
Submitted:
30 May 2024
Posted:
30 May 2024
You are already at the latest version
Abstract
Abstract: Physicians, physical therapists, and occupational therapists have traditionally assessed hand motor function in hemiplegic patients but often struggle to evaluate complex hand move-ments. To address this issue, in 2019, we developed Fahrenheit, a device and algorithm that uses infrared camera image processing to estimate hand paralysis. However, due to Fahrenheit's de-pendency on specialized equipment, we conceived a simpler solution: developing a smartphone app that integrates MediaPipe. The objective of this study was to measure hand movements in stroke patients using both MediaPipe and Fahrenheit and to assess their criterion-related validity. The analysis revealed moderate-to-high correlations between the two methods. Consistent results were also observed in the peak angle and velocity comparisons across severity stages. Because Fahrenheit determines finger recovery status based on these measures, it has the potential to transfer this function to MediaPipe. This study highlighted the potential use of MediaPipe in pa-ralysis estimation applications.
Keywords:
MediaPipe
; hand tracking
; paralysis estimation
1. Introduction
The human "hand" contains a unique set of features within its complex assembly of joints, finely tuned for its specialized role as a delicate manipulative organ [1]. Understanding that hand function relies on specialized areas within the central nervous system to monitor the environment via sensory receptors and control fine movements through both exogenous and endogenous muscles is crucial [2]. Therefore, impairments in finger function following stroke are significant issues that directly affect the activities of daily living (ADL) and quality of life (QOL), making the improvement of finger function a key goal in the rehabilitation of stroke survivors [3].
To rehabilitate paralyzed fingers, it is important to optimize the quality and quantity of tasks. Quality refers to the appropriate level of difficulty, and quantity refers to the appropriate amount of practice[4,5]. To improve the quality of training, it is necessary to grade training according to its severity [6], and accurate evaluation is required to make this possible.
Typical measures of motor function in stroke include the Fugl-Meyer assessment [7], Brunnstrom stage [8], and Stroke Impairment Assessment Set (SIAS) [9], all of which score motor function based on the expert's visualization of motor onset and end. Since motor function assessment is performed and judged by experts, it can be performed in a short time without special equipment and has been widely used. However, visual evaluation of the starting and stopping positions of movements does not include factors related to the speed and trajectory of hand movements. In addition, the accurate evaluation of complex and high-speed hand motions using human vision is limited.
The development of image analysis in recent years has been remarkable, and various three-dimensional (3D) motion analyzers have been applied to provide temporal and spatial analyses of human motion. Our research team has also demonstrated that a binocular camera can be used to determine the severity of paralysis[10,11]. This device, called the Fahrenheit development code, is a method for recording hand motions and estimating hand functions by estimating joint centers and calculating motion features from difference images captured by binocular cameras. Fahrenheit can help both the rehabilitation specialist and patient record and analyze the motor functions of the patient's hand to determine the effectiveness of training. However, Fahrenheit requires a dedicated infrared camera and computer terminal running an application for analysis, making its use at the bedside somewhat labor-intensive. To widely apply this system in clinical practice, we conceived the idea of implementing a dedicated application on a smartphone using a camera. MediaPipe [12] is an open-source AI solution that can estimate joint centers from videos of fingers captured using an optical monocular camera. In fact, accuracy comparisons between infrared and optical cameras have been made using pose discrimination accuracy [13,14]; however, because they do not consider the temporal component, they do not evaluate the equivalence of motion velocity and trajectory, which is our goal. To replace MediaPipe with the binocular camera imaging function of Fahrenheit, we must verify the equivalence of the hand motion estimation.
Therefore, in this study, we examined the temporal and spatial criterion-related validity of the Fahrenheit and MediaPipe functions. If the equivalence of both functions is ensured, a simple smartphone-based paralysis estimation application can be developed. This will not only assist physicians and therapists in their clinical evaluations but also serve as a basis for the development of independent training devices for patients.
2. Materials and Methods
2.1. Research Design
This study is a retrospective observational design.
2.2. Target
Patients with post-stroke sequelae who participated in the Fahrenheit Development Project at Saitama Prefectural University were included in this study. Participants were patients aged 20 years or older who were admitted to the Tokyo Dental University Ichikawa General Hospital between June 1, 2016, and March 31, 2021, and were recruited from among all inpatients who had suffered a stroke. Patients were classified into 6 groups, stages I–VI, according to the Brunnstrom Recovery Stages (BRS), with reference to previous studies [10,11]. Using G*power to construct models for F tests and ANCOVA, encompassing fixed effects, main effects, and interactions (with α=.05, 1-β=. 8, effect size f=.5, and six groups), the minimum sample size was calculated to be 34. The exclusion criteria were as follows: (1) history of multiple cerebral infarctions or transient ischemic attacks; (2) loss of one or more fingers; (3) severely limited range of motion (ROM); (4) difficulty in understanding verbal instructions due to impaired consciousness, dementia, or aphasia; (5) a history of stroke or transient ischemic attack; (6) patients who needed bed rest; (7) patients who had difficulty maintaining a sitting position for at least 30 min, and (8) patients who had difficulty maintaining the required position during measurements even with assistance. Data in which the patient's fingers were not included in the angle of view from which the image was taken were excluded from the analysis.
2.3. Device
2.3.1. MediaPipe
MepipPipe is an open-source machine learning (ML) solution framework provided by Google Inc. There are several solutions available for MediaPipe; in this study, we used MediaPipe Hands, a hand-tracking solution released in 2019. MediaPipe Hands uses machine learning to infer 21 3D hand-finger landmarks from a single frame captured by a monocular camera, providing highly accurate hand and finger tracking. According to the Google AI, Blogs [15], the average accuracy of hand tracking is 95.7%. One of the features of this system is that it runs in mobile and powerful desktop environments [12].
2.3.2. Fahrenheit
Fahrenheit, developed by Hamaguchi et al., contains an infrared sensor, the Leap Motion Controller (LMC), and obtains the coordinates of the joint centers using Unity game software (http://japan.unity3d.com/) (Code name, Fahrenheit; patent number, 6375328; Saitama Prefectural University, Japan). Fahrenheit has 24 joint landmarks and can measure the ROM of the hand based on conventional joint range-of-motion measurements. Fahrenheit was operated on a laptop computer with a 64-bit Windows 8 (Microsoft, Kobe, Japan), and the generated data were stored on the hard drive of the same computer. It was implemented with a resolution of 0.001 mm and a sampling rate of 60 frames per second (fps) [10].
2.3.3. Basic Performance of Fahrenheit and MediaPipe
To realize delicate hand movements, including dexterity movements, in real time, the processing frame rate of hand tracking must be sufficiently fast. In terms of frame rate, Fahrenheit is superior because processing is performed on the device, whereas MediaPipe is considerably affected by the frame rate of the data from the camera used and the performance of the terminal running the processing algorithm (Table 1).
Regarding joint landmarks, Fahrenheit includes the metacarpals of each finger, whereas MediaPipe does not. Therefore, it is difficult to obtain accurate flexion angles of finger MP joints using conventional ROM measurement methods. Fahrenheit is limited to 90° in terms of the estimated range of motion of the hand MP joints, and values exceeding 90° are corrected to 90° or less.
2.4. Protocol
The patients were seated in a chair or wheelchair with the shoulder joint in a resting position, elbow joint in approximately 90° of flexion, forearm in a rotated position, and wrist in an intermediate position, and their hand movements were measured. The subjects were instructed to assume the starting posture of each task at approximately 20 cm above Fahrenheit and to maintain the starting posture for 5 s from the starting cue while watching the monitor on a laptop computer. After 5 s, on the verbal cue, the participants were instructed to repeat hand flexion and extension for as long as possible for 20 s and then maintain the maximum reaching position for 15 s after the start cue. Participants were provided with virtual hand images obtained from the recordings to show their hand movements in real time. The coordinate data obtained by the infrared camera were used as the Fahrenheit data (Figure 1a and 1b). The videos for the MediaPipe analysis were captured from a video camera used to capture the entire hand motion during the acquisition of the Fahrenheit data. The video was divided into images at a sampling rate of 30 fps, the coordinates were extracted from each image using MediaPipe keypoints, and the keypointed images were converted to video. The images with keypoints were converted into movies (Figure 1c). In both cases, data from 10 to 20 s after the start of the measurement were used for analysis.
2.5. Preprocessing
2.5.1. Data Specification and Angle Conversion
Because both Fahrenheit and MediaPipe were taken from different angles of view, the acquired data were angle-transformed and the evaluations were aligned. In addition, considering the occlusion task of Fahrenheit, in which the DIP joint of each finger is hidden when the hand is maximally flexed, and the task of MediaPipe, in which there are no coordinate data for the metacarpals of each joint, the PIP joint of each finger was targeted for analysis. The Fahrenheit’s angular transformation method was the same as that used in previous studies [10]. For the Mediapipe, a function was programmed to acquire data. This function is used to calculate the angle of each joint of the body. The angles were calculated using analytic geometry. For example, there are three points, A (x, y1, z1), B (x2, y2, z2), and C (x3, y3, z3) (Figure 2). Consider A and C as a skeletal structure (two bones). The intersection of line segments A and C lies on point B. The angle between A and C can be found as follows
Find the inner product of AB and BC:
Find the norm (distance) of AB/BC:
Convert the cosine of the angle formed by・:
2.5.2. Smoothing Process
A low-pass filter (Butterworth 2nd order, cutoff 12 Hz) was used for the first processing of the angle-transformed data. This method is commonly used for marker-based motion capture data, and the optimal cutoff values have been reported [16]. Second, optimal ensemble Kalman smoothing was performed [17]. The ensemble Kalman involves a two-way pass to determine the optimal state estimation for a given keypoint trajectory. Hyperparameters, including measurement and transition noises, were optimized using a grid search and cross-validation (Figure 3).
2.5.3. Detection and Completion of Mis-Estimated Frames
Based on previous studies, misestimation of the coordinate data at frame i was detected by comparing the absolute value of the difference between the previous and subsequent frames [18]. The absolute value of the difference is defined as:
The mean value and standard deviation were calculated for dx, and the acquired xi values were considered as mis-estimated frames and excluded if any value exceeding the mean ± 3SD was detected. Each frame was then linearly interpolated, and spline smoothing was subsequently applied to obtain new data (Figure 4).
2.6. Statistical Analysis
2.6.1. DTW Distance
For the preprocessed data, the maximum flexion angle, maximum angular velocity, and average angular velocity were compared for each BRS phase. The DTW distance was calculated for each subject, and the degree of agreement was calculated using cross-correlation analysis.
DTW is a method for calculating the similarity between two time-series data with different phases [19]. DTW calculates the distance between each element of two time-series data on a round-robin basis and then maps the two time-series data to minimize the total distance (DTW distance) between the two time-series data. Even if the lengths of the two time-series data are different, a DTW correspondence is possible. The DTW distance D(A, B) of two time series data, A = {a1, a2, ..., aM} and B = {b1, b2, ..., bN}, is defined as follows:
D (𝐴, 𝐵) = 𝑑 (𝑀, 𝑁)
Let C be the distance function between two time series data and C(am) be the distance between element bn of one time series data and element bn of the other time series data, then d(m, n) is calculated recursively as follows:
The conditional equation for this case is as follows:
𝑑 (0, 0) = 0, 𝑑 (𝑚, 0) = 𝑑 (0, 𝑛) = ∞
1 ≤ 𝑚 ≤ 𝑀, 1 ≤ 𝑛 ≤ 𝑁, 𝑚, 𝑛 ∈ ℕ (2.4)
1 ≤ 𝑚 ≤ 𝑀, 1 ≤ 𝑛 ≤ 𝑁, 𝑚, 𝑛 ∈ ℕ (2.4)
A drawback of DTW is its vulnerability to noise. When noise occurs, the actual distance between elements that should correspond to each other may differ from the distance between elements that should correspond to each other, resulting in inaccurate correspondence. The Euclidean distance between two elements is often used as the distance function of DTW. In this case, DTW is robust to the expansion and contraction or shift of time-series data in the time direction but weak against the expansion and contraction or shift in the space direction. In other words, when two time-series data have the same trajectory but move in the same spatial direction, accurate correspondence is not possible [19]. An example of mapping using DTW is shown in Figure 5.
2.6.2. Cross-Correlation Analysis
Using Lin‘s cross-correlation coefficients (CCC) [20], we evaluated the criterion-related validity of Mediapipe and Fahrenheit. Fleiss proposed CCC limits that were used for agreement interpretation: very good (CCC>0.9), acceptable (0.71<CCC0.9), moderate(0.51<CCC<0.7), poor (0.31<CCC<0.5), or no agreement (CCC<0.31) [21].
3. Results
3.1. Subjects
Patients were classified into six groups according to disease severity per the BRS: stage I (2 patients), stage II (8 patients), stage III (6 patients), stage IV (6 patients), stage V (9 patients), and stage VI (9 patients) (Table 2).
3.2. Comparison of Corrections
False estimation frames were detected in three patients using MediaPipe and in nine patients using Fahrenheit. The variation in values in patients with BRS I and II without joint motion was considered noise, and the amount of noise for each patient was evaluated using the Mean Absolute Deviation (MAD). The average values for MediaPipe and Fahrenheit were 2.46 and 1.42, respectively. After smoothing and correction, the MAD improved to an average of 0.81 for MediaPipe and 0.02 for Fahrenheit (Table 3).
3.3. Comparison of the Results
The three therapists agreed upon the results of the BRS for all subjects on the day of the experiment. The histograms of the middle finger PIP recorded during the 10-s exercise period for each BRS are shown in Figure 6. The histograms show that the percentages of extension (approximately 0–20°) and flexion (approximately 80–100°) increased as the BRS increased, and the distribution became closer to bimodal. This trend was common for both MediaPipe and Fahrenheit (Figure 6). The maximum flexion angle of each finger increased with the BRS stage (Spearman's rank correlation coefficient; MediaPipe: r=0.723, p=0.002; Fahrenheit: r=0.691, p=0.04) (Table 4). The maximum angular velocity of each finger increased during the BRS phase (Spearman's rank correlation coefficient; MediaPipe: r=0. 784, p=0.0001; Fahrenheit: r=0.796, p=0.001) (Table 5). The mean angular velocity of each finger increased during the BRS phase (Spearman's rank correlation coefficient; MediaPipe: r=0.816, p<0.0001; Fahrenheit: r=0.832, p<0.001) (Table 5).
3.4. Comparison of Agreement between Measurements
The DTW distance between MediaPipe and Fahrenheit for each subject and the results of the cross-correlation analysis are shown as box plots for each BRS (Figure 7). The results showed a “moderate” or “better” correlation for all data, except for patients with BRS I and II (DTW=0.092–0.579, CCC=0.374–0.986). In particular, the middle and ring fingers exhibited a strong average correlation (DTW mean = 0.216, CCC=0.758). The data of the 10 patients with BRS I and II were highly variable (DTW =0.106–0.535, CCC = 0. 251–0. 963), and two patients showed a weak correlation (CCC<0. 3).
4. Discussion
This study verified the criterion-related validity of Mediapipe and Fahrenheit. For the data preprocessed by angle transformation and smoothing, the CCC results and DTW distance showed more than moderate correlations. The results for the peak angle and peak angular velocity were also in general agreement. In a previous study on the development of Fahrenheit, the peak angle and peak angular velocity indicated by the LMC were evaluated to distinguish the recovery state of the finger, and identifiers were created [10]. These identifiers were eventually developed into the Fahrenheit as an application for evaluating the recovery stage of paralysis. Based on the concordance of the measurements shown in this study, we believe that the transfer of the Fahrenheit functionality to MediaPipe, which can be used on smartphones and tablet devices, will enhance the effectiveness of hand-movement analysis in clinical practice. This motion analysis system integrated with a camera for capturing video images can analyze minute changes and movement patterns of the subject and will be a powerful tool for sharing practice goals between therapists and patients in evaluation and treatment.
Another advantage of moving from Fahrenheit to MediaPipe is that MediaPipe is a simple motion analysis system. In general, image processing methods, such as Mediapipe, have a wider effective distance for hand tracking than detection algorithms based on LMC [12,14]. Fahrenheit's data acquisition was limited by the installation position, subject's posture, and calibration [11]. The MediaPipe data were obtained from a video camera that was used to capture the hand motions from the start to the end of the hand motions during the Fahrenheit data acquisition. However, the position of the camera and the ratio of the hand on the image to that on the entire screen were not specified. The reason why the agreement of the index and little fingers was lower than that of the other fingers is considered to be that the index and little fingers were occluded by the other fingers and did not appear on the screen sufficiently. Even under these conditions, moderate or better agreement suggests the usefulness of MediaPipe.
In the analysis of the time-series data, some limitations of both Mediapipe and Fahrenheit were identified. One of the limitations of Mediapipe is its high noise levels. Because both Mediapipe and Fahrenheit use frame processing to detect hand motions, this limitation may be directly related to the high accuracy of MediaPipe. Although patients with BRS I and II are inherently incapable of voluntary hand movements, angle fluctuations were detected in both MediaPipe and Fahrenheit. The MAD of variation was 2.46 for MediaPipe and 1.42 for Fahrenheit. In other words, the raw data for MediaPipe showed variability within 2.4° on average of the mean value. After preprocessing, based on a previous study, the MAD improved to an average of 0.81 for MediaPipe and 0.02 for Fahrenheit. Fahrenheit eliminated most angle fluctuations, whereas those of MediaPipe remained. These factors can be attributed to problems with the detection algorithm and its accuracy. The frame processing in both Mediapipe and Fahrenheit does not retain the time-axis information of the previous and subsequent frames; therefore, the detected hand position deviates from the previous and subsequent frames, which results in noise. Previous studies have also shown that the accuracy can be improved by improving the ratio of the hand to the entire screen and resolution [15,22]. Although this is not a simple comparison of accuracy because the results have not been compared under the conditions that optimize the performance of the two methods, it should be considered that there is a need to set measurement conditions for MediaPipe as well and that data processing after the measurement alone is not sufficient. This problem may be solved using a machine learning method such as Recurrent neural network, which is also used for processing time-series data, and by incorporating an algorithm that preserves information on the time axis before and after measurement.
One limitation of Fahrenheit is the large number of dropped frames. The breakdown of the subjects for whom false-estimated frames were detected was five patients with BRS I and II, two patients with BRS III, one patient with BRS V, and one patient with BRS VI. The low body surface temperature of the subjects may have influenced the high number of dropped frames detected at lower motion speeds. The infrared sensor also provides quantitative information by measuring the difference in temperature between the fingers and back of the hand. Patients with BRS I and II who have difficulty with voluntary movements tend to have weaker muscle contractions and lower body surface temperatures [23]. Limitations of infrared sensors in patients with severe peripheral edema have also been reported [24]. The detectable range of LMC is -30°C to 60°C [25], but it is possible that the difference in body surface temperature affected the accuracy of detection. In addition, stroke patients without joint motion are prone to peripheral edema in the acute phase [26], which may also have affected the misestimation. In other words, MediaPipe could not completely eliminate the noise due to a drop in accuracy, and Fahrenheit showed many false estimations in patients with BRS I and II, which may have affected the variability of data in patients with BRS I and II (DTW =0.106-0.535, CCC = 0.251-0.963 ).
It is difficult to discriminate the hand movements of patients with BRS I and II who are unable to perform voluntary movements using image analysis. To process the severity of paralysis, identified by the presence or absence of muscle contractions, using a machine, it is necessary to use electromyogram data.
This study compared the measurement agreement and performance of the Mediapipe and Fahrenheit according to a patient's recovery stage.
5. Conclusions
The results showed a moderate-to-high correlation, indicating the possibility of transferring the functionality of Fahrenheit to MediaPipe, which can be used on smartphones and tablets. Fahrenheit’s weakness, which causes instability in the joint center estimation when a hand grasps an object (occlusion problem), can be solved by image processing using AI. Mediapipe has an Objectron library that can detect objects [12]. By developing an application that can run the MediaPipe hands and MediaPipe Objectron, it is possible to obtain the positional information of the object and hand simultaneously. This enables an accurate evaluation of human tool manipulation based on the positional relationship with an object, even when the hand is occluded. The beginning of Form Conventional motion captures only human motion. The development of an application that can simultaneously track the motion of a human and that of an object generated by human motion can revolutionize the world of motion capture. The next task of our research team is to develop such an application and verify its performance in tracking hand motions with an object.
Author Contributions
“Conceptualization, R.S. and T.H.; methodology, R.S.; software, R.S.; validation, R.S., T.H. and T.S.; formal analysis, R.S.; investigation, R.S.; resources, R.S.; data curation, R.S.; writing—original draft preparation, R.S.; writing—review and editing, R.S.; visualization, R.S.; supervision, T.H.; project administration, T.H.; funding acquisition, T.S. All authors have read and agreed to the published version of the manuscript.”
Funding
This project was supported by the Saitama Prefectural University (SPU) Grant (15001) and JSPS KAKENHI (C) (21K11220).
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Saitama Prefectural University (approval No. 27083) and the Independent Ethics Committee of Tokyo Dental College Ichikawa General Hospital (I15-71).
Data Availability Statement
Study data will be provided upon request from the corresponding authors.
Acknowledgments
The authors would like to thank Masateru Katayama, Hiraku Hotta, Shin Doumae, Sasympti Shibui, and Asympti Enami, Department of Neurosurgery and Rehabilitation at Tokyo Dental College Ichikawa General Hospital, for their contributions and operational approval to conduct this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kivell, T.L.; Baraki, N.; Lockwood, V.; Williams-Hatala, E.M.; Wood, B.A. Form, Function and Evolution of the Human Hand. Am. J. Biol. Anthropol. 2023, 181 (Suppl. 76), 6–57. [Google Scholar] [CrossRef]
- Ji, Q.; Luo, Z.-X.; Yuan, C.-X.; Wible, J.R.; Zhang, J.-P.; Georgi, J.A. The Earliest Known Eutherian Mammal. Nature 2002, 416, 816–822. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. 2011. Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke Rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, H.; Jørgensen, H.S.; Raaschou, H.O.; Olsen, T.S. Recovery of Upper Extremity Function in Stroke Patients: The Copenhagen Stroke Study. Arch. Phys. Med. Rehabil. 1994, 75, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Norouzi-Gheidari, N.; Archambault, P.S.; Fung, J. Effects of Robot-Assisted Therapy on Stroke Rehabilitation in Upper Limbs: Systematic Review and Meta-analysis of the Literature. In, J. Rehabil. Res. Dev. 2012, 49, 479–496. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.H.; Hsiao, S.F.; Chang, C.M.; Huang, M.H.; Liu, C.K.; Lin, Y.T. Factors Influencing Functional Independence Outcome in Stroke Patients After Rehabilitation. Kaohsiung J. Med. Sci. 2000, 16, 351–359. [Google Scholar] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post Stroke Hemiplegic Patient. I. A Method for Evaluation of Physical Performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef]
- Lrvine, R.E. Movement Therapy in Hemiplegia: A Neurophysiological Approach. Gerontologist 1972, 12, 205–208. [Google Scholar] [CrossRef]
- Liu, M.; Chino, N.; Tuji, T.; Masakado, Y.; Hase, K.; Kimura, A. Psychometric Properties of the Stroke Impairment Assessment Set (SIAS). Neurorehab. Neural Repair 2002, 16, 339–351. [Google Scholar] [CrossRef]
- Hamaguchi, T.; Saito, T.; Suzuki, M.; Ishioka, T.; Tomisawa, Y.; Nakaya, N.; Abo, M. Support Vector Machine-Based Classifier for the Assessment of Finger Movement of Stroke Patients Undergoing Rehabilitation. J. Med. Biol. Eng. 2020, 40, 91–100. [Google Scholar] [CrossRef]
- Saito, T.; Ishioka, T.; Yoshimura, S.; Hamaguchi, T. Predictive Ability of Fahrenheit, a Hand Motion Recording System for Assessing Hand Motor Function in Patients with Hemiplegia Post-cerebrovascular Disease—A Pilot Study. Appl. Sci. 2021, 11. [Google Scholar] [CrossRef]
- 12. Google. Mediapipe. Github.
- Asta, A.K.A.A.A.; Yuniarno, E.M.; Nugroho, S.M.S.; Avian, C. Handwriting Classification Based on Hand Movement Using ConvLSTM. Proceeding International Seminar on Intelligent Technology and Its Applications: Leveraging Intelligent Systems to Achieve. Sustainable Development Goals, ISITIA 2023; Vol. 2023, 2023. [CrossRef]
- Christian, S.-C.; Dan, G.; Alexandra, F.; Adela, P.P.; Ovidiu, S.; Honoriu, V.; Liviu, M. Hand Gesture Recognition and Infrared Information System. Inf. Syst. 23rd International Carpathian Control. Conference, ICCC 2022; Vol. 2022, 2022. [CrossRef]
- Bazarevsky, V.; Zhang, F. On-Device, Real-Time Hand Tracking with MediaPipe. In Google AI Blog, 2019.
- Challis, J.H. A Procedure for the Automatic Determination of Filter Cutoff Frequency for the Processing of Biomechanical Data. J. Appl. Biomech. 1999, 15, 303–317. [Google Scholar] [CrossRef]
- Rauch, H.E.; Tung, F.; Striebel, C.T. Maximum Likelihood Estimates of Linear Dynamic Systems. AIAA J. 1965, 3, 1445–1450. [Google Scholar] [CrossRef]
- Sugiyama, Y.; Uno, K.; Matsui, Y. Types of Anomalies in Two-Dimensional Videobased Gait Analysis in Uncontrolled Environments. PLOS Comp. Biol. 2023, 19, e1009989. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, K.; Yamada, Y.; Suzuki, E. Fast Clustering for Time-Series Data with Average-Time-Sequence-Vector Generation Based on Dynamic Time Warping. Trans. Jpn. Soc. Artif. Intell. 2003, 18, 144–152. [Google Scholar] [CrossRef]
- Lin, L.I.-K. A Concordance Correlation Coefficient to Evaluate Reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Hills, M.; Fleiss, J.L. The Design and Analysis of Clinical Experiments. J. R. Stat. Soc. A (Gen.) 1987, 150. [Google Scholar] [CrossRef]
- Dill, S.; Rösch, A.; Rohr, M.; Güney, G.; De Witte, L.; Schwartz, E.; Hoog Antink, C. Accuracy Evaluation of 3D Pose Estimation with MediaPipe Pose for Physical Exercises. Curr. Dir. Biomed. Eng. 2023, 9, 563–566. [Google Scholar] [CrossRef]
- Alfieri, F.M.; Massaro, A.R.; Filippo, T.R.; Portes, L.A.; Battistella, L.R. Evaluation of Body Temperature in Individuals with Stroke. NeuroRehabilitation 2017, 40, 119–128. [Google Scholar] [CrossRef]
- Anderson, M.E.; Moore, T.L.; Lunt, M.; Herrick, A.L. The “Distal-Dorsal Difference”: A Thermographic Parameter by Which to Differentiate Between Primary and Secondary Raynaud’s Phenomenon. Rheumatology (Oxford) 2007, 46, 533–538. [Google Scholar] [CrossRef]
- Ultraleap. Tracking | Leap Motion Controller | Ultraleap. In Ultraleap, 2019.
- Giang, T.A.; Ong, A.W.G.; Krishnamurthy, K.; Fong, K.N.K. Rehabilitation Interventions for Poststroke Hand Oedema: A Systematic Review. In Hong Kong J. Occup. Ther. 2016, 27, 7–17. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Fahrenheit and MediaPipe measurement method. (a) Patient position during measurement. (b) Virtual hand motion displayed in real time. Vertical axis indicates the numerical value of finger movement, and horizontal axis indicates the time of measurement. (c) Keypoint detection method of Mediapipe for video data. The video is cut out at 30 frames per second, the keypoints are detected, and the successive images are merged into a video.
Figure 1.
Fahrenheit and MediaPipe measurement method. (a) Patient position during measurement. (b) Virtual hand motion displayed in real time. Vertical axis indicates the numerical value of finger movement, and horizontal axis indicates the time of measurement. (c) Keypoint detection method of Mediapipe for video data. The video is cut out at 30 frames per second, the keypoints are detected, and the successive images are merged into a video.
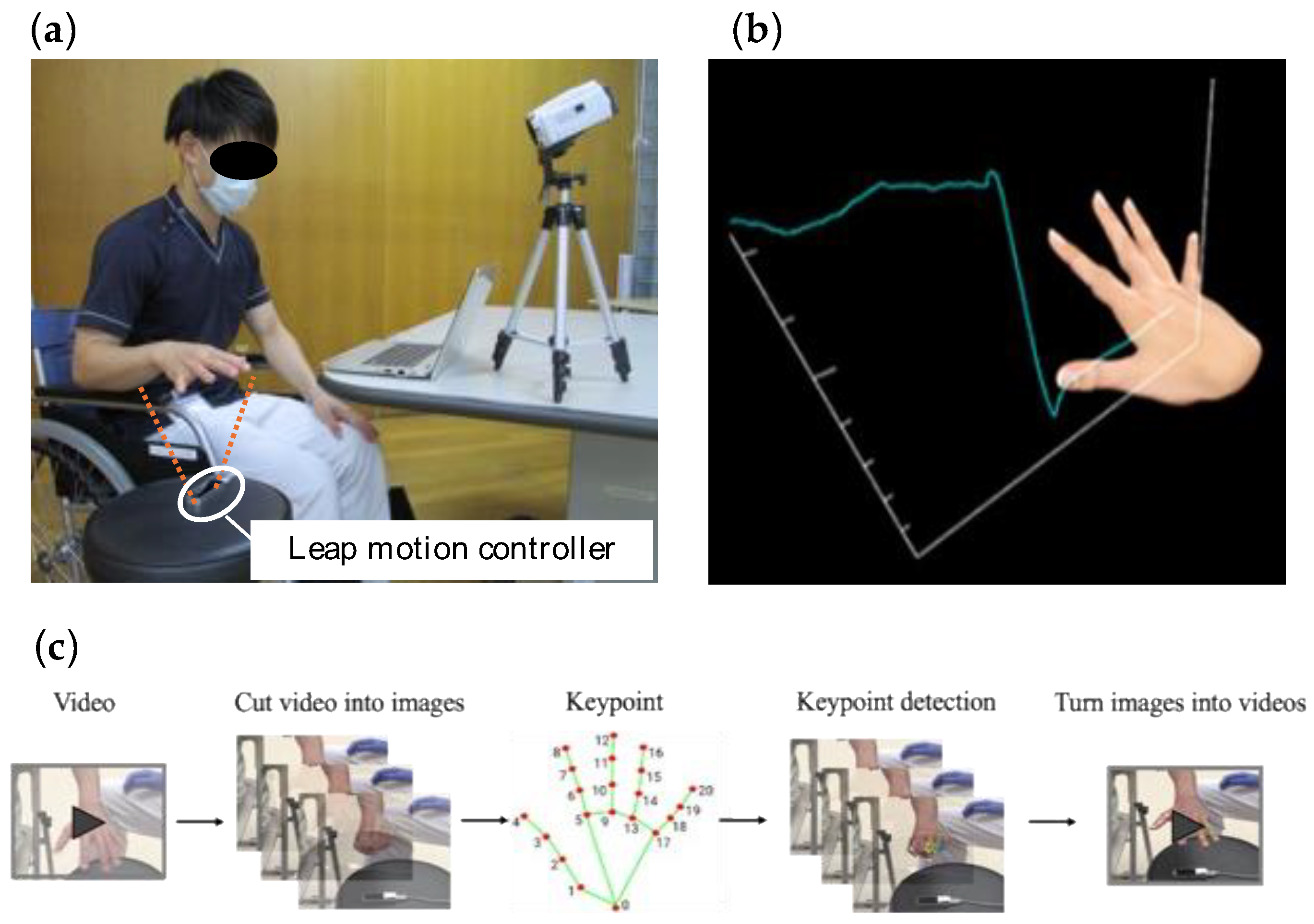
Figure 2.
Method of angle conversion. (a) Calculation method of joint angles. (b) An example of the obtained motion trajectory. The blue and red lines in the plots show the motion trajectories of Fahrenheit and MediaPipe, respectively. The horizontal and vertical axes represent time and joint angle, respectively.
Figure 2.
Method of angle conversion. (a) Calculation method of joint angles. (b) An example of the obtained motion trajectory. The blue and red lines in the plots show the motion trajectories of Fahrenheit and MediaPipe, respectively. The horizontal and vertical axes represent time and joint angle, respectively.
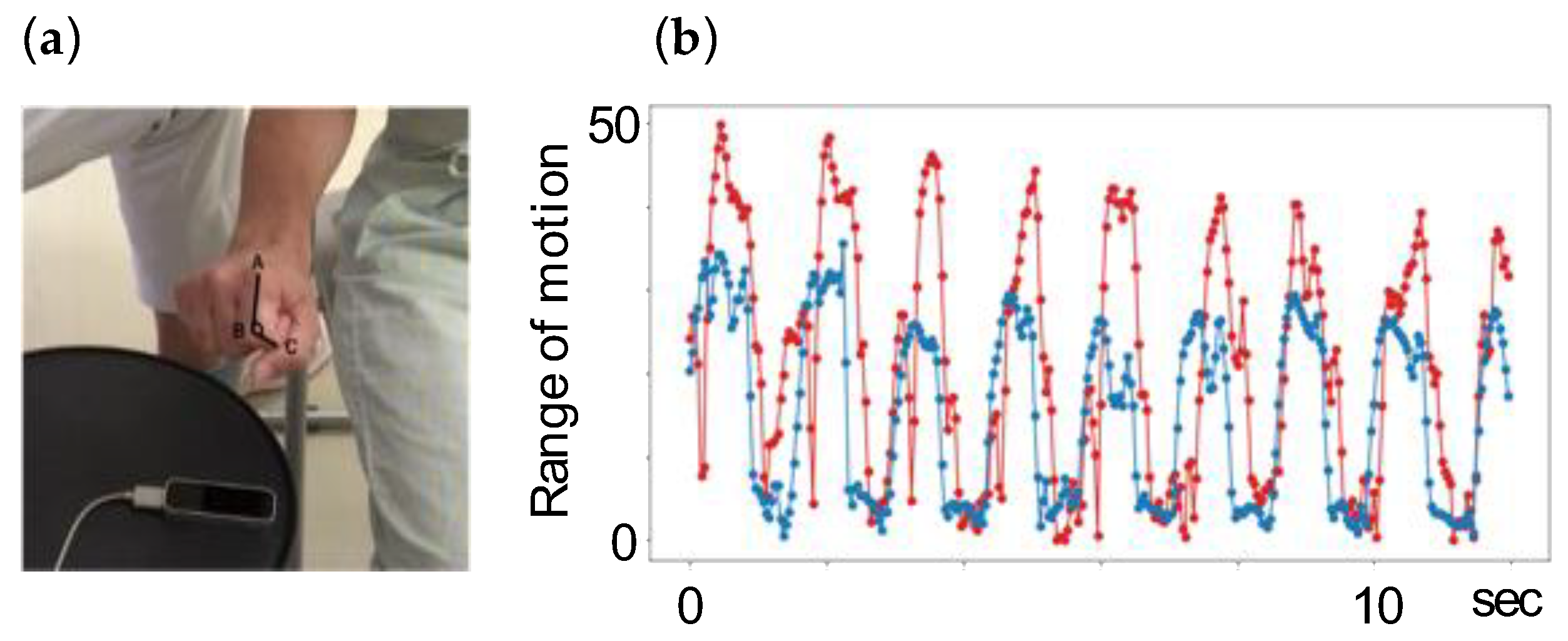
Figure 3.
Smoothing of kinematics data obtained by MediaPipe and Fahrenheit. (a) Raw data. (b) Data after smoothing. Blue and red plots indicate the motion trajectories of Fahrenheit and MediaPipe, respectively.
Figure 3.
Smoothing of kinematics data obtained by MediaPipe and Fahrenheit. (a) Raw data. (b) Data after smoothing. Blue and red plots indicate the motion trajectories of Fahrenheit and MediaPipe, respectively.
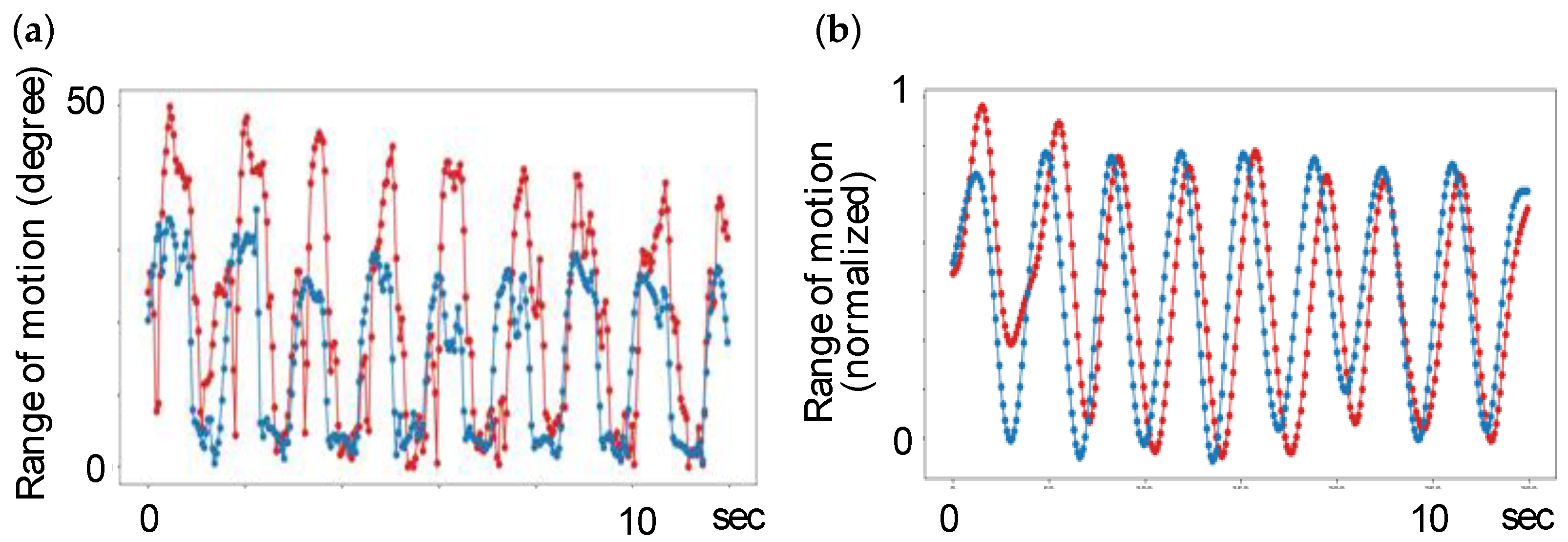
Figure 4.
Detection and completion of mis-estimated frames and completion method. (a) The absolute difference dx in the mother finger PIP. Values exceeding the mean ± 3SD are detected in the area circled in red. (b) The time frames. (c) Implementation of spline smoothing, excluding the mis-estimated frames. (d) Excluded frames.
Figure 4.
Detection and completion of mis-estimated frames and completion method. (a) The absolute difference dx in the mother finger PIP. Values exceeding the mean ± 3SD are detected in the area circled in red. (b) The time frames. (c) Implementation of spline smoothing, excluding the mis-estimated frames. (d) Excluded frames.
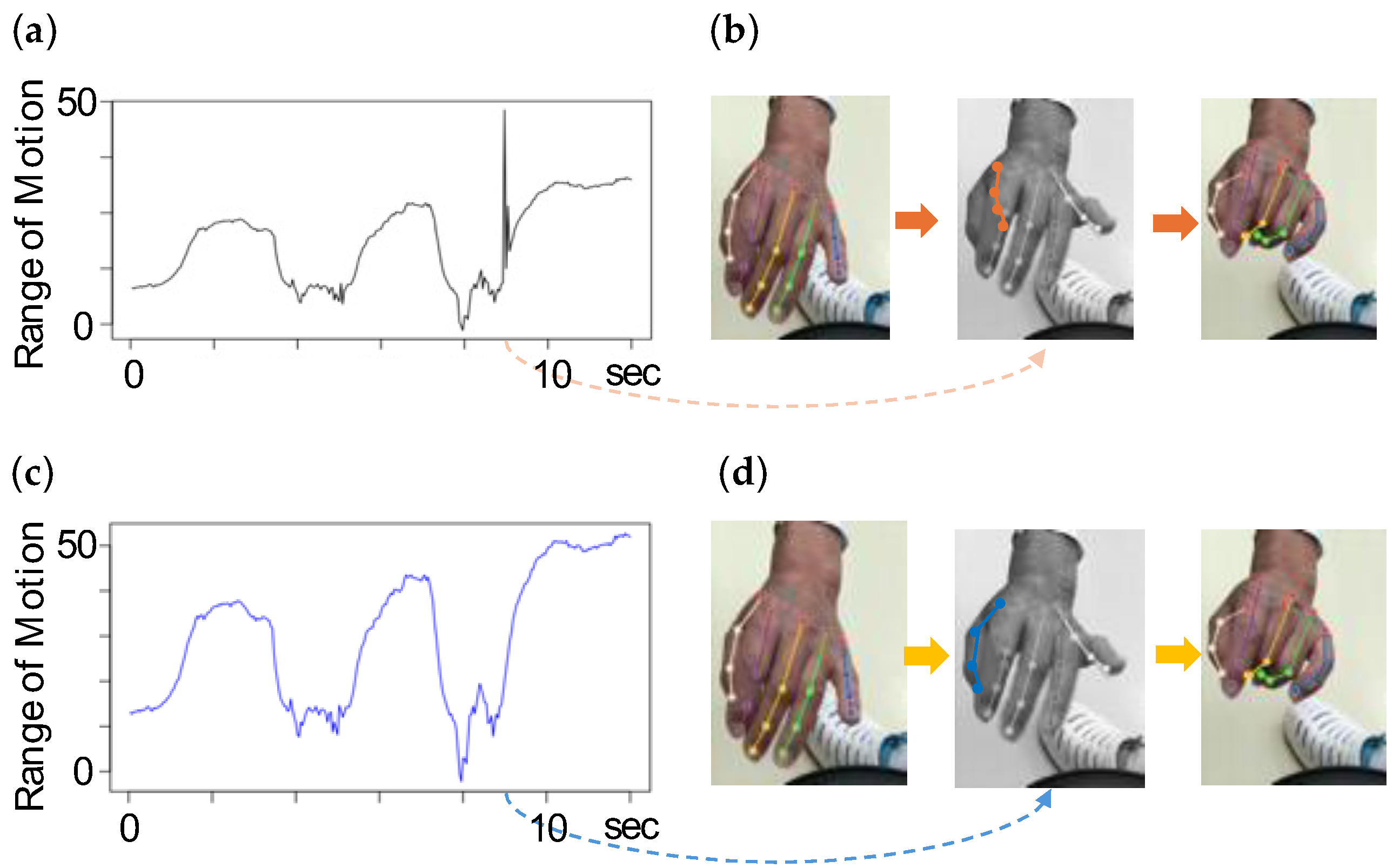
Figure 5.
Dynamic Time Warping (DTW) distance calculation. Blue and red indicate the motion trajectories of Fahrenheit and Mediapipe, respectively. The line connecting them indicates the DTW distance.
Figure 5.
Dynamic Time Warping (DTW) distance calculation. Blue and red indicate the motion trajectories of Fahrenheit and Mediapipe, respectively. The line connecting them indicates the DTW distance.
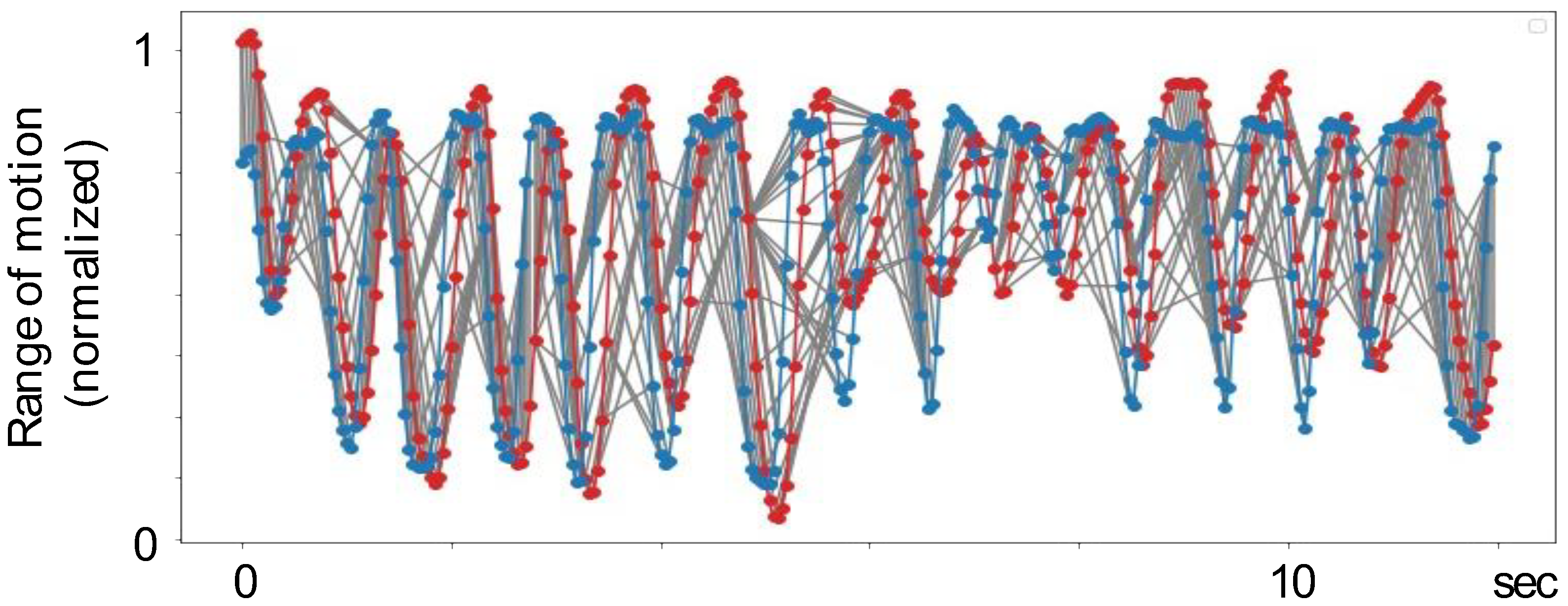
Figure 6.
Histograms for each Brunnstrom Recovery Stage (BRS) phase. The x-axis indicates the observed range of motion (ROM), divided into intervals of 2° each. The y-axis indicates the number of data observed in the interval. Each histogram includes the data of all the subjects divided into BRS phases.
Figure 6.
Histograms for each Brunnstrom Recovery Stage (BRS) phase. The x-axis indicates the observed range of motion (ROM), divided into intervals of 2° each. The y-axis indicates the number of data observed in the interval. Each histogram includes the data of all the subjects divided into BRS phases.
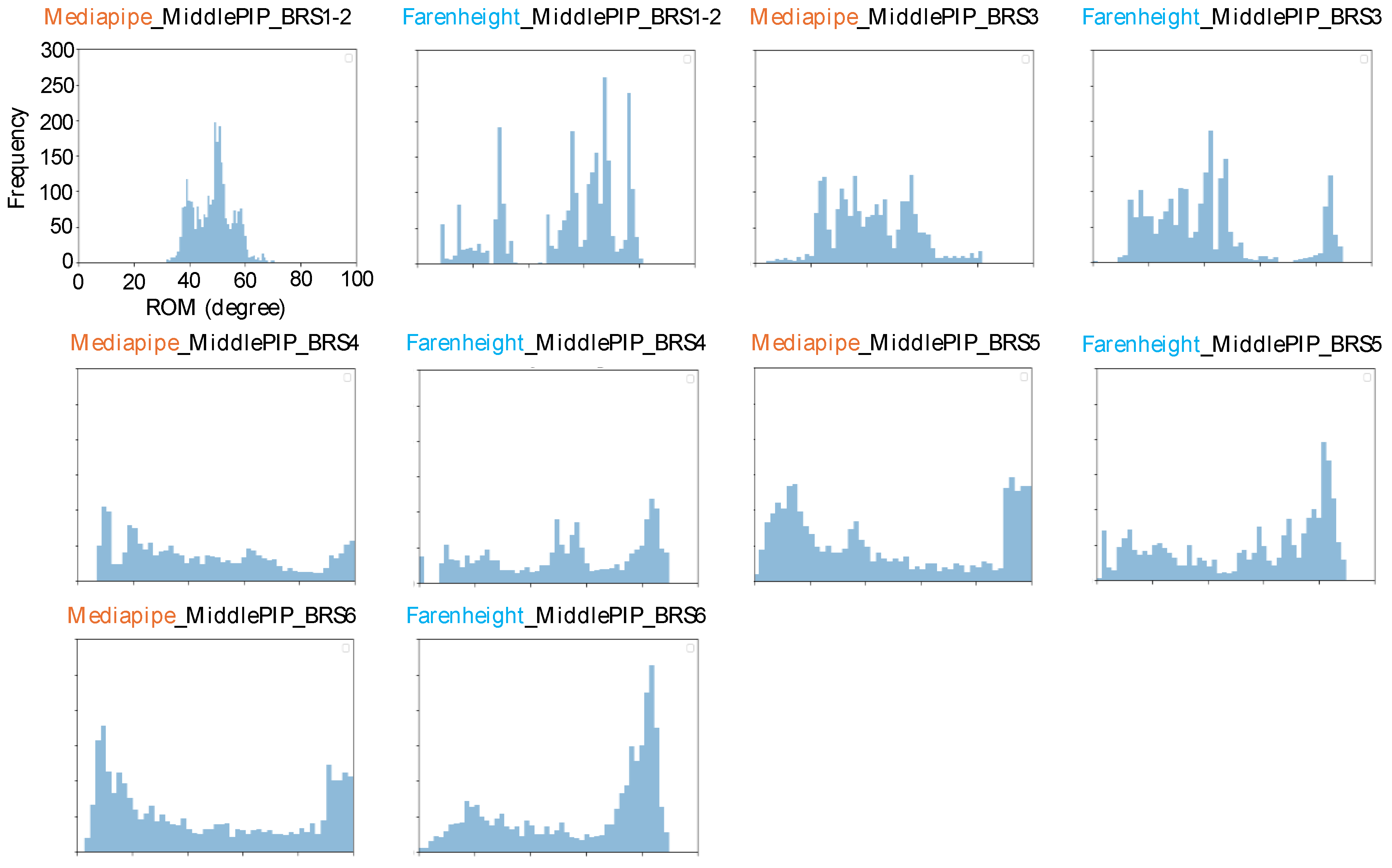
Figure 7.
Comparison of the agreement of the measurements. Dynamic Time Warping (DTW) distance between MediaPipe and Farenhight for each subject is shown on the left, and cross-correlation analysis is shown on the right for each Brunnstrom Recovery Stage (BRS). The bottom line of the error bar indicates the minimum value, the center line indicates the median value, the × mark indicates the mean value, and the top line indicates the maximum value. Boxes indicate interquartile ranges.
Figure 7.
Comparison of the agreement of the measurements. Dynamic Time Warping (DTW) distance between MediaPipe and Farenhight for each subject is shown on the left, and cross-correlation analysis is shown on the right for each Brunnstrom Recovery Stage (BRS). The bottom line of the error bar indicates the minimum value, the center line indicates the median value, the × mark indicates the mean value, and the top line indicates the maximum value. Boxes indicate interquartile ranges.
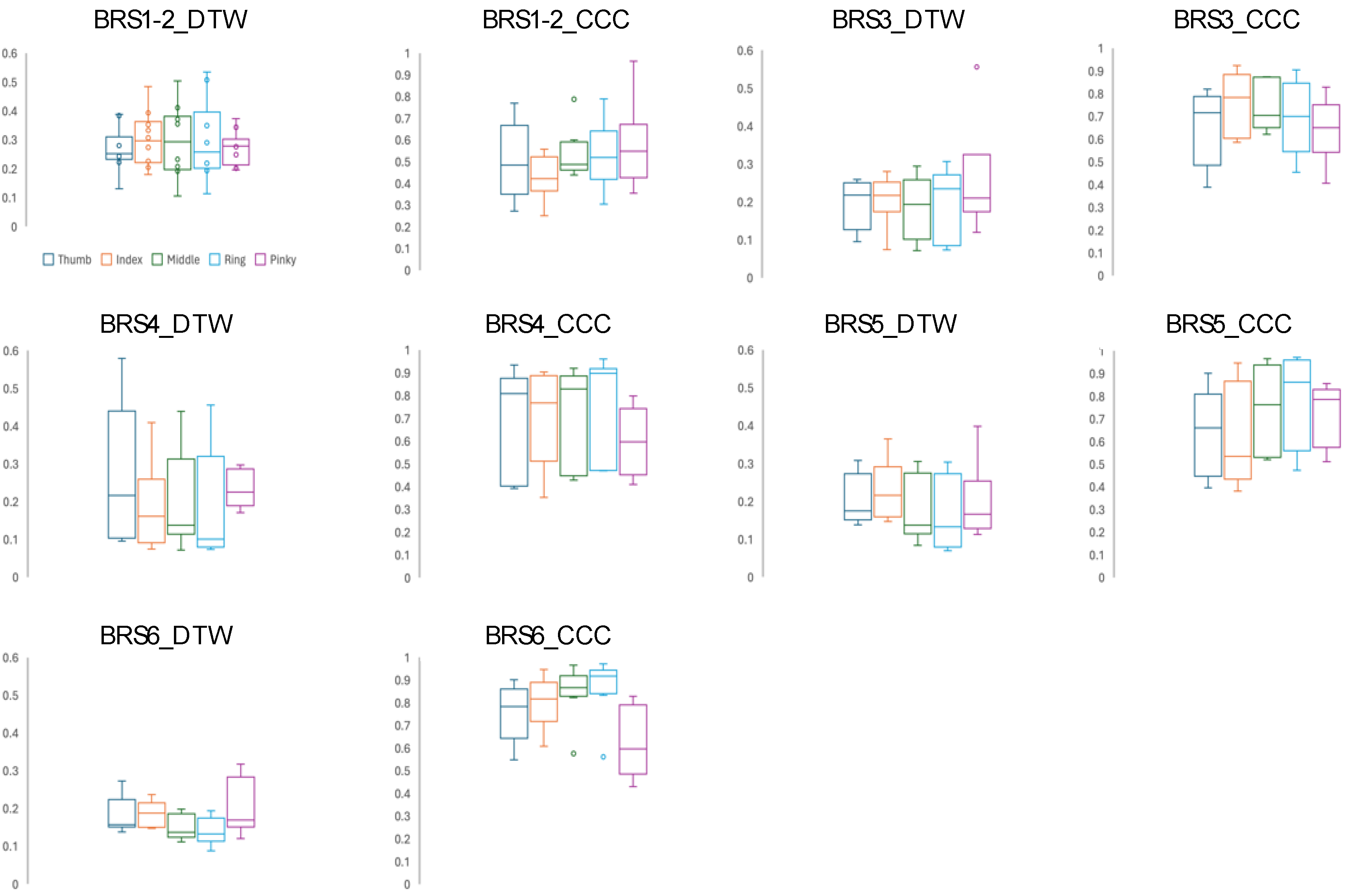

Table 1.
Comparison of basic performance.
| MediaPipe | Fahrenheit | |
|---|---|---|
| frame rate | 30 | 60*detune to 30 |
| number of joint landmarks | 21 | 24 |
| Observable joint range of motion | 180 | 90 |
Values are expressed as real numbers. * Fahrenheit was downsampled and analyzed at 30 fps.
Table 2.
Demographic data of the subjects.
| Attribute | Classification | Values |
|---|---|---|
| Age | 71 ± 11 | |
| Gender | Male/Female | 30 / 10 |
| Paralyzed side | Right/Left | 23 / 17 |
| day of a patient's illness | 13.5 ± 14.8 | |
| Diagnosis | Cerebral hemorrhage/cerebral infarction | 9 / 31 |
| Brunnstrom stage (Finger) | Ⅰ/Ⅱ/Ⅲ/Ⅳ/Ⅴ/Ⅵ | 2 / 8 / 6 / 6 / 9 / 9 |
Categorical data are presented as real values, and numerical data are presented as mean ± standard deviation.
Table 3.
Comparison of corrections.
| Mediapipe | Fahrenheit | |
|---|---|---|
| Subjects with mis-estimated frames detected | 3 / 40 | 9 / 40 |
| MAD of raw data | 2.46 ± 0.87 | 1.42 ± 0.46 |
| MAD after preprocessing | 0.81 ± 0.32 | 0.02 ± 0.01 |
Categorical data are presented as real values, and numerical data are presented as mean ± standard deviation.
Table 4.
Maximum flexion angle.
| Peak_flexion (deg) | BRSⅠ–Ⅱ (n=10) | BRSⅢ (n=6) | BRSⅣ (n=6) | BRSⅤ (n=9) | BRSⅥ (n=9) |
|---|---|---|---|---|---|
|
MediaPipe Thumb Index Middle Ring Pinky |
35.1 ± 14.4 54.5 ± 15.6 52.8 ± 9.4 60.8 ± 8.8 52.8 ± 10.2 |
34.9 ± 14.5 45.5 ± 26.6 56.0 ± 20.6 60.7 ± 18.2 59.9 ± 21.2 |
55.6 ± 16.3 75.9 ± 25.9 87.6 ± 11.3 91.5 ± 7.2 68.5 ± 15.7 |
41.3 ± 12.6 93.5 ± 10.7 99.5 ± 0.6 99.5 ± 1.1 98.9 ± 1.3 |
42.3 ± 8.1 99.2 ± 0.8 98.6 ± 3.2 99.4 ± 1.1 97.4 ± 6.0 |
|
Fahrenheit Thumb Index Middle Ring Pinky |
53.3 ± 24.0 60.1 ± 19.4 60.5 ± 18.1 59.7 ± 17.7 18.2 ± 11.6 |
52.1 ± 22.0 52.9 ± 22.4 51.6 ± 20.6 51.3 ± 21.0 14.2 ± 22.2 |
68.3 ± 17.7 73.6 ± 20.0 73.3 ± 20.9 72.4 ± 19.7 37.8 ± 15.7 |
31.5 ± 6.0 86.4 ± 3.1 87.1 ± 2.6 86.8 ± 3.1 87.2 ± 2.3 |
40.2 ± 15.4 89.1 ± 1.3 88.1 ± 2.2 88.0 ± 2.5 88.1 ± 2.7 |
Values are presented as mean ± standard deviation.
Table 5.
Comparison of angular velocities.
| Peak_velocity / Average_velocity (deg/s) | BRSⅠ–Ⅱ (n=10) |
BRSⅢ (n=6) |
BRSⅣ (n=6) |
BRSⅤ (n=9) |
BRSⅥ (n=9) |
|---|---|---|---|---|---|
|
MediaPipe Thumb Index Middle Ring Pinky |
87.9 / 6.2 82.6 / 9.8 61.1 / 9.7 58.5 / 9.4 104.2 / 9.6 |
111.2 / 14.7 236.1 / 29.7 240.0 / 26.8 256.2 / 27.6 187.8 / 25.8 |
274.7 / 55.3 505.0 / 101.6 544.8 / 108.6 573.6 / 110.6 574.8 / 96.6 |
667.6 / 110.1 1296.6 / 231.1 1309.0 / 239.9 1233.8 / 227.6 1198.8 / 177.8 |
780.8 / 186.9 1400.5 / 365.9 1425.9 / 380.4 1392.0 / 365.5 1231.8 / 282.3 |
|
Fahrenheit Thumb Index Middle Ring Pinky |
43.7 / 7.9 72.7 / 12.3 69.2 / 13.2 77.5 / 14.9 79.9 / 13.3 |
126.0 / 10.8 214.0 / 28.3 225.8 / 27.0 216.8 / 24.7 165.7 / 22.5 |
167.9 / 49.6 506.4 / 114.2 501.6 / 102.6 587.2 / 100.2 501.6 / 74.4 |
271.7 / 99.4 1295.8 / 214.7 1240.1 / 217.7 1300.6 / 200.2 1225.1 / 205.3 |
672.0 / 207.5 1412.8 / 355.7 1448.2 / 373.8 1403.1 / 351.1 1208.5 / 345.7 |
Each cell shows the maximum or average angular velocity. Values are shown as mean ± standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



