
Submitted:
20 May 2024
Posted:
20 May 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Patients with chronic kidney disease (CKD), particularly those with end-stage kidney disease (ESKD) undergoing dialysis or kidney transplantation, face ongoing challenges in relation to the risk of COVID-19. In addition to their underlying condition, factors such as immune-evasive variants, immunosuppressive therapies, and the need for dialysis contribute to poor COVID-19 outcomes in this population. Severe COVID-19 can lead to the deterioration of CKD/ESKD, resulting in acute kidney injury, septic shock, and respiratory failure. Moreover, patients with CKD/ESKD have shown impaired response to COVID-19 vaccination, with seroconversion failures associated with the burden of immunosuppressive treatments, further heightening their vulnerability to severe disease. Despite the current endemic, it is crucial to acknowledge the ongoing significance of COVID-19 as a serious threat to patients burdened with chronic diseases like CKD and ESRD. Understanding the impact of COVID-19 on these patients is essential, as they remain at risk of severe disease progression. This paper presents the results of a literature review to enhance our understanding of COVID-19-related risks in patients with CKD/ESKD. Expert insights and illustrative scenarios provide practical perspectives and highlight the importance of risk stratification based on clinical factors for guiding targeted measures and treatments to mitigate COVID-19 risks in these vulnerable patients.
Keywords:
COVID-19
; Omicron
; chronic kidney disease (CKD)
; end-stage kidney disease (ESKD)
; dialysis
; kidney transplantation
; immunocompromised
; immunosuppressed
Introduction
The SARS-CoV-2 pandemic has had a disproportionate impact on immunocompromised (IC) individuals, specifically those with CKD [1]. Compared to healthy individuals, patients with CKD had an elevated risk of severe COVID-19 outcomes including prolonged hospitalizations, intensive care unit (ICU) admissions, and deaths [1]. Despite the decreased severity of the Omicron variant in the general population, [2] patients with CKD continue to face high mortality rates, particularly those with low vaccine responses and inadequate preventive measures [3]. Therefore, it is crucial to recognize the persistent threat of COVID-19 in these patients, address their unique challenges, and implement necessary strategies to mitigate COVID-19 risks for this vulnerable population.
Previous evidence has established the link between CKD and increased mortality from COVID-19 [4,5]. This increased risk was attributed to factors such as high exposure setting of in-center hemodialysis and the emergence of SARS-CoV-2 variants capable of evading vaccines and the immune system (e.g. Omicron BA.2.75, BQ.1, XBB, and XBBP.1.5) [6,7,8,9]. Primary risk factors for COVID-19-related deaths included organ transplant, estimated glomerular filtration rate (eGFR) <30 ml/min/1.73m2 and immunosuppression [5]. Patients with CKD or ESKD experienced more complications, deaths and severe morbidities than those without CKD or ESKD [5,10,11,12]. In large population studies, patients receiving dialysis had a 20%–30% mortality rate, four times higher than that of non-dialysis patients [4,5,7,13]. Moreover, kidney transplant recipients (KTRs) with chronic immunosuppression have been shown to exhibit reduced vaccine responses and viral clearance capacity, [14] further underscoring the need for a multi-pronged vaccination strategy and early preventive measures or treatment.
This review aims to enhance understanding of the risks and disease management related to COVID-19 in patients with CKD, including those receiving dialysis and with kidney transplantation. Through a comprehensive analysis of the available literature, our objective is to identify individuals who are particularly vulnerable to severe COVID-19 outcomes and require specialized attention, taking into consideration their specific treatment modalities and transplantation status. Evidence on COVID-19 vaccine responses in these patient populations is also examined and discussed. To provide practical insights into real-life management challenges, we present two illustrative cases and provide considerations for minimizing COVID-19 risks and adverse outcomes. By contextualizing our findings in the ongoing endemic phase, this review underscores the continued magnitude and burden of COVID-19 on patients with CKD and emphasizes the need for stratifying patients based on their individual risk profiles.
Understanding the Effects of Covid-19 on CKD, Dialysis and Kidney Transplantation
COVID-19 Mortality in ESKD, Dialysis and Kidney Transplantation
Studies have shown that when infected with SARS-CoV-2, individuals with pre-existing ESKD and maintenance dialysis had a faster progression to ICU admission than those without [15]. Within 28 days of ICU admission, half of the patients with CKD (both dialysis-dependent and non-dependent) had died, compared to 35% without pre-existing CKD, emphasizing the need for targeted COVID-19 treatments in this high-risk group [15]. Furthermore, COVID-19 patients with ESKD on dialysis who did not survive were found to have significantly higher median initial white blood cell counts and C-reactive protein levels [16]. Several studies have reported higher COVID-19 rates and mortality in individuals on dialysis [4,17]. Interestingly, home dialysis showed a 23% reduction in COVID-19 risk but an 18% increase in mortality [18]. An Italian study reported stopping immunosuppressants in KTRs with on-admission COVID-19 infection and starting methylprednisolone, antiviral therapy and hydroxychloroquine.[19] However, by day seven, 87% of patients worsened, 73% needed oxygenation, and six developed AKI. By day 15, five KTRs had died, highlighting of the risk of disease progression and death in this population. In another study of hospitalized COVID-19 patients on dialysis, 31% had died within a median of six days post-admission while 75% needed mechanical ventilation [20]. Altogether, these findings underscore the need to prevent the spread of SARS-CoV-2 in this high-risk group.
Impact of CKD on COVID-19 Risks and Outcomes
Compared to the general population, individuals with CKD face a 14 to 16-fold higher risk of COVID-19-related pneumonia, severity and associated mortality, leading to a proportional increase in adverse outcomes including hospitalization, respiratory failure and death [21]. Additionally, kidney dysfunction has been identified as an independent predictor of poor COVID-19 outcomes [22]. A Japanese study found that on-admission kidney dysfunction (defined as eGFR <60 mL/min/1.73 m2 or dipstick proteinuria ≥1+) was associated with disease severity and poor short-term prognosis among patients with COVID-19 [22], suggesting that the severity of CKD can serve as a stratification factor for assessing the risks associated with COVID-19. In line with our expert recommendation, COVID-19 patients with on-admission kidney dysfunction require careful clinical attention, including considerations such as withholding nephrotoxic treatments and implementing hemodynamic interventions. Assessing kidney function and markers of kidney damage in COVID-19 patients aids in identifying individuals in urgent need of early interventions to mitigate disease progression. Specifically, proteinuria, observed in 24% to 84% of CKD patients with COVID-19,[20] may indicate underlying kidney pathology or comorbidities and has been shown to predict mortality regardless of acute kidney injury independently (AKI) or hematuria [23].
Kidney Complications in CKD and COVID-19 Outcomes
Data indicated that COVID-19 patients with underlying CKD were 66% more likely to develop AKI, which increases mortality risks, and had a greater than threefold higher risk of requiring acute kidney replacement therapy (KRT) [24]. Transplant recipients also face a higher prevalence of AKI compared to other COVID-19 patients, with estimates ranging from 75% to 83% [24]. A US study found that solid organ transplant recipients hospitalized with COVID-19 were 3.5-times more likely to require dialysis than non-transplant patients [24]. Compared to individuals without CKD, mortality rates at 28 days post-ICU admission were higher in patients with CKD who did not require dialysis (51%) and those requiring KRT (50%) [25]. It remains unclear why kidney dysfunction independently increases the risk of death in patients with COVID-19. However, it has been suggested that severe kidney disease may complicate fluid therapy in patients with respiratory failure. Among patients with COVID-19, the most common causes of death were respiratory failure, kidney failure and septic shock [26].
COVID-19 Risks and Considerations for Dialysis Patients
During the pandemic, patients on dialysis have been identified as one of the highest-risk groups for mortality, not only due to their susceptibility to severe illness but also because of the potential for missed treatments [27]. A study demonstrated that patients on hemodialysis had an ICU mortality rate that was 14.4 times higher than the general population when infected with COVID-19 [28]. Moreover, patients on in-center hemodialysis face an additional risk of exposure as they need to attend dialysis centers, even during lockdowns, which can become hotspots for widespread infection [24]. These patients often rely on shared patient transportation and interact with other patients and dialysis staff, further increasing their exposure risk. As a result, the incidence of COVID-19 among patients receiving in-center hemodialysis is higher compared to the general population [24]. Alarmingly, studies have reported that approximately 20% of patients on dialysis died within 1 month of contracting SARS-CoV-2, a significantly higher mortality risk than that associated with other infections or many cardiovascular events [24]. However, while earlier studies have indicated high short-term mortality among dialysis patients with COVID-19, data on long-term outcomes provide more reassurance [29]. Survivors of COVID-19 in this high-risk group tend to have good outcomes at three months post-diagnosis [29]. Additionally, it is important to note that despite the perception that PD patients may be less vulnerable due to home-based treatment, recent Omicron data from Hong Kong reported similarly high COVID-19 mortality rates among PD and hemodialysis patients [30]. Notably, 73% of PD deaths occurred in unvaccinated patients. Altogether, these findings underscore the importance of providing unrestricted and optimal treatment for COVID-19 in dialysis patients.
COVID-19 and Arterial and Venous Thromboembolic Complications
COVID-19 can induce a prothrombotic state, increasing the risk of venous and arterial thromboembolic events [24]. It remains uncertain whether individuals with CKD are at greater risk of thromboembolic events after COVID-19 than those with normal kidney function. Existing findings have been mixed so far, partly due to inadequate baseline definition or documentation of CKD and lack of follow-up [24]. A large registry study on patients with COVID-19 reported a significant association between CKD and a greater than twofold increased risk of venous or arterial thromboembolic complications, as well as all-cause mortality within 90 days of discharge; however, the study did not provide a definition of CKD [24]. Poor outcomes in patients with CKD and COVID-19 may be due to SARS-CoV-2 interacting with the angiotensin-converting enzyme 2 transmembrane protein in kidney proximal tubular and podocyte cells [31]. Kidney injury can occur directly due to SARS-CoV-2 presence, infection and replication in renal tubular epithelium,[32] or indirectly due to hyperinflammation resulting from tubular injury and renal vasculitis. Additionally, the use of nephrotoxic dialysis drugs, nonsteroidal anti-inflammatory drugs, or volume depletion can worsen glomerular filtration.
Effectiveness of COVID-19 Vaccination in IC and is Patients
Compared to healthy individuals, IC individuals, exhibit higher non-responder rates [1]. A study evaluating the efficacy of SARS-CoV-2 vaccine against COVID-19-related hospitalization found an effectiveness of 62.9% in IC populations, which was lower than non-IC populations (91.3%) [33]. Post-vaccination humoral responses are influenced by factors such as the type of transplantation, immunosuppressive treatments, duration after transplantation, and diminished eGFR [34,35,36,37]. In both dialysis patients and KTRs, the number and type of immunosuppressive drugs are most critical risk factors for seroconversion failure [37]. Negative humoral responses were associated with triple-drug immunosuppression, whereas positive humoral responses were less likely with mycophenolate-based agents [38,39]. Moreover, comorbidities including diabetes mellitus has been identified as a risk factor for vaccine unresponsiveness in a kidney transplant cohort [35].
Based on our systematic review of the literature (Appendix A), there is a wide variation in vaccine response rates across the CKD populations. Overall, seroconversion rates in hemodialysis and peritoneal dialysis patients were comparable to those in non-IC individuals (Figure 1). Notably, hemodialysis patients showed improved seroconversion rates after the second vaccine dose, although still lower than observed in healthy individuals [40]. On the other hand, there is strong evidence that patients with solid organ transplant including KTRs exhibit higher non-response rates to COVID-19 vaccination [33].
Illustrative Cases
*The cases presented are for illustrative purposes only and do not represent specific individuals. They are hypothetical scenarios derived from the authors’ collective clinical experience.
To provide a comprehensive understanding of post-treatment outcomes, we describe two contrasting cases of individuals with ESKD undergoing dialysis and with indications for kidney transplantation. One of them contracted COVID-19, while the other remained unaffected by the virus. These cases were deliberately selected to highlight the challenges that may arise in clinical practice and to emphasize the variability in patient profiles and COVID-19 outcomes within this population.
Patient 1
Introduction: A 29-year-old female was diagnosed with IgM nephropathy at age 3 secondary to IgA nephropathy, with non-compliance in adolescent years resulting in progression to ESKD by age 21. At the age of 28 years, she underwent a kidney transplantation (November 2018) and received post-transplant immunosuppression, which included prednisone.
Case Report: She received one dose of mRNA vaccine in May 2020, and another in November 2020. Her first SARS-CoV-2 infection occurred in June 2021, presenting with moderate disease symptoms of high fever, chills, rigors, severe fatigue, nausea with vomiting, body aches, mild shortness of breath, sore throat, nasal congestion, and bilateral coarse crackles on lung examination. Nasopharyngeal swabs for reverse transcription polymerase chain reaction (RT-PCR) were positive for SARS-CoV-2, while chest X-rays showed ground glass opacities in bilateral lower fields, confirming both upper and lower respiratory tract infection. Vital signs showed elevated blood pressure, heart rate and respiratory rate. Blood work indicated abnormalities in white blood cell count, hemoglobin levels, platelet count, urea, and creatinine levels. Her glycated hemoglobin and tacrolimus levels were within normal ranges. She was admitted to the hospital for five days and received treatment for symptomatic COVID-19 in line with established protocols for IC patients admitted with moderate COVID-19: intravenous remdesivir daily for three days with symptomatic treatment (acetaminophen, nasal decongestants, cough suppressant, throat lozenges and throat antiseptic sprays). During hospitalization, reduced-dose azathioprine was given (25 mg every other day), with 25 mg daily resumed on discharge. She was hospitalized for seven days, and when her nasal swab RT-PCR reached a Ct value of >25 on day 14, she had a further seven days of a “virtual ward”, at-home program, with de-isolation. She received a third dose of mRNA vaccine (November 2021), and pre-exposure prophylaxis (PrEP) tixagevimab-cilgavimab (TIX-CIL) (April 2022) without adverse effects. Currently, she is on immunosuppressants with no rejection or other episode of COVID-19. At one month post-isolation, she displayed normal baseline laboratory values with no further sequelae.
Patient 2
Introduction: A 38-year-old female had IgA nephropathy that resulted in ESKD and required a kidney transplantation. She was on hemodialysis via an arteriovenous fistula for the previous five years and prescribed medications including antihypertensives, calcium-based phosphate binders, and vitamin supplements, but no immunosuppression. Due to her treatment adherence, laboratory assays demonstrate values within normal limits or target ranges and that her condition is stable, with the patient wait-listed for kidney transplantation from a deceased donor.
Case Report: During the pandemic, she received two doses of viral vector vaccine administered four months apart, and after five months, two doses of mRNA vaccine. She is currently in a state of good health, doing well with thrice-weekly hemodialysis, and is awaiting a kidney transplantation.
Protecting CKD Patients and KTRS from Covid-19 Infection and Severe Disease
Vaccination and Booster Doses for Effective COVID-19 Prevention
The cases underscore the importance of implementing effective vaccination strategies, timely booster doses, and prompt treatment to prevent the progression to severe disease, particularly given the ongoing high COVID-19 prevalence and deaths and declining population immunity. A recent Thai study has provided crucial evidence on the effectiveness of booster (third, fourth and fifth doses) in protecting against severe COVID-19 outcomes and deaths with newer Omicron sub-lineages [41]. The findings highlight the ongoing significance of timely booster vaccinations in protecting the population and provide urgently needed evidence to support the continued rollout of booster dose schedules in Thailand and other regions in Asia. To ensure optimal protection, booster campaigns should prioritize improving coverage by utilizing all available vaccines [41].
Non-Pharmacological Measures in COVID-19 Prevention
IC individuals, who often interact more frequently with healthcare systems, face an elevated risk of acquiring healthcare-associated infections, including COVID-19 and other respiratory illnesses [42]. To mitigate this risk and ensure these patients receive essential care, modifications to routine and preventive healthcare delivery are necessary. For those with suspected or confirmed COVID-19, key infection control measures include rigorous hand hygiene, universal use of personal protective equipment, targeted utilization of negative pressure rooms, vigilance regarding secondary infections, and a tailored approach to de-escalating isolation precautions [42]. While it is recognized that most IC patients were already practicing some degree of social distancing and hand hygiene before and during the pandemic, they should be routinely reminded to maintain preventive measures to protect themselves as societies and communities gradually reopen.
Therapeutic Strategies for COVID-19 Management
Therapeutic strategies for protecting patients with CKD and KTRs from COVID-19 involve maintaining updated vaccinations and providing PrEP or post-exposure prophylaxis with monoclonal antibodies and antiviral small molecules [43,44]. Early treatment in high-risk populations focus on halting SARS-CoV-2 replication and reducing viral loads (Figure 2). For KTRs, COVID-19 treatment is similar to non-transplant patients,[45] with adjustments to immunosuppression levels based on disease severity [46].
Monoclonal Antibodies for COVID-19 Prophylaxis
Considering the diminishing effectiveness of immunity and the emergence of immune-evading variants, booster vaccinations [46] or monoclonal antibodies PrEP can be beneficial for dialysis patients and individuals with persistent poor vaccine responses [41]. Several anti-SARS-CoV-2 monoclonal antibodies have proven to be safe and effective in reducing the severity and mortality of COVID-19 in IC individuals, and early initiation of treatment should be considered for non-hospitalized patients to reduce the risk of hospital visits [47,48,49]. Previous studies have shown that TIX-CIL PrEP reduced the risk of symptomatic illness by 82.8% at the six-month follow-up for unvaccinated adults at high risk of inadequate vaccine responses or SARS-CoV-2 exposure [50]. However, the impact of prophylactic TIX-CIL on mortality remains uncertain, as newer variants like BA.5 have shown resistance to neutralization [51,52,53]. Similarly, the effectiveness of the monoclonal antibody sotrovimab against Omicron variants is reduced compared to ancestral variants [54]. Due to the waning effectiveness of these agents and the risk of increased viral resistance in IC individuals,[55,56], it is advisable to reserve their use for patients who are at high risk of complications [57]. In Singapore, the implementation of TIX-CIL PrEP during the late 2022 Omicron wave in a hemodialysis patient cohort resulted in low rates of SARS-CoV-2 infections (7%;14/198 patients), hospitalizations (2%;4/200 patients), ICU admissions (1%; 2/200 patients), and no deaths or adverse events [58].
Monoclonal Antibodies for COVID-19 Treatment
Monoclonal antibodies such as bebtelovimab, sotrovimab, TIX-CIL, and casirivimab/imdevimab (CAS-IMD) have shown effectiveness in providing passive immunization against SARS-CoV-2 in KTRs [34]. CAS-IMD has been found to reduce viral loads and hospitalizations, and early use of bebtelovimab or sotrovimab in KTRs resulted in similar hospitalization and mortality rates during previous Omicron waves [59]. Sotrovimab has demonstrated effectiveness in reducing disease severity and may help neutralize Omicron, thus preventing severe COVID-19 in outpatient KTRs who are at high risk. However, it is worth noting that the effectiveness of monoclonal antibodies against Omicron variants has diminished. While BA.2 showed some sensitivity to CIL and IMD, it was resistant to sotrovimab and adintrevimab [60]. IC individuals receiving CAS-IMD showed no neutralization against BA.1 and weak neutralization against BA.2. TIX-CIL, although active against BA.2 and the Delta variant, was significantly weaker against BA.1, with reported breakthrough cases of Omicron [60]. Recent data on bamlanivimab/etesevimab (BAM-ETE) indicate significant reductions in COVID-19 hospitalizations and deaths, although some instances of drug resistance have been observed.[61]. Despite the increased risk of severe COVID-19 and death in KTRs due to chronic morbidities and immunosuppression, studies suggest that newer agents can be part of PrEP or early treatment strategies in early-diagnosed or mild COVID-19, serving as an alternative to vaccinations. A case report noted successful COVID-19 management without worsening the condition or organ rejection in a KTR receiving CAS-IMD, suggesting its potential role in preventing COVID-19 progression in KTRs [62].
Conclusions and Clinical Implications
The emergence of less-severe SARS-CoV-2 variants and milder disease has led to a reduced overall burden of disease in both the general population and IC patients. However, this has sometimes resulted in a false sense of security among IC patients, leading to relaxed attitudes toward personal protection, which can increase their risks of severe outcomes. While effective vaccination programs and improved clinical understanding have reduced the danger posed by SARS-CoV-2, the unpredictable nature of variant mutations may lead to the emergence of more virulent strains. Therefore, there is a need for continued vigilance and patient education and counselling to mitigate the risks of COVID-19 infections and severe outcomes in vulnerable patient groups.
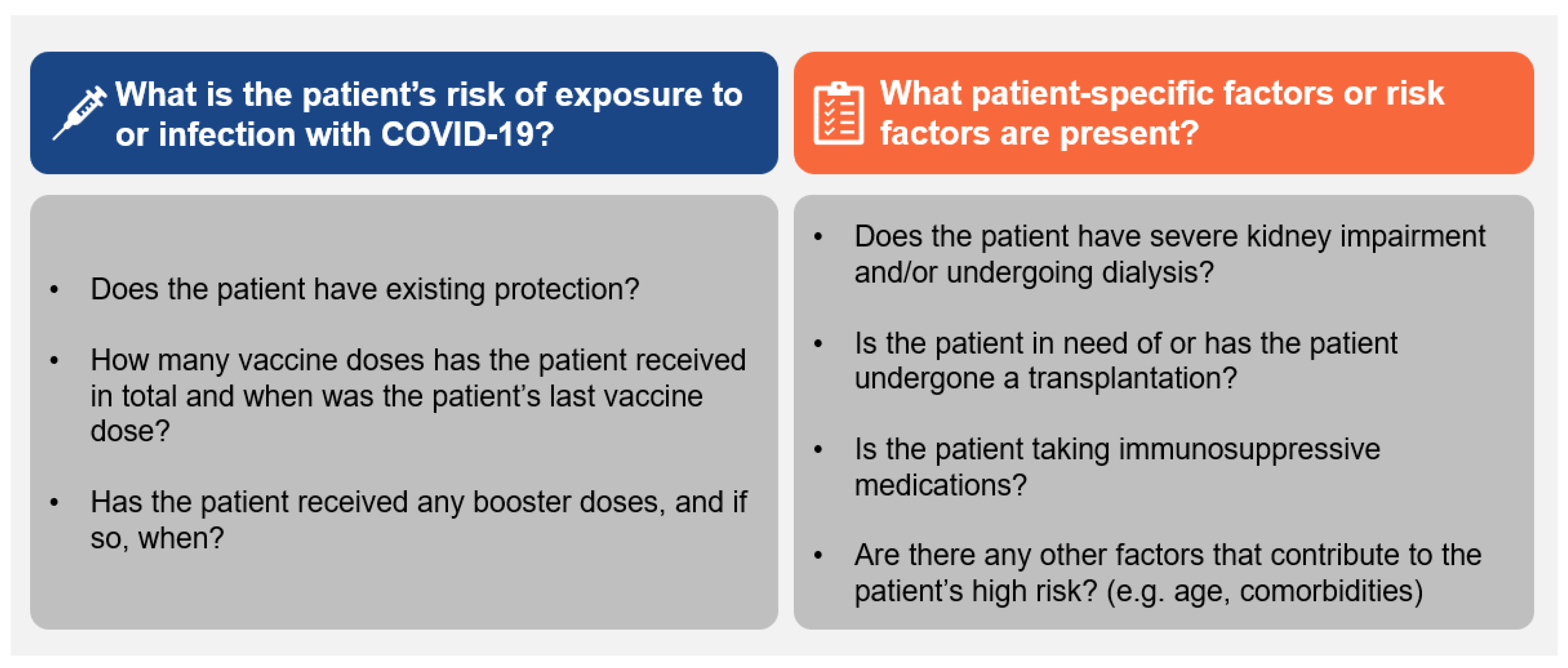
This expert group recognizes that COVID-19 continues to indirectly impact the lives of patients with kidney disease. Active COVID-19 infections can cause missed follow-up appointments, disruptions in dialysis sessions or treatments, and persistent infections that interfere with routine clinical management. Given the evolving COVID-19 situation, clinicians should assess CKD patients based on the following factors (Figure 3): (1) risk of exposure or infection, (2) existing protection including vaccination status and booster doses, (3) patient-specific factors such as the nature and severity of kidney disease and the degree of immunosuppression resulting from disease state or treatment, and (4) clinical risk factors including age, complexity and severity of IC state and presence of other high-risk conditions. Based on this assessment, clinicians can determine the urgency of preventative measures and the appropriate course of treatment for infections. In this endemic phase, CKD patients including those undergoing dialysis and KTRs should be considered as still vulnerable to severe COVID-19 progression and risk-stratified accordingly.
Funding
Funding for this manuscript was provided by AstraZeneca for medical writing support to summarize the existing literature and develop draft visuals for review and interpretation by the authors.
Declaration of Interest
Following the International Committee of Medical Journal Editors’ (ICMJE) guidelines, BAK reports receiving consulting fees and honoraria from AstraZeneca for lectures, and seminars. KN reports receiving consulting fees and honoraria from AstraZeneca, Otsuka, Sanofi-Aventis, Boehringer Ingelheim, Novo Nordisk, Celltrion, Novartis, Roche, Kyowa Kirin, Abbott, Sandoz, Zuellig Pharma, Astellas Pharma, Takeda, Bayer, Siam Pharmaceuticals, LG Life Sciences, Sanofi, Kowa, and Organon for lectures and seminars, and AstraZeneca, Novo Nordisk, Takeda and Bayer for advisory board attendance. Additionally, he has received a research grant from Visterra Inc., Alexion, AstraZeneca, Novo Nordisk, and ProKidney. He is also on the Board of Directors for the Thai Transplant Society. SC reports receiving consulting fees, honoraria for presentations and meeting attendance support from AstraZeneca. SK reports receiving consulting fees from Pfizer, MSD, Janssen, AstraZeneca, GSK, Takeda, and Sanofi. She also received honoraria for lectures/presentations from Pfizer, Astellas, MSD, Janssen, AstraZeneca, GSK, DKSH, Bristol Myers Squibb, AbbVie, Meiji, Siam, Daiichi Sankyo, Takeda, Sanofi, Mylan, DCH Auriga, Biopharm, BLHua, Roche, Berlin, Zuellig Pharma, Medtronic, Biogenetech, Celltrion, and Novartis. Additionally, she received meeting attendance support from Astellas, Pfizer, MSD, Janssen, DKSH, Bristol Myers Squibb, AbbVie, Siam, Daiichi Sankyo and Takeda. JB reports receiving honoraria and travel grants from AstraZeneca. BWT reports receiving consulting fees from AstraZeneca. He is also the President of the Singapore Hypertension Society and the Secretary-General, the Asian Pacific Society of Hypertension. Additionally, he holds stocks (non-controlling interest) of Alcon, Baxter, Haleon, GSK, CVS, Pfizer, MSD, Novo Nordisk, Sanofi, Takeda, Organon, Abbott, Becton-Dickinson, Amgen, AstraZeneca, and Bristol Myer Squibb. IR reports receiving a grant from Biotek. She also reports receiving honoraria from Pfizer, Takeda, Prodia, Dexamedica and Kalventis. She is also the Head of the Indonesian Society of Allergy and Immunology (ISAI/ PERALMUNI). ZH has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants, or patents received or pending, or royalties.
Acknowledgment
The authors wish to thank Hennis Tung of GCI Health and Shawna Tan of Medical Writers Asia for writing of the manuscript and Glen Halliwell, and Samantha Chua of GCI Health for literature review, data analysis, data visualizations and editorial input.
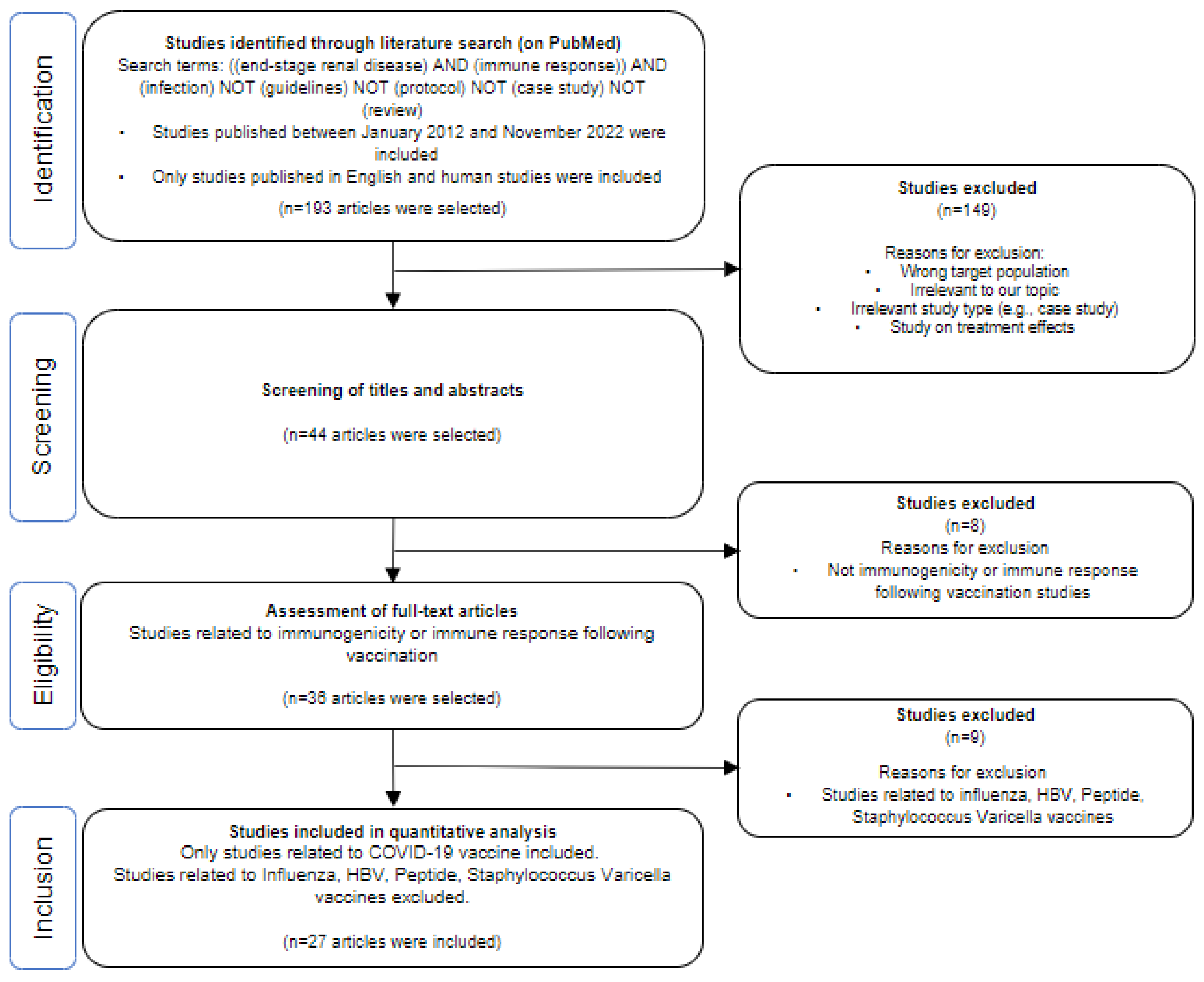
Appendix A: Flow Diagram Describing Systematic Selection of Studies on COVID-19 Vaccination Response for Literature Review
References
- Nejad, M.-M.M.; Moosaie, F.; Dehghanbanadaki, H.; Ghadery, A.H.; Shabani, M.; Tabary, M.; Aryannejad, A.; SeyedAlinaghi, S.; Rezaei, N. Immunogenicity of COVID-19 mRNA vaccines in immunocompromised patients: a systematic review and meta-analysis. Eur. J. Med Res. 2022, 27, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chavarot, N.; Gueguen, J.; Bonnet, G.; Jdidou, M.; Trimaille, A.; Burger, C.; Amrouche, L.; Weizman, O.; Pommier, T.; Aubert, O.; et al. COVID-19 severity in kidney transplant recipients is similar to nontransplant patients with similar comorbidities. Am. J. Transplant. 2020, 21, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Y.; Flahault, A.; Chavarot, N.; Melenotte, C.; Cheminant, M.; Deschamps, P.; Carlier, N.; Lafont, E.; Thomas, M.; Flamarion, E.; et al. Pre-exposure prophylaxis with tixagevimab and cilgavimab (Evusheld) for COVID-19 among 1112 severely immunocompromised patients. Clin. Microbiol. Infect. 2022, 28, 1654.e1–1654.e4. [Google Scholar] [CrossRef]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Clarke CL, Prendecki M, Dhutia A; et al. Longevity of SARS-CoV-2 immune responses in hemodialysis patients and protection against reinfection. Kidney Int 2021, 99, 1470–1477. [Google Scholar] [CrossRef]
- De Meester, J.; De Bacquer, D.; Naesens, M.; Meijers, B.; Couttenye, M.M.; De Vriese, A.S. ; for the NBVN Kidney Registry Group Incidence, Characteristics, and Outcome of COVID-19 in Adults on Kidney Replacement Therapy: A Regionwide Registry Study. J. Am. Soc. Nephrol. 2020, 32, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Pulliam JRC, van Schalkwyk C, Govender N; et al. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022, 376, eabn4947. [Google Scholar] [CrossRef] [PubMed]
- SARS-CoV-2 variants of concern as of 19 January 2024. [cited 2024 Jan 24]. Available at: https://www.ecdc.europa.eu/en/covid-19/variants-concern.
- El Karoui, K.; Hourmant, M.; Ayav, C.; Glowacki, F.; Couchoud, C.; Lapidus, N.; Registry, E. Vaccination and COVID-19 Dynamics in Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2022, 17, 395–402. [Google Scholar] [CrossRef]
- Cancarevic, I.; Nassar, M.; Daoud, A.; Ali, H.; Nso, N.; Sanchez, A.; Parikh, A.; Hosna, A.U.; Devanabanda, B.; Ahmed, N.; et al. Mortality rate of COVID-19 infection in end stage kidney disease patients on maintenance hemodialysis: A systematic review and meta-analysis. World J. Virol. 2022, 11, 352–361. [Google Scholar] [CrossRef]
- Sanders, J.-S.F.; Bemelman, F.J.; Messchendorp, A.L.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Frolke, S.C.; Geers, D.; GeurtsvanKessel, C.H.; et al. The RECOVAC Immune-response Study: The Immunogenicity, Tolerability, and Safety of COVID-19 Vaccination in Patients With Chronic Kidney Disease, on Dialysis, or Living With a Kidney Transplant. Transplantation 2022, 106, 821–834. [Google Scholar] [CrossRef]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; de Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: results of the ERACODA collaboration. Nephrol. Dial. Transplant. 2020, 35, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Garcia, I.; Perales-Fraile, I.; Gonzalez-Garcia, A.; Munoz-Blanco, A.; Manzano, L.; Fabregate, M.; Diez-Manglano, J.; Aizpuru, E.F.; Fernandez, F.A.; Garcia, A.G.; et al. In-hospital mortality among immunosuppressed patients with COVID-19: Analysis from a national cohort in Spain. PLOS ONE 2021, 16, e0255524. [Google Scholar] [CrossRef] [PubMed]
- Flythe, J.E.; Assimon, M.M.; Tugman, M.J.; Chang, E.H.; Gupta, S.; Sosa, M.A.; Renaghan, A.D.; Melamed, M.L.; Wilson, F.P.; Neyra, J.A.; et al. Characteristics and Outcomes of Individuals With Pre-existing Kidney Disease and COVID-19 Admitted to Intensive Care Units in the United States. Am. J. Kidney Dis. 2021, 77, 190–203. [Google Scholar] [CrossRef]
- Valeri, A.M.; Robbins-Juarez, S.Y.; Stevens, J.S.; Ahn, W.; Rao, M.K.; Radhakrishnan, J.; Gharavi, A.G.; Mohan, S.; Husain, S.A. Presentation and Outcomes of Patients with ESKD and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1409–1415. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.M.; Weiner, D.E.; Aweh, G.; Salenger, P.; Johnson, D.S.; Lacson, E. Epidemiology and Outcomes of COVID-19 in Home Dialysis Patients Compared with In-Center Dialysis Patients. J. Am. Soc. Nephrol. 2021, 32, 1569–1573. [Google Scholar] [CrossRef]
- Alberici F, Delbarba E, Manenti C; et al. A single center observational study of the clinical characteristics and short-term outcome of 20 kidney transplant patients admitted for SARS-CoV2 pneumonia. Kidney Int 2020, 97, 1083–1088. [Google Scholar] [CrossRef]
- Tannor, E.K.; Bajpai, D.; Nlandu, Y.M.; Wijewickrama, E. COVID-19 and Kidney Disease: Progress in Health Inequity From Low-Income Settings. Semin. Nephrol. 2022, 42, 151318. [Google Scholar] [CrossRef]
- Chou C-Y, Wang S-M, Liang C-C; et al. Risk of pneumonia among patients with chronic kidney disease in outpatient and inpatient settings: A nationwide population-based study. Medicine (Baltimore) 2014, 93, e174. [Google Scholar] [CrossRef]
- Sato, R.; Matsuzawa, Y.; Ogawa, H.; Kimura, K.; Tsuboi, N.; Yokoo, T.; Okada, H.; Konishi, M.; Kirigaya, J.; Fukui, K.; et al. Chronic kidney disease and clinical outcomes in patients with COVID-19 in Japan. Clin. Exp. Nephrol. 2022, 26, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Mohamed MMB, Velez JCQ. Proteinuria in COVID-19. Clin Kidney J 2021, 14, i40–i47.
- Mahalingasivam, V.; Su, G.; Iwagami, M.; Davids, M.R.; Wetmore, J.B.; Nitsch, D. COVID-19 and kidney disease: insights from epidemiology to inform clinical practice. Nat. Rev. Nephrol. 2022, 18, 485–498. [Google Scholar] [CrossRef]
- Brogan, M.; Ross, M.J. The Impact of Chronic Kidney Disease on Outcomes of Patients with COVID-19 Admitted to the Intensive Care Unit. Nephron 2021, 146, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Hayek, S.S.; Wang, W.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Factors Associated With Death in Critically Ill Patients With Coronavirus Disease 2019 in the US. JAMA Intern. Med. 2020, 180, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Geetha, D.; Kronbichler, A.; Rutter, M.; Bajpai, D.; Menez, S.; Weissenbacher, A.; Anand, S.; Lin, E.; Carlson, N.; Sozio, S.; et al. Impact of the COVID-19 pandemic on the kidney community: lessons learned and future directions. Nat. Rev. Nephrol. 2022, 18, 724–737. [Google Scholar] [CrossRef] [PubMed]
- Behlul, S.; Ozdal, M.A. Risk of COVID-19 and Cost Burden in End-Stage Renal Disease Patients and Policy Implications for Managing Nephrology Services during the COVID-19 Pandemic. Healthcare 2022, 10, 2351. [Google Scholar] [CrossRef] [PubMed]
- Hemmelder, M.H.; Noordzij, M.; Vart, P.; Hilbrands, L.B.; Jager, K.J.; Abrahams, A.C.; Arroyo, D.; Battaglia, Y.; Ekart, R.; Mallamaci, F.; et al. Recovery of dialysis patients with COVID-19: health outcomes 3 months after diagnosis in ERACODA. Nephrol. Dial. Transplant. 2022, 37, 1140–1151. [Google Scholar] [CrossRef] [PubMed]
- Impact of COVID-19 on the mortality of dialysis patients and kidney transplant recipients during the Omicron fifth wave in Hong Kong. HKMJ.. [cited 2024 Jan 25]. Available at: https://www.hkmj.org/abstracts/v29n1/82.htm.
- Pan, X.W.; Xu, D.; Zhang, H.; Zhou, W.; Wang, L.-H.; Cui, X.G. Identification of a potential mechanism of acute kidney injury during the COVID-19 outbreak: a study based on single-cell transcriptome analysis. Intensive Care Med. 2020, 46, 1114–1116. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef]
- Galmiche, S.; Nguyen, L.B.L.; Tartour, E.; de Lamballerie, X.; Wittkop, L.; Loubet, P.; Launay, O. Immunological and clinical efficacy of COVID-19 vaccines in immunocompromised populations: a systematic review. Clin. Microbiol. Infect. 2022, 28, 163–177. [Google Scholar] [CrossRef] [PubMed]
- Bertrand D, Hamzaoui M, Lemée V; et al. Antibody and T Cell Response to SARS-CoV-2 Messenger RNA BNT162b2 Vaccine in Kidney Transplant Recipients and Hemodialysis Patients. J Am Soc Nephrol 2021, 32, 2147–2152. [Google Scholar] [CrossRef] [PubMed]
- Cucchiari D, Egri N, Bodro M; et al. Cellular and humoral response after MRNA-1273 SARS-CoV-2 vaccine in kidney transplant recipients. Am J Transplant 2021, 21, 2727–2739. [Google Scholar] [CrossRef] [PubMed]
- Rozen-Zvi B, Yahav D, Agur T; et al. Antibody response to SARS-CoV-2 mRNA vaccine among kidney transplant recipients: A prospective cohort study. Clin Microbiol Infect 2021, 27, 1173–e1. [Google Scholar]
- Stumpf J, Siepmann T, Lindner T; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg Health Eur 2021, 9, 100178. [Google Scholar] [CrossRef] [PubMed]
- See, K.C. Vaccination for the Prevention of Infection among Immunocompromised Patients: A Concise Review of Recent Systematic Reviews. Vaccines 2022, 10, 800. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. Jama-Journal Am. Med Assoc. 2021, 326, 2043–2054. [Google Scholar] [CrossRef]
- Falahi, S.; Sayyadi, H.; Kenarkoohi, A. Immunogenicity of COVID-19 mRNA vaccines in hemodialysis patients: Systematic review and meta-analysis. Heal. Sci. Rep. 2022, 5, e874. [Google Scholar] [CrossRef] [PubMed]
- Intawong, K.; Chariyalertsak, S.; Chalom, K.; Wonghirundecha, T.; Kowatcharakul, W.; Thongprachum, A.; Chotirosniramit, N.; Noppakun, K.; Khwanngern, K.; Teacharak, W.; et al. Waning vaccine response to severe COVID-19 outcomes during omicron predominance in Thailand. PLOS ONE 2023, 18, e0284130. [Google Scholar] [CrossRef]
- COVID-19 Related Infection Prevention for the Immunocompromised Host - ISID. [cited 2024 Jan 25]. Available at: https://isid.org/guide/pathogens/covid-19-infection-prevention/. https://isid.org/guide/pathogens/covid-19-infection-prevention/.
- Gruell H, Vanshylla K, Tober-Lau P; et al. mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. Nat Med 2022, 28, 477–480. [Google Scholar] [CrossRef]
- Pérez-Then E, Lucas C, Monteiro VS; et al. Neutralizing antibodies against the SARS-CoV-2 Delta and Omicron variants following heterologous CoronaVac plus BNT162b2 booster vaccination. Nat Med 2022, 28, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Thammathiwat, T.; Tungsanga, S.; Tiankanon, K.; Torvorapanit, P.; Chumpangern, W.; Udomkarnjananun, S.; Avihingsanon, Y.; Sriprasart, T.; Srisawat, N.; Jutivorakool, K.; et al. A case of successful treatment of severe COVID-19 pneumonia with favipiravir and tocilizumab in post–kidney transplant recipient. Transpl. Infect. Dis. 2020, 23, e13388. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Lin, H.; Wu, Y.; Fang, Y.; Kumar, R.; Chen, G.; Lin, S. COVID-19 in posttransplant patients—report of 2 cases. Am. J. Transplant. 2020, 20, 1879–1881. [Google Scholar] [CrossRef] [PubMed]
- Hilhorst, M.; Bemelman, F.J.; Bruchfeld, A.; Fernandez-Juarez, G.M.; Floege, J.; Frangou, E.; Goumenos, D.; van Kooten, C.; Kronbichler, A.; I Stevens, K.; et al. Prophylactic and early outpatient treatment of COVID-19 in patients with kidney disease: considerations from the Immunonephrology Working Group of the European Renal Association (ERA-IWG). Nephrol. Dial. Transplant. 2023, 38, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Hus, I.; Szymczyk, A.; Mańko, J.; Drozd-Sokołowska, J. COVID-19 in Adult Patients with Hematological Malignancies—Lessons Learned after Three Years of Pandemic. Biology 2023, 12, 545. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, MW. Outpatient treatment options to address the SARS-CoV-2 variant Omicron. Expert Rev Anti Infect Ther 2022, 20, 1129–1133. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.J.; Ustianowski, A.; De Wit, S.; Launay, O.; Avila, M.; Templeton, A.; Yuan, Y.; Seegobin, S.; Ellery, A.; Levinson, D.J.; et al. Intramuscular AZD7442 (Tixagevimab–Cilgavimab) for Prevention of Covid-19. New Engl. J. Med. 2022, 386, 2188–2200. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Akerman, A.; Milogiannakis, V.; Silva, M.R.; Walker, G.; Stella, A.O.; Kindinger, A.; Angelovich, T.; Waring, E.; Amatayakul-Chantler, S.; et al. SARS-CoV-2 Omicron BA.5: Evolving tropism and evasion of potent humoral responses and resistance to clinical immunotherapeutics relative to viral variants of concern. EBioMedicine 2022, 84, 104270. [Google Scholar] [CrossRef] [PubMed]
- Hirsch C, Park YS, Piechotta V; et al. SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19. Cochrane Database Syst Rev 2022, 6, CD014945. [Google Scholar]
- Focosi, D.; Casadevall, A. A Critical Analysis of the Use of Cilgavimab plus Tixagevimab Monoclonal Antibody Cocktail (Evusheld™) for COVID-19 Prophylaxis and Treatment. Viruses 2022, 14, 1999. [Google Scholar] [CrossRef]
- Takashita, E.; Yamayoshi, S.; Simon, V.; Van Bakel, H.; Sordillo, E.M.; Pekosz, A.; Fukushi, S.; Suzuki, T.; Maeda, K.; Halfmann, P.; et al. Efficacy of Antibodies and Antiviral Drugs against Omicron BA.2.12.1, BA.4, and BA.5 Subvariants. New Engl. J. Med. 2022, 387, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Huygens, S.; Munnink, B.O.; Gharbharan, A.; Koopmans, M.; Rijnders, B. Sotrovimab Resistance and Viral Persistence After Treatment of Immunocompromised Patients Infected With the Severe Acute Respiratory Syndrome Coronavirus 2 Omicron Variant. Clin. Infect. Dis. 2022, 76, E507–E509. [Google Scholar] [CrossRef] [PubMed]
- Destras G, Bal A, Simon B, Lina B, Josset L. Sotrovimab drives SARS-CoV-2 omicron variant evolution in immunocompromised patients. Lancet Microbe 2022, 3, e559. [Google Scholar] [CrossRef] [PubMed]
- Tao K, Tzou PL, Kosakovsky Pond SL, Ioannidis JPA, Shafer RW. Susceptibility of SARS-CoV-2 Omicron Variants to Therapeutic Monoclonal Antibodies: Systematic Review and Meta-analysis. Microbiol Spectr 2022, 10, e0092622. [Google Scholar]
- Khan BA, Pagsinohin M, Lu LM, Tan P, Teo R. Tixagevimab and Cilgavimab Administration for Hemodialysis Patients at Community-Based Dialysis Centers in Singapore as Pre-Exposure Prophylaxis for SARS-CoV-2 Infection. Cureus 2023, 15, e41297. [Google Scholar]
- Yetmar, Z.A.; Beam, E.; O'Horo, J.C.; Seville, M.T.; Brumble, L.; Ganesh, R.; Razonable, R.R. Outcomes of bebtelovimab and sotrovimab treatment of solid organ transplant recipients with mild-to-moderate coronavirus disease 2019 during the Omicron epoch. Transpl. Infect. Dis. 2022, 24, e13901. [Google Scholar] [CrossRef] [PubMed]
- Bruel T, Hadjadj J, Maes P; et al. Serum neutralization of SARS-CoV-2 Omicron sublineages BA.1 and BA.2 in patients receiving monoclonal antibodies. Nat Med 2022, 28, 1297–1302. [Google Scholar] [CrossRef]
- Tai, Y.-L.; Lee, M.-D.; Chi, H.; Chiu, N.-C.; Lei, W.-T.; Weng, S.-L.; Liu, L.Y.-M.; Chen, C.-C.; Huang, S.-Y.; Huang, Y.-N.; et al. Effects of bamlanivimab alone or in combination with etesevimab on subsequent hospitalization and mortality in outpatients with COVID-19: a systematic review and meta-analysis. PeerJ 2023, 11, e15344. [Google Scholar] [CrossRef] [PubMed]
- Kijima, Y.; Shimizu, T.; Kato, S.; Kano, K.; Horiuchi, T.; Nozaki, T.; Omoto, K.; Inui, M.; Toma, H.; Iida, S.; et al. Case Report of COVID-19 Infection After Kidney Transplant Treated With Casirivimab-Imdevimab and Mycophenolate Mofetil Changed to Everolimus. Transplant. Proc. 2021, 54, 1561–1563. [Google Scholar] [CrossRef]
- Arbel, R.; Sagy, Y.W.; Hoshen, M.; Battat, E.; Lavie, G.; Sergienko, R.; Friger, M.; Waxman, J.G.; Dagan, N.; Balicer, R.; et al. Nirmatrelvir Use and Severe Covid-19 Outcomes during the Omicron Surge. New Engl. J. Med. 2022, 387, 790–798. [Google Scholar] [CrossRef]
- Zhou S, Hill CS, Sarkar S; et al. β-d-N4-hydroxycytidine Inhibits SARS-CoV-2 Through Lethal Mutagenesis But Is Also Mutagenic To Mammalian Cells. J Infect Dis 2021, 224, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Kabinger F, Stiller C, Schmitzová J; et al. Mechanism of molnupiravir-induced SARS-CoV-2 mutagenesis. Nat Struct Mol Biol 2021, 28, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Caraco, Y.; Crofoot, G.E.; Moncada, P.A.; Galustyan, A.N.; Musungaie, D.B.; Payne, B.; Kovalchuk, E.; Gonzalez, A.; Brown, M.L.; Williams-Diaz, A.; et al. Phase 2/3 Trial of Molnupiravir for Treatment of Covid-19 in Nonhospitalized Adults | NEJM Evidence. [cited 2024 Jan 25]. Available at: https://evidence.nejm.org/doi/full/10.1056/EVIDoa2100043. [CrossRef] [PubMed]
- Jayk Bernal A, Gomes da Silva MM, Musungaie DB; et al. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N Engl J Med 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Hobbs, F.D.R.; A Gbinigie, O.; Rahman, N.M.; Hayward, G.; Richards, D.B.; Dorward, J.; Lowe, D.M.; Standing, J.F.; Breuer, J.; et al. Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): an open-label, platform-adaptive randomised controlled trial. Lancet 2023, 401, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Poissy, J.; Belhadi, D.; Diallo, A.; Lê, M.-P.; Peytavin, G.; Staub, T.; et al. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): a phase 3, randomised, controlled, open-label trial. Lancet Infect. Dis. 2022, 22, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients. New Engl. J. Med. 2021, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Pettit NN, Pisano J, Nguyen CT; et al. Remdesivir Use in the Setting of Severe Renal Impairment: A Theoretical Concern or Real Risk? Clin Infect Dis 2021, 73, e3990–e3995. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19. New Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef]
- Shah S, Ackley TW, Topal JE. Renal and Hepatic Toxicity Analysis of Remdesivir Formulations: Does What Is on the Inside Really Count? Antimicrob Agents Chemother 2021, 65, e0104521. [Google Scholar] [CrossRef]
Figure 1.
Literature review findings on seropositive conversion rates following two-dose vaccination in patients on hemodialysis and peritoneal dialysis and KTRs.
Figure 1.
Literature review findings on seropositive conversion rates following two-dose vaccination in patients on hemodialysis and peritoneal dialysis and KTRs.
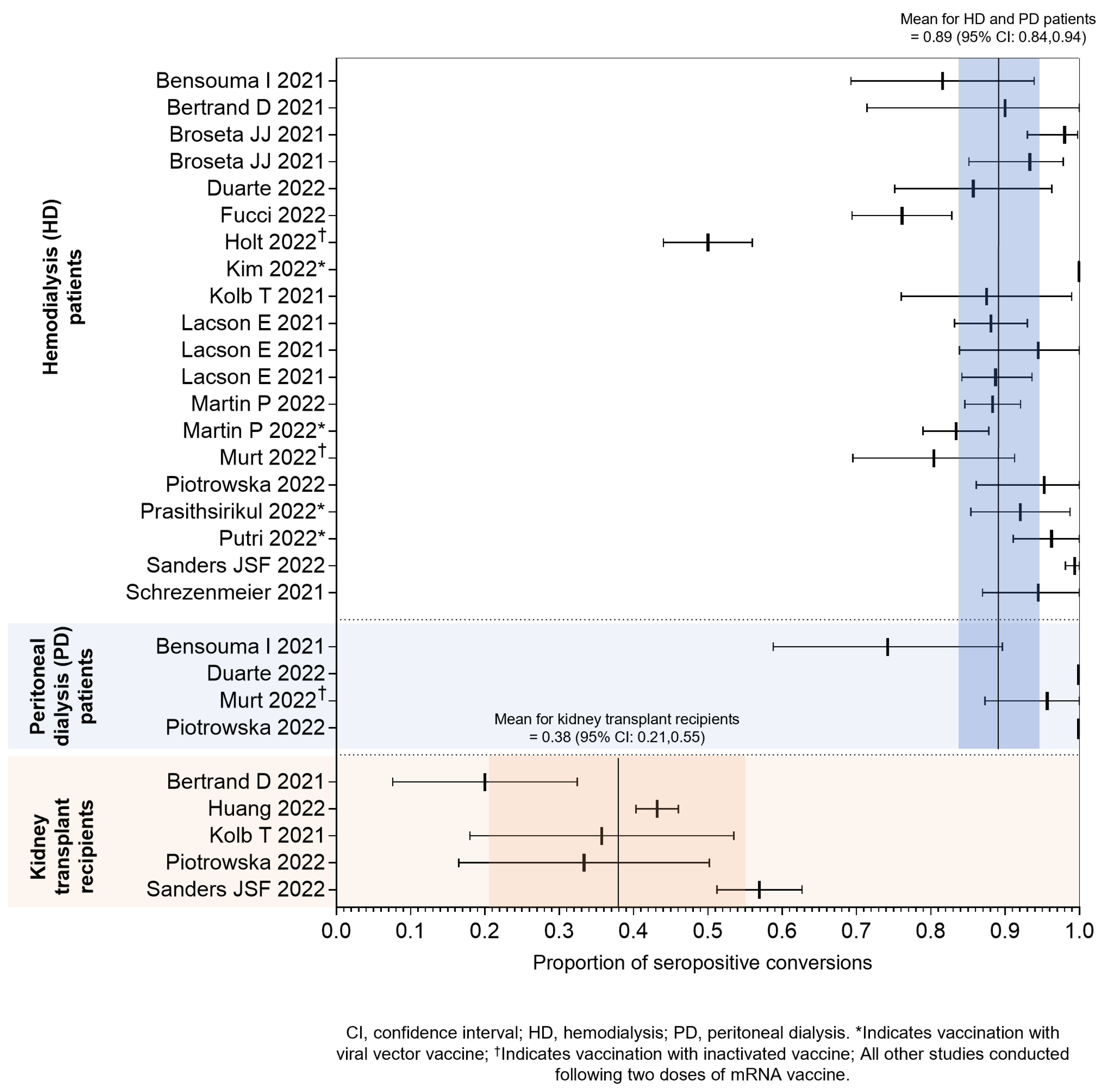
Figure 2.
COVID-19 risk mitigation strategies for CKD/ESKD patients and KTRs.
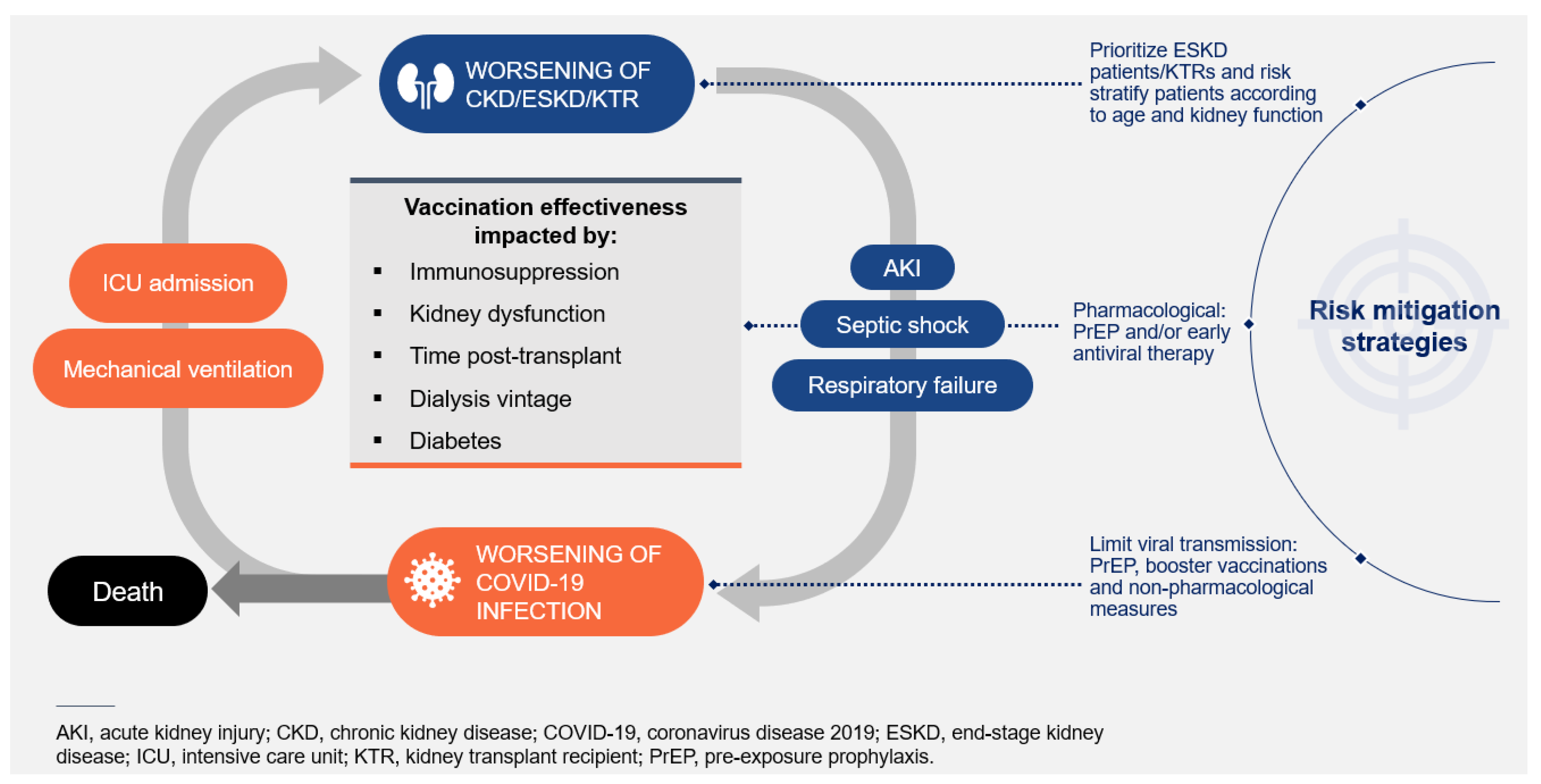
Figure 3.
Key questions for guiding risk assessment and management of patients with CKD and KTRs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



