
Submitted:
04 June 2024
Posted:
04 June 2024
You are already at the latest version
Abstract
CAR-T cell therapy has emerged as a groundbreaking approach in cancer treatment, leveraging the immune system to target and eliminate cancer cells. While currently focused on hematologic malignancies, the future holds promise for expanding CAR-T cell therapy to diverse cancers, enhancing its efficacy, and improving safety profiles. Recent advances in tumor immunology have propelled CAR-T cell therapy as a game-changer in treating diseases such as relapsed/refractory B-cell acute lymphocytic leukemia (B-ALL), non-Hodgkin lymphoma (NHL), and multiple myeloma (MM). Six CAR-T cell products have received FDA approval for treating R/R B cell malignancies. However, challenges persist, including complications like cytokine release syndrome (CRS), coagulopathy, and cytopenias. Strategies to mitigate these complications involve targeting distinct antigens with dual- or multi-targeted CAR-T cells and enhancing immunogenicity. Additionally, γδ CAR-T cells show promise in recognizing antigen- negative leukemia cells in an MHC-independent manner while reducing the risk of inducing graft-versus-host disease (GVHD). As CAR-T cell therapy continues to evolve through innovation and discovery, it holds the potential to revolutionize cancer treatment, offering new hope to patients and reshaping the landscape of oncology with its precision and efficacy.
Keywords:
CAR-T cell therapy
; Hematologic malignancies
; Cytokine release syndrome
; Antigen mutation
; γδ CAR-T cells
; Multi-targeted CAR-T cells
; Precision medicine
1. Introduction
CAR-T cell therapy has emerged as a revolutionary approach in cancer treatment, harnessing the power of the immune system to target and destroy cancer cells. While its current applications predominantly focus on hematologic malignancies, the future holds immense promise for expanding CAR-T cell therapy to a wider spectrum of cancers and enhancing its efficacy and safety profile.
Traditionally, treatments for hematological cancers included chemotherapy, radiotherapy, and stem cell transplantation. However, recent breakthroughs in tumor immunology have led to innovative therapies. One such game-changer is CAR-T cell therapy, which has shown remarkable results in relapsed/refractory B-cell acute lymphocytic leukemia (B-ALL), non- Hodgkin lymphoma (NHL), and multiple myeloma (MM). CAR-T cell therapy involves modifying a patient’s own immune cells (T cells) to specifically target cancer cells. These modified cells are equipped with chimeric antigen receptors (CARs) that recognize specific antigens on cancer cells [1,2,3]. Notably, six CAR-T cell products (Table 1) have received FDA approval for treating R/R B cell malignancies:
1.2. Enhancing Efficacy through Multi-Targeting:
One of the key future directions of CAR-T cell therapy is the development of multi-targeted CAR-T cells. Currently, CAR-T cells are engineered to recognize a single antigen present on cancer cells. However, tumors can evade single-target therapies by downregulating the targeted antigen or developing resistance mechanisms. By designing CAR-T cells that target multiple antigens simultaneously, researchers aim to overcome tumor heterogeneity and enhance treatment efficacy. This approach not only improves tumor recognition but also reduces the likelihood of relapse, leading to more durable responses in patients [17,18].
1.3. Improving Persistence and Longevity:
Another important aspect of future CAR-T cell therapy lies in enhancing the persistence and longevity of engineered T cells within the body. While CAR-T cells can induce potent anti- tumor responses initially, their persistence is often limited, resulting in the eventual loss of therapeutic effect. To address this challenge, scientists are exploring various strategies, including the incorporation of co-stimulatory domains into CAR constructs, cytokine modulation, and genetic engineering techniques to promote T cell survival and expansion. By prolonging the presence of CAR-T cells in the tumor microenvironment, researchers aim to achieve sustained tumor control and long-term remissions in patients [19].
1.4. Expanding the Scope to Solid Tumors:
Currently, CAR-T cell therapy has shown remarkable success in treating hematologic malignancies such as leukemia and lymphoma. However, its application to solid tumors presents unique challenges due to the immunosuppressive tumor microenvironment, tumor heterogeneity, and off-target toxicity. Despite these obstacles, significant efforts are underway to adapt CAR-T cell therapy for solid tumor treatment. This includes the development of novel CAR constructs with improved tumor penetration and targeting capabilities, as well as the incorporation of additional genetic modifications to enhance T cell function and overcome immune evasion mechanisms. Additionally, combinatorial approaches involving CAR-T cells and other immunotherapies, such as checkpoint inhibitors and cytokine therapies, hold promise in overcoming the immunosuppressive barriers inherent to solid tumors [20,21].
1.5. Addressing Safety Concerns:
While CAR-T cell therapy has demonstrated remarkable efficacy, it is also associated with significant toxicities, including cytokine release syndrome (CRS), neurotoxicity, and on- target/off-tumor effects. As the field advances, ensuring the safety of CAR-T cell therapy remains a critical focus. Future research efforts will continue to refine treatment protocols, optimize dosing strategies, and develop innovative mitigation strategies to minimize adverse events while preserving anti-tumor efficacy. This includes the implementation of predictive biomarkers and personalized approaches to identify patients at risk of severe toxicities and tailor treatment regimens accordingly.
1.6. CD19 Is a Crucial Target Antigen in B Cell Malignancies
CD19 is a crucial target antigen in B cell malignancies, and anti-CD19 CAR-T cell therapy has significantly improved the treatment landscape of these diseases, with four such products already approved by the FDA [22,23,24]. Despite these advancements, CD19 antigen loss is a common issue, prompting the exploration of alternative targets for CAR-T cell therapy [25,26,27]. CD20, overexpressed in most B cell lymphomas, has shown promise as a target, with anti-CD20 CAR-T cell therapy achieving an overall response rate of 86% in early clinical trials [27]. To prevent antigen escape, a combination of anti-CD19 and anti-CD20 CAR-T cells has been investigated and found to be safe and feasible [1,28,29]. CD22, highly expressed on most B cell malignancies but not on hematopoietic stem cells, is another promising target, with anti-CD22 CAR-T cell therapy showing excellent efficacy in patients who have failed previous anti-CD19 CAR-T cell therapy [1,30]. Table 2 shows the preparation process of CAR-T cell products.
CAR-T cell therapy is a type of cancer treatment that uses a patient’s own immune cells to fight cancer. These immune cells, called T cells, are modified in a laboratory to better recognize and attack cancer cells when they are infused back into the patient’s body. While CAR-T cell therapy can be effective in treating certain types of cancer, it can also lead to complications. One common complication is called cytokine release syndrome (CRS), which happens when the immune system responds strongly to the therapy, causing symptoms like fever and low blood pressure. Another complication is coagulopathy, which affects the blood’s ability to clot properly and can lead to bleeding or blood clot formation. It is important for patients undergoing CAR-T cell therapy to be aware of these potential complications and work closely with their healthcare team to monitor and manage them effectively. Early detection and treatment of complications can help improve outcomes and reduce the risk of serious side effects.
2. Pathophysiology of CAR-T Cell Therapy Related Toxicities
2.1. Cytokine-Release Syndrome (CRS)
CRS, a common toxicity of CAR-T cell therapy, varies in incidence depending on factors like disease characteristics, CAR structure, and tumor burden [48]. Clinical manifestations range from fever to organ dysfunction, with severe cases progressing rapidly to life-threatening conditions [49]. IL-6 plays a pivotal role in CRS, making tocilizumab the primary recommendation for symptom relief [50]. Treatment regimens vary based on CRS grading, with tocilizumab and corticosteroids reserved for severe cases. Anakinra, an IL-1 receptor antagonist, has shown promise in alleviating both CRS and CRES. GM-CSF deficiency or inhibition not only alleviates CRS and CRES but also enhances CAR-T cell anti-tumor effects. Tumor burden positively correlates with CRS severity, highlighting the importance of reducing it with traditional chemotherapy or radiotherapy before CAR-T cell infusion. Mechanistically, CAR-T cells rapidly activate upon antigen recognition, leading to the secretion of various cytokines and the initiation of inflammatory responses primarily by macrophages and monocytes. Interactions between CD40/CD40L further amplify immune activation and cytokine release, implicating multiple cell types in CRS pathology. Additionally, CD40/CD40L interactions contribute to endothelial cell activation, further elucidating the complex mechanisms underlying CRS [51,52,53].
2.2. T and B Lymphocytes Aplasia and Opportunistic Infections
CD19, CD20, and BCMA are enticing targets for CAR-T cell therapy in B-cell malignancies due to their expression on malignant B cells. However, these therapies may also affect normal B cells, leading to complications like impaired humoral immunity [54]. Lymphodepleting chemotherapy before CAR-T cell infusion can further compromise host immunity, increasing susceptibility to infections, predominantly occurring within the first 30 days post-infusion, with bacterial infections being predominant [1,55]. Long-term follow-up and monitoring of gamma globulin levels are essential for managing infections. Immunoglobulin supplementation is necessary to restore humoral immunity in immune-compromised individuals [56,57,58]. High-dose CAR-T cell infusion may exacerbate infection risk, suggesting the utility of dose-escalation regimens] [59].
HBV reactivation is a concern in patients with resolved infections, necessitating antiviral prophylaxis and regular monitoring. In T-cell malignancies, CAR-T cell therapy may induce T- cell aplasia due to shared target antigens on normal T cells [54,60,61]. Distinguishing between CRS and infections is challenging due to overlapping clinical manifestations, emphasizing the importance of early infection recognition and management. IL-6 plays a crucial role in infection- induced cytokine storms and CRS, with serum IL-6 elevation occurring typically within three weeks post-infusion. Employing the “double peaks of IL-6” pattern may expedite the prediction of life-threatening infections compared to blood culture. Empiric anti-infective treatment should be promptly initiated, especially in neutropenic patients. Prophylactic acyclovir administration is recommended to prevent herpesvirus infections during CAR-T cell therapy [62].
2.3. CRS-Related Coagulopathy
Coagulopathy, often observed within a month after CAR-T cell infusion, correlates positively with CRS grade and IL-6 levels, termed CRS-related coagulopathy. Recent studies suggest a 50% incidence during CAR-T cell therapy, characterized by abnormal coagulation parameters and stages of hypercoagulability, consumptive hypo-coagulability, and hyperfibrinolysis.
Treatment strategies vary with stages, including anticoagulant drugs and replacement therapy, to mitigate risks of complications like disseminated intravascular coagulation. Early management of CRS may aid in reducing coagulopathy incidence, highlighting the importance of timely intervention [63,64,65].
2.4. Cytopenias
Cytopenia is a common occurrence during CAR-T cell therapy, lasting from several days to months and encompassing conditions such as anemia, thrombocytopenia, and leukopenia [4]. Research indicates a correlation between cytopenia and severe CRS. In inflammatory environments, granulocytic progenitor/precursor cells exhibit up-regulation of CD40 along with low levels of CD40L, leading to enhanced apoptosis via CD40/CD40L interactions. Pro- inflammatory cytokines like TNF-α, IL-1, and HMGB1 can inhibit erythropoietin production, while activated macrophages may destroy erythrocytes [66]. The diminished hematopoietic capacity resulting from prior chemotherapy and HSCT may also contribute to cytopenia.
Moreover, some target antigens are co-expressed on normal hematopoietic stem or progenitor cells, making them susceptible to destruction by CAR-T cells. Clinical management of cytopenia typically involves transfusions of red blood cells and platelets, along with the administration of hematopoietic growth factors such as granulocyte colony-stimulating factor (G-CSF) and thrombopoietin (TPO), as well as TPO receptor agonists and sirolimus [67].
2.5. Antigen Mutation
The phenomenon of antigen mutation poses a significant challenge in the context of CAR-T cell therapy, particularly in the treatment of relapsed or refractory (R/R) B cell malignancies. Despite the notable success of CAR-T cell therapy in many cases, a considerable proportion of patients experience relapse, with antigen loss being a primary mechanism behind this recurrence. Antigen mutations can occur under the therapeutic pressure exerted by CAR-T cell therapy. These mutations are often diverse, encompassing mechanisms such as splice variants, lineage switching, and biallelic mutations [35,68]. Furthermore, the endocytosis of CAR-T cells can contribute to a decrease in antigen density on tumor cell surfaces, facilitating immune escape.
Additionally, a concerning scenario involves the inadvertent transfer of the anti-CD19 CAR to leukemic B cells during the manufacturing process. This transfer results in the CAR binding to the CD19 epitope on leukemic blasts, thereby masking the epitope and preventing recognition by anti-CD19 CAR-T cells [1,35,68,69].
To combat antigen-negative relapse, strategies such as targeting distinct antigens have been explored. Dual-targeting CAR-T cells, capable of recognizing two distinct target antigens simultaneously, have shown promise in reducing the risk of antigen-negative relapse. Examples include bispecific CAR-T cells in B cell lymphoma/leukemia and APRIL-based CAR-T cells targeting both BCMA and TACI in multiple myeloma (MM). Moreover, multi-targeted CAR-T cells have been investigated, such as tri-specific CD19-CD20-CD22-targeting CAR-T cells, which demonstrated rapid elimination of B cell lymphoma in preclinical studies. Furthermore, increasing the immunogenicity of target cells, for instance, using small molecule γ-secretase inhibitors to reduce BCMA shedding, can enhance recognition by CAR-T cells. An emerging approach involves utilizing γδ T cells, a subset of peripheral blood cytotoxic T cells expressing both T cell receptors (TCRs) and natural killer receptors (NKRs). NKRs expressed on γδ T cells play a crucial role in tumor cell recognition, particularly in hematological malignancies [70,71,72,73,74,75,76].
γδ CAR-T cells have shown promise in recognizing antigen-negative leukemia cells via NKRs in an MHC-independent manner. Importantly, γδ T cells have demonstrated a reduced risk of inducing graft-versus-host disease (GVHD), making them a potentially safer option for universal CAR-T cell development. In summary, addressing antigen mutation challenges in CAR-T cell therapy requires innovative strategies such as dual-targeting or multi-targeted CAR-T cells and leveraging alternative cell types like γδ T cells to enhance recognition and efficacy while minimizing adverse effects like antigen-negative relapse and GVHD [77,78,79].
2.6. Neurotoxicity in CAR-T Cell Therapy
The study by Gust et al. (2017) emphasized the importance of understanding the incidence and severity of neurotoxicity in patients undergoing CAR-T cell therapy for B-cell malignancies. This research underscores the need for further investigation into the specific mechanisms underlying CAR-T cell therapy-related neurotoxicity, as well as the development of strategies to predict, monitor, and mitigate these neurological side effects. Neurotoxicity is a significant concern associated with CAR-T cell therapy, and it can manifest in various forms, ranging from mild cognitive impairment to severe and life-threatening cerebral edema. One major contributor to neurotoxicity is the phenomenon known as cytokine release syndrome (CRS), wherein the activated CAR-T cells release a surge of pro-inflammatory cytokines. This can lead to the activation of microglia and subsequent neuroinflammation [80].
Neurological complications are among the significant adverse events associated with CAR-T cell therapy. These complications can range from mild neurotoxicity to severe neurologic events, including encephalopathy, seizures, and cerebral edema. Understanding and effectively managing these complications are essential for the safe and successful use of CAR-T cell therapy [81]. This consensus document provides guidelines for grading cytokine release syndrome (CRS) and neurologic toxicity associated with CAR-T cell therapy, offering a standardized approach for assessing and managing these complications. This study investigates the underlying mechanisms of neurotoxicity following CD19 CAR-T cell therapy, focusing on endothelial activation and blood-brain barrier disruption, providing insights into potential therapeutic targets for mitigating neurologic complications [80].
2.7. Graft-Versus-Host Disease (GVHD) in CAR-T Cell Therapy:
The study by Brudno and Kochenderfer (2016) delves into the complexities of managing GVHD in the context of CAR-T cell therapy. Understanding and controlling the allogeneic immune response is crucial for mitigating GVHD risk. GVHD is a potential toxicity associated with CAR-T cell therapy, especially when allogeneic T cells (from a donor) are used. In GVHD, the transplanted T cells recognize the recipient’s tissues as foreign, leading to an immune response against them. This complication can affect various organs and systems, posing challenges to the safety and success of CAR-T cell therapy [85]. Ongoing research, such as the work by Lee et al. (2019), aims to explore the incidence and severity of GVHD in patients undergoing CAR-T cell therapy, identifying potential risk factors and informing strategies to improve the safety profile of this innovative treatment [81]. Understanding and addressing these themes are critical for enhancing the safety and efficacy of CAR-T cell therapy, ultimately improving outcomes for patients undergoing this innovative treatment.
3. CAR-T Cell Therapy Related Toxicities
3.1. Management of Cytokine-Release Syndrome (CRS)
Management of cytokine-release syndrome (CRS) involves a multi-faceted approach aimed at controlling symptoms, reducing inflammation, and managing potential life-threatening complications [35,86,87].
- Tocilizumab: Tocilizumab is a monoclonal antibody that targets the interleukin-6 (IL-6) receptor, thereby inhibiting the pro-inflammatory effects of IL-6. It is considered the primary recommendation for symptom relief in CRS associated with CAR-T cell therapy [36] .
- Corticosteroids: Corticosteroids may be used in conjunction with tocilizumab, particularly in severe cases of CRS. They help suppress inflammation and mitigate immune responses [88].
- Anakinra: Anakinra is an IL-1 receptor antagonist that has shown promise in alleviating both CRS and CRES (CAR-T cell-related encephalopathy syndrome). It can be used as an alternative or adjunctive therapy in managing CRS [88]
- GM-CSF deficiency or inhibition: Granulocyte-macrophage colony-stimulating factor (GM-CSF) deficiency or inhibition has been found to alleviate CRS and CRES while enhancing CAR-T cell anti-tumor effects. This suggests that targeting GM-CSF may be a potential therapeutic strategy for managing CRS [89].
- Reduction of tumor burden: Tumor burden positively correlates with CRS severity. Therefore, reducing tumor burden with traditional chemotherapy or radiotherapy before CAR-T cell infusion may help mitigate the risk and severity of CRS [36].
- Mechanistic understanding: Understanding the underlying mechanisms of CRS, including rapid CAR-T cell activation, cytokine secretion, and immune cell interactions (such as CD40/CD40L), can aid in developing targeted therapies and improving management strategies [87].
3.2. Management of CRS-Related Coagulopathy
In addition to the treatment strategies mentioned, several other considerations are important when managing CRS-related coagulopathy in patients undergoing CAR-T cell therapy:
- Monitoring: Regular monitoring of coagulation parameters, including prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrinogen levels, and D-dimer levels, is essential for early detection of coagulopathy and timely intervention [59]. Imaging studies such as ultrasound or computed tomography (CT) scans may also be necessary to assess for thrombotic complications.
- Risk stratification: Identifying patients at higher risk for developing CRS-related coagulopathy based on factors such as disease characteristics, tumor burden, and baseline coagulation profile can help tailor monitoring and treatment approaches [81].
- Individualized treatment: Treatment strategies should be individualized based on the severity of coagulopathy and the patient’s clinical status. In addition to anticoagulant drugs and replacement therapy, interventions such as fluid resuscitation and vasopressor support may be necessary to maintain hemodynamic stability [90].
- Management of underlying conditions: Addressing underlying conditions that may predispose patients to coagulopathy, such as infections or pre-existing coagulopathies, is crucial for optimal management [82] .
- Collaborative care: Close collaboration between hematologists, oncologists, intensivists, and other healthcare providers is essential for the multidisciplinary management of CRS- related coagulopathy, ensuring timely diagnosis and appropriate treatment [91].
3.3. The Management of T and B Lymphocytes Aplasia and Opportunistic Infections in the Context of CAR-T Cell Therapy Involves Several Key Strategies to Mitigate the Risks and Complications Associated with Immune System Compromise
- Immunoglobulin Supplementation: Given the impaired humoral immunity resulting from the depletion of normal B cells, immunoglobulin supplementation is crucial to restore humoral immunity and reduce the risk of infections. Regular monitoring of gamma globulin levels is essential, and supplementation should be initiated as necessary [92,93,94].
- Infection Monitoring and Prophylaxis: Patients undergoing CAR-T cell therapy are at increased risk of infections, particularly within the first 30 days post-infusion. Close monitoring for signs and symptoms of infection is essential. Prophylactic measures, such as administering acyclovir to prevent herpesvirus infections, are recommended [81].
- Management of Cytokine Release Syndrome (CRS): CRS is a common complication of CAR-T cell therapy and can present with symptoms similar to those of infections. Distinguishing between CRS and infections is crucial for appropriate management. IL-6 plays a significant role in both CRS and infection-induced cytokine storms. Monitoring serum IL-6 levels can help differentiate between the two conditions. Prompt initiation of empiric anti-infective treatment, especially in neutropenic patients, is essential [81].
- Antiviral Prophylaxis for HBV Reactivation: Patients with resolved HBV infections are at risk of HBV reactivation following CAR-T cell therapy. Antiviral prophylaxis and regular monitoring for HBV reactivation are necessary to prevent complications [81].
- Dose-Escalation Regimens: High-dose CAR-T cell infusion may increase the risk of infections. Utilizing dose-escalation regimens may help mitigate this risk while maintaining therapeutic efficacy [86]. Long-term follow-up of patients undergoing CAR-T cell therapy is essential to monitor for potential late-onset complications, including infections and immune system dysregulation.
3.4. Management of Cytopenias
CAR-T cell therapy has revolutionized cancer treatment, particularly for hematologic malignancies. However, one of the significant side effects associated with CAR-T cell therapy is cytopenia, which refers to a reduction in the number of blood cells. Managing cytopenia is crucial for the overall success and safety of CAR-T cell therapy. Here are some strategies for the treatment of cytopenia secondary to CAR-T cell therapy:
- Cytokine Support: Administering cytokines such as interleukin-6 (IL-6), granulocyte colony- stimulating factor (G-CSF), or erythropoietin can help stimulate the production of specific blood cell types, thereby mitigating cytopenia. For example, IL-6 receptor blockade with tocilizumab has been used to manage cytokine release syndrome (CRS) associated with CAR-T cell therapy, which can also help in restoring blood cell counts [88].
- Transfusion Support: Blood transfusions, including packed red blood cells (PRBCs), platelets, and sometimes granulocyte transfusions, may be necessary to manage anemia, thrombocytopenia, and neutropenia resulting from CAR-T cell therapy-induced cytopenia [95].
- Growth Factors: Administration of growth factors such as G-CSF and erythropoietin can stimulate the production of neutrophils and red blood cells, respectively, thereby aiding in the recovery from neutropenia and anemia [96].
- Supportive Care: Maintaining hydration, electrolyte balance, and nutritional support is crucial for patients undergoing CAR-T cell therapy to support bone marrow recovery and mitigate the effects of cytopenia [97].
- Adjusting CAR-T Dose and Conditioning Regimens: Modifying the dose of CAR-T cells administered or adjusting the conditioning regimens used before CAR-T infusion may help reduce the severity of cytopenia while maintaining anti-tumor efficacy [98] .
These studies provide a starting point for further exploration of the management of cytopenia secondary to CAR-T cell therapy. Additionally, consulting recent reviews and guidelines in the field of CAR-T cell therapy can offer comprehensive insights into current strategies for managing cytopenia and other associated adverse events.
3.5. GVHD Management
GVHD is a complication that can occur after a stem cell or bone marrow transplant, where the donor’s immune cells attack the recipient’s tissues. Managing GVHD involves a combination of preventive measures and therapeutic interventions. Here are some general strategies and references for studying GVHD management [99,100,101,102]:
-
Immunosuppressive Medications:
- -
- Corticosteroids (e.g., prednisone) are often used as a first-line treatment.
- -
- Calcineurin inhibitors (e.g., cyclosporine, tacrolimus) are commonly employed to suppress the immune response.
-
Anti-thymocyte Globulin (ATG):
- -
- ATG can be used as part of the conditioning regimen before transplantation to reduce the risk of GVHD.
-
T-Cell Depletion:
- -
- Techniques to selectively remove T cells from the donor graft can reduce the risk of GVHD.
-
Photopheresis:
- -
- Extracorporeal photopheresis is a therapeutic option that involves collecting the patient’s white blood cells, treating them with a photosensitizing agent, and then exposing them to ultraviolet light before returning them to the patient.
-
Topical Therapy:
- -
- For skin involvement, topical corticosteroids or other skin-directed therapies may be employed.
-
Supportive Care:
- -
- Nutritional support, hydration, and infection prevention are crucial components of GVHD management.
Significant studies that have contributed to the advancement of chimeric antigen receptor (CAR) T cell therapy, particularly in the treatment of B-cell malignancies like acute lymphoblastic leukemia (ALL) and chronic lymphocytic leukemia (CLL)
This study focuses on CD19 CAR-T cell therapy in adult patients with B-cell acute lymphoblastic leukemia (B-ALL). The researchers aimed to determine the optimal CD4+:CD8+ T cell composition of CAR-T cells for therapeutic efficacy. They found that a defined CD4+:CD8+ composition of CAR-T cells led to improved clinical outcomes in B-ALL patients, with higher complete remission rates and prolonged remission durations. This study highlights the importance of optimizing the composition of CAR-T cells to enhance their anti-tumor activity and improve patient outcomes in B-cell malignancies [98].
This landmark study demonstrates the efficacy of CD19 CAR-T cell therapy in pediatric and young adult patients with relapsed or refractory ALL. The researchers reported high rates of complete remission and durable responses following CD19 CAR-T cell infusion, leading to sustained remissions in a significant proportion of patients. The study highlights the potential of CAR-T cell therapy as a promising treatment approach for patients with relapsed or refractory leukemia, offering the possibility of long-term disease control and even cure [36].
This study investigates the use of CD19 CAR-T cell therapy in patients with relapsed or refractory chronic lymphocytic leukemia (CLL), a type of B-cell malignancy. The researchers observed sustained remissions and durable responses in a subset of CLL patients treated with CD19 CAR-T cells, with some patients achieving long-term disease control. This study underscores the potential of CAR-T cell therapy as a promising treatment option for patients with CLL who have failed conventional therapies, offering the possibility of prolonged survival and improved quality of life [103]. Overall, these studies highlight the significant therapeutic potential of CAR-T cell therapy in the treatment of B-cell malignancies, providing hope for patients with relapsed or refractory disease who have limited treatment options.

| CAR-T cell Therapy | Targeted antigen |
Cancer Type | Notes |
|---|---|---|---|
| bb21217 | BCMA | Multiple myeloma | Enhanced persistence CAR-T therapy; in clinical trials |
| CTL019 | CD19 | B-cell malignancies | Early version of Kymriah; basis for FDA-approved therapy |
| CART-PSMA | PSMA | Prostate cancer | Investigational CAR-T therapy; in early-phase trials |
| CAR-EGFRvIII | EGFRvIII | Glioblastoma | Investigational CAR-T therapy targeting specific EGFR mutation |
| Mesothelin-CAR-T | Mesothelin | Mesothelioma, ovarian cancer | Experimental CAR-T therapy targeting mesothelin |
| MUC1-CAR-T | MUC1 | Various solid tumours | Investigational CAR-T therapy for multiple epithelial cancers |
| Kymriah (tisagenlecleucel) | CD19 | B-cell acute lymphoblastic leukemia (ALL) | First FDA-approved CAR-T therapy for paediatric and young adult patients |
| Yescarta (axicabtagene ciloleucel) | CD19 | Large B-cell lymphoma | Approved for adults with relapsed or refractory large B-cell lymphoma |
| Tecartus (brexucabtagene autoleucel) | CD19 | Mantle cell lymphoma | Approved for adults with relapsed or refractory mantle cell lymphoma |
| Breyanzi (lisocabtagene maraleucel) | CD19 | Large B-cell lymphoma | Approved for adults with relapsed or refractory large B-cell lymphoma |
| Abecma (idecabtagene vicleucel) | BCMA | Multiple myeloma | First FDA-approved CAR-T therapy targeting BCMA for multiple myeloma |
| Carvykti (ciltacabtagene autoleucel) | BCMA | Multiple myeloma | Another BCMA-targeting CAR-T therapy for multiple myeloma |
| ALLO-501 (Allogeneic) | CD19 | Non-Hodgkin lymphoma | Allogeneic CAR-T therapy under investigation; uses donor-derived cells |
| JCARH125 | BCMA | Multiple myeloma | Experimental CAR-T therapy; in clinical trials |
| CT053 | BCMA | Multiple myeloma | Investigational CAR-T therapy; in clinical trials |
This table highlights some of the key CAR-T cell therapies, their targeted antigens, the cancer types they treat, and any relevant notes regarding their approval status or investigational stage.
Table 5.
Methods for studying the binding of CAR-T cells to antigens.
| Method Type |
Method | Description | Advantages | Limitations |
|---|---|---|---|---|
| Conventional Methods |
Flow cytometry | Uses fluorescently labeled antibodies to measure the binding of CAR-T cells to antigens | High throughput, quantitative, multiple parameters | Requires fluorophore-labelled antibodies, can be costly |
| Conventional Methods |
Enzyme-Linked Immunosorbent Assay (ELISA) | Measures binding indirectly by detecting cytokines or other proteins released upon CAR-T cell activation | Sensitive, quantitative | Indirect measurement, labor-intensive, endpoint analysis |
| Conventional Methods |
Immunohistochemistry (IHC) | Detects CAR-T cell binding to antigens in tissue sections using specific antibodies | Visual localization, can analyse tissue architecture | Qualitative, less quantitative, requires tissue samples |
| Conventional Methods |
Radioimmunoassay (RIA) | Uses radiolabelled antigens to study binding interactions | Highly sensitive, quantitative | Use of radioisotopes, safety concerns, expensive equipment |
| Advanced Methods |
Surface Plasmon Resonance (SPR) | Measures real-time binding kinetics of CAR-T cells to antigens on a sensor chip | Real-time data, kinetic analysis, no labelling required | Expensive, requires Specialized equipment |
| Advanced Methods |
Single-Cell RNA Sequencing (scRNA-seq) | Analyses gene expression of individual CAR-T cells to infer binding and activation states | High resolution, comprehensive data | Complex data analysis, high cost |
| Advanced Methods |
CRISPR Screening | Uses CRISPR/Cas9 to identify genes involved in CAR-T cell binding and activation | High-throughput, functional insights | Requires extensive validation, expensive |
| Advanced Methods |
Microscopy (Confocal, TIRF) | Visualizes the interaction of CAR-T cells with antigen-expressing cells using high-resolution imaging | High spatial resolution, dynamic studies possible | Limited to surface interactions, expensive equipment |
| Advanced Methods |
Mass Cytometry (CyTOF) | Combines flow cytometry with mass spectrometry for detailed phenotypic analysis | Multiparametric, high dimensional data | Requires specialized equipment, complex data interpretation |
| Advanced Methods |
Biolayer Interferometry (BLI) | Measures binding interactions by detecting changes in optical thickness on a biosensor surface | Real-time data, label-free | Less sensitive than SPR, limited to specific applications |
| Advanced Methods |
Multiplexed Cytokine Assays | Simultaneously measures multiple cytokines released upon CAR-T cell binding using bead-based methods | High throughput, comprehensive profiling | Requires multiplexing capability, can be costly |
| Advanced Methods |
Atomic Force Microscopy (AFM) | Measures the forces involved in CAR-T cell binding to antigens at the nanoscale | High sensitivity, detailed mechanical data | Technically challenging, expensive, limited throughput |
Conventional methods such as flow cytometry, ELISA, and immunohistochemistry are widely used for studying CAR-T cell binding to antigens due to their accessibility and established protocols. These methods provide quantitative and qualitative insights but may have limitations in terms of sensitivity and throughput. Advanced methods like surface plasmon resonance (SPR), single-cell RNA sequencing (scRNA-seq), and CRISPR screening offer deeper insights into binding kinetics, gene expression, and functional genomics. These techniques, while more expensive and complex, provide high-resolution data and comprehensive analysis, enabling a more detailed understanding of CAR-T cell interactions with target antigens [106,107,108].
4. Conclusion
In conclusion, CAR-T cell therapy represents a transformative approach in cancer treatment, particularly in hematological malignancies. The FDA-approved CAR-T cell products have demonstrated remarkable efficacy in patients with relapsed or refractory B-cell acute lymphocytic leukemia, non-Hodgkin lymphoma, and multiple myeloma, significantly improving treatment outcomes. However, several challenges and opportunities lie ahead in advancing this therapy further. Firstly, the development of multi-targeted CAR-T cells holds immense promise in overcoming tumor heterogeneity and reducing the likelihood of relapse. By targeting multiple antigens simultaneously, researchers aim to enhance treatment efficacy and achieve more durable responses in patients. Secondly, efforts to improve the persistence and longevity of CAR-T cells within the body are crucial for achieving sustained tumor control and long-term remissions.
Strategies such as incorporating co-stimulatory domains into CAR constructs and cytokine modulation show potential in promoting T cell survival and expansion. Thirdly, expanding the scope of CAR-T cell therapy to solid tumors presents unique challenges, including the immunosuppressive tumor microenvironment and off-target toxicity. Nonetheless, ongoing research endeavors aim to adapt CAR-T cell therapy for solid tumor treatment through the development of novel CAR constructs and combinatorial approaches with other immunotherapies.
Addressing safety concerns associated with CAR-T cell therapy remains paramount. While significant progress has been made in mitigating toxicities such as cytokine release syndrome and coagulopathy, further refinement of treatment protocols and personalized approaches are essential to minimize adverse events while preserving anti-tumor efficacy. Furthermore, strategies to combat antigen-negative relapse, such as dual-targeting or multi-targeted CAR-T cells and leveraging alternative cell types like γδ T cells, offer promising avenues for enhancing recognition and efficacy while minimizing adverse effects. In summary, CAR-T cell therapy represents a paradigm shift in cancer treatment, with ongoing research and innovation poised to further enhance its efficacy, expand its applicability to a broader range of cancers, and improve its safety profile. With continued advancements in CAR-T cell technology and translational research, the future holds immense promise for revolutionizing cancer therapy and improving outcomes for patients worldwide.
Author Contributions
The manuscript was conceptualized by Angel Justiz-Vaillant and planning and discussion were conducted by all authors. Angel Justiz-Vaillant wrote the initial draft of the manuscript. A.J.-V. and all authors investigated and reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study did not receive any external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Data are available within the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhang, X.; Zhu, L.; Zhang, H.; Chen, S.; Xiao, Y. CAR-T Cell Therapy in Hematological Malignancies: Current Opportunities and Challenges. Front Immunol. 2022, 13, 927153. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- Sang, W.; Shi, M.; Yang, J.; Cao, J.; Xu, L.; Yan, D.; Yao, M.; Liu, H.; Li, W.; Zhang, B.; et al. Phase II Trial of Co-Administration of CD19- and CD20-Targeted Chimeric Antigen Receptor T Cells for Relapsed and Refractory Diffuse Large B Cell Lymphoma. Cancer Med. 2020, 9, 5827–5838. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T- Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Jacobson, C.A.; Chavez, J.C.; Sehgal, A.R.; William, B.M.; Munoz, J.; Salles, G.; Munshi, P.N.; Casulo, C.; Maloney, D.G.; de Vos, S.; et al. Axicabtagene Ciloleucel in Relapsed or Refractory Indolent Non-Hodgkin Lymphoma (ZUMA-5): A Single-Arm, Multicentre, Phase 2 Trial. Lancet Oncol. 2022, 23, 91–103. [Google Scholar] [CrossRef]
- Locke, F.L.; Ghobadi, A.; Jacobson, C.A.; Miklos, D.B.; Lekakis, L.J.; Oluwole, O.O.; Lin, Y.; Braunschweig, I.; Hill, B.T.; Timmerman, J.M.; et al. Long-Term Safety and Activity of Axicabtagene Ciloleucel in Refractory Large B-Cell Lymphoma (ZUMA-1): A Single-Arm, Multicentre, Phase 1-2 Trial. Lancet Oncol. 2019, 20, 31–42. [Google Scholar] [CrossRef]
- Watanabe, N.; Mo, F.; McKenna, M.K. Impact of Manufacturing Procedures on CAR T Cell Functionality. Front. Immunol. 2022, 13, 876339. [Google Scholar] [CrossRef]
- Labbé, R.P.; Vessillier, S.; Rafiq, Q.A. Lentiviral Vectors for T Cell Engineering: Clinical Applications, Bioprocessing and Future Perspectives. Viruses 2021, 13. [Google Scholar] [CrossRef]
- Kamdar, M.; Solomon, S.R.; Arnason, J.; Johnston, P.B.; Glass, B.; Bachanova, V.; Ibrahimi, S.; Mielke, S.; Mutsaers, P.; Hernandez-Ilizaliturri, F.; et al. Lisocabtagene Maraleucel versus Standard of Care with Salvage Chemotherapy Followed by Autologous Stem Cell Transplantation as Second-Line Treatment in Patients with Relapsed or Refractory Large B-Cell Lymphoma (TRANSFORM): Results from an Interim Analysis of an Open-Label, Randomised, Phase 3 Trial. Lancet 2022, 399, 2294–2308. [Google Scholar]
- Sehgal, A.; Hoda, D.; Riedell, P.A.; Ghosh, N.; Hamadani, M.; Hildebrandt, G.C.; Godwin, J.E.; Reagan, P.M.; Wagner-Johnston, N.; Essell, J.; et al. Lisocabtagene Maraleucel as Second-Line Therapy in Adults with Relapsed or Refractory Large B-Cell Lymphoma Who Were Not Intended for Haematopoietic Stem Cell Transplantation (PILOT): An Open-Label, Phase 2 Study. Lancet Oncol. 2022, 23, 1066–1077. [Google Scholar] [CrossRef]
- Kharfan-Dabaja, M.A.; Yassine, F.; Moustafa, M.A.; Iqbal, M.; Murthy, H. Lisocabtagene Maraleucel in Relapsed or Refractory Diffuse Large B Cell Lymphoma: What Is the Evidence? Hematol. Oncol. Stem Cell Ther. 2022, 15, 168–175. [Google Scholar] [CrossRef]
- Munshi, N.C.; Anderson, L.D., Jr; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef]
- Hansen, D.K.; Sidana, S.; Peres, L.C.; Colin Leitzinger, C.; Shune, L.; Shrewsbury, A.; Gonzalez, R.; Sborov, D.W.; Wagner, C.; Dima, D.; et al. Idecabtagene Vicleucel for Relapsed/Refractory Multiple Myeloma: Real-World Experience From the Myeloma CAR T Consortium. J. Clin. Oncol. 2023, 41, 2087–2097. [Google Scholar] [CrossRef]
- Jagannath, S.; Lin, Y.; Goldschmidt, H.; Reece, D.; Nooka, A.; Senin, A.; Rodriguez-Otero, P.; Powles, R.; Matsue, K.; Shah, N.; et al. KarMMa-RW: Comparison of Idecabtagene Vicleucel with Real-World Outcomes in Relapsed and Refractory Multiple Myeloma. Blood Cancer J. 2021, 11, 116. [Google Scholar] [CrossRef]
- Berdeja, J.G.; Madduri, D.; Usmani, S.Z.; Jakubowiak, A.; Agha, M.; Cohen, A.D.; Stewart, A.K.; Hari, P.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene Autoleucel, a B-Cell Maturation Antigen-Directed Chimeric Antigen Receptor T-Cell Therapy in Patients with Relapsed or Refractory Multiple Myeloma (CARTITUDE-1): A Phase 1b/2 Open-Label Study. Lancet 2021, 398, 314–324. [Google Scholar] [CrossRef]
- Mi, J.-Q.; Zhao, W.; Jing, H.; Fu, W.; Hu, J.; Chen, L.; Zhang, Y.; Yao, D.; Chen, D.; Schecter, J.M.; et al. Phase II, Open-Label Study of Ciltacabtagene Autoleucel, an Anti-B- Cell Maturation Antigen Chimeric Antigen Receptor-T-Cell Therapy, in Chinese Patients With Relapsed/Refractory Multiple Myeloma (CARTIFAN-1). J. Clin. Oncol. 2023, 41, 1275–1284. [Google Scholar] [CrossRef]
- Lindo, L.; Wilkinson, L.H.; Hay, K.A. Befriending the Hostile Tumor Microenvironment in CAR T-Cell Therapy. Front. Immunol. 2020, 11, 618387. [Google Scholar] [CrossRef]
- Bell, M.; Gottschalk, S. Engineered Cytokine Signaling to Improve CAR T Cell Effector Function. Front. Immunol. 2021, 12, 684642. [Google Scholar] [CrossRef]
- López-Cantillo, G.; Urueña, C.; Camacho, B.A.; Ramírez-Segura, C. CAR-T Cell Performance: How to Improve Their Persistence? Front. Immunol. 2022, 13, 878209. [Google Scholar] [CrossRef]
- Corti, C.; Venetis, K.; Sajjadi, E.; Zattoni, L.; Curigliano, G.; Fusco, N. CAR-T Cell Therapy for Triple-Negative Breast Cancer and Other Solid Tumors: Preclinical and Clinical Progress. Expert Opin. Investig. Drugs 2022, 31, 593–605. [Google Scholar] [CrossRef]
- Guzman, G.; Reed, M.R.; Bielamowicz, K.; Koss, B.; Rodriguez, A. CAR-T Therapies in Solid Tumors: Opportunities and Challenges. Curr. Oncol. Rep. 2023, 25, 479–489. [Google Scholar] [CrossRef]
- Roex, G.; Campillo-Davo, D.; Flumens, D.; Shaw, P.A.G.; Krekelbergh, L.; De Reu, H.; Berneman, Z.N.; Lion, E.; Anguille, S. Two for One: Targeting BCMA and CD19 in B-Cell Malignancies with off-the-Shelf Dual-CAR NK-92 Cells. J. Transl. Med. 2022, 20, 124. [Google Scholar] [CrossRef]
- Viardot, A.; Locatelli, F.; Stieglmaier, J.; Zaman, F.; Jabbour, E. Concepts in Immuno- Oncology: Tackling B Cell Malignancies with CD19-Directed Bispecific T Cell Engager Therapies. Ann. Hematol. 2020, 99, 2215–2229. [Google Scholar] [CrossRef]
- Hay, K.A.; Turtle, C.J. Chimeric Antigen Receptor (CAR) T Cells: Lessons Learned from Targeting of CD19 in B-Cell Malignancies. Drugs 2017, 77, 237–245. [Google Scholar] [CrossRef]
- Strati, P.; Neelapu, S.S. CAR-T Failure: Beyond Antigen Loss and T Cells. Blood 2021, 137, 2567–2568. [Google Scholar] [CrossRef]
- Mulgaonkar, A.; Udayakumar, D.; Yang, Y.; Harris, S.; Öz, O.K.; Ramakrishnan Geethakumari, P.; Sun, X. Current and Potential Roles of Immuno-PET/-SPECT in CAR T- Cell Therapy. Front. Med. 2023, 10, 1199146. [Google Scholar] [CrossRef]
- Duell, J.; Leipold, A.M.; Appenzeller, S.; Fuhr, V.; Rauert-Wunderlich, H.; Da Via, M.; Dietrich, O.; Toussaint, C.; Imdahl, F.; Eisele, F.; et al. Sequential Antigen Loss and Branching Evolution in Lymphoma after CD19- and CD20-Targeted T-Cell-Redirecting Therapy. Blood 2024, 143, 685–696. [Google Scholar] [CrossRef]
- Al-Haideri, M.; Tondok, S.B.; Safa, S.H.; Maleki, A.H.; Rostami, S.; Jalil, A.T.; Al-Gazally, M.E.; Alsaikhan, F.; Rizaev, J.A.; Mohammad, T.A.M.; et al. CAR-T Cell Combination Therapy: The next Revolution in Cancer Treatment. Cancer Cell Int. 2022, 22, 365. [Google Scholar] [CrossRef]
- Liu, Z.; Lei, W.; Wang, H.; Liu, X.; Fu, R. Challenges and Strategies Associated with CAR-T Cell Therapy in Blood Malignancies. Exp. Hematol. Oncol. 2024, 13, 22. [Google Scholar] [CrossRef] [PubMed]
- Baird, J.H.; Frank, M.J.; Craig, J.; Patel, S.; Spiegel, J.Y.; Sahaf, B.; Oak, J.S.; Younes, S.F.; Ozawa, M.G.; Yang, E.; et al. CD22-Directed CAR T-Cell Therapy Induces Complete Remissions in CD19-Directed CAR-Refractory Large B-Cell Lymphoma. Blood 2021, 137, 2321–2325. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Laetsch, T.W.; Buechner, J.; Rives, S.; Boyer, M.; Bittencourt, H.; Bader, P.; Verneris, M.R.; Stefanski, H.E.; Myers, G.D.; et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Maus, M.V.; June, C.H. Making Better Chimeric Antigen Receptors for Adoptive T-Cell Therapy. Clin. Cancer Res. 2016, 22, 1875–1884. [Google Scholar] [CrossRef] [PubMed]
- Sadelain, M.; Brentjens, R.; Rivière, I. The Basic Principles of Chimeric Antigen Receptor Design. Cancer Discov. 2013, 3, 388–398. [Google Scholar] [CrossRef] [PubMed]
- June, C.H.; Sadelain, M. Chimeric Antigen Receptor Therapy. N. Engl. J. Med. 2018, 379, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Kochenderfer, J.N.; Stetler-Stevenson, M.; Cui, Y.K.; Delbrook, C.; Feldman, S.A.; Fry, T.J.; Orentas, R.; Sabatino, M.; Shah, N.N.; et al. T Cells Expressing CD19 Chimeric Antigen Receptors for Acute Lymphoblastic Leukaemia in Children and Young Adults: A Phase 1 Dose-Escalation Trial. Lancet 2015, 385, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Frey, N.; Shaw, P.A.; Aplenc, R.; Barrett, D.M.; Bunin, N.J.; Chew, A.; Gonzalez, V.E.; Zheng, Z.; Lacey, S.F.; et al. Chimeric Antigen Receptor T Cells for Sustained Remissions in Leukemia. N. Engl. J. Med. 2014, 371, 1507–1517. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.L.; Miskin, J.; Wonnacott, K.; Keir, C. Global Manufacturing of CAR T Cell Therapy. Mol Ther Methods Clin Dev 2017, 4, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Turtle, C.J.; Hanafi, L.-A.; Berger, C.; Hudecek, M.; Pender, B.; Robinson, E.; Hawkins, R.; Chaney, C.; Cherian, S.; Chen, X.; et al. Immunotherapy of Non-Hodgkin’s Lymphoma with a Defined Ratio of CD8+ and CD4+ CD19-Specific Chimeric Antigen Receptor-Modified T Cells. Sci. Transl. Med. 2016, 8, 355ra116. [Google Scholar] [CrossRef] [PubMed]
- Heuser, C.; Hombach, A.; Lösch, C.; Manista, K.; Abken, H. T-Cell Activation by Recombinant Immunoreceptors: Impact of the Intracellular Signalling Domain on the Stability of Receptor Expression and Antigen-Specific Activation of Grafted T Cells. Gene Ther. 2003, 10, 1408–1419. [Google Scholar] [CrossRef]
- Guedan, S.; Posey, A.D., Jr; Shaw, C.; Wing, A.; Da, T.; Patel, P.R.; McGettigan, S.E.; Casado-Medrano, V.; Kawalekar, O.U.; Uribe-Herranz, M.; et al. Enhancing CAR T Cell Persistence through ICOS and 4-1BB Costimulation. JCI Insight 2018, 3. [Google Scholar] [CrossRef]
- Finney, H.M.; Akbar, A.N.; Lawson, A.D.G. Activation of Resting Human Primary T Cells with Chimeric Receptors: Costimulation from CD28, Inducible Costimulator, CD134, and CD137 in Series with Signals from the TCR Zeta Chain. J. Immunol. 2004, 172, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Song, D.-G.; Ye, Q.; Poussin, M.; Harms, G.M.; Figini, M.; Powell, D.J., Jr. CD27 Costimulation Augments the Survival and Antitumor Activity of Redirected Human T Cells in Vivo. Blood 2012, 119, 696–706. [Google Scholar] [CrossRef] [PubMed]
- Guercio, M.; Orlando, D.; Di Cecca, S.; Sinibaldi, M.; Boffa, I.; Caruso, S.; Abbaszadeh, Z.; Camera, A.; Cembrola, B.; Bovetti, K.; et al. CD28.OX40 Co-Stimulatory Combination Is Associated with Long in Vivo Persistence and High Activity of CAR.CD30 T-Cells. Haematologica 2021, 106, 987–999. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Xia, K.; Xie, Y.; Ye, S.; Ding, Y.; Liu, Z.; Zheng, R.; Long, J.; Wei, Q.; Li, Y.; et al. Combination of 4-1BB and DAP10 Promotes Proliferation and Persistence of NKG2D(bbz) CAR-T Cells. Front. Oncol. 2022, 12, 893124. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Chen, Z.; Sun, M.; Li, B.; Pan, F.; Ma, A.; Liao, J.; Yin, T.; Tang, X.; Huang, G.; et al. IL-12 Nanochaperone-Engineered CAR T Cell for Robust Tumor-Immunotherapy. Biomaterials 2022, 281, 121341. [Google Scholar] [CrossRef] [PubMed]
- Avanzi, M.P.; Yeku, O.; Li, X.; Wijewarnasuriya, D.P.; van Leeuwen, D.G.; Cheung, K.; Park, H.; Purdon, T.J.; Daniyan, A.F.; Spitzer, M.H.; et al. Engineered Tumor-Targeted T Cells Mediate Enhanced Anti-Tumor Efficacy Both Directly and through Activation of the Endogenous Immune System. Cell Rep. 2018, 23, 2130–2141. [Google Scholar] [CrossRef] [PubMed]
- Chmielewski, M.; Abken, H. CAR T Cells Releasing IL-18 Convert to T-Bethigh FoxO1low Effectors That Exhibit Augmented Activity against Advanced Solid Tumors. Cell Rep. 2017, 21, 3205–3219. [Google Scholar] [CrossRef] [PubMed]
- Obstfeld, A.E.; Frey, N.V.; Mansfield, K.; Lacey, S.F.; June, C.H.; Porter, D.L.; Melenhorst, J.J.; Wasik, M.A. Cytokine Release Syndrome Associated with Chimeric-Antigen Receptor T-Cell Therapy: Clinicopathological Insights. Blood 2017, 130, 2569–2572. [Google Scholar] [CrossRef] [PubMed]
- Dong, R.; Jiang, S.; Chen, Y.; Ma, Y.; Sun, L.; Xing, C.; Zhang, S.; Yu, K. Prognostic Significance of Cytokine Release Syndrome in B Cell Hematological Malignancies Patients After Chimeric Antigen Receptor T Cell Therapy. J. Interferon Cytokine Res. 2021, 41, 469–476. [Google Scholar] [CrossRef]
- Norelli, M.; Camisa, B.; Barbiera, G.; Falcone, L.; Purevdorj, A.; Genua, M.; Sanvito, F.; Ponzoni, M.; Doglioni, C.; Cristofori, P.; et al. Monocyte-Derived IL-1 and IL-6 Are Differentially Required for Cytokine-Release Syndrome and Neurotoxicity due to CAR T Cells. Nat. Med. 2018, 24, 739–748. [Google Scholar] [CrossRef]
- Qi, C.; Tian, S.; Wang, J.; Ma, H.; Qian, K.; Zhang, X. Co-Expression of CD40/CD40L on XG1 Multiple Myeloma Cells Promotes IL-6 Autocrine Function. Cancer Invest. 2015, 33, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Giavridis, T.; van der Stegen, S.J.C.; Eyquem, J.; Hamieh, M.; Piersigilli, A.; Sadelain, M. CAR T Cell-Induced Cytokine Release Syndrome Is Mediated by Macrophages and Abated by IL-1 Blockade. Nat. Med. 2018, 24, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; Cron, R.Q.; Hartwell, J.; Manson, J.J.; Tattersall, R.S. Silencing the Cytokine Storm: The Use of Intravenous Anakinra in Haemophagocytic Lymphohistiocytosis or Macrophage Activation Syndrome. Lancet Rheumatol 2020, 2, e358–e367. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Zhou, L.; Ye, S.; Zhang, W.; Wang, J.; Tang, X.; Liu, J.; Xu, Y.; Qian, W.; Liang, A. Risk of HBV Reactivation in Patients With Resolved HBV Infection Receiving Anti-CD19 Chimeric Antigen Receptor T Cell Therapy Without Antiviral Prophylaxis. Front. Immunol. 2021, 12, 638678. [Google Scholar] [CrossRef]
- Wei, J.; Zhao, J.; Han, M.; Meng, F.; Zhou, J. SARS-CoV-2 Infection in Immunocompromised Patients: Humoral versus Cell-Mediated Immunity. J Immunother Cancer 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- deHaas, P.A.; Young, R.D. Attention Styles of Hyperactive and Normal Girls. J. Abnorm. Child Psychol. 1984, 12, 531–546. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, F.A.; Bernstein, I.L.; Khan, D.A.; Ballas, Z.K.; Chinen, J.; Frank, M.M.; Kobrynski, L.J.; Levinson, A.I.; Mazer, B.; Nelson, R.P., Jr; et al. Practice Parameter for the Diagnosis and Management of Primary Immunodeficiency. Ann. Allergy Asthma Immunol. 2005, 94, S1–S63. [Google Scholar] [CrossRef] [PubMed]
- Chapel, H.; Cunningham-Rundles, C. Update in Understanding Common Variable Immunodeficiency Disorders (CVIDs) and the Management of Patients with These Conditions. Br. J. Haematol. 2009, 145, 709–727. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Romero, F.A.; Taur, Y.; Sadelain, M.; Brentjens, R.J.; Hohl, T.M.; Seo, S.K. Cytokine Release Syndrome Grade as a Predictive Marker for Infections in Patients With Relapsed or Refractory B-Cell Acute Lymphoblastic Leukemia Treated With Chimeric Antigen Receptor T Cells. Clin. Infect. Dis. 2018, 67, 533–540. [Google Scholar] [CrossRef]
- Mak, J.W.Y.; Law, A.W.H.; Law, K.W.T.; Ho, R.; Cheung, C.K.M.; Law, M.F. Prevention and Management of Hepatitis B Virus Reactivation in Patients with Hematological Malignancies in the Targeted Therapy Era. World J. Gastroenterol. 2023, 29, 4942–4961. [Google Scholar] [CrossRef]
- Wei, J.; Zhu, X.; Mao, X.; Huang, L.; Meng, F.; Zhou, J. Severe Early Hepatitis B Reactivation in a Patient Receiving Anti-CD19 and Anti-CD22 CAR T Cells for the Treatment of Diffuse Large B-Cell Lymphoma. J Immunother Cancer 2019, 7, 315. [Google Scholar] [CrossRef]
- Murthy, H.; Iqbal, M.; Chavez, J.C.; Kharfan-Dabaja, M.A. Cytokine Release Syndrome: Current Perspectives. Immunotargets Ther 2019, 8, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Johnsrud, A.; Craig, J.; Baird, J.; Spiegel, J.; Muffly, L.; Zehnder, J.; Tamaresis, J.; Negrin, R.; Johnston, L.; Arai, S.; et al. Incidence and Risk Factors Associated with Bleeding and Thrombosis Following Chimeric Antigen Receptor T-Cell Therapy. Blood Adv 2021, 5, 4465–4475. [Google Scholar] [CrossRef]
- Wang, Y.; Qi, K.; Cheng, H.; Cao, J.; Shi, M.; Qiao, J.; Yan, Z.; Jing, G.; Pan, B.; Sang, W.; et al. Coagulation Disorders after Chimeric Antigen Receptor T Cell Therapy: Analysis of 100 Patients with Relapsed and Refractory Hematologic Malignancies. Biol. Blood Marrow Transplant. 2020, 26, 865–875. [Google Scholar] [CrossRef]
- Shao, M.; Yu, Q.; Teng, X.; Guo, X.; Wei, G.; Xu, H.; Cui, J.; Chang, A.H.; Hu, Y.; Huang, H. CRS-Related Coagulopathy in BCMA Targeted CAR-T Therapy: A Retrospective Analysis in a Phase I/II Clinical Trial. Bone Marrow Transplant. 2021, 56, 1642–1650. [Google Scholar] [CrossRef] [PubMed]
- Mavroudi, I.; Papadaki, V.; Pyrovolaki, K.; Katonis, P.; Eliopoulos, A.G.; Papadaki, H.A. The CD40/CD40 Ligand Interactions Exert Pleiotropic Effects on Bone Marrow Granulopoiesis. J. Leukoc. Biol. 2011, 89, 771–783. [Google Scholar] [CrossRef]
- Xing, L.; Wang, Y.; Liu, H.; Gao, S.; Shao, Q.; Yue, L.; Liu, Z.; Wang, H.; Shao, Z.; Fu, R. Case Report: Sirolimus Alleviates Persistent Cytopenia After CD19 CAR-T-Cell Therapy. Front. Oncol. 2021, 11, 798352. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, R.; Graham, C.; Yallop, D.; Jozwik, A.; Mirci-Danicar, O.C.; Lucchini, G.; Pinner, D.; Jain, N.; Kantarjian, H.; Boissel, N.; et al. Genome-Edited, Donor-Derived Allogeneic Anti-CD19 Chimeric Antigen Receptor T Cells in Paediatric and Adult B-Cell Acute Lymphoblastic Leukaemia: Results of Two Phase 1 Studies. Lancet 2020, 396, 1885–1894. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Tang, K.; Luo, Y.; Seery, S.; Tan, Y.; Deng, B.; Liu, F.; Xu, X.; Ling, Z.; Song, W.; et al. Sequential CD19 and CD22 Chimeric Antigen Receptor T-Cell Therapy for Childhood Refractory or Relapsed B-Cell Acute Lymphocytic Leukaemia: A Single-Arm, Phase 2 Study. Lancet Oncol. 2023, 24, 1229–1241. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.N.; Fry, T.J. Mechanisms of Resistance to CAR T Cell Therapy. Nat. Rev. Clin. Oncol. 2019, 16, 372–385. [Google Scholar] [CrossRef]
- Xu, X.; Sun, Q.; Liang, X.; Chen, Z.; Zhang, X.; Zhou, X.; Li, M.; Tu, H.; Liu, Y.; Tu, S.; et al. Mechanisms of Relapse After CD19 CAR T-Cell Therapy for Acute Lymphoblastic Leukemia and Its Prevention and Treatment Strategies. Front. Immunol. 2019, 10, 2664. [Google Scholar] [CrossRef] [PubMed]
- Schultz, L. Chimeric Antigen Receptor T Cell Therapy for Pediatric B-ALL: Narrowing the Gap Between Early and Long-Term Outcomes. Front. Immunol. 2020, 11, 1985. [Google Scholar] [CrossRef] [PubMed]
- Leahy, A.B.; Newman, H.; Li, Y.; Liu, H.; Myers, R.; DiNofia, A.; Dolan, J.G.; Callahan, C.; Baniewicz, D.; Devine, K.; et al. CD19-Targeted Chimeric Antigen Receptor T-Cell Therapy for CNS Relapsed or Refractory Acute Lymphocytic Leukaemia: A Post-Hoc Analysis of Pooled Data from Five Clinical Trials. Lancet Haematol 2021, 8, e711–e722. [Google Scholar] [CrossRef] [PubMed]
- Hayden, P.J.; Roddie, C.; Bader, P.; Basak, G.W.; Bonig, H.; Bonini, C.; Chabannon, C.; Ciceri, F.; Corbacioglu, S.; Ellard, R.; et al. Management of Adults and Children Receiving CAR T-Cell Therapy: 2021 Best Practice Recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann. Oncol. 2022, 33, 259–275. [Google Scholar] [PubMed]
- Ganapathy, T.; Radhakrishnan, R.; Sakshi, S.; Martin, S. CAR γδ T Cells for Cancer Immunotherapy. Is the Field More Yellow than Green? Cancer Immunol. Immunother. 2023, 72, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, H.R.; Mirzaei, H.; Lee, S.Y.; Hadjati, J.; Till, B.G. Prospects for Chimeric Antigen Receptor (CAR) γδ T Cells: A Potential Game Changer for Adoptive T Cell Cancer Immunotherapy. Cancer Lett. 2016, 380, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Deng, B.; Yin, Z.; Lin, Y.; An, L.; Liu, D.; Pan, J.; Yu, X.; Chen, B.; Wu, T.; et al. Combination of CD19 and CD22 CAR-T Cell Therapy in Relapsed B-Cell Acute Lymphoblastic Leukemia after Allogeneic Transplantation. Am. J. Hematol. 2021, 96, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Wu, Z.; Jia, H.; Tong, C.; Guo, Y.; Ti, D.; Han, X.; Liu, Y.; Zhang, W.; Wang, C.; et al. Bispecific CAR-T Cells Targeting Both CD19 and CD22 for Therapy of Adults with Relapsed or Refractory B Cell Acute Lymphoblastic Leukemia. J. Hematol. Oncol. 2020, 13, 30. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Ding, L.; Shi, W.; Wan, X.; Yang, X.; Yang, J.; Wang, T.; Song, L.; Wang, X.; Ma, Y.; et al. Safety and Efficacy of Co-Administration of CD19 and CD22 CAR-T Cells in Children with B-ALL Relapse after CD19 CAR-T Therapy. J. Transl. Med. 2023, 21, 213. [Google Scholar] [CrossRef]
- Gust, J.; Hay, K.A.; Hanafi, L.-A.; Li, D.; Myerson, D.; Gonzalez-Cuyar, L.F.; Yeung, C.; Liles, W.C.; Wurfel, M.; Lopez, J.A.; et al. Endothelial Activation and Blood-Brain Barrier Disruption in Neurotoxicity after Adoptive Immunotherapy with CD19 CAR-T Cells. Cancer Discov. 2017, 7, 1404–1419. [Google Scholar] [CrossRef]
- Lee, D.W.; Santomasso, B.D.; Locke, F.L.; Ghobadi, A.; Turtle, C.J.; Brudno, J.N.; Maus, M.V.; Park, J.H.; Mead, E.; Pavletic, S.; et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol. Blood Marrow Transplant. 2019, 25, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Tummala, S.; Kebriaei, P.; Wierda, W.; Gutierrez, C.; Locke, F.L.; Komanduri, K.V.; Lin, Y.; Jain, N.; Daver, N.; et al. Chimeric Antigen Receptor T-Cell Therapy - Assessment and Management of Toxicities. Nat. Rev. Clin. Oncol. 2018, 15, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Santomasso, B.D.; Park, J.H.; Salloum, D.; Riviere, I.; Flynn, J.; Mead, E.; Halton, E.; Wang, X.; Senechal, B.; Purdon, T.; et al. Clinical and Biological Correlates of Neurotoxicity Associated with CAR T-Cell Therapy in Patients with B-Cell Acute Lymphoblastic Leukemia. Cancer Discov. 2018, 8, 958–971. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B.; Danish, H.H.; Ali, A.B.; Li, K.; LaRose, S.; Monk, A.D.; Cote, D.J.; Spendley, L.; Kim, A.H.; Robertson, M.S.; et al. Neurological Toxicities Associated with Chimeric Antigen Receptor T-Cell Therapy. Brain 2019, 142, 1334–1348. [Google Scholar] [CrossRef] [PubMed]
- Brudno, J.N.; Kochenderfer, J.N. Toxicities of Chimeric Antigen Receptor T Cells: Recognition and Management. Blood 2016, 127, 3321–3330. [Google Scholar] [CrossRef] [PubMed]
- Grupp, S.A.; Kalos, M.; Barrett, D.; Aplenc, R.; Porter, D.L.; Rheingold, S.R.; Teachey, D.T.; Chew, A.; Hauck, B.; Wright, J.F.; et al. Chimeric Antigen Receptor-Modified T Cells for Acute Lymphoid Leukemia. N. Engl. J. Med. 2013, 368, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Hay, K.A.; Hanafi, L.-A.; Li, D.; Gust, J.; Liles, W.C.; Wurfel, M.M.; López, J.A.; Chen, J.; Chung, D.; Harju-Baker, S.; et al. Kinetics and Biomarkers of Severe Cytokine Release Syndrome after CD19 Chimeric Antigen Receptor-Modified T-Cell Therapy. Blood 2017, 130, 2295–2306. [Google Scholar] [CrossRef]
- Lee, D.W.; Gardner, R.; Porter, D.L.; Louis, C.U.; Ahmed, N.; Jensen, M.; Grupp, S.A.; Mackall, C.L. Current Concepts in the Diagnosis and Management of Cytokine Release Syndrome. Blood 2014, 124, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Teachey, D.T.; Lacey, S.F.; Shaw, P.A.; Melenhorst, J.J.; Maude, S.L.; Frey, N.; Pequignot, E.; Gonzalez, V.E.; Chen, F.; Finklestein, J.; et al. Identification of Predictive Biomarkers for Cytokine Release Syndrome after Chimeric Antigen Receptor T-Cell Therapy for Acute Lymphoblastic Leukemia. Cancer Discov. 2016, 6, 664–679. [Google Scholar] [CrossRef]
- Karschnia, P.; Jordan, J.T.; Forst, D.A.; Arrillaga-Romany, I.C.; Batchelor, T.T.; Baehring, J.M.; Clement, N.F.; Gonzalez Castro, L.N.; Herlopian, A.; Maus, M.V.; et al. Clinical Presentation, Management, and Biomarkers of Neurotoxicity after Adoptive Immunotherapy with CAR T Cells. Blood 2019, 133, 2212–2221. [Google Scholar] [CrossRef]
- Frey, N.V.; Shaw, P.A.; Hexner, E.O.; Pequignot, E.; Gill, S.; Luger, S.M.; Mangan, J.K.; Loren, A.W.; Perl, A.E.; Maude, S.L.; et al. Optimizing Chimeric Antigen Receptor T-Cell Therapy for Adults With Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2020, 38, 415–422. [Google Scholar] [CrossRef] [PubMed]
- & Hu, S. Overview of Immunosuppressive Therapy in Solid Organ Transplantation. Mayo Clin. Proc. 2019, 94, 1975–1986. [Google Scholar]
- Kruetzmann, S.; Rosado, M.M.; Weber, H.; Germing, U.; Tournilhac, O.; Peter, H.-H.; Berner, R.; Peters, A.; Boehm, T.; Plebani, A.; et al. Human Immunoglobulin M Memory B Cells Controlling Streptococcus Pneumoniae Infections Are Generated in the Spleen. J. Exp. Med. 2003, 197, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Gupta S & Patel Approach to Immunodeficiency Diseases. Mayo Clin. Proc. 2020, 95, 544–550.
- Author Index. Vox Sang. 2011, 101, 135–142. [CrossRef]
- Panitsas, F.P.; Theodoropoulou, M.; Kouraklis, A.; Karakantza, M.; Theodorou, G.L.; Zoumbos, N.C.; Maniatis, A.; Mouzaki, A. Adult Chronic Idiopathic Thrombocytopenic Purpura (ITP) Is the Manifestation of a Type-1 Polarized Immune Response. Blood 2004, 103, 2645–2647. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Bohlke, K.; Lyman, G.H.; Carson, K.R.; Crawford, J.; Cross, S.J.; Goldberg, J.M.; Khatcheressian, J.L.; Leighl, N.B.; Perkins, C.L.; et al. Recommendations for the Use of WBC Growth Factors: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2015, 33, 3199–3212. [Google Scholar] [CrossRef] [PubMed]
- Turtle, C.J.; Hanafi, L.-A.; Berger, C.; Gooley, T.A.; Cherian, S.; Hudecek, M.; Sommermeyer, D.; Melville, K.; Pender, B.; Budiarto, T.M.; et al. CD19 CAR-T Cells of Defined CD4+:CD8+ Composition in Adult B Cell ALL Patients. J. Clin. Invest. 2016, 126, 2123–2138. [Google Scholar] [CrossRef] [PubMed]
- Penack, O.; Holler, E.; van den Brink, M.R.M. Graft-versus-Host Disease: Regulation by Microbe-Associated Molecules and Innate Immune Receptors. Blood 2010, 115, 1865–1872. [Google Scholar] [CrossRef]
- Malard, F.; Mohty, M. Updates in Chronic Graft-versus-Host Disease Management. Am. J. Hematol. 2023, 98, 1637–1644. [Google Scholar] [CrossRef]
- Dhir, S.; Slatter, M.; Skinner, R. Recent Advances in the Management of Graft-versus- Host Disease. Arch. Dis. Child. 2014, 99, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Tu, S.; Zhong, D.; Xie, W.; Huang, W.; Jiang, Y.; Li, Y. Role of Toll-Like Receptor Signaling in the Pathogenesis of Graft-versus-Host Diseases. Int. J. Mol. Sci. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Porter, D.L.; Hwang, W.-T.; Frey, N.V.; Lacey, S.F.; Shaw, P.A.; Loren, A.W.; Bagg, A.; Marcucci, K.T.; Shen, A.; Gonzalez, V.; et al. Chimeric Antigen Receptor T Cells Persist and Induce Sustained Remissions in Relapsed Refractory Chronic Lymphocytic Leukemia. Sci. Transl. Med. 2015, 7, 303ra139. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med. 2019, 380, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Munshi, N.C.; Anderson, L.D., Jr.; Shah, N.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N Engl J Med. 2021, 384, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Riviere, I. Clinical manufacturing of CAR T cells: foundation of a promising therapy. Mol Ther Oncolytics. 2016, 3, 16015. [Google Scholar] [CrossRef]
- June, C.H.; O’Connor, R.S.; Kawalekar, O.U.; et al. CAR T cell immunotherapy for human cancer. Science. 2018, 359, 1361–1365. [Google Scholar] [CrossRef]
- Maecker, H.T.; McCoy, J.P.; Nussenblatt, R. Standardizing immunophenotyping for the Human Immunology Project. Nat Rev Immunol. 2012, 12, 191–200. [Google Scholar] [CrossRef]
Figure 1.
Generations of CAR-T cells.
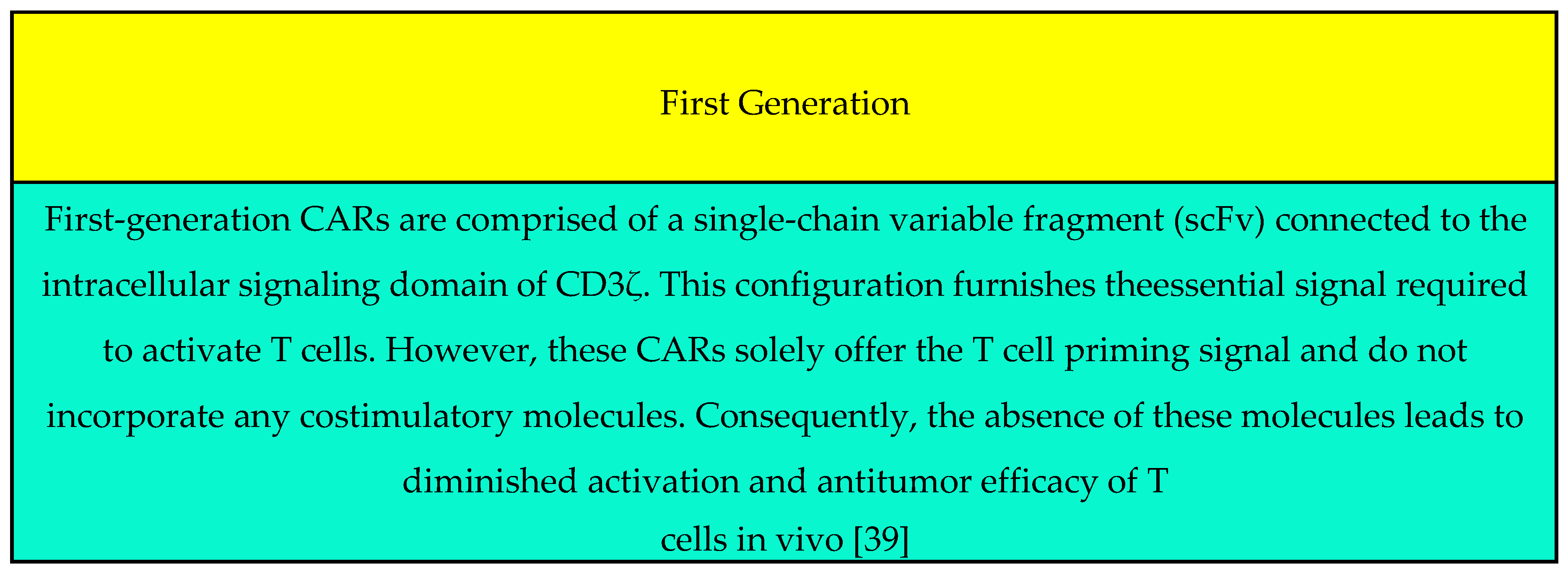
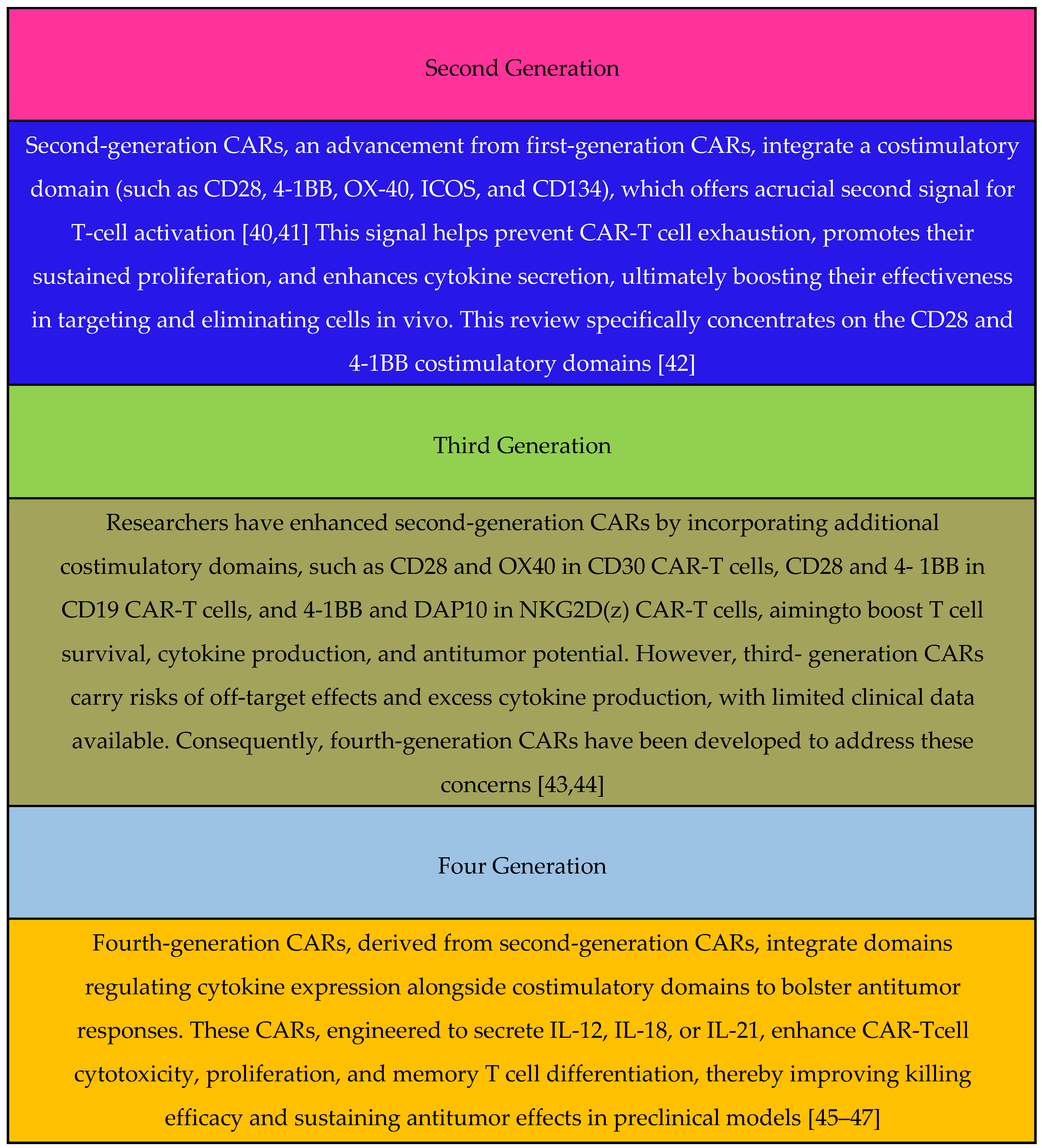
Table 1.
CAR-T cells products that have received FDA approval for treating R/R B cell malignancies.
| Brand names | Company | Targets | References |
| Tisagenlecleucel (Kymriah) | Novartis | CD19 and B cell maturation antigen (BCMA) |
[2] |
| Axicabtagene ciloleucel (Yescarta) | Gilead | CD19 and B cell maturation antigen (BCMA) |
[4,5,6] |
| Brexucabtagene autoleucel (Tecartus) | Gilead | CD19 and B cell maturation antigen (BCMA) |
[7,8] |
| Lisocabtagene maraleucel | Bristol Myers Squibb | CD19 and B cell maturation antigen (BCMA) |
[9,10,11] |
| Idecabtagene vicleucel | Bristol Myers Squibb and Bluebird Bio |
CD19 and B cell maturation antigen (BCMA) |
[1,12,13,14] |
| Ciltacabtagene autoleucel (Carvykti) | Legend and Janssen | CD19 and B cell maturation antigen (BCMA) |
[15,16] |
Table 2.
Preparation process of CAR-T cell products.
|
Steps |
Process |
Reference |
|---|---|---|
| T Cell Collection | T cells are harvested from either the peripheral blood of patients or healthy donors. These T cells are isolated and prepared for their transformation. | [1,31] |
| Genetic Engineering |
CAR construction comprises of: Extracellular domain (scFv) that recognizes specific tumor surface antigens. Transmembrane Domain: Anchors the CAR in the cell membrane. Intracellular Signaling Domain: Transmits activation signals upon antigen recognition. |
[32,33] |
| Antigen Independence: | (i) CAR-T cells recognize tumor antigens independently of Major Histocompatibility Complex (MHC) presentation. | [34] |
|
Generation: (It can be found in Figure 1) |
(ii) First-Generation CAR: Limited proliferative capacity due to lack of costimulatory signals. Second-Generation CAR: Enhanced proliferation and cytokine release. Third-Generation CAR: Combines distinct costimulatory molecules. |
[35,36] |
| “In vitro” Expansion | Cell Culturing: Modified T cells undergo extensive expansion in vitro. | [37] |
| Lymphodepletion |
Preparation: Patients receive lymphodepleting chemotherapy. Infusion: Genetically engineered CAR-T cells are re- infused into the patient. |
[1,38] |
| Target Recognition and Proliferation |
Deployment: CAR-T cells circulate in the patient’s bloodstream. Target Lock-On: CARs recognize specific antigens (often Tumor- Associated Antigens (TAAs). 1. Rapid Proliferation: Activated CAR-T cells multiply, mounting an anti-tumor assault. |
[4] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



