
Submitted:
05 June 2024
Posted:
06 June 2024
You are already at the latest version
Abstract
Background: Pediatric forearm fractures represent a substantial proportion of childhood injuries, requiring effective and minimally invasive treatments. Our study investigated the mid-term outcomes of biodegradable poly-L-lactide-co-glycolide (PLGA) intramedullary implants in managing diaphyseal forearm fractures in children. Methods: A follow-up cohort study was conducted with 38 patients treated with PLGA implants. Control examinations were performed one year post-operation, assessing bone healing through radiographic evaluations and functional outcomes using injured and uninjured limb range of motion (ROM) comparisons. Scarring was evaluated employing the Vancouver Scar Scale (VSS), and satisfaction via a questionnaire. Results: Children were predominantly female (76.4%), with a mean age of 9.71 (SD: 2.69) years. Effective fracture stabilization and bone healing were found in all patients, with a minor reduction (mean difference of -1.5°, p = 0.282) in elbow flexion on the operated side (139.3°) compared to the intact (140.8°). Elbow extension presented negligible average changes (0.2°, p= 0.098). Forearm movements were slightly reduced on the operated side (mean pronation: 80.8° vs. 83.7°, p= 0.166; average supination: 83.5° vs. 85.7°, p= 0.141). Wrist palmar flexion and dorsiflexion showed no significant differences. VSS ratings indicated minimal scarring (mean guardian and doctor scores were 1.13 and 0.55, respectively, p= 0.020), and all patients reported satisfaction with the treatment outcomes. Conclusion: Biodegradable implants are effective for pediatric forearm fractures, providing stable bone healing while preserving functional ROM with minimal scarring and high patient satisfaction. PLGA proved to be a viable alternative to traditional metal implants, eliminating secondary removal surgeries.
Keywords:
pediatric
; diaphyseal
; forearm
; fracture
; biodegradable
; implants
; intramedullary
; poly-L-lactide-co-glycolide
; PLGA
; follow-up
1. Introduction
Among pediatric skeletal injuries, forearm fractures represent a prevalent and clinically significant challenge, accounting for approximately 17.8% of all childhood fractures in the United States, out of an annual incidence rate of 9.47 per 1000 children [1]. The later this damage is adequately addressed, the resultant loss of forearm motion and subsequent functional and social limitations in performing the activities of daily living, along with the psychological and esthetic impact will be more severe [2]. Anatomy of the pediatric forearm provides essential guidance for fracture management. Relatively, the ulna is straight and static, while the radius is curved and rotates over the ulna during pronation and supination [3]. These bones are connected by the interosseous membrane in the middle, and at the joints—both at the wrist and elbow through the proximal and distal radioulnar joints. Each bone has a proximal and distal physis, with the distal physis contributing significantly to longitudinal growth, accounting for 75% in the radius and 81% in the ulna [4]. Growth polarization correlates with observations that fractures nearer to the distal ends have a higher remodeling potential than those closer to the elbow.
Location and nature of the fracture change with age; complete, displaced fractures are more common in adolescence, while younger children more frequently experience plastic deformation or greenstick fractures [5]. Bilateral forearm fractures often result from indirect trauma, most commonly from falling onto an outstretched hand (FOOSH) [2]. During a fall, a child typically extends the arm to protect against the impact, stiffening the wrist, which leads to fracture due to the axial load, that can injure the hand, wrist, forearm, elbow, and shoulder.
Deformities of the limb can indicate a FOOSH injury, but the diagnosis is primarily confirmed through anterioposterior (AP) and lateral orthogonal forearm radiographs, occasionally supplemented by CT or MR scans [6]. Alternatively, a recent trial found the cost-effective, rapid, and radiation-free ultrasound as a viable diagnostic option [7]. Distal pulses and capillary refill must be assessed too. Direct impacts can also cause isolated ulnar mid-shaft fractures (“nightstick fractures”) or less commonly of the radius. Abuse should be considered in children younger than three years old [8].
Classification of pediatric diaphyseal fractures can be done using the internationally employed “AO Pediatric Comprehensive Classification of Long-Bone Fractures” (PCCF), which provides detailed guidelines for categorizing fractures based on the location and morphology of the break and covering different segments and subsegments of long bones [9]. Fracture location is designated by numbers: the forearm bones are labeled with ‘2’, the proximal segment with ‘1’, the diaphyseal with ‘2’, and the distal with ‘3’. The letters ‘r’ and ‘u’ denote the radius and ulna, respectively. The specific subsegment of the bone (epiphysis, metaphysis, diaphysis) is indicated by “E”, “M”, and “D”. The second part of the code describes fracture morphology, including patterns specific to children. Severity is classified into two levels: simple (.1) and comminuted (broken into multiple fragments) (.2). Displacement is indicated by Roman numerals aiding in a clear and concise description of fractures. In case the fracture involves the growth plate, the Salter and Harris classification is utilized [10].
Conservative therapy, which primarily involves immobilization with a cast, is a widely accepted and effective treatment for pediatric forearm fractures, especially when displacement is minimal [8]. Typically, conservative treatment includes closed reduction followed by casting to restore alignment and immobilize the fracture. Casting type and duration depend on the characteristics of the fracture and the age of the child; for example, children under ten with angulations less than ten degrees often achieve complete remodeling and good function with casting alone. Intact periosteum in many of these fractures enhances stability and facilitates natural splinting, making conservative treatment particularly effective. For greenstick fractures, this is especially true, where the bone bends and cracks without breaking completely [11]. Younger children benefit significantly from this method due to the higher remodeling potential of their bones, allowing for healing with minimal intervention and good functional outcomes. However, careful monitoring is essential to prevent complications such as repeated displacement, inadequate healing, or joint stiffness, with follow-up X-rays ensuring proper alignment. Despite these challenges, conservative therapy remains a cornerstone of pediatric fracture management, offering a less invasive option with excellent outcomes in many cases.
Operative therapy serves as a critical intervention for pediatric forearm fractures that are unstable, significantly displaced, involving both the radius and ulna, or unresponsive to conservative treatment [12]. Warranting proper alignment and stability is essential for optimal healing and function preventing long-term complications.
Elastic Stable Intramedullary Nailing (ESIN) is a widely employed minimally invasive procedure for pediatric forearm fractures, which involves inserting flexible, strong metal rods into the medullary cavity of the bone, providing internal stabilization [13]. Habitually, the nails are left in place for 6-12 months before removal. Casting is often used postoperatively for 3-4 weeks to ensure stability, with the elbow at 90 degrees and the forearm in neutral rotation. Advantages of ESIN include small incisions, reduced postoperative pain, and fast recovery times while allowing early mobilization beneficial for maintaining muscle strength and joint function compared to metal plating [12]. Due to the drawbacks of metal implants, new resorbable intramedullary implants have been developed for the surgical treatment of pediatric forearm diaphyseal fractures, composed of biodegradable materials such as poly-L-lactide-co-glycolide (PLGA), offering temporary support during the healing process while gradually dissolving within the body, eliminating the need for a secondary procedure to remove the hardware [14].
For more complex fractures, plate and screw fixation is often employed, applying a metal plate secured with screws to ensure precise alignment of the fracture. Plate and screw fixation proves particularly effective for fractures near joints or those that are comminuted, providing robust stability and promoting proper healing. Plates are habitually left in place for at least six months, and removal is considered if they cause discomfort or impede function. Postoperative immobilization usually involves casting or splinting for 4-6 weeks.
External fixation (fixateur externe) is another valuable option involving the stabilization of the bones from outside the body using a frame attached with pins or wires, allowing for adjustment, and is particularly useful in managing complex fractures with extensive soft tissue injuries [15]. Typically, the fixator remains in place for 6-8 weeks, followed by a transition to a cast or splint for an additional 4-6 weeks, depending on the healing progress of the fracture. Hybrid fixation combines different methods to achieve optimal results [16]. Surgical intervention carries inherent risks, such as infection or hardware-related irritation, but the benefits often outweigh these concerns in appropriately selected cases. Ensuring accurate bone healing, restoring full function, and preventing long-term sequelae such as deformity or chronic pain remains the primary objective of operative therapy.
Despite the apparent advantages of resorbable implants research on their use in pediatric populations has been limited. Only one study has investigated the outcomes of intramedullary PLGA implants for pediatric diaphyseal forearm fractures, with follow-ups at two [17] and four [18] years post-surgery. Another trial focused on distal fracture management [19]. Therefore, our study aims to assess the mid-term functional and cosmetic results of bioabsorbable intramedullary implants in treating this common condition, providing a deeper understanding of their capabilities in pediatric diaphyseal forearm fractures.
2. Materials and Methods
2.1. Study Design and Patient Selection
A single-center, single-arm, descriptive cohort follow-up study was conducted at the Pediatric Surgical Division of the University of Pécs in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [20]. Data were retrospectively collected from our hospital’s recordings of pediatric patients who underwent surgery for diaphyseal forearm fractures using PLGA intramedullary implants between May 2021 and March 2023. Then, they were prospectively recalled to evaluate their functional, esthetic, and psychological recovery one year post-surgery.
A total of 38 pediatric patients met the inclusion criteria, which were: (1) pediatric patients under the age of 18 years at the time of follow-up with (2) forearm fractures treated with absorbable intramedullary PLGA implants and (3) had at least one year of postoperative recovery. Eight patients were excluded due to loss of follow-up attributable to (1) missing contact information (2) not appearing on control examination (3) or because of bilateral fractures.
2.2. Intervention
PLGA implants (Activa IM-Nail™, Bioretec Ltd., Tampere, Finland) function by maintaining their mechanical strength throughout the critical period of bone healing (Figure 1).
These polymers degrade through hydrolysis, breaking down into lactic acid and glycolic acid monomers. Subsequently, the monomers are metabolized via the citric acid cycle, producing water and carbon dioxide as end products. This process lowers the local pH, creating an acidic environment around the implant which facilitates its gradual resorption. Complete degradation of PLGA typically occurs within 9-12 months, making it a reliable material for temporary internal fixation in pediatric patients. Additionally, the implants feature a tricalcium phosphate (β-TCP) marker for precise fluoroscopic placement (Figure 1/C-F).
2.3. Surgical Protocol
PLGA implants are particularly advantageous for fractures of the radius, ulna, or both, provided proper immobilization is ensured. However, they are not suitable for oblique spiral, comminuted, or epiphyseal fractures, and are contraindicated in the presence of local infection or poor patient compliance.
Several key steps are involved in the surgical procedure for inserting PLGA implants in a minimally invasive manner. After cleaning and disinfecting the operative area and administering general anesthesia, the patient was positioned supine with the affected arm placed on a radiolucent table. Additional management, such as analgesia with 0.1–0.2 mg/kg nalbuphine injections (Nubain, ALTAMEDICS GmbH, Cologne, Germany), and sedation with midazolam (Dormicum, Egis Gyógyszergyár Zrt, Budapest, Hungary) were administered perioperatively based on clinical indications and parental consent. Small incisions were made dorsally on the distal radius and laterally on the proximal ulna. Entry points into the cortical bone had been created using an awl or drill. For the radius, an entry hole was made by positioning the drill perpendicular to the cortex and gradually angling it to form the smallest possible angle with the diaphyseal axis. Then, the medullary canal was reamed with a dilator that matched the implant size - and this process was repeated for the ulna.
Once the canals were prepared, the PLGA implants were introduced using an inserter, guaranteeing no rotational movements to prevent misalignment. Implant diameter choice is critical and should match the smallest diameter of the medullary canal, with available options being 2.7, and 3.2 mm in diameter, and lengths of 200, 300, and 400 mm. Fluoroscopy was used to verify implant positions, with the β-TCP tips aiding in visualization. Protruding ends of the implants were trimmed and smoothed to avoid soft tissue irritation, and the incisions were closed with absorbable sutures. Postoperative care includes immobilizing the limb in a cast above the elbow at a 90-degree angle for 4-6 weeks, with sports and strenuous activities avoided for 2-6 months.
2.5. Evaluated Metrics
Endpoints included patient demographics (such as age, sex, dominant hand) and fracture characteristics (time of injury, and affected side and bone), collected in Microsoft Excel 2021 (Microsoft Corporation, Redmond, WA, USA). Primary outcomes included the joint function evaluation via their range of motion (ROM) using a goniometer. ROM was calculated by adding the absolute values of opposing motions. Measurements from the operated extremity were compared to those of the unharmed limb to determine any discrepancies in ROM for the following movements:
- Elbow Flexion and Extension: normal range is -10 to 150 degrees (°). Patients were instructed to fully extend and flex their elbows while standing with arms at their sides.
- Forearm Pronation and Supination: standard interval is 80 to 90° in both directions from the neutral position. Children held a pen in a fist with elbows at 90°, rotating their forearms to achieve maximum pronation and supination.
- Wrist Palmar Flexion and Dorsiflexion: typical ROM is 80° dorsiflexion and 70° palmar flexion. Patients placed their forearms on a horizontal surface, moving their wrists to the maximum palmar and dorsiflexion positions.
Surgical scars were evaluated using the Vancouver Scar Scale (VSS) [21], assessing the composite score of four criteria:
- Pigmentation: scored from 0 (normal) to 2 (severe hyperpigmentation).
- Vascularity: counted from 0 (normal) to 3 (severe vascularity).
- Pliability: graded from 0 (normal) to 5 (severe contracture).
- Height: recorded from 0 (flat) to 3 (more than 5 mm).
Satisfaction was assessed through a questionnaire asking if the patient or their guardian would choose the same surgical method again under similar circumstances. This survey aimed to capture subjective satisfaction with the functional and aesthetic outcomes of the surgery.
2.6. Data Analysis and Visualization
Descriptive statistics were calculated until two decimals for all continuous outcomes utilizing means, standard deviations (SD), medians, interquartile ranges (IQR), 25th percentiles (IQR25), 75th percentiles (IQR75), counts, and ranges, while discrete endpoints were analyzed via count and percentage distributions. This study employed Python 3.12.3 (Python Software Foundation, Wilmington, DE, USA) for data visualization and statistical analysis, a versatile and open-source language, that facilitated data handling and testing operating several specialized libraries. Statistical analysis was conducted using scipy and numpy libraries. Shapiro-Wilk test was utilized to determine normality, suitable for smaller sample sizes. Two-sample t-tests were used to compare means from two independent groups when both samples were normally distributed, while non-parametric Mann-Whitney U tests differentiated not normally distributed samples. Additionally, a Chi-square (χ²) test determined the association between categorical variables. Differences were deemed significant p ≤ 0.05. Matplotlib was utilized for fundamental plot creation and customization while seaborn provided advanced plotting functions and aesthetic enhancements.
3. Results
This study included 38 pediatric patients with diaphyseal forearm fractures treated using PLGA implants. Patients age ranged from 5 to 15 years, with a mean age of 9.71 (SD = 2.69) years. Regarding sex distribution, the majority of the patients (76.32% of all cases) were female, and the affected side was more often the right forearm (55.26%, n = 21) (Table 1). Dominant hand analysis revealed that 85.71% (n = 18) of the patients were right-handed, moreover, the non-dominant hand was involved in slightly more (52.12%, n = 12) injuries, which was not statistically significant (p = 0.513). In terms of fracture type, most of the fractures involved both the radius and ulna (84.21%, n = 32), with only five children (13.16%) having fractures of the radius alone and one patient (2.63%) having a fracture of the ulna alone. Restricted elbow flexion (< 137°) was linked significantly (p = 0.017) with radius-only fractures (80% of patients had limited mobility), while wide ROM (≥ 137°) was marginally associated (p = 0.052) with fractures of both bones (64.52% of children had high mobility).
Functional outcomes were assessed via ROM for various movements of the forearm, including the elbow and wrist performance as well, and are summarized in Table 2 and visualized in Figure 2.
For elbow flexion, the mean maximum angle for the operated side (Figure 3/D) was 139.3° (SD = 6.2) compared to 140.8° (SD = 6.2) on the intact side (Figure 3/B). The minor reduction of -1.45° on the operated side suggests effective restoration of function by the PLGA implants, despite a statistically significant difference (p = 0.282). Elbow extension showed mean ROM values of -1.1° (SD = 2.9) for the PLGA-treated (Figure 3/C) and -1.3° (SD = 2.9) for the intact side (Figure 3/A), with a negligible mean difference of 0.05° (p = 0.098), indicating that the surgical intervention had no significant impact on extension capability.
Forearm pronation (Figure 4/A) exhibited a mean ROM of 80.8° (SD = 6.6) on the operated side and 82.4° (SD = 6.6) on the intact side. The slight reduction of -1.61° in pronation on the operated side (p = 0.166), suggests a clinically minimal impact on rotational movement. Supination of the forearm (Figure 4/B) demonstrated a mean ROM loss of 0.24° (p = 0.141) for the operated side, representing no significant difference and thus supporting the efficacy of the PLGA implants in maintaining rotational movement.
Wrist dorsiflexion showed a mean difference of -0.34° (p = 0.070) between the operated (Figure 4/F) and intact sides (Figure 4/C), representing no significant impact on wrist extension and underscoring the implant’s capacity to maintain wrist flexibility. Palmar flexion measurements indicated a mean difference of -0.89° (p = 0.563) between the operated (Figure 4/E) and intact (Figure 4/D) sides, showing no statistically significant variation and highlighting the implant’s ability to preserve a wide range of wrist movements.
For the total scores, guardians rated the forearm scars with a mean score of 1.13 (SD = 1.14), while medical professionals provided a significantly (p = 0.020) lower mean VSS score of 0.55 (SD = 0.80) (Figure 5/C-D). Patient satisfaction was universally high, with all 38 patients reported as satisfied with the treatment outcomes. Comparisons are presented in brief in Table 3.
4. Discussion
Restoring function while ensuring proper bone healing is the primary objective of pediatric fracture management [8]. Our results indicate that PLGA intramedullary implants are effective in achieving this balance. PLGA is a biodegradable polymer that has garnered attention for its biocompatibility, controlled degradation properties, and minimal toxicity. Due to these characteristics, it is also one of the most promising drug delivery systems in nanoparticle formulation [22]. It is possible to add further active ingredients (such as IGF1) into the implant with timed-release properties, for osteostimulation or to prevent infections [23]. In pediatric traumatology, its features are particularly advantageous, as the implants gradually degrade, eliminating the need for a second surgery to remove hardware [14]. Fewer interventions reduce the overall healthcare burden and mitigate the psychological impact of additional surgical interventions on young patients and their families. Eliminating a second surgical procedure also translates into fewer anesthesia-related risks and a reduced likelihood of postoperative complications, such as bleeding, infections, or scar tissue formation, which are particularly pertinent in pediatric populations [24]. Furthermore, the shorter hospital stays and reduced need for follow-up visits significantly decrease the disruption to a child’s education and social life, which are vital for their overall development. Despite PLGA materials being generally well-tolerated, the potential for allergic reactions or adverse responses in certain patients should be investigated. Additionally, PLGA implants are nearly invisible on X-ray imaging, while they are compatible with MRI. To decrease the cost of control examinations and better compliance, β-TCP bits were incorporated into the tips of the implants, which show up as hyper-opacities on X-ray.
Expanding on our previous investigations [25,26], the current cohort included 38, predominantly female (76.32%) pediatric patients, generally with both of their diaphysis (84.21%) fractured on a single forearm with a mean age of 9.71. A novel observation was that originally, slightly limited elbow flexion (< 137°) correlated significantly (p = 0.017) with radius-only fractures (80% of patients had restricted mobility), while a broad original ROM (≥ 137°) was marginally associated (p = 0.052) with fractures of both diaphyseal bones (64.52% of children had high mobility) - which might also reveal to be significant within a larger analyzed population.
A minor reduction in mean elbow (absolute flexion difference: -1.45°, p = 0.282; extension: 0.05°, p = 0.098) forearm (pronation: -1.61°, p = 0.166; supination: 0.24°, p = 0.141) and wrist (palmar flexion: -0.89°, p = 0.563; dorsiflexion: -1.55°, p = 0.070) mobility highlights the precision of these implants in preserving near-normal ROM. A randomized controlled trial (RCT) found similar patterns regarding preserved ROM using PLGA. Moreover, they showed that the currently gold standard ESIN utilization slightly reduced forearm rotational ROM on the injured side, and increased postoperative pain compared to PLGA [17]. These findings are significant given the crucial role of elbow and forearm movements in daily activities and play, which are essential for children’s development and quality of life. Consistent functional outcomes across ages, genders, and different fracture types underscore the versatility and reliability of PLGA implants. Another study found that they were also applicable in osteochondral fractures of the lateral condyle of the femur, patella, and radial head [27]. Therefore, the observed uniformity suggests that surgeons can confidently employ these implants across a wide range of fractures, ensuring optimal outcomes irrespective of specific characteristics. This adaptability could be further enhanced by individualizing management to patient needs, considering factors such as the dominant hand and specific activity requirements. Advances in 3D printing and bioengineering could enable the creation of such patient-specific PLGA implants. Tailoring the size and shape of the implants to fit the unique anatomical and physiological needs of each child may further enhance the effectiveness and comfort of the treatment.
Our results also indicate a generally positive outcome for pediatric forearm fractures treated with PLGA implants, with high satisfaction rates and minor VSS scores, suggesting minimal scarring as assessed by both guardians and doctors. Although both groups gave low total VSS scores, it must be underscored, that guardians rated the scars 104.76% worse than healthcare professionals, which correlates with recent observations [28]. Educating patients and their families about the benefits and care associated with PLGA implants can enhance compliance and satisfaction. Clear communication regarding the implant’s degradation process and expected recovery timeline is essential for setting realistic expectations.
Traditional methods of managing pediatric forearm fractures often involve metallic implants, which, while effective, necessitate removal surgeries and pose risks of long-term complications such as hardware irritation or migration [14]. A rigid, non-degradable material may increase postoperative pain and distress, which can lead to a less comfortable recovery period for pediatric patients. Corrosion or mechanical wear can exacerbate cellular toxicity and tissue reactions [29]. Chronic inflammation due to metal debris may also play a role in carcinogenesis [30]. Using PLGA implants circumvents these issues, offering a more patient-friendly approach with fewer long-term risks. Given that PLGA degrades over time, it might also affect the growth plate less. A disadvantage of the degradation process is that it is theorized to lead to intermediary byproducts, which are acidic in nature and halt osteoblast activity thereby hindering recanalization. This has been studied in maxillo-facial surgeries and pediatric pelvic osteotomies with over 90% bone recanalization within two years and another study regarding the bone regrowth of the implant canal is underway by Hermann et al. [31,32]. On the other hand, one of its byproducts, lactate, has a crucial part in biochemical pathways and could exert therapeutic effects such as angiogenesis [33]. Another important consideration is the environmental impact of materials. Metal implants contribute to medical waste and require energy-intensive production processes [34]. In contrast, PLGA implants degrade naturally within the body, reducing the ecological footprint of surgical interventions, and aligning with the broader global efforts toward sustainability in healthcare practices.
Future perspectives and limitations of this research must also be discussed. Expanding the study to include larger and more diverse populations whose data was collected prospectively will provide more comprehensive insights into the generalizability of these findings and reduce possible bias. While the current study corroborates the efficacy of PLGA implants in maintaining functional outcomes, future research should explore the long-term effects of these implants on bone health and growth. Given the dynamic nature of pediatric bone development, it is essential to monitor how the gradual degradation of PLGA implants influences bone remodeling over more extended periods. Longitudinal studies tracking patients into adolescence and adulthood would provide valuable insights into any delayed effects and further solidify the implants’ safety profile. Additionally, investigating the economic impact of PLGA implants, including cost-effectiveness analyses directly compared to traditional methods, could further substantiate their adoption in clinical practice. Potential research could explore their usefulness in other pediatric orthopedic conditions, such as fractures of the femur, tibia, or even more complex multi-fragmentary fractures. Expanding the use of PLGA implants could standardize treatment protocols and streamline surgical training for pediatric surgeons. Lastly, the scar scales and questionnaires are subjective measurements, which could be further objectivized by specialized instruments, such as Laser Doppler Imaging (LDI) for quantifying scar blood flow, Cutometers for measuring elasticity, or ColorMeters for calculating the melanin index [35]. Using advanced imaging techniques, for example, MRI would also reveal implant resorption rates [18].
Management of pediatric forearm fractures using PLGA intramedullary implants has demonstrated promising outcomes, reflecting advancements in biomaterial technology and surgical techniques. Our study presents compelling evidence supporting the capabilities of PLGA implants in maintaining functional ROM while minimizing complications, thereby enhancing the overall recovery experience for young patients.
5. Conclusions
Our study demonstrates that PLGA intramedullary implants effectively restore function and ensure proper bone healing in pediatric diaphyseal forearm fractures. Children showed only a minor reduction in mobility, indicating the precision of these implants in preserving a near-normal range of motion. Consistent functional outcomes across different ages, genders, and fracture types highlight the versatility of PLGA implants. They offer a patient-friendly alternative to traditional metallic implants, which often require removal surgeries and pose long-term risks such as hardware irritation or migration. The biodegradable nature of PLGA eliminates the need for a second surgery, reducing healthcare burdens and psychological impacts on young patients and their families while decreasing anesthesia-related risks and postoperative complications such as bleeding, infections, or scar tissue formation. Additionally, fewer hospital stays and follow-up visits minimize disruptions to a child’s education and social life, crucial for their overall development. While PLGA’s degradation process may introduce some intermediary byproducts, the overall benefits seem to outweigh these concerns.
Future research should focus on the long-term effects of PLGA implants on bone health and growth, expanding to larger, diverse populations to validate findings. Additionally, investigating the economic impact and exploring their application in other pediatric orthopedic conditions could further substantiate PLGA implants’ adoption in clinical practice. Overall, PLGA implants represent a significant advancement in pediatric fracture management, enhancing recovery experiences for young patients.
Author Contributions
Conceptualization, A.L., Á.M.L. and G.J.; methodology, A.K., A.L, G.J. and H.N.; software, A.K., A.L. and H.N.; validation, A.K., A.L., Á.M.L, H.N. and G.J.; formal analysis., A.K., A.L., Á.M.L. and H.N.; investigation, Á.M.L., H.N. and G.J.; resources, G.J.; data curation, A.K., A.L., Á.M.L., and H.N. .; writing—original draft preparation, A.L.; writing—review and editing, A.K., Á.M.L., A.L. G.J., and H.N.; visualization, A.K., A.L. and H.N.; supervision, A.K., A.L. and G.J.; project administration, A.K., A.L., and G.J.; funding acquisition, G.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. All resources were funded by the University of Pécs, Medical School.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Regional Research Ethics Committee, Clinical Complex, University of Pécs [Pécsi Tudományegyetem, Klinikai Komplex, Regionális és Intézményi Kutatás—Etikai Bizottság] on 23 April 2021 (8737-PTE2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the guardians of the patients to publish this paper.
Data Availability Statement
All data is contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Naranje, S.M.; Erali, R.A.; Warner, W.C.J.; Sawyer, J.R.; Kelly, D.M. Epidemiology of Pediatric Fractures Presenting to Emergency Departments in the United States. J. Pediatr. Orthop. 2016, 36, e45. [Google Scholar] [CrossRef] [PubMed]
- Chia, B.; Kozin, S.H.; Herman, M.J.; Safier, S.; Abzug, J.M. Complications of Pediatric Distal Radius and Forearm Fractures. Instr. Course Lect. 2015, 64, 499–507. [Google Scholar] [PubMed]
- Salvi, A.E. Forearm Diaphyseal Fractures: Which Bone to Synthesize First? Orthopedics 2006, 29, 669–671. [Google Scholar] [CrossRef] [PubMed]
- Manson, T.T.; Pfaeffle, H.J.; Herdon, J.H.; Tomaino, M.M.; Fischer, K.J. Forearm Rotation Alters Interosseous Ligament Strain Distribution. J. Hand Surg. 2000, 25, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Widnall, J.; Bruce, C. Paediatric Forearm Fractures. Orthop. Trauma 2018, 32, 372–377. [Google Scholar] [CrossRef]
- Noonan, K.J.; Price, C.T. Forearm and Distal Radius Fractures in Children. J. Am. Acad. Orthop. Surg. 1998, 6, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Epema, A.C.; Spanjer, M.J.B.; Ras, L.; Kelder, J.C.; Sanders, M. Point-of-Care Ultrasound Compared with Conventional Radiographic Evaluation in Children with Suspected Distal Forearm Fractures in the Netherlands: A Diagnostic Accuracy Study. Emerg. Med. J. EMJ 2019, 36, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Caruso, G.; Caldari, E.; Sturla, F.D.; Caldaria, A.; Re, D.L.; Pagetti, P.; Palummieri, F.; Massari, L. Management of Pediatric Forearm Fractures: What Is the Best Therapeutic Choice? A Narrative Review of the Literature. Musculoskelet. Surg. 2021, 105, 225–234. [Google Scholar] [CrossRef] [PubMed]
- The AO Pediatric Comprehensive Classification of Long Bone Fractures (PCCF) | Acta Orthopaedica. Available online: https://actaorthop.org/actao/article/view/9669 (accessed on 31 May 2024).
- Randsborg, P.-H.; Sivertsen, E.A. Distal Radius Fractures in Children: Substantial Difference in Stability between Buckle and Greenstick Fractures. Acta Orthop. 2009, 80, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Atanelov, Z.; Bentley, T.P. Greenstick Fracture. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2024. [Google Scholar]
- Poutoglidou, F. Flexible Intramedullary Nailing in the Treatment of Forearm Fractures in Children and Adolescents, a Systematic Review. J. Orthop. 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.M.; Jones, K.J.; Garner, M.R.; Goebel, J. Eleven Years Experience in the Operative Management of Pediatric Forearm Fractures. J. Pediatr. Orthop. 2010, 30, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Heye, P.; Matissek, C.; Seidl, C.; Varga, M.; Kassai, T.; Jozsa, G.; Krebs, T. Making Hardware Removal Unnecessary by Using Resorbable Implants for Osteosynthesis in Children. Child. Basel Switz. 2022, 9, 471. [Google Scholar] [CrossRef] [PubMed]
- Helber, M.U.; Ulrich, C. External Fixation in Forearm Shaft Fractures. Injury 2000, 31 Suppl 1, 45–47. [Google Scholar] [CrossRef]
- Elhalawany, A.S.; Afifi, A.; Anbar, A.; Galal, S. Hybrid Fixation for Adolescent Both-Bones Diaphyseal Forearm Fractures: Preliminary Results of a Prospective Cohort Study. J. Clin. Orthop. Trauma 2020, 11, S46–S50. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, L.; Perhomaa, M.; Kyrö, A.; Pokka, T.; Serlo, W.; Merikanto, J.; Sinikumpu, J.-J. Intramedullary Nailing of Forearm Shaft Fractures by Biodegradable Compared with Titanium Nails: Results of a Prospective Randomized Trial in Children with at Least Two Years of Follow-Up. Biomaterials 2018, 185, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Perhomaa, M.; Pokka, T.; Korhonen, L.; Kyrö, A.; Niinimäki, J.; Serlo, W.; Sinikumpu, J.-J. Randomized Controlled Trial of the Clinical Recovery and Biodegradation of Polylactide-Co-Glycolide Implants Used in the Intramedullary Nailing of Children’s Forearm Shaft Fractures with at Least Four Years of Follow-Up. J. Clin. Med. 2021, 10, 995. [Google Scholar] [CrossRef] [PubMed]
- Varga, M.; Józsa, G.; Hanna, D.; Tóth, M.; Hajnal, B.; Krupa, Z.; Kassai, T. Bioresorbable Implants vs. Kirschner-Wires in the Treatment of Severely Displaced Distal Paediatric Radius and Forearm Fractures - a Retrospective Multicentre Study. BMC Musculoskelet. Disord. 2022, 23, 362. [Google Scholar] [CrossRef] [PubMed]
- Elm, E. von; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Fearmonti, R.; Bond, J.; Erdmann, D.; Levinson, H. A Review of Scar Scales and Scar Measuring Devices. Eplasty 2010, 10, e43. [Google Scholar] [PubMed]
- Chereddy, K.K.; Payen, V.L.; Préat, V. PLGA: From a Classic Drug Carrier to a Novel Therapeutic Activity Contributor. J. Control. Release Off. J. Control. Release Soc. 2018, 289, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Żywicka, B.; Krucińska, I.; Garcarek, J.; Szymonowicz, M.; Komisarczyk, A.; Rybak, Z. Biological Properties of Low-Toxic PLGA and PLGA/PHB Fibrous Nanocomposite Scaffolds for Osseous Tissue Regeneration. Evaluation of Potential Bioactivity. Mol. J. Synth. Chem. Nat. Prod. Chem. 2017, 22, 1852. [Google Scholar] [CrossRef] [PubMed]
- Paterson, N.; Waterhouse, P. Risk in Pediatric Anesthesia: Risk in Pediatric Anesthesia. Pediatr. Anesth. 2011, 21, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Roeder, C.; Alves, C.; Balslev-Clausen, A.; Canavese, F.; Gercek, E.; Kassai, T.; Klestil, T.; Klingenberg, L.; Lutz, N.; Varga, M.; et al. Pilot Study and Preliminary Results of Biodegradable Intramedullary Nailing of Forearm Fractures in Children. Children 2022, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Józsa, G.; Kassai, T.; Varga, M. Preliminary Experience with Bioabsorbable Intramedullary Nails for Paediatric Forearm Fractures: Results of a Mini-Series. Genij Ortop. 2023, 29, 640–644. [Google Scholar] [CrossRef]
- Nudelman, H.; Lőrincz, A.; Lamberti, A.G.; Varga, M.; Kassai, T.; Józsa, G. Management of Juvenile Osteochondral Fractures Utilising Absorbable PLGA Implants. J. Clin. Med. 2024, 13, 375. [Google Scholar] [CrossRef] [PubMed]
- Válik, A.; Harangozó, K.; Garami, A.; Juhász, Z.; Józsa, G.; Lőrincz, A. Mid-Term Follow-Up Study of Children Undergoing Autologous Skin Transplantation for Burns. Life 2023, 13, 762. [Google Scholar] [CrossRef] [PubMed]
- Navratilova, P.; Emmer, J.; Tomas, T.; Ryba, L.; Burda, J.; Loja, T.; Veverkova, J.; Valkova, L.; Pavkova Goldbergova, M. Plastic Response of Macrophages to Metal Ions and Nanoparticles in Time Mimicking Metal Implant Body Environment. Environ. Sci. Pollut. Res. 2024, 31, 4111–4129. [Google Scholar] [CrossRef]
- Sun, C.W.Y.; Lau, L.C.M.; Cheung, J.P.Y.; Choi, S.-W. Cancer-Causing Effects of Orthopaedic Metal Implants in Total Hip Arthroplasty. Cancers 2024, 16, 1339. [Google Scholar] [CrossRef] [PubMed]
- Hedelin, H.; Larnert, P.; Antonsson, P.; Lagerstrand, K.; Brisby, H.; Hebelka, H.; Laine, T. Stability in Pelvic Triple Osteotomies in Children Using Resorbable PLGA Screws for Fixation. J. Pediatr. Orthop. 2021, 41, e787–e792. [Google Scholar] [CrossRef] [PubMed]
- Landes, C.A.; Ballon, A.; Roth, C. Maxillary and Mandibular Osteosyntheses with PLGA and P(L/DL)LA Implants: A 5-Year Inpatient Biocompatibility and Degradation Experience. Plast. Reconstr. Surg. 2006, 117, 2347–2360. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Fukumura, D.; Jain, R.K. Acidic Extracellular pH Induces Vascular Endothelial Growth Factor (VEGF) in Human Glioblastoma Cells via ERK1/2 MAPK Signaling Pathway: MECHANISM OF LOW pH-INDUCED VEGF*. J. Biol. Chem. 2002, 277, 11368–11374. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Singh, A.; Jackson, M.J.; Coelho, R.T.; Prakash, D.; Charalambous, C.P.; Ahmed, W.; da Silva, L.R.R.; Lawrence, A.A. A Comprehensive Review on Metallic Implant Biomaterials and Their Subtractive Manufacturing. Int. J. Adv. Manuf. Technol. 2022, 120, 1473–1530. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, M.E.H.; Moortgat, P. Objective Assessment Tools: Physical Parameters in Scar Assessment. In Textbook on Scar Management: State of the Art Management and Emerging Technologies; Téot, L., Mustoe, T.A., Middelkoop, E., Gauglitz, G.G., Eds.; Springer: Cham (CH), 2020 ISBN 978-3-030-44765-6.
Figure 1.
An 11-year-old boy fell while playing football and had a deformed left arm. Preoperative anteroposterior (AP) (A) and lateral (B) radiographic views of the forearm exposed subperiosteal fractures of both ulna and radius. X-rays post-surgery (C - AP, D – lateral aspects) show the successful insertion of PLGA implants, confirmed by the radiopaque markers. Six-month control images (E - AP, F -lateral views) revealed completely healed fractures with good axial alignment.
Figure 1.
An 11-year-old boy fell while playing football and had a deformed left arm. Preoperative anteroposterior (AP) (A) and lateral (B) radiographic views of the forearm exposed subperiosteal fractures of both ulna and radius. X-rays post-surgery (C - AP, D – lateral aspects) show the successful insertion of PLGA implants, confirmed by the radiopaque markers. Six-month control images (E - AP, F -lateral views) revealed completely healed fractures with good axial alignment.

Figure 2.
Histograms showing measured ROMs and trendlines predicting expected functionality one year after PLGA treatment of forearm fractures in children.
Figure 2.
Histograms showing measured ROMs and trendlines predicting expected functionality one year after PLGA treatment of forearm fractures in children.
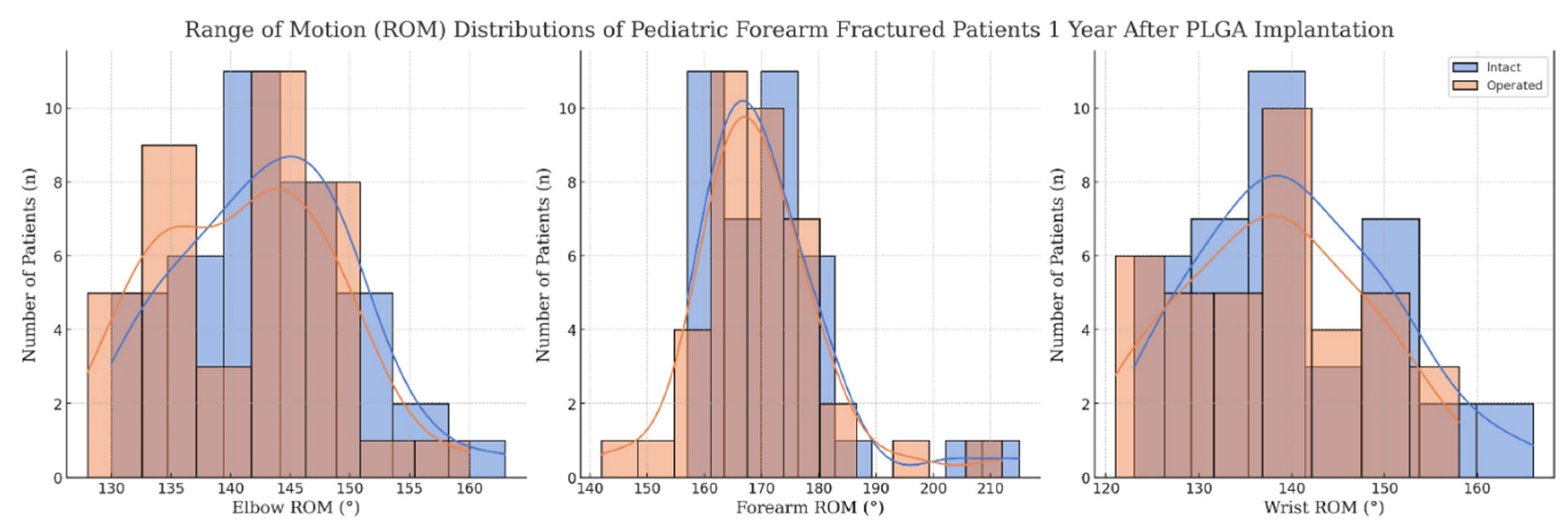
Figure 3.
Photographs showing elbow extension (A) and flexion (B) of the uninjured arm of an 11-year-old boy. One year after surgery, the cubital extension (C) and flexion (D) of the operated arm demonstrate intact functionality.
Figure 3.
Photographs showing elbow extension (A) and flexion (B) of the uninjured arm of an 11-year-old boy. One year after surgery, the cubital extension (C) and flexion (D) of the operated arm demonstrate intact functionality.
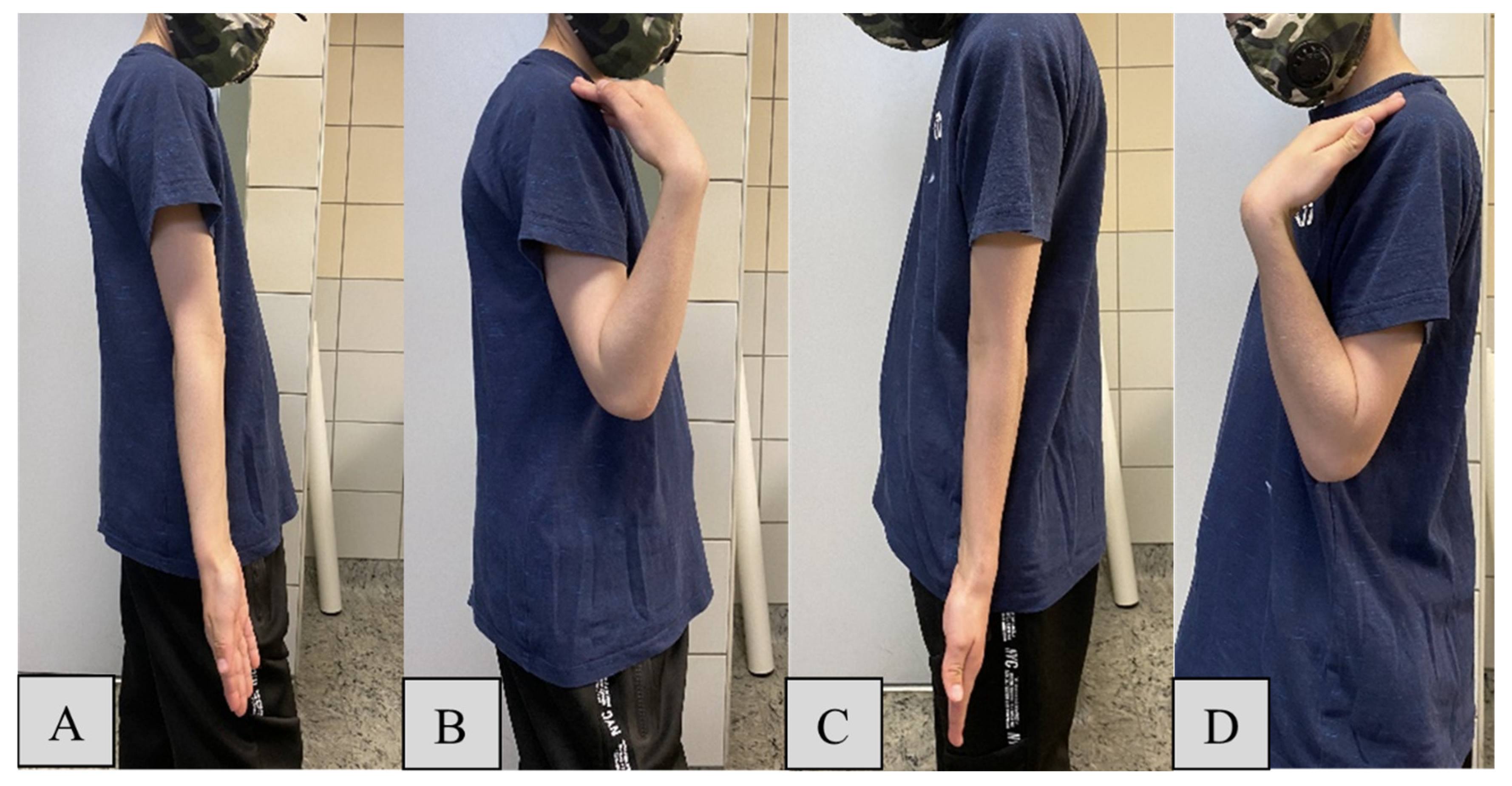
Figure 4.
One year post-PLGA implantation, images showing the pronation (A) and supination (B) of the forearm, while the intact hand holds a red pen and the healed grasps the blue writing implement. Baseline wrist function is demonstrated with the dorsal- (C) and palmar flexion (D) of the uninjured extremity, which can be compared to the ROM of the operated arm (E-F).
Figure 4.
One year post-PLGA implantation, images showing the pronation (A) and supination (B) of the forearm, while the intact hand holds a red pen and the healed grasps the blue writing implement. Baseline wrist function is demonstrated with the dorsal- (C) and palmar flexion (D) of the uninjured extremity, which can be compared to the ROM of the operated arm (E-F).
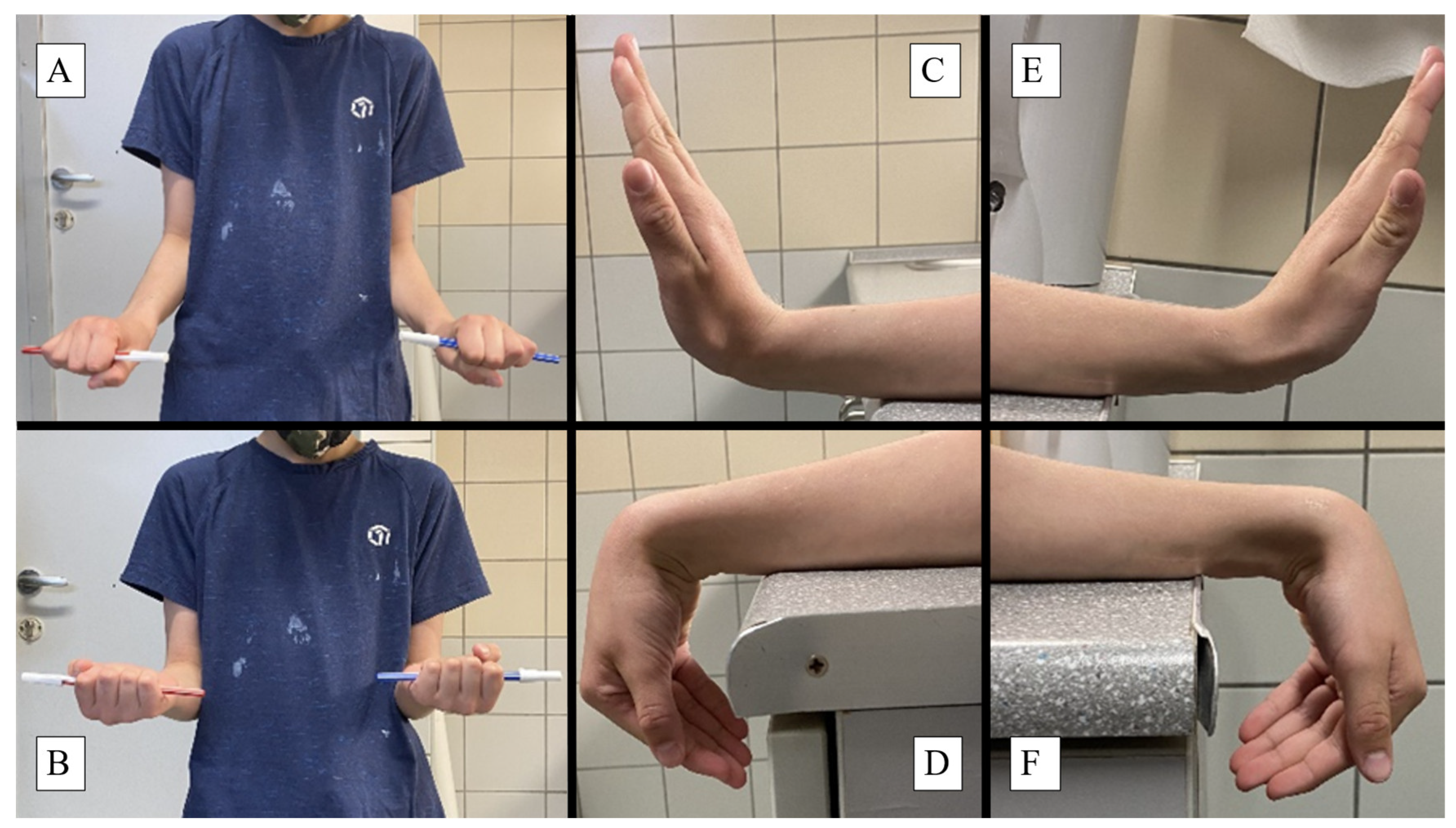
Figure 5.
X-rays captured at the one-year follow-up examination of a pediatric forearm fracture treated with PLGA implants from lateral (A) and AP (B) views show intact bone growth and development. Surgical scars were evaluated via the VSS on the olecranon (C, 0 point) and the distal end of the radius (D, 1 point).
Figure 5.
X-rays captured at the one-year follow-up examination of a pediatric forearm fracture treated with PLGA implants from lateral (A) and AP (B) views show intact bone growth and development. Surgical scars were evaluated via the VSS on the olecranon (C, 0 point) and the distal end of the radius (D, 1 point).
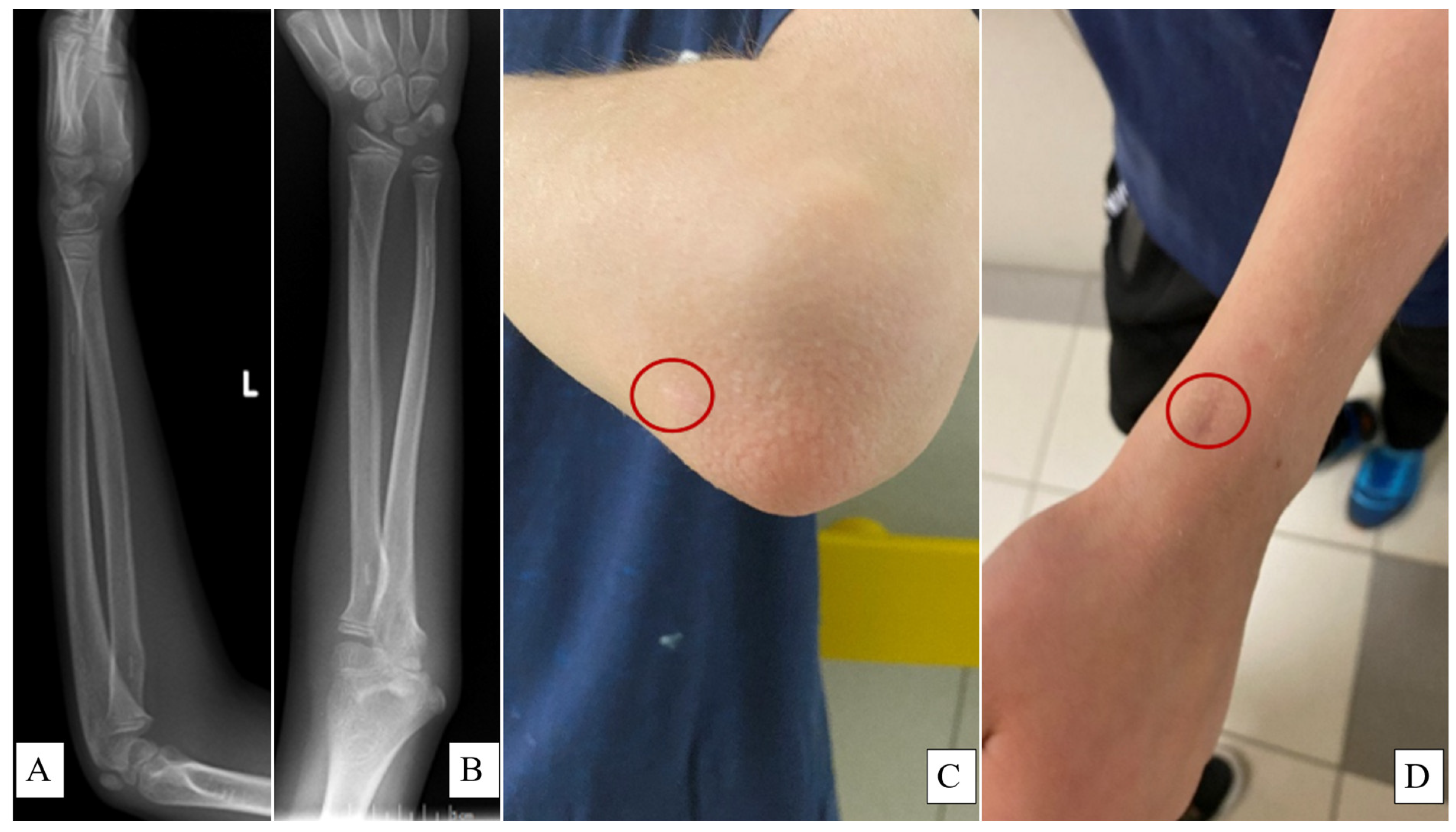

Table 1.
Discrete outcome distribution of children and their PLGA-treated forearm fractures, one year postoperation. Dominant hand analysis was only available for 21 cases, the rest was evaluated in every patient.
Table 1.
Discrete outcome distribution of children and their PLGA-treated forearm fractures, one year postoperation. Dominant hand analysis was only available for 21 cases, the rest was evaluated in every patient.
| Variable | Category | Count | Percentage |
| Sex | Female | 29 | 76.32% |
| Male | 9 | 23.68% | |
| Affected side | Left | 17 | 44.74% |
| Right | 21 | 55.26% | |
| Fracture type | Radius | 5 | 13.16% |
| Both | 32 | 84.21% | |
| Ulna | 1 | 2.63% | |
| Dominant hand | Right | 18 | 85.71% |
| Left | 3 | 14.29% | |
| Satisfaction | Satisfied | 38 | 100.00% |
Table 2.
Summary of continuous variables from 38 pediatric patients with forearm fractures treated with PLGA, resulting from the one-year postsurgical follow-up examination.
Table 2.
Summary of continuous variables from 38 pediatric patients with forearm fractures treated with PLGA, resulting from the one-year postsurgical follow-up examination.
| Endpoint (Unit) | Region | Status | Mean | SD | Min | Max | Median | IQR | IQR25 | IQR75 |
|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | ∞ | Child | 9.71 | 2.69 | 5.00 | 15.00 | 10.00 | 4.00 | 8.00 | 12.00 |
| Flexion (°) | Elbow | Operated | 139.30 | 6.20 | 130.00 | 155.00 | 140.50 | 8.25 | 136.50 | 144.75 |
| Intact | 140.80 | 6.20 | 130.00 | 155.00 | 140.50 | 8.25 | 136.50 | 144.75 | ||
| Extension (°) | Operated | -1.10 | 2.90 | -10.00 | 0.00 | 0.00 | 3.00 | -3.00 | 0.00 | |
| Intact | -1.30 | 2.90 | -10.00 | 0.00 | 0.00 | 3.00 | -3.00 | 0.00 | ||
| Pronation (°) | Forearm | Operated | 80.80 | 6.60 | 70.00 | 90.00 | 85.00 | 6.75 | 83.25 | 90.00 |
| Intact | 83.70 | 6.60 | 75.00 | 90.00 | 85.00 | 6.75 | 83.25 | 90.00 | ||
| Supination (°) | Operated | 83.50 | 6.60 | 72.00 | 110.00 | 84.00 | 5.00 | 80.00 | 85.00 | |
| Intact | 85.70 | 6.60 | 75.00 | 90.00 | 85.00 | 6.75 | 83.25 | 90.00 | ||
| Palmar Flexion (°) | Wrist | Operated | 64.90 | 6.70 | 50.00 | 75.00 | 68.00 | 5.75 | 65.00 | 70.75 |
| Intact | 68.60 | 6.10 | 50.00 | 80.00 | 70.00 | 7.00 | 66.50 | 73.50 | ||
| Dorsiflexion (°) | Operated | 73.20 | 6.70 | 60.00 | 86.00 | 68.00 | 6.00 | 65.00 | 71.00 | |
| Intact | 74.20 | 6.40 | 64.00 | 86.00 | 72.00 | 5.00 | 70.00 | 75.00 | ||
| VSS (total score) | Upper Limb | Guardian | 1.13 | 1.14 | 0.00 | 4.00 | 1.00 | 2.00 | 0.00 | 2.00 |
| Doctor | 0.55 | 0.80 | 0.00 | 3.00 | 0.00 | 1.00 | 0.00 | 1.00 |
Table 3.
Synopsis of functional and esthetic statistical comparison results.
| Measurement | Absolute Difference | Relative Difference | Test Used | p-value |
|---|---|---|---|---|
| Elbow Flexion (°) | -1.45 | 1.03% | Two-sample t | 0.282 |
| Elbow Extension (°) | 0.05 | 3.70% | Two-sample t | 0.098 |
| Pronation (°) | -1.61 | 1.31% | Mann-Whitney U | 0.166 |
| Supination (°) | 0.24 | -3.55% | Mann-Whitney U | 0.141 |
| Palmar Flexion (°) | -0.89 | 1.31% | Two-sample t | 0.563 |
| Dorsiflexion (°) | -1.55 | -3.55% | Mann-Whitney U | 0.070 |
| Dominant Hand Fracture (n) | -1 | -4.74% | Chi (χ²)-squared | 0.513 |
| VSS (Total Score) | 0.58 | 104.76% | Mann-Whitney U | 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



