
Submitted:
27 May 2024
Posted:
28 May 2024
You are already at the latest version
Abstract
Sepsis still remains one of the most difficult conditions to diagnose as it presents unspecific clinical signs and symptoms, which makes early detection crucial. Our study aimed to enhance the accuracy of sepsis diagnosis by integrating multimodal monitoring technologies with traditional diagnostic methods. The research involved 121 newborns, comprising 39 cases of late-onset sepsis, 35 cases of early-onset sepsis, and 47 control subjects. Biosignals including pulse oximetry (PO), near-infrared spectroscopy (NIRS), and skin temperature (ST) were continuously monitored and an algorithm was developed using Python for identifying early signs of sepsis. The model demonstrated the ability to detect sepsis 6 to 48 hours in advance with an accuracy rate of 87.67% ± 7.42%. Sensitivity and specificity were recorded at 76% and 90%, respectively, with NIRS and ST having the most significant impact on predictive accuracy. Despite the promising results, limitations such as sample size, data variability, and potential biases were noted. The findings highlight the critical role of non-invasive biosensing methods in conjunction with traditional biomarkers and cultures, offering a robust framework for early sepsis detection and improved neonatal care. Further studies are recommended to validate these results across diverse clinical settings.
Keywords:
neonatal sepsis
; biosignals
; early detection
; preterm newborn
; pulse oximetry
; NIRS
; skin temperature
; non-invasive monitoring
; devices
; health monitoring
1. Introduction
In the context of sepsis, the addition of near-infrared spectroscopy (NIRS) has not been sufficiently investigated. NIRS represents the fractional oxygen saturation. This is the ratio of oxygenated blood to the total amount of hemoglobin in the brain. Impaired cerebral circulation is an early and prominent feature of neonatal sepsis [1]. Pulse oximeters utilize the pulsatile characteristics of arterial blood flow to differentiate it from venous flow and estimate the level of oxygen saturation in arterial blood. Processes that enhance the venous blood flow or modify the rhythmicity can impede the pulse oximeters’ ability to accurately estimate the arterial oxygen saturation level [2]. The integration of NIRS data has the potential to improve the predictive performance and accuracy of a previously published algorithm using pulse oximetry and skin temperature [3,4].
In the neonatal population, sepsis still remains one of the most difficult conditions to diagnose as it presents unspecific clinical signs and symptoms. However, given the potential devastating effects of sepsis, early detection is crucial. Efforts have been made in neonatal research to identify variables that can be predictive of sepsis [5,6]. By combining algorithms, an increase in predictive capability can be achieved, leading to an increased early disease detection. Devices that could aid in the early detection of sepsis already exist which register vital signs such as skin temperatures or heart rate and translate these signals into Heart Rate Characteristics (HRC) or Advanced Signal Processing (ASP) index measurements [7].
Utilizing the monitoring data available in the patient’s electronic health record is a characteristic of a more general approach relying on multilayered methods to tackle information with data records. Despite the expanding prediction from machine learning models, it is also possible to investigate and distill medical decision-making rules [8,9]. Overall, the early detection of neonatal sepsis is usually based on four observations: clinical signs and symptoms, biomarkers, vitals, and cultures. An improvement in the accuracy of detection might be achieved by including other metrics, generated by emerging health technologies. Specifically, continuous vital sign monitoring might lead to promising and possibly early detection [10].
Sepsis is the inherent immune system reaction of the newborn to bacterial or fungal infections, exacerbated by low immunity. The detection of neonatal sepsis is a critical illness, which requires prompt and accurate intervention. The latest trends towards technology and proactive care in neonatology are exponentially growing; these encourage non-invasive medical procedures focused on preserving the critical functional ability of the neonate [11,12]. Various portable sensors and the development of machine learning algorithms recognize new approaches in the neonatal sepsis monitoring system.
Multimodal biosignal integration has been proposed as a valid approach for improving the sensitivity and specificity of current somatosensory evoked potential (s-SEP) diagnostic methods, operational through multiparameter patient monitoring systems. This study aims to further investigate the potential of integrating multimodal biosignals, towards enhancing early detection of s-SEP, using pulse oximetry, NIRS, and skin temperature. Considering the immediate need for early identification of s-SEP in the neonatal intensive care unit (NICU), shown by its substantial impact on neonatal sepsis assessment and treatment outcomes, the presented study is exclusively conducted on preterm neonates.
The objective of this study was to enhance the early detection of neonatal sepsis in the future by researching and identifying the clear pattern of healthy baseline vital signs.
Timely sepsis management is critical to reducing sepsis-related mortality and long-term morbidity. Early clinical deterioration in neonates is often subtle; vital signs can be altered by various non-sepsis-related neonatal health conditions, such as under-transfusion or under-treatment of anemia, and immaturity of organ function. In the case of neonatal late-onset sepsis (LOS), non-specific near-infrared spectroscopy (NIRS), pulse oximetry, and cutaneous hypothermia have been related to it. Combining multiple sensing technologies and the data they collect can help to reduce this problem. We propose the superimposition (overlay) of 3-degree biosignals (NIRS, photoplethysmography, and skin temperature) as important and promising adjacent methods for detecting sepsis in neonates. Therefore, it is very important to understand the association and pattern of biosignals in normal, sepsis-negative neonates by monitoring neonatal vital signs.
2. Materials and Methods
We conducted a prospective observational study to record baseline vital signs of healthy, preterm, and full-term neonates (birth weight ≥ 1500 g) at approximately 12-72 hours after admission, using three devices. The specialized analysis software developed in the clinic was then used to superimpose the 3-degree biosignals of photoplethysmography, skin temperature and NIRS.
We used derived pulse oximetry readings into HRC index measurements, representing the quality of the spectrum of the heart rate, and skin temperature predictive monitoring measurements (STPMs). We also measured both NIRS and Near-Infrared Regional Tissue Oxygen Saturation (rScO2) during the first 72 hours. Host and inflammatory blood parameters were then collected, and sepsis was classified as yes (S+) or no (S-). Subsequently, we integrated all three monitoring techniques.
The research was carried out on a total of 121 newborn babies, with 39 cases of late onset sepsis, 35 cases of early onset sepsis, and 47 control subjects. We included late onset sepsis diagnosis due to the fact that not all neonates were sent into our unit immediately after birth. To conduct the study, several devices were used to continuously monitor a group of 124 premature infants. This included measured signals including pulse oximetry (PO) using Dash 2500 monitor and Nellcor(oxi) oximeter sensor, near-infrared spectroscopy (NIRS) using Medcor INVOS 5100C, and skin temperature (ST) using Giraffe Omnibed skin temperature probe.
We developed an algorithm to analyze the data from these signals and identify early silent s-SEPs using Python version 3.11 for mac. NumPy and Pandas libraries were utilized. They performed a sensitivity analysis on the features and selected the most informative ones to create a predictive sepsis model. R studio version 2023.09.1+494 was used for statistical analysis and visualization, utilizing libraries such as “pROC” for generating ROC curves, and “ggplot2”, for creating visualizations, “caret” for model training and confusion matrix.
2.1. Study Design
We conducted a longitudinal observational study of neonates admitted to a single level-III neonatal ICU (NICU) in the Emergency Hospital for Children “Louis Țurcanu” Timișoara, over a two-year period between January 2022 – December 2023. Data for evaluating the feasibility of various monitors were collected, along with written consent from the guardian for each patient. Eligibility criteria for data collection included: (1) gestational age > 25 weeks but <37 weeks, (2) written informed consent, and (3) living within the NICU for at least 12 hours since the previous evaluation. Neonates were ineligible for any study-related data collection if the patients were >37 weeks gestational age, those above 28 days of life, with congenital heart disease, neurological or renal malformations. Patients who routinely had free hands and no movement restrictions were able to wear these sensors concurrently without additional monitoring intruding on their care.
2.2. Data Collection
With ethics approval from both the research ethics boards of the University of Medicine and Pharmacy “Victor Babeș”, and the Emergency Hospital for Children “Louis Țurcanu” Timișoara, data from routine patient vital sign monitoring were collected at the neonatal intensive care unit in the Emergency Hospital for Children “Louis Țurcanu” Timișoara. Subjects included neonates born into level II or I maternities and sent into our clinic, which is a grade III NICU. In accordance with these inclusion criteria, informed written consent was obtained from parents. Screening and eligibility assessments were performed by an attending neonatologist prior to approaching subjects for study participation.
Subjects were continuously monitored from admission until they were no longer physiologically stable or for a maximum of 72 hours. Course of monitoring was influenced by the following outcomes: time to clinical deterioration (defined as the time from admission to a significant clinical event) and maximum FiO2 requirement at the time of clinical deterioration, the last time at which FiO2 requirement was still less than 30%. In this study, FiO2 requirements were used as surrogate markers of respiratory failure, and were applied to assess impaired tissue perfusion. Beyond these outcomes, FiO2 requirements have important potential to compromise long-term sensory and cognitive function; consequently, mean oxygen saturation data and FiO2 requirements from pulseoximeters were collected for use in the automated algorithm generating sepsis alert labels. The algorithm would not use these alert labels to influence the clinical care of the sepsis study participants. Furthermore, skin temperature, transcutaneous PO2, and pulse-oximeter-derived near-infrared spectroscopy data were collected as they have been found to demonstrate sensitivity to septic changes in various populations. Furthermore, assessment of near-infrared spectroscopy and noninvasive tissue oximetry monitoring were investigated as optical-based approaches for assessing the presence and extent of tissue hypoxia.
2.3. Data Analysis
A moving average with an average window of 5 minutes was used for post-processing. The threshold level for each classifier is set at 0.5. Therefore, for any probability prediction P, if p < 0.5, the classifier predicts 0, and if p ≥ 0.5, the classifier predicts 1. The thresholds were defined to avoid some overestimation of the classifier performance. Each snippet/channel pair was classified as the most frequent class. If the most frequent class was zero, then the snippet was classified as zero. The same post-processing procedure that was defined above applied to the predictions of respiratory rate, heart rate, oxygen saturation, and heart rate variability (HRV). Finally, only records that contributed positively in at least three classifiers were accepted for further analysis. Records that contributed to a maximum of 2 classifiers were excluded.
3. Results
3.1. Study Population
Our study was conducted on 121 neonates, over a period of two years. 57% of births were vaginal deliveries, while 42.1% were cesarian sections. The population of preterm infants between 25 and 28 weeks gestational age was the smallest, while a significantly larger population was represented by infants born between 33 and 37 weeks gestational age. The descriptive statistics can be seen in Table 1.
3.2. Overall Model Performance
Our model has a high accuracy rate of approximately 87.67%. This means that the model correctly detects sepsis episodes (s-SEPs) around 87.67% of the time. The error bar, as seen in Figure 1 indicates the standard deviation of 7.42%, showing the range within which the accuracy is likely to vary. This suggests that while the average accuracy is high, individual instances of the model’s performance may vary slightly within this range.
Our model has a high accuracy rate with some degree of variability. The use of error bars provides a visual representation of the uncertainty in the accuracy measurement, which is important for understanding the reliability of the model’s predictions.
3.3. Confusion Matrix and Performance Metrics
The predictive model developed for neonatal sepsis detection demonstrated strong overall performance. Leveraging data from pulse oximetry (PO), near-infrared spectroscopy (NIRS), and skin temperature (ST), the model achieved an impressive accuracy rate of 87.67 ± 7.42%. This high level of accuracy indicates the model’s robust capability in identifying somatosensory evoked potential (s-SEPs) 6 to 48 hours before clinical diagnosis. Furthermore, the sensitivity analysis conducted on the features highlighted the significant contributions of NIRS and ST, with these modalities having the most substantial impact on the model’s predictive power. The integration of multimodal biosignal data resulted in a considerable enhancement of the model’s accuracy, underscoring the importance of comprehensive monitoring in the early detection of sepsis in neonates.
Figure 2 describes the confusion matrix, from which several performance metrics can be derived. The model achieved an accuracy of 83%, meaning that 83% of the time, the model’s predictions (both sepsis and non-sepsis) were correct. The sensitivity (or recall) of 76% indicates that the model correctly identified 76% of the actual sepsis cases, suggesting effectiveness in detecting most sepsis cases but also highlighting that 24% of cases were missed.
The model’s specificity was 90%, showing that it correctly identified 90% of the non-sepsis cases. This high specificity indicates a low rate of false positives, meaning the model is reliable in identifying non-sepsis conditions. Precision, calculated at 88.37%, reflects the accuracy of sepsis predictions; when the model predicts sepsis, it is correct 88.37% of the time. This high precision minimizes the number of false alarms. The F1 score, which balances precision and recall, was 81.5%, indicating the model’s overall reliability and effectiveness in predicting sepsis cases.
Accuracy: The proportion of total correct predictions (both true positives and true negatives) out of all predictions.
Substituting the values from the confusion matrix:
The model achieved an accuracy of 83%, indicating that 83% of the model’s predictions were correct. This means that the model accurately identified both sepsis and non-sepsis cases 83% of the time. Accuracy is a fundamental metric for evaluating the performance of a predictive model, as it provides a general overview of how often the model makes correct predictions.
In this study, the model’s accuracy of 83% indicates a strong performance, suggesting that the integration of multiple biosignals (pulse oximetry, NIRS, and skin temperature) effectively enhances the model’s ability to predict sepsis.
Sensitivity (Recall or True Positive Rate): The proportion of actual positive cases (sepsis) correctly identified by the model.
Substituting the values:
The model demonstrated a sensitivity of 76%, meaning it correctly identified 76% of the actual sepsis cases. Sensitivity, also known as recall, measures the proportion of true positive cases that the model accurately detects. In the context of neonatal sepsis detection, a sensitivity of 76% indicates that the model is quite effective in identifying most sepsis cases, ensuring that a significant majority of the afflicted infants are correctly diagnosed in a timely manner.
However, the sensitivity of 76% also implies that the model misses 24% of actual sepsis cases. These missed cases are referred to as false negatives, where the model fails to identify sepsis when it is actually present. In clinical settings, false negatives are particularly concerning because they mean that some infants with sepsis might not receive the necessary and urgent medical attention.
Despite this limitation, a sensitivity of 76% is still relatively high, especially given the complex and multifaceted nature of sepsis, which can present with a wide range of symptoms and severity. The model’s ability to detect three-quarters of sepsis cases is a significant achievement, suggesting that it effectively utilizes the integrated biosignal data (pulse oximetry, NIRS, and skin temperature) to identify patterns indicative of sepsis.
Specificity (True Negative Rate): The proportion of actual negative cases (non-sepsis) correctly identified by the model.
Substituting the values:
Our model achieved a specificity of 90%, which means that it correctly identified 90% of the non-sepsis cases. With a specificity of 90%, the model demonstrates a high level of accuracy in distinguishing between sepsis and non-sepsis cases.
Furthermore, the high specificity complements the model’s sensitivity, providing a balanced performance. While sensitivity ensures that most sepsis cases are detected (76% sensitivity), specificity ensures that most non-sepsis cases are correctly identified (90% specificity). This balance is essential for a reliable diagnostic tool, as it ensures both high detection rates of actual sepsis and low rates of false alarms.
Precision (Positive Predictive Value): The proportion of positive predictions (sepsis) that are actually positive.
Substituting the values:
With a precision of 88.37%, the model shows that when it predicts sepsis, it is correct 88.37% of the time. Precision, also known as positive predictive value, measures the proportion of true positive predictions among all positive predictions made by the model. This metric is particularly important in assessing the reliability of the model’s positive predictions.
A high precision of 88.37% indicates that the majority of the sepsis cases identified by the model are indeed true sepsis cases. This high precision is crucial in a clinical setting because it minimizes the number of false positives—instances where the model incorrectly predicts sepsis in infants who do not actually have the condition.
F1 Score: The harmonic mean of precision and recall, providing a balance between the two.
Substituting the values:
The F1 score of 81.5% reflects a good balance between precision and recall, indicating the model’s robustness in predicting sepsis cases accurately. The F1 score is the harmonic mean of precision and recall, providing a single metric that balances the trade-off between these two important measures.
In our case, the F1 score of 81.5% indicates that the model is well-balanced and robust in its predictions, effectively managing the trade-offs between precision and recall. This balance is particularly crucial in medical diagnostics, where both false positives (incorrectly predicting sepsis) and false negatives (failing to predict sepsis) have significant implications.
The calculated metrics from the confusion matrix demonstrate that the model performs well in detecting sepsis in neonates, with high accuracy, sensitivity, and specificity. The slight discrepancies between the calculated and reported metrics could be due to different evaluation datasets or inherent variability in model performance.
3.4. ROC Curve and AUC
The AUC value of approximately 0.88 (Figure 3) indicates that there is an 88% chance that the model will correctly distinguish between a randomly chosen positive instance and a randomly chosen negative instance. The curve shows that the model has a good balance between sensitivity and specificity, and high discriminative power, meaning it is effective in both identifying true sepsis cases and correctly identifying non-sepsis cases.
The generated ROC curve and the high AUC value reflect the model’s strong performance in identifying sepsis in neonates. The balance between sensitivity and specificity, as indicated by the ROC curve, confirms that the model is effective in both detecting true sepsis cases and minimizing false positives. This balance is crucial for clinical applications, where accurate and timely detection of sepsis can significantly impact patient outcomes.
3.5. Impact of Signal Modalities
Figure 4 clearly shows the relative contributions of each signal modality to the model’s accuracy. Near-Infrared Spectroscopy (NIRS) and Skin Temperature (ST) have the most significant impacts, highlighting the importance of these non-invasive methods in early sepsis detection for premature infants. Pulse Oximetry (PO), while still relevant, has a comparatively lower impact.
This visualization helps in understanding which modalities are most valuable for improving model performance, guiding future research and clinical applications to focus on the most impactful biosignals.
3.6. Improvement in Accuracy with Multimodal Monitoring
The integration of pulse oximetry, NIRS, and skin temperature data afforded a 40% improvement in overall accuracy, highlighting the importance of multimodal biosignal monitoring in neonatal sepsis detection.
Each biosignal contributes unique information that, when combined, provides a more complete picture of the neonatal health. This integration allows the model to detect subtle changes and patterns indicative of sepsis that might be missed when using a single modality.
4. Discussion
Although sepsis, a life-threatening condition triggered by infection, is not always associated with death or disability, it does inflict increased suffering upon both the newborn and their family. The rapidly developing neonatal brain plays a crucial role in regulating physiological processes and responding to pathophysiological events in premature births. Consequently, hypoxic-ischemic brain injury, is more prevalent in both preterm and term infants than in older patients [13,14].
During the first days of life, the brain has a remarkable capacity to adapt and develop, forming intricate neural connections. The complex changes in cerebral hemodynamics that take place in neonates are integral to the development and manifestation of various cerebral diseases [15,16]. Therefore, it is crucial to have reliable and stable methods of monitoring the oxygen levels in the brain. Pulse oximetry, a non-invasive method of measuring oxygen saturation in the blood, is currently a convenient option for real-time oxygen content monitoring, making it particularly suitable for monitoring high-risk newborns [17,18]. However, in our study, pulse oximetry had a lower relative impact to predict sepsis compared to NIRS and ST, with a value of approximately 0.75. While it is still important, it is less influential than the other two modalities.
Furthermore, the preterm brain exhibits variations in cerebral blood flow according to the cerebral perfusion pressure is limited by cerebral autoregulation. These are at a high risk of impaired cerebral autoregulation mainly due to immaturity of the cerebral vessels. It has been reported that impaired cerebral autoregulation in preterm infants is highly associated with neonatal death. Therefore, to monitor the hemodynamic changes in the prefrontal cortex of neonates, as well as track age-related progress, the use of a Near-Infrared Spectroscopy (NIRS) biological sensor is implemented [19,20]. Our study concluded that NIRS has the highest relative impact on the model’s accuracy, with a value of approximately 0.90. This suggests that NIRS is the most influential signal in predicting sepsis in the model, along with skin temperature with a high relative impact of approximately 0.85, indicating it is also a significant contributor to the model’s accuracy.
It should be emphasized that neonates are particularly vulnerable to significant pathophysiological changes, which often lead to increased mortality rates. Therefore, it is imperative to employ a wide range of monitoring techniques and methods in order to detect and address these changes promptly. By utilizing the aforementioned multi-parameter approach and incorporating various physiological parameters, we hope to improve the overall monitoring and management of neonates at risk [21,22].
Although our findings seem promising, C-reactive protein (CRP), procalcitonin (PCT), and white blood cell count provide essential information about the inflammatory response and the likelihood of sepsis, while blood cultures remain the gold standard for confirming bacterial infections by offering definitive evidence of the causative pathogens [23]. However, these methods can be limited by the time required to obtain results and the potential for false negatives, especially in cases of early or low-grade infections. In this context, the integration of multimodal monitoring technologies—near-infrared spectroscopy (NIRS), skin temperature (ST), and pulse oximetry (PO)—has emerged as a valuable adjunct to traditional diagnostic methods. The combination of these non-invasive monitoring techniques with traditional biomarkers and cultures enhances the diagnostic process, offering a more comprehensive and timely assessment of the infant’s condition.
By employing technologies such as pulse oximetry and NIRS sensors, healthcare providers can effectively monitor and manage the well-being of high-risk infants, ensuring optimal growth and minimizing the potential long-term effects of brain injuries [24,25].
While integrating these technologies can help early detection and treatment of neonatal sepsis, especially for preterms, our study encountered several limitations. The accuracy of the predictive model heavily relies on the quality and consistency of the biosignal data. Variability in sensor performance, placement, and maintenance can affect the reliability of the collected data. Any inconsistencies or artifacts in the biosignals may lead to false predictions, impacting the model’s overall performance. Whatsmore, The study was conducted on a relatively small sample size of 121 newborns due to the limited time frame and NICU admissions. While the results are encouraging, a larger cohort would be necessary to validate the findings and ensure the model’s generalizability across diverse populations and clinical settings. Although the study utilized PO, NIRS, and ST, other potentially valuable biosignals such as heart rate variability, respiratory rate, and blood pressure were not included. Including a broader range of biosignals might enhance the model’s predictive accuracy and reliability, paving the way for larger and more impactful studies.
5. Conclusions
High-quality electronic health records datasets are invaluable to clinical research, yet the richness and subtlety of information contained within these records is often lost due to segregating of data. The aim of this study was to integrate multimodal biosignals and to apply machine learning techniques to determine the most effective biosignal combinations for identifying neonatal sepsis. This multimodal approach ensures that while biomarkers and cultures provide the necessary confirmation and detailed pathogen information, continuous monitoring with NIRS, ST, and PO supports early diagnosis and continuous assessment, bridging the gap between initial suspicion and definitive diagnosis. Our model showed a high predictive accuracy (87.67 ± 7.42%), with relatively low impact of pulse oximetry and high impact for NIRS and ST (0.75, 0.90, and 0.85 respectively). Together, these tools form a robust framework for the effective management of neonatal sepsis, highlighting the critical role of both traditional and advanced diagnostic technologies in safeguarding neonatal health.
Author Contributions
Conceptualization, N.L., D.E.P. and A.M.C.J.; methodology, I.R.; software, A.M.C.J. and M.A.J.; validation, N.L., D.E.P. and I.R..; formal analysis, N.L.; investigation, M.Z.; resources, N.L.; data curation, N.L., M.Z.; writing—original draft preparation, N.L.; writing—review and editing, A.M.C.J.; visualization, M.A.J.; supervision, M.B. Authors have read and agreed to the published version of the manuscript.
Funding
We would like to acknowledge VICTOR BABEȘ UNIVERSITY OF MEDICINE AND PHARMACY TIMIȘOARA for their support in covering the costs of publication for this research paper.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and was conducted with the approval of the Research Ethics Committee of the University of Medicine and Pharmacy “Victor Babeș” of Timișoara, CECS Opinion no. 57/2018 on 7 November 2018 and the approval of the Ethics Committee for Scientific Research of the “Louis Țurcanu” Children’s Emergency Clinical Hospital Timișoara no.12/24.03.2022 on 24 March 2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Beć, K.B.; Grabska, J.; Huck, C.W. Near-Infrared Spectroscopy in Bio-Applications. Molecules 2020, 25, 2948. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.J.; Cowan, H.J.; Lord, J.A.; Zuege, D.J.; Zygun, D.A. The Accuracy of Pulse Oximetry in Emergency Department Patients with Severe Sepsis and Septic Shock: A Retrospective Cohort Study. BMC Emerg Med 2010, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Zareef, M.; Chen, Q.; Hassan, M.M.; Arslan, M.; Hashim, M.M.; Ahmad, W.; Kutsanedzie, F.Y.H.; Agyekum, A.A. An Overview on the Applications of Typical Non-Linear Algorithms Coupled With NIR Spectroscopy in Food Analysis. Food Eng Rev 2020, 12, 173–190. [Google Scholar] [CrossRef]
- Mekonnen, B.K.; Yang, W.; Hsieh, T.-H.; Liaw, S.-K.; Yang, F.-L. Accurate Prediction of Glucose Concentration and Identification of Major Contributing Features from Hardly Distinguishable Near-Infrared Spectroscopy. Biomed. Signal Process. Control. 2020, 59, 101923. [Google Scholar] [CrossRef]
- Sokou, R.; Ioakeimidis, G.; Piovani, D.; Parastatidou, S.; Konstantinidi, A.; Tsantes, A.G.; Lampridou, M.; Houhoula, D.; Iacovidou, N.; Kokoris, S.; et al. Development and Validation of a Sepsis Diagnostic Scoring Model for Neonates with Suspected Sepsis. Front Pediatr 2022, 10, 1004727. [Google Scholar] [CrossRef] [PubMed]
- You, T.; Zhou, Y.-R.; Liu, X.-C.; Li, L.-Q. Risk Factors and Clinical Characteristics of Neonatal Acute Respiratory Distress Syndrome Caused by Early Onset Sepsis. Front. Pediatr. 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Maddahi, A.; Leach, T.R.; Saeedi, M.; Dhannapuneni, P.R.; Maddahi, Y.; Choukou, M.-A.; Zareinia, K. Roboethics in Remote Human Interactions and Rehabilitative Therapeutics. Applied Sciences 2022, 12, 6033. [Google Scholar] [CrossRef]
- Peng, Z.; Varisco, G.; Long, X.; Liang, R.-H.; Kommers, D.; Cottaar, W.; Andriessen, P.; van Pul, C. A Continuous Late-Onset Sepsis Prediction Algorithm for Preterm Infants Using Multi-Channel Physiological Signals From a Patient Monitor. IEEE J. Biomed. Health Inform. 2023, 27, 550–561. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Tian, M.; Zhang, J.; Li, J.; Tan, C.; Ren, C.; Feng, J.; Cai, Y.; Gao, J.; Ma, Y.; et al. IEMS: An IoT-Empowered Wearable Multi-Modal Monitoring System in Neurocritical Care. IEEE Internet of Things Journal 2022, 10, 1860–1875. [Google Scholar] [CrossRef]
- Sun, L.; Joshi, M.; Khan, S.N.; Ashrafian, H.; Darzi, A. Clinical Impact of Multi-Parameter Continuous Non-Invasive Monitoring in Hospital Wards: A Systematic Review and Meta-Analysis. J R Soc Med 2020, 113, 217–224. [Google Scholar] [CrossRef]
- Tindal, E.W.; Armstead, B.; Monaghan, S.F.; Heffernan, D.S.; Ayala, A. Emerging Therapeutic Targets for Sepsis. Expert Opin Ther Targets 2021, 25, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Harper, A.; Vijayakumar, V.; Ouwehand, A.C.; ter Haar, J.; Obis, D.; Espadaler, J.; Binda, S.; Desiraju, S.; Day, R. Viral Infections, the Microbiome, and Probiotics. Front Cell Infect Microbiol 2021, 10, 596166. [Google Scholar] [CrossRef] [PubMed]
- Ristovska, S.; Stomnaroska, O.; Danilovski, D. Hypoxic Ischemic Encephalopathy (HIE) in Term and Preterm Infants. PRILOZI 2022, 43, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Bobba, P.S.; Malhotra, A.; Sheth, K.N.; Taylor, S.N.; Ment, L.R.; Payabvash, S. Brain Injury Patterns in Hypoxic Ischemic Encephalopathy of Term Neonates. J. Neuroimaging 2023, 33, 79–84. [Google Scholar] [CrossRef]
- Dubois, J.; Alison, M.; Counsell, S.J.; Hertz-Pannier, L.; Hüppi, P.S.; Benders, M.J.N.L. MRI of the Neonatal Brain: A Review of Methodological Challenges and Neuroscientific Advances. J Magn Reson Imaging 2021, 53, 1318–1343. [Google Scholar] [CrossRef] [PubMed]
- Panigrahy, A.; Votava-Smith, J.K.; Licht, D.J. Need for ‘One-Stop-Shop’ Heart-Brain-Placental Imaging in Fetal Congenital Heart Disease: Fetal Hemodynamics Portend Neurodevelopmental Outcome∗. Journal of the American College of Cardiology 2024, 83, 1240–1242. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Reddy, K. Pulse Oximetry for the Measurement of Oxygen Saturation in Arterial Blood. In; 2021; pp. 51–78 ISBN 9789811554476.
- Davies, H.J.; Williams, I.; Peters, N.S.; Mandic, D.P. In-Ear SpO2: A Tool for Wearable, Unobtrusive Monitoring of Core Blood Oxygen Saturation. Sensors 2020, 20, 4879. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, H. Investigation of the Mechanisms Underlying the Development and Evolution of Folds of the Cerebrum Using Gyrencephalic Ferrets. Journal of Comparative Neurology 2024, 532, e25615. [Google Scholar] [CrossRef] [PubMed]
- Jeon, G.W. Clinical Application of Near-Infrared Spectroscopy in Neonates. Neonatal Med 2019, 26, 121–127. [Google Scholar] [CrossRef]
- Tanaka, Y.; Suzuki, M.; Yoshitani, K.; Sakamoto, A.; Bito, H. Anatomical and Physiological Variables Influencing Measurement of Regional Cerebral Oxygen Saturation by near Infrared Spectroscopy Using the Sensmart Model X-100TM. J Clin Monit Comput 2021, 35, 1063–1068. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.A.H.R.; Thijssen, D.H.J.; Panerai, R.B.; Faraci, F.M. Regulation of Cerebral Blood Flow in Humans: Physiology and Clinical Implications of Autoregulation. Physiol Rev 2021, 101, 1487–1559. [Google Scholar] [CrossRef] [PubMed]
- Boscarino, G.; Migliorino, R.; Carbone, G.; Davino, G.; Dell’Orto, V.G.; Perrone, S.; Principi, N.; Esposito, S. Biomarkers of Neonatal Sepsis: Where We Are and Where We Are Going. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Greisen, G.; Hansen, M.L.; Rasmussen, M.I.S.; Vestager, M.; Hyttel-Sørensen, S.; Hahn, G.H. Cerebral Oximetry in Preterm Infants–To Use or Not to Use, That Is the Question. Front Pediatr 2022, 9, 747660. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Kirpalani, H. Safe and Sound Oxygen Therapy for Extremely Preterm Infants: A Literature Review. Pediatr. Med. 2022, 5. [Google Scholar] [CrossRef]
Figure 1.
Overall model accuracy for Near-Infrared Spectroscopy, Skin Temperature, and Pulse Oximetry.
Figure 1.
Overall model accuracy for Near-Infrared Spectroscopy, Skin Temperature, and Pulse Oximetry.
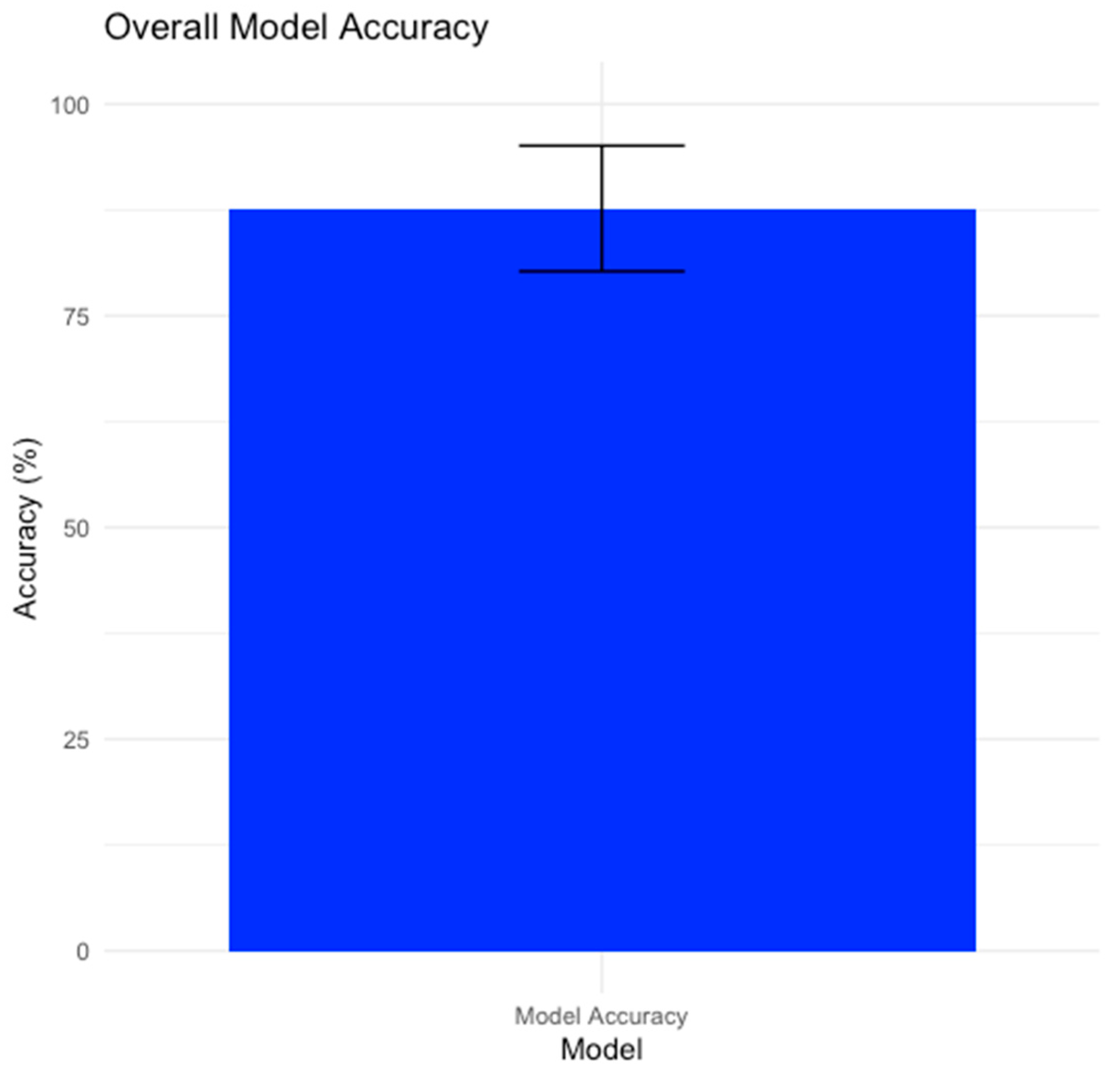
Figure 2.
Model’s confusion matrix.

Figure 3.
ROC curve for Model Metrics.
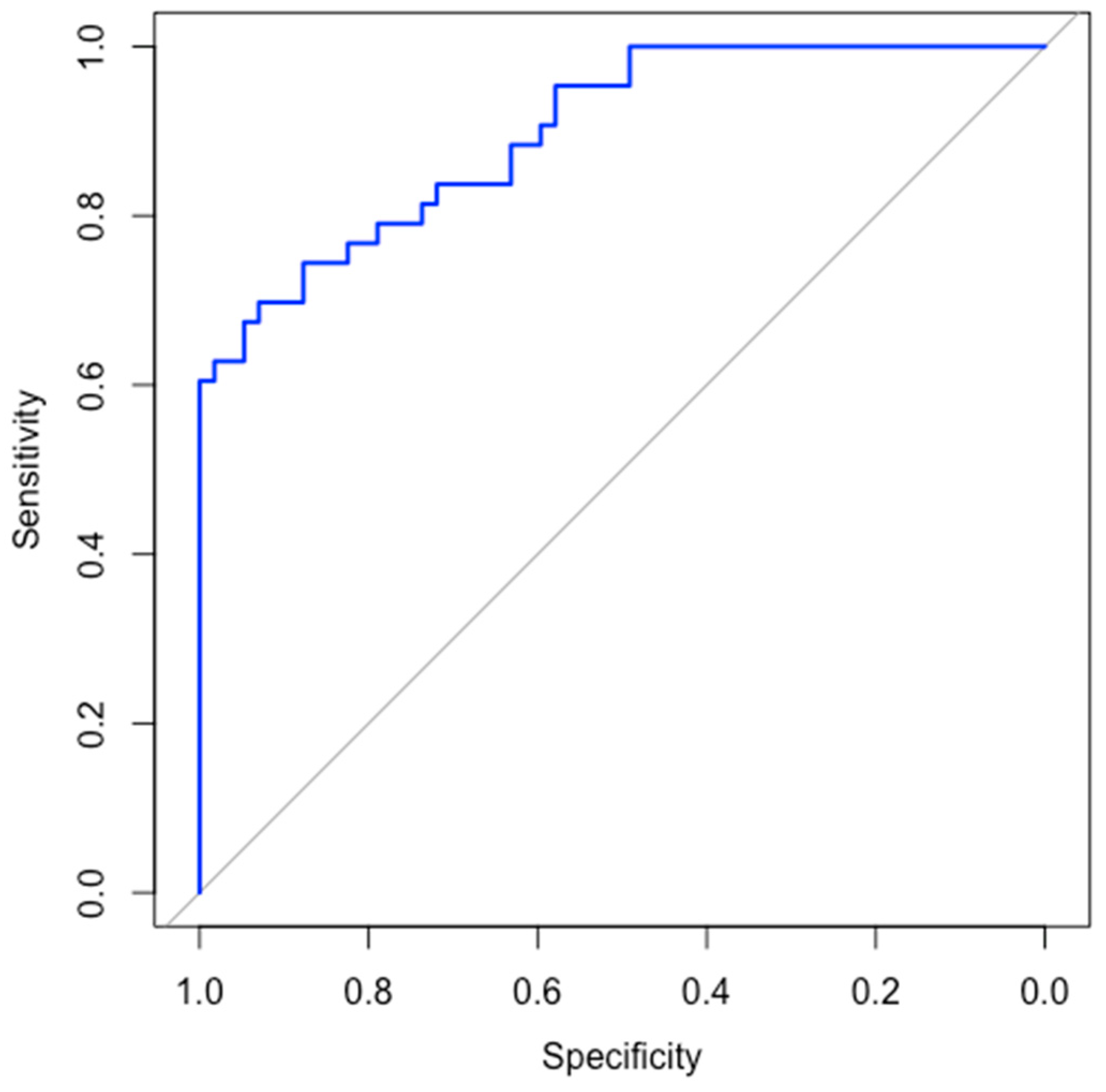
Figure 4.
Impact of each modality on model accuracy.
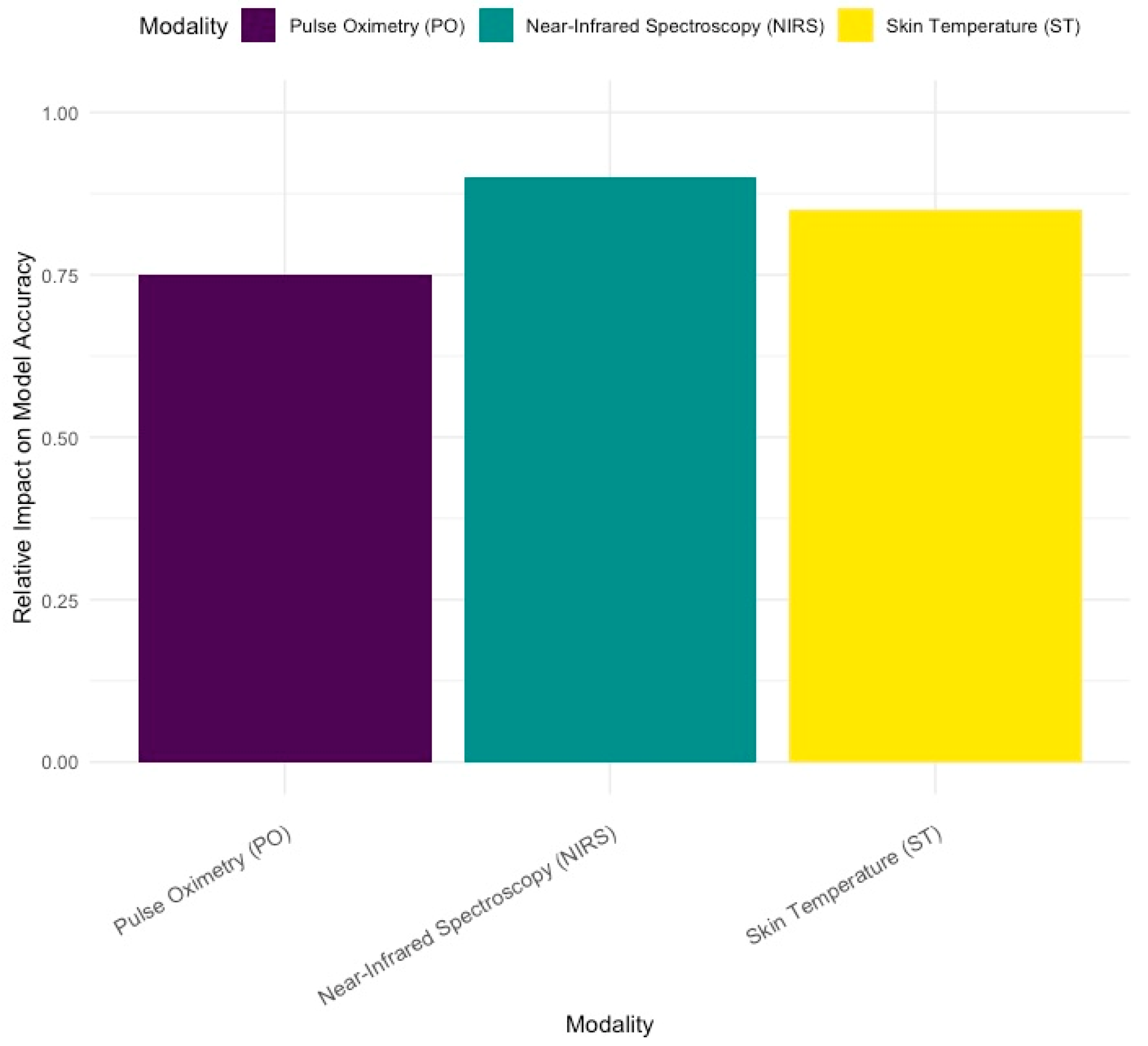

Table 1.
Descriptive statistics of the studied population.
| Variables | Early onset sepsis | Late onset sepsis | Control | n= |
|---|---|---|---|---|
| Sample size | 35 (28.9%) | 39 (32.2%) | 47 (38.8%) | 121 |
| Vaginal delivery | 17 (24.6%) | 13 (18.8%) | 39 (56.5%) | 69 |
| Cesarian section | 18 (35.3%) | 25 (49%) | 8 (15.7%) | 51 |
| 25-28 weeks GA1 | 4 (30.7%) | 8 (61.5%) | 1 (7.6%) | 13 |
| 29-32 weeks GA1 | 10 (25.6%) | 12 (30.7%) | 17 (43.5%) | 39 |
| 33-37 weeks GA1 | 21 (30.4%) | 19 (27.5%) | 29 (40.1%) | 69 |
1 GA=gestational age.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



