
Submitted:
31 May 2024
Posted:
03 June 2024
You are already at the latest version
Abstract
Abstract: Background: In 2021, two randomized controlled trials (RCTs), TheraP and VISION, demonstrated that 177Lu-PSMA-617 as monotherapy was more effective for enhancing the decline of PSA than the comparator third-line treatments. Methods: Our review summarizes new RCTs that add to the use of radioligand therapy (RLT) for patients with high-risk prostate cancer (PCa). Results: Five past and present RCTs include 1139 patients. A RCT, ENZA-p, studied first-line treatment of patients with metastatic castration-resistant PCa (mCRPC). A combination of enzalutamide (ENZA) and 177Lu-PSMA-617 gave longer progression-free survival than ENZA as monotherapy. Other RCTs of patients with mCRPC, including the PSMAfore, and SPLASH trials, showed 177Lu-PSMA-617 as second-line treatment gave better progression-free survival than androgen receptor pathway inhibitors (combined p value 6 x 10-8). Conclusion: Patients with PCa may gain if they are given PSMA-RLT early in the treatment of PCa and as part of combination therapies.
Keywords:
combination therapy
; nuclear medicine
; prostate neoplasm
; prostate specific membrane antigen
; randomized controlled trials
1. Introduction
Prostate cancer (PCa) is a frequent male cancer and has the highest cancer mortality among men next to lung cancer. So efforts to reduce the mortality are important. Pilot trials of neoadjuvant treatment with two androgen receptor pathway inhibitors (ARPIs), enzalutamide (ENZA) and darolutamide, reported positive results [1,2]. Neoadjuvant treatment can reduce the five-year risk of PSA relapse (PSAR, biochemical recurrence, BCR) after the routine initial treatments with up to 50%.
Without neoadjuvant treatments, up to half of the patients who initially are treated with radical prostatectomy (RP) or radiation therapy (RT) recurs. The first phase of recurrence is PSA relapse (PSAR, biochemical recurrence, BCR), as indicated in Figure 1. The second phase is non-metastatic PCa (nmPC). For patients with nmPC, a combination of androgen deprivation therapy (ADT) and androgen receptor pathway inhibitors (ARPIs) prolongs recurrence-free survival more than ADT as the only treatment [3,4,5,6].
After ADT, the next phase is metastatic castration-resistant PCa (mCRPC). In real-world analyses. first-line treatment for two thirds of the patients with mCRPC was ARPIs (especially ENZA or abiraterone (ABI)), and docetaxel (DOC) for a sixth to a third of the patients [7,8]. The CARD trial is a RCT that investigated third-line treatment of patients with mCRPC who had failed to docetaxel (DOC) and an ARPI [9]. Patients given cabazitaxel (CABA) lived longer than those given a second ARPI: median 13 months versus 11 months, respectively. Real-world studies of third-line treatment confirmed that CABA gives a better outcome than a second ARPI [10,11].
A trend for treatment is early use of drugs that are effective as third-line treatments [12]. RCTs for patients with mCRPC supported doublets of ADT and ARPI [13] and triplets of ADT, ARPI, and DOC. For patients with metastatic hormone-sensitive PCa (mHSPC), RCTs support adding DOC to the doublet of ADT and ARPI.
Another development is PSMA-based theranostics [14,15]. Two RCTs, TheraP and VISION, of patients with mCRPC studied [177Lu]Lu-PSMA-617 as third-line treatment [14,15,16]. 177Lu-PSMA-617 increased the rate of patients with PSA decline > 50% relative to the rate of PSA decline after the control treatments. The 177Lu-PSMA-617 groups in the two trials lived grossly similarly, as shown in Figure 2. Many aspects can optimize PSMA-RLT for patients with PCa [17].
[225Act]Act-PSMA-RLT is more effective than [177Lu]Lu-PSMA-RLT but increases adverse effects such as xerostomia [18,19]. To reduce adverse effect of 225Act-PSMA-RLT, nuclear medicine specialists developed tandem PSMA-RLT [20]. It combines cycles with reduced activity of 225Act-PSMA-RLT with reduced activity of 177Lu-PSMA-RLT. A study compared tandem treatment with 177Lu-PSMA-617 monotherapy [21]. The tandem treatment gave a significantly higher rate of PSA decline than the monotherapy. Another study of tandem PSMA-RLT reported adverse effects of saliva glands remained a challenge [22].
Our review aims to highlight recent promising RCTs of patients with high-risk PCa.
2. Material and Methods
We searched for relevant RCTs from 2021 to March 2024 in Google scholar and PubMed. We included original studies of PSMA-RLT based on small molecules, published in English. We included published trials and trials presented at major conferences. We included trials irrespective of the phase of PCa and number of patients. We excluded RCTs where PSMA-RLT was combined with non-established drugs, RCTs that addressed only bone metastases, and RCT without reported results. We used rate of PSA decline >50%, radiologic progression-free survival, and overall survival (OS) as effect measures.
Patients included in our RCTs had positive sites on PSMA PET/CT. Our RCTs followed the European Association for Nuclear Medicine (EANM) guidelines for PSMA-RLT [23]. The RCTs recorded adverse effects according to the Common Terminology Criteria for Adverse Effects (CTCAE).
We calculated a combined p value based on the individual p values of the trials in STATA using the method of Tobias [24].
3. Recent RCTs
Table 1 shows the selected trials. A RCT reported that combining abiraterone (ABI) and PSMA-RLT gave a better outcome than PSMA-RLT monotherapy [25]. The combination can give a long-lasting complete remission [26]. The RCT ENZA-p of first-line treatment of high-risk patients with mCRPC compared a combination of ENZA and 177Lu-PSMA-617 with ENZA monotherapy [27]. 83 patients were given the combination, and 79 patients were given ENZA monotherapy. With the combination, more patients had a PSA decline > 50% than patients had after ENZA monotherapy: 93% versus 78%, respectively, hazard ratio (HR) = 0.43, p < 0.001. Patients given the combination lived longer free of PSAR than patients given ENZA monotherapy (median 13 months versus 7.8 months, respectively, p < 0.0001). The rates of PSA decline >50% were higher in the ENZA-p trial than in the TheraP and VISION trials, as shown in Figure 3, A randomized non-inferiority trial compared PSMA-RLT and DOC as second-line treatments [28].
Other important RCTs were presented at major conferences from 2022 to 2024. The European Society of Medical Oncology (ESMO) conference in Madrid, Spain, October 2023 presented the PSMAfore trial (NCT04689838)[29]. The trial is an open-label prospective multicenter RCT of second-line treatment of patients with PSMA-PET/CT-positive mCRPC. The control treatment is a second ARPI. After the patients had been informed that third-line CABA treatment prolongs life more than a second ARPI, all preferred to be treated in the trial.[30]
The patients had failed ARPIs, mainly ABI and ENZA. The trial enrolled 468 patients, and compared the outcomes after 177Lu-PSMA-617 and a second ARPI. Patients treated with 177Lu-PSMA-617 lived longer without radiological progression than patients treated with a second-line ARPI: median 12 months versus 5.6 months, respectively, HR = 0.41, p < 0.0001. The rates of complete radiographic response were 21% and 2.6%, respectively. Most control patients who failed on the second ARPI were later given 177Lu-PSMA-617. Severe, grade 3/4, adverse effects were infrequent.
4. Discussion
Our review provides perspectives on recent progress in treatment of PCa. We selected five important RCTs of PSMA-RLT that investigate 1139 patients. Two trials documented the efficacy of combining 177Lu-PSMA-617 with ARPIs [25,27]. As first-line treatment, the ENZA-p RCT showed a combination of ENZA and 177Lu-PSMA-617 increased the effect of ENZA [27], and the Suman RCT of second-line treatment showed that a combination of ABI and 177Lu-PSMA-617 increased OS relative to that of 177Lu-PSMA-617 monotherapy [25]. The two trials argue for combining PSMA-RLT with ARPI. Another study reported real-world data on 177Lu-PSMA-617 as first line treatment [32].
Our RCTs are in accordance with recommendations of the Prostate Cancer clinical trials Working Group 3 (PCWG3)[12]. It recommends that drugs that are effective as third-line treatment (such as 177Lu-PSMA-617) should be investigated in earlier phases of PCa. The ENZA-p trial illustrates two promising concepts for PSMA-RLT: early use and use combined with other drugs. The two concepts add to those detailed in a previous review on optimizing PSMA-RLT for the patients with PCa [17].
The TheraP and VISION trials showed that PSMA-RLT as third-line monotherapy is as effective as other drugs, but has fewer severe adverse effects [14,15]. The following RCTs show that first- and second-line treatment with PSMA-RLT improved outcomes, so the efficacy is a class-phenomenon.
The European Association of Nuclear Medicine carried out a Focus 5 conference in Granada, Spain, in 2023 [33]. Leading experts at the conference reported consensus regarding PSMA-RLT for patients with advanced PCa. Another review summarized 13 ongoing trials of PSMA RLT [34]. The trials combined 177Lu-PSMA RLT with established and non-established drugs. Complementarily, our review summarizes findings of RCTs of PSMA-RLT in an early phase of PCa.
Other studies also supported early use of 177Lu-PSMA-617. Retrospective studies and a meta-analysis showed that DOC-naive patients given second-line monotherapy with 177Lu-PSMA-617 lived longer than DOC-failing patients given third-line monotherapy with 177Lu-PSMA-617, as shown in Figure 4 [35,36,37]. The publications summarized 739 DOC-naïve patients and 1910 DOC-failing patients. DOC-naïve patients lived median up to one year longer than DOC-failing patients. A randomized non-inferiority trial compared PSMA-RLT and DOC as second-line treatments [28].
In accordance with the FDA approval of 177Lu-PSMA RLT, the PSMAfore trial includes PSMA RLT as relapse treatment for the control patients after they had failed to the second ARPI. So the trial does not indicate whether 177Lu-PSMA-617 has impact on OS. Sartor et al. defended the priority of the trial for radiographic progression-free survival [30]. Radiographic progression-free survival may be a more relevant study endpoint than rate of PSA decline >50%.
The study design is important for the conclusion of RCTs. Regarding third-line treatment with 177Lu-PSMA-RLT, the VISION trial showed that 177Lu-PSMA-617 significantly improved OS in contrast to the conclusion of the TheraP trial [15,16]. The difference reflects the selection criteria for the control groups. 177Lu-PSMA-617 gave grossly similar OS in the two trials, whereas the control group in the TheraP trial survived longer than the control group in the VISION trial, as shown in Figure 2. Correspondingly, the CARD trial found that third-line treatment with CABA prolonged OS compared with a second ARPI [9].
177Lu-PSMA-617 is especially effective for subgroups of patients with mCRPC. Oligometastatic PCa is an interesting subgroup of patients with metastatic PCa. Retrospective studies showed that oligometastatic patients treated with PSMA-RLT lived impressively long [38]. Further, treated with PSMA-RLT, other retrospective studies showed that patients with only lymph node metastases (LNM) lived longer than patients with bone, lung, and liver metastases [39,40]. Treated with PSMA-RLT, docetaxel (DOC)-naïve LNM patients lived longer free of PSAR than LNM patients who had failed to DOC [41].
A challenge for PSMA-RLT is that some PSMA PET/CT-positive patients do not respond to the treatment [42]. Resistance to RLT may have a background in molecular biology [43]. A study indicated that androgen receptor gene amplification has a role for the resistance [44]. Similarly, some patients are resistant to radiation therapy. Many studies have investigated molecular mechanisms for the radiotherapy-resistance [45]. But it remains to be shown whether mechanisms leading to resistance to PSMA-RLT are similar to those for resistance to radiation therapy.
Recent progress of PCa has implications for management of the patients. The terms “first-line, second-line, and third-line treatment” reflect previous routines of patients with mCRPC as a sequence of monotherapies. Only half of the patients with mCRPC who failed to first-line treatment underwent a second-line treatment, and only half of the patients who failed to second-line treatment underwent a third-line treatment [8,10]. Now increasingly patients with mCRPC are treated with doublets or triplets. So future trials should categorize patients according to previous treatments with ARPIs and taxane chemotherapies irrespective of the “line of treatment”.
Increasingly, patients undergo staging and restaging with PSMA PET/CT. Where units have access to PSMA PET/CT, more than half of the patients undergo initial staging with PSMA PET/CT and nearly all patient with PSAR undergo restaging with PSMA PET/CT. The development motivates a shift from TNM staging based on conventional imaging (cT, cN, cM) to staging with PSMA PET/CT as miT, miN, and miM. based on positive findings in the prostate bed, lymph nodes, and distant organs [46]. Compared with the stage based on conventional imaging, stage based on PSMA PET/CT is closer to the pathologic stage (pT, pN, pM), the gold standard reference.
Neoadjuvant treatment has a growing role in oncology. Neoadjuvant treatment is effective for patients with breast cancer [47], non-small-cell lung cancer [48], muscle-invasive urinary bladder cancer [49], and rectal cancer [50]. Neoadjuvant treatment of patients with high-risk PCa is not similarly established. Neoadjuvant ADT was ineffective [51,52], but ENZA and darolutamide are more effective than ADT. DOC may add to the effect of ADT on radiation therapy [52]. A recent meta-analysis summarized state-of-the-art for neoadjuvant treatments in prostate cancer [53]. Two pilot trials indicated 177Lu-PSMA-617 is effective as neoadjuvant treatment [54,55]. As neoadjuvant treatment, 177Lu-PSMA-617 had a brilliant impact on OS, as demonstrated in Figure 5.
[161Tb]Tb is another effective radioisotope for PSMA-RLT of patients with PCa [56]. Mice models of PCa have shown that [161Tb]Tb-PSMA-RLT is more effective than [177Lu]Lu-PSMA-RLT. In two case reports of patients with mCRPC, treatment with [161Tb]Tb-PSMA-RLT gave promising results [57,58]. New trials further investigate the efficacy of [161Tb]Tb-PSMA-RLT [59,60].
Our review has strengths and limitations. As strength, our review points out that PSMA theranostics is a rapidly expanding field. The trials gave consistent positive findings. As limitations, the US Federal Drug Administration (FDA) approved only one radioligand, 177Lu-PSMA-167, as third-line monotherapy of patients with mCRPC. Despite major international conferences have presented our RCTs, journals have published two of the trials only as conference abstracts. Patients with BRAC2 mutations is a subgroup of patients. They may be treated with a PARP inhibitor, such as olaparib. A RCT, LuPARP, trial investigates a combination of PSMA RLT and olaparib [61].
5. Conclusion
Patients with PCa may gain from treatments that use PSMA-RLT in an early phase of the cancer, and use PSMA-RLT combined with other established drugs.
6. Future Directions
Based on the ENZA-p trial a question is: would neoadjuvant treatment of high-risk PCa patients be more effective than first-line treatment of patients with mCRPC? Another question is: would a combination of ADT, ENZA, and 177Lu-PSMA-617 for patients with mHSPC be more effective than a combination of ENZA and 177Lu-PSMA-617 for patients with mCRPC? Protocols for trials that investigate the questions is being developed.
Authors contributions
Conceptualization; FEvE. Data retrieval, data analyses, figures, statistics, and first draft: FEvE. Data interpretation, supervision: IV and RB. All authors have read and agreed to the published version of the review. All authors have read and approved the cover letter.
Funding
The review received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
List of Abbreviations
| ABI | abiraterone |
| Act | Actinium |
| ADT | androgen deprivation therapy |
| ARPI | androgen receptor pathway inhibitor |
| BCR | Biochemical recurrence |
| CABA | cabazitaxel |
| CT | computed tomography |
| DOC | docetaxel |
| ENZA | enzalutamide |
| ENZA-P | randomized controlled phase 2 trial of the combination of enzalutamide and PSMA-based radioligand therapy |
| ESMO | European Society of Medical Oncology |
| LNM | lymph node metastases |
| Lu | lutetium |
| mCRPC | metastatic castration-resistant prostate cancer |
| mHSPC | metastatic hormone-sensitive prostate cancer |
| nmCRPC | nonmetastatic prostate cancer |
| OS | overall survival |
| PCa | prostate cancer |
| PCWG3 | Prostate cancer clinical trial working group 3 |
| PET | positron emission tomography |
| PSA | prostate specific antigen |
| PSAR | prostate specific antigen relapse |
| PSMA | prostate specific membrane antigen |
| Ra | Radium |
| RCT | randomized controlled trial |
| RLT | radioligand therapy |
| rPFS | radiological progression-free survival |
| Tb | Terbium |
References
- Montgomery, B.; Tretiakova, M.S.; Joshua, A.M.; Gleave, M.E.; Fleshner, N.; Bubley, G.J.; Mostaghel, E.A.; Chi, K.N.; Lin, D.W.; Sanda, M.; et al. Neoadjuvant Enzalutamide Prior to Prostatectomy. Clin. Cancer Res. 2017, 23, 2169–2176. [Google Scholar] [CrossRef]
- McKay, R.R.; Ye, H.; Xie, W.; Lis, R.; Calagua, C.; Zhang, Z.; Trinh, Q.D.; Chang, S.L.; Harshman, L.C.; Ross, A.E.; et al. Evaluation of Intense Androgen Deprivation Before Prostatectomy: A Randomized Phase II Trial of Enzalutamide and Leuprolide With or Without Abiraterone. J. Clin. Oncol. 2019, 37, 923–931. [Google Scholar] [CrossRef]
- Fizazi, K.; Shore, N.; Tammela, T.L.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; Kuss, I.; et al. Darolutamide in Nonmetastatic, Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2019, 380, 1235–1246. [Google Scholar] [CrossRef]
- Attard, G.; Murphy, L.; Clarke, N.W.; Cross, W.; Jones, R.J.; Parker, C.C.; Gillessen, S.; Cook, A.; Brawley, C.; Amos, C.L.; et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022, 399, 447–460. [Google Scholar] [CrossRef]
- Small, E.J.; Saad, F.; Chowdhury, S.; Oudard, S.; Hadaschik, B.A.; Graff, J.N.; Olmos, D.; Mainwaring, P.N.; Lee, J.Y.; Uemura, H.; et al. Apalutamide and overall survival in non-metastatic castration-resistant prostate cancer. Ann. Oncol. 2019, 30, 1813–1820. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Fizazi, K.; Saad, F.; Shore, N.D.; De Giorgi, U.; Penson, D.F.; Ferreira, U.; Efstathiou, E.; Madziarska, K.; Kolinsky, M.P.; et al. Enzalutamide and Survival in Nonmetastatic, Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2197–2206. [Google Scholar] [CrossRef]
- Anton, A.; Pillai, S.; Semira, M.C.; Wong, S.; Shapiro, J.; Weickhardt, A.; Azad, A.; Kwan, E.M.; Spain, L.; Gunjur, A.; et al. Real-world first-line systemic therapy patterns in metastatic castration-resistant prostate cancer. BJUI Compass. 2022, 3, 205–213. [Google Scholar] [CrossRef]
- George, D.J.; Sartor, O.; Miller, K.; Saad, F.; Tombal, B.; Kalinovsky, J.; Jiao, X.; Tangirala, K.; Sternberg, C.N.; Higano, C.S. Treatment Patterns and Outcomes in Patients With Metastatic Castration-resistant Prostate Cancer in a Real-world Clinical Practice Setting in the United States. Clin. Genitourin. Cancer 2020, 18, 284–294. [Google Scholar] [CrossRef]
- de Wit, R.; de Bono, J.; Sternberg, C.N.; Fizazi, K.; Tombal, B.; Wulfing, C.; Kramer, G.; Eymard, J.C.; Bamias, A.; Carles, J.; et al. Cabazitaxel versus abiraterone or enzalutamide in metastatic prostate cancer. N. Engl. J. Med. 2019, 381, 2506–2518. [Google Scholar] [CrossRef]
- Freedland, S.J.; Davis, M.; Epstein, A.J.; Arondekar, B.; Ivanova, J.I. Real-world treatment patterns and overall survival among men with Metastatic Castration-Resistant Prostate Cancer (mCRPC) in the US Medicare population. Prostate Cancer Prostatic Dis. 2023. [Google Scholar] [CrossRef]
- de Wit, R.; Freedland, S.J.; Oudard, S.; Marinov, G.; Capart, P.; Combest, A.J.; Peterson, R.; Ozatilgan, A.; Morgans, A.K. Real-world evidence of patients with metastatic castration-resistant prostate cancer treated with cabazitaxel: comparison with the randomized clinical study CARD. Prostate Cancer Prostatic Dis. 2023, 26, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1410. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; de Almeida Luz, M.; De Giorgi, U.; Gleave, M.; Gotto, G.T.; Pieczonka, C.M.; Haas, G.P.; Kim, C.S.; Ramirez-Backhaus, M.; Rannikko, A.; et al. Improved outcomes with enzalutamide in biochemically recurrent prostate cancer. N. Engl. J. Med. 2023, 389, 1453–1465. [Google Scholar] [CrossRef] [PubMed]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Buteau, J.P.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; et al. Overall survival with [(177)Lu]Lu-PSMA-617 versus cabazitaxel in metastatic castration-resistant prostate cancer (TheraP): secondary outcomes of a randomised, open-label, phase 2 trial. Lancet Oncol 2024, 25, 99–107. [Google Scholar] [CrossRef] [PubMed]
- von Eyben, F.E.; Bauman, G.; von Eyben, R.; Rahbar, K.; Soydal, C.; Haug, A.R.; Virgolini, I.; Kulkarni, H.; Baum, R.; Paganelli, G. Optimizing PSMA radioligand therapy for patients with metastatic castration-resistant prostate cancer. A systematic review and meta-analysis. Int. J. Mol. Sci. 2020, 21, 9054. [Google Scholar] [CrossRef] [PubMed]
- Parida, G.K.; Panda, R.A.; Bishnoi, K.; Agrawal, K. Efficacy and Safety of Actinium-225 Prostate-Specific Membrane Antigen Radioligand Therapy in Metastatic Prostate Cancer: A Systematic Review and Metanalysis. Med. Princ. Pract. 2023, 32, 178–191. [Google Scholar] [CrossRef]
- Sathekge, M.M.; Lawal, I.O.; Bal, C.; Bruchertseifer, F.; Ballal, S.; Cardaci, G.; Davis, C.; Eiber, M.; Hekimsoy, T.; Knoesen, O.; et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): a multicentre, retrospective study. Lancet Oncol. 2024, 25, 175–183. [Google Scholar] [CrossRef]
- Khreish, F.; Ebert, N.; Ries, M.; Maus, S.; Rosar, F.; Bohnenberger, H.; Stemler, T.; Saar, M.; Bartholoma, M.; Ezziddin, S. (225)Ac-PSMA-617/(177)Lu-PSMA-617 tandem therapy of metastatic castration-resistant prostate cancer: pilot experience. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 721–728. [Google Scholar] [CrossRef]
- Banda, A.; Prive, B.M.; Allach, Y.; Uijen, M.J.K.; Peters, S.M.B.; Loeff, C.C.; Gotthardt, M.; Muselaers, C. .J.; Witjes, J.A.; van Oooprt, I.M.; et al. PSMA-RLT in Patients with Metastatic Hormone-Sensitive Prostate Cancer: A Retrospective Study. Cancers 2023, 15, 297. [Google Scholar] [CrossRef]
- Langbein, T.; Kulkarni, H.R.; Schuchardt, C.; Mueller, D.; Volk, G.F.; Baum, R.P. Salivary Gland Toxicity of PSMA-Targeted Radioligand Therapy with (177)Lu-PSMA and Combined (225)Ac- and (177)Lu-Labeled PSMA Ligands (TANDEM-PRLT) in Advanced Prostate Cancer: A Single-Center Systematic Investigation. Diagnostics 2022, 12, 1986. [Google Scholar] [CrossRef]
- Kratochwil, C.; Fendler, W.P.; Eiber, M.; Hofman, M.S.; Emmett, L.; Calais, J.; Osborne, J.R.; Iravani, A.; Koo, P.; Lindenberg, L.; et al. Joint EANM/SNMMI procedure guideline for the use of (177)Lu-labeled PSMA-targeted radioligand-therapy ((177)Lu-PSMA-RLT). Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 2830–2845. [Google Scholar] [CrossRef]
- Tobias, A. Meta-analysis of p values. Stata Technical Bulletin 1999, 49, 15–17. [Google Scholar]
- Suman, S.; Parghane, R.V.; Joshi, A.; Prabhash, K.; Talole, S.; Basu, S. Combined 177Lu-PSMA-617 PRLT and abiraterone acetate versus 177Lu-PSMA-617 PRLT monotherapy in metastatic castration-resistant prostate cancer. An observational study comparing the response and durability. Prostate 2021, 81, 1225–1234. [Google Scholar] [CrossRef] [PubMed]
- Parker, D.; Zambelli, J.; Lara, M.K.; Wolf, T.H.; McDonald, A.; Lee, E.; Abou-Elkacem, L.; Gordon, E.J.; Baum, R.P. Case Report: long-term complete response to PSMA-targeted radioligand therapy and abiraterone in a metastatic prostate cancer patient. Front. Oncol. 2023, 13, 1192792. [Google Scholar] [CrossRef] [PubMed]
- Emmett, L.; Subramaniam, S.; Crumbaker, M.; Nguyen, A.; Joshua, A.M.; Weickhardt, A.; Lee, S.T.; Ng, S.; Francis, R.J.; Goh, J.C.; et al. [(177)Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): an open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2024, 25, 563–571. [Google Scholar] [CrossRef]
- Satapathy, S.; Mittal, B.R.; Sood, A.; Das, C.K.; Mavuduru, R.S.; Goyal, S.; Shukla, J.; Singh, S.K. (177)Lu-PSMA-617 versus docetaxel in chemotherapy-naive metastatic castration-resistant prostate cancer: a randomized, controlled, phase 2 non-inferiority trial. Eur. J. Nucl. Med. Mol. Imaging 2021, 49, 1754–1764. [Google Scholar] [CrossRef] [PubMed]
- Sartor, O.C.; Castellano Gauna, D.E.; Herman, K.; de Bono, J.S.; Shore, N.D.; Chi, K.N.N.; Crosby, N.; Piulats Rodriguez, J.M.; Flechon, A.; et al. LBA13 phase 3 trial of [177Lu]Lu-PSMA-617 in taxane-naive patients with metastatic castration-resistant prostate cancer (PSMAfore. Ann. Oncol. 2023, 34, S1324–S1325. [Google Scholar] [CrossRef]
- Sartor, O.; Fizazi, K.; Herrmann, K.; Morris, M.J. Design Considerations in the PSMAfore Trial. J. Nucl. Med. 2024, 65, 226–227. [Google Scholar] [CrossRef]
- Hansen, A.R.; Probst, S.; Tulane, R.F.; Osman, M.M.; Delpassand, E.S.; Viglianti, B.L.; Michalski, J.; Beauregard, J.-M.-; Oz, O.K.; Courtney, K.; et al. 1400P Efficacy and Safety of 177Lu PNT2002 Prostate-Specific Membrane Antigen (PSMA) Therapy in Metatatic Castration-Resistant Prostate Cancer (mCRPC) Initial Results from SPLASH. Ann. Oncol. 2022, 33, S1185. [Google Scholar] [CrossRef]
- Satapathy, S.; Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Bal, C. [(177)Lu]Lu-PSMA-617 as first-line systemic therapy in patients with metastatic castration-resistant prostate cancer: a real-world study. Eur. J. Nucl. Med. Mol. Imaging 2024. [Google Scholar] [CrossRef]
- Oprea-Lager, D.E.; MacLennan, S.; Bjartell, A.; Briganti, A.; Burger, I.A.; de Jong, I.; De Santis, M.; Eberlein, U.; Emmett, L.; Fizazi, K.; et al. European Association of Nuclear Medicine Focus 5: Consensus on Molecular Imaging and Theranostics in Prostate Cancer. Eur. Urol. 2024, 85, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Mattana, F.; Muraglia, L.; Barone, A.; Colandrea, M.; Saker Diffalah, Y.; Provera, S.; Cascio, A.S.; Omodeo Sale, E.; Ceci, F. Prostate-Specific Membrane Antigen-Targeted Therapy in Prostate Cancer: History, Combination Therapies, Trials, and Future Perspective. Cancers 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Barber, T.W.; Singh, A.; Kulkarni, H.R.; Niepsch, K.; Billah, B.; Baum, R.P. Clinical outcomes of (177)Lu-PSMA radioligand therapy in earlier and later phases of metastatic castration-resistant prostate cancer grouped by previous taxane chemotherapy. J. Nucl, Med. 2019, 60, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Rahbar, K.; Baum, R.P.; Seifert, R.; Kessel, K.; Bogemann, M.; Kulkarni, H.R.; Zhang, J.; Gerke, C.; Fimmers, R.; et al. Prior therapies as prognostic factors of overall survival in metastatic castration-resistant prostate cancer patients treated with [(177)Lu]Lu-PSMA-617. A WARMTH multicenter study (the 617 trial). Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 113–122. [Google Scholar] [CrossRef]
- Satapathy, S.; Sahoo, R.K.; Bal, C. [(177)Lu]Lu-PSMA-radioligand therapy efficacy outcomes in taxane-naive versus taxane-treated patients with metastatic castration-resistant prostate cancer: a systematic review and metaanalysis. J, Nucl, Med, 2023, 64, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Mader, N.; Schoeler, C.; Pezeshkpour, N.; Klimek, K.; Groener, D.; Happel, C.; Tselis, N.; Mandel, P.; Grunwald, F.; Sabet, A. Intermittent radioligand therapy with (177)Lu-PSMA-617 for oligometastatic castration-resistant prostate cancer. Cancers 2023, 15, 4605. [Google Scholar] [CrossRef] [PubMed]
- Edler von Eyben, F.; Singh, A.; Zhang, J.; Nipsch, K.; Meyrick, D.; Lenzo, N.; Kairemo, K.; Joensuu, T.; Virgolini, I.; Soydal, C.; et al. (177)Lu-PSMA radioligand therapy of predominant lymph node metastatic prostate cancer. Oncotarget 2019, 10, 2451–2461. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Kulkarni, H.R.; Baum, R.P. Metastatic extent predicts survival as patients with metastatic castration-resistant prostate cancer are treated with (177)Lu-PSMA radioligand therapy. Theranostics 2020, 10, 4900–4902. [Google Scholar] [CrossRef]
- Yaxley, W.J.; McBean, R.; Wong, D.; Grimes, D.; Vasey, P.; Frydenberg, M.; Yaxley, J.W. Should Lutetium-prostate specific membrane antigen radioligand therapy for metastatic prostate cancer be used earlier in men with lymph node only metastatic prostate cancer? Investig. Clin. Urol. 2021, 62, 650–657. [Google Scholar] [CrossRef]
- Kostos, L.; Buteau, J.P.; Hofman, M.S.; Azad, A.A. Determinants of outcome following PSMA-based radioligand therapy and mechanisms of resistance in patients with metastatic castration-resistant prostate cancer. Ther. Adv. Med. Oncol. 2023, 15, 17588359231179309. [Google Scholar] [CrossRef]
- Stuparu, A.D.; Capri, J.R.; Meyer, C.A.L.; Le, T.M.; Evans-Axelsson, S.L.; Current, K.; Lennox, M.; Mona, C.E.; Fendler, W.P.; Calais, J.; et al. Mechanisms of Resistance to Prostate-Specific Membrane Antigen-Targeted Radioligand Therapy in a Mouse Model of Prostate Cancer. J. Nucl. Med. 2021, 62, 989–995. [Google Scholar] [CrossRef]
- De Giorgi, U.; Sansovini, M.; Severi, S.; Nicolini, S.; Monti, M.; Gurioli, G.; Foca, F.; Casadei, C.; Conteduca, V.; Celli, M.; et al. Circulating androgen receptor gene amplification and resistance to (177)Lu-PSMA-617 in metastatic castration-resistant prostate cancer: results of a Phase 2 trial. Br. J, Cancer 2021, 125, 1226–1232. [Google Scholar] [CrossRef]
- Chaiswing, L.; Weiss, H.L.; Jayswal, R.D.; Clair, D.K.S.; Kyprianou, N. Profiles of Radioresistance Mechanisms in Prostate Cancer. Crit. Rev. Oncog. 2018, 23, 39–67. [Google Scholar] [CrossRef]
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed miTNM Classification for the Interpretation of PSMA-Ligand PET/CT. J. Nucl. Med. 2018, 59, 469–478. [Google Scholar] [CrossRef]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.R.; Brahmer, J.R.; Swanson, S.J.; et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef]
- Roviello, G.; Catalano, M.; Santi, R.; Santoni, M.; Galli, I.C.; Amorosi, A.; Polom, W.; De Giorgi, U.; Nesi, G. Neoadjuvant Treatment in Muscle-Invasive Bladder Cancer: From the Beginning to the Latest Developments. Front. Oncol. 2022, 12, 912699. [Google Scholar] [CrossRef]
- Horesh, N.; Freund, M.R.; Garoufalia, Z.; Gefen, R.; Nagarajan, A.; Suarez, E.; Emile, S.H.; Wexner, S.D. Total Neoadjuvant Therapy Is a Predictor for Complete Pathological Response in Patients Undergoing Surgery for Rectal Cancer. J. Gastrointest. Surg. 2022, 26, 2579–2584. [Google Scholar] [CrossRef]
- Schulman, C.C.; Debruyne, F.M.; Forster, G.; Selvaggi, F.P.; Zlotta, A.R.; Witjes, W.P. 4-Year follow-up results of a European prospective randomized study on neoadjuvant hormonal therapy prior to radical prostatectomy in T2-3N0M0 prostate cancer. European Study Group on Neoadjuvant Treatment of Prostate Cancer. Eur. Urol. 2000, 38, 706–713. [Google Scholar] [CrossRef]
- Carles, J.; Gallardo, E.; Domenech, M.; Font, A.; Bellmunt, J.; Figols, M.; Mellado, B.; Saez, M.I.; Suarez, C.; Mendez, M.J.; et al. Phase 2 Randomized Study of Radiation Therapy and 3-Year Androgen Deprivation With or Without Concurrent Weekly Docetaxel in High-Risk Localized Prostate Cancer Patients. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 344–352. [Google Scholar] [CrossRef]
- Perera, M.B.; Beech, B.B.; De Jesus Escano, M.; Gmelich, C.; Yip, Y.; Boorjan, S.A.; Eastham, J. Neoadjuvant Systemic Therapy Prior to Radical Prostatectomy for Clinically Localized High-Risk Prostate Cancer. Front. Oncol. 2022. [Google Scholar] [CrossRef]
- Eapen, R.S.; Buteau, J.P.; Jackson, P.; Mitchell, C.; Oon, S.F.; Alghazo, O.; McIntosh, L.; Dhiantravan, N.; Scalzo, M.J.; O'Brien, J.; et al. Administering [(177)Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localised Prostate Cancer (LuTectomy): A Single-centre, Single-arm, Phase 1/2 Study. Eur. Urol. 2024, 85, 217–226. [Google Scholar] [CrossRef]
- Golan, S.; Frumer, M.; Zohar, Y.; Rosenbaum, E.; Yakimov, M.; Kedar, D.; Margel, D.; Baniel, J.; Steinmetz, A.P.; Groshar, D.; et al. Neoadjuvant (177)Lu-PSMA-I&T Radionuclide Treatment in Patients with High-risk Prostate Cancer Before Radical Prostatectomy: A Single-arm Phase 1 Trial. Eur. Urol. Oncol. 2023, 6, 151–159. [Google Scholar]
- Muller, C.; van der Meulen, N.P.; Schibli, R. Opportunities and potential challenges of using terbium-161 for targeted radionuclide therapy in clinics. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 3181–3184. [Google Scholar] [CrossRef]
- Baum, R.P.; Singh, A.; Kulkarni, H.R.; Bernhardt, P.; Ryden, T.; Schuchardt, C.; Gracheva, N.; Grundler, P.V.; Koster, U.; Muller, D.; et al. First-in-Humans Application of (161)Tb: A Feasibility Study Using (161)Tb-DOTATOC. J. Nucl. Med, 2021, 62, 1391–1397. [Google Scholar] [CrossRef]
- Schaefer-Schuler, A.; Burgard, C.; Blickle, A.; Maus, S.; Petrescu, C.; Petto, S.; Bartholoma, M.; Stemler, T.; Ezziddin, S.; Rosar, F. [(161)Tb]Tb-PSMA-617 radioligand therapy in patients with mCRPC: preliminary dosimetry results and intra-individual head-to-head comparison to [(177)Lu]Lu-PSMA-617. Theranostics 2024, 14, 1829–1840. [Google Scholar] [CrossRef]
- Al-Ibraheem, A.; Scott, A.M. (161)Tb-PSMA Unleashed: a Promising New Player in the Theranostics of Prostate Cancer. Nucl. Med. Mol, Imaging 2023, 57, 168–171. [Google Scholar] [CrossRef]
- Budeau, J.P.; Kostos, A.; Aliiour, R.; Jackson, P.; McIntouch, L.; Emmerson, P.; Husted, M.B.; et al. VIOLET: A phase I/II trial evaluation of radioligand treatment in men with metastatic castration-resistant prostatecancer with [161Tb]Tb-PSMA I&T. J. Clin. Oncol. 2023, 41 (suppl), TPS281. [Google Scholar]
- Sandhu, S.L.; Josha, A.; Emmett, L.; Crumbaker, M.A.; Bressel, M.; Huynh, R.; Banks, P.; Wallace, R.; Hemd, D.; Interjeeh, A.; et al. LuPARP: Phase 1 trial of 177Lu-PSMA-617 and olaparib in patients with metastatic castration resistant prostate cancer (mCRPPC). J. Clin. Oncol. 2023; 41 (Suppl). [Google Scholar]
Figure 1.
Flow scheme of phases of prostate cancer. The figure shows the phases from PSA relapse (PSAR), over non-metastatic PCa (nmPC), to metastatic castration-resistant PCa (mCRPC). The Figure shows the established monotherapies for the phases of recurrent PCa. Today most often first-line routine treatment of mCRPC (1. Line) is an androgen receptor pathway inhibitor (ARPI). Second-line treatment (2. Line) most often is docetaxel (DOC), and third-line treatment (3. Line) is cabazitaxel (CABA). Five randomized controlled trials (RCT) of PSMA-RLT, including VISION, TheraP, and ENZA-p, are reported in full length publications and are shown with a green background [14,15,27]. Two other RCTs, PSMAfore and SPLASH , have been presented at major international conferences. The presented RCTs are shown with a yellow background.
Figure 1.
Flow scheme of phases of prostate cancer. The figure shows the phases from PSA relapse (PSAR), over non-metastatic PCa (nmPC), to metastatic castration-resistant PCa (mCRPC). The Figure shows the established monotherapies for the phases of recurrent PCa. Today most often first-line routine treatment of mCRPC (1. Line) is an androgen receptor pathway inhibitor (ARPI). Second-line treatment (2. Line) most often is docetaxel (DOC), and third-line treatment (3. Line) is cabazitaxel (CABA). Five randomized controlled trials (RCT) of PSMA-RLT, including VISION, TheraP, and ENZA-p, are reported in full length publications and are shown with a green background [14,15,27]. Two other RCTs, PSMAfore and SPLASH , have been presented at major international conferences. The presented RCTs are shown with a yellow background.
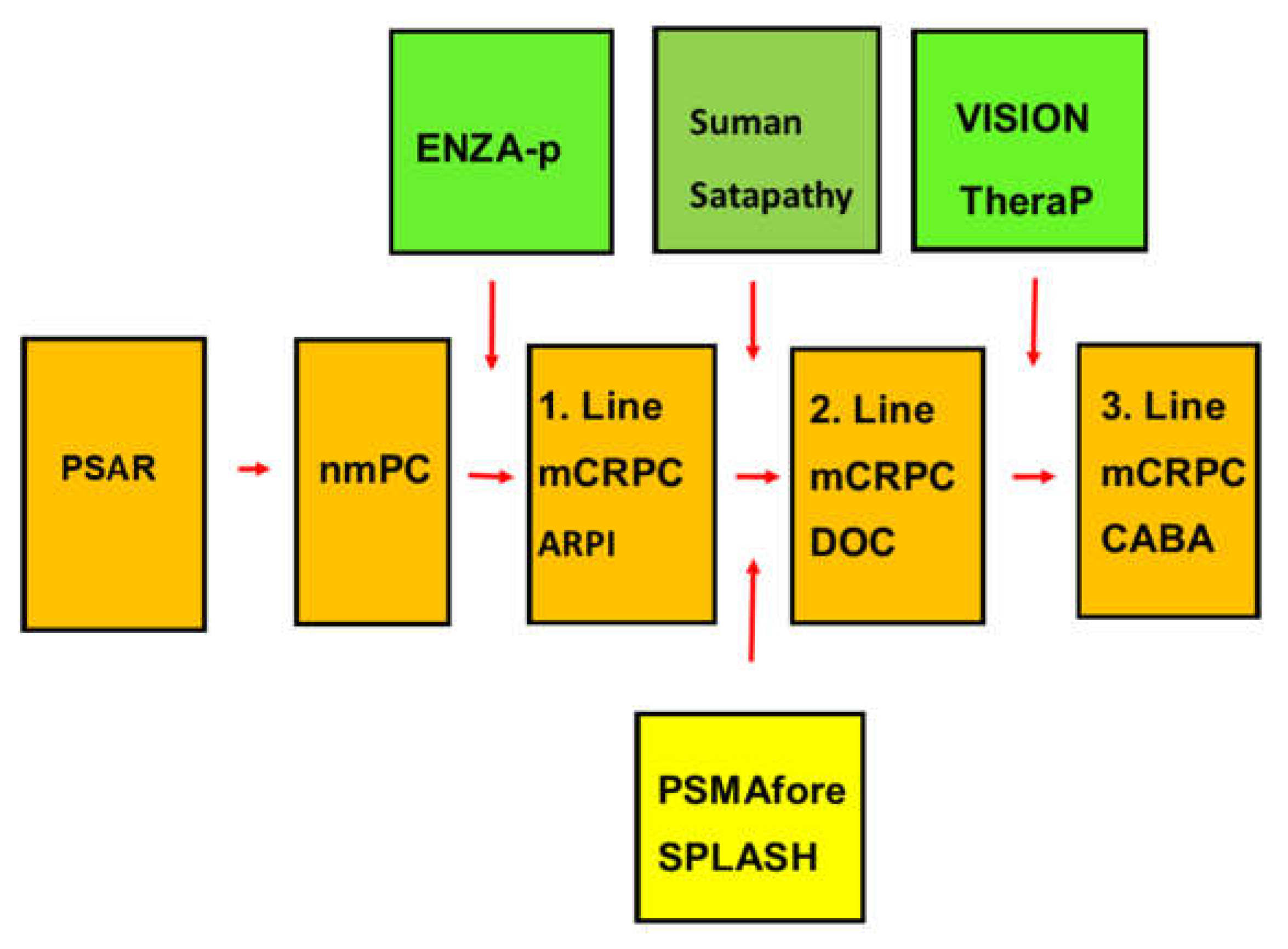
Figure 2.
Overall survival (OS) for the TheraP and the VISION trials. The VISION trial showed that the PSMA-RLT group had a significantly better OS than the control group in contrast to the TheraP trial. However, the PSMA-RLT groups in the two trials had a grossly similar OS whereas the CABA treated control group in the TheraP trial (TheraP CABA) had a much better OS than the non-cabazitaxel control group in the VISION trial (VISION non-CABA).
Figure 2.
Overall survival (OS) for the TheraP and the VISION trials. The VISION trial showed that the PSMA-RLT group had a significantly better OS than the control group in contrast to the TheraP trial. However, the PSMA-RLT groups in the two trials had a grossly similar OS whereas the CABA treated control group in the TheraP trial (TheraP CABA) had a much better OS than the non-cabazitaxel control group in the VISION trial (VISION non-CABA).
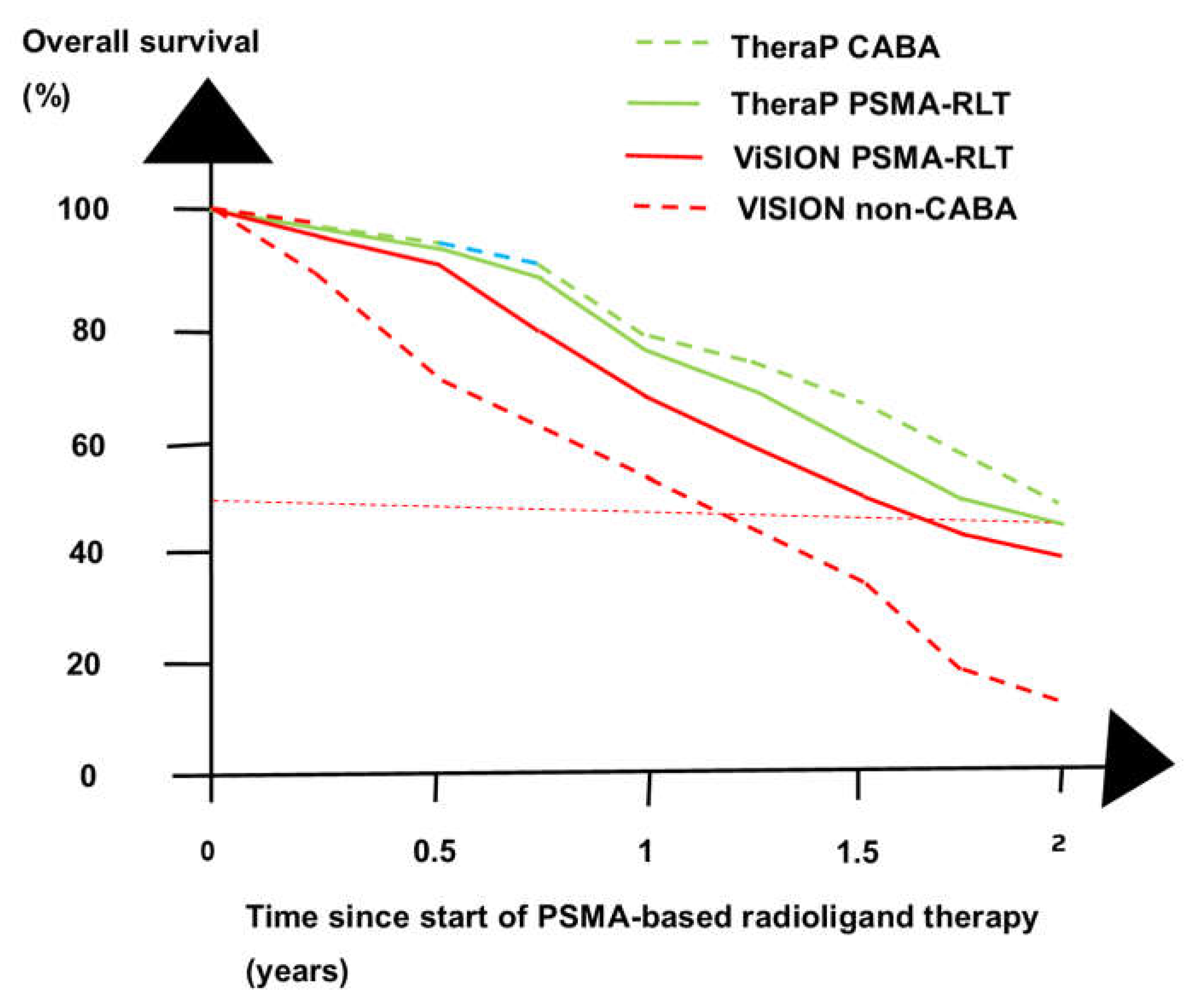
Figure 3.
Rate of PSA decline >50% in the VISION, TheraP, and the ENZA-p randomized controlled trials [14,15,27]. The patients given PSMA-based radioligand therapy (RLT) had a higher rate of PSA decline than the control patients (CONTROL).
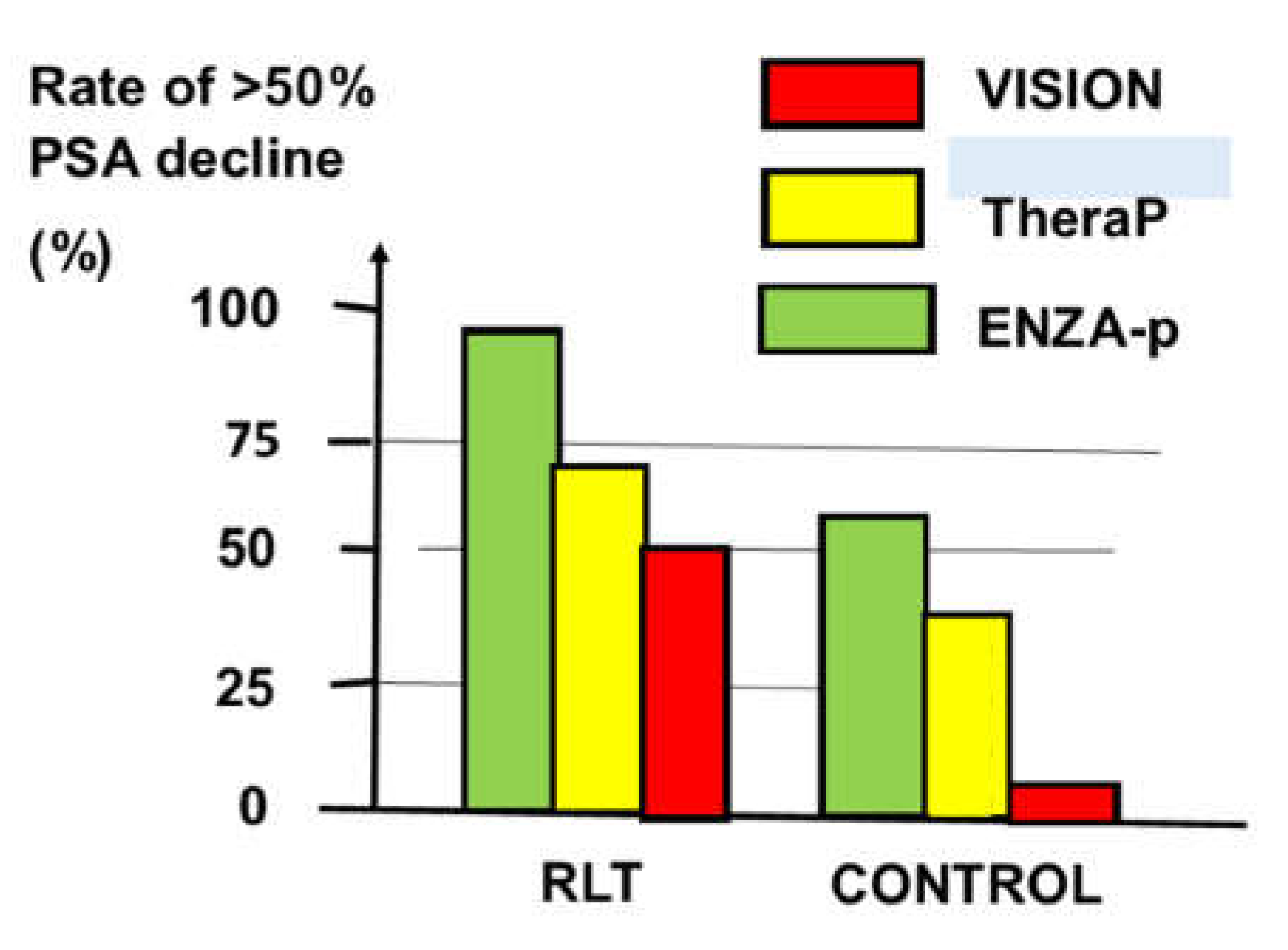
Figure 4.
Overall survival (OS) in two retrospective studies of patients treated with [177Lu]Lu-PSMA-617 . Patients treated with second-line PSMA-RLT (2. line) lived longer than patients treated with third-line PSMA RFLT.(3. line). The figure shows the Barber study [35] with stippled lines and the Ahmadzadehfar (WARMTH) study [36] with full lines. The figure shows PSMA-RLT as second-line treatment of taxane-naive patients with green lines and PSMA-RLT as third-line treatment of patients with failure to docetaxel with red lines.
Figure 4.
Overall survival (OS) in two retrospective studies of patients treated with [177Lu]Lu-PSMA-617 . Patients treated with second-line PSMA-RLT (2. line) lived longer than patients treated with third-line PSMA RFLT.(3. line). The figure shows the Barber study [35] with stippled lines and the Ahmadzadehfar (WARMTH) study [36] with full lines. The figure shows PSMA-RLT as second-line treatment of taxane-naive patients with green lines and PSMA-RLT as third-line treatment of patients with failure to docetaxel with red lines.
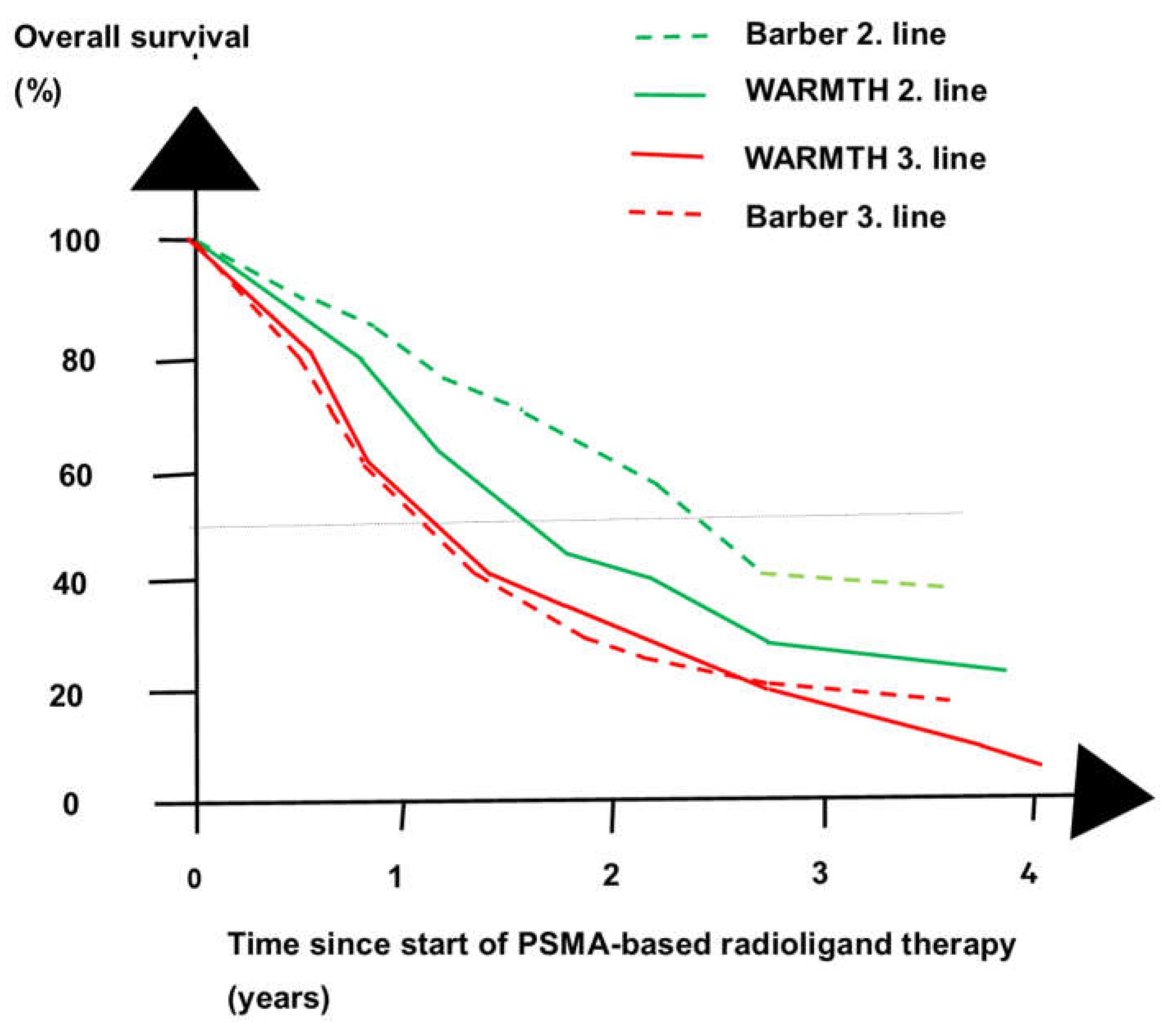
Figure 5.
Overall survival (OS) for radioligand therapy in three phases of prostate cancer. PSMA-RLT gave a better OS as neoadjuvant treatment than as second-line (2. line) and third-line (3. line) treatment of patients with metastatic castration-resistant prostate cancer.
Figure 5.
Overall survival (OS) for radioligand therapy in three phases of prostate cancer. PSMA-RLT gave a better OS as neoadjuvant treatment than as second-line (2. line) and third-line (3. line) treatment of patients with metastatic castration-resistant prostate cancer.
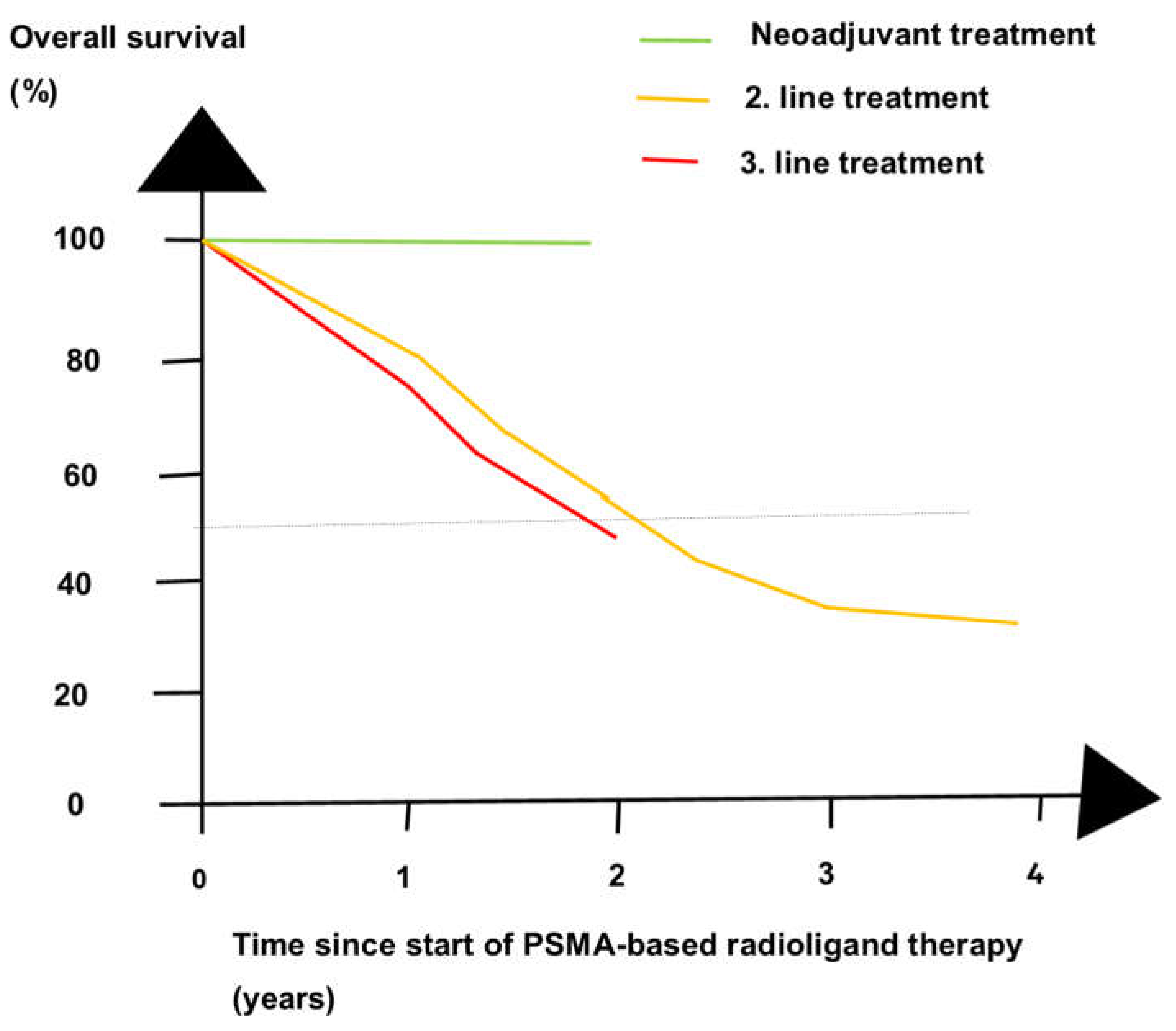

Table 1.
RCTs investigating PSMA-RLT in PCa patients.
| Phase of Treatment |
Author/NCT Number | Reference | Name of Trial |
Type of RLT | No of Patients |
|---|---|---|---|---|---|
| First-line treatment | Emmett 2024 | [27] | ENZA-p | PSMA-617 | 162 |
| Second-line treatment | Suman 2021 | [25] | NR | PSMA-617 | 58 |
| NCT04689838 | [29] | PSMAfore | PSMA-617 | 467 | |
| Hansen 2022 | [31] | SPLASH | PSMA I&T | 412 | |
| Satapathy 2023 | [28] | NR | 40 | ||
| Overall total | 1139 |
The table counts the enrolled or planned enrolled number of PCa patients in the RCTs of PSMA RLT. For one RCT, the table refers to the trial number that is registered at ClinicalTrials.gov. Abbreviaion: NR = not reported.
Table 2.
Radiological progression-free survival gain with PSMA-RLT in the RCTs.
| Trial | Reference | Radiological Progression Free Survival (Months) |
Hazard Ratio | Single p Value | Combined p Value |
|---|---|---|---|---|---|
| PSMAfore | [29] | 12 vs. 5.6 | 0.41 | <0.0001 | |
| Suman | [25] | >18 vs. 7 | NR | <0.0005 | |
| SPLASH | [31] | 9.5 vs. 6 | 0.71 | 0.0088 | |
| Combined | 6 x 10−8 |
Abbreviation NR = not reported.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



