
Submitted:
22 May 2024
Posted:
23 May 2024
You are already at the latest version
Abstract
Consumption of ultra-processed foods is associated with abdominal obesity, but this association has not yet been investigated in individuals on hemodialysis. This cross-sectional study, developed with 1014 individuals, aimed to analyze the prevalence of abdominal obesity and its association with the consumption of ultra-processed foods in individuals on hemodialysis. Consumption of ultra-processed foods was measured using a questionnaire, whose list of foods was based on the Surveillance System of Risk and Protective Factors for Chronic Non-Communicable Diseases through Telephone Enquiry. Waist circumference was used to determine the presence of abdominal obesity. The difference in proportions between the independent variables and the outcome was verified using Pearson's chi-square test. Hierarchical logistic regression was used to determine the association between the outcome and the independent variables. The prevalence of abdominal obesity was 77.22%. In the final model, higher consumption of ultra-processed foods, be male and an adult, have between 8 and 11 years of schooling and practice physical activity below the recommended level increased the chances of having abdominal obesity. The research provides a basis for the creation and improvement of public policies that promote improvements in these health determinants.
Keywords:
Diet. Nutrition. Central obesity. Visceral obesity. Chronic kidney disease.
1. Introduction
The group of ultra-processed foods (UPF) consists of industrial formulations typically made with five or more ingredients, which include substances and additives used in the manufacture of processed foods, such as sugar, oils, fats, and salt, in addition to antioxidants, stabilizers, and preservatives [1]. An expansion of UPF, both in volume and variety, available in the world’s food supply, is occurring primarily in high-income countries, but is growing in middle-income countries [2]. This provides evidence that a transition to a more processed diet globally is underway and accelerated [3]. In Brazil, data from the latest Family Budget Survey show that the contribution of UPF to total calories purchased increased from 12.6% in 2002–2003 to 18.4% in 2017–2018, furthermore, there was a decrease in the caloric participation of in natura foods [4].
In this context, statistics indicate that excess body weight affects more than two billion people, approximately 30% of the world’s population [5]. In Brazil, data from the Food and Nutrition Surveillance System reveal that the prevalence of obesity in adults has increased from 15.6% in 2009 to 28.5% in 2019 [6]. Excess fat deposition in the central region is called abdominal obesity and is associated with greater health risks, mainly cardiometabolic complications [7,8,9,10]. For diagnosis, one of the simplest anthropometric measurements is waist circumference (WC) [11], recommended by the World Health Organization for screening the risk of metabolic and cardiovascular diseases [12], in addition to being a better predictor for these diseases than the body mass index (BMI) [11,13,14,15]. Data from representative national samples in the United States [16], United Kingdom [17], Australia [18], and Korea [19], and a longitudinal study with civil servants in Brazil [20], found that higher consumption of UPF was positively associated with abdominal obesity.
Chronic kidney disease (CKD), as well as abdominal obesity, is a non-transmissible chronic disease and consists of abnormalities in renal function or structure for a period greater than or equal to three months [21]. It can be classified into five stages, and in the fifth stage the individual is considered an end-stage renal patient [21]. At this stage, there is a need for renal replacement therapy, with hemodialysis being the main treatment modality [21,22]. CKD affects 10% of adults worldwide and results in about 1.2 million deaths each year [23]. It is estimated that in 2040 it will become the fifth leading cause of death in the world [23]. In Brazil, the total estimated number of individuals on dialysis during the year 2019 was 144,779, of which 92.6% were on hemodialysis [24].
UPF contain, in most of their composition, inorganic phosphorus additives [25]. In individuals with kidney disease, there is difficulty in completely eliminating phosphorus from the body, leading to hyperphosphatemia, which is associated with cardiovascular morbidity and mortality in individuals with CKD [26,27,28,29,30,31]. Obesity, in turn, affects the progression of stable kidney disease [32]. In addition, in individuals undergoing dialysis, abdominal obesity was positively associated with cardiovascular morbidity [33,34] and mortality [34,35,36,37,38].
However, the relationship between the consumption of UPF and abdominal obesity in individuals with CKD undergoing hemodialysis has not yet been investigated in studies, and this is the first one. Therefore, this study aims to analyze the prevalence of abdominal obesity and its association with the consumption of ultra-processed foods in individuals on hemodialysis.
2. Materials and Methods
2.1. Design
This is an epidemiological, observational, cross-sectional investigation, carried out with individuals undergoing hemodialysis in clinics in the metropolitan region of a state located in southeastern Brazil.
2.2. Population
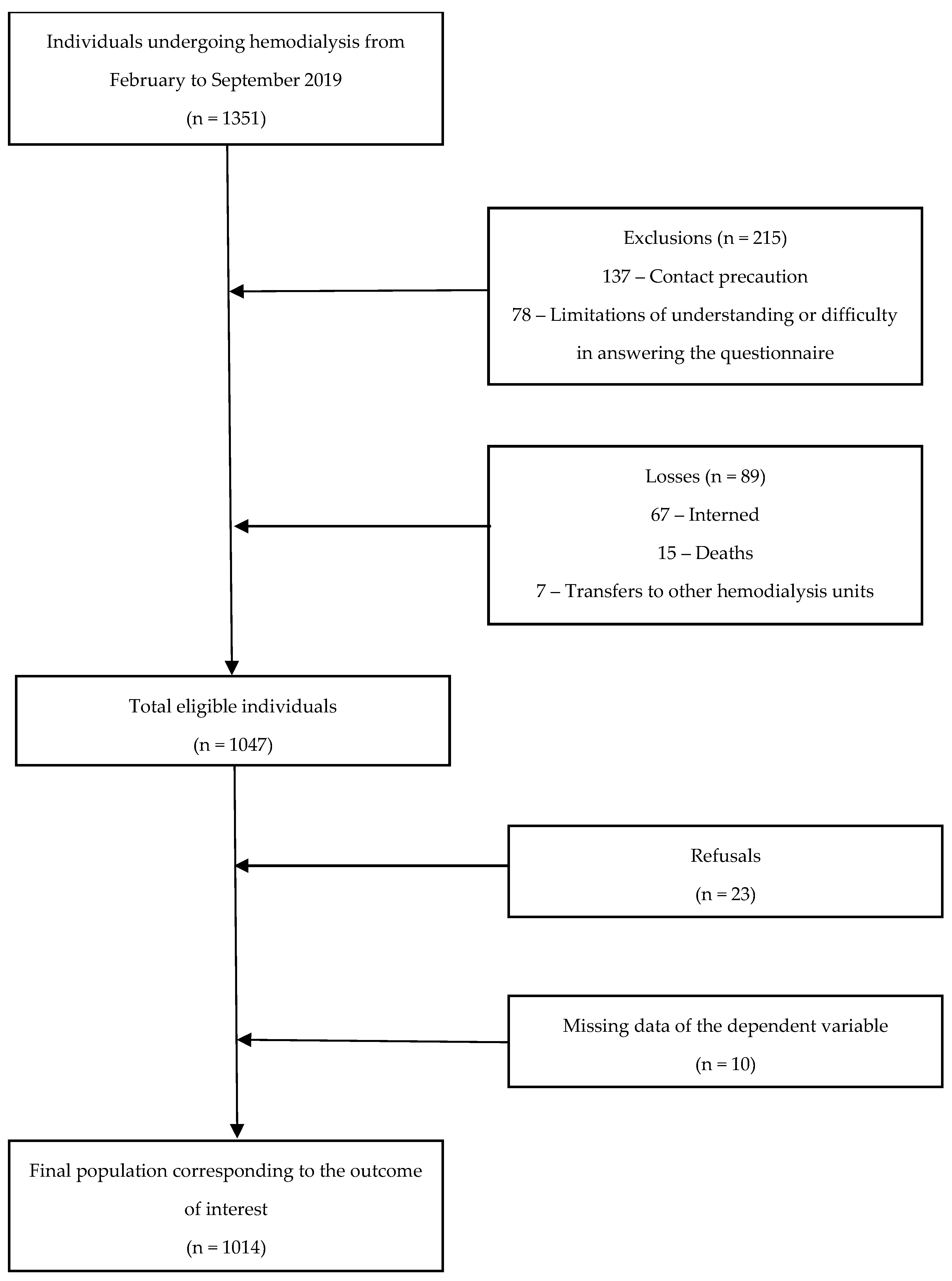
The population of this study consisted of 1014 individuals (Figure 1). To participate in the research, the individual should meet the following inclusion criteria: be 18 years old or older, have a confirmed diagnosis of CKD in the medical records, be on hemodialysis treatment for at least six months, and be ambulatory. We excluded from the survey: individuals under contact precaution, those with an acute condition that limited their participation in the study, who did not reside in one of the municipalities in the studied region, who were transferred to another clinic and, those with missing data on the outcome.
Of the 1351 individuals undergoing hemodialysis in the region studied, after the exclusions, we obtained a final population of 1014 individuals (Figure 1).
Figure 1.
Flowchart of study participants.
2.3. Data Collection
Data collection took place from February to September 2019, after inviting all individuals undergoing hemodialysis, who attended the units in the studied region, to participate. All assessments were performed by previously trained researchers.
Each individual was approached during their stay at the clinic, responding, during the hemodialysis session, to a semi-structured questionnaire on sociodemographic characteristics, lifestyle habits, and food consumption, and then, after the session, submitted to the collection of anthropometric data.
2.4. Sociodemographic and Clinical Characteristics
The variables of sex, age range, marital status, and race/color were dichotomized, respectively, into: female and male, adult (18–59 years) and elderly (>60 years), with a partner and no partner, and white and non-white (self-declared race/color).
The categories used to define income were based on the family’s minimum wage, defined as the lowest wage a company can pay an employee according to the number of hours worked. It has Brazilian validity by law and is reassessed annually based on the cost of living of the population. It is creation was based on the minimum amount that a person spends to ensure their survival. In the year the study was carried out, a minimum wage was R$ 998.00 or $235.37 USD.
The variables of education, work activity and smoking were separated into three categories, respectively: < 8 years, 8–11 years, and > 11 years of study; with paid activity, no paid activity, and retired or on sick leave; smoker, former smoker, and never smoked.
We collected the duration of CKD and the date of initiation of hemodialysis from the medical records of the participants, being categorized according to the number of years. We asked participants about their medical history, so that diabetes and hypertension were dichotomized into absence and presence.
Regarding the practice of physical activity, we questioned the individuals about the type and frequency performed. All individuals who accumulated at least 150 minutes of physical activity per week were considered physically active and those who did not fit these characteristics were considered physically inactive [39].
2.5. Anthropometry
To obtain height, we measured participants barefoot using a portable stadiometer, with a precision of one mm, from the Sanny® brand. The individuals were instructed to stand upright, arms extended along the body and gaze fixed on a point on the horizon [40].
In addition, we weighed them on portable scales, with a capacity of 150 kg and accuracy of 0.1 kg, from the Tanita® brand. For measurement, they were invited to step on the scale barefoot, in an upright position and with as little clothing as possible [40].
BMI was obtained by dividing weight (kg) by height (m) squared [41]. The classification adopted for adults and the elderly was: BMI < 18.5 kg/m² (underweight), ≥ 18.5 kg/m² to < 25 kg/ m² (eutrophy), ≥ 25 kg/m² to < 30 kg/m² (overweight), and ≥ 30 kg/m² (obesity) [41]. Subsequently, we dichotomized the data into absence of excess weight (underweight and eutrophic) and presence of excess weight (overweight and obesity) [41].
We used WC to determine the presence and absence of abdominal obesity. For the measurement, we used the Sanny® brand inextensible measuring tape. The examinee was instructed to remain standing, with arms extended along the body and feet together. The tape was positioned at the midpoint between the lower margin of the last rib and the iliac crest [40]. When it was not possible to measure the midpoint, we used the measurement two cm above the umbilicus [42]. We considered the presence of abdominal obesity as ≥ 80 cm for women and ≥ 94 cm for men [41].
2.6. Consumption of Ultra-Processed Foods
In order to analyze the participants’ consumption of UPF, we applied a questionnaire, whose list of foods included was based on the Surveillance System of Risk and Protective Factors for Chronic Non-Communicable Diseases through Telephone Enquiry [43], by the Brazilian Ministry of Health, which annually assesses the food in the capitals of the country. We used the NOVA food classification, proposed by Monteiro et al. [1], and in this study only the fourth group was considered. The questionnaire examined four food items, by frequency of consumption of isolated foods and food groups, namely: soft drinks and artificial juices (powder or box); sausages (ham, mortadella, salami, sausage); biscuits (chips, filled) and sweets (ice cream, chocolates, cakes, biscuits, sweets).
To assess the reliability of the questions and the reproducibility of the food consumption questionnaire in this population, we conducted a pilot test in January 2019 [44]. Details on the stipulated frequency categories and the conversion of reported consumption frequencies into daily rates are provided in Marques et al. [44]. We evaluated the distribution of consumption of UPF in quartiles. The first (Q1) and second (Q2) quartile corresponded to the lowest consumption, while the third (Q3) and fourth (Q4) quartile corresponded to the highest consumption of UPF.
2.7. Ethical Aspects
This study was approved by the Research Ethics Committee nº. 4.023.221 (CAAE 68528817.4.0000.5060) and all participants signed the informed consent form, in accordance with the principles of the Declaration of Helsinki.
2.8. Statistical Analysis
To describe the study variables, we used absolute and relative frequencies. To verify whether there was a difference in the proportions between the independent variables and the outcome, we used Pearson’s chi-square test (x²) for qualitative variables.
We performed hierarchical logistic regression to associate the outcome with the independent variables, including the variables that had a value of p ≤ 0.1 in the bivariate analysis. In the first model, only sociodemographic variables (sex, age range, and education) were included; for the second model, the work activity variable was added; in the third model, lifestyle, and health variables (CKD time, hemodialysis time, and physical activity) were included. Diabetes and BMI were not included in model three, respectively, because it was self-reported and showed general obesity only. In all models, the UPF consumption variable was added. The final model was performed using the Forward LR method, in which the variables work activity, CKD time, and hemodialysis time were removed by the mathematical model itself. For all of them, we respect the assumptions of absence of multicollinearity and absence of outliers.
We performed the statistical analyses using the statistical software R (4.0.3) for Windows, with a significance level of α < 5%.
3. Results
In Table 1, we have the descriptive and bivariate analysis of the variable outcome in relation to independent variables. The prevalence of abdominal obesity was 77.22%. Among the individuals undergoing hemodialysis in the studied region, most were male (56.71%, p < 0.001) and elderly (69.22%, p < 0.001); had no diabetes (63.41%, p < 0.001); did not practice physical activity (77.5%, p < 0.001); had less than 8 years of study (51.39%, p = 0.004), had 5 or less years of CKD (59.86%, p = 0.01), and had 1 to 5 years of hemodialysis (58.04%, p = 0.02); had no overweight (51.3%, p < 0.001); and were in quartiles one and two of the UPF consumption (57.89%, p < 0.001).
In Table 2, we have the logistics regression models for the variables that presented p < 0.1 in the bivariate analysis. In the final model, increased the chances of having abdominal obesity: in 1.72 times, be in quartiles three and four of consumption of UPF (p = 0.001, OR = 1.72, 95% CI: 1.23–2.39); in 2.21 times, be male (p < 0.001, OR = 2.21, 95% CI: 1.55–3.16); in 2 times, be an adult (p < 0.001, OR = 2, 95% CI: 1.38–2.91); in 1.7 times, have between 8 and 11 years of schooling (p = 0.035, OR = 1.7, 95% CI: 1.03–2.79); and in 1.97 times, practice physical activity below the recommended level (p = 0.004, OR = 1.97, CI 95%: 1.23–3.14).
4. Discussion
The results of our study demonstrate that the prevalence of abdominal obesity in individuals undergoing hemodialysis is high. In addition, higher consumption of UPF, be male and an adult, have less education and practice physical activity below the recommended level increased the chances of having abdominal obesity in these individuals.
In our study, the prevalence of abdominal obesity was 77.22%. Studies have found a prevalence of abdominal obesity in the North American [16], British [17], and Australian [18] adult populations of 53%, 40.7%, and 40.2%, respectively. In individuals with CKD, the prevalence values of abdominal obesity were 30.7% in stages four and five [45], and 60% in stages three to five in pre-dialysis clinics [46]. In those treated with hemodialysis, the values were 39% in Norway [47] and 44.77% in Brazil [48]. Thus, we noticed that the prevalence of abdominal obesity in our study is high and is higher than that of others found in the literature, including those with a population similar to our study [49].
Those with higher consumption of UPF were 1.72 times more likely to have abdominal obesity. Other studies have already shown that higher consumption of UPF increases the chances of having abdominal obesity. For example, when analyzing nationally representative samples of North Americans [16] and Australians [18], those with higher consumption of UPF were 1.62 and 1.32 times more likely to be abdominal obesity, respectively. In Brazil, a longitudinal study noted that public servants with higher consumption of UPF, had a 1.33 times greater risk of WC gain [20]. Several mechanisms can explain the relationship between consumption of UPF and abdominal obesity. The formulation and ingredients of these products make them convenient, accessible, hyperpalatable, and attractive, leading to ingestion in larger quantities [1,50,51]. As for the nutritional profile, they are more dense in energy [3,52,53,54] and have higher levels of fat, mainly saturated and trans fats, simple sugars and sodium, in addition to lower levels of protein, fiber, vitamins, and minerals [55,56,57,58,59,60]. As a result, they are nutritionally unbalanced [1,50,51], contributing to the increased prevalence of obesity in the population [52].
Furthermore, the deconstruction of the food matrix, together with the orosensory properties, increase the rate of food intake [54,61], delay the signs of satiety and increase the glycemic response [39,62,63], resulting in greater oral intake [64,65,66] and, consequently, greater body weight gain [17,64,67]. Added cosmetic additives are also related to changes in the composition and metabolic behavior of the intestinal microbiota, causing inflammatory processes and diseases, with potential implications for body weight and adiposity [68,69,70,71,72]. Among the main ones, monosodium glutamate [73], carboxymethylcellulose, and polysorbate-80 stand out [74]. Finally, chemical compounds present in plastic packaging may be associated with obesity, for example, phthalates [7,75,76] and bisphenol A [66,75,76,77,78,79,80,81]. These mechanisms highlight the importance of encouraging individuals on hemodialysis to limit the consumption of UPF in order to improve the nutritional status of abdominal obesity.
In our study, men were 2.21 times more likely to have abdominal obesity compared to women, corroborating the work by Jang and Oh [82], which found an increase of approximately 52% in the prevalence of abdominal obesity in Koreans after 20 years, but with less change observed in women. Men and women differ with regard to the distribution of adipose tissue, given that in men, adipose tissue preferentially accumulates in the visceral deposit, while the accumulation of fat occurs mainly in the subcutaneous deposit, in women [83,84]. The magnitude of this difference is amplified from the end of puberty to early adulthood, as males develop the typical android body shape, while females develop the gynoid form [83]. There is a hypothesis that for survival, through hunting and escape, fast, prehistoric man would need a more easily mobilized source of energy, hence the preference for storing fat in the visceral deposit [7,83]. Furthermore, these differences in fat distribution between genders can be attributed to the influence of sex hormones [85], since studies have shown a positive association between testosterone and android adiposity, as well as between estrogen and gynoid fat deposition [86].
We also found that adults were 2 times more likely to have abdominal obesity than the elderly. This finding is similar to studies that found, in men, a higher risk [87,88] and chance [89] of abdominal obesity in adults when compared to the elderly. For example, in a population-based cohort from Tehran, those aged 30 to 39 years had a 1.05 times greater risk of developing abdominal obesity, while those aged 50 to 69 years had a negative association with abdominal obesity, so being in this age range was considered a protective factor [87]. Furthermore, in Norway, during eight years of follow-up, those aged between 35 and 69 years were the ones who developed an increase in WC, while those aged 70 to 80 years developed a reduction [88]. And finally, in China, the annual OR for abdominal obesity decreased significantly with age [89]. A possible justification for the results found, in our and in the aforementioned studies, is that adipose tissue increases in middle age and decreases at the end of life [90], and during the aging process, fat is redistributed from the subcutaneous tissue to abdominal deposits, as well as to skeletal muscle, heart, liver, pancreas, or blood vessels [91,92].
In our study, lower education increased the chances of having abdominal obesity, corroborating representative data from Korea [45] and Portugal [93] Accordingly, higher education was considered a protective factor for abdominal obesity in Spanish [94] and Iranian adults [95]. Several factors must be considered to explain the effects of education on abdominal obesity. People with low education are less concerned with the consequences of abdominal obesity, mainly because they do not receive formal education, awareness about cardiovascular risk factors [96], and are exposed to the selection of unhealthy diets [97]. In contrast, educated people are more aware of the consequences of the disease [98,99] and tend to have a healthier diet, characterized by higher consumption of fruits and vegetables, together with lower consumption of fats, thus maintaining preventive measures for abdominal obesity [95]. We observe, therefore, that health professionals need to use health education strategies in order to make the information passed on more understandable, since individuals with less education have less perception of the consequences of abdominal obesity.
Finally, those who practiced physical activity below the recommended level were 1.95 times more likely to have abdominal obesity. Similar results were found in: Burkina Faso [100], Ivory Coast [96], United Kingdom [17], Ethiopia [101], and Korea [102]. Individuals with low and moderate physical activity were 1.51 and 1.19 times more likely to have abdominal obesity, respectively [100]. In Ivory Coast [96] and the United Kingdom [17], the prevalence of abdominal obesity was higher among those with less physical activity. Lastly, a sedentary lifestyle increased the chances of having abdominal obesity in Ethiopia [101] and Korea [102]. Physical inactivity plays a central role as an independent and strong risk factor for the accumulation of visceral fat [103], with repercussions on general and abdominal obesity [104,105]. The literature also shows that stress is associated with a lack of physical activity, which tends to increase cortisol secretion and the risk of abdominal obesity [100]. In this sense, the practice of physical exercise is important to help prevent abdominal obesity [101], since the contraction of skeletal muscles releases myokines, which function similarly to a hormone, exerting specific endocrine effects on visceral fat, while other myokines act locally within muscle, through paracrine mechanisms, exerting effects on signaling pathways involved in fat oxidation [103]. Physical activity is, therefore, an important determinant of health for the intervention of health professionals working in hemodialysis clinics.
As strengths of our study, we have the originality, considering that this is the first study to our knowledge, to analyze the relationship between the consumption of UPF and abdominal obesity in individuals undergoing hemodialysis. Also, the study population, consisted of patients from all hemodialysis clinics in the analyzed region. Another strength was the use of the NOVA food classification system, which has been recognized as a valid tool for nutrition and public health research and policy by Pan American Health Organization [106]. As limitations, we have the possible reverse causality, due to the cross-sectional design of the research. In addition, the instrument used to collect the consumption of UPF, which did not collect the ingested portions and was subject to memory bias, may not have allowed an accurate estimate of consumption.
5. Conclusions
The results of our study demonstrate that the prevalence of abdominal obesity in individuals undergoing hemodialysis is high. In addition, they point out that higher consumption of UPF, be male and adult, have less education and practice physical activity below the recommended level increased the chances of having abdominal obesity in these individuals. Our work highlights health determinants for which health professionals who work in this population should pay attention and intervene. In addition, it provides a basis for the creation and improvement of public policies that promote changes in these determinants. We suggest future research to investigate whether the associations remain in individuals undergoing hemodialysis in other regions of the world, in addition to longitudinal studies, to establish causality between the variables.
Author Contributions
Sara Jarske Gering, Cleodice Alves Martins and Luciane Bresciani Salaroli conceptualized the idea. Nina Mara Paterlini Marques, Monica Cattafesta, Alexandre Cardoso da Cunha, Luciane Bresciani Salaroli, Fabíola Lacerda Pires Soares, and Edson Theodoro dos Santos Neto developed the protocol and instruments to data collection. Cleodice Alves Martins conducted the statistical analysis. Sara Jarske Gering, Cleodice Alves Martins, Luciane Bresciani Salaroli, Nina Mara Paterlini Marques, Monica Cattafesta, Fabíola Lacerda Pires Soares, Alexandre Cardoso da Cunha, and Edson Theodoro dos Santos Neto wrote the essay for the article and provided critical manuscript revisions. Luciane Bresciani Salaroli supervised all the aspects of the project. All authors approved the final manuscript prior to submission.
Funding
This study received financial support from the Fundação de Amparo à Pesquisa e Inovação do Espírito Santo (FAPES) no. 35081.543.19306.18042018. Notice no. 03/2018 - Programa de Pesquisa para o SUS (PPSUS). City: Vitória, State: Espírito Santo and Country: Brasil.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Research Ethics Committee nº. 4.023.221 (CAAE 68528817.4.0000.5060, 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be partially available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.-C.; Jaime, P.; Martins, A.P.; Canela, D.; Louzada, M.; Parra, D. NOVA. The Star Shines Bright. World Nutr. 2016, 7, 28–38. [Google Scholar]
- Baker, P.; Machado, P.; Santos, T.; Sievert, K.; Backholer, K.; Hadjikakou, M.; Russell, C.; Huse, O.; Bell, C.; Scrinis, G.; et al. Ultra-processed Foods and the Nutrition Transition: Global, Regional and National Trends, Food Systems Transformations and Political Economy Drivers. Obes. Rev. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-Processed Products Are Becoming Dominant in the Global Food System. Obes. Rev. 2013, 14, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares: 2017-2018: Avaliação Nutricional da Disponibilidade Domiciliar de Alimentos no Brasil / IBGE, Coordenação de Trabalho e Rendimento; Instituto Brasileiro de Geografia e Estatística: Rio de Janeiro, 2020. Available online: https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=2101704.
- Caballero, B. Humans Against Obesity: Who Will Win? Adv. Nutr. 2019, 10 (Suppl. 1), S4–S9. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.P.C.; Vergara, C.M.A.C.; Sampaio, H.A.d.C.; Vasconcelos Filho, J.E.; Strozberg, F.; Ferreira Neto, J.F.R.; Mafra, M.L.P.; Garcia Filho, C.; Carioca Filho, A.A.F. Food and Nutrition Surveillance System: Temporal Trend of Coverage and Nutritional Status of Adults Registered on the System, Brazil, 2008-2019. Epidemiologia Serv. Saude 2022, 31. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-l.; Lv, J.; Du, Z.-p.; Feng, S.; Sheng, J.; Jin, Z.-x.; Liu, K.-y.; Gao, H.; Li, X.-d.; Cao, H.-j.; et al. The Levels of Phthalate Exposure and Associations With Obesity in an Elderly Population in China. Ecotoxicol. Environ. Saf. 2020, 201, 110749. [Google Scholar] [CrossRef] [PubMed]
- Perez-Campos, E.; Mayoral, L.-C.; Andrade, G.; Mayoral, E.-C.; Huerta, T.; Canseco, S.; Rodal Canales, F.; Cabrera-Fuentes, H.; Cruz, M.; Pérez Santiago, A.; et al. Obesity Subtypes, Related Biomarkers & Heterogeneity. Indian J. Med. Res. 2020, 151, 11. [Google Scholar] [CrossRef] [PubMed]
- Eickemberg, M.; Amorim, L.D.A.F.; Almeida, M.d.C.C.d.; Pitanga, F.J.G.; Aquino, E.M.L.d.; Fonseca, M.d.J.M.d.; Matos, S.M.A. Obesidade abdominal no ELSA-Brasil: Construção de padrão-ouro latente e avaliação da acurácia de indicadores diagnósticos. Cienc. & Saude Coletiva 2020, 25, 2985–2998. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, D.; Sharma, S. Abdominal Obesity, Adipokines and Non-Communicable Diseases. J. Steroid Biochem. Mol. Biol. 2020, 203, 105737. [Google Scholar] [CrossRef]
- Bosomworth, N.J. Normal-Weight Central Obesity: Unique Hazard of the Toxic Waist. Can. Fam. Physician 2019, 65, 399–408. [Google Scholar]
- Fang, H.; Berg, E.; Cheng, X.; Shen, W. How to Best Assess Abdominal Obesity. Curr. Opin. Clin. Nutr. & Metab. Care 2018, 21, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Raynor, H.A.; Champagne, C.M. Position of the Academy of Nutrition and Dietetics: Interventions for the Treatment of Overweight and Obesity in Adults. J. Acad. Nutr. Diet. 2016, 116, 129–147. [Google Scholar] [CrossRef] [PubMed]
- Balkau, B.; Deanfield, J.E.; Després, J.-P.; Bassand, J.-P.; Fox, K.A.A.; Smith, S.C.; Barter, P.; Tan, C.-E.; Van Gaal, L.; Wittchen, H.-U.; et al. International Day for the Evaluation of Abdominal Obesity (IDEA). Circulation 2007, 116, 1942–1951. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Katzmarzyk, P.T.; Ross, R. Waist Circumference and Not Body Mass Index Explains Obesity-Related Health Risk. Am. J. Clin. Nutr. 2004, 79, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Juul, F.; Martinez-Steele, E.; Parekh, N.; Monteiro, C.A.; Chang, V.W. Ultra-Processed Food Consumption and Excess Weight Among US Adults. Br. J. Nutr. 2018, 120, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Rauber, F.; Steele, E.M.; Louzada, M.L.d.C.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Indicators of Obesity in the United Kingdom Population (2008-2016). PLOS ONE 2020, 15, e0232676. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.P.; Steele, E.M.; Levy, R.B.; da Costa Louzada, M.L.; Rangan, A.; Woods, J.; Gill, T.; Scrinis, G.; Monteiro, C.A. Ultra-Processed Food Consumption and Obesity in the Australian Adult Population. Nutr. & Diabetes 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Park, J.M.; Oh, S.U.; Ha, K.; Joung, H. Consumption of Ultra-Processed Foods Increases the Likelihood of Having Obesity in Korean Women. Nutrients 2021, 13, 698. [Google Scholar] [CrossRef] [PubMed]
- Canhada, S.L.; Luft, V.C.; Giatti, L.; Duncan, B.B.; Chor, D.; Fonseca, M.d.J.M.d.; Matos, S.M.A.; Molina, M.d.C.B.; Barreto, S.M.; Levy, R.B.; et al. Ultra-Processed Foods, Incident Overweight and Obesity, and Longitudinal Changes in Weight and Waist Circumference: The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Public Health Nutr. 2019, 23, 1076–1086. [Google Scholar] [CrossRef]
- KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 Update. Am. J. Kidney Dis. 2012, 60, 850–886. [CrossRef]
- Neves, P.D.M. d. M.; Sesso, R.d.C.C.; Thomé, F.S.; Lugon, J.R.; Nascimento, M.M. Brazilian Dialysis Survey 2019. Braz. J. Nephrol. 2021, 43, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic Kidney Disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef] [PubMed]
- Nerbass, F.B.; Lima, H. d. N.; Thomé, F.S.; Vieira Neto, O.M.; Lugon, J.R.; Sesso, R. Brazilian Dialysis Survey 2020. Braz. J. Nephrol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.T.; Araujo, R.M.; Vogt, B.P.; Barretti, P.; Caramori, J.C.T. Most Consumed Processed Foods by Patients on Hemodialysis: Alert for Phosphate-Containing Additives and the Phosphate-to-Protein Ratio. Clin. Nutr. ESPEN 2016, 14, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Hulbert-Shearon, T.; Levin, N.; Port, F. Association of Serum Phosphorus and Calcium X Phosphate Product With Mortality Risk in Chronic Hemodialysis Patients: A National Study. Am. J. Kidney Dis. 1998, 31, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Foley, R.; Parfrey, P.; Sarnak, M. Clinical Epidemiology of Cardiovascular Disease in Chronic Renal Disease. Am. J. Kidney Dis. 1998, 32, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Kestenbaum, B.; Sampson, J.N.; Rudser, K.D.; Patterson, D.J.; Seliger, S.L.; Young, B.; Sherrard, D.J.; Andress, D.L. Serum Phosphate Levels and Mortality Risk Among People With Chronic Kidney Disease. J. Am. Soc. Nephrol. 2004, 16, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Block, G.A. Mineral Metabolism, Mortality, and Morbidity in Maintenance Hemodialysis. J. Am. Soc. Nephrol. 2004, 15, 2208–2218. [Google Scholar] [CrossRef] [PubMed]
- Parpia, A.S.; L’Abbé, M.; Goldstein, M.; Arcand, J.; Magnuson, B.; Darling, P.B. The Impact of Additives on the Phosphorus, Potassium, and Sodium Content of Commonly Consumed Meat, Poultry, and Fish Products Among Patients With Chronic Kidney Disease. J. Ren. Nutr. 2018, 28, 83–90. [Google Scholar] [CrossRef]
- Osté, M.C.J.; Duan, M.J.; Gomes-Neto, A.W.; Vinke, P.C.; Carrero., J.J.; Avesani., C.; Cai., Q.; Dekker, L.H.; Navis, G.J.; Bakker, S.J.L.; Corpeleijn, E. Ultra-Processed Foods and Risk of All-Cause Mortality in Renal Transplant Recipients. Am J Clin Nutr. 2022, 115. [Google Scholar] [CrossRef]
- Prasad, R.; Jha, R.K.; Keerti, A. Chronic Kidney Disease: Its Relationship With Obesity. Cureus 2022. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, Y.; Eriguchi, R.; Sato, Y.; Nakaya, Y. Chronic hemodialysis patients with visceral obesity have a higher risk for cardiovascular events. Asia Pac. J. Clin. Nutr. 2011, 20. [Google Scholar]
- El Said, H.W.; Mohamed, O.M.; El Said, T.W.; El Serwi, A.B. Central Obesity and Risks of Cardiovascular Events and Mortality in Prevalent Hemodialysis Patients. Int. Urol. Nephrol. 2017, 49, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Postorino, M.; Marino, C.; Tripepi, G.; Zoccali, C. Abdominal Obesity and All-Cause and Cardiovascular Mortality in End-Stage Renal Disease. J. Am. Coll. Cardiol. 2009, 53, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.; Sozio, S.M.; Jaar, B.G.; McAdams-DeMarco, M.A.; Estrella, M.M.; Tereshchenko, L.G.; Monroy-Trujillo, J.M.; Parekh, R.S. Association of Abdominal Adiposity With Cardiovascular Mortality in Incident Hemodialysis. Am. J. Nephrol. 2018, 48, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Han, K.-D.; Choi, H.S.; Bae, E.H.; Ma, S.K.; Kim, S.W. Association of Body Mass Index and Waist Circumference With All-Cause Mortality in Hemodialysis Patients. J. Clin. Med. 2020, 9, 1289. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, H.; Lan, X.; Qin, X.; Huang, Y.; Wang, J.; Luo, P.; Wen, Z.; Li, Y.; Kong, Y.; et al. Low BMI and High Waist-to-Hip Ratio Are Associated With Mortality Risk Among Hemodialysis Patients: A Multicenter Prospective Cohort Study. Clin. Kidney J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Waxman, A. Who Global Strategy on Diet, Physical Activity and Health. Food Nutr. Bull. 2004, 25, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.J.; Roache, A.F.; Martorell, R. Anthropometric standardization reference manual; Human Kinetics Books; 1988. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, 2000; Available online: https://apps.who.int/iris/handle/10665/42330.
- Hunter, G.R.; Kekes-Szabo, T.; Snyder, S.W.; Nicholson, C.; Nyikos, I.; Berland, L. Fat Distribution, Physical Activity, and Cardiovascular Risk Factors. Med. &Amp;amp Sci. Sports &Amp;amp Exerc. 1997, 29, 362–369. [Google Scholar] [CrossRef]
- Ministério da Saúde. Vigitel Brasil 2019 - Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico: Estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados brasileiros e no Distrito Federal em 2019; Brasil, Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis; 2020. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2019_vigilancia_fatores_risco.pdf.
- Marques, N.M.P.; Cattafesta, M.; Soares, F.L.P.; Petarli, G.B.; Paixão, M.P.C.P.; Martins, C.A.; Neto, E.T.S.N.; Salaroli, L.B. Consumption of Minimally Processed and Ultra-Processed Foods by Individuals on Hemodialysis in Southeastern Brazil. J. Hum. Growth Dev. 2022, 32, 237–251. [Google Scholar] [CrossRef]
- Evangelista, L.S.; Cho, W.-K.; Kim, Y. Obesity and Chronic Kidney Disease: A Population-Based Study Among South Koreans. PLOS ONE 2018, 13, e0193559. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, Z.; Moosa, M.R.; Blaauw, R. Obesity and Other Nutrition Related Abnormalities in Pre-Dialysis Chronic Kidney Disease (CKD) Participants. Nutrients 2020, 12, 3608. [Google Scholar] [CrossRef]
- Dierkes, J.; Dahl, H.; Lervaag Welland, N.; Sandnes, K.; Sæle, K.; Sekse, I.; Marti, H.-P. High Rates of Central Obesity and Sarcopenia in CKD Irrespective of Renal Replacement Therapy – An Observational Cross-Sectional Study. BMC Nephrol. 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.T.V. d. S.; Vaz, I.M.F.; Ferraz, S.F.; Peixoto, M.d.R.G.; Campos, M.I.V.M.; Fornés, N.S. Prevalence and associated factors with abdominal obesity in hemodialysis patients in Goiânia - GO. J. Bras. Nefrol. 2013, 35, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.A.; Ferreira, J.R.S.; Cattafesta, M.; Neto, E.T.D.S.; Rocha, J.L.M.; Salaroli, L.B. Cut Points of the Conicity Index as an Indicator of Abdominal Obesity in Individuals Undergoing Hemodialysis: An Analysis of Latent Classes. Nutrition 2022, 111890. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA Food Classification and the Trouble With Ultra-Processing. Public Health Nutr. 2017, 21, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; de Castro, I.R.R.; Cannon, G. Increasing Consumption of Ultra-Processed Foods and Likely Impact on Human Health: Evidence From Brazil. Public Health Nutr. 2010, 14, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Moubarac, J.-C.; Martins, A.P.B.; Claro, R.M.; Levy, R.B.; Cannon, G.; Monteiro, C.A. Consumption of Ultra-Processed Foods and Likely Impact on Human Health. Evidence From Canada. Public Health Nutr. 2012, 16, 2240–2248. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e3. [Google Scholar] [CrossRef]
- Shim, J.-S.; Shim, S.Y.; Cha, H.-J.; Kim, J.; Kim, H.C. Association Between Ultra-Processed Food Consumption and Dietary Intake and Diet Quality in Korean Adults. J. Acad. Nutr. Diet. 2021. [Google Scholar] [CrossRef] [PubMed]
- Poti, J.M.; Mendez, M.A.; Ng, S.W.; Popkin, B.M. Is the Degree of Food Processing and Convenience Linked With the Nutritional Quality of Foods Purchased by US Households? Am. J. Clin. Nutr. 2015, 101, 1251–1262. [Google Scholar] [CrossRef] [PubMed]
- Rauber, F.; da Costa Louzada, M.L.; Steele, E.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef] [PubMed]
- Martínez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The Share of Ultra-Processed Foods and the Overall Nutritional Quality of Diets in the US: Evidence From a Nationally Representative Cross-Sectional Study. Popul. Health Metr. 2017, 15. [Google Scholar] [CrossRef] [PubMed]
- Louzada, M.L. d. C.; Ricardo, C.Z.; Steele, E.M.; Levy, R.B.; Cannon, G.; Monteiro, C.A. The Share of Ultra-Processed Foods Determines the Overall Nutritional Quality of Diets in Brazil. Public Health Nutr. 2017, 21, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Marrón-Ponce, J.A.; Flores, M.; Cediel, G.; Monteiro, C.A.; Batis, C. Associations Between Consumption of Ultra-Processed Foods and Intake of Nutrients Related to Chronic Non-Communicable Diseases in Mexico. J. Acad. Nutr. Diet. 2019, 119, 1852–1865. [Google Scholar] [CrossRef] [PubMed]
- Wee, M.S.M.; Goh, A.T.; Stieger, M.; Forde, C.G. Correlation of Instrumental Texture Properties From Textural Profile Analysis (TPA) With Eating Behaviours and Macronutrient Composition for a Wide Range of Solid Foods. Food & Funct. 2018, 9, 5301–5312. [Google Scholar] [CrossRef]
- Fardet, A. Minimally Processed Foods Are More Satiating and Less Hyperglycemic Than Ultra-Processed Foods: A Preliminary Study With 98 Ready-to-Eat Foods. Food & Funct. 2016, 7, 2338–2346. [Google Scholar] [CrossRef]
- Fardet, A.; Méjean, C.; Labouré, H.; Andreeva, V.A.; Feron, G. The Degree of Processing of Foods Which Are Most Widely Consumed by the French Elderly Population Is Associated With Satiety and Glycemic Potentials and Nutrient Profiles. Food & Funct. 2017, 8, 651–658. [Google Scholar] [CrossRef]
- de Graaf, C.; Kok, F.J. Slow Food, Fast Food and the Control of Food Intake. Nat. Rev. Endocrinol. 2010, 6, 290–293. [Google Scholar] [CrossRef]
- Forde, C.G.; van Kuijk, N.; Thaler, T.; de Graaf, C.; Martin, N. Texture and Savoury Taste Influences on Food Intake in a Realistic Hot Lunch Time Meal. Appetite 2013, 60, 180–186. [Google Scholar] [CrossRef] [PubMed]
- McCrickerd, K.; Lim, C.M.; Leong, C.; Chia, E.M.; Forde, C.G. Texture-Based Differences in Eating Rate Reduce the Impact of Increased Energy Density and Large Portions on Meal Size in Adults. J. Nutr. 2017, 147, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Forde, C.G.; Mars, M.; de Graaf, K. Ultra-Processing or Oral Processing? A Role for Energy Density and Eating Rate in Moderating Energy Intake From Processed Foods. Curr. Dev. Nutr. 2020, 4. [Google Scholar] [CrossRef] [PubMed]
- Zinöcker, M.; Lindseth, I. The Western Diet–Microbiome-Host Interaction and Its Role in Metabolic Disease. Nutrients 2018, 10, 365. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.N.; Chassard, C.; Lacroix, C. Gut Microbial Adaptation to Dietary Consumption of Fructose, Artificial Sweeteners and Sugar Alcohols: Implications for Host-Microbe Interactions Contributing to Obesity. Obes. Rev. 2012, 13, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Pearlman, M.; Obert, J.; Casey, L. The Association Between Artificial Sweeteners and Obesity. Curr. Gastroenterol. Rep. 2017, 19. [Google Scholar] [CrossRef]
- Suez, J.; Korem, T.; Zeevi, D.; Zilberman-Schapira, G.; Thaiss, C.A.; Maza, O.; Israeli, D.; Zmora, N.; Gilad, S.; Weinberger, A.; et al. Artificial Sweeteners Induce Glucose Intolerance by Altering the Gut Microbiota. Nature 2014, 514, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Miclotte, L.; Van de Wiele, T. Food Processing, Gut Microbiota and the Globesity Problem. Crit. Rev. Food Sci. Nutr. 2019, 60, 1769–1782. [Google Scholar] [CrossRef] [PubMed]
- Shannon, M.; Green, B.; Willars, G.; Wilson, J.; Matthews, N.; Lamb, J.; Gillespie, A.; Connolly, L. The Endocrine Disrupting Potential of Monosodium Glutamate (MSG) on Secretion of the Glucagon-Like Peptide-1 (GLP-1) Gut Hormone and GLP-1 Receptor Interaction. Toxicol. Lett. 2017, 265, 97–105. [Google Scholar] [CrossRef]
- Chassaing, B.; Koren, O.; Goodrich, J.K.; Poole, A.C.; Srinivasan, S.; Ley, R.E.; Gewirtz, A.T. Dietary Emulsifiers Impact the Mouse Gut Microbiota Promoting Colitis and Metabolic Syndrome. Nature 2015, 519, 92–96. [Google Scholar] [CrossRef]
- Zhang, Y.; Dong, T.; Hu, W.; Wang, X.; Xu, B.; Lin, Z.; Hofer, T.; Stefanoff, P.; Chen, Y.; Wang, X.; et al. Association Between Exposure to a Mixture of Phenols, Pesticides, and Phthalates and Obesity: Comparison of Three Statistical Models. Environ. Int. 2019, 123, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Kolena, B.; Hlisníková, H.; Kečkéšová, Ľ.; Šidlovská, M.; Trnovec, T.; Petrovičová, I. Risk of Abdominal Obesity Associated With Phthalate Exposure of Nurses. Toxics 2022, 10, 143. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Li, M.; Chen, B.; Xu, M.; Xu, Y.; Huang, Y.; Lu, J.; Chen, Y.; Wang, W.; Li, X.; et al. Urinary Bisphenol a (BPA) Concentration Associates With Obesity and Insulin Resistance. J. Clin. Endocrinol. & Metab. 2012, 97, E223–E227. [Google Scholar] [CrossRef] [PubMed]
- Ko, A.; Hwang, M.-S.; Park, J.-H.; Kang, H.-S.; Lee, H.-S.; Hong, J.-H. Association Between Urinary Bisphenol a and Waist Circumference in Korean Adults. Toxicol. Res. 2014, 30, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Savastano, S.; Tarantino, G.; D’Esposito, V.; Passaretti, F.; Cabaro, S.; Liotti, A.; Liguoro, D.; Perruolo, G.; Ariemma, F.; Finelli, C.; et al. Bisphenol-a Plasma Levels Are Related to Inflammatory Markers, Visceral Obesity and Insulin-Resistance: A Cross-Sectional Study on Adult Male Population. J. Transl. Med. 2015, 13. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Lehmler, H.-J.; Sun, Y.; Xu, G.; Liu, Y.; Zong, G.; Sun, Q.; Hu, F.B.; Wallace, R.B.; Bao, W. Bisphenol a Substitutes and Obesity in US Adults: Analysis of a Population-Based, Cross-Sectional Study. Lancet Planet. Health 2017, 1, e114–e122. [Google Scholar] [CrossRef] [PubMed]
- Hao, M.; Ding, L.; Xuan, L.; Wang, T.; Li, M.; Zhao, Z.; Lu, J.; Xu, Y.; Chen, Y.; Wang, W.; et al. Urinary Bisphenol a Concentration and the Risk of Central Obesity in Chinese Adults: A Prospective Study. J. Diabetes 2017, 10, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.-J.; Oh, H. Trends and Inequalities in Overall and Abdominal Obesity by Sociodemographic Factors in Korean Adults, 1998–2018. Int. J. Environ. Res. Public Health 2021, 18, 4162. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Clegg, D.J. The Sexual Dimorphism of Obesity. Mol. Cell. Endocrinol. 2015, 402, 113–119. [Google Scholar] [CrossRef]
- Valencak, T.G.; Osterrieder, A.; Schulz, T.J. Sex Matters: The Effects of Biological Sex on Adipose Tissue Biology and Energy Metabolism. Redox Biol. 2017, 12, 806–813. [Google Scholar] [CrossRef]
- Peters, S.A.E.; Bots, S.H.; Woodward, M. Sex Differences in the Association Between Measures of General and Central Adiposity and the Risk of Myocardial Infarction: Results From the UK Biobank. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Karastergiou, K.; Smith, S.R.; Greenberg, A.S.; Fried, S.K. Sex Differences in Human Adipose Tissues – The Biology of Pear Shape. Biol. Sex Differ. 2012, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Barzin, M.; Piri, Z.; Serahati, S.; Valizadeh, M.; Azizi, F.; Hosseinpanah, F. Incidence of Abdominal Obesity and Its Risk Factors Among Tehranian Adults. Public Health Nutr. 2018, 21, 3111–3117. [Google Scholar] [CrossRef] [PubMed]
- Løvsletten, O.; Jacobsen, B.K.; Grimsgaard, S.; Njølstad, I.; Wilsgaard, T.; Løchen, M.-L.; Eggen, A.E.; Hopstock, L.A. Prevalence of General and Abdominal Obesity in 2015–2016 and 8-Year Longitudinal Weight and Waist Circumference Changes in Adults and Elderly: The Tromsø Study. BMJ Open 2020, 10, e038465. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Peng, Q.; Yang, Y.; Zheng, S.; Wang, Y.; Lu, W. The Prevalence and Increasing Trends of Overweight, General Obesity, and Abdominal Obesity Among Chinese Adults: A Repeated Cross-Sectional Study. BMC Public Health 2019, 19. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Pahor, M.; Tylavsky, F.; Kritchevsky, S.B.; Cauley, J.A.; Newman, A.B.; Blunt, B.A.; Harris, T.B. One- And Two-Year Change in Body Composition as Measured by DXA in a Population-Based Cohort of Older Men and Women. J. Appl. Physiol. 2003, 94, 2368–2374. [Google Scholar] [CrossRef] [PubMed]
- Kuk, J.L.; Saunders, T.J.; Davidson, L.E.; Ross, R. Age-Related Changes in Total and Regional Fat Distribution. Ageing Res. Rev. 2009, 8, 339–348. [Google Scholar] [CrossRef]
- Tchkonia, T.; Morbeck, D.E.; Von Zglinicki, T.; Van Deursen, J.; Lustgarten, J.; Scrable, H.; Khosla, S.; Jensen, M.D.; Kirkland, J.L. Fat Tissue, Aging, and Cellular Senescence. Aging Cell 2010, 9, 667–684. [Google Scholar] [CrossRef] [PubMed]
- Sardinha, L.B.; Santos, D.A.; Silva, A.M.; Coelho-e-Silva, M.J.; Raimundo, A.M.; Moreira, H.; Santos, R.; Vale, S.; Baptista, F.; Mota, J. Prevalence of Overweight, Obesity, and Abdominal Obesity in a Representative Sample of Portuguese Adults. PLoS ONE 2012, 7, e47883. [Google Scholar] [CrossRef]
- López-Sobaler, A.M.; Rodríguez-Rodríguez, E.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. General and Abdominal Obesity Is Related to Physical Activity, Smoking and Sleeping Behaviours and Mediated by the Educational Level: Findings From the ANIBES Study in Spain. PLOS ONE 2016, 11, e0169027. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K.O.; Heidari, B. Association of Educational Level With Risk of Obesity and Abdominal Obesity in Iranian Adults. J. Public Health 2009, 32, 202–209. [Google Scholar] [CrossRef]
- Malik, K.S.; Kouame, J.; Gbane, M.; Coulibaly, M.; Ake, D.M.; Ake, O. Prevalence of Abdominal Obesity and Its Correlates Among Adults in a Peri-Urban Population of West Africa. AIMS Public Health 2019, 6, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Dagne, S.; Menber, Y.; Petrucka, P.; Wassihun, Y. Prevalence and Associated Factors of Abdominal Obesity Among the Adult Population in Woldia Town, Northeast Ethiopia, 2020: Community-Based Cross-Sectional Study. PLOS ONE 2021, 16, e0247960. [Google Scholar] [CrossRef]
- Czernichow, S.; Bertrais, S.; Preziosi, P.; Galan, P.; Hercberg, S.; Oppert, J. Indicators of Abdominal Adiposity in Middle-Aged Participants of the SU.VI.MAX Study: Relationships With Educational Level, Smoking Status and Physical Inactivity. Diabetes & Metab. 2004, 30, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Vernay, M.; Malon, A.; Oleko, A.; Salanave, B.; Roudier, C.; Szego, E.; Deschamps, V.; Hercberg, S.; Castetbon, K. Association of Socioeconomic Status With Overall Overweight and Central Obesity in Men and Women: The French Nutrition and Health Survey 2006. BMC Public Health 2009, 9. [Google Scholar] [CrossRef]
- Cisse, K.; Samadoulougou, S.; Ouedraogo, M.; Kouanda, S.; Kirakoya-Samadoulougou, F. Prevalence of Abdominal Obesity and Its Association With Cardiovascular Risk Among the Adult Population in Burkina Faso: Findings From a Nationwide Cross-Sectional Study. BMJ Open 2021, 11, e049496. [Google Scholar] [CrossRef] [PubMed]
- Dagne, S.; Menber, Y.; Petrucka, P.; Wassihun, Y. Prevalence and Associated Factors of Abdominal Obesity Among the Adult Population in Woldia Town, Northeast Ethiopia, 2020: Community-Based Cross-Sectional Study. PLOS ONE 2021, 16, e0247960. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, T.S.; Zeleke, T.M.; Alemu, W.; Argaw, D.; Bedane, T.K. Dietary Diversity and Physical Activity as Risk Factors of Abdominal Obesity Among Adults in Dilla Town, Ethiopia. PLOS ONE 2020, 15, e0236671. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K. The Diseasome of Physical Inactivity - And the Role of Myokines in Muscle-Fat Cross Talk. J. Physiol. 2009, 587, 5559–5568. [Google Scholar] [CrossRef]
- Slentz, C.A.; Houmard, J.A.; Kraus, W.E. Exercise, Abdominal Obesity, Skeletal Muscle, and Metabolic Risk: Evidence for a Dose Response. Obesity 2009, 17, S27–S33. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C.J. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Forceon Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World HeartFederation; International Atherosclerosis Society; And International Association for the Study of Obesity. Obes. Metab. 2010, 7, 63–65. [Google Scholar] [CrossRef]
- Pan American Health Organization. Ultra-Processed Food and Drink Products in Latin America: Trends, Impact on Obesity, Policy Implications; Washington, Pan American Health Organization; 2015; Available online: https://iris.paho.org/handle/10665.2/7699.

Table 1.
Descriptive characterization and bivariate analysis between the independent variables and the outcome in individuals undergoing hemodialysis. (to be continued).
Table 1.
Descriptive characterization and bivariate analysis between the independent variables and the outcome in individuals undergoing hemodialysis. (to be continued).
| Variables | Abdominal obesity | |||
|---|---|---|---|---|
| ABSENCE n = 231 (22.78%) |
PRESENCE n = 783 (77.22%) |
p-value a | Total n = 1014 (100%) |
|
| Sex n = 1014 | < 0.001 | |||
| Female | 65 (6.41) | 374 (36.88) | 439 (43.29) | |
| Male | 166 (16.37) | 409 (40.34) | 575 (56.71) | |
| Age range n = 1014 | < 0.001 | |||
| Adult | 168 (16.57) | 414 (40.83) | 582 (57.4) | |
| Elderly | 63 (6.21) | 369 (36.39) | 432 (69.22) | |
| Marital status n = 1014 | 0.919 | |||
| With partner | 128 (12.62) | 439 (43.29) | 567 (55.91) | |
| No partner | 103 (10.16) | 344 (33.93) | 447 (44.09) | |
| Race/Color n = 1013 | 0.494 | |||
| White | 57 (5.63) | 214 (21.12) | 271 (26.75) | |
| No white | 173 (17.08) | 569 (56.17) | 742 (73.25) | |
| Income (Minimum Wages) n = 971 | 0.179 | |||
| < 1 | 31 (3.19) | 74 (7.62) | 105 (10.81) | |
| 1–5 | 165 (17) | 570 (58.7) | 5.7) | |
| > 5–10 | 21 (2.16) | 66 (6.8) | 8.96) | |
| > 10 | 6 (0.62) | 38 (3.91) | 44 (4.53) | |
| Education (years) n = 1012 | 0.004 | |||
| < 8 | 95 (9.39%) | 425 (42) | 520 (51.39) | |
| 8 – 11 | 105 (10.37) | 231 (22.83) | 336 (33.2) | |
| > 11 | 31 (3.06) | 125 (12.35) | 156 (15.41) | |
| Work activity n = 1000 | 0.083 | |||
| With paid activity | 127 (12.7) | 365 (36.5) | 492 (49.2) | |
| No paid activity | 11 (1.1) | 37 (3.7) | 48 (4.8) | |
| Retired or on sick leave | 91 (9.1) | 369 (36.9) | 460 (46) | |
| Smoking n = 1008 | 0.329 | |||
| Smoker | 12 (1.19) | 41 (4.07) | 53 (5.26) | |
| Former smoker | 74 (7.34) | 293 (29.07) | 367 (36.41) | |
| Never smoked | 143 (14.18) | 445 (44.15) | 588 (58.33) | |
| CKD b Time (years) n = 1009 | 0.01 | |||
| ≤ 5 | 121 (11.99) | 483 (47.87) | 604 (59.86) | |
| > 5 | 110 (10.9) | 295 (29.24) | 405 (40.14) | |
| Hemodialysis time (years) n = 958 | 0.02 | |||
| < 1 | 10 (1.04) | 49 (5.11) | 59 (5.15) | |
| 1–5 | 107 (11.17) | 449 (46.87) | 8.04) | |
| > 5–10 | 54 (5.64) | 141 (14.72) | 195 (20.36) | |
| > 10 | 41 (4.28) | 107 (11.17) | 148 (15.45) | |
| Diabetes n = 1014 | < 0.001 | |||
| Absence | 175 (17.26) | 468 (46.15) | 643 (63.41) | |
| Presence | 56 (5.52) | 315 (31.07) | 371 (36.59) | |
| Hypertension n = 1014 | 0.323 | |||
| Absence | 42 (4.14) | 119 (11.74) | 161 (15.88) | |
| Presence | 189 (18.64) | 664 (65.48) | 853 (84.12) | |
| Physical activity n = 1013 | < 0.001 | |||
| Below recommended | 40 (3.95) | 71 (7.01) | 111 (10.96) | |
| Within the recommended | 34 (3.35) | 83 (8.19) | 117 (11.54) | |
| Does not practice | 156 (15.4) | 629 (62.1) | 785 (77.5) | |
| BMI c n = 951 | < 0.001 | |||
| No overweight | 195 (20.5) | 293 (30.8) | 488 (51.3) | |
| Overweight | 24 (2.5) | 439 (46.2) | 463 (48.7) | |
| UPF d Consumption n = 1014 | < 0.001 | |||
| Q1 + Q2 e | 102 (10.06) | 485 (47.83) | 587 (57.89) | |
| Q3 + Q4 e | 129 (12.72) | 298 (29.39) | 427 (42.11) | |
a p-value: Pearson’s chi-square test (x²) for qualitative variables. b CKD: Chronic Kidney Disease. c BMI: Body Mass Index. d UPF: Ultra-processed Foods. e Q1: Quartile 1. Q2: Quartile 2. Q3: Quartile 3. Q4: Quartile 4.
Table 2.
Hierarchical logistic regression between the associated variables in the bivariate analysis and the outcome of individuals undergoing hemodialysis. (to be continued).
Table 2.
Hierarchical logistic regression between the associated variables in the bivariate analysis and the outcome of individuals undergoing hemodialysis. (to be continued).
| Variables | Model 1 a | Model 2 b | Model 3 c | Final model d | ||||
|---|---|---|---|---|---|---|---|---|
| p-value e | OR f (CI95% g) | p-value e | OR f (CI95% g) | p-value e | OR f (CI95% g) | p-value e | OR f (CI95% g) | |
| UPF Consumption | ||||||||
| Q1 + Q2 i | 1 | 1 | 1 | 1 | ||||
| Q3 + Q4 i | < 0.001 | 1.77 (1.30–2.41) | 0.001 | 1.83 (1.34–2.50) | 0.001 | 1.72 (1.23–2.39) | 0.001 | 1.72 (1.23–2.39) |
| Sex | ||||||||
| Female | 1 | 1 | 1 | 1 | ||||
| Male | < 0.001 | 2.36 (1.70–3.28) | < 0.001 | 2.42 (1.72–3.38) | < 0.001 | 2.21 (1.55–3.16) | < 0.001 | 2.21 (1.55–3.16) |
| Age range | ||||||||
| Adult | < 0.001 | 2.31 (1.65–3.22) | < 0.001 | 2.23 (1.57–3.17) | < 0.001 | 2.00 (1.38–2.91) | < 0.001 | 2.00 (1.38–2.91) |
| Elderly | 1 | 1 | 1 | 1 | ||||
| Education (years) | ||||||||
| < 8 | 0.525 | 1.16 (0.73–1.84) | 0.498 | 1.17 (0.73–1.87) | 0.532 | 1.16 (0.71–1.90) | 0.532 | 1.16 (0.71–1.90) |
| 8–11 | 0.036 | 1.66 (1.03–2.67) | 0.034 | 1.67 (1.03–2.71) | 0.035 | 1.70 (1.03–2.79) | 0.035 | 1.70 (1.03–2.79) |
| > 11 | 1 | 1 | 1 | 1 | ||||
| Work activity | ||||||||
| With paid activity | 0.470 | 1.13 (0.80–1.58) | 0.507 | 1.12 (0.79–1.59) | ||||
| No paid activity | 0.812 | 1.10 (0.49–2.43) | 0.920 | 0.95 (0.40–2.28) | ||||
| Retired or on sick leave | 1 | 1 | ||||||
| Physical activity | ||||||||
| Below recommended | 1 | 1 | ||||||
| Within the recommended | 0.004 | 1.97 (1.23–3.14) | 0.004 | 1.97 (1.23–3.14) | ||||
| Does not practice | 0.389 | 1.23 (0.76–2.00) | 0.389 | 1.23 (0.76–2.00) | ||||
| CKD j time (years) | ||||||||
| ≤ 5 | 1 | |||||||
| > 5 | 0.698 | 1.29 (0.73–2.28) | ||||||
| Hemodialysis time (years) | ||||||||
| < 1 | 1 | |||||||
| 1–5 | 0.698 | 0.86 (0.40–1.81) | ||||||
| > 5–10 | 0.906 | 1.05 (0.44–2.51) | ||||||
| > 10 | 0.888 | 0.93 (0.38–2.30) | ||||||
a Model 1: Adjusted for UPF consumption + sociodemographic variables (sex, age range, and education). b Model 2: Adjusted for model variables 1 + work activity. c Model 3: Adjusted for model variables 2 + lifestyle and health variables (CKD time, hemodialysis time, and physical activity). Diabetes and BMI were not included in model 3, respectively, because it was self-reported and showed general obesity only. d Final model: Performed using the Forward LR method, in which the variables work activity, CKD time, and hemodialysis time were removed by the mathematical model itself. e p-value: Hierarchical logistic regression for the association of the outcome with the independent variables, including the variables that presented a value of p ≤ 0.1 in the bivariate analysis. f OR: Odds Ratio. g CI: 95% Confidence Interval. h UPF: Ultra-processed Foods. i Q1: Quartile 1. Q2: Quartile 2. Q3: Quartile 3. Q4: Quartile 4. j CKD: Chronic Kidney Disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



