
Submitted:
22 May 2024
Posted:
23 May 2024
You are already at the latest version
Abstract
Purpose: Proximal Femur Fractures (PFFs) in elder patients lead to decreased productivity. Skilled nursing facilities (SNFs) and inpatient rehabilitation facilities (IRFs) are non-home destinations for post-discharge disposition. This study aims to evaluate the loss of independence (LOI) following PFFs and examine the economic impact it entails. Method: Literature from various databases was collected and analyzed retrospectively. The inclusion criteria included patients age >18 years and articles published after 1990. All studies were screened and a PRISMA chart was used to demonstrate the search process. 24 studies were finally used for review. Results: LOI following PFFs significantly increases with age. Fractures in geriatrics avail a significant amount of post-care resources and had longer lengths of stay. Furthermore, six pre-operative risk factors were identified for non-home disposition including age >75, female, non-Caucasian race, Medicare status, prior depression, Charlson Comorbidity Index. Patients discharged directly to home have lower total cost compared to those discharged to rehabilitation units. Loss of independence increases with advancing age. Discussion: PFFs can lead to serious loss of independence among elderly patients with direct impact on economic, social, psychological aspects and the healthcare system.
Keywords:
Loss of independence
; proximal femur fracture
; geriatric patients
; frailty measures
; Disposition
; Economic Impacts
; Psychological Impacts
Introduction:
Proximal femur fractures (PFF) are common injuries among elderly patients.[1] The etiology of PFF in orthopedic patients varies between age groups, with geriatric patients tending to suffer from increased risk of falls, frailty, more co-morbidities, and osteoporosis.[2] More than one million fractures of the proximal femur occur worldwide every year, with more than 90% of cases occurring in patients over the age of 50 years.[3,4] Furthermore, it has been predicted that the total worldwide number of femur fractures will exceed 3.94 million in 2025 and 6.26 million in 2050 due to increased longevity and the aging Baby Boomer population.[2,3]
The outcomes of PFF impact patients in various ways, ranging from the loss of productivity, depressive symptoms, and contribution to higher mortality rates.[4] In recent studies, it has been shown that 1 out of every 6 geriatric patient’s needs to permanently move to a nursing facility following a PFF due to serious loss of independence (LOI), defined as the loss of function and ability to live independently, and the need for external care.[2,5]
The management of proximal femur fractures entails a large socioeconomic burden as major costs can result from impaired functional recovery, which leads to the need for prolonged, and expensive, care in inpatient rehabilitation facilities (IRFs) and skilled nursing facilities (SNFs). [6] Chandra et al. found that long-term hospital care, IRFs, and SNFs were the fastest-growing major spending category from 1994–2009.[7] The direct cost for healthcare from resulting loss of independence in the first six months post-injury has been shown to be as high as $23,000 per isolated limb fracture in the United States.[8]. Hip fractures figure is projected to rise to 6.26 million by 2050 with 3.25 million of these in Asia which is an alarming issue for modern medicine. [9]
The objective of this study is to evaluate loss of independence following proximal femur fractures in orthopedic patients and to examine the economic impact it entails.
Materials and Methods:
For this retrospective study PubMed, Science Direct, Cochrane and Google Scholar were used to obtain literature on loss of independence and proximal femur fractures from 1990 till August 2023. Reference lists of chosen publications were also searched to collect a wide pool of data. MeSH terms used included “loss of independence”, “proximal femur fracture”, “geriatric patients”, “frailty measures”, “disposition”, “economic impacts” and “psychological impacts”. This study was exempt from institutional board review approval.
The inclusion criteria included patients aged >=18 years, gender, economic impact, those living at home with family member or caretaker or living alone or at rehabilitation center at the time of injury, nutritional status, co-morbidities, length of hospital stay, loss of independence, mental health (pre-operatively as well as post-operatively), mode of deposition with any kind of proximal femur fracture. In addition, both qualitative and quantitative studies were included.
The exclusion criteria include patients who died during hospitalization, who didn’t give consent for selected study, those transferred to other hospitals due to complications, those with incomplete medical records, types of fracture sustained, histologically confirmed pathological, benign and malignant fractures, studies that did not include age of the patients, economic impact, prior surgical interventions; medication used prior fracture, disposition information after surgery.
In addition, two authors screened the abstracts independently while being guided by the exclusion and inclusion criteria. The third and fourth author retrieved the full text if found eligible and resolved the conflicts in order to decrease bias. After discussion all the authors reached to a consensus.
In order to select relevant studies, screening of abstracts was conducted that returned 43 publications with 26 publications identified through a search from the primary articles reference lists. After accounting with the exclusion and inclusions criteria, 24 studies in total were included for this study. Approximately 35 minutes was spent on the review of each article. Lastly, a 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram was utilized to demonstrate the search process.[10] (Figure 1).
Results:
Study Characteristics
The average age of the patients was 69.16 years, with most studies focusing on geriatric patients (>65 years and old). Article publication dates ranged from 1990 - August 2023. The sample size of the studies identified ranged from 9-250000 per study. Due to focusing more on the surgical complications of fractures, research regarding the loss of independence following proximal femur fracture and the economic impacts resulting has been very limited.
Prevalence
Berian et al. conducted a study that included 5077 patients. They concluded that loss of independence significantly increased with age. It occurred in 49.9% of the patients aged 65 to 74 years, 67.3% aged 75 to 84 years, and 83.9% in patients aged 85 years and older. Care needs were observed in 46.0% patients with almost 30% requiring additional skilled services and 18.2% requiring complete discharge to a destination other than home.[5] Patients experiencing LOI were found to be older and sicker; patients 85 years and older experienced a 4.4-fold increased risk for LOI compared with patients aged 65 to 74 years.[5] Furthermore, a study conducted by Van Der Vliet QMJ et al. included 1074 long bone fracture patients over the age of 65. Almost 878 patients were discharged to 207 various rehabilitation facilities (acute rehabilitation or subacute rehabilitation/skilled nursing facility) and were observed for length of stay (LOS) during their interval at rehabilitation facilities.[11] They concluded that geriatric patients following fractures avail a significant amount of post care resources and longer LOS. Different factors such as pre-injury ambulatory aid, pre-existing immobility also influenced their LOS.
Assessment of everyday activities can be measured by Katz Index of Activities of Daily Living (ADL), a short questionnaire that is utilized to determine an older adult’s level of dependency and whether they need additional care.[12] The measures of functional status include evaluation of transferring, dressing, making meals, and toileting as recommended by the American College of Surgeons National Surgical Quality Improvement Program. This assessment also identifies elderly adults who are more at risk of functional decline and may benefit from supplemental aid.[12] Kugelman et al. found that over a quarter of the participants who had a lateral compression type 1 (LC1) pelvic fracture continue to use an aid at long term for ambulation.[13] Similarly, they also found that older age and other factors were found to be associated with the need for extra assistance.
Keswani A. et al. analyzed 106,360 total joint arthroplasty patients (TJA). They aimed to compare the risks of post discharge adverse events in TJA patients in regard to discharge destination. They found that the most common discharge destinations included home (70%), skilled nursing facility (19%), and inpatient rehabilitation facility (11%). Based on the adverse events, they identified that IRFs and SNFs were associated with higher risk as compare to home discharge.[14] Furthermore, a study conducted by Rondon et al. investigated 43 variables, in which 6 were found to be crucial pre- operative risk factors for discharge disposition other than home. Among these 6 variables, age 75 or greater was found as a significant predictor for patients going to IRFs. Other variables included female gender, non-Caucasian race, Medicare status, history of depression, and Charlson Comorbidity Index were also an important determinant for nonhome disposition. In addition, any complication during hospitalization led to a higher chance of the patient being discharged to IRF and SNF.[15] Franz Muller et al. study in population in 10th decade of life reflects that the occurrence of proximal femoral fractures results in high postoperative mortality just within the first 6 months (nearly 50%). [16] Another study in population above 100 years by J. Moore et.al suggests that the inpatient cost of treating hip fractures in centenarians was 18% above that of hip fractures of any age with expected mortality of 71% within 1 year of surgery. [17]
Patient Demographics and Risk Factors
Risk factors for poor recovery that can lead to the need for additional assistant include frailty, advancing age, female gender, functional disability, and cognitive impairment. Poor preoperative activity has been a crucial risk factor of impaired postoperative function. Further, delay in timely , proper and appropriate surgical intervention for PFF management i.e taking >24 hours, lack of proper coordination with multi-disciplinary team and lack of proper physiotherapy postoperatively have a direct impact in returning to independence, early mobility and pre fracture living status. Poor mental well-being pre surgery as well as post-surgery may also contribute to poor functional activity.[12] Elderly patients who sustain orthopedic trauma are at increased risks of sustaining a fracture due to increased vulnerability resulting from age-related decline in reserve and function across many physiological systems such as ability to cope everyday stressors. This is due to many aspects such as poor bone quality and low-energy mechanisms.[13] Studies examining discharge to nonhome destinations have recognized that frailty significantly increases the risk by 1.5 to a 20-fold.[5,12].
Female predominance was more in most of the papers. According to Tim Chesser et.al hip fracture will occur in 1 in 3 women and 1 in 7 men over the age of 50. [9] In support of this, Nicola Veronese et. al. study showed that worldwide hip fractures occurred in 18% of women and 6% in men.[18] With advancing age one third of women in 80 ‘s will have hip fracture, with white women predominance living at higher altitude.[18] Van Der Vliet et.al study showed that higher Charlson Comorbidity Index (CCI) (P=0.048), male sex (P<0.001) and pre-injury use of an ambulatory device (P = 0.006) were associated with longer hospital stay which increases the post-operative complications as well as mortality rate. [11] A. Morice study showed that Mini Nutritional Assessment (MNA) (range: 2-12) score was 7.46±2.23 with no association to 3 months mortality whether patient is living at home or not (p<0.08). [19]
Deposition after Discharge:
The mode of deposition also played a significant role in overall outcome and progress in an individual post-operatively. Studied have reflected that home-based rehabilitation have a significantly better outcome and rapid gain in pre fracture state as compared to institutionalized rehabilitation. Home based rehabilitation have multiple benefit over institutionalized rehabilitation i.e., gain in mobility, functional ability, decrease in length of hospital stay, decrease in cost and lower rate of complications. Lavernia CJ et.al study reflects that the total costs were significantly lower in patients discharged directly to home was lower vs those sent to the institutional rehabilitation center ($2405 V/S $13435 with p <0.001). [20] Rehabilitation in the 85+ age group was found to be less effective as compared to the age group <84. [21]
Economic Impact:
In a study conducted on orthopedic patients needing total knee arthroplasty (TKA), Rondon et al. found that orthopedic surgeries have become a global massive financial burden. They established that as much as 36% of TKA related expenses occur in the post-operative period, of which 70% represent expenses related to post-acute care facilities. Recently many other studies have consistently shown that IRF stays are still very costly.[14] Lavernia et al. compared patients with primary arthroplasty surgeries and post-discharge economic impact between comprehensive rehabilitation units (CRU) with subsequent home care (HC) and those who returned home with limited care needed. According to their study, total cost was significantly lower in patients discharged directly to home compared to those who were sent to CRU and subsequently received HC ($2,405 vs $13,435, p <0.001). They reported that this results in an annual cost of $3.2 billion for post-surgical rehabilitation after arthroplasty.[20] Although this data represents the population undergoing TKA, the economic impact can be applied to those with a PFF in need of extended rehabilitation and home care. Furthermore, the percentage of patients in need of this extended care is higher in those with a PFF, amplifying the economic impact. In a study by J. Moore et.al suggest that the average inpatient cost of treating hip fractures in centenarians was 18% above that of hip fractures of any age i.e., €14,898 in Ireland. [17] Kyle T et.al. explains the impact of early intervention for hip fracture on total cost i.e., the average cost of the early intervention was $49,900 & the average cost of late intervention was $65,300 (p= 0.0086). [22] Adding more, study conducted by Ian D Cameron et.al on PFF showed that the total cost was approximately A$ 10,600 for accelerated rehabilitation and A$ 12,800 for conventional care (p value=0.186). With the reduction in length of hospital stay, the post-surgical component was markedly reduced for the accelerated rehabilitation group (A$6420 v/s A$ 8870(p value= 0.138). [23] Further Nicola Veronese et.al study gives us an idea about increase in trend of incidence of hip fracture globally and cost required for long term care (LTC) facility which is estimated between 6% and 60% of people suffering from hip fracture, with cost ranging from $19,000 to $66,000. [18] Kyosuke Fukuda et.al. study from showed that Japan’s long-term care insurance system that allow elderly people to receive appropriate support in their daily living according to their level of independence and physical and mental functions which is not present in developed country of world.[24] Comparing studies from developed to developing country the study of Kyle T. Judd et.al based in USA showed the average cost of the early intervention per patient was $49,900 and the average cost of late intervention per patient was $65,300 (p= 0.0086) [25] while R. Aigner et.al. study based in India showed that the mean total acute care costs per patient was 8853 € ± 5676 €.[26] These two studies reveals that the average cost of treatment in USA is 6 to 8 folds higher as compared to Indian treatment cost. Furthermore, reoperation in acute care of PFF patient was associated with 31% higher rate than the corresponding cost of the primary operation and according to Tiihonen, reoperation was primarily occurring during the first year of initial procedure. [27] So, high treatment cost for PFF management will be an economic burden to the developed country in near future.
Social and Psychological Impact:
Morice et.al study in centerians showed 36% dementia in patient undergoing surgery for PFF. [19] In another study by Tim Chesser et.al on hip fracture provides us the evidence that 30% patients have dementia prior surgery and another 20 % have impaired cognitive function following hip fracture episode [9]. Further, study by Franz Muller et.al on population on their 10th decade of life showed that dementia was present in 60% patient prior surgery who landed up in nursing home for rehabilitation. [16] Most of the patient having dementia and cognitive impairment pre or post PFF surgery significantly guide the health professional for appropriate selection of mode of deposition after discharge from hospital.[28] Thus having dementia and some sorts of cognitive impairment will eventually increase the cost of total treatment process.
Loss of Workdays:
Andrea Giusti et.al study reflects that during the follow-up, both groups showed a significant decline of functional ability (Barthel Index). Home based rehabilitation (HBR) group had higher Barthel Index scores than the Institutional Based Rehabilitation (IBR) group at follow-up (p value= 0.007). Barthel Index score decreased 10.8% for the HBR group from the pre-fracture level (85.5 +/-23.4) to 12 months (76.2+/- 32.1) and decreased 25.6% for the IBR group from the pre-fracture level (82.4 +/-22.6) to 12 months (58.92+/- 33.3).[25] Another study by Kyosuke Fukuda et.al. highlights the relation of the staying with co-residents or family members and walking ability after 1 week of PFF surgery i.e., Barthel Index at discharge of Home group v/s Hospital referred group (75.6 ± 22.7 )v/s(58.0 ± 24.6), p value<0.01,odds ratios are walking ability one week after surgery 1.9, p <o.o5,staying with Co-residents 4.6, p < o.o1.[24] Suguru Ohsawa et.al study suggest that all the patients in the assertive rehabilitation group recovered their ability to walk (FIM score) to some extent, while those in the conventional group did not. Ambulationd (FIM): Assertive method (18.29+/-7.9) v/s Conventional method (9.49+/-4.3, p- value=0.00135). The 6 months follow-up, the FIM score was significantly higher in the patients treated with assertive rehabilitation (p value=0.0135) which reflects the gain of independence following surgery by the patients. [29] Jean Taillandier et.al study reflects that loss of weight bearing and advancing age were the key factor for longer hospital stay and reason for institutionalization. After 1 year, only 36.6% of the patients had the same level of self-sufficiency as before the fracture. [30] Apart from this, Till Berk et.al study suggest that higher BS (Braden Score) increased the odds of developing decubitus by 6.2 times (95% CI 1.5 to 25.7, p < 0.001) which will limit the daily activities significantly. [31] Additionally Tim Chesser et.al papers emphasize on weight bearing without restriction in the immediate postoperative period and initiation of physiotherapy on the day after surgery unless contraindicated for better functional gain and mobility following PFF surgery.[9] (Table 1)
Discussion:
The management of elderly patients who sustain orthopedic fractures is an increasingly relevant topic in current practice. Due to the elderly population growing rapidly in recent years, a larger number of patients are more susceptible to fractures and loss of independence.[5,12] This narrative review aimed to evaluate loss of independence following proximal femur fractures in orthopedic patients as well as examine its economic impact. Proximal femur fractures are known to be a highly prevalent injury in the geriatric population, hence necessitating the understanding of loss of independence ensuing and its financial impact. There is also a major physical impact on the patient, including loss of physical activity and feelings of anxiety and depression. Loss of independence encompasses the inability to perform tasks necessary for survival, personal care such as ADLs, and additional aid with physical activity either at home or in an inpatient rehabilitation facility or skilled nursing facilities.[12]
This study demonstrates that PFF has hefty costs associated with surgery, with a large portion needing expensive post-operative care in rehabilitation facilities and nursing facilities due to loss of functional independence.[15] Patients have even reported selling possessions to pay for expenses incurred during surgery and care needed at rehabilitation facilities, with others having to reach out to friends and family as a source of financial aid.[31] Patients losing independence also resulted in the ability to work or sustain a job, exponentially increasing their financial burden. Proximal femur fractures also place a patient at a higher risk of sustaining another fracture later as well as increases the chances of other infections in early stage of recovery. Beside this, in later days it worsen the pre-existing morbid condition leading to increase in rate of morbidity and mortality mostly within 3 – 6 months of surgical interventions which have a direct impact in creating additional costs to the individual.[32] Also, hospital acquired conditions following the orthopedic procedures also contribute to the length of stay and the postoperative disposition to the rehabilitation centers. [33]
There is a significant difference in the overall cost of management of PFF in developed country as compared to developing ones. Few studies have shown that the average cost of treatment in overall management of PFF in developed country is 6-8 folds higher as compared to developing one. This reflects that the proportional increase in cost of management of PFF in developed country will be a burden in near future. [24,34] The cost is higher due to longer hospital stay which accounts for nearly one third of total cost of treatment. [34] Further, rapid intervention for fracture management significantly decreases the burden of higher expense in treatment. Adding more the site of fracture, severity of fracture and the Charlson Comorbidity Score plays a pivotal role in increasing the cost during the fracture management. Adding more to it, cognitive impairment also has a significant role in increasing the acute care costs. [24,34] Also, according to few studies, level of trauma centers plays a significant role in the timing of intervention that impacts the disposition and recovery period for these fractured population. [35,36]
These findings may be best interpreted by considering loss of independence and the need for discharge to a faculty other than home. Previously, it was very common for patients to be discharged to IRFs following surgery due to the safety and assistance they would receive from the staff.[12,15] This notion has recently changed, as surgeons routinely opt against sending their patients IRFs after surgery due to the increased costs. This creates a fine line of balancing patient needs and safety with increased cost, necessitating a proper analysis of who truly needs this extra care. Additionally, this brings increased attention to “why” some patients experience loss of independence what can be done to prevent this and increase self-motivation among patients. There is a significant gain of functional ability in those population whose disposition is directly to their home or with their loved ones as compared to those population whose disposition is in nursing home setup or institutional rehabilitation center. [14,23,32] Studies have shown that loss of independence following surgical management of PFF is greater in advancing age population. [5,13,34] Thus the importance and need of regular, proper, adequate and timely physiotherapy in rapid gain in pre-fracture independence state is in increasing trend. [32,37] Future studies should examine these variables and attempt to create risk assessment and stratification tools that may better optimize patients prior to surgery.
This study did have its limitations. We acknowledge that our inclusion and exclusion criteria prevented assessment of the financial and physical burdens of proximal femur fractures and loss of independence in other countries. In this narrative review, various heterogenous studies were included and hence bias of each study was also incorporated. Like other narrative reviews, this study also lacked the explicit criteria for the article selection and hence there was no evaluation of selected articles for validity. Moreover, the included studies in his review were retrospective in nature, so we don’t have a consistent measure of frailty.
Conclusion:
Proximal femur fractures are highly prevalent, with incidence steadily increasing as the Baby Boomer population ages. Female gender, advancing age, white population, co-existing morbidities, lack of proper care, post-operative infections, limitation in mobility following surgery, impaired cognitive function following surgery are the factors which contributes to decline in the rate of appropriate recovery following surgery. These fractures can lead to serious loss of independence among elderly patients and, therefore, could necessitate permanent residence in a nursing facility (IRFs and SNFs). In addition, PFFs have a considerable economic impact on the patient and healthcare system. These findings are crucial and should prompt further investigation into risk factors for loss of independence, as well as discussion with orthopedic patients prior to surgery.
Author Contributions
Study conception and design: HAM, AP, AS, KJS; acquisition, analysis, and interpretation of the data: All Authors; drafting of the manuscript: All Authors; critical revision of the manuscript for important intellectual content: HAM, AP, AS, KJS.; statistical analysis: HAM; study supervision: AS, KJS and AP. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgements
There are no acknowledgements for this review.
Conflicts of Interest
The authors declare that there are no conflicts of interest to disclose and there are no financial or non-financial interests related to the work submitted.
References
- Backer HC, Wu CH, Maniglio M, Wittekindt S, Hardt S, Perka C. Epidemiology of proximal femoral fractures. J Clin Orthop Trauma. 2021;12(1):161-5. [CrossRef]
- Becker N, Hafner T, Pishnamaz M, Hildebrand F, Kobbe P. Patient-specific risk factors for adverse outcomes following geriatric proximal femur fractures. Eur J Trauma Emerg Surg. 2022;48(2):753-61. [CrossRef]
- Mosquera MT, Maurel DL, Pavon S, Arregui A, Moreno C, Vazquez J. [Incidence and risk factors in fractures of the proximal femur due to osteoporosis]. Rev Panam Salud Publica. 1998;3(4):211-9.
- Mittal R, Banerjee S. Proximal femoral fractures: Principles of management and review of literature. J Clin Orthop Trauma. 2012;3(1):15-23. [CrossRef]
- Berian JR, Mohanty S, Ko CY, Rosenthal RA, Robinson TN. Association of Loss of Independence With Readmission and Death After Discharge in Older Patients After Surgical Procedures. JAMA Surg. 2016;151(9):e161689.
- Stoicea N, Magal S, Kim JK, Bai M, Rogers B, Bergese SD. Post-acute Transitional Journey: Caring for Orthopedic Surgery Patients in the United States. Front Med (Lausanne). 2018;5:342. [CrossRef]
- Chandra A, Dalton MA, Holmes J. Large increases in spending on postacute care in Medicare point to the potential for cost savings in these settings. Health Aff (Millwood). 2013;32(5):864-72. [CrossRef]
- Ekegren CL, Edwards ER, de Steiger R, Gabbe BJ. Incidence, Costs and Predictors of Non-Union, Delayed Union and Mal-Union Following Long Bone Fracture. Int J Environ Res Public Health. 2018;15(12). [CrossRef]
- Chesser T, Kelly M. Management of hip fractures in the elderly. Vol. 31, Surgery (United Kingdom). Elsevier Ltd.; 2013. p. 456–9. [CrossRef]
- Preferred Reorting Items for Systematic Reviews and Meta-Analysis (PRISMA). https://www.prisma-statement.
- Van Der Vliet QMJ, Weaver MJ, Heil K, McTague MF, Heng M. Factors for Increased Hospital Stay and Utilization of Post -Acute Care Facilities in Geriatric Orthopaedic Fracture Patients. Arch Bone Jt Surg. 2021;9(1):70-8.
- Brinson Z, Tang VL, Finlayson E. Postoperative Functional Outcomes in Older Adults. Curr Surg Rep. 2016;4(6). [CrossRef]
- Kugelman DN, Fisher N, Konda SR, Egol KA. Loss of Ambulatory Independence Following Low-Energy Pelvic Ring Fractures. Geriatr Orthop Surg Rehabil. 2019;10:2151459319878101. [CrossRef]
- Keswani A, Tasi MC, Fields A, Lovy AJ, Moucha CS, Bozic KJ. Discharge Destination After Total Joint Arthroplasty: An Analysis of Postdischarge Outcomes, Placement Risk Factors, and Recent Trends. J Arthroplasty. 2016;31(6):1155-62. [CrossRef]
- Rondon AJ, Tan TL, Greenky MR, Goswami K, Shohat N, Phillips JL, et al. Who Goes to Inpatient Rehabilitation or Skilled Nursing Facilities Unexpectedly Following Total Knee Arthroplasty? J Arthroplasty. 2018;33(5):1348-51 e1.
- Müller F, Galler M, Zellner M, Bäuml C, Füchtmeier B. The fate of proximal femoral fractures in the 10th decade of life: An analysis of 117 consecutive patients. Injury. 2015 Oct 1;46(10):1983–7. [CrossRef]
- Moore J, Carmody O, Carey B, Harty JA, Reidy D. The cost and mortality of hip fractures in centenarians. Ir J Med Sci. 2017 Nov 1;186(4):961–4. [CrossRef]
- Veronese N, Maggi S. Epidemiology and social costs of hip fracture. Injury. 2018 Aug 1;49(8):1458–60. [CrossRef]
- Morice A, Reina N, Gracia G, Bonnevialle P, Laffosse JM, Wytrykowski K, et al. Proximal femoral fractures in centenarians. A retrospective analysis of 39 patients. Orthopaedics and Traumatology: Surgery and Research. 2017 Feb 1;103(1):9–13.
- Lavernia CJ, D’Apuzzo MR, Hernandez VH, Lee DJ, Rossi MD. Postdischarge costs in arthroplasty surgery. J Arthroplasty. 2006;21(6 Suppl 2):144-50.
- Lieberman D, Lieberman D. Rehabilitation after proximal femur fracture surgery in the oldest old. Arch Phys Med Rehabil. 2002;83(10):1360–3.
- Kyle T. Judd, Eric Christianson. Expedited Operative Care Of Hip Fractures Results In Significantly Lower Cost Of Treatment. Iowa Orthop J. 2015; 35: 62–64.
- Cameron ID, Lyle DM, Qujnb’ S. 2Epidemiology and Health Services Evaluation Branch, N.S.W. Health Department, Locked Bag 961. Vol. 47, J Cttn Epidemiol. 1994.
- Fukuda K, Amari T, Yoshino K, Izumiya H, Yamaguchi K. Influence of patients’ walking ability at one-week post-proximal femur fracture surgery on the choice of discharge destination in Japan. [CrossRef]
- Giusti A, Barone A, Oliveri M, Pizzonia M, Razzano M, Palummeri E, et al. An Analysis of the Feasibility of Home Rehabilitation Among Elderly People With Proximal Femoral Fractures. Arch Phys Med Rehabil. 2006 Jun;87(6):826–31. [CrossRef]
- Aigner R, Meier Fedeler T, Eschbach D, Hack J, Bliemel C, Ruchholtz S, et al. Patient factors associated with increased acute care costs of hip fractures: a detailed analysis of 402 patients. Arch Osteoporos. 2016 Dec 1;11(1). [CrossRef]
- Tiihonen R, Alaranta R, Helkamaa T, Nurmi-Lüthje I, Kaukonen JP, Lüthje P. A 10-Year Retrospective Study of 490 Hip Fracture Patients: Reoperations, Direct Medical Costs, and Survival. Scandinavian Journal of Surgery. 2019 Jun 1;108(2):178–84. [CrossRef]
- Singaram S, Naidoo M. The physical, psychological and social impact of long bone fractures on adults: A review. Afr J Prim Health Care Fam Med. 2019;11(1):e1-e9. [CrossRef]
- Ohsawa S, Miura A, Yagyu M, Oizumi A, Yamada E. Asserive rehabilitation for intracapsular fracture of the proximal femur. Clin Rehabil. 2007 Jan;21(1):36–40.
- Taillandier J, Langue F, Alemanni M, Taillandier-Heriche E. Mortality and functional outcomes of pelvic insufficiency fractures in older patients. Joint Bone Spine. 2003;70(4):287–9. [CrossRef]
- Berk T, Thalmann M, Jensen KO, Schwarzenberg P, Jukema GN, Pape HC, Halvachizadeh S. Implementation of a novel nursing assessment tool in geriatric trauma patients with proximal femur fractures. PLoS One. 2023 Jun 9;18(6):e0284320. [CrossRef] [PubMed]
- Amling M, Oheim R, Barvencik F. A holistic hip fracture approach: Individualized diagnosis and treatment after surgery. Vol. 40, European Journal of Trauma and Emergency Surgery. Springer Science and Business Media Deutschland GmbH; 2014. p. 265–71. [CrossRef]
- Pearl A, Crespi Z, Ismail A, Daher M, Hasan A, Awad M, Maqsood H, Saleh KJ. Hospital Acquired Conditions Following Spinal Surgery: Epidemiology and Risk Factors. Frontiers in Medicine and Health Research (FMHR-5-122, Vol 5(2);1-7. [CrossRef]
- Schurch MA, Rizzoli IR, Mermillod B, Vasey H, Michel JP, Bonjour JP. A Prospective Study on Socioeconomic Aspects of Fracture of the Proximal Femur. Vol. II, JOURNAL OF BONE AND MINERAL RESEARCH. Blackwell Science, Inc; 1996. [CrossRef]
- Gleich J, Neuerburg C, Schoeneberg C, Knobe M, Böcker W, Rascher K, et al. Time to surgery after proximal femur fracture in geriatric patients depends on hospital size and provided level of care: analysis of the Registry for Geriatric Trauma (ATR-DGU). European Journal of Trauma and Emergency Surgery. 2023. [CrossRef]
- Simunovic N, Devereaux PJ, Bhandari M. Surgery for hip fractures: Does surgical delay affect outcomes. Indian J Orthop. 2011 Jan;45(1):27–32. [CrossRef]
- Tiwari N, Patil S, Popalbhat R. Efficacy of Physiotherapy Rehabilitation for Proximal Femur Fracture. Cureus. 2022 Oct 26. [CrossRef]
Figure 1.
PRISMA FLOWCHART of the included studies:.
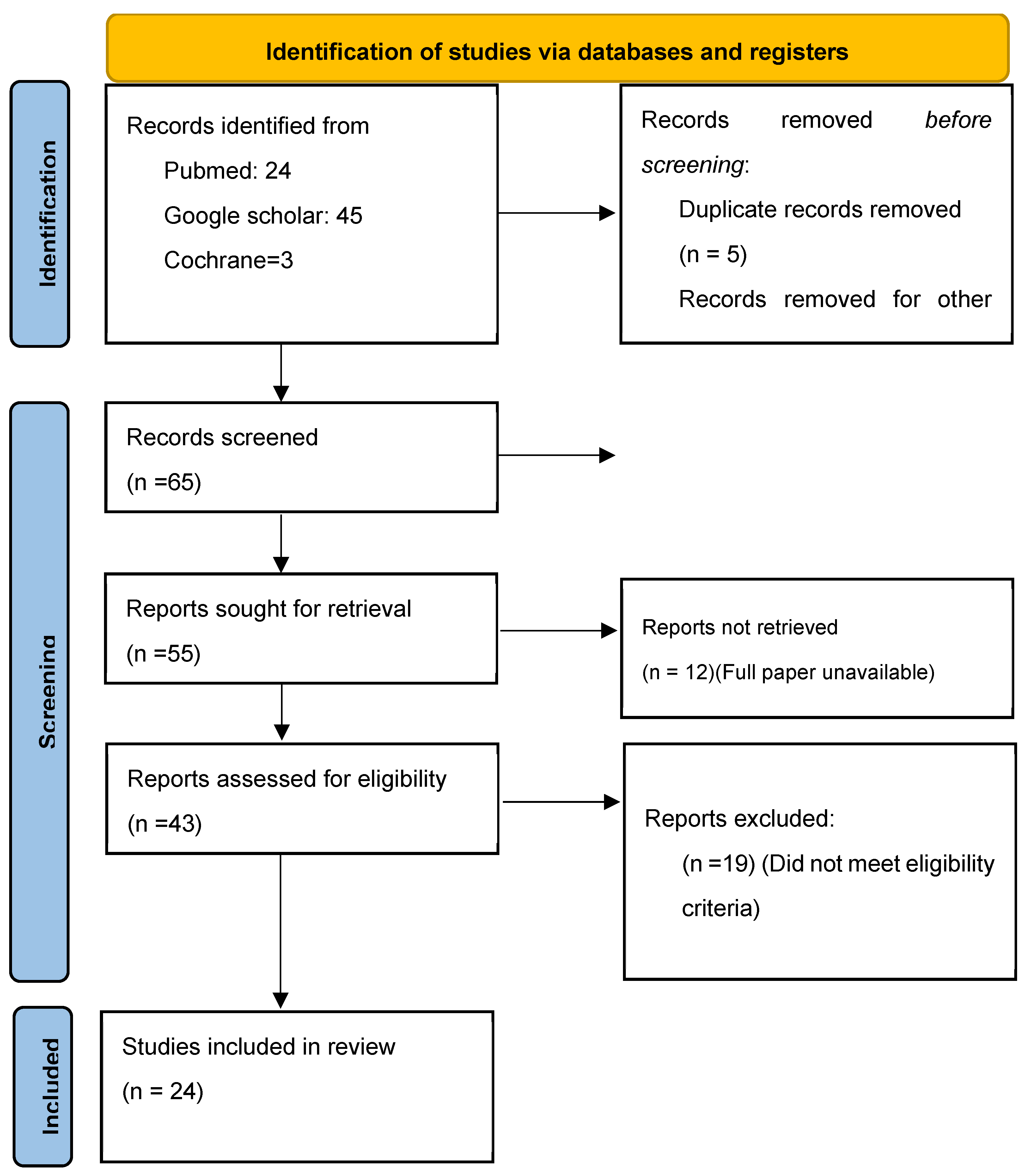

Table 1.
Summary of Studies included for Proximal Femur Fractures and Significant Outcomes.
| # | Article author name | Year of Publication | # patients | Age (SD) |
Race | Gender | Disposition to home | Disposition to rehabilitation facility | Length of stay in the facility or hospital | Economic impact | mental status | Results | Conclusions |
| 1 | Van Der Vliet QMJ, Weaver MJ, Heil K, McTague MF, Heng M. | 2021 | 1074 patients | >65 | N/A |
N/A | 168 patients (15.6%) | 878 (81.75%) with 45% being discharged <20 days. | Median hospital stay = 5 days & Median ICU stay days= 4 days. LOS for rehabilitations =19 days. (<20 days LOS was found in 398 patients and >=20 days LOS was found in 392 patients) |
N/A |
N/A |
•10% (n = 108) were re-admitted <90 days of their discharge. •924 patients were still alive one year after the injury. •Higher Charlson Comorbidity Index (CCI) (P=0.048), male sex (P<0.001), pre-injury use of an ambulatory device (P = 0.006), and undergoing surgical treatment (P<0.001) were associated with longer hospital LOS. •Older age (P<0.001), pre-injury ambulatory aid (P<0.001), and pre-existing immobility (P<0.001) were independent risk factors for LOS >20 days in a rehabilitation facility. |
•Elderly fracture patients utilize a significant amount of post-acute care resources and age, CCI, surgery, fracture location, pre-injury ambulatory status, and injury living status were found to be associated with the use of these resources. |
| 2 | Kugelman DN, Fisher N, Konda SR, Egol KA. | 2019 | 161 | The average age was 63 years (range: 18-94 years) |
N/A |
38 (76%) Females,12 (24%) males. | N/A | N/A | Average LOS in hospital= 6.32 ± 5.7 days |
N/A | N/A | •50 patients were available for long-term outcomes (mean: 36 months); as measured by SMFA subgroup scores were demonstrated to be 3 times higher in patients currently using assistive devices for walking (P = .012). •Increased age (P = .050) was associated with the continued use of assistive walking devices. •Of the patients who did not use an ambulatory device prior to lateral compression type 1(LC1) pelvic ring injury, 5 (11.6%) sustained a fall. 43 (86%) patients didn’t use an assistive ambulatory device prior to sustaining the LC1 fracture. 7 (14%) patients utilized assistive devices both before and after the LC1 injury. |
•More than a quarter of the patients sustaining an LC1 pelvic fracture continue to use an aid for ambulation at long-term follow-up. • Older age, complications, and falls within 30 days of this injury are associated with the utilization of an assistive ambulatory device. |
| 3 | Berian JR, Mohanty S, Ko CY, Rosenthal RA, Robinson TN. | 2016 | 9972 | A mean (SD) age of 75 (7) years. | 3876 (76.3%) were white, 563 (11.1%) were black and 639 (12.6%) were other races. | 2736 (53.9%) female | >Increased care need was observed in 2339 (46%) patients. >1414 (27.8%) required additional skilled or supportive services at home. | >Out of the care requiring 2339(46%) patients, 925 (18.2%) required discharge to a nonhome destination. | Patients with LOI stayed longer in hospital (mean LOS was 7.3 day) as compared to those without LOI (mean LOS was 3.3 days) | N/A | N/A | •517 patients require readmission (10.2%). • In a risk-adjusted model, Loss of independence was strongly associated with readmission. •Death after discharge occurred in 69 patients (1.4%). •After risk adjustment, LOI was the strongest factor associated with death after discharge (odds ratio, 6.7; 95% CI, 2.4-19.3). |
•Loss of independence (LOI)was associated with postoperative readmissions and death after discharge. •Loss of independence can feasibly be collected across multiple hospitals in a national registry. •Clinical initiatives to minimize LOI will be important for improving surgical care for older adults. |
| 4 | Brinson Z, Tang VL, Finlayson E. | 2016 | N/A | >= 60 years | N/A | N/A | N/A | N/A | 2 - 25 days | N/A | N/A | •A randomized control trial showed that implementation of an inpatient intervention with a focus on maintenance of the patient’s functional status had significant improvements in activities of daily living (p <0.001) and physical performance (p <0.001) at discharge compared to usual care. •Another study showed that Implementation of a modified Hospital Elder Life Program (HELP) intervention that included ambulation or active range-of-motion exercise 3 times daily resulted in significantly less functional decline at discharge (p < 0.001) in older adults who had had abdominal surgery compared to usual care. |
•Postoperative functional status is an important patient-centered outcome. •Living independently is one of the most important aspects in deciding to undergo surgery. •Risk factors for poor functional recovery include baseline frailty, functional disability and cognitive impairment. |
| 5 | Keswani A, Tasi MC, Fields A, Lovy AJ, Moucha CS, Bozic KJ. | 2016 | 106,360 patients | Average age was 64.3 at home, and 71.0 at non-home. (71.6 at SNF, 69.7 at IRF). |
Race at home was: Caucassian (72%), Hispanic (2.6%), African Americans (5.4%), Asian (1.7%) and others (18%). Race at Non- home destination was: Caucasians (75%), Hispanics (3.9), African Americans (8.7%), Asians (2.3%) and Others (9 |
>Home destination, 44% =Male ,56%= females. >Non home setting, 30%=Male,70%=Female. >In non-home (29% male at SNF and 71% female at SNF 32% male at IRF and 68% females at IRF) | Disposition to home 74,637 (70%). |
Discharge to non-home destination was 31,220 (30%) with: skilled nursing facility 19,847 (SNF) (19%), and inpatient rehabilitation facility 11,373 (IRF; 11%). |
Length of stay (LOS) tended to be longer in nonhome patients (nonhome: 3.8 days, home: 3.1 days, P < .001) LOS at SNF was 3.6 days and IRF was 3.8 days. |
N/A | N/A | •Bivariate analysis revealed that rates of post-discharge adverse events were higher in SNF and IRF patients (all P ≤ .001). •In multivariate analysis controlling for patient characteristics, comorbidities, and incidence of complication predischarge, SNF and IRF patients were more likely to have post-discharge severe adverse events. |
•SNF or IRF discharge increases the risk of post-discharge adverse events compared to home. •Modifiable risk factors for nonhome discharge and post-discharge adverse events should be addressed preoperatively to improve patient outcomes across discharge settings. |
| 6 | Rondon AJ, Tan TL, Greenky MR, Goswami K, Shohat N, Phillips JL, Purtill JJ. | 2018 | 2281 patients (IRF=218 and Home=2063) |
•Average age : 73.8 In rehabilitation & 65.7 at home. | Race (non-Caucasian): IRF=74 (34.9) and Home=409 (20.2) | Gender (male) IRF=45 (20.6%) & Home=880 (42.7%) | 90.4% (2063/2281) of the cohort | •Discharged to post-acute care facilities :9.6% (218/2281). | LOS: IRF= 3.4 days and Home=2.0 days | N/A | N/A | •Among 43 variables studied, 6 were found to be significant pre-operative risk factors for discharge disposition other than home. •Age 75 or greater, female, non-Caucasian race, Medicare status, history of depression, and Charlson Comorbidity Index were predictors for patients going to IRFs. •Any in-hospital complications led to higher likelihood of being discharged to IRFs and SNFs. •Both models had excellent predictive assessments with area under curve values of 0.79 and 0.80 for pre-operative visit and hospital course. |
•Pre-operative and in-hospital factors that predispose patients to non-routine discharges allows surgeons to better predict patient post-operative disposition. |
| 7 | Lavernia CJ, D’Apuzzo MR, Hernandez VH, Lee DJ, Rossi MD. | 2006 | 136 patients | •Average age = 72.5. | Race: White (80.4), Black (6.3%) and others (13.3%). | •Female =69.9%. |
•81.1%. | •Discharge to non-home destination was 31,220 (30%) with: •skilled nursing facility 19,847 (SNF) (19%), •inpatient rehabilitation facility 11,373 (IRF; 11%). |
N/A | •Total cost was significantly lower in patients discharged directly to home compared to those who were sent to CRU and subsequently received HC ($2,405 vs $13,435, p <0.001) | N/A | •These patients underwent primary arthroplasty were observed for total cost difference between comprehensive rehabilitation unit (CRU) and homecare (HC). •According to this study, total costs were significantly lower in patients discharged directly to home was lower vs those sent to the CRU and subsequently received HC. ($2405 vs $13435 with p <0.001). •An estimated $3.2 billion is spent annually on postsurgical rehabilitation after arthroplasty. |
•Post discharge costs are significantly higher for patients going to a CRU vs those discharged home; yet, both groups had comparable short-term outcomes. |
| 8 | R. Tiihonen1, R. Alaranta1, T. Helkamaa2, I. Nurmi-Lüthje3, J.-P. Kaukonen1, R. Tiihonen, R. Alaranta1, T. Helkamaa, I. Nurmi-Lüthje, J.-P. Kaukonen,P. Lüthje |
The Finnish Surgical Society 2018 | 70 0f 490 | N/A | N/A | N/A | N/A | N/A | N/A |
•The mean direct costs of primary fracture care were lower than the mean costs of reoperations (€7500 vs €9800) |
N/A | • Reoperations after operative treatment of hip fracture patients may be associated with higher costs and inferior survival. The costs of reoperations were calculated using the diagnosis-related groups (DRG)-based prices. • In all, 70/490 patients (14.3%) needed reoperations. Of all reoperations, 34.2% were performed during the first month and 72.9% within 1 year after the primary operation. •Alcohol abuse was associated with a heightened risk of reoperation |
•Cost per patient of reoperation in acute care was 31% higher than the corresponding cost of a primary operation. •Reoperations increased the overall immediate costs of index fractures by nearly 20%. One-third of all reoperations were performed during the first month and almost 75% within 1 year after the primary operation |
| 9 | Andrea Giusti, Antonella Barone, Mauro Oliveri, Monica Pizzonia, Monica Razzano,Ernesto Palummeri,Giulio Pioli, | 2006 | 194 | >70, averaged 83.6 6 years old | N/A | 14.5% male | 99(49.7%) | •HBR group presented with a slightly better health status, with a lower rate of in-hospital delirium and a lower degree of functional impairment in BADLs and IADLs, and a higher proportion of these patients were living at home with relatives. • 14 % (22 ) needs Long-Term Institutionalization After 12 months •Delirium (%) during hospitalization seen in HBR 29 & IBR 45 , p value =0.022, |
• In the multiple logistic regression model, the only significant variable affecting the choice of IBR at discharge was the absence of relatives at home (odds ratio [OR], 6.7; 95% confidence interval [CI], 3.33–13.46; P .001), whereas a prefracture functional impairment in more than 3 IADLs (at 12mo:OR 3.99; 95% CI, 1.57–10.18; P .004), the absence of relatives at home (at 12mo: OR 8.81; 95% CI, 2.47–31.46; P .001), and delay to surgery longer than 3 days (at 12 mo: OR 5.51; 95% CI, 1.28–23.81; P .022) resulted in significant risk factors for longterm institutionalization. •Those discharged home showed—after controlling for prefracture Barthel Index score, IADLs, cognitive status and age—a slightly lower functional decline and a higher rate of recovery during the follow-up (mean change in Barthel Index score standard deviation at 12mo:HBR, 11.2 +/-24.7 vs IBR, 23.7+/- 28.5; P value= .015). •At 3, 6, and 12 months,the number of surviving subjects was 178, 167, and 158 respectively, and the number of subjects institutionalized was 52 (29%), 26 (16%), and 22 (14%), respectively. •Subjects living alone (%) HBR 23 v/s IBR 62 ,p value<.001, •Mean Barthel Index score +/- SD HBR 85.5+/-23.4, IBR 82.4+/-22.6 , p value =0.033 •Mean Katz Index score +/- SD HBR 4.7+/-1.8, IBR 4.3+/-1.9 , p value = 0.041, •Delirium (%) during hospitalization seen in HBR 29 & IBR 45 , p value =0.022, •The number of patients with complete recovery was higher in the HBR group during the follow-up even if the differences between the groups were highly significant only at 12 months (52.7% in HBR vs 32.9% in IBR, P .008). •The only factors associated with discharge to the rehabilitation facility were the living situation and the occurrence of delirium during hospital stay. |
•In an unselected population of hip-fractured older adults previously living in the community, HBR seems to be a feasible alternative to IBR in those subjects living with relatives. | |||
| 10 | Devora Lieberman, David Lieberman | 2002 | 424 | >75, Mean age +/-SD (y) 85+ GROUP 88.8+/-3.1, 75-84 YEARS GROUP 79.3+/-2.9, |
Israel |
Female gender (85+ Group 96 (76), 75–84 Group 233 (79) |
Discharged to home: 85+ Group 105 (83), 75- 84 group 270 (91), p value= .02 |
N/A | Days waiting until surgery 85 + GROUP 4.0+/-2.5 , 75-84 group 4.4+/-3.2, >Days in orthopedic surgery ward after surgery 85 + group 8.0+/-4.3, 75- 84 group 7.1+/-3.5 >Days hospitalized for rehabilitation 85 + group 22.0+/-8.2, 75- 84 group :22.0+/-9.0, | N/A | Discharge FIM (mean +/- SD) 85+ Group 74.8+/-22.1, 75–84 Group 90.5+/-18.8, p value=.0000001 | •Compared with patients aged 75 to 84 years, the older study group was in a worse mental state (P=0.00005), | •Rehabilitation after surgery for PFF is less successful in >85 group than in a group of 75-to-84 year olds. •No different in terms of duration or the rate of most complications or mortality during the process |
| 11 | Kyosuke Fukuda, Takashi Amari, Kohei Yoshino, Hikaru Izumiya,Kenichiro Yamaguchi | 2022 | 228((Home group (n=110), Hospital transfer group(n=118) | Home group 86.2 ± 6.1, Hospital transfer group 88.0 ± 6.7,p value <0.05 | Japanese | (female: %) Home group 86 (78.1%), Hospital transfer group 86 (72.8%) | N/A | N/A |
•Japan’s long-term care insurance system that allows elderly people to receive appropriate support in their daily lives according to their level of independence and physical and mental functions . •In acute care, a support system called the “community comprehensive care system”, supported by the long-term care insurance system, facilitates community support projects and networks to ensure that elderly people transition smoothly from acute care back into society. |
N/A | N/A | •Walking ability before injury (independence: %) 99 (90.0%) 95 (80.5%), p value< 0.05, Preoperative waiting days 2.1 ± 1.9 2.1 ± 1.9 •Postoperative hospitalization days Home group 40.0 ± 16.6, Hospital transferred group: 39.7 ± 17.7, •Walking ability one week after surgery (FAC3≤: %) Home group :49 (44.5%), Hospital refered group: 34 (28.8%), p value<0.01 •Barthel Index at discharge : Home group:75.6 ± 22.7 ,Hospital refered group:58.0 ± 24.6, p value<0.01 •Odds ratios are Walking ability one week after surgery 1.9 ,p <o.o5,staying with Co-residents 4.6 ,p < o.o1, |
•The walking ability after 1 week of surgery and the staying with co-residents or family members significantly increases the rate of home discharge after PFF surgery. |
| 12 | Suguru Ohsawa, Aiko Miura, Mie Yagyu, Anzu Oizumi , Eiji Yamada | 2006 | 20( Assertive method = 13, conventional method = 7) | Age (years) Assertive method=86.79+/-4.3, Conventional Method= 87.99+/-4.1 , p value=0.658 | Japanese | female=18, p= 0.787 | •The mental state (MMSE) in the assertive group was significantly better than that in the conventional one at the start of rehabilitation in our study (P value=0.0029). | •All the patients in the assertive rehabilitation group recovered their ability to walk (FIM score) to some extent, while those in the conventional group did not Ambulationd (FIM) Assertive method =18.29+/-7.9 , Conventional method=9.49+/-4.3 , p- value=0.00135 . •In 6 months follow-up, the FIM score was significantly higher in the patients treated with assertive rehabilitation (p value=0.0135) which reflects the gain of independence following surgery by the patients. •However, the mental state (MMSE) in the assertive group was significantly better than that in the conventional one at the start of rehabilitation in (P value =0.0029). |
•Assertive conservative therapy is beneficial in gain in ability to walk over conventional treatment after intracapsular fracture of the proximal femur in frail elderly patients who have not had surgery. |
||||
| 13 | J. Moore,O. Carmody, B. Carey, J. A. Harty, D. Reidy | 2017 | 9 | >100(101 years and 7 months. |
Ireland | FEMALES= 8, MALE = 1 | N/A | All patients were discharged to long term care residence | Mean =14.43 days. | •Average inpatient cost of €14,898. | •This study shows that there is no association with age and longer length of hospital stay in hip fracture patients . • Average inpatient cost of €14,898—this cost is exclusive of component cost, rehabilitation (e.g., physiotherapy, occupational therapy),convalescent care, and outpatient follow-up. •The most recent figures show that the inpatient cost of treating the average hip fracture in Ireland is €12,600 while The inpatient cost of treating hip fractures in centenarians was 18% above that of hip fractures of any age. |
•The inpatient, 30-day and 1-year mortality rate were 22, 22, and 71%. •Operative management of hip fracture patients over the age of 100 years is associated with an acceptable mortality rate. |
|
| 14 | R. Aigner, T. Meier Fedeler, D. Eschbach, J. Hack,C. Bliemel,S. Ruchholtz,B. Bücking | 2016 | 402 | Age in years 81 ± 8 | N/A | Female 293 (73%) | N/A | N/A | •Length of stay in hospital (in days) 14 ± 6 days. •The length of hospital stay was shorter for patients with an MMSE ≤20 (12 vs. 15 days; p < 0.001). |
•The mean total acute care costs per patient = 8853 ± 5676 euro€ with ward costs (5828 ± 4294 €) and costs for surgical treatment (1972 ± 956 €) representing the major cost factors.======== •Pre-fracture Charlson index: 2.4 ± 2.3, •That ward costs accounted for the biggest proportion of total hospitalization costs(5828 ± 4294 € 65.8%) |
•Cognitive impairment (Mini Mental State Examination <20) did not have a significant effect on total costs (MMSE ≤20 8248 € vs. MMSE >20 9176 €;p = 0.616). | •Only 3% of total costs were spent on physiotherapy 262 ± 224 euro (3.0%). If physiotherapy can be done properly then the total cost could be minimized significantly. • Cost of treatment in male is about 800 euro higher than female ,p value= 0.128 due to pre existing premorbid conditions and longer hospital stay. •Charlson comorbidity index : <4 : 8,353 ± 4,616 euros, ≥ 4: 10,383 ± 7,939 euros, p value= 0.047, •Cognitively impaired patients were discharged sooner because these patients often did not have the potential for rehabilitation, resulting in shorter lengths of hospital stay. •Cost for Pre existing Cognitive impairment (MMSE):MMSE ≤20 8,248 ± 3,662 euros & MMSE >20 9,176 ± 6,459 euros ,p value=0.616 |
•Thus individual patients specific factor plays a great role in cost of management of fracture . •To reduce the socio-economic burden, fracture prevention programs and cost-effective treatment models are necessary. |
| 15 | Jean Taillandier , Fabrice Langue, Martine Alemanni, Elodie Taillandier-Heriche | 2003 | 60 | 83 ± 7.1 years | N/A | 54 (90%)female ,6 (10%)Male | N/A | N/A | Mean length of hospital stay was 45 ± 28 d (range, 10-130 d). |
N/A | N/A | •Insufficiency fractures of the pelvis occur in older patients, either spontaneously or after a trivial trauma such as a fall from the standing position. •52 patients reported a minor fall on the day of admission or within the last few days while in 8 the fractures were considered spontaneous • A history of osteoporotic fracture was present in 24 (40%) patients (vertebral fracture, n = 16; femoral neck fracture, n = 10). •A simple fall caused the fracture in 86.6% of patients. •56 (93%) patients lived at home before the fracture (11 with their spouse or children and 12 with visits from home aides) and the other 4 lived in nursing homes; •41 (68.3%) were fully self-sufficient before the fracture, 11 used a cane to walk outside their home, and 8 were not self-sufficient. •Complete elimination of weight bearing was required in 52 patients, the mean duration being 12.7 d (range, 3-55 d), whereas 8 patients were able to continue walking, with analgesic treatment. •Length of stay was significantly longer in the patients who were not selfsufficient before the fracture; •Lower degree of self-sufficiency is the reason for instutionalization. • 44 patients returned to their previous place of residence, but 15 were discharged to institutions (11 to nursing homes and four to extended-stay hospitals). • Only 22 patients had the same level of self-sufficiency as before the fracture and 10 experienced a decrease in selfsufficiency. 7 patients (14.3%) died within the year after the fracture. •Only age was significantly associated with loss of self-sufficiency; patients who experienced a marked decrease in self-sufficiency were significantly older than those who recovered their previous level of self-sufficiency (88.2 years vs. 78.5 years; P = 0.0001). •After 1 year, only 36.6% of our patients had the same level of self-sufficiency as before the fracture. • 25% of patients were discharged to institutions. |
•Pelvic insufficiency fractures are fairly common in older patients and can raise diagnostic challenges • Pelvic fractures adversely affected self-sufficiency in this study |
| 16 | Kyle T. Judd, Eric Christianson | 2015 | 657,(111 =early interventions, 546= Late interventions) |
•Average age for the early intervention group = 79 years. •Average age for the late intervention group = 81 years |
N/A | N/A | N/A | N/A | •The average LOS for the early intervention group was 4.11 days . •Average LOS 5.68 days for the late intervention group (p=0.0005). |
The average cost of the early intervention = $49,900 & •The average cost of late intervention =$65,300 (p= 0.0086). |
N/A | •High costs and an increasing burden of care, there has been interest in newer methods to increase efficiency of care. • One such method is expedited fracture care, with earlier operative intervention. The purpose of this study was to determine if intervention within 6 hours of admission decreased costs with no change in the rate of major complications. • Patients were divided into two groups: those undergoing operative intervention < 6 hours after admission (early) and those undergoing operative intervention > 6 hours after admission.. •The average length of stay for the early intervention group was 4.11 days & it was 5.68 days for the late intervention group (p=0.0005). • The average cost of the early intervention was $49,900, with the average cost of late intervention being $65,300 (p= 0.0086). |
•Expedited fracture care, with earlier operative intervention helps to decrease the cost significantly. The purpose of this study was to determine if intervention within 6 hours of admission decreased costs with no change in the rate of major complications. •Programs emphasizing early intervention for hip fractures have the potential for large healthcare savings, with an average savings of $15,400 |
| 17 | IAN D CAMERON,DAVID M. LYLE,SUSAN QUINE | 1994 | 252 | 84 years | N/A | (83% = female, 17% =male) | N/A | 39% lived in nursing homes prior to sustaining their fracture. |
•The mean length of hospital stay was 19.5 days for the accelerated rehabilitation group & • 28.1 days for the conventional care group. |
•Total cost was approximately A$ 10,600 for accelerated rehabilitation and A$ 12,800 for conventional care (p value=0.186) •Because of the reduction in length of stay, the post surgical component is markedly reduced for the accelerated rehabilitation group(A$6420 v/s A$ 8870( pvalue= 0.138).) |
N/A | •The focus of the analysis in this paper is that of a third party funding agency (in Australia the Commonwealth and State Government finance most of the cost of PFF). •.Community services were utilised more frequently by the accelerated rehabilitation group while the conventional care patients utilised more institutional care. •Physical independence of patients, at 4 months after fracture as measured by Barthel Index, Accelerated rehabilitation v/s conventional care(50% v/s 41%) which reflects the benefit of accelerated rehabilatation •The major factor contributing to cost of treatment for PFF in this study was the length of hospital stay. •Accelerated rehabilitation is potentially applicable to most hospitals providing care for patients with proximal femoral fracture. |
• This study shows that accelerated rehabilitation is cost-effective in treating PFF and appears superior to conventional orthogeriatric care. •The major factor contributing to cost of treatment for PFF in this study was the length of hospital stay. |
| 18 | Franz Muller, Michael Galler, Michael Zellner, Christian Bauml, Bernd Fuchtmeier | 2015 | 117(121 fractures) | Patient in 10th decade of life (90-99 years) •Mean age= 92.3 years. |
N/A | 81% Female | N/A | N/A | N/A | N/A | The incidence of dementia was 60% before surgery. • Patient with dementia were refered to niursing home for care. • In revision surgery 20.5% have dementia who survived (n=34) |
•At the time of follow-up, 83/117 patients (71%) were already deceased. The mortality after 30 days, 6 months, 1 year and 2 years was 16%, 37%, and 43%, and 55%, respectively •22 (19%) required revision surgery •The proximal femoral fractures in the 10th decade of life are associated with high postoperative mortality within the first 6 months •Surgical revision due to complications did not result in a statistically significant reduction of the survival time. |
•The occurrence of proximal femoral fractures in the 10th decade of life results in high postoperative mortality just within the first 6 months. •No explanation regarding cost and limitations of activties. Or loss of independence |
| 19 | Till Berk ,Marion Thalmann,Kai Oliver Jensen,Peter Schwarzenberg,Gerrolt Nico Jukema,Hans-Christoph Pape,Sascha Halvachizadeh | 2023 | 71 | >=70 •Mean =83.54+/- 7.78 |
N/A | •Male: 24( 33.8%),Female: 47( 66.2%) | N/A | N/A | LOS= 14.85 days | N/A | N/A | •Proximal femur fractures (PFF) are among the most common injuries in the geriatric population; they require hospitalisation and surgical treatment. •Mechansim of injury= Low energy impact in 67(94.4%) •The ePA-AC was assessed on admission by the nursing staff and repeated daily over the course of the inpatient stay. This reflects the condition of patient from the date of admission until discharge on daily basis ----Helps in assessing the patiets progress. •49 patients (67.7%) developed at least one complication. • Most common complication was delirium (n = 22, 44.9%) • Group with complications (Group C) had a significantly higher FFI(Fried Fraility Index) compared with the group without complications (Group NC) (1.7 ± 0.5 vs 1.2 ± 0.4, p = 0.002) •A higher FFI score increased the risk of developing complications (OR 9.8, 95% confidence interval [CI] 2.00 to 47.7, p < 0.005) • A higher CDD(confusion,delerium and dementia score increased the risk of developing delirium (OR 9.3, 95% CI 2.9 to 29.4, p < 0.001). •A higher BS (Braden Score)increased the odds of developing decubitus by 6.2 times (95% CI 1.5 to 25.7, p < 0.001). •Postoperative complications influence the course and outcome following surgery and are associated with increased socioeconomic burden • The results of this study have shown that the ePA-AC could represent such a multidimensional assessment tool–especially because it seems that the search for an ideal score for the assessment of elderly patients has not yet been achieved. |
•The FFI has the highest predictive value for an increased risk of developing complications in general • CDD is a promising tool for identifying geriatric trauma patients at risk of delirium. • Utilisation of the appropriate assessment tool for geriatric trauma patients might support individualised treatment strategies. |
| 20 | Nicola Veronese, Stefania Maggi | 2018 | N/A | N/A | N/A | •worldwide hip fractures occurred in 18% of women and 6% in men •higher incidence in white women than in men |
N/A | N/A | N/A | N/A | N/A | •Hip fracture is an important and debilitating condition in older people, particularly affecting women. •It is globally estimated that hip fractures will affect around 18% of women and 6% of men.(1992 DATA) •The direct costs associated with this condition are enormous since it requires a long period of hospitalisation and subsequent rehabilitation. •CAUSE OF HIP FRACTURE:decreasing bone mineral density (BMD) and those increasing the rate of fall. •Gender is one of the factor which is influence hip fracture.Higher incidence in white women than in men •1/3 rd of women in 80 ‘s will have hip fracture. •severity : above 80 years : 1/3 rd of male die within 1 year after hip fracture as compared to female. •RACE: Whites living at higher latitudes exhibit a higher incidence of hip fractures ranging from 420/100,000 new hip fractures each year in Norway to 195/100,000 in USA. •Their more recent data (2012) showed that the highest incidence of hip fracture was observed in Denmark (439/100,000), the lowest in Ecuador(55/100,000) •It is noteworthy that every year about 300,000 subjects are hospitalised for hip fractures in the United States alone. •The estimated cost of treatment in the US was approximately 17 billion dollar in 2002. •Worldwide, in women, the lowest annual incidence rate was seen in Nigeria (2/100,000), the highest in Northern Europe countries, such as Denmark (574/100,000). •Asians demonstrate a risk of hip fracture intermediate between whites and blacks [31,32,33] with about 30% of the world’s hip fractures occurring in China, making this a public health concern.. • People requiring a long term care (LTC) facility is estimated between 6 and 60% of people suffering from hip fracture with cost ranging from $19,000 to $66,000 . •costs were significantly greater for rehabilitation hospital patients than for nursing home patients |
•Hip fracture is a common condition, frequently leading to disability ,a higher rate of social isolation and consequently mortality. •The global incidence of hip fracture is rising, underlining the need for focussing on its prevention, which is possible through the treatment of osteoporosis and falls risk. |
| 21 | A. Morice, N. Reina, G. Gracia, P. Bonnevialle, J-M. Laffosse, K. Wytrykowski, E. Cavaignac ,N. Bonnevialle |
2016 | 39 | >100 years •mean age of 101.3 years (range, 100-108 years) |
France | •33 women,and 6 men | •15 patients living at home at the time of the injury, 3 returned home, 5 entered nursing homes for dependent senior citizens, and 7 were admitted to geriatric rehabilitation units | >>15 patients living at home at the time of injury 5 entered nursing homes for dependent senior citizens, and 7 were admitted to geriatric rehabilitation units >>>7 patients who were in nursing homes for dependent senior citizens at the time of injury returned to the same institution >>>>?>>>?>Of the 14 retirement home patients, 8 returned to their previous institution, 5 entered nursing homes for dependent senior citizens, and 1 was admitted to a geriatric hospital. |
Mean hospital stay = 9.5 days [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28] | N/A | •Most patients (61.5%) were institutionalised and many (36%) had dementia | •15 were living at home and 24 in an institution at the time of the injury(retirement home, n=16; nursing home for dependent senior citizens, n=7; or extended-stay hospital, n=1). •On functional outcomes: of the patients living at home at the time of the injury, 20% returned home after surgery and 15% recovered their previous walking capabilities •26 patients alive after 3 months had a mean total Parker score decrease of 0.83±0.51 (0-4) and a mean Katz index increase of 0.33±0.18 which signifies the loss of independence of the patietns. •After a mean follow-up of 23±14 months (6-60 months), 29 patients had died, including 3 within 48 h, 10 within 3 months, and 15 within 1 year. Complication :confusional state (n=2) •Mini Nutritional Assessment (MNA) ( range :2-12) score was 7.46±2.23 with no association to 3 months mortality whether patient is living at home or not (p<0.08). |
•PFF carry a high risk of death among centerians. •Mortality is high in centenarians after a PFF. • Multi discipilinary approach is necessary for better outcome. |
| 22 | Nicole Simunovic, PJ Devereaux, Mohit Bhandari | 2011 | >50 years the guideline is applicable | >50 years the guideline is applicable | N/A | N/A | N/A | N/A | N/A |
•In Canada, the cost of hip fractures is $650 million annually, and is expected to rise to $2.4 billion7 based on a projected number of 88,124 hip fracture patients by 2041. •The estimated lifetime cost for all hip fractures in the United States in 1997 likely exceeded $20 billion. • In the United Kingdom, direct hospital costs alone were estimated to be $125 million in 2003. |
N/A | •Hip fractures are associated with a high rate of in hospital mortality7-14% and profound temporary and sometimes permanent impairment of quality of life. •Surgery within <24 hr, have association with better functional outcome and lower rates of perioperative complications and mortality. •surgical delay increasess the rate of pressure ulcer and avascular necrosis •Early surgery helps in improved ability of patients to return to independence, mobility and to pre fracture living status •early surgical correction directly proportional to shorter hospital stay |
•The current evidence for optimal surgical timing is entirely observational and often conflicting for the outcomes of mortality, most postoperative complications, length of hospital stay, and return to living status. •The current evidence for optimal surgical timing is entirely observational and often conflicting for the outcomes of mortality, most postoperative complications, length of hospital stay, and return to living status. |
| 23 | Nidhi Tiwari,Shubhangi Patil,Rupali Popalbhat | 2022 | 21 years male | 21 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | •A patient’s ability to carry out activities of daily living effectively and efficiently post-surgery is hampered by a variety of obstacles •Physiotherapy procedures commenced with the purpose of alleviating pain and establishing a normal range of motion •A significant portion of trauma-related hospitalizations is due to proximal femoral fractures. •To reinstate hip and knee moements to normal, or at the very least to a functional ROM to improve and regain the strength of hip movements, and to restore ROM for hip and knee joints, the patient underwent physiotherapy •After proper rehabilitation, the patient’s ROM i.e., both active and passive, was increased at the time of discharge • After 8 weeks The ADL(Activity of Daily living was done with assistive devices. •Muscle strength increased i.e pre-treatment v/s post treatment((1 v/s +3))-manual muscle testing (MMT) |
•Patient’s ROM and muscle strength in the lower limb and face muscles were enhanced with physiotherapy. |
| 24 | Johannes Gleich, Carl Neuerburg,Carsten Schoeneberg,Matthias Knobe, Wolfgang Böcker,Katherine Rascher, Evi Fleischhacker | 2023 | 19712(data taken from Registry for Geriatric Trauma founded by German Trauma Society---------All hospitals certified as AltersTraumaZentrum DGU) |
>=70 years •Median age =85 (IQR 80–89) years. |
•80 hospitals from Germany,Austria and Switzerland were involved) •19 level I and 61 level II/III trauma center |
72% female | N/A | N/A | •LOS in hospital = 14.1 days of level I & 16 days of level II/III patients with p value=0.005 | N/A | N/A | •Proximal femur fractures predominantly affect older patients and can mark a drastic turning point in their lives. •Recommended surgical treatment within 24–48 h after admission for better outcome. •When surgery is performed more than 48 h after admission, worse outcome regarding mobilization and mobility as well as significantly increased mortality have been observed •28.6% of patients were treated in level I, 37.7% in level II, and 33.7% in level III trauma centers. •LOS in hospital was 14.1 days of level I and 16 days of level II/III patients with p value=0.005 •38.4% of level I and 32.3% of level II/III patients could walk unaided and nearly 80% of all patients had no existing osteoporosis treatment. •38.4% of level I and 32.3% of level II/III patients could walk unaided and nearly 80% of all patients had no existing osteoporosis treatment •Mean time to surgery was 19.2 h (9.0–29.8) in level I trauma centers and 16.8 h (6.5–24) in level II/III trauma centers (p < 0.001). •Surgery in the first 24 h after admission was provided for 64.7% of level I and 75.0% of level II/III patients (p < 0.001). •Treatment in hospitals with higher level of care and subsequent increased time to surgery showed •Increased odds for worse walking ability 7 days after surgery were found in level I trauma centers •Mobilization on the first day after surgery was performed significantly more often in level II/III trauma centers. |
•Longer time in level I trauma centers compared to level II/III trauma centers, with 64.7% and 75.0% of patients undergoing surgery within 24 h after admission. •Better walking ability 7 days after treatment was observed in hospitals providing lower level of care, which also showed shorter time to surgery. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



