
Submitted:
07 June 2024
Posted:
10 June 2024
You are already at the latest version
Abstract
The appropriate concentration of vitamin D in the athlete’s body is essential for its proper functioning, especially in terms of muscular health, by enhancing recovery and oxygen consumption. Soccer players are required to perform frequent sprints and change of directions during training and competition. The aim of the present study was to establish whether the level of vitamin D (measured by 25-hydroxyvitamin D concentrations- 25(OH)D) in blood serum has any influence on speed (s) and change of direction (COD, s) performance. Material and methods: Twenty male soccer players from the top league in Poland participated in the study. All subjects' were evaluated for the serum concentration of 25(OH)D at the beginning of the preseason. . The linear sprint test was performed at 5m and 30m and COD (time and deficit), was evaluated at 30m at the beginning and after 6 weeks of preparatory period. Results: The results revealed that 50% of soccer players had an insufficient level or a deficit of 25(OH)D (≤ 30 ng/ml), with 20% having a significant deficiency of 30 ng/ml).There were no statistically significant correlations between the training effect for the variables ∆5m (before - after) and ∆30m (before - after). Statistically significant positive correlations were found between the training effect for the variables ∆COD (before - after) (R=0.62/p=0.003) and ∆deficit (before-after) (R=0.47/p=0.039). With a higher concentration of vitamin D in the blood, the training effect for COD and the deficit increased, which was visible in the faster performance of the COD test. No statistically significant differences were found for the mean values of the variables ∆5m (before - after) and ∆30m (before - after) in the group of subjects whose 25(OH)D concentration was 30mg /ml. Significant differences were noticed for the variables ∆COD (m=0.60 [s]) and ∆deficit (m=0.56[s]) in the group of subjects whose 25(OH)D concentration was 30mg /ml. The training effect was significantly higher for the group of subjects whose 25(OH)D concentration was above 30 mg/ml, which was observed by the faster performance of the COD test in this group of subjects. Conclusions: The serum concentration of vitamin D affects training adaptations of muscles. A lower concentration of Vitamin D seems to have a detrimental effect on the change of direction performance. Soccer players whose blood serum 25(OH)D concentrations were >30mg/ml achieved better results in the applied fitness tests.
Keywords:
vitamin D
; speed
; change of direction (COD)
; soccer’s
1. Introduction
Over the years, numerous studies have been conducted on the effects of vitamin D on the human body [1,2,3]. Previous research has revealed its significant impact on calcium-phosphate metabolism of the body's skeletal system [2,4,5]. However, the discovery of the vitamin D receptor (VDR), which mediates the biological effect of vitamin D, has transformed the understanding of this vitamin [6,7]. 25 hydroxyvitamin D (25(OH)D) is a fat-soluble vitamin that, when converted into its biologically-active form, 1,25-dihydroxyvitamin, influences the expression of over 900 genes [6,8,9]. These genes impact a wide variety of health and performance aspects, such as the immune and endocrine systems, exercise-induced inflammation, cardiovascular health, cancer prevention, neurological function, glucose metabolism, as well as bone and muscle structure and metabolism [3,6,8,10,11]. Vitamin D also has a significant impact on mental health, including depression, cognitive disorders, and neurological impairments [1,3,12]. The crucial impact of vitamin D on muscle cells results from its effects on calcium homeostasis, energy metabolism, phospholipid metabolism, cell proliferation and differentiation, protein synthesis, and mitochondrial function [1,6,13,14]. Vitamin D also plays an important role in the regulation of skeletal muscle tone and contraction, and it is necessary for a high oxygen consumption rate, muscle strength, power, and preventing muscle weakness and fatigue [15,16,17,18,19,20]. Vitamin D also regulates the synthesis of testosterone and insulin-like growth factor-1, which critically influence muscle structure and function [21,22,23].
The primary source of vitamin D, aside from the diet which provides small amounts, is skin synthesis during exposure to solar ultraviolet (UVB) radiation [6,20,22]. Skin synthesis supplies over 90% of the vitamin to the body [6,24]. Small amounts of this vitamin can be obtained from the diet by consuming fatty fish, egg yolks, mushrooms, or dairy products [25]. Unfortunately, despite two sources from which vitamin D can be replenished in the body, most inhabitants of countries located at an altitude of 35 N are diagnosed with deficiencies of this vitamin, especially in autumn, winter, and early spring when the daily dose of sunlight is low [1]. On the other hand, recent studies revealed that inhabitants of equatorial countries, where daily sunshine is high all year round, are also diagnosed with vitamin D deficiency [9]. This discovery was a huge revelation.
According to the latest standards for serum vitamin D, a concentration below 20 ng/ml indicates deficiency, between 20 to 30 ng/ml is considered insufficiency, between 30 to 50 ng/ml is categorized as sufficient, and between 50 to 100 ng/ml is deemed optimal [26]. Concentrations above 100 ng/ml indicate toxicity [26,27]. By applying these standards, a number of different authors confirm that vitamin D deficiency in athletes can reach even 60-90% [9,19,28,29,30], especially in athletes who live at or above 35° latitude and train indoors or outdoors but use sunscreen in the summer and protect themselves from the cold in autumn and winter, putting them at risk for serum 25(OH)D insufficient levels or deficits [9,19,22]. Among soccer players from England, Spain, and Poland, deficits were observed in more than 50% [9,22,31,32,33]. The greatest surprise was the results of serum vitamin D levels in soccer players from the Middle East. In Qatar, where daily sunshine is very high, over 80% of 342 soccer players were diagnosed as deficient in vitamin D [34]. Interestingly, even during strenuous training, a decline in vitamin D levels was recorded [35]. This decrease was significant, although training was performed outdoors in the summer and early autumn months. In athletes, low levels of vitamin D, lower than 30 ng/ml, may decrease anaerobic and aerobic performance and increase frequent injuries and infections [9,19]. It has been hypothesized that a serum 25(OH)D level above the normal reference range (up to 50 ng/ml) could induce beneficial adaptations in skeletal muscle, such as enhanced aerobic performance, both strength and power production, and recovery [15,36,37,38,39].
Soccer is a team sport where aerobic and anaerobic capacity, muscular strength, and speed are important factors for most of the actions during the match [22,40,41,42]. Due to the great demands of the game, soccer players must possess numerous skills to perform repetitive activities such as sprinting, jumping, accelerating, decelerating, changing direction (COD), which are interspersed with low to medium intensity, e.g., walking or jogging [43,44]. Running with high speed in a straight line and in different directions is particularly important, and during the match, these abilities enable soccer players to make decisions faster [22,42,44]. Speed and COD abilities require a rapid application of force. According to the latest research, vitamin D deficiency may reduce the ability of muscles to generate force [15]. Soccer players who are deficient in vitamin D showed a reduction in performance [22]. Studies have shown a correlation between serum 25(OH)D concentration, speed and power efficiency in young soccer players, and speed, endurance, and muscle strength in adult professional players [15,20,42,45,46,47].
The relationship between vitamin D and muscle performance in soccer players has been studied by several researchers [17,19,22,32,45,47,48]. Some researchers confirm its influence [19,22,45], while others do not [32,48]. Koundourakis et al. [45] observed a positive correlation between vitamin D levels and muscle performance in a cohort of Greek football players. Michalczyk et al. [22] also confirmed such a correlation. Similarly, a randomized study performed by Close et al. [19] showed the beneficial effects of vitamin D on muscle strength and power, as well as better sprint and vertical jump test results. In contrast, Hamilton et al. [17] found no significant association between serum 25(OH)D levels and muscle function. Similarly, Bezuglov et al. [32] did not confirm such a correlation. Additionally, in a study by Jastrzebska et al., [48] higher vitamin D levels in serum after supplementation did not significantly affect the measured performance parameters of soccer players.
Therefore, two aims of this study were: first of all, to determine the level of 25(OH)D in serum in professional soccer players during winter, and secondly, to evaluate whether the serum level of 25(OH)D affects the speed and change of direction performance (COD) in soccer players on two different occasions, prior to the beginning and at the end of the winter preparatory period. Additionally, we examined whether soccer players whose vitamin D level was below 30 ng/ml, i.e., insufficient concentrations, and those whose level was above 30 ng/ml, i.e., sufficient concentrations, achieved the same results in these tests. We hypothesized that a higher 25(OH)D serum concentration positively correlates with soccer players' sprint and COD results.
2. Material and Methods
2.1. Study Design
The experiment lasted for 6 weeks and covered the preparation period for the summer season. The athletes trained on an everyday basis (approximately 2 h/d) with an official soccer game on Saturday/Sunday. Additionally, twice a week, the players performed a strength and conditioning training session. After the end of the 6-weeks training period, a test protocol identical to the baseline one was administered. The participants who received vitamin D supplements 30 days or less prior to blood sampling or suffered from acute respiratory viral infections or any other diseases that resulted in absence from three or more training sessions 30 days or less prior to the examination were excluded from the study. The players were advised to adhere to their usual dietary routines throughout the study and refrain from the consumption of any supplements or stimulants throughout the experiment. Additional eligibility criteria to participate in the study were outlined as follows: a) a minimum of 10 years of training experience, b) participation in a first-league team, c) absence of injuries in the 6 months leading up to the assessments, and d) consistent engagement in training sessions a minimum of 5 times per week over the last 6 months. All participants were informed verbally and in writing about the procedures, possible risks and benefits of the tests and provided written consent before the commencement of the study. All research procedures were reviewed and approved by the bioethical committee of the Academy of Physical Education in Katowice (ethic references KB-05/2017, December 5, 2017); furthermore, the study conformed to the tenets of the Declaration of Helsinki for medical research involving human subjects.
The experimental sessions were conducted between 8:00 and 10:00 a.m. The session was preceded by a warm-up protocol, which included 5 minutes of cycling, 5 minutes of treadmil running, several upper and lower body exercise with targeted DROM Exercises (Dynamic Range of Motion Exercise) [43], followed by5 m and 30 m sprints, COD tests (90°) and two sets of running with submaximal speed. All sprint tests were performed on an indoor field with an artificial grass surface.
2.2. Subjects
Twenty male elite soccer players from the First Polish League (age = 22.8± 8.2 years, body mass = 75.1 ± 15,3 kg, body height = 178.3 ± 13.5 cm, soccer training experience = 12 ± 3,4 years) took part in this study. The participants were all full-time professionals who trained daily.
2.3. Sprint Test
The running times were recorded by two pairs of dual-beam Witty Gate photocells (Microgate, Bolzano, Italy). Following the warm-up phase, participants executed two successive 30-m sprints with a 5-minute rest interval in between the trials (Figure 1 and Figure 2). To avert premature activation of the starting gate, participants commenced with their leading foot positioned 0.5 m behind the initial timing gate. The best time from the two trials, both at 5 and 30 m, was preserved for further analysis.
2.4. Change of Direction Test
After the linear sprint test, participants rested for 5 minutes and then performed the COD tests (Figure 3). Each participant performed tests with a 90° COD (ZigZag test). The participant's task’ was to cover a 30 m section with designated cones with changes in direction and proper movement pattern [44]. The running test was performed twice with a 5-minute rest interval between attempts. The fastest time from each COD test was retained for further analysis.
2.5. Change of Direction Deficits
The COD deficit was calculated by the difference in run time in 30m COD test [s] and 30m linear sprint time.
2.6. Vitamin D Serum Analysis
Serum 25OH-Vitamin D was determined by RIA-CT KIP1971/KIP1974 (DIAsource ImmunoAssays SA, Louvain-la-Neuve, Belgium). For statistical analysis participants were divided into two groups according to the concentration of 25(OH)D : inadequate levels of 25(OH)D (vitamin D deficiency/insufficiency, <30 mg/ml), and adequate levels of 25(OH)D (vitamin D sufficiency, >30 mg/ml).
2.7. Statistical Analysis
All statistical analyses were performed using Statistica 13.1. The Shapiro-Wilk test was used in order to verify the normality of the distribution. Pearson's correlation and regression analysis were used to analyze the relationships between variables. Student's t-test was used to verify the significance of differences for paired values. For pairwise comparisons, effect sizes were determined by Cohen’s d which was characterized as large (d > 0.8), moderate (d between 0.8 and 0.5), small (d between 0.49 and 0.20) and trivial (d < 0.05). Percent changes with 95% confidence intervals (95CI) were also calculated. Statistical significance was set at p < 0.05.
3. Results
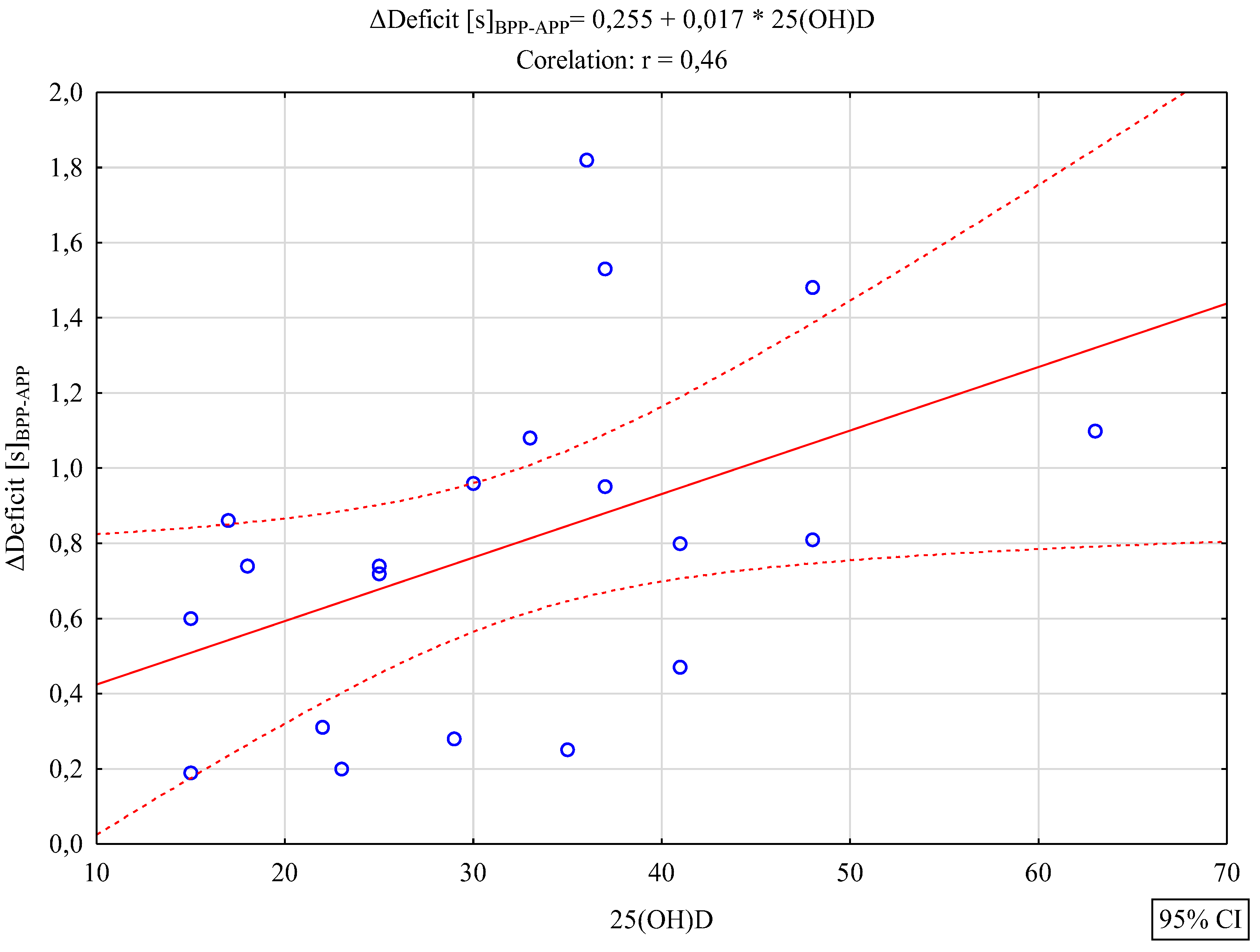
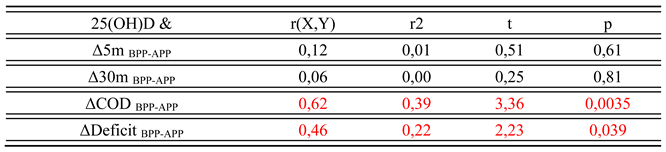
Table 1 presents basic descriptive statistics for the analyzed variables. Further analysis aimed to verify whether there were significant correlations between the level of vitamin D and variables illustrating the effects of the experiment. Between 25(OH)D and Δ5m [s]BPP-APP R=0,12; p=0,61 and between 25(OH)D and Δ30m [s]BPP-APP R=0,06; p=0,81 no significant correlations were found. Statistically significant correlations were found between vitamin D level and the effect of the experiment in the case of the variables ΔCOD [s]BPP-APP R=0,62; p=0,0035 (strong correlation) and ΔDeficit [s]BPP-APP R=0,46; p=0,039 (average correlation).It was found that the increasing trend was also statistically significant F(1,18)=13.25, p<0.0018, SE=0.28 and ΔDeficit [s]BPP-APP R=0.46, p=0.039 (average correlation). It was also found that the increasing trend was statistically significant F(1,18)=6.91, p<0.017, SE=0.39. In both cases, positive correlations were found, which indicates that with an increase in the concentration of vitamin D, a significantly higher training effect was found, i.e. a improvement of the test time in the case of COD and a reduction in the size of the deficit. These results are confirmed by the Figures below.
Figure 4.
Scatterplot with regression function for the analyzed variables. 25(OH)D & ΔCOD [s]BPP-APP.
Figure 4.
Scatterplot with regression function for the analyzed variables. 25(OH)D & ΔCOD [s]BPP-APP.
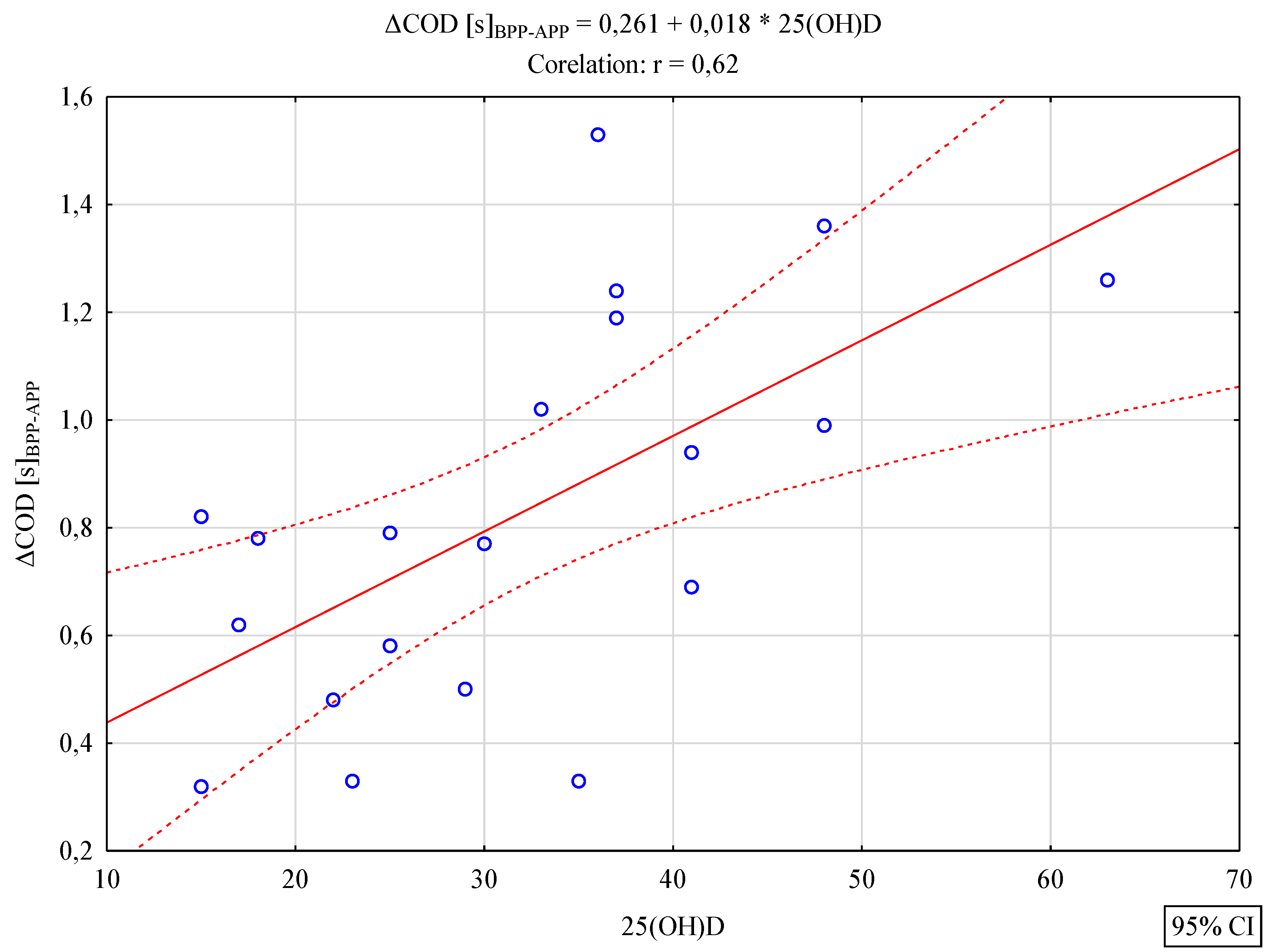
Figure 5.
Scatterplot with regression function for the analyzed variables. 25(OH)D & ΔDeficit [s]BPP-APP.
Figure 5.
Scatterplot with regression function for the analyzed variables. 25(OH)D & ΔDeficit [s]BPP-APP.
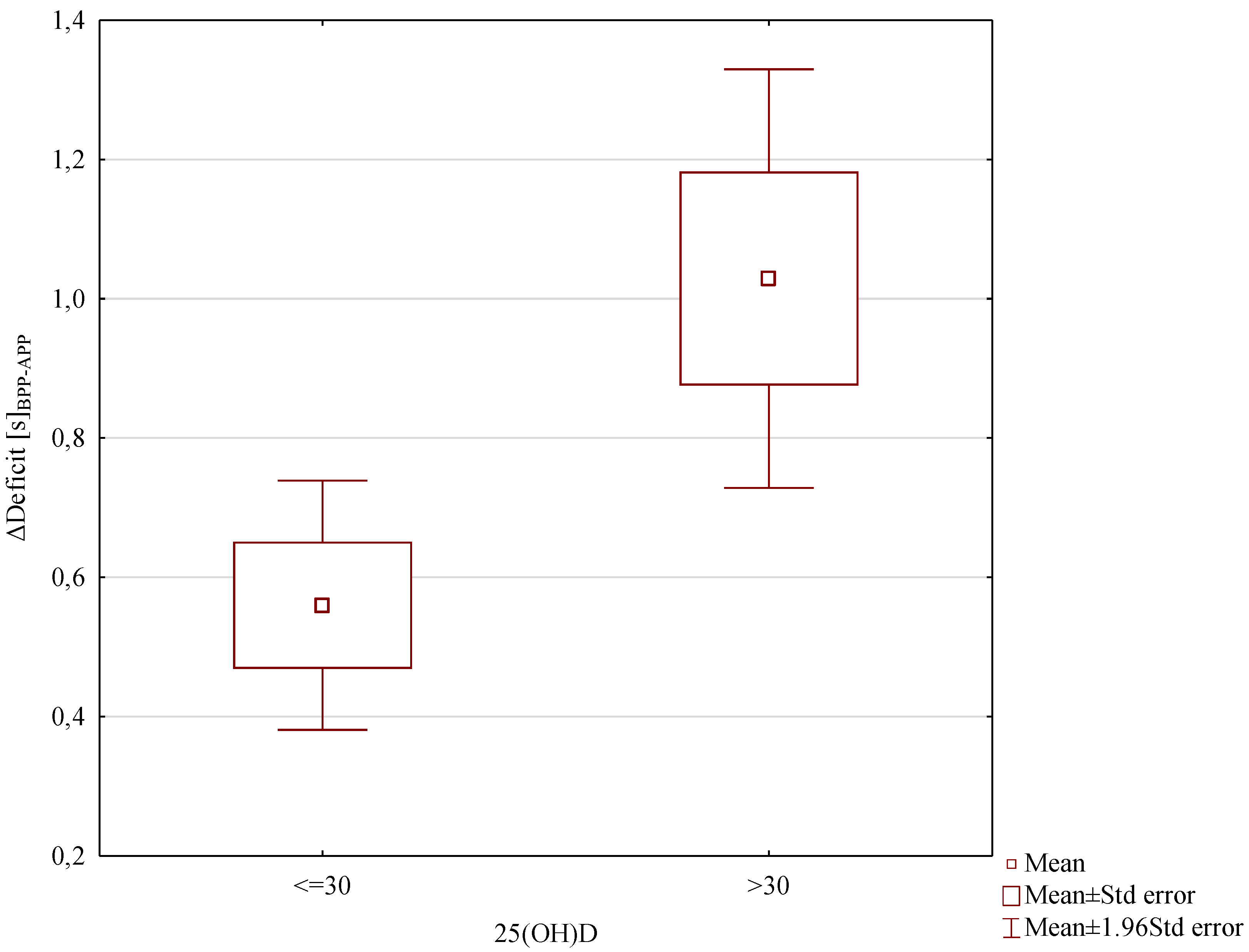
In further analyses, it was verified whether the level of 25(OH)D ≤30 or 25(OH)D >30 significantly differentiated the results of training effects. For this purpose, the Student's t test for independent samples was used. The level of 25(OH)D ≤30 or 25(OH)D >30 did not significantly differentiate training effects for the variables Δ5m [s]BPP-APP T=-0,19; df=18; p=0,85 and Δ30m [s]BPP-APP T=0,15; df=18; p=0,87. A significantly higher training effect ΔCOD [s]BPP-APP was found in the 25(OH)D >30 group M=1.055±0.35; compared to the 25(OH)D group ≤30 M=0.60±0.19; T=-3.64; df=18; p=0.0019; d=1.63. A significantly higher training effect was also found in case of the ΔDeficit [s]BPP-APP in the 25(OH)D >30 group M=1.029±0.49; compared to the 25(OH)D group ≤30 M=0.56±0.29; T=-2.63; df=18; p=0.017; d=1.13. These results are also confirmed by the Figures below.
Figure 6.
ΔCOD [s]BPP-APP results due to 25(OH)D levels.
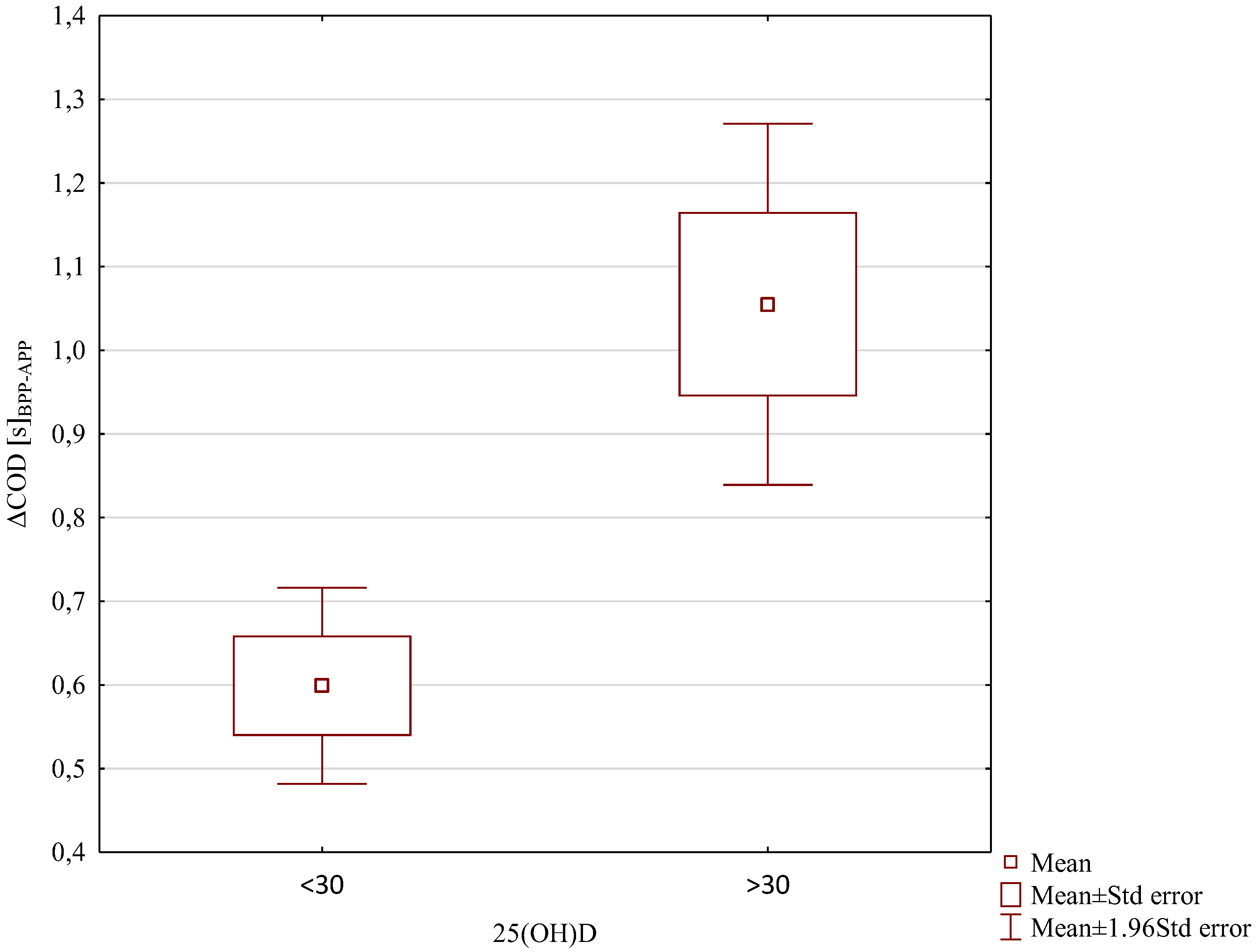
Figure 7.
ΔDeficit [s]BPP-APP results due to 25(OH)D levels.
4. Discussion
In our study, we focused on two main aspects. Firstly, we measured the levels of 25(OH)D in soccer players' serum during winter and compared the number of participants with insufficient and sufficient concentrations. The results revealed that 50% of soccer players had an insufficient level or deficit of 25(OH)D (≤ 30 ng/ml), with 20% having a deficiency of 25(OH)D (<20 ng/ml) and 30% having insufficient 25(OH)D levels (between 20-30 ng/ml). The remaining 50% had sufficient 25(OH)D levels (> 30 ng/ml).
Similar results of serum vitamin D concentration, as measured in our study, were also reported by other authors [20,22,45,47]. Gilic et al.[20] found that among the studied youth Croatia soccer players, 54% of 52 had 25(OH)D insufficient concentrations, even though they were living at a southern latitude. Bezuglov et al. [32] reported low 25(OH)D levels in 42.8% of 131 youth Russian soccer players residing in Moscow at a north latitude of 55.9°. Bezuglov and colleagues [32] explained this by lower training loads during winter compared to the summer.
In our previous study [22], we observed that during winter, 12 out of 28 soccer players had 25(OH)D serum concentrations below 20 ng/ml, and 14 out of 28 had concentrations below 30 ng/ml. Jastrzebska and co-authors [47] observed lower 25(OH)D concentration during periods of low sunlight exposure with 24 young soccer players. Conversely, Kondurakis et al.[45] observed significantly higher vitamin D concentrations following the six-week off-season period.
These results align with other studies measuring vitamin D concentration in soccer players, indicating a high prevalence of insufficiency and deficiency even in regions with sufficient sunlight [22,28,32,33,45,48]. In addition to disturbed skin synthesis in the winter, authors suggest that intense soccer training affects vitamin D levels [31,49]. Morton et al. [31] observed much lower vitamin D levels during training periods compared to the six-week detraining period, despite the fact that both periods happened in the summer [31,49]. Kondurakis et al. [45] proposed that intense training sessions, by inducing stress, weaken the athletes' immune system and play a regulatory role in vitamin D levels [45,50,51]. They supported their hypothesis by testing soccer players during the pre-season and at the beginning of the season, periods of high training and frequent soccer matches [45]. Vitamin D status is strongly associated with geographic location, season, outdoor or indoor training, and the intensity of training [27,32,52,53]. According to recent scientific reports, the increased utilization of 25(OH)D by cells of the immune system for the synthesis of defence substances against stress induced by daily high training loads is a crucial factor [19,31,50]. Additionally, during winter, immune cells use vitamin D more frequently due to the particularly intense period of infections [19].
Vitamin D and Performance
In the second aspect of our study, we investigated whether serum concentration of 25(OH)D affects speed and change of direction performance (COD) in professional soccer players. The main finding was that serum 25(OH)D concentration did not correlate with 5m and 30m linear sprint times, but it did correlate with COD performance. Comparisons between the level of 25(OH)D and Δ5m [s] before-after and between 25(OH)D and Δ30m [s] before-after did not reveal any significant associations.
Significant correlations were found between the level of vitamin D and the effect of training on ΔCOD [s] before-after (p=0.0035) (strong correlation) and Δdeficit [s] before-after (p=0.039) (average correlation). In both cases, positive correlations were found, indicating that with an increase in the level of vitamin D, a significantly higher training effect was found. This resulted in a improvement of COD performance and a reduction in the deficit value.
We also examined whether soccer players with a vitamin D level below 30 ng/ml (insufficient concentration) and those with a level above 30 ng/ml (sufficient concentration) experienced the same training effects and achieved similar results in the speed and COD tests. The level of 25(OH)D ≤30 or 25(OH)D >30 did not significantly differentiate training effects for the variables Δ5m [s] before-after and Δ30m [s] before-after. However, a significantly higher training effect in the ΔCOD [s] before-after was found in soccer players with 25(OH)D >30 compared to soccer players with 25(OH)D ≤30 (p=0.0019). Also, a significantly higher training effect was found in case of Δdeficit [s] before-after in soccer players with 25(OH)D >30 compared to soccer players with 25(OH)D ≤30 (p=0.017).
The results presented by other authors on the effect of vitamin D levels on performance are inconsistent. Most researchers studying soccer players confirm a positive correlation between vitamin D levels and speed and strength [20,22,27,42,45]. In Gilic et al.'s [20] study with 52 young Croatian soccer players, better results were observed in speed tests over distances of 10m and 20m, as well as in COD tests in players with higher 25(OH)D. In our previous study [22] with 28 soccer players, we observed that the level of vitamin D at different times of the year influenced the results of speed tests over distances of 5m and 30m. Significant differences in 25(OH)D and 5m speed test results were observed following summer compared with winter.
Our results are consistent with the data presented by Jastrzebska et al. [42], Koundourakis et al. [45], and Książek [30]. In our research, similar to Jastrzebska et al. [42], soccer players with higher concentrations of 25(OH)D achieved better results in COD tests. They also achieved significantly better results on the deficit variable, which determines the differences in time over a distance of 30m in a straight line and 30m in a zig-zag manner. Unlike in our research, Jastrzebska and colleagues [42] found significant positive correlations between 25(OH)D concentration and sprint results over distances of 10m and 30m. The authors confirmed that players with a higher vitamin D level reached better results in the speed tests. They explained this by stating that the vitamin D resources stored in athletes' bodies effectively influence the level of their anaerobic fitness. However, they concluded that it is still unclear whether the observed changes are due to differences in 25(OH)D concentration or applied training loads. In their opinion, the changes in speed and explosive power demonstrated in their study were caused by the applied training loads rather than by changes in 25(OH)D concentration.
In turn, Skalska et al. [54] suggested that a higher 25(OH)D concentration with the same training load can effectively improve the level of anaerobic fitness. Also, Książek and colleagues [29] determined the relationship between 25-(OH)D concentration and performance in 24 soccer players. These authors showed a significant association between 3-epi-25-(OH)D3 and handgrip strength and vertical jump variables in soccer players and concluded that vitamin D metabolites might be involved in skeletal muscle function [18,55].
Contrary to the previous study, some authors did not confirm an association between vitamin D serum concentrations and strength performance in soccer players [5,29]. Książek et al.[29] did not find any correlations between 25(OH)D concentration and muscle strength or maximum oxygen uptake in Polish youth soccer players. Also, Branstrom [5] in a study with Swedish female soccer players did not confirm a correlation between 25(OH)D and muscle performance assessed through isokinetic knee extension and flexion, countermovement jump, and sprint running.
Mechanisms by which vitamin D can influence speed performance are still hypothetical [20,34,36]. Vitamin D controls and regulates the expression of muscle proteins and other cellular proteins synthesis, which are involved in calcium signaling and phosphate-dependent cellular metabolism, including energy resynthesis from ATP and phosphocreatine [34,38,56]. Also, vitamin D influences muscle cellular calcium concentrations, which directly impact muscle contraction [19,57]. Vitamin D increases the influx of calcium into the cytoplasm by activating cellular kinases, empowering calcium to bind to the troponin-tropomyosin complex, resulting in exposure to active binding sites and allowing muscle contraction [20,58]. The more calcium ions are released into the cytoplasmic area, the more efficient the movement of myosin fibers through actin filaments, which may result in greater muscle contractile force and directly impact results in sprint and change of direction performance [9,56]. Additionally, VDR receptors present in myofibrils suggest a vitamin D genomic effect in their area by increasing the synthesis of muscle fibers [57]. Vitamin D influences the size of fast-twitch fibers [37], which are important for the explosive type of human movement. Fast-twitch muscles can increase the muscle's ability to generate energy very fast, resulting in higher speed and better neuromuscular coordination [20,59]. Vitamin D also increases the expression of IGF-1, which has an important role in muscle remodeling and hypertrophy [31]. It is also worth adding that a higher level of vitamin D affects the synthesis of testosterone, which increases the synthesis of muscle proteins and indirectly affects muscle cellular metabolism and, finally, muscular speed and strength [9,21,37].
Due to the high use of vitamin D by athletes’bodies every day, its level should be monitored throughout the year [17,22]. In the case of football players whose blood tests show a deficit or low level of 25(OH)D, it should be supplemented [32,45]. Our results confirmed previous studies that in soccers whose 25(OH)D level was above 30 ng/ml at the beginning of the preparatory period, training loads significantly improved speed [22,32,45]. However, much research still needs to be done in this area to clearly confirm our results.
Our study has several limitations. Firstly, the absence of a control group impacts the robustness of our findings. Additionally, we did not measure dietary vitamin D intake and serum vitamin D concentration after the preparatory period. The study also did not assess other molecules such as 1.25(OH)D, Vitamin D Binding Protein (VDBP), or molecular variables such as vitamin D receptor (VDR) polymorphism or its mutations. These omissions limit the accuracy of interpreting potential mechanisms influencing vitamin D's impact on performance. Furthermore, the study's small sample size, limited to professional soccer players, restricts the generalizability of our results to other sports. Exploring the effects of various training stresses on vitamin D status could yield interesting insights but was not addressed in this study.
5. Conclusions
For athletes, optimal functioning of muscles and the nervous system is crucial for achieving peak sports performance, and vitamin D plays a positive role in this regard [20,29]. In soccer players, this is reflected in their ability to efficiently undertake frequent sprints, maintain high concentration, and exhibit coordination for quick changes in running direction during matches [15,24]. These factors are pivotal in ensuring success in soccer matches. Participants with higher 25(OH)D levels achieved superior results in the COD test and demonstrated better deficit outcomes, affirming the positive influence of 25(OH)D on muscle metabolism. Our results align with previous research, indicating that a higher serum vitamin D concentration corresponds to enhanced muscle metabolism and improved muscle function.
Funding
This research received no external funding.
Acknowledgments
The authors declare no conflicts of interest and do not have any financial disclosures. Conceptualization, M.M.M. and A.G.; software, R.R; formal analysis, R.R; investigation, A.G; resources M.M.M and AG ; data curation, ; writing—original draft preparation, M.M.M., A.G, R.R; writing—review and editing, M.M.M., A.G and R.R; visualization, M.M.M., A.G; supervision, A.G.; project administration, A.G.; funding acquisition, A.G.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A. Vitamin D and disease prevention with special reference to cardiovascular disease. Prog Biophys Mol Biol. 2006, 92, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Rupprecht, M.; Wagenpfeil, S.; Schöpe, J.; Vieth, R.; Vogt, T.; Reichrath, J. Meta-Analysis of European Clinical Trials Characterizing the Healthy-Adult Serum 25-hydroxyvitamin D Response to Vitamin D Supplementation. Nutrients. 2023, 15, 3986. [Google Scholar] [CrossRef] [PubMed]
- Peterlik, M.; Cross, H.S. Vitamin D and calcium insufficiency-related chronic diseases: molecular and cellular pathophysiology. Eur J Clin Nutr. 2009, 63, 1377–86. [Google Scholar] [CrossRef]
- Brännström, A.; Yu, J.G.; Jonsson, P. , Åkerfeldt, T.; Stridsberg, M.; Svensson, M. Vitamin D in relation to bone health and muscle function in young female soccer players. Eur J Sport Sci. 2017, 17, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Lips, P. Vitamin D physiology. Prog Biophys Mol Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef]
- Tanaka, M.; Kishimoto, K.N.; Okuno, H.; Saito, H.; Itoi, E. Vitamin D receptor gene silencing effects on differentiation of myogenic cell lines. Muscle Nerve. 2014, 49, 700–708. [Google Scholar] [CrossRef]
- Verstuyf, A.; Carmeliet, G.; Bouillon, R. ; Mathieu, C “Vitamin D: a pleiotropic hormone”. Kidney Int. 2010, 78, 140–145. [Google Scholar] [CrossRef]
- Dahlquist, D.T.; Dieter, B.P.; Koehle, M.S. Plausible ergogenic effects of vitamin D on athletic performance and recovery. J Int Soc Sports Nutr. 2015, 12, 33, eCollection 2015. [Google Scholar] [CrossRef]
- Charoenngam, N.; Holick, M.F. Immunologic effects of vitamin D on human health and disease. Nutrients. 2020, 12, 2097. [Google Scholar] [CrossRef]
- Zittermann, A. “Vitamin D in preventive medicine: are we ignoring the evidence?”. Br J Nutr. 2003, 89, 552–572. [Google Scholar] [CrossRef] [PubMed]
- Polak, M.A.; Houghton, L.A.; Reeder, A.I.; Harper, M.J.; Conner, T.S. Serum 25-hydroxyvitamin D concentrations and depressive symptoms among young adult men and women. Nutrients. 2014, 6, 4720–30. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, K.R.; Cruzat, V.; Carlessi, R.; Newsholme, P. Mechanisms of vitamin D action in skeletal muscle. Nutr Res Rev. 2019, 32, 192–204. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Kwon, J.; Kim, H.; Shimada, H.; Yoshida, Y.; Iwasa, H.; Yoshida, H. Low serum 25-hydroxyvitamin D levels associated with falls among Japanese community-dwelling elderly. J Bone Miner Res. 2008, 23, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Barker, T.; Henriksen, V.T.; Martins, T.B.; Hill, H.R.; Kjeldsberg, C.R.; Schneider, E.D.; Dixon, B.M.; Brian, M.; Weaver, L.K. Higher serum 25-hydroxyvitamin D concentrations associate with a faster recovery of skeletal muscle strength after muscular injury. Nutrients. 2013, 5, 1253–1275. [Google Scholar] [CrossRef] [PubMed]
- Most, A.; Dorr, O.; Nef, H.; Hamm, C.; Bauer, T.; Bauer, P. Influence of 25-hydroxy-vitamin D insufficiency on maximal aerobic power in elite indoor athletes: a cross-sectional study. Sports Med - Open, 7.
- Hamilton, B.; Whiteley, R.; Farooq, A.; Chalabi, H. Vitamin d concentration in 342 professional football players and association with lower limb isokinetic function. J. Sci. Med. Sport. 2014, 17, 139–143. [Google Scholar] [CrossRef]
- Girgis, C.M.; Clifton-Bligh, R.J.; Hamrick, M.W.; Holick, M.F.; Gunton, J.E. The roles of vitamin D in skeletal muscle: form, function, and metabolism. Endocr Rev. 2013, 34, 33–83. [Google Scholar] [CrossRef] [PubMed]
- Close, G.L.; Russell, J.; Cobley, J.N.; Owens, D.J.; Wilson, G.; Gregson, W.; Fraser, W.D.; Morton, J.P. Assessment of vitamin D concentration in non-supplemented professional athletes and healthy adults during the winter months in the UK: Implications for skeletal muscle function. J. Sports Sci. 2013, 31, 344–353. [Google Scholar] [CrossRef]
- Gilic, B.; Kosor, J.; Jimenez-Pavon, D.; Markic, J.; Karin, Z.; Domic, D.S.; Sekulic, D. Associations of Vitamin D Levels with Physical Fitness and Motor Performance; A Cross-Sectional Study in Youth Soccer Players from Southern Croatia. Biology. 2021, 10, 751. [Google Scholar] [CrossRef]
- Nimptsch, K.; Platz, E.A.; Willett, W.C.; Giovannucci, E. Association Between Plasma 25-oh Vitamin D and Testosterone Levels in Men. Clin. Endocrinol. 2012, 77, 106–112. [Google Scholar] [CrossRef]
- Michalczyk, M.M.; Golas, A.; Maszczyk, A.; Zajac, A. Influence of sunlight and oral D(3) supplementation on serum 25(OH)D concentration and exercise performance in elite soccer players. Nutrients. 2020, 12, 1311. [Google Scholar] [CrossRef] [PubMed]
- Ameri, P.; Giusti, A.; Boschetti, M.; Murialdo, G.; Minuto, F.; Ferone, D. Interactions between Vitamin D and IGF-I: From Physiology to Clinical Practice. Clin. Endocrinol. 2013, 79, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, L.Y.; Wortsman, J.; Dannenberg, M.J.; Hollis, B.W.; Lu, Z.; Holick, M.F. Clothing prevents ultraviolet-B radiation-dependent photosynthesis of vitamin D3. J. Clin. Endocrinol. Metab. 1992, 75, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Holden, J.M.; Lemar, L.E.; Exler, J. Vitamin D in foods: development of the US Department of Agriculture database. Am J Clin Nutr. 2008, 87, 1092S–6S. [Google Scholar] [CrossRef]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; Rudenka, E.; Misiorowski, W.; Zakharova, I.; Rudenka, A.; Łukaszkiewicz, J.; Marcinowska-Suchowierska, E.; Łaszcz, N.; Abramowicz, P.; Bhattoa, H.P.; Wimalawansa, S.J. Vitamin D supplementation guidelines. J Steroid Biochem Mol Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Hollis, W.B. Circulating 25-Hydroxyvitamin D levels indicative of Vitamin D insufficiency: Implications of establishing a new effective dietary intake. Recommendations for Vitamin, D. J Nutr. 2005; 135, 317–22. [Google Scholar]
- Cashman, K.D.; Dowling, K.G.; Skrabakova, Z.; Gonzalez-Gross, M.; Valtuena, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Molgaard, C.; et al. Vitamin D deficiency in Europe-Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Ksiazek, A.; Zagrodna, A.; Dziubek, W.; Pietraszewski, B.; Ochmann, B.; Słowińska-Lisowska, M. 25(OH)D3 levels relative to muscle strength and maximum oxygen uptake in athletes. J Hum Kinet. 2016, 50, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Ksiazek, A.; Zagrodna, A.; Slowinska-Lisowska, M.; Lombardi, G. Relationship between metabolites of vitamin D, free 25-(OH)D, and physical performance in indoor and outdoor athletes. Front Physiol. 2022, 13, 909086, eCollection 2022. [Google Scholar] [CrossRef] [PubMed]
- Morton, J.P.; Iqbal, Z.; Drust, B.; Burgess, D.; Close, G.L.; Brukner, P.D. Seasonal variation in vitamin D status in professional soccer players of the English premier league. Appl. Physiol. Nutr. Metab. 2012, 37, 798–802. [Google Scholar] [CrossRef]
- Bezuglov, E.; Tikhonova, A.; Zueva, A.; Khaitin, V.; Lyubushkina, A.; Achkasov, E.; Waśkiewicz, Z.; Gerasimuk, D.; Żebrowska, A.; Nikolaidis, P.T.; Rosemann, T.; Knechtle, B. The Dependence of Running Speed and Muscle Strength on the Serum Concentration of Vitamin D in Young Male Professional Football Players Residing in the Russian Federation. Nutrients. 2019, 11, 1960. [Google Scholar] [CrossRef]
- Bezuglov, E.; Tikhonova, A.; Zueva, A.; Khaitin, V.; Waśkiewicz, Z.; Gerasimuk, D.; Żebrowska, A.; Rosemann, T.; Nikolaidis, P.; Knechtle, B. Prevalence and Treatment of Vitamin D Deficiency in Young Male Russian Soccer Players in Winter. Nutrients. 2019, 11, 2405. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, B. Vitamin D and Human Skeletal Muscle. Scand. J. Med. Sci. Sports. 2010, 20, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Andersen, N.E.; Karl, J.P.; Cable, S.J.; Williams, K.W.; Rood, J.C.; Young, A.J.; Lieberman, H.R.; McClung, J.P. Vitamin D status in female military personnel during combat training. J Int Soc Sports Nutr. 2010, 14, 7–38. [Google Scholar] [CrossRef] [PubMed]
- Von Hurst, P.R.; Beck, K.L. Vitamin D and skeletal muscle function in athletes. Curr. Opin. Clin. Nutr. Metab. Care. 2014, 17, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Ardestani, A.; Parker, B.; Mathur, S.; Clarkson, P.; Pescatello, L.S.; Hoffman, H.J.; Polk, D.M.; Thompson, P.D. Relation of vitamin d level to maximal oxygen uptake in adults. Am J Cardiol. 2011, 107, 1246–1249. [Google Scholar] [CrossRef] [PubMed]
- Butscheidt, S.; Rolvien, T.; Ueblacker, P.; AmLing, M.; Barvencik, F. Impact of Vitamin D in Sports: Does vitamin D insufficiency compromise athletic performance? Sportverletz. Sportschaden. 2017, 31, 37–44. [Google Scholar] [PubMed]
- Agergaard, J.; Trøstrup, J.; Uth, J.; Iversen, J.V.; Boesen, A.; Andersen, J.L.; Schjerling, P.; Langberg, H. Does Vitamin-D Intake During Resistance Training Improve the Skeletal Muscle Hypertrophic and Strength Response in Young and Elderly men?—A Randomized Controlled Trial. Nutr. Metab. 2015, 2, 32. [Google Scholar] [CrossRef] [PubMed]
- Giminiani, R.D.; Visca, C. Explosive strength and endurance adaptations in young elite soccer players during two soccer seasons. PLoS One. 2017; 12, e0171734, Published online 2017 Feb 13. [Google Scholar] [CrossRef]
- Zajac, A.; Golas, A.; Chycki, J.; Halz, M.; Michalczyk, M. The Effects of Long-Term Magnesium Creatine Chelate Supplementation on Repeated Sprint Ability (RAST) in Elite Soccer Players. Nutrients. 2020, 12, 2961. [Google Scholar] [CrossRef]
- Jastrzębska, J.; Skalska, M.; Radzimiński, Ł.; López-Sánchez, G.F.; Weiss, K.; Hill, L.; Knechtle, B. Changes of 25(OH)D Concentration, Bone Resorption Markers and Physical Performance as an Effect of Sun Exposure, Supplementation of Vitamin D and Lockdown among Young Soccer Players during a One-Year Training Season. Nutrients. 2022, 14, 521. [Google Scholar] [CrossRef]
- Askar, P.V.; Pais, V.; Mohan, N.; Saad, S.; Shaikhji, N.M. Effectivness of eccentric training, dynamic range of motion exercise and static stretching on flexibility of hamstring muscle among football players. Int J Physio, 2015; 2, 1012–1018. [Google Scholar]
- Papla, M.; Latocha, A.; Grzyb, W.; Golas, A. Relationship between lower limb power output, sprint and change of direction performance in soccer players. Balt J Health Phys Act. 2022, 14, 3. [Google Scholar] [CrossRef]
- Koundourakis, N.E.; Androulakis, N.E.; Malliaraki, N.; Margioris, A.N. Vitamin D and exercise performance in professional soccer players. PLoS ONE. 2014, 9, e101659. [Google Scholar] [CrossRef] [PubMed]
- Bezrati, I.; Ben Fradj, M.K.; Hammami, R.; Ouerghi, N.; Padulo, J.; Feki, M. A Single Mega Dose of Vitamin D(3) Improves Selected Physical Variables in Vitamin D-Deficient Young Amateur Soccer Players: A Randomized Controlled Trial. Appl. Physiol. Nutr. Metab. 2020, 45, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Jastrzebska, M.; Kaczmarczyk, M.; Michalczyk, M.; Radziminski, L.; Stepien, P.; Jastrzebska, J.; Wakuluk, D.; Suarez, A.D.; Lopez Sanchez, G.F.; Cieszczyk, P.; Godlewski, P.; Król, P.; Jastrzębski, Z. Can Supplementation of Vitamin D Improve Aerobic Capacity in Well Trained Youth Soccer Players? J. Hum. Kinet. 2018, 61, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Jastrzębska, M.; Kaczmarczyk, M.; Jastrzębski, Z. The effect of vitamin d supplementation on training adaptation in well trained soccer players. J. Strength Cond. Res. 2016, 30, 2648–2655. [Google Scholar] [CrossRef] [PubMed]
- Kopeć, A.; Solarz, K.; Majda, F.; Słowińska-Lisowska, M.; Mędraś, M. An evaluation of the levels of vitamin d and bone turnover markers after the summer and winter periods in polish professional soccer players. J Hum Kinet. 2013, 38, 135–40, eCollection 2013. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.F.; Liu, P.T.; Modlin, R.L.; Adams, J.S.; Hewison, M. Impact of vitamin D on immune function: lessons learned from genome-wide analysis. Front Physiol. 2014, 5, 151. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M. Immune function in sport and exercise. J Appl Physiol. 2007, 103, 693–9. [Google Scholar] [CrossRef] [PubMed]
- Solarz, K.; Kopeć, A.; Pietraszewska, J.; Majda, F.; Słowińska-Lisowska, M.; Mędraś, M. An evaluation of the levels of 25-hydroxyvitamin D3 and bone turnover markers in professional football players and in physically inactive men. Physiol. Res. 2014, 63, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Barcal, J.N.; Thomas, J.T.; Hollis, B.W.; Austin, K.J.; Alexander, B.M.; Larson-Meyer, D.E. Vitamin D and weight cycling: Impact on injury, illness, and inflammation in collegiate wrestlers. Nutrients. 2016, 8, E775. [Google Scholar] [CrossRef]
- Skalska, M.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.J.; Radzimiński, Ł.; Jastrzębska, J.; Kaczmarczyk, M.; Myśliwiec, A.; Dragos, P.; López-Sánchez, G.F.; Jastrzębski, Z. Vitamin D Supplementation and Physical Activity of Young Soccer Players during High-Intensity Training. Nutrients. 2019, 11, E349. [Google Scholar] [CrossRef]
- Dzik, K.P.; Kaczor, J.J. Mechanisms of vitamin D on skeletal muscle function: oxidative stress, energy metabolism and anabolic state. Eur J Appl Physiol. 2019, 119, 825–839, Published online 2019 Mar 4. [Google Scholar] [CrossRef] [PubMed]
- Berchtold, M.W.; Brinkmeier, H.; Muntener, M. Calcium Ion in Skeletal Muscle: Its Crucial Role for MuscleFunction, Plasticity, and Disease. Physiol. Rev. 2000, 80, 1215–1265. [Google Scholar] [CrossRef] [PubMed]
- Wiciński, M.; Adamkiewicz, D.; Adamkiewicz, M.; Śniegocki, M.; Podhorecka, M.; Szychta, P.; Malinowski, B. Impact of Vitamin D on Physical Efficiency and Exercise Performance- A Review. Nutrients. 2019, 11, 2826, Published online 2019 Nov 19. [Google Scholar] [CrossRef] [PubMed]
- Santillán, G.; Katz, S.; Vazquez, G.; Boland, R.L. TRPC3-Like Protein and Vitamin D Receptor Mediate 1alpha,25(OH)2D3-Induced SOC Influx in Muscle Cells. Int. J. Biochem. Cell Biol. 2004, 36, 1910–1918. [Google Scholar] [CrossRef]
- Deschenes, M.R.; Kraemer, W.J. Performance and Physiologic Adaptations to Resistance Training. Am. J. Phys. Med. Rehabil. 2002, 81, S3–S16. [Google Scholar] [CrossRef]
Figure 1.
Schematic presentation of the 5m (A) and 30m (B) sprint test. Circles represent the position of photocells.
Figure 1.
Schematic presentation of the 5m (A) and 30m (B) sprint test. Circles represent the position of photocells.
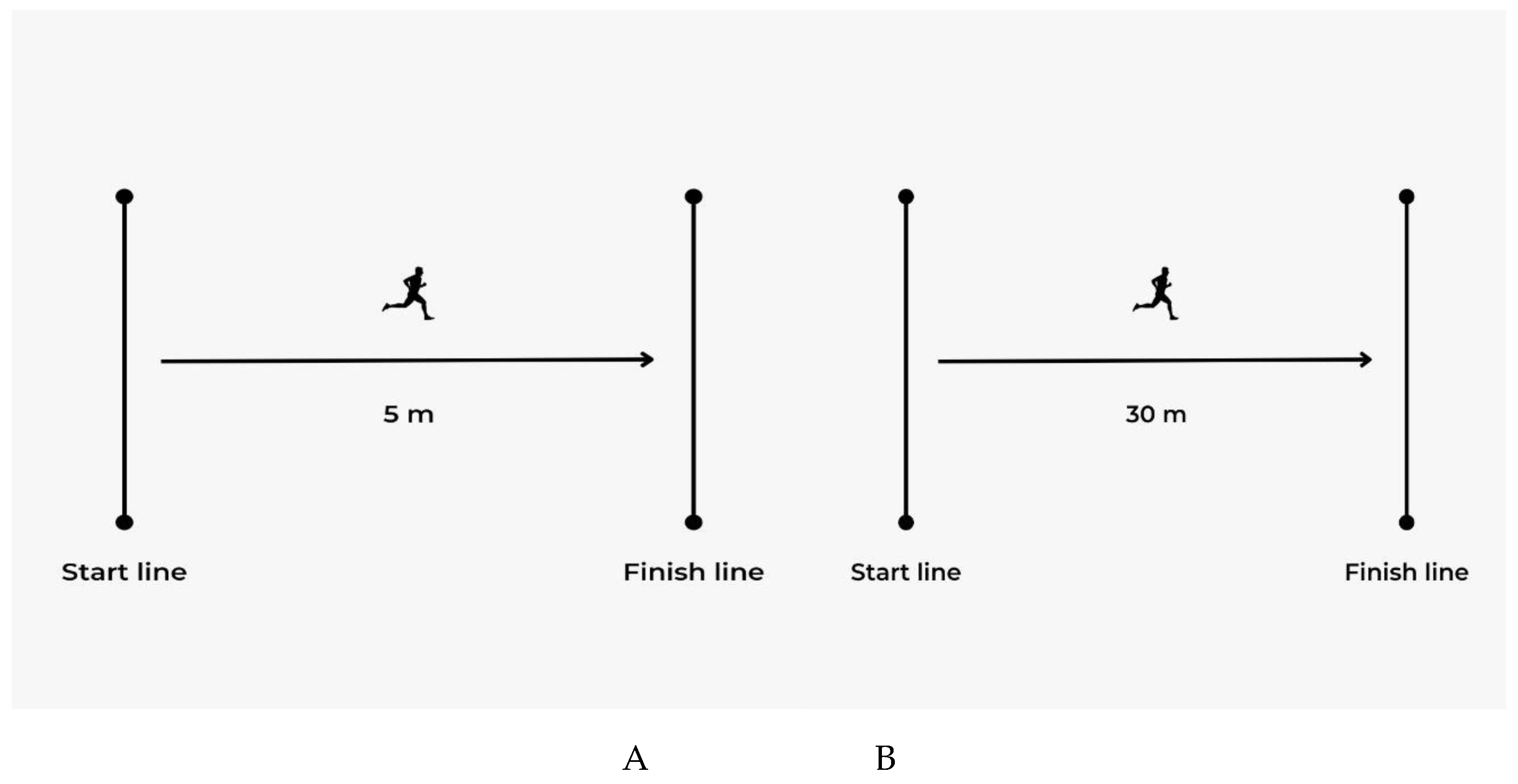
Figure 2.
Schematic presentation of the 90º change of direction test. Circles represent the position of photocells.
Figure 2.
Schematic presentation of the 90º change of direction test. Circles represent the position of photocells.
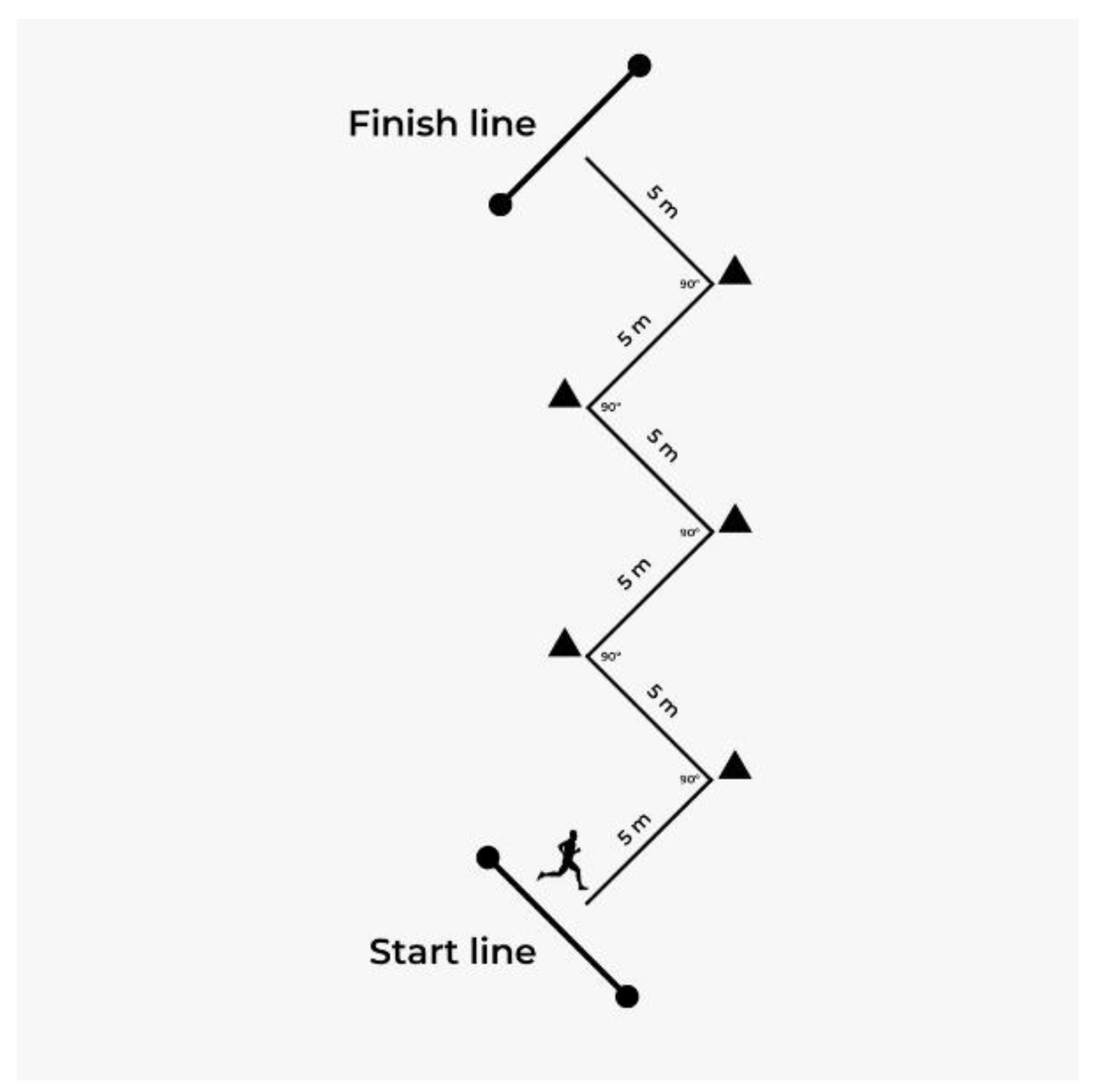

Table 1.
Basic descriptive statistics for the analyzed variables.
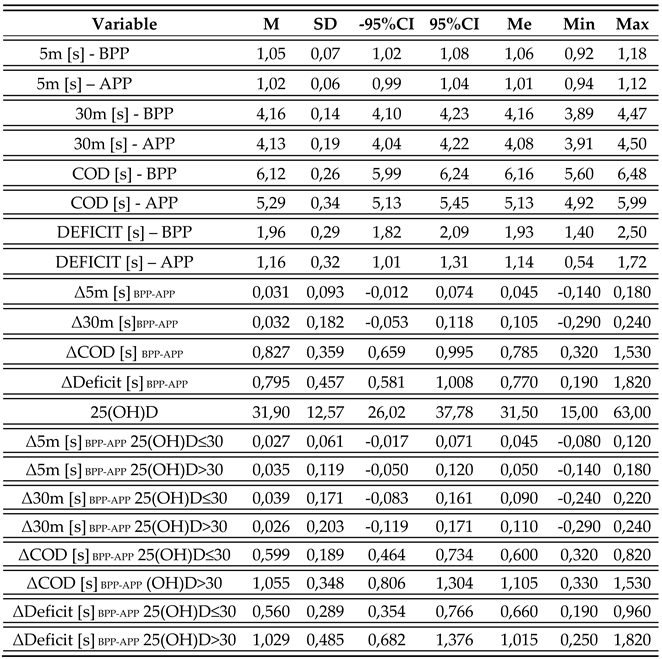
M – mean, SD – standard deviation, 95%CI – confidence interval, Me – median, BPP- before the preparation period of the summer season, APP- after the preparation period of the summer season.
Table 2.
Pearson’s correlation. 25(OH)D & dependent variables.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



