
Submitted:
07 June 2024
Posted:
10 June 2024
You are already at the latest version
Abstract
Background: Despite advances in the treatment of hepatocellular carcinoma (HCC) over the last few decades, treatment opportunities for patients with HCC remain limited. HCC is the most common form of liver cancer, accounting for approximately 90% of all cases worldwide. Moreover, apart from the current pharmacological interventions, hepatic resection and liver transplantation are the mainstay curative approaches for patients with HCC.
Methods: This systematic review included phase I, II, III, and IV clinical trials (CTs) and randomized controlled trials (RCTs) on current treatments for patients with HCC in an Asian population (2013–2023). A total of 427 articles were screened, and 184 non-duplicate publications were identified. After screening titles and abstracts, 96 publications were excluded, and another 28 were excluded after full-text screening. The remaining 60 eligible RCTs/CTs were finally included.
Results: Sixty clinical trials fulfilled our inclusion criteria and screened 36 drugs as monotherapy or combination therapy for HCC. Most studies used sorafenib alone or in combination with any of the treatment regimens. Lenvatinib or atezolizumab with bevacizumab was used for HCC after initial sorafenib treatment. Eighteen studies compared the efficacy of sorafenib with that of other drugs, including lenvatinib, cabozantinib, tepotinib, tigatuzumab, linifanib, erlotinib, resminostat, brivanib, tislelizumab, selumetinib, and refametinib.
Conclusion: This study provides comprehensive insights into effective treatment interventions for HCC in Asian populations. The overall assessment indicated that sorafenib alone or in combination with atezolizumab and bevacizumab has been the first treatment choice in the past decade to achieve better outcomes in patients with HCC in an Asian population
Keywords:
Hepatocellular carcinoma
; Systematic
; Asian Population
; Treatment
1. Introduction
The increasing incidence of hepatocellular carcinoma (HCC) poses a global health challenge [1,2]. According to a recent report by GLOBOCAN 2020, Mongolia has the highest age-standardized rate for both mortality and incidence of HCC. It is also estimated that in Asia, China alone accounts for 62.4% of the cases, followed by Japan (7.0%), India (5.3%), Thailand (4.2%), and Vietnam (4%) [3]. In Asia, liver cancer is the fifth most common cancer after thyroid, stomach, colon, and lung cancers and is the second most common cause of malignancy-related deaths in Asia [4]. In Asia, HCC accounts for the highest incidence and mortality among patients with liver cancer. [4].
Over the last 3 decades, the annual crude mortality rate of HCC has increased in Asia. In addition to surgical intervention, several systemic therapies, including chemotherapy, immunotherapy, and molecular target-based therapies, have been proposed for advanced HCC. With technological advancements in research, molecular-targeted therapies are the mainstream approach for treating patients with HCC either alone or in combination with other drugs, especially in Asian populations.
The etiology of HCC varies according to geographical region, as reported by a recently published study [5]. In the Asia-Pacific region, hepatitis virus infection is among the major causes of HCC; 70% of the patients from these regions have chronic hepatitis B virus (HBV) infection, whereas 20% have hepatitis C viral (HCV) infection [5]. A study from the Asia-Pacific region has reported that 75% of the patients with HCC in Japan have HCV infection [6].
The incidence of liver cancer varies among the Asian populations. According to statistics from a recently published study, East Asian regions, including China, South Korea, and Japan, and Southeast Asian regions, including the Philippines, demonstrated a sharp decline in the incidence rate of liver cancer [7]. The same study observed a decline in the annual average percent change in the incidence rate of liver cancer in countries, including China (-1.6%), South Korea (-2.2%), and the Philippines (-1.7%), since 1978 [7]. However, a significant increase in the incidence of liver cancer has been reported in southwestern Asian countries, especially Israel [7]. HCC accounts for the majority of liver cancer cases and affects 27% of the population in Thailand alone [7]. In recent decades, the incidence of liver cancer has significantly increased in Iran, Afghanistan, Qatar, Iraq, Azerbaijan, and Nepal [3].
Among Asian countries, liver cancer in South Korea is the fourth most common cancer in men and the sixth most common in women. The decrease in the incidence of liver cancer in South Korea is mainly because of the sharp decline in HBV, which is considered a major cause of HCC. Moreover, large-scale HBV vaccination has affected the incidence of HCC in the South Korean population. Despite several pharmaceutical and technological advancements, the advanced stage of HCC at the time of diagnosis in South Korea still requires serious attention. In a previous study, the 5-year survival rate of HCC among Korean patients was relatively lower than that of other cancer types owing to several effective surveillance drives among the high-risk population in South Korea [8].
Sorafenib is among the first Food and Drug Administration (FDA)-approved interventions that are accepted worldwide for the treatment of advanced-stage HCC. It exhibits a molecularly targeted therapeutic approach by targeting and inhibiting several pathways, including vascular endothelial growth factor receptor-2 (VEGFR-2), platelet-derived growth factor receptor (PDGFR), and extracellular signal-regulated kinase (ERK)/mitogen-activated protein kinase-ERK (MEK)/ rapidly accelerated fibrosarcoma (RAF), thereby offering antiproliferative, antiangiogenic, and antiapoptotic effects [9,10]. In the Asia-Pacific phase III clinical trial (CT), sorafenib alone demonstrated a median overall survival of 6.5 months compared to placebo in patients with HCC, and thereafter, sorafenib was approved as a first-line therapeutic approach in these patients [11].
Another drug known for treating HCC is regorafenib, a multikinase inhibitor that inhibits angiogenesis and oncogenesis, thereby altering the tumor microenvironment. One phase III RESORCE trial has demonstrated regorafenib as a second-line drug for HCC treatment after sorafenib treatment [12]. Similarly, another multikinase inhibitor, lenvatinib, is considered the first-line therapy for patients with unresectable HCC [13]. Sorafenib is among the first-line therapies for advanced-stage HCC in Asia, whereas atezolizumab and bevacizumab are among the second-line therapies for progressive HCC.
Moreover, owing to the high incidence and prevalence of HCC in Asia and the Asia-Pacific region, an extensive approach to the selection of appropriate therapies against HCC is necessary. Currently, the available treatment options are limited in Asia and the Asia-Pacific region; therefore, a reliable first-line therapy should be selected to treat HCC, without any side-effects. Therefore, this study aimed to distinguish between drug therapies among the approaches available for the treatment of HCC in an Asian population.
2. Material and Methods
Search Strategy and Selection Criteria
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis criteria (Figure 1). A systematic search for eligible studies in the EMBASE, MEDLINE (via PubMed), and CENTRAL (via the Cochrane Library) databases was conducted from 2013 to 2023 (Figure 2). A total of 427 articles were screened, and among them, 184 non-duplicate publications were identified. We excluded 96 publications after screening titles and abstracts and another 28 published papers after full-text screening. Finally, the remaining 60 eligible randomized controlled trials (RCTs)/CTs were included in this systematic review.
The inclusion criteria for this systematic review were CTs (phases I, II, III, and IV) and RCTs conducted on adult patients (>18 years), including men and women with all stages of HCC, who received the intervention compared to those who received either placebo or active comparator in Asia or any multicentric trial wherein one study center was located in Asia.
The quality of this systematic review was assessed using the grade system. Briefly, the grade system is divided into four levels: very low, low, moderate, and high. All eligible studies included in this systematic review were screened for imprecision, inconsistency, risk of bias, and publication bias. The validity and authenticity of the included studies were assessed by two independent reviewers using kappa statistics with inter- and intrarater agreements. The outcomes of the extracted studies were noted in the form of the majority of the use of particular drugs for the treatment of HCC in Asia.
3. Results
We performed a systematic review of phases I, II, III, and IV CTs and RCTs on current treatments for patients with HCC (2013–2023). A total of 427 articles were screened, and among them, 184 non-duplicate publications were identified. We excluded 96 publications after screening titles and abstracts and another 28 published papers after full-text screening. The remaining 60 eligible RCTs/CTs were included in this systematic review (Figure 1).
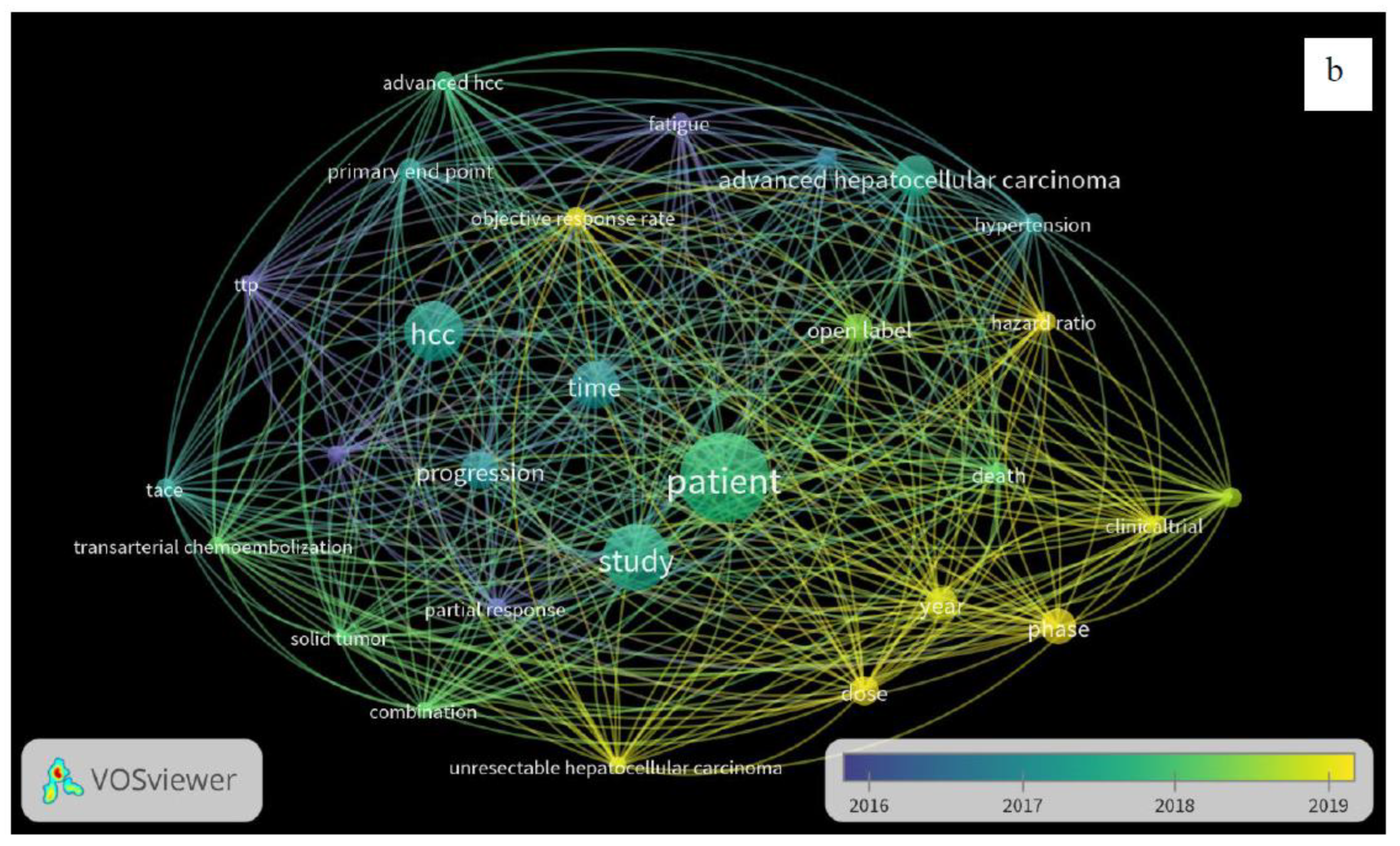
A total of 60 CTs fulfilled our inclusion criteria and screened 36 drugs for monotherapy or combination therapy for HCC. Most studies used sorafenib alone or in combination with any of the treatment regimens. Lenvatinib or atezolizumab with bevacizumab was used for HCC after initial sorafenib treatment. Eighteen studies compared the efficacy of sorafenib with that of other drugs, including lenvatinib, cabozantinib, tepotinib, tigatuzumab, linifanib, erlotinib, resminostat, brivanib, tislelizumab, selumetinib, and refametinib (Table 1). Three studies have reported on the use of a combination of lenvatinib and sorafenib (Table 1). Three studies have also reported the use of nivolumab monotherapy for the pharmacological intervention of HCC, while one study utilized a combination of ipilimumab and sorafenib (Table 1). Single-arm studies have reported each of cabozantinib, sorafenib, and immunotherapy using cytokines and enzalutamide (Table 1). Two studies have reported the treatment of HCC using ramucirumab and pembrolizumab (Table 1). This study provides comprehensive insights into effective treatment interventions for HCC in an Asian population. The overall assessment suggests that sorafenib, alone or in combination with atezolizumab and bevacizumab, has remained the first treatment choice in the past decade to provide better outcomes in patients with HCC in an Asian population. A systematic review of the published articles has reported consistency in validity appraisal among the two raters, as assessed by a kappa statistic of 0.86. The weighted bar plots of the distribution of the risk of bias judgments within each bias domain are presented in Figure 3. A network visualization of the selected articles is shown in Figure 4. Altogether, these findings suggest that sorafenib, as a combination approach with other drugs, is the first-line treatment for patients with HCC in an Asian population.

Table 1.
Eligible studies included in the systematic review showing the application in treatment of hepatocellular carcinoma.
Table 1.
Eligible studies included in the systematic review showing the application in treatment of hepatocellular carcinoma.
| Author names | Year | Drugs used | Phase | No. of participants (n) | Design | Dosage | References |
|---|---|---|---|---|---|---|---|
| Finn et al. | 2020 | Atezolizumab + Bevacizumab v/s Sorafenib |
III | 501 | Open-label RCT | Atezolizumab = 1200 mg Bevacizumab = 15 mg Sorafenib = 400 mg |
[33] |
| Kudo M et al. | 2018 | Lenvatinib v/s Sorafenib | III | 468 | Open-label RCT | Lenvatinib = 12 mg Sorafenib = 400 mg |
[34] |
| Cheng AN et al. | 2021 | Atezolizumab + Bevacizumab v/s Sorafenib |
III | 501 | Open-label RCT | Atezolizumab = 1200 mg Bevacizumab = 15 mg Sorafenib = 400 mg |
[35] |
| El-Khoueiry AB et al. | 2017 | Nivolumab | I/II | 262 | Open-label, on-comparative, dose escalation and expansion trial | 1–10 mg | [36] |
| Abou-Alfa GK et al. | 2018 | Cabozantinib | III | 707 | Double-blind, RCT | 60 mg | [37] |
| Yau T et al. | 2020 | Nivolumab + ipilimumab | I/II | 148 | Open-label, Multicohort | Nivolumab = 3 mg Ipilimumab = 1 mg | [38] |
| Kelley RK et al. | 2021 | Tremelimumab + Durvalumab | I/II | 332 | Open-label RCT | Tremelimumab = 300 mg Durvalumab = 1,500 mg |
[39] |
| Lee JH et al. | 2015 | Autologous CIK cells | III | 230 | Open-label RCT | 6.4 × 109 | [40] |
| Bruix J et al. | 2015 | Sorafenib | III | 900 | Randomized, double-blind, placebo-controlled trial | 577 mg | [41] |
| Yau T et al. | 2019 | Nivolumab | I/II | 267 | Open-label RCT | 3 mg | [42] |
| Kelley RK et al. | 2022 | Cabozantinib + atezolizumab V/S sorafenib |
III | 837 | Open-label RCT | Cabozantinib = 40 mg Atezolizumab = 1200 mg Sorafenib = 400 mg | [43] |
| Yau T et al. | 2020 | Nivolumab | III | 743 | Open-label RCT | 240 mg | [44] |
| Galle PR et al. | 2021 | Atezolizumab + Bevacizumab v/s Sorafenib |
III | 501 | Open-label RCT | Atezolizumab = 1200 mg Bevacizumab = 15 mg Sorafenib = 400 mg |
[45] |
| Zhu AX et al. | 2019 | Ramucirumab | III | 197 | Open-label RCT | 8 mg | [46] |
| Lencioni R et al. | 2016 | Transarterial chemoembolization with doxorubicin-eluting beads (DC Bead®; DEB-TACE) + Sorafenib | II | 307 | Open-label RCT | DEB-TACE = 150 mg Sorafenib = 400 mg |
[47] |
| Vogel A et al. | 2021 | Lenvatinib v/s Sorafenib |
III | 954 | Randomized, open-label, non-inferiority | Lenvatinib = 12 mg Sorafenib = 400 mg |
[48] |
| Finn RS et al. | 2019 | Pembrolizumab | III | 413 | Randomized, double-blind | 200 mg | [49] |
| Lee MS et al. | 2020 | Atezolizumab + Bevacizumab | Ib | 104 | Open-label RCT | Atezolizumab = 1200 mg Bevacizumab = 15 mg |
[50] |
| Cheon J et al. | 2022 | Atezolizumab + Bevacizumab | III | 138 | Retrospective | Atezolizumab = 1200 mg Bevacizumab = 15 mg |
[51] |
| Park JW et al. | 2019 | Sorafenib | III | 339 | Open-label RCT | Sorafenib = 600 mg | [52] |
| Choi NR et al. | 2022 | Lenvatinib+ Sorafenib | 206 | Open-label RCT | Lenvatinib = 12 mg Sorafenib = 400 mg |
[53] | |
| Cheon J et al. | 2020 | Lenvatinib | III | 67 | Retrospective | Lenvatinib = 12 mg | [54] |
| Yoon SM et al. | 2018 | Sorafenib | - | 99 | Open-label RCT | Sorafenib = 400 mg | [55] |
| Hong JY et al. | 2022 | Pembrolizumab | II | 55 | Open-label RCT | 200 mg | [56] |
| Chow PKH et al. | 2018 | Sorafenib | III | 360 | Open-label RCT | 800 mg | [57] |
| Ryoo BY et al. | 2021 | Enzalutamide | II | 165 | Randomized, Double-blind | 160 mg | [58] |
| Ryoo BY et al. | 2021 | Tepotinib v/s Sorafenib | Ib/II | 117 | Open-label RCT | Tepotinib = 1200 mg Sorafenib = 400 mg |
[59] |
| Cheng AL et al | 2015 | Tigatuzumab + sorafenib | II | 163 | Open-label RCT | Tigatuzumab = 6 mg Sorafenib = 400 mg |
[60] |
| Cainap C et al. | 2015 | Linifanib v/s Sorafenib | III | 1035 | Open-label RCT | Linifanib = 17.5 mg Sorafenib = 400 mg |
[61] |
| Zhu AX et al. | 2015 | Sorafenib + Erlotinib | III | 720 | Open-label RCT | Erlotinib = 150 mg Sorafenib = 400 mg |
[62] |
| Tak WY et al. | Sorafenib +Resminostat v/s Sorafenib |
I/II | 179 | Open-label RCT | Sorafenib + resminostat = 3+400 mg Sorafenib = 400 mg |
[63] | |
| Johnson PJ et al. | 2013 | Brivanib v/s Sorafenib | III | 1150 | Open-label RCT | Brivanib = 800 mg Sorafenib = 400 mg |
[64] |
| Zhu AX et al. | 2015 | Ramucirumab | III | 283 | Randomized, double-blind | 8 mg | [65] |
| Lim HY et al. | 2014 | Refametinib + Sorafenib | II | 95 | Open-label RCT | Refametinib= 50 mg Sorafenib= 600 mg |
[66] |
| Chung YH et al. | 2017 | Ramucirumab | III | 565 | Open-label RCT | 8 mg | [67] |
| Qin S et al. | 2020 | Camrelizumab | II | 220 | Open-label RCT | 3 mg | [68] |
| Qin S et al. | 2021 | Apatinib | III | 400 | Randomized, double-blind | 750 mg | [69] |
| Llovet JM et al. | 2022 | Lenvatinib + Pembrolizumab | III | 950 | Randomized, double-blind | Lenvatinib= 12 mg Pembrolizumab = 400 mg |
[70] |
| Ding X et al. | 2021 | Lenvatinib v/s Sorafenib | III | 64 | Open-label RCT | Lenvatinib= 12 mg Sorafenib = 400 mg |
[71] |
| Peng Z et al. | 2022 | Lenvatinib | III | 338 | Open-label RCT | Lenvatinib= 12 mg | [72] |
| He M et al. | 2019 | Sorafenib v/s Oxaliplatin, Fluorouracil, and Leucovorin+ Sorafenib |
II | 818 | Open-label RCT | Sorafenib = 400 mg Oxaliplatin= 85 mg Leucovorin = 400 mg Fluorouracil = 400 mg |
[73] |
| Qin S et al. | 2019 | Tislelizumab v/s Sorafenib | III | 640 | Open-label RCT | Tislelizumab = 200 mg Sorafenib = 400 mg |
[74] |
| Mei K et al. | 2021 | Camrelizumab + Apatinib | Ib/II | 28 | Open-label RCT | Camrelizumab = 3 mg Apatinib = 500 mg |
[75] |
| Kia Y et al. | 2022 | Camrelizumab + Apatinib | II | 20 | Open-label RCT | Camrelizumab = 200 mg Apatinib = 250 mg |
[76] |
| Xu J et al. | 2021 | Camrelizumab + Apatinib | II | 120 | Open-label | Camrelizumab = 200 mg Apatinib = 250 mg |
[77] |
| Qin S et al. | 2021 | Donafenib v/s Sorafenib | II/III | 668 | Open-label RCT | Donafenib = 200 mg Sorafenib = 400 mg |
[78] |
| Lyu N et al. | 2022 | Oxaliplatin+ Leucovorin +Fluorouracil v/s Sorafenib |
III | 262 | Open-label RCT | Oxaliplatin = 130 mg Leucovorin = 200 mg Fluorouracil = 400 mg Sorafenib = 400 mg |
[79] |
| Ren Z et al. | 2021 | Sintilimab + bevacizumab v/s Sorafenib |
II/III | 595 | Open-label RCT | Sintilimab = 200 mg bevacizumab = 15 mg Sorafenib = 400 mg |
[80] |
| Li QJ et al. | 2022 | Oxaliplatin + Leucovorin + Fluorouracil v/s Epirubicin + Lobaplatin |
III | 315 | Open-label RCT | Oxaliplatin = 130 mg Leucovorin = 400 mg Fluorouracil = 400 mg Epirubicin = 50 mg Lobaplatin = 50 mg |
[81] |
| Kang YK et al. | 2015 | Axitinib | II | 202 | Double-blind RCT | Axitinib = 5 mg | [82] |
| Llovet JM et al. | 2013 | Brivanib | III | 395 | Double-blind RCT | Brivanib = 800 mg | [83] |
| Yau TCC et al. | 2017 | Foretinib | I/II | 32 | Single-arm | Foretinib = 60 mg | [84] |
| Zhu AX et al. | 2014 | Everolimus | I | 546 | Open-label RCT | Everolimus = 7.5 mg | [85] |
| Kelley RK et al. | 2020 | Cabozantinib | II | 331 | Open-label RCT | Cabozantinib = 60 mg | [86] |
| Verset G et al. | 2022 | Pembrolizumab | II | 51 | Open-label RCT | Pembrolizumab = 200 mg | [87] |
| Abou-Alfa GK et al. | 2018 | Cabozantinib | III | 707 | Double-blind RCT | Cabozantinib = 60 mg | [88] |
| Tai WM et al. | 2016 | Selumetinib +Sorafenib | Ib | 27 | Open-label RCT | Selumetinib= 75 mg Sorafenib = 400 mg | [89] |
| Toh HC et al. | 2013 | Linifanib | II | 44 | Single-arm, open-label | Linifanib = 0.25 mg | [90] |
| Lim HY et al. | 2018 | Refametinib v/s Refametinib + Sorafenib |
II | 1318 | Open-label RCT | Refametinib = 50 mg Sorafenib = 400 mg |
[91] |
| Chow PK et al. | 2014 | Sorafenib | II | 29 | Open-label RCT | Sorafenib = 400 mg | [92] |
RCT, randomized clinical trial.
4. Discussion
This review evaluated the drugs used to treat HCC in Asia over the past decade. Sorafenib is a multikinase kinase inhibitor with a molecular weight of 637 g/mol that inhibits protein pathways that act as anticancer agents. Sorafenib acts on RAF, vascular endothelial growth factor (VEGF), and Platelet-derived growth factors receptors (PDGFR), as previously demonstrated [14]. RAF is a serine/threonine kinase that initiates the activation of gene transcription responsible for tumor promotion upon activation by the ras protein present on the membrane. Moreover, VEGF is responsible for angiogenesis in both normal and cancerous tissues, which is mediated through endothelial cell division and migration. The interaction of VEGF with VEGFRs 1, 2, and 3 promotes autophosphorylation of tyrosine receptor kinase, resulting in the activation of a cascade of downstream proteins.
Additionally, sorafenib inhibits the activities of VEGFR-2/3, PDGFR-β, Flt3, and c-Kit [15,16]. The precise molecular mechanism underlying the antitumor activity of sorafenib remains unclear, although previously published studies have suggested that sorafenib acts on RAF/MEK/ERK-dependent or -independent protein kinases [17,18,19]. Another study demonstrated that sorafenib inhibits the expression of the β-catenin oncoprotein in HepG2 cells and activates the c-Jun N-terminal kinase (JNK) and p38MAPK pathways [20]. A similar study also observed that sorafenib is actively involved in the downregulation of several DNA repair and recombination genes (XRCC-2, XRCC-5, FANCA, and FANCD2), along with genes involved in cell cycle regulation (CDC45L, CDC6, and CDCA5) that further exert anticancer activities [20].
Sorafenib is associated with common adverse effects, including diarrhea and weight loss, as well as other secondary effects, such as alopecia, anorexia, and voice changes. A previously published study revealed that sorafenib has a significant survival benefit in patients with advanced HCC, although many patients demonstrated disease progression after a reduction in dosage or treatment discontinuation [21,22]. In the Study of Heart and Renal Protection (SHARP) trial, sorafenib exerted primary and acquired resistance, which hampered the survival benefit [23]. Previous studies have demonstrated the antitumor activity of sorafenib monotherapy with some limitations, such as drug resistance and adverse effects, discouraging its use as monotherapy. A combination with nivolumab can resolve the problems associated with sorafenib monotherapy. Our results also demonstrated a trend toward the increased use of sorafenib combination therapy.
Nivolumab is a human recombinant monoclonal G4 immunoglobulin with anticancer activity mediated through programmed cell death receptor-1 (PD-1). T-cell response is commonly mediated through the PD-1 mechanism. The blockade of PD-1 receptors present on T-cells inhibits the proliferation of T-cells through a programmed cell death mechanism. In a recently published study, nivolumab was associated with some grade 1–2 adverse events, including the development of colitis and pneumonitis, along with increased alanine aminotransferase and aspartate aminotransferase activities [24].
Another anticancer drug, atezolizumab, exhibits anticancer properties by targeting PD-L1 on tumor cells, thereby preventing the binding of PD-L1 to its receptors, PD-1 and B7-1. The binding of PD-L1 to its receptor PD-1 inhibits the proliferation of T-cells, along with the inhibition of cytokine production and cytolytic activity, which in turn leads to T-cell inactivation. Similarly, T-cells and antigen-presenting cells (APCs) inhibit immune responses, including T-cell activation and cytokine release, owing to the active binding of PD-L1 to B7-1 present on T cells and APCs [25,26]. Similar to other FDA-approved PD-1/PD-L1 targeted therapies, atezolizumab is also associated with adverse immune responses, including grade 1–4 immune-mediated colitis, hepatitis, and pneumonitis [27].
Bevacizumab is a recombinant humanized monoclonal immunoglobulin G that binds to the VEGF protein and prevents it from binding to its receptor, thereby exerting a neutralizing effect [28]. HCC is an extensively vascularized solid tumor with immense dense microvessels owing to angiogenesis. Hence, targeting VEGF is a crucial step in preventing tumor angiogenesis. Adverse reactions associated with bevacizumab include hypertension, fatigue, and proteinuria [28]. Bevacizumab can be used in combination with sorafenib to overcome these side-effects.
A previously published study reported portal vein tumor invasion in 30% of the Korean patients with HCC [29]. A single-center Korean RCT reported that conventional transarterial chemoembolization (cTACE) with radiation therapy had better outcomes than sorafenib monotherapy in HCC patients with portal vein invasion. However, two other RCTs conducted in the Korean population revealed that sorafenib monotherapy did not result in survival gain compared to transarterial radioembolization (TARE) [30,31]. The study concluded that TARE, sorafenib, and cTACE did not result in any survival gains [32].
Despite several drugs in the pharmaceutical market, HCC is a highly uncontrollable cancer with a tendency to metastasize to distant organs, including the lungs and stomach. Moreover, the gap between the etiology and genetic mutations contributes to poor treatment outcomes. The current boom in nanotechnology can provide new hope for the early intervention and treatment of HCC without any associated side-effects, as in the case of drugs. Nanotechnology offers alterations to several nanoparticles that have been widely implicated in biomedical research related to cancer therapeutics. Nanoparticles improve the accessibility of drugs to human cells and increase their metabolic tendency along with delayed and prolonged therapeutic action. Its modified surface area offers greater drug loading and mitigates the side-effects of drugs. Enhanced penetration and retention mechanisms, along with active targeting, exhibit highly specific targeted anticancer therapeutics. Owing to their low or negligible toxicity, enhanced biocompatibility, and biodegradability, anticancer nanoparticles have also been the focus of research. In addition to the aforementioned characteristics, such nanoparticles also exhibit antiinflammatory, antioxidant, and antiangiogenic effects, which are useful properties for use as anticancer therapeutics.
5. Conclusion
Sorafenib as a monotherapy or in combination with atezolizumab and bevacizumab has remained the first choice of drug in the past decade to provide better outcomes in patients with HCC in an Asian population. Other approaches, including cytokine-based immunotherapy, for the treatment of HCC, with minimal side-effects and significant benefits, have also been implicated in Asia. However, newer therapeutic approaches, including nanotechnology-based delivery, need to be explored further for effective treatment of patients with HCC.
Funding
None.
Acknowledgments
The authors thank the Brain Pool Program funded by the Ministry of Science and ICT through the National Research Foundation of Korea (Grant Number 2022H1D3A2A01096346) for supporting this research. We also thank Editage (www.editage.co.kr) for English language editing.
Conflicts of Interest
The authors declare no conflict of interest, financial or otherwise.
References
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2016, 2. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular Carcinoma. New Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Cheng, Y.; Zhang, S.; Fan, J.; Gao, Q. Changing epidemiology of hepatocellular carcinoma in Asia. Liver Int. 2022, 42, 2029–2041. [Google Scholar] [CrossRef] [PubMed]
- Umemura, T.; Kiyosawa, K. Epidemiology of hepatocellular carcinoma in Japan. Hepatol. Res. 2007, 37, S95–S100. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm SM, Carter C, Tang L, et al. BAY 43–9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ MERK pathway and receptor tyrosine kinases involved in tumour progression and angiogenesis. Cancer Res 2004;64:7099–109.
- Petrick, J.L.; Florio, A.A.; Znaor, A.; Ruggieri, D.; Laversanne, M.; Alvarez, C.S.; Ferlay, J.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in hepatocellular carcinoma incidence, 1978–2012. Int. J. Cancer 2019, 147, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.K.; Chun, H.G. Status of hepatocellular carcinoma in South Korea. 2, 39. [CrossRef]
- Wilhelm SM, Adnane L, Newell P, et al. Preclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signalling. Mol Cancer Ther 2008;7:3129–40.
- Cheng, A.-L.; Kang, Y.-K.; Chen, Z.; Tsao, C.-J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.-S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2008, 10, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Roberts, P.J.; Der, C.J. Targeting the Raf-MEK-ERK mitogen-activated protein kinase cascade for the treatment of cancer. Oncogene 2007, 26, 3291–3310. [Google Scholar] [CrossRef]
- Cervello, M.; McCubrey, J.A.; Cusimano, A.; Lampiasi, N.; Azzolina, A.; Montalto, G. Targeted therapy for hepatocellular carcinoma: novel agents on the horizon. Oncotarget 2012, 3, 236–260. [Google Scholar] [CrossRef]
- Samant, R.S.; Shevde, L.A. Recent Advances in Anti-Angiogenic Therapy of Cancer. Oncotarget 2011, 2, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, M.; Davis, E.M.; Crabtree, T.R.; Habibi, J.R.; Nguyen, T.K.; Dent, P.; Grant, S. The Kinase Inhibitor Sorafenib Induces Cell Death through a Process Involving Induction of Endoplasmic Reticulum Stress. Mol. Cell. Biol. 2007, 27, 5499–5513. [Google Scholar] [CrossRef] [PubMed]
- Tai, W.-T.; Cheng, A.-L.; Shiau, C.-W.; Huang, H.-P.; Huang, J.-W.; Chen, P.-J.; Chen, K.-F. Signal transducer and activator of transcription 3 is a major kinase-independent target of sorafenib in hepatocellular carcinoma. J. Hepatol. 2011, 55, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, P.; Arienti, C.; Amadori, D.; Fabbri, F.; Carloni, S.; Tesei, A.; Vannini, I.; Silvestrini, R.; Zoli, W. Role of RAF/MEK/ERK pathway, p-STAT-3 and Mcl-1 in sorafenib activity in human pancreatic cancer cell lines. J. Cell. Physiol. 2009, 220, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Cervello, M.; Bachvarov, D.; Lampiasi, N.; Cusimano, A.; Azzolina, A.; McCubrey, J.A.; Montalto, G. Molecular mechanisms of sorafenib action in liver cancer cells. Cell Cycle 2012, 11, 2843–2855. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.-L.; Kang, Y.-K.; Chen, Z.; Tsao, C.-J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.-S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2008, 10, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Iavarone, M.; Cabibbo, G.; Piscaglia, F.; Zavaglia, C.; Grieco, A.; Villa, E.; Cammà, C.; Colombo, M. ; on behalf of the SOFIA (SOraFenib Italian Assessment) study group Field-practice study of sorafenib therapy for hepatocellular carcinoma: A prospective multicenter study in Italy. Hepatology 2011, 54, 2055–2063. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Gao, F.; Yang, J.; Fan, H.; Xie, Q.; Jiang, K.; Gong, J.; Gao, B.; Yang, Q.; Lei, Z. Risk of Adverse Events in Cancer Patients Receiving Nivolumab With Ipilimumab: A Meta-Analysis. Front. Oncol. 2022, 12, 877434. [Google Scholar] [CrossRef] [PubMed]
- Butte, M.J.; Keir, M.E.; Phamduy, T.B.; Sharpe, A.H.; Freeman, G.J. Programmed Death-1 Ligand 1 Interacts Specifically with the B7-1 Costimulatory Molecule to Inhibit T Cell Responses. Immunity 2007, 27, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Riella, L.V.; Chock, S.; Liu, T.; Zhao, X.; Yuan, X.; Paterson, A.M.; Watanabe, T.; Vanguri, V.; Yagita, H.; et al. The Novel Costimulatory Programmed Death Ligand 1/B7.1 Pathway Is Functional in Inhibiting Alloimmune Responses In Vivo. J. Immunol. 2011, 187, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Aleem A, Shah H. Atezolizumab. [Updated 2022 ]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK567758/.
- Roviello, G.; Bachelot, T.; Hudis, C.A.; Curigliano, G.; Reynolds, A.R.; Petrioli, R.; Generali, D. The role of bevacizumab in solid tumours: A literature based meta-analysis of randomised trials. Eur. J. Cancer 2017, 75, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Casak, S.J.; Donoghue, M.; Fashoyin-Aje, L.; Jiang, X.; Rodriguez, L.; Shen, Y.-L.; Xu, Y.; Jiang, X.; Liu, J.; Zhao, H.; et al. FDA Approval Summary: Atezolizumab Plus Bevacizumab for the Treatment of Patients with Advanced Unresectable or Metastatic Hepatocellular Carcinoma. Clin. Cancer Res. 2020, 27, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.-W.; Park, J.-W.; Nam, B.-H.; Yu, A.; Woo, S.M.; Kim, T.H.; Kim, S.H.; Koh, Y.H.; Kim, H.B.; Park, S.J.; et al. Clinical outcomes of a cohort series of patients with hepatocellular carcinoma in a hepatitis B virus-endemic area. J. Gastroenterol. Hepatol. 2014, 29, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Chow PK, Gandhi M. Phase III multicenter open-label randomized controlled trial of selective internal radiation therapy (SIRT) versus sorafenib in locally advanced hepatocellular carcinoma: the SIRveNIB study. J Clin Oncol 2017;35 15_Suppl:4002.
- Vilgrain, V.; Pereira, H.; Assenat, E.; Guiu, B.; Ilonca, A.D.; Pageaux, G.-P.; Sibert, A.; Bouattour, M.; Lebtahi, R.; Allaham, W.; et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1624–1636. [Google Scholar] [CrossRef] [PubMed]
- Korean Liver Cancer Association; National Cancer Center; Practice Guideline Revision Committee. 2018 Korean Liver Cancer Association–National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Gut Liver 2019, 13, 227–299. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.-L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2021, 76, 862–873. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.-Y.; Choo, S.-P.; Trojan, J.; Welling, T.H., 3rd; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Kang, Y.-K.; Kim, T.-Y.; El-Khoueiry, A.B.; Santoro, A.; Sangro, B.; Melero, I.; Kudo, M.; Hou, M.-M.; Matilla, A.; et al. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients With Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib: The CheckMate 040 Randomized Clinical Trial. JAMA Oncol. 2020, 6, e204564. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Sangro, B.; Harris, W.; Ikeda, M.; Okusaka, T.; Kang, Y.-K.; Qin, S.; Tai, D.W.-M.; Lim, H.Y.; Yau, T.; et al. Safety, Efficacy, and Pharmacodynamics of Tremelimumab Plus Durvalumab for Patients With Unresectable Hepatocellular Carcinoma: Randomized Expansion of a Phase I/II Study. J. Clin. Oncol. 2021, 39, 2991. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, J.-H.; Lim, Y.-S.; Yeon, J.E.; Song, T.-J.; Yu, S.J.; Gwak, G.-Y.; Kim, K.M.; Kim, Y.J.; Lee, J.W.; et al. Adjuvant Immunotherapy With Autologous Cytokine-Induced Killer Cells for Hepatocellular Carcinoma. Gastroenterology 2015, 148, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Takayama, T.; Mazzaferro, V.; Chau, G.-Y.; Yang, J.; Kudo, M.; Cai, J.; Poon, R.T.; Han, K.-H.; Tak, W.Y.; et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2015, 16, 1344–1354. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Hsu, C.; Kim, T.-Y.; Choo, S.-P.; Kang, Y.-K.; Hou, M.-M.; Numata, K.; Yeo, W.; Chopra, A.; Ikeda, M.; et al. Nivolumab in advanced hepatocellular carcinoma: Sorafenib-experienced Asian cohort analysis. J. Hepatol. 2019, 71, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Rimassa, L.; Cheng, A.-L.; Kaseb, A.; Qin, S.; Zhu, A.X.; Chan, S.L.; Melkadze, T.; Sukeepaisarnjaroen, W.; Breder, V.; et al. Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2022, 23, 995–1008. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Park, J.-W.; Finn, R.S.; Cheng, A.-L.; Mathurin, P.; Edeline, J.; Kudo, M.; Harding, J.J.; Merle, P.; Rosmorduc, O.; et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2021, 23, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Finn, R.S.; Qin, S.; Ikeda, M.; Zhu, A.X.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.; et al. Patient-reported outcomes with atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma (IMbrave150): an open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kang, Y.-K.; Yen, C.-J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M.; Han, G.; Tak, W.Y.; Yang, J.; Guglielmi, A.; Paik, S.W.; Reig, M.; Kim, D.Y.; Chau, G.-Y.; et al. Sorafenib or placebo plus TACE with doxorubicin-eluting beads for intermediate stage HCC: The SPACE trial. J. Hepatol. 2016, 64, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Qin, S.; Kudo, M.; Su, Y.; Hudgens, S.; Yamashita, T.; Yoon, J.-H.; Fartoux, L.; Simon, K.; López, C.; et al. Lenvatinib versus sorafenib for first-line treatment of unresectable hepatocellular carcinoma: patient-reported outcomes from a randomised, open-label, non-inferiority, phase 3 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Ryoo, B.-Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Ryoo, B.-Y.; Hsu, C.-H.; Numata, K.; Stein, S.; Verret, W.; Hack, S.P.; Spahn, J.; Liu, B.; Abdullah, H.; et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): an open-label, multicentre, phase 1b study. Lancet Oncol. 2020, 21, 808–820. [Google Scholar] [CrossRef] [PubMed]
- Cheon, J.; Yoo, C.; Hong, J.Y.; Kim, H.S.; Lee, D.; Lee, M.A.; Kim, J.W.; Kim, I.; Oh, S.; Hwang, J.; et al. Efficacy and safety of atezolizumab plus bevacizumab in Korean patients with advanced hepatocellular carcinoma. Liver Int. 2021, 42, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-W.; Kim, Y.J.; Kim, D.Y.; Bae, S.-H.; Paik, S.W.; Lee, Y.-J.; Kim, H.Y.; Lee, H.C.; Han, S.Y.; Cheong, J.Y.; et al. Sorafenib with or without concurrent transarterial chemoembolization in patients with advanced hepatocellular carcinoma: The phase III STAH trial. J. Hepatol. 2018, 70, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.R.; Kim, J.Y.; Hong, J.H.; Hur, M.H.; Cho, H.; Park, M.K.; Kim, J.; Bin Lee, Y.; Cho, E.J.; Lee, J.-H.; et al. Comparison of the outcomes between sorafenib and lenvatinib as the first-line systemic treatment for HBV-associated hepatocellular carcinoma: a propensity score matching analysis. BMC Gastroenterol. 2022, 22, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Cheon, J.; Chon, H.J.; Bang, Y.; Park, N.H.; Shin, J.W.; Kim, K.M.; Lee, H.C.; Lee, J.; Yoo, C.; Ryoo, B.-Y. Real-World Efficacy and Safety of Lenvatinib in Korean Patients with Advanced Hepatocellular Carcinoma: A Multicenter Retrospective Analysis. Liver Cancer 2020, 9, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.M.; Ryoo, B.-Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.; Lee, H.C.; Lim, Y.-S. Efficacy and Safety of Transarterial Chemoembolization Plus External Beam Radiotherapy vs Sorafenib in Hepatocellular Carcinoma With Macroscopic Vascular Invasion: A randomized clinical trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hong, J.Y.; Cho, H.J.; Sa, J.K.; Liu, X.; Ha, S.Y.; Lee, T.; Kim, H.; Kang, W.; Sinn, D.H.; Gwak, G.-Y.; et al. Hepatocellular carcinoma patients with high circulating cytotoxic T cells and intra-tumoral immune signature benefit from pembrolizumab: results from a single-arm phase 2 trial. Genome Med. 2022, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chow, P.K.; Gandhi, M.; Tan, S.-B.; Khin, M.W.; Khasbazar, A.; Ong, J.; Choo, S.P.; Cheow, P.C.; Chotipanich, C.; Lim, K.; et al. SIRveNIB: Selective Internal Radiation Therapy Versus Sorafenib in Asia-Pacific Patients With Hepatocellular Carcinoma. J. Clin. Oncol. 2018, 36, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, B.-Y.; Palmer, D.H.; Park, S.R.; Rimassa, L.; Sarker, D.; Daniele, B.; Steinberg, J.; López, B.; Lim, H.Y. Efficacy and Safety Results from a Phase 2, Randomized, Double-Blind Study of Enzalutamide Versus Placebo in Advanced Hepatocellular Carcinoma. Clin. Drug Investig. 2021, 41, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.-L.; Kang, Y.-K.; He, A.R.; Lim, H.Y.; Ryoo, B.-Y.; Hung, C.-H.; Sheen, I.-S.; Izumi, N.; Austin, T.; Wang, Q.; et al. Safety and efficacy of tigatuzumab plus sorafenib as first-line therapy in subjects with advanced hepatocellular carcinoma: A phase 2 randomized study. J. Hepatol. 2015, 63, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Cainap, C.; Qin, S.; Huang, W.-T.; Chung, I.J.; Pan, H.; Cheng, Y.; Kudo, M.; Kang, Y.-K.; Chen, P.-J.; Toh, H.-C.; et al. Linifanib Versus Sorafenib in Patients With Advanced Hepatocellular Carcinoma: Results of a Randomized Phase III Trial. J. Clin. Oncol. 2015, 33, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Rosmorduc, O.; Evans, T.J.; Ross, P.J.; Santoro, A.; Carrilho, F.J.; Bruix, J.; Qin, S.; Thuluvath, P.J.; Llovet, J.M.; et al. SEARCH: A Phase III, Randomized, Double-Blind, Placebo-Controlled Trial of Sorafenib Plus Erlotinib in Patients With Advanced Hepatocellular Carcinoma. J. Clin. Oncol. 2015, 33, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Tak, W.Y.; Ryoo, B.-Y.; Lim, H.Y.; Kim, D.-Y.; Okusaka, T.; Ikeda, M.; Hidaka, H.; Yeon, J.-E.; Mizukoshi, E.; Morimoto, M.; et al. Phase I/II study of first-line combination therapy with sorafenib plus resminostat, an oral HDAC inhibitor, versus sorafenib monotherapy for advanced hepatocellular carcinoma in east Asian patients. Investig. New Drugs 2018, 36, 1072–1084. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Qin, S.; Park, J.-W.; Poon, R.T.; Raoul, J.-L.; Philip, P.A.; Hsu, C.-H.; Hu, T.-H.; Heo, J.; Xu, J.; et al. Brivanib Versus Sorafenib As First-Line Therapy in Patients With Unresectable, Advanced Hepatocellular Carcinoma: Results From the Randomized Phase III BRISK-FL Study. J. Clin. Oncol. 2013, 31, 3517–3524. [Google Scholar] [CrossRef]
- Zhu, A.X.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Poon, R.; Pastorelli, D.; Blanc, J.-F.; Chung, H.C.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.Y.; Heo, J.; Choi, H.J.; Lin, C.-Y.; Yoon, J.-H.; Hsu, C.; Rau, K.-M.; Poon, R.T.; Yeo, W.; Park, J.-W.; et al. A Phase II Study of the Efficacy and Safety of the Combination Therapy of the MEK Inhibitor Refametinib (BAY 86-9766) Plus Sorafenib for Asian Patients with Unresectable Hepatocellular Carcinoma. Clin. Cancer Res. 2014, 20, 5976–5985. [Google Scholar] [CrossRef] [PubMed]
- Chau, I.; Peck-Radosavljevic, M.; Borg, C.; Malfertheiner, P.; Seitz, J.F.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Kudo, M.; Poon, R.; et al. Ramucirumab as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib: Patient-focused outcome results from the randomised phase III REACH study. Eur. J. Cancer 2017, 81, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Ren, Z.; Meng, Z.; Chen, Z.; Chai, X.; Xiong, J.; Bai, Y.; Yang, L.; Zhu, H.; Fang, W.; et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Li, Q.; Gu, S.; Chen, X.; Lin, L.; Wang, Z.; Xu, A.; Chen, X.; Zhou, C.; Ren, Z.; et al. Apatinib as second-line or later therapy in patients with advanced hepatocellular carcinoma (AHELP): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Vogel, A.; Madoff, D.C.; Finn, R.S.; Ogasawara, S.; Ren, Z.; Mody, K.; Li, J.J.; Siegel, A.B.; Dubrovsky, L.; et al. Randomized Phase 3 LEAP-012 Study: Transarterial Chemoembolization With or Without Lenvatinib Plus Pembrolizumab for Intermediate-Stage Hepatocellular Carcinoma Not Amenable to Curative Treatment. Cardiovasc. Interv. Radiol. 2022, 45, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Sun, W.; Li, W.; Shen, Y.; Guo, X.; Teng, Y.; Liu, X.; Zheng, L.; Li, W.; Chen, J. Transarterial chemoembolization plus lenvatinib versus transarterial chemoembolization plus sorafenib as first-line treatment for hepatocellular carcinoma with portal vein tumor thrombus: A prospective randomized study. Cancer 2021, 127, 3782–3793. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Fan, W.; Zhu, B.; Wang, G.; Sun, J.; Xiao, C.; Huang, F.; Tang, R.; Cheng, Y.; Huang, Z.; et al. Lenvatinib Combined With Transarterial Chemoembolization as First-Line Treatment for Advanced Hepatocellular Carcinoma: A Phase III, Randomized Clinical Trial (LAUNCH). J. Clin. Oncol. 2023, 41, 117–127. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Li, Q.; Zou, R.; Shen, J.; Fang, W.; Tan, G.; Zhou, Y.; Wu, X.; Xu, L.; Wei, W.; et al. Sorafenib Plus Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin vs Sorafenib Alone for Hepatocellular Carcinoma With Portal Vein Invasion: A Randomized Clinical Trial. JAMA Oncol. 2019, 5, 953–960. [Google Scholar] [CrossRef]
- Qin, S.; Finn, R.S.; Kudo, M.; Meyer, T.; Vogel, A.; Ducreux, M.; Macarulla, T.M.; Tomasello, G.; Boisserie, F.; Hou, J.; et al. RATIONALE 301 study: tislelizumab versus sorafenib as first-line treatment for unresectable hepatocellular carcinoma. Futur. Oncol. 2019, 15, 1811–1822. [Google Scholar] [CrossRef] [PubMed]
- Mei, K.; Qin, S.; Chen, Z.; Liu, Y.; Wang, L.; Zou, J. Camrelizumab in combination with apatinib in second-line or above therapy for advanced primary liver cancer: cohort A report in a multicenter phase Ib/II trial. J. Immunother. Cancer 2021, 9, e002191. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Tang, W.; Qian, X.; Li, X.; Cheng, F.; Wang, K.; Zhang, F.; Zhang, C.; Li, D.; Song, J.; et al. Efficacy and safety of camrelizumab plus apatinib during the perioperative period in resectable hepatocellular carcinoma: a single-arm, open label, phase II clinical trial. J. Immunother. Cancer 2022, 10, e004656. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Shen, J.; Gu, S.; Zhang, Y.; Wu, L.; Wu, J.; Shao, G.; Zhang, Y.; Xu, L.; Yin, T.; et al. Camrelizumab in Combination with Apatinib in Patients with Advanced Hepatocellular Carcinoma (RESCUE): A Nonrandomized, Open-label, Phase II Trial. Clin. Cancer Res. 2021, 27, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Bi, F.; Gu, S.; Bai, Y.; Chen, Z.; Wang, Z.; Ying, J.; Lu, Y.; Meng, Z.; Pan, H.; et al. Donafenib Versus Sorafenib in First-Line Treatment of Unresectable or Metastatic Hepatocellular Carcinoma: A Randomized, Open-Label, Parallel-Controlled Phase II-III Trial. J. Clin. Oncol. 2021, 39, 3002–3011. [Google Scholar] [CrossRef] [PubMed]
- Lyu, N.; Wang, X.; Li, J.-B.; Lai, J.-F.; Chen, Q.-F.; Li, S.-L.; Deng, H.-J.; He, M.; Mu, L.-W.; Zhao, M. Arterial Chemotherapy of Oxaliplatin Plus Fluorouracil Versus Sorafenib in Advanced Hepatocellular Carcinoma: A Biomolecular Exploratory, Randomized, Phase III Trial (FOHAIC-1). J. Clin. Oncol. 2022, 40, 468–480. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.; Xu, J.; Bai, Y.; Xu, A.; Cang, S.; Du, C.; Li, Q.; Lu, Y.; Chen, Y.; Guo, Y.; et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2–3 study. Lancet Oncol. 2021, 22, 977–990. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.-J.; He, M.-K.; Chen, H.-W.; Fang, W.-Q.; Zhou, Y.-M.; Xu, L.; Wei, W.; Zhang, Y.-J.; Guo, Y.; Guo, R.-P.; et al. Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin Versus Transarterial Chemoembolization for Large Hepatocellular Carcinoma: A Randomized Phase III Trial. J. Clin. Oncol. 2022, 40, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.-K.; Yau, T.; Park, J.-W.; Lim, H.Y.; Lee, T.-Y.; Obi, S.; Chan, S.L.; Qin, S.; Kim, R.D.; Casey, M.; et al. Randomized phase II study of axitinib versus placebo plus best supportive care in second-line treatment of advanced hepatocellular carcinoma. Ann. Oncol. 2015, 26, 2457–2463. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Decaens, T.; Raoul, J.-L.; Boucher, E.; Kudo, M.; Chang, C.; Kang, Y.-K.; Assenat, E.; Lim, H.-Y.; Boige, V.; et al. Brivanib in Patients With Advanced Hepatocellular Carcinoma Who Were Intolerant to Sorafenib or for Whom Sorafenib Failed: Results From the Randomized Phase III BRISK-PS Study. J. Clin. Oncol. 2013, 31, 3509–3516. [Google Scholar] [CrossRef]
- Yau, T.C.; Lencioni, R.; Sukeepaisarnjaroen, W.; Chao, Y.; Yen, C.-J.; Lausoontornsiri, W.; Chen, P.-J.; Sanpajit, T.; Camp, A.; Cox, D.S.; et al. A Phase I/II Multicenter Study of Single-Agent Foretinib as First-Line Therapy in Patients with Advanced Hepatocellular Carcinoma. Clin. Cancer Res. 2017, 23, 2405–2413. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kudo, M.; Assenat, E.; Cattan, S.; Kang, Y.-K.; Lim, H.Y.; Poon, R.T.P.; Blanc, J.-F.; Vogel, A.; Chen, C.-L.; et al. Effect of Everolimus on Survival in Advanced Hepatocellular Carcinoma After Failure of Sorafenib. JAMA 2014, 312, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Ryoo, B.-Y.; Merle, P.; Park, J.-W.; Bolondi, L.; Chan, S.L.; Lim, H.Y.; Baron, A.D.; Parnis, F.; Knox, J.; et al. Second-line cabozantinib after sorafenib treatment for advanced hepatocellular carcinoma: a subgroup analysis of the phase 3 CELESTIAL trial. ESMO Open 2020, 5, e000714. [Google Scholar] [CrossRef] [PubMed]
- Verset, G.; Borbath, I.; Karwal, M.; Verslype, C.; Van Vlierberghe, H.; Kardosh, A.; Zagonel, V.; Stal, P.; Sarker, D.; Palmer, D.H.; et al. Pembrolizumab Monotherapy for Previously Untreated Advanced Hepatocellular Carcinoma: Data from the Open-Label, Phase II KEYNOTE-224 Trial. Clin. Cancer Res. 2022, 28, 2547–2554. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Tai, W.M.; Yong, W.P.; Lim, C.; Low, L.S.; Tham, C.K.; Koh, T.S.; Ng, Q.S.; Wang, W.W.; Wang, L.Z.; Hartano, S.; et al. A phase Ib study of selumetinib (AZD6244, ARRY-142886) in combination with sorafenib in advanced hepatocellular carcinoma (HCC). Ann. Oncol. 2016, 27, 2210–2215. [Google Scholar] [CrossRef] [PubMed]
- Toh, H.C.; Chen, P.-J.; Carr, B.I.; Knox, J.J.; Gill, S.; Ansell, P.; McKeegan, E.M.; Dowell, B.; Pedersen, M.; Qin, Q.; et al. Phase 2 trial of linifanib (ABT-869) in patients with unresectable or metastatic hepatocellular carcinoma. Cancer 2012, 119, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.Y.; Merle, P.; Weiss, K.H.; Yau, T.; Ross, P.; Mazzaferro, V.; Blanc, J.-F.; Ma, Y.T.; Yen, C.J.; Kocsis, J.; et al. Phase II Studies with Refametinib or Refametinib plus Sorafenib in Patients with RAS-Mutated Hepatocellular Carcinoma. Clin. Cancer Res. 2018, 24, 4650–4661. [Google Scholar] [CrossRef] [PubMed]
- Chow, P.K.H.; Poon, D.Y.H.; Khin, M.-W.; Singh, H.; Han, H.-S.; Goh, A.S.W.; Choo, S.-P.; Lai, H.-K.; Lo, R.H.G.; Tay, K.-H.; et al. Multicenter Phase II Study of Sequential Radioembolization-Sorafenib Therapy for Inoperable Hepatocellular Carcinoma. PLOS ONE 2014, 9, e90909. [Google Scholar] [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart.
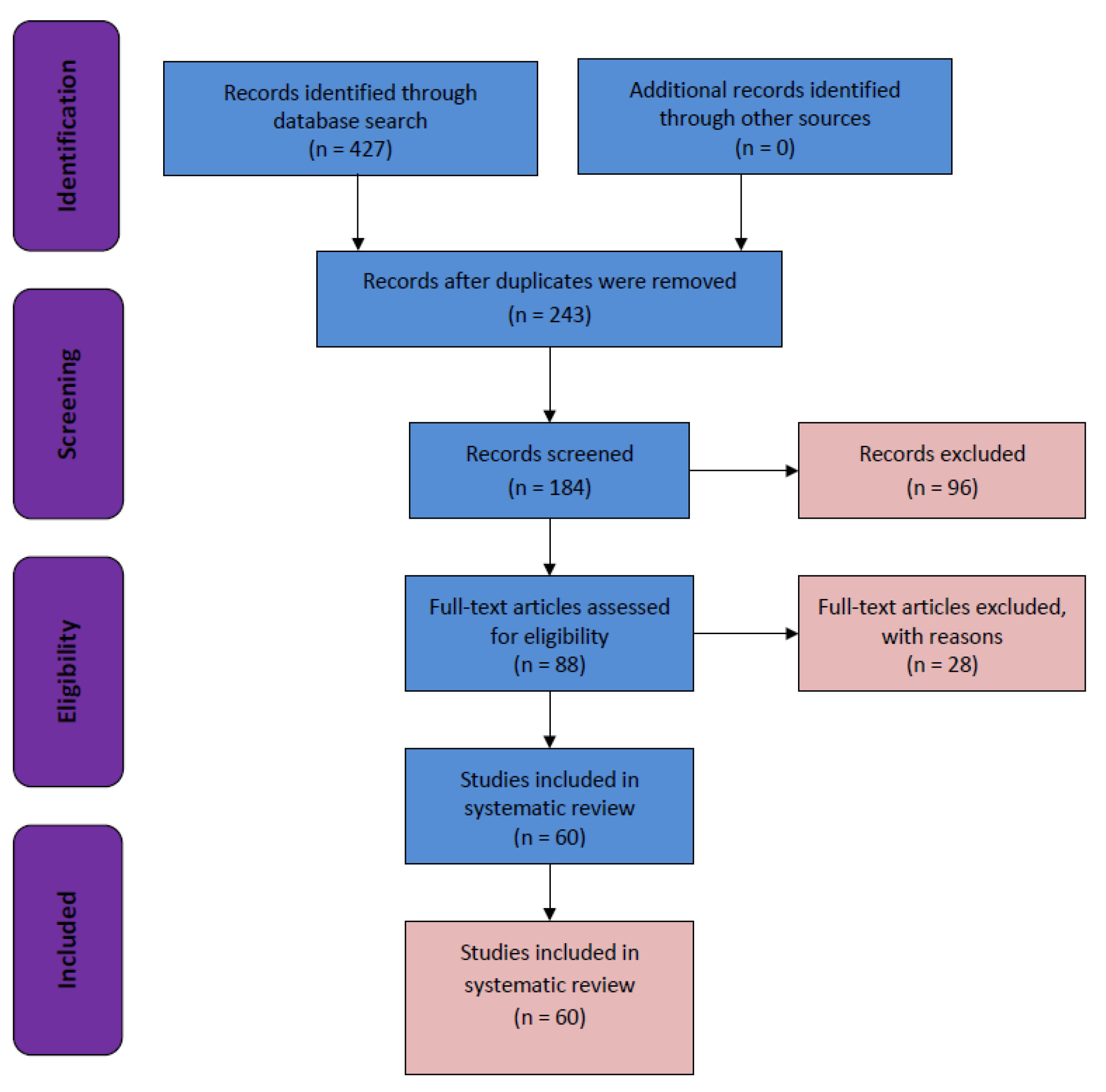
Figure 2.
Number of publications in the last 10 years (2013 to 2023) extracted from the PubMed database on phase I–IV clinical trials related to hepatocellular carcinoma that were conducted in South Korea.
Figure 2.
Number of publications in the last 10 years (2013 to 2023) extracted from the PubMed database on phase I–IV clinical trials related to hepatocellular carcinoma that were conducted in South Korea.
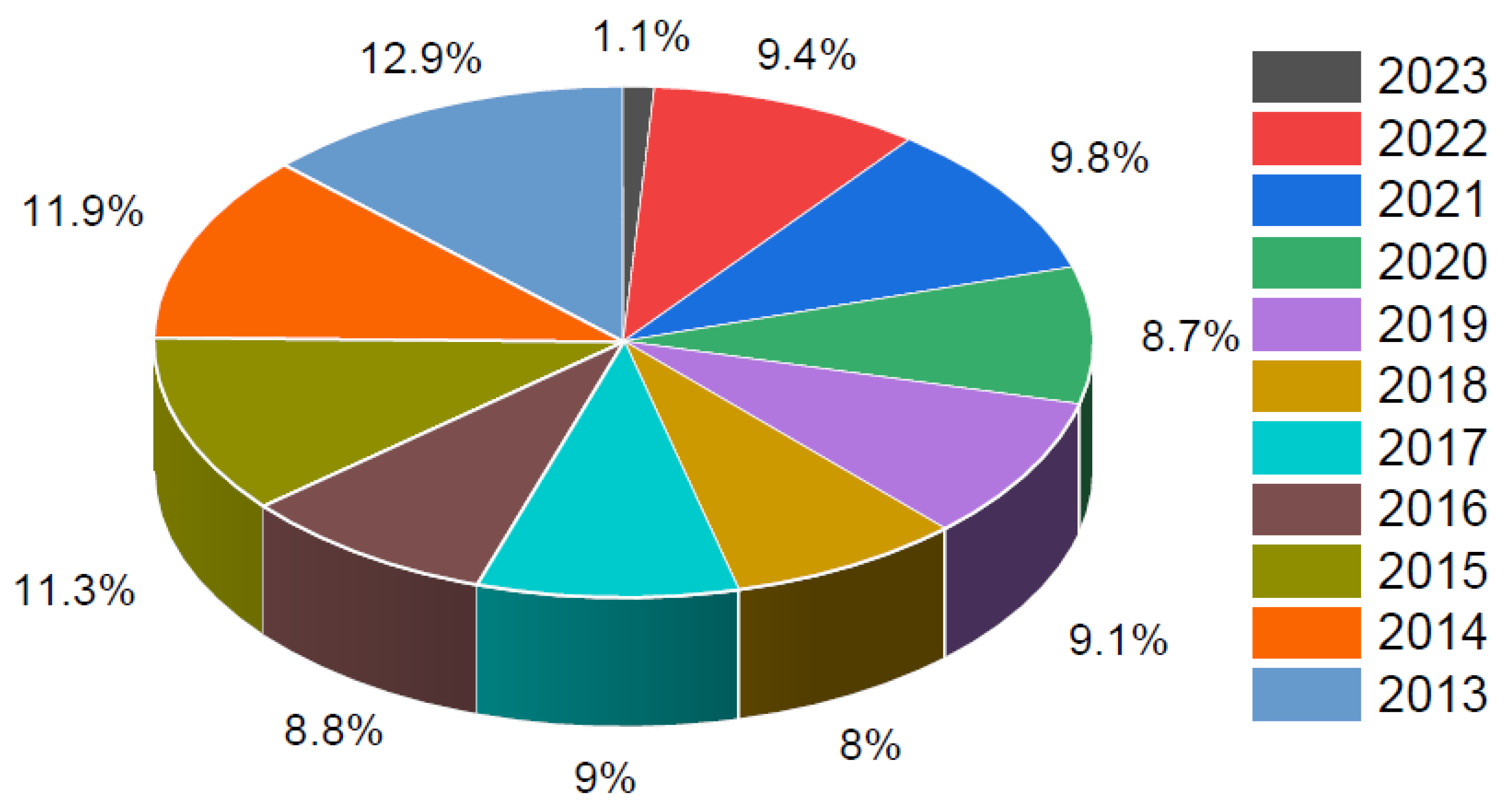
Figure 3.
Plot demonstrating risk of bias (a) Traffic light plots of domain-level judgments for each individual result. (b) Weighted bar plots of the distribution of risk of bias judgments within each bias domain.
Figure 3.
Plot demonstrating risk of bias (a) Traffic light plots of domain-level judgments for each individual result. (b) Weighted bar plots of the distribution of risk of bias judgments within each bias domain.
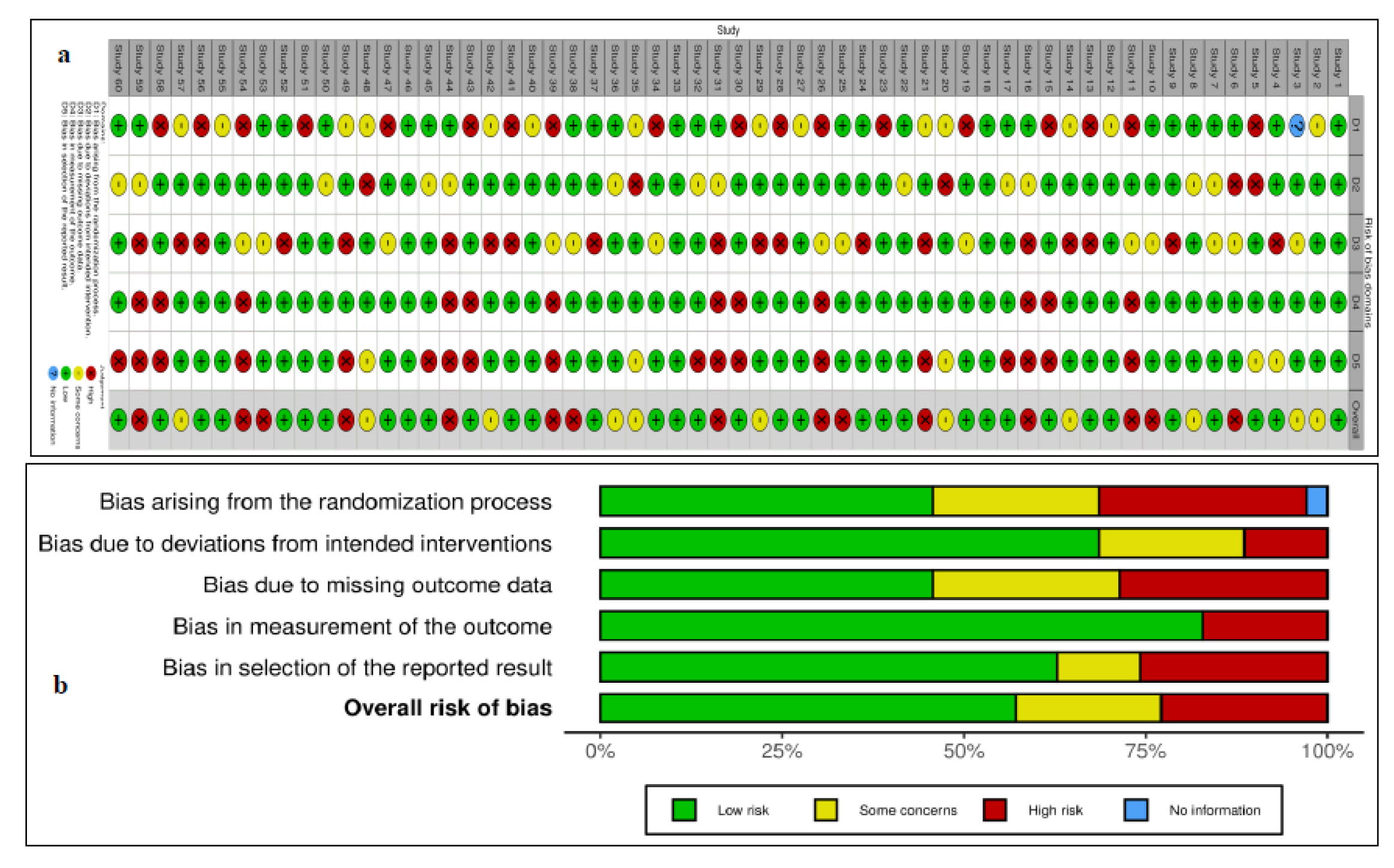
Figure 4.
Visualization of bibliometric networks of eligible articles using the VOSviewer software (n = 60): (a) network visualization and (b) overlay visualization.
Figure 4.
Visualization of bibliometric networks of eligible articles using the VOSviewer software (n = 60): (a) network visualization and (b) overlay visualization.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



