
Submitted:
18 May 2024
Posted:
21 May 2024
You are already at the latest version
Abstract
Background: Youth experiencing homelessness (YEH) in East Asia Pacific (EAP) represent one of the most at-risk populations due to cultural and geographical factors. Effective mental health interventions, primarily researched in Western contexts, may not fully apply to YEH in EAP. Their lack of stable shelter, disrupted social networks, and limited access to mental health services elevate their susceptibility to adverse mental health, making urgent interventions essential to address their needs. Objective: To explore and provide systematic evidence on the types of mental health services and interventions for YEH in EAP and their impact on overall quality of life and wellbeing. Methods: Electronic databases(e.g., Medline, PsychInfo, PubMed, Scopus) were systematically searched(publication dates between 01/01/1990-13/05/2023), as well as additional online resources specific to homelessness. Articles were screened, and a critical appraisal assessed the quality of the included studies. Results: Eight studies with different interventions were identified in Indonesia(n = 2), Malaysia(n = 1), South Korea(n = 3), and The Philippines(n = 1). These were thematically clustered into six categories: art, cognitive behavioural therapy, life skills education, resilience enhancement, family strengthening and government interventions/services. Conclusion: This review highlights effective mental health interventions’ positive impact on YEH mental health outcomes and quality of life in EAP, stressing the urgent need to implement socio-culturally sensitive services. Future research should address knowledge gaps through comprehensive studies covering diverse EAP regions and populations, prioritising socio-culturally specific psychological measures.
Keywords:
youth experiencing homelessness
; East Asia Pacific
; mental health interventions
; Cognitive Behavioural Therapy
; inclusion health
; resilience enhancement
; life skills education
; government programs
; emotional health
Introduction
- Background
Youth experiencing homelessness (YEH) is a serious global public health concern—they represent one of the most at-risk populations in many countries worldwide.[1] Globally, 1.6 billion people are estimated to experience some form of inadequate housing[2]; however, the true prevalence of homelessness is unknown.[3] In East Asia Pacific (EAP) regions, youth homelessness demands urgent attention. Although there is not a single unifying cause found to elucidate routes that lead youth into homelessness, poverty plays a significant role in exacerbating homelessness in EAP regions.[4,5] EAP suffers the most significant damage caused by natural hazards (e.g., earthquakes, tsunamis, tropical cyclones/typhoons)[6] that are often neglected by the state during recovery and rebuilding periods .[7] As such, economic inequality has been shown to exacerbate stress within families, which can manifest negative outcomes; these include selling or abandoning their children[5,8] or family dysfunction such as domestic violence and abuse which are considered major forces that push children and young people (CYP) to self-migrate, leave home, or run away,[9,10] and therefore, often left to fend for themselves.
YEH are at high risk for various adverse mental health outcomes.[1] They experience abuse and neglect, both prior to leaving home and while living on the streets (i.e., rough sleeping), that often lead to significant, long-lasting trauma.[11] For instance, high rates of depression, post-traumatic stress disorder (PTSD), substance abuse, suicidal ideation and bipolar disorder have been reported among YEH.[12,13] YEH are faced with multiple daily stressors associated with street life and often demonstrate a lack of coping strategies, resilience and essential social skills needed to sustain social support.[14,15,16,17,18] Therefore, they are likely to resort to maladaptive coping strategies[19] and decreased quality of life compared with the general population.[20] Notably, suicidality is the leading cause of death among YEH[21] and high rates of suicide attempts have been reported among this population (80%).[22] Furthermore, previous research documented that YEH were highly susceptible to becoming targets of sexual exploitation and prostitution,[23] even among sheltered youth.[24] While the mentioned studies were valuable in shedding light on the risks associated with YEH, they were all conducted in Western countries. This observation underscores a gap in the existing literature, which could potentially leave an incomplete understanding of the broader issue of homelessness and its associated risks in other parts of the world.
- Problems of defining ‘homelessness’
Defining ‘homelessness’ is complex: There is no internationally agreed definition as it plays out along a continuum.[1,3] Finding overall figures on YEH in EAP is extremely challenging given the different local and government definitions of homelessness from each country in this region, along with the absence of reliable data.[1,3] The most commonly used term to refer to YEH in academic literature and policymakers in EAP regions (e.g., China and Indonesia) is ‘street children’, defining those under age 18 years who live or work in public areas with little or no parental supervision.[25,26] ‘Runaway youths’ is another term used mainly in Korean literature,[27,28] along with ‘street sleeping’, ‘rough sleeping’ and ‘pavement dwelling’ to describe primary homelessness.[29,30] CYP experiencing secondary homelessness, defined by their lack of stable long-term housing, frequent between temporary accommodation such as shelters, orphanages, and refugee camps.[3,30] ‘Invisible homelessness’ is a phenomenon observed in many EAP countries, where young people couch-surf between friends’ homes, 24-hour cafés or fast-food restaurants due to cultural norms and societal pressures,[31] making their housing instability less visible but equally pressing.
Different government definitions of homelessness vary across border lines. For example, in Singapore, ‘homelessness’ is defined as “any person found begging in a public place in such a way as to cause or be likely to cause annoyance to persons frequenting the place or otherwise to create a nuisance”,[32] whereas in South Korea, it is defined as “persons who have used/lived homeless facilities for a substantial period”.[33] As highlighted by Rosenthal et al.(2021), the varying definitions of homelessness can have significant implications for the provision of mental health services depending on how it is recognised within a given jurisdiction,[34] and therefore, could act as a barrier to accessing mental health services. There is a lack of government policies that mention mental health services for this population based on those definitions[25] implying that mental health services are not adequately addressed by the government.
- Challenges of YEH in EAP and rationale for the review
YEH in EAP are a distinct population and influenced by a combination of cultural, socio-economic, and contextual factors. While both the West and East grapple with the challenges of youth homelessness, the unique dynamics of the EAP region amplify the importance of research in this area. For instance, cultural norms and values, along with rapid urbanisation and migration might contribute to different pathways into homelessness.[3,5] Barriers to accessing mental health services may differ from Western countries. Some examples were, but not limited to, low perceived need,[35] rural and financial constraints,[36,37] and a lack of mental health professionals and resources, who only practice in urban areas.[38,39,40] These factors can reinforce stigmatisation and marginalisation in countries where there is a strong societal stigma and shame already attached to homelessness.[41,42] The associated risks and effective mental health interventions aforementioned for this population were experiences of YEH in Western countries with Western therapeutic systems. These experiences and risks may differ for Asian adolescents experiencing homelessness living in EAP, as an extensive body of literature places emphasis on the different perceptions of mental illness cross-culturally,[43,44,45,46] which then can in turn influence both their receptiveness and adherence to treatment plans. Understanding these cross-cultural differences is crucial for mental health professionals to provide effective and culturally sensitive care for YEH, as it involves adapting treatment strategies that align with cultural norms[47] in EAP. Although several studies have evaluated the effectiveness of interventions for this population,[48,49,50] there is a lack of understanding of the different mental health interventions and programs for youth homelessness in EAP regions. Most systematic reviews and previous studies have focused on interventions conducted primarily in Western countries.[51,52,53] Yet, to date, there is a lack of comprehensive overview of literature surrounding interventions and programs for youth homelessness in EAP alone.
To address the research gap in international literature, the primary objective of this review was to provide systematic evidence on the different types of mental health services and interventions for YEH in EAP and their impact on overall quality of life and wellbeing for YEH. Thus, a scoping review[54,55] was selected to help map out the existing literature on this topic by gaining a comprehensive understanding of the current state of such services and interventions for YEH in the region. This review can hopefully provide valuable insights for future research, policy formulation, and program development that is tailored to this distinct and at-risk population, in order to improve quality of life and positive health outcomes for YEH in EAP regions.
2.Methods
This review followed the Centre for Evidence-Based Management (CEBMa) for Critically Appraised Topics guidelines[54] and PRISMA Extension for Scoping Reviews checklist[55] (Appendix A) to ensure that the review process was conducted in a comprehensive manner and to minimise potential researcher bias.[56] The research question was formulated using the PICO (population, intervention, comparison, and outcome) framework.[57] Table 1 presents the full inclusion and exclusion criteria with definitions.
Insert Table 1 Here.
- Databases and search strategy
The following major electronic databases were searched for this review: Medline, PsychInfo, PubMed, Scopus, and Web of Science. Additional records were hand-searched through other sources, such as web-based publications and grey literature specific to homelessness, reference lists of included texts and related publications. These included Centre for Homelessness Impact (CHI)[60]: A non-profit organisation dedicated to providing evidence-based solutions and innovations with the goal of improving the outcomes of people experiencing homelessness. The search was conducted on 13th May 2023 and was limited and filtered to English records published between 1990 and 2023 in all databases. Table 2 presents an example of search terms used for Medline, with slight variations employed in each database. See Appendix B for full search terms used in all academic databases. A prior search was conducted across official government websites to compare different definitions of homelessness within EAP and to inform the search terms used (Table 2; Appendix B).
Insert Table 2 Here.
- Screening process
Results were imported into EndNote 2.0 for screening and deduplication. An initial title and abstract screening was conducted. Full-text articles were then read and thoroughly evaluated to determine eligibility for inclusion in the systematic scoping review. Studies meeting the inclusion criteria were selected, and subsequent data extraction was carried out. Any conflicts were discussed between co-authors KCE and DMR until a consensus was reached. This is demonstrated in the PRISMA Flow diagram[61] in Figure 1.
- Analysis
A study quality assessment was performed using The Critical Appraisal Skills Programme (CASP) checklists[62,63,64,65] (see Appendix C for the CASP checklist that was matched and employed for each selected text and its study design). Each selected study was evaluated to assess its methodological robustness, validity, and relevance to the research question. Applicability to clinical practice and ability to generalise results were also assessed, which was crucial for this review. This ensured that the evaluated interventions and programs were relevant for addressing specific mental health needs of YEH. CASP[62,63,64,65] aims to inform evidence-based practice as generalisability helps identify interventions that have demonstrated its effectiveness across diverse settings for the target population.[66] Lastly, interventions/programs in the results were thematically grouped based on the type of interventions they encompassed.
3. Results
- Study selection
A total of 3,543 publications were identified from the literature search across all databases and through hand searching additional resources, which represented 3,467 publications after duplicates were removed and screened for eligibility. After the selection process, a total of eight studies published between 2000-2023 met the inclusion criteria and were included in this review. Fig. 1 is the PRISMA Flow diagram[61] showing individual database numbers and articles retrieved.
Insert Figure 1 Here.
- Study characteristics
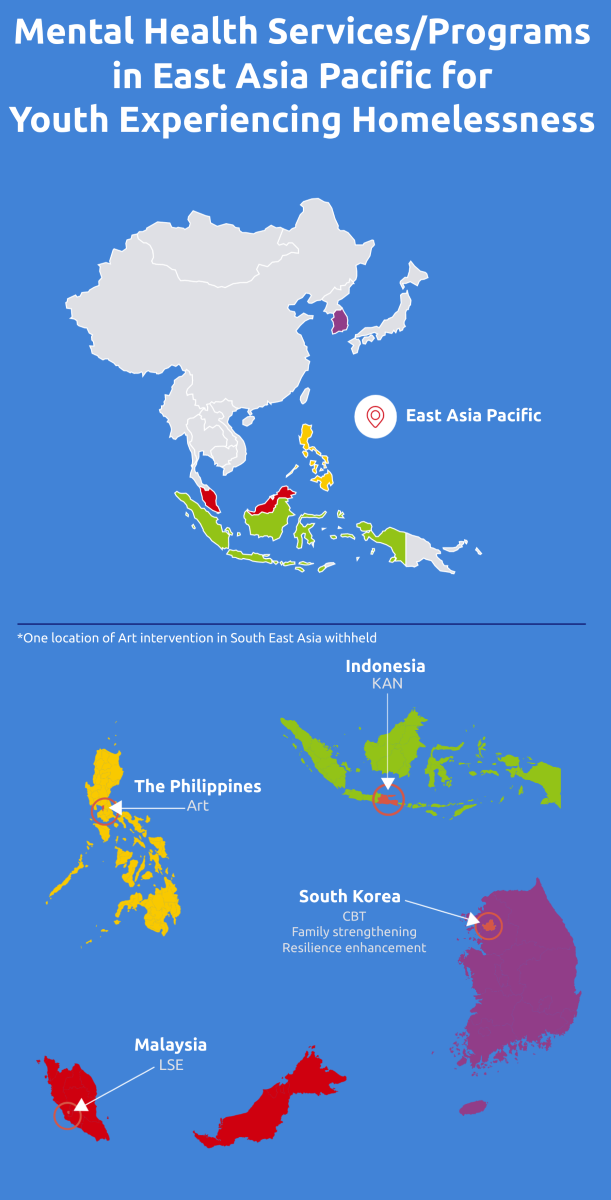
All included articles were conducted within the EAP region: Indonesia (n = 2),[67,68] Malaysia (n = 1),[69] South Korea (n = 3)[27,70,71], and The Philippines (n = 1).[72] The location of one study (n = 1) was withheld for confidentiality reasons, but, it was conducted in Southeast Asia[73] e.g., Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Thailand, and Vietnam,[74,75] indicating it still fit the inclusion criteria. Outreach settings for YEH primarily consisted of participants residing in orphanages (n = 8), shelters (n = 8), centres (n = 4), and children residing on the street (n = 2).
Participant characteristics
The age range of the participants varied across the studies, with the majority falling between the inclusion criteria age 12 to 18 yrs. (n = 4).[27,69,71],[72] However, a case study included participants as young as seven yrs. old,[67] with the oldest participants in another study being 21.[70] Both male and female participants were included in the studies; some studies focused exclusively on one gender to examine gender-specific effects of interventions for YEH[27,70] while others had a balanced representation of both genders.[69] A summary of the study and participant characteristics is reflected in Table 3. As the selected studies were conducted within the EAP regions, the studies encompassed a diverse range of participant ethnic and religious backgrounds, such as Christianity and Islam. In the Malaysian study,[69] there were different ethnicities included as participants, although they only reflected a small percentage. For example, a large percentage of participants in this study were of Malay ethnicity (67.5%), followed by Indian (21.8%), Chinese (4.8%), and Indonesian and Orang Asli [indigenous] (5.9%). Lastly, a large majority of participants across all eight studies belonged to families of low socioeconomic position (SEP). (Table 3).
Insert Table 3 Here.
Study designs
Of the eight studies, three involved some type of randomised-control trial (RCT) study design. One of these included a parallel single-blind (subject-masked) RCT[69]; one study had randomly assigned participants to either a control group or intervention group[27]; the other study was a development of an intervention program for YEH, with the aims of using an RCT to evaluate its effectiveness of the developed program.[71] Four studies used quasi-experimental and qualitative designs,[68,70,72,73] and the remaining one was a case study[67] (Table 3). Each selected study was subjected to quality checks using the CASP checklists[62,63,64,65] matched by study design (see Appendix C).
Outcome measures
A structured overview of measures and outcomes for each selected study is displayed in Table 4. Evidently, a range of outcome measures were utilised to evaluate various aspects of mental wellbeing and health status of YEH. For example, depression was measured with different scales across the studies: Brillantes-Evangelista[72] used the Self-Rating Depression Scale (SDS),[76,77] while Hyun et al.[27] and Mohammadzadeh et al.[69] used alternative scales to measure depression (Beck Depression Inventory [BDI] and Depression, Anxiety and Stress Scales [DASS-21]; respectively).[78,79] For specific outcome measures, the choice of instruments varied across studies which were usually translated into the country’s main language (Filipino, Malay, or Korean).
Insert Table 4 Here.
- Mental health interventions/programs
1. This review identified eight unique mental health programs and interventions for YEH in EAP. These were clustered thematically into six categories:
- cognitive behavioural therapy: an intervention that targets negative emotional states and cognitive distortions by developing coping strategies[27];
- life skills education: interventions that equip YEH with essential practical abilities in the real world[69];
- resilience enhancement: an intervention to improve protective factors associated with resilience[70];
- family strengthening: interventions that explicitly target families in the program as a key focus that fosters positive relationships and support networks[71];
Each selected study was organised by thematic category below and subjected to quality checks using the CASP checklists[62,63,64,65] matched by study design (see Appendix C).
Art Two studies used a quasi-experimental design to evaluate the effectiveness of different forms of art as a therapeutic intervention for abused youth in orphanages and militarised children in centres, which took place in the Philippines[72] and in Southeast Asia. [73] Art as an intervention for these studies included art psychotherapy, poetry psychotherapy and art without boundaries as a general communication and therapeutic tool.
The objectives of these studies were to evaluate the effectiveness of visual arts and poetry as interventions to alleviate depression and PTSD symptomatology,[72] as well as to understand the children’s perceptions of hope. [73] Although each study reported on different measures of art as an intervention, both studies reported themes of art creating a sense of agency, catharsis, and personal empowerment for YEH. In one study, Brillantes-Evangelista (2013)[72] measured PTSD and depression symptoms using various instruments (see Table 4), including self-reported scales and participant observation throughout the intervention period. Results showed a decrease of depressive symptoms in mean scores pre-test to post-test among the group receiving poetry psychotherapy, indicating a positive impact on their wellbeing (Table 4). Whereas a reduction of PTSD symptoms in mean scores was evident among the visual arts group, suggesting that this form of art therapy was beneficial for addressing trauma-related symptoms for YEH.[72] Brillantes-Evangelista[72] noted that although these results suggest that visual arts and poetry psychotherapy were effective in reducing psychological symptoms for abused adolescents living in orphanages, art seemed to have been helpful in other ways by empowering YEH to actively engage in their own healing and recovery. For instance, poetry allowed youth to find meaning and purpose in their experiences, by transforming hardships into something meaningful and artistic which can inspire hope. The notion of ‘hope’ was also noted in the second study[73] where militarised children had visualised their aspirations, dreams, and personal goals through art. Miles (2000)[73] concluded that despite their circumstances, art had allowed them to envision a positive future and work towards achieving it, instilling hope for a better tomorrow.
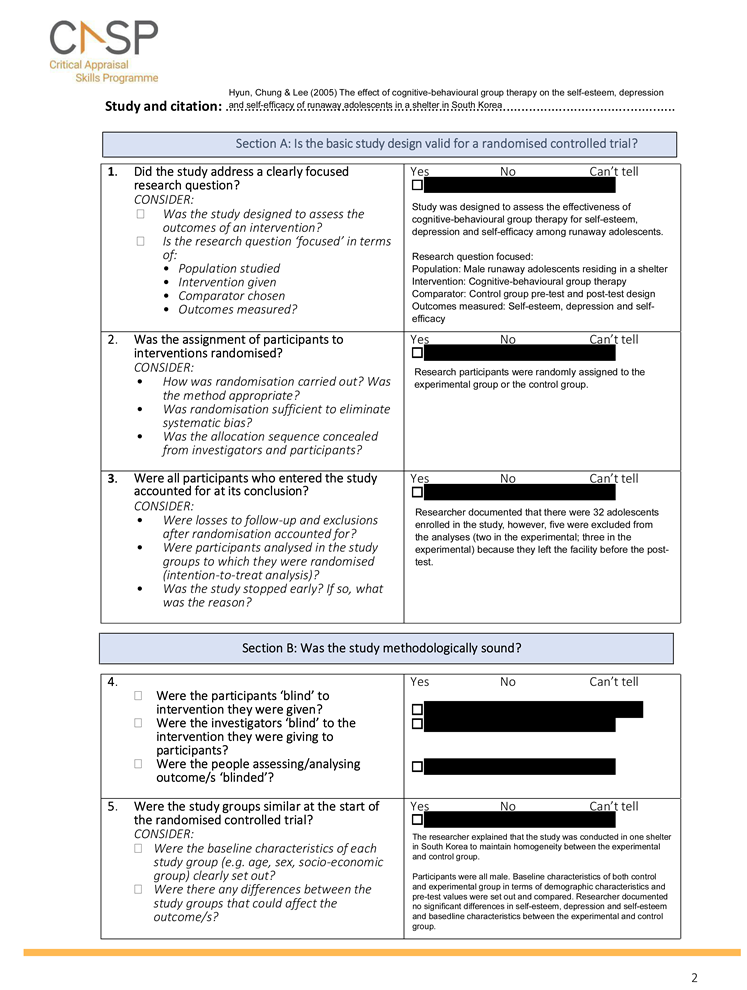
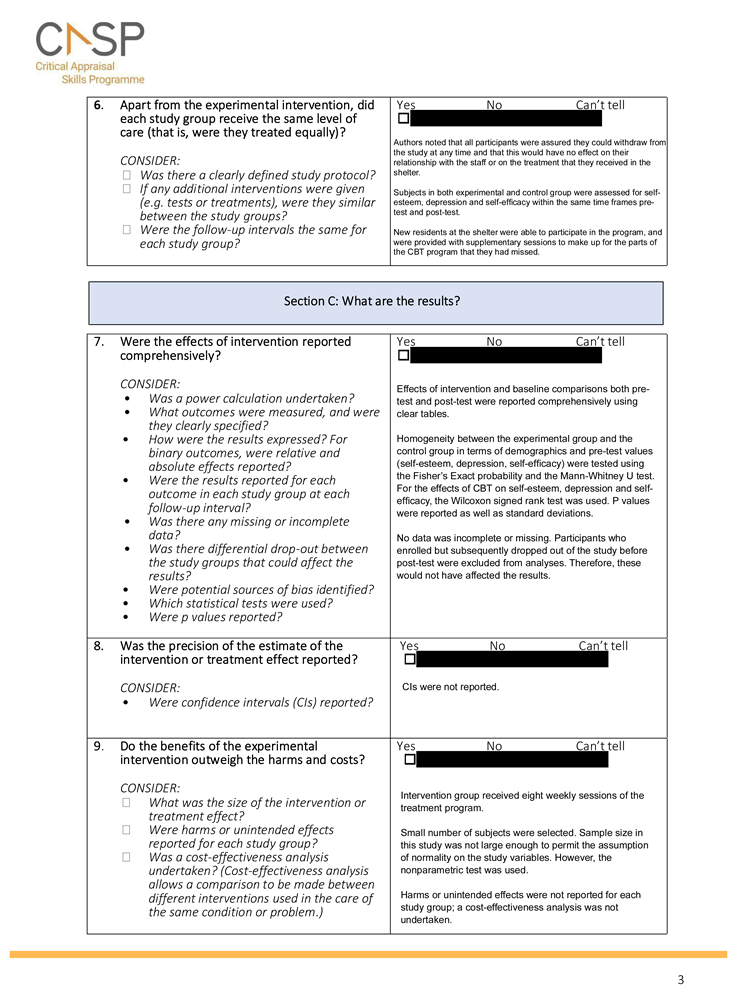
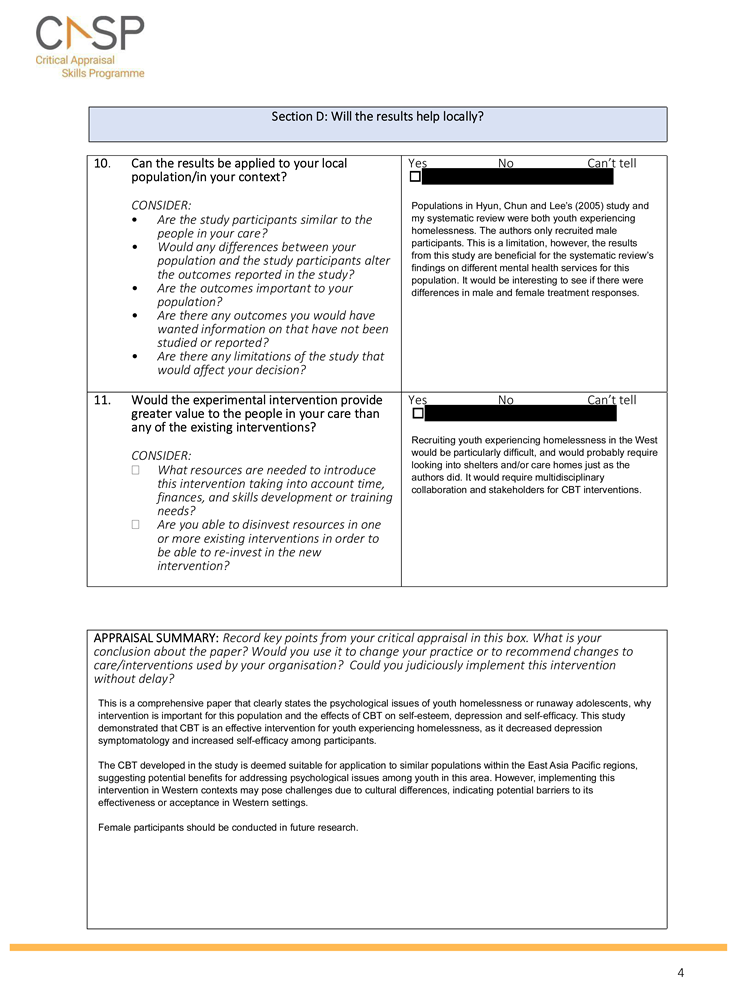
CBT One RCT study conducted by Hyun, Chung and Lee (2005) in South Korea evaluated the effects of group CBT on self-esteem, depression and self-efficacy of runaway adolescents residing in shelters.[27] The authors measured these using Western-derived scales (Table 4) that were translated into Korean and employed at pre- and post-test. In this study, the most common reason for running away was parental abuse, especially by their father (40.7%), and family conflict (29.6%). There were also high rates of reported problem drinking (66.7%) and smoking (77.8%) among YEH. Results demonstrated a reduction in depression and improved self-efficacy in the experimental group from pre-test to post-test, while there were no significant changes in self-esteem documented pre- and post-test for both experimental and control groups (see Table 4). However, the authors revealed that an eight-week intervention period may be too short to yield noticeable results to self-esteem.[27] The study’s RCT design and use of validated measures (e.g., BDI[78]; Table 4) enhanced the reliability of the study’s findings (CASP[64]; Appendix C).[62] However, the geographical limitations should be considered when applying the results to YEH populations in different regions in EAP (see Table 5 for the full strengths and limitations of each study).
Insert Table 5 Here.
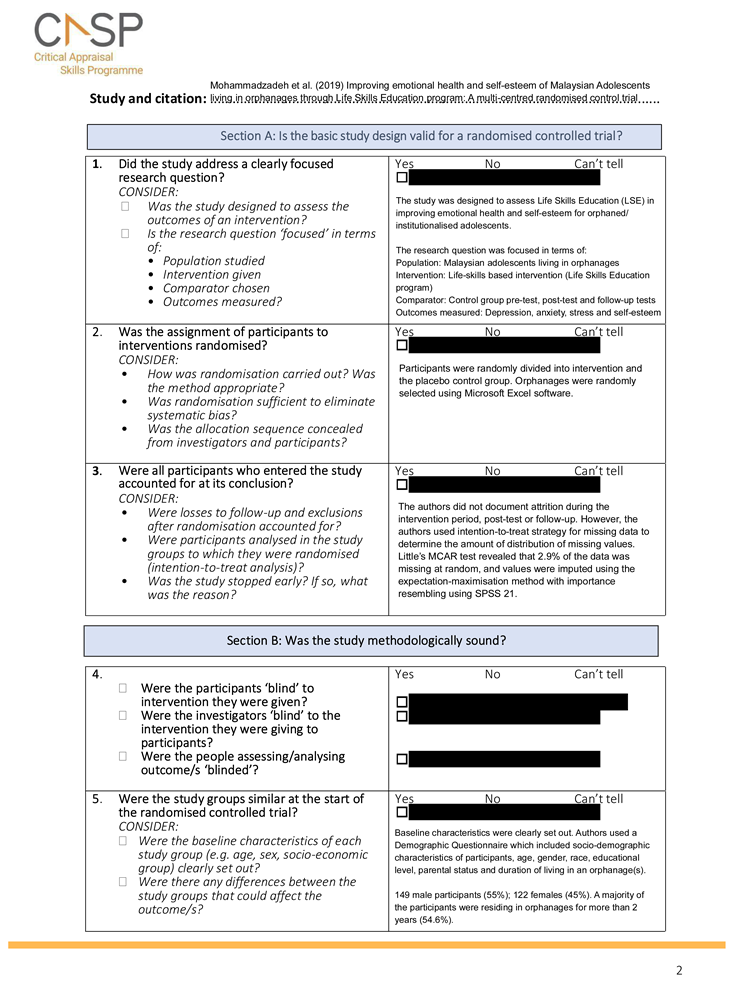
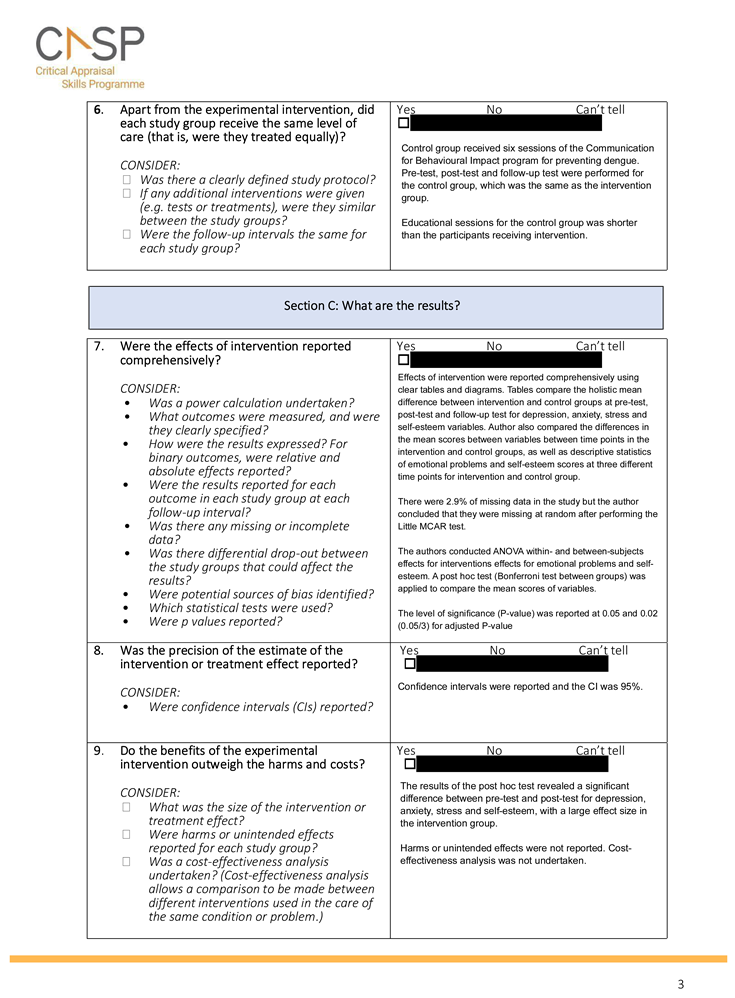
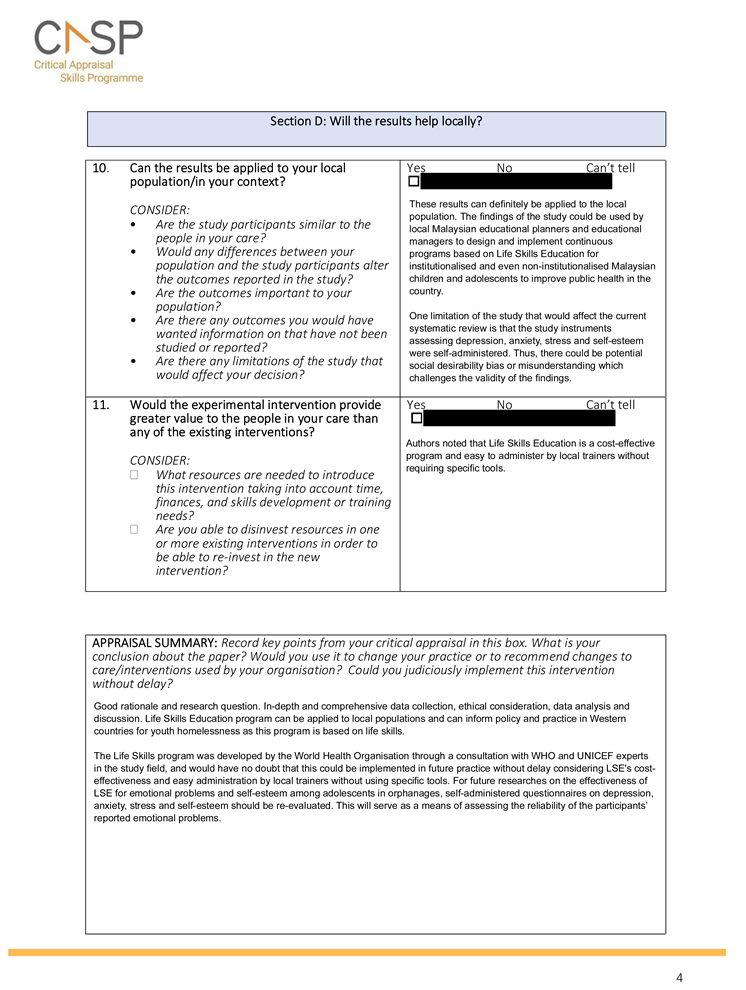
Life skills education Mohammadzadeh et al. (2017)[69] conducted a parallel single-blind (subject-masked) RCT conducted in Malaysia which evaluated the effects of life skills-based intervention programs on the emotional health and self-esteem of adolescents residing in orphanages.[69] This program was designed based on the Life Skills Education (LSE) formulated by the World Health Organisation (WHO)[96]— a structured evidence-based guideline for children and adolescents, stemming from the stress-coping theory by Lazarus and Folkman.[97] The LSE framework was a valuable resource for YEH, as it equipped them with essential skills and abilities to effectively navigate challenges they experienced in everyday life, promoting personal growth and resilience.[96] The study’s intervention sessions focused on a range of life skills: self-awareness, critical and creative thinking, communication, intra- and interpersonal relationships, problem solving, decision making, empathy, and coping with emotion and stress. Outcomes were assessed using DASS-21[79] and a Malay version of Rosenberg’s[86] Self-esteem Scale (RSES)[87] at pre-test, post-test and at a four-month follow-up (F/U). Results revealed that the LSE program significantly decreased mean scores for anxiety, depression and stress, and increased self-esteem from pre-test to post-test for participants receiving intervention. Notably, there was an increase of depression scores from post-test to the four-month F/U implying that LSE demonstrated efficacy in addressing depression, yet its impact was insufficient for sustainable change beyond the four-month period (Table 4). These findings[69] could have high potential for research in different regions in EAP because of its good replicability and RCT design, especially because this study had a diverse range of ethnicities. However, an important consideration was that the intervention period was not specified (Table 5).
Resilience enhancement A study on Korean female runaway adolescents by Noh (2018) assessed the efficacy of a Resilience Enhancement Program using a quasi-experimental design.[70] This design was appropriate based on ethical considerations and real-world settings, as it allowed the researcher to observe the program in an orphanage without compromising ethical guidelines or manipulating variables (CASP[64]; Appendix C). The Resilience Enhancement Program was developed based on interviews with female runaway adolescents residing in shelters and a comprehensive review of literature focused on individual protective factors relevant to YEH and runaway adolescents. Resilience, depression, anxiety, and problem drinking were assessed using self-reported questionnaires (Table 4) at pre-test, post-test, and at a one-month F/U. While the intervention group exhibited notable reductions in depression at pre-test and at a one-month F/U, this decrease was not exclusive to the overall study period: Depressive symptoms decreased over the study duration for both the intervention and control groups. Reductions of anxiety levels were also observed in the intervention group compared with control; and interestingly, the control group experienced a rise in anxiety levels at the one-month F/U.[70] In terms of problem drinking, the average levels decreased consistently for the intervention group throughout the three time points (Table 4). Although these were preliminary results, the small p-value suggested that the program had an effect on the dependant variables that was unlikely to occur by random chance alone.[70]
Family strengthening Noh and Choi (2020) developed a family-based mental health program for runaway adolescents residing in youth shelters using an intervention mapping (IM) protocol.[71] Despite its efficacy and effectiveness not yet being evaluated, this program focused on family strengthening that aligned with Korean cultural values that shaped their context. It was developed by conducting a comprehensive literature review and interviews with runaway adolescents and shelter workers. A logical framework outlining family relationship and mental health issues faced by runaway adolescents was then developed based on the problems that were identified during the preliminary IM process. The program used theory- and evidence-based methods for practical applications such as motivational interviewing, cognitive reappraisal, consciousness-raising, skills training, guided practice, social modelling, improving emotional states and verbal persuasion. Runaway adolescents receiving the intervention will have a total of eight individual and family sessions altogether. The family sessions consisted of four themes: family engagement and establishing motivation for change, rebuilding relationships with family, improving family communication and improving collaborative problem-solving. The effectiveness of the developed program will be evaluated using a RCT on adolescents residing in shelters aged 12 to 18.[71] Data will be collected using self-reported questionnaires.
The developed family-based mental health program has high study potential for YEH specific to the EAP context. However, to date, this program has not been tested for its efficacy and effectiveness and might not yield the positive health outcomes expected from the authors.
Government interventions/services The following two papers[67,68] focused on government interventions/programs and/or policies regarding mental health of YEH, thereby met the inclusion criteria (Table 1).
One research case study paper addressed the policies implemented by the Makassar City Regional in Indonesia in managing street children by collecting primary data (field observations and key informants) and secondary data (official government documents and literature publications on street children).[68] They identified three social services implemented by the Makassar City Regional in managing street children (Table 6).
Insert Table 6 Here
Despite these service policies, Solong et al.(2023) [68] identified factors inhibiting government policy in managing street children. These included insufficient quantity of human resources, budget limitations, insufficient facilities and infrastructure, unstable community economy and a lack of strict implementations for regional regulations regarding the management of street children. In spite of that, initial steps have been carried out by the government to prevent the development and expansion of street children. These included collaboration with Civil Service Police Units to patrol street children’s activities and/or removing them from street environment and into police stations so that they can be then placed into orphanages. [68]
The Kampung Anak Negeri (KAN) was a children’s village established by the Surabaya City Government in Indonesia that protected the rights of street children, aiming to empower street children, with the goal of granting them agency to enhance their self-resilience to deter them from returning to the street. Sarmini and Sukartiningsih (2018) evaluated the role of the KAN in facilitating the transition of street children towards a regular life.[67] Data was gathered by participatory observation and in-depth interviews with the street children placed in the KAN. The KAN established by the Surabaya City Government had six roles and responsibilities.[67] These responsibilities were described in Table 7.
Insert Table 7 Here.
Overall, KAN served as a comprehensive support system for street children that respects and integrates Indonesian culture into its program, aiming to improve mental health outcomes and ultimately break the cycle of street life and create a better future for themselves.[67]
4. Discussion
The main objective of this review was to provide systematic evidence on the different types of mental health services and interventions for YEH in EAP and their impact on overall quality of life and wellbeing for YEH. A wide variety of mental health interventions and programs for YEH in EAP was identified. These included art and poetry psychotherapy for abused Filipino adolescents living in shelters,[72] art without boundaries for militarised children,[73] CBT for runaway Korean adolescents,[27] a life skills education program for Malaysian adolescents living in orphanages,[69] a resilience enhancement program for female runaway Korean adolescents[70] and development of a family-based mental health program for runaway adolescents.[71] In essence, these mental health interventions and programs were effective in alleviating symptoms of anxiety, depression, stress, and PTSD, as well as targeting problem drinking. Additionally, there were notable increases in overall resilience and self-efficacy for YEH in EAP, and they were taught various life skills to tackle any daily stressors they may experience.
Notably, there were only two programs and social services found in this review that were established and implemented by the government that targeted street children.[67,68] While the researchers did not directly assess the outcomes of these services, their reports underscored the importance of creating culturally sensitive programs empowering and improving the quality of life for YEH in Indonesia, as well as identifying factors inhibiting the effective implementation of government policies aimed at addressing the needs and challenges faced by street children.[67,68]
Prior to this review, most systematic reviews and previous studies had mainly focused on interventions conducted in Western countries. Furthermore, there was a lack of comprehensive overview of literature surrounding interventions and programs for YEH in EAP alone, although there was an extensive body of literature emphasising the different perceptions of mental illness cross-culturally, which may impact the acceptability of treatment options and adherence to treatment plans.[43] In this review, risks associated with youth homelessness in EAP, such as stress, maladaptive behaviour, and suicidal behaviours were reportedly similar compared to Western countries (e.g., Hyun et al. [27]; Moskowitz et al. [19]; respectively). Additionally, consistent with findings from Western literature,[11,13] baseline assessments also revealed high levels of adverse mental health outcomes in various studies conducted in EAP.[27,69,70],[72] Nonetheless, Western-developed therapeutic systems such as CBT and LSE were also found to be effective in alleviating symptoms in Korean and Malay adolescents.[27,69]
Having said that, it is essential to highlight that these instruments and measures were socio-cultural specific which could have influenced the efficacy and effectiveness in treatment response. For example, five studies translated the measures into the country’s main language.[27,69,70],[72,73] Translating the psychological instruments into the country’s language was crucial, given the nature of the targeted population for this review. YEH may have limited proficiency in the English language, especially if most of the participants belong to families of low SEP and were residing in orphanages, shelters or on the street and have not completed or received formal education.[27,67,68,69,70,71,72,73] Although this was not specified in the studies, YEH with limited education may lead to feelings of discomfort or shame when responding to instruments in a language they were unfamiliar with. Therefore, using their first language may have reduced stigma and encouraged them to share their experiences openly, promoting accessibility and inclusivity in the research process for this population.[98]
- Exploring mental health interventions and programs
Six key themes were identified among the eight included studies: art, CBT, LSE, resilience enhancement, family strengthening, and government interventions/services.
- Art
Art-based interventions utilise creative mediums that do not primarily rely on spoken language to convey emotions, thoughts and experiences.[99] This has been well documented in numerous past and recent Western literature with adolescents in bridging that gap between therapists and adolescents.[100,101] It uses a child-centred approach.[102] As demonstrated in a sample of militarised children in SE Asia,[73] it broke down communication barriers and acts as a facilitator between the researcher and the CYP.[73] This was especially beneficial for YEH, as art can be used as a tool to amplify their voices in a society where it is marginalised and unheard.[99] This, in turn, may reduce the overall stigma surrounding homelessness, shifting the focus from defining youth homelessness solely by their housing status to appreciating their artistic talents and creativity; it helps people see their multifaceted identities beyond homelessness as shown in The Philippines.[72] Yet, it is important to note these findings may not be generalised to youth who have learning disabilities (LDs) and/or cognitive difficulties in engaging in complex art or poetry activities. Even so, with tailored interventions and adaptations, art and poetry psychotherapy can minimise barriers and promote autonomy, which empowers YEH with LDs to enhance their self-expression and build confidence, wherein traditional therapeutic approaches can lack.[103]
- CBT
Findings from South Korea[27] have been reported in previous literature by Rohde et al. [104] for adolescents with comorbid substance abuse and in parallel with more recent findings for street children in Mexico City[105] and in Iran[106]. The effectiveness of cognitive techniques in CBT for reconstructing positive worldviews was notable as it identified and challenged negative thought patterns.[107] Importantly, the two themes in Hyun et al.’s study ‘developing coping strategies’ and ‘planning for future life’,[27] equipped runaway youths with practical coping skills suited to their circumstance. For example, it encouraged them with long-term thinking beyond immediate survival needs, thus promoting a sense of direction and pathways to stability such as housing, employment, and education. Additionally, improved self-efficacy, indicated by the theme ‘raising self-consciousness', aligned with Bandura’s[108] model of self-efficacy. In the context of homelessness, this model postulated that with the appropriate training, runaway adolescents can interpret emotional and physical reactions (e.g., anxiety and stress) as signs of competency which increased their overall self-efficacy evident in this study.[108]
Although results from this study demonstrated that CBT had no effect on self-esteem, this has been challenged by a recent meta-analysis that found CBT-based interventions to be efficacious for treating low self-esteem.[109] Yet, these findings may not be generalisable to Korean adolescents, as it was conducted on adults in the UK, where self-esteem is prioritised in Western cultures.[110] In contrast, self-esteem is conceptualised differently as shown elsewhere in the East among a more comparable sample of Chinese children.[111] Self-esteem is multifaceted and complex, influenced by a myriad of internal and external factors; it could simply be that the intervention period of eight weeks was too short to yield a noticeable impact on self-esteem.[27] Short intervention periods may not adequately address cultural nuances and beliefs that impact how self-esteem is perceived and influenced in Korean runaway adolescents.[43] Additionally, it should be highlighted that the subjects of this study were all male, and there could be potential gender disparities in self-efficacy, depression and self-esteem presentations and responsiveness to CBT.[27] Thus, future research could benefit in this area by exploring the long-term effects of cultural-specific and extended interventions to develop more comprehensive and effective interventions that address unique challenges for this vulnerable population.
- LSE
LSE for depressive symptoms was found insufficient for sustainable change.[69] This observation could be attributed to the inherent characteristics of youth homelessness. The lack of continued support that they had received during the intervention period may lead to a resurgence of depressive symptoms, given that depression is a highly recurrent disorder.[112] In other words, if the adolescent returned to the same challenging or unstable living conditions or environment after the intervention, the stressors associated with homelessness could be precipitating factors for the re-emergence of depressive symptoms. It appeared LSE had a more sustainable effect on anxiety, stress, and self-esteem.[69] Comparable outcomes have been observed in previous studies among Indian adolescents[113] and more recently in Indonesian students.[114]
In contrast, LSE illustrated positive effects on self-esteem and resilience for YEH living in orphanages.[69] This phenomenon could be explained by the intricate interplay between life skills development and positive feelings of self-worth. Learning and mastering certain life skills can contribute to a positive self-perception and higher self-esteem from feelings of accomplishment,[115] and conversely, having positive self-worth can motivate them to develop and practice their life skills.[113] As YEH develop practical skills, their self-worth and confidence are likely to improve and in turn can motivate them to further enhance their life skills and actively engage in efforts to overcome their challenges. Ultimately, this positive cycle can empower this population by equipping them with valuable tools and a stronger sense of self, fostering resilience and assisting their journey towards stability and self-sufficiency.
- Resilience enhancement
Resilient enhancement programs[70] offered significant advantages for runaway adolescents, as these can positively influence mental wellbeing, and appeared promising for enhancing resilience and mitigating problem drinking. Factors associated with resilience such as self-esteem and self-regulation, have been well documented in previous literature with Korean adults[18,116]; while relational and problem-solving skills[117] and goal-setting skills[118] have been considered as protective factors for runaway adolescents. Since the intervention program used in Noh’s study[70] integrated the abovementioned protective factors linked to resilience, these elements were believed to have contributed to the observed increase in resilience among participants in the intervention group.[70]
In terms of explaining reduced anxiety, Noh’s study[70] had provided progressive relaxation training and deep breathing techniques that counteracted physiological responses to stress.[119] These equipped YEH with immediate skills to manage moments of crisis and distress which therefore increased their overall resilience.[120] The issue of youth homelessness is often interconnected with the challenge of problem drinking in both the East and the West, as YEH may resort to alcohol as a coping mechanism to navigate the hardships and uncertainties they encounter on the streets.[121,122] The current finding of decreased problem drinking was consistent with previous findings in the UK by Rew et al. [123]; both Noh[70] and Rew et al. [123] included components assertive and effective communication, as well as goal-setting skills in their interventions, which are recognised as protective factors in building resilience. In essence, resilience enhancement programs hold the promise of catalysing positive transformation in the lives of female runaway adolescents by fostering their growth.[70]
- Family strengthening
The role of family in addressing runaway behaviour is important as it holds paramount importance in not only Korean culture, but many EAP cultures.[71] Although psychological interventions for youth homelessness have been evaluated in previous Western studies, the authors suggested that these interventions do not reflect the actual situation Korean runaway adolescents experience.[71] Thus, the family-based mental health program Noh and Choi[71] developed aimed to improve mental health outcomes for this at-risk population using socio-cultural contexts. During their literature review, the authors identified that runaway adolescents experience high rates of dissatisfaction with family life.[124] Additionally, family factors such as poor communication and emotional support at home, financial problems, and poor psychological well-being of the parent or caregiver[125] can affect mental health and their quality of life. As a result, the runaway adolescents who participated in the interviews revealed they were more likely to engage in risky and maladaptive behaviours as a response to stress from family problems.[125] These issues identified have been supported by a range of parent—child theories. For example, the parental monitoring theory[126] emphasised the importance of parental supervision and awareness of adolescent’ activities. If the runaway adolescent experienced a lack of parental warmth because of their poor communication and emotional support, they were more likely to be involved in risky behaviour associated with homelessness/running away. As the developed program recognised the cultural significance of family in Korean society, it emphasised the importance of re-establishing strong family connections to deter adolescents from engaging in runaway behaviour.[71] Ultimately, the parent—child collaboration aligned with the cultural fabric of Korean society and aimed to create a nurturing environment where adolescents feel supported and understood without resorting to running away. Understanding the parent—child dynamic can offer valuable insights for other EAP societies facing similar challenges. It underscores the significance of familial bonds, open communication, and community support structures to provide a safety net for YEH. This emphasises a proactive intervention in addressing root causes of youth homelessness, offering effective strategies that prioritise prevention and holistic support.
- Government interventions/services
Interestingly, while both EAP and Western countries aim to address youth homelessness, there are notable differences in their government interventions/services due to varying cultural, social, and economic contexts. For example, while Western programs often emphasise individual autonomy and direct service provision,[127] government interventions/services in EAP regions may place greater emphasis on familial or community support networks that implement spiritual values.[67] Moreover, there exists a more established network of government-funded health and wellbeing services in the West, encompassing mental health and substance abuse counselling.[128] In contrast, the selected studies in this review revealed that access to healthcare services in EAP regions were more limited, with fewer specialised services for YEH provided by the government. In summary, tailoring support specific to sociocultural contexts is crucial for effectively addressing the unique needs of YEH and future efforts should focus on bridging these gaps to ensure equitable access to comprehensive support services for this vulnerable population in EAP.
- Limitations
To the best of our knowledge, there have been no previous systematic or scoping reviews on the different types of mental health services and interventions for YEH in EAP and their impact on overall quality of life and wellbeing for YEH. Despite finding positive mental health outcomes for YEH resulting from these psychological interventions and programs, there were several limitations of this review that should be noted. First, one of the primary objectives of this review was to identify different mental health interventions and programs for youth homelessness in EAP. According to The World Bank,[58,59] there are 15 countries within EAP, and yet, this review only found evidence of effective interventions and government programs in four named countries (i.e., Indonesia, Malaysia, South Korea, The Philippines) with the majority being conducted in South Korea (n = 3). Importantly, seven (87.5%) of the reviewed studies were conducted in urban areas or in the capital city which might not be reflective of the broader population. Homelessness patterns might differ significantly between urban and rural settings. Factors contributing to homelessness, available resources, programs or interventions, and support networks can be different in various parts of a country, especially if many of the EAP cultures rely on traditional folk medicine and healers.[129]
Second, subpopulations of youth homelessness, such as LGBTQ+ or indigenous youth, might be more prevalent in certain regions or outside the capital city. Focusing solely on urban areas could also neglect the unique challenges faced by these groups. Additionally, the only variation of ‘homelessness’ that was not included in this review was ‘invisible homelessness’ as there was no existing literature that met this review’s inclusion criteria. Third, differential definitions of homelessness used by the studies and the data that were collected do not make them comparable. However, considering shared characteristics and successes of similar programs in both Western and Eastern countries, this might not have been a significant factor contributing to the effectiveness of Western therapies suggesting that tailoring and adaption could enhance their efficacy. The differences in age of YEH and sampling may have affected comparability and generalisability as some YEH were mixed with higher age groups and some studies only reported the mean age for the sample. Therefore, these settings and groups may not be comparable.
Despite these limitations, a notable aspect where this review excels was that it was not limited to one study design and high-quality methodologies (e.g., RCTs, quasi-experimental design), but it also included case studies for in-depth qualitative data, enabling a more comprehensive and nuanced understanding of youth homelessness in EAP regions. Additionally, six papers (75%) out of the eight selected for this review were all conducted and published relatively recently, ensuring that the findings provided were accurate and relevant to the current mental health interventions, policies, and outcomes for YEH in EAP.
- Implications for future research, policy, and practice
The findings of this review suggest that different mental health interventions and programs have positive impacts on overall mental health outcomes and quality of life for YEH. Despite that, a large gap of robust evidence-based research in the EAP region is still evident. Future research should prioritise filling these substantial knowledge gaps by conducting comprehensive studies that encompass various EAP regions and diverse populations like YEH. There should be a pressing need to engage in co-designing research and programs with YEH to authentically incorporate lived experience voices. For example, two included studies in this review effectively integrated YEH voices,[70,71] underscoring the importance of this approach in comprehending cultural nuances. This inclusive methodology fosters a deeper understanding of the diverse challenges faced by YEH and can enhance the relevance and effectiveness of interventions or programs aimed at supporting them.
Importantly, researchers should strive for inclusive sampling that covers urban, suburban, and rural areas to provide a holistic understanding of unique challenges faced by YEH in different settings. Providing robust research across different EAP regions could provide comparative studies that highlight disparities, commonalities, and explanations for the different pathways that lead to homelessness. This holds particular significance in EAP regions for youth homelessness when contrasted with Western studies, as it helps avoid making assumptions and generalisations that might not hold true across cultural boundaries. For instance, many of the comparative studies were compared with Western studies (such as Bandura et al. [124]; Kolubinski et al.)[109] that do not underpin cultural nuances and local dynamics such as family structures and social norms that are important EAP cultures.[71] Mixed-method studies may be useful for exploring this by combining qualitative and quantitative research techniques to understand the corresponding data while checking the validity of statistical findings.[130] In addition, although some type of RCT study design was used in three studies, there were various limitations, e.g., the intervention period was not specified,[69,70,72] too short[27,72] or yet to be conducted.[71] Robust longitudinal analysis should also be implemented to track current situations and identify trends and changes.
Subpopulations such as LGBTQ+ youth who experience homelessness, also presents a critical avenue for gaining insights into the intersection of cultural and identity dynamics in EAP regions, particularly if these dynamics contribute to pathways to homelessness. This subgroup is a very at-risk population in both the West[131] and the East[132] signifying an urgency for research. For example, Confucianism is deeply ingrained in some EAP societies that can shape perceptions of family, community, gender,[133] and perhaps even perceptions of homelessness. From a political perspective, LGBTQ+ youths represent the most fastest growing demographic within South Korea’s homeless populations.[134] They face exclusion from certain homeless shelters, thus being deprived of human rights protections and social benefits.[134] Future research working with this subgroup of youth homelessness could identify the potential multi-level barriers these youth encounter when seeking assistance. Not only will it contribute to a more comprehensive understanding of lived experiences of LGBTQ+ youth who experience homelessness, but it could also reduce marginalisation for an already marginalised group in a society where homelessness is heavily stigmatised.[41,42]
The scarcity of published literature (such as government services/programs) concerning the management and policies for youth homelessness in EAP underscores the significance gap in addressing this issue. The lack of documented programs reflects a limited institutional response to the challenges faced by this at-risk population, possibly resulting from varying levels of awareness, available resources, and prioritisation.[68] Nonetheless, the findings of positive mental health, health outcomes and quality of life from mental health interventions and programs for YEH in EAP provide valuable insight for policymakers, which has global relevance to ensure that the Sustainable Development Goals[135] are met for 2030. For instance, evidence-based policies can be developed that are rooted in the specific lived experiences and realities of EAP regions. These could potentially include root causes of youth homelessness, such as family conflict,[27] or economic factors such as being at risk of homelessness.[68] Thus, addressing these potential root causes can allow for a prioritisation of preventative measures.
Lastly, this review emphasises the importance of implementing culturally sensitive services adaptable to the diverse cultural contexts within EAP, such as translating psychological instruments and measures into the country’s language,[27,69,70],[72,73] or understanding religious values that are deeply rooted in EAP societies.[67,68] Some implications for practice should highlight the importance of collaborative learning for practitioners dealing with YEH. This fosters a more comprehensive approach to acknowledging the multifaceted challenges these youth experience, which can, in turn enhance, the quality and impact of interventions for this population.
Conclusion
Despite the positive mental health outcomes found in this review, a lack of established evidence-based interventions/programs and the existing research gap in EAP underscores the urgent need for comprehensive efforts. A strength of the review lies in its emphasis on tailoring and adapting interventions and programs to suit the socio-cultural contexts of EAP regions, and this review demonstrates its potential to inform future interventions and policy decisions. Tailoring and adapting interventions and programs for socio-cultural contexts can also pave the way for improved services and holistic solutions that address the multifaceted challenges faced by these vulnerable populations. In conclusion, while small steps have been made towards devising effective interventions, programs, and policies, it is evident that there is still significant progress to be made.
Supplementary Materials
Table S1: Definitions, inclusion, and exclusion criteria.; Table S2: Example search terms. Search terms used for Medline.; Figure S1: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers, and other sources.; Table S3: Summary of study characteristics.; Table S4: Mental health services/programs and outcomes for youth experiencing homelessness.; Table S5: Strengths and limitations of each paper.; Table S6: Three services implemented by the Makassar City Regional.; Table S7: Responsibilities of the KAN.; Appendices S1: Appendix A, Appendix B, Appendix C.
Author Contributions
Conceptualization, K.C.E. and D.M.R.; Methodology, K.C.E. and D.M.R.; Validation, K.C.E. and D.M.R.; Formal Analysis, K.C.E.; Investigation, K.C.E.; Resources, D.M.R.; Writing – Original Draft Preparation, K.C.E.; Writing – Review & Editing, K.C.E. and D.M.R.; Visualization, K.C.E.; Supervision, D.M.R.
Funding
This research received no funding.
Acknowledgements
There are no acknowledgements.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist
| SECTION | ITEM | PRISMA-ScR CHECKLIST ITEM | REPORTED ON PAGE # |
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 4–5 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 5 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | 5 |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 5 |
| Information sources* | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 5–6 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | 6 |
| Selection of sources of evidence† | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 6 |
| Data charting process‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 6 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 8 |
| Critical appraisal of individual sources of evidence§ | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | 6 |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 7 |
| RESULTS | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 7–8 (Table 3) |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 8 (Table 4) |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | 6–11 (Appendix C) |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 8 (Table 4) |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 8–12 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 12–13 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 17 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 18–19 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 20 |
| JBI = Joanna Briggs Institute; PRISMA-ScR = Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. * Where sources of evidence (see second footnote) are compiled from, such as bibliographic databases, social media platforms, and Web sites. † A more inclusive/heterogeneous term used to account for the different types of evidence or data sources (e.g., quantitative and/or qualitative research, expert opinion, and policy documents) that may be eligible in a scoping review as opposed to only studies. This is not to be confused with information sources (see first footnote). ‡ The frameworks by Arksey and O’Malley (6) and Levac and colleagues (7) and the JBI guidance (4, 5) refer to the process of data extraction in a scoping review as data charting. § The process of systematically examining research evidence to assess its validity, results, and relevance before using it to inform a decision. This term is used for items 12 and 19 instead of "risk of bias" (which is more applicable to systematic reviews of interventions) to include and acknowledge the various sources of evidence that may be used in a scoping review (e.g., quantitative and/or qualitative research, expert opinion, and policy document). From: Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann Intern Med. 2018;169:467–473. | |||
Appendix B
Search terms used
Medline
| Category | Search terms |
| YEH | ((homeless* and (child* or youth* or adolescen* or teen* or young person* or young people*)) or street child* or street sleep* or "homeless* youth" or ill-housed person* or rough sleeper* or railway boy* or street dweller* or refugee*) (Homeless persons or Homelessness or Homeless family or Homeless Shelters or Homeless Youth or Homeless single person or "outreach to the homeless" or homeless mentally ill or homeless shelter resident or Homeless Health Concerns) (Runaways or Runaway children or Street Youth) |
|
AND |
|
| Mental health intervention | (mental health service* or therapeutic support* or counselling or counseling or housing program* or temporary shelter* or homeless shelter* or psychological counseling or psychological counselling or short-term temporary care or short-term care or youth homeless* shelter or non government* organisation* or non government* organization* or non-government* organisation* or non-government* organization* or NGO* or mental health care or mental health support* or cognitive behavioural therap* or cognitive behavioral therap* or CBT* or substance abuse therap* or outreach program* or outreach support* or mental health intervention* or mental health* or life counseling or life counselling or overcrowded or refugee* or emergency accommodation* or homeless* facilit* or rehabilitation* or prevention approach* or social work* or therap*) Mental Health Services/ or Child Guidance/ or Community Mental Health Services/ or Counseling/ or Emergency Services, Psychiatric/ or Social Work, Psychiatric/ (health service, mental or health services, mental or hygiene service, mental or hygiene services, mental or mental health service or mental health services or mental hygiene service or mental hygiene services or service, mental health or service, mental hygiene or services, mental health or services, mental hygiene) |
|
AND |
|
| EAP countries | (east asia* pacific or east asia* pacific countr* or cambodia* or china or chinese* or hong kong or indonesia* or japan* or south korea* or lao* pdr or macau or macanese or malaysia* or mongolia* or myanmar or pacific island* or papua new guinea or papuans or philippin* or filipin* or the philippine* or singapore* or taiwan* or thai or timor-leste or vietnam*) exp Cambodia/ or exp Indochina/ or exp Indonesia/ or exp Laos/ or exp Malaysia/ or exp Myanmar/ or exp Philippines/ or exp Singapore/ or exp Thailand/ or exp Timor-Leste/ or exp Vietnam/ or exp China/ or exp Japan/ or exp Korea/ or exp Mongolia/ or exp Taiwan/ or exp Indonesia/ or exp Japan/ or exp Macau/ or exp Philippines/ or exp Taiwan/ |
| Results: 120 |
PsychInfo
| Category | Search terms |
| YEH | ((homeless* and (child* or youth* or adolescen* or teen*)) or street child* or street sleep* or ill-housed person* or rough sleep* or street dwell* or railway boy*) (child, homeless or child, street or children, homeless or children, street or homeless child or homeless children or homeless youth or homeless youths or runaway or runaways or street child or street children or street youth or youth, homeless or youth, street or youths, homeless or youths, street) |
|
AND |
|
| Mental health intervention | (mental health service* or therapeutic support* or counselling or counseling or housing program* or temporary shelter* or homeless shelter* or psychological counseling or psychological counselling or short-term temporary care or short-term care or youth homeless* shelter or non government* organisation* or non government* organization* or non-government* organisation* or non-government* organization* or NGO* or mental health care or mental health support* or cognitive behavioural therap* or cognitive behavioral therap* or CBT* or substance abuse therap* or outreach program* or outreach support* or mental health intervention* or mental health* or life counseling or life counselling or overcrowded or centre base* or center base* or emergency accommodation* or homeless* facilit* or food bank* or rehabilitation* or prevention approach* or social work* or therap*) (Rehabilitation Counseling or School Counseling or Aftercare or School Counseling or Mental Health Services or Community Mental Health Services or Early Intervention or Family Intervention or School Based Intervention or Mental Health Programs or Crisis Intervention Services or Hot Line Services or Suicide Prevention Centers or Home Visiting Programs or Suicide Prevention Centers) |
|
AND |
|
| EAP countries | (east asia* pacific or east asia* pacific countr* or cambodia* or china or chinese* or hong kong or indonesia* or japan* or south korea* or lao* pdr or macau or macanese or malaysia* or mongolia* or myanmar or pacific island* or papua new guinea or papuans or philippin* or filipin* or the philippine* or singapore* or taiwan* or thai or timor-leste or vietnam*) (Pacific Islanders or Asia Southeastern or Asia Eastern) |
| Results: 153 |
| Category | Search terms |
| YEH | (((((((((((((homeless*)) AND (child*)) OR (youth*)) OR (adolescen*)) OR (teen*)) OR (ill-housed person*)) OR ("homeless teen")) OR ("street sleeper"[tiab:~0])) OR ("children of the street"[tiab:~0])) OR ("street youth")) OR ("runaway* child*")) OR ("runaway* adolescen*")) OR ("street child*") |
| AND | |
| Mental health intervention | ((((((((((((((((((((((((((((((((((mental health service*) OR (therapeutic support*)) OR (counselling)) OR (counseling)) OR ("housing program*")) OR ("temporary shelter*")) OR ("homeless shelter*")) OR ("psychological counseling")) OR ("psychological counselling")) OR ("temporary care")) OR ("short-term care")) OR ("youth homeless* shelter"[tiab:~10])) OR ("non government* organisation")) OR ("non government* organization")) OR ("non-government* organisation")) OR ("non-government* organization")) OR ("NGO"[tiab])) OR ("mental health care")) OR ("mental health support*")) OR ("cognitive behavioural therap*")) OR ("cognitive behavioral therap*")) OR (CBT[tiab])) OR ("substance abuse therap*")) OR ("outreach program*")) OR ("outreach support*")) OR ("mental health intervention")) OR ("rehabilitation counseling")) OR ("community mental health service*")) OR ("family intervention*")) OR ("mental health program*")) OR ("crisis intervention service*")) OR ("hot line service*")) OR ("suicide prevention center*") ) OR (psychotherap*)) OR ("homeless intervention*") |
| AND | |
| EAP countries | ((((((((((((((((((((((((((((east asia* pacific) OR (east asia* pacific countr*)) OR (cambodia*)) OR (china)) OR (chinese)) OR (hong kong)) OR (indonesia*)) OR (japan*)) OR (south korea*)) OR (lao* pdr)) OR (macau)) OR (macanese)) OR (malaysia*)) OR (mongolia*)) OR (myanmar)) OR (pacific island*)) OR (papua new guinea)) OR (papuans)) OR (philippin*)) OR ("the philippin*")) OR (filipin*)) OR (singapore*)) OR (taiwan*)) OR (thai)) OR (timor-leste)) OR (vietnam*)) OR ("south-east asia*")) OR ("southeast asia*")) OR ("east asia*") |
| Results: 2,546 |
Scopus
| Category | Search terms |
| YEH | "homeless*" OR "homeless* youth" OR "homeless* child*" OR "homeless* adolescen*" OR "homeless* teen" OR " homeless* young person*" OR "homeless* young people*" OR "street child*" OR "street sleeper" OR "homeless* youth" OR "ill-housed person" OR "street youth" OR runaway* OR "runaway youth*" OR "street youth*" OR "rough sleep*" OR "railway boy*" OR "street dwell*" OR "refugee*” |
| AND |
|
| Mental health intervention | "mental health service*" OR "mental health intervention*" OR "psychological intervention*" OR "therap* support*" OR counseling OR “counselling” OR "psychological counseling" OR “psychological counselling” OR "short-term temporary care" OR "short-term care" OR "youth homeless* shelter" OR "homeless* shelter*" OR "non-government* organisation*" OR “non-governmen* organization” OR NGO* OR "mental health care" OR "mental health support" OR "cognitive behavioural therap*" OR “cognitive behavioral therap*” OR CBT OR "outreach program*" OR "outreach support*" OR "outreach work*" OR "homeless* policy*" OR "homeless* policies" OR "homeless* law*" OR "policies" or "policy" OR "community service*" OR "community mental health service*" OR "emergency service*" OR "family therap*" OR "family intervention*" OR "mental health program*" OR "crisis intervention* service*" OR "hotline service*" OR "school based intervention*" OR "suicide prevention cent*" OR "home visiting program*" OR "community program*" OR "family based intervention*" OR "family based intervention*" OR "emergency accommodation*" OR "homeless* facilit*" OR "food bank*" OR rehabilitation* OR "social work*" |
| AND |
|
| EAP countries | "east asia* pacific" OR "east asia* pacific countr*" OR cambodia* OR china OR chinese OR "hong kong" OR indonesia* OR japan* or "south korea*" OR "lao* pdr" OR macau OR macanese OR malaysia* OR mongolia* OR myanmar OR "pacific island*" OR "papua new guinea" OR papuans OR philippin* OR "the philippin*" OR filipin* OR singapore* OR taiwan* OR thai* OR "timor-leste" OR viet* |
| Results: 613 |
Web of Science
| Category | Search terms |
| YEH | ((((((((((((((((ALL=(homeless*)) AND ALL=(youth*)) OR ALL=(child*)) OR ALL=(adolescen*)) OR ALL=(teen)) OR ALL=("street child*")) OR ALL=("street sleeper")) OR ALL=("ill-housed person*")) OR ALL=("street youth*")) OR ALL=(runaway*)) OR ALL=("runaway youth*")) OR ALL=("homeless youth*")) OR ALL=("rough sleep*")) OR ALL=("railway boy*")) OR ALL=("street dwell*")) OR ALL=("refugee*")) OR ALL=("left behind child*") |
|
AND |
|
| Mental health intervention | (((((((((((((((((((((((((((((((((((((ALL=("mental health service*")) OR ALL=("mental health intervention*")) OR ALL=("psychological intervention*")) OR ALL=("therap* support*")) OR ALL=(counseling)) OR ALL=(counselling)) OR ALL=("psychological counseling")) OR ALL=("psychological counselling")) OR ALL=("short-term temporary care")) OR ALL=("short-term care")) OR ALL=("youth homeless* shelter*")) OR ALL=("homeless* shelter")) OR ALL=("non-government* organisation*")) OR ALL=("non-government* organization*")) OR ALL=(NGO*)) OR ALL=("mental health care")) OR ALL=("mental health support*")) OR ALL=("cognitive behavioural therap*")) OR ALL=("cognitive behavioral therap*")) OR ALL=(CBT)) OR ALL=("motivation* interview*")) OR ALL=("substance abuse therap*")) OR ALL=("outreach program*")) OR ALL=("outreach support*")) OR ALL=("outreach work*")) OR ALL=(policy)) OR ALL=("mental health*")) OR ALL=("life counseling")) OR ALL=("life counselling")) OR ALL=("overcrowded")) OR ALL=("centre based")) OR ALL=("center based")) OR ALL=("emergency accommodation")) OR ALL=("homeless* facilit*")) OR ALL=("food bank*")) OR ALL=("rehabilitation*")) OR ALL=("social work*")) OR ALL=("therap*") |
|
AND |
|
| EAP countries | (((((((((((((((((((((((((ALL=("east asia* pacific")) OR ALL=("east asia* pacific countr*")) OR ALL=(cambodia*)) OR ALL=(china)) OR ALL=(chinese)) OR ALL=("hong kong")) OR ALL=(indonesia*)) OR ALL=(japan*)) OR ALL=("south korea*")) OR ALL=("lao* pdr")) OR ALL=(macau)) OR ALL=(manganese)) OR ALL=(malaysia*)) OR ALL=(mongolia*)) OR ALL=(myanmar)) OR ALL=("pacific island*")) OR ALL=("papua new guinea")) OR ALL=(papuans)) OR ALL=(philippin*)) OR ALL=("the philippin*")) OR ALL=("filipin*")) OR ALL=(singapore*)) OR ALL=(tawain*)) OR ALL=(thai*)) OR ALL=("timor-leste")) OR ALL=(vietnam*) |
| Results: 92 |
Appendix C
The Critical Appraisal Skills Programme (CASP) checklists


References
- OECD. HC3.1. Homeless populations. https://www.oecd.org/els/family/HC3-1-Homeless-population.pdf.
- United Nations. Affordable housing and social protection systems for all to address homelessness: report of the Secretary-General. 2020;
- Speak S. The state of homelessness in developing countries ‘Affordable housing and social protection systems for all to address homelessness’ United Nations Office at Nairobi. https://www.un.org/development/desa/dspd/wp-content/uploads/sites/22/2019/05/SPEAK_Suzanne_Paper.pdf.
- Alif Jasni M, Hassan N, Ibrahim F, Kamaluddin MR, Che Mohd Nasir N. The interdepence between poverty and homelessness in Southeast Asia: The case of Malaysia, Indonesia, Thailand, and Singapore. International Journal of Law, Government and Communication. 09/09 2022;7:205-222. https://doi.org/10.35631/IJLGC.729015. [CrossRef]
- Asian Development Bank. At the Margins: Street children in Asia and the Pacific. Asian Development Bank, Regional and Sustainable Development Department; 2003.
- Internal Displacement Monitoring Centre [IDMC]. Disaster displacement in Asia and the Pacific. [online] https://www.internal-displacement.org/sites/default/files/publications/documents/220919_IDMC_Disaster-Displacement-in-Asia-and-the-Pacific.pdf.
- Su Z, Bentley BL, Cheshmehzangi A, et al. Mental health of homeless people in China amid and beyond COVID-19. The Lancet Regional Health – Western Pacific. 2022;25doi:10.1016/j.lanwpc.2022.100544. [CrossRef]
- Klatt T, Cavner D, Egan V. Rationalising predictors of child sexual exploitation and sex-trading. Child Abuse & Neglect. 2014/02/01/ 2014;38(2):252-260. https://doi.org/10.1016/j.chiabu.2013.08.019. [CrossRef]
- Aptekar L, Stoecklin D. Street children and homeless youth: A cross-cultural perspective. vol 9789400773561. 2013:1-240.
- Bhukuth A, Jerome B. Children of the street: Why are they in the street? How do they live? Economics & Sociology. 12/20 2015;8:134-148. https://doi.org/10.14254/2071-789X.2015/8-4/10. [CrossRef]
- Bender KA, Thompson SJ, Ferguson KM, Yoder JR, Kern L. Trauma among street-involved youth. Journal of Emotional and Behavioral Disorders. 2014;22(1):53-64. https://doi.org/10.1177/1063426613476093. [CrossRef]
- Saddichha S, Linden I, Krausz MR. Physical and mental health issues among homeless youth in British Columbia, Canada: Are they different from older homeless adults? . Can Acad Child Adolesc Psychiatry. 2014;23(3):200-206.
- Yoder KA, Longley SL, Whitbeck LB, Hoyt DR. A dimensional model of psychopathology among homeless adolescents: Suicidality, internalising, and externalising disorders. Journal of Abnormal Child Psychology. 2008/01/01 2008;36(1):95-104. https://doi.org/10.1007/s10802-007-9163-y. [CrossRef]
- Bender K, Begun S, Durbahn R, Ferguson K, N S. My own best friend: Homeless youths’ sesitance to seek help and strategies for coping independently after distressing and traumatic experiences. Social Work in Public Health. 2018;33(3):149--162. https://doi.org/10.1080/19371918.2018.1424062 , note = PMID: 29377774. [CrossRef]
- Falci CD, Whitbeck LB, D.R H, Rose T. Predictors of change in self-reported social networks among homeless young people. Journal of Research on Adolescence. 2011;21(4):827-841.
- Kolar K, Erickson PG, Stewart D. Coping strategies of street-involved youth: exploring contexts of resilience. Journal of Youth Studies. 2012/09/01 2012;15(6):744-760. https://doi.org/10.1080/13676261.2012.677814. [CrossRef]
- Lee S-J, Liang L-J, Rotheram-Borus MJ, Milburn NG. Resiliency and survival skills among newly homeless adolescents: Implications for future interventions. Vulnerable Children and Youth Studies. 2011/12/01 2011;6(4):301-308. https://doi.org/10.1080/17450128.2011.626468. [CrossRef]
- Lee Y, Hyoung LM. Effects of drinking, self-esteem and social networks on resilience of the homeless. Alcohol and Health Behaviour Research. 2014;15(1):51–63.
- Moskowitz A, Stein JA, Lightfoot M. The mediating roles of stress and maladaptive behaviours on self-harm and suicide attempts among runaway and homeless youth. Journal of Youth and Adolescence. 2013/07/01 2013;42(7):1015-1027. https://doi.org/10.1007/s10964-012-9793-4. [CrossRef]
- Hubley AM, Russell LB, Palepu A, Hwang SW. Subjective quality of life among individuals who are homeless: A review of current knowledge. Social Indicators Research. 2014/01/01 2014;115(1):509-524. https://doi.org/10.1007/s11205-012-9998-7. [CrossRef]
- Perlman S, Willard J, Herbers JE, Cutuli JJ, Garg KME. Youth homelessness: Prevalence and mental health correlates. Journal of the Society for Social Work and Research. 2014;5(3):361-377. https://doi.org/10.1086/677757. [CrossRef]
- Slesnick N, Zhang J, Walsh L. Youth experiencing homelessness with suicidal ideation: Understanding risk associated with peer and family social networks. Community Mental Health Journal. 2021/01/01 2021;57(1):128-135. https://doi.org/10.1007/s10597-020-00622-7. [CrossRef]
- Tyler KA, Whitbeck LB, Hoyt DR, Cauce AM. Risk factors for sexual victimisation among male and female homeless and runaway youth. Journal of Interpersonal Violence. 2004;19(5):503-520. https://doi.org/10.1177/0886260504262961. [CrossRef]
- Mostajabian S, Santa Maria D, Wiemann C, Newlin E, Bocchini C. Identifying sexual and labour exploitation among sheltered youth experiencing homelessness: A comparison of screening methods. International Journal of Environmental Research and Public Health. 2019;16(3):363.
- Gao Y, Atkinson-Sheppard S, Yu Y, Xiong G. A review of the national policies on street children in China. Children and Youth Services Review. 2018/10/01/ 2018;93:79-87. https://doi.org/10.1016/j.childyouth.2018.07.009. [CrossRef]
- Nurwati N, Fedryansyah M, Achmad W. Social policy in the protection of street children in Indonesia. Journal of Governance. 2022;7(3)doi:10.31506/jog.v7i3.16366. [CrossRef]
- Hyun M-S, Chung H-IC, Lee Y-J. The effect of cognitive–behavioural group therapy on the self-esteem, depression, and self-efficacy of runaway adolescents in a shelter in South Korea. Applied Nursing Research. 2005/08/01/ 2005;18(3):160-166. https://doi.org/10.1016/j.apnr.2004.07.006. [CrossRef]
- Noh D, Kim E. Experiences of family conflict in shelter-residing runaway youth: A phenomenological study. Journal of Family Issues. 2021;42(10):2335-2352. https://doi.org/10.1177/0192513x20979624. [CrossRef]
- United Nations. United Nations demographic yearbook review national reporting of household characteristics, living arrangements and homeless households Implications for international recommendations. https://unstats.un.org/unsd/demographic-social/products/dyb/documents/techreport/hhchar.pdf.
- UN-Habitat. Homelessness and the right to adequate housing. https://www.ohchr.org/sites/default/files/Documents/Issues/Housing/Homelessness/UNagencies_regionalbodies/13112015-UN_Habitat.docx.
- Iwata M. What is the problem of homelessness in Japan? Conceptualisation, research, and policy response. International Journal on Homelessness. 2021;1(1):98–124. https://doi.org/10.5206/ijoh.2021.1.13629. [CrossRef]
- Tan H. ‘We are not like them’: stigma and the Destitute Persons Act of Singapore. International Journal of Law in Context. 2021;17(3):318-335. https://doi.org/10.1017/S1744552321000410. [CrossRef]
- Korea Legislation Research Institute. Acts on support for welfare and self-reliance of the homeless. elaw.klri.re.kr. https://elaw.klri.re.kr/eng_service/lawView.do?hseq=45559&lang=ENG.
- Rosenthal D, Lewis C, Heys M, et al. Barriers to optimal health for Under 5s experiencing homelessness and living in temporary accommodation in high-income countries: A scoping review. Ann Public Health Res. 2021;8(1).
- Kanehara A, Umeda M, Kawakami N, World Mental Health Japan Survey Group. Barriers to mental health care in Japan: Results from the world mental health Japan survey. Psychiatry Clin Neurosci. 2015/09// 2015;69(9):523-533. https://doi.org/10.1111/pcn.12267. [CrossRef]
- Lasco G, Gregory Yu V, David CC. The lived realities of health financing: A qualitative exploration of catastrophic health expenditure in the Philippines. Acta Medica Philippina. 2022;56(11)doi:10.47895/amp.vi0.2389. [CrossRef]
- Martinez AB, Co M, Lau J, Brown JSL. Filipino help-seeking for mental health problems and associated barriers and facilitators: A systematic review. Social Psychiatry and Psychiatric Epidemiology. 2020/11/01 2020;55(11):1397-1413. https://doi.org/10.1007/s00127-020-01937-2. [CrossRef]
- Cipta D, Saputra A. Changing landscape of mental health from early career psychiatrists’ perspective in Indonesia. Journal of Global Health Neurology and Psychiatry. 08/05 2022;doi:10.52872/001c.37413. [CrossRef]
- Lally J, Tully J, Samaniego R. Mental health services in the Philippines. BJPsych International. 2019;16(3):62-64. https://doi.org/10.1192/bji.2018.34. [CrossRef]
- Meshvara D. Mental health and mental health care in Asia. World Psychiatry. Jun 2002;1(2):118-20.
- Cheng L-C, Yang Y-S. Homeless problems in Taiwan: Looking beyond legality toward social issues. City, Culture and Society. 2010/09/01/ 2010;1(3):165-173. https://doi.org/10.1016/j.ccs.2010.10.005. [CrossRef]
- Kubota H, Clandinin DJ, Caine V. ‘I hope one more flower will bloom in my life’: Retelling the stories of being homeless in Japan through narrative inquiry. Journal of Social Distress and Homelessness. 2019/01/02 2019;28(1):14-23. https://doi.org/10.1080/10530789.2018.1541638. [CrossRef]
- Biswas J, Gangadhar BN, Keshavan M. Cross cultural variations in psychiatrists’ perception of mental illness: A tool for teaching culture in psychiatry. Asian Journal of Psychiatry. 2016/10/01/ 2016;23:1-7. https://doi.org/10.1016/j.ajp.2016.05.011.
- Kirmayer LJ. The cultural diversity of healing: Meaning, metaphor and mechanism. British Medical Bulletin. 2004;69(1):33-48. https://doi.org/10.1093/bmb/ldh006.
- Liu J, Yan F, Ma X, et al. Perceptions of public attitudes towards persons with mental illness in Beijing, China: Results from a representative survey. Social Psychiatry and Psychiatric Epidemiology. 2016/03/01 2016;51(3):443-453. https://doi.org/10.1007/s00127-015-1125-z. [CrossRef]
- Yang F, Yang BX, Stone TE, et al. Stigma towards depression in a community-based sample in China. Comprehensive Psychiatry. 2020/02/01/ 2020;97:152152. https://doi.org/10.1016/j.comppsych.2019.152152. [CrossRef]
- Gopalkrishnan N. Cultural diversity and mental health: Considerations for policy and practice. Review. Frontiers in Public Health. 2018-June-19 2018;6doi:10.3389/fpubh.2018.00179. [CrossRef]
- Helfrich CA, Fogg LF. Outcomes of a life skills intervention for homeless adults with mental illness. The Journal of Primary Prevention. 2007/07/01 2007;28(3):313-326. https://doi.org/10.1007/s10935-007-0103-y. [CrossRef]
- Slesnick N, Guo X, Brakenhoff B, Bantchevska D. A comparison of three interventions for homeless youth evidencing substance use disorders: Results of a randomised clinical trial. Journal of Substance Abuse Treatment. 2015;54:1-13. https://doi.org/10.1016/j.jsat.2015.02.001. [CrossRef]
- Spiegel JA, Graziano PA, Arcia E, et al. Addressing mental health and trauma-related needs of sheltered children and families with Trauma-Focused Cognitive-Behavioral Therapy (TF-CBT). Administration and Policy in Mental Health and Mental Health Services Research. 2022/09/01 2022;49(5):881-898. https://doi.org/10.1007/s10488-022-01207-0. [CrossRef]
- Altena AM, Brilleslijper-Kater SN, Wolf JRLM. Effective interventions for homeless youth: A systematic review. American Journal of Preventive Medicine. 2010;38(6):637-645. https://doi.org/10.1016/j.amepre.2010.02.017. [CrossRef]
- Morton MH, Kugley S, Epstein R, Farrell A. Interventions for youth homelessness: A systematic review of effectiveness studies. Children and Youth Services Review. 2020/09/01/ 2020;116:105096. https://doi.org/10.1016/j.childyouth.2020.105096. [CrossRef]
- Wang JZ, Mott S, Magwood O, et al. The impact of interventions for youth experiencing homelessness on housing, mental health, substance use, and family cohesion: A systematic review. BMC Public Health. 2019/11/14 2019;19(1):1528. https://doi.org/10.1186/s12889-019-7856-0. [CrossRef]
- Centre for Evidence-Based Management (CEBMa). CEBMa Guideline for Critically Appraised Topics in Management and Organisations. [online]. Centre for Evidence-Based Management. https://www.cebma.org/wp-content/uploads/CEBMa-CAT-Guidelines.pdf.
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for Scoping Reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine. 2018;169(7):467-473. https://doi.org/10.7326/m18-0850 %m 30178033.
- Rojon C, Okupe A, McDowall A. Utilisation and development of systematic reviews in management research: What do we know and where do we go from here? International Journal of Management Reviews. 2021;23(2):191-223. https://doi.org/10.1111/ijmr.12245. [CrossRef]
- Richardson WS, Wilson MC, Nishikawa J, Hayward RS. The well-built clinical question: A key to evidence-based decisions. ACP J Club. Nov-Dec 1995;123(3):A12-3.
- The World Bank. The World Bank In East Asia Pacific. https://www.worldbank.org/en/region/eap/overview Accessed in May 2023 and April 2024.
- The World Bank. The World Bank in East Asia Pacific. https://www.worldbank.org/en/region/eap Accessed in May 2023 and April 2024.
- Centre for Homelessness Impact (CHI). Centre for homelessness impact. https://www.homelessnessimpact.org/.
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71. [CrossRef]
- Critical Appraisal Skills Programme (CASP). CASP Randomised Controlled Trial Checklist [online]. https://casp-uk.net/checklists/casp-rct-randomised-controlled-trial-checklist.pdf.
- Critical Appraisal Skills Programme (CASP). CASP Qualitative Studies Checklist [online]. https://casp-uk.net/checklists/casp-qualitative-studies-checklist-fillable.pdf.
- Critical Appraisal Skills Programme (CASP). CASP Case Control Study Checklist [online]. 2018;
- Critical Appraisal Skills Programme (CASP). CASP Cohort Study Checklist [online]. 2018;
- Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Research Methods in Medicine & Health Sciences. 2020;1(1):31-42. https://doi.org/10.1177/2632084320947559. [CrossRef]
- Sarmini M, Sukartiningsih S. From the road to the arena: The role of Kampung Anak Negeri for street children. Atlantis Press; 2018:1572-1577.
- Solong A, Rahman M, Aras D, Alim A. Street child management policy at social office of Makassar City, Indonesia. International Journal of Research 2023;11(4):33-50. https://doi.org/10.29121/granthaalayah.v11.i4.2023.5128. [CrossRef]
- Mohammadzadeh M, Awang H, Hayati K.S, Ismail S. The effects of a life skills-based intervention on emotional health, self-esteem and coping mechanisms in Malaysian institutionalised adolescents: Protocol of a multi-centre randomised controlled trial. International Journal of Educational Research. 2017/01/01/ 2017;83:32-42. https://doi.org/10.1016/j.ijer.2017.02.010. [CrossRef]
- Noh D. The effect of a resilience enhancement programme for female runaway youths: A quasi-experimental study. Issues in Mental Health Nursing. 2018/09/02 2018;39(9):764-772. doi:10.1080/01612840.2018.1462871. [CrossRef]
- Noh D, Choi S. Development of a family-based mental health program for runaway adolescents using an intervention mapping protocol. International Journal of Environmental Research and Public Health. 2020;17(21):7794.
- Brillantes-Evangelista G. An evaluation of visual arts and poetry as therapeutic interventions with abused adolescents. The Arts in Psychotherapy. 2013/02/01/ 2013;40(1):71-84. https://doi.org/10.1016/j.aip.2012.11.005. [CrossRef]
- Miles GM. Drawing together hope: 'listening' to militarised children. Journal of Child Health Care. 2000;4(4):137-142. https://doi.org/10.1177/136749350000400401. [CrossRef]
- The Metropolitan Museum of Art. ‘Southeast Asia, 1900 A.D.–present.’ In Heilbrunn Timeline of Art History. https://www.metmuseum.org/toah/ht/11/sse.html.
- The World Bank. Southeast Asian countries reach milestone agreement to strengthen resilience. https://www.worldbank.org/en/events/2017/05/05/southeast-asian-countries-reach-milestone-agreement.
- Corcoran K, Fischer J. Measures for clinical practice and research: A sourcebook. 3 ed. Simon & Schuster Inc. ; 2000.
- WK Z. A self-rating depression scale. Archives of General Psychiatry. 1965;12(1):63-70. https://doi.org/10.1001/archpsyc.1965.01720310065008. [CrossRef]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. Jun 1961;4:561-71. https://doi.org/10.1001/archpsyc.1961.01710120031004. [CrossRef]
- Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. Mar 1995;33(3):335-43. https://doi.org/10.1016/0005-7967(94)00075-u. [CrossRef]
- Greenwald R, Rubin A. Assessment of posttraumatic symptoms in children: Development and preliminary validation of parent and child scales. Research on Social Work Practice. 1999;9(1):61-75. https://doi.org/10.1177/104973159900900105. [CrossRef]
- Coopersmith S. The antecedents of self-esteem. Series of books in behavioral science. W.H. Freeman; 1967.
- Chang D. The effects of parent’s nurturing behaviour on self-esteem of children. Kyungbuk University; 1984.
- Lee Y, Song J. A study of the reliability and the validity of the BDI, SDS, and MMPI-D scales. Korean J Clin Psychol. 1991;10:98–113.
- Sherer M, Maddux JE, Mercandante B, Prentice-Dunn S, Jacobs B, Rogers RW. The self-efficacy scale: Construction and validation. Psychological Reports. 1982;51(2):663-671. https://doi.org/10.2466/pr0.1982.51.2.663. [CrossRef]
- Oh H. Health promoting behaviours and quality of life of Korean women with arthritis. Unpublished doctoral dissertation. University of Texas, Austin; 1993.
- Rosenberg M. Society and the adolescent self-image. Princeton University Press; 1965.
- Jamil Mohd Y, Mohd B. Validity and reliability study of Rosenberg self-esteem scale in Seremban school children. Malaysian Journal of Psychiatry. 2006;15:35-39.
- Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. Jun 1978;6(6):1231-1239.
- Kang S, Yoon B, Lee H, Lee D, Shim U. A study of family APGAR scores for evaluating family function. Korean Academy of Family Medicine. 12 1984;5(12):6-13.
- Shin W, Kim M, Kim J. Developing measures of resilience for Korean adolescents and testing cross, convergent, and discriminant validity. Studies on Korean Youth. 2009;20(4):105–131.
- Beck AT, Steer RA, Brown G. Beck Depression Inventory–II (BDI-II) [Database record]. APA PsycTests. 1996;doi:https://doi.org/10.1037/t00742-000. [CrossRef]
- Kim J-H, Lee E-H, Hwang S-T, Hong S-H. Manual for the Korean BDI-II. Korea Psychology Corporation; 2014.
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. Dec 1988;56(6):893-7. https://doi.org/10.1037//0022-006x.56.6.893. [CrossRef]
- Kim J-H, Lee E-H, Hwang S-T, Hong S-H. Manual for the Korean BAI. Korea Psychology Corporation; 2014.
- Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction. 1993;88(6):791-804. https://doi.org/10.1111/j.1360-0443.1993.tb02093.x. [CrossRef]
- World Health Organisation. Life skills education for children and adolescents in schools: Introduction and guidelines to facilitate the development and implementation of life skills programme.
- Lazarus RS, Folkman S. Stress, appraisal, and coping. Springer publishing company; 1984.
- Willis A, Isaacs T, Khunti K. Improving diversity in research and trial participation: The challenges of language. The Lancet Public Health. 2021;6(7):e445-e446. https://doi.org/10.1016/S2468-2667(21)00100-6. [CrossRef]
- Malchiodi CA. Art therapy, attachment, and parent-child dyads. Creative arts and play therapy for attachment problems. The Guilford Press; 2014:52-66. Creative arts and play therapy.
- Allen JD, Carter K, Pearson M. Frangible emotion becomes tangible expression: Poetry as therapy with adolescents. 2019:.
- Bowman DO, Halfacre DL. Poetry therapy with the sexually abused adolescent: A case study. The Arts in Psychotherapy. 1994/01/01/ 1994;21(1):11-16. https://doi.org/10.1016/0197-4556(94)90032-9. [CrossRef]
- Moula Z, Aithal S, Karkou V, Powell J. A systematic review of child-focused outcomes and assessments of arts therapies delivered in primary mainstream schools. Children and Youth Services Review. 2020/05/01/ 2020;112:104928. https://doi.org/10.1016/j.childyouth.2020.104928. [CrossRef]
- Hackett SS, Ashby L, Parker K, Goody S, Power N. UK art therapy practice-based guidelines for children and adults with learning disabilities. International Journal of Art Therapy. 2017/04/03 2017;22(2):84-94. https://doi.org/10.1080/17454832.2017.1319870. [CrossRef]
- Rohde P, Clarke GN, Lewinsohn PM, Seeley JR, Kaufman NK. Impact of comorbidity on a cognitive-behavioural group treatment for adolescent depression. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40(7):795-802. https://doi.org/10.1097/00004583-200107000-00014. [CrossRef]
- Shein-Szydlo J, Sukhodolsky DG, Kon DS, Tejeda MM, Ramirez E, Ruchkin V. A randomized controlled study of cognitive–behavioural therapy for posttraumatic stress in street children in Mexico City. Journal of Traumatic Stress. 2016;29(5):406-414. https://doi.org/10.1002/jts.22124. [CrossRef]
- Ghodousi N, Sajedi F, Mirzaie H, Rezasoltani P. The effectiveness of cognitive-behavioural play therapy on externalising behaviour problems among street and working children. Original Research Articles. Iranian Rehabilitation Journal. 2017;15(4):359-366. https://doi.org/10.29252/nrip.irj.15.4.359. [CrossRef]
- Hofmann SG, Asnaani A, Vonk IJJ, Sawyer AT, Fang A. The efficacy of cognitive behavioural therapy: A review of meta-analyses. Cognitive Therapy and Research. 2012/10/01 2012;36(5):427-440. https://doi.org/10.1007/s10608-012-9476-1. [CrossRef]
- Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review. 1977;84(2):191-215. https://doi.org/10.1037/0033-295X.84.2.191. [CrossRef]
- Kolubinski DC, Frings D, Nikčević AV, Lawrence JA, Spada MM. A systematic review and meta-analysis of CBT interventions based on the Fennell model of low self-esteem. Psychiatry Research. 2018/09/01/ 2018;267:296-305. https://doi.org/10.1016/j.psychres.2018.06.025. [CrossRef]
- Falk CF, Heine SJ. What is implicit self-esteem, and does it vary across cultures? Personality and Social Psychology Review. 2015;19(2):177-198. https://doi.org/10.1177/1088868314544693. [CrossRef]
- Wang Y, Ollendick TH. A cross-cultural and developmental analysis of self-esteem in Chinese and Western children. Clinical Child and Family Psychology Review. 2001/09/01 2001;4(3):253-271. https://doi.org/10.1023/A:1017551215413. [CrossRef]
- Bockting CL, Hollon SD, Jarrett RB, Kuyken W, Dobson K. A lifetime approach to major depressive disorder: The contributions of psychological interventions in preventing relapse and recurrence. Clinical Psychology Review. 2015/11/01/ 2015;41:16-26. https://doi.org/10.1016/j.cpr.2015.02.003. [CrossRef]
- Yadav P, Iqbal N. Impact of life skill training on self-esteem, adjustment and empathy among adolescents. Journal of the Indian Academy of Applied Psychology. 01/01 2009;35(10):61-70.
- Winarsunu T, Iswari Azizaha BS, Fasikha SS, Anwar Z. Life skills training: Can it increases self esteem and reduces student anxiety? Heliyon. 2023;9(4)doi:10.1016/j.heliyon.2023.e15232. [CrossRef]
- Maryam E, Davoud MM, Zahra G, somayeh B. Effectiveness of life skills training on increasing self-esteem of high school students. Procedia - Social and Behavioural Sciences. 2011/01/01/ 2011;30:1043-1047. https://doi.org/10.1016/j.sbspro.2011.10.203. [CrossRef]
- Shin J, Baek J. The effect of self-esteem and social support on depression for middle-aged and elderly male homeless. Journal of the Korea Gerontological Society. 2010;30(4).
- Development Services Group Inc., & Child Welfare Information Gateway. Promoting protective factors for in-risk families and youth: A guide for practitioners U.S Department of Health and Human Services, Administration on Children, Youth and Families, Children’s Bureau; 2015.
- Lightfoot M, Stein JA, Heather T, Preston K. Protective factors associated with fewer multiple problem behaviours among homeless/runaway youth. Journal of Clinical Child & Adolescent Psychology. 2011/11/01 2011;40(6):878-889. https://doi.org/10.1080/15374416.2011.614581. [CrossRef]
- Hamdani SU, Zill e H, Zafar SW, et al. Effectiveness of relaxation techniques ‘as an active ingredient of psychological interventions’ to reduce distress, anxiety and depression in adolescents: A systematic review and meta-analysis. International Journal of Mental Health Systems. 2022/06/28 2022;16(1):31. https://doi.org/10.1186/s13033-022-00541-y. [CrossRef]
- Alvord MK, Zucker BG, Grados JJ. Resilience Builder Program for children and adolescents: Enhancing social competence and self-regulation—A cognitive-behavioral group approach. 2011:.
- Swahn MH, Culbreth R, Tumwesigye NM, Topalli V, Wright E, Kasirye R. Problem drinking, alcohol-related violence, and homelessness among youth living in the slums of Kampala, Uganda. International Journal of Environmental Research and Public Health. 2018;15(6):1061.
- Tyler KA, Johnson KA. Pathways in and out of substance use among homeless-emerging adults. Journal of Adolescent Research. 2006;21(2):133-157. https://doi.org/10.1177/0743558405285494. [CrossRef]
- Rew L, Powell T, Brown A, Becker H, Slesnick N. An intervention to enhance psychological capital and health outcomes in homeless female youths. Western Journal of Nursing Research. 2016; 39(3):356–373. https://doi.org/10.1177/0193945916658861. [CrossRef]
- Bandura A, Caprara GV, Barbaranelli C, Regalia C, Scabini E. Impact of family efficacy beliefs on quality of family functioning and satisfaction with family life. Applied Psychology: An International Review. 2011;60(3):421-448. https://doi.org/10.1111/j.1464-0597.2010.00442.x. [CrossRef]
- Pinto AC, Luna IT, Sivla Ade A, Pinheiro PN, Braga VA, Souza AM. Risk factors associated with mental health issues in adolescents: An integrative review. Rev Esc Enferm USP. Jun 2014;48(3):555-64. Fatores de risco associados a problemas de saúde mental em adolescentes: revisão integrativa. https://doi.org/10.1590/s0080-623420140000300022. [CrossRef]
- Dishion TJ, McMahon RJ. Parental monitoring and the prevention of child and adolescent problem behaviour: A conceptual and empirical formulation. Clinical Child and Family Psychology Review. 1998/03/01 1998;1(1):61-75. https://doi.org/10.1023/A:1021800432380. [CrossRef]
- Centrepoint. Independent living programme. https://centrepoint.org.uk/what-we-do/independent-living-programme.
- Centrepoint. How we can end youth homelessness. 2024;
- World Health Organisation. Traditional medicine in the WHO South-East Asia Region: Review of progress 2014–2019. World Health Organisation. Regional Office for South-East Asia; 2020.
- Johnson RB, Onwuegbuzie AJ, Turner LA. Toward a Definition of Mixed Methods Research. Journal of Mixed Methods Research. 2007;1(2):112-133. https://doi.org/10.1177/1558689806298224. [CrossRef]
- Abramovich I. LGBTQ youth homelessness in Canada: Reviewing the Literature. Canadian Journal of Family and Youth/Le Journal Canadien de Famille et de la Jeunesse. 2012;4(1):29-51. https://doi.org/10.29173/cjfy16579. [CrossRef]
- OHCHR. Equal Asia Foundation’s inputs to the UN special rapporteur on housing. Understanding the sheltering and housing needs of LGBTIQ+ persons in Asia. https://www.ohchr.org/sites/default/files/documents/issues/housing/climate/submissions/2022-10-24/Submission-ClimateChange-CSO-EqualAsiaFoundation_0.docx.
- Feng Y, Lou C, Gao E, et al. Adolescents' and young adults' perception of homosexuality and related factors in three Asian cities. Journal of Adolescent Health. 2012;50(3):S52-S60. https://doi.org/10.1016/j.jadohealth.2011.12.008. [CrossRef]
- United Nations. End of mission statement to Republic of Korea. UN Human Rights Office of the High Commissioner. https://www.ohchr.org/en/statements/2018/05/end-mission-statement-republic-korea?LangID=E&NewsID=23116.
- United Nations Department of Economics and Social Affairs. Sustainable Development Goals. (2023) https://unstats.un.org/sdgs/report/2023/.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



