
Submitted:
25 May 2024
Posted:
27 May 2024
You are already at the latest version
Abstract
Abstract
Sodium glucose cotransporter type 2 inhibitors are a new class of drugs acting on cardiovascular system, renal and metabolism in a multiple way. Indeed, even their principal action is on the transporter of sodium and glucose in the convoluted distal tubule, they have multiple actions as antifibrotic and endothelial protective action. Their principal mechanism consist in the loss of sodium and glucose. Therefore, they have effect on blood pressure and glucose metabolism. In a first period their use has been in the diabetic general population, later on some studies documented their activity in non-diabetic general population, in heart failure in chronic kidney disease. Only in recent years several small studies documented their efficacy in diabetic and non-diabetic kidney transplant patients, larger studies are few and very recent and open new ways for these drugs
Keywords:
Keywords. Sodium-glucose- cotransporters type 2 inhibitors
; glucose reabsorption
; sodium reabsorption
; randomized clinical trials
; diabetes
; heart failure
; chronic kidney disease
; kidney transplantati
Introduction
Since 2015, sequential randomized controlled trials (RCTs) have documented the efficacy of Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors in improving both kidney and cardiovascular outcomes. This was firstly documented in general population, later in patients with diabetes [1]. By 2020, 4 compounds (empagliflozin, canagliflozin, dapagliflozin and ertugliflozin) were studied in 47,000 patients with diabetes. Due to its action, later on these compounds were studied in patients with chronic kidney disease with or without diabetes. More recently, SGLT2 inhibitors have been used in kidney transplant patients. Several studies document the heart and renal protective effect in particular empaglifozin [2], canaglifozin [3], dapaglifozin [4].
Mechanism of action
The SGLT2 inhibitors mechanism of action is complex and exerted on heart, metabolism (Figure 1A) and renal (Figure 1B). The cardio protective effect includes direct cardiovascular effect and is manifested through improvements in cardiac parameters, decrease in heart failure as well as promotion in cardiac remodeling. In addition, there is an effect on cardiac fibrosis by modulating macrophage phagocytosis and downregulating of reactive oxygen and nitrogen specific pathways [5]. The indirect cardiovascular effect is exerted through the action on renal system. Additionally, the heart effect is exerted by the improvement of endothelial dysfunction and by the effect on sympathetic nervous system that lead to vasodilation, reduction of heart rate, reduction of preload and reduction in blood pressure.
The metabolic effect is exerted by increase in glucagon, increase in non-esterified fatty acids (NEFA), increase in ketone utilization, increase in lipolysis, increase in gluconeogenesis, and decrease of insulin. All these facts lead to a decrease in body weight, decrease in LDL and increase in HDL.
In addition, the renal effects of SGLT2 inhibitors are exerted by a direct and an indirect effect. A reduction in proinflammatory and profibrotic molecules, decrease in glomerular hyper filtration with dilation of afferent arterioles and increase in renal blood perfusion mediate the direct effect. By binding to Na+-H+ exchanger 3 enzyme there is a reduction in Na+ reabsorption. Finally there is a reduction in glomerular mesangial expansion, a reduction in macrophage infiltration and a reduction in interstitial fibrosis [6]. All these facts lead to glycosuria, natriuresis, reduction in proteinuria, reduction in kidney injury molecules.
The indirect effect is induced by a reduced in insulin secretion, an increase in glucagon secretion, an increase in erythropoietin and an increase in hematocrit and reticulocyte count. Additionally, the renal indirect effect adds beneficial effect on the heart.
Factors as glycosuria, natriuresis and tubule-glomerular feedback induce a reduction in body weight, reduction of blood pressure and improvement in HbA1c [7,8]. The ketone metabolism induced by glycosuria improves the heart failure (HF) [9]. Additionally, SGLT2 Inhibitors produce cardio renal benefits by promoting adaptive cellular reprogramming to induce a state of fasting mimicry. This happens by activating the sirtuin 1/AMP activated protein kinase (SIRT1/AMPK) pathway that have an antioxidant and anti-inflammatory effect, an enhanced autophagic flux and an activation of hypoxia- inducible factor (HIF-2α). The latter stimulates erythrocytosis. [10,11,12,13,14]. In addition, the SGLT2 inhibitors improve the endoplasmic reticulum stress [15,16]. Finally, Canagliflozin reduces inflammation and fibrosis biomarkers as documented in diabetic kidney disease [17].
All SGLT2 inhibitors are metabolized in less than 24 hours by O-glucuronization. In particular, they are only in part metabolized by cytochromes. SGLT2 inhibitors slightly inhibit CYP3A4 and ABCB1 [18]. Concerning canagliflozin, has been documented a 23% increase of cyclosporine in the blood [19].
Due to its complex mechanism of action SGLT2 inhibitors have been used principally in patients affected by type 2 diabetes, often in association with other antidiabetic drugs. In general population its efficacy has been documented in patients affected by heart failure and by metabolic diseases.
More recently, in consideration that type 2 diabetes, heart disease and metabolic diseases are often related to chronic kidney diseases and kidney transplantation and concur to their poor outcomes, several small and large studies have been made to investigate the SGLT2 inhibitors effect in kidney disease and kidney transplantation
It should also considered that several adverse events have been reported with the use of SGLT2 inhibitors.
SGLT2i act inhibiting the co-transportation of sodium-glucose in the proximal part of convoluted tubule, where 90% of glucose is reabsorbed [20,21]. As collateral effect, SGLT2 inhibitors may cause urinary and genital infections because of the osmotic diuresis. In older people, an additional collateral effect is the hypotension due the loss of volume.
Other less frequent adverse events are euglycemic diabetic acidosis, distal limb amputation and acute kidney injury [22]. Physiologically, SGLT2 inhibitors cause a vasoconstriction of the afferent arterial that may rarely cause a reduction in GFR. Euglycemic ketoacidosis is more frequent in type 1 diabetes, principally in kidney transplant patients. An increased risk of lower extremity amputation was seen in the CREDENCE trial with the use of Canagliflozin [23].
SGLT2i Action on Heart, Metabolism and Kidney in Patients without Diabetes
Multiple RCTs have examined the therapeutic effectiveness of SGLT2 inhibitors in patients affected by type 2 diabetes mellitus. Notably several studies have documented the effectiveness of SGLT2 inhibitors in non-diabetic patients affected by heart, metabolic, renal dysfunction.
Anker et al. [24] on 1874 patients documented that Empagliflozin decreased the risk of cardiovascular death and total hospitalization for heart failure (HF) by 25, 30% and decreased the rate of decline of eGFR (estimated glomerular filtration rate) and risk of adverse effect by 50%.
Diaz-Cruz et al. [25] documented that 3 months of Dapaglifozin decreased blood pressure by lowering 24 hours systolic blood pressure (SBP), nighttime SBP, mean arterial pressure, nocturnal hypertension.
Petrie et al. [26] demonstrated that Dapaglifozin was effective in reducing cardiovascular mortality and morbidity in patients with HF and reduced Ejection Fraction (EF).
Anker et al. again [27] documented on 5988 patients that Empaglifozin reduced the risk of cardiovascular deaths or hospitalization for HF in patients with left ventricular ejection fraction (LVEF) of 40% regardless of presence or absence of diabetes.
Several trials are looking at the efficacy of SGLT2 inhibitors on metabolic outcomes in patients without diabetes.
Bays et al. [28] documented that in overweight and obese subjects without diabetes, Canagliflozin significantly reduce body weight compared to placebo.
Neeland et al. [29] documented that Empagliflozin reduced endogenous glycerol-gluconeogenesis in obese adults without diabetes. Additionally, SGLT2 inhibitors may prevent type 2 diabetes in obesity.
Faerch et al. [30] demonstrated that treatment with Depagliflozin and interval-based exercise lead to similar but small improvements in glycemic variability compared to control and metformin therapy.
Finally, Veelen et al. [31] documented that Depagliflozin treatment of prediabetes insulin resistant individuals for 14 days resulted in significant metabolic adaptations, skeletal muscle metabolism, improved fat oxidation and mitochondrial oxidative capacity.
SGLT2 inhibitors trials looking at the efficacy of SGLT2 inhibitors on renal outcomes.
Heerspink et al. [32] in the DAPA-CKD trial on 4304 patients, documented the effect of Dapagliflozin were similar in participants with or without diabetes. It proven the most effective class of drug to prevent CKD progression since discovery of renin-angiotensin-system (RAS) inhibitor.
Harrington et al. [33] in the EMPA-KIDNEY trial on 6609 patients demonstrated that Empagliflozin lowered the risk of disease progression from kidney disease or death from CVD compared to placebo.
Most patients included in the above trials were affected by IgA nephropathy. As a result, the EMPA-KIDNEY and DAPA-CKD trials showed a 51% reduction in the risk of CKD progression in IgA nephropathy [34].
SGLT2 Inhibitors in Kidney Transplant Patients
The above-mentioned rationale also applies to kidney transplant patients, whose outcomes is deeply influenced by post-transplant diabetes, cardiovascular diseases and metabolic dysfunction.
A particular caution should be observed in treating kidney transplant patients because the incidence of infections (urinary tract infections and genital infections) could be enhanced by the immunosuppression. In addition, the incidence of acute kidney injury and the ketoacidosis encountered sometimes after transplantation could be enhanced by the SGTL2 inhibitors use.
Probably, this has been the cause of the less frequent use of SGLT2 inhibitors in kidney transplant patients until recently. Indeed, recently two large studies [35,36]
The potential benefits of SGLT2 inhibitors in CKD and kidney transplant patients are documented in Figure 2.
SGLT2 inhibitors have a direct effect on the tubular co-trans carrier that increases natriuresis and glycosuria. Indirectly, increased natriuresis has been shown to decrease glomerular hyper filtration by regulating the dense macula. This effect leads to a decrease in renal hyper filtration and albuminuria, which has been historically associated with a slowing of the progression of CKD. Additionally, this increase in natriuresis results in a diuretic effect. In addition, another direct effect of SGLT2 inhibitors is that of the reduction in glycosuria reabsorption, which means better glycemic control and a better control of the metabolic profile thanks to the effects also demonstrated by these drugs (weight loss, improved lipid profile. The most important demonstrated benefits of these drugs are the reduction in the risk of cardiovascular events, reduced mortality from cardiovascular and renal causes, and the slowing of the progression of CKD. However, these great benefits may in part be ascribed to a beneficial balance between oxidant and antioxidant pathways that are associated with anti-inflammatory or antifibrotic effects or even an erythropoiesis stimulation.
The most important studies on kidney transplant patients are reported on Table 1. We may observe that only recently two large studies have been reported [35,36]. Previous studies, consisting in only one RCT, several case series and retrospective studies, could not give an answer of long-term efficacy and safety. In addition, as immunosuppression is more intensive in the first year after transplantation, the majority of the studies on SGLT2 inhibitor in kidney transplant patients have excluded patients in the first period after transplantation.
Due to these limitations, all these studies [37,38,39,40,41,42,43,44,45,46] were less potent to studies on general population or renal patients in terms of the number of patients enrolled and the quality of study design. However, the benefits observed in these studies were similar to those observed in the general population [47,48,49,50]. Similarly, the incidence of side effects observed in this series of kidney transplant patients was mcg/mg; p<similar to that observed in general population [51]. Two studies just recently have shed new light on the efficacy of SGLT2 inhibitors in kidney transplant patients. Lim et al. [35] enrolled 2083 kidney transplant recipients from six Korean hospitals. 226 patients assumed SGLT2 inhibitors. Patients were observed for 63 months and the multivariate analysis consistently showed a decreased risk of death-censored graft failure and serum creatinine doubling in the SGTL2 inhibitors users. A 15.6% of the SGLT2 inhibitors users showed acute eGFR dip during the first month, but the eGFR recovered thereafter. The risk for infections was very low as documented in previous studies [39,40].
In the other large observational study [36], 339 diabetic kidney transplant patients were given SGLT2 inhibitors for 6 month’s treatment. The most frequent side effect was urinary tract infection (14%) and the risk factor for developing UTI were a prior episode and the female sex. The efficacy evaluated at 6 months was a reduction in body weight (-2.22 kg), a reduction in blood pressure, in fasting glycemia, serum acid decreased of 0.44 mg/dl as well as urinary protein creatinine ratio. Hemoglobin level rose 0.44g/dl. According to the authors, SGLT2 should be prescribed in these patients, only with caution for UTI.
Conclusions and Recommendation
An acute reduction of eGFR at the beginning of treatment with SGLT2 inhibitors in kidney transplant patients is due to a feedback tubuloglomerular and is followed by an eGFR stabilization. The study of Kwon et al. [52] evaluated the dapagliflozin efficacy on microalbuminuria. Urinary albumin creatinine ratio (UACR) at 6 months was reduced (118.9 ±231.0 mcg/mg to 82.7±152.1mcg/mg; p, 0.009).
A recent meta-analysis [50] documented that the use of SGLT2 inhibitors reduced the mean of HbA1c of 0.57% and the most relevant reductions were observed in patients with the highest levels.
The treatment with SGLT2 inhibitors reduced the body weight in the majority of patients as documented in the meta-analysis of Chewcharat et al. [50]
The most common side effects in kidney transplant patients is the urinary tract infection, whose incidence is 11.5%, similar to the incidence reported in a previous meta-analysis [53].
On these bases, the following recommendation should be followed.
- a)
- Start treatment with SGLT” inhibitors at least 6 months after transplantation
- b)
- Start treatment if no previous rejection happened
- c)
- Start treatment in patients with no history of UTI 6 months before starting therapy
- d)
- No history of vascular disease
Legends to Figure 1A,B: NFKB, nuclear factor kappa B; MCP 1 Monocyte chemoattractant protein 1; TFGβTransforming growth factor β; NEFA Non-esterified fatty acids; NO Nitric oxide; O2 Oxygen; N2 Nitrogen; LDL low density lipoprotein; HDL High density lipoprotein
Authors Contributions
Salvadori M, Rosati A and Rosso G contributed equally to the manuscript; Salvadori M designed the study. Rosso G collected the data from the literature; Salvadori M and Rosatin A analyzed the collected data; Salvadori M, Rosati A and Rosso G wrote the manuscript. All the authors performed and approved the last revision.
Conflicts of Interest
Maurizio Salvadori, Alberto Rosati and Giuseppina Rosso do not have any conflict of interest in relation with the manuscript.
References
- McGuire DK, Shih WJ, Cosentino F, Charbonnel B, Cherney DZI, Dagogo-Jack S, Pratley R, Greenberg M, Wang S, Huyck S, Gantz I, Terra SG, Masiukiewicz U, Cannon CP. Association of SGLT2 Inhibitors With Cardiovascular and Kidney Outcomes in Patients With Type 2 Diabetes: A Meta-analysis. JAMA Cardiol. 2021 ; 6:148-158.
- Hurren KM, Pinelli NR. Drug-drug interactions with glucagon-like peptide-1 receptor agonists. Ann Pharmacother. 2012; 46:710-717.
- Zinman B, Lachin JM, Inzucchi SE. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2016; 374, 1094.
- Neal B, Perkovic V, Matthews DR. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017;377: 2099.
- Lee TM, Chang NC, Lin SZ. Dapagliflozin, a selective SGLT2 Inhibitor, attenuated cardiac fibrosis by regulating the macrophage polarization via STAT3 signaling in infarcted rat hearts. Free Radic Biol Med. 2017; 104: 298-310.
- Hasan I, Rashid T, Jaikaransingh V, Heilig C, Abdel-Rahman EM, Awad AS. SGLT2 inhibitors: Beyond glycemic control. J Clin Transl Endocrinol. 2024 35:100335.
- List JF, Woo V, Morales E, Tang W, Fiedorek FT. Sodium-glucose cotransport inhibition with dapagliflozin in type 2 diabetes. Diabetes Care. 2009; 32: 650-657.
- Dekkers CCJ, Sjöström CD, Greasley PJ, Cain V, Boulton DW, Heerspink HJL. Effects of the sodium-glucose co-transporter-2 inhibitor dapagliflozin on estimated plasma volume in patients with type 2 diabetes. Diabetes Obes Metab. 2019 ; 21: 2667-2673.
- Crawford PA. Refueling the Failing Heart: A Case for Sodium-Glucose Cotransporter 2 Inhibition in Cardiac Energy Homeostasis. JACC Basic Transl Sci. 2018; 3: 588-590.
- Packer M. SGLT2 Inhibitors Produce Cardiorenal Benefits by Promoting Adaptive Cellular Reprogramming to Induce a State of Fasting Mimicry: A Paradigm Shift in Understanding Their Mechanism of Action. Diabetes Care. 2020; 43: 508-511.
- Inoue MK, Matsunaga Y, Nakatsu Y, Yamamotoya T, Ueda K, Kushiyama A, Sakoda H, Fujishiro M, Ono H, Iwashita M, Sano T, Nishimura F, Morii K, Sasaki K, Masaki T, Asano T. Possible involvement of normalized Pin1 expression level and AMPK activation in the molecular mechanisms underlying renal protective effects of SGLT2 inhibitors in mice. Diabetol Metab Syndr. 2019; 11: 57.
- Chang YK, Choi H, Jeong JY, Na KR, Lee KW, Lim BJ, Choi DE. Dapagliflozin, SGLT2 Inhibitor, Attenuates Renal Ischemia-Reperfusion Injury. PLoS One. 2016 ; 11:e0158810.
- Aragón-Herrera A, Feijóo-Bandín S, Otero Santiago M, Barral L, Campos-Toimil M, Gil-Longo J, Costa Pereira TM, García-Caballero T, Rodríguez-Segade S, Rodríguez J, Tarazón E, Roselló-Lletí E, Portolés M, Gualillo O, González-Juanatey JR, Lago F. Empagliflozin reduces the levels of CD36 and cardiotoxic lipids while improving autophagy in the hearts of Zucker diabetic fatty rats. Biochem Pharmacol. 2019; 170: 113677.
- Mizuno M, Kuno A, Yano T, Miki T, Oshima H, Sato T, Nakata K, Kimura Y, Tanno M, Miura T. Empagliflozin normalizes the size and number of mitochondria and prevents reduction in mitochondrial size after myocardial infarction in diabetic hearts. Physiol Rep. 2018; 6: e13741.
- Ren FF, Xie ZY, Jiang YN, Guan X, Chen QY, Lai TF, Li L. Dapagliflozin attenuates pressure overload-induced myocardial remodeling in mice via activating SIRT1 and inhibiting endoplasmic reticulum stress. Acta Pharmacol Sin. 2022; 43:1721-1732.
- Wang CC, Li Y, Qian XQ, Zhao H, Wang D, Zuo GX, Wang K. Empagliflozin alleviates myocardial I/R injury and cardiomyocyte apoptosis via inhibiting ER stress-induced autophagy and the PERK/ATF4/Beclin1 pathway. J Drug Target. 2022; 30: 858-872.
- Heerspink HJL, Perco P, Mulder S, Leierer J, Hansen MK, Heinzel A, Mayer G. Canagliflozin reduces inflammation and fibrosis biomarkers: a potential mechanism of action for beneficial effects of SGLT2 inhibitors in diabetic kidney disease. Diabetologia. 2019; 62: 1154-1166.
- Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Ruff CT, Gause-Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS; DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019; 380: 347-357.
- Scheen AJ. Drug-drug interactions with sodium-glucose cotransporters type 2 (SGLT2) inhibitors, new oral glucose-lowering agents for the management of type 2 diabetes mellitus. Clin Pharmacokinet. 2014; 53: 295-304.
- Kruger DF, Bode B, Spollett GR. Understanding GLP-1 analogs and enhancing patients success. Diabetes Educ. 2010 ;36 Suppl 3:44S-72S.
- Whaley JM, Tirmenstein M, Reilly TP, Poucher SM, Saye J, Parikh S, List JF. Targeting the kidney and glucose excretion with dapagliflozin: preclinical and clinical evidence for SGLT2 inhibition as a new option for treatment of type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2012; 5:135-148.
- Patel N, Hindi J, Farouk SS. Sodium-Glucose Cotransporter 2 Inhibitors and Kidney Transplantation: What Are We Waiting For? Kidney360. 2021; 2:1174-1178.
- Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, Cannon CP, Capuano G, Chu PL, de Zeeuw D, Greene T, Levin A, Pollock C, Wheeler DC, Yavin Y, Zhang H, Zinman B, Meininger G, Brenner BM, Mahaffey KW; CREDENCE Trial Investigators. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019; 380: 2295-2306.
- 24. Anker SD, Butler J, Filippatos G, Khan MS, Marx N, Lam CSP, Schnaidt S, Ofstad AP, Brueckmann M, Jamal W, Bocchi EA, Ponikowski P, Perrone SV, Januzzi JL, Verma S, Böhm M, Ferreira JP, Pocock SJ, Zannad F, Packer M. Effect of Empagliflozin on Cardiovascular and Renal Outcomes in Patients With Heart Failure by Baseline Diabetes Status: Results From the EMPEROR-Reduced Trial. Circulation. 2021 ;143: 337-349.
- Díaz-Cruz C, González-Ortiz M, Rosales-Rivera LY, Patiño-Laguna AJ, Ramírez-Rodríguez ZG, Díaz-Cruz K, Martínez-Abundis E. Effects of dapagliflozin on blood pressure variability in patients with prediabetes and prehypertension without pharmacological treatment: a randomized trial. Blood Press Monit. 2020 ; 25: 346-350.
- Petrie MC, Verma S, Docherty KF, Inzucchi SE, Anand I, Belohlávek J, Böhm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukát A, Ge J, Howlett J, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O’Meara E, Vinh PN, Schou M, Tereshchenko S, Køber L, Kosiborod MN, Langkilde AM, Martinez FA, Ponikowski P, Sabatine MS, Sjöstrand M, Solomon SD, Johanson P, Greasley PJ, Boulton D, Bengtsson O, Jhund PS, McMurray JJV. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA. 2020; 323:1353-1368.
- Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, Brunner-La Rocca HP, Choi DJ, Chopra V, Chuquiure-Valenzuela E, Giannetti N, Gomez-Mesa JE, Janssens S, Januzzi JL, Gonzalez-Juanatey JR, Merkely B, Nicholls SJ, Perrone SV, Piña IL, Ponikowski P, Senni M, Sim D, Spinar J, Squire I, Taddei S, Tsutsui H, Verma S, Vinereanu D, Zhang J, Carson P, Lam CSP, Marx N, Zeller C, Sattar N, Jamal W, Schnaidt S, Schnee JM, Brueckmann M, Pocock SJ, Zannad F, Packer M; EMPEROR-Preserved Trial Investigators. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med. 2021; 385:1451-1461.
- Bays HE, Weinstein R, Law G, Canovatchel W. Canagliflozin: effects in overweight and obese subjects without diabetes mellitus. Obesity (Silver Spring). 2014 ; 22:1042-1049.
- Neeland IJ, de Albuquerque Rocha N, Hughes C, Ayers CR, Malloy CR, Jin ES. Effects of Empagliflozin Treatment on Glycerol-Derived Hepatic Gluconeogenesis in Adults with Obesity: A Randomized Clinical Trial. Obesity (Silver Spring). 2020 ; 28:1254-1262.
- Færch K, Blond MB, Bruhn L, Amadid H, Vistisen D, Clemmensen KKB, Vainø CTR, Pedersen C, Tvermosegaard M, Dejgaard TF, Karstoft K, Ried-Larsen M, Persson F, Jørgensen ME. The effects of dapagliflozin, metformin or exercise on glycaemic variability in overweight or obese individuals with prediabetes (the PRE-D Trial): a multi-arm, randomised, controlled trial. Diabetologia. 2021; 64: 42-55.
- Veelen A, Andriessen C, Op den Kamp Y, Erazo-Tapia E, de Ligt M, Mevenkamp J, Jörgensen JA, Moonen-Kornips E, Schaart G, Esterline R, Havekes B, Oscarsson J, Schrauwen-Hinderling VB, Phielix E, Schrauwen P. Effects of the sodium-glucose cotransporter 2 inhibitor dapagliflozin on substrate metabolism in prediabetic insulin resistant individuals: A randomized, double-blind crossover trial. Metabolism. 2023 ; 140:155396.
- Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, Mann JFE, McMurray JJV, Lindberg M, Rossing P, Sjöström CD, Toto RD, Langkilde AM, Wheeler DC; DAPA-CKD Trial Committees and Investigators. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020 ; 383:1436-1446.
- The EMPA-KIDNEY Collaborative Group; Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, Emberson JR, Preiss D, Judge P, Mayne KJ, Ng SYA, Sammons E, Zhu D, Hill M, Stevens W, Wallendszus K, Brenner S, Cheung AK, Liu ZH, Li J, Hooi LS, Liu W, Kadowaki T, Nangaku M, Levin A, Cherney D, Maggioni AP, Pontremoli R, Deo R, Goto S, Rossello X, Tuttle KR, Steubl D, Petrini M, Massey D, Eilbracht J, Brueckmann M, Landray MJ, Baigent C, Haynes R. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023 ; 388:117-127.
- Podestà MA, Sabiu G, Galassi A, Ciceri P, Cozzolino M. SGLT2 Inhibitors in Diabetic and Non-Diabetic Chronic Kidney Disease. Biomedicines. 2023; 11:279.
- Lim JH, Kwon S, Jeon Y, Kim YH, Kwon H, Kim YS, Lee H, Kim YL, Kim CD, Park SH, Lee JS, Yoo KD, Son HE, Jeong JC, Lee J, Lee JP, Cho JH. The Efficacy and Safety of SGLT2 Inhibitor in Diabetic Kidney Transplant Recipients. Transplantation. 2022;106: e404-e412.
- Sánchez Fructuoso AI, Bedia Raba A, Banegas Deras E, Vigara Sánchez LA, Valero San Cecilio R, Franco Esteve A, Cruzado Vega L, Gavela Martínez E, González Garcia ME, Saurdy Coronado P, Morales NDV, Zarraga Larrondo S, Ridao Cano N, Mazuecos Blanca A, Hernández Marrero D, Beneyto Castello I, Paul Ramos J, Sierra Ochoa A, Facundo Molas C, González Roncero F, Torres Ramírez A, Cigarrán Guldris S, Pérez Flores I. Sodium-glucose cotransporter-2 inhibitor therapy in kidney transplant patients with type 2 or post-transplant diabetes: an observational multicentre study. Clin Kidney J. 2023; 16:1022-1034.
- Rajasekeran H, Kim SJ, Cardella CJ, Schiff J, Cattral M, Cherney DZI, Singh SKS. Use of Canagliflozin in Kidney Transplant Recipients for the Treatment of Type 2 Diabetes: A Case Series. Diabetes Care. 2017;40:e75-e76.
- Shah M, Virani Z, Rajput P, Shah B. Efficacy and Safety of Canagliflozin in Kidney Transplant Patients. Indian J Nephrol. 2019; 29: 278-281.
- Schwaiger E, Burghart L, Signorini L, Ristl R, Kopecky C, Tura A, Pacini G, Wrba T, Antlanger M, Schmaldienst S, Werzowa J, Säemann MD, Hecking M. Empagliflozin in posttransplantation diabetes mellitus: A prospective, interventional pilot study on glucose metabolism, fluid volume, and patient safety. Am J Transplant. 2019 ; 19: 907-919.
- Halden TAS, Kvitne KE, Midtvedt K, Rajakumar L, Robertsen I, Brox J, Bollerslev J, Hartmann A, Åsberg A, Jenssen T. Efficacy and Safety of Empagliflozin in Renal Transplant Recipients With Posttransplant Diabetes Mellitus. Diabetes Care. 2019 ; 42:1067-1074.
- Mahling M, Schork A, Nadalin S, Fritsche A, Heyne N, Guthoff M. Sodium-Glucose Cotransporter 2 (SGLT2) Inhibition in Kidney Transplant Recipients with Diabetes Mellitus. Kidney Blood Press Res. 2019; 44: 984-992.
- Attallah N, Yassine L. Use of Empagliflozin in Recipients of Kidney Transplant: A Report of 8 Cases. Transplant Proc. 2019; 51: 3275-3280.
- Kong j, Joon J, Chul Y, Eun W, Hyuk K, Hyun SS Sodium/glucose cotransporter 2 inhibitor for the treatment of diabetes in kidney transplant patients Nephrol Dial Transplant 2019, 34.
- AlKindi F, Al-Omary HL, Hussain Q, Al Hakim M, Chaaban A, Boobes Y. Outcomes of SGLT2 Inhibitors Use in Diabetic Renal Transplant Patients. Transplant Proc. 2020; 52:175-178.
- Song CC, Brown A, Winstead R, Yakubu I, Demehin M, Kumar D, Gupta G. Early initiation of sodium-glucose linked transporter inhibitors (SGLT-2i) and associated metabolic and electrolyte outcomes in diabetic kidney transplant recipients. Endocrinol Diabetes Metab. 2020; 4:e00185.
- Lemke A, Brokmeier HM, Leung SB, Mara KC, Mour GK, Wadei HM, Hill JM, Stegall M, Kudva YC, Shah P, Kukla A Sodium-glucose cotransporter 2 inhibitors for treatment of diabetes mellitus after kidney transplantation. Clin Transplant. 2022 ; 36: e14718.
- Oikonomaki D, Dounousi E, Duni A, Roumeliotis S, Liakopoulos V. Incretin based therapies and SGLT-2 inhibitors in kidney transplant recipients with diabetes: A systematic review and meta-analysis. Diabetes Res Clin Pract. 2021;172:108604.
- Nissaisorakarn P, Pavlakis M, Aala A. Novel Glucose-Lowering Therapies in the Setting of Solid Organ Transplantation. Adv Chronic Kidney Dis. 2021; 28: 361-370.
- Kanbay M, Demiray A, Afsar B, Karakus KE, Ortiz A, Hornum M, Covic A, Sarafidis P, Rossing P. Sodium-glucose cotransporter 2 inhibitors for diabetes mellitus control after kidney transplantation: Review of the current evidence. Nephrology (Carlton). 2021; 26:1007-1017.
- Chewcharat A, Prasitlumkum N, Thongprayoon C, Bathini T, Medaura J, Vallabhajosyula S, Cheungpasitporn W. Efficacy and Safety of SGLT-2 Inhibitors for Treatment of Diabetes Mellitus among Kidney Transplant Patients: A Systematic Review and Meta-Analysis. Med Sci (Basel). 2020; 8: 47.
- Schwarzenbach M, Bernhard FE, Czerlau C, Sidler D. Chances and risks of sodium-glucose cotransporter 2 inhibitors in solid organ transplantation: A review of literatures. World J Transplant. 2021;11: 254-262.
- Kwon H, Son SH, Kim K Sodium-Glucose Cotransprter 2 inhibitors reduce microalbuminuria in diabetic renal transplant patients. Transplantation 104 (S3): p S430.
- Menne J, Dumann E, Haller H, Schmidt BMW. Acute kidney injury and adverse renal events in patients receiving SGLT2-inhibitors: A systematic review and meta-analysis. PLoS Med. 2019;16: e1002983.
Figure 1.
A SGLT2 action on heart and metabolism. B Action of SGLT2 on the kidney.
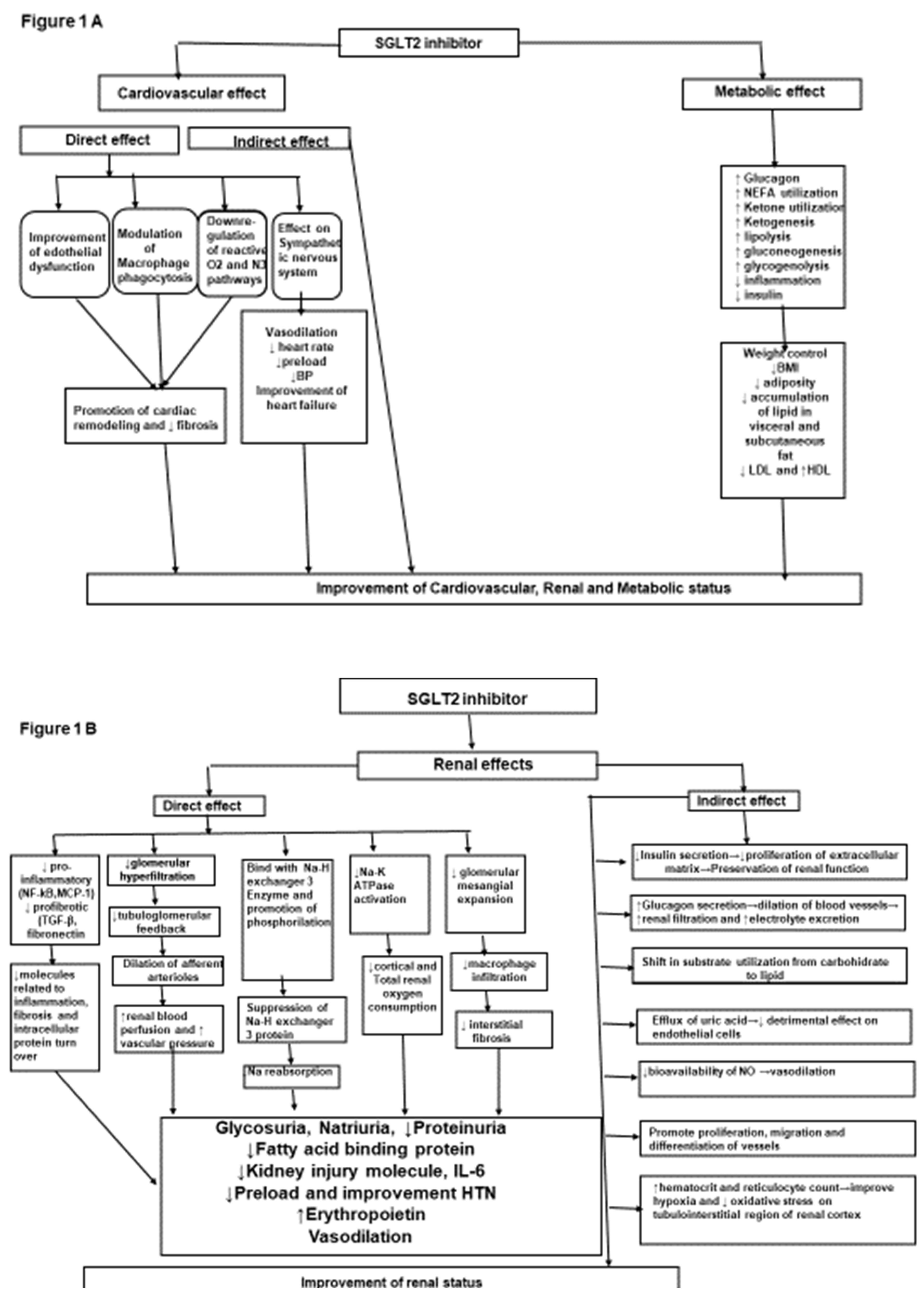
Figure 2.
Potential benefits of SGLT2 inhibitors in chronic kidney disease and renal transplants.
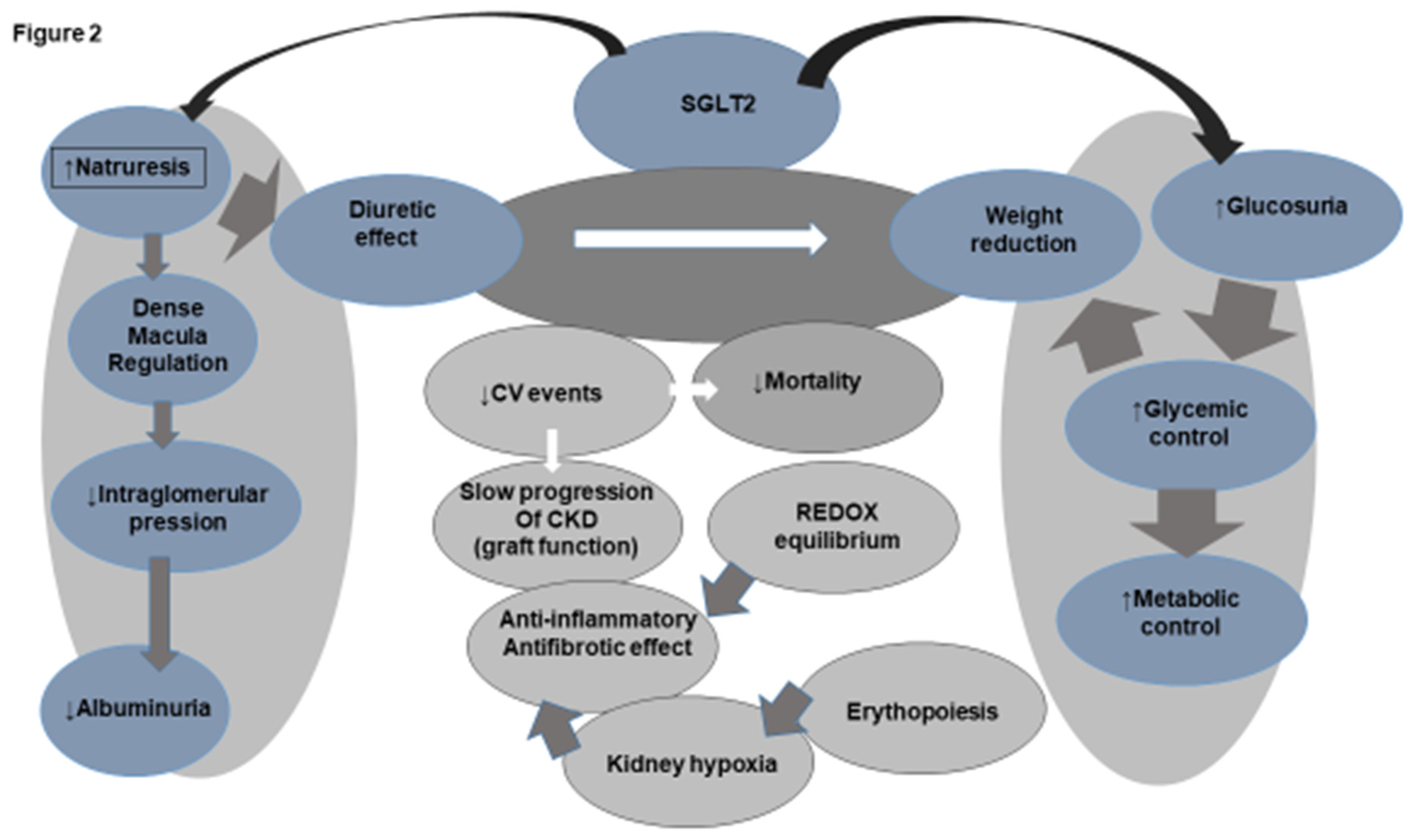

Table 1.
More studies that are relevant for SGLT2 inhibitors on kidney transplant recipients.
| Author, Year, Study type, Follow-up | Basal eGFR (ml/min) |
Effect in Renal Function (eGFR mL/min/1.73) | Proteinuria (uPCR) g/d/(uACR mg/g | Adverse Events |
|---|---|---|---|---|
| Rajasekeran, (37) 2017, CS n6, 8mo | 78.6±18.2 | No differences | NA | Cellulitis |
| Shah, (38) 2019, PS n25, 8mo | 86±20 | No differences | NA | None |
| Schwaiger,(39) 2019, PS, n14, 12mo | 55.6±20.3 | Decrease and then stabilize | ΔuACR: -25 ΔuACR: -73 |
UTI 5 |
| Halden, (40) 2019, RCT, n44, 6mo | 66±10.5 | No differences | NA | UTI 3 |
| Mahling, (41) 2019, PS, n10, 6mo | 57±19.3 | No differences | NA | UTI 2 |
| Attallah, (42) 2019, CS, n25, 12mo | NA | Decrease and than stabilize | ΔuPCR -0.6 g/d | UTI 2 |
| Kong, (43) 2019, PS, n42, 12mo | 60.36±17 | No differences | ΔuACR No significant change | Acute cystitis 3 |
| Alkindi,(44) 2020, CS, n8, 12mo | 75.8±13.4 | No differences | NA | UTI 1 |
| Song, (45) 2021, RS, n50, 6mo | 66.7 | No differences | NA | UTI 7 |
| Lemke,(46) 2021, RS, n39, 12mo | NA | No differences | NA | UTI 6, Ketoacidosis 1 |
| S-Fructuoso,(36) 2022, MCO, n339, 12mo | 58.4 (56.2-60.6) | No differences | ΔuPCR: -230 at 6 mo | UTI 14%, AKI 1.8% |
| Lim, (35) 2022, OR, PSM, n2083, 63mo | S: 66.9±17.7 C: 68.4±20.1 |
Decrease, stabilization and amelioration | ΔuPCR: the urine PCR significantly decreased after SGTLi p=0.005 | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



