
Submitted:
04 June 2024
Posted:
04 June 2024
You are already at the latest version
Abstract
(1) Background: This study aims to investigate differences in the perspectives of exercise intensity for resistance exercise of healthcare professionals (HCPs) and adults living with spinal cord injury (SCI) in Asian countries. Also, it verifies the appropriateness of the conventional indicators for resistance exercise intensity in an Asian context; (2) Methods: 121 certified HCPs and 107 adults with SCI participated in a survey conducted in Indonesian, Japanese, Korean and Thai languages. The survey asked what principles are important for prescribing resistance exercise, and if ‘moderate’ and ‘vigorous’ were appropriate terms for indicating an intensity level. Perspective differences were examined between both groups and, further, between countries from a psychosocial perspective; (3) Results: Of the HCPs, 92% perceived that resistance exercise intensity was far more important than frequency, time or type of exercise while frequency (61%) followed by intensity (58%) was perceived as important by respondents with SCI. Only Japanese respondents with SCI agreed with HCP’s perception of intensity. Both HCPs and respondents with SCI showed unfavorable responses on the usage of ‘moderate’ and ‘vigorous’ for describing resistance exercise intensity, especially Japanese HCP and respondents with SCI from Indonesia; (4) Conclusion: Our findings suggest that non-HCPs must improve their perceptions of exercise intensity. Findings also suggest the need for more explicit and user-friendly terms or expressions indicating the level of intensity in a local (Asian) context.
Keywords:
resistance exercise
; intensity
; Asia
; moderate
; vigorous
1. Introduction
Adults with spinal cord injury (SCI) should be encouraged to participate in physical activities including aerobic exercise [1,2,3] to benefit physical health including reducing risk of chronic disease, improving body functional independence, social reintegration and psychological health [4,5]. For those benefits, most studies have focused on aerobic exercise for people with SCI but resistance exercise is also regarded as a crucial training to improve muscle strength, endurance, power output and muscle mass [1,6]. This improves fitness and metabolic health too [1,2].
Among various systematic reviews and meta-analyses reviewing the benefits of exercise for persons with SCI [7,8,9], an international multidisciplinary team undertook a systematic review to develop evidence-based exercise guidelines for adults with SCI helping to improving cardiorespiratory fitness, muscle strength and cardiometabolic health [2,10]. This Scientific Exercise Guidelines for Adults with Spinal Cord Injury (SEG-SCI) describe the minimum dose of aerobic and resistance exercises for those aged 18-64 with chronic SCI levelled C3 and below [11,12]. This guideline provides the minimum frequency, intensity, and duration of exercise involving combined upper-body aerobic plus strength exercise, yielding significant improvements in fitness outcomes. The resistance exercise needed to improve muscle strength is ‘3 sets of strength exercises for each major functioning muscle group should be conducted at a moderate to vigorous intensity, 2 times per week’ [11].
The international guidelines have been adopted in some European countries and Canada [13]. Four Asian countries (Indonesia, Japan, Korea and Thailand) collaborated on the cultural validation of the SEG-SCI by conducting systematic review including their local and international publications written either in their local languages or in English [14]. Those selected publications confirmed the validity of the SEG-SCI. The SEG-SCI was then translated into Bahasa Indonesian, Japanese, Korean and Thai languages [14] to be disseminated to healthcare professionals (HCPs) and people living with SCI in those countries.
However, the review revealed several limitations, including inconsistency in the exercise prescriptions used across studies and countries [14]. This led us to conduct a survey to reveal any different views across countries on aerobic exercise prescriptions. As the SEG-SCI recommend minimum thresholds for aerobic and resistance intensity exercises [11], a sample of HCPs and people with SCI in Asia were surveyed about their perceptions of the relative importance of the four FITT exercise prescription principles (Frequency, Intensity, Time and Type) [15]. For aerobic exercise, we discovered that among HCPs, the most important principle was intensity. But among the SCI group, the most important principle was frequency [15]. When also asked if the exercise intensity was appropriately described by the terms ‘moderate’ or ‘vigorous’, both groups shared a similar negative view on this [15]. Additionally, irrespective to the group, only 34% of the total respondents agreed that these terms provided enough information for aerobic exercise intensity prescription [15].
The present study examines if these findings also apply to perceptions of resistance exercise intensity prescription in Asia, and whether there are differences across study participants from the four Asian participating nations in their perceptions with regard to resistance exercise prescription.
2. Materials and Methods
A cross-sectional design and survey was employed in Indonesia, Japan, Korea and Thailand with the questionnaire translated into their local languages. HCP specializing in SCI healthcare and adults with SCI (aged 18 or higher with traumatic or non-traumatic SCI, and one year post-onset) anonymously participated in the survey. A convenience sampling method was adopted as respondents with SCI were chosen by the facilities where HCPs belonged or engaged. The procedures adhered to the ethical standards of the respective committees in each country and the 2008 Declaration of Helsinki.
The respondents were required to provide informed consent forms prior to completion of the questionnaire. The questionnaire included ranking the perceived importance of resistance exercise intensity, and multiple-choice questions using a 5-point Likert scale asking the frequency of considering a target intensity and if the terms ‘moderate’ and ‘vigorous’ were appropriate and provide enough information about resistance exercise intensity. The data was analyzed by χ2 analysis using the Statistical Package for the Social Sciences V.26 software (SPSS).
Our study focuses on analyzing perceptions about intensity from a psychosocial perspective, rather than a physiological perspective, since we aim to understand if the nature of intensity is importantly perceived and is well-delivered by using the terms, ‘moderate’ and ‘vigorous’ in Asian contexts.
3. Results
Demographics: 228 responses were collected in Indonesia, Japan, Korea and Thailand, including 121 certified HCP (mean age 39±9 years, 23-61) and 107 adults with SCI (mean age 46±13 years, 20-74); ≥1 year ranging C1-L4) [15]. On average, participants who were physiotherapist (49%), physiatrist (30%), occupational therapist (18%) and nurse (3%) had 12±10 years of experience of rehabilitative treatment. The respondents with SCI had an average of 15±12 years post onset after a thoracic injury (50.5%), cervical injury (29%), lumbar injury (14%) along with 6.5% unknown injury level, and there were 43% complete injury, 52% incomplete injury and 5% unspecified [15].
3.1. Perception of Resistance Exercise Intensity
Altogether, 92% of HCP (rank1+rank2) put a significant emphasis on intensity. Frequency was revealed as top priority by the majority of the SCI group in Asia with 61% ranking it as the number 1 or 2 priority (Table 1).
However, nearly 58% of adults with SCI also considered intensity to be important. When asked how often a target intensity was considered (Table 2), there was a big difference between both groups (p<0.001).
While the Asian HCP unified their views with the greatest importance on intensity (Figure 1a), the SCI groups did not rank intensity as the top priority except for the Japanese SCI group emphasizing resistance exercise intensity reaching 78% (Figure 1b).
Accordingly, only both HCP and adults with SCI from Japan considered a target intensity to be a high priority for resistance exercises (Figure 2).
3.2. Appropriateness of Exercise Intensity Terms ‘Moderate’ and ‘Vigorous’ for Strength Training
There were no different views on using terms, ‘moderate’ and ‘vigorous’ between groups (p=0.839, p=0.801, respectively) (Figure 3).
Both groups also similarly agreed that the terms were somewhat inappropriate when asked if these terms provide enough information regarding resistance exercise intensity (p=0.899, p=0.615, respectively) (Figure 4).
Japanese HCP and adults with SCI from Indonesia had the fewest number of respondents who believed the terms were ‘extremely’ or ‘very’ appropriate (Figure 5).
4. Discussion
4.1. Perception of Resistance Exercise Intensity
We conducted a survey to understand perceptions of the importance of intensity and appropriateness of the terminology, from a psychosocial perspective. We discovered that HCP believed intensity was top priority for resistance exercise while the SCI group did place as much importance on intensity (Table 1). In fact, when asked how often a target intensity was considered, 84% of HCP ‘always’ or ‘often’ considered intensity compared to only 52% of the SCI group (Table 2).
Studies have shown aerobic exercise improves cardiorespiratory fitness in adults with SCI and that moderate and vigorous exercise is more effective than light intensity exercise [1,2,16]. Intensity is an important element to prevent cardiometabolic disease [17,18,19,20] and further, vigorous intensity is better than moderate intensity [21,22]. Promoting resistance exercise is also beneficial to cardiovascular fitness [23] and power output [24] and muscular strength [24] Maximal-intensity resistance training resulted in an increase of strength in comparison of conventional training [25]. In general, moderate-vigorous intensity exercise benefits the improvement of cardiorespiratory fitness [26] and the reduction of risk of mortality and morbidity [27,28]. Therefore, it is important for HCP to prescribe moderate and vigorous intensity exercise and for people with SCI to understand and do this prescription.
Our study revealed that HCP acknowledged the importance of intensity for resistance exercise while people with SCI did not. The similar results were found in our companion paper on aerobic exercise as the majority of HCP regarded intensity as the most important aspect for prescribing aerobic exercise while the SCI group largely ranked frequency as the most important element [15]. However, more respondents with SCI appeared to focus on resistance exercise intensity (58%) than aerobic exercise intensity (38%).
Interestingly, only Japanese respondents with SCI (78%) ranked intensity as the most important element for resistance exercise (Figure 2). As applying convenience sampling, all Japanese respondents had experienced a rehabilitation program called PROr (physiatrist and registered therapist operating acute rehabilitation) [29] offered by Wakayama Medical University (WMU) Rehabilitation Center. This program aims for high intensity exercise and high frequency mobilization [29]. This experience can possibly explain why Japanese HCP and respondents with SCI both highly evaluated the importance of intensity for resistance exercise. It likely also explains why the largest number of Japanese SCI and HCP ‘always’ considered a target intensity for resistance exercises.
In Thailand, nearly half of respondents with SCI ranked type of exercise as the most important element for resistance exercise while HCP chose intensity. This result may be due to patient education programs and also SCI exercise guidelines mostly classifying exercise into 2 major groups; aerobic for cardiovascular health and resistance exercise for muscle strength [30]. On the other hand, standard exercise guidelines for HCP are the American College of Sports Medicine (ACSM) guidelines, for which exercise intensity is considered as the most important of the primary variables [31,32].
In our companion paper, there was the hypothesis that people with SCI might have had a lack of knowledge and understanding of the concept of exercise intensity and the physiological consequences of SCI [15]. A knowledge translation gap exists between evidence and implementation [33,34] and the gap in exercise prescription knowledge is broadly appeared in people with SCI [35]. What we supposed from this study was that HCP should be able to do the knowledge translation. For instance, those living with SCI who have ever experienced the intensity-focused rehabilitation program in Japan can be aware how important exercise intensity was. Only a few Indonesian participants with SCI set a target intensity during resistance exercises while 77% of Indonesian HCPs positively do (p<0.001) (Figure 2). We can suppose that the HCP in Indonesia can play a key role in narrowing the gap in knowledge. That said, our finding supports our assumption that the HCP’s knowledge translation could improve the perception of exercise intensity in the SCI population.
4.2. Appropriateness of Exercise Intensity Prescription ‘Moderate’ and ‘Vigorous’
Building on the results of our first report from the survey [11], the present study found that HCP and the SCI group both similarly showed that ‘moderate’ and ‘vigorous’ were unlikely to be appropriate (p=0.839, p=0.801 respectively). When the international SCI Exercise Guidelines were introduced to Asian countries, an issue was a language barrier as Asia is not an English-speaking continent and the guidelines were developed in English. To produce a high-quality version of translated guidelines, those who are rich in rehabilitation knowledge or were language professionals joined the translation process [10]. In this process, it naturally brought up a question on the appropriateness of terms ‘moderate’ and ‘vigorous’.
When again asked if these terms ‘completely’ or ‘mostly’ provide enough information regarding resistance exercise intensity, both groups similarly agreed but the response of HCP was slightly more positive than that of the SCI group (Figure 4). On the contrary, adults with SCI showed more positive attitudes towards aerobic exercise prescription [11], as reported in the companion paper.
When breaking down the data across countries, both groups in Japan were relatively unfavorable to these terms for aerobic exercise intensity [11] and the same for resistance exercise intensity. As noted earlier, Japanese respondents with SCI and HCPs both highly evaluated exercise intensity in that WMU PROr has facilitated adults with SCI to be aware of the importance of exercise intensity, but both groups assessed these terms as relatively inappropriate. Thus, we hypothesize that moderate and vigorous should be substituted by more understandable or conveyable terminology in the Japanese context.
Interestingly, Indonesian HCPs were highly comfortable with these terms while the SCI group was not. We assumed that Indonesian language has been well translated but that this was probably the case of the matter of knowledge translation too. Communication between HCP and people with SCI would also influence the understanding of exercise intensity in SCI [36]. Also, HCPs have lower confidence for physical activity counselling and prescribe exercise in their regular clinical practice [37]. If the Indonesians with SCI were actively instructed by their HCPs, the knowledge translation would occur, and in turn, their perception of exercise intensity would be improved and exercise prescription would be familiarized. Jung et al. [15] implied that “the term intensity is operationally more difficult to define compared with frequency and duration” (p. 5). Accordingly, if there are gaps between both groups, this would suggest that people with SCI and HCP need more appropriate resources/information to explain/understand the prescription of intensity.
These is another possibility that the use of RPE (Rating of Perceived Exercise, or Borg scale) was mostly acceptable for non-HCP due to different level of exposure to medical knowledge and environment [11] and thus, it might be necessary to find more appropriate and familiar terminology or words to convey a level of exercise intensity by using the RPE, if possible.
5. Implications of the Findings
The survey results revealed two issues: knowledge translation of exercise intensity and an end-user friendly prescription. Considering a knowledge translation gap, this problem is not unique to people with SCI, and there is also a problem for the general population because there are many different definitions of moderate-to-vigorous and different ways of monitoring it [38]. Also, as people with SCI are more familiar with RPE scale, RPE scale might attain a clearer perception of the resistance exercise intensity for individuals with SCI, which enables individuals with SCI to apply the guidelines to their daily life activities and exercises. This implies that the international SCI exercise guidelines should be more informative and locally customized to deliver in a different medical or social context. This section is not mandatory but may be added if there are patents resulting from the work reported in this manuscript.
6. Conclusions
Exercise intensity has widely been emphasized for resistance exercises by a health care professional along with aerobic exercise yet individuals with SCI have challenges of living up to exercise intensity recommendations. By facilitating an intensity-focused rehabilitative program with a user-friendly scale, a successful knowledge translation can be effectively occurred between HCP and individuals with SCI. This enables the SCI population to be aware of the importance of exercise intensity and thus, improve their fitness, health and physical function.
Author Contributions
Conceptualization, Kyung Su Jung. and Chayaporn Chotiyarnwong.; methodology, Kyung Su Jung. Chayaporn Chotiyarnwong. Damayanti Tinduh. and Seung-Hyun Yoon.; software, Kyung Su Jung. and Pojchong Chotiyarnwong.; validation, Martha K. Kusumawardani., Chayaporn. Chotiyarnwong. and Seung-Hyun Yoon.; formal analysis, Kyung Su Jung.; investigation, Inggar Narasinta.; resources, Kyung Su Jung. Chayaporn Chotiyarnwong. Seung-Hyun Yoon. Martha K. Kusumawardani. and Inggar Narasinta.; data curation, Kyung Su Jung. and Pojchong Chotiyarnwong.; writing—original draft preparation, Kyung Su Jung.; writing—review and editing, Kyung Su Jung. and Chayaporn Chotiyarnwong.; visualization, Kyung Su Jung and Pojchong Chotiyarnwong; supervision, Fumihiro Tajima.; project administration, Fumihiro Tajima. and Ken Kouda; funding acquisition, Kyung Su Jung. Ken Kouda. and Fumihiro Tajima. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Joint Usage/Research Center of Sport for Persons with Impairments authorized by the Ministry of Education, Culture, Sports, Science and Technology at Wakayama Medical University, Japan, grant number SP2020-01.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Universitas Airlangga, Indonesia (0318/LOE/301.1.2/I/2021, 30th January 2021); Wakayama Medical University, Japan (3109, 3rd March 2021); Siriraj Hospital, Mahidol University, Thailand (036/2564(IRB2)), 2nd February 2021) and Ajou University Hospital, Korea (AJOUIRB-SUR-2021-051, 16th March 2021).
Informed Consent Statement
Written informed consent was obtained by all subjects involved in the study.
Data Availability Statement
The data are available upon request.
Acknowledgments
K.A. Martin Ginis provided advice on the statistical analyses and preparation of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hicks, A.L.; Martin Ginis, K.A.; Pelletier, C.A.; Ditor, D.S.; Foulon, B.; Wolfe, D.L. The effects of exercise training on physical capacity, strength, body composition and functional performance among adults with spinal cord injury: a systematic review. Spinal Cord. 2011, 49, 1103–1127. [Google Scholar] [CrossRef] [PubMed]
- van der Scheer, J.W.; Martin Ginis, K.A.; Ditor, D.S.; Goosey-Tolfrey, V.L.; Hicks, A.L.; West, C.R.; Wolfe, D.L. Effects of exercise on fitness and health of adults with spinal cord injury: a systematic review. Neurology. 2017, 89, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Selph, S.S.; Skelly, A.C.; Wasson, N.; Dettori, J.R.; Brodt, E.D.; Ensrud, E.; Elliot, D.; Dissinger, K.M.; McDonagh, M. Physical activity and the health of wheelchair users: a systematic review in multiple sclerosis, cerebral palsy, and spinal cord injury. Arch. Phys. Med. Rehabil. 2021, 102, 2464–2481. [Google Scholar] [CrossRef] [PubMed]
- Foulon, B.L.; Lemay, V.; Ainsworth, V.; Ginis, K.A.M. Enhancing physical activity guidelines: a needs survey of adults with spinal cord injury and health care professionals. Adapted Physical Activity Quarterly. 2012, 29, 329–345. [Google Scholar] [CrossRef] [PubMed]
- Martin Ginis, K.A.; Jetha, A.; Mack, D.E.; Hetz, S. Physical activity and subjective well-being among people with spinal cord injury: A meta-analysis. Spinal Cord. Advance online publication, July 7, 2009. [CrossRef]
- Pelletier, C. Exercise prescription for persons with spinal cord injury: a review of physiological considerations and evidence-based guidelines. Appl. Physiol. Nutr. Metab. 2023, 48, 882–895. [Google Scholar] [CrossRef] [PubMed]
- Farrow, M.; Nightingale, T.E.; Maher, J.; McKay, C.D.; Thompson, D.; Bilzon, J.L.J. Effect of exercise on cardiometabolic risk factors in adults with chronic spinal cord injury: a systematic review. Arch. Phys. Med. Rehabil. 2020, 101, 2177–2205. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.; Abou, L.; Rice, L.A.; Dandeneau, K.; Alluri, A.; Salvador, A.F.; Rice, I. The effectiveness of vigorous training on cardiorespiratory fitness in persons with spinal cord injury: a systematic review and meta-analysis. Spinal Cord. 2021, 59, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
- Chiou, S.Y.; Clarke, E.; Lam, C.; Harvey, T.; Nightingale, T.E. Effects of arm-crank exercise on fitness and health in adults with chronic spinal cord injury: a systematic review. Front. Physiol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Martin Ginis, K.A.; van der Scheer, J.W.; Latimer-Cheung, A.E.; Barrow, A.; Bourne, C.; Carruthers, P.; Bernardi, M.; Ditor, D.S.; Gaudet, S.; de Groot, S.; Hayes, K.C.; Hicks, A.L.; Leicht, C.A.; Lexell, J.; Macaluso, S.; Manns, P.J.; McBride, C.B.; Noonan, V.K.; Pomerleau, P.; Rimmer, J.H.; Shaw, R.B.; Smith, B.; Smith, K.M.; Steeves, J.D.; Tussler, D.; West, C.R.; Wolfe, D.L.; Goosey-Tolfrey, V.L. Evidence-Based scientific exercise guidelines for adults with spinal cord injury: an update and a new guideline. Spinal Cord. 2018, 56, 308–321. [Google Scholar] [CrossRef] [PubMed]
- Scientific exercise guidelines for adults with spinal cord injury. Available online: https://www.physio-pedia.com/Physical_Activity_Guidelines_for_Spinal_Cord_Injury#:~:text=20%20minutes%20of%20moderate%20to,intensity%2C%202%20%20times%20per%20week (accessed on 5 June 2023).
- Goosey-Tolfrey, V.L.; van der Scheer, J.W.; Lexell, J.; Clements, K.; Martin Ginis, K.A.; International SCI Exercise Guidelines Project Group. Development of scientific exercise guidelines for adults with spinal cord injury. Br J Sports Med. 2018, 52, 18–1166. [Google Scholar] [CrossRef] [PubMed]
- Martin Ginis, K.A.; van der Scheer, J.W.; Todd, K.R.; Davis, J.C.; Gaudet, S.; Hoekstra, F.; Karim, M.E.; Kramer, J.L.K.; Little, J.P.; Singer, J.; Townson, A.; West, C.R. A pragmatic randomized controlled trial testing the effects of the International scientific SCI exercise guidelines on SCI chronic pain: protocol for the EPIC-SCI trial. Spinal Cord. 2020, 58, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Mikami, Y.; Tinduh, D.; Lee, K.; Chotiyarnwong, C.; van der Scheer, J.W.; Jung, K.S.; Shinohara, H.; Narasinta, I.; Yoon, S.H.; Kanjanapanang, N.; Sakai, T.; Kusumawardhani, M.K.; Park, J.; Prachgosin, P.; Obata, F.; Utami, D.A.; Laohasinnarong, P.; Wardhani, I.L.; Limprasert, S.; Tajima, F.; Goosey-Tolfrey, V.L.; Martin Ginis, K.A. Cultural validation and language translation of the scientific SCI exercise guidelines for use in Indonesia, Japan, Korea, and Thailand. J Spinal Cord Med. 2022, 45, 821–832. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.S.; Hutchinson, M.J.; Chotiyarnwong, C.; Kusumawardani, M.K.; Yoon, S.H.; Mikami, Y.; Laohasinnarong, P.; Tinduh, D.; Prachgosin, P.; Narasinta, I.; Chotiyarnwong, P.; Utami, D.A.; Umemoto, Y.; Tajima, F.; Goosey-Tolfrey, V.L. Dissonance in views between healthcare professionals and adults with a spinal cord injury with their understanding and interpretation of exercise intensity for exercise prescription. BMJ Open Sport & Exercise Medicine. 2023, 9, e001487. [Google Scholar] [CrossRef] [PubMed]
- Hodgkiss, D.D.; Bhangu, G.S.; Lunny, C.; Jutzeler, C.R.; Chiou, S.Y.; Walter, M.; Lucas, S.J.E.; Krassioukov, A.V.; Nightingale, T.E. The effect of exercise on aerobic capacity in individuals with spinal cord injury: A systematic review with meta-analysis and meta-regression. PLOS Medicine. 2023. [Google Scholar] [CrossRef] [PubMed]
- Gillen, J.B.; Martin, B.J.; MacInnis, M.J.; Skelly, L.E.; Tarnopolsky, M.A.; Gibala, M.J. Twelve weeks of sprint interval training improves indices of cardiometabolic health similar to traditional endurance training despite a five-fold lower exercise volume and time commitment. PLoS One. 2016, 11, e0154075. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Hsieh, C.C. Paffenbarger RS. Exercise intensity and longevity in men. The Harvard alumni health study. JAMA. 1995, 273, 1179–1184. [Google Scholar] [CrossRef] [PubMed]
- MacInnis, M.J.; Gibala, M.J. Physiological adaptations to interval training and the role of exercise intensity. J Physiol. 2017, 595, 2915–2930. [Google Scholar] [CrossRef] [PubMed]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of high-intensity interval training (HIT) and continuous endurance training for VO2max improvements: a systematic review and meta-analysis of controlled trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [PubMed]
- Swain, D.P. Moderate or vigorous intensity exercise: which is better for improving aerobic fitness? Prev. Cardiol. 2005, 8, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Shiroma, E.J.; Sesso, H.D.; Moorthy, M.V.; Buring, J.E.; Lee, I.M. Do moderate-intensity and vigorous-intensity physical activities reduce mortality rates to the same extent? J Am Heart Assoc. 2014, 3, e000802. [Google Scholar] [CrossRef] [PubMed]
- Cooney, M.M.; Walker, J.B. Hydraulic resistance exercise benefits cardiovascular fitness of spinal cord injured. Med Sci Sports Exerc. 1986, 18, 522–525. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, P.L. Effects of resistance and endurance training in persons with paraplegia. Med Sci Sports Exerc. 2009, 41, 992–997. [Google Scholar] [CrossRef] [PubMed]
- Jayaraman, A.; Thompson, C.K.; Rymer, W.Z.; Hornby, T.G. Short-term maximal-intensity resistance training increases volitional function and strength in chronic incomplete spinal cord injury: a pilot study. J Neurol Phys Ther. 2013, 37, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; de Lannoy, L.; Stotz, P.J. Separate effects of intensity and amount of exercise on interindividual cardiorespiratory fitness response. Mayo Clin. Proc. 2015, 90, 1506–1514. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Paffenbarger Jr, R.S. Associations of light, moderate, and vigorous intensity physical activity with longevity: the Harvard alumni health study. Am. J. Epidemiol. 2000, 151, 293–299. [Google Scholar] [CrossRef]
- Wen, C.P.; Wai, J.P.M.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.D.; Lee, M.C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. 2011, 378, 1244–1253. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Nishimura, Y.; Nakamura, T.; Hashizaki, T.; Kojima, D.; Kawanishi, M.; Uenishi, H.; Arakawa, H.; Ogawa, T.; Kamijo, Y.; Kawasaki, T.; Tajima, F. Effects of physiatrist and registered therapist operating acute rehabilitation (PROr) in patients with stroke. PLoS ONE. 2017, 12, e0187099. [Google Scholar] [CrossRef] [PubMed]
- Eitivipart, A.C.; de Oliveira, C.Q.; Arora, M.; Middleton, J.; Davis, G.M. Overview of systematic reviews of aerobic fitness and muscle strength training after spinal cord injury. J Neurotrauma. 2019, 36, 2943–2963. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, P.; Tschakert, G. Special needs to prescribe exercise intensity for scientific studies. Cardiol Res Pract. 2010, 2011, 209302. [Google Scholar] [CrossRef] [PubMed]
- ACSM’s Guidelines for Exercise Testing and Prescription. 11th ed.; Senior Editor, Gary Liguori., Associate Editors, Yuri Feito, Charles Fountaine, Brad A. Roy.; Wolters Kluwer: Two Commerce Square, 2001 Market Street, Philadelphia, PA 19103, USA, 2022.
- Fullagar, H.H.K.; McCall, A.; Impellizzeri, F.M.; Favero, T.; Coutts, A.J. The translation of sport science research to the field: a current opinion and overview on the perceptions of practitioners, researchers and coaches. Sports Med. 2019, 49, 1817–1824. [Google Scholar] [CrossRef] [PubMed]
- Leggat, F.J.; Wadey, R.; Day, M.C.; Winter, S.; Sanders, P. Bridging the know-do gap using integrated knowledge translation and qualitative inquiry: a narrative review. Qual. Res. Sport Exerc. Health. 2023, 15, 188–201. [Google Scholar] [CrossRef]
- Martin Ginis, K.A.; Lawrason, S.V.C.; Berrisford, H.A. Translational physical activity research involving people with disabilities: a review and a call to action. Kinesiol. Rev. 2023, 12, 87–97. [Google Scholar] [CrossRef]
- Jenerette, C.M.; Mayer, D.K. Patient-Provider Communication: The Rise of Patient Engagement. Seminars in Oncology Nursing. 2016, 32, 134–143. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.W.; Shields, C.A.; Oh, P.I.; Fowles, J.R. Health care provider confidence and exercise prescription practices of Exercise is Medicine Canada workshop attendees. Appl. Physiol. Nutr. Metab. 2017, 42, 384–390. [Google Scholar] [CrossRef] [PubMed]
- MacIntosh, B.R.; Murias, J.M.; Keir, D.A.; Weir, J.M. What is moderate to vigorous exercise intensity. Front. Physiol. 22 September 2021, Sec. Exercise Physiology Volume 12. [CrossRef]
Figure 1.
The question ‘rank these aspects in order of importance when conducting RESISTANCE exercise: (a) HCP Respondents in each nation’s categorization; (b) Respondents with SCI in each nation’s categorization.
Figure 1.
The question ‘rank these aspects in order of importance when conducting RESISTANCE exercise: (a) HCP Respondents in each nation’s categorization; (b) Respondents with SCI in each nation’s categorization.
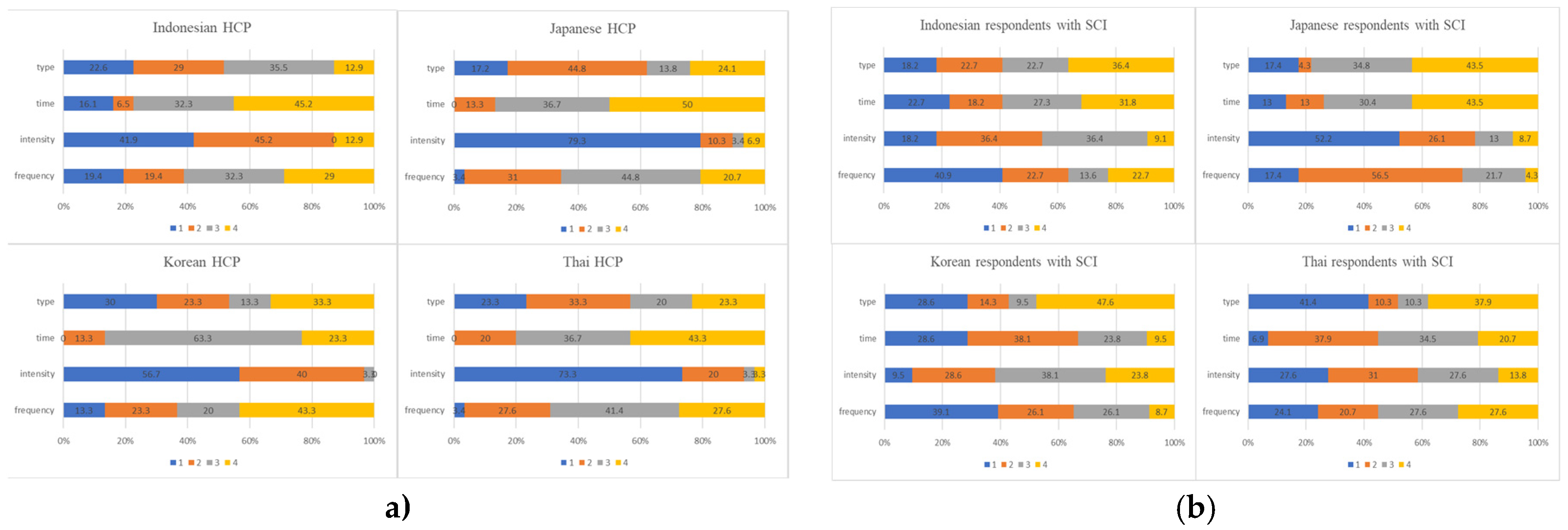
Figure 2.
How often a target intensity is considered during resistance exercise in each Asian nation?
Figure 2.
How often a target intensity is considered during resistance exercise in each Asian nation?
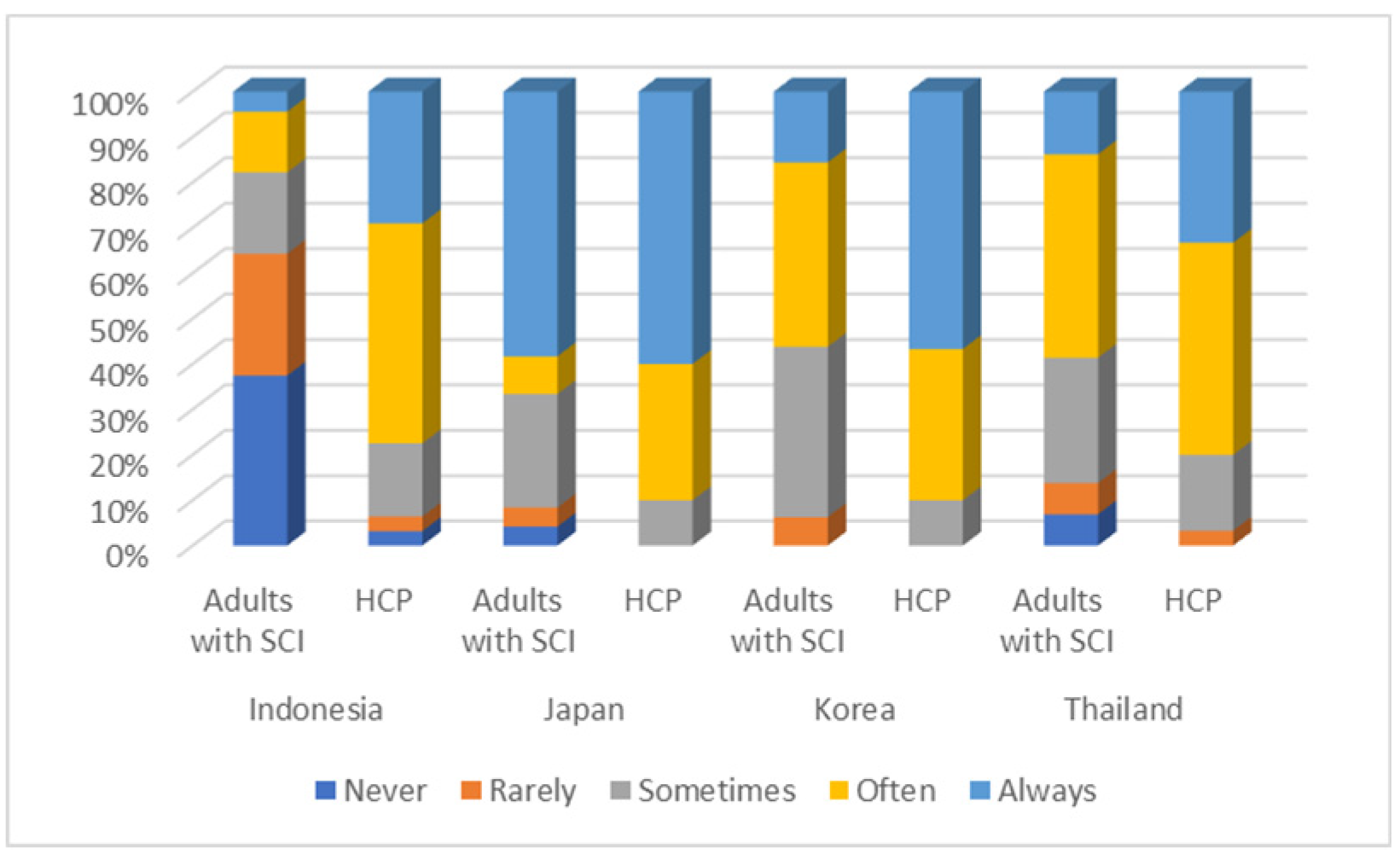
Figure 3.
How appropriate the terms, ‘moderate’ and ‘vigorous’ are in resistance exercise.
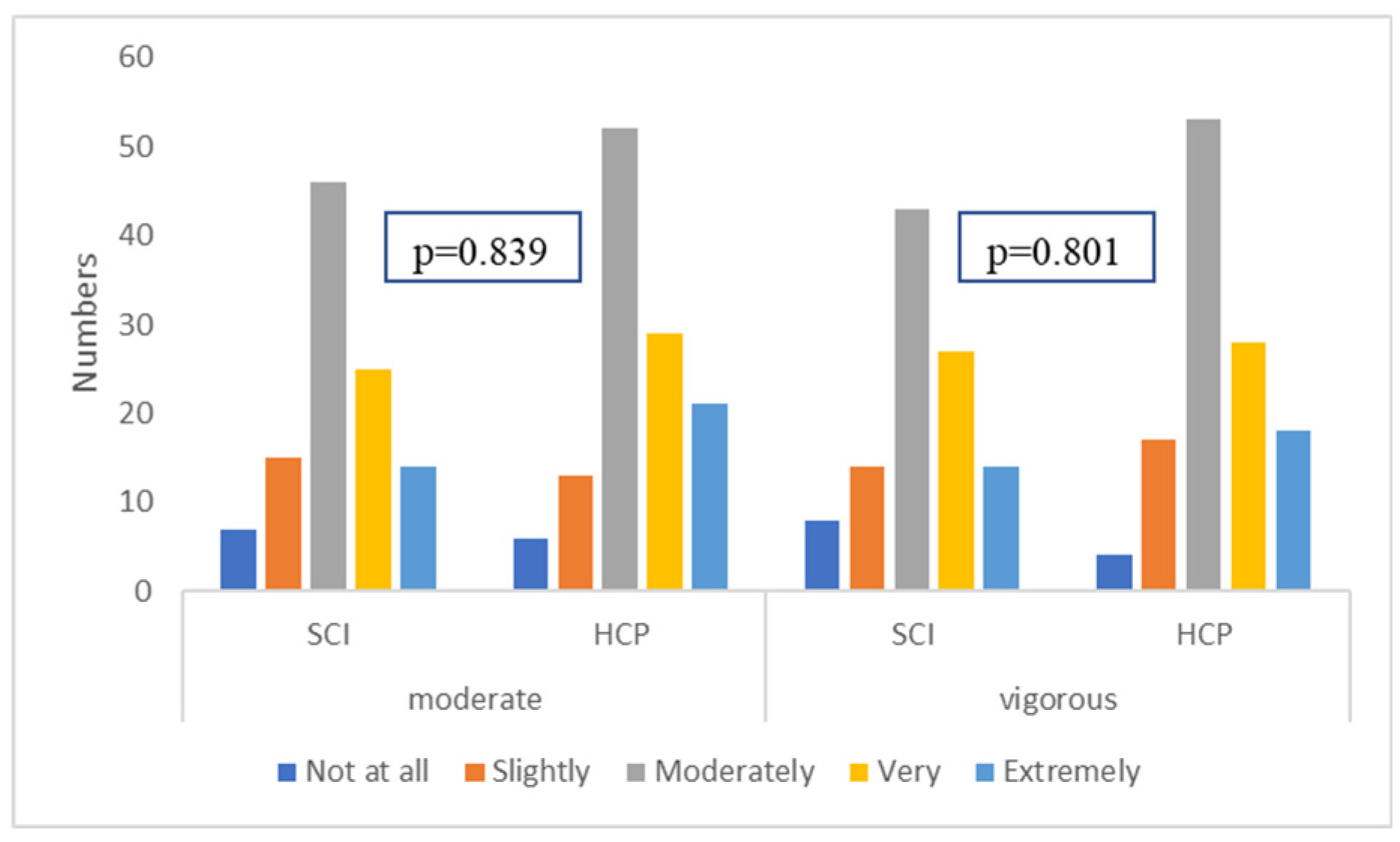
Figure 4.
Whether the terms, ‘moderate’ and ‘vigorous’ provide enough information in Asian nations.
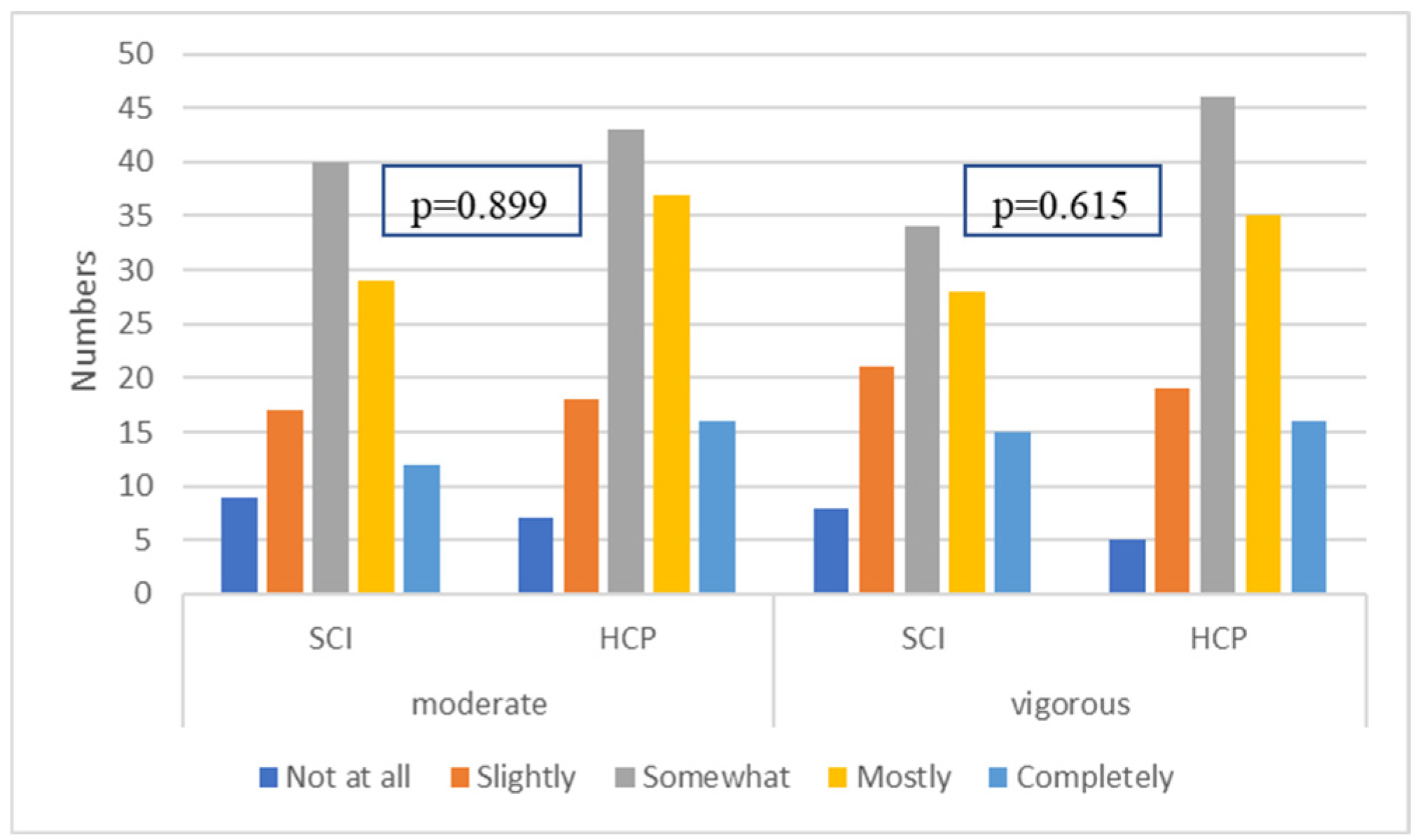
Figure 5.
How appropriate the terms, ‘moderate’ and ‘vigorous’ are in resistance exercise in each Asian country.
Figure 5.
How appropriate the terms, ‘moderate’ and ‘vigorous’ are in resistance exercise in each Asian country.
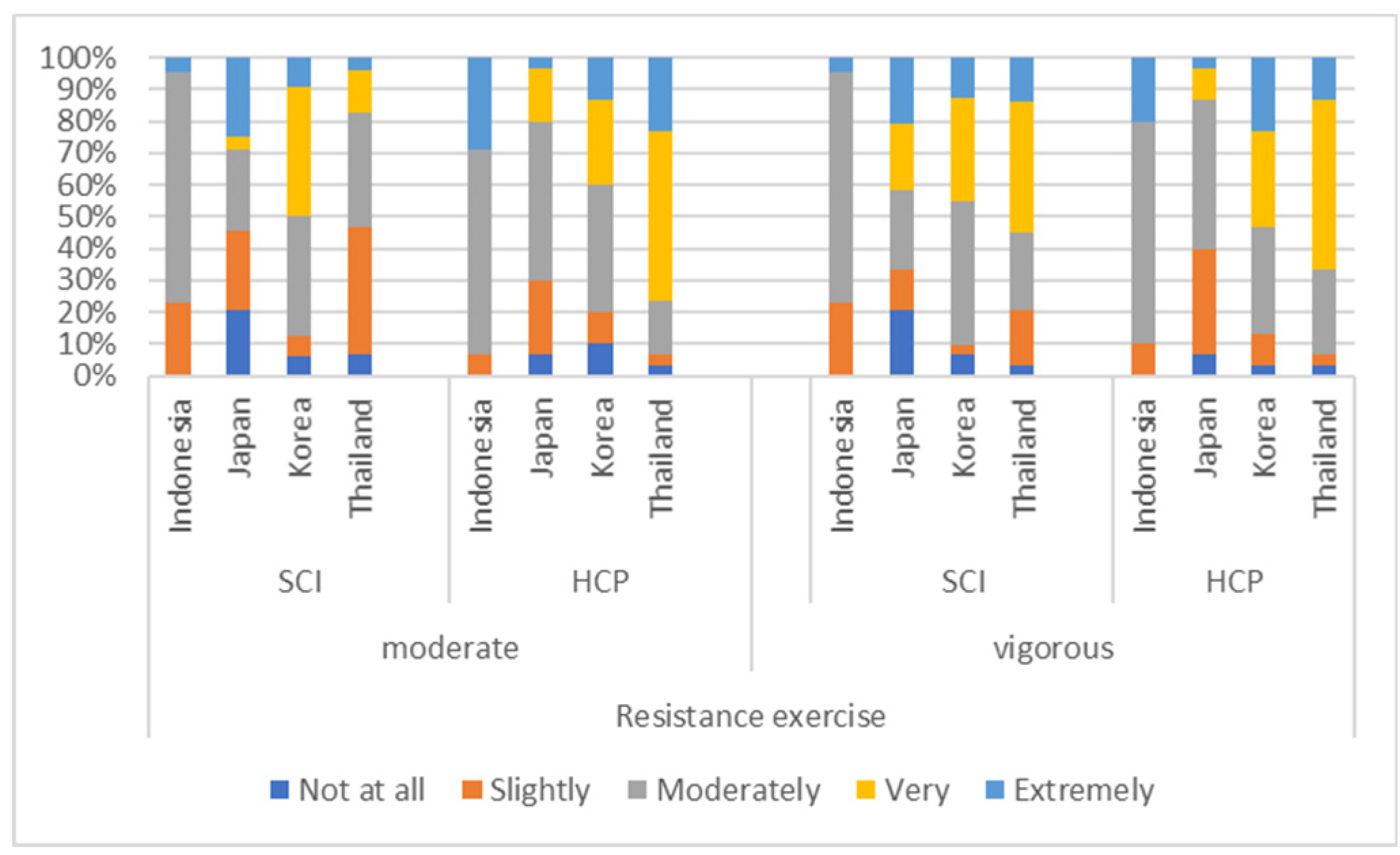

Table 1.
The ranking of the four aspects in order of importance when conducting resistance exercise in the four Asian nations (count (per cent %)).
Table 1.
The ranking of the four aspects in order of importance when conducting resistance exercise in the four Asian nations (count (per cent %)).
| Parameter | Rank | Resistance Exercise | ||
|---|---|---|---|---|
| Adults with SCI | HCP | (x2) p value |
||
| Frequency | 1 | 29 (30) | 12 (10) | p<0.001 |
| 2 | 30 (31) | 30 (25) | ||
| 3 | 22 (23) | 41 (35) | ||
| 4 | 16 (16) | 36 (30) | ||
| Intensity | 1 | 26 (27) | 75 (63) | p<0.001 |
| 2 | 29 (31) | 35 (29) | ||
| 3 | 27 (28) | 3 (2) | ||
| 4 | 13 (14) | 7 (6) | ||
| Time(duration) | 1 | 16 (17) | 5 (4) | p<0.001 |
| 2 | 26 (27) | 16 (13) | ||
| 3 | 28 (30) | 51 (43) | ||
| 4 | 25 (26) | 48 (40) | ||
| Type | 1 | 26 (27) | 28 (23) | p=0.002 |
| 2 | 12 (13) | 39 (33) | ||
| 3 | 18 (19) | 25 (21) | ||
| 4 | 39 (41) | 28 (23) | ||
Table 2.
How often a target intensity is considered during resistance exercise in the four Asian nations? (count (per cent %)).
Table 2.
How often a target intensity is considered during resistance exercise in the four Asian nations? (count (per cent %)).
| How often | Resistance exercise | |
|---|---|---|
| Adults with SCI | HCP | |
| Never | 11 (10) | 1 (1) |
| Rarely | 11 (10) | 2 (2) |
| Sometimes | 30 (28) | 16 (13) |
| Often | 31 (29) | 48 (40) |
| Always | 24 (23) | 54 (44) |
| (x2) p value | p<0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



