
Submitted:
28 May 2024
Posted:
29 May 2024
You are already at the latest version
Abstract
Reducing under-five mortality is a key indicator of a country's overall development, yet in Angola, understanding the factors contributing to hospital deaths in this vulnerable demographic remains incomplete despite improvements in healthcare infrastructure and public health policies. With one of the highest under-five mortality rates in Sub-Saharan Africa, Angola grapples with significant challenges, including malaria, malnutrition, pneumonia, neonatal conditions, and intestinal infectious diseases, as leading causes of death among children. This study aimed to identify factors associated with these hospital deaths in children aged 28 days to five years admitted to DBPH in Luanda between May 2022 and June 2023. Utilizing a hospital-based case-control design, a total of 1020 children were studied, with 340 cases of hospital deaths. Notably, distal and intermediate determinants emerged as primary predictors of hospital mortality, revealing significant associations with maternal education status, maternal alcohol consumption during pregnancy, short hospital stays (≤24h), poor nutritional status, short interbirth intervals, maternal age ≤19 years, and maternal age ≥35 years. These findings underscore the preventable nature of most under-five hospital deaths and emphasize the urgent need to address social inequities and enhance the quality of primary healthcare services to effectively mitigate child mortality.
Keywords:
under-five mortality
; hierarchical approach
; risk factors
; case-control studies
; hospitalization
; logistic regression
1. Introduction
The under-five mortality rate is a crucial indicator of a country’s overall development. It reflects the availability and quality of healthcare services, as well as the social and economic conditions that influence child survival[1,2]. It is included in the Sustainable Development Goals (SDGs) as an unfinished agenda of the Millennium Development Goals (MDGs) [3].
According to the World Health Organization (WHO), the global under-five mortality rate decreased by 60%, dropping from 93 per 1,000 live births in 1990 to 37 in 2020; despite
This progress, 5 million children under the age of five died in 2020, with the highest rates recorded in the Sub-Saharan Africa region, reaching 76 deaths per 1000 live births in 2017 and resulting in 2.7 million deaths in the region[1].
Among the leading causes of hospital mortality in children under five worldwide are complications from premature birth, birth asphyxia/trauma, pneumonia, diarrhea, and malaria[1,4].
Socioeconomic factors such as place of residence, maternal education level, household wealth, as well as maternal health status and limited access to healthcare, are strongly associated with the risk of under-five mortality in Sub-Saharan Africa, a region responsible for nearly 50% of child mortality, despite comprising only 11% of the world’s population[4,5].
Angola is among the seven countries with the highest under-five mortality rates in Sub-Saharan Africa[2,5]; these countries accounted for about one-fifth of under-five mortality worldwide[2].
There are some gaps in documenting hospital mortality among children under five in Angola. However, available data suggest that malaria, malnutrition, pneumonia, neonatal conditions, meningitis, intestinal infectious diseases, and acute respiratory infections are the leading causes of mortality in this age group[6,7].
Significant improvements have been observed in Angola’s healthcare infrastructure and public health policies, particularly focused on families, pregnant women, and children. However, the country faces major challenges in reducing its child and adolescent mortality rates[8,9]. With the support of the UN, the country has been working on implementing the SDGs and the African Union’s Agenda 2063, demonstrating its commitment by presenting its first Voluntary National Review (VNR) in 2021[10].
The hierarchical approach is a useful tool for understanding under-five mortality, and the conceptual framework proposed by Mosley and Chen is often used as an ideal hierarchical approach to analyze determinants of child mortality in developing countries[11].
This framework identifies three levels of determinants of child mortality: distal, intermediate, and proximal. Distal determinants refer to socioeconomic, cultural, and environmental factors that affect the overall health and well-being of a population. Intermediate determinants include factors related to access and utilization of healthcare, such as availability and quality of healthcare services; finally, proximal determinants include factors related to each child, such as their nutritional status and exposure to infectious diseases[11,12,13].
This approach helps identify the relative contribution of different factors to the variability in under-five mortality in developing countries; and the hierarchization of determinants into distal, intermediate, and proximal expresses, on the one hand, the relevance of factors associated with death and, on the other hand, the chronological order of events, facilitating the identification of links between factors and the corrective and preventive measures to be applied.
The present study aims to identify the factors associated with death in children from 28 days to five years of age at the David Bernardino Pediatric Hospital in Luanda through a hierarchical approach.
2. Materials and Methods
2.1. Study Type and Location
A hospital-based case-control study was conducted at a ratio of 1:2, from May 1, 2022, to June 30, 2023. The one-year period allows for the avoidance of potential seasonal bias. The study was carried out in Luanda, at the David Bernardino Pediatric Hospital (DBPH), a tertiary-level hospital that serves as a teaching and research center, being the main reference for pediatric care in the Angolan National Health Service. With 554 inpatient beds and structured into 12 services, the hospital admits an average of 1500 patients per month and has an occupancy rate of 97%. The emergency department, the gateway for hospital admissions, is equipped with 150 observation beds and receives an average of 9000 children per month.
2.2. Population and Sample
The study population consisted of children admitted to DBPH during the study period. Cases included children aged between 28 days and five years who died during hospitalization, regardless of associated clinical condition, and controls included children from the same age group who survived during the same period. Cases were identified through hospital records, while controls were selected from patients meeting discharge criteria, matched by age (± 6 months) and sex. Final diagnoses were reviewed by the principal investigator, and the primary diagnosis was defined. Discrepant cases were discussed with team members and decided upon by consensus. The International Classification of Diseases (ICD-10) was used to classify the underlying causes of death.
Cases that died after 4:00 PM and on weekends were automatically excluded due to the inability to interview caregivers. Additionally, those who died from accidents, those for whom sufficient information could not be obtained, controls with readmissions and prior participation in the study, and those whose primary caregiver refused to participate were also excluded.
The sample was systematically obtained by applying predefined exclusion criteria to both the case and control populations. Thus, out of the 1237 children who died, 503 occurred after 4:00 PM and 145 on weekends. 589 caregivers were interviewed, of whom 108 refused to participate in the study, 131 did not have sufficient information, 8 were due to road accidents, and two withdrew during the interview, resulting in a response rate of 81.7% (Figure 1).
2.3. Procedures and Data Collection Instrument
Data collection was conducted daily, from Monday to Friday, from 8:00 AM to 4:00 PM. Data were obtained through interviews conducted by the researcher with the child’s caregiver, either at admission or within 24 hours of hospitalization, using a standardized and coded form containing closed-ended questions regarding sociodemographic aspects, clinical characteristics, and care-related factors. Additional data were obtained through clinical record review.
2.4. Definition and Categorization of Variables
Entry into the labor market: An adaptation of the definition by the Brazilian Institute of Geography and Statistics (IBGE) [14] was used, considering the following categories: a) employed - engages in economic activity or works in a public or private establishment, business, or institution, formally or informally employed; b) inactive - without productive activity or seeking employment, i.e., homemakers, students, and retirees; c) unemployed - not working but seeking employment. Obtained through information from parents and, for stratified analysis purposes, categorized as non-unemployed (if a) and unemployed (if b or c).
- Family income: average earnings of the family in the three previous months. Categorized into minimum wages (MW): up to 1.0 MW; 2.0-3.00 MW; 3.01-4.00 MW; > 4.0 MW. Assessed by the respondent; considering the national minimum wage at the time of data collection [15]. For stratified analysis, categorized as ≤ 1 MW; 2-3 MW; and ≥ 4 MW.
- Housing condition: A housing score adapted from Ludermir AB (16) was used, considering the components of the residence, to which a score was assigned. Thus, the wall was scored as 1 or 0 depending on whether it was made of brick or other material; the roof was assigned a score of 1 and 0 (tile/slab and other material); floor: 2-ceramic/wood, 1-cement, 0-dirt; water supply: 3-public network, 2-fountain, 1-well or spring, 0-other water supply forms; sewage system: 2-public network, 1-septic tank, 0-no sewage system. The arithmetic mean of the sum of each item was calculated, and individuals with a value below the mean were classified as having poor housing conditions; those with a value around the mean (mean ± 1 standard deviation (SD)), as medium, and those above the mean + 1 SD, as having good conditions. Stratified in the analysis into two categories: not precarious (good and medium) and precarious;
- Household overcrowding: The overcrowding index proposed by Hill et al. [17] was used, considering three categories: 1- no overcrowding: fewer than four people per household and fewer than two people per room; 2- moderate overcrowding: fewer than four people per household and two or more people per room, or four or more people per household but fewer than two per room; 3- intense overcrowding: four or more people per household and at least two per room. For analysis, two categories were considered: no overcrowding and overcrowded (moderate/intense).
- Nutritional status: The weight-for-age anthropometric index was used, calculated at the time of inclusion in the study using the table recommended by the WHO [18]. For analysis, children with nutritional deficits were considered those who had two z-scores below the median value of the reference population in this index; and those without nutritional deficits were those who had two or more z-scores above the median reference value.
- Maternal education: Number of years of completed education. Stratified into: level 1 (no formal education and/or unable to read or write, except for own name); level 2 (able to read and write and/or up to six years of schooling); level 3 (seven to 12 years of schooling); level 4 (>12 years of schooling).
- Frequent alcohol use was considered the consumption of at least one alcoholic drink, equivalent to 10 or 12g of alcohol [19], per week during pregnancy.
2.5. Data Analysis Strategy: Hierarchical Modeling
From an operational standpoint, the predictive factors under investigation were grouped into three hierarchical levels, each corresponding to a block of variables, according to the conceptual model proposed by Mosley and Chen [11]. (Figure 2).
2.6. Statistical Analysis
The data analysis was conducted in two stages:
1. Initial descriptive analysis:
Quantitative variables were reported as mean ± SD or median with interquartile range if they did not follow a normal distribution. Categorical variables were described using absolute and relative frequencies.
The chi-square test for trend was used to study ordinal categorical variables. The effect size of explanatory variables was estimated by calculating the odds ratio (OR), with a 95% confidence interval (95% CI).
2. Binary logistic regression analysis, hierarchical method.
Categorical and discrete variables were kept as such, adopting cutoff points used in the literature. The hierarchical theoretical framework was used as a reference for building a model that allowed adjustment for confounding factors (see Figure 1). Beforehand, the absence of multicollinearity among explanatory variables was verified, as well as the goodness-of-fit of the data through the Hosmer-Lemeshow test.
The proposed model discriminated hierarchically higher predictive factors (distal) as exerting their action on those situated lower (intermediate and proximal) [20].
Since many factors under study could confound the associations, the variables were hierarchically organized into blocks for selection of confounding factors most strongly associated with deaths in children under five years old.
Initially, variables with a p-value ≤ 0.20 in univariate analysis were selected. These variables were then analyzed together with the variables from the block to which they belonged in the conceptual model. Those that, in the intra-block analysis, had a p-value ≤ 0.10 were considered confounding factors and included as adjustment variables for the hierarchically lower variables according to the model. This procedure obviously relativizes the importance of the statistical significance of the distal factors, by their successive insertion in the subsequent steps of the analysis regardless of losing statistical significance in this procedure.
In summary, according to the model, Block A of more distal variables, which will adjust all hierarchically lower ones, consists of variables that in univariate analysis had a p-value ≤ 0.20 and in analysis with other variables in the same block had a p-value ≤ 0.10. These variables from the more distal block were used to adjust those from subsequent blocks, in which the process and criteria for statistical significance were the same.
Binary logistic regression analysis, hierarchical method, from the SPSS 26.0 software for Windows (SPSS Inc., Chicago, USA), was used with initial model saturation by including all variables from each block that had a univariate analysis p-value ≤ 0.20. Then, the variables from the block that had a p-value ≤ 0.10 after adjustment by other variables in the block were adjusted by hierarchically higher variables until only those within each block had a p-value < 0.10.
3. Results
3.1. Sample Characterization
A total of 1020 children, 340 cases, and 680 controls, were recruited for the study, with a slight predominance of males (55.9%). The median weight of the children at admission and respective interquartile range (IQR) was 7600g (5000), and the median (IQR) age was 15 (30) months. The mean (SD) maternal age was 24.6 (6) years, with the majority having less than six years of schooling (62.2%). The sample characterization is further detailed in Table 2, Table 3 and Table 4.
Respiratory infections topped the list of hospitalizations (31.6%), followed by malnutrition (20.2%) and malaria (15.3%). The leading cause of death was malaria (21.8%). 76.1% of deaths occurred within the first 24 hours of admission.
The primary causes of death (cases) and hospitalization (controls) are presented in Table 1.

Table 1.
Frequency distribution of diagnoses for cases (cause of death) and controls (hospital discharge). David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
Table 1.
Frequency distribution of diagnoses for cases (cause of death) and controls (hospital discharge). David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
| ICD-10 | Diagnosis | Discharge status | Total | ||||
|---|---|---|---|---|---|---|---|
| Control | Case | ||||||
| No | % | No | % | No | % | ||
| R10.0 | Acute abdomen | 5 | 0,7 | 5 | 1,5 | 10 | 1,0 |
| D64.9 | Severe anemia | 23 | 3,4 | 21 | 6,2 | 44 | 4,3 |
| Q20 –Q26 | Congenital heart disease | 20 | 2,9 | 10 | 2,9 | 30 | 2,9 |
| E43 | Severe unspecified protein-energy malnutrition | 137 | 20,1 | 50 | 14,7 | 187 | 18,3 |
| A09 | Diarrhea and Presumed Infectious Gastroenteritis | 53 | 7,8 | 32 | 9,4 | 85 | 8,3 |
| G00-G09 | Inflammatory diseases of the central nervous system | 22 | 3,2 | 26 | 7,6 | 48 | 4,7 |
| J00 - J99 | Acute Respiratory Infections | 215 | 31,6 | 62 | 18,2 | 277 | 27,2 |
| D57 | Sickle cell disease | 20 | 2,9 | 9 | 2,6 | 29 | 2,8 |
| K92.2 | Upper gastrointestinal bleeding | 2 | 0,3 | 4 | 1,2 | 6 | 0,6 |
| G91 | Hydrocephalus | 19 | 2,8 | 5 | 1,5 | 24 | 2,4 |
| L08.9 | Localized infection of skin and subcutaneous tissue | 13 | 1,9 | 2 | 0,6 | 15 | 1,5 |
| T18 | Foreign body ingestion | 8 | 1,2 | - | - | 8 | 0,8 |
| B50.8 | Unspecified malaria by Plasmodium falciparum | 104 | 15,3 | 74 | 21,8 | 178 | 17,5 |
| Q44 | Congenital malformations of the gallbladder, bile ducts, and other unspecified liver diseases | 1 | 0,1 | 4 | 1,2 | 5 | 0,5 |
| C80 | Malignant neoplasm, unspecified site | 3 | 0,4 | - | - | 3 | 0,3 |
| P20-P29;M069;E10;A35;G81.0;B05;K40; I27 | Others: Hypoxia, Arthritis, Diabetes, Tetanus, Non-specific flaccid paralysis, AIDS, Measles, Hernia, and Pulmonary Hypertension | 15 | 2,2 | 10 | 2,9 | 25 | 2,5 |
| P07 | Prematurity | - | - | 6 | 1,8 | 6 | 0,6 |
| A41.9 | Unspecified sepsis | 7 | 1,0 | 13 | 3,8 | 20 | 2,0 |
| S09.9 | Traumatic brain injury | 13 | 1,9 | 7 | 2,1 | 20 | 2,0 |
| Total | 680 | 100,0 | 340 | 100,0 | 1020 | 100,0 | |
Table 2.
Association between socioeconomic and environmental factors and the occurrence of deaths in children under five years old. David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
Table 2.
Association between socioeconomic and environmental factors and the occurrence of deaths in children under five years old. David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
| Level 1 | Case: n (%) | Control: n (%) | OR (CI 95%) | |
|---|---|---|---|---|
| Maternal education | ||||
| No schooling | 97(44,7) | 120(55,3) | 10,5(4,5-22,7) | |
| ≤6 years | 157(38,2) | 254(61,8) | 7,7(3,5-17,0) | |
| 7 – 12 years | 79(27,5) | 208(72,5) | 4,7 (2,1-10,6) | |
| >12 years | 7(7,4) | 87(92,6) | 1,0 | |
| Maternal marital status | ||||
| Single | 158(37,4) | 264(62,6) | 1,4(1,1-1,8) | |
| With partner | 182(30,4) | 416(69,6) | 1,00 | |
| Housing conditions | ||||
| Precarious | 136(35,5) | 247(64,5) | 1,2(0,3-1,5) | |
| Non-precarious | 204(32,0) | 433(68,0) | 1,00 | |
| Family income | ||||
| Unknown | 493(66,5) | 248(33,5) | 1,2(0,7-2,0) | |
| ≤ 1 MW | 20(62,5) | 12(37,5) | 1,4 (0,6-3,4) | |
| 1,01 - 3 MW | 107(66,0) | 55(34,0) | 1,2(0,7-2,2) | |
| ≥ 3,01 MW | 60(70,6) | 25(29,4) | 1,00 | |
| Intra-household crowding | ||||
| Moderate to intense crowding | 340(35,0) | 632(65,0) | 0,7(0,6-0,7) | |
| No crowding | -- | 48(100,0) | 1,00 | |
| Caregiver’s integration into the workforce | ||||
| Unemployed | 137(30,6) | 311(69,4) | 0,8(0,6-1,0) | |
| Not unemployed | 203(35,5) | 369(64,5) | 1,00 | |
| Household waste collection and treatment | ||||
| Inappropriate | 180(30,3) | 415(69,7) | 1,4(1,1-1,8) | |
| Appropriate | 160(37,6) | 265(62,4) | 1,00 | |
| Source of drinking water | ||||
| Not appropriate | 324(34,5) | 614(65,5) | 2,2(1,2-3,8) | |
| Appropriate | 16(19,5) | 66(80,5) | 1,00 | |
Table 3.
Association between maternal and care-related characteristics and the occurrence of deaths in children under five years old. David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
Table 3.
Association between maternal and care-related characteristics and the occurrence of deaths in children under five years old. David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
| Level 2 | Cases: n (%) | Controls: n (%) | OR (CI 95%) |
|---|---|---|---|
| Parity | |||
| ≥ 3 | 151(33,1) | 305(66,9) | 1,0(0,8-1,3) |
| ≤ 2 | 189(33,5) | 375(66,5) | 1,00 |
| Alcohol consumption during pregnancy | |||
| Yes | 222(48,5) | 236(51,5) | 3,5(2,7-4,7) |
| No | 118 (21,0) | 444(79,0) | 1,00 |
| Number of prenatal visits | |||
| ≤ 5 | 219 (33,7) | 430(66,3) | 1,1(0,8-1,4) |
| ≥ 6 | 121 (32,6) | 250(67,4) | 1,00 |
| Type of delivery | |||
| Cesarean | 13(19,1) | 55(80,9) | 0,5(0,2-0,8) |
| Vaginal | 327(34,3) | 625(65,7) | 1,00 |
| Place of delivery | |||
| Non-Hospital | 106(38,0) | 173(62,0) | 1,3(1,0-1,8) |
| Hospital | 234(31,6) | 507(68,4) | 1,00 |
| Length of hospital stay: | |||
| ≤ 24h | 70(76,1) | 22(23,9) | 7,8(4,7-12,8) |
| >24h | 270(29,1) | 658(70,9) | 1,00 |
| Nutritional status | |||
| With nutritional deficit | 202(39,1) | 314(60,9) | 1,7(1,3-2,2) |
| No nutritional deficit | 138(27,4) | 366(72,6) | 1,00 |
| Vaccination schedule | |||
| Incomplete for the age | 88(39,5) | 135(60,5) | 1,4(1,0-1,9) |
| Complete for age | 252(31,6) | 545(68,4) | 1,00 |
| Interbirth interval | |||
| ≤ 24 months | 113 (39,9) | 170(60,1) | 2,0(1,4-2,8) |
| >24 months | 85(25,2) | 252(74,8) | 1,00 |
Table 4.
Association between biological factors (maternal and child) and the occurrence of deaths in children under five years old. David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
Table 4.
Association between biological factors (maternal and child) and the occurrence of deaths in children under five years old. David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
| Level 3 | Case: n (%) | Control: n (%) | OR (CI95%) |
|---|---|---|---|
| Gender | |||
| Male | 190(33,3) | 380(66,7) | 1,0(0,8-1,3) |
| Female | 150(33,7) | 300(66,7) | 1,00 |
| Child’s age | |||
| ≤ 12 months | 152(33,3) | 305(66,7) | 1,0(0,8-1,3) |
| >12 months | 188(33,4) | 375(66,6) | 1,00 |
| Maternal age at delivery | |||
| 10-19 Years | 142(46,0) | 167(54,0) | 2,5(1,9-3,4) |
| 20 -34 Years | 152(25,3) | 449(74,7) | 1,00 |
| ≥35 Years | 46(41,8) | 64(58,2) | 2,1(1,4-3,2) |
In the bivariate analysis, among distal determinants, maternal education revealed a statistically significant difference concerning the occurrence of death, with mothers without education or with low education having 10 times higher odds of having children who died before the age of five. Similarly, increased odds of death were observed with moderate to intense intrahousehold crowding, unemployed parents or caregivers, inappropriate household waste disposal methods, consumption of water from inappropriate sources, as well as mothers who do not cohabit with their partners. The values of the socioeconomic and environmental variables found in this analysis are presented in Table 2.
Among intermediate determinants, statistically significant factors include alcohol consumption during pregnancy and hospitalization time ≤24h. The odds of death in children under five were 3.5 times higher in mothers who consumed alcoholic beverages during pregnancy and eight times higher within the first 24 hours of hospitalization. Poor nutritional status, incomplete vaccination schedules for age, and short interbirth intervals were also associated with death occurrence, as observed in Table 3.
Among proximal determinants, only maternal age (≤19 years and ≥35 years) was associated with death in children under five, showing twice the odds of deaths in children under five when compared to mothers aged 20 to 34 years (Table 4).
The hierarchical analysis revealed that the final model (stage 3) containing the variables caregiver’s education level, maternal marital status, caregiver’s occupation, alcohol consumption during pregnancy, type of delivery, length of hospital stay, nutritional status, interbirth interval, and maternal age at the time of pregnancy was statistically significant in predicting deaths in this group of children [X2 (12) = 191.584; p <0.001. R2 Nagelkerke = 0.375]. Table 5 presents the final model of binary logistic regression analysis using the hierarchical method.
4. Discussion
Reducing mortality in children under five to at least 25 per 1000 live births is one of the sustainable development goals related to child health[3]. The study assessed the influence of distal, intermediate, and proximal determinants on hospital deaths in children under five at David Bernardino Pediatric Hospital, a reference in pediatric care in Angola. The most relevant findings reveal that the majority of deaths occurred due to preventable causes, with an emphasis on distal and intermediate determinants.
Among the factors associated with under-five mortality in developing countries, socioeconomic factors are pointed out as deterministic relative to environmental factors, maternal characteristics, healthcare, nutritional status, and pre-existing health conditions[12,13,21].
Hierarchical modeling was chosen in this study as an alternative to traditional analysis methods due to the advantage of considering both "biological" and "statistical" aspects, structuring the investigation of risk factors and facilitating the interpretation of results [22,23]. The hierarchy of independent variables established in the conceptual framework[22] was maintained throughout the data analysis, allowing for the selection of those most strongly associated with the outcome of interest.
In this study, malaria was the leading cause of death followed by acute respiratory diseases, malnutrition, and gastrointestinal diseases. Approximately 35% of the demand for curative care in Angola is attributed to malaria, a pathology responsible for 20% of hospital admissions and 40% of perinatal deaths [9]. These findings are supported by previous studies conducted in Angola [24–26] and other African countries [27,28]. It is possible that the results are related to the high endemicity of the disease in the country, where it remains a significant public health problem, compounded by a lack of access to quality healthcare services associated with precarious socioeconomic conditions.
Poor environmental sanitation and failure to comply with basic prevention measures such as water treatment and food safety, as described in the country’s Multiple Indicator Cluster Survey [9], also contribute to the high prevalence of both acute diarrheal diseases and respiratory diseases. These findings underscore the need for improvements in environmental conditions, expanded access to healthcare services, and greater effectiveness in case management.
Among the distal (socioeconomic) factors, maternal education level was of great importance in predicting deaths in children under five, both in univariate and hierarchical analysis, showing a higher likelihood of deaths in children under five born to mothers with no education or low education compared to those with more than 12 years of schooling. Several studies in Africa have described a significant association between low maternal education and deaths in children under five [29–32]. The relevance of this data may be due to the fact that maternal education is considered an important marker of the mother’s and family’s socioeconomic status, playing a significant role in adopting healthy behaviors and habits with a direct impact on the health of their children [29,31].
Although some studies[4,33] have shown an association between unemployment, family income, and higher mortality in children under five, in this study, these variables did not show statistical significance even in univariate analysis. This could be due to the culturally sensitive nature and complex approach of this information, as most surveyed mothers were unaware of their partners’ monthly income, and it is very likely that the information provided by the mother does not reflect reality in the same way. Additionally, unemployed caregivers also did not have higher chances of having children who died before the age of five.
Alcohol consumption during pregnancy has been associated with mortality in children under five and various other health problems [34,35]. In this study, the odds of death were 3.8 times higher in mothers who had frequent alcohol habits during pregnancy. The consumption of alcoholic beverages and other legal or illegal drugs can directly affect fetal development; it can alter placental function, reducing the exchange of oxygen and nutrients between the fetus and the mother[36]. This is likely to increase the risk of childhood death due to the negative impact on the mother’s nutritional status during pregnancy and considering the biological relationship between mother and fetus during this period, where the latter are extremely dependent on the maternal organism for their development.
The odds of death were 13.7 times higher in children with less than 24 hours of hospitalization, highlighting the weight of epidemiological factors independent of the hospital in child mortality. This result aligns with findings from previous studies in the same hospital [37] and underscores the need to strengthen primary healthcare strategies for populations and improve the referral and counter-referral system. On the other hand, the findings may be justified by the late arrival of children at the hospital, often in advanced stages of illness, either directly from home or from alternative treatment institutions.
Children with moderate to severe malnutrition had twice the chance of dying during hospitalization compared to those without malnutrition, even after adjusting for all other variables; findings that coincide with others described in the literature [25–27]. Indeed, malnourished children have a deficient immune response, with more severe infections than well-nourished children; thus, measures aimed at preventing low birth weight and maintaining adequate nutritional status, provided through proper prenatal care and follow-up in childcare consultations, are interventions that can significantly reduce the risk of hospitalization and death in this age group.
Short interbirth spacing presented, in this study, a chance of about twice as high in predicting deaths in children under five. The WHO identifies the period between two consecutive live births as a critical determinant of childhood mortality risks and recommends a spacing of three to five years between two consecutive births to reduce risks to the health of children and mothers[38]. Short intervals between births are described in the literature as important predictors of adverse outcomes for children, especially in developing countries[31,32,39], and maternal depletion, infection transmission, and sibling competition may be some of the main explanations for this association [40].
In summary, shorter birth intervals do not allow women to fully recover their physical well-being and the ideal distribution of energy and micronutrients from the previous pregnancy, which may result in suboptimal fetal development and increased risk of mortality for the child born after the short interval [40,41]. Short intervals between births predispose the younger child to a set of diseases similar to those of the older sibling, compromising the development of the immune system, which for certain communicable diseases, such as measles, tends to have significantly higher fatality rates[42]; and finally, because developing countries typically have a large number of extended and poor families, children with close spacing are more likely to compete for the same family resources, especially for breast milk, a fundamental food in the first years of life for the index child [43].
Higher mortality in children under five among live births of mothers at extreme ages, (aged ≤19 years and those over 35 years), is suggested in several studies [44–47]. In this study, maternal age was found to be associated with the outcome in both univariate analysis and hierarchical logistic regression; the findings demonstrate the need for reinforcement in family planning efforts and strengthening of primary healthcare. However, in some studies, this association is not sufficiently clear as the variable may be influenced by various factors, such as the quality of access to healthcare services, socioeconomic conditions, and education [48].
Several physiological, cultural, and socioeconomic factors may contribute to this unfavorable outcome. Physiologically, the younger the mother’s body, the higher the likelihood of pregnancy and childbirth complications that increase the risk of mortality in children under five [47]. Socioculturally, adolescent mothers are more likely to face stigma and barriers in accessing maternal health services, predisposing children to a higher risk of death[49,50]; and, socioeconomically, compared to adults, adolescent mothers are more likely to have low levels of education and unfavorable economic conditions, which have been considered predictors of mortality in children under five [4,33,51].
On the other hand, advanced maternal age is associated with increased stillbirths, premature births, intrauterine growth restriction, as well as chromosomal abnormalities resulting from multiple factors. In some contexts, it is women with lower socioeconomic status, lower education levels, and higher parity, while in others, it is educated women who delayed pregnancy for career reasons. Older mothers are at higher risk of obesity, diabetes, hypertension, and pregnancy-related complications [48,52].
The lack of association between socioeconomic factors—family income, household overcrowding, housing conditions, and unemployment—and higher mortality in children under 5 years old in this study suggests that other determinants may be more relevant. However, it is necessary to consider that these factors may indirectly influence child health through access and quality of healthcare services, and therefore, the lack of direct association does not imply that these factors are irrelevant. Additionally, the study only analyzed hospital mortality, excluding possible impacts on deaths occurring outside the hospital environment. The sample size may have affected the results, highlighting the need for additional studies, including those with longitudinal designs covering different levels of healthcare, to achieve a more comprehensive understanding of determinants of mortality in children under five in Angola and to guide more effective public policies.
5. Conclusions
The predominance of deaths due to malaria, respiratory diseases, gastrointestinal infectious diseases, and malnutrition indicates precarious living conditions, poor environmental sanitation, unfavorable environmental conditions, and deficiencies in child healthcare, with an emphasis on the limitations of primary healthcare and early treatment of patients. The prioritization of risk factors revealed that the majority of hospital deaths in children under five at DBPH occurred due to preventable causes; distal and intermediate determinants exerted a strong influence on the occurrence of deaths in children under five. Reducing social inequalities and improving the quality of services provided in primary healthcare are essential for reducing child and adolescent mortality.
Author Contributions
Authors ICA, LV, and JCV worked on the conception, study design, and final article review. LV and JCV also contributed to refining the methodology, critical review of the article, as well as analysis and interpretation of the data. All authors read and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Pedagogical Directorate of DBPH following approval from the Ethics Committee of the Angolan Institute of Health Research with opinion No. 19 C.E/MINSA.INIS/2022. All caregivers and legal guardians of the children who participated in the study provided their informed consent. Patient information was anonymized prior to analysis.
Informed Consent Statement
Informed consent was obtained from all subjects (caregivers) involved in the study.
Data Availability Statement
The data used in this study belong to DBPH and are under the auspices of IHMT. They may be available upon request to researchers who meet the criteria for accessing confidential data. Data requests should be directed to Professor Luís Varandas, Supervisor of the lead researcher of this study and Professor at IHMT, whose email address is varandas@ihmt.unl.pt. Requestors should provide details about the purpose of the request and must meet the requirements of the Scientific Council of IHMT, and should only be used for the purpose defined in the request.
Acknowledgments
We thank the statistics department of DBPH and the healthcare professionals of that institution for their support.
Conflicts of Interest
The authors declare that they have no conflicting interests.
References
- WHO. Child mortality (under 5 years): WHO; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-under-5-mortality-in-2020.
- Yaya S, Bishwajit G, Okonofua F, Uthman OA. Under five mortality patterns and associated maternal risk factors in sub-Saharan Africa: A multi-country analysis. PloS one [Internet]. 2018 Pmc6201907]; 13(10):[e0205977 p.]. Available from: https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0205977.
- Jeffrey D. Sachs GL, Grayson Fuller, Drumm aE. SUSTAINABLE DEVELOPMENT REPORT 2023. Paris: Dublin University Press, 2023 Contract No.: 10.25546/102924.
- Van Malderen C, Amouzou A, Barros AJD, Masquelier B, Van Oyen H, Speybroeck N. Socioeconomic factors contributing to under-five mortality in sub-Saharan Africa: a decomposition analysis. BMC public health. 2019;19(1):760.
- Shoo R. Reducing child mortality: the challenges in Africa. UN Chron [Internet]. 2007 [cited 2023 05/November]. Available from: https://www.researchgate.net/profile/Rumishael-Shoo/publication/265619672_Reducing_Child_Mortality_The_Challenges_in_Africa/links/54cb56470cf2517b7561885b/Reducing-Child-Mortality-The-Challenges-in-Africa.pdf.
- e Pinto EA, Alves JG. The causes of death of hospitalized children in Angola. Tropical doctor [Internet]. 2008 Jan [cited 2023 05/November]; 38(1):[66-7 pp.]. Available from: https://pubmed.ncbi.nlm.nih.gov/18302879/.
- Rosário EV, Costa D, Timóteo L, Rodrigues AA, Varanda J, Nery SV, et al. Main causes of death in Dande, Angola: results from Verbal Autopsies of deaths occurring during 2009-2012. BMC public health [Internet]. 2016 Aug 4 [cited 2023 05/November]; 16:[719 p.]. Available from: https://pubmed.ncbi.nlm.nih.gov/27491865/.
- Rodrigues EC, Alves BdCA, da Veiga GL, Adami F, Carlesso JS, dos Santos Figueiredo FW, et al. Mortalidade neonatal em Luanda, Angola: o que pode ser feito para sua redução? Journal of Human Growth and Development [Internet]. 2019 [cited 2023 09/November]; 29(2):[161 p.]. Available from: https://scholar.google.com.br/scholar?hl=pt-BR&as_sdt=0%2C5&q=Mortalidade+neonatal+em+Luanda%2C+Angola%3A+o+que+pode+ser+feito+para+sua+redu%C3%A7%C3%A3o%3F&btnG=.
- Angola MdPedDTM. Inquérito de Indicadores Múltiplos e de Saúde (IIMS) - 2015-2016. Final report. Angola: Instituto Nacional de Estatística, Ministério da Saúde (MINSA), 2015-2016 2017. Report No.: Contract No.: 01.
- Federation, R. Voluntary National Review on the Implementation of the 2030 Agenda for Sustainable Development. Analytical Center under the Government of the Russian Federation: Moscow, Russia [Internet]. 2020 [cited 2023 10/Novenmer]. Available from: https://sustainabledevelopment.un.org/content/documents/286012021_VNR_Report_Angola.pdf.
- Mosley WH, Chen LC. An analytical framework for the study of child survival in developing countries. 1984. Bulletin of the World Health Organization [Internet]. 2003 [cited 2023 10/November]; 81(2):[140-5 pp.]. Available from: https://pubmed.ncbi.nlm.nih.gov/12756980/.
- Lima S, Carvalho ML, Vasconcelos AG. [Proposal for a hierarchical framework applied to investigation of risk factors for neonatal mortality]. Cadernos de saude publica [Internet]. 2008 Aug [cited 2023 10/November]; 24(8):[1910-6 pp.]. Available from: https://pubmed.ncbi.nlm.nih.gov/18709231/.
- Bizzego A, Gabrieli G, Bornstein MH, Deater-Deckard K, Lansford JE, Bradley RH, et al. Predictors of Contemporary under-5 Child Mortality in Low- and Middle-Income Countries: A Machine Learning Approach. International journal of environmental research and public health [Internet]. 2021 Feb 1 [cited 2023 10/November]; 18(3). Available from: https://pubmed.ncbi.nlm.nih.gov/33535688/.
- IBGE. Indicadores IBGE. Rio de Janeiro: Fundação Instituto Brasileiro de Geografia e Estatística, 1991.
- Advogados, Sd. Actualizaçao do valor da retribuiçao mínima mensal garantida. Luanda: 2017.
- Ludermir, AB. unemplyement, informal work, gender and mental health. Cad Saúde Pública. 2000;16(3):647 - 59.
- Hill PC, Jackson-Sillah D, Donkor SA, Otu J, Richard A, Adegbola A, et al. Risk factors for pulmonary tuberculosis: a clinic-based case control study in The Gambia.. BMC Public Health. 2006;6(156).
- WHO WHO. Physical status: the use and interpretation of anthropometry.. Geneva: World Health Organization, 1995.
- World Health, O. Self-help strategies for cutting down or stopping substance use: a guide2010 2010 [cited 2023 11/Dezembro]. Available from: https://iris.who.int/handle/10665/44322.
- Victora CG, Huttly SR, Fuchs SC, Olinto MTA. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. International Journal of Epidemiology. 1997;26(1):224 - 7.
- Olinto, M. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. International journal of epidemiology [Internet]. 1997 [cited 2023 04/September]; 26(1):[224-7 pp.]. Available from: https://academic.oup.com/ije/article/26/1/224/730584?login=true.
- Fuchs SC, Victora CG, Fachel J. Modelo hierarquizado: uma proposta de modelagem aplicada à investigação de fatores de risco para diarréia grave. Revista de Saúde Pública [Internet]. 1996 [cited 2023 04/09]; 30:[168-78 pp.]. Available from: https://www.scielo.br/j/rsp/a/hP6yDbh7HWXmLymbyvScBMw/?lang=pt&format=html.
- Greenland, S. Modeling and variable selection in epidemiologic analysis. American journal of public health [Internet]. 1989 [cited 2023 04/September]; 79(3):[340-9 pp.]. Available from: https://ajph.aphapublications.org/doi/abs/10.2105/AJPH.79.3.340.
- Pinto EAE, Alves JG. The causes of death of hospitalized children in Angola. Tropical doctor [Internet]. 2008 [cited 2023 03/September]; 38(1):[66-7 pp.]. Available from: https://journals.sagepub.com/doi/abs/10.1258/td.2006.006352.
- Rosário EVN, Costa D, Timóteo L, Rodrigues AA, Varanda J, Nery SV, et al. Main causes of death in Dande, Angola: results from Verbal Autopsies of deaths occurring during 2009–2012 2016 [cited 2023 05/September]. Available from: https://link.springer.com/article/10.1186/s12889-016-3365-6.
- Simão R, Gallo PR. Mortes infantis em Cabinda, Angola: desafio para as políticas públicas de saúde. Revista Brasileira de Epidemiologia [Internet]. 2013 [cited 2023 03/September]; 16:[826-37 pp.]. Available from: https://www.scielo.br/j/rbepid/a/wGTtzSgJPvqXBqJjtm5kD4c/?lang=pt.
- Tette E, Nyarko MY, Nartey ET, Neizer ML, Egbefome A, Akosa F, et al. Under-five mortality pattern and associated risk factors: a case-control study at the Princess Marie Louise Children’s Hospital in Accra, Ghana. BMC pediatrics [Internet]. 2016 [cited 2023 04/September]; 16(1):[1-10 pp.]. Available from: https://bmcpediatr.biomedcentral.com/articles/10.1186/s12887-016-0682-y.
- Mutombo AM, Mukuku O, Tshibanda KN, Swana EK, Mukomena E, Ngwej DT, et al. Severe malaria and death risk factors among children under 5 years at Jason Sendwe Hospital in Democratic Republic of Congo. Pan African Medical Journal. 2018;29(1):1-8.
- Tesema GA, Seifu BL, Tessema ZT, Worku MG, Teshale AB. Incidence of infant mortality and its predictors in East Africa using Gompertz gamma shared frailty model. Archives of Public Health [Internet]. 2022 [cited 2023 05/September]; 80(1):[1-12 pp.]. Available from: https://archpublichealth.biomedcentral.com/articles/10.1186/s13690-022-00955-7.
- GT K, C C, D B, TY T, D L. The effect of maternal education on infant mortality in Ethiopia: A systematic review and meta-analysis. PloS one. 2019;14(7):e0220076.
- Ezeh OK, Agho KE, Dibley MJ, Hall JJ, Page AN. Risk factors for postneonatal, infant, child and under-5 mortality in Nigeria: a pooled cross-sectional analysis. BMJ open [Internet]. 2015 [cited 2023 05/September]; 5(3):[e006779 p.]. Available from: https://bmjopen.bmj.com/content/bmjopen/5/3/e006779.full.pdf.
- Yaya S, Ahinkorah BO, Ameyaw EK, Seidu A-A, Darteh EKM, Adjei NK. Proximate and socio-economic determinants of under-five mortality in Benin, 2017/2018. BMJ global health [Internet]. 2020 [cited 2023 05/September]; 5(8):[e002761 p.]. Available from: https://gh.bmj.com/content/5/8/e002761.abstract.
- Ahinkorah BO, Seidu AA, Budu E, Armah-Ansah EK, Agbaglo E, Adu C, et al. Proximate, intermediate, and distal predictors of under-five mortality in Chad: analysis of the 2014-15 Chad demographic and health survey data. BMC public health. 2020;20(1):1873.
- Bohland AK, Gonçalves AR. Mortalidade atribuível ao consumo de bebidas alcoólicas. SMAD, Revista Electrónica en Salud Mental, Alcohol y Drogas [Internet]. 2015 [cited 2023 06 Dezembro]; 11(3):[136-44 pp.]. Available from: https://www.redalyc.org/pdf/803/80342807004.pdf.
- Grinfeld, H. Consumo nocivo de álcool durante a gravidez. Álcool e suas consequências: uma abordagem multiconceitual São Paulo: Manole [Internet]. 2009 [cited 2023 06 Dezember]; 8(3):[179-99 pp.]. Available from: https://www.saudedireta.com.br/docsupload/1333063336alcoolesuasconsequencias-pt-cap9.pdf.
- Ahumada LA, Anunziata F, Molina JC. Alcohol consumption during pregnancy. Archivos argentinos de pediatria [Internet]. 2021 Feb [cited 2023 08/September]; 119(1):[6-8 pp.]. Available from: https://pubmed.ncbi.nlm.nih.gov/33458973/.
- Pinto, E. Perfil epidemiológico, clínico e fatores associados ao óbito em crianças internadas no hospital pediátrico de referência de Angola: um estudo transversal: Doctoral Dissertation. Instituto Materno Infantil Professor Fernando Figueira; 2005.
- Organization WH. Report of a WHO technical consultation on birth spacing: Geneva, Switzerland 13-15 June 20052007 [cited 2023 05/September]. Available from: https://apps.who.int/iris/bitstream/handle/10665 /69855/WHO_RHR_07.1_eng.pdf?sequence=1.
- Sharaf MF, Rashad AS. Socioeconomic inequalities in infant mortality in Egypt: analyzing trends between 1995 and 2014. Social Indicators Research [Internet]. 2018 [cited 2023 06/September]; 137:[1185-99 pp.]. Available from: https://link.springer.com/article/10.1007/s11205-017-1631-3.
- Molitoris J, Barclay K, Kolk M. When and where birth spacing matters for child survival: an international comparison using the DHS. Demography [Internet]. 2019 [cited 2023 05/September]; 56(4):[1349-70 pp.]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6667399/.
- Greenberg JA, Bell SJ, Guan Y, Yu Y-h. Folic acid supplementation and pregnancy: more than just neural tube defect prevention. Reviews in obstetrics and gynecology [Internet]. 2011 [cited 2023 06/September]; 4(2):[52 p.]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3218540/.
- Garenne M, Aaby P. Pattern of exposure and measles mortality in Senegal. Journal of infectious diseases [Internet]. 1990 [cited 2023 06/September]; 161(6):[1088-94 pp.]. Available from: https://academic.oup.com/jid/article-abstract/161/6/1088/905326?login=false.
- Molitoris, J. Breastfeeding during pregnancy and its association with childhood malnutrition and pregnancy loss in low-and middle-income countries. Lund Papers Econ Demogr [Internet]. 2018 [cited 2023 06/September]; 3:[1-81 pp.]. Available from: https://www.ed.lu.se/media/ed/papers/working_papers/LPED%202018%203.pdf.
- Gibbs CM, Wendt A, Peters S, Hogue CJ. The impact of early age at first childbirth on maternal and infant health. Paediatric and perinatal epidemiology. 2012;26 Suppl 1(0 1):259-84.
- Finlay JE, Özaltin E, Canning D. The association of maternal age with infant mortality, child anthropometric failure, diarrhoea and anaemia for first births: evidence from 55 low- and middle-income countries. BMJ Open. 2011;1(2):e000226.
- Sinha S, Aggarwal AR, Osmond C, Fall CH, Bhargava SK, Sachdev HS. Maternal Age at Childbirth and Perinatal and Under five Mortality in a Prospective Birth Cohort from Delhi. Indian pediatrics. 2016;53(10):871-7.
- Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Bommarito K, Madden T, Olsen MA, et al. Maternal age and risk of labor and delivery complications. Maternal and child health journal. 2015;19(6):1202-11.
- Lima LCd. Idade materna e mortalidade infantil: efeitos nulos, biológicos ou socioeconômicos? Revista Brasileira de Estudos de População [Internet]. 2010 [cited 2023 07 Dezembro]; 27:[211-26 pp.]. Available from: https://www.scielo.br/j/rbepop/a/79fgFBtcB5VgRqshmTkBC9K/.
- Chirwa GC, Mazalale J, Likupe G, Nkhoma D, Chiwaula L, Chintsanya J. An evolution of socioeconomic related inequality in teenage pregnancy and childbearing in Malawi. PloS one. 2019;14(11):e0225374.
- Atuyambe L, Mirembe F, Tumwesigye NM, Annika J, Kirumira EK, Faxelid E. Adolescent and adult first time mothers’ health seeking practices during pregnancy and early motherhood in Wakiso district, central Uganda. Reproductive health [Internet]. 2008 Dec 30 [cited 2023 08/September]; 5:[13 p.]. Available from: https://www.ajol.info/index.php/pamj/article/view/176605.
- Yaya S, Ahinkorah BO, Ameyaw EK, Seidu AA, Darteh EKM, Adjei NK. Proximate and socio-economic determinants of under-five mortality in Benin, 2017/2018. BMJ global health. 2020;5(8).
- Fall CH, Sachdev HS, Osmond C, Restrepo-Mendez MC, Victora C, Martorell R, et al. Association between maternal age at childbirth and child and adult outcomes in the offspring: a prospective study in five low-income and middle-income countries (COHORTS collaboration). Lancet Glob Health [Internet]. 2015 Jul [cited 2023 07 Dezembro]; 3(7):[e366-77 pp.]. Available from: https://pubmed.ncbi.nlm.nih.gov/25999096/.
Figure 1.
Population selection for the study.
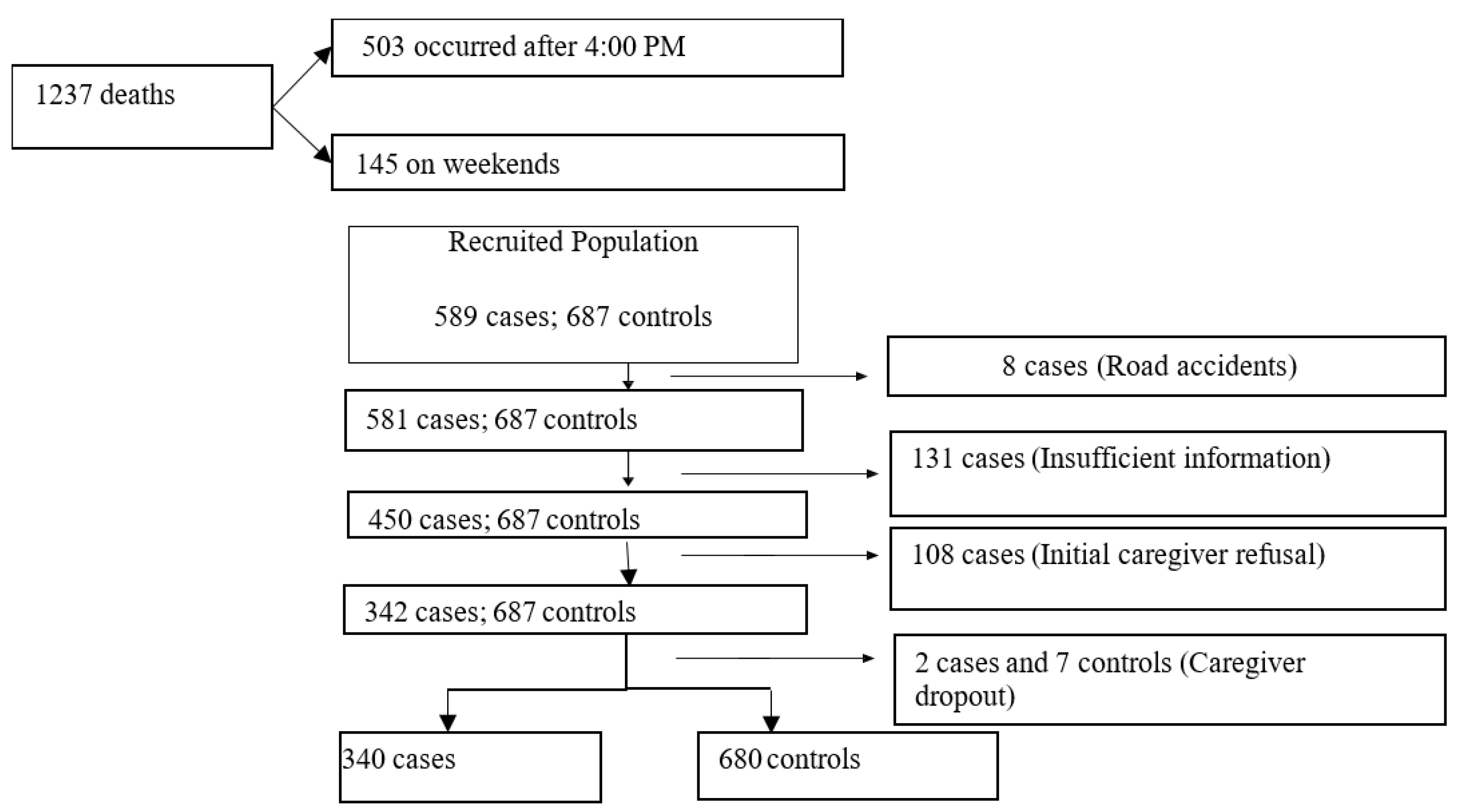
Figure 2.
Explanatory Model for Under-Five Mortality (Adapted from Mosley Chen, 1984).
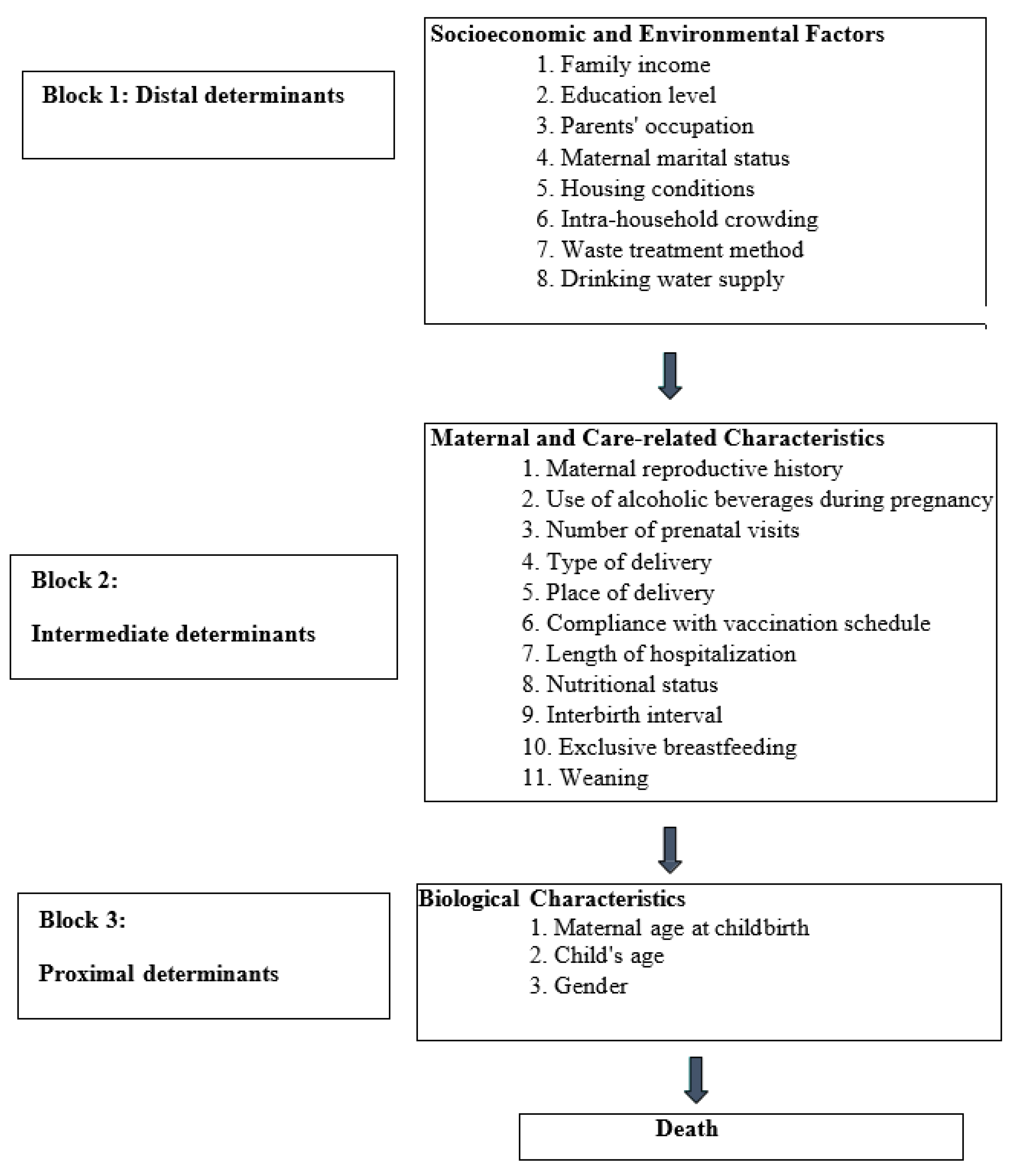
Table 5.
Final model of hierarchical binary logistic regression analysis of risk factors for deaths in children under five years old: David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
Table 5.
Final model of hierarchical binary logistic regression analysis of risk factors for deaths in children under five years old: David Bernardino Pediatric Hospital (Angola): May 1, 2022 - June 30, 2023.
| Factors | β | S.E | Wald | Df | Sig. | OR (CI 95%) | |
|---|---|---|---|---|---|---|---|
| Caregiver’s occupation (unemployed) | -0,8 | 0,3 | 10,1 | 1 | 0,001 | 0,4(0,3-0,7) | |
| Marital status (without a partner) | -0,1 | 0,3 | 0,3 | 1 | 0,580 | 0,9(0,5-1,4) | |
| Maternal education | |||||||
| No education | 1,5 | 0,7 | 4,9 | 1 | 0,027 | 4,3(1,2-15,7) | |
| ≤6 Years | 1,2 | 0,7 | 3,5 | 1 | 0,060 | 3,4-(1,0-12,1) | |
| 7-12 Years | 1,1 | 0,7 | 2,9 | 1 | 0,087 | 3,1(0,9-11,5) | |
| >12 Years | 5,4 | 3 | 0,144 | ||||
| Frequent alcohol consumption during pregnancy (Yes) | 1,4 | 0,2 | 38,0 | 1 | 0,001 | 3,8(2,5-5,9) | |
| Type of delivery (cesarean section) | -1,4 | 0,8 | 3,3 | 1 | 0,071 | 0,3(0,1-1,1) | |
| Length of hospital stay (≤24 hours) | 2,6 | 0,4 | 40,7 | 1 | 0,001 | 13,8(6,2-30,8) | |
| Nutritional status (with deficit) | 0,8 | 0,2 | 12,3 | 1 | 0,001 | 2,1(1,4-3,2) | |
| Interbirth interval (≤24 months) | 0,5 | 0,2 | 6,1 | 1 | 0,014 | 1,7(1,1-2,5) | |
| Maternal age at the time of delivery | |||||||
| ≤19 Years | 1,7 | 0,3 | 27,4 | 1 | 0,001 | 5,6(3,0-10,8) | |
| 20 a 34 Years | 30,5 | 2 | 0,001 | ||||
| ≥35 Years | 0,8 | 0,3 | 7,4 | 1 | 0,006 | 2,1(1,2-3,7) | |
| Constant | -3,5 | 0,7 | 28,4 | 1 | 0,001 | 0,03 | |
| Model 1 = caregiver’s education + marital status + caregiver’s occupation; Model 2 = Model 1 + alcohol consumption during pregnancy + type of delivery + length of hospital stay + nutritional status + interpregnancy interval; Model 3 = Model 2 + maternal age at time of pregnancy | |||||||
β = Coefficient; Standard error (SE); df= degrees of freedom; sig. = Statistical significance; OR Odds ratio; CI = confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



