
Submitted:
30 May 2024
Posted:
31 May 2024
You are already at the latest version
Abstract
Ankle sprains are the most frequently occurring musculoskeletal injuries among recreational athletes. Ankle support through bandages following the initial orthotic treatment might be beneficial for rehabilitation purposes. Since hardly any study has investigated the impact of bandages in the acute phase of ankle sprains, our study examined the immediate effects of wearing an ankle bandage on fine coordination, proprioception, and motor performance in subjects five weeks after an acute ankle injury. In total, 70 subjects with acute unilateral supination trauma were tested. All subjects completed several rating questionnaires and biomechanical investigations, including a fine coordination and proprioception test, single leg stances, the Y-Balance test and gait analysis. All biomechanical investigations were conducted for the subject's injured leg with and without a bandage (MalleoTrain® Bauerfeind AG) and the healthy leg. Subjects reported moderate to strong improvements in ankle stability and pain when wearing the bandage. Wearing the bandage significantly normalized subjects’ single leg stance performance, as well as the stance phase duration, and the vertical ground reaction forces during walking. However, the bandage did not have a clear effect on fine coordination and proprioception. Wearing a bandage in the acute phase of an ankle sprain may immediately improve motor performance, including standing and walking.
Keywords:
acute ankle sprain
; ankle joint
; ankle bandage
; soft ankle orthoses
; fine coordination and proprioception
; single leg stance
; Y-Balance test
; modified Star Excursion Balance test
; gait
; rehabilitation
1. Introduction
The ankle is a complex joint with three degrees of freedom that enables the body to adapt to different surfaces during physical activities and to absorb shocks and forces. During running and jumping, those forces can reach multiple times the body weight [1,2]. Consequently, the ankle joint is one of the most stressed joints of the body, which can cause pain from injuries, such as fractures or sprains [3,4,5]. Ankle sprains mostly occur following uncontrolled, sudden movements, such as plantarflexion and inversion, which can lead to excessive force or strain in the ligaments of the joint. As a consequence, various ligamentous structures can be damaged, whereas the intensity of the trauma determines, whether it results in a strain or a rupture [4,6,7,8,9]. Depending on the injured ligaments involved, three types of ankle sprains can be distinguished: medial, lateral, and syndesmotic [9,10,11].
Nevertheless, sprains do not only affect components of the musculoskeletal system, but also damage various components of the proprioceptive system [3,9,12,13,14,15,16,17]. This includes damage of specialized receptors, which are located in muscles, tendons, ligaments, and the joint capsule, such as Golgi tendon organs, muscle spindles, joint receptors and various mechanoreceptors. As these receptors provide important information about muscle length, muscle contraction speed, muscle tension, and joint position, for planning, adapting and executing movements, any disruption may negatively affect motor control [13,14,15,18,19,20,21,22].
Ankle sprains are classified by severity and duration. Severity is ranked in three grades based on the extent of tissue damage, assessed through radiological and clinical examinations. Although there exist different classifications, duration is categorized as acute (up to 4 days post-injury), subacute (1 to 8 weeks post-injury), and chronic (more than 8 weeks post-injury). However, the exact timing for developing chronic ankle instability (CAI) is still debated [9,23,24].
From an epidemiological point of view, ankle sprains are the predominant type of injury among recreational athletes in various sports, accounting for approximately 49% of all injuries [5,6]. This includes non-contact sports, such as volleyball and running, as well as contact sports, such as basketball, handball and soccer [5,9]. The lateral ligamentous structures of the ankle joint are mostly affected, which account for approx. 85% of the cases [9,10,11,24,25,26,27,28]. Due to its high incidence, ankle sprains account for at least 14% of all emergency hospital visits, potentially even higher considering that 50% of individuals with ankle injuries do not report or seek hospital treatment [4,7,29,30,31]. As those study results underline the excessive incidence of ankle sprains, as well as the high impact on the economic and the healthcare system, an effective treatment, preferably in the acute and subacute phase seems crucial.
The standardized treatment algorithm for high-grade (grade 2 & 3) ankle sprains describes with all-day orthotic treatment for at least 5 weeks accompanied by active and passive physiotherapy [10,11,27,28,32]. The orthosis should be semi-rigid and stabilize the ankle joint. Therefore, it provides mechanical support and controls the range of motion (ROM) of the ankle joint [33,34,35]. Moreover, it enhances proprioceptive acuity, due to stimulating cutaneous mechanoreceptors, and joint receptors by compressing the underlying musculoskeletal structures [12,36,37]. In case of inadequate therapeutic support, residual symptoms, including pain, giving way, and impaired proprioception and neuromuscular control, can lead to chronic ankle instability (CAI) in 40 to 75% of individuals with ankle sprains [3,8,38,39,40,41]. In the worst-case scenario, CAI increases the risk of articular damage and the development of osteoarthritis. Additionally, it leads to substantial therapy costs and has a dramatic impact on patients quality of life [42,43].
An additional bandage treatment following the 5-week orthotic therapy could be advantageous in supporting the healing process and mitigating the risk of reinjury and the development of CAI. However, most studies that have investigated the effects of bandages on ankle sprains have primarily focused on healthy subjects or patients with CAI, with very limited research examining the effects of bandages during the acute or subacute phases of the injury. Therefore, the aim of our study was to investigate the immediate effects of wearing an ankle bandage on fine coordination, proprioception, and motor performance, five weeks after orthotic treatment in patients with acute lateral ankle sprains. We hypothesized that wearing the bandage helps to reduce pain and improve fine coordination and proprioception. Moreover, it may also enhance motor performance, such as improving quasi static and dynamic balance performance, as well as normalizing gait.
2. Materials and Methods
2.1. Participants
In total, 70 subjects with an acute ankle sprain, caused by unilateral supination trauma (minimum grade 2) were recruited for this study. Subjects were included with an age 18-60 years and if they presented the injury within a maximum of three days after the incidence at the Hospital Chemnitz (Germany). Exclusion criteria comprised grade 1 ankle sprain, upper leg sprain occurring within the last 12 months, acute concomitant osseous injuries, a history of a confirmed lateral ligament injury, CAI or neurological dysfunction, concomitant diseases of the affected upper leg (rheumatism, gout, arthrosis, surgery in past), use of anticoagulants or corticosteroids, and other injuries or diseases affecting motor performance and proprioception. If the patients were still suffering from the injury two to three weeks after the trauma, they were included in the study on a voluntary basis. After the initial treatment with orthotic supply according to the guidelines [10,11], the follow-up examination was performed approximately five weeks post-injury. This involved extensive clinical examination of the ankle joint (swelling, tenderness over the lateral ligament complex, and pain perception), followed by questionnaires and biomechanical investigations. Prior to the examination, all subjects were informed about the purpose of this study and provided written informed consent. All procedures were conducted according to the recommendations of the Declaration of Helsinki and were approved by the Ethics Committee of the Faculty of Behavioural and Social Sciences of Chemnitz University of Technology (V-320-17-LN-MalleoTrain-07042019).
2.2. Experimental Setup and Data Acquisition
All biomechanical investigations were conducted for subjects injured leg and the healthy leg with and without bandage in a randomized order, to minimize the influence of fatigue and habituation. Prior to the main trails, all subjects performed various test trials in order to become familiar with the bandage and the task. All tests were carried out barefoot. The bandage, which was used in this study (MalleoTrain® Bauerfeind AG), consisted of an elastic but tight-fitting high-low knit. Therefore, it exerts an alternating pressure massage during moving.
2.2.1. Subjective Ratings
Prior to the biomechanical investigations, the patients provided their anthropometric data, as well as indicating the pain they experienced when walking and standing barefoot, in shoes, with and without bandage. Afterwards, patients rated pain and stability improvements due to wearing the bandage during the biomechanical tests completing visual analogue scales (0 to 10). Additionally, patients reported whether the bandage provided improvements during the execution of different biomechanical tests.
2.2.2. Fine Coordination and Proprioception Test
A customized foot pedal was implemented to examine the fine coordination and proprioception of the ankle joint. The pedal was designed to allow for inversion and eversion movements of the foot with a maximum range of 5°, respectively (Figure 1A). A target sine wave was presented on a screen in front of the subject, moving from the right to the left side of the screen with a velocity of approx. 7 cm/s. All subjects were instructed to trace the target sine wave as accurately as possible by moving the pedal with inversion and eversion movements of the foot. The extent of the target sine wave ranged from 3° inversion to 3° eversion (Figure 1B). To ensure high test quality, the rotation center of the ankle joint was aligned vertically with the pivot point of the pedal. Additionally, subjects’ lateral side of the lower leg must have maintained permanent contact with the device to guarantee that the ankle joint and not the hip joint performed the movement (Figure 1A). Five trials each lasting 18 s were performed for each testing condition. The mean deviation from the target sine wave from trial four and five within the time interval 6-16 s was calculated for further statistical analysis.
2.2.3. Single Leg Stance (Quasi-Static Postural Stability)
Subjects’ quasi-static postural stability was quantified while performing single leg stances using a pressure distribution platform (Zebris FDM 1.5; Isny, Germany, sampling frequency 100 Hz). Subjects had to stand as still as possible with an upright posture, keeping the knee of the stance leg straightened but not locked, both arms crossed in front of the chest, and directing their gaze ahead. For each subject one trial, lasting 20 s was collected for each testing condition, respectively. For further statistically analysis, the center of pressure (COP) parameters COP length and 95% COP confidence area were calculated for each of the mentioned conditions.
2.2.4. Y-Balance Test (Dynamic Postural Stability)
The Y-Balance test, also known as the modified Star Excursion Balance Test (mSEBT) was used to assess subjects' dynamic postural stability [12,44,45,46,47,48,49]. The test quantifies the ability to maintain a stable base of support, while reaching as far as possible with the lower limbs. To perform the test, subjects stood with one foot in the centre of the measuring grid, ensuring that it was precisely aligned with the grid lines (Figure 4). Thereafter, subjects had to reach out their unloaded foot in one of the three directions (anterior, posterior-medial or posterior-lateral), attempting to reach the furthest point possible, before returning to the starting position. The examiner marked this point and measured the distance from the centre of the grid. If any subject exerted excessive weight on the reaching limb, moved their stance foot from the starting position, or lost balance, the trial had to be repeated. To minimize the influence of inter-individual anthropometrical data, the maximum reach distance was normalized to subjects' individual leg length (Gribble et al. 2003). All subjects completed three main trials for each direction for the three testing conditions healthy stance leg, injured stance leg with and without bandage.
2.2.5. Gait
For subjects’ safety, the pressure distribution platform was integrated in a walk way to be level with the ground. Subjects were instructed to walk at least ten times over the platform (sampling frequency 100 Hz), to collect sufficient data. Gait speed had to be quick but comfortable and safe, and could be chosen individually. For all testing conditions, spatial-temporal gait parameters, such as gait velocity and step length were exported from the Software Zebris winFDM (version 0.1.11, Isny, Germany). Additionally, from the curve of the vertical ground reaction force, the first and second peaks, as well as the relative durations of the single stance phase and double stance phase, were identified for further statistical analysis (Figure 2).
2.3. Statistical Analysis
Mean and standard deviations (mean ± SD) were calculated for all biomechanical variables. Given that the variables were normally distributed according to the Shapiro–Wilk test, a one-way analysis of variance (ANOVA) for repeated measurements followed by the Bonferroni post-hoc test was used to determine whether differences existed between the three conditions healthy leg and the injured leg with and without bandage. Statistical significance was set at α = 0.05 for all analyses. In addition, effect size (Cohen’s d) was calculated to quantify the magnitude of differences when statistical significance was found. The coefficients were interpreted as trivial (d < 0.2), small (d < 0.5), medium (d < 0.8), or large effects (d ≥ 0.8).
3. Results
3.1. Demographic and Clinical Data:
As shown in Table 1, the gender and the side of the injured leg were distributed almost evenly. There were slightly more male subjects and injuries of the right leg. The most frequently structures of the ankle joint with pressure pain were the anterior talofibular ligament, followed by calcaneofibular ligament and the posterior talofibular ligament. Those injuries were accompanied frequently by swelling and other complaints.
Prior to the investigations, the patients generally reported mild to moderate pain, whereas during walking they felt more pain compared to standing. Wearing the bandage, generally eased pain (Table 2). Walking barefoot or in shoes did not reveal major differences for subjective pain perception.
Various improvements have been reported by the subjects due to wearing the bandage (Figure 3). While one half of the cohort reported from strong stabilizing effects when wearing the bandage, the other half reported rather moderate stabilizing effects. Pain was improved mostly moderate. For the biomechanical investigations most self-reported improvements due to wearing the bandage were found for the single leg stance and the Y-Balance test. The fine coordination and proprioception test, as well as the gait test also showed improvements, however a notable number of patients reported from no improvements when wearing the bandage.
3.2. Fine Coordination and Proprioception Test:
For the fine coordination and proprioception test, no statistically significant differences were found between any condition. However, there was a trend towards smaller deviations, especially for the injured leg with the bandage compared to the healthy leg (Table 3).
3.3. Single Leg Stance (Quasi-Static Postural Stability):
As presented in Table 4, statistically significant differences between study conditions could only be found for the COP length, however not for the COP 95% confidence area. Subjects showed especially longer COP excursions for the injured leg without bandage compared to the injured leg when wearing the bandage and the healthy leg. Nevertheless, the COP 95% confidence area showed the same result as the COP length, however as a trend and not statistically significant.
3.4. Y-Balance Test (Dynamic Postural Stability):
The Y-Balance test revealed higher values for the maximum reach distance, when subjects were standing on their healthy leg compared to when subjects were standing on their injured leg with or without bandage. These statistically significant differences with medium effect sizes were exclusively found for the anterior direction (Figure 4).
3.5. Gait:
As shown in Table 5, various statistically significant differences between the three walking conditions could be found. With respect to the healthy leg, the injured leg showed a shorter single stance phase and decreased second peak of the vertical force, regardless of wearing the bandage or not. The step length and the first peak of the vertical force did only reveal differences between the healthy and the injured leg without wearing the bandage. The step length for the healthy leg was decreased and the first peak of the vertical force was significantly higher.
When comparing walking with and without bandage, the healthy leg showed longer steps with higher vertical forces of the second peak when walking with bandage. The injured leg showed a longer relative single stance phase and higher vertical forces of the first and second peak, when walking with a bandage.
The parameters gait velocity and relative double stance phase, however, did not show any significant differences between the conditions walking with bandage and walking without bandage.
4. Discussion
The aim of this study was to investigate the effects of wearing an ankle bandage on fine coordination and proprioception as well as on motor performance in subjects 5 weeks after orthotic treatment for acute ankle injuries. We hypothesized that wearing the bandage helps to reduce pain and improve fine coordination and proprioception. Moreover, it may also enhance motor performance, such as improving quasi static and dynamic balance performance, as well as normalizing gait.
4.1. Fine Coordination and Proprioception Test
4.1.1. Effects of the Injury
We found no statistically significant differences between any testing condition for the fine coordination and proprioception test. However, we observed a trend towards worse fine coordination for the healthy leg and the best fine coordination for the injured leg when wearing the bandage. These results were somewhat surprising since various other studies have shown impaired proprioceptive abilities as a consequence of damaged articular mechanoreceptors after spraining the ankle joint [3,13,14,15,16,17,18,29,51,52]. Therefore, we raised the question of what could have led to better performance of the injured ankle compared to the healthy ankle. Since those studies primarily investigated proprioception in CAI, rather than in the acute phase our results might possibly be attributed to increased awareness and caution when moving the injured leg. This notion is supported by the fact that our subjects still reported pain during the test [29,53,54]. Also, various compensation mechanisms could have played an important role. Since our patients were tested in an acute phase of the injury, the influence of active healing processes, such as increased blood flow and tissue supply, could have helped compensate possible injury-related proprioceptive impairments, resulting in slightly better performance [32,55]. There are also various types of mechanoreceptors found in different anatomical structures of the ankle joint, gathering afferent information to control movements. These receptors are situated within the ligaments, tendons, the joint capsule, surrounding muscles, and even the skin. Due to this redundancy, potentially unaffected structures might have compensated and reweighted the impaired function of those affected by the injury [56,57,58]. Since our test required subjects to move a pedal with inversion and eversion movements of the ankle joint to follow a presented target sine wave on the screen, the results of this test might also be dominated and possibly overcompensated by the visual system [20,56].
4.1.2. Effects of the Bandage
A more plausible result of our study suggests that the injured leg with the bandage showed a trend towards better proprioceptive performance compared to without it. Although the literature yields inconsistent findings regarding the effects of bandages and elastic tapes on ankle joint fine coordination and proprioception, there may be several explanations for our results [26,59,60,61,62,63]. Since the bandage mechanically stabilizes the ankle joint, it increases resistance during joint movement. Consequently, it may have assisted and restricted the inversion and eversion movements of the ankle joint, especially at the reversal points of the pedal, which led to smaller error values during our test [33,34,35,64]. This gets supported by the results of the subjective data, where the subjects ranked the effects of wearing the bandage. The vast majority of the subjects reported from strong (50%) to moderate (48.6%) stabilizing effects of the ankle joint. For the fine coordination and proprioception test, 30% of the subjects reported strong improvements, while 50% still reported slight improvements when wearing the bandage. Another reason for enhanced proprioceptive performance using ankle supports, like bandages might have to do with the compression of the underlying musculoskeletal structures. Consequently, this might stimulate a greater number of cutaneous mechanoreceptors, as well as receptors of the joint capsule and ligaments, enhancing proprioceptive acuity and ankle movements [3,26,53,59,60]. Given that we only found a trend towards better proprioceptive performance and that hardly any other studies besides ours have investigated the effects of ankle support on proprioception in the acute phase rather than in CAI, the benefits of bandages on fine coordination and proprioception still appear elusive. One should also consider that our testing setup differed from that of other studies, which used detection of passive motion or active joint position tests. Therefore, comparing our results to those of other studies should be done carefully.
4.2. Motor Performance
4.2.1. Effects of the Injury
In terms of motor performance, the injured leg showed significant impairments compared to the healthy leg. This was demonstrated by higher sway values for the single leg stances, reduced reach distance for the Y-Balance test and impaired gait performance with longer steps, shorter single stance phases and smaller vertical ground reaction forces.
Two main causes might help to explain those findings: mechanical ankle instability (MAI) and functional ankle instability (FAI). Although those terms have primarily been used to describe the development of CAI, they also apply to the acute phase of ankle injuries, which has been analyzed in our study. While MAI is associated with complaints of mechanical instability and laxity, as well as pain and swelling, FAI is more related to impaired functional muscle control due to compromised proprioceptive and sensory structures [29,48,65,66]. Although both causes interact and overlap each other, higher sway values during quasi-static balance tasks, such as single leg stances might predominantly be explained by MAI [29,55,67]. That makes sense, considering that our patients reported complaints of laxity and instability. Our results are in line with various other studies [17,29,68,69,70]. For example, Hertel et al. reported that during single leg stances postural sway length and velocity increased significantly on the injured leg as compared with the uninjured leg [68]. Pourkazemi et al., even stated that single leg stances most strongly discriminated between participants with ankle sprains and healthy control subjects [69]. These results may be due to changes in postural strategies. Maintaining balance is usually accomplished by using either the ankle strategy or the hip strategy. The ankle strategy shifts the center of gravity by moving the entire body as a single-segmented inverted pendulum around the ankle joint, whereas the hip strategy involves moving the body as a double-segmented inverted pendulum with counter-phase motions around both the hip and ankle joints [22,68,69,71]. As a result of the injury, the subjects may switch from the typical ankle strategy to the hip strategy, which is less effective for quasi-static balance tasks [69,72,73]. Nevertheless, there are also several studies, which contradict our study findings for the single leg stance test [32,74,75]. Possible explanations for this contradiction might include varying methodological factors, such as differences in test paradigms and study groups. Most of those studies investigated patients with CAI, however not patients in the acute phase of the injury. As suggested by Ross and Guskiewicz, quasi-static balance tests might have limited sensitivity, because they only assesses a single component of balance and therefore should be supplemented by additional, more challenging measures, like the Y-Balance test [69,75].
The Y-Balance test quantifies the ability to maintain a stable base of support while reaching as far as possible with the lower limbs. In our study, the maximum reach distance was significantly reduced when subjects were standing on their injured leg without a bandage compared to when they were standing on the healthy leg. However, we only found this for the anterior direction, but not for the posterior-medial or posterior-lateral directions. While the literature yields inconsistent results regarding the most impaired reaching direction, some studies have also reported impairments in the anterior direction [47,49,69,76]. For example, Pourkazemi et al. reported that a reduced anterior reach distance most strongly discriminated between subjects with ankle sprains and healthy subjects [69]. Similar results have also been found in the study by McCann et al., where the study group with CAI achieved lower anterior test scores compared to subjects coping with lateral ankle sprains [76]. Since the Y-Balance test is considered a measure of dynamic postural stability, patients’ diminished reach distance might predominantly be related to FAI [69]. This might be true, as some studies have reported altered lower limb muscle activity in patients with CAI when performing anterior reaches [77,78]. In both studies they found less activity for the tibialis anterior and peroneus longus muscles compared to patients coping with CAI. Another key factor contributing to patients' impaired anterior reach distance could be altered kinematics resulting from reduced ROM of the ankle joint [44,45,69,79]. In the studies from Pourkazemi et al. and Basnett et al. subjects with CAI exhibited restricted dorsiflexion motion in comparison to healthy control groups. Patients’ limited ROM moderately correlated with the anterior reach distance of the Y-Balance test [69,79]. It has also been reported that individuals with CAI showed reduced hip and knee flexion while executing the test in the anterior direction. Furthermore, knee flexion and torso rotation have been identified as the primary kinematic predictors of reach distance during performance in the anterior direction [45,76]. Hence, limited ankle dorsiflexion ROM is a strongly limiting factor for the Y-Balance test anterior performance [44,48,80]. However, other than in our study, various authors reported from significantly diminished reach distances not only for the anterior direction, but also for the posterior-lateral [44,46,47,49,78] and posterior-medial [46,81] directions among patients with CAI when compared to healthy subjects, CAI copers, or the injured and uninjured sides. Similar to the anterior direction, diminished reach distance in both posterior directions might include reduced activity of lower limb muscles [77,78,82], as well as altered kinematics due to restricted dorsiflexion ROM [44,45,46,47,76]. Other factors may include pain and fear of falling due to ankle instability. Although the results are controversial, proprioceptive and neuromuscular deficits might also play a role [29,44,47,53,57,59,68].
During walking, we found significant differences in spatial-temporal parameters for the injured leg compared to the healthy leg. In more detail, the injured leg showed longer steps and shorter single stance phases during walking. Since longer steps typically signify higher gait quality, our observation might seem confusing at the first glance. It even seems to contradict various other studies in which reduced step lengths were reported for patients with ankle injuries [54,83,84,85]. However, there is a simple methodological explanation for this contradiction. In the mentioned studies they conducted inter-individual investigations, comparing a group with ankle injuries to another group of healthy subjects. In contrast, we observed intra-individual effects of the ankle injury by comparing the injured leg with the healthy leg within the same subjects. As the healthy leg compensates for impairments of the injured leg, patients in our study attempted to extend the step length of the injured leg to increase swing time and consequently minimize the loading time of the injured leg. This gets supported by our findings of reduced single stance phases for the injured leg during walking [54,83,84,85]. Since our patients were tested in the acute phase of the injury, this effect is likely driven by the pain they reported, as well as by fear of falling [54,84]. Other spatial-temporal parameters reported in the literature to characterize impaired gait performance in patients with ankle sprains include reduced walking speed, decreased cadence, and wider steps [54,83,84,85,86]. Other studies also reported from a decrease in vertical foot-floor clearance before heel strike, an increased inversion velocity during heel strike, reduced maximum plantar flexion during the stance phase, and a more inverted foot position throughout the entire gait cycle [44,54,65,86,87,88]. The altered kinematics of the patients may help to explain the differences we found for the kinetic parameters comparing the injured and healthy legs. In more detail, we observed diminished ground reaction forces for the injured leg for the first peak, corresponding to the loading response, and the second peak, corresponding to the terminal stance phase of the gait cycle [50]. Accordingly, our results overlap with those of several other studies [54,89,90]. For example, Nyska et al. reported a reduced impact at the beginning and end of the stance phase with a significant reduction in the relative forces under the heel and toes in subjects with CAI during walking. The authors also reported slower weight transfer from the heel to toe, and a lateral shift of the foot’s COP, probably caused by a more inverted foot position [90]. Similarly, in the studies by Punt et al. and Doherty et al., the authors observed decreased maximum power and reduced maximum moments in patients with ankle sprains compared to healthy individuals [54,89]. The findings of patients unloading their injured leg during walking contrast those of Koldenhoven et al., which found increased ankle plantarflexion moments during the late stance phase to toe-off [86]. Nevertheless, this may be due to differences in study methods. In their study, subjects walked on a split belt treadmill and wore standardized shoes, whereas in our study, patients were barefoot and walked across a pressure distribution platform. Furthermore, they tested patients with CAI, whereas our patients were in the acute phase of the injury and reported pain during walking. The impaired gait pattern from patients with ankle sprains is considered to have a multifactorial pathology and can be attributed to several co-existing factors. This includes mechanical instability, proprioceptive impairments, neuromuscular control deficits, postural instability, reduced ROM of the ankle joint, altered activation of lower limb muscles, as well as pain and fear [15,17,29,44,54,55,57,65,69,83,84,86,87,88,91,92,93,94].
4.2.2. Effects of the Bandage
Wearing the bandage in the acute phase of the injury significantly enhanced our subjects’ single leg stance performance and normalized gait. However, the bandage did not improve our subjects’ reach distance for the Y-Balance test.
Our findings of reduced sway when wearing the bandage during single leg stances are supported by two studies from Hadadi et al. In those studies, the authors concluded that both the immediate use of soft or semi-rigid ankle braces and their continuous use for four weeks improved single leg stance performance in subjects with CAI [12,95]. Small but significant and effective benefits on single leg stances in patients with ankle injuries using soft or semi-rigid orthosis have also been found in the studies from Best et al. and Faraji et al. [3,32]. Moreover, in the study from Baier and Hopf, the authors found that in athletes with functional ankle instability, a flexible ankle orthosis significantly reduced the medio-lateral sway velocity during single leg stances and changed the sway pattern by reducing the percentage of linear movements [96]. The positive effects of ankle support on quasi-static balance tasks, such as single leg stances, may predominantly be explained by proprioceptive stimulation, and by mechanical support. By stimulating cutaneous mechanoreceptors and exerting pressure on underlying musculoskeletal structures, ankle supports might offer additional sensory input about joint position and movements. Therefore, ankle supports may help detecting internal balance perturbations, thereby improving the control of postural sway in individuals with ankle sprains. [3,12,96,97]. The observation that the decrease in postural sway due to wearing ankle supports is more pronounced in patients than in healthy subjects reinforces this theory [96,97,98]. Apart from proprioception, a noticeable portion of the improvements could be attributed to mechanical stabilization [12,53,96,99]. This gets supported, by the study from Thonnard et al., in which they investigated the inversion torque of bare and braced ankles under static and dynamic conditions using a customized mechanical apparatus. In their study they found that the additional inversion ankle torque generated by an elastic brace effectively increased the passive resistance against ankle inversion movement compared with the bare ankle tests. Although the additional torque provided by the braces was small relative to the torques and forces applied to the foot during a typical sprain situation, it might contribute to additional stability during single leg stances, resulting in reduced sway [34,64]. That also aligns with findings that ankle-injured subjects report feeling more stable and comfortable during balance testing when wearing orthotics [97,99]. Also, in our study, the vast majority of subjects reported strong (50%) to moderate (48.6%) stabilizing effects on the ankle joint when wearing the bandage. For the single leg stance test, 27.1% of the subjects reported strong improvements, while 40.0% still reported slight improvements when wearing the bandage. Furthermore, reduced pain perception when wearing the bandage might have had a positive effect on postural sway.
In our assessment of dynamic postural stability using the Y-Balance test, we did not observe any improvements in patients' reach distances while wearing the bandage, regardless of the testing direction. This seems surprising, since wearing the bandage enhanced single leg stance performance and gait in our study. However, there might be some explanations. In the study from Alawna et al. they investigated the effects of ankle taping and bandages on the reach distance of one-hundred patients with CAI. They conducted measurements at baseline, immediately after support, and then at 2 weeks and 2 months post-support. Their results showed that ankle taping and bandaging does not immediately improve reach distance, however after 2 weeks and 2 months [59]. Moreover, in the study by Hadidi et al., they investigated the effects of ankle taping and soft or semirigid ankle braces on the reach distance of the Y-Balance test before and after a 4-week intervention period. Their findings showed that the use of tape and a soft or a semirigid ankle brace for 4 weeks were all beneficial in improving the reach distance in individuals with CAI [51]. Also, in the study from John et al., they investigated the effects of an elastic ankle support on dynamic balance in patients with CAI using the Y-Balance Test. The authors concluded that the acute use of elastic ankle support was ineffective in enhancing dynamic balance [100]. Considering those as well as our results, it seems that patients may need some time to adapt to the bandage in order to fully experience its positive effects on mechanically stabilizing the ankle joint and enhancing proprioception for this specific test. This might be true, as the Y-balance test is particularly challenging and differs from more daily activities, such as standing on one leg or walking. Because we tested patients in the acute phase, their pain and fear of falling might have been more severe compared to studies involving patients with CAI, further potentially limiting the effectiveness of the bandage condition in our study.
Regarding gait, we were surprised to find only one study investigating the influence of orthotic support in patients with ankle injuries [85]. In this study, 10 subjects with CAI walked without a brace, with a flexible brace, and with a semi-rigid ankle brace while their kinematics and kinetics were recorded using a marker-based system and a force plate. Although the effects were small, few differences were noted between the brace and no brace conditions. In summary, the authors described the effect of wearing braces during walking, noting altered foot angles at the heel strike and toe-off, altered braking forces, reduced step lengths, and a reduction in the stance phase. Therefore, this study partly confirms our findings, of extended stance phases and higher vertical ground reaction forces for the loading response and the terminal stance phase when walking with the bandage compared to walking without the bandage. Noteworthy, wearing the bandage during walking also improved our subjects' healthy leg performance, resulting in longer steps and higher vertical ground reaction forces during the terminal stance phase. Consequently, wearing the bandage might aid in reducing asymmetry, which could potentially mitigate the risk of injuries [101,102]. The proposed mechanisms explaining the effectiveness of ankle orthoses during walking might include mechanical support, improving proprioceptive and sensorimotor function, as well as enhancing ankle positioning and muscular efficiency around the ankle joint [12,53,64,99,103]. Spaulding et al., suggested that ankle braces affect forward progression without significantly impacting gait characteristics or causing compensatory or adaptive motion elsewhere in the lower limb [85]. Specifically, the reduction of pain when wearing the bandage might have encouraged our patients to exert more and longer-lasting loads on the injured leg during the single stance phase of the gait.
Interpreting our results should be done in light of some restrictions. First, comparability to other studies might predominantly be restricted to those studies which methodologically come close to our study design. Since a wide variety of ankle supports has been investigated in the literature, studies that utilized soft ankle supports may be most comparable to the ankle bandages we used in our study. In this regard, it should also be noted that while most other studies investigated the effects of ankle support in patients suffering from CAI, we focused on patients in the acute phase of ankle injuries. Specific limitations of our study include the inability to identify the exact ankle injury due to the absence of Magnetic Resonance Imaging (MRI) investigations. Further studies should include kinematic analysis of the subjects’ motion, as well as analyzing leg muscle activity using electromyographic sensors. It also would be interesting to compare the efficacy of different ankle supports, as our study focused solely on ankle bandages.
5. Conclusion
Five weeks after the ankle injury, subjects reported mild to moderate pain and ankle instability, and showed impaired motor performance in the injured leg compared to the healthy leg when not wearing the bandage. This included higher sway values for single leg stances, reduced reach distance in the Y-Balance test, and impaired gait performance characterized by longer steps, shorter stance phases, and smaller vertical ground reaction forces. No impairments were found in the fine coordination and proprioception tests. Subjects reported moderate to strong improvements in ankle stability and pain when wearing the bandage. Wearing the bandage significantly normalized subjects’ single leg stance performance, as well as the single stance phase duration, and the vertical ground reaction force during walking. However, the bandage did not have a clear effect on fine coordination and proprioception. Therefore, we conclude that wearing a bandage in the acute phase of an ankle sprain may immediately improve motor performance, including standing and walking.
Author Contributions
Conceptualization, A.K., T.L.M.; methodology, A.K., T.L.M.; software, T.H., C.M.; validation, T.H., C.M; formal analysis, T.H., C.M.; investigation, A.K.; resources, A.K.; T.H., C.M., T.L.M.; data curation, C.M., T.H., T.L.M; writing—original draft preparation, T.H., C.M., A.K.; writing—review and editing, T.H., C.M., A.K., T.L.M.; visualization, T.H., C.M.; supervision, C.M., T.L.M., A.K.; project administration, T.H., C.M., A.K.; funding acquisition, T.H, C.M. All authors have read and agreed to the published version of the manuscript.
Funding
Bauerfeind AG provided financial and material support for this study. The publication of this article was funded by Chemnitz University of Technology and by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) project number 491193532.
Institutional Review Board Statement
All procedures were conducted according to the recommendations of the Declaration of Helsinki and were approved by the Ethics Committee of the Faculty of Behavioural and Social Sciences of Chemnitz University of Technology (V-320-17-LN-MalleoTrain-07042019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset used and analyzed in this study is available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all subjects and Bauerfeind AG for supporting this study. We would also like to extend special thanks to Laura Niklaus for data acquisition, and to Ralph Dörfler and Philip Schulze for providing technical support.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in writing the manuscript, or in the decision to publish the results.
References
- Lieberman, D.E.; Venkadesan, M.; Werbel, W.A.; Daoud, A.I.; D’Andrea, S.; Davis, I.S.; Mang’Eni, R.O.; Pitsiladis, Y. Foot strike patterns and collision forces in habitually barefoot versus shod runners. Nature 2010, 463, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Ericksen, H.M.; Gribble, P.A.; Pfile, K.R.; Pietrosimone, B.G. Different modes of feedback and peak vertical ground reaction force during jump landing: a systematic review. J. Athl. Train. 2013, 48, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Faraji, E.; Daneshmandi, H.; Atri, A.E.; Onvani, V.; Namjoo, F.R. Effects of prefabricated ankle orthoses on postural stability in basketball players with chronic ankle instability. Asian J. Sports Med. 2012, 3, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.T.-P.; Hong, Y.; Chan, L.-K.; Yung, P.S.-H.; Chan, K.-M. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007, 37, 73–94. [Google Scholar] [CrossRef] [PubMed]
- Luciano, A.d.P.; Lara, L.C.R. Epidemiological study of foot and ankle injuries in recreational sports. Acta Ortop. Bras. 2012, 20, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.C.G.; Hendler, K.G.; Kuriki, H.U.; Barbosa, R.I.; das Neves, L.M.S.; Guirro, E.C.d.O.; Guirro, R.R.d.J.; Marcolino, A.M. Influence of neoprene ankle orthoses on dynamic balance during a vertical jump in healthy individuals and with sprain history: A cross-sectional study. Gait Posture 2023, 101, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M.; Dick, R.; Agel, J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J. Athl. Train. 2007, 42, 311–319. [Google Scholar] [PubMed]
- Abbasi, F.; Bahramizadeh, M.; Hadadi, M. Comparison of the effect of foot orthoses on Star Excursion Balance Test performance in patients with chronic ankle instability. Prosthet. Orthot. Int. 2019, 43, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Wallmann, H.W.; Quiambao, K.L.; Grimes, B.M. The Effects of Whole Body Vibration on the Limits of Stability in Adults With Subacute Ankle Injury. Int. J. Sports Phys. Ther. 2021, 16, 749–755. [Google Scholar] [CrossRef]
- Kerkhoffs, G.M.; van den Bekerom, M.; Elders, L.A.M.; van Beek, P.A.; Hullegie, W.A.M.; Bloemers, G.M.F.M.; de Heus, E.M.; Loogman, M.C.M.; Rosenbrand, K.C.J.G.M.; Kuipers, T.; et al. Diagnosis, treatment and prevention of ankle sprains: an evidence-based clinical guideline. Br. J. Sports Med. 2012, 46, 854–860. [Google Scholar] [CrossRef]
- Ruiz-Sánchez, F.J.; Ruiz-Muñoz, M.; Martín-Martín, J.; Coheña-Jimenez, M.; Perez-Belloso, A.J.; Pilar Romero-Galisteo, R.; Gónzalez-Sánchez, M. Management and treatment of ankle sprain according to clinical practice guidelines: A PRISMA systematic review. Medicine (Baltimore) 2022, 101, e31087. [Google Scholar] [CrossRef] [PubMed]
- Hadadi, M.; Haghighat, F.; Mohammadpour, N.; Sobhani, S. Effects of Kinesiotape vs Soft and Semirigid Ankle Orthoses on Balance in Patients With Chronic Ankle Instability: A Randomized Controlled Trial. Foot Ankle Int. 2020, 41, 793–802. [Google Scholar] [CrossRef] [PubMed]
- de Vasconcelos, G.S.; Cini, A.; Sbruzzi, G.; Lima, C.S. Effects of proprioceptive training on the incidence of ankle sprain in athletes: systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Anson, J.; Waddington, G.; Adams, R.; Liu, Y. The Role of Ankle Proprioception for Balance Control in relation to Sports Performance and Injury. Biomed Res. Int. 2015, 2015, 842804. [Google Scholar] [CrossRef] [PubMed]
- Willems, T.; Witvrouw, E.; Verstuyft, J.; Vaes, P.; de Clercq, D. Proprioception and Muscle Strength in Subjects With a History of Ankle Sprains and Chronic Instability. J. Athl. Train. 2002, 37, 487–493. [Google Scholar] [PubMed]
- Fu, A.S.N.; Hui-Chan, C.W.Y. Ankle joint proprioception and postural control in basketball players with bilateral ankle sprains. Am. J. Sports Med. 2005, 33, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Hiller, C.E.; Nightingale, E.J.; Lin, C.-W.C.; Coughlan, G.F.; Caulfield, B.; Delahunt, E. Characteristics of people with recurrent ankle sprains: a systematic review with meta-analysis. Br. J. Sports Med. 2011, 45, 660–672. [Google Scholar] [CrossRef] [PubMed]
- Jerosch, J.; Prymka, M. Proprioception and joint stability. Knee Surg. Sports Traumatol. Arthrosc. 1996, 4, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Pearson, K.G. Proprioceptive regulation of locomotion. Curr. Opin. Neurobiol. 1995, 5, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Riemann, B.L.; Lephart, S.M. The Sensorimotor System, Part II: The Role of Proprioception in Motor Control and Functional Joint Stability. J. Athl. Train. 2002, 37, 80–84. [Google Scholar]
- Heß, T.; Milani, T.L.; Meixensberger, J.; Krause, M. Postural performance and plantar cutaneous vibration perception in patients with idiopathic normal pressure hydrocephalus. Heliyon 2021, 7, e05811. [Google Scholar] [CrossRef] [PubMed]
- Heß, T.; Themann, P.; Oehlwein, C.; Milani, T.L. Does Impaired Plantar Cutaneous Vibration Perception Contribute to Axial Motor Symptoms in Parkinson's Disease? Effects of Medication and Subthalamic Nucleus Deep Brain Stimulation. Brain Sci. 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Terada, M.; Pietrosimone, B.G.; Gribble, P.A. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review. J. Athl. Train. 2013, 48, 696–709. [Google Scholar] [CrossRef] [PubMed]
- Delahunt, E.; Bleakley, C.M.; Bossard, D.S.; Caulfield, B.M.; Docherty, C.L.; Doherty, C.; Fourchet, F.; Fong, D.T.; Hertel, J.; Hiller, C.E.; et al. Clinical assessment of acute lateral ankle sprain injuries (ROAST): 2019 consensus statement and recommendations of the International Ankle Consortium. Br. J. Sports Med. 2018, 52, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Roos, K.G.; Kerr, Z.Y.; Mauntel, T.C.; Djoko, A.; Dompier, T.P.; Wikstrom, E.A. The Epidemiology of Lateral Ligament Complex Ankle Sprains in National Collegiate Athletic Association Sports. Am. J. Sports Med. 2017, 45, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, S.; Papadopoulos, K.; Bampouras, T.M.; Maestroni, L. What is the effect of ankle disk training and taping on proprioception deficit after lateral ankle sprains among active populations? - A systematic review. J. Bodyw. Mov. Ther. 2022, 31, 62–71. [Google Scholar] [CrossRef]
- Röpke, M.; Piatek, S.; Ziai, P. Akute Sprunggelenkinstabilität durch Distorsion. Arthroskopie 2015, 28, 116–123. [Google Scholar] [CrossRef]
- Stürmer, K.M.; Rammelt, S.; Richter, M.; Walther, M. Frische Außenbandruptur am Oberen Sprunggelenk. Leitlinien Unfallchirurgie 2017. [Google Scholar]
- Alghadir, A.H.; Iqbal, Z.A.; Iqbal, A.; Ahmed, H.; Ramteke, S.U. Effect of Chronic Ankle Sprain on Pain, Range of Motion, Proprioception, and Balance among Athletes. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef]
- Fong, D.T.-P.; Man, C.-Y.; Yung, P.S.-H.; Cheung, S.-Y.; Chan, K.-M. Sport-related ankle injuries attending an accident and emergency department. Injury 2008, 39, 1222–1227. [Google Scholar] [CrossRef]
- McKay, G.D.; Goldie, P.A.; Payne, W.R.; Oakes, B.W. Ankle injuries in basketball: injury rate and risk factors. Br. J. Sports Med. 2001, 35, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Best, R.; Böhle, C.; Schiffer, T.; Petersen, W.; Ellermann, A.; Brueggemann, G.P.; Liebau, C. Early functional outcome of two different orthotic concepts in ankle sprains: a randomized controlled trial. Arch. Orthop. Trauma Surg. 2015, 135, 993–1001. [Google Scholar] [CrossRef]
- Fuerst, P.; Gollhofer, A.; Wenning, M.; Gehring, D. People with chronic ankle instability benefit from brace application in highly dynamic change of direction movements. J. Foot Ankle Res. 2021, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Hartsell, H.D.; Spaulding, S.J. Effectiveness of external orthotic support on passive soft tissue resistance of the chronically unstable ankle. Foot Ankle Int. 1997, 18, 144–150. [Google Scholar] [CrossRef]
- Scheuffelen, C.; Rapp, W.; Gollhofer, A.; Lohrer, H. Orthotic devices in functional treatment of ankle sprain. Stabilizing effects during real movements. Int. J. Sports Med. 1993, 14, 140–149. [Google Scholar] [CrossRef]
- Halseth, T.; McChesney, J.W.; Debeliso, M.; Vaughn, R.; Lien, J. The effects of kinesio™ taping on proprioception at the ankle. J. Sports Sci. Med. 2004, 3, 1–7. [Google Scholar] [PubMed]
- Perlau, R.; Frank, C.; Fick, G. The effect of elastic bandages on human knee proprioception in the uninjured population. Am. J. Sports Med. 1995, 23, 251–255. [Google Scholar] [CrossRef]
- Anandacoomarasamy, A.; Barnsley, L. Long term outcomes of inversion ankle injuries. Br. J. Sports Med. 2005, 39, e14. [Google Scholar] [CrossRef]
- Safran, M.R.; Benedetti, R.S.; Bartolozzi, A.R., 3rd; Mandelbaum, B.R. Lateral ankle sprains: A comprehensive review: part 1: Etiology, pathoanatomy, histopathogenesis, and diagnosis. Med. Sci. Sports Exerc. 1999, 31, S429–S437. [Google Scholar] [CrossRef]
- Yeung, M.S.; Chan, K.M.; So, C.H.; Yuan, W.Y. An epidemiological survey on ankle sprain. Br. J. Sports Med. 1994, 28, 112–116. [Google Scholar] [CrossRef]
- Kilper, A.; Lederer, A.-K.; Niklaus, L.; Milani, T.; Langenhan, R.; Schütz, L.; Reimers, N. Heilungsverlauf und Behandlungsergebnisse nach akutem Supinationstrauma des oberen Sprunggelenkes. Sports Orthopaedics and Traumatology 2023, 39, 39–49. [Google Scholar] [CrossRef]
- Hintermann, B.; Boss, A.; Schäfer, D. Arthroscopic findings in patients with chronic ankle instability. Am. J. Sports Med. 2002, 30, 402–409. [Google Scholar] [CrossRef]
- Hupperets, M.D.W.; Verhagen, E.A.L.M.; van Mechelen, W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised controlled trial. BMJ 2009, 339, b2684. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Mei, Q.; Xiang, L.; Fernandez, J.; Gu, Y. Differences in the locomotion biomechanics and dynamic postural control between individuals with chronic ankle instability and copers: a systematic review. Sports Biomech. 2022, 21, 531–549. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.; Wilson, C.S.; Becker, J. Kinematic and Kinetic Predictors of Y-Balance Test Performance. Int. J. Sports Phys. Ther. 2021, 16, 371–380. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Dynamic balance deficits in individuals with chronic ankle instability compared to ankle sprain copers 1 year after a first-time lateral ankle sprain injury. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1086–1095. [Google Scholar] [CrossRef] [PubMed]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Dynamic Balance Deficits 6 Months Following First-Time Acute Lateral Ankle Sprain: A Laboratory Analysis. J. Orthop. Sports Phys. Ther. 2015, 45, 626–633. [Google Scholar] [CrossRef]
- Gabriner, M.L.; Houston, M.N.; Kirby, J.L.; Hoch, M.C. Contributing factors to star excursion balance test performance in individuals with chronic ankle instability. Gait Posture 2015, 41, 912–916. [Google Scholar] [CrossRef]
- Olmsted, L.C.; Carcia, C.R.; Hertel, J.; Shultz, S.J. Efficacy of the Star Excursion Balance Tests in Detecting Reach Deficits in Subjects With Chronic Ankle Instability. J. Athl. Train. 2002, 37, 501–506. [Google Scholar]
- Perry. Gait Analysis: Normal and Pathological Function, 2nd Edition; Slack Incorporated, 2010. ISBN 978-1-55642-766-4.
- Hadadi, M.; Haghighat, F.; Mohammadpour, N.; Sobhani, S. Effects of Kinesiotape vs Soft and Semirigid Ankle Orthoses on Balance in Patients With Chronic Ankle Instability: A Randomized Controlled Trial. Foot Ankle Int. 2020, 41, 793–802. [Google Scholar] [CrossRef]
- Konradsen, L.; Magnusson, P. Increased inversion angle replication error in functional ankle instability. Knee Surg. Sports Traumatol. Arthrosc. 2000, 8, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Alawna, M.; Unver, B.; Yuksel, E. Effect of ankle taping and bandaging on balance and proprioception among healthy volunteers. Sport Sci Health 2021, 17, 665–676. [Google Scholar] [CrossRef]
- Punt, I.M.; Ziltener, J.-L.; Laidet, M.; Armand, S.; Allet, L. Gait and physical impairments in patients with acute ankle sprains who did not receive physical therapy. PM R 2015, 7, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, T.J.; Cordova, M. Mechanical instability after an acute lateral ankle sprain. Arch. Phys. Med. Rehabil. 2009, 90, 1142–1146. [Google Scholar] [CrossRef] [PubMed]
- Kabbaligere, R.; Lee, B.-C.; Layne, C.S. Balancing sensory inputs: Sensory reweighting of ankle proprioception and vision during a bipedal posture task. Gait Posture 2017, 52, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, Q.; Sun, W.; Song, Q. Balancing sensory inputs: somatosensory reweighting from proprioception to tactile sensation in maintaining postural stability among older adults with sensory deficits. Front. Public Health 2023, 11, 1165010. [Google Scholar] [CrossRef] [PubMed]
- Pavailler, S.; Hintzy, F.; Horvais, N.; Forestier, N. Cutaneous stimulation at the ankle: a differential effect on proprioceptive postural control according to the participants' preferred sensory strategy. J. Foot Ankle Res. 2016, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Alawna, M.; Mohamed, A.A. Short-term and long-term effects of ankle joint taping and bandaging on balance, proprioception and vertical jump among volleyball players with chronic ankle instability. Phys. Ther. Sport 2020, 46, 145–154. [Google Scholar] [CrossRef]
- Refshauge, K.M.; Raymond, J.; Kilbreath, S.L.; Pengel, L.; Heijnen, I. The effect of ankle taping on detection of inversion-eversion movements in participants with recurrent ankle sprain. Am. J. Sports Med. 2009, 37, 371–375. [Google Scholar] [CrossRef]
- Refshauge, K.M.; Kilbreath, S.L.; Raymond, J. The effect of recurrent ankle inversion sprain and taping on proprioception at the ankle. Med. Sci. Sports Exerc. 2000, 32, 10–15. [Google Scholar] [CrossRef]
- Spanos, S.; Brunswic, M.; Billis, E. The effect of taping on the proprioception of the ankle in a non-weight bearing position, amongst injured athletes. The Foot 2008, 18, 25–33. [Google Scholar] [CrossRef]
- Jerosch, J.; Hoffstetter, I.; Bork, H.; Bischof, M. The influence of orthoses on the proprioception of the ankle joint. Knee Surg. Sports Traumatol. Arthrosc. 1995, 3, 39–46. [Google Scholar] [CrossRef]
- Thonnard, J.L.; Bragard, D.; Willems, P.A.; Plaghki, L. Stability of the braced ankle. A biomechanical investigation. Am. J. Sports Med. 1996, 24, 356–361. [Google Scholar] [CrossRef]
- Monaghan, K.; Delahunt, E.; Caulfield, B. Ankle function during gait in patients with chronic ankle instability compared to controls. Clin. Biomech. (Bristol, Avon) 2006, 21, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.J.; Liu, W. Possible factors related to functional ankle instability. J. Orthop. Sports Phys. Ther. 2008, 38, 150–157. [Google Scholar] [CrossRef]
- Lohrer, H.; Nauck, T.; Gehring, D.; Wissler, S.; Braag, B.; Gollhofer, A. Differences between mechanically stable and unstable chronic ankle instability subgroups when examined by arthrometer and FAAM-G. J. Orthop. Surg. Res. 2015, 10, 32. [Google Scholar] [CrossRef]
- Hertel, J.; Denegar, C.R.; Buckley, W.E.; Sharkey, N.A.; Stokes, W.L. Effect of rearfoot orthotics on postural sway after lateral ankle sprain. Arch. Phys. Med. Rehabil. 2001, 82, 1000–1003. [Google Scholar] [CrossRef] [PubMed]
- Pourkazemi, F.; Hiller, C.; Raymond, J.; Black, D.; Nightingale, E.; Refshauge, K. Using Balance Tests to Discriminate Between Participants With a Recent Index Lateral Ankle Sprain and Healthy Control Participants: A Cross-Sectional Study. J. Athl. Train. 2016, 51, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.; Dyson, R.; Hale, T.; Abraham, C. Biomechanics of ankle instability. Part 2: Postural sway-reaction time relationship. Med. Sci. Sports Exerc. 2008, 40, 1522–1528. [Google Scholar] [CrossRef]
- Heß, T.; Oehlwein, C.; Milani, T.L. Anticipatory Postural Adjustments and Compensatory Postural Responses to Multidirectional Perturbations-Effects of Medication and Subthalamic Nucleus Deep Brain Stimulation in Parkinson's Disease. Brain Sci. 2023, 13. [Google Scholar] [CrossRef]
- Pintsaar, A.; Brynhildsen, J.; Tropp, H. Postural corrections after standardised perturbations of single limb stance: effect of training and orthotic devices in patients with ankle instability. Br. J. Sports Med. 1996, 30, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Bullock-Saxton, J.E. Local sensation changes and altered hip muscle function following severe ankle sprain. Phys. Ther. 1994, 74, 17–28, discussion 28-31. [Google Scholar] [CrossRef] [PubMed]
- McKeon, P.O.; Hertel, J. Systematic review of postural control and lateral ankle instability, part I: can deficits be detected with instrumented testing. J. Athl. Train. 2008, 43, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.E.; Guskiewicz, K.M. Examination of static and dynamic postural stability in individuals with functionally stable and unstable ankles. Clin. J. Sport Med. 2004, 14, 332–338. [Google Scholar] [CrossRef] [PubMed]
- McCann, R.S.; Crossett, I.D.; Terada, M.; Kosik, K.B.; Bolding, B.A.; Gribble, P.A. Hip strength and star excursion balance test deficits of patients with chronic ankle instability. J. Sci. Med. Sport 2017, 20, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, F.; Moffat, M.; Gutierrez, G. NEUROMUSCULAR CONTROL DURING PERFORMANCE OF A DYNAMIC BALANCE TASK IN SUBJECTS WITH AND WITHOUT ANKLE INSTABILITY. Int. J. Sports Phys. Ther. 2015, 10, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Jaber, H.; Lohman, E.; Daher, N.; Bains, G.; Nagaraj, A.; Mayekar, P.; Shanbhag, M.; Alameri, M. Neuromuscular control of ankle and hip during performance of the star excursion balance test in subjects with and without chronic ankle instability. PLoS One 2018, 13, e0201479. [Google Scholar] [CrossRef] [PubMed]
- Basnett, C.R.; Hanish, M.J.; Wheeler, T.J.; Miriovsky, D.J.; Danielson, E.L.; Barr, J.B.; Grindstaff, T.L. Ankle dorsiflexion range of motion influences dynamic balance in individuals with chronic ankle instability. Int. J. Sports Phys. Ther. 2013, 8, 121–128. [Google Scholar] [PubMed]
- Terada, M.; Harkey, M.S.; Wells, A.M.; Pietrosimone, B.G.; Gribble, P.A. The influence of ankle dorsiflexion and self-reported patient outcomes on dynamic postural control in participants with chronic ankle instability. Gait Posture 2014, 40, 193–197. [Google Scholar] [CrossRef]
- Kosik, K.B.; Johnson, N.F.; Terada, M.; Thomas, A.C.; Mattacola, C.G.; Gribble, P.A. Decreased dynamic balance and dorsiflexion range of motion in young and middle-aged adults with chronic ankle instability. J. Sci. Med. Sport 2019, 22, 976–980. [Google Scholar] [CrossRef]
- Dundas, M.A.; Gutierrez, G.M.; Pozzi, F. Neuromuscular control during stepping down in continuous gait in individuals with and without ankle instability. Journal of Sports Sciences 2014, 32, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Tenenbaum, S.; Chechik, O.; Bariteau, J.; Bruck, N.; Beer, Y.; Falah, M.; Segal, G.; Mor, A.; Elbaz, A. Gait abnormalities in patients with chronic ankle instability can improve following a non-invasive biomechanical therapy: a retrospective analysis. J. Phys. Ther. Sci. 2017, 29, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Gigi, R.; Haim, A.; Luger, E.; Segal, G.; Melamed, E.; Beer, Y.; Nof, M.; Nyska, M.; Elbaz, A. Deviations in gait metrics in patients with chronic ankle instability: a case control study. J. Foot Ankle Res. 2015, 8, 1. [Google Scholar] [CrossRef]
- Spaulding, S.J.; Livingston, L.A.; Hartsell, H.D. The influence of external orthotic support on the adaptive gait characteristics of individuals with chronically unstable ankles. Gait Posture 2003, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Koldenhoven, R.M.; Hart, J.; Saliba, S.; Abel, M.F.; Hertel, J. Gait kinematics & kinetics at three walking speeds in individuals with chronic ankle instability and ankle sprain copers. Gait Posture 2019, 74, 169–175. [Google Scholar] [CrossRef]
- Delahunt, E.; Monaghan, K.; Caulfield, B. Altered neuromuscular control and ankle joint kinematics during walking in subjects with functional instability of the ankle joint. Am. J. Sports Med. 2006, 34, 1970–1976. [Google Scholar] [CrossRef]
- Louwerens, J.W.; van Linge, B.; de Klerk, L.W.; Mulder, P.G.; Snijders, C.J. Peroneus longus and tibialis anterior muscle activity in the stance phase. A quantified electromyographic study of 10 controls and 25 patients with chronic ankle instability. Acta Orthop. Scand. 1995, 66, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Locomotive biomechanics in persons with chronic ankle instability and lateral ankle sprain copers. J. Sci. Med. Sport 2016, 19, 524–530. [Google Scholar] [CrossRef]
- Nyska, M.; Shabat, S.; Simkin, A.; Neeb, M.; Matan, Y.; Mann, G. Dynamic force distribution during level walking under the feet of patients with chronic ankle instability. Br. J. Sports Med. 2003, 37, 495–497. [Google Scholar] [CrossRef]
- Witchalls, J.B.; Waddington, G.; Adams, R.; Blanch, P. Chronic ankle instability affects learning rate during repeated proprioception testing. Phys. Ther. Sport 2014, 15, 106–111. [Google Scholar] [CrossRef]
- Lee, A.J.Y.; Lin, W.-H. Twelve-week biomechanical ankle platform system training on postural stability and ankle proprioception in subjects with unilateral functional ankle instability. Clin. Biomech. (Bristol, Avon) 2008, 23, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Vaes, P.; Duquet, W.; van Gheluwe, B. Peroneal Reaction Times and Eversion Motor Response in Healthy and Unstable Ankles. J. Athl. Train. 2002, 37, 475–480. [Google Scholar] [PubMed]
- Wikstrom, E.A.; Naik, S.; Lodha, N.; Cauraugh, J.H. Bilateral balance impairments after lateral ankle trauma: a systematic review and meta-analysis. Gait Posture 2010, 31, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Hadadi, M.; Abbasi, F. Comparison of the Effect of the Combined Mechanism Ankle Support on Static and Dynamic Postural Control of Chronic Ankle Instability Patients. Foot Ankle Int. 2019, 40, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Baier, M.; Hopf, T. Ankle orthoses effect on single-limb standing balance in athletes with functional ankle instability. Arch. Phys. Med. Rehabil. 1998, 79, 939–944. [Google Scholar] [CrossRef]
- Guskiewicz, K.M.; Perrin, D.H. Effect of orthotics on postural sway following inversion ankle sprain. J. Orthop. Sports Phys. Ther. 1996, 23, 326–331. [Google Scholar] [CrossRef]
- Orteza, L.C.; Vogelbach, W.D.; Denegar, C.R. The effect of molded and unmolded orthotics on balance and pain while jogging following inversion ankle sprain. J. Athl. Train. 1992, 27, 80–84. [Google Scholar]
- Janssen, K.; van den Berg, A.; van Mechelen, W.; Verhagen, E. User Survey of 3 Ankle Braces in Soccer, Volleyball, and Running: Which Brace Fits Best? J. Athl. Train. 2017, 52, 730–737. [Google Scholar] [CrossRef] [PubMed]
- John, C.; Stotz, A.; Gmachowski, J.; Rahlf, A.L.; Hamacher, D.; Hollander, K.; Zech, A. Is an Elastic Ankle Support Effective in Improving Jump Landing Performance, and Static and Dynamic Balance in Young Adults With and Without Chronic Ankle Instability? J. Sport Rehabil. 2020, 29, 789–794. [Google Scholar] [CrossRef]
- Carpes, F.P.; Mota, C.B.; Faria, I.E. On the bilateral asymmetry during running and cycling - a review considering leg preference. Phys. Ther. Sport 2010, 11, 136–142. [Google Scholar] [CrossRef]
- Helme, M.; Tee, J.; Emmonds, S.; Low, C. Does lower-limb asymmetry increase injury risk in sport? A systematic review. Phys. Ther. Sport 2021, 49, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, E.S.; Nicolopoulos, C.; Anderson, E.G.; Curran, M.; Athanasopoulos, S. The role of ankle bracing in injury prevention, athletic performance and neuromuscular control: A review of the literature. The Foot 2005, 15, 1–6. [Google Scholar] [CrossRef]
Figure 1.
Fine coordination and proprioception test; A) Hardware: Foot pedal for inversion and eversion movements of the ankle joint; B) Software: Target sine wave (solid black line) which gets traced by a random subject, which was wearing the bandage (dashed grey line). The grey box indicates the analysed area, in which the mean deviation between both signals was calculated.
Figure 1.
Fine coordination and proprioception test; A) Hardware: Foot pedal for inversion and eversion movements of the ankle joint; B) Software: Target sine wave (solid black line) which gets traced by a random subject, which was wearing the bandage (dashed grey line). The grey box indicates the analysed area, in which the mean deviation between both signals was calculated.
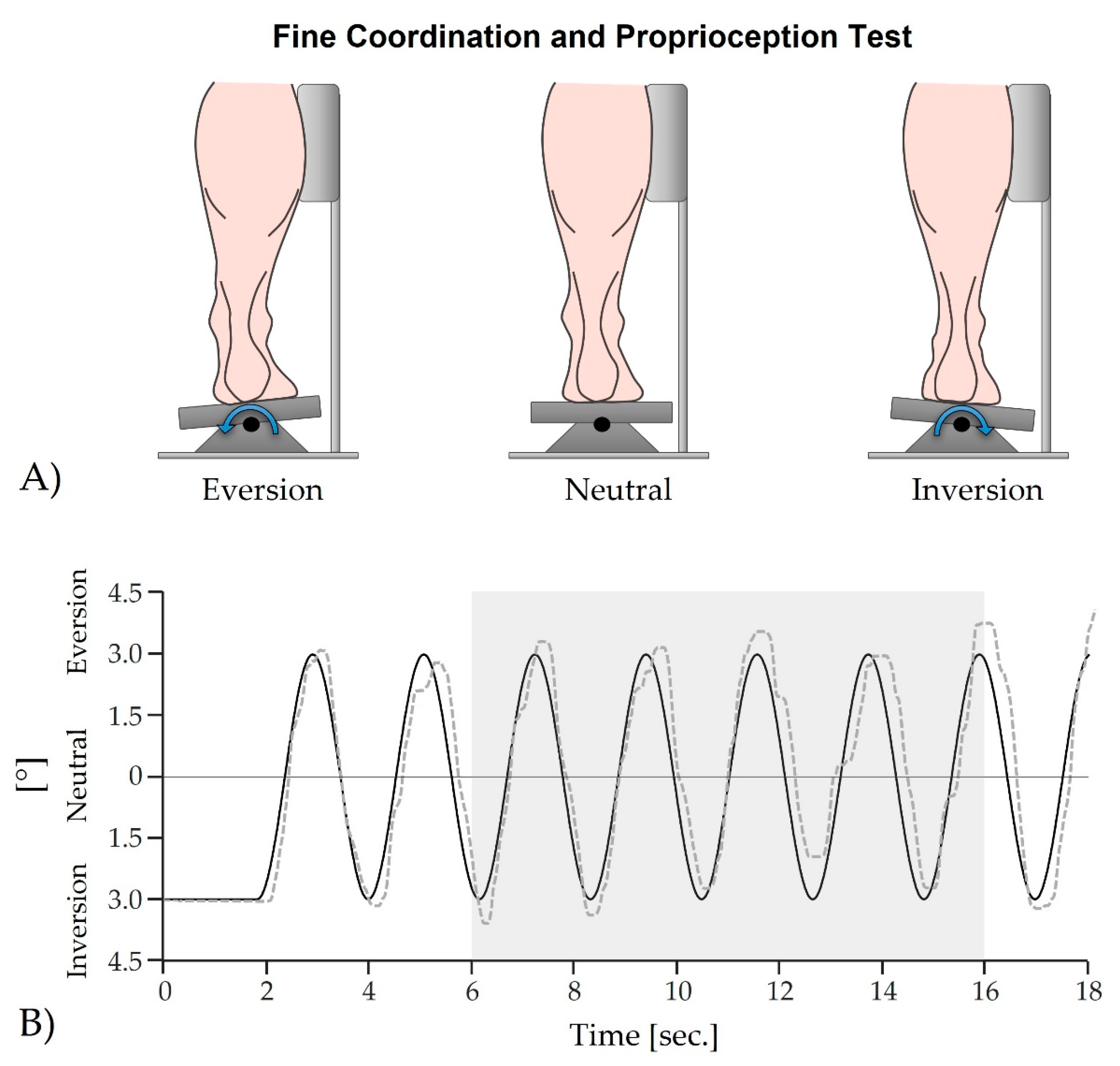
Figure 2.
Illustration of an actual vertical ground reaction force curve during walking from a random subject. The black solid line indicates the curve of the ground reaction force for the injured leg with a bandage, while the grey dashed line indicates the curve for the healthy leg. Shown are the first peak, corresponding to the loading response, and the second peak, corresponding to the terminal stance phase of the gait cycle [50]. The illustration also displays the relative duration of the single stance phase and both double stance phases (grey area). Note that for the statistical analysis, the relative double stance phase is the sum of both the initial and terminal double stance phases.
Figure 2.
Illustration of an actual vertical ground reaction force curve during walking from a random subject. The black solid line indicates the curve of the ground reaction force for the injured leg with a bandage, while the grey dashed line indicates the curve for the healthy leg. Shown are the first peak, corresponding to the loading response, and the second peak, corresponding to the terminal stance phase of the gait cycle [50]. The illustration also displays the relative duration of the single stance phase and both double stance phases (grey area). Note that for the statistical analysis, the relative double stance phase is the sum of both the initial and terminal double stance phases.
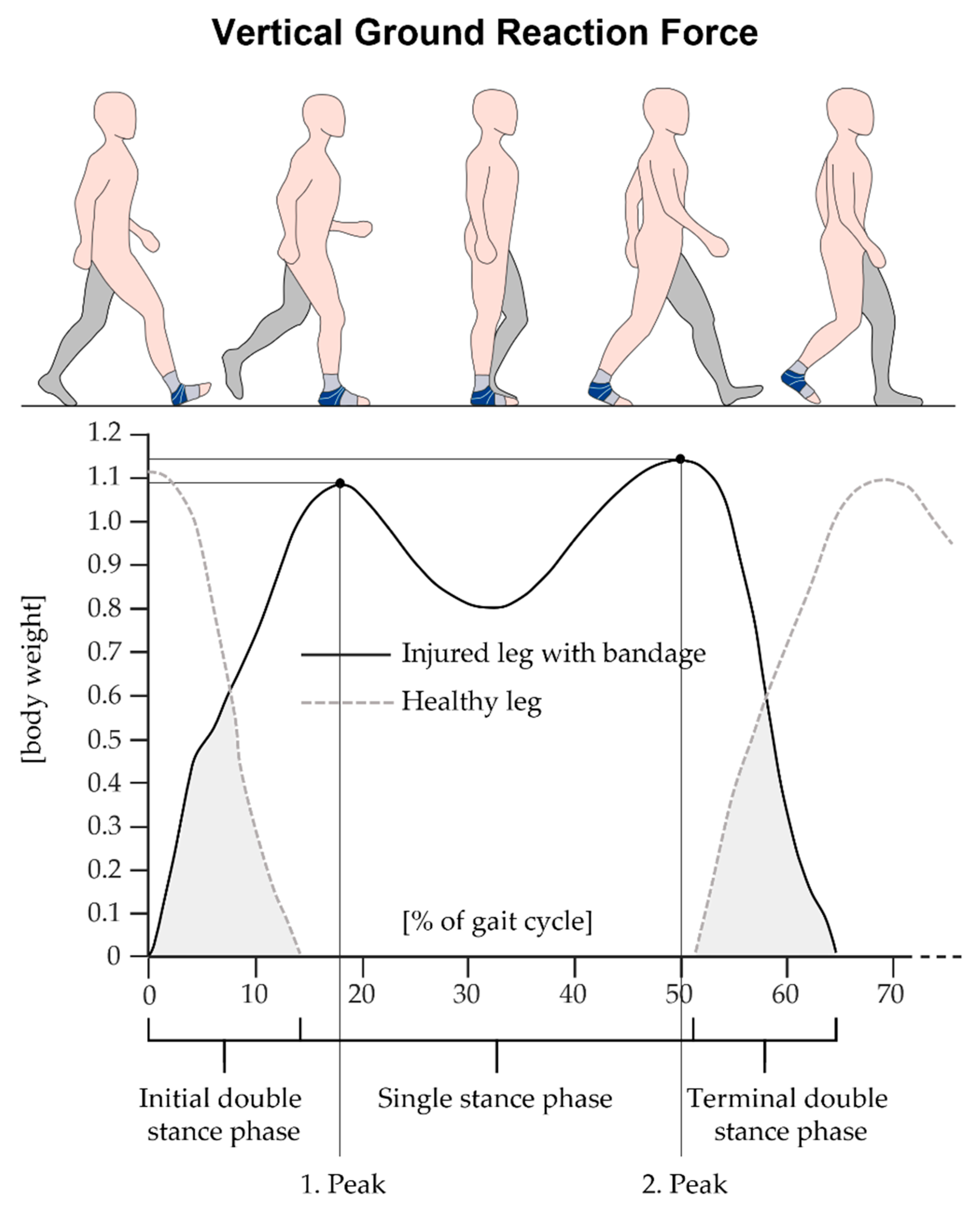
Figure 3.
Self-ranked improvements due to wearing the bandage, data presented as percentage of n.
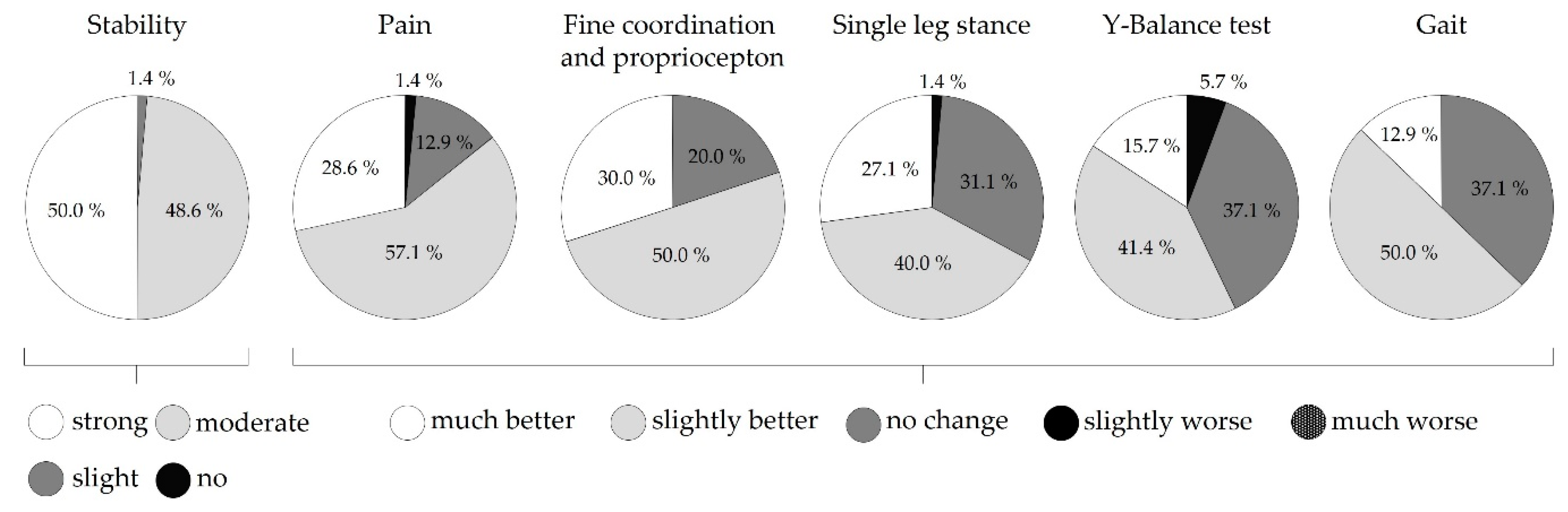
Figure 4.
Comparisons of the three Y-Balance test directions between all three conditions healthy stance leg, injured stance leg without and with bandage. Data presented as percentage of the leg length. The cross additionally marks the mean value.
Figure 4.
Comparisons of the three Y-Balance test directions between all three conditions healthy stance leg, injured stance leg without and with bandage. Data presented as percentage of the leg length. The cross additionally marks the mean value.
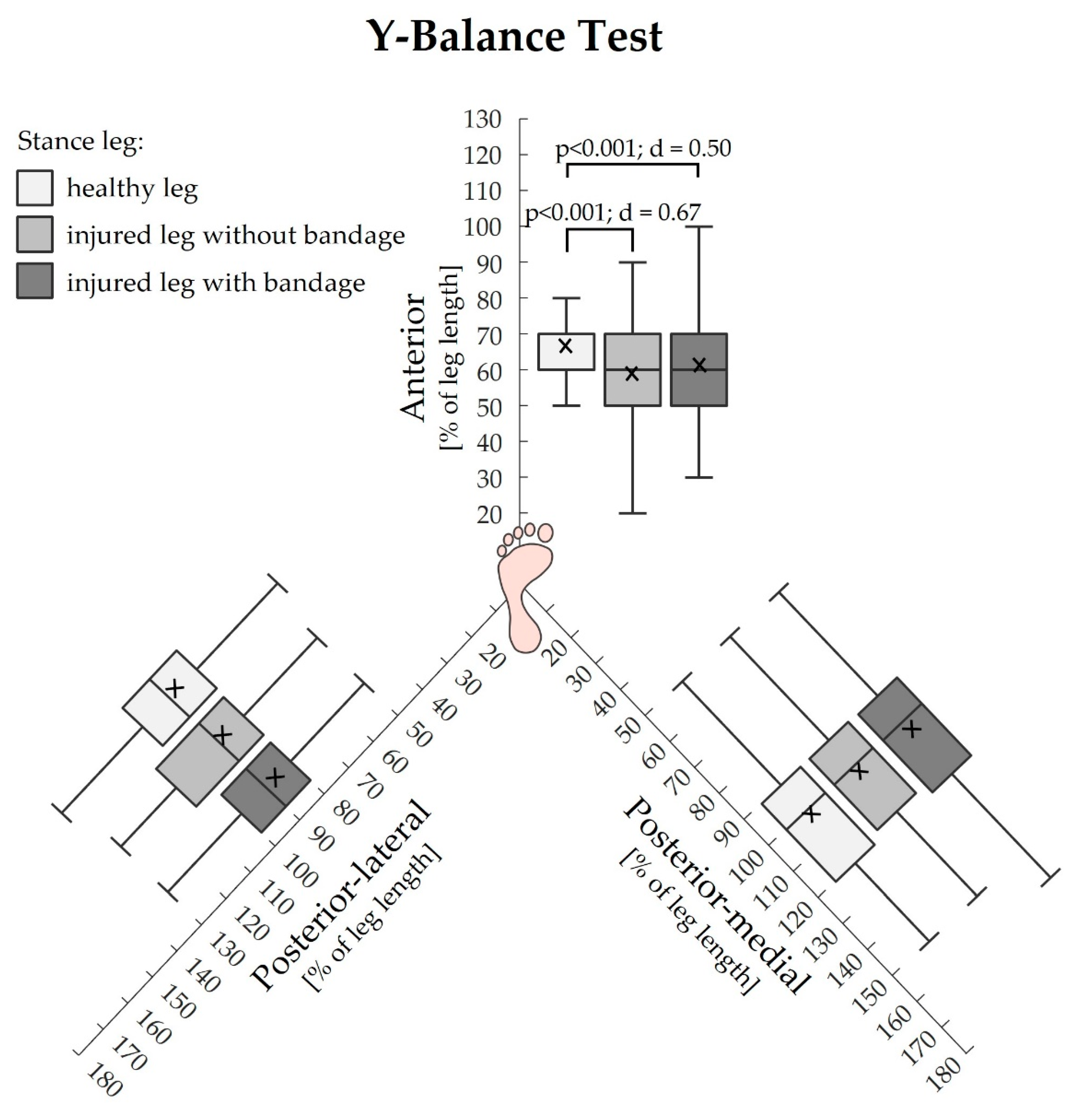

Table 1.
Demographic and clinical data (structures of the ankle joint with pressure pain), presented as mean ± SD.
Table 1.
Demographic and clinical data (structures of the ankle joint with pressure pain), presented as mean ± SD.
| Age [years] | Height [cm] |
Weight [kg] |
Gender | Side of the injured leg |
Pain rating |
Instability rating |
|---|---|---|---|---|---|---|
| 34.8±11.8 | 173.3±10.1 | 78.7±16.4 | male 36; female 34 | left 32; right 38 | 1.6 ± 1.3 | 3.0 ± 2.2 |
| Injured structures of the ankle joint | n | Relative n to total number of subjects (70) [%] | ||||
| Anterior talofibular ligament | 54 | 84.4 | ||||
| Posterior talofibular ligament | 31 | 48.4 | ||||
| Calcaneofibular ligament | 38 | 59.4 | ||||
| Swelling | 53 | 82.8 | ||||
| General complaints | 61 | 95.3 | ||||
Table 2.
Self-rated pain perception of the injured ankle joint (visual analogue scale from 0 to 10). Data are presented as mean ± SD, minimum and maximum.
Table 2.
Self-rated pain perception of the injured ankle joint (visual analogue scale from 0 to 10). Data are presented as mean ± SD, minimum and maximum.
| pain | walking barefoot | standing barefoot | walking in shoes | standing in shoes | walking with bandage | standing with bandage |
|---|---|---|---|---|---|---|
| mean ± SD | 1.60 ± 1.58 | 1.13 ± 1.45 | 1.69 ± 1.45 | 1.09 ± 1.27 | 1.18 ± 1.46 | 0.88 ± 1.25 |
| range [Min Max] |
[0 7] | [0 7] | [0 6] | [0 5] | [0 6] | [0 6] |
Table 3.
Comparison of the deviation value between the target sine wave and the signal drawn by the subjects between all three conditions healthy leg, injured leg with and without bandage. Data presented as mean ± SD.
Table 3.
Comparison of the deviation value between the target sine wave and the signal drawn by the subjects between all three conditions healthy leg, injured leg with and without bandage. Data presented as mean ± SD.
| Parameter | healthy leg |
Injured leg without bandage | Injured leg with bandage | p-value | d |
|---|---|---|---|---|---|
| Mean deviation [°] | 1.30 ± 0.5 | 1.26 ± 0.5 | 1.20 ± 0.5 | 0.078 | - |
Table 4.
Comparison of the COP parameters between all three conditions healthy leg, injured leg with and without bandage. Data presented as mean ± SD.
Table 4.
Comparison of the COP parameters between all three conditions healthy leg, injured leg with and without bandage. Data presented as mean ± SD.
| Parameter | healthy leg |
Injured leg without bandage | Injured leg with bandage | p-value | d |
|---|---|---|---|---|---|
| COP length [mm] | 470.0 ± 115.9 a |
548.8 ± 145.1 a;b |
477.5 ± 106.7 b |
< 0.001 a < 0.001 b < 0.001 |
1.1 a 0.60 b 0.56 |
| COP 95% confidence area [mm²] | 217.6 ± 101.5 | 238.2 ± 91.1 | 216.3 ± 79.0 | 0.263 | - |
Table 5.
Intra-group and inter-group comparisons (between the healthy leg and the injured leg for the conditions walking with and without bandage) of the spatial-temporal and kinetic gait parameters. Data are presented as mean ± SD.
Table 5.
Intra-group and inter-group comparisons (between the healthy leg and the injured leg for the conditions walking with and without bandage) of the spatial-temporal and kinetic gait parameters. Data are presented as mean ± SD.
| Parameter | Walking injured leg without bandage | Walking injured leg with bandage | p-value | d | ||
|---|---|---|---|---|---|---|
| gait velocity [km/h] | 3.98 ± 0.67 | 4.01±0.59 | 0.251 | - | ||
| rel. double stance phase [% of gait cycle] |
29.17 ± 4.20 | 29.46 ± 4.22 | 0.121 | - | ||
| Parameter | healthy leg |
Injured leg without bandage | healthy leg |
Injured leg with bandage | p-value | d |
| rel. single stance phase [% of gait cycle] |
65.3 ± 2.7 a |
64.1 ± 2.5 a;b |
65.4 ± 3.2 c |
64.7 ± 2.9 b;c |
a < 0.001 b 0.018 c 0.013 |
a 0.46 b 0.22 c 0.24 |
| step length [cm] | 57.7 ± 6.1 a;b |
61.1 ± 7.8 a |
61.1 ± 8.5 b |
61.0 ± 7.3 |
a < 0.001 b < 0.001 |
a 0.49 b 0.46 |
| 1. Peak of the vertical force [body weight] |
1.07 ± 0.07 a |
1.05 ± 0.06 a;b |
1.07 ± 0.07 |
1.07 ± 0.07 b |
a 0.004 b 0.004 |
a 0.31 b 0.31 |
| 2. Peak of the vertical force [body weight] |
1.11 ± 0.07 a;b |
1.08 ± 0.07 b;c |
1.13 ± 0.06 a;d |
1.11 ± 0.06 c;d |
a 0.039 b < 0.001 c < 0.001 d 0.001 |
a 0.31 b 0.43 c 0.33 d 0.31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



