
Submitted:
29 May 2024
Posted:
30 May 2024
You are already at the latest version
Abstract
Respiratory Syncytial Virus (RSV) continues to pose a significant challenge, contributing to elevated hospitalization rates among children up to 5 years old, with a disproportionate burden on newborn and infants under 6 months old. The unique characteristics of the young immune system make it prone to altered responses to infections and vaccinations, requiring a tailored approach to disease prevention. The recent approval of the maternal RSV vaccine, (brand name ABRYSVO), represents a pivotal advancement in preventive strategies among newborns and infants, marking a milestone in RSV research as the first market-approved maternal vaccine. The present review examines clinical trial data on both recent and previous vaccine candidates, as well as the licensed vaccine, focusing on the prevention of RSV disease in newborns and young infants through the passive acquisition of antibodies following maternal immunization. Additionally, it evaluates the safety profile of these vaccines.
Keywords:
infant immunity
; maternal antibody transfer
; respiratory syncytial virus
; maternal immunization
; RSV vaccine
; clinical trial
; safety
; immunogenicity
1. Introduction
Infections exhibit a notably higher prevalence within the neonatal population compared to other age demographics. Based on data from the World Health Organization (WHO), it is reported that more than 550,000 infections per year result in fatal outcomes affecting primarily the low and middle income countries (LMICs) [1].
Respiratory syncytial virus (RSV) substantially impacts morbidity and mortality especially in early childhood. Following a brief period of decline in reported cases during the COVID-19 pandemic, there was a notable increase in the incidence of severe RSV-disease [2]. According to the CDC the seasonality pattern has altered with a tendency towards the spring and summer months after the pandemic, estimating the hospitalized patients until 5 years of age in the United States (U.S.) at a range number of 58,000-80,000 yearly [3]. According to a multicenter analysis including data extracted from 6 European countries the annual hospitalization rate for RSV-associated cases exceeds 4% for neonates and infants up to 2 months old, whereas it ranges from approximately 0.1% to 1% for children aged 1 to 2 years old [4]. Interestingly, approximately half of hospital admissions and deaths in the hospital environment due to RSV infection of the lower respiratory tract affect the newborns and infants up to 6 months of age [5]. In neonates, RSV infection can result in severe disease, necessitating mechanical ventilation hospitalization in the Neonatal Intensive Care Unit (NICU) [6].
Immunity in young children exhibits unique specificities compared to adult immune responses, necessitating a targeted approach to disease prevention in this sensitive age group. Immediate postpartum active immunization significantly protects the newborns from serious diseases, including the Hepatitis B vaccine and the Bacillus Calmette-Guerine (BCG) vaccine [7]. However, the immunity induction requires time and possibly several doses of the vaccine to reach the desired immunity response [7]. Another strategy of providing protection to this age group is maternal immunization during pregnancy [7]. This approach offers a dual benefit, as both the mother and the newborn can acquire immunity against the disease, facilitating birth conditions and the perinatal period [7]. IgG antibodies originating from maternal immunization during pregnancy, pass transplacentally to the fetus, conferring efficient protection [8]. Antibodies provided from the mother are detectable for up to 6-12 months [9]. Concomitantly, evidence suggests that the presence of maternally acquired antibodies may diminish the B cell-induced immunity of the newborn through interventions at various stages of the immune response [9]. The CDC recommends protective vaccination against pertussis (Tdap vaccine), influenza and COVID-19 in the period of pregnancy [10]. Recently, prevention of RSV has become available in this vulnerable age group, following the market authorization of a maternal RSV vaccine. ABRYSVO is the only market authorized vaccine from both the FDA and the EMA for maternal administration during pregnancy targeting the protection of newborns and infants [11,12].
This review article focuses on the analysis of the maternal vaccination in the context of RSV vaccines. A comprehensive review of the clinical trials of the currently approved and actively developed vaccines, as well as the vaccine failures is provided. The analysis closely examines the outcomes related to preventing RSV disease in newborns and young infants, with a particular emphasis on the passive acquisition of antibodies following maternal immunization. Furthermore, it assesses the safety profile of these vaccines.
2. Materials and Methods
The search strategy involved extensive research of databases including the Cochrane Database, MEDLINE and EMBASE, as well as clinical trial registries, to encompass all previous and current vaccines developed as maternal RSV vaccine candidates. Only active immunization agents were included in the review, without limitations on publication date or language. The data was last updated on May 2, 2024. A narrative synthesis approach was employed to analyze the gathered data (Figure 1).
3. Results
Maternal vaccination for the prevention of infantile RSV disease is recently a key focus of research, given the availability of an approved vaccine. A comprehensive overview of current and previous clinical trials is presented in Table 1.
3.1. Abrysvo
Pfizer Inc. developed Abrysvo in order to induce specific immunity against the prefusion form of the F RSV structural protein. In August 2023, regulatory authorities, beginning with the FDA and followed by the EMA, provided a positive opinion for its marketing authorization as a maternal vaccine. The recommended window for vaccination during pregnancy extends from 32 to 36 weeks of gestation in order to achieve protection to the newborn and infant up to 6 months of age against RSV associated lower respiratory tract disease (LRTD) and severe manifestations of LRTD [17]. A phase I/II trial (NCT03529773) included, among other participants, healthy nonpregnant women and tested different dose levels, adjuvant use, and a co-administration with the seasonal inactivated influenza vaccine (SIIV) in the phase II. Notably, a greater increase in the geometric mean titers (GMTs) of neutralizing antibodies was observed in the female participants, particularly those with low antibody levels at baseline. Although a decrease was noted within a year, the levels remained 4-5 times higher compared to baseline, supporting the principle of maternal vaccination in the late second or third trimester for optimal peripartum protection. The high IgG1 titers observed are also promising, as they pass through the placenta [13]. Additionally, the administration of both RSV and influenza vaccines did not result in significant changes in the specified RSV immune responses. However, concerning influenza immunity, young adults in the study exhibited reduced responsiveness to the SIIV following coadministration [14]. A sub-study was conducted to attempt revaccination of some participants from the parent study one year after the initial vaccination. This sub-study successfully demonstrated the induction of immunogenicity following revaccination [32]. In the subsequent phase IIb study (NCT04071158), healthy nonpregnant women were recruited for a non-inferiority trial evaluating the RSV and tetanus, diphtheria, and acellular pertussis (Tdap) vaccine coadministration. According to the study results, the non-inferiority criteria regarding the antibody-induced immunity were met for the desired pathogens, except for immunity against pertussis. Coadministration did not yield similar immunogenicity results as the single Tdap administration for pertussis. These data further support the maternal vaccination concept against multiple pathogens [15]. Pregnant women between the 24th and 36th gestational week were vaccinated in the context of another phase IIb trial (NCT04032093) receiving two different dose levels and formulations, one with adjuvant and one without adjuvant. An interim analysis of the 6-month data provided evidence supporting the activation of immunity during pregnancy, eliciting maternal neutralizing antibody production and transmission to the infant. Based on a post hoc analysis, the acquired antibodies prevented infantile disease at high rates. Measurements in infants revealed higher antibody levels with the unadjuvanted formulation, which were not correlated with the gestational age spectrum during vaccination. Pregnancy, labor and delivery related adverse events, including preterm deliveries, exhibited a similar distribution between the placebo and vaccine groups. A rate of 3.7% of newborns were premature across all groups. Investigators noted that the majority of congenital anomalies were not attributed to the vaccination and were of mild severity [16]. Based on updated information provided in the vaccine’s package insert, preterm births were found to be unevenly distributed between the active and placebo groups, with rates of 5.3% and 2.6%, respectively [17]. A phase 2a RSV challenge study (NCT04785612) conducted in young adults, which included non-pregnant female participants, demonstrated effective protection against symptomatic manifestation of RSV infection following RSV challenge [18]. MATISSE (NCT04424316) is a phase III trial with a large number of participants. Pregnant women in low-risk pregnancies between 24 and 36 weeks of gestation were enrolled in the study. According to interim analysis, the vaccine effectively prevented RSV medically attended severe lower respiratory tract illness within the first 3 months after birth in infants at a rate of 81.8%. However, the corresponding efficacy rate for lower respiratory tract illness was 57.1%, failing to meet the statistical success criterion. The protection rate for severe disease within the first 6 months after birth exceeded 69%. The vaccine was proved safe for both pregnant women and their infants, while final data analysis is anticipated. Specifically, regarding the safety profile, preeclampsia occurred in 1.8% of the vaccinees compared to 1.4% among placebo recipients, with comparable rates for fetal distress syndrome. Premature delivery experienced 0.8% of the vaccine recipients and 0.6% of the placebo recipients, while stillbirth and spontaneous abortion were reported at even lower rates. The serious adverse events regarding pregnancy outcomes occurred in a comparable distribution between the groups [19]. As summarized in the vaccine’s package insert, the rate of recorded preterm births was 5.7% for the Abrysvo recipients and 4.7% for the participants of the control group [17]. Another phase III trial (NCT05096208), which also included female participants, proved the consistent safety and reactogenicity of three different lots of the vaccine [20]. MORISOT (NCT06325657) is a recently announced phase III clinical trial intending to investigate the effects of vaccinating pregnant women living with HIV and their infants. Eligible participants are female individuals being in their 24th to 36th week of pregnancy, demonstrating stable HIV disease status.
3.2. RSV MAT
The maternal vaccine candidate developed by GSK plc targeting the safe protein as Abrysvo, was deemed safe in the first-in-human clinical trial (NCT03674177) in nonpregnant women. Immunization data from this phase I trial supported the further evaluation of the vaccine during pregnancy [21]. In the phase II clinical trial (NCT04126213) the vaccine was evaluated during 28 to 33 weeks of pregnancy. An acceptable safety profile was demonstrated, with similar rates of adverse events observed between vaccine recipients and placebo recipients. Pregnancy and peripartum abnormalities including preterm labor, preterm birth or congenital anomalies were observed on a similar trend between the groups. While an increased reporting rate of hypertension and preeclampsia was noted in the active immunization group, it did not exceed the rates observed in the general pregnant population. Specific antibody titers were measured at elevated levels for both vaccinated mothers and their infants [22]. In a co-administration phase II study (NCT04138056), the safety and immunogenicity profile of Diphtheria-Tetanus-Pertussis co-vaccination with the RSV vaccine candidate was examined in non-pregnant women. The study found no evidence of interference between the vaccinations, and specific RSV antibody reactions remained evident up to one to one and a half years postvaccination. However, interference was observed with the Diphtheria-Tetanus-Pertussis vaccination, with no clinical significancy for the diphtheria and tetanus antigens, and unknown clinical interpretation for the pertussis part of the vaccination [23]. The GRACE trial, a phase III clinical study (NCT04605159), was designed to evaluate the safety profile and efficacy rates of vaccination in pregnant individuals, while also investigating their infants. Regarding vaccine efficacy in protecting infants against medically assessed RSV-lower respiratory tract disease, the rates were found to be satisfactorily high. However, significant safety signals emerged, leading to the early discontinuation of the trial before enrolling the planned participants. Specifically, an association with increased possibilities of preterm birth was observed, with a rate of 6.8% for the infants of vaccinated mothers compared to 4.9% in the placebo group [29]. Consequently, another phase III clinical study (NCT04980391) in high-risk pregnancies was prematurely discontinued, and a re-vaccination trial (NCT05229068) involving previously vaccinated individuals from earlier trials was withdrawn. Additionally, the phase III (NCT05169905) clinical trial in non-pregnant girls and females included only 9 participants due to the decision to terminate the study. Concurrently, another already ongoing phase III trial (NCT05045144) enrolled non-pregnant women for testing different lots and evaluating co-administration with influenza vaccine in this population. Recently, the company initiated a safety-focused phase IIIb clinical trial (NCT05705440) without any intervention. This open label trial involves the follow-up of participants from all previous trials monitoring safety parameters among participants from both the active and placebo groups. Previously, GSK had developed another vaccine candidate (GSK3003891A) based on the same protein, however, the formulation was found to be unstable, and this particular vaccination was not further pursued.
3.3. ResVax
A nanoparticle vaccine encoding the F RSV protein was developed by Novavax Inc. The vaccine candidate underwent testing in a phase I clinical trial (NCT01290419) in 2011, involving young male and female participants. The results from this trial supported further evaluation in phase 2 trials, as the vaccine demonstrated no association with toxicity and elicited an increase in specific antibody titers [24]. In the subsequent phase II studies (NCT01704365, NCT01960686), healthy women aged 18 to 35 years were enrolled to investigate the dose range and adjuvant addition. The trials yielded no safety concerns, and cases of RSV were less common after vaccination. Based on the results, the high antigen dose combined with the middle adjuvant dose was selected for further evaluation as a maternal vaccine [25,26]. Another phase II clinical trial (NCT02247726) enrolled pregnant women in the third-trimester with a follow-up period of one year for their infants. Vaccination provided protection against severe RSV disease for both the maternal participants and their infants, with no significant safety issues. Infants exhibited high levels of antibodies measured from cord blood, with an average half-life of 40 days [27]. In the phase III clinical trial (NCT02624947) of the vaccine a larger number of pregnant women between 28- and 36-weeks of gestation age participated. No serious safety signals were observed, with similarity noted between the groups in terms of low birth weight, small for dates, premature birth and intrauterine growth restriction. However, vaccine efficacy did not meet the prespecified criterion for RSV-specific medically-significant lower respiratory tract infection. Up to 3 months of age, the rate of vaccine efficacy for this primary outcome was 39.4%, while it increased to 58.8% for disease manifesting with severe hypoxemia in the same period. Notably, similar rates of vaccine efficacy were achieved for all-cause lower respiratory tract infection, including related hospitalizations and severe hypoxemia, which is an important finding. A higher incidence of protection against hospitalizations and severe cases in LMICs emerged from the data of this study. This noteworthy observation highlights the need for further investigation in subsequent vaccine studies, since the trial lacked the necessary statistical power to assess efficacy on a country-by-country basis [30]. The vaccine is no longer part of the company’s pipeline [33].
3.4. mRNA-1345
Utilizing mRNA vaccine technology and lipid-nanoparticles as a transport system, Moderna Inc. manufactured mRNA-1345 targeting the RSV F protein. In the phase I clinical trial (NCT04528719), the vaccine was administered to healthy young adults, including women, with promising outcomes for further development of the vaccine as a maternal candidate. Elevated levels of antibody titers were observed within a 6-month period after vaccination [28]. A subsequent phase II clinical trial (NCT06143046) is currently enrolling pregnant women between 28 to 36 weeks of gestation, with the intention of also following up their infants.
3.5. V-306
The V-306 vaccine candidate, developed by Virometix AG, has a particular vaccine target of an antigen epitope (FsIIm) of the RSV F protein. In the phase I clinical trial (NCT04519073), the vaccine candidate did not demonstrate the expected induction of neutralizing and IgG specific immunity. A possible development of V-306 presupposes vaccine formulation alterations [31].
4. Discussion
The anti-inflammatory tendency of neonatal immune reactivity is associated with an altered pathway of response to pathogens and immunizing agents [34]. The constituent elements of the neonatal and infantile immune system shape a distinct entity, diverging significantly from conventional perceptions of it as an immature form of the adult immune system. The newborn rapidly adapts to the extra-uterine conditions, confronting with a plethora of pathogens. Immunity serves the dual purpose of tolerating the development in the intra-uterine environment of the mother and limiting the pathogenic threats postpartum. Research demonstrates that responses during early infancy are predominantly mediated by Th2 and Th17 immunity, with the development of Th1 immunity occurring to a lesser extent [35]. Inflammation is primarily countered by the innate immunity mechanisms and consequently, infants are more susceptible to intracellular infections [35]. The neutrophilic activity is impaired in producing extracellular traps (NETs) and facilitating the attachment process to the endothelium [36]. Further factors impacting function include numerical insufficiency, along with diminished leucocyte activation upon chemotactic signaling [37]. The functionality of monocytes and macrophages in neonates closely resemble that of adults, albeit with distinct activation patterns [38]. Neonatal immunity tends to lean towards Th2 induction, explained by the reduced MHC-II expression [36]. While TLR receptors operate quantitatively similar to adult receptors, qualitative deficiencies, such as reduced expression of pro-inflammatory cytokines, are observed [39]. These characteristics along with the reduced adhesion ability and chemotactic activity collectively impact the function of the neonatal monocytes [36]. The NK cells in neonates exhibit a distinct phenotype compared to adult NK cells, characterized by lower adhesive capacity and pathogen-killing ability, attributed to reduced expression of certain cytokines [40,41]. Current evidence suggests that IL-15 stimulation effectively enhances and boosts NK cell function [40].
Early life T cells are basically naïve, identified as recent thymic emigrants (RTEs), contributing to an innate-like immune response through regulatory T cells (Tregs)[42]. The significance of Tregs lies in their ability to exert immunosuppressive activity against the maternal environment providing tolerance during pregnancy[43]. In infants, particularly when exposed to allergens and RSV, Th2 responses are triggered [44]. The development of this response appears to be influenced by exposure to pathogens [44]. B cell repertoire is also limited in early life, due to restricted cytokine signaling and attachment of antigens through maternal antibodies [45]. Multidose vaccine schedules administered to infants trigger IgG antibody induction, which typically persists for only 6-9 months [45]. This temporary immune response increases the likelihood of infections during this vulnerable age [45].
The recent licensure of maternal vaccine heralds a significant stride in the prevention of RSV among the vulnerable demographic of newborns and young infants. The United States Food and Drug Administration (FDA) set a narrower window between 32 and 36 weeks of gestation as maternal vaccination indication, while the European Medicines Agency (EMA) advocates for vaccination within the broader range of 24 and 36 weeks of gestation [12,46]. Preterm infants, particularly those born prematurely, are disproportionally affected by RSV-related illness, experiencing notably higher rates of hospitalization. These findings emphasize the need of potential immunization early during pregnancy [47]. The FDA mandated a specialized report on preterm births and hypertension during pregnancy using real-world data through the Vaccine Adverse Event Reporting System (VAERS) and established precise pharmacovigilance objectives for ABRYSVO. Detailed post-marketing pharmacovigilance trials are delineated by the FDA in order to ensure safety [48]. It is essential to highlight that, despite the lack of data concerning the frequency and complications of RSV infection during pregnancy, emerging evidence suggests a plausible association between RSV infection and preterm delivery [49]. Similarly, available data regarding influenza indicate a correlation with abortions, preterm births, and stillbirths [50]. Consequently, the systematic collection of data regarding peripartum outcomes subsequent to RSV infection during pregnancy holds the potential to modify the vaccination strategies.
Recently, Nirsevimab, which is a long-acting monoclonal antibody, was market-approved as an RSV passive immunization agent for the infants. Immunizing infants <8 months within their first RSV season and infants and children 8-19 months of age with high-risk factors for severe infection belong to the indications of Nirsevimab [51]. To date, there is no evidence to indicate that either of the two agents is more effective. However, simultaneous administration of both immune agents is not substantiated, except in specific rare cases where it is considered clinically useful [52]. Conducting studies to assess the effects of each medication under specific circumstances could facilitate the optimization of population benefits through an individualized clinical approach. A recent analysis funded by the National Institute for Health Research suggested that infants benefit from the use of either the long-acting monoclonal antibodies or maternal vaccination. An additional protective effect is also expected for pregnant individuals in the case of the maternal vaccination [53]. Modified immune responses occur during pregnancy increasing the mother’s susceptibility to severe manifestation of infections [54]. Fetal acquisition of maternal antibodies initiates around the 13th week of gestation and escalates after the 28th week, intending to protect the infant during the critical phase of immune system adaptation [55].
Prioritizing widespread access to maternal vaccination in LMICs is a high priority. Gavi, the Vaccine Alliance advocated RSV maternal vaccine efforts through its Vaccine Investment Strategy. Infants uninfected but exposed to HIV may experience higher rates of morbidity because of infectious diseases such as RSV, making maternal immunization important for the prevention of infectious diseases in this population [56]. A specific mathematical model predicted a prevention rate of RSV related deaths of 94% for vaccination at 24 weeks of gestation age and 82% for vaccination at 32 weeks of gestation age with data extracted from trials in LMICs. Considering that the out-of-hospital mortality rates are three times than in-hospital rates, over 3,000 deaths in infants under 6 months of age could be prevented through maternal vaccination [57]. Tailored models projected significant potential for an RSV maternal vaccine to mitigate disease impact in infants within 6 months of life across 73 Gavi-supported countries. Such analyses serve as crucial resources for guiding targeted prevention strategies of global organizations like Gavi and World Health Organization (WHO) [58]. Mathematical models provide valuable insights into cost-effectiveness of vaccination strategies in these settings. Results from a mathematical model concerning RSV associated mortality within the first 6 months of life indicate that vaccination could substantially have an impact in reducing the death rates in LMICs [59]. An analysis based on data from Kenya and South Africa illustrates that considering the disease prevalence in these countries among infants younger than 6 months, preventive methods would offer cost-effective solutions[60]. Further cost-effectiveness analyses conducted across various geographical distributions, including LMICs, and tailored to the epidemiological characteristics of the virus can actively participate in the global implementation of RSV maternal vaccination. Critical factors such as vaccine manufacturing, delivery, affordability, and financing need to be carefully assessed and determined.
5. Conclusions
Summarizing the results of maternal RSV vaccination provides an overview of its development over the years. The report of vaccine failures highlights the significant points that must be taken under consideration for the future vaccine development and pharmacovigilance. In-depth research and analysis of the reasons for vaccine withdrawal or failure may unveil potential mediating mechanisms. Real-world clinical data are essential to address gaps in safety and efficacy of the already approved vaccine, while cost-effectiveness analyses can inform the guidelines on RSV prevention. Long-term follow-up studies and rigorous safety monitoring, by encouraging the report of any adverse events, as well as clinical data on specific populations, such as immunosuppressed pregnant women are needed for the further vaccine evaluation.
Author Contributions
Conceptualization, G.P.; methodology, X.T.; data curation, X.T.; writing—original draft preparation, X.T.; writing—review and editing, G.P; supervision, G.P; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Acknowledgments
none.
Conflicts of Interest
none to declare.
References
- Newborn Infections Available online: https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/newborn-health/newborn-infections.
- Hultquist, J.; Rios-Guzman, E.; Simons, L.; Dean, T.; Agnes, F.; Pawlowski, A.; Alisoltanidehkordi, A.; Nam, H.; Ison, M.; Ozer, E.; et al. Altered RSV Epidemiology and Genetic Diversity Following the COVID-19 Pandemic. Res. Sq. 2023. [Google Scholar] [CrossRef] [PubMed]
- RSV Surveillance & Research Available online: https://www.cdc.gov/rsv/research/index.html.
- Johannesen, C.K.; van Wijhe, M.; Tong, S.; Fernández, L. V; Heikkinen, T.; van Boven, M.; Wang, X.; Bøås, H.; Li, Y.; Campbell, H.; et al. Age-Specific Estimates of Respiratory Syncytial Virus-Associated Hospitalizations in 6 European Countries: A Time Series Analysis. J. Infect. Dis. 2022, 226, S29–S37. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children in 2015: A Systematic Review and Modelling Study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Pichler, K.; Assadian, O.; Berger, A. Viral Respiratory Infections in the Neonatal Intensive Care Unit—A Review. Front. Microbiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, T. Vaccinations in the Newborn. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 76, 66–82. [Google Scholar] [CrossRef]
- Kollmann, T.R.; Kampmann, B.; Mazmanian, S.K.; Marchant, A.; Levy, O. Protecting the Newborn and Young Infant from Infectious Diseases: Lessons from Immune Ontogeny. Immunity 2017, 46, 350–363. [Google Scholar] [CrossRef] [PubMed]
- Niewiesk, S. Maternal Antibodies: Clinical Significance, Mechanism of Interference with Immune Responses, and Possible Vaccination Strategies. Front. Immunol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Pregnancy & Vaccines Available online: https://www.cdc.gov/vaccines/parents/by-age/pregnancy.html.
- First RSV Vaccine to Protect Infants up to 6 Months of Age and Older Adults Available online: https://www.ema.europa.eu/en/news/first-rsv-vaccine-protect-infants-6-months-age-and-older-adults.
- FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV in Infants Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infant.
- Walsh, E.E.; Falsey, A.R.; Scott, D.A.; Gurtman, A.; Zareba, A.M.; Jansen, K.U.; Gruber, W.C.; Dormitzer, P.R.; Swanson, K.A.; Radley, D.; et al. A Randomized Phase 1/2 Study of a Respiratory Syncytial Virus Prefusion F Vaccine. J. Infect. Dis. 2022, 225, 1357–1366. [Google Scholar] [CrossRef]
- Falsey, A.R.; Walsh, E.E.; Scott, D.A.; Gurtman, A.; Zareba, A.; Jansen, K.U.; Gruber, W.C.; Dormitzer, P.R.; Swanson, K.A.; Jiang, Q.; et al. Phase 1/2 Randomized Study of the Immunogenicity, Safety, and Tolerability of a Respiratory Syncytial Virus Prefusion F Vaccine in Adults With Concomitant Inactivated Influenza Vaccine. J. Infect. Dis. 2022, 225, 2056–2066. [Google Scholar] [CrossRef]
- Peterson, J.T.; Zareba, A.M.; Fitz-Patrick, D.; Essink, B.J.; Scott, D.A.; Swanson, K.A.; Chelani, D.; Radley, D.; Cooper, D.; Jansen, K.U.; et al. Safety and Immunogenicity of a Respiratory Syncytial Virus Prefusion F Vaccine When Coadministered With a Tetanus, Diphtheria, and Acellular Pertussis Vaccine. J. Infect. Dis. 2022, 225, 2077–2086. [Google Scholar] [CrossRef]
- Simões, E.A.F.; Center, K.J.; Tita, A.T.N.; Swanson, K.A.; Radley, D.; Houghton, J.; McGrory, S.B.; Gomme, E.; Anderson, M.; Roberts, J.P.; et al. Prefusion F Protein–Based Respiratory Syncytial Virus Immunization in Pregnancy. N. Engl. J. Med. 2022, 386, 1615–1626. [Google Scholar] [CrossRef] [PubMed]
- Package Insert - ABRYSVO Available online: https://www.fda.gov/media/168889/download.
- Schmoele-Thoma, B.; Zareba, A.M.; Jiang, Q.; Maddur, M.S.; Danaf, R.; Mann, A.; Eze, K.; Fok-Seang, J.; Kabir, G.; Catchpole, A.; et al. Vaccine Efficacy in Adults in a Respiratory Syncytial Virus Challenge Study. N. Engl. J. Med. 2022, 386, 2377–2386. [Google Scholar] [CrossRef] [PubMed]
- Kampmann, B.; Madhi, S.A.; Munjal, I.; Simões, E.A.F.; Pahud, B.A.; Llapur, C.; Baker, J.; Pérez Marc, G.; Radley, D.; Shittu, E.; et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N. Engl. J. Med. 2023, 388, 1451–1464. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.; Aliabadi, N.; Munjal, I.; Jiang, Q.; Feng, Y.; Brock, L.G.; Cooper, D.; Anderson, A.S.; Swanson, K.A.; Gruber, W.C.; et al. Equivalent Immunogenicity across Three RSVpreF Vaccine Lots in Healthy Adults 18–49 Years of Age: Results of a Randomized Phase 3 Study. Vaccine 2024. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, T.F.; Johnson, C.; Grigat, C.; Apter, D.; Csonka, P.; Lindblad, N.; Nguyen, T.L.-A.; Gao, F.F.; Qian, H.; Tullio, A.N.; et al. Three Dose Levels of a Maternal Respiratory Syncytial Virus Vaccine Candidate Are Well Tolerated and Immunogenic in a Randomized Trial in Nonpregnant Women. J. Infect. Dis. 2022, 225, 2067–2076. [Google Scholar] [CrossRef] [PubMed]
- Bebia, Z.; Reyes, O.; Jeanfreau, R.; Kantele, A.; De Leon, R.G.; Sánchez, M.G.; Banooni, P.; Gardener, G.J.; Rasero, J.L.B.; Pardilla, M.B.E.; et al. Safety and Immunogenicity of an Investigational Respiratory Syncytial Virus Vaccine (RSVPreF3) in Mothers and Their Infants: A Phase 2 Randomized Trial. J. Infect. Dis. 2023, 228, 299–310. [Google Scholar] [CrossRef]
- Hermida, N.; Ferguson, M.; Leroux-Roels, I.; Pagnussat, S.; Yaplee, D.; Hua, N.; van den Steen, P.; Anspach, B.; Dieussaert, I.; Kim, J.H. Safety and Immunogenicity of Respiratory Syncytial Virus Prefusion Maternal Vaccine Coadministered With Diphtheria-Tetanus-Pertussis Vaccine: A Phase 2 Study. J. Infect. Dis. 2023. [Google Scholar] [CrossRef] [PubMed]
- Glenn, G.M.; Smith, G.; Fries, L.; Raghunandan, R.; Lu, H.; Zhou, B.; Thomas, D.N.; Hickman, S.P.; Kpamegan, E.; Boddapati, S.; et al. Safety and Immunogenicity of a Sf9 Insect Cell-Derived Respiratory Syncytial Virus Fusion Protein Nanoparticle Vaccine. Vaccine 2013, 31, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Glenn, G.M.; Fries, L.F.; Thomas, D.N.; Smith, G.; Kpamegan, E.; Lu, H.; Flyer, D.; Jani, D.; Hickman, S.P.; Piedra, P.A. A Randomized, Blinded, Controlled, Dose-Ranging Study of a Respiratory Syncytial Virus Recombinant Fusion (F) Nanoparticle Vaccine in Healthy Women of Childbearing Age. J. Infect. Dis. 2016, 213, 411–422. [Google Scholar] [CrossRef] [PubMed]
- August, A.; Glenn, G.M.; Kpamegan, E.; Hickman, S.P.; Jani, D.; Lu, H.; Thomas, D.N.; Wen, J.; Piedra, P.A.; Fries, L.F. A Phase 2 Randomized, Observer-Blind, Placebo-Controlled, Dose-Ranging Trial of Aluminum-Adjuvanted Respiratory Syncytial Virus F Particle Vaccine Formulations in Healthy Women of Childbearing Age. Vaccine 2017, 35, 3749–3759. [Google Scholar] [CrossRef]
- Muňoz, F.M.; Swamy, G.K.; Hickman, S.P.; Agrawal, S.; Piedra, P.A.; Glenn, G.M.; Patel, N.; August, A.M.; Cho, I.; Fries, L. Safety and Immunogenicity of a Respiratory Syncytial Virus Fusion (F) Protein Nanoparticle Vaccine in Healthy Third-Trimester Pregnant Women and Their Infants. J. Infect. Dis. 2019, 220, 1802–1815. [Google Scholar] [CrossRef] [PubMed]
- Shaw, C.A.; Essink, B.; Harper, C.; Mithani, R.; Kapoor, A.; Dhar, R.; Wilson, L.; Guo, R.; Panozzo, C.A.; Wilson, E.; et al. Safety and Immunogenicity of an MRNA-Based RSV Vaccine Including a 12-Month Booster in a Phase 1 Clinical Trial in Healthy Older Adults. J. Infect. Dis. 2024. [Google Scholar] [CrossRef] [PubMed]
- Dieussaert, I.; Hyung Kim, J.; Luik, S.; Seidl, C.; Pu, W.; Stegmann, J.-U.; Swamy, G.K.; Webster, P.; Dormitzer, P.R. RSV Prefusion F Protein–Based Maternal Vaccine — Preterm Birth and Other Outcomes. N. Engl. J. Med. 2024, 390, 1009–1021. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Polack, F.P.; Piedra, P.A.; Munoz, F.M.; Trenholme, A.A.; Simões, E.A.F.; Swamy, G.K.; Agrawal, S.; Ahmed, K.; August, A.; et al. Respiratory Syncytial Virus Vaccination during Pregnancy and Effects in Infants. N. Engl. J. Med. 2020, 383, 426–439. [Google Scholar] [CrossRef]
- Leroux-Roels, I.; Bruhwyler, J.; Stergiou, L.; Sumeray, M.; Joye, J.; Maes, C.; Lambert, P.-H.; Leroux-Roels, G. Double-Blind, Placebo-Controlled, Dose-Escalating Study Evaluating the Safety and Immunogenicity of an Epitope-Specific Chemically Defined Nanoparticle RSV Vaccine. Vaccines 2023, 11, 367. [Google Scholar] [CrossRef]
- Walsh, E.E.; Falsey, A.R.; Zareba, A.M.; Jiang, Q.; Gurtman, A.; Radley, D.; Gomme, E.; Cooper, D.; Jansen, K.U.; Gruber, W.C.; et al. Respiratory Syncytial Virus Prefusion F Vaccination: Antibody Persistence and Revaccination. J. Infect. Dis. 2024. [Google Scholar] [CrossRef] [PubMed]
- Pipeline—Creating Tomorrow’s Vaccines Today Available online: https://www.novavax.com/science-technology/vaccine-pipeline.
- Mohr, E.; Siegrist, C.-A. Vaccination in Early Life: Standing up to the Challenges. Curr. Opin. Immunol. 2016, 41, 1–8. [Google Scholar] [CrossRef]
- Cuenca, A.G.; Wynn, J.L.; Moldawer, L.L.; Levy, O. Role of Innate Immunity in Neonatal Infection. Am. J. Perinatol. 2013, 30, 105–112. [Google Scholar] [CrossRef] [PubMed]
- 36. Yu, J.C.; Khodadadi, H.; Malik, A.; Davidson, B.; Salles, É. da S.L.; Bhatia, J.; Hale, V.L.; Baban, B. Innate Immunity of Neonates and Infants. Front. Immunol. 2018, 9. [CrossRef]
- Basha, S.; Surendran, N.; Pichichero, M. Immune Responses in Neonates. Expert Rev. Clin. Immunol. 2014, 10, 1171–1184. [Google Scholar] [CrossRef]
- Sedney, C.J.; Harvill, E.T. The Neonatal Immune System and Respiratory Pathogens. Microorganisms 2023, 11, 1597. [Google Scholar] [CrossRef] [PubMed]
- Holm, S.R.; Jenkins, B.J.; Cronin, J.G.; Jones, N.; Thornton, C.A. A Role for Metabolism in Determining Neonatal Immune Function. Pediatr. Allergy Immunol. 2021, 32, 1616–1628. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-C.; Lin, S.-J. Neonatal Natural Killer Cell Function: Relevance to Antiviral Immune Defense. Clin. Dev. Immunol. 2013, 2013, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Strauss-Albee, D.M.; Liang, E.C.; Ranganath, T.; Aziz, N.; Blish, C.A. The Newborn Human NK Cell Repertoire Is Phenotypically Formed but Functionally Reduced. Cytom. Part B Clin. Cytom. 2017, 92, 33–41. [Google Scholar] [CrossRef]
- Hassan, J.; Reen, D.J. Human Recent Thymic Emigrants–Identification, Expansion, And Survival Characteristics. J. Immunol. 2001, 167, 1970–1976. [Google Scholar] [CrossRef]
- Jørgensen, N.; Persson, G.; Hviid, T.V.F. The Tolerogenic Function of Regulatory T Cells in Pregnancy and Cancer. Front. Immunol. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Semmes, E.C.; Chen, J.L.; Goswami, R.; Burt, T.D.; Permar, S.R.; Fouda, G.G. Understanding Early-Life Adaptive Immunity to Guide Interventions for Pediatric Health. Front. Immunol. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Siegrist, C.-A.; Aspinall, R. B-Cell Responses to Vaccination at the Extremes of Age. Nat. Rev. Immunol. 2009, 9, 185–194. [Google Scholar] [CrossRef]
- Assessment Report Abrysvo Available online: https://www.ema.europa.eu/en/documents/assessment-report/abrysvo-epar-public-assessment-report_en.pdf.
- Wang, X.; Li, Y.; Shi, T.; Bont, L.J.; Chu, H.Y.; Zar, H.J.; Wahi-Singh, B.; Ma, Y.; Cong, B.; Sharland, E.; et al. Global Disease Burden of and Risk Factors for Acute Lower Respiratory Infections Caused by Respiratory Syncytial Virus in Preterm Infants and Young Children in 2019: A Systematic Review and Meta-Analysis of Aggregated and Individual Participant Data. Lancet 2024, 403, 1241–1253. [Google Scholar] [CrossRef]
- BLA APPROVAL-ABRYSVO Available online: https://www.fda.gov/media/171492/download?attachment.
- Kenmoe, S.; Chu, H.Y.; Dawood, F.S.; Milucky, J.; Kittikraisak, W.; Matthewson, H.; Kulkarni, D.; Suntarattiwong, P.; Frivold, C.; Mohanty, S.; et al. Burden of Respiratory Syncytial Virus–Associated Acute Respiratory Infections During Pregnancy. J. Infect. Dis. 2024, 229, S51–S60. [Google Scholar] [CrossRef]
- Röbl-Mathieu, M.; Kunstein, A.; Liese, J.; Mertens, T.; Wojcinski, M. Vaccination in Pregnancy. Dtsch. Arztebl. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M.; Fleming-Dutra, K.E.; Prill, M.M.; Roper, L.E.; Brooks, O.; Sánchez, P.J.; Kotton, C.N.; Mahon, B.E.; Meyer, S.; Long, S.S.; et al. Use of Nirsevimab for the Prevention of Respiratory Syncytial Virus Disease Among Infants and Young Children: Recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR. Morb. Mortal. Wkly. Rep. 2023, 72, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Fleming-Dutra, K.E.; Jones, J.M.; Roper, L.E.; Prill, M.M.; Ortega-Sanchez, I.R.; Moulia, D.L.; Wallace, M.; Godfrey, M.; Broder, K.R.; Tepper, N.K.; et al. Use of the Pfizer Respiratory Syncytial Virus Vaccine During Pregnancy for the Prevention of Respiratory Syncytial Virus–Associated Lower Respiratory Tract Disease in Infants: Recommendations of the Advisory Committee on Immunization Practices — United St. MMWR. Morb. Mortal. Wkly. Rep. 2023, 72, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.; Wilkins, N.; van Leeuwen, E.; Watson, C.H.; Crofts, J.; Flasche, S.; Jit, M.; Atkins, K.E. Protecting Infants against RSV Disease: An Impact and Cost-Effectiveness Comparison of Long-Acting Monoclonal Antibodies and Maternal Vaccination. Lancet Reg. Heal. - Eur. 2024, 38, 100829. [Google Scholar] [CrossRef] [PubMed]
- Arora, M.; Lakshmi, R. Vaccines - Safety in Pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 76, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Kong, K.L.; Krishnaswamy, S.; Giles, M.L. Maternal Vaccinations. Aust. J. Gen. Pract. 2020, 49, 630–635. [Google Scholar] [CrossRef]
- Dauby, N.; Gagneux-Brunon, A.; Martin, C.; Mussi-Pinhata, M.M.; Goetghebuer, T. Maternal Immunization in Women Living with HIV. AIDS 2024, 38, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, J.E.; Borghans, J.A.M.; Bont, L.J.; Drylewicz, J. Disagreement FDA and EMA on RSV Maternal Vaccination: Possible Consequence for Global Mortality. Pediatr. Infect. Dis. J. 2024, 43, e1–e2. [Google Scholar] [CrossRef]
- Baral, R.; Li, X.; Willem, L.; Antillon, M.; Vilajeliu, A.; Jit, M.; Beutels, P.; Pecenka, C. The Impact of Maternal RSV Vaccine to Protect Infants in Gavi-Supported Countries: Estimates from Two Models. Vaccine 2020, 38, 5139–5147. [Google Scholar] [CrossRef]
- Willemsen, J.E.; Borghans, J.A.M.; Bont, L.J.; Drylewicz, J. Maternal Vaccination against RSV Can Substantially Reduce Childhood Mortality in Low-Income and Middle-Income Countries: A Mathematical Modeling Study. Vaccine X 2023, 15, 100379. [Google Scholar] [CrossRef]
- Koltai, M.; Moyes, J.; Nyawanda, B.; Nyiro, J.; Munywoki, P.K.; Tempia, S.; Li, X.; Antillon, M.; Bilcke, J.; Flasche, S.; et al. Estimating the Cost-Effectiveness of Maternal Vaccination and Monoclonal Antibodies for Respiratory Syncytial Virus in Kenya and South Africa. BMC Med. 2023, 21, 120. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Modified PRISMA 2020 flow diagram.
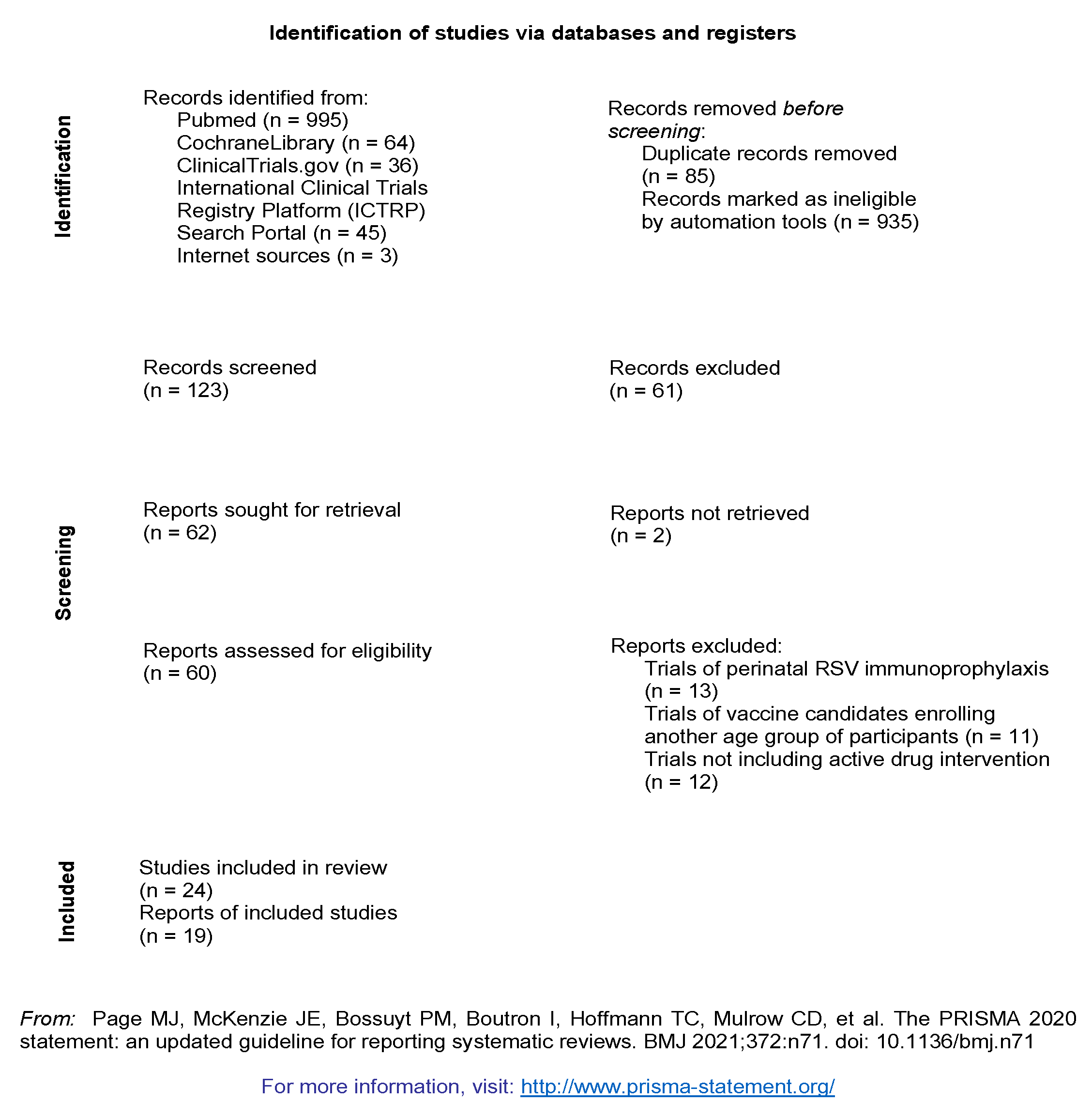

Table 1.
Clinical trials of the maternal RSV vaccines categorized by clinical study status.
| Vaccine | Registration number | Phase | Population | Results |
|---|---|---|---|---|
| Completed clinical trials | ||||
| Abrysvo (Pfizer) | NCT03529773 | I/II | adults including non-pregnant female participants | -Higher titers of neutralizing antibodies in female participants, supporting the principal of maternal vaccination, levels above baseline within a year -no differences in RSV responses after coadministration with influenza vaccine (reduces responsiveness to influenza vaccination) [13,14] |
| NCT04071158 | IIb | non-pregnant female participants | -non-inferiority coadministration trial with tetanus, diphtheria and acellular pertussis vaccine (Tdap) -non-inferiority of coadministration was proved for all the pathogens except for pertussis, supporting vaccination against multiple pathogens [15] |
|
| NCT04032093 | IIb | pregnant female participants (24th -36th gestational week) | -interim analysis: maternal neutralizing antibody production and adequate infant transmission -post-hoc analysis: adequate prevention of infantile disease[16] -5.3% of preterm births in the active group compared to 2.6% in the placebo group [17] |
|
| NCT04785612 | IIa | young adults including non-pregnant female participants | -RSV challenge study -effective against symptomatic disease after RSV exposure [18] |
|
| MATISSE NCT04424316 | III | pregnant female participants (24th -36th gestational week), low-risk pregnancy | -interim analysis -avoidance of RSV-severe lower respiratory tract disease in the first 3 months of life in 81.8% -efficacy rate for lower respiratory tract illness was not statistically significant (57.1%) -protection rate against severe disease within the first 6 months after birth exceeded 69% [19] -premature births were recorded at a rate of 5.7% for the vaccine recipients and 4.7% for the placebo recipients [17] |
|
| NCT05096208 | III | adults including female participants | -consistency and safety of three different vaccine lots [20] | |
| RSV MAT (GSK) | NCT03674177 | I | non-pregnant female participants | -positive data for further evaluation of the vaccine during pregnancy [21] |
| NCT04126213 | II | pregnant female participants (28th-33rd gestational week) | -pregnancy and peripartum abnormalities in similar rates between groups, more cases of hypertension and preeclampsia in the active group without exceeding the general pregnant population rates -elevated titers of antibodies for mothers and their infants [22] |
|
| NCT04138056 | II | non-pregnant female participants | -no interference in RSV-related outcomes after coadministration with Tdap and altered responses for the Tdap pathogens with no (diphtheria and tetanus) or unknown (pertussis) clinical significancy [23] | |
| NCT05045144 | III | non-pregnant female participants | -different vaccine lots and co-administration with influenza vaccine | |
| ResVax (Novavax) | NCT01290419 | I | young male and female participants | -positive results, no association with toxicity, increase of antibody titers -supported further evaluation [24] |
| NCT01704365 | II | non-pregnant female participants | -no serious safety concerns were raised -specific antibody immunity was triggered [25] |
|
| NCT01960686 | II | non-pregnant female participants | -the high antigen dose formulation achieved high titers of antibodies remaining until 3 months post-vaccination and proved safe [26] | |
| NCT02247726 | II | pregnant female participants (33rd – 35th gestational week) | -protection against severe disease for both mothers and their infants, with high antibody titers for the infants -no significant safety issues [27] |
|
| Currently ongoing clinical trials | ||||
| mRNA-1345 | NCT04528719 | I | young adults including female participants | -promising outcomes for further development as a maternal candidate with elevated antibody titers within a 6-month period [28] |
| NCT06143046 | II | pregnant female participants (28th – 36th gestational week) | - | |
| ABRYSVO | MORISOT NCT06325657 |
III | pregnant female participants living with HIV (24th – 36th gestational week) |
- |
| RSV MAT | NCT05705440 | IIIb | participants from all previous trials | -safety monitoring |
| Discontinued clinical trials | ||||
| RSV MAT | GRACE trial NCT04605159 |
III | pregnant female participants (24th – 34th gestational week) | -high protection rates against RSV lower respiratory tract disease -Safety signals: risk of preterm birth (6.8% in the active group and 4.9% in the placebo group) [29] -termination of the study |
| NCT04980391 | III | pregnant female participants (24th – 36th gestational week), high-risk pregnancy | -premature discontinuation based on the findings of the GRACE trial | |
| NCT05229068 | III | re-vaccination trial | -withdrawn, based on the findings of the GRACE trial | |
| NCT05169905 | III | non-pregnant female participants | -early termination of the trial |
|
| Trials that did not achieve the outcome | ||||
| ResVax | NCT02624947 | III | pregnant female participants (28th – 36th gestational age) | -similar rates of pregnancy and birth adverse events between groups with no safety signals -Vaccine efficacy did not meet the primary outcome for protection against RSV lower respiratory tract infection within 3 months of age (39.4%) -VE of 58.8% for disease manifesting with severe hypoxemia [30] |
| V-306 (Virometix) | NCT04519073 | I | non-pregnant female participants | -the expected induction of antibodies and immunity was not achieved [31] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



