
Submitted:
20 May 2024
Posted:
22 May 2024
You are already at the latest version
Abstract
Background: The aim of the current study is to evaluate the effects of inflammation markers, on infection and mortality in patients over 65 years of age monitored in the intensive care unit. In the study, the significance of pan-immune inflammation (PIV), neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), monocyte-lymphocyte ratio (MLR), systemic immune-inflammatory index (SII), systemic immune response index (SIRI), multi-inflammatory index (MII) 1-2-3, and CRP/albumin ratios, new biomarkers, were attempted to be determined as prognostic and mortality markers in patients over 65 years of age monitored in the ICU. Methods: This multicenter, retrospective cohort study was conducted in two tertiary-level ICUs with patients aged 65 and over who were admitted. Patients with cirrhosis, bone marrow transplantation, hematologic malignancy, undergoing chemotherapy, and neutropenia at admission to the ICU were excluded from the study. Results: A total of 333 patients were included in the study. The 28-day mortality was found to be 31.8%. When each inflammatory marker associated with 28-day mortality was examined the CRP/albumin ratio performed better than both NLR and SIRI, and the results were statistically significant (AUC: 0.665, 95% CI: 0.604-0.726 and p <0.001). NLR had a moderate discriminative ability in distinguishing mortality risk (AUC: 0.593, 95% CI: 0.526-0.660 and p = 0.006). Although SIRI was lower than NLR, it had a statistically significant result (AUC: 0.580, 95% CI: 0.514-0.646 and p = 0.019). CRP/albumin ratio was the most effective inflammatory marker in predicting mortality risk in geriatric patients admitted to the ICU.
Keywords:
intensive care unit
; inflammatory markers
; scoring systems
; geriatric patient
1. Introduction
The World Health Organization (WHO), in its latest classification, categorizes individuals under 65 years old as young, those between 65 and 85 years old as young-old, and those 85 years and older as advanced-old, in parallel with the increase in the elderly population and extended lifespan. In recent years, there has been a consistent increase in the proportion of individuals over 60 years old in the total population [1]. Aging leads to changes in the effectiveness of the immune system, resulting in a decline in immune function with age. These changes, also known as "immune aging," initially involve higher levels of proinflammatory cytokine secretion and a decrease in the ability of the immune system to respond to antigens. Immunological aging also leads to chronic overstimulation of the immune system and a likely increase in the risk of an irregular systemic response to infection [2].
Medical advancements in the management of acute illnesses have indeed reduced overall hospital mortality rates, but these rates remain high in geriatric patients. Therefore, it is an urgent and crucial need in routine clinical practice to identify prognostic indicators, especially for geriatric patients admitted to the intensive care unit (ICU) [3]. The Sequential Organ Failure Assessment (SOFA) and Acute Physiologic Assessment and Chronic Health (APACHE)-II scoring systems are widely used to determine the severity of acute illness and chronic outcomes in patients admitted to the ICU. These scoring systems, used to determine patient prognosis, also assist in resource allocation, continuous quality improvement, and the evaluation of treatment effectiveness [4]. However, recent studies have drawn attention to the importance of certain inflammatory markers obtained from complete blood count (CBC) in determining the morbidity and mortality of individuals with various disease conditions, owing to their ease of application and cost-effectiveness. New inflammatory biomarkers such as neutrophil-lymphocyte ratio (NLR), systemic immune-inflammatory index (SII), systemic immune response index (SIRI), monocyte-lymphocyte ratio (MLR), platelet-lymphocyte ratio (PLR), multi-inflammatory index (MII), and pan-immune inflammation (PIV) have gained popularity in assessing mortality risk in various diseases [5,6]. In a retrospective study by Yoldaş et al. [7], the effectiveness of NLR and PLR in predicting mortality in critical patient populations was demonstrated, highlighting the ease and affordability of evaluating these markers and suggesting that high PLR and NLR in patients admitted to the ICU should be closely monitored for predicting chronic outcomes. In a prospective observational study by Turan et al. [8], the effect of PIV on predicting mortality and prognosis in patients with septic shock was evaluated, demonstrating that PIV could significantly predict median survival time in patients with septic shock. In a study by Ayrancı et al. [9] evaluating NLR and CRP as predictors of in-hospital mortality in geriatric emergency department patients, simultaneous elevation of CRP and NLR was found to be more effective in predicting in-hospital mortality, suggesting that simultaneous monitoring of CRP and NLR by emergency department physicians may help identify geriatric patients at high risk of mortality at an early stage.
To the best of our knowledge, there has been no previous study evaluating the predictive value of inflammatory markers in geriatric patients admitted to the ICU independently of admission diagnosis and across a wide range of disease conditions and laboratory parameters. Therefore, the aim of the current study is to identify factors affecting short- and long-term prognosis and survival in patients aged 65 and over admitted to the ICU, considering the increase in the number of patients aged 65 and over and high ICU costs, and to investigate the guiding role of new inflammatory markers on survival.
2. Materials and Methods
2.1. Study Location, Duration, and Ethical Approval
The current study was conducted at the Internal Medicine Intensive Care Unit of the Akdeniz University Faculty of Medicine and the General Intensive Care Unit of Antalya Kepez State Hospital between June 2022 and December 2023. Ethical approval was obtained from the Akdeniz University Faculty of Medicine Ethics Committee prior to the study (Decision No: KAEK-753, Appendix 1). The study was conducted in accordance with the principles outlined in the Helsinki Declaration.
2.2. Study Method
The research is a retrospective clinical study based on the collection of retrospective data. The study has an observational research nature. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed for patient recording and allocation.
2.3. Study Population
Patients aged 65 and over admitted to the ICU were included in the study. Patients with missing common variable data for multivariate analysis, those followed up in the postoperative ICU, those undergoing bone marrow transplantation, those with cirrhosis or hematologic malignancies, those developing bone marrow suppression after chemotherapy, and those who died within the first 24 hours of ICU admission were excluded from the study. For patients with multiple admissions to the ICU, only data from their first admission was considered.
2.4. Data Collection Methods
The necessary data for the current study were obtained from ICU patient follow-up forms, hospital electronic databases, physician daily observation notes, nurse observation notes, test results, and pre-ICU admission service observation forms.
2.5. Blood Measurements and Reference Values
Routine blood samples are taken from all patients admitted to the ICU for hemograms and biochemistry. Patients' neutrophil, platelet, monocyte, and lymphocyte values are routinely evaluated by taking blood samples and placing them in tubes containing ethylenediaminetetraacetic acid (EDTA), which are then sent to the hospital's laboratory center.
Among the parameters recorded at the time of admission to the ICU and during follow-up in the ICU at the time of secondary endpoint, the following parameters are included: platelet count (x109/L; reference range 100-300), hemoglobin (g/L; reference range 130.0-175.0), lymphocyte count (x109/L; reference range 1.1-3.2), neutrophil count (x109/L; reference range 42.3-77.8), monocyte count (x109/L; reference range 0.4-1.2), creatinine (μmol/L; reference range 53.0-106.0), albumin (g/L; reference range 35.0-55.0)ve C-reactive protein (CRP) (mg/L).
2.6. Data Recording
Patients' age, gender, comorbidities, lactate, neutrophil, monocyte, platelet, lymphocyte, NLR, PLR, MLR, PIV, SII, SIRI, MII 1-2-3, CRP/albumin values, as well as SOFA and APACHE-II scores at admission to the ICU, are routinely recorded. PIV is calculated using the formula: [neutrophil count (103/μL) x platelet count (103/μL) x monocyte count (103/μL)/lymphocyte count (103/μL)], NLR: [neutrophil count (103/μL)/lymphocyte count (103/μL)], PLR: [platelet count (103/μL)/lymphocyte count (103/μL)], SII: [neutrophil count (103/μL) x platelet count (103/μL)/lymphocyte count (103/μL)], MLR: [monocyte count (103/μL)/lymphocyte count (103/μL)], SIRI: [neutrophil count (103/μL) x monocyte count (103/μL)/lymphocyte count (103/μL)], MII-1: [neutrophil count (103/μL) x CRP], MII-2: [PLR x CRP], MII-3: [SII x CRP].
2.7. Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) version 26 was used to statistically analyze the data obtained from the study. Whether the variables obtained as measurement values were suitable for a normal distribution was evaluated using the Shapiro-Wilk or Kolmogorov-Smirnov tests. Continuous variables were expressed as mean ± standard deviation (SD) or median [interquartile range] according to the normal distribution status. Categorical variables were presented as numbers (n) and percentages (%). Pearson's chi-square test, or Fisher's exact test, was used to compare categorical variables. For the comparison of numerical data, the Student t-test was used for normally distributed independent variables, and the Mann-Whitney U test was used for non-normally distributed independent variables. The Wilcoxon test was used to evaluate changes between the median values of repeated (dependent) variables. Binary Logistic Regression Analysis, or Linear Regression Analysis, was applied to evaluate the relationships of statistically significant variables with outcome points independently of other factors. The goodness of fit of the models was evaluated using the Hosmer-Lemeshow test. The Kaplan-Meier test, log-rank test, and Cox regression analysis were used for survival analyses. Survival curves were drawn, and differences between groups were evaluated using Kaplan-Meier analysis. The log-rank test was applied to statistically evaluate survival differences between groups. Cox regression analysis was applied to determine the factors affecting survival. In the study, a significance level of p <0.05 was accepted as statistically significant.
3. Results
After excluding 72 patients with insufficient data, cirrhosis, bone marrow transplantation, hematological malignancy, bone marrow suppression after recent chemotherapy, postoperative patients, and death in the first 24 hours after admission to the ICU, a total of 333 patients were finally included. As seen in Figure 1, the patients were divided into two groups: the deceased group (n=106) and the survived group (n=227).
Of the whole study group, 31.8% were deceased in the 28-day period, and 68.2% survived. The mean age of the deceased group was 77.2±8.5 years, and it was 78.1±8.6 years in the survived group; the difference was not significant (p=0.38). The distribution of sexes was also not different between the two groups; 44.3% (47) of the deceased group and 51.1% (86) of the survived group were female (p=0.25). The chronic conditions were also similar in both groups (p >0.05). The most commonly seen chronic condition was hypertension (HT), followed by diabetes mellitus (DM) (p=0.40, and p=0.64; respectively). The most common indication for admission to the ICU was acute respiratory failure (p=0.94). This was followed by sepsis, altered consciousness, and acute kidney failure (p=0.11, p=0.28, and p=0.19, respectively). The baseline characteristics of the study population are shown in Table 1.
Clinical characteristics of the patients in the ICU according to 28-day mortality are shown in Table 2. Variables include culture growth, steroid use, platelet and erythrocyte transfusion, progression to sepsis in the ICU, mechanical ventilation (MV) before and in the ICU, days related to MV, hospitalization stay, ICU admission, pre- and post-ICU days, as well as SOFA and APACHE scores. The rate of cultural growth was significantly higher in the deceased group, as well as steroid use and progression to sepsis (p<0.001, p<0.001, and p=0.024; respectively). The need for ventilation before or during the ICU admission and the duration of ventilator use were also more common in the deceased group than in the survived group (p<0.001, p<0.001, and p<0.001; respectively). The duration of hospitalization was not different between groups; median duration of hospitalization was 13.5 (18.3) days in the deceased group and 12.0 (12.0) days in the survived group (p=0.68). Higher SOFA and APACHE scores were observed in the deceased group than in the survived group (p<0.001 and p<0.001; respectively).
Table 3 shows inflammatory biomarkers and ratios related to 28-day mortality, comparing values between the deceased and the survived groups. There was a statistically significant difference in NLR, SIRI, MII1, MII2, MII3, and CRP/albumin ratios between the deceased group and survived group (p=0.007, p=0.03, p<0.001, p<0.001, p=0.06, and p<0.001; respectively). PIV, MLR, PLR, and SII values were statistically similar between the groups (p=0.47, p=0.092, p=0.68, and p=0.22; respectively).
Each inflammatory marker related to 28-day mortality is investigated by cox-regression univariate analysis in Table 4. MLR, MII1, MII2, and MII3 did not show statistically significant associations with 28-day mortality (p=0.19, p=0.32, p=0.37, and p=0.14; respectively). Meanwhile, NLR (HR:1.022, 95% CI:1.006-1.038, and p=0.007), SIRI (HR:1.023, 95% CI: 1.000-1.047, and p=0.049), and CRP/albumin ratio (HR:1.154, 95% CI:1.086-1.226, and p<0.001) were statistically and significantly associated with 28-day mortality.
The predictive capability of inflammatory markers and scoring systems on 28-day mortality risk is assessed by ROC analysis, and their cutoff values with specificity and sensitivity are presented in Figure 2 and Table 5. The NLR had a fair discriminatory ability in distinguishing mortality risk with a statistically significant result (AUC:0.593, 95% CI: 0.526-0.660, and p=0.006). The SIRI also had a fair discriminatory ability, though slightly lower than the NLR, with a statistically significant result (AUC: 0.580, 95% CI: 0.514-0.646, and p=0.019). The CRP/albumin ratio showed moderate discriminatory ability and performed better than both NLR and SIRI, with a highly statistically significant result (AUC:0.665, 95% CI: 0.604-0.726, and p<0.001). The CRP/albumin ratio was the most effective among the inflammatory markers in discriminating mortality risk in ICU patients. On the other hand, the APACHE score had an AUC of 0.647 with a 95% CI of 0.579-0.714, and its predictive performance is statistically significant (p<0.001) and the SOFA score had a higher AUC of 0.723 with a 95% CI of 0.663-0.783, also statistically significant (p<0.001). The SOFA score appeared to have the highest AUC among the scoring system predictors listed, and CRP/albumin had the highest predictive capability among the inflammatory markers.
4. Discussion
According to the results of the current study, in patients aged 65 and older admitted to the ICU and who died, it was found that there was a higher incidence of culture positivity, steroid use, and progression to sepsis compared to surviving patients. Additionally, it was observed that the need for ventilation and the duration of ventilator use were longer both before and during ICU admission in patients who died. Furthermore, the SOFA and APACHE-II scores were higher in deceased patients compared to survivors. Regarding 28-day mortality, it was found that NLR, SIRI, MII 1-2-3, and CRP/albumin ratios were higher in deceased patients compared to survivors. However, the values of PIV, MLR, PLR, and SII did not show a significant impact on 28-day mortality. NLR (moderate level), SIRI (moderate level), and CRP/albumin ratio (moderate level) were identified as discriminative factors for the 28-day mortality risk assessment. The CRP/albumin ratio showed better performance than both NLR and SIRI in predicting 28-day mortality. However, despite higher SOFA scores, both SOFA and APACHE II scores were found to have a high predictive value for determining 28-day mortality in patients aged 65 and older admitted to the ICU.
Neutrophils and lymphocytes represent a significant percentage of all immune cells in the bloodstream, making the NLR a relatively simple inflammation index to calculate. In the current study, it was found that the NLR ratio was statistically higher in patients aged 65 and older who died in the ICU compared to survivors, demonstrating the prognostic value of the NLR ratio in critical patients aged 65 and older. It is assumed that systemic inflammation and stress lead to neutrophilia and lymphopenia, consequently increasing the NLR ratio [10]. The increased NLR as a result of an increase in neutrophil count secondary to an increase in the granulocyte series during inflammation and a decrease in lymphocyte count during inflammatory stress may serve as an indicator of systemic inflammation [7]. Additionally, the rise in NLR has been attributed to increased neutrophil production and lymphocyte apoptosis during inflammatory stress [11]. In a prospective cohort study involving 5,034 patients aimed at predicting mortality in geriatric patients admitted to the hospital, similar to our study's findings, it was shown that deceased patients had significantly higher NLR ratios compared to survivors during their hospital stay. The study also suggests that NLR could facilitate the early identification of geriatric patients at high risk of death, as it is easily applicable and cost-effective [3]. In another study evaluating the effect of NLR on postoperative ICU admission and mortality in elderly patients undergoing hip surgery, it was also shown that a high NLR value could be beneficial for predicting ICU admission and subsequent mortality in geriatric patients [12].
SIRI, a novel prognostic marker based on the counts of neutrophils, monocytes, and lymphocytes, reflects the balance between inflammatory response and immune status [13]. It was first identified in a study involving patients with hepatocellular carcinoma (HCC) in 2014. It has been described as a strong prognostic indicator of poor outcomes and a promising marker for treatment strategy decisions in HCC [14]. Subsequently, it has been reported that SIRI elevation could be used in the diagnosis of certain cancers, particularly gastric cancer [15,16]. and colorectal carcinoma [17], indicating worsening inflammatory processes and a poor prognosis in these patients. In a study evaluating the relationship between the inflammatory mechanisms and intracerebral hemorrhage with pneumonia, although NLR showed a stronger association with pneumonia severity, high predictive accuracy for early recognition of pneumonia severity after intracranial hemorrhage and association with poor neurological outcomes upon discharge were demonstrated for SIRI [18]. However, data evaluating the predictive value of SIRI for mortality and prognosis in geriatric patients admitted to the ICU are limited in the literature. In the present study, it was found that although SIRI is lower than the CRP/albumin ratio in predicting 28-day mortality in critical geriatric patients, it can still be a strong indicator, marking the first study to demonstrate the independent significance of SIRI as a predictor of mortality in critical geriatric patients.
In our study, the CRP/albumin ratio was identified as an independent risk factor for 28-day mortality in critical patients, and our findings were consistent with previous studies. Despite the numerous scoring systems used to predict the prognosis of critical patients, the CRP/albumin ratio remains valuable. This is because it is a relatively simple marker that is easy to use in all settings. C-reactive protein (CRP) is an acute-phase protein produced in response to various cytokines after infection, ischemia, trauma, and other inflammatory conditions [19]. The association of high CRP levels and low serum albumin levels with prognosis and mortality in critical patients has been demonstrated in many studies [20,21]. Additionally, it has been noted in the literature that the CRP/albumin ratio is more consistent in predicting prognosis compared to CRP alone or albumin alone [22]. In our study, it was found that the CRP/albumin ratio is a biomarker with a high predictive value for survival in patients aged 65 and older. Supporting results from the literature are available. In a retrospective study by Par et al. [23], evaluating the CRP/albumin ratio as a determinant of mortality in ICU patients, it was shown that the CRP/albumin ratio is an independent determinant of 28-day mortality in ICU patients, and a higher CRP/albumin ratio is associated with increased mortality in critical patients. In another study evaluating the CRP/albumin ratio as a determinant of in-hospital mortality in geriatric patients presenting to the emergency department, it was found that a high CRP/albumin ratio upon admission to the emergency department is an independent determinant of all-cause in-hospital mortality in patients aged 65 and older [24].
MII indices were initially developed by Gardini et al. [25]. The current ITACa (Italian Trial in Advanced Colorectal Cancer) study demonstrated the usefulness of all MII indices as prognostic markers in patients with metastatic colon cancer. MII allows the evaluation of hematological parameters such as neutrophils, platelets, and lymphocytes, along with the chronic inflammatory marker CRP, enabling a powerful marker for systemic conditions [26]. It has been found to be a strong, simple, and practical marker for early prediction of mortality in COVID-19 patients at high risk of mortality in the ICU [27]. Studies in the literature have also indicated that MII could be an independent determinant in ischemic stroke patients [28]. The results of the current study represent the first demonstration of the independent significance of all MII indices as determinants of mortality in critical geriatric patients. However, given the limitations of the data in the literature, we believe that more studies are needed to evaluate the prognostic importance of both SIRI and all MII indices in critical geriatric patients.
In our study, no relationship was observed between PIV, NLR, PLR, and SII values and mortality. Various studies in the literature can be observed. Recent studies have shown that PIV is being used as an inflammatory marker for various diseases. In the literature, high PIV levels have been indicated to correlate with poor prognosis in cancer patients [6]. A prospective study conducted on 82 sepsis patients in the intensive care unit investigated the relationship between PIV and sepsis; however, no statistically significant relationship was found between mortality and PIV [8]. In a study by Mangalesh et al. [29], NLR, PLR, and SII were shown to be independent determinants of in-hospital mortality in sepsis patients, with SII performing better than both NLR and PLR and the addition of SII to the SOFA score leading to a significant increase in prognostic performance. A total of 5,537 patients were analyzed in a study where sepsis patient data was examined, and a significant relationship between PLR and mortality was observed only in subgroups without vasopressor use and without AKI, or with a SOFA score ≤10 [30]. In a study evaluating decreased cognitive abilities after surgery in elderly patients, an increased SII was found to be independently associated with the presence of high SII levels as a risk factor for decreased cognitive abilities after surgery [31].
4.1. Limitation
There were several limitations to the current study. Firstly, the laboratory data used in the study were collected on the first day of admission to the ICU; therefore, continuous changes could not be analyzed. Secondly, this was a retrospective observational study, and selection bias and confounding bias were inevitable. Lastly, although the data in our study were multicenter, the number of cases was low. This may not be representative of the results. Future, larger, multicenter prospective studies are needed to confirm or refute the findings of this study.
5. Conclusions
In geriatric patients admitted to the ICU, it has been determined that among the scoring systems used in the ICU, the SOFA score and, among the inflammatory markers, the CRP/albumin ratio have the highest predictive ability for 28-day mortality. However, in critically ill geriatric patients, monitoring NLR, SIRI, MII 1-2-3, and CRP/albumin ratios is also important for predicting 28-day mortality. Nevertheless, the effect of PIV, MLR, PLR, and SII values on predicting 28-day mortality could not be demonstrated in the current study. Therefore, we believe that further clinical studies are needed to determine the effects of PIV, MLR, PLR, and SII on short- and long-term prognosis and survival in geriatric patients admitted to the ICU.
Author Contributions
Conceptualization, Ö.Ç. and M.Y.A.; Methodology, A.K. ; Software, Ö.Ç. ; Validation, A.K., A.G. ; Formal Analysis, M.Y.A.; Investigation, Ö.E.Y. ; Resources, A.G. and Ö.Ç. ; Data Curation, A.K. ; Writing – Original Draft Preparation, Ö.Ç. ; Writing – Review & Editing, Ö.Ç. and AK. ; Visualization, M.Y.A.; Supervision, Ö.Ç. ; Project Administration, Ö.Ç. and A.K. ; Funding Acquisition, nobody
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Akdeniz University Faculty of Medicine Ethics Committee (approval number TBAEK-178 and 28.03.2024)
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this work.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available in order to maintain participant privacy.
Acknowledgments
No acknowledgments.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sherrington, C.; Fairhall, N.; Kwok, W.; Wallbank, G.; Tiedemann, A.; Michaleff, Z. A.; Ng, C. A. C. M.; Bauman, A. Evidence on physical activity and falls prevention for people aged 65+ years: systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int J Behav Nutr Phys Act. 2020, 17, 144. [Google Scholar] [CrossRef]
- Flaatten, H.; Beil, M.; Guidet, B. Elderly Patients in the Intensive Care Unit. Semin Respir Crit Care Med. 2021, 42, 10–19. [Google Scholar] [CrossRef]
- Di Rosa, M.; Sabbatinelli, J.; Soraci, L.; Corsonello, A.; Bonfigli, A. R.; Cherubini, A.; Sarzani, R.; Antonicelli, R.; Pelliccioni, G.; Galeazzi, R.; et al. Neutrophil-to-lymphocyte ratio (NLR) predicts mortality in hospitalized geriatric patients independent of the admission diagnosis: a multicenter prospective cohort study. J Transl Med. 2023, 21(1), 835.
- Beniwal, A.; Juneja, D.; Singh, O.; Goel, A.; Singh, A.; Beniwal, H. K. Scoring systems in critically ill: Which one to use in cancer patients? World J Crit Care Med., 2022,11(6), 364–374.
- Celiksoz, A.; Kavak, M.; Tarlacık, A. O. Inflammatory Index as a Predictor of Mortality in Elderly Patients with Intracapsular Femoral Neck Fracture. 2023, Cureus, 15(10), e46318.
- Guven, D. C.; Sahin, T. K.; Erul, E.; Kilickap, S.; Gambichler, T.; Aksoy, S. The Association between the Pan-Immune-Inflammation Value and Cancer Prognosis: A Systematic Review and Meta-Analysis. Cancers (Basel). 2022, 14(11), 2675.
- Yoldas, H.; Karagoz, I.; Ogun, M. N.; Velioglu, Y.; Yildiz, I.; Bilgi, M.; Demirhan, A. Novel Mortality Markers for Critically Ill Patients. J Intensive Care Med. 2020, 35(4), 383–385.
- Turan Y. B. The prognostic importance of the pan-immune-inflammation value in patients with septic shock. BMC Infect Dis. 2024, 24(1), 69.
- Ayrancı, M. K.; Küçükceran, K.; Dundar, Z. D. NLR and CRP to albumin ratio as a predictor of in-hospital mortality in the geriatric ED patients. Am J Emerg Med. 2021, 44, 50–55.
- Zahorec R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001, 102(1), 5–14.
- Le Tulzo, Y.; Pangault, C.; Gacouin, A.; Guilloux, V.; Tribut, O.; Amiot, L.; Tattevin, P.; Thomas, R.; Fauchet R.; Drénou, B. Early circulating lymphocyte apoptosis in human septic shock is associated with poor outcome. Shock. 2002,18(6), 487–494.
- Miniksar, Ö. H.; Kaçmaz, O. The effect of neutrophil-lymphocyte ratio on admission to postoperative intensive care and mortality in elderly patients undergoing hip fracture surgery with spinal anesthesia. The European Research Journal. 2021, 7, 628–634. [Google Scholar] [CrossRef]
- Zhang, P.; Li, Y.; Zhang, H.; Wang, X.; Dong, L.; Yan, Z.; She, L.; Wang, X.; Wei, M.; Tang, C. Prognostic value of the systemic inflammation response index in patients with aneurismal subarachnoid hemorrhage and a Nomogram model construction. Br J Neurosurg. 2023, 37(6), 1560–1566.
- Hu, B.; Yang, X. R.; Xu, Y.; Sun, Y. F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W. M.; Qiu, S. J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014, 20(23), 6212–6222.
- Jomrich, G.; Paireder, M.; Kristo, I.; Baierl, A.; Ilhan-Mutlu, A.; Preusser, M.; Asari, R.; Schoppmann, S. F. High Systemic Immune-Inflammation Index is an Adverse Prognostic Factor for Patients with Gastroesophageal Adenocarcinoma. Ann Surg. 2021, 273(3), 532–541.
- Wang, K.; Diao, F.; Ye, Z.; Zhang, X.; Zhai, E.; Ren, H.; Li, T.; Wu, H.; He, Y.; Cai, S.; et al. Prognostic value of systemic immune-inflammation index in patients with gastric cancer. Chin J Cancer. 2017, 36(1), 75.
- Xie, Q. K.; Chen, P.; Hu, W. M.; Sun, P.; He, W. Z.; Jiang, C.; Kong, P. F.; Liu, S. S.; Chen, H. T.; Yang, Y. Z., et al. The systemic immune-inflammation index is an independent predictor of survival for metastatic colorectal cancer and its association with the lymphocytic response to the tumor. J Transl Med. 2018, 16(1), 273.
- Wang, R. H.; Wen, W. X.; Jiang, Z. P.; Du, Z. P.; Ma, Z. H.; Lu, A. L.; Li, H. P.; Yuan, F.; Wu, S. B.; Guo, J. W.; et al. The clinical value of neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR) and systemic inflammation response index (SIRI) for predicting the occurrence and severity of pneumonia in patients with intracerebral hemorrhage. Front Immunol. 2023, 14, 1115031.
- Thijs, L. G.; Hack, C. E. Time course of cytokine levels in sepsis. Intensive Care Med. 1995, 21 Suppl 2, S258–S263. [Google Scholar] [CrossRef]
- Ho, K. M.; Lee, K. Y.; Dobb, G. J.; Webb, S. A. C-reactive protein concentration as a predictor of in-hospital mortality after ICU discharge: a prospective cohort study. Intensive Care Med. 2008, 34(3), 481–487.
- Artero, A.; Zaragoza, R.; Camarena, J. J.; Sancho, S.; González, R.; Nogueira, J. M. Prognostic factors of mortality in patients with community-acquired bloodstream infection with severe sepsis and septic shock. J Crit Care. 2010, 25(2), 276–281.
- Ranzani, O. T.; Zampieri, F. G.; Forte, D. N.; Azevedo, L. C.; Park, M. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS One. 2013, 8(3), e59321.
- Park, J. E.; Chung, K. S.; Song, J. H.; Kim, S. Y.; Kim, E. Y.; Jung, J. Y.; Kang, Y. A.; Park, M. S.; Kim, Y. S.; Chang, J.; et al. The C-Reactive Protein/Albumin Ratio as a Predictor of Mortality in Critically Ill Patients. J Clin Med. 2018, 7(10), 333.
- Oh, J.; Kim, S. H.; Park, K. N.; Oh, S. H.; Kim, Y. M.; Kim, H. J.; Youn, C. S. High-sensitivity C-reactive protein/albumin ratio as a predictor of in-hospital mortality in older adults admitted to the emergency department. Clin Exp Emerg Med. 2017, 4(1), 19–24.
- Casadei Gardini, A.; Scarpi, E.; Valgiusti, M.; Monti, M.; Ruscelli, S.; Matteucci, L.; Bartolini, G.; Vertogen, B.; Pagan, F.; Rovesti, G.; et al. Prognostic role of a new index (multi inflammatory index) in patients with metastatic colorectal cancer: results from the randomized ITACa trial. Ther Adv Med Oncol. 2020, 12, 1758835920958363.
- Dikici S. Novel Indices for Lumbar Discectomy: Systemic Immune Inflammation Index, Systemic Inflammatory Response Index, Multi Inflammatory Index, and Prognostic Nutrition Index. Turk Neurosurg. 2024, 34(2), 243–249.
- Gozdas, H. T.; Kayis, S. A.; Damarsoy, T.; Ozsari, E.; Turkoglu, M.; Yildiz, I.; Demirhan, A. Multi-inflammatory Index as a Novel Mortality Predictor in Critically Ill COVID-19 Patients. J Intensive Care Med. 2022, 37(11), 1480–1485.
- Demirel, M. E.; Akunal Türel, C. The Role of the Multi-Inflammatory Index as a Novel Predictor of Hospital Mortality in Acute Ischemic Stroke. Cureus. 2023, 15(8), e43258.
- Mangalesh, S.; Dudani, S.; Malik, A. The systemic immune-inflammation index in predicting sepsis mortality. Postgrad Med. 2023, 135(4), 345–351.
- Shen, Y.; Huang, X.; Zhang, W. Platelet-to-lymphocyte ratio as a prognostic predictor of mortality for sepsis: interaction effect with disease severity-a retrospective study. BMJ Open. 2019, 9(1), e022896.
- Lu, W.; Zhang, K.; Chang, X.; Yu, X.; Bian, J. The Association Between Systemic Immune-Inflammation Index and Postoperative Cognitive Decline in Elderly Patients. Clin Interv Aging. 2022, 17, 699–705.
Figure 1.
Study flow chart.
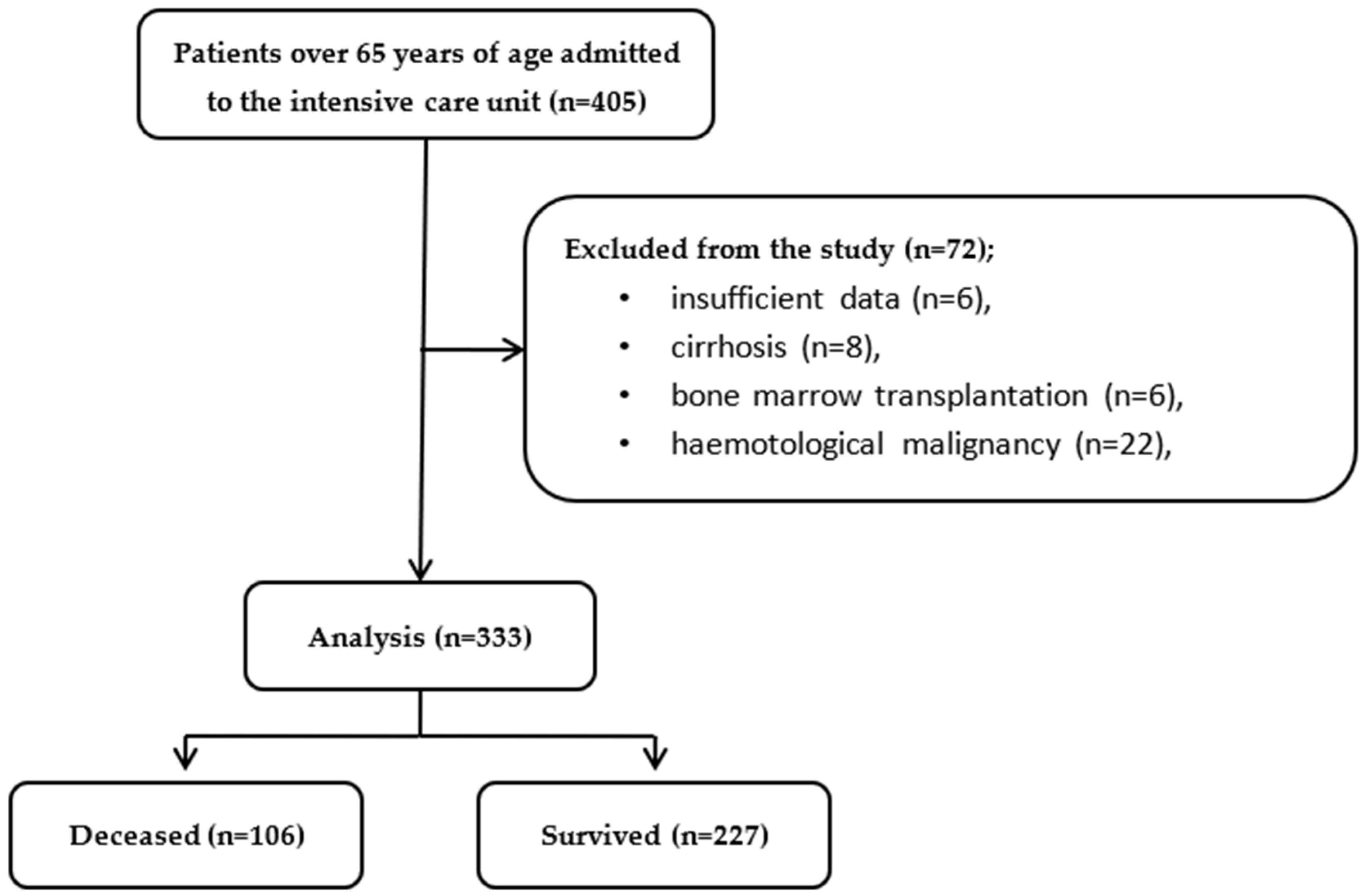
Figure 2.
ROC-Curve of 28-day mortality of inflammatory markers.
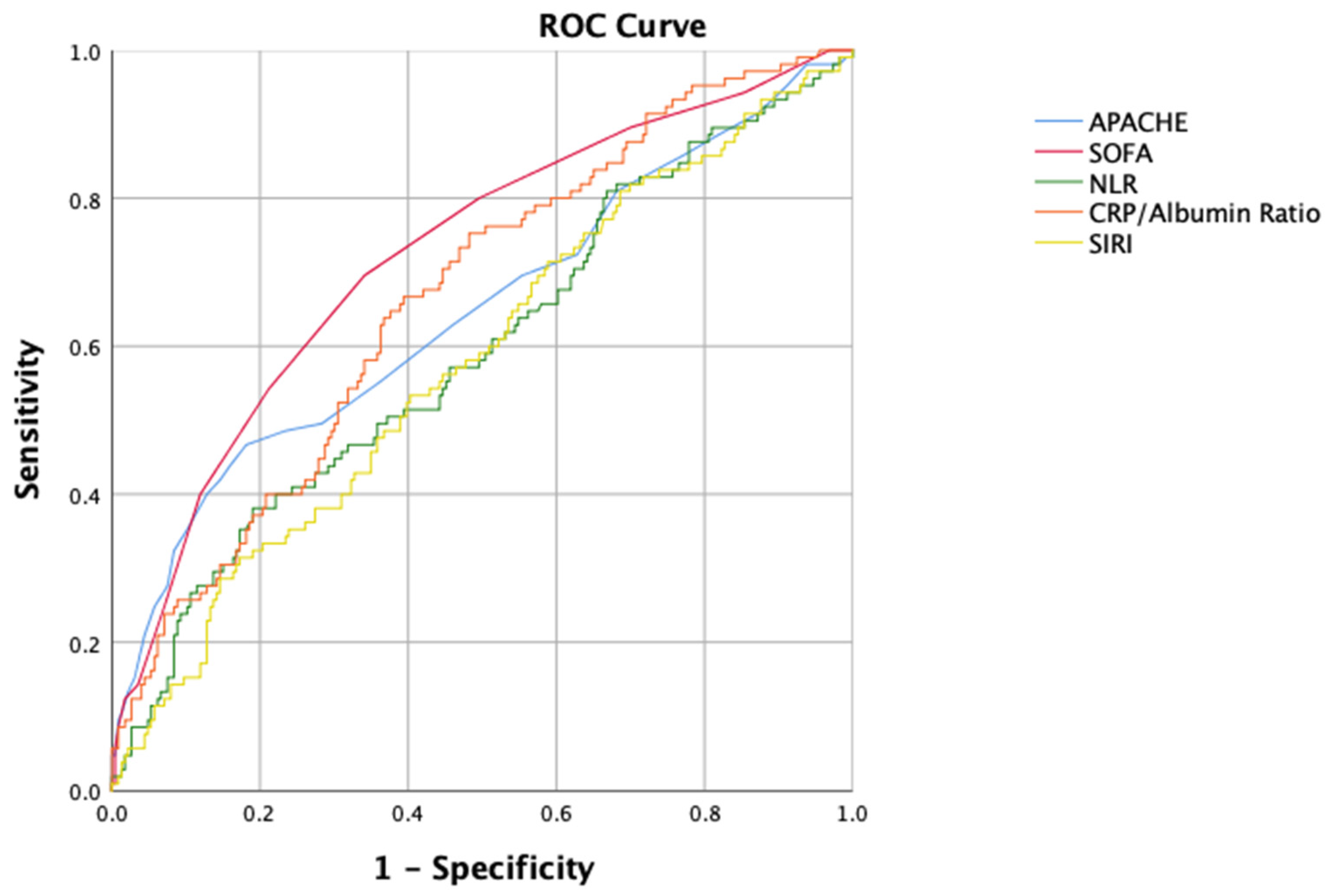

Table 1.
Baseline characteristics of patients according to in-hospital mortality and 28-day mortality [values presented as mean ± standard deviation or number (percentage)].
Table 1.
Baseline characteristics of patients according to in-hospital mortality and 28-day mortality [values presented as mean ± standard deviation or number (percentage)].
| 28-day Mortality | |||
| Deceased (n=106) | Survived (n=227) | p-value | |
| Age, years | 77.2±8.5 | 78.1±8.6 | 0.38 |
| Sex, female | 47 (44.3) | 116 (51.1) | 0.25 |
| Chronic Diseases | |||
| Diabetes mellitus | 43 (40.6) | 86 (37.9) | 0.64 |
| Hypertension | 48 (45.3) | 114 (50.2) | 0.40 |
| Hyperlipidemia | 5 (4.7) | 7 (3.1) | 0.46 |
| Coronary artery disease | 12 (11.3) | 31 (13.7) | 0.55 |
| Atrial fibrillation | 15 (14.2) | 24 (10.6) | 0.34 |
| Chronic kidney disease | 13 (12.3) | 22 (9.7) | 0.48 |
| Pulmonary disease | 19 (17.9) | 46 (20.3) | 0.62 |
| Cerebrovascular disease | 10 (9.4) | 37 (16.3) | 0.94 |
| Multimorbidity | 72 (67.9) | 131 (57.7) | 0.075 |
| Indication of ICU | |||
| Sepsis | 32 (30.2) | 50 (22.0) | 0.11 |
| Acute respiratory failure | 42 (39.6) | 91 (40.1) | 0.94 |
| Acute kidney disease | 12 (11.3) | 16 (7.0) | 0.19 |
| Pancreatitis | 0 | 3 (1.3) | 0.55 |
| Trauma | 1 (0.9) | 7 (3.1) | 0.24 |
| Hepatorenal syndrome | 0 | 1 (0.4) | 0.49 |
| Cardiorenal syndrome | 1 (0.9) | 1 (0.4) | 0.58 |
| Altered conciousness | 24 (22.6) | 40 (17.6) | 0.28 |
| Hemorrhagic shock | 6 (5.7) | 20 (8.8) | 0.32 |
| Postoperative care | 9 (8.5) | 26 (11.5) | 0.41 |
| ICU intensive care unit. | |||
Table 2.
Clinical characteristics of patients in intensive care unit according to 28-day mortality [values presented as median [interquarter range] or number (percentage)].
Table 2.
Clinical characteristics of patients in intensive care unit according to 28-day mortality [values presented as median [interquarter range] or number (percentage)].
| Deceased (n=106) | Survived (n=227) | p-value | |
| Culture growth | 71 (67.0) | 93 (41.0) | <0.001 |
| Steroid use | 71 (67.0) | 87 (38.3) | <0.001 |
| Platelet tx | 13 (12.3) | 15 (6.6) | 0.083 |
| Erythrocyte tx | 48 (45.3) | 86 (37.9) | 0.20 |
| Sepsis in ICU | 64 (60.4) | 107 (47.1) | 0.024 |
| MV before ICU | 26 (24.5) | 14 (6.2) | <0.001 |
| MV in ICU | 64 (60.4) | 16 (7.0) | <0.001 |
| Day of MV | 3.0 [3.0] | 0.0 [2.0] | <0.001 |
| Day of hospitalization | 13.5 [18.3] | 12.0 [12.0] | 0.68 |
| Day of ICU | 7.0 [10.0] | 6.0 [5.0] | 0.016 |
| Daybefore ICU | 1.5 [11.0] | 0.0 [1.0] | <0.001 |
| Dayafter ICU | 0.0 [0.0] | 4.0 [7.0] | <0.001 |
| SOFA score | 6.0 [4.0] | 3.0 [3.0] | <0.001 |
| APACHE-II score | 24.5 [15.3] | 20.0 [8.0] | <0.001 |
| APACHE Acute Physiologic Asessment and Chronic Health, ICU intensive care unit, MV mechanical ventilation, SOFA Sequantial Organ Failure Assessment, tx transfusion. | |||
Table 3.
Inflammatory markers of patients according to 28-day mortality [values presented as median [interquarter range]].
Table 3.
Inflammatory markers of patients according to 28-day mortality [values presented as median [interquarter range]].
| 28-day Mortality | |||
| Deceased (n=106) | Survived (n=227) | p-value | |
| PIV | 1104.3 [2003.4] | 952.0 [1969.8] | 0.47 |
| NLR | 11.6 [20.2] | 9.3 [11.6] | 0.007 |
| MLR | 0.6 [0.6] | 0.5 [0.6] | 0.092 |
| SIRI | 5.8 [11.2] | 4.5 [8.3] | 0.03 |
| PLR | 223.2 [258.8] | 203.5 [240.7] | 0.68 |
| SII | 22.2 [26.6] | 26.7 [29.3] | 0.22 |
| MII1 | 813.8 [2153.1] | 416.3 [1997.1] | <0.001 |
| MII2 | 20182 [46303] | 6993.6 [28048.2] | <0.001 |
| MII3 | 2026.9[4630.6] | 965.5 [3134.3] | 0.006 |
| CRP/Albumin | 4.03 [6.5] | 1.6 [4.7] | <0.001 |
| CRP C-reaktive protein, MII multi-inflamatory index, MLR monocyte-lymphocyte ratio, NLR neutrophil- lymphocyte ratio, PIV pan-immune inflammation, PLR platelet-lymphocyte ratio, SII systemic immune-inflammatory index, SIRI systemic immune response index. | |||
Table 4.
Cox regression analysis of inflammatory markers of the patients related to28-day mortality (univariate analysis, enter method).
Table 4.
Cox regression analysis of inflammatory markers of the patients related to28-day mortality (univariate analysis, enter method).
| Hazard Ratio | 95% CI | p-value | |
| NLR | 1.022 | 1.006 to 1.038 | 0.007 |
| MLR | 1.267 | 0.891 to 1.801 | 0.19 |
| SIRI | 1.023 | 1.000 to 1.047 | 0.049 |
| MII1 | 1.0 | 1.0 to 1.0 | 0.32 |
| MII2 | 1.0 | 1.0 to 1.0 | 0.37 |
| MII3 | 1.0 | 1.0 to 1.0 | 0.14 |
| CRP/Albumin | 1.154 | 1.086 to 1.226 | <0.001 |
| CRP C-reaktive protein, MII multi-inflamatory index, MLR monocyte-lymphocyte ratio, NLR neutrophil- lymphocyte ratio, SIRI systemic immune response index. | |||
Table 5.
ROC-Curve analysis of the possible predictors of 28-day mortality.
| Cut-off | Sensitivity | Specifity | AUC | 95% CI | p-value | |
| APACHE | 21.5 | 59.0 | 58.8 | 0.647 | 0.579 to 0.714 | <0.001 |
| SOFA | 4.5 | 69.5 | 65.9 | 0.723 | 0.663 to 0.783 | <0.001 |
| NLR | 7.79 | 61.9 | 46.9 | 0.593 | 0.526 to 0.660 | 0.006 |
| SIRI | 5.00 | 56.2 | 54.9 | 0.580 | 0.514 to 0.646 | 0.019 |
| CRP/Albumin | 2.15 | 70.5 | 55.3 | 0.665 | 0.604 to 0.726 | <0.001 |
|
APACHE Acute Physiologic Asessment and Chronic Health, CRP C-reaktive protein, NLR neutrophil- lymphocyte ratio, SIRI systemic immune response index, SOFA Sequantial Organ Failure Assessment. | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



