
Submitted:
20 May 2024
Posted:
21 May 2024
You are already at the latest version
Abstract
Background/Objectives: The aim of this study was to investigate feasibility and safety of neuromuscular electrical stimulation (NMES) in patients on extracorporeal membrane oxygenation (ECMO) and assess thoroughly any potential adverse events. Methods: We conducted a safety and feasibility study including 16 ICU patients on ECMO support who were admitted to the cardiac surgery ICU from January 2022 to December 2023. Patients underwent a 45-minute NMES session, still on ECMO support, that included a warm up phase of 5 minutes, a main phase of 35 minutes and a recovery phase of 5 minutes. NMES was implemented on vastus lateralis, vastus medialis, gastrocnemius and peroneus longus muscle of both lower extremities. Two stimulators delivered biphasic, symmetric impulses of 75 Hz, with 400 μsec pulse duration, 5 sec on (1,6 sec ramp up and 0,8 sec ramp down) and 21 sec off. The intensity levels aimed to cause visible contractions and be well tolerated. Primary outcomes of the study were feasibility and safety, evaluated by whether the NMES sessions were successfully achieved, and by any adverse events and complications. Secondary outcomes included indices of rhabdomyolysis from biochemical blood test, 24 hours after the application of NMES. Results: All patients successfully completed their 45-minute NMES session, without presenting hemodynamic deterioration, adverse events or signs of rhabdomyolysis. The majority of patients achieved type 4 and 5 quality of muscle contraction. Conclusions: NMES is a safe and feasible exercise methodology in patients supported with ECMO.
Keywords:
neuromuscular electrical stimulation (NMES)
; extracorporeal membrane oxygenation (ECMO)
; intensive care unit (ICU)
; safety
; feasibility
1. Introduction
Neuromuscular Electrical Stimulation (NMES) is a modality of muscle exercise that applies electrical currents over muscles and nerves in a manner that produces smooth tetanic muscle contractions that simulate an exercise therapy session [1]. It has been used during the last 2 decades to improve muscle strength, prevent muscle atrophy, maintain the range of motion around a joint, and increase functional capacity through the activity of large muscle groups [2].
The implementation of NMES in stroke, heart failure and chronic obstructive pulmonary disease rehabilitation has been shown promising as an alternative modality of exercise training [3,4,5]. There is also growing evidence that NMES may prevent Intensive Care acquired weakness (ICUAW) promoting early mobilization in critically ill patients with sepsis or those who require mechanical ventilation [6,7,8]. Moreover, in a recent systematic review we have also shown that NMES is safe, feasible and has beneficial effects on muscle strength and function in patients after cardiac surgery [9].
Extracorporeal Membrane Oxygenation (ECMO) is a short-term lifesaving mechanical organ support therapy for patients with severe respiratory failure, cardiogenic shock or cardiac arrest refractory to conventional therapy. However, patients requiring ECMO support usually present ICUAW with significant muscle wasting and weakness with high risk of post-intensive care syndrome that affect ECMO survivors’ quality of life [10,11].
Despite the potential beneficial effects of NMES implementation in ECMO patients, no relevant study has been reported so far to allow further investigation.
Our study hypothesis was that the use of NMES in ECMO patients is safe and feasible. The aim of our study was to investigate feasibility and safety of NMES in patients on ECMO and assess thoroughly any potential adverse events.
2. Materials and Methods
2.1. Study Design
This is an observational safety and feasibility study assessing NMES in patients on ECMO support. The study was conducted in the cardiac surgery ICU of in Athens, Greece within a 2-year time period; from January 2022 to December 2023. The study was in accordance with the ethical guidelines of the Declaration of Helsinki, and the institutional review board (IBR) and the Ethics Committee of Onassis Cardiac Surgery Center approved this study and data management (IRB number 664/12.12.2019, December 12, 2019, The effects of neuromuscular electrical stimulation in patients with extracorporeal membrane oxygenation support).
2.2. Patients
Patients were fully informed about the intervention including the potential benefits and risks, and a written informed consent form was obtained prior to the intervention from all patients or their next of kin.
Inclusion criteria were: i. hemodynamically stable patients in the cardiac surgery ICU after cardiac surgery, cardiogenic shock or heart/lung transplantation [mean arterial blood pressure more than 65 mm Hg, use of vasopressors <50% of the maximum dose, heart rate between 50 and 140 bpm, without arrhythmias with hemodynamic consequences or myocardial ischemia, temperature between 34 and 38oC, intracranial pressure <20 cmH2O, no significant decrease in peripheral oxygen saturation (SpO2) baseline value or <88% for more than 1 minute] and ii. age ≥18 years.
Exclusion criteria were patients who had active tissue infection at the areas where the electrodes would be placed, pregnant women, patients with body mass index greater than 35 kg/m2, other contraindications of NMES including fractures, burns, skin lesions, thromboembolic disease, deep vein thrombosis, lower limb amputations.
All ECMO patients had ECMO configuration according to our Institute protocol (femoro-femoral Veno-arterial ECMO and femoro-jugular Veno-venous ECMO).
2.3. NMES Protocol
NMES was implemented on vastus lateralis, vastus medialis, gastrocnemius and peroneus longus muscle of both lower extremities. The single session had a duration of 45 minutes and included a warm up phase of 5 minutes, a main phase of 35 minutes and a recovery phase of 5 minutes. We used two stimulators (4-channel T-One Medi Sport Electric stimulator, I-TECH Medical Division, Scorzè, Italy) which delivered biphasic, symmetric impulses of 75 Hz, with 400 μsec pulse duration, 5 sec on (1,6 sec ramp up and 0,8 sec ramp down) and 21 sec off. The intensity levels aimed to cause visible contractions and be tolerated by the patients. In case of doubt, contraction was confirmed by palpation (Figure 1).
The quality of muscle contraction was rated using a 5-point scoring system: (type 1) no palpable or visible contraction, (type 2) just palpable but no visible contraction, (type 3) just palpable and visible contraction, (type 4) palpable and visible contraction (partial muscle bulk) and (type 5) palpable and visible contraction (full muscle bulk) [12,13]. The target quality of contraction was type 3 at warming up and recovery phase t and type 4 or 5 at the main phase.
2.4. Outcomes
Primary outcomes of the study were feasibility and safety, evaluated by whether the NMES sessions were successfully achieved, and by any adverse events and complications such as severe arrhythmias, hypotension or dizziness, decrease in saturation, signs of pain during the electrical stimulation, muscle damage, cardiogenic shock or decannulation during the NMES implementation, respectively. The quality of muscle contraction was also rated during the 3 time points of NMES session; warm-up, main phase and recovery phase.
Secondary outcomes were pH and lactate from the arterial blood gas test, as well as indices of muscle damage from biochemical blood test including creatine phosphokinase (CPK), aspartate aminotransferase (AST), alanine aminotransferase (ALT) and lactate dehydrogenase (LDH), that were measured before and 24 hours after the application of NMES.
2.5. Statistical Analysis
Normality of distribution was checked with Shapiro-Wilk test. Variables are expressed as frequency and percentage, mean ± standard deviation (SD) or median (25th-75th percentiles). Paired two sample Student t test analyzed differences of dependent parameters with normal distribution while Wilcoxon signed-rank test analyzed differences for nonparametric data. Differences between time points were assessed with repeated measures factorial analysis of variance (ANOVA). All tests were two tailed and level of statistical significance was set at 0.05. Statistical analyses were performed with IBM SPSS 25 Statistics software (Armonk, NY, United States).
3. Results
Demographics and clinical data regarding ECMO patients are demonstrated in detail in Table 1. Initially, 16 patients met the inclusion criteria to enroll the study. However, 2 patients were finally excluded; the first patient presented significant edema of the lower limbs and no contraction could be observed during NMES, while the second patient experienced a brief episode of intense anxiety and we avoided performing NMES and deteriorating the situation. Our final sample size in the analysis of the parameters of interest consisted of 14 ICU patients on ECMO support.
No adverse events or complications due to NMES were observed. Median intensities of the electrical stimulation for both limbs according to NMES phases are presented in Table 1. With regards to the quality of muscle contraction, the majority of patients achieved type 4 and 5 contraction (Table 1).
All patients successfully completed their 45-minute NMES session, without presenting hemodynamic deterioration or any event such as hypotension, severe arrhythmia, desaturation or discomfort. Hemodynamic parameters did not change during NMES session; before NMES, 5 minutes, 35 minutes and 40 minutes after NMES initiation (Table 2). Arterial blood gas indices including pH and lactate remained unchanged within 2 time points (before and after NMES, Table 2). Finally, biochemical blood test did not show any difference in CPK, AST, and LDH 24 hours after the NMES session, indicating that there were no signs of rhabdomyolysis (muscle damage) due to the intervention. ALT significantly decreased 24 hours after the intervention (Table 2).
4. Discussion
The findings of our study have shown that NMES implementation is safe and feasible in patients on ECMO support. To the best of our knowledge our study is the first to demonstrate NMES safety and feasibility in ECMO patients. assessing adverse events and complications but also respiratory, hemodynamic and biochemical parameters and arterial blood gas indices before and after NMES session.
There has been only a single crossover feasibility case study in the literature where authors investigated the effects of NMES applied to the quadriceps muscle on the pedal perfusion of patients receiving veno-venous ECMO (VV-ECMO) via bifemoral cannulation [14].
In accordance to our findings, NMES application seemed to be well tolerated, with no alteration to ECMO flows, sedation requirements, or observed cardiovascular parameters, indicating that NMES may be a viable exercise modality in bifemorally cannulated VV-ECMO patients who cannot perform early mobilization exercises or other modalities of exercise. However, the sample size was quite small, including only 3 patients, and, as a result, no safe conclusions could be extracted from that study.
ICUAW is a common complication of critically ill patients on ECMO or patients on ECMO as a bridge to lung/heart transplantation or as a bridge to recovery in the ICU, leading to persistent functional disability and decreased quality of life after hospital discharge [15]. The major risk factors for ICUAW are immobilization, multiple organ failure, systemic inflammatory response syndrome, gram-negative septicemia [16], hyperglycemia [17,18], and medications such as aminoglycosides and corticosteroids. There are various proposed modalities of early rehabilitation, especially in patients with ECMO, that have the potential to prevent skeletal-muscle weakness and wasting in critically ill patients [19,20]. These interventions include passive mobilization via stretching, splinting and passive movements, continuous passive motion, functional electrical stimulation of the lower limb muscles and passive cycling for unconscious patients of higher severity or intubated patients, as well as active range of motion and resistance exercises such as leg press, squats from sitting position, active cycling, mobilization in a standing position and walking, and respiratory rehabilitation and breathing exercises for awake patients with satisfying level of consciousness who can follow orders or give feedback [20].
NMES is an exercise modality that can be applied even in sedated critical ill patients which has been also shown to be effective in reducing ICUAW incidence [21]. NMES prescription includes the NMES frequency in Hz, which is the number of pulses in one second (20-50 pulses per second), the pulse duration in microseconds (for small muscles is approximately 150-200 and for large muscles 200-300), the ramp time which is at least 2 seconds, the exercise / recovery time ratio which should be set to allow enough time for muscle recovery from exercise, the treatment session which should be at least 20 to 30 minutes, and the frequency of the sessions which should be at least three times a week when it is applied systemically at the patient [1,22]. NMES normally involves frequencies between 20 and 50 Hz and pulse widths between 200 and 400 μs [23] and should recruit motor axons preferentially to sensory axons [24]. Higher exercise/recovery ratio (1:5) provides more rest time between muscle contractions and cause less muscle fatigue [1]. In our study, we used biphasic, symmetric impulses of 75 Hz, with 400 μsec pulse duration, 5 sec on (1,6 sec ramp up and 0,8 sec ramp down) and 21 sec off based on previous studies [25,26]. Although the intensity levels were higher than suggested, we aimed to cause visible contractions and be tolerated by the patients. Moreover, our higher exercise/recovery time ratio may have prevented muscle fatigue by providing more rest time between muscle contractions.
Motor impairment and activity limitation have been shown to reduce after the implementation of NMES, without however, fully understanding the potential mechanisms. One hypothesis is that therapeutic effects of NMES are probably due to a combination of peripheral cardiovascular and musculoskeletal effects. Peripheral effects of NMES include increase in contractile force and fatigue resistance [27,28], increase in muscle mass [29], reduction of edema [30], conversion of fast-twitch fast-fatiguing glycolytic type II muscle fibers to slow-twitch fatigue-resistant oxidative type I muscle fibers [28], and enhanced hyperemic arterial response and endothelium-dependent cutaneous vasodilation [31]. Another beneficial effect of NMES may also be the fact that it affects the central nervous system and promote motor relearning by uniquely providing an artificial way of ensuring synchronized presynaptic and postsynaptic activity (Hebbian plasticity), especially if the electrical stimulation is paired with simultaneous voluntary effort that activates the residual upper motor neurons [32]. This mechanism of NMES could be quite useful for patients’ rehabilitation after stroke. Severe systematic inflammation, along with electrolyte changes, as well as intense edema may seriously affect conductivity and thus electrical current diffusion [33], and could reduce any systemic effect of NMES. Indeed, in our study we excluded 1 patient due to the severe edema that he presented at the lower limbs. However, a recent systematic review supports the use of NMES for ameliorating edema, indicating that it could be effective even in the treatment of both upper and lower limb edema [34]. This could be a future direction for randomized controlled trials, in order to investigate the treatment effect of NMES in patients with upper and lower limb edema.
Similar studies assessing NMES in critically ill patients have been previously performed by our research group. Specifically, the first study was performed by Gerovasili V et al. [35] back in 2009, who assessed the short-term effect of NMES of the lower extremities on the thenar muscle microcirculation of 29 critically ill ICU patients. Authors concluded that NMES had a systemic effect on microcirculation by improving oxygen consumption rate during vascular occlusion and reperfusion rate, as well as on hemodynamics by increasing heart rate and systolic BP. Some years later, in 2013, Angelopoulos E et al. [25] compared the effects on muscle microcirculation of a single NMES session using medium frequency currents of 45 Hz and high frequency currents of 75 Hz in ICU patients with systemic inflammatory response syndrome (SIRS) or sepsis. The study showed that a single NMES session affected local and systemic skeletal muscle microcirculation by improving endothelial reactivity and vascular reserve in both frequencies, with equally effective results between medium and high frequency currents. Interestingly, NMES has been also shown to promote endothelial progenitor cells (EPCs) after NMES session in critical ill patients indicating the potential beneficial effects on endothelial injury [26]. Finally, another recent study from our Institute investigated whether a high-frequency NMES protocol of 75Hz could result in a smaller loss of muscle mass than a moderate-frequency protocol of 45Hz in ICU patients [36]. Indeed, high frequency seemed to be more effective than moderate frequency as there was less loss of muscle layer thickness in the vastus intermedius and rectus femoris in ICU patients.
This is a safety and feasibility study with some limitations. The sample size was small including 16 patients on ECMO in the ICU. A multicenter randomized controlled trial with more patients on ECMO support is required in order to have robust results regarding NMES potentially beneficial effects. In our study we performed a single NMES session and thus, we did not investigate the chronic effect of NMES after regular implementation in these patients; however, this study was not designed to test NMES efficacy.
5. Conclusions
In conclusion, the findings of our study have shown that NMES is a safe and feasible exercise methodology in patients supported with ECMO. Further studies are required to assess NMES efficacy as a valid preventive and therapeutic tool for ICUAW promoting early mobilization in these patients.
Author Contributions
Conceptualization, S.A. and S.D.; methodology, E.K., S.N. and S.D.; validation, E.K., S.N. and S.D.; formal analysis, C.K. and S.D.; investigation, C.K., V.R., M.A., M.D., A.K., T.P., K.I., T.C. and S.D.; data curation, C.K., V.R., M.A., M.D. and S.D.; writing—original draft preparation, C.K.; writing—review and editing, V.R., M.A., M.D., A.K., E.K., T.P., K.I., S.N., S.A., T.C. and S.D.; supervision, S.N., S.A. and S.D.; funding acquisition, S.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Onassis Foundation and carried out in collaboration with Biomedical Research Foundation of the Academy of Athens (BRFAA).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Onassis Cardiac Surgery Center (IRB number 664/12.12.2019, December 12, 2019, The effects of neuromuscular electrical stimulation in patients with extracorporeal membrane oxygenation support).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nussbaum, E.L.; Houghton, P.; Anthony, J.; Rennie, S.; Shay, B.L.; Hoens, A.M. Neuromuscular Electrical Stimulation for Treatment of Muscle Impairment: Critical Review and Recommendations for Clinical Practice. Physiother. Can. 2017, 69, 1–76. [Google Scholar] [CrossRef] [PubMed]
- The Association of Paediatric Charted Physiotherapists. Publications. Available from: https://apcp.csp.org.uk/content/guide-use-electrical-stimulation-paediatric-neurodisabilityn (accessed 18/12/2022).
- Osman, H.; Siu, R.; Makowski, N.S.; Knutson, J.S.; Cunningham, D.A. Neurostimulation After Stroke. Phys. Med. Rehabil. Clin. N. Am. 2024, 35, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Ploesteanu, R.L.; Nechita, A.C.; Turcu, D.; Manolescu, B.N.; Stamate, S.C.; Berteanu, M. Effects of neuromuscular electrical stimulation in patients with heart failure - review. J. Med. Life 2018, 11, 107–118. [Google Scholar] [PubMed]
- LoMauro, A.; Gervasoni, F. 20 years of neuromuscular electrical stimulation in COPD. Eur. Respir. Rev. 2024, 33, 220247. [Google Scholar] [CrossRef] [PubMed]
- Gerovasili, V.; Stefanidis, K.; Vitzilaios, K.; Karatzanos, E.; Politis, P.; Koroneos, A.; Chatzimichail, A.; Routsi, C.; Roussos, C.; Nanas, S. Electrical muscle stimulation preserves the muscle mass of critically ill patients: a randomized study. Crit. Care 2009, 13, R161. [Google Scholar] [CrossRef] [PubMed]
- Karatzanos, E.; Gerovasili, V.; Zervakis, D.; Tripodaki, E.S.; Apostolou, K.; Vasileiadis, I.; Papadopoulos, E.; Mitsiou, G.; Tsimpouki, D.; Routsi, C.; et al. Electrical muscle stimulation: an effective form of exercise and early mobilization to preserve muscle strength in critically ill patients. Crit. Care Res. Pract. 2012, 2012, 432752. [Google Scholar] [CrossRef]
- Rodriguez, P.O.; Setten, M.; Maskin, L.P.; Bonelli, I.; Vidomlansky, S.R.; Attie, S.; Frosiani, S.L.; Kozima, S.; Valentini, R. Muscle weakness in septic patients requiring mechanical ventilation: protective effect of transcutaneous neuromuscular electrical stimulation. J. Crit. Care 2012, 27, 319.e1-8. [Google Scholar] [CrossRef] [PubMed]
- Kourek, C.; Kanellopoulos, M.; Raidou, V.; Antonopoulos, M.; Karatzanos, E.; Patsaki, I.; Dimopoulos, S. Safety and effectiveness of neuromuscular electrical stimulation in cardiac surgery: A systematic review. World J. Cardiol. 2024, 16, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Hayes, K.; Holland, A.E.; Pellegrino, V.A.; Mathur, S.; Hodgson, C.L. Acute skeletal muscle wasting and relation to physical function in patients requiring extracorporeal membrane oxygenation (ECMO). J. Crit. Care 2018, 48, 1–8. [Google Scholar] [CrossRef]
- Chen, X.; Lei, X.; Xu, X.; Zhou, Y.; Huang, M. Intensive Care Unit-Acquired Weakness in Patients With Extracorporeal Membrane Oxygenation Support: Frequency and Clinical Characteristics. Front. Med. (Lausanne) 2022, 9, 792201. [Google Scholar] [CrossRef]
- Segers, J.; Hermans, G.; Bruyninckx, F.; Meyfroidt, G.; Langer, D.; Gosselink, R. Feasibility of neuromuscular electrical stimulation in critically ill patients. J. Crit. Care 2014, 29, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.M.; Berney, S.; Warrillow, S.; El-Ansary, D.; Bryant, A.L.; Hart, N.; Puthucheary, Z.; Koopman, R.; Denehy, L. Functional electrical stimulation with cycling in the critically ill: a pilot case-matched control study. J. Crit. Care 2014, 29, 695–e1. [Google Scholar] [CrossRef]
- McCormack, P.F.; Tronstad, O.; Walsh, J.R. Does exercising the quadriceps muscle of patients on extracorporeal membrane oxygenation (ECMO) with electrical stimulation affect the blood flow to their feet? A feasibility study. J. Intensive Care Soc. 2023, 24, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Herridge, M.S.; Tansey, C.M.; Matté, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional disability 5 years after acute respiratory distress syndrome. N. Engl. J. Med. 2011, 364, 1293–304. [Google Scholar] [CrossRef]
- Nanas, S.; Kritikos, K.; Angelopoulos, E.; Siafaka, A.; Tsikriki, S.; Poriazi, M.; Kanaloupiti, D.; Kontogeorgi, M.; Pratikaki, M.; Zervakis, D.; et al. Predisposing factors for critical illness polyneuromyopathy in a multidisciplinary intensive care unit. Acta Neurol. Scand. 2008, 118, 175–181. [Google Scholar] [CrossRef] [PubMed]
- de Jonghe, B.; Lacherade, J.C.; Sharshar, T.; Outin, H. Intensive care unit-acquired weakness: risk factors and prevention. Crit. Care Med. 2009, 37, S309–315. [Google Scholar] [CrossRef]
- Deem, S. Intensive-care-unit-acquired muscle weakness. Respir. Care 2006, 51, 1042–1052; discussion 1052-1053. [Google Scholar] [PubMed]
- Lee, C.M.; Fan, E. ICU-acquired weakness: what is preventing its rehabilitation in critically ill patients? BMC Med. 2012, 10, 115. [Google Scholar] [CrossRef] [PubMed]
- Kourek, C.; Nanas, S.; Kotanidou, A.; Raidou, V.; Dimopoulou, M.; Adamopoulos, S.; Karabinis, A.; Dimopoulos, S. Modalities of Exercise Training in Patients with Extracorporeal Membrane Oxygenation Support. J. Cardiovasc. Dev. Dis. 2022, 9, 34. [Google Scholar] [CrossRef]
- Routsi, C.; Gerovasili, V.; Vasileiadis, I.; Karatzanos, E.; Pitsolis, T.; Tripodaki, E.; Markaki, V.; Zervakis, D.; Nanas, S. Electrical muscle stimulation prevents critical illness polyneuromyopathy: a randomized parallel intervention trial. Crit. Care 2010, 14, R74. [Google Scholar] [CrossRef]
- Baldwin, E.R.; Klakowicz, P.M.; Collins, D.F. Wide-pulse-width, high-frequency neuromuscular stimulation: implications for functional electrical stimulation. J. Appl. Physiol. (1985) 2006, 101, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Bowman, B.R.; Baker, L.L. Effects of waveform parameters on comfort during transcutaneous neuromuscular electrical stimulation. Ann. Biomed. Eng. 1985, 13, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Panizza, M.; Nilsson, J.; Roth, B.J.; Basser, P.J.; Hallett, M. Relevance of stimulus duration for activation of motor and sensory fibers: implications for the study of H-reflexes and magnetic stimulation. Electroencephalogr. Clin. Neurophysiol. 1992, 85, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulos, E.; Karatzanos, E.; Dimopoulos, S.; Mitsiou, G.; Stefanou, C.; Patsaki, I.; Kotanidou, A.; Routsi, C.; Petrikkos, G.; Nanas, S. Acute microcirculatory effects of medium frequency versus high frequency neuromuscular electrical stimulation in critically ill patients - a pilot study. Ann. Intensive Care 2013, 3, 39. [Google Scholar] [CrossRef] [PubMed]
- Stefanou, C.; Karatzanos, E.; Mitsiou, G.; Psarra, K.; Angelopoulos, E.; Dimopoulos, S.; Gerovasili, V; Boviatsis, E. ; Routsi, C.; Nanas, S. Neuromuscular electrical stimulation acutely mobilizes endothelial progenitor cells in critically ill patients with sepsis. Ann. Intensive Care 2016, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Peckham, P.H.; Mortimer, J.T.; Marsolais, E.B. Alteration in the force and fatigability of skeletal muscle in quadriplegic humans following exercise induced by chronic electrical stimulation. Clin. Orthop. Relat. Res. 1976, 114, 326–33. [Google Scholar] [CrossRef]
- Gondin, J.; Brocca, L.; Bellinzona, E.; D’Antona, G.; Maffiuletti, N.A.; Miotti, D.; Pellegrino, M.A.; Bottinelli, R. Neuromuscular electrical stimulation training induces atypical adaptations of the human skeletal muscle phenotype: a functional and proteomic analysis. J. Appl. Physiol. (1985) 2011, 110, 433–450. [Google Scholar] [CrossRef]
- Arija-Blázquez, A.; Ceruelo-Abajo, S.; Díaz-Merino, M.S.; Godino-Durán, J.A.; Martínez-Dhier, L.; Martin, J.L.; Florensa-Vila, J. Effects of electromyostimulation on muscle and bone in men with acute traumatic spinal cord injury: A randomized clinical trial. J. Spinal Cord Med. 2014, 37, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Meijer, J.W.; Voerman, G.E.; Santegoets, K.M.; Geurts, A.C. Short-term effects and long-term use of a hybrid orthosis for neuromuscular electrical stimulation of the upper extremity in patients after chronic stroke. J. Rehabil. Med. 2009, 41, 157–161. [Google Scholar] [CrossRef]
- Wang, J.S.; Chen, S.Y.; Lan, C.; Wong, M.K.; Lai, J.S. Neuromuscular electric stimulation enhances endothelial vascular control and hemodynamic function in paretic upper extremities of patients with stroke. Arch. Phys. Med. Rehabil. 2004, 85, 1112–1116. [Google Scholar] [CrossRef]
- Rushton, D.N. Functional electrical stimulation and rehabilitation--an hypothesis. Med. Eng. Phys. 2003, 25, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Harper, N.J.; Greer, R.; Conway, D. Neuromuscular monitoring in intensive care patients: milliamperage requirements for supramaximal stimulation. Br. J. Anaesth. 2001, 87, 625–627. [Google Scholar] [CrossRef] [PubMed]
- Burgess, L.C.; Immins, T.; Swain, I.; Wainwright, T.W. Effectiveness of neuromuscular electrical stimulation for reducing oedema: A systematic review. J. Rehabil. Med. 2019, 51, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Gerovasili, V.; Tripodaki, E.; Karatzanos, E.; Pitsolis, T.; Markaki, V.; Zervakis, D.; Routsi, C.; Roussos, C.; Nanas, S. Short-term systemic effect of electrical muscle stimulation in critically ill patients. Chest 2009, 136, 1249–1256. [Google Scholar] [CrossRef]
- Georgopoulos, C.; Katsogianni, A.; Patsaki, E.; Sidiras, G.; Vasileiadis, I.; Magira, E.; Nanas, S.; Karatzanos, E. High- vs medium-frequency neuromuscular electrical stimulation protocols on muscle mass in Intensive Care Unit patients, a pilot study. Health Res. J. 2023, 9, 219–236. [Google Scholar] [CrossRef]
Figure 1.
NMES session in a patient under VA-ECMO support in the cardiac surgery ICU.
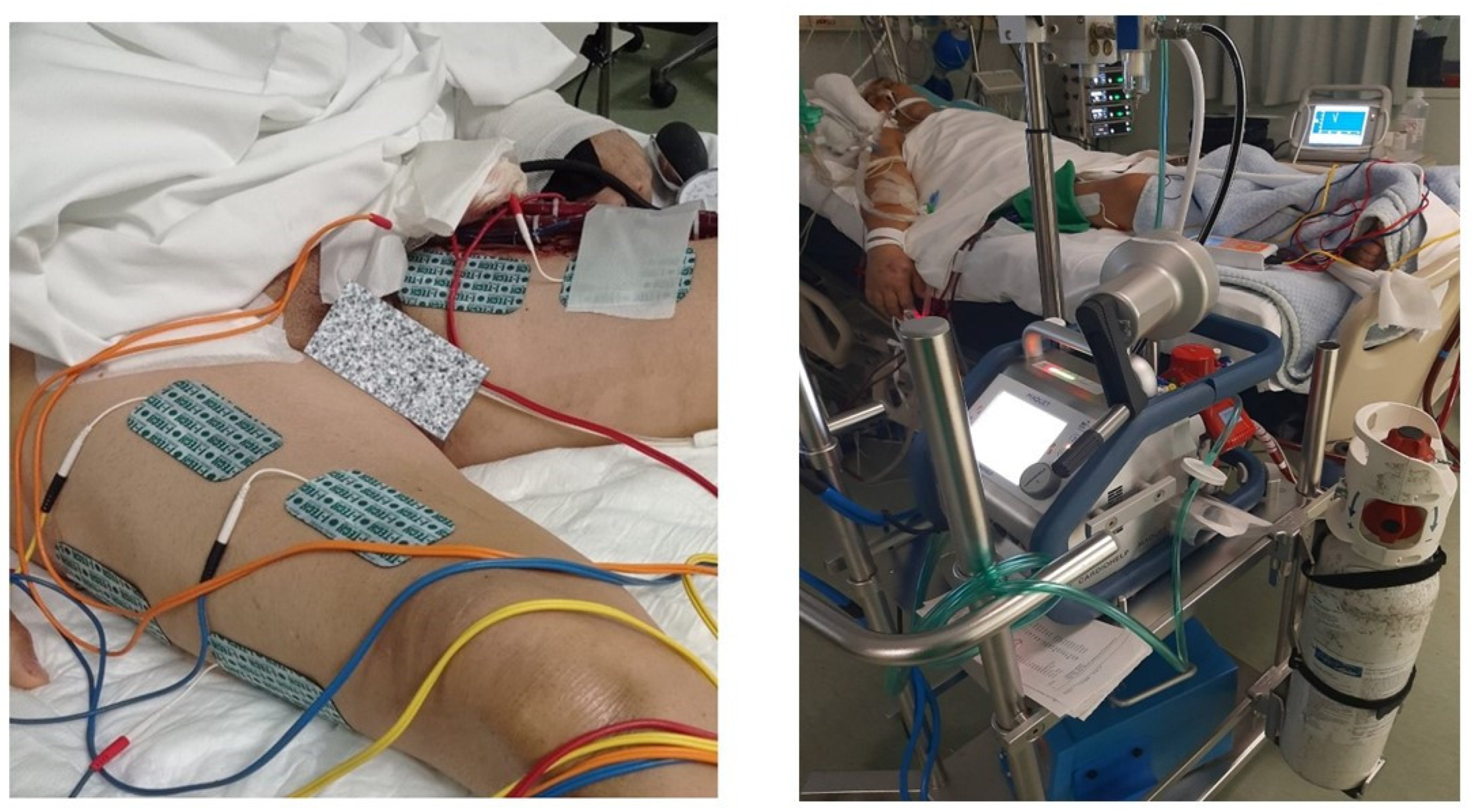

Table 1.
Demographic characteristics for patients under ECMO support who underwent a single NMES session.
Table 1.
Demographic characteristics for patients under ECMO support who underwent a single NMES session.
| Demographic characteristics | |
|---|---|
| Number of patients (N) | 16 |
| Gender (Females) | 10 (63%) |
| Age (years)a | 46.6 ± 13.7 |
| BMI (kg/m2)a | 25.8 ± 3.1 |
| Cause of ECMO | |
| Cardiogenic shock | 11 (69%) |
| Respiratory failure | 5 (31%) |
| ECMO parameters | |
| FiO2 (%)a | 71.6 ± 19.1 |
| LPM (L/min)a | 2.62 ± 1.03 |
| RPM (rounds/min)a | 2478.0 ± 611.5 |
| Type of ECMO | |
| VA-ECMO (femo-femoral) | 13 (81%) |
| VV-ECMO (femo-jugular) | 3 (19%) |
| Duration of ECMO (days)b | 8 (5-28.75) |
| Ventilation during NMES | 13 (81%) |
| Sedation during NMES | 9 (56%) |
| Type of muscle contractionb | |
| Warm up | 4 (3-4) |
| Main phase | 5 (4-5) |
| Recovery phase | 4 (2-4) |
| Amplitude of NMESb | |
| Warm up (mA) | 30 (20-55) |
| Main phase (mA) | 53 (30-86) |
| Recovery phase (mA) | 43 (36-74) |
ECMO, extracorporeal membrane oxygenation; BMI, body mass index; NMES, neuromuscular electrical stimulation; FiO2, fraction of inspired oxygen of ECMO circuit; LPM, flow rate of the ECMO circuit; RPM, pump speed of the ECMO circuit; VV-ECMO, veno-venous ECMO; VA-ECMO, veno-arterial ECMO; SD, standard deviation. a Values are expressed as mean ± SD. b Values are expressed as median (25th-75th percentiles).
Table 2.
Hemodynamic, respiratory, biochemical parameters and arterial blood gas indices during different time points, before and after NMES session.
Table 2.
Hemodynamic, respiratory, biochemical parameters and arterial blood gas indices during different time points, before and after NMES session.
| Hemodynamic parametersa | During NMES | ||||
|---|---|---|---|---|---|
| Before NMES | 5 min | 35 min | 40 min | P value | |
| Systolic BP (mmHg) | 114.1 ± 26.7 | 114.8 ± 22.3 | 114.4 ± 25.2 | 112.2 ± 21.1 | 0.484 |
| Diastolic BP (mmHg) | 68.4 ± 15.4 | 67.6 ± 17.5 | 66.8 ± 15.9 | 65.9 ± 16.1 | 0.181 |
| Mean BP (mmHg) | 82.1 ± 18.2 | 82.6 ± 15.3 | 82.7 ± 16.4 | 82.0 ± 16.0 | 0.964 |
| HR (beats/min) | 102.4 ± 19.7 | 101.1 ± 20.1 | 101.4 ± 20.5 | 100.2 ± 19.5 | 0.475 |
| SpO2 (%) | 95.1 ± 10.4 | 96.7 ± 3.8 | 97.2 ± 3.4 | 97.2 ± 3.2 | 0.442 |
| RR (breaths/min) | 17.3 ± 6.2 | 18.3 ± 5.5 | 18.9 ± 6.7 | 17.9 ± 6.2 | 0.457 |
| ABG indicesa | Before NMES | After NMES | P value | ||
| Arterial blood pH | 7.43 ± 0.07 | 7.45 ± 0.06 | 0.468 | ||
| Lactate (mmol/L) | 1.68 ± 0.78 | 1.44 ± 0.60 | 0.242 | ||
| Biochemical parametersb | Before NMES | After NMES | P value | ||
| CPK (IU/L) | 327.5 (113.0-1234.5) | 257.5 (129.5-637.5) | 0.657 | ||
| AST-SGOT (IU/L) | 70.0 (32.0-118.8) | 57.5 (33.0-110.3) | 0.470 | ||
| ALT-SGPT (IU/L) | 50.0 (25.3-280.5) | 43.0 (23.8-136.3) | 0.006 | ||
| LDH (IU/L) | 488.0 (288.0-776.5) | 556.5 (321.5-756.8) | 0.972 | ||
ECMO, extracorporeal membrane oxygenation; BMI, body mass index; NMES, neuromuscular electrical stimulation; BP, blood pressure; SpO2, oxygen saturation; HR, heart rate; RR, respiratory rate; ABG, arterial blood gas; CPK, creatine phosphokinase; AST, aspartate aminotransferase; SGOT, serum glutamic-oxaloacetic transaminase; ALT, alanine aminotransferase; SGPT, serum glutamic-pyruvic transaminase; LDH, lactate dehydrogenase; SD, standard deviation. a Values are expressed as mean ± SD. b Values are expressed as median (25th-75th percentiles).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



