease, 14, 2787–2798. [CrossRef]
- Gao, J.i, Ouyang, B. S., Sun, G., Fan, C., Wu, Y. J., & Ji, L. L. (2011). Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 31(10), 893–897.
- Ge, Y., Yao, H., Tong, J., He, Y., Li, G., & Kong, X. (2017). Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 37(4), 366–371. [CrossRef]
- Feng, J., Wang, X., Li, X., Zhao, D., & Xu, J. (2016). Acupuncture for chronic obstructive pulmonary disease (COPD): A multicenter, randomized, sham-controlled trial. Medicine, 95(40), e4879. [CrossRef]
- Tong, J., Guo, Y. M., He, Y., Li, G. Y., Chen, F., & Yao, H. (2014). Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 34(9), 846–850.
- Suzuki, M., Muro, S., Ando, Y., Omori, T., Shiota, T., Endo, K., Sato, S., Aihara, K., Matsumoto, M., Suzuki, S., Itotani, R., Ishitoko, M., Hara, Y., Takemura, M., Ueda, T., Kagioka, H., Hirabayashi, M., Fukui, M., & Mishima, M. (2012). A randomized, placebo-controlled trial of acupuncture in patients with chronic obstructive pulmonary disease (COPD): the COPD-acupuncture trial (CAT). Archives of internal medicine, 172(11), 878–886. [CrossRef]
- Suzuki, M., Namura, K., Ohno, Y., Tanaka, H., Egawa, M., Yokoyama, Y., Akao, S., Fujiwara, H., & Yano, T. (2008). The effect of acupuncture in the treatment of chronic obstructive pulmonary disease. Journal of alternative and complementary medicine (New York, N.Y.), 14(9), 1097–1105. [CrossRef]
- Zhou, C., Wu, M. Z., Liu, Q., Xin, J. J., Wu, S., Zhao, Y. X., Zhang, W. X., Yu, X. C., & Gao, J. H. (2022). Synergistic and Attenuating Effect of Electroacupuncture on Aconitine in Improving Heart Failure and Its Calcium Regulation Mechanism. Evidence-based complementary and alternative medicine : eCAM, 2022, 4940745. [CrossRef]
- Wu, Z., Xia, Y., Wang, C., Lu, W., Zuo, H., Wu, D., Li, Y., Guo, R., Lu, J., & Zhang, L. (2023). Electroacupuncture at Neiguan (PC6) attenuates cardiac dysfunction caused by cecal ligation and puncture via the vagus nerve. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie, 162, 114600. [CrossRef]
- Ma, L., Cui, B., Shao, Y., Ni, B., Zhang, W., Luo, Y., & Zhang, S. (2014). Electroacupuncture improves cardiac function and remodeling by inhibition of sympathoexcitation in chronic heart failure rats. American journal of physiology. Heart and circulatory physiology, 306(10), H1464–H1471. [CrossRef]
- Lee, H., Kim, T. H., & Leem, J. (2016). Acupuncture for heart failure: A systematic review of clinical studies. International journal of cardiology, 222, 321–331. [CrossRef]
- Pullamsetti, S. S., Mamazhakypov, A., Weissmann, N., Seeger, W., & Savai, R. (2020). Hypoxia-inducible factor signaling in pulmonary hypertension. The Journal of clinical investigation, 130(11), 5638–5651. [CrossRef]
- Hewes J.L., Lee J.Y., Fagan K.A., Bauer N.N. (2020). The changing face of pulmonary hypertension diagnosis: a historical perspective on the influence of diagnostics and biomarkers. Pulmonary Circulation 10:2045894019892801.
- Szidon, J. P., & Flint, J. F. (1977). Significance of sympathetic innervation of pulmonary vessels in response to acute hypoxia. Journal of applied physiology: respiratory, environmental and exercise physiology, 43(1), 65–71. [CrossRef]
- Kummer W. (2011). Pulmonary vascular innervation and its role in responses to hypoxia: size matters!. Proceedings of the American Thoracic Society, 8(6), 471–476. [CrossRef]
- Iturriaga, R., & Castillo-Galán, S. (2019). Potential Contribution of Carotid Body-Induced Sympathetic and Renin-Angiotensin System Overflow to Pulmonary Hypertension in Intermittent Hypoxia. Current hypertension reports, 21(11), 89. [CrossRef]
- Del Rio, R., Andrade, D. C., Lucero, C., Arias, P., & Iturriaga, R. (2016). Carotid Body Ablation Abrogates Hypertension and Autonomic Alterations Induced by Intermittent Hypoxia in Rats. Hypertension (Dallas, Tex. : 1979), 68(2), 436–445. [CrossRef]
- Iturriaga R. (2018). Carotid Body Ablation: a New Target to Address Central Autonomic Dysfunction. Current hypertension reports, 20(6), 53. [CrossRef]
- Marina, N., Tang, F., Figueiredo, M., Mastitskaya, S., Kasimov, V., Mohamed-Ali, V., Roloff, E., Teschemacher, A. G., Gourine, A. V., & Kasparov, S. (2013). Purinergic signalling in the rostral ventro-lateral medulla controls sympathetic drive and contributes to the progression of heart failure following myocardial infarction in rats. Basic research in cardiology, 108(1), 317. [CrossRef]
- Costa-Silva, J. H., Zoccal, D. B., & Machado, B. H. (2012). Chronic intermittent hypoxia alters glutamatergic control of sympathetic and respiratory activities in the commissural NTS of rats. American journal of physiology. Regulatory, integrative and comparative physiology, 302(6), R785–R793. [CrossRef]
- Sharpe, A. L., Calderon, A. S., Andrade, M. A., Cunningham, J. T., Mifflin, S. W., & Toney, G. M. (2013). Chronic intermittent hypoxia increases sympathetic control of blood pressure: role of neuronal activity in the hypothalamic paraventricular nucleus. American journal of physiology. Heart and circulatory physiology, 305(12), H1772–H1780. [CrossRef]
- Chao, D. M., Shen, L. L., Tjen-A-Looi, S., Pitsillides, K. F., Li, P., & Longhurst, J. C. (1999). Naloxone reverses inhibitory effect of electroacupuncture on sympathetic cardiovascular reflex responses. The American journal of physiology, 276(6), H2127–H2134. [CrossRef]
- Li, P., Pitsillides, K. F., Rendig, S. V., Pan, H. L., & Longhurst, J. C. (1998). Reversal of reflex-induced myocardial ischemia by median nerve stimulation: a feline model of electroacupuncture. Circulation, 97(12), 1186–1194. [CrossRef]
- Li, P., Tjen-A-Looi, S. C., & Longhurst, J. C. (2006). Excitatory projections from arcuate nucleus to ventrolateral periaqueductal gray in electroacupuncture inhibition of cardiovascular reflexes. American journal of physiology. Heart and circulatory physiology, 290(6), H2535–H2542. [CrossRef]
- Li, P., Tjen-A-Looi, S., & Longhurst, J. C. (2001). Rostral ventrolateral medullary opioid receptor subtypes in the inhibitory effect of electroacupuncture on reflex autonomic response in cats. Autonomic neuroscience : basic & clinical, 89(1-2), 38–47. [CrossRef]
- Tjen-A-Looi, S. C., Fu, L. W., Zhou, W., Syuu, Z., & Longhurst, J. C. (2005). Role of unmyelinated fibers in electroacupuncture cardiovascular responses. Autonomic neuroscience : basic & clinical, 118(1-2), 43–50. [CrossRef]
- Tjen-A-Looi, S. C., Li, P., & Longhurst, J. C. (2003). Prolonged inhibition of rostral ventral lateral medullary premotor sympathetic neurons by electroacupuncture in cats. Autonomic neuroscience : basic & clinical, 106(2), 119–131. [CrossRef]
- Guo, Z. L., & Longhurst, J. C. (2010). Activation of reciprocal pathways between arcuate nucleus and ventrolateral periaqueductal gray during electroacupuncture: involvement of VGLUT3. Brain research, 1360, 77–88. [CrossRef]
- Kakall, Z. M., Pilowsky, P. M., & Farnham, M. M. J. (2018). PACAP-(6-38) or kynurenate microinjections in the RVLM prevent the development of sympathetic long-term facilitation after acute intermittent hypoxia. American journal of physiology. Heart and circulatory physiology, 314(3), H563–H572. [CrossRef]
- Farnham, M. M. J., Tallapragada, V. J., O'Connor, E. T., Nedoboy, P. E., Dempsey, B., Mohammed, S., Fong, A. Y., Lung, M. S. Y., Derakhshan, F., Wilson, R. J. A., & Pilowsky, P. M. (2019). PACAP-PAC1 Receptor Activation Is Necessary for the Sympathetic Response to Acute Intermittent Hypoxia. Frontiers in neuroscience, 13, 881. [CrossRef]
- Zhou, W., Fu, L. W., Tjen-A-Looi, S. C., Guo, Z. L., & Longhurst, J. C. (2006). Role of glutamate in a visceral sympathoexcitatory reflex in rostral ventrolateral medulla of cats. American journal of physiology. Heart and circulatory physiology, 291(3), H1309–H1318. [CrossRef]
- Silva, A. Q., & Schreihofer, A. M. (2011). Altered sympathetic reflexes and vascular reactivity in rats after exposure to chronic intermittent hypoxia. The Journal of physiology, 589(Pt 6), 1463–1476. [CrossRef]
- Zhou, W., Fu, L. W., Guo, Z. L., & Longhurst, J. C. (2007). Role of glutamate in the rostral ventrolateral medulla in acupuncture-related modulation of visceral reflex sympathoexcitation. American journal of physiology. Heart and circulatory physiology, 292(4), H1868–H1875. [CrossRef]
- Tjen-A-Looi, S. C., Li, P., & Longhurst, J. C. (2009). Processing cardiovascular information in the vlPAG during electroacupuncture in rats: roles of endocannabinoids and GABA. Journal of applied physiology (Bethesda, Md. : 1985), 106(6), 1793–1799. [CrossRef]
- Fu, L. W., & Longhurst, J. C. (2009). Electroacupuncture modulates vlPAG release of GABA through presynaptic cannabinoid CB1 receptors. Journal of applied physiology (Bethesda, Md. : 1985), 106(6), 1800–1809. [CrossRef]
- Li, P., Tjen-A-Looi, S. C., Guo, Z. L., Fu, L. W., & Longhurst, J. C. (2009). Long-loop pathways in cardiovascular electroacupuncture responses. Journal of applied physiology (Bethesda, Md. : 1985), 106(2), 620–630. [CrossRef]
- Oliveira, A. C., Karas, M. M., Alves, M., He, J., de Kloet, A. D., Krause, E. G., Richards, E. M., Bryant, A. J., & Raizada, M. K. (2023). ACE2 overexpression in corticotropin-releasing-hormone cells offers protection against pulmonary hypertension. Frontiers in neuroscience, 17, 1223733. [CrossRef]
- Goncharuk, V. D., Van Heerikhuize, J., Swaab, D. F., & Buijs, R. M. (2002). Paraventricular nucleus of the human hypothalamus in primary hypertension: activation of corticotropin-releasing hormone neurons. The Journal of comparative neurology, 443(4), 321–331. [CrossRef]
- Dampney, R. A., Michelini, L. C., Li, D. P., & Pan, H. L. (2018). Regulation of sympathetic vasomotor activity by the hypothalamic paraventricular nucleus in normotensive and hypertensive states. American journal of physiology. Heart and circulatory physiology, 315(5), H1200–H1214. [CrossRef]
- Li, D. P., Zhou, J. J., Zhang, J., & Pan, H. L. (2017). CaMKII Regulates Synaptic NMDA Receptor Activity of Hypothalamic Presympathetic Neurons and Sympathetic Outflow in Hypertension. The Journal of neuroscience : the official journal of the Society for Neuroscience, 37(44), 10690–10699. [CrossRef]
- Ruyle, B. C., Martinez, D., Heesch, C. M., Kline, D. D., & Hasser, E. M. (2019). The PVN enhances cardiorespiratory responses to acute hypoxia via input to the nTS. American journal of physiology. Regulatory, integrative and comparative physiology, 317(6), R818–R833. [CrossRef]
- King, T. L., Heesch, C. M., Clark, C. G., Kline, D. D., & Hasser, E. M. (2012). Hypoxia activates nucleus tractus solitarii neurons projecting to the paraventricular nucleus of the hypothalamus. American journal of physiology. Regulatory, integrative and comparative physiology, 302(10), R1219–R1232. [CrossRef]
- Silva, T. M., Takakura, A. C., & Moreira, T. S. (2016). Acute hypoxia activates hypothalamic paraventricular nucleus-projecting catecholaminergic neurons in the C1 region. Experimental neurology, 285(Pt A), 1–11. [CrossRef]
- Wang, L. A., Nguyen, D. H., & Mifflin, S. W. (2019). Corticotropin-releasing hormone projections from the paraventricular nucleus of the hypothalamus to the nucleus of the solitary tract increase blood pressure. Journal of neurophysiology, 121(2), 602–608. [CrossRef]
- Wang, L. A., Nguyen, D. H., & Mifflin, S. W. (2018). CRHR2 (Corticotropin-Releasing Hormone Receptor 2) in the Nucleus of the Solitary Tract Contributes to Intermittent Hypoxia-Induced Hypertension. Hypertension (Dallas, Tex. : 1979), 72(4), 994–1001. [CrossRef]
- Zhu, L., Ye, Z., Zhang, M., Xu, W., Wang, R., Wu, S., & Gao, H. (2023). Electroacupuncture intervention on stress-induced cardiac autonomic imbalance in rats involves corticotropin-releasing hormone system activity. Neuroreport, 34(7), 401–410. [CrossRef]
- Ye, Z., Zhu, L., Li, X. J., Gao, H. Y., Wang, J., Wu, S. B., Wu, Z. J., & Gao, H. R. (2023). PC6 electroacupuncture reduces stress-induced autonomic and neuroendocrine responses in rats. Heliyon, 9(4), e15291. [CrossRef]
- Zhang, M., Sun, J., Wang, Y., & Tian, Z. (2021). Secretagogin Mediates the Regulatory Effect of Electroacupuncture on Hypothalamic-Pituitary-Adrenal Axis Dysfunction in Surgical Trauma. Neural plasticity, 2021, 8881136. [CrossRef]
- Zhou, Q. Z., Peng, X. H., Wu, Q. F., Yu, S. G., Wei, J. L., Xu, H. Y., Wang, W., & Yin, H. Y. (2008). Zhen ci yan jiu = Acupuncture research, 33(6), 372–376.
- Huang, J., Tamisier, R., Ji, E., Tong, J., & Weiss, W. J. (2007). Chronic intermittent hypoxia modulates nNOS mRNA and protein expression in the rat hypothalamus. Respiratory physiology & neurobiology, 158(1), 30–38. [CrossRef]
- Ogoshi, T., Tsutsui, M., Kido, T., Sakanashi, M., Naito, K., Oda, K., Ishimoto, H., Yamada, S., Wang, K. Y., Toyohira, Y., Izumi, H., Masuzaki, H., Shimokawa, H., Yanagihara, N., Yatera, K., & Mukae, H. (2018). Protective Role of Myelocytic Nitric Oxide Synthases against Hypoxic Pulmonary Hypertension in Mice. American journal of respiratory and critical care medicine, 198(2), 232–244. [CrossRef]
- Kim, J. I., Kim, Y. S., Kang, S. K., Kim, C., Park, C., Lee, M. S., & Huh, Y. (2008). Electroacupuncture decreases nitric oxide synthesis in the hypothalamus of spontaneously hypertensive rats. Neuroscience letters, 446(2-3), 78–82. [CrossRef]
- Maeda, M., Kachi, H., Ichihashi, N., Oyama, Z., & Kitajima, Y. (1998). The effect of electrical acupuncture-stimulation therapy using thermography and plasma endothelin (ET-1) levels in patients with progressive systemic sclerosis (PSS). Journal of dermatological science, 17(2), 151–155. [CrossRef]
- Lim, H. D., Kim, M. H., Lee, C. Y., & Namgung, U. (2016). Anti-Inflammatory Effects of Acupuncture Stimulation via the Vagus Nerve. PloS one, 11(3), e0151882. [CrossRef]
- Liu, S., Wang, Z., Su, Y., Qi, L., Yang, W., Fu, M., Jing, X., Wang, Y., & Ma, Q. (2021). A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis. Nature, 598(7882), 641–645. [CrossRef]
- Liu, S., Wang, Z. F., Su, Y. S., Ray, R. S., Jing, X. H., Wang, Y. Q., & Ma, Q. (2020). Somatotopic Organization and Intensity Dependence in Driving Distinct NPY-Expressing Sympathetic Pathways by Electroacupuncture. Neuron, 108(3), 436–450.e7. [CrossRef]
- Torres-Rosas, R., Yehia, G., Peña, G., Mishra, P., del Rocio Thompson-Bonilla, M., Moreno-Eutimio, M. A., Arriaga-Pizano, L. A., Isibasi, A., & Ulloa, L. (2014). Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nature medicine, 20(3), 291–295. [CrossRef]
- Zhao, Y. X., He, W., Jing, X. H., Liu, J. L., Rong, P. J., Ben, H., Liu, K., & Zhu, B. (2012). Transcutaneous auricular vagus nerve stimulation protects endotoxemic rat from lipopolysaccharide-induced inflammation. Evidence-based complementary and alternative medicine : eCAM, 2012, 627023. [CrossRef]
- Zhang, L., Wu, Z., Zhou, J., Lu, S., Wang, C., Xia, Y., Ren, H., Tong, Z., Ke, L., & Li, W. (2021). Electroacupuncture Ameliorates Acute Pancreatitis: A Role for the Vagus Nerve-Mediated Cholinergic Anti-Inflammatory Pathway. Frontiers in molecular biosciences, 8, 647647. [CrossRef]
- Abe, C., Inoue, T., Inglis, M. A., Viar, K. E., Huang, L., Ye, H., Rosin, D. L., Stornetta, R. L., Okusa, M. D., & Guyenet, P. G. (2017). C1 neurons mediate a stress-induced anti-inflammatory reflex in mice. Nature neuroscience, 20(5), 700–707. [CrossRef]
- Kim, S. K., Kim, J., Woo, H. S., Jeong, H., Lee, H., Min, B. I., Nam, S., & Bae, H. (2010). Electroacupuncture induces Fos expression in the nucleus tractus solitarius via cholecystokinin A receptor signaling in rats. Neurological research, 32 Suppl 1, 116–119. [CrossRef]
- Kim, M. H., Park, Y. C., & Namgung, U. (2012). Acupuncture-stimulated activation of sensory neurons. Journal of acupuncture and meridian studies, 5(4), 148–155. [CrossRef]
- Ju, S., Liu, M., Wang, B., Yu, D., Zhang, H., Zhang, M., & Li, J. (2023). Transcutaneous electrical acupoint stimulation improves pulmonary function by regulating oxidative stress during one-lung ventilation in patients with lung cancer undergoing thoracoscopic surgery: a randomized controlled trial. BMC complementary medicine and therapies, 23(1), 463. [CrossRef]
- Ma, W., Li, Z., Lu, Z., Tan, W., Zhang, Z., Li, Y., Yang, Z., Zhou, J., Tang, H., & Cui, H. (2017). Protective Effects of Acupuncture in Cardiopulmonary Bypass-Induced Lung Injury in Rats. Inflammation, 40(4), 1275–1284. [CrossRef]
- Tang, W., Dong, M., Teng, F., Cui, J., Zhu, X., Wang, W., Wuniqiemu, T., Qin, J., Yi, L., Wang, S., Dong, J., & Wei, Y. (2021). TMT-based quantitative proteomics reveals suppression of SLC3A2 and ATP1A3 expression contributes to the inhibitory role of acupuncture on airway inflammation in an OVA-induced mouse asthma model. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie, 134, 111001. [CrossRef]
- Zhang, L., Tian, Y., Zhao, P., Jin, F., Miao, Y., Liu, Y., & Li, J. (2022). Electroacupuncture attenuates pulmonary vascular remodeling in a rat model of chronic obstructive pulmonary disease via the VEGF/PI3K/Akt pathway. Acupuncture in medicine : journal of the British Medical Acupuncture Society, 40(4), 389–400. [CrossRef]
- Li, X., Wang, L., Ying, X., Zheng, Y., Tan, Q., Yu, X., Gong, J., Li, M., Deng, X., Yang, G., Li, S., & Jiang, S. (2022). Electroacupuncture pre-treatment alleviates sepsis-induced cardiac inflammation and dysfunction by inhibiting the calpain-2/STAT3 pathway. Frontiers in physiology, 13, 961909. [CrossRef]
- Gong, L. R., Kan, Y. X., Lian, Y., Dong, S. A., Zhao, D. H., Shi, J., & Yu, J. B. (2020). Electroacupuncture Attenuates Limb Ischemia-Reperfusion-Induced Lung Injury Via p38 Mitogen-Activated Protein Kinase-Nuclear Factor Erythroid-2-Related Factor-2/Heme Oxygenase Pathway. The Journal of surgical research, 246, 170–181. [CrossRef]
- Luo, J., Yan, R., Ding, L., Ning, J., Chen, M., Guo, Y., Liu, J., Chen, Z., & Zhou, R. (2024). Electroacupuncture Attenuates Ventilator-Induced Lung Injury by Modulating the Nrf2/HO-1 Pathway. The Journal of surgical research, 295, 811–819. [CrossRef]
- Chen, T., Xiong, Y., Long, M., Zheng, D., Ke, H., Xie, J., Yin, N., & Chen, Z. (2019). Electro-acupuncture Pretreatment at Zusanli (ST36) Acupoint Attenuates Lipopolysaccharide-Induced Inflammation in Rats by Inhibiting Ca2+ Influx Associated with Cannabinoid CB2 Receptors. Inflammation, 42(1), 211–220. [CrossRef]
- Li, Y., Zhang, H., Yang, J., Zhan, M., Hu, X., Liu, Y., Yu, L., Yan, X., Liang, S., Zhang, R., Lu, Y., Li, B., Liu, C., & Li, M. (2021). P2Y12 receptor as a new target for electroacupuncture relieving comorbidity of visceral pain and depression of inflammatory bowel disease. Chinese medicine, 16(1), 139. [CrossRef]
- Jung, Y. S., Lee, S. W., Park, J. H., Seo, H. B., Choi, B. T., & Shin, H. K. (2016). Electroacupuncture preconditioning reduces ROS generation with NOX4 down-regulation and ameliorates blood-brain barrier disruption after ischemic stroke. Journal of biomedical science, 23, 32. [CrossRef]
- Lu, J., Xie, J. J., Xiang, S. Y., Li, Y., Cong, W. J., Lin, X. G., & Liu, Z. B. (2018). Zhen ci yan jiu = Acupuncture research, 43(12), 759–766. [CrossRef]
- Zhang, X. F., Zhu, J., Geng, W. Y., Zhao, S. J., Jiang, C. W., Cai, S. R., Cheng, M., Zhou, C. Y., & Liu, Z. B. (2014). Electroacupuncture at Feishu (BL13) and Zusanli (ST36) down-regulates the expression of orexins and their receptors in rats with chronic obstructive pulmonary disease. Journal of integrative medicine, 12(5), 417–424. [CrossRef]
- Tjen-A-Looi, S., Ekman, R., Lippton, H., Cary, J., & Keith, I. (1992). CGRP and somatostatin modulate chronic hypoxic pulmonary hypertension. The American journal of physiology, 263(3 Pt 2), H681–H690. [CrossRef]
- Tjen-A-Looi, S., Kraiczi, H., Ekman, R., & Keith, I. M. (1998). Sensory CGRP depletion by capsaicin exacerbates hypoxia-induced pulmonary hypertension in rats. Regulatory peptides, 74(1), 1–10. [CrossRef]
- Champion, H. C., Bivalacqua, T. J., Toyoda, K., Heistad, D. D., Hyman, A. L., & Kadowitz, P. J. (2000). In vivo gene transfer of prepro-calcitonin gene-related peptide to the lung attenuates chronic hypoxia-induced pulmonary hypertension in the mouse. Circulation, 101(8), 923–930. [CrossRef]
- Li, W. J., Li, S. M., Ding, Y., He, B., Keegan, J., Dong, H., Ruan, J. W., & Zeng, Y. S. (2012). Electro-acupuncture upregulates CGRP expression after rat spinal cord transection. Neurochemistry international, 61(8), 1397–1403. [CrossRef]
- Kawakita, K., Itoh, K., & Okada, K. (2008). Experimental model of trigger points using eccentric exercise. Journal of Musculoskeletal Pain, 16(1-2), 29-35.
- Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Irnich, D., Witt, C. M., Linde, K., & Acupuncture Trialists' Collaboration (2018). Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis. The journal of pain, 19(5), 455–474. [CrossRef]
- Yuan, C. X., Wang, X., Yu, Z., Lian, X. Y., & Xu, B. (2024). Electroacupuncture improves peripheral neuropathy by up-regulating Sirt1/PGC-1α/TFAM pathway in type 2 diabetes rats with peripheral neuropathy. 基于Sirt1/PGC-1α/TFAM通路探讨电针治疗2型糖尿病周围神经病变的机制. Zhen ci yan jiu = Acupuncture research, 49(4), 349–357. [CrossRef]
- Hoerder, S., Habermann, I. V., Hahn, K., Meyer-Hamme, G., Ortiz, M., Grabowska, W., Roll, S., Willich, S. N., Schroeder, S., Brinkhaus, B., & Dietzel, J. (2023). Acupuncture in diabetic peripheral neuropathy-neurological outcomes of the randomized acupuncture in diabetic peripheral neuropathy trial. World journal of diabetes, 14(12), 1813–1823. [CrossRef]
- Yang, N. N., Lin, L. L., Li, Y. J., Li, H. P., Cao, Y., Tan, C. X., Hao, X. W., Ma, S. M., Wang, L., & Liu, C. Z. (2022). Potential Mechanisms and Clinical Effectiveness of Acupuncture in Depression. Current neuropharmacology, 20(4), 738–750. [CrossRef]
- Chen, S., Li, J., Yan, L., Zhang, X., Huang, J., & Zhou, P. (2024). Electroacupuncture alleviates the symptom of depression in mice by regulating the cGAS-STING-NLRP3 signaling. Aging, 16(8), 6731–6744. [CrossRef]
Table 1.
Etiological and Clinical Classification of Pulmonary Hypertension (PH).
Group 1: Pulmonary Arterial Hypertension (PAH)
|
| HIV = human immunodeficiency virus; PCH = pulmonary capillary hemangiomatosis; PVOD = pulmonary veno-occlusive disease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



